Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by obstructive airflow limitation. It is the fourth leading cause of death worldwide, responsible for 3.5 million deaths in 2021. The main symptoms include shortness of breath, cough, sputum production, and wheezing. Beyond its physical impact, COPD also significantly affects mental health, with patients experiencing higher rates of depression compared to the general population. Depression in COPD patients contributes to a lower quality of life, social disability, and an increased risk of suicide. The pathophysiological mechanisms behind depression in COPD are complex and multifactorial, involving chronic inflammation, hypoxemia, oxidative stress, and various risk factors such as smoking, severe dyspnea, poor health-related quality of life (HRQoL), lower educational levels, socio-economic disadvantage, and the presence of non-psychological comorbidities. This review aims to summarize the existing data on the association between COPD and depression, analyze their pathophysiological connections, explore treatment possibilities, and highlight the interrelationships between these conditions.
Keywords:
depression
; COPD
; smoking
; health-related quality of life
; inflammation
; oxidative stress
1. Introduction
COPD is considered one of the primary causes of morbidity and mortality worldwide and at the same time, creating a growing social and economic burden. [1]. The prevalence, morbidity, and mortality of COPD may vary between countries depending on the risk factors populations are exposed to. [2]. According to the World Health Organization (WHO), COPD is the fourth leading cause of death worldwide, causing 3.5 million deaths in 2021, which represent approximately 5% of all global deaths [3]. In addition, according to disability-adjusted life years, COPD is the eighth leading cause of poor health worldwide [3].
It is estimated that 80% of COPD patients are likely to have at least one comorbidity [4]. The relationship between COPD and mental health has recently gained significant research interest due to its impact on quality of life [5]. COPD significantly impacts mental health, pacients experiencing higher rates of depression compared to the general population. According to Atlantis et al., the relative risk of developing depression among COPD patients is 1.69 times higher than in the general population. [6]. The prevalence of depression among patients with stable COPD in primary care settings varies significantly, with a range of 10% to 57% [7]. Among patients with severe COPD (FEV1 <50% predicted), the prevalence of depression was 25.0%, compared to 17.5% in controls and 19.6% in persons with mild to moderate COPD [8].
Quality of life in COPD is significantly impacted by the progressive charactere of the disease. Moreover, depression in subjects with COPD worsens this impact and has been found to have the strongest correlation with self-reported health status and reduced HRQoL[9].
COPD is a chronic condition that typically requires the ongoing use of pharmacotherapy [10,11]. Nonadherence to treatment is a significant issue in COPD, with adherence rates estimated to be below 50% [12]. A meta-analysis has revealed that patients with symptoms of depression are three times more likely to be non-adherent to their prescribed medications [13]. Nonadherence to COPD treatments results in higher hospitalization rates, increased costs, and more frequent emergency department visits [14,15] .
Exacerbations of chronic obstructive pulmonary disease (COPD) represent a significant challenge for worldwide health-care systems; they are a major cause of morbidity, mortality, and reduced health status[16]. A recent study identified depression as an independent factor for acute exacerbations of COPD (AECOPD), associated with a higher risk of readmission for AECOPD (OR 2.06, 95% CI 1.28 - 3.31), regardless of lung function or previous severe exacerbations in the prior year [17].
2. Risk Factors
Several studies have identified risk factors for depression in patients with COPD including smoking, severe dyspnea, poor HRQoL, lower education levels and socio-economic status, as well as association with non-psychological comorbidities [18,19].
2.1. Smoking
Psychiatrists have observed that cigarette smoke seems to have an antidepressant effect [20], potentially providing temporary relief for symptoms of depression. This may explain why studies consistently reported that patients with COPD who also suffer from depression or anxiety are significantly more likely to be smokers [21,22]. The relationship between smoking and depression is, however, bidirectional. Young adults with a history of depression are more likely to start smoking compared with healthy counterparts who have no symptoms of depression. On the other hand, long-term cigarette use has been proven to heighten susceptibility to developing depression due to nicotine-induced changes in neurophysiology, including disruptions in neurotransmitter systems essential for mood regulation [23,24]. In addition, the prevalence of depression and anxiety tends to rise with the increasing duration of smoking (in years) and the number of cigarette pack-years [25].
Depression as a comorbidity has been shown to have a statistically significant relationship with patients’ HRQoL and smoking status [26].
2.2. Pulmonary Function
Spirometry is widely regarded as the gold standard
for assessing lung function in patients with chronic lung diseases Several studies
have proven a significant association between reduced
lung function and symptoms of depression in subjects with respiratory disease [27] . Specifically, parameters such as FEV1
(P<0.001), FVC (P<0.001), and the FEV1/FVC ratio (P=0.022) were markedly
lower in the group of subjects diagnosed with depression compared with subjects with no symptoms of depression [28] . Moderate-to-severe symptoms of depression have
actually been proven to have a significant and independent correlation
with the progression of lung function decline in young adults [29] .
2.3. Socio-Economic Factors
Several studies suggest that younger persons with COPD may be more susceptible to depression [18,30,31], possibly as a result of early onset of the disease, which affects their work productivity, social engagement and quality of life. However, other research presents the opposite, that older adults are more vulnerable to depression, possibly due to the cumulative effects of chronic illness and age-related comorbidities [19,32]. A recent study showed that people with higher educational qualifications had a 40% lower risk of experiencing depression than those with less educational background. Additionally, the study reported younger age and a psychological history as significant risk factors for depression in COPD patients [33]. It’s important to recognize that studies exploring the relationship between depression and COPD vary widely, influenced by factors such as sample size, geographic location, and cultural differences [34].
3. Pathogenesis and Pathophysiology
The relationship between COPD and depression can be bidirectional [6], meaning that depression can aggravate the condition of patients suffering from COPD, leading to an increased risk of exacerbation and can indirectly lead to death. The pathophysiologic mechanisms for the development of depression in patients with COPD are complex and include the following: the anxiogenic effects of hyperventilation [35,36,37], misinterpretation of respiratory symptoms [35,38,39,40,41,42], neurobiologic sensitivity to CO2, lactate and other signals of suffocation [35,38,43,44], smoking [45,46,47,48,49,50,51,52,53], hypoxia [54,55,56,57,58] and inflammation [59,60,61,62,63,64,65,66,67,68,69,70].
3.1. The Anxiogenic Effects of Hyperventilation. Misinterpretation of Respiratory Symptoms
Anxiety in COPD patients manifests as dyspnea, sweating, and tachycardia; these symptoms are often linked to fear of dyspnea attacks and death [35,36]. A complex relationship exists between dyspnea, hyperventilation, and anxiety [35], as anxiety increases respiratory rate, worsening dyspnea through shallow breathing [38]. COPD exacerbates this with increased ventilatory load, reduced capacity, and neural respiratory drive [39]. When perceived respiratory effort exceeds a threshold, it triggers emotional reactions, leading to avoidance behaviors that may temporarily reduce anxiety [40,41], but can activate a 'dyspnea-anxiety-dyspnea cycle,' exacerbating breathlessness and impairing quality of life [42].
3.2. Neurobiological Sensitivity to CO2, Lactate, and Other Suffocation Signals in COPD and Depression
Hyperventilation that exceeds the metabolic demands of the body leads to a reduction in CO₂ levels and in consequence, induces respiratory alkalosis. This, in turn, induces vasoconstriction and characteristic symptoms of panic, including feelings of numbness, breathlessness, dizziness, and tingling sensations—symptoms that can occur in healthy persons [38]. In patients with COPD, an increased respiratory rate contributes to dynamic hyperinflation. This hyperinflation, in turn, increases elastic load and the work of breathing and decreases inspiratory reserve capacity, thereby exacerbating dyspnea [43]. In severe cases of COPD, chronic hypoventilation leads to hypercapnia [38]. The resulting elevation in pCO₂ levels stimulates the medullary chemoreceptors, which excites noradrenergic neurons and precipitates a panic response [44]. Furthermore, hypoxia is associated with the generation of lactic acid, which is strongly implicated in the provocation of panic attacks. In addition, patients with COPD and comorbid anxiety are more sensitive to both hyperventilation and lactic acid buildup [35].
