Submitted:
18 March 2025
Posted:
19 March 2025
You are already at the latest version
Abstract
Introduction: Inlet Patch (IP) is a congenital anomaly characterized by gastric heterotopia in the cervical esophagus. While extensively described in adults, it remains poorly characterized in pediatric populations.Material and Methods: This retrospective, single-center study included all pediatric patients (0–14 years) diagnosed with IP between 2018 and 2025. Sociodemographic and clinical data were collected. A blinded pathologist assessed the presence and severity of gastritis within the IP.Results: Nine patients (median age: 12 years) were included, 78% male. Cervical esophageal symptoms were identified in 67%, primarily dysphagia and gastroesophageal reflux disease-related complaints, although concomitant conditions such as eosinophilic esophagitis were frequently present. Endoscopic examination revealed characteristic well-demarcated salmon-red plaques in all patients, with multiple lesions observed in three cases. Histology confirmed gastric heterotopia with varying degrees of chronic inflammation in all cases. A strong correlation was observed between the severity of gastritis in the stomach, the severity of inflammation in the IP, and the presence of H. pylori, with 75% of patients with moderate-to-severe IP inflammation also exhibiting gastric H. pylori-associated gastritis. All patients except one received proton pump inhibitors, and symptoms improved in all cases.Conclusions: A thorough and targeted examination of the cervical esophagus significantly increased IP detection at our center, with most cases (88%) being diagnosed in the last 12 months. While mostly asymptomatic and incidental, IP can be symptomatic. In this case series, we found a correlation between the severity of inflammation in the IP, the severity of gastritis and the presence of H. pylori. Further studies are needed to define pediatric IP clinical significance and optimal management.
Keywords:
pediatric
; inlet patch
; endoscopy
; inflammation
; gastritis
; Helicobacter pylori
; dysphagia
Introduction
Inlet Patch (IP) is an anomaly characterized by gastric heterotopia in the cervical esophagus [1,2,3]. It is considered an infrequent pathology, especially in pediatric populations, although the literature regarding its prevalence is inconsistent [1,2,3,4,5,6,7].
IP etiology is presumed to be congenital, resulting from abnormal epithelial development during embryogenesis [8,9]. Clinically, in most cases, it is an asymptomatic lesion that is incidentally diagnosed during an upper gastrointestinal endoscopy (UGIE) performed for other reasons. However, a wide range of symptoms associated with the lesion has been described to varying degrees, including dyspepsia, dysphagia, esophageal strictures or membranes, gastroesophageal reflux, bleeding, and even respiratory symptoms such as chronic bronchitis or laryngospasm [9,10,11,12,13].
From an endoscopic perspective, it is a distinctive and easily identifiable lesion, appearing as a well-demarcated pink or salmon-colored patch. It is typically located in the upper third of the esophagus, just below the upper esophageal sphincter (UES). However, it has also been described, albeit exceptionally, in other locations, such as the mid-esophagus [14].
Although there is general agreement that incidentally detected IP should not be treated in asymptomatic patients, evidence on the management of symptomatic IP remains scarce. Proton pump inhibitors (PPIs) are considered the first-line treatment [1,2,3], as they are effective in most cases, while endoscopic therapies, such as argon plasma coagulation, are reserved for refractory cases [15]. This study aims to characterize pediatric cases diagnosed with IP at our center from 2018 to 2025.
Material and Methods
This retrospective, single-center study included all pediatric patients (0–14 years) diagnosed with IP at our institution between 2018 and 2025. Two researchers collected and anonymized the patients’ sociodemographic and clinical data. A blinded pathologist evaluated all biopsies and classified the degree of gastritis using a qualitative scale: absence of gastritis, mild chronic gastritis, moderate to severe chronic gastritis, and acute gastritis. A descriptive analysis was performed. The study was approved by our Institutional Review Board (code 24227), and informed consent was obtained from all legal guardians before inclusion. It was conducted following the principles of the Declaration of Helsinki (2013).
Results
Nine patients were included, with a median age at diagnosis of 12 years (range: 6–14). Seven were male (78%), and two were female (22%).
