Submitted:
21 March 2025
Posted:
24 March 2025
You are already at the latest version
Abstract
Disorders of metabolism have been seen in multiple autoimmune diseases including SLE and Sjogren’s disease. The current studies were designed to evaluate mutations in genes involved with metabolism in a cohort of patients with Sjogren’s disease diagnosed from clinical criteria and the presence of antibodies to salivary gland antigens. Patients included in these studies met criteria for Sjogren’s disease and were able to get genetic studies. There were 194 of these patients and 192 had mutations in one or more gene involved with metabolism: 188 patients had mutations in mitochondrial respiratory chain genes, 17 patients had mutations in mitochondrial tRNA genes, 10 patients had mutations in mitochondrial DLOOP regions, 6 patients had mutations involved with carnitine transport, 6 patients had mutations in genes causing mitochondrial depletion and 7 patients had glycogen storage diseases. In all cases, treatment of the metabolic disorder led to symptomatic improvement in energy, exercise tolerance, gastrointestinal dysmotility and management of infections. In conclusion, metabolic disorders are common in patients with Sjogren’s disease and may be one of the factors leading to the initiation of the disease. Treatment of patients with Sjogren’s disease should include treatment of the underlying / associated metabolic disorder.
Keywords:
Sjogren’s disease
; metabolism
; autoantibodies
1. Introduction
Understanding of the pathophysiology of autoimmune diseases has been rapidly advancing in the last several years. While dysregulated immune function has been appreciated for decades, appreciation of dysregulated metabolism in autoimmune diseases is relatively recent [1,2,3,4,5,6,7]. Abnormal mitochondrial function was first observed in SLE [8,9,10,11,12,13,14,15] but has been observed in Sjogren’s disease as well [16,17,18,19,20,21,22,23,24,25,26]. We observed that many of the symptoms attributable to Sjogren’s disease were in fact related to the underlying metabolic disease in particular patients. We therefore sought to determine the number of patients with mutations in genes associated with metabolism in a cohort of patients with Sjogren’s disease seen in our clinics.
2. Results
The first issue to address is the autoantibodies expressed by the patients in this study. They all met American – European clinical criteria for Sjogren’s disease with clinical signs of dry eye and dry mouth and positive Schirmer’s tests, except only 13 of the patients had SSA antibodies. All the patients had autoantibodies associated with Sjogren’s disease, but the majority had antibodies to SP1 and CA6 (Figure 1), which are salivary gland specific antigens [27,28,29,30]. Many of the patients expressed more than one autoantibody. Interestingly, 54% of the patients with SP1 autoantibodies expressed IgM autoantibodies while 67% of the patients with CA6 autoantibodies expressed IgG autoantibodies. These patients might by called seronegative Sjogren’s patients by some investigators because of their lack of SSA expression.
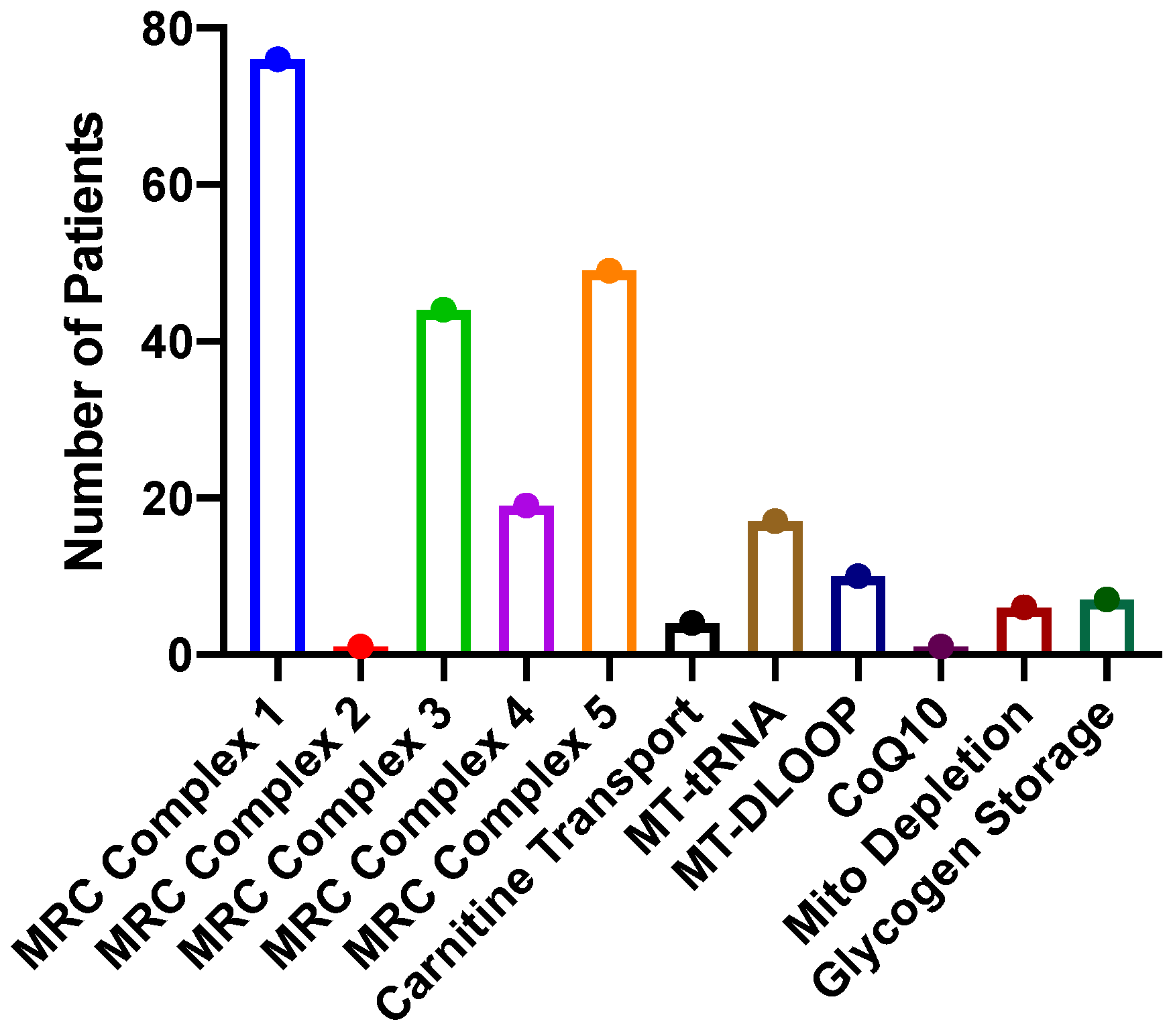