3.3. The Role of Nicotine Dependence and Smoking in COPD and Depression
The characteristic symptoms of depression in COPD patients include sleep disturbances, difficulty with concentration, loss of appetite, feelings of hopelessness, functional impairment in daily activities, difficulties with self-management during exacerbations, widespread negativity, and social withdrawal [47,48,49]. In COPD patients, depressive symptomatology is often exacerbated by guilt, stemming from the belief that they are a burden to others or responsible for the onset of their illness [50].
Adolescents with a genetic predisposition for depression or with a history of depressive episodes have an increased risk of developing COPD through nicotine addiction [51,52]. This creates a vicious cycle: depression leads to smoking, and smoking, as a major risk factor, contributes to the development of COPD. In turn, COPD exacerbates depression through various pathophysiological mechanisms [53]. Several studies [71,72], support a strong association between tobacco consumption and mental disorders.
3.4. The Impact of Hypoxia on COPD and Depression
Chronic, subclinical hypoxemia is a common finding in patients with COPD. Low arterial oxygen saturation has been linked to the presence of periventricular white matter lesions [54], which are similarly observed in older adults with depression[55]. Several studies have also indicated a relation between neuropsychologic impairment and persistent hypoxemia, with manifestations that include both cognitive impairments and depressive symptoms [56,57].
Research on sleep apnea has provided key insights into the relationship between hypoxemia and depression, suggesting that intermittent nocturnal hypoxemia is considered a significant cause for developing depressive states [58].
3.5. The Role of Inflammation in COPD and Depression
Various studies have found that pro-inflammatory cytokines, such as IL-6, affect the brain, contributing to depressive symptoms in COPD patients [58]. Elevated IL-6 levels are found in both COPD and depression, with IL-6, IFN-γ, and IL-2 involved in producing symptoms of depression [61].
IL-6 is produced at sites of inflammation and plays a key role in the acute phase response. It amplifies chronic inflammation by stimulating T- and B-cells [62]; therefore high concentrations of IL-6 suggest a relation between depression and COPD. Additionally, IL-6 modulates monocyte and macrophage differentiation [64], which is a key component of the immune system. When activated by pro-inflammatory signals such as IFN-γ or lipopolysaccharides, macrophages release nitric oxide (NO) [64]. Activated macrophages, in addition to producing NO, also secrete neopterin, a molecule that serves as a biomarker for T helper cell activation [65]. Elevated neopterin levels have been consistently identified in both COPD patients [62] and in subjects with depression [66], and thus underline the interconnected nature of chronic inflammation, COPD, and mood disorders. In humans, the administration of IFN-γ has been shown to induce various depression-like symptoms, such as headache, weight loss, fatigue, anorexia, irritability, and difficulties in concentration [73]. Similarly, IL-2 can cross the blood-brain barrier, causing cognitive and motor impairments [74].
Taken together, these findings highlight the significant role of inflammation, particularly mediated by cytokines like IL-2, IL-6, and IFN-γ, in the pathogenesis of both COPD and depression.
3.6. Oxidative Stress
Oxidative stress, resulting from an imbalance between reactive oxygen species (ROS), reactive nitrogen species (RNS), and antioxidant defenses, plays a key role in the pathogenesis of COPD. In the lungs, oxidants damage nucleic acids, lipids, and proteins, trigger redox-cycling reactions, deplete antioxidants (e.g., glutathione), initiate carcinogenesis, and inactivate protease inhibitors such as α1-antitrypsin [75]. Cigarette smoke is a major exogenous oxidant source and significantly contributes to COPD [76,77].
Air pollution, containing nitrogen dioxide (NO₂), ozone, polycyclic aromatic hydrocarbons (PAHs), and endotoxins, also induces oxidative stress and is a significant cause of COPD development [78].
Endogenous oxidant sources include mitochondria, which generate superoxide, a key ROS, along with membrane-bound oxidases like cytochrome P450 [79,80]. Increased plasma lipid peroxidation markers, such as malondialdehyde, and biomarkers like exhaled ethane and 8-isoprostanes, indicate oxidative damage in COPD patients [81,82,83,84,85].
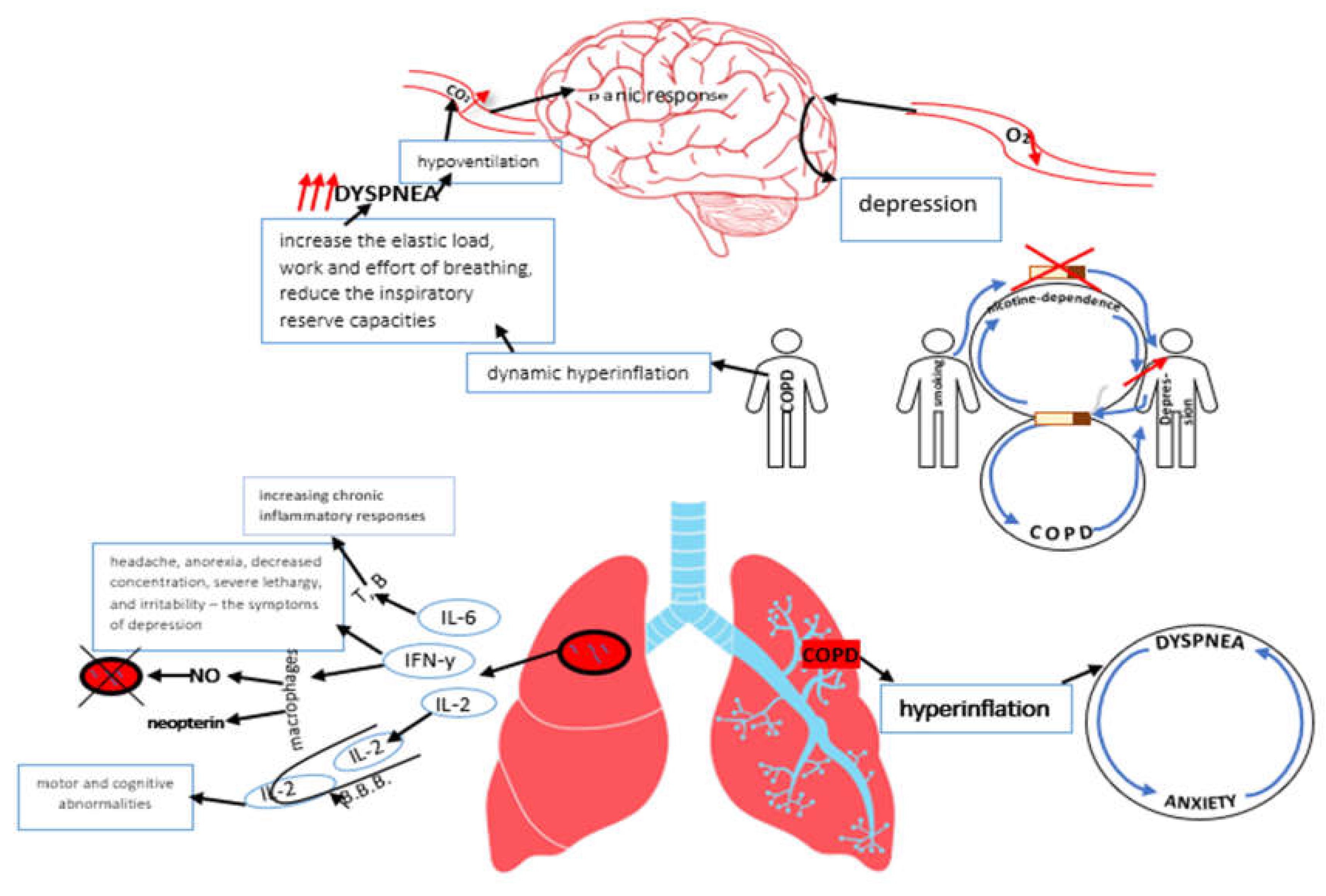
Figure 1.
Pathogenesis and pathophysiology of depression in COPD.
4. Depression and COPD Exacerbations
The progression of COPD is largely influenced by the frequency of exacerbations and the presence of comorbidities, both of which significantly impact the disease course and worsen prognosis [86,87,88]. Depressive symptoms in COPD patients are associated with more frequent severe exacerbations, reduced physical activity, increased dyspnea, and a lower quality of life, suggesting that depression may contribute to faster disease progression [89].
