
Submitted:
17 March 2025
Posted:
19 March 2025
You are already at the latest version
Abstract
Background: Sputum culture and smear conversion are key indicators of treatment response in drug-resistant tuberculosis (DR-TB). This study aimed to assess sputum conversion and regimen efficacy among DR-TB patients and identify factors influencing conversion rates. Methods: This retrospective cohort study analyzed medical records of DR-TB patients treated between 2018 and 2020 in the Eastern Cape Province, South Africa. Kaplan-Meier curves, Spearman correlation, and logistic regression models were used to assess time-to-sputum conversion and its predictors. Results: Among the 88% of patients who achieved sputum conversion, the median time ranged from 29 to 59 days. Patients on short treatment regimens converted significantly faster than those on long regimens (p = 7.55 × 10⁻¹⁵), with 90% of short-regimen patients achieving favorable outcomes compared to 52% in the long regimen group (p = 0.0000040). Spearman correlation revealed a weak but significant positive association between comorbidities and conversion time (r = 0.041, p = 0.041). HIV-positive patients had a slower conversion rate than HIV-negative patients, but this association was not statistically significant (χ² = 0.426, p = 0.514). Logistic regression identified older age as a predictor of favorable outcomes (coefficient = 0.039, p = 0.045), while regimen type and HIV status did not show significant predictive power. Conclusions: Shorter treatment regimens significantly improve sputum conversion rates and treatment outcomes. The findings support optimizing DR-TB treatment through personalized regimens based on patient health status and drug resistance patterns. This study provides evidence to enhance TB control efforts in high-burden regions, with implications for global treatment strategies.
Keywords:
tuberculosis
; drug-resistant tuberculosis
; HIV
; sputum conversion
; treatment outcome
; treatment success
; short regimen
; long regimen
; efficacy
1. Introduction
Globally, tuberculosis (TB), due to its transmissible nature, exerts an enormous impact on both individual and public health, resulting in significant morbidity and mortality and, fundamentally, posing a menace to the well-being of the populace in this 21st century [1,2]. On an annual basis, over 10 million people get sick with TB; this number has not abated since 2021, thereby making TB the leading cause of demise from a single infectious agent globally [3,4]. The emergence of the COVID-19 pandemic resulted in a global surge in TB incidence and mortality. Hence, a concerted effort to minimize TB transmission must be implemented [2]. Three significant components explored in the global approach to TB control involve optimizing prevention, timely detection, and prompt initiation of anti-TB treatment [5,6].
The possibility of transmission of infection of multidrug-resistant TB (MDR-TB) is high when the infected patients are culture-positive hence infection control measures aim to reduce the time to culture conversion as MDR-TB patients with culture-positive outcomes are more likely to transmit the infection to others [7,8]. According to the WHO guideline, while treating MDR-TB, culture negative results for two consecutive months, usually 30 days apart, is mandatory for concluding culture conversion [7,9,10]. In its guidelines, the WHO recommended that all TB patients undergoing treatment should be under close monitoring to evaluate their treatment response [11]. First-line anti-TB treatment is carried out in two phases, namely intensive and continuation phases, with drugs ranging from isoniazid, rifampicin, ethambutol, and pyrazinamide [12]. During treatment, monitoring for the presence of acid-fact bacilli (AFB) in the respiratory tract of patients with pulmonary TB (PTB) is done in the form of sputum smear examination (sputum smear microscopy) or sputum culturing [13]. Sputum smear-conversion, a transition from baseline smear-positive to smear-negative, during the 2nd or 5th month of treatment initiation, is a fundamental measure and indicator of treatment success [12,13,14,15,16]. Ideally, most TB cases are estimated to convert to smear-negative after anti-TB treatment in the intensive phase; on the contrary, a significant figure remains unchanged bacteriologically, thereby in-creasing the duration of infectivity [17].
Delayed sputum conversion patients (DSCPs) are usually characterized by the persistence of sputum-positive PTB status upon completion of the intensive treatment phase, contributing to higher treatment costs and additional burden on healthcare ser-vices (16]. Non-conversion of sputum smear at the end of the intensive phase of treatment has been documented to be associated with unfavorable outcomes, more specifically with default and failure.
The Eastern Cape is a high-burden region for TB particularly MDR-TB which is characterized by lowest TB case detection and coupled with the fact that no previous research had been carried out recently on sputum smear conversion during treatment among PTB patients. Additionally, it has the third-highest burden of HIV with a 25.2% prevalence rate in the country. Limited funds, deficient standardized training, and competing clinical attention priorities are some of the factors that impede timely and efficient provision of HIV services and care in the Eastern Cape [18,19,20]. This dual disease burden profoundly impacts sputum conversion rates and treatment outcomes with the propensity of straining its population bedeviled with preexisting socioeconomic inequality further, leading to deteriorating health conditions. The study findings will provide evidence-based results to districts and regional-level TB control programs to make informed decisions to control factors and improve the effectiveness of the anti-TB treatment follow-up period. Therefore, the aim of the current research was to review retrospectively medical records evaluating factors influencing sputum conversion during anti-TB treatment, focusing on demographics, clinical conditions, and treatment regimens among drug-resistant TB patients in Eastern Cape South Africa.
2. Materials and Methods
2.1. Study Design and Setting
This was a retrospective cohort study, where we reviewed medical records and mined clinical and demographic data of DR-TB patients who were 11 years and older and were started on DR-TB treatment from 01 January 2018 to 31 December 2020 in selected TB clinics and hospitals in the Eastern Cape Province, South Africa. Eastern Cape is the fourth most populated province in South Africa constituting 13% of the land surface of the Republic of South Africa and the second-largest province in the country. About 85% of the population lives in rural areas. It serves a population of 7,230,204 with 92 hospitals, 28 Community Health Centres, and 711 clinics. Oliver Tambo Reginald district municipality, one of the 7 municipalities in the province, has a total estimated population of 1,501,702 in 2022 [21].
2.2. Data Collection
Patients who were started on DR-TB treatment in the hospitals and clinics, from January 2018 to December 2020, were eligible for the study. A list of all eligible patients was obtained from the MDR-TB register on-site. Medical records for all patients who met inclusion criteria were obtained and reviewed and a structured data extraction tool was used to abstract data. Explanatory variables were patient demographics, clinical characteristics and diagnostic data, sputum conversion and treatment outcomes data. The outcome variable was treatment outcome and sputum conversion defined as the duration, in days, between DR-TB treatment initiation and the date of collection of the first sputum culture specimen that was culture negative after a prior positive culture. Data was captured in excel spreadsheet.
2.3. Data Analysis
Data were analysed using Python version 3.8. and R version 4.1.1 software. A p < 0.05 was considered to be significant. Continuous demographic and clinical data were described by medians and interquartile ranges (IQRs) and compared by MDR-TB and XDR-TB using the Wilcoxon-sum rank test. Frequencies were determined for categorical variables and compared by MDR-TB and XDR-TB using the chi-square test. Time to sputum culture conversion was determined using the Spearman correlation and Kruskal-Wallis-test which compared the differences between MDR-TB and XDR-TB by various explanatory variables. Predictors of favourable treatment outcome were determined by the logistic regression in the multivariate analysis.
2.4. Operational Definitions
Sputum smear conversion is described as a change from smear-positive pulmonary-TB cases to smear-negative subsequent to an anti-TB treatment. This is usually confirmed by two consecutive negative sputum AFB done every 30 days apart.
Sputum conversion time is the length of time needed for a patient with TB to have negative sputum smear or cultures for Mycobacterium tuberculosis during anti-TB treatment.
3. Results
3.1. Demographic Analysis
The heatmap clearly visualizes the percentage distribution of demographic factors (gender, education, and income) among patients achieving sputum conversion. Each cell's color intensity corresponds to the proportion within its category. The male category has the highest percentage of sputum conversion, as indicated by the darker color, while females have a lower conversion rate percentage compared to males. Secondary education shows the darkest intensity, indicating it is the most common education level among patients achieving sputum conversion, followed by patients with primary education. Patients with no education and tertiary education are less represented, with lighter colors. No income has the darkest cell, showing a high percentage of patients with sputum conversion fall into this category. Other income sources, such as salary or casual work, are less common, as shown by lighter shades. The heatmap confirms that sputum conversion is most prevalent among male patients, those with secondary education, and those reporting no income. These findings suggest potential socio-economic and gender-related patterns in achieving sputum conversion.