Genetic studies looking for metabolic disorders were done on these patients because of symptoms that are consistent with adult- onset metabolic disorders: fatigue, exercise intolerance, recurrent infections, accelerated osteoarthritis, gastrointestinal dysmotility including gastroparesis, gastroesophageal reflux and constipation and in some cases dyspnea. In all cases, whole exome sequencing and sequencing of the mitochondrial genome was performed by GeneDx. Of the patients studied, 192 (99%) had mutations in genes associated with metabolic function (Figure 2). Some patients carried more than one mutation. Rare missense mutations in mitochondrial respiratory chain genes were common: complex 1 – 76, complex 3 – 44, complex 4 – 19 and complex 5 – 49. One patient had a mutation in the succinate dehydrogenase gene, which is involved with complex 2 of the mitochondrial respiratory chain but also the citric acid cycle. Six patients had mutations associated with carnitine: CPT2 – 4 and SLC22A5 – 2. Mutations in various mitochondrial tRNA were seen in 17 patients and 10 patients had rare MT-DLOOP mutations. One patient had a PDSS2 mutation associated with CoQ10 deficiency, and 6 patients had mutations associated with mitochondrial depletion syndrome: POLG – 3, MCME1 – 1, RRMP8 – 1 and thymidine kinase – 1. Seven patients had mutations in genes causing glycogen storage diseases: Pompe disease – 1, Forbes – Cori disease – 1, McArdle’s Disease -1, phosphofructokinase deficiency (type IX) – 1 and lactate dehydrogenase deficiency (type XI) – 3. The result in all these mutations is inefficient generation of ATP and in the case of the glycogen storage diseases, difficulty handling complex carbohydrates.
The treatment of mitochondrial disorders involves several medications, each of which works by a different mechanism, so a synergistic effect is seen [31]. The first medication is CoQ10, which is involved with transporting electrons between complex 1 and 3 of the mitochondrial respiratory chain and helps generate ATP more efficiently [32,33]. Creatine generates ATP through the creatine phosphate shuttle and discourages replication of abnormal mitochondria [34]. Carnitine brings fatty acids into the mitochondria so they can undergo beta oxidation to generate NADH [26,35]. Folic acid is a co-factor for several respiratory chain enzymes [36]. N-acetyl cysteine is a potent antioxidant [37,38] and the amino acid glutamine acts as an alternative energy source [39,40]. The doses of these medications vary for individual patients, but all patients have noted some benefit from them with regards to fatigue, exercise tolerance and decreasing infection rate. With regards to the glycogen storage diseases, patients are taught to avoid complex carbohydrates and supplement with simple sugars [41,42,43,44,45,46]. At the same time, since glycogen storage diseases are generally associated with mitochondrial dysfunction, we usually add the medications listed above that are used to treat mitochondrial diseases [47,48]. These patients saw significant improvement in fatigue and exercise tolerance with this regimen.
3. Discussion
We have demonstrated in this study that Sjogren’s patients with symptoms consistent with a metabolic disorder, fatigue, exercise intolerance, gastrointestinal dysmotility and recurrent infections, often have mutations in genes important for metabolism. The identification of the metabolic disorder is helpful in suggesting therapies to improve disease symptoms. It is certainly true that all these patients come from a clinic that specializes in metabolic disorders so there is some bias regarding patient selection. Interestingly, when patients with metabolic disorders are evaluated as a group there is a very high incidence of Sjogren’s disease [26,49].
