Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Background: Mitral valve transcatheter edge-to-edge repair (TEER) is a widely adopted therapeutic approach for managing significant mitral regurgitation (MR) in high-risk surgical candidates. While procedural safety and efficacy have been demonstrated, the impact of institutional expertise on outcomes remains unclear. We aimed at evaluating whether institutional monthly volume of TEER influences short- and long-term clinical results. Methods: This analysis from the multicenter, prospective GIOTTO trial study evaluated the impact of institutional monthly volume on outcomes of TEER for significant mitral regurgitation. Centers were stratified into tertiles based on monthly volumes (≤2.0 cases/month, 2.1-3.5 cases/month, >3.5 cases/month), and key clinical, echocardiographic, and procedural outcomes were analyzed. Statistical analysis was based on standard bivariate tests as well as unadjusted and multivariable adjusted Cox models. Results: A total of 2,213 patients were included, stratified into tertiles based on institutional procedural volume: 645 (29.1%) patients in the first tertile, 947 (42.8%) patients in the second tertile, and 621 (28.1%) patients in the third tertile. Several baseline differences were found, with some features disfavoring less busy centers (eg functional class and surgical risk, both p< 0.05), and others suggesting a worse risk profile in those treated in busier institutions (eg frailty and history of prior mitral valve intervention, both p< 0.05). Procedural success rates were higher in busier centers (p< 0.001), and hospital stay was also shorter there (p< 0.001). Long-term follow-up (median 14 months) suggested worse outcomes in patients treated in less busy centers at unadjusted analysis (eg p=0.018 for death, p=0.015 for cardiac death, p=0.014 for death or hospitalization for heart failure, p< 0.001 for cardiac death or hospitalization for heart failure), even if these associations proved no longer significant after multivariable adjustment, except for cardiac death or hospitalization for heart failure, which appeared significantly less common in the busiest centers (p< 0.05). Similar trends were observed when focusing on tertiles of overall center volume and when comparing for each center the first 50 cases with the following ones. Conclusion: High institutional monthly volume in TEER mitral valve repair appears to correlate with improved procedural success rate and shorter hospitalizations. Similarly favorable results were found for long-term rates of cardiac death or hospitalization for heart failure. These findings inform on the importance of operator experience and center expertise to achieve state-of-the-art results with TEER, while confirming the usefulness of the proctoring approach when naïve centers begin a TEER program.
Keywords:
caseload
; experience
; mitral regurgitation
; mitraclip
; volume
Introduction
Transcatheter edge-to-edge repair (TEER) has emerged as an effective alternative to surgical valve repair in high-risk patients, and to conservative medical therapy only in carefully selected individuals considered unfit for surgery.(1-2) Indeed, given its ability to improve functional outcomes and reduce heart failure hospitalizations, TEER is increasingly performed worldwide.(3) However, the early and long-term effectiveness of TEER is impacted by several factors, ranging from patient to anatomic and procedural ones.(4-13)
On top of patient, procedural and operator features, institutional characteristics have been the focus of attentive recommendations and analysis.(14) Indeed, in most settings TEER is only provided as long as surgical mitral valve repair/replacement is also available. Yet, this minimum requirement might be too lenient, as long as expertise in patient screening and selection, procedural efficiency and seamless quality of care are paramount to achieve optimal outcomes with TEER.(15) In particular, a number of cut-offs have been proposed and tested formally in the past, under the key premise that higher volume centers may provide better results, shortly after the procedure as well as subsequently. However, results have been inconsistent so far, with some studies suggesting that no evident cut-off can be envisioned, and others ending up recommending a minimum yearly volume ranging from 8 to 24 cases.(16-18)
We have previously leveraged the extensive and detailed dataset of the ongoing prospective GIOTTO (GIse registry Of Transcatheter treatment of mitral valve regurgitaTiOn) registry, an Italian multicenter observational study including patients undergoing TEER with MitraClip (Abbott Vascular, Santa Clara, CA, USA), for inferential purposes.(5,19-20) We hereby aimed at conducting an analysis explicitly dedicated to investigate the impact of institutional TEER volume on clinical outcomes in patients undergoing transcatheter mitral valve repair with the MitraClip device. Key strengths of GIOTTO include its contemporary stance and follow-up which goes well beyond discharge. The key underlying hypothesis of this study was that higher volume/time centers could provide better care for patients undergoing TEER than institutions characterized by fewer procedures over time.
Methods
This study was based on the dataset accrued in the GIOTTO trial, which is sponsored by the Italian Society of Invasive Cardiology (GISE - Società Italiana di Cardiologia Interventistica, Milan, Italy) and is registered online in ClinicalTrials.gov (NCT03521921).(5) Notably, ethical approval was obtained from all participating institutions, and all patients provided written informed consent.
For the purpose of this analysis, which we labelled GIOTTO-VAT (Volume And Time), we mainly focused on comparing tertiles of cases per month, center-wise, with the first tertile up to 2.0 cases per month, the second tertile with more than 2.0 and up to 3.5 cases per month, and the third tertile with more than 3.5 cases per month. Exploratory analyses were conducted according to tertiles of total volume, center-wise, with the first tertile up to 100 cases, the second tertile with more than 100 and up to 200 cases, and the third tertile with more than 200 cases, as well as distinguishing between the first 50 cases per center and the subsequent ones.