3.2. Comorbidity and Sputum Conversion
Patients with no comorbidities have a relatively fast median sputum conversion time of 59 days. Comorbidities such as hypertension and diabetes show shorter conversion times, ranging from 29 to 37.5 days. Patients with a combination of comorbidities, mental illness, and type two diabetes mellitus (T2DM) exhibit the longest sputum conversion time of 118 days. This suggests that managing multiple or complex conditions significantly impacts the effectiveness of TB treatment. Patients with comorbidity T2DM achieve sputum conversion in a median time of around 35 days. Spearman correlation (p-value 0.041) reveals a weak but statistically significant positive correlation between comorbidities and sputum conversion times. This suggests that as comorbidity complexity increases, sputum conversion times tend to increase slightly.
3.3. Social History Factors and Sputum Conversion Times
In Figure 2, social history factors (smoking and drinking) and (smoking and drugs) show lower medians and relatively tight distributions, indicating quicker and more consistent conversion times. They are characterized by a relatively narrow IQR showing consistent outcomes. Patients who have a combined history of smoking, drinking, and drugs have the largest spread and the highest median, reflecting substantial delays and variability in conversion times. A broad IQR and extreme outliers highlight the challenges faced by this group, reflecting severe delays and variability in outcomes. With this group, there are notable conversion delays, while those with a single or a pair of social history habits show better outcomes.
3.4. HIV Status and Sputum Conversion
HIV-negative patients display a higher sputum conversion rate (Figure 3). This suggests that the absence of HIV allows for a more effective immune response to TB treatment, leading to quicker and more successful sputum conversion. HIV-positive patients have a lower conversion rate. This reflects the challenges faced by HIV-positive individuals, such as weakened immune systems, potential drug interactions, or higher disease complexity. The statistical analysis of the association and correlation between HIV status and sputum conversion rates reveals no statistically significant association (Chi-squared test statistic: 0.426 and p-value: 0.514). The correlation between HIV status and sputum conversion rates is weak and insignificant (Spearman correlation statistic: -0.060, and p-value: 0.395).
3.5. Time to Sputum Conversion Stratified by HIV Status (Kaplan-Meier Survival Curve)
The curve in Figure 4 shows a slower decline in the HIV-positive group, indicating a higher probability of delayed sputum conversion. Patients in this group tend to take longer to convert their sputum. With patients in the HIV-negative group, the curve declines more rapidly, indicating a faster sputum conversion rate. This group achieves conversion sooner than the HIV-positive group. The statistical analysis (log-rank test) confirmed this difference with a highly significant p-value of 4.56 × 10⁻²⁶, which is extremely small. This indicates a highly significant difference between the survival curves of the two groups (HIV-positive and HIV-negative) in terms of time to sputum conversion.
3.6. Treatment Regimen
The curve in Figure 5 for the short regimen declines more rapidly, indicating that patients on this regimen achieve sputum conversion faster on average. The curve for the long regimen declines more slowly, suggesting a delayed sputum conversion compared to the short regimen. The separation between the curves indicates a significant difference in time to sputum conversion based on the treatment regimen. Patients on short regimens generally achieve faster conversion, which aligns with the goal of shorter treatment durations. The log-rank test for treatment regimens (p-value: 7.55 × 10⁻¹⁵) indicates a highly significant difference in sputum conversion times between the short and long regimens. Patients on the short regimen achieve sputum conversion significantly faster than those on the long regimen.
3.7. Impact of Regimen Type on Treatment Outcome
In Figure 6, a short regimen demonstrates a significantly higher percentage of favorable outcomes (~90%), with very few unfavorable outcomes (~10%). This highlights the effectiveness of the short regimen in achieving treatment success. However, the long regimen shows a much lower percentage of favorable outcomes (~52%) and a higher proportion of unfavorable outcomes (~48%). The chi-squared test (p-value: 0.0000040) shows a strong association between regimen type and treatment outcomes, with the short regimen significantly more likely to result in favorable outcomes.
3.8. Treatment Outcomes Based on Different Types of Drug Regimen
In patients with favorable outcomes ("Cured" and "Treatment Completed"), the short regimen shows a higher rate of "Cured" outcomes compared to the long regimen indicating that the short regimen is more effective in achieving sputum conversion and completing treatment successfully. The long regimen shows lower rates of "Cured," but the "Treatment Completed" rate is closer to that of the short regimen. In patients with unfavorable outcomes, the long regimen has a slightly higher rate of death, indicating potentially worse outcomes for some patients. The long regimen also shows a higher failure rate, suggesting potential challenges in efficacy or adherence for longer treatments.
The line chart (Figure 7) displays the rate (percentage) of various treatment outcomes across the short-regimen and long-regimen groups.
3.9. Relationship Between Age, HIV-Status and Comorbidities
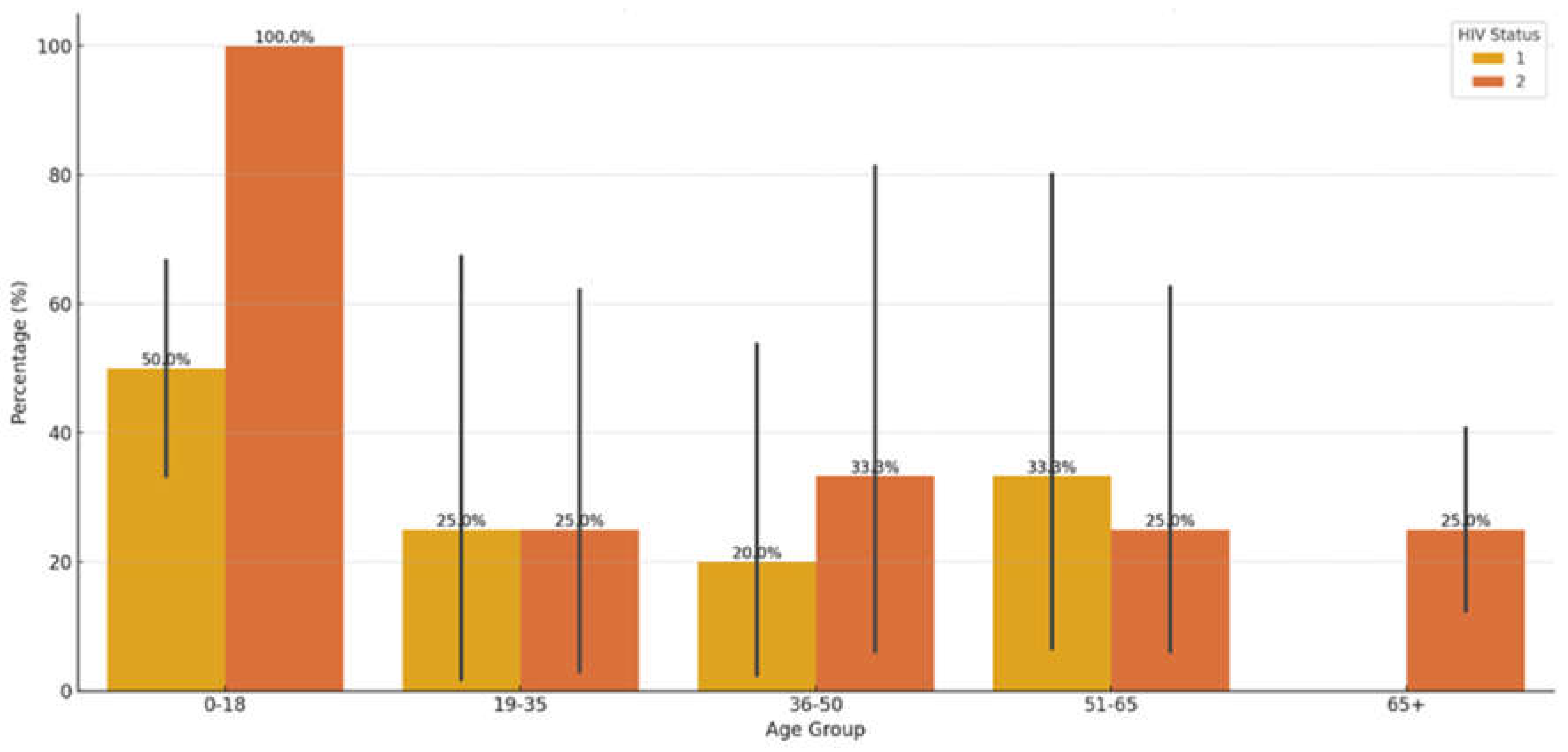
In Figure 8, the younger age groups (e.g., 0-18 and 19-35), the proportion of HIV-positive patients tends to be smaller compared to older age groups (e.g., 51-65). In older age groups (e.g., 36-50, 51-65, and 65+), the percentage of patients with comorbidities appears more balanced between HIV- positive and HIV-negative statuses. Younger age groups (e.g., 0-18) show lower percentages for both HIV statuses, potentially due to fewer comorbidities being recorded or a smaller sample size. The older the age group, the more evenly distributed the percentages tend to be, suggesting that comorbidities may increase with age, irrespective of HIV status. Younger age groups are more likely to have no comorbidities and a higher proportion of HIV-negative patients. Older age and HIV-positive status might independently or jointly contribute to more comorbidities, which could influence treatment outcomes. Young patients with no comorbidities might have better baseline conditions, allowing for more favorable treatment outcomes. The chi-squared test comparing age groups and HIV status has a p-value of 1.62 × 10⁻⁵. The very small p-value indicates a statistically significant association between age group and HIV status. This suggests that the distribution of HIV-positive and HIV-negative patients varies significantly across age groups.