Mitochondrial dysfunction has been observed in patients with Sjogren’s disease by several investigators [16,17,21,22,50,51,52]. The question becomes whether mitochondrial dysfunction occurs secondary to the inflammation in the salivary glands or whether it is a primary process contributing to the development of the disease. One way that mitochondrial dysfunction could contribute to disease pathogenesis is by decreasing the ability to handle infections thus leading to more tissue damage and the increased likelihood that normal autorecognition is turned into pathologic autoreactivity [53,54,55,56]. Mitochondrial dysfunction could lead to modification of various proteins and other molecules involved with signaling and genetic function [56]. Alternatively, inefficient mitochondrial function could lead to reliance on glycolytic metabolism, which tends to encourage the actions of effector rather than regulatory lymphocytes and other immune cells [57,58,59,60,61,62,63,64]. Interesting, IL-14 (a-taxilin) was recently shown to stimulate glycolysis [65]. The Il-14 transgenic mouse has been shown to be an excellent model for Sjogren’s disease [66,67]. Recent studies have demonstrated that blocking glycolysis inhibits the development of Sjogren’s disease manifestations in this animal model [68].
This manuscript has weaknesses because it describes patients followed as part of normal clinical service and does not describe a research study designed to address a particular research question. Furthermore, while all of the patients had autoantibodies associated with Sjogren’s disease, only a few patients had SSA antibodies, which are the only autoantibodies in the official America – European diagnostic criteria for Sjogren’s disease [69]. Nonetheless, these patients all met the necessary clinical criteria and demonstrated autoreactivity by the presence of autoantibodies directed towards salivary and lacrimal gland antigens – the diagnostic criteria may have to expand to include additional autoantibodies. Furthermore, expression of SSA versus SP1/CA6/ PSP may denote different stages of disease and/or different types of Sjogren’s disease that are driven by different metabolic and immunologic abnormalities [27,66,68,70,71,72].
Whether metabolic abnormalities are a primary or secondary function in patients with Sjogren’s disease, treatment based on these abnormalities is helpful for the patients symptomatically and may lead to other new forms of therapy.
4. Materials and Methods
4.1. Patients
All the patients discussed in this manuscript were followed in the Immunology clinics of SUNY at Buffalo School of Medicine. They had clinical symptoms of xerostomia and xerophthalmia with positive Schirmer’s tests performed by their Ophthalmologists. Some patients had demonstration of decreased salivary flow. All patients had serologic testing for antibodies to SSA, SSB, salivary gland protein 1 (SP1), carbonic anhydrase 6 (CA6) and parotid secretory protein (PSP) as part of their routine medical care. Because all patients had complaints of fatigue, exercise intolerance, accelerated osteoarthritis and recurrent infections, genetic studies were obtained as part of their routine medical care. Twenty-seven percent of the patients had associated gastrointestinal dysmotility. The patients ranged in age from 21-81 years (mean 54.2 +/- 13.5 years). Eighty-nine percent of the patients were female.
4.2. Genetic Studies
Sequencing of the mitochondrial genome and whole exome sequencing was performed by GeneDx (Gaithersburg, MD).
5. Conclusions
Patient with Sjogren’s disease frequently have an underlying metabolic disorder that is responsible for some of the symptoms attributed to the disease. Treatment of the metabolic disorder leads to symptomatic improvement in the patients.
Author Contributions
Julian L. Ambrus Jr., took care of the patients, obtained the genetic studies and wrote the paper. Alexander Jacob helped with autoantibody analysis and reviewed the paper. Abhay Shukla performed the autoantibody studies and reviewed the paper.
Funding
These data were obtained from routine clinical care. No external funding was utilized.
Institutional Review Board Statement
The data were obtained from routine clinical care and did not involve identification of individual patients. No IRB approval was required.
Informed Consent Statement
The data were obtained from routine clinical care and did not involve identification of individual patients. No informed consent was required..
Data Availability Statement
All the data are included in this manuscript.
Acknowledgments
We acknowledge the nurses who helped with the care of these patients: Eileen Esposito and Amy Forsyth.