Details on baseline variables were collected, including demographic data, comorbidities, functional class, prior cardiac procedures, and medication history. Echocardiographic parameters being assessed included left atrial diameter, left ventricular dimensions, mitral valve gradient, and severity of tricuspid regurgitation. Procedural variables of interest included number and generation of MitraClip devices implanted, fluoroscopy time, device time, and procedural success. Fatal and non-fatal outcomes occurring during the index hospitalization and during follow-up were systematically collected, with specific attention to the following events: death, cardiac death, the composite of death or hospitalization, and the composite of death or hospitalization for heart failure
Descriptive statistics were computed for all variables, with medians, 1st and 3rd quartiles provided for continuous variables and counts and percentages for categorical variables. Bivariate analysis was based on Kruskal-Wallis tests for continuous variables and Fisher exact tests for categorical variables. Censored outcomes were analyzed with Cox proportional hazard models, unadjusted as well as adjusted for potential confounders. No missing data imputation was performed. Statistical significance was set at a 2-tailed p-value of 0.05, without multiplicity adjustments, and all analyses were conducted using Stata 18 (StataCorp, College Station, TX, USA).
Results
A total of 2,213 patients were included, with 645 (29.1%) individuals treated in centers performing ≤2.0 cases/month, 947 (42.8%) treated in institutions reporting between 2.1 and 3.5 cases/month, 621 (28.1%) patients treated in hospitals with >3.5 cases/month (Table 1). Several differences according to such stratifications were found in key baseline features, with some suggesting a higher complexity in patients treated in lower volume centers, such as age, functional class, and surgical risk score (all p<0.05), and others suggesting a higher risk in those treated in busier centers, such as smoking, dyslipidemia, prior mitral valve intervention, prior stroke, peripheral artery disease, and frailty score (all p<0.05).
Other significant differences were found for left ventricular dimensions and function, and mitral valve tenting area (Table 2), disfavoring less busy centers (all p<0.05), and for left atrial dimensions, mitral valve calcification, mitral valve prolapse, tricuspid regurgitation severity, concomitant ECG abnormalities, and prevalence of atrial fibrillation, disfavoring higher volume institutions (all p<0.05).
In terms of procedural details, significant differences were found in rates of implantation of multiple MitraClips, type of MitraClips used, device time, and fluoroscopy time (all p<0.05; Table 3). Notably, device success rates were similar across tertiles, but procedural success marginally albeit significantly higher in busier centers (p<0.001), with concomitantly lower rates of severe residual mitral regurgitation (p=0.001). Patients in high-volume centers experienced fewer in-hospital bleeding events (p=0.006) but more vascular complications (p=0.008), without significant differences in in-hospital mortality (p=0.123). Length of hospital stay was significantly shorter in higher-volume centers (p<0.001).
During a median follow-up of 14 months, details on a total of 539 (24.4%) deaths, 286 (12.9%) cardiac deaths, 685 (31.0%) deaths or hospitalizations, and 359 (16.2%) cardiac deaths or hospitalizations for heart failure were accrued (Table 4). Moderate or severe mitral regurgitation was reported overall in 308 (14.3%). Survival analysis was performed using first unadjusted models (Table 5), and these suggested worse outcomes in less busy centers for death, cardiac death, the composite of death or hospitalization, and the composite of cardiac death or hospitalization for heart failure (all p<0.05). However, after taking into account potential confounders, all these differences were no longer significant, except for cardiac death or hospitalization for heart failure, which appeared significantly less common in busiest centers (all p<0.05; Figure 1).
Similar trends were observed when leveraging tertiles of overall center volume and when comparing for each center the first 50 cases with the following ones (Tables S1–S4), with higher procedural success rates in busier/more experienced centers, and similarly trends favoring them for long-term clinical outcomes.
Discussion
High institutional monthly volume in TEER mitral valve repair appear to correlate with improved procedural success rate and shorter hospitalizations. Similarly favorable results were found for long-term rates of cardiac death or hospitalization for heart failure.
The evidence base appraising the impact of institutional volume and expertise on TEER outcomes is complex and heterogeneous, but some studies have indeed suggested that some thresholds are important to achieve satisfactory procedural, in-hospital and mid-term outcomes (Table S5) (12,14,16-18,21). The findings from the present GIOTTO-VAT study support the concept that institutional volume in TEER may significantly impact on clinical outcomes. Notably, centers with higher monthly case volumes demonstrated greater procedural success. Furthermore, similarly favorable results were evident for long-term outcomes at unadjusted and adjusted analysis. These results align with existing evidence in the field of structural heart interventions, where operator and institutional experience have been shown to positively impact clinical outcomes.(12-13)
Interestingly, while higher-volume centers showed better procedural metrics, long-term clinical outcomes, including mortality, were comparable across tertiles. This suggests that while experience improves technical execution and immediate safety, patient selection and underlying clinical conditions remain key determinants of long-term prognosis. Moreover, the impact of experienced proctors affiliated at high volume centers providing careful guidance to lower volume institutions cannot be discounted, in person or remotely.(22) Indeed, the impact of proctors should be carefully appraised in future studies, together with detailed analyses on post-procedural care and management protocols.
A notable finding was the reduced hospitalization duration in high-volume centers compared to lower-volume ones. This may reflect more efficient perioperative management, shorter procedural times, and faster post-operative recovery.(23) Shorter hospital stays can also reduce healthcare costs, which is a significant consideration in the growing adoption of TEER for mitral regurgitation management, thus reinforcing the call for established expertise in all phases of management of patients with significant mitral regurgitation.(24)
Despite some clear hints that higher volumes over time are associated with better outcomes in patients undergoing TEER for significant mitral regurgitation, results were not altogether consistent. In addition, even adjusted analyses cannot be considered devoid of risk of residual confounding. Furthermore, the risk of duplicity and type I error inflation due to a plethora of statistical tests remains substantial, and thus external replication of the present findings is paramount.