Regarding medical history, four patients (44%) had a prior diagnosis of eosinophilic esophagitis (EoE). Among them, one also had a concomitant diagnosis of celiac disease (CD), while another had a serological and genetic profile compatible with CD but did not meet the ESPGHAN 2012 criteria nor had histopathological confirmation of CD. Additionally, one patient in the series had insulin-resistant type 1 diabetes mellitus, and another had a previous diagnosis of gastroesophageal reflux (GER) secondary to H. pylori infection. Two patients had no relevant medical history.
Cervical esophageal symptoms were identified in six cases (67%). The most common symptoms were chronic dysphagia (60%) and GER-related symptoms (60%). Two of these six patients (40%) had experienced at least one prior episode of food impaction. When considering symptomatic IP, those in which there were no gastrointestinal comorbidities or those in which cervical esophageal symptoms were present despite the absence of underlying disease activity (e.g., cases where IP was diagnosed during an UGIE follow-up for EoE with biopsies showing no active EoE), we identified three patients (33%) with symptoms potentially attributable to PI (Case 1, Case 8, Case 9). In two of these cases, the predominant symptom was dysphagia, while in the other case, it was gastroesophageal reflux disease (GERD)-related symptoms. IP symptoms (subacute dysphagia) in the absence of other gastrointestinal comorbidities were identified in only one case (20%) [12]. Notably, this patient had an unusually extensive IP, covering a large portion of the esophageal circumference (Figure 1, Case 1).
In all cases, a distinct lesion was identified at the level of the cervical esophagus, just below the upper esophageal sphincter. The lesion appeared as a well-demarcated, salmon-red plaque (Figure 1). Lesion size and the percentage of the affected esophageal circumference varied, with multiple IP lesions observed in three cases (Case 1, Case 2, Case 6). A nodular or villous pattern was sometimes present at the center of the plaque (Case 1, Case 3, Case 6). In nearly all cases, the IP exhibited friability upon contact with the endoscope and during biopsy sampling, with a tendency to bleed after endoscopic manipulation. Additionally, endoscopic findings of gastric antritis were identified in two cases (22%), while endoscopic findings suggestive of EoE were observed in four cases (44%).
Histopathological analysis of all cases confirmed gastric heterotopia in the biopsied lesions, establishing the diagnosis of IP (Figure 2). The proportion of specialized gastric epithelium (with oxyntic glands) and non-specialized gastric epithelium (with mucinous glands) varied across biopsies. Regarding the degree of inflammation, all cases exhibited different levels of chronic inflammation. Chronic inflammation was classified as "mild" in five cases (56%) and "moderate-to-severe" in four cases (44%). Among the latter, H. pylori was identified in gastric biopsies from three patients (75%), with one case (25%) also testing positive for H. pylori at the IP site using Giemsa staining. Acute inflammation was not identified histologically in any case. No cytological atypia, dysplasia, or malignancy was observed in the analyzed cases.
Regarding treatment, all patients except one received oral proton pump inhibitors (PPI). PPI therapy was indicated even in asymptomatic cases due to concomitant conditions such as EoE or H. pylori-associated gastritis. Patients diagnosed with H. pylori gastritis underwent antibiotic treatment with subsequent confirmation of eradication. Additionally, three patients received dietary modifications as part of their management. All patients responded favorably to PPI therapy, with symptom improvement or complete resolution. None exhibited refractory symptoms or required endoscopic ablation of the IP.
The duration of follow-up varied among patients; however, eight of the nine cases were diagnosed within the past 12 months, while one was diagnosed seven years ago. Table 1 presents the main sociodemographic and clinical characteristics of the patients included in the study.
Discussion
The present study reports a series of nine pediatric patients diagnosed with IP, providing a comprehensive characterization from clinical, endoscopic, and histological perspectives.