Conflicts of Interest
None of the authors had any conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
CA6 = carbonic anhydrase 6
SP1 = salivary gland protein 1
PSP = parotic secretory protein
SSA = Sjogren’s syndrome A = anti – Ro
SSB = Sjogren’s syndrome B = anti- LA
ATP = adenosine triphosphate
References
- Blanco, L. P., and M. J. Kaplan. 2023. Metabolic alterations of the immune system in the pathogenesis of autoimmune diseases. Plos Biology 21: 13. [CrossRef]
- Chavez, M. D., and H. M. Tse. 2021. Targeting Mitochondrial-Derived Reactive Oxygen Species in T Cell-Mediated Autoimmune Diseases. Frontiers in immunology 12: 14. [CrossRef]
- Clayton, S. A., L. MacDonald, M. Kurowska-Stolarska, and A. R. Clark. 2021. Mitochondria as Key Players in the Pathogenesis and Treatment of Rheumatoid Arthritis. Frontiers in immunology 12. [CrossRef]
- Freitag, J., L. Berod, T. Kamradt, and T. Sparwasser. 2016. Immunometabolism and autoimmunity. Immunology and Cell Biology 94: 925-934. [CrossRef]
- Huang, N., and A. Perl. 2018. Metabolism as a Target for Modulation in Autoimmune Diseases. Trends in Immunology 39: 562-576. [CrossRef]
- Mubariki, R., and Z. Vadasz. 2022. The role of B cell metabolism in autoimmune diseases. Autoimmunity reviews 21: 5. [CrossRef]
- Perl, A. 2017. Metabolic Control of Immune System Activation in Rheumatic Diseases. Arthritis & Rheumatology 69: 2259-2270. [CrossRef]
- Choi, S. C., A. A. Titov, R. Sivakumar, W. Li, and L. Morel. 2016. Immune Cell Metabolism in Systemic Lupus Erythematosus. Curr Rheumatol Rep 18: 66. [CrossRef]
- Lightfoot, Y. L., L. P. Blanco, and M. J. Kaplan. 2017. Metabolic abnormalities and oxidative stress in lupus. Current Opinion in Rheumatology 29: 442-449. [CrossRef]
- Monteith, A. J., J. M. Miller, J. M. Williams, K. Voss, J. C. Rathmell, L. J. Crofford, and E. P. Skaar. 2022. Altered Mitochondrial Homeostasis during Systemic Lupus Erythematosus Impairs Neutrophil Extracellular Trap Formation Rendering Neutrophils Ineffective at Combating Staphylococcus aureus. Journal of Immunology 208: 454-463. [CrossRef]
- Morel, L. 2017. Immunometabolism in systemic lupus erythematosus. Nature Reviews Rheumatology 13: 280-290. [CrossRef]
- Robinson, G. A., M. G. L. Wilkinson, and C. Wincup. 2022. The Role of Immunometabolism in the Pathogenesis of Systemic Lupus Erythematosus. Frontiers in immunology 12: 9. [CrossRef]
- Sharabi, A., and G. C. Tsokos. T cell metabolism: new insights in systemic lupus erythematosus pathogenesis and therapy. Nature Reviews Rheumatology. [CrossRef]
- Takeshima, Y., Y. Iwasaki, K. Fujio, and K. Yamamoto. 2019. Metabolism as a key regulator in the pathogenesis of systemic lupus erythematosus. Seminars in Arthritis and Rheumatism 48: 1142-1145. [CrossRef]
- Zhang, C. X., H. Y. Wang, L. Yin, Y. Y. Mao, and W. Zhou. 2020. Immunometabolism in the pathogenesis of systemic lupus erythematosus. J. Transl. Autoimmun. 3: 10. [CrossRef]
- Colafrancesco, S., E. Simoncelli, R. Priori, and M. Bombardieri. 2023. The pathogenic role of metabolism in Sjögren's syndrome. Clinical and Experimental Rheumatology 41: 2538-2546. [CrossRef]
- Luo, D. Y., L. Li, Y. C. Wu, Y. Yang, Y. L. Ye, J. W. Hu, Y. M. Gao, N. Y. Zeng, X. C. Fei, N. Li, and L. T. Jiang. 2023. Mitochondria-related genes and metabolic profiles of innate and adaptive immune cells in primary Sjogren's syndrome. Frontiers in immunology 14: 16. [CrossRef]
- Apaydin, H., C. K. Bicer, E. F. Yurt, M. A. Serdar, I. Dogan, and S. Erten. Elevated Kynurenine Levels in Patients with Primary Sjogren's Syndrome. Lab. Med.: 7.
- Blokland, S. L. M., M. R. Hillen, C. G. K. Wichers, M. Zimmermann, A. A. Kruize, T. Radstake, J. C. A. Broen, and J. A. G. van Roon. 2019. Increased mTORC1 activation in salivary gland B cells and T cells from patients with Sjogren's syndrome: mTOR inhibition as a novel therapeutic strategy to halt immunopathology? RMD Open 5: e000701. [CrossRef]
- Katsiougiannis, S., A. Stergiopoulos, K. Moustaka, S. Havaki, M. Samiotaki, G. Stamatakis, R. Tenta, and F. N. Skopouli. 2023. Salivary gland epithelial cell in Sjogren?s syndrome: Metabolic shift and altered mitochondrial morphology toward an innate immune cell function. Journal of Autoimmunity 136: 8. [CrossRef]
- Li, N., Y. Li, J. Hu, Y. Wu, J. Yang, H. Fan, L. Li, D. Luo, Y. Ye, Y. Gao, H. Xu, W. Hai, and L. Jiang. 2022. A Link Between Mitochondrial Dysfunction and the Immune Microenvironment of Salivary Glands in Primary Sjogren's Syndrome. Front Immunol 13: 845209. [CrossRef]
- Pagano, G., G. Castello, and F. V. Pallardo. 2013. Sjogren's syndrome-associated oxidative stress and mitochondrial dysfunction: prospects for chemoprevention trials. Free Radic Res 47: 71-73. [CrossRef]
- Wadan, A. S., M. A. Ahmed, A. H. Ahmed, D. E. Ellakwa, N. H. Elmoghazy, and A. Gawish. 2024. The Interplay of Mitochondrial Dysfunction in Oral Diseases: Recent Updates in Pathogenesis and Therapeutic Implications. Mitochondrion 78: 21. [CrossRef]
- Ambrus, J. L., A. Jacob, G. A. Weisman, and J. He. 2018. Metabolic changes in the evolution of Sjogren's syndrome in a mouse model. Clinical and Experimental Rheumatology 36: S301-S301.