3.10. Logistic Regression Results
The logistic regression model assessed the likelihood of achieving a favorable treatment outcome ("Cured" or "Treatment Completed") based on various predictors. Older age is positively associated with favorable outcomes, though the effect size is small (coefficient: 0.039 and p-value: 0.045). The regimen type does not appear to significantly influence favorable outcomes, likely due to multicollinearity in the dataset (coefficient: -1.143 (for long regimen relative to the short regimen); p-value: 1.000 (not significant)) Male patients may have a slightly higher likelihood of favorable outcomes (coefficient 0.940; p-value 0.056 (marginal significance)). HIV-positive patients are less likely to achieve favorable outcomes, but this is not statistically significant. (coefficient: -0.753 p-value: 0.124). In Model Fit, Pseudo R-squared is 0.1554, indicating the model explains ~15.5% of the variance in outcomes—Log-Likelihood Ratio (LLR) p-value: 3.15×10−53.15, showing that the model is statistically significant. Age has a significant but small positive impact on achieving favorable outcomes. Regimen type and HIV status, though important clinically, do not show significant effects in this model, potentially due to overlapping effects with other variables. The model failed to converge fully, and the Pseudo R-squared of 0.1847, indicating an improvement over the initial model, with ~18.5% variance explained. Older age is associated with a slightly higher likelihood of favorable outcomes (coefficient: 0.047; p-value: 0.034).
4. Discussion
Early sputum culture conversion is prognostic of favorable TB treatment outcomes. This retrospective cohort study explores patient sputum conversion dynamics during tuberculosis treatment. Our analysis revealed that the median time to sputum smear conversion varied depending on the presence or absence of comorbidities. The patients with no comorbidities had a median conversion time of 59 days. This was comparable to other studies with a median time of 56 days [22], 59 days [23,24] 60 days [25], and 62 days [8]. In contrast, some other studies reported lower median sputum conversion times of 21 days [17], 24 days [13], and 35 days [26], while other studies had higher conversion times [24,27]. Differences in socioeconomic status, study period, follow-up term, clinical characteristics of study participants, and the effectiveness of the TB control program could account for the disparities among the different studies [28].
Approximately 88% of the DR-TB patients included in this study achieved sputum conversion in the first two months of treatment, ranging from median time of 29 days to 59 days. However, other studies in different countries have reported lower percentage of conversion at the second month including Latvia (30%) [29], Dominican Republic (48.8%) [30], and Pakistan 53.4% [31]. In this study, 7.7% and 0.2% of the patients achieved sputum conversion by the third and fourth months, respectively. In contrast to our study, higher conversion rates were reported in India (57%) [32] at the third month of treatment, while other studies reported relatively higher conversion rates in India (79-98%) [32,33,34], South Africa (89%) [35], and Peru (92.9%) [23] at the sixth month. Reduced time to sputum culture conversion is a crucial infection control prevention strategy since there is reduced possibility of spreading infections to other members of the family, healthcare personnel, and the community. Hence, attaining a faster sputum smear conversion enhances easier therapy, efficacy and comfortability for the patient by reducing injectable drug administration and the associated vestibular toxicity and aural loss [36,37,38].
In this study, DR-TB patients who were HIV coinfected had a longer time of sputum smear conversion than HIV-negative patients. HIV infection compromises the immune system, which could hinder the body's ability to respond effectively to TB treatment. In theory, HIV-negative individuals might have a more robust immune response, potentially leading to quicker sputum conversion. This finding is corroborated by other studies done in Northern Ethiopia [37], Eastern Ethiopia [15], Peru [23] and a prospective cohort study conducted in nine countries [39], showing that HIV co-infected patients had significantly longer time to culture conversion as compared with HIV negative; although in our study the analysis of the association and correlation between HIV status and sputum conversion rates reveals no statistically significant association. The lack of significant association suggests that HIV status alone may not strongly predict sputum conversion rates in this dataset. Other factors such as treatment adherence and comorbidities might play a larger role. However, the study of Rieu et al., Senkoro et al., and Hafkin et al. conducted in London, Tanzania, and Botswana, respectively, showed that there was no significant difference in sputum smear conversion time between HIV-positive and negative individuals [24,40,41]. Some studies suggest that HIV-negative patients might achieve sputum culture conversion slightly later than HIV-positive patients, but this does not necessarily translate to a higher conversion rate overall. Contrary to our finding, a study in Lesotho found that HIV-positive patients achieved sputum culture clearance at a median of 54.22 days, while HIV-negative patients took 60.84 days [42]. The reasons that support this finding could be due to a wholly integrated TB/HIV and MDR-TB/HIV continuum of care model which prioritized prompt ART initiation and patient follow-up thus improving patient outcome [37]. According to Gamachu et al. [15], the difference between the intensity of follow-up and screening for TB-HIV coinfection may account for this disparity since early and timely screening forms part of the objectives of the TB/HIV integrated programs thereby ensuring these patients are kept under a close watch.
Recent studies highlight the growing adoption of shorter regimens (6–9 months) for DR-TB to improve adherence and reduce loss to follow-up. In the current study, patients on short regimen generally achieved faster conversion, which aligns with the goal of shorter treatment durations. Studies indicate that patients on short treatment regimen (STR) for DR-TB tend to achieve sputum culture conversion more quickly than those on longer regimen. Our finding is supported by a study in Pakistan which found that the mean time to sputum culture conversion (SCC) was significantly shorter in the STR group compared to the longer treatment regimen (LTR) group, with mean times of 2.03 months for STR versus 2.69 months for LTR [43]. These findings provide strong evidence to support the efficacy of the short regimen for faster sputum conversion. Patients on longer treatment regimens often experience slower sputum culture conversion. This could be due to several factors, including the complexity of drug resistance patterns and the need for more extensive treatment to ensure cure. However, there is no significant difference in the proportion of patients achieving SCC between the two groups.
Regarding treatment outcome, our study confirms that short regimen demonstrated a significantly higher percentage of favorable outcomes (~90%), with very few unfavorable outcomes (~10%). This highlights the effectiveness of the short regimen in achieving treatment success. However, the long regimen shows a much lower percentage of favorable outcomes (~52%) and a higher proportion of unfavorable outcomes (~48%). Studies have shown that short regimens often achieve higher treatment success rates compared to longer regimens. In agreement with our study, a systematic review and meta-analysis reported that the pooled proportion of successful treatment outcomes was 80.0% for shorter regimens versus 75.3% for longer regimens, largely as a result of loss to follow-up with the former [44,45]. Notably, another study in Eastern Cape, South Africa reported a 69% success rate with short regimens compared to 58% for long regimens [46], while another study from Tanzania documented that the majority of DR-TB patients on short treatment regimen (STR) achieved a better treatment outcome than on standard longer regimen (SLR) [47]. Short regimen tend to have lower rates of loss to follow-up, which contributes to their higher overall success rates. This is attributed to the shorter duration and potentially fewer side effects, making it easier for patients to adhere to treatment [44]. But in some cases, there is the possibility of a higher risk of treatment failure or relapse when the issue of drug resistance arises. However, some studies suggest that longer regimen might offer better long-term efficacy by reducing the risk of relapse, although this comes at the cost of longer treatment durations and potential side effects [45].