In conclusion, the present GIOTTO-VAT study suggests that hospitals with a higher volume of cases over time may yield improved procedural success rates, with ensuing shorter hospitalizations. Long-term rates of cardiac death or hospitalization for heart failure also favored centers with higher case/month figures. These findings inform on the importance of operator experience and center expertise to achieve state-of-the-art results with TEER, while confirming the usefulness of the proctoring approach when naïve centers begin a TEER program.
Disclosure
Giuseppe Biondi-Zoccai has consulted for Aleph, Amarin, Balmed, Cardionovum, Crannmedical, Endocore Lab, Eukon, Guidotti, Innovheart, Meditrial, Menarini, Microport, Opsens Medical, Terumo, and Translumina, outside the present work. All other authors report no conflict of interest.
Funding
The GIOTTO (GIse registry Of Transcatheter treatment of mitral valve regurgitaTiOn) registry is sponsored by the Italian Society of Invasive Cardiology, with an unrestricted grant by Abbott Vascular, Santa Clara, CA, USA.
References
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; Loghin, C.; Trento, A.; Skipper, E.R.; Fudge, T.; Letsou, G.V.; Massaro, J.M.; Mauri, L. EVEREST II Investigators. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med 2011, 364, 1395–406. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; Rajagopal, V.; Sarembock, I.J.; Brieke, A.; Marx, S.O.; Cohen, D.J.; Weissman, N.J.; Mack, M.J. COAPT Investigators. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N Engl J Med 2018, 379, 2307–2318. [Google Scholar] [CrossRef]
- Zhou, S.; Egorova, N.; Moskowitz, G.; Giustino, G.; Ailawadi, G.; Acker, M.A.; Gillinov, M.; Moskowitz, A.; Gelijns, A. Trends in MitraClip, mitral valve repair, and mitral valve replacement from 2000 to 2016. J Thorac Cardiovasc Surg 2021, 162, 551–562.e4. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Zhang, W.; Zhang, D.; Ye, G.; Ding, C. Mortality and Clinical Predictors After Percutaneous Mitral Valve Repair for Secondary Mitral Regurgitation: A Systematic Review and Meta-Regression Analysis. Front. Cardiovasc. Med. 2022, 9, 918712. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, F.; Testa, L.; Rubbio, A.P.; Bianchi, G.; Grasso, C.; Scandura, S.; De Marco, F.; Tusa, M.; Denti, P.; Alfieri, O.; et al. Real-World Safety and Efficacy of Transcatheter Mitral Valve Repair With MitraClip: Thirty-Day Results From the Italian Society of Interventional Cardiology (GIse) Registry Of Transcatheter Treatment of Mitral Valve RegurgitaTiOn (GIOTTO). Cardiovasc. Revascularization Med. 2020, 21, 1057–1062. [Google Scholar] [CrossRef]
- Salvatore, T.; Ricci, F.; Dangas, G.D.; Rana, B.S.; Ceriello, L.; Testa, L.; Khanji, M.Y.; Caterino, A.L.; Fiore, C.; Rubbio, A.P.; et al. Selection of the Optimal Candidate to MitraClip for Secondary Mitral Regurgitation: Beyond Mitral Valve Morphology. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef]
- Giordano, A.; Biondi-Zoccai, G.; Finizio, F.; Ferraro, P.; Denti, P.; Rubbio, A.P.; Petronio, A.S.; Bartorelli, A.L.; Mongiardo, A.; De Felice, F.; et al. Characteristics and outcomes of MitraClip in octogenarians: Evidence from 1853 patients in the GIOTTO registry. Int. J. Cardiol. 2021, 342, 65–71. [Google Scholar] [CrossRef]
- Giordano, A.; Ferraro, P.; Finizio, F.; Biondi-Zoccai, G.; Denti, P.; Bedogni, F.; Rubbio, A.P.; Petronio, A.S.; Bartorelli, A.L.; Mongiardo, A.; Giordano, S.; DEFelice, F.; Adamo, M.; Montorfano, M.; Baldi, C.; Tarantini, G.; Giannini, F.; Ronco, F.; Monteforte, I.; Villa, E.; Ferrario, M.; Fiocca, L.; Castriota, F.; Tamburino, C. Implantation of one, two or multiple MitraClip™ for transcatheter mitral valve repair: insights from a 1824-patient multicenter study. Panminerva Med 2022, 64, 1–8. [Google Scholar] [CrossRef]
- Giordano, A.; Ferraro, P.; Finizio, F.; Cimmino, M.; Albanese, M.; Morello, A.; Biondi-Zoccai, G.; Denti, P.; Rubbio, A.P.; Bedogni, F.; et al. Incidence and Predictors of Cerebrovascular Accidents in Patients Who Underwent Transcatheter Mitral Valve Repair With MitraClip. Am. J. Cardiol. 2024, 228, 24–33. [Google Scholar] [CrossRef]
- Giordano, A.; Ferraro, P.; Finizio, F.; Corcione, N.; Cimmino, M.; Biondi-Zoccai, G.; Denti, P.; Rubbio, A.P.; Petronio, A.S.; Bartorelli, A.L.; et al. Transcatheter Mitral Valve Repair With the MitraClip Device for Prior Mitral Valve Repair Failure: Insights From the GIOTTO-FAILS Study. J. Am. Hear. Assoc. 2024, 13, e033605. [Google Scholar] [CrossRef]