- Suresh, L., J. Ambrus, L. Shen, and S. Vishwanath. 2014. Metabolic Disorders Causing Fatigue in Sjogren's Syndrome. Arthritis & Rheumatology 66: S1113-S1113.
- Bax, K., P. J. Isackson, M. Moore, and J. L. Ambrus. 2020. Carnitine Palmitoyl Transferase Deficiency in a University Immunology Practice. Current rheumatology reports 22. [CrossRef]
- De Langhe, E., X. Bossuyt, L. Shen, K. Malyavantham, J. L. Ambrus, and L. Suresh. 2017. Evaluation of Autoantibodies in Patients with Primary and Secondary Sjogren's Syndrome. Open Rheumatol J 11: 10-15. [CrossRef]
- Everett, S., S. Vishwanath, V. Cavero, L. Shen, L. Suresh, K. Malyavantham, N. Lincoff-Cohen, and J. L. Ambrus, Jr. 2017. Analysis of novel Sjogren's syndrome autoantibodies in patients with dry eyes. BMC Ophthalmol 17: 20. [CrossRef]
- Jin, Y., J. Li, J. Chen, M. Shao, R. Zhang, Y. Liang, X. Zhang, X. Zhang, Q. Zhang, F. Li, Y. Cheng, X. Sun, J. He, and Z. Li. 2019. Tissue-Specific Autoantibodies Improve Diagnosis of Primary Sjogren's Syndrome in the Early Stage and Indicate Localized Salivary Injury. J Immunol Res 2019: 3642937. [CrossRef]
- Karakus, S., A. N. Baer, and E. K. Akpek. 2019. Clinical Correlations of Novel Autoantibodies in Patients with Dry Eye. Journal of Immunology Research. [CrossRef]
- Tarnopolsky, M. A. 2008. The mitochondrial cocktail: rationale for combined nutraceutical therapy in mitochondrial cytopathies. Adv Drug Deliv Rev 60: 1561-1567. [CrossRef]
- Garrido-Maraver, J., M. D. Cordero, M. Oropesa-Avila, A. F. Vega, M. de la Mata, A. D. Pavon, E. Alcocer-Gomez, C. P. Calero, M. V. Paz, M. Alanis, I. de Lavera, D. Cotan, and J. A. Sanchez-Alcazar. 2014. Clinical applications of coenzyme Q10. Frontiers in Bioscience-Landmark 19: 619-633.
- Nicolson, G. L. 2014. Mitochondrial dysfunction and chronic disease: treatment with natural supplements. Altern Ther Health Med 20 Suppl 1: 18-25.
- Glover, E. I., J. Martin, A. Maher, R. E. Thornhill, G. R. Moran, and M. A. Tarnopolsky. 2010. A RANDOMIZED TRIAL OF COENZYME Q(10) IN MITOCHONDRIAL DISORDERS. Muscle & Nerve 42: 739-748. [CrossRef]
- Barcelos, I., E. Shadiack, R. D. Ganetzky, and M. J. Falk. 2020. Mitochondrial medicine therapies: rationale, evidence, and dosing guidelines. Current Opinion in Pediatrics 32: 707-718. [CrossRef]
- Bhattacharjee, A., S. K. Prasad, O. Banerjee, S. Singh, A. Banerjee, A. Bose, S. Pal, B. K. Maji, and S. Mukherjee. 2018. Targeting mitochondria with folic acid and vitamin B-12 ameliorates nicotine mediated islet cell dysfunction. Environmental Toxicology 33: 988-1000. [CrossRef]
- Avula, S., S. Parikh, S. Demarest, J. Kurz, and A. Gropman. 2014. Treatment of Mitochondrial Disorders. Current Treatment Options in Neurology 16. [CrossRef]
- Ezerina, D., Y. Takano, K. Hanaoka, Y. Urano, and T. P. Dick. 2018. N-Acetyl Cysteine Functions as a Fast-Acting Antioxidant by Triggering Intracellular H2S and Sulfane Sulfur Production. Cell Chemical Biology 25: 447-+. [CrossRef]
- Cruzat, V., M. Macedo Rogero, K. Noel Keane, R. Curi, and P. Newsholme. 2018. Glutamine: Metabolism and Immune Function, Supplementation and Clinical Translation. Nutrients 10. [CrossRef]
- Bornstein, R., M. T. Mulholland, M. Sedensky, P. Morgan, and S. C. Johnson. 2023. Glutamine metabolism in diseases associated with mitochondrial dysfunction. Mol. Cell. Neurosci. 126: 12. [CrossRef]
- Hannah, W. B., T. G. J. Derks, M. L. Drumm, S. C. Gruenert, P. S. Kishnani, and J. Vissing. 2023. Glycogen storage diseases. Nature Reviews Disease Primers 9: 23. [CrossRef]
- Kishnani, P. S., A. A. Beckemeyer, and N. J. Mendelsohn. 2012. The new era of Pompe disease: Advances in the detection, understanding of the phenotypic spectrum, pathophysiology, and management. American Journal of Medical Genetics Part C-Seminars in Medical Genetics 160C: 1-7.