A recent study found a high prevalence of depression in COPD patients with frequent exacerbations, with more severe depressive symptoms observed in advanced disease stages. [90]. The pathophysiological mechanisms involved in the impact of depression on acute AECOPD remain poorly understood [89]. Psychophysiological, behavioral, and psychosocial factors likely contribute to this association. Depression, marked by hopelessness and fear, can reduce self-care, treatment adherence, and increase smoking[91,92] all of which may contribute to AECOPD. Cognitive impairments may also amplify dyspnea perception, raising healthcare utilization and hospitalization risk [89].
5. Depression and COPD in the Elderly
Depression is a common problem for older people. According to reports, 80% of older adults with COPD suffer from depression [93,94]. Older adults with COPD are more likely to experience dyspnea after physical activity, leading to a long-term decline in activity levels, which in turn results in reduced muscle mass and function [95].
Patients with both COPD and comorbid depression tend to have a poorer prognosis, including lower exercise tolerance, greater functional limitations, more frequent acute exacerbations, and an increased risk of mortality compared to those without depression [96].
Depression in patients with COPD was associated with length of hospital stay and increases in both 30- and 60-day hospital readmission rates [97]. Older adults with COPD exhibit a higher prevalence of severe social disengagement (4.5% vs 2.1%; adjusted odds ratio [OR], 0.7; 95% confidence interval [CI], 0.1-4.8) and loneliness (57.7% vs 42.1%; unadjusted OR, 1.9; 95% CI, 1.4-2.5) compared to their counterparts without COPD [98].
6. COPD and Depression: Clinical Differences Between Men and Women
The global prevalence of COPD is estimated at approximately 12%, and its burden continues to rise worldwide [99,100], furthermore, COPD has become the leading cause of death among female smokers [98]. Biological differences between males and females include differences in airway development, inflammatory responses, and susceptibility to inhaled substances such as tobacco smoke [101]. One key distinction is that females tend to have smaller airways relative to lung volume compared to males [102]. This may partially explain why women experience more severe small airway disease than men, even with comparable tobacco smoke exposure [103].
Female sex is a significant risk factor for depression in COPD, along with lower BMI, living alone, smoking, and greater disease severity, particularly in GOLD stage III/IV. Risk factors for depression differ by sex: in males, they include low BMI, low income, living alone, and multiple comorbidities, while in females, they involve lower education, urban living, and smoking [104]. Women with COPD report higher levels of depression and reduced quality of life compared to males [105], even after adjusting for lung function, age, smoking history, and emphysema severity [106]. Additionally, female sex, depression, and anxiety are linked to increased exacerbations and mortality [103].
7. Screening for Depression in COPD
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends the use of the COPD Assessment Test (CAT) for evaluating patients with COPD [107]. Research suggests that the CAT Test may serve as a indicator of major depression in COPD patients with mild hypoxemia [108] . Although various screening tools are available to identify depression— such as the Beck Depression Inventory (second revision), the Center for Epidemiologic Studies Depression Scale (CES-D), the Geriatric Depression Scale (GDS), the Hospital Anxiety and Depression Scale (HADS), and the Patient Health Questionnaire-9 (PHQ-9) [109] , none of these instruments are routinely implemented in primary care practices [110,111].
8. Scales/Scores for Assessment of Depression in COPD
| BDI | GDS | CES-D | HADS | |
| Number of questions/time for evaluation | -21 items -2 past weeks |
-30 items (long version) -15 items (short version) -current/past week |
-20 items [112] (and other versions) -1 past week |
-14 items (7-anxiety-related, 7-depression-related) |
| Are evaluated | patients with somatic, affective, cognitive and vegetative symptoms | normal community-dwelling elderly and elders hospitalized for depression | patients with positive/negative effect, somatic problems, evaluating their activity level | psychiatric and medical patients, including cancer, traumatic brain injury, cardiac, stroke, intellectual disabilities, epilepsy, chronic obstructive pulmonary disease, etc., ages 16–65 years |
| Scale |
*a 4-point scale: 0-means not at all 3-extreme form of each symptom |
*a scale – «yes or no» |
*a 4-point scale: 0-rarely(<1/day) 1-some/little of the time (1-2 days) 2-occasionally or a moderate amount of time (3-4 days) 3-most or all of the time (5-7 days) |
*a 4 point Likert scale, ranging from 0-3 |
| Score interpretation | *minimal range= 0-13 *mild depression= 14-19 *moderate depression= 20-28 *severe depression= 29-63 |
*long form: 0-9-normal, 10-19-mild depression, 20-30-severe depression *short form: >5-suggestive for depression and >10-highly likely depression |
Easily hand scored. The items should be summed to obtain a total score. | *0-7-normal *8-10-mild *11-15-moderate *>=16-severe |
| Time to administer/complete | *self-administration= 5-10 min. *oral administration= 15 min. |
*long version – 5-10 min. *short version – 2-5 min. |
10 minutes | <=5 min. (1-2 min.) |
| Response format | 0-3 rating scale | «yes» or «no» | 4 point Likert scale | *0-3 rating scale |
| Sensitivity to change | *5-point difference=minimally important clinical difference *10-19points =moderate difference *>20 points =large difference [113] |
*the short form shows the sensitivity of 81.3% *the long form shows the sensitivity of 77.4% |
*ranges of 13-21 have been provided for detecting of 80-90% reliable change. | *sensitivity = 56-100 % |
| Restrictions/ limitations | Overlapping symptoms between other medical conditions and depression, cost and reading level | It is valid in younger samples. In needs caution when used with cognitively impaired individuals and severely cognitively impaired individuals | Response format can be difficult in original 20-item instrument, and is a contributing reason for the development of shorter versions | It is better to compare HADS to other measures of depression |
| Ease to use | time to complete – 5-15 min. | self-administered questionnaire | Time to interpret <10 min. Easily self-administered/ administered by interviewer. | self-administered questionnaire |
9. Impact of COPD Medication on Depression and Vice Versa
Managing anxiety and depression in COPD need a multidisciplinary approach. COPD progression impact mental health and targeted strategies such as smoking cessation [114], influenza vaccination [115], oxygen therapy [116], pharmacological interventions [117], surgical procedures for select patients [118], structured exercise programs to condition peripheral muscles[119], and self-management strategies [120] becomes more pronounced.
While COPD medications help relieve symptoms, corticosteroids especially in asthma-COPD overlap [121,122], such as depression, psychosis, mania, anxiety, and delirium [123]. The use of corticosteroids is strongly associated with psychiatric and neurological side effects, with reported rates of depression (40.5%), mania (27.8%), psychosis (13.9%), and delirium (10.1%) [124]. A case study documented severe mania induced by the combined use of prednisone and clarithromycin [125].
Although rare, such effects require careful monitoring. Another study assessed the impact of long-acting beta-agonists (LABAs) and theophylline on suicidal ideation, finding no significant link with LABAs but an increased risk with theophylline, underscoring the need for psychological risk assessment. [126]. Beta-2 adrenergic agonists, such as albuterol, indacaterol, and salmeterol, are known to cause dose-dependent prolongation of the QT interval and potassium depletion. Similarly, serotonin reuptake inhibitors (e.g., escitalopram, citalopram, fluoxetine) and tricyclic antidepressants (e.g., nortriptyline, doxepin) also have the potential to prolong the QT interval. When used together, these medications may increase the risk of ventricular arrhythmias, including torsade de pointes, and could elevate the risk of sudden death[127]. Pulmonary rehabilitation (PR) is a key COPD treatment approved by the American Thoracic Society and the European Respiratory Society [128]. It benefits patients with moderate-to-severe disease, functional limitations, and stable conditions without severe comorbidities [129]. PR improve independence, quality of life, and symptom control [130]. Beyond respiratory benefits, it also reduce depression and cognitive decline [131]. According to its effectiveness, PR should be included in treatment plans for all COPD stages [132,133].
Even with the high prevalence of depression in people with COPD and the impact on quality of life, research on its management remains limited [134]. With the pressing need for effective treatment options, it is essential to consider factors such as the risk of respiratory depression, potential side effects, and possible drug interactions when prescribing antidepressants [135].