- Giordano, A.; Pepe, M.; Biondi-Zoccai, G.; Corcione, N.; Finizio, F.; Ferraro, P.; Denti, P.; Popolo Rubbio, A.; Petronio, S.; Bartorelli, A.L.; Nestola, P.L.; Mongiardo, A.; DEFelice, F.; Adamo, M.; Montorfano, M.; Baldi, C.; Tarantini, G.; Giannini, F.; Ronco, F.; Monteforte, I.; Villa, E.; Ferrario Ormezzano, M.; Fiocca, L.; Castriota, F.; Bedogni, F.; Tamburino, C. Impact of coronary artery disease on outcome after transcatheter edge-to-edge mitral valve repair with the MitraClip system. Panminerva Med 2023, 65, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Chhatriwalla, A.K.; Vemulapalli, S.; Holmes DRJr Dai, D.; Li, Z.; Ailawadi, G.; Glower, D.; Kar, S.; Mack, M.J.; Rymer, J.; Kosinski, A.S.; Sorajja, P. Institutional Experience With Transcatheter Mitral Valve Repair and Clinical Outcomes: Insights From the TVT Registry. JACC Cardiovasc Interv 2019, 12, 1342–1352. [Google Scholar] [CrossRef]
- Chhatriwalla, A.K.; Vemulapalli, S.; Szerlip, M.; Kodali, S.; Hahn, R.T.; Saxon, J.T.; Mack, M.J.; Ailawadi, G.; Rymer, J.; Manandhar, P.; et al. Operator Experience and Outcomes of Transcatheter Mitral Valve Repair in the United States. Circ. 2019, 74, 2955–2965. [Google Scholar] [CrossRef]
- Bonow, R.O.; O'Gara, P.T.; Adams, D.H.; Badhwar, V.; Bavaria, J.E.; Elmariah, S.; Hung, J.W.; Lindenfeld, J.; Morris, A.; Satpathy, R.; et al. Multisociety expert consensus systems of care document 2019 AATS/ACC/SCAI/STS expert consensus systems of care document: Operator and institutional recommendations and requirements for transcatheter mitral valve intervention: A Joint Report of the American Association for Thoracic Surgery, the American College of Cardiology, the Society for Cardiovascular Angiography and Interventions, and The Society of Thoracic Surgeons. Catheter. Cardiovasc. Interv. 2019, 95, 866–884. [Google Scholar] [CrossRef]
- Basso, C.; Musumeci, G.; Saia, F.; Tarantini, F. Percutaneous approaches to mitral valve disease. Torino, 2019: Minerva Medica.
- Kolte, D.; Butala, N.M.; Kennedy, K.F.; Wasfy, J.H.; Jena, A.B.; Sakhuja, R.; Langer, N.; Melnitchouk, S.; Sundt, T.M., 3rd; Passeri, J.J.; Palacios, I.F.; Inglessis, I.; Elmariah, S. Association Between Hospital Cardiovascular Procedural Volumes and Transcatheter Mitral Valve Repair Outcomes. Cardiovasc Revasc Med 2022, 36, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Keller, K.; Hobohm, L.; Schmidtmann, I.; Münzel, T.; Baldus, S.; von Bardeleben, R.S. Centre procedural volume and adverse in-hospital outcomes in patients undergoing percutaneous transvenous edge-to-edge mitral valve repair using MitraClip® in Germany. Eur. J. Hear. Fail. 2021, 23, 1380–1389. [Google Scholar] [CrossRef]
- Shoji, S.; Kuno, T.; Malik, A.; Briasoulis, A.; Inohara, T.; Kampaktsis, P.N.; Kohsaka, S.; Latib, A. Association between institutional volume of transcatheter mitral valve repair and readmission rates: A report from the Nationwide Readmission Database. Int. J. Cardiol. 2023, 383, 70–74. [Google Scholar] [CrossRef]
- Corcione, N.; Ferraro, P.; Finizio, F.; Cimmino, M.; Albanese, M.; Morello, A.; Biondi-Zoccai, G.; Denti, P.; Rubbio, A.P.; Bedogni, F.; et al. Overall impact of tethering and of its symmetric and asymmetric subtypes on early and long-term outcome of transcatheter edge-to-edge repair of significant mitral valve regurgitation. Int. J. Cardiol. 2024, 421, 132874. [Google Scholar] [CrossRef]
- Corcione, N.; Ferraro, P.; Morello, A.; Cimmino, M.; Albanese, M.; Avellino, R.; Turino, S.; Polimeno, M.; Messina, S.; Maresca, G.; et al. A 25-year-long journey into interventional cardiology: looking back, and rushing forward. Minerva Medica 2024. [Google Scholar] [CrossRef]
- Bansal, K.; Pawar, S.; Gupta, T.; Gilani, F.; Khera, S.; Kolte, D. Association Between Hospital Volume and 30-Day Readmissions After Transcatheter Mitral Valve Edge-to-Edge Repair. Am. J. Cardiol. 2023, 203, 149–156. [Google Scholar] [CrossRef]
- Ascione, G.; Rossini, G.; Schiavi, D.; Guicciardi, N.A.; Saccocci, M.; Buzzatti, N.; Godino, C.; Alfieri, O.; Agricola, E.; Maisano, F.; et al. Remote proctoring during structural heart procedures: Toward a widespread diffusion of knowledge using mixed reality. Catheter. Cardiovasc. Interv. 2024, 104, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Nita, N.; Schneider, L.; Dahme, T.; Markovic, S.; Keßler, M.; Rottbauer, W.; Tadic, M. Trends in Transcatheter Edge-to-Edge Mitral Valve Repair Over a Decade: Data From the MiTra ULM Registry. Front. Cardiovasc. Med. 2022, 9, 850356. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W. Volume-Outcome Relationships for Transcatheter Mitral Valve Repair: More Is Better. JACC Cardiovasc Interv 2019, 12, 1353–1355. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hazard ratios (95% confidence intervals) at unadjusted and adjusted Cox proportional hazard analysis comparing different tertiles (T) of monthly volume, center-wise. HF=heart failure; Hosp=hospitalization.