Regarding the prevalence of Inlet Patch (IP), recent series have reported an endoscopic prevalence rate of 1.4% [1]. However, significant variability exists among reported rates [1,4], with some specialized centers focused on adult esophageal pathology documenting an endoscopic prevalence of up to 14.8% [5]. Although outdated, pediatric autopsy series have reported even higher prevalence rates, reaching 21% [6]. A plausible explanation for this discrepancy is the underdiagnosis of IP in cases where a thorough and targeted evaluation of the cervical esophagus is not performed during UGIE. In this regard, recent meta-analyses have demonstrated that studies in which endoscopists specifically focused on detecting this lesion reported a higher pooled prevalence of IP [7]. The endoscopists’ expertise in this series, who systematically examined the cervical esophageal region in all patients, likely contributed to a higher number of diagnoses in a relatively short period, potentially identifying cases that might have otherwise been missed. Given that this is a relatively unknown endoscopic finding, selectively located in a region that is challenging to explore and not routinely assessed systematically, we believe that many patients with IP remain undiagnosed.
Immunohistochemical studies have demonstrated that IP and Barrett’s esophagus (BE) share a similar expression profile for Alcian blue pH 2.5/PAS [8], high iron diamine/Alcian blue pH 2.5 [8], cytokeratins 7/20 [9], and mucin-secreting glycoproteins (MUC) [9]. This profile differs from that observed in the ectopic gastric mucosa of Meckel’s diverticulum [8] and healthy antral mucosa [9]. These findings suggest that both IP and BE may originate from submucosal esophageal glands, which are particularly abundant at both ends of the esophagus [9]. Based on this hypothesis, one proposed etiopathogenic mechanism for IP is focal upper esophageal mucosal misdevelopment [9]. This theory may also be relevant to the malignant potential of IP through the classic BE metaplasia-dysplasia-carcinoma sequence, as cases of adenocarcinoma arising from IP have been reported [16,17,18,19,20,21,22]. Further supporting this hypothesis, some studies have documented cases of synchronous adenocarcinoma arising from cervical IP and BE-related dysplasia [23].
It is also important to note that the definition of BE varies geographically. In Asian studies, BE is often used interchangeably with gastric metaplasia. In contrast, European and Western studies refer specifically to intestinal metaplasia, which carries a higher risk of progression to adenocarcinoma. The fact that Asian studies establish a diagnosis of BE based solely on the presence of columnar epithelium in the esophagus may contribute to an overestimation of BE cases. From an endoscopic perspective, recent studies have reported concomitant BE in up to 17% of patients with IP [24]. To the best of our knowledge, malignant transformation of IP has not been documented in pediatric patients, likely due to the relatively short pediatric period within a lifetime and the low incidence of BE and esophageal neoplasms in childhood. However, given the unclear malignant potential of IP, this possibility should not be disregarded. Further studies are required to determine whether follow-up protocols for IP are necessary.
In our patient series, a significant proportion had comorbid conditions, including EoE, CD, and Insulin-dependent type 1 diabetes mellitus. However, there is a considerable selection bias, as routine UGIE is not performed in healthy and asymptomatic pediatric patients. Establishing a causal relationship between these conditions and IP is not feasible, and we believe that IP was most likely an incidental finding in patients undergoing UGIE for other indications. The same consideration applies to H. pylori-related gastritis, another reason for sometimes performing a UGIE.
Three of our patients exhibited symptoms attributable to IP, while six did not. Determining whether IP solely causes symptoms is challenging, particularly in patients with concomitant conditions, such as EoE, which can present with similar clinical manifestations. The most illustrative case in our series is Case 1, in which the patient had no gastrointestinal comorbidities. In two other cases, gastrointestinal comorbidities were present; however, the absence of EoE activity in the diagnostic UGIE for IP (Case 9) and the lack of other gastrointestinal abnormalities that could justify the symptoms(Case 8) suggest that their cervical esophageal symptoms may be attributed to IP. Nevertheless, it is essential to acknowledge that symptom attribution in these two cases remains challenging.
Some studies have attempted to demonstrate the potential role of IP in symptom development through acid secretion monitoring. In 1985, Jabbari et al. [25] reported a decrease in pH at the IP site following intravenous administration of pentagastrin, though this was only observed in cases with large IPs. Similarly, in 2001, Kim et al. [26] described a patient with pharyngeal symptoms in whom 24-hour ambulatory pH monitoring demonstrated acid secretion in the cervical esophagus, with symptom improvement following PPI treatment. In our series, only one patient underwent 24-hour pH monitoring, which yielded normal results.