- Kley, R. A., M. A. Tarnopolsky, and M. Vorgerd. 2008. Creatine treatment in muscle disorders: a meta-analysis of randomised controlled trials. J Neurol Neurosurg Psychiatry 79: 366-367. [CrossRef]
- Llavero, F., A. A. Sastre, M. L. Montoro, P. Galvez, H. M. Lacerda, L. A. Parada, and J. L. Zugaza. 2019. McArdle Disease: New Insights into Its Underlying Molecular Mechanisms. International Journal of Molecular Sciences 20. [CrossRef]
- Meena, N. K., and N. Raben. 2020. Pompe Disease: New Developments in an Old Lysosomal Storage Disorder. Biomolecules 10. [CrossRef]
- Vissing, J., and R. G. Haller. 2003. The effect of oral sucrose on exercise tolerance in patients with McArdle's disease. N Engl J Med 349: 2503-2509. [CrossRef]
- Raben, N., A. Wong, E. Ralston, and R. Myerowitz. 2012. Autophagy and mitochondria in Pompe disease: Nothing is so new as what has long been forgotten. American Journal of Medical Genetics Part C-Seminars in Medical Genetics 160C: 13-21. [CrossRef]
- Mishra, K., and O. Kakhlon. 2024. Mitochondrial Dysfunction in Glycogen Storage Disorders (GSDs). Biomolecules 14: 24. [CrossRef]
- Ambrus, J. J., P. J. Isackson, M. Moore, J. Butsch, and L. Balos. 2020. Investigating Fatigue and Exercise Inotolerance in a University Immunology Clinic. Archives of Rheumatology and Arthritis Research 1: 1-8. [CrossRef]
- Barrera, M. J., S. Aguilera, I. Castro, P. Carvajal, D. Jara, C. Molina, S. Gonzalez, and M. J. Gonzalez. 2021. Dysfunctional mitochondria as critical players in the inflammation of autoimmune diseases: Potential role in Sjo & uml;gren & rsquo;s syndrome. Autoimmunity reviews 20: 12.
- Ryo, K., H. Yamada, Y. Nakagawa, Y. Tai, K. Obara, H. Inoue, K. Mishima, and I. Saito. 2006. Possible involvement of oxidative stress in salivary gland of patients with Sjogren's syndrome. Pathobiology 73: 252-260. [CrossRef]
- Norheim, K. B., S. Le Hellard, G. Nordmark, E. Harboe, L. Goransson, J. G. Brun, M. Wahren-Herlenius, R. Jonsson, and R. Omdal. 2014. A possible genetic association with chronic fatigue in primary Sjogren's syndrome: a candidate gene study. Rheumatology International 34: 191-197. [CrossRef]
- Amaya-Uribe, L., M. Rojas, G. Azizi, J. M. Anaya, and M. E. Gershwin. 2019. Primary immunodeficiency and autoimmunity: A comprehensive review. Journal of Autoimmunity 99: 52-72. [CrossRef]
- Maslinska, M., and K. Kostyra-Grabczak. 2022. The role of virus infections in Sjogren's syndrome. Frontiers in immunology 13: 18. [CrossRef]
- Costagliola, G., S. Cappelli, and R. Consolini. 2021. Autoimmunity in Primary Immunodeficiency Disorders: An Updated Review on Pathogenic and Clinical Implications. Journal of Clinical Medicine 10: 20. [CrossRef]
- Zheng, X. Q., and A. H. Sawalha. The Role of Oxidative Stress in Epigenetic Changes Underlying Autoimmunity. Antioxidants & redox signaling: 18. [CrossRef]
- Sharma, R., R. M. Smolkin, P. Chowdhury, K. C. Fernandez, Y. Kim, M. Cols, W. Alread, W. F. Yen, W. Hu, Z. M. Wang, S. Violante, R. Chaligne, M. O. Li, J. R. Cross, and J. Chaudhuri. 2023. Distinct metabolic requirements regulate B cell activation and germinal center responses. Nature Immunology: 33. [CrossRef]
- Tomaszewicz, M., A. Ronowska, M. Zielinski, A. Jankowska-Kulawy, and P. Trzonkowski. 2023. T regulatory cells metabolism: The influence on functional properties and treatment potential. Frontiers in immunology 14: 11. [CrossRef]
- Abboud, G., S. C. Choi, X. J. Zhang, Y. P. Park, N. Kanda, L. Zeumer-Spataro, M. Terrell, X. Y. Teng, K. Nundel, M. J. Shlomchik, and L. Morel. 2023. Glucose Requirement of Antigen-Specific Autoreactive B Cells and CD4+T Cells. Journal of Immunology 210: 377-388. [CrossRef]