Figure 1.
Hazard ratios (95% confidence intervals) at unadjusted and adjusted Cox proportional hazard analysis comparing different tertiles (T) of monthly volume, center-wise. HF=heart failure; Hosp=hospitalization.
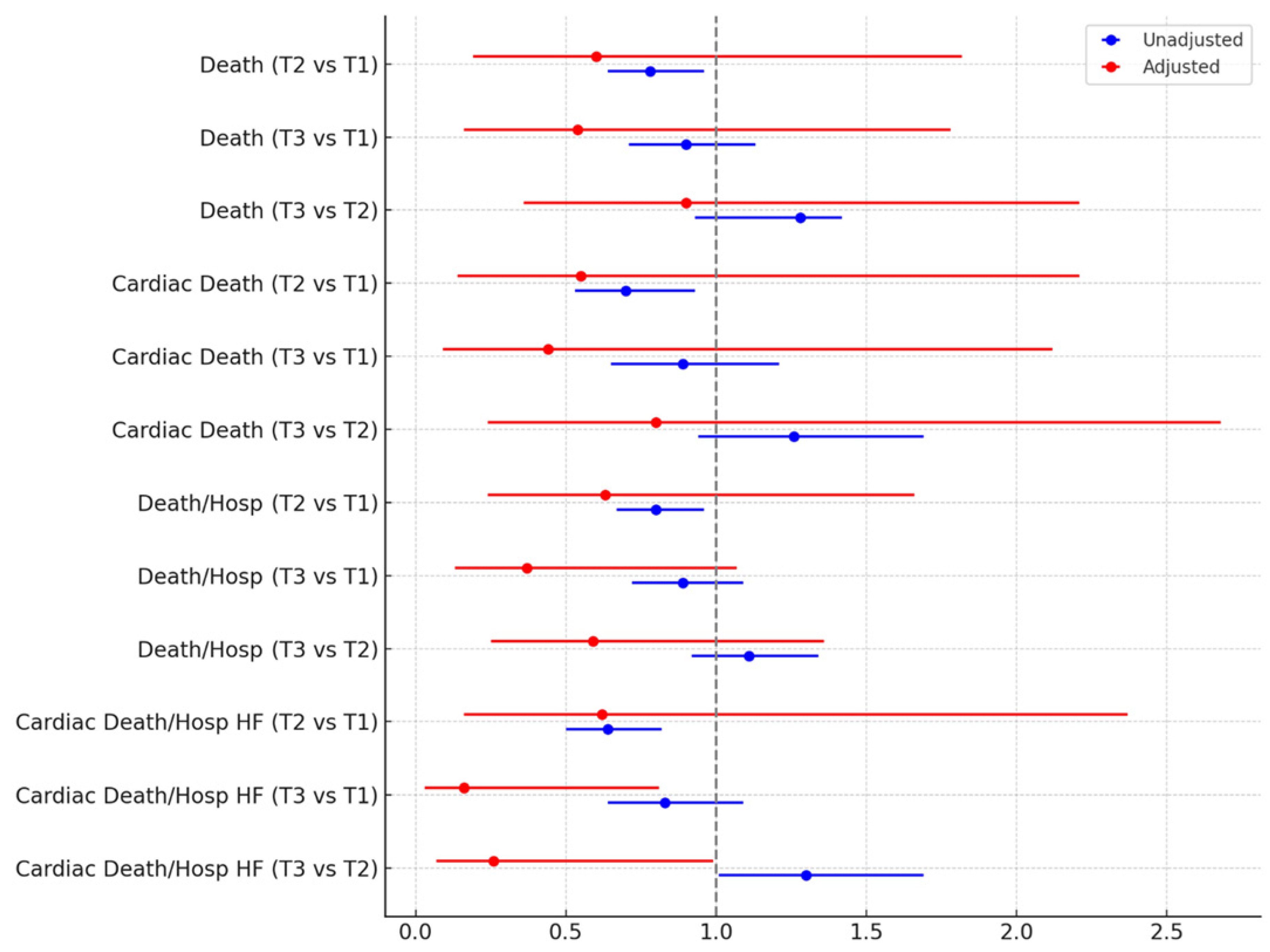

Table 1.
Baseline clinical features according to tertiles of monthly volume, center-wise.*.