In the current study, the multivariable analysis revealed that older age showed a small positive association with favorable outcomes (coefficient: 0.039, p = 0.045). This is similar to the study conducted at Alemgena Health Center, located in Sebeta district of Ethiopia where treatment success rate was 3.582 (95% CI 1.958–6.554, p-value = 0.000) times higher in the age group 44 and below compared to the age group 45 and above [48]. However, contrary findings were reported by Leketa et al. [49] and Massud et al. [50] where the authors found statistically significant lower odds of unfavourable treatment outcomes among the patients who were ≤ 44 years old compared to those who were > 44 years old and patients aged >50 years had higher odds of unsuccessful outcomes (OR = 2.149, p = 0.048), respectively. Our results suggest older age improves outcomes, while other studies associate younger age or middle age with better outcomes. This discrepancy may arise from differences in study populations (e.g., comorbidities in older adults or variations in adherence patterns. Male gender in our study had marginal significance (coefficient: 0.940, p = 0.056). The findings reported from a study carried out in Bilene, Mozambique [51], also identified male sex as a factor associated with unfavorable TB treatment outcomes (aOR 1.48). This suggests males may have a slightly higher likelihood of favorable outcomes. Male gender was significantly associated with successful outcomes (AOR = 2.40, CI 1.16, 4.98, p < 0.05) in Northwest Ethiopia while gender was not a significant predictor in another study conducted in the Eastern Cape of South Africa [52,53]. The stronger association in Limenh et al. may reflect regional gender-specific healthcare access or adherence behaviors while our result suggests gender’s role may vary by population. Furthermore, in our study, HIV-positive patients are less likely to achieve favorable outcomes, but this is not statistically significant (coefficient: -0.753 p-value: 0.124). Similarly, a study in Northwest Ethiopia found that HIV-negative patients were significantly more likely to have successful TB treatment outcomes (AOR = 3.35, 95% CI: 1.31, 8.60, p < 0.05) [52].
The limitations highlighted in this study include the retrospective nature of the study design which may introduce biases related to data completeness, and the exclusion of certain variables due to a lack of a complete set of laboratory and clinical data. In addition, the study did not include the CD4 count and ART status of HIV patients, so the logistic regression model analysis was not adjusted for ART; the data quality, including self-reported smoking and drinking status, was also subject to selection of response and recall bias.
5. Conclusions
Most of the subjects in our study had effective sputum culture conversion within the first four months. Interestingly, about 88% of the patients who underwent TB treatment converted in the first two months with a median time ranging from 29 to 59 days. Our study's median time to culture conversion was within the range the WHO recommends. Our results highlight how crucial it is to assess the treatment response of DR-TB patients, especially those who have history of comorbidities that may interfere with their treatment. Notably, patients on short regimen demonstrated faster sputum conversion rates, aligning with the goal of reducing treatment duration. Moreover, these patients exhibited a significantly higher percentage of favorable outcomes, approximately 90%, with only about 10% experiencing unfavorable outcomes. These results support the use of a short regimen as an effective strategy for improving treatment outcomes in DR-TB patients. The faster sputum conversion and higher success rates observed in this study suggest that short regimen can enhance patient adherence and reduce the risk of treatment failure or relapse. However, it is crucial to consider individual patient factors, such as drug resistance patterns and health status, when selecting treatment regimens. With rural areas in South Africa facing systemic barriers such as healthcare access and stigma which complicate DR-TB management, it is anticipated that the effort of the South African National TB Recovery Plan 3.0 in rolling out shorter regimens with better drugs for the treatment of DR-TB, with the notable launch of the BPAL-L program, having over 2,000 patients on a six-month DR-TB regimen will contribute greatly to the reduction of the TB burden even in the rural areas if implemented to scale.
Overall, this study contributes valuable evidence to the continued efforts to optimize DR-TB treatment strategies, highlighting the potential benefits of shorter treatment durations in achieving favorable outcomes and enhancing public health outcomes. Future research should continue to explore the long-term efficacy and safety of short regimens in diverse patient populations to further inform treatment guidelines.
Author Contributions
Conceptualization, M.C.H.; methodology, M.C.H. and L.M.F; validation, M.C.H., L.M.F. and T.A.; formal analysis, M.C.H.; L,M.F.; investigation, M.C.H.; L.M.F.; data curation, M.C.H.; L.M.F.; writing—original draft preparation, M.C.H.; writing— review and editing, M.C.H.; L.M.F.; and T.A.; visualization, M.C.H.; and L.M.F.; supervision, T.A.; project administration, L.M.F.; funding acquisition, L.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by South African Medical Research Council; Pilot grant and The APC was funded by Walter Sisulu University.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Health Sciences Research Ethics Committee of Walter Sisulu University (ref. no. 026/2019) and permission to carry out the study was obtained from the Eastern Cape Department of Health (ref. No. EC_201904_011).
Informed Consent Statement
This was a retrospective study that involved review of medical files, hence there was no need for written informed consent.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
The authors are grateful to the healthcare managers and workers in the healthcare facilities who granted us access to medical records. The authors appreciate the assistance of colleagues who helped with data collection and management.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| TB | Tuberculosis |
| MDR-TB | Multidrug-resistant tuberculosis |
| XDR-TB | Extensively drug-resistant tuberculosis |
| AFB | Acid-fast bacilli |
| DCSPs | Delayed sputum conversion patients |
| PTB | Pulmonary tuberculosis |
| STR | short treatment regimen |
| LTR | longer treatment regimen |
| SCC | sputum culture conversion |
| SLR | standard longer regimen |
| ART | Antiretroviral therapy |
References
- Ordonez, A.A.; Tucker, E.W.; Anderson, C.J.; Carter, C.L.; Ganatra, S.; Kaushal, D.; Kramnik, I.; Lin, P.L.; Madigan, C.A.; Mendez, S.; et al. Visualizing the dynamics of tuberculosis pathology using molecular imaging. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Shah, M., Dansky, Z., Nathavitharana, R., Behm, H., Brown, S., Dov, L., Fortune, D., Gadon, N.L., Gardner Toren, K., Graves, S, Haley, C.A., 2024. NTCA Guidelines for Respiratory Isolation and Restrictions to Reduce Transmission of Pulmonary Tuberculosis in Community Settings. Clin. Infect. Dis. 2024, ciae199.
- Weldemhret, L.; Atsbaha, A.H.; Bekuretsion, H.; Desta, A.; Legesse, L.; Kahsay, A.G.; Hagos, D. Time to Sputum Culture Conversion and Its Predictors Among Multidrug Resistant Tuberculosis Patients in Tigray, Northern Ethiopia: Retrospective Cohort Study. Infect. Drug Resist. 2023, 16, 3671–3681. [Google Scholar] [CrossRef]
- Global tuberculosis report 2024. Geneva: World Health Organization; 2024. Licence: CC BY-NC-SA 3.0 IGO (Accessed 5 January 2025).
- World Health Organization. Global tuberculosis report 2021. Geneva,Switzerland: World Health Organization; 2021 (Accessed 5 January 2025).