Selective serotonin reuptake inhibitors (SSRIs) are considered the first-line treatment for depression in COPD patients, but they inhibit cytochrome P450 enzymes [136], which play a crucial role in the oxidative metabolism of therapeutic substances [137]. The initiation or use of SSRIs, SNRIs, and tricyclic antidepressants (TCAs), whether individually or in combination, has been significantly associated with an elevated risk of pneumonia [138].Particular attention is needed when prescribing tricyclic antidepressants (TCAs) and mirtazapine to COPD patients with hypercapnia [139,140]. Likewise, benzodiazepines can induce respiratory depression, posing a significant risk for COPD patients who retain CO₂ [141]. Frequently, bupropion, a dopaminergic agent, is prescribed for smoking cessation. However, data suggest that dopamine agonists may impair ventilatory responses to hypoxemia and hypercapnia by inhibiting carotid-body chemoreception through dopamine-mediated mechanisms[142]. Medication tolerance should be assessed over 1–3 weeks, with psychiatric referral for suicidal behavior or severe psychiatric comorbidities [143].
10. Future Perspective
Despite the impact of depression on COPD prognosis, clinical guidance on its management is limited. Future research should integrate mental health into COPD management, with regular screening for depression. Long-term efficacy of treatment needs to be assessed in large studies, including personalized pharmacological approaches with fewer side effects. By addressing these gaps, a more comprehensive and patient-centered approach to COPD care can be developed, ultimately improving both physical and mental health outcomes.
11. Conclusions
COPD is a severe and disabling condition with significant complications, one of the most troubling being comorbid depression. While there is substantial evidence supporting the connection between COPD and depression, the exact pathogenetic mechanisms are still not fully understood, and a universal treatment that works for most patients has not yet been established. Although current therapies help many individuals, they still need refinement and further development to enhance their effectiveness. Significant improvements in patient care and global health outcomes can only be achieved by advancing our understanding and treatment of both COPD and depression.
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef] [PubMed]
- Lange, P.; Celli, B.R.; Agustí, A.; Jensen, G.B.; Divo, M.; Faner, R.; Guerra, S.; Marott, J.L.; Martinez, F.D.; Martinez-Camblor, P.; et al. Lung-Function Trajectories Leading to Chronic Obstructive Pulmonary Disease. New Engl. J. Med. 2015, 373, 111–122. [Google Scholar] [CrossRef] [PubMed]
- WHO. Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease- (accessed on day month year).
- Corlateanu, A.; Covantev, S.; Mathioudakis, A.G.; Botnaru, V.; Siafakas, N. Prevalence and burden of comorbidities in Chronic Obstructive Pulmonary Disease. Respir. Investig. 2016, 54, 387–396. [Google Scholar] [CrossRef]
- Zareifopoulos, N.; Bellou, A.; Spiropoulou, A.; Spiropoulos, K. Prevalence, Contribution to Disease Burden and Management of Comorbid Depression and Anxiety in Chronic Obstructive Pulmonary Disease: A Narrative Review. COPD: J. Chronic Obstr. Pulm. Dis. 2019, 16, 406–417. [Google Scholar] [CrossRef]
- Atlantis E, Fahey P, Cochrane B, Smith S. Bidirectional associations between clinically relevant depression or anxiety and COPD: A systematic review and meta-analysis. Chest [Internet]. 2013 Sep 1 [cited 2025 Jan 28];144(3):766–77. Available from: http://journal.chestnet.org/article/S0012369213605929/fulltext.
- Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression—Important psychological comorbidities of COPD. J Thorac Dis [Internet]. 2014 [cited 2025 Jan 28];6(11):1615–31. Available from: https://jtd.amegroups.org/article/view/3329/html.
- van Manen, J.G.; E Bindels, P.J.; Dekker, F.W.; Ijzermans, C.J.; van der Zee, J.S.; Schadé, E. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax 2002, 57, 412–416. [Google Scholar] [CrossRef]
- Ioanna, T.; Kocks, J.; Tzanakis, N.; Siafakas, N.; van der Molen, T. Factors that influence disease-specific quality of life or health status in patients with COPD: a systematic review and meta-analysis of Pearson correlations. Prim. Care Respir. J. 2011, 20, 257–268. [Google Scholar] [CrossRef]
- Toy, E.L.; Beaulieu, N.U.; McHale, J.M.; Welland, T.R.; Plauschinat, C.A.; Swensen, A.; Duh, M.S. Treatment of COPD: Relationships between daily dosing frequency, adherence, resource use, and costs. Respir. Med. 2010, 105, 435–441. [Google Scholar] [CrossRef]
- Coquart, J.B.; Le Rouzic, O.; Racil, G.; Wallaert, B.; Grosbois, J.-M. Real-life feasibility and effectiveness of home-based pulmonary rehabilitation in chronic obstructive pulmonary disease requiring medical equipment. Int. J. Chronic Obstr. Pulm. Dis. 2017, ume 12, 3549–3556. [Google Scholar] [CrossRef]
- Lareau, S.C.; Yawn, B.P. Improving adherence with inhaler therapy in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2010, 5, 401–6. [Google Scholar] [CrossRef]
- DiMatteo MR, Lepper HS, Croghan TW. Depression Is a Risk Factor for Noncompliance With Medical Treatment: Meta-analysis of the Effects of Anxiety and Depression on Patient Adherence. Arch Intern Med [Internet]. 2000 Jul 24 [cited 2025 Jan 28];160(14):2101–7. Available from: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/485411.
- van Boven, J.F.; Chavannes, N.H.; van der Molen, T.; Mölken, M.P.R.-V.; Postma, M.J.; Vegter, S. Clinical and economic impact of non-adherence in COPD: A systematic review. Respir. Med. 2014, 108, 103–113. [Google Scholar] [CrossRef]
- Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax [Internet]. 2008 Sep 1 [cited 2025 Jan 28];63(9):831–8. Available from: https://thorax.bmj.
- Wedzicha, J.A.; Seemungal, T.A.R. COPD exacerbations: defining their cause and prevention. Lancet 2007, 370, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Gestoso, S.; García-Sanz, M.-T.; Carreira, J.-M.; Salgado, F.-J.; Calvo-Álvarez, U.; Doval-Oubiña, L.; Camba-Matos, S.; Peleteiro-Pedraza, L.; González-Pérez, M.-A.; Penela-Penela, P.; et al. Impact of anxiety and depression on the prognosis of copd exacerbations. BMC Pulm. Med. 2022, 22, 1–6. [Google Scholar] [CrossRef]
- Hanania, N.A.; Müllerova, H.; Locantore, N.W.; Vestbo, J.; Watkins, M.L.; Wouters, E.F.M.; Rennard, S.I.; Sharafkhaneh, A. Determinants of Depression in the ECLIPSE Chronic Obstructive Pulmonary Disease Cohort. Am. J. Respir. Crit. Care Med. 2011, 183, 604–611. [Google Scholar] [CrossRef]
- Holm, K.E.; Plaufcan, M.R.; Ford, D.W.; Sandhaus, R.A.; Strand, M.; Strange, C.; Wamboldt, F.S. The impact of age on outcomes in chronic obstructive pulmonary disease differs by relationship status. J. Behav. Med. 2013, 37, 654–663. [Google Scholar] [CrossRef]
- Wilson I. Depression in the patient with COPD. Int J Chron Obstruct Pulmon Dis [Internet]. 2006 [cited 2025 Jan 28];1(1):61–4. Available from: https://pubmed.ncbi.nlm.nih.gov/18046903/.