| Feature | First tertile | Second tertile | Third tertile | P |
|---|---|---|---|---|
| Patients | 645 | 947 | 621 | - |
| Age (years) | 78 (72; 83) | 77 (70; 82) | 79 (70; 83) | <0.001 |
| Female gender | 211 (32.7%) | 586 (61.9%) | 380 (61.2%) | 0.039 |
| Body mass index | 24.9 (22.7; 27.6) | 24.8 (22.1; 27.8) | 23.4 (2.0; 25.6) | 0.356 |
| Smoking history | 72 (11.1%) | 88 (9.3%) | 163 (26.3%) | <0.001 |
| Hypertension | 462 (71.6%) | 696 (73.5%) | 445 (71.7%) | 0.628 |
| Dyslipidemia | 212 (32.9%) | 256 (27.0%) | 267 (43.0%) | <0.001 |
| Diabetes mellitus | 157 (24.3%) | 220 (23.2%) | 144 (23.2%) | 0.851 |
| Diagnosis | 0.002 | |||
| Degenerative MR | 176 (27.3%) | 330 (34.9%) | 198 (31.9%) | |
| Functional dilated MR | 199 (30.9%) | 277 (29.3%) | 180 (29.0%) | |
| Functional ischemic MR | 194 (30.1%) | 230 (24.3%) | 194 (31.2%) | |
| Mixed etiology | 76 (11.8%) | 110 (11.6%) | 49 (7.9%) | |
| New York Association class | <0.001 | |||
| I | 4 (0.6%) | 11 (1.2%) | 17 (2.8%) | |
| II | 110 (17.1%) | 215 (22.7%) | 196 (31.9%) | |
| III | 452 (70.1%) | 660 (69.7%) | 350 (57.0%) | |
| IV | 79 (12.3%) | 61 (6.4%) | 51 (8.3%) | |
| Coronary artery disease | 0.711 | |||
| None | 201 (63.8%) | 134 (60.1%) | 275 (64.0%) | |
| Single vessel disease | 49 (15.6%) | 42 (18.8%) | 67 (15.6%) | |
| Two vessel disease | 25 (7.9%) | 23 (10.3%) | 48 (11.2%) | |
| Three vessel disease | 22 (7.0%) | 13 (5.8%) | 22 (5.1%) | |
| Left main disease | 18 (5.7%) | 11 (4.9%) | 18 (4.2%) | |
| Prior pacemaker implantation | ||||
| Prior myocardial infarction | 213 (33.0%) | 312 (33.0%) | 194 (31.2%) | 0.735 |
| Prior coronary artery bypass grafting | 83 (12.9%) | 126 (13.3%) | 104 (16.8%) | 0.087 |
| Prior mitral valve intervention | 17 (2.6%) | 14 (1.5%) | 38 (6.1%) | <0.001 |
| Prior cerebrovascular event | <0.001 | |||
| None | 601 (93.2%) | 891 (94.1%) | 548 (88.2%) | |
| Transient ischemic attack | 12 (1.9%) | 14 (1.5%) | 31 (5.0%) | |
| Minor stroke | 17 (2.6%) | 22 (2.3%) | 12 (1.9%) | |
| Major stroke | 15 (2.3%) | 20 (2.1%) | 30 (4.8%) | |
| Peripheral artery disease | 54 (8.4%) | 38 (4.0%) | 74 (11.9%) | <0.001 |
| Frailty | 116 (18.0%) | 118 (12.5%) | 418 (67.3%) | <0.001 |
| Dialysis | 15 (2.3%) | 18 (1.9%) | 9 (1.5%) | 0.521 |
| Logistic EuroSCORE | 10.5 (6.5; 16.4) | 10.4 (6.2; 19.5) | 3.9 (3.4; 4.5) | 0.007 |
| CHADS2 score | 2 (2; 3) | 2 (2; 3) | 2 (1; 3) | 0.004 |
| CHADS2Vasc score | 4 (3; 5) | 4 (3; 5) | 4 (3; 4) | 0.443 |
*descriptive statistics are based on count (%) or median (1st quartile; 3rd quartile), whereas inferential statistics are based on Fisher exact or Kruskal-Wallis tests; MR=mitral regurgitation.
Table 2.
Baseline imaging and ECG features according to tertiles of monthly volume, center-wise.*.
| Feature | First tertile | Second tertile | Third tertile | P |
|---|---|---|---|---|
| Patients | 645 | 947 | 621 | - |
| LA AP diameter (mm) | 45 (40; 50) | 49 (44; 55) | 49 (45; 55) | 0.089 |
| LV EDD (mm) | 61 (54; 68) | 58 (52; 64) | 58 (50; 65) | <0.001 |
| LV ESD (mm) | 49 (38; 56) | 41 (33; 51) | 45 (35; 54) | <0.001 |
| LV EDV (mL) | 164 (120; 212) | 137 (105; 181) | 140 (100; 189) | <0.001 |
| LV ESV (mL) | 97 (55; 146) | 73 (48; 116) | 81 (47; 130) | <0.001 |
| LVEF (%) | 38 (30; 55) | 42 (31; 55) | 40 (30; 57) | 0.008 |
| Tenting area (cm2) | 3.0 (2.2; 3.7) | 2.3 (1.6; 3.0) | 1.9 (1.3; 2.4) | <0.001 |
| Mean mitral valve gradient (mm Hg) | 2 (1; 3) | 2 (1; 2) | 2 (2; 3) | 0.148 |
| Severe mitral regurgitation | 495 (76.7%) | 739 (78.0%) | 493 (79.4%) | 0.525 |
| Severe mitral calcification | 22 (3.4%) | 28 (3.0%) | 55 (8.9%) | <0.001 |
| Mitral valve prolapse | 163 (25.3%) | 262 (27.7%) | 205 (33.0%) | 0.007 |
| Flail leaflet | 132 (20.5%) | 176 (18.6%) | 146 (23.5%) | 0.063 |
| Tricuspid regurgitation | <0.001 | |||
| None or trace | 23 (3.6%) | 62 (6.6%) | 22 (3.5%) | |
| Mild | 282 (43.7%) | 324 (34.2%) | 234 (37.7%) | |
| Moderate | 273 (42.3%) | 458 (48.4%) | 239 (38.5%) | |
| Severe | 67 (10.4%) | 103 (10.9%) | 126 (20.3%) | |
| Systolic pulmonary artery pressure (mm Hg) | 46 (40; 55) | 45 (37; 55) | 45 (35; 55) | 0.071 |
| Any ECG abnormality | 152 (23.6%) | 163 (17.2%) | 296 (47.7%) | <0.001 |
| Second-degree atrioventricular block | 1 (0.2%) | 0 | 3 (0.5%) | 0.039 |
| Third-degree atrioventricular block | 1 (0.2%) | 4 (0.4%) | 2 (0.3%) | 0.806 |
| Right bundle branch block | 17 (2.6%) | 20 (2.1%) | 18 (2.9%) | 0.577 |
| Left bundle branch block | 27 (4.2%) | 27 (2.9%) | 28 (4.5%) | 0.165 |
| Atrial fibrillation | 111 (17.2%) | 118 (12.5%) | 248 (39.9%) | <0.001 |
| Coronary angiography performed | 315 (48.8%) | 223 (23.6%) | 430 (69.2%) | <0.001 |
| Coronary artery disease | 0.711 | |||
| No | 201 (63.8%) | 134 (60.1%) | 275 (64.0%) | |
| 1-vessel disease | 49 (15.6%) | 42 (18.8%) | 67 (15.6%) | |
| 2-vessel disease | 25 (7.9%) | 23 (10.3%) | 48 (11.2%) | |
| 3-vessel disease | 22 (7.0%) | 13 (5.8%) | 22 (5.1%) | |
| Left main disease | 18 (5.7%) | 11 (4.9%) | 18 (4.2%) |
*descriptive statistics are based on count (%) or median (1st quartile; 3rd quartile), whereas inferential statistics are based on Fisher exact or Kruskal-Wallis tests; AP=antero-posterior; EDD=end-diastolic diameter; EDV=end-diastolic volume; ESD=end-systolic diameter; ESV=end-systolic volume; LA=left atrium; LV=left ventricle; LVEF=left ventricular ejection fraction.