- Dimeloe, S., A. V. Burgener, J. Grahlert, and C. Hess. 2017. T-cell metabolism governing activation, proliferation and differentiation; a modular view. Immunology 150: 35-44. [CrossRef]
- Yin, Y., S. C. Choi, Z. Xu, D. J. Perry, H. Seay, B. P. Croker, E. S. Sobel, T. M. Brusko, and L. Morel. 2015. Normalization of CD4+ T cell metabolism reverses lupus. Sci Transl Med 7: 274ra218. [CrossRef]
- Yu, H. Y., N. Jacquelot, and G. T. Belz. 2022. Metabolic features of innate lymphoid cells. Journal of Experimental Medicine 219: 15. [CrossRef]
- Shiraz, A. K., E. J. Panther, and C. M. Reilly. 2022. Altered Germinal-Center Metabolism in B Cells in Autoimmunity. Metabolites 12: 16. [CrossRef]
- Buck, M. D., D. O'Sullivan, and E. L. Pearce. 2015. T cell metabolism drives immunity. Journal of Experimental Medicine 212: 1345-1360.
- Sarkar, A., D. Chakraborty, S. Malik, S. Mann, P. Agnihotri, M. Monu, V. Kumar, and S. Biswas. 2024. Alpha-Taxilin: A Potential Diagnosis and Therapeutics Target in Rheumatoid Arthritis Which Interacts with Key Glycolytic Enzymes Associated with Metabolic Shifts in Fibroblast-Like Synoviocytes. Journal of Inflammation Research 17: 10027-10045. [CrossRef]
- Shen, L., L. Suresh, K. Malyavantham, P. Kowal, J. X. Xuan, M. J. Lindemann, and J. L. Ambrus. 2013. Different Stages of Primary Sjogren's Syndrome Involving Lymphotoxin and Type 1 IFN. Journal of Immunology 191: 608-613. [CrossRef]
- Shen, L., C. Gao, L. Suresh, Z. Xian, N. Song, L. D. Chaves, M. Yu, and J. L. Ambrus, Jr. 2016. Central role for marginal zone B cells in an animal model of Sjogren's syndrome. Clin Immunol 168: 30-36. [CrossRef]
- Jacob, A., J. He, A. Peck, A. Jamil , V. Bunya, J. Alexander, and A. J. JL. 2025. Metabolic changes during evolution of Sjogren’s in both an animal model and human patients. Heliyon 11: e41082. [CrossRef]
- Shiboski, C. H., S. C. Shiboski, R. Seror, L. A. Criswell, M. Labetoulle, T. M. Lietman, A. Rasmussen, H. Scofield, C. Vitali, S. J. Bowman, X. Mariette, and W. Int Sjogren's Syndrome Criteria. 2017. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjogren's Syndrome A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis & Rheumatology 69: 35-45.
- Sheppard, J. D., M. C. Jasek, K. Malyavantham, L. Suresh, J. L. Ambrus, and D. Pardo. 2015. Two Year Results with IgG, IgA and IgM Antibody Specific to SP-1, PSP and CA-6 early Novel Antigens Compared to Classic Biomarkers in 2306 Dry Eye Patients. Scandinavian Journal of Immunology 81: 348-349.
- Suresh, L., K. Malyavantham, L. Shen, and J. L. Ambrus. 2015. Investigation of novel autoantibodies in Sjogren's syndrome utilizing Sera from the Sjogren's international collaborative clinical alliance cohort. Bmc Ophthalmology 15. [CrossRef]
- Shen, L., E. K. Kapsogeorgou, M. X. Yu, L. Suresh, K. Malyavantham, A. G. Tzioufas, and J. L. Ambrus. 2014. Evaluation of salivary gland protein 1 antibodies in patients with primary and secondary Sjogren's syndrome. Clinical Immunology 155: 42-46. [CrossRef]
Figure 1.
Autoantibodies Identified in Patients in this Study. Figure Legend: This figure demonstrates the number of patients with particular autoantibodies included in this study. SP1 = salivary protein 1, CA6 = carbonic anhydrase 6, PSP = parotid secretory protein, SS = Sjogren’s syndrome.
Figure 1.
Autoantibodies Identified in Patients in this Study. Figure Legend: This figure demonstrates the number of patients with particular autoantibodies included in this study. SP1 = salivary protein 1, CA6 = carbonic anhydrase 6, PSP = parotid secretory protein, SS = Sjogren’s syndrome.