- Paradkar, M.S.; Pradhan, N.N.; Balaji, S.; Gaikwad, S.N.; Chavan, A.; Dharmashale, S.N.; Sahasrabudhe, T.; Lokhande, R.; Deshmukh, S.A.; Barthwal, M.; et al. Early Microbiologic Markers of Pulmonary Tuberculosis Treatment Outcomes. Ann. Am. Thorac. Soc. 2023, 20, 1760–1768. [Google Scholar] [CrossRef]
- Abebe, M.; Atnafu, A.; Tilahun, M.; Sero, N.; Neway, S.; Alemu, M.; Tesfaye, G.; Mihret, A.; Bobosha, K.; Wan, C. Determinants of sputum culture conversion time in multidrug-resistant tuberculosis patients in ALERT comprehensive specialized hospital, Addis Ababa, Ethiopia: A retrospective cohort study. PLOS ONE 2024, 19, e0304507. [Google Scholar] [CrossRef]
- Assemie, M.A.; Alene, M.; Petrucka, P.; Leshargie, C.T.; Ketema, D.B. Time to sputum culture conversion and its associated factors among multidrug-resistant tuberculosis patients in Eastern Africa: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 98, 230–236. [Google Scholar] [CrossRef]
- Ncha, R.; Variava, E.; Otwombe, K.; Kawonga, M.; Martinson, N.A. Predictors of time to sputum culture conversion in multi-drug-resistant tuberculosis and extensively drug-resistant tuberculosis in patients at Tshepong-Klerksdorp Hospital. South. Afr. J. Infect. Dis. 2019, 34, 1–8. [Google Scholar] [CrossRef]
- Lee, H.H.; Jo, K.-W.; Yim, J.-J.; Jeon, D.; Kang, H.; Shim, T.S. Interim treatment outcomes in multidrug-resistant tuberculosis patients treated sequentially with bedaquiline and delamanid. Int. J. Infect. Dis. 2020, 98, 478–485. [Google Scholar] [CrossRef]
- Djouma, F.N.; Noubom, M.; Ateudjieu, J.; Donfack, H. Delay in sputum smear conversion and outcomes of smear-positive tuberculosis patients: a retrospective cohort study in Bafoussam, Cameroon. BMC Infect. Dis. 2015, 15, 139–139. [Google Scholar] [CrossRef] [PubMed]
- Kateete, D.P.; Mbabazi, M.M.; Nakazzi, F.; Katabazi, F.A.; Kigozi, E.; Ssengooba, W.; Nakiyingi, L.; Namiiro, S.; Okwera, A.; Joloba, M.L.; et al. Sputum microbiota profiles of treatment-naïve TB patients in Uganda before and during first-line therapy. Sci. Rep. 2021, 11, 24486. [Google Scholar] [CrossRef]
- Bisognin, F.; Amodio, F.; Lombardi, G.; Reggiani, M.L.B.; Vanino, E.; Attard, L.; Tadolini, M.; Re, M.C.; Monte, P.D. Predictors of time to sputum smear conversion in patients with pulmonary tuberculosis under treatment. New Microbiologica 2018, 42, 171–175. [Google Scholar]
- Ibrahim, M.N.; Husain, N.R.N.; Daud, A.; Chinnayah, T. Epidemiology and Risk Factors of Delayed Sputum Smear Conversion in Malaysian Aborigines with Smear-Positive Pulmonary Tuberculosis. Int. J. Environ. Res. Public Heal. 2022, 19, 2365. [Google Scholar] [CrossRef]
- Gamachu, M.; Deressa, A.; Birhanu, A.; Ayana, G.M.; Raru, T.B.; Negash, B.; Merga, B.T.; Alemu, A.; Ahmed, F.; Mohammed, A.; et al. Sputum smear conversion and treatment outcomes among drug-resistant pulmonary tuberculosis patients in eastern Ethiopia: A 9-years data analysis. Front. Med. 2022, 9, 1007757. [Google Scholar] [CrossRef]
- Pang, M.; Dai, X.; Wang, N.; Yi, J.; Sun, S.; Miao, H.; Zhang, J.; Zhang, H.; Li, J.; Ding, B.; et al. A study on factors influencing delayed sputum conversion in newly diagnosed pulmonary tuberculosis based on bacteriology and genomics. Sci. Rep. 2024, 14, 18550. [Google Scholar] [CrossRef]
- Asemahagn, M.A. Sputum smear conversion and associated factors among smear-positive pulmonary tuberculosis patients in East Gojjam Zone, Northwest Ethiopia: a longitudinal study. BMC Pulm. Med. 2021, 21, 118–210. [Google Scholar] [CrossRef] [PubMed]
- Hansoti, B.; Mishra, A.; Rao, A.; Chimoyi, L.; Redd, A.D.; Reynolds, S.J.; Stead, D.F.; Black, J.; Maharaj, R.; Hahn, E.; et al. The geography of emergency department-based HIV testing in South Africa: Can patients link to care? eClinicalMedicine 2021, 40, 101091. [Google Scholar] [CrossRef] [PubMed]
- UNICEF commemorates World AIDS Day 2024 at launch of Eastern Cape Global Alliance chapter. Available online at: https://www.unicef.org/southafrica/press-releases/unicef-commemorates-world-aids-day-2024-launch-eastern-cape-global-alliance-chapter#:~:text=The%20Eastern%20Cape%20province%20is,Eastern%20Cape%20province%20in%202023 [accessed 17 March 2025].
- Peltzer, K.; Davids, A. Lay Counsellors' Experiences of Delivering HIV Counselling Services in Public Health Facilities in a Eastern Cape Province District of South Africa. J. Psychol. Afr. 2011, 21, 53–61. [Google Scholar] [CrossRef]
- Statistics South Africa Available online: https://www.statssa.gov.za/?p=16760 [accessed 10 March 2025].
- Kim, J.; Kwak, N.; Lee, H.Y.; Kim, T.S.; Kim, C.-K.; Han, S.K.; Yim, J.-J. Effect of drug resistance on negative conversion of sputum culture in patients with pulmonary tuberculosis. Int. J. Infect. Dis. 2016, 42, 64–68. [Google Scholar] [CrossRef]
- Tierney, D.B.; Franke, M.F.; Becerra, M.C.; Virú, F.A.A.; Bonilla, C.A.; Sánchez, E.; Guerra, D.; Muñoz, M.; Llaro, K.; Palacios, E.; et al. Time to Culture Conversion and Regimen Composition in Multidrug-Resistant Tuberculosis Treatment. PLOS ONE 2014, 9, e108035. [Google Scholar] [CrossRef]
- Rieu, R.; Chang, C.; Collin, S.M.; Fazekas, J.; Dassanaike, S.; Abbara, A.; Davidson, R.N. Time to detection in liquid culture of sputum in pulmonary MDR-TB does not predict culture conversion for early discharge. J. Antimicrob. Chemother. 2016, 71, 803–806. [Google Scholar] [CrossRef]
- Putri, F.A.; Burhan, E.; Nawas, A.; Soepandi, P.Z.; Sutoyo, D.K.; Agustin, H.; Isbaniah, F.; Dowdy, D.W. Body mass index predictive of sputum culture conversion among MDR-TB patients in Indonesia. Int. J. Tuberc. Lung Dis. 2014, 18, 564–570. [Google Scholar] [CrossRef]
- Parikh, R.; Nataraj, G.; Kanade, S.; Khatri, V.; Mehta, P. Time to sputum conversion in smear positive pulmonary TB patients on category I DOTS and factors delaying it. J. Assoc. Physicians India 2012, 60, 22–26. [Google Scholar]
- Shah, N.S.; Pratt, R.; Armstrong, L.; Robison, V.; Castro, K.G.; Cegielski, J.P. Extensively Drug-Resistant Tuberculosis in the United States, 1993-2007. JAMA 2008, 300, 2153–2160. [Google Scholar] [CrossRef] [PubMed]
- Alzarea, A.I.; Saifullah, A.; Khan, Y.H.; Alanazi, A.S.; Alatawi, A.D.; Algarni, M.A.; Almalki, Z.S.; Alahmari, A.K.; Alhassan, H.H.; Mallhi, T.H. Evaluation of time to sputum smear conversion and its association with treatment outcomes among drug-resistant tuberculosis patients: a retrospective record-reviewing study. Front. Pharmacol. 2024, 15, 1370344. [Google Scholar] [CrossRef]
- Holtz, T.H.; Sternberg, M.; Kammerer, S.; Laserson, K.F.; Riekstina, V.; Zarovska, E.; Skripconoka, V.; Wells, C.D.; Leimane, V. Time to Sputum Culture Conversion in Multidrug-Resistant Tuberculosis: Predictors and Relationship to Treatment Outcome. Ann. Intern. Med. 2006, 144, 650–659. [Google Scholar] [CrossRef]
- Rodriguez, M.; Monedero, I.; Caminero, J.A.; Encarnación, M.; Dominguez, Y.; Acosta, I.; Muñoz, E.; Camilo, E.; Martinez-Selmo, S.; Santos, S.d.L.; et al. Successful management of multidrug-resistant tuberculosis under programme conditions in the Dominican Republic. Int. J. Tuberc. Lung Dis. 2013, 17, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Basit, A.; Ahmad, N.; Khan, A.H.; Javaid, A.; Sulaiman, S.A.S.; Afridi, A.K.; Adnan, A.S.; Haq, I.U.; Shah, S.S.; Ahadi, A.; et al. Predictors of Two Months Culture Conversion in Multidrug-Resistant Tuberculosis: Findings from a Retrospective Cohort Study. PLOS ONE 2014, 9, e93206. [Google Scholar] [CrossRef]
- Velayutham, B.; Nair, D.; Kannan, T.; Padmapriyadarsini, C.; Sachdeva, K.S.; Bency, J.; Klinton, J.S.; Haldar, S.; Khanna, A.; Jayasankar, S.; et al. Factors associated with sputum culture conversion in multidrug-resistant pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2016, 20, 1671–1676. [Google Scholar] [CrossRef]
- Joseph, P.; Desai, V.B.R.; Mohan, N.S.; Fredrick, J.S.; Ramachandran, R.; Raman, B.; Wares, F.; Ramachandran, R.; Thomas, A. Outcome of standardized treatment for patients with MDR-TB from Tamil Nadu, India. 2011, 133, 529–534.