A notable finding in our series was that all IP cases presented some degree of chronic gastritis, with some reaching moderate to severe levels. Interestingly, a strong correlation was observed between the severity of gastritis in the stomach, the severity of gastritis in the IP, and the presence of H. pylori. Specifically, four patients exhibited moderate to severe gastritis in the IP, and in three of them (75%), the same severity was confirmed in the gastric chamber, accompanied by H. pylori infection. Additionally, in one of these cases, H. pylori was detected within the IP tissue through Giemsa staining. However, the pathological significance of this finding remains unclear.
Several mechanisms could contribute to the development of chronic gastritis in IP, including repeated mechanical trauma due to its location in a high-transit region during swallowing (both saliva and food). It should also be considered that the IP may act as a potential reservoir for H. pylori. Further studies systematically comparing the degree of gastritis in IP and the gastric chamber are necessary to elucidate this aspect. Similarly, future research should explore the relationship between IP and H. pylori regarding prevalence, therapeutic response, and associated symptoms.
Additionally, we identified both types of gastric mucosa within the IP lesions. However, we could not assess their relative proportions due to limitations, including the small tissue samples obtained from endoscopic biopsies and the potential heterogeneous epithelial distribution within the IP. We hypothesize that certain lesion areas may predominantly contain oxyntic glands (gastric corpus-type epithelium), while others may be enriched with mucin-secreting glands (gastric antrum-type epithelium). Investigating this further in living patients is highly challenging; however, autopsy studies, which allow for a comprehensive examination of the entire IP lesion, could provide valuable insights.
IP remains an underdiagnosed and poorly characterized entity in pediatric populations. It is likely congenital in origin and, while often asymptomatic, may occasionally be associated with clinical manifestations. In most cases within our series, IP was an incidental finding during UGIE, and most patients had concomitant gastrointestinal conditions. Chronic inflammation was present in all reported cases.
Reporting additional case series with detailed endoscopic and histopathological correlation is essential to further our understanding of this malformation’s etiopathogenesis, pathophysiology, diagnosis, treatment, and prognosis.
Author Contributions
JAM: Conceptualization and study design; literature search and selection; data curation and extraction; formal analysis; investigation; methodology; project administration; resources; validation; visualization; writing – original draft; writing – review and editing. SSA: Data curation and extraction; formal analysis; investigation; methodology; project administration; resources; validation; visualization; writing – review and editing. AHM: literature search and selection; data curation and extraction; writing – review and editing. CIB: Resources; investigation; writing – review and editing. AFG: writing – review and editing.
Funding
This review did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors, and none of the authors has external funding to declare.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
Our center’s Institutional Review Board reviewed and approved this study under code 24227. Before the submission of this article, verbal and written informed consent was obtained from the patients’ legal guardians. This study was conducted following the principles of the Helsinki Declaration (2013).
Statement of Availability of the Data Used During the Study
The data used to carry out this study are available upon reasonable request from the corresponding author.