- van Manen, J.G.; E Bindels, P.J.; Dekker, F.W.; Ijzermans, C.J.; van der Zee, J.S.; Schadé, E. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax 2002, 57, 412–416. [Google Scholar] [CrossRef]
- Wagena, E.J.; Kant, I.; Huibers, M.J.; van Amelsvoort, L.G.; Swaen, G.M.; Wouters, E.F.; van Schayck, C.P. Psychological distress and depressed mood in employees with asthma, chronic bronchitis or emphysema: A population-based observational study on prevalence and the relationship with smoking cigarettes. Eur. J. Epidemiology 2003, 19, 147–153. [Google Scholar] [CrossRef]
- Breslau, N.; Peterson, E.L.; Schultz, L.R.; Chilcoat, H.D.; Andreski, P. Major Depression and Stages of Smoking. Arch. Gen. Psychiatry 1998, 55, 161–166. [Google Scholar] [CrossRef]
- Markou, A.; Kenny, P.J. Neuroadaptations to chronic exposure to drugs of abuse: Relevance to depressive symptomatology seen across psychiatric diagnostic categories. Neurotox. Res. 2002, 4, 297–313. [Google Scholar] [CrossRef]
- Lou, P.; Chen, P.; Zhang, P.; Yu, J.; Wang, Y.; Chen, N.; Zhang, L.; Wu, H.; Zhao, J. Effects of Smoking, Depression, and Anxiety on Mortality in COPD Patients: A Prospective Study. Respir. Care 2014, 59, 54–61. [Google Scholar] [CrossRef]
- Floyd, J.; Mallow, J.; Theeke, L. Health-Related Quality of Life, Depression, and Smoking Status in Patients with COPD: Results from the Behavioral Risk Factor Surveillance System Data. Open J. Nurs. 2018, 08, 779–794. [Google Scholar] [CrossRef]
- Sharma, S.; Shore, X.; Mohite, S.; Myers, O.; Kesler, D.; Vlahovich, K.; Sood, A. Association between Spirometric Parameters and Depressive Symptoms in New Mexico Uranium Workers. Southwest J. Pulm. Crit. Care 2021, 22, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Jung, J.Y.; Kim, Y.S.; Chung, K.S.; Song, J.H.; Kim, S.Y.; Kim, E.Y.; Kang, Y.A.; Park, M.S.; Chang, J.; et al. Relationship between depression and lung function in the general population in Korea: a retrospective cross-sectional study. Int. J. Chronic Obstr. Pulm. Dis. 2018, ume 13, 2207–2213. [Google Scholar] [CrossRef]
- Guo, L.; Cao, J.; Cheng, P.; Shi, D.; Cao, B.; Yang, G.; Liang, S.; Su, N.; Yu, M.; Zhang, C.; et al. Moderate-to-Severe Depression Adversely Affects Lung Function in Chinese College Students. Front. Psychol. 2020, 11, 652. [Google Scholar] [CrossRef] [PubMed]
- Schane RE, Woodruff PG, Dinno A, Covinsky KE, Walter LC. Prevalence and risk factors for depressive symptoms in persons with chronic obstructive pulmonary disease. J Gen Intern Med [Internet]. 2008 Nov [cited 2025 Jan 29];23(11):1757–62. Available from: https://pubmed.ncbi.nlm.nih.gov/18690488/.
- A Cleland, J.; Lee, A.J.; Hall, S. Associations of depression and anxiety with gender, age, health-related quality of life and symptoms in primary care COPD patients. Fam. Pr. 2007, 24, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Jácome, C.; Figueiredo, D.; Gabriel, R.; Cruz, J.; Marques, A. Predicting anxiety and depression among family carers of people with Chronic Obstructive Pulmonary Disease. Int. Psychogeriatrics 2014, 26, 1191–1199. [Google Scholar] [CrossRef]
- Martínez-Gestoso, S.; García-Sanz, M.-T.; Carreira, J.-M.; Salgado, F.-J.; Calvo-Álvarez, U.; Doval-Oubiña, L.; Camba-Matos, S.; Peleteiro-Pedraza, L.; González-Pérez, M.-A.; Penela-Penela, P.; et al. Impact of anxiety and depression on the prognosis of copd exacerbations. BMC Pulm. Med. 2022, 22, 1–6. [Google Scholar] [CrossRef]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef]
- Smoller JW, Pollack MH, Otto MW, Rosenbaum JF, Kradin RL. Panic anxiety, dyspnea, and respiratory disease. Theoretical and clinical considerations. Am J Respir Crit Care Med [Internet]. 1996 [cited 2025 Jan 29];154(1):6–17. Available from: https://pubmed.ncbi.nlm.nih.gov/8680700/.
- Klein DF. False suffocation alarms, spontaneous panics, and related conditions. An integrative hypothesis. Arch Gen Psychiatry [Internet]. 1993 [cited 2025 Jan 29];50(4):306–17. Available from: https://pubmed.ncbi.nlm.nih.gov/8466392/.
- Patton GC, Hibbert M, Rosier MJ, Carlin JB, Caust J, Bowes G. Is smoking associated with depression and anxiety in teenagers? Am J Public Health [Internet]. 1996 [cited 2025 Jan 29];86(2):225. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC1380332/.
- O'Donnell, D.E.; Banzett, R.B.; Carrieri-Kohlman, V.; Casaburi, R.; Davenport, P.W.; Gandevia, S.C.; Gelb, A.F.; Mahler, D.A.; Webb, K.A. Pathophysiology of Dyspnea in Chronic Obstructive Pulmonary Disease: A Roundtable. Proc. Am. Thorac. Soc. 2007, 4, 145–168. [Google Scholar] [CrossRef]
- Jolley, C.J.; Moxham, J. A physiological model of patient-reported breathlessness during daily activities in COPD. Eur. Respir. Rev. 2009, 18, 66–79. [Google Scholar] [CrossRef]
- Liotti, M.; Brannan, S.; Egan, G.; Shade, R.; Madden, L.; Abplanalp, B.; Robillard, R.; Lancaster, J.; Zamarripa, F.E.; Fox, P.T.; et al. Brain responses associated with consciousness of breathlessness (air hunger). Proc. Natl. Acad. Sci. 2001, 98, 2035–2040. [Google Scholar] [CrossRef]
- Evans, K.C.; Banzett, R.B.; Adams, L.; McKay, L.; Frackowiak, R.S.J.; Corfield, D.R. BOLD fMRI Identifies Limbic, Paralimbic, and Cerebellar Activation During Air Hunger. J. Neurophysiol. 2002, 88, 1500–1511. [Google Scholar] [CrossRef] [PubMed]
- Bailey PH. The dyspnea-anxiety-dyspnea cycle - COPD patients’ stories of breathlessness: “It’s scary/when you can’t breathe.” Qual Health Res [Internet]. 2004 [cited 2025 Jan 29];14(6):760–78. Available from: https://www.researchgate.net/publication/8506490_The_Dyspnea-Anxiety-Dyspnea_Cycle-COPD_Patients’_Stories_of_Breathlessness_It’s_Scary_When_you_Can’t_Breathe.
- McKenzie, D.K.; Butler, J.E.; Gandevia, S.C.; Lagerquist, O.; Walsh, L.D.; Blouin, J.-S.; Collins, D.F. Respiratory muscle function and activation in chronic obstructive pulmonary disease. J. Appl. Physiol. 2009, 107, 621–629. [Google Scholar] [CrossRef]
- Schmidt, N.B.; Telch, M.J.; Jaimez, T.L. Biological challenge manipulation of PCO₂ levels: A test of Klein's (1993) suffocation alarm theory of panic. J. Abnorm. Psychol. 1996, 105, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Roomi, J.; Baldwin, R.C.; Connolly, M.J. Depression in elderly outpatients with disabling chronic obstructive pulmonary disease. Age and Ageing 1998, 27, 155–160. [Google Scholar] [CrossRef]
- Kim, H.F.S.; Kunik, M.E.; Molinari, V.A.; Hillman, S.L.; Lalani, S.; Orengo, C.A.; Petersen, N.J.; Nahas, Z.; Goodnight-White, S. Functional Impairment in COPD Patients: The Impact of Anxiety and Depression. Psychosomatics 2000, 41, 465–471. [Google Scholar] [CrossRef] [PubMed]
- A Dowson, C.; Town, G.; Frampton, C.; Mulder, R.T. Psychopathology and illness beliefs influence COPD self-management. J. Psychosom. Res. 2004, 56, 333–340. [Google Scholar] [CrossRef]
- PDF) Neuropsychiatric function in chronic lung disease: The role of pulmonary rehabilitation [Internet]. [cited 2025 Jan 29]. Available from: https://www.researchgate.net/publication/23185128_Neuropsychiatric_function_in_chronic_lung_disease_The_role_of_pulmonary_rehabilitation.
- Graydon, J.E.; Ross, E. Influence of symptoms, lung function, mood, and social support on level of functioning of patients with COPD. Res. Nurs. Heal. 1995, 18, 525–533. [Google Scholar] [CrossRef]
- Post, L.; Collins, C. The Poorly Coping COPD Patient: A Psychotherapeutic Perspective. Int. J. Psychiatry Med. 1982, 11, 173–182. [Google Scholar] [CrossRef]
- Breslau N, Marlyne Kilbey M, Andreski P. Nicotine withdrawal symptoms and psychiatric disorders: findings from an epidemiologic study of young adults. Am J Psychiatry [Internet]. 1992 [cited 2025 Jan 29];149(4):464–9. Available from: https://pubmed.ncbi.nlm.nih.gov/1554030/.