Table 3.
Procedural and in-hospital outcomes according to tertiles of monthly volume, center-wise.
| Outcome | First tertile | Second tertile | Third tertile | P |
|---|---|---|---|---|
| Patients | 645 | 947 | 621 | |
| Implantation of ≥2 MitraClip devices | 421 (65.3%) | 508 (53.6%) | 377 (60.7%) | <0.001 |
| Implantation on NT device | 433 (67.1%) | 499 (52.7%) | 308 (49.6%) | <0.001 |
| Implantation on NTr device | 98 (15.2%) | 178 (18.8%) | 92 (14.8%) | 0.062 |
| Implantation of XTr device | 160 (24.8%) | 358 (37.8%) | 249 (40.1%) | <0.001 |
| Device time (minutes) | 2.3 (1.5; 3.5) | 2.1 (1.5; 2.7) | 3.5 (2.1; 4.4) | <0.001 |
| Fluoroscopy time (minutes) | 0.8 (0.6; 1.7) | 1.3 (0.8; 1.9) | 0.4 (0.2; 0.8) | <0.001 |
| Device success | 641 (99.4%) | 942 (99.5%) | 620 (99.8%) | 0.513 |
| Procedural success | 600 (93.0%) | 926 (97.8%) | 593 (95.5%) | <0.001 |
| Procedural death | 3 (0.5%) | 0 | 2 (03%) | 0.104 |
| Mitral valve gradient at end of procedure | 3 (2; 4) | 3 (2; 4) | 3 (3; 5) | <0.001 |
| Mitral regurgitation at end of procedure | <0.001 | |||
| None | 386 (59.8%) | 561 (59.2%) | 453 (73.0%) | |
| Mild | 209 (32.4%) | 348 (36.8%) | 147 (23.7%) | |
| Moderate | 34 (5.3%) | 26 (2.8%) | 12 (1.9%) | |
| Severe | 16 (2.5%) | 12 (1.3%) | 9 (1.5%) | |
| Inhospital death | 18 (2.8%) | 20 (2.1%) | 24 (3.9%) | 0.123 |
| Inhospital stroke | 0 | 0 | 0 | - |
| Inhospital bleeding | 0.006 | |||
| None | 644 (99.8%) | 939 (99.2%) | 610 (98.2%) | |
| Minor | 0 | 5 (0.5%) | 7 (1.1%) | |
| Major | 0 | 1 (0.1%) | 4 (0.6%) | |
| Disabling | 1 (0.2%) | 2 (0.2%) | 0 | |
| Inhospital vascular complication | 1 (0.2%) | 5 (0.5%) | 10 (1.6%) | 0.008 |
| Days of hospitalization | 8 (5; 12) | 5 (4; 8) | 5 (4; 8) | <0.001 |
| Mitral regurgitation at discharge | 0.001 | |||
| None | 347 (55.3%) | 503 (54.3%) | 388 (65.0%) | |
| Mild | 226 (36.0%) | 354 (38.2%) | 171 (28.6%) | |
| Moderate | 39 (6.2%) | 59 (6.4%) | 27 (4.5%) | |
| Severe | 15 (2.4%) | 11 (1.2%) | 11 (1.0%) | |
| Systolic pulmonary artery pressure (mm Hg) | 40 (32; 46) | 40 (35; 50) | 40 (30; 45) | <0.001 |
Table 4.