References
- Rodríguez-Martínez A, Salazar-Quero JC, Tutau-Gómez C, Espín-Jaime B, Rubio-Murillo M, Pizarro-Martín A. Heterotopic gastric mucosa of the proximal oesophagus (inlet patch): endoscopic prevalence, histological and clinical characteristics in paediatric patients. Eur J Gastroenterol Hepatol. 2014, 26, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Georges A, Coopman S, Rebeuh J, Molitor G, Rebouissoux L, Dabadie A, Kalach N, Lachaux A, Michaud L. Inlet patch: clinical presentation and outcome in children. J Pediatr Gastroenterol Nutr. 2011, 52, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo G, Cremon C, Bertelli L, Oliva S, De Giorgio R, Pagano N. Esophageal Inlet Patch: An Under-Recognized Cause of Symptoms in Children. J Pediatr. 2016, 176, 99–104.e1. [Google Scholar] [CrossRef] [PubMed]
- Borhan-Manesh F, Farnum JB. Incidence of heterotopic gastric mucosa in the upper oesophagus. Gut. 1991, 32, 968–972. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Akar T, Aydın S. The true prevalence of cervical inlet patch in a specific center dealing with esophageal diseases. Eur Rev Med Pharmacol Sci. 2022, 26, 3127–3131. [Google Scholar] [CrossRef] [PubMed]
- Variend S, Howat AJ. Upper oesophageal gastric heterotopia: a prospective necropsy study in children. J Clin Pathol. 1988, 41, 742–745. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yin Y, Li H, Feng J, Zheng K, Yoshida E, Wang L, Wu Y, Guo X, Shao X, Qi X. Prevalence and Clinical and Endoscopic Characteristics of Cervical Inlet Patch (Heterotopic Gastric Mucosa): A Systematic Review and Meta-Analysis. J Clin Gastroenterol. 2022, 56, e250–e262. [Google Scholar] [CrossRef] [PubMed]
- Bogomoletz WV, Geboes K, Feydy P, et al. Mucin histochemistry of heterotopic gastric mucosa of the upper esophagus in adults: possible pathogenic implications. Hum Pathol. 1988, 19, 1301–1306. [Google Scholar] [CrossRef]
- Lauwers GY, Mino M, Ban S, Forcione D, Eatherton DE, Shimizu M, Sevestre H. Cytokeratins 7 and 20 and mucin core protein expression in esophageal cervical inlet patch. Am J Surg Pathol. 2005, 29, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Meliț LE, Dincă AL, Borka Balas R, Mocanu S, Mărginean CO. Not Every Dyspepsia Is Related to Helicobacter pylori-A Case of Esophageal Inlet Patch in a Female Teenager. Children (Basel). 2023, 10, 229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trippel M, Casaulta C, Sokollik C. Heterotopic gastric mucosa: Esophageal inlet patch in a child with chronic bronchitis. Dig Endosc. 2016, 28, 688. [Google Scholar] [CrossRef] [PubMed]
- Fernández-García A, Sáez Álvarez S, González-Lamuño Sanchis C, Iglesias Blázquez C, Rodríguez Ruiz M, Arredondo Montero J. Esophageal inlet patch in a 7-year-old girl with subacute dysphagia. Pediatr Neonatol. 2024, 65, 603–604. [Google Scholar] [CrossRef] [PubMed]
- Macha S, Reddy S, Rabah R, Thomas R, Tolia V. Inlet patch: heterotopic gastric mucosa--another contributor to supraesophageal symptoms? J Pediatr. 2005, 147, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto K, Shibagaki K, Nonomura S, Sumi S, Fukuda N, Takahashi Y, Kotani S, Okimoto E, Oshima N, Kawashima K, Ishimura N, Ishihara S. Heterotopic Gastric Mucosa in Middle Esophagus Complicated with Esophageal Ulcers. Intern Med. 2022, 61, 2735–2740. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alberty JB, Chanis R, Khoshoo V. Symptomatic gastric inlet patches in children treated with argon plasma coagulation: a case series. J Interv Gastroenterol. 2012, 2, 91–93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ajmal S, Young JS, Ng T. Adenocarcinoma arising from cervical esophageal gastric inlet patch. J Thorac Cardiovasc Surg. 2015, 149, 1664–1665. [Google Scholar] [CrossRef] [PubMed]