- Singla, R.; Sarin, R.; Khalid, U.; Mathuria, K.; Singla, N.; Jaiswal, A.; Puri, M.M.; Visalakshi, P.; Behera, D. Seven-year DOTS-Plus pilot experiencein India: results, constraints and issues. Int J Tuberc Lung Dis, 2009, 13: 976–981.
- Brust, J.C.M.; Lygizos, M.; Chaiyachati, K.; Scott, M.; van der Merwe, T.L.; Moll, A.P.; Li, X.; Loveday, M.; Bamber, S.A.; Lalloo, U.G.; et al. Culture Conversion Among HIV Co-Infected Multidrug-Resistant Tuberculosis Patients in Tugela Ferry, South Africa. PLOS ONE 2011, 6, e15841. [Google Scholar] [CrossRef]
- Akalu, T.Y.; Muchie, K.F.; Gelaye, K.A. Time to sputum culture conversion and its determinants among Multi-drug resistant Tuberculosis patients at public hospitals of the Amhara Regional State: A multicenter retrospective follow up study. PLOS ONE 2018, 13, e0199320. [Google Scholar] [CrossRef]
- Shibabaw, A.; Gelaw, B.; Wang, S.-H.; Tessema, B. Time to sputum smear and culture conversions in multidrug resistant tuberculosis at University of Gondar Hospital, Northwest Ethiopia. PLOS ONE 2018, 13, e0198080. [Google Scholar] [CrossRef]
- Wenlu, Y.; Xia, Z.; Chuntao, W.; Qiaolin, Y.; Xujue, X.; Rong, Y.; Dan, S.; Xi, Y.; Bin, W. Time to sputum culture conversion and its associated factors among drug-resistant tuberculosis patients: a systematic review and meta-analysis. BMC Infect. Dis. 2024, 24, 169. [Google Scholar] [CrossRef]
- Kurbatova, E.V.; Cegielski, J.P.; Lienhardt, C.; Akksilp, R.; Bayona, J.; Becerra, M.C.; Caoili, J.; Contreras, C.; Dalton, T.; Danilovits, M.; et al. Sputum culture conversion as a prognostic marker for end-of-treatment outcome in patients with multidrug-resistant tuberculosis: a secondary analysis of data from two observational cohort studies. Lancet Respir. Med. 2015, 3, 201–209. [Google Scholar] [CrossRef]
- Senkoro, M.; Mfinanga, S.G.; Mørkve, O. Smear microscopy and culture conversion rates among smear positive pulmonary tuberculosis patients by HIV status in Dar es Salaam, Tanzania. BMC Infect. Dis. 2010, 10, 210. [Google Scholar] [CrossRef]
- Hafkin, J.; Modongo, C.; Newcomb, C.; Lowenthal, E.; MacGregor, R.R.; Steenhoff, A.P.; Friedman, H.; Bisson, G.P. Impact of the human immunodeficiency virus on early multidrug-resistant tuberculosis treatment outcomes in Botswana. Int. J. Tuberc. Lung Dis. 2013, 17, 348–353. [Google Scholar] [CrossRef]
- Alakaye, O.J. Time to sputum culture conversion of Multi-Drug Resistant Tuberculosis in HIV positive versus HIV negative patients in Lesotho. University of Pretoria (South Africa). 2018.
- Wahid, A.; Ghafoor, A.; Khan, A.W.; Al-Worafi, Y.M.; Latif, A.; Shahwani, N.A.; Atif, M.; Saleem, F.; Ahmad, N. Comparative effectiveness of individualized longer and standardized shorter regimens in the treatment of multidrug resistant tuberculosis in a high burden country. Front. Pharmacol. 2022, 13, 973713. [Google Scholar] [CrossRef]
- Abidi, S.; Achar, J.; Neino, M.M.A.; Bang, D.; Benedetti, A.; Brode, S.; Campbell, J.R.; Casas, E.C.; Conradie, F.; Dravniece, G.; et al. Standardised shorter regimens versus individualised longer regimens for rifampin- or multidrug-resistant tuberculosis. Eur. Respir. J. 2020, 55, 1901467. [Google Scholar] [CrossRef] [PubMed]
- Karnan, A.; Jadhav, U.; Ghewade, B.; Ledwani, A.; Shivashankar, P. A Comprehensive Review on Long vs. Short Regimens in Multidrug-Resistant Tuberculosis (MDR-TB) Under Programmatic Management of Drug-Resistant Tuberculosis (PMDT). Cureus 2024, 16, e52706. [Google Scholar] [CrossRef]
- Lotz, J.-D.K.; Porter, J.; Conradie, H.; Boyles, T.; Gaunt, B.; Dimanda, S.; Cort, D. Treating drug-resistant tuberculosis in an era of shorter regimens: Insights from rural South Africa. South Afr. Med J. 2023, 113, 47–56. [Google Scholar] [CrossRef]
- Mleoh, L.; Mziray, S.R.; Tsere, D.; Koppelaar, I.; Mulder, C.; Lyakurwa, D. Shorter regimens improved treatment outcomes of multidrug-resistant tuberculosis patients in Tanzania in 2018 cohort. Trop. Med. Int. Heal. 2023, 28, 357–366. [Google Scholar] [CrossRef]
- Hayre, K.; Takele, M.K.; Birri, D.J. Tuberculosis treatment outcomes and associated factors at Alemgena Health Center, Sebeta, Oromia, Ethiopia. PLOS ONE 2024, 19, e0303797. [Google Scholar] [CrossRef]
- Leketa, M.M.; Zondi, S.; Cele, L.; Mathibe, M.; Ngwepe, P. Factors associated with unfavourable treatment outcomes among tuberculosis patients at health facilities of Maseru, Lesotho. South Afr. Fam. Pr. 2024, 66, 6–e6. [Google Scholar] [CrossRef]
- Massud, A.; Khan, A.H.; Sulaiman, S.A.S.; Ahmad, N.; Shafqat, M.; Ming, L.C. Unsuccessful treatment outcome and associated risk factors. A prospective study of DR-TB patients from a high burden country, Pakistan. PLOS ONE 2023, 18, e0287966. [Google Scholar] [CrossRef]
- Osório, D.; Munyangaju, I.; Nacarapa, E.; Nhangave, A.-V.; Ramos-Rincon, J.-M. Predictors of unfavourable tuberculosis treatment outcome in Bilene District, Gaza Province, Mozambique: A retrospective analysis, 2016 - 2019. South Afr. Med J. 2022, 112, 234–239. [Google Scholar] [CrossRef]
- Limenh, L.W.; Kasahun, A.E.; Sendekie, A.K.; Seid, A.M.; Mitku, M.L.; Fenta, E.T.; Workye, M.; Simegn, W.; Ayenew, W. Tuberculosis treatment outcomes and associated factors among tuberculosis patients treated at healthcare facilities of Motta Town, Northwest Ethiopia: a five-year retrospective study. Sci. Rep. 2024, 14, 7695. [Google Scholar] [CrossRef]
- Hosu, M.C.; Faye, L.M.; Apalata, T. Comorbidities and Treatment Outcomes in Patients Diagnosed with Drug-Resistant Tuberculosis in Rural Eastern Cape Province, South Africa. Diseases 2024, 12, 296. [Google Scholar] [CrossRef]
Figure 1.