Cumulative outcomes at follow-up according to tertiles of monthly volume, center-wise.
| Outcome | First tertile | Second tertile | Third tertile | P |
|---|---|---|---|---|
| Patients | 645 | 947 | 621 | |
| Follow-up (months) | 12 (1; 24) | 21 (10; 36) | 13 (1; 25) | <0.001 |
| Death | 152 (23.6%) | 251 (26.5%) | 136 (21.9%) | 0.101 |
| Cardiac death | 86 (13.3%) | 125 (13.2%) | 75 (12.1%) | 0.764 |
| Hospitalization | 107 (16.6%) | 114 (12.0%) | 68 (11.0%) | 0.007 |
| Hospitalization for heart failure | 82 (12.7%) | 86 (9.1%) | 65 (10.5%) | 0.070 |
| Death or hospitalization | 199 (30.1%) | 307 (32.4%) | 179 (28.8%) | 0.323 |
| Cardiac death or hospitalization for heart failure | 142 (22.0%) | 189 (20.0%) | 127 (20.5%) | 0.596 |
| Mitral valve surgery | 4 (0.6%) | 8 (0.8%) | 13 (2.1%) | 0.034 |
| Cerebrovascular accident | 12 (1.9%) | 13 (1.4%) | 9 (1.5%) | 0.722 |
| New York Heart Association | 0.006 | |||
| I | 59 (14.0%) | 159 (21.3%) | 55 (13.3%) | |
| I | 270 (64.0%) | 425 (56.9%) | 254 (61.2%) | |
| III | 85 (20.1%) | 153 (20.5%) | 98 (23.6%) | |
| IV | 8 (1.9%) | 10 (1.3%) | 8 (1.9%) | |
| Atrial fibrillation | 124 (19.2%) | 135 (14.3%) | 258 (41.6%) | <0.001 |
| End-diastolic diameter (mm) | 60 (53; 67) | 57 (50; 64) | 56 (49; 62) | <0.001 |
| End-systolic diameter (mm) | 48 (38; 56) | 40 (31; 50) | 40 (35; 53) | <0.001 |
| End-diastolic volume (mL) | 159 (120; 220) | 131 (100; 180) | 133 (98; 187) | <0.001 |
| End-systolic volume (mL) | 90 (56; 138) | 73 (45; 115) | 85 (45; 130) | 0.004 |
| Left ventricular ejection fraction (%) | 38 (28; 51) | 42 (30; 55) | 38 (27; 52) | <0.001 |
| Mitral valve gradient (mm Hg) | 3 (3; 5) | 4 (3; 5) | 4 (3; 5) | 0.023 |
| Mitral regurgitation | 0.113 | |||
| None | 281 (44.7%) | 433 (46.7%) | 297 (49.8%) | |
| Mild | 250 (39.8%) | 365 (39.4%) | 219 (36.7%) | |
| Moderate | 66 (10.5%) | 103 (11.1%) | 53 (8.9%) | |
| Severe | 32 (5.1%) | 26 (2.8%) | 28 (4.7%) | |
| Angiotensin receptor blockers | 219 (52.4%) | 246 (33.1%) | 85 (22.3%) | <0.001 |
| Calcium channel antagonists | 34 (8.1%) | 77 (10.4%) | 41 (10.8%) | 0.367 |
| Betablockers | 348 (82.7%) | 362 (75.4%) | 299 (78.3%) | 0.015 |
| Ivabradine | 23 (5.5%) | 30 (4.0%) | 18 (4.7%) | 0.495 |
| Furosemide | 393 (92.7%) | 677 (90.6%) | 361 (90.5%) | 0.421 |
| Aspirin | 185 (44.2%) | 318 (42.5%) | 183 (48.3%) | 0.183 |
| Thienopyridines | 64 (15.4%) | 161 (21.6%) | 89 (23.5%) | <0.001 |
| Novel oral anticoagulants | 154 (24.8%) | 262 (28.6%) | 113 (18.7%) | <0.001 |
| Warfarin | 167 (26.9%) | 221 (24.2%) | 148 (24.6%) | 0.455 |
| Intravenous inotropes | 11 (2.6%) | 3 (0.4%) | 6 (1.6%) | 0.003 |
Table 5.
Unadjusted and adjusted survival analysis according to tertiles of monthly volume, center-wise.*.
Table 5.
Unadjusted and adjusted survival analysis according to tertiles of monthly volume, center-wise.*.
| Outcome | Unadjusted effect estimates | Adjusted effect estimates |
|---|---|---|
| Death | ||
| Tertile 2 vs 1 | 0.78 (0.64-0.96), p=0.018 | 0.60 (0.19-1.82), p=0.364 |
| Tertile 3 vs 1 | 0.90 (0.71-1.13), p=0.365 | 0.54 (0.16-1.78), p=0.308 |
| Tertile 3 vs 2 | 1.28 (0.93-1.42), p=0.191 | 0.90 (0.36-2.21), p=0.814 |
| Cardiac death | ||
| Tertile 2 vs 1 | 0.70 (0.53-0.93), p=0.015 | 0.55 (0.14-2.21), p=0.398 |
| Tertile 3 vs 1 | 0.89 (0.65-1.21), p=0.456 | 0.44 (0.09-2.12), p=0.304 |
| Tertile 3 vs 2 | 1.26 (0.94-1.69), p=0.117 | 0.80 (0.24-2.68), p=0.713 |
| Death or hospitalization | ||
| Tertile 2 vs 1 | 0.80 (0.67-0.96), p=0.014 | 0.63 (0.24-1.66), p=0.351 |
| Tertile 3 vs 1 | 0.89 (0.72-1.09), p=0.246 | 0.37 (0.13-1.07), p=0.065 |
| Tertile 3 vs 2 | 1.11 (0.92-1.34), p=0.265 | 0.59 (0.25-1.36), p=0.213 |
| Cardiac death or hospitalization for heart failure | ||
| Tertile 2 vs 1 | 0.64 (0.50-0.82), p<0.001 | 0.62 (0.16-2.37), p=0.488 |
| Tertile 3 vs 1 | 0.83 (0.64-1.09), p<0.001 | 0.16 (0.03-0.81), p=0.026 |
| Tertile 3 vs 2 | 1.30 (1.01-1.69), p=0.045 | 0.26 (0.07-0.99), p=0.048 |
*reported as hazard ratio (95% confidence interval), p value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