- Probst A, Schaller T, Messmann H. Adenocarcinoma arising from ectopic gastric mucosa in an esophageal inlet patch: treatment by endoscopic submucosal dissection. Endoscopy. 2015, 47 (Suppl. 1), E337–E338. [Google Scholar] [CrossRef] [PubMed]
- Carrie, A. Adenocarcinoma of the upper end of the esophagus arising from ectopic gastric epithelium. Br J Surg. 1950, 37, 474. [Google Scholar] [CrossRef]
- Christensen WN, Sternberg SS. Adenocarcinoma of the upper esophagus arising in ectopic gastric mucosa: two case reports and review of the literature. Am J Surg Pathol. 1987, 11, 397–402. [Google Scholar] [CrossRef]
- Clemente, C. A case of adenocarcinoma of the upper third of the esophagus arising on ectopic gastric tissue. Tumori. 1974, 60, 17–24. [Google Scholar] [CrossRef]
- Sakamoto G, Nakamura K, Saito K, et al. Primary adenocarcinoma of the esophagus arising from heterotopic gastric glands. Gan No Rinsho. 1970, 16, 1105–1110. [Google Scholar]
- Schmidt H, Riddell RH, Walther B, et al. Adenocarcinoma of heterotopic gastric mucosa in the proximal esophagus. Leber Magen Darm. 1985, 15, 144–147. [Google Scholar]
- Tanaka M, Ushiku T, Ikemura M, Shibahara J, Seto Y, Fukayama M. Esophageal adenocarcinoma arising in cervical inlet patch with synchronous Barrett’s esophagus-related dysplasia. Pathol Int. 2014, 64, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Khatri R, Patel J, Song J, Malik Z, Smith MS, Parkman HP. Esophageal Inlet Patch: Association with Barrett’s Esophagus. Dig Dis Sci. 2023, 68, 3671–3678. [Google Scholar] [CrossRef] [PubMed]
- Jabbari M, Goresky CA, Lough J, Yaffe C, Daly D, Côté C. The inlet patch: heterotopic gastric mucosa in the upper esophagus. Gastroenterology. 1985, 89, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Kim EA, Kang DH, Cho HS, Park DK, Kim YK, Park HC, Kim JH. Acid secretion from a heterotopic gastric mucosa in the upper esophagus demonstrated by dual probe 24-hour ambulatory pH monitoring. Korean J Intern Med. 2001, 16, 14–17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Endoscopic findings. First row, left: Case 4. First row, right: Case 8. Second row, left: Case 2 (showing multiple lesions). Second row, right: Case 5. Third row, left and right: Case 6 (showing multiple lesions with a villous/nodular pattern). Fourth row, left: Case 1 (showing two large lesions covering most of the esophageal circumference with a villous/nodular pattern). Fourth row, right: Case 3 (showing a villous/nodular pattern).
Figure 1.
Endoscopic findings. First row, left: Case 4. First row, right: Case 8. Second row, left: Case 2 (showing multiple lesions). Second row, right: Case 5. Third row, left and right: Case 6 (showing multiple lesions with a villous/nodular pattern). Fourth row, left: Case 1 (showing two large lesions covering most of the esophageal circumference with a villous/nodular pattern). Fourth row, right: Case 3 (showing a villous/nodular pattern).

Figure 2.
Histological findings. First row, left: Hematoxylin & Eosin, Case 4. First row, right: Hematoxylin & Eosin, Case 7. Second row, left: Hematoxylin & Eosin, Case 9. Second row, right: Case 3 (note the presence of specialized gastric epithelium (oxyntic) and foveolar epithelium). Third row, left: Hematoxylin & Eosin, Case 8. Third row, right: Giemsa stain, Case 6 (highlighting bacillary bacterial microorganisms compatible with H. pylori).
Figure 2.
Histological findings. First row, left: Hematoxylin & Eosin, Case 4. First row, right: Hematoxylin & Eosin, Case 7. Second row, left: Hematoxylin & Eosin, Case 9. Second row, right: Case 3 (note the presence of specialized gastric epithelium (oxyntic) and foveolar epithelium). Third row, left: Hematoxylin & Eosin, Case 8. Third row, right: Giemsa stain, Case 6 (highlighting bacillary bacterial microorganisms compatible with H. pylori).