Demographics distribution heatmap (Gender: 1=M, 2=F; Education: 1=nil, 2=primary, 3=secondary, 4=tertiary; Income: 1=salary or wages, 2=casual, 3=unemployment insurance fund (UIF), 4=disability grant (DG), 5=none, 6=self-employed).
Figure 1.
Demographics distribution heatmap (Gender: 1=M, 2=F; Education: 1=nil, 2=primary, 3=secondary, 4=tertiary; Income: 1=salary or wages, 2=casual, 3=unemployment insurance fund (UIF), 4=disability grant (DG), 5=none, 6=self-employed).
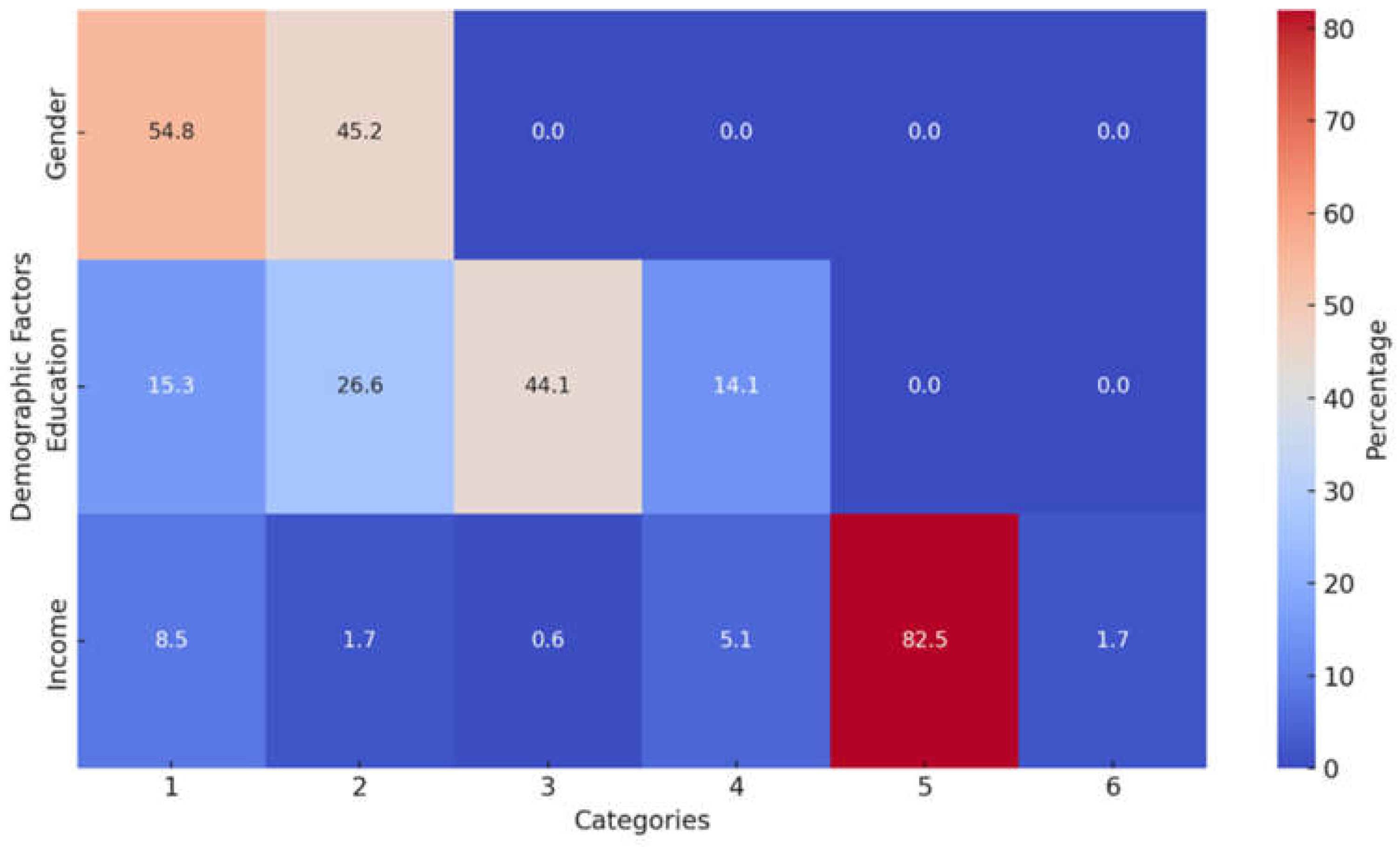
Figure 2.
Distribution of sputum conversion times stratified by social history factors (1.0=smoking, 2.0=drinking, 4.0=smoking and drinking, 5.0=smoking and drugs, 6.0=smoking, drinking and drugs, 7=none).
Figure 2.
Distribution of sputum conversion times stratified by social history factors (1.0=smoking, 2.0=drinking, 4.0=smoking and drinking, 5.0=smoking and drugs, 6.0=smoking, drinking and drugs, 7=none).
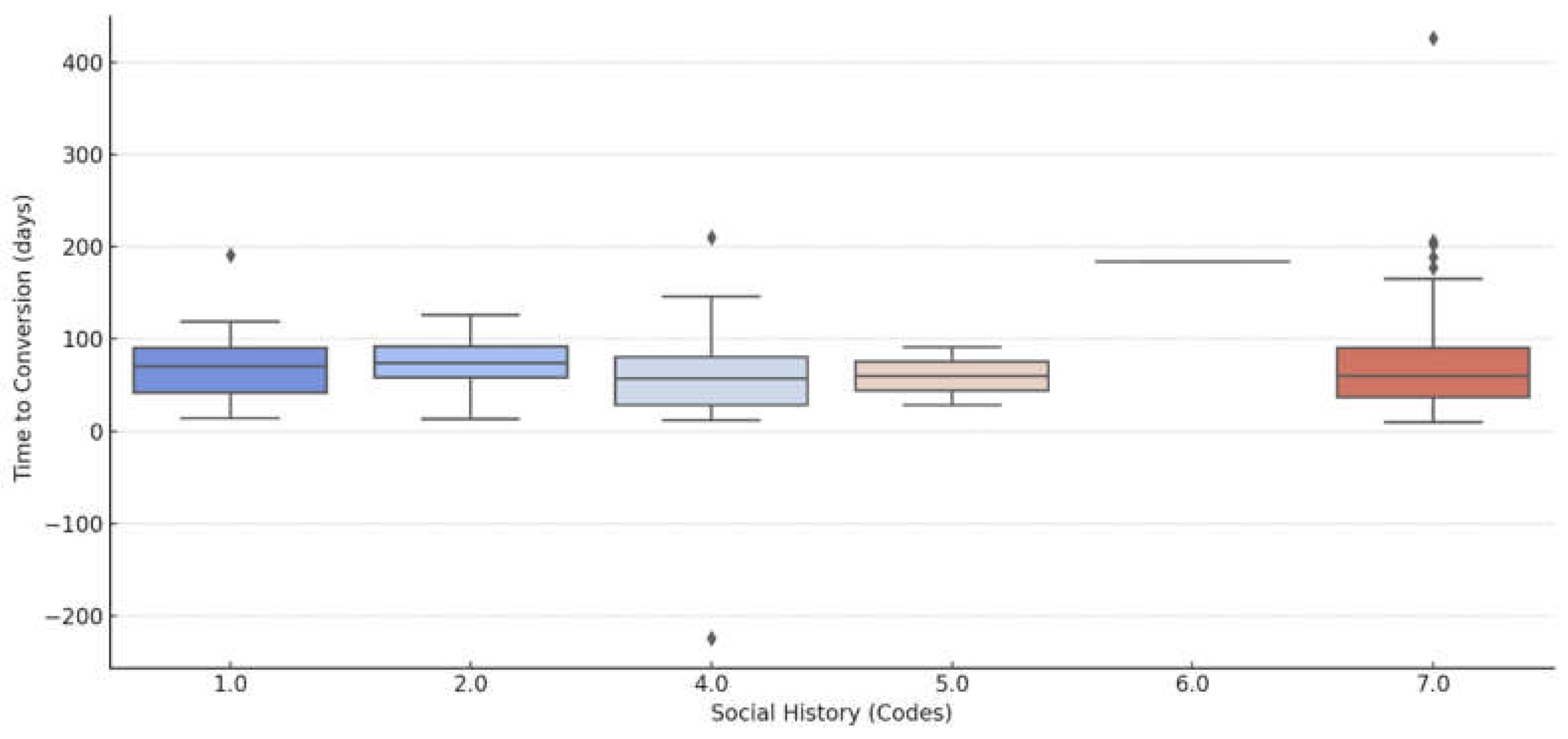
Figure 3.