- Fergusson, D.M.; Lynskey, M.T.; Horwood, L.J. Comorbidity Between Depressive Disorders and Nicotine Dependence in a Cohort of 16-Year-Olds. Arch. Gen. Psychiatry 1996, 53, 1043–1047. [Google Scholar] [CrossRef]
- Norwood, R.J. A review of etiologies of depression in COPD. 2007, 2, 485–491.
- Van Dijk EJ, Vermeer SE, De Groot JC, Van De Minkelis J, Prins ND, Oudkerk M, et al. Arterial oxygen saturation, COPD, and cerebral small vessel disease. J Neurol Neurosurg Psychiatry [Internet]. 2004 [cited 2025 Jan 29];75(5):733. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC1763550/.
- Campbell JJ, Coffey CE. Neuropsychiatric significance of subcortical hyperintensity. J Neuropsychiatry Clin Neurosci [Internet]. 2001 [cited 2025 Jan 29];13(2):261–88. Available from: https://pubmed.ncbi.nlm.nih.gov/11449035/.
- El-Ad B, Lavie P. Effect of sleep apnea on cognition and mood. Int Rev Psychiatry [Internet]. 2005 Aug [cited 2025 Jan 29];17(4):277–82. Available from: https://www.researchgate.net/publication/7569893_Effect_of_sleep_apnea_on_cognition_and_mood.
- zge C, Özge A, Ünal Ö. Cognitive and functional deterioration in patients with severe COPD. Behav Neurol [Internet]. 2006 [cited 2025 Jan 29];17(2):121–30. Available from: https://pubmed.ncbi.nlm.nih.gov/16873924/.
- Aloia, M.S.; Arnedt, J.T.; Davis, J.D.; Riggs, R.L.; Byrd, D. Neuropsychological sequelae of obstructive sleep apnea-hypopnea syndrome: A critical review. J. Int. Neuropsychol. Soc. 2004, 10, 772–785. [Google Scholar] [CrossRef]
- Maes, M. Evidence for an immune response in major depression: A review and hypothesis. 2000, 19, 11–38, https://doi.org/10.1016/0278-5846(94)00101-m. [CrossRef]
- Hughes, M.M.; Connor, T.J.; Harkin, A. Stress-Related Immune Markers in Depression: Implications for Treatment. Int. J. Neuropsychopharmacol. 2016, 19, pyw001. [Google Scholar] [CrossRef] [PubMed]
- Rybka, J.; Korte, S.M.; Czajkowska-Malinowska, M.; Wiese, M.; Kędziora-Kornatowska, K.; Kędziora, J. The links between chronic obstructive pulmonary disease and comorbid depressive symptoms: role of IL-2 and IFN-γ. Clin. Exp. Med. 2015, 16, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Gabay C. Interleukin-6 and chronic inflammation. Arthritis Res Ther [Internet]. 2006 Jul [cited 2025 Jan 29];8 Suppl 2(Suppl 2). Available from: https://pubmed.ncbi.nlm.nih.gov/16899107/.
- Campbell, I.L.; Erta, M.; Lim, S.L.; Frausto, R.; May, U.; Rose-John, S.; Scheller, J.; Hidalgo, J. Trans-Signaling Is a Dominant Mechanism for the Pathogenic Actions of Interleukin-6 in the Brain. J. Neurosci. 2014, 34, 2503–2513. [Google Scholar] [CrossRef] [PubMed]
- Chomarat, P.; Banchereau, J.; Davoust, J.; Palucka, A.K. IL-6 switches the differentiation of monocytes from dendritic cells to macrophages. Nat. Immunol. 2000, 1, 510–514. [Google Scholar] [CrossRef]
- Murr, C.; Widner, B.; Wirleitner, B.; Fuchs, D. Neopterin as a Marker for Immune System Activation. Curr. Drug Metab. 2002, 3, 175–187. [Google Scholar] [CrossRef]
- Maes, M.; Scharpé, S.; Meltzer, H.Y.; Okayli, G.; Bosmans, E.; D'Hondt, P.; Bossche, B.V.; Cosyns, P. Increased neopterin and interferon-gamma secretion and lower availability of L-tryptophan in major depression: Further evidence for an immune response. Psychiatry Res. 1994, 54, 143–160. [Google Scholar] [CrossRef]
- Barnes, P.J. The Cytokine Network in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2009, 41, 631–638. [Google Scholar] [CrossRef]
- Connor, T.J.; Leonard, B.E. Depression, stress and immunological activation: The role of cytokines in depressive disorders. Life Sci. 1998, 62, 583–606. [Google Scholar] [CrossRef]
- Torvinen, M.; Campwala, H.; Kilty, I. The role of IFN-γ in regulation of IFN-γ-inducible protein 10 (IP-10) expression in lung epithelial cell and peripheral blood mononuclear cell co-cultures. Respir. Res. 2007, 8, 80–80. [Google Scholar] [CrossRef]
- Schoenborn JR, Wilson CB. Regulation of interferon-gamma during innate and adaptive immune responses. Adv Immunol [Internet]. 2007 [cited 2025 Jan 29];96:41–101. Available from: https://pubmed.ncbi.nlm.nih.gov/17981204/.
- Lasser K, Boyd JW, Woolhandler S, Himmelstein DU, McCormick D, Bor DH. Smoking and mental illness: A population-based prevalence study. JAMA [Internet]. 2000 [cited 2025 Jan 29];284(20):2606–10. Available from: https://pubmed.ncbi.nlm.nih.gov/11086367/.
- Berlin, I.; Covey, L.S. Pre-cessation depressive mood predicts failure to quit smoking: the role of coping and personality traits*. Addiction 2006, 101, 1814–1821. [Google Scholar] [CrossRef]
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and Its Discontents: The Role of Cytokines in the Pathophysiology of Major Depression. Biol. Psychiatry 2009, 65, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Torvinen, M.; Campwala, H.; Kilty, I. The role of IFN-γ in regulation of IFN-γ-inducible protein 10 (IP-10) expression in lung epithelial cell and peripheral blood mononuclear cell co-cultures. Respir. Res. 2007, 8, 80–80. [Google Scholar] [CrossRef] [PubMed]
- Bowler, R.P.; Barnes, P.J.; Crapo, J.D. The Role of Oxidative Stress in Chronic Obstructive Pulmonary Disease. COPD: J. Chronic Obstr. Pulm. Dis. 2004, 1, 255–277. [Google Scholar] [CrossRef]
- PRYOR WA, STONE K. Oxidants in cigarette smoke. Radicals, hydrogen peroxide, peroxynitrate, and peroxynitrite. Ann N Y Acad Sci [Internet]. 1993 [cited 2025 Jan 30];686(1):12–27. Available from: https://pubmed.ncbi.nlm.nih.gov/8512242/.
- Langen, R.; Korn, S.; Wouters, E. ROS in the local and systemic pathogenesis of COPD. Free. Radic. Biol. Med. 2003, 35, 226–235. [Google Scholar] [CrossRef]
- Sunyer, J. Urban air pollution and chronic obstructive pulmonary disease: a review. Eur. Respir. J. 2001, 17, 1024–1033. [Google Scholar] [CrossRef]
- Halliwell, B. Reactive Species and Antioxidants. Redox Biology Is a Fundamental Theme of Aerobic Life. Plant Physiol. 2006, 141, 312–322. [Google Scholar] [CrossRef]
- Goeptar, A.R.; Scheerens, H.; Vermeulen, N.P.E. Oxygen and Xenobiotic Reductase Activities of Cytochrome P450. Crit. Rev. Toxicol. 1995, 25, 25–65. [Google Scholar] [CrossRef]
- Şahin, Ü.; Ünlü, M.; Özgüner, F.; Sütçü, R.; Akkaya, A.; Delibaş, Ν. Lipid Peroxidation and Changes of Glutathione Peroxidase Activity in Treatment of Chronic Obstructive Pulmonary Disease Exacerbation: Prognostic Value of Malondialdehyde. J. Basic Clin. Physiol. Pharmacol. 2001, 12, 59–68. [Google Scholar] [CrossRef]
- Rahman, I.; Skwarska, E.; MacNee, W. Attenuation of oxidant/antioxidant imbalance during treatment of exacerbations of chronic obstructive pulmonary disease. Thorax 1997, 52, 565–568. [Google Scholar] [CrossRef]
- alikoǧlu M, Ünlü A, Tamer L, Ercan B, Buǧdayci R, Atik U. The levels of serum vitamin C, malonyldialdehyde and erythrocyte reduced glutathione in chronic obstructive pulmonary disease and in healthy smokers. Clin Chem Lab Med [Internet]. 2002 [cited 2025 Jan 30];40(10):1028–31. Available from: https://pubmed.ncbi.nlm.nih.gov/12476943/.