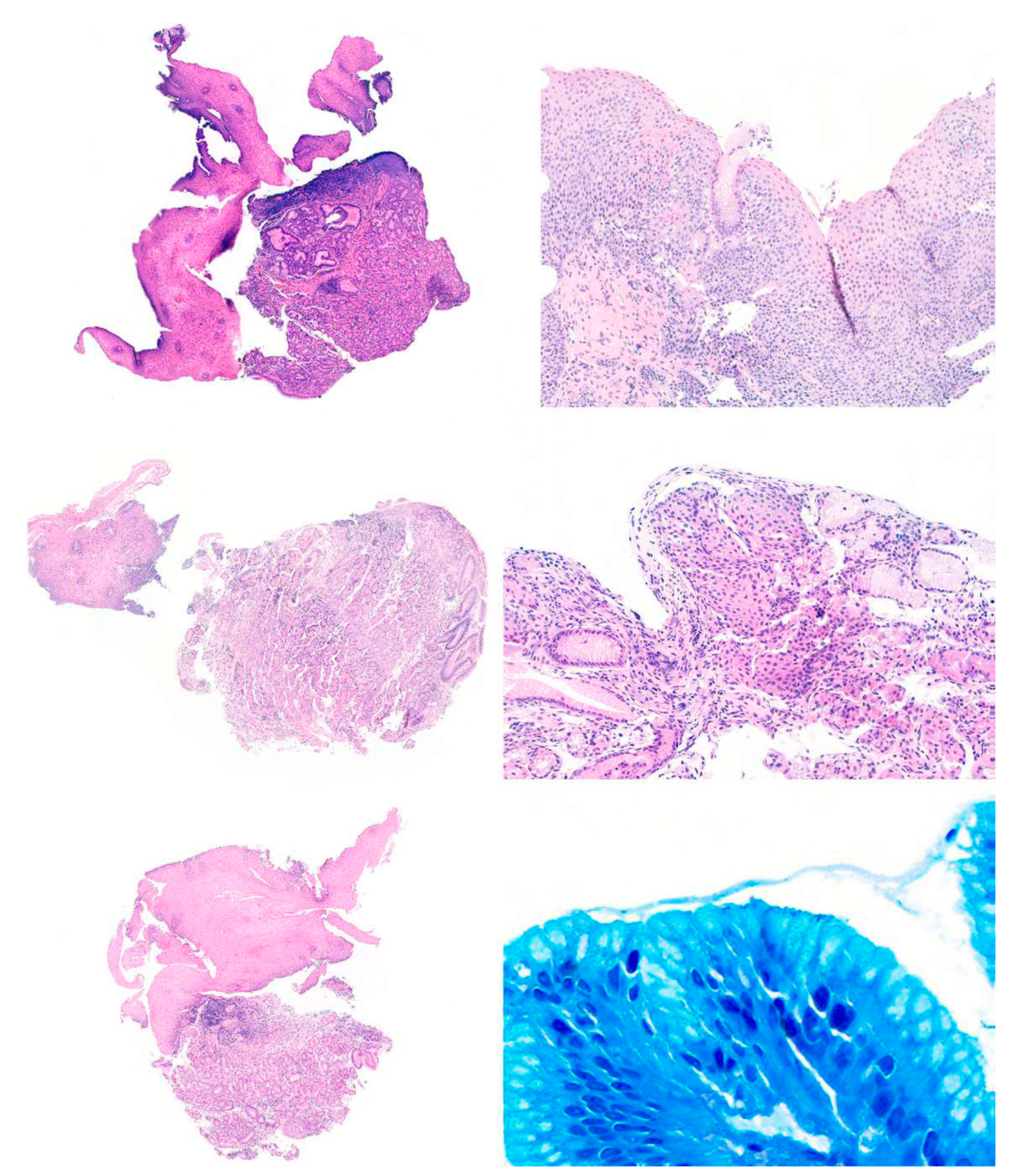

Table 1.
Summary of the patients’ main sociodemographic and clinical characteristics.