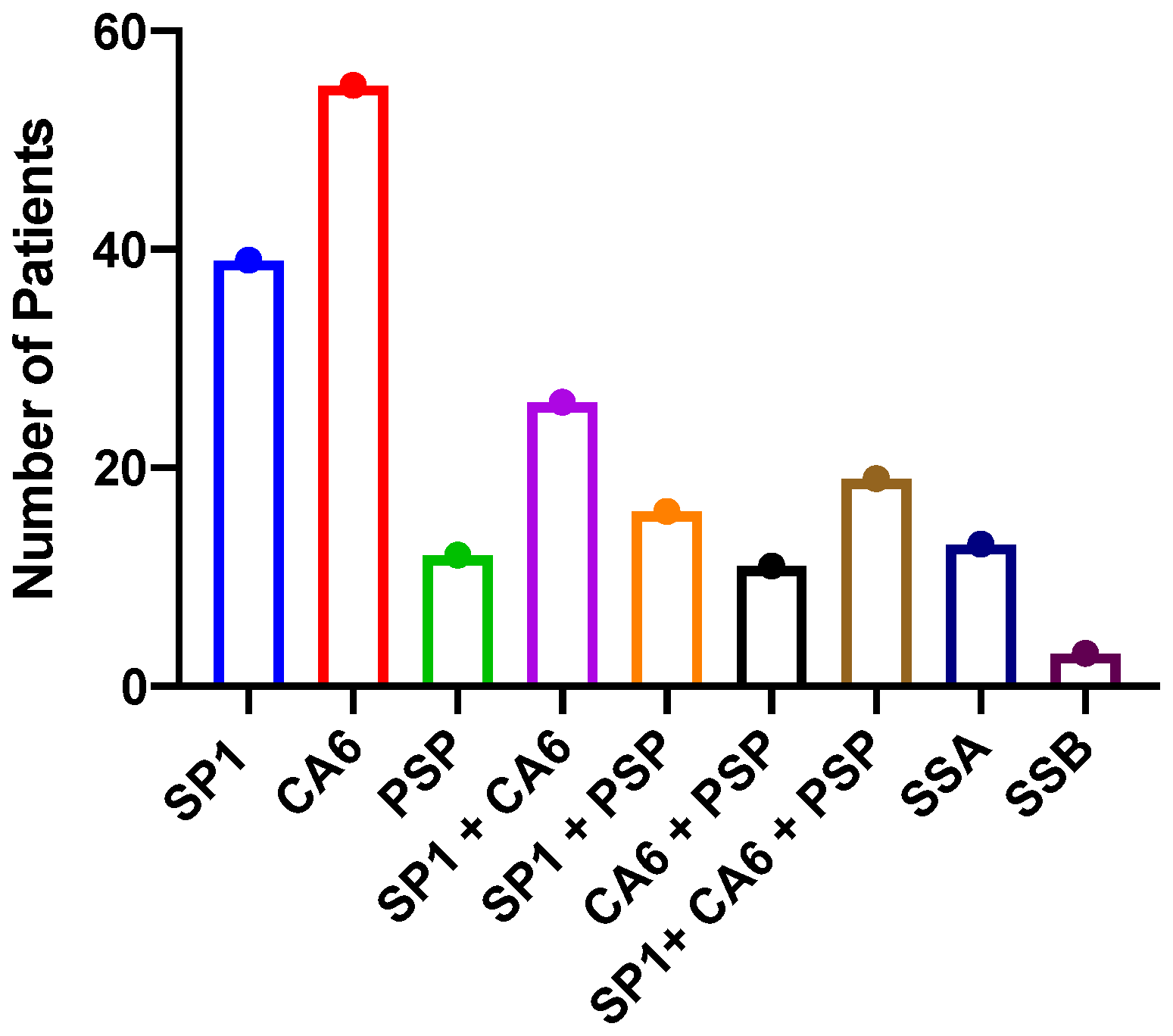
Figure 2.
Mutations in Genes Involved with Metabolism in Patients with Sjogren’s Disease. Figure Legend: This figure demonstrates the number of patients with particular mutations in genes involved with metabolism. MRC = mitochondrial respiratory chain.MT = mitochondrial, Mito depletion genes included POLG, MCME, RRMP8 and thymidine kinase. Glycogen storage diseases included Pompe, Forber – Cori, McArdle’s, phosphofructokinase deficiency and lactate dehydrogenase deficiency.
Figure 2.
Mutations in Genes Involved with Metabolism in Patients with Sjogren’s Disease. Figure Legend: This figure demonstrates the number of patients with particular mutations in genes involved with metabolism. MRC = mitochondrial respiratory chain.MT = mitochondrial, Mito depletion genes included POLG, MCME, RRMP8 and thymidine kinase. Glycogen storage diseases included Pompe, Forber – Cori, McArdle’s, phosphofructokinase deficiency and lactate dehydrogenase deficiency.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