- Paredi P, Kharitonov SA, Leak D, Ward S, Cramer D, Barnes PJ. Exhaled ethane, a marker of lipid peroxidation, is elevated in chronic obstructive pulmonary disease. Am J Respir Crit Care Med [Internet]. 2000 [cited 2025 Jan 30];162(2 Pt 1):369–73. Available from: https://pubmed.ncbi.nlm.nih.gov/10934055/.
- Montuschi, P.; Collins, J.V.; Ciabattoni, G.; Lazzeri, N.; Corradi, M.; Kharitonov, S.A.; Barnes, P.J. Exhaled 8-Isoprostane as an In Vivo Biomarker of Lung Oxidative Stress in Patients with COPD and Healthy Smokers. Am. J. Respir. Crit. Care Med. 2000, 162, 1175–1177. [Google Scholar] [CrossRef]
- Iglesias JR, Díez-Manglano J, García FL, Peromingo JAD, Almagro P, Aguilar JMV. Management of the COPD Patient with Comorbidities: An Experts Recommendation Document. Int J Chron Obstruct Pulmon Dis [Internet]. 2020 [cited 2025 Jan 31];15:1015–37. Available from: https://pubmed.ncbi.nlm.nih.gov/32440113/.
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet (London, England) [Internet]. 2007 Sep 1 [cited 2025 Jan 31];370(9589):765–73. Available from: https://pubmed.ncbi.nlm.nih.gov/17765526/.
- Aggarwal, A.N. The 2022 update of the Global Initiative for Chronic Obstructive Lung Disease guidelines for chronic obstructive pulmonary disease. Int. J. Noncommunicable Dis. 2022, 7, 53–54. [Google Scholar] [CrossRef]
- Martínez-Gestoso, S.; García-Sanz, M.-T.; Carreira, J.-M.; Salgado, F.-J.; Calvo-Álvarez, U.; Doval-Oubiña, L.; Camba-Matos, S.; Peleteiro-Pedraza, L.; González-Pérez, M.-A.; Penela-Penela, P.; et al. Impact of anxiety and depression on the prognosis of copd exacerbations. BMC Pulm. Med. 2022, 22, 1–6. [Google Scholar] [CrossRef]
- Deng, D.; Zhou, A.; Ping, C.; Shuang, Q. CODEXS: A New Multidimensional Index to Better Predict Frequent COPD Exacerbators with Inclusion of Depression Score. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 249–259. [Google Scholar] [CrossRef]
- Ouellette, D.R.; Lavoie, K.L. Recognition, diagnosis, and treatment of cognitive and psychiatric disorders in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, ume 12, 639–650. [Google Scholar] [CrossRef]
- Rábade Castedo C, de Granda-Orive JI, González-Barcala FJ. Incremento de la prevalencia del tabaquismo: ¿causas y actuación? Arch Bronconeumol [Internet]. 2019 Nov 1 [cited 2025 Jan 31];55(11):557–8. Available from: https://www.academia.edu/113125541/Incremento_de_la_prevalencia_del_tabaquismo_causas_y_actuación.
- Nair, P.; Walters, K.; Aw, S.; Gould, R.; Kharicha, K.; Marta College Marta College Buszewicz,; Frost, R. Self-management of depression and anxiety amongst frail older adults in the United Kingdom: A qualitative study. PLOS ONE 2022, 17, e0264603. [CrossRef]
- Bugajski, A.; Morgan, H.; Wills, W.; Jacklin, K.; Alleyne, S.; Kolta, B.; Lengerich, A.; Rechenberg, K. Anxiety and Depressive Symptoms in Patients with COPD: Modifiable Explanatory Factors. West. J. Nurs. Res. 2022, 45, 316–326. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, X.; Li, X.; Zhang, R.; Chang, Y.; Li, Y.; Lu, H. Unraveling the mediation role of frailty and depression in the relationship between social support and self-management among Chinese elderly COPD patients: a cross-sectional study. BMC Pulm. Med. 2024, 24, 1–8. [Google Scholar] [CrossRef]
- Taunque, A.; Li, G.; MacNeil, A.; Gulati, I.; Jiang, Y.; de Groh, M.; Fuller-Thomson, E. Breathless and Blue in the Canadian Longitudinal Study on Aging: Incident and Recurrent Depression Among Older Adults with COPD During the COVID-19 Pandemic. Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 1975–1993. [Google Scholar] [CrossRef]
- Kaplan, A.G. Do Antidepressants Worsen COPD Outcomes in Depressed Patients with COPD? Pulm. Ther. 2024, 10, 411–426. [Google Scholar] [CrossRef]
- Witt, L.J.; Wroblewski, K.E.; Pinto, J.M.; Wang, E.; McClintock, M.K.; Dale, W.; White, S.R.; Press, V.G.; Huisingh-Scheetz, M. Beyond the Lung: Geriatric Conditions Afflict Community-Dwelling Older Adults With Self-Reported Chronic Obstructive Pulmonary Disease. Front. Med. 2022, 9, 814606. [Google Scholar] [CrossRef]
- Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. https://doi.org/101164/rccm201204-0596PP [Internet]. 2013 Mar 22 [cited 2025 Jan 31];187(4):347–65. Available from: www.goldcopd.org.
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLOS Med. 2006, 3, e442. [Google Scholar] [CrossRef]
- Gut-Gobert C, Cavaillès A, Dixmier A, Guillot S, Jouneau S, Leroyer C, et al. Women and COPD: do we need more evidence? Eur Respir Rev [Internet]. 2019 Feb 27 [cited 2025 Jan 31];28(151). Available from: https://publications.ersnet.org/content/errev/28/151/180055.
- Sheel, A.W.; Guenette, J.A.; Yuan, R.; Holy, L.; Mayo, J.R.; McWilliams, A.M.; Lam, S.; Coxson, H.O. Evidence for dysanapsis using computed tomographic imaging of the airways in older ex-smokers. J. Appl. Physiol. 2009, 107, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.J.; Curtis, J.L.; Sciurba, F.; Mumford, J.; Giardino, N.D.; Weinmann, G.; Kazerooni, E.; Murray, S.; Criner, G.J.; Sin, D.D.; et al. Sex Differences in Severe Pulmonary Emphysema. Am. J. Respir. Crit. Care Med. 2007, 176, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Choi JS, Kwak SH, Son NH, Oh JW, Lee S, Lee EH. Sex differences in risk factors for depressive symptoms in patients with COPD: The 2014 and 2016 Korea National Health and Nutrition Examination Survey. BMC Pulm Med [Internet]. 2021 Dec 1 [cited 2025 Jan 31];21(1). Available from: https://www.researchgate.net/publication/351953327_Sex_differences_in_risk_factors_for_depressive_symptoms_in_patients_with_COPD_The_2014_and_2016_Korea_National_Health_and_Nutrition_Examination_Survey.
- Milne, K.M.; Mitchell, R.A.; Ferguson, O.N.; Hind, A.S.; Guenette, J.A. Sex-differences in COPD: from biological mechanisms to therapeutic considerations. Front. Med. 2024, 11, 1289259. [Google Scholar] [CrossRef]
- Thun, M.J.; Carter, B.D.; Feskanich, D.; Freedman, N.D.; Prentice, R.; Lopez, A.D.; Hartge, P.; Gapstur, S.M. 50-Year Trends in Smoking-Related Mortality in the United States. N. Engl. J. Med. 2013, 368, 351–364. [Google Scholar] [CrossRef]
- Kendrová, L.; Kuriplachová, G.; Ištoňová, M.; Nechvátal, P.; Mikuľáková, W.; Takáč, P. Assessment of depression in patients with chronic obstructive pulmonary disease. Kontakt 2014, 16, e203–e208. [Google Scholar] [CrossRef]
- Júnior, J.L.R.S.; Conde, M.B.; Corrêa, K.d.S.; da Silva, C.; Prestes, L.d.S.; Rabahi, M.F. COPD Assessment Test (CAT) score as a predictor of major depression among subjects with chronic obstructive pulmonary disease and mild hypoxemia: a case–control study. BMC Pulm. Med. 2014, 14, 186. [Google Scholar] [CrossRef]
- Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res. 2011 Nov;63(SUPPL. 11).