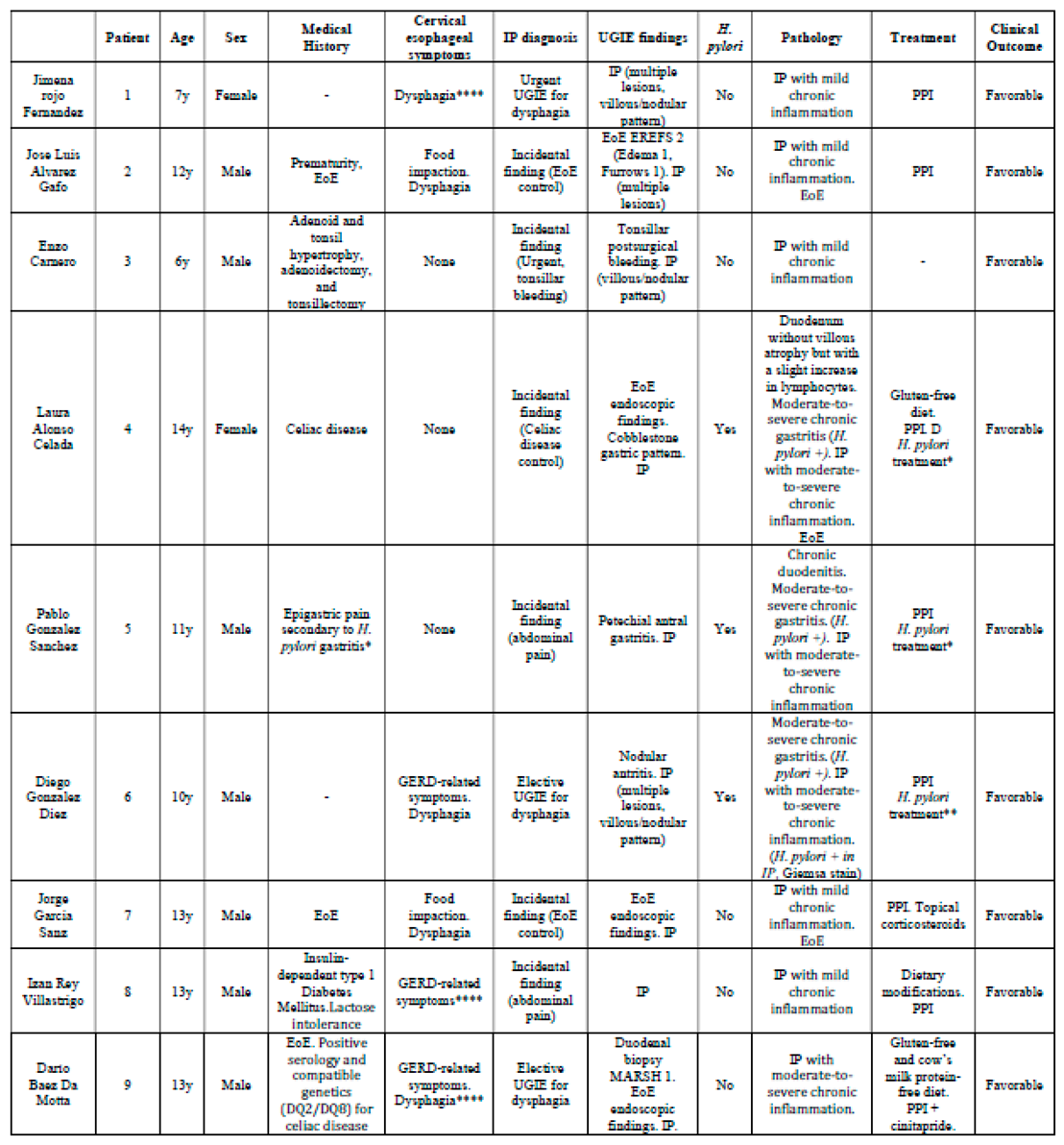 |
y: years; IP: Inlet Patch; EoE: Eosinophilic esophagitis; PPI: Proton pump inhibitors; GERD: Gastroesophageal reflux disease; UGIE: Upper gastrointestinal endoscopy, EREFS: Eosinophilic Esophagitis Endoscopic Reference Score. *: Treatment with bismuth potassium subcitrate, metronidazole, and tetracycline. Confirmation of eradication after completing the treatment; **: Treatment with omeprazole, amoxicillin, and metronidazole. Confirmation of eradication after completing the treatment; ***: Normal pH-metry; ****: Attributable to the IP either due to the absence of gastrointestinal comorbidities or the lack of underlying gastrointestinal disease activity at the time of IP diagnosis (e.g., controlled EoE after treatment, with biopsies showing no alterations consistent with EoE at the time of IP diagnosis).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