- Rebbapragada, V.; Hanania, N.A. Can We Predict Depression in COPD? COPD: J. Chronic Obstr. Pulm. Dis. 2007, 4, 3–4. [Google Scholar] [CrossRef]
- Lee, Y.S.; Park, S.; Oh, Y.-M.; Lee, S.-D.; Park, S.-W.; Kim, Y.S.; In, K.H.; Jung, B.H.; Lee, K.H.; Ra, S.W.; et al. Chronic Obstructive Pulmonary Disease Assessment Test Can Predict Depression: A Prospective Multi-Center Study. J. Korean Med Sci. 2013, 28, 1048–1054. [Google Scholar] [CrossRef]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas [Internet]. 1977 [cited 2025 Feb 10];1(3):385–401. Available from: https://hdl.handle.net/11299/98561.
- Wada K, Yamada N, Suzuki H, Lee Y, Kuroda S. Recurrent cases of corticosteroid-induced mood disorder: clinical characteristics and treatment. J Clin Psychiatry [Internet]. 2000 [cited 2025 Feb 10];61(4):261–7. Available from: https://pubmed.ncbi.nlm.nih.gov/10830146/.
- Fletcher, C.; Peto, R. The natural history of chronic airflow obstruction. BMJ 1977, 1, 1645–1648. [Google Scholar] [CrossRef]
- Poole, P.; E Chacko, E.; Wood-Baker, R.; Cates, C.J. Influenza vaccine for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2006, CD002733. [Google Scholar] [CrossRef]
- Kvale PA, Conway WA, Coates EO. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med [Internet]. 1980 [cited 2025 Jan 31];93(3):391–8. Available from: https://pubmed.ncbi.nlm.nih.gov/6776858/.
- Donohue, J.F.; van Noord, J.A.; Bateman, E.D.; Langley, S.J.; Lee, A.; Witek, T.J.; Kesten, S.; Towse, L. A 6-Month, Placebo-Controlled Study Comparing Lung Function and Health Status Changes in COPD Patients Treated With Tiotropium or Salmeterol. Chest 2002, 122, 47–55. [Google Scholar] [CrossRef] [PubMed]
- A F, F M, K N, S P, R W, A R, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med [Internet]. 2003 May 22 [cited 2025 Jan 31];348(21):2059–73. Available from: https://pubmed.ncbi.nlm.nih.gov/12759479/.
- Lacasse Y, Goldstein R, Lasserson TJ, Martin S. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Lacasse Y, editor. Cochrane database Syst Rev [Internet]. 2006 Oct 18 [cited 2025 Jan 31];(4). Available from: https://pubmed.ncbi.nlm.nih.gov/17054186/.
- Effing, T.; Monninkhof, E.M.; van der Valk, P.D.; van der Palen, J.; van Herwaarden, C.L.; Partidge, M.R.; Walters, E.H.; Zielhuis, G.A. Self-management education for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2007, 4, CD002990–1. [Google Scholar]
- Ahmad, M.; Rasul, F.M. Steroid-induced psychosis treated with haloperidol in a patient with active chronic obstructive pulmonary disease. Am. J. Emerg. Med. 1999, 17, 735. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.S.; Suppes, T.; Khan, D.A.; Carmody, T.J. Mood Changes During Prednisone Bursts in Outpatients With Asthma. J. Clin. Psychopharmacol. 2002, 22, 55–61. [Google Scholar] [CrossRef]
- Lewis DA, Smith RE. Steroid-induced psychiatric syndromes. A report of 14 cases and a review of the literature. J Affect Disord [Internet]. 1983 [cited 2025 Jan 31];5(4):319–32. Available from: https://pubmed.ncbi.nlm.nih.gov/6319464/.
- Ciriaco M, Ventrice P, Russo G, Scicchitano M, Mazzitello G, Scicchitano F, et al. Corticosteroid-related central nervous system side effects Case Review. J Pharmacol Pharmacother [Internet]. 2013 [cited 2025 Jan 31]; Available from: www.jpharmacol.com.
- Keul, F.; Hamacher, K. Consistent Quantification of Complex Dynamics via a Novel Statistical Complexity Measure. Entropy 2022, 24, 505. [Google Scholar] [CrossRef]
- Boylan, P.M.; Abdalla, M.; Bissell, B.; Malesker, M.A.; Santibañez, M.; Smith, Z. Theophylline for the management of respiratory disorders in adults in the 21st century: A scoping review from the American College of Clinical Pharmacy Pulmonary Practice and Research Network. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2023, 43, 963–990. [Google Scholar] [CrossRef]
- Yohannes AM, Alexopoulos GS. Pharmacologic Treatment of Depression in Older Patients with COPD: Impact on the Course of the Disease and Health Outcomes. Drugs Aging [Internet]. 2014 [cited 2025 Mar 6];31(7):483. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4522901/.
- ZuWallack, R. The Nonpharmacologic Treatment of Chronic Obstructive Pulmonary Disease: Advances in Our Understanding of Pulmonary Rehabilitation. Proc. Am. Thorac. Soc. 2007, 4, 549–553. [Google Scholar] [CrossRef]
- Stockley RA. Biomarkers in chronic obstructive pulmonary disease: confusing or useful? Int J Chron Obstruct Pulmon Dis [Internet]. 2014 Feb 7 [cited 2025 Jan 31];9:163. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3923613/.
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Emery CF, Schein RL, Hauck ER, MacIntyre NR. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol [Internet]. 1998 [cited 2025 Jan 31];17(3):232–40. Available from: https://pubmed.ncbi.nlm.nih.gov/9619472/.
- Jácome, C.; Marques, A. Impact of Pulmonary Rehabilitation in Subjects With Mild COPD. Respir. Care 2014, 59, 1577–1582. [Google Scholar] [CrossRef]
- Güell, R.; Resqueti, V.; Sangenis, M.; Morante, F.; Martorell, B.; Casan, P.; Guyatt, G.H. Impact of Pulmonary Rehabilitation on Psychosocial Morbidity in Patients With Severe COPD. Chest 2006, 129, 899–904. [Google Scholar] [CrossRef]
- Mikkelsen, R.L.; Middelboe, T.; Pisinger, C.; Stage, K.B. Anxiety and depression in patients with chronic obstructive pulmonary disease (COPD). A review. Nord. J. Psychiatry 2004, 58, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis [Internet]. 2015 Jan 7 [cited 2025 Jan 31];10:95. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4293292/.
- Anxiety: Management of anxiety (panic disorder, with or without agoraphobia, and generalised anxiety disorder) in adults in primary, secondary and community care | Guidance | NICE.
- Nelson, D.R. The Cytochrome P450 Homepage. Hum. Genom. 2009, 4, 59–65. [Google Scholar] [CrossRef]
- A Siraj, R.; E Bolton, C.; McKeever, T.M. Association between antidepressants with pneumonia and exacerbation in patients with COPD: a self-controlled case series (SCCS). Thorax 2023, 79, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Cafarella, P.A.; Effing, T.W.; Usmani, Z.; Frith, P.A. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: A literature review. Respirology 2012, 17, 627–638. [Google Scholar] [CrossRef]
- Stewart, R.C. Respiratory depression with diazepam: potential complications and contraindications.. 1978, 25, 117–8.
- Man, G.; Hsu, K.; Sproule, B. Effect of Alprazolam on Exercise and Dyspnea in Patients with Chronic Obstructive Pulmonary Disease. Chest 1986, 90, 832–836. [Google Scholar] [CrossRef]
- Kaplan AG, Kaplan AG. Do Antidepressants Worsen COPD Outcomes in Depressed Patients with COPD? Pulm Ther [Internet]. 2024 Dec 1 [cited 2025 Mar 6];10(4):411. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11574234/.
- Hegerl U, Mergl R. Depression and suicidality in COPD: understandable reaction or independent disorders? Eur Respir J [Internet]. 2014 Sep 1 [cited 2025 Jan 31];44(3):734–43. Available from: https://pubmed.ncbi.nlm.nih.gov/24876171/.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