Sputum conversion rates stratified by HIV status.
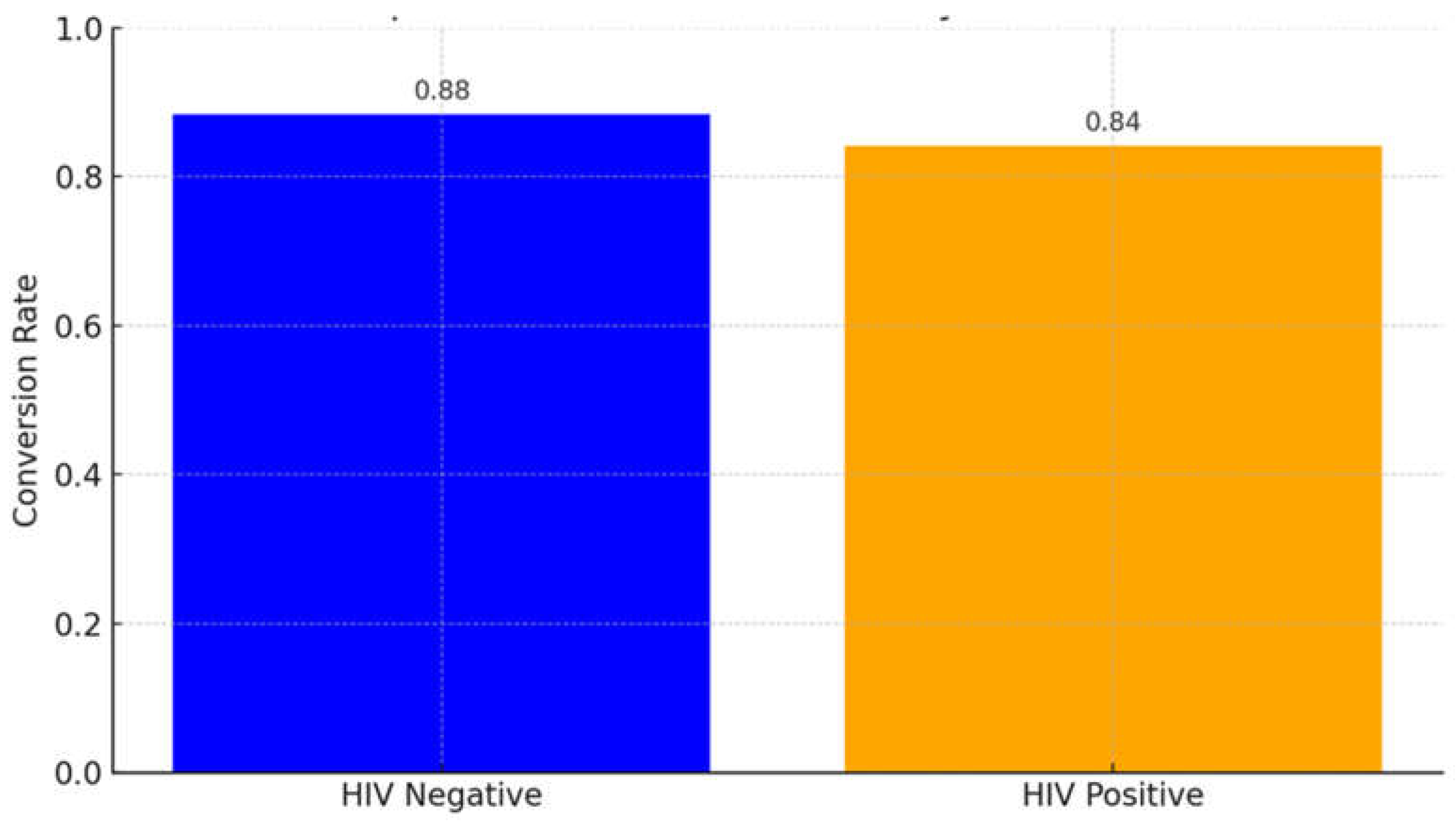
Figure 4.
Kaplan-Meier survival curve - Time to sputum conversion by HIV status.

Figure 5.
Kaplan-Meier Survival curve- Time to sputum conversion by treatment regimen.
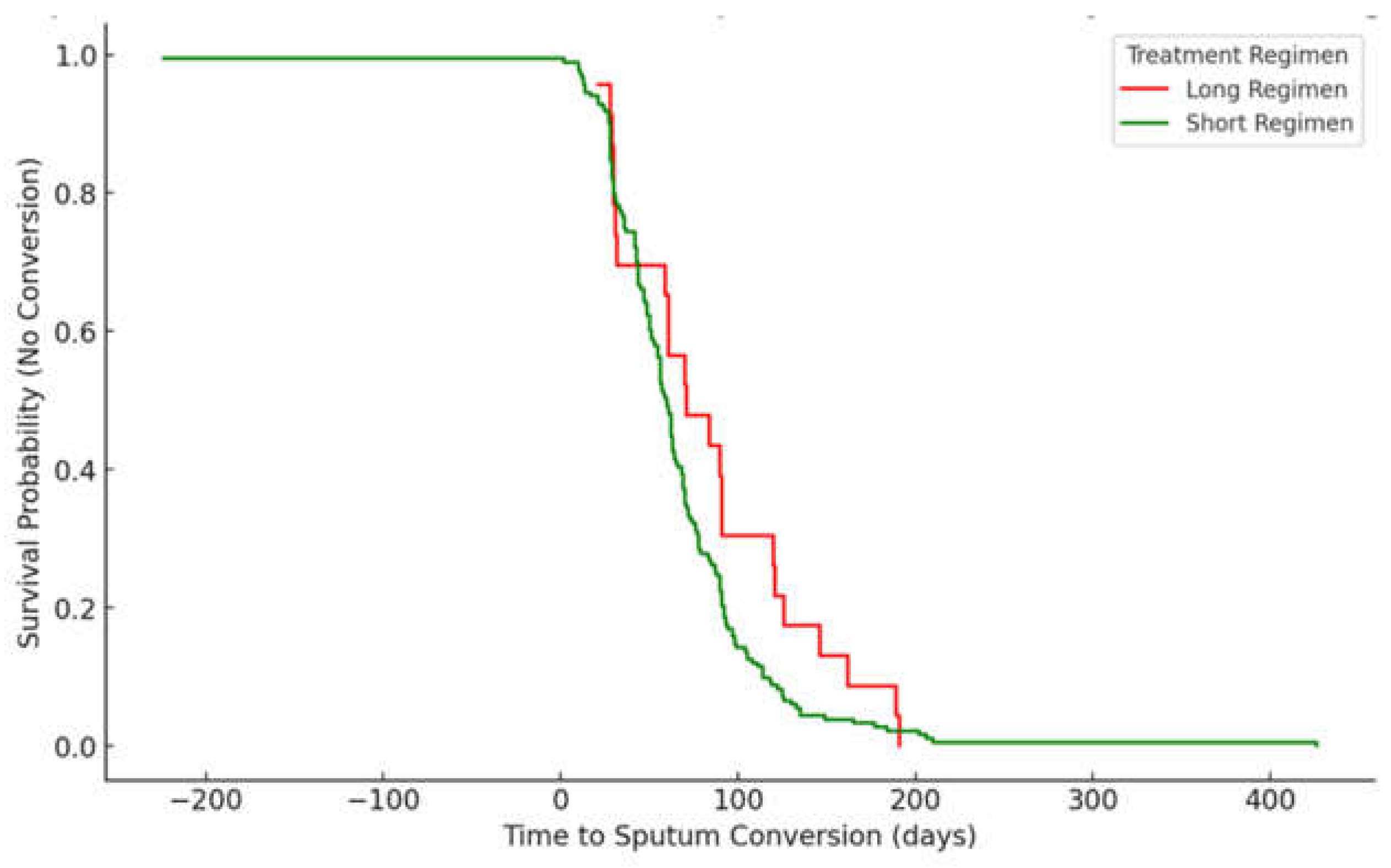
Figure 6.
Impact of regimen type on treatment outcomes.
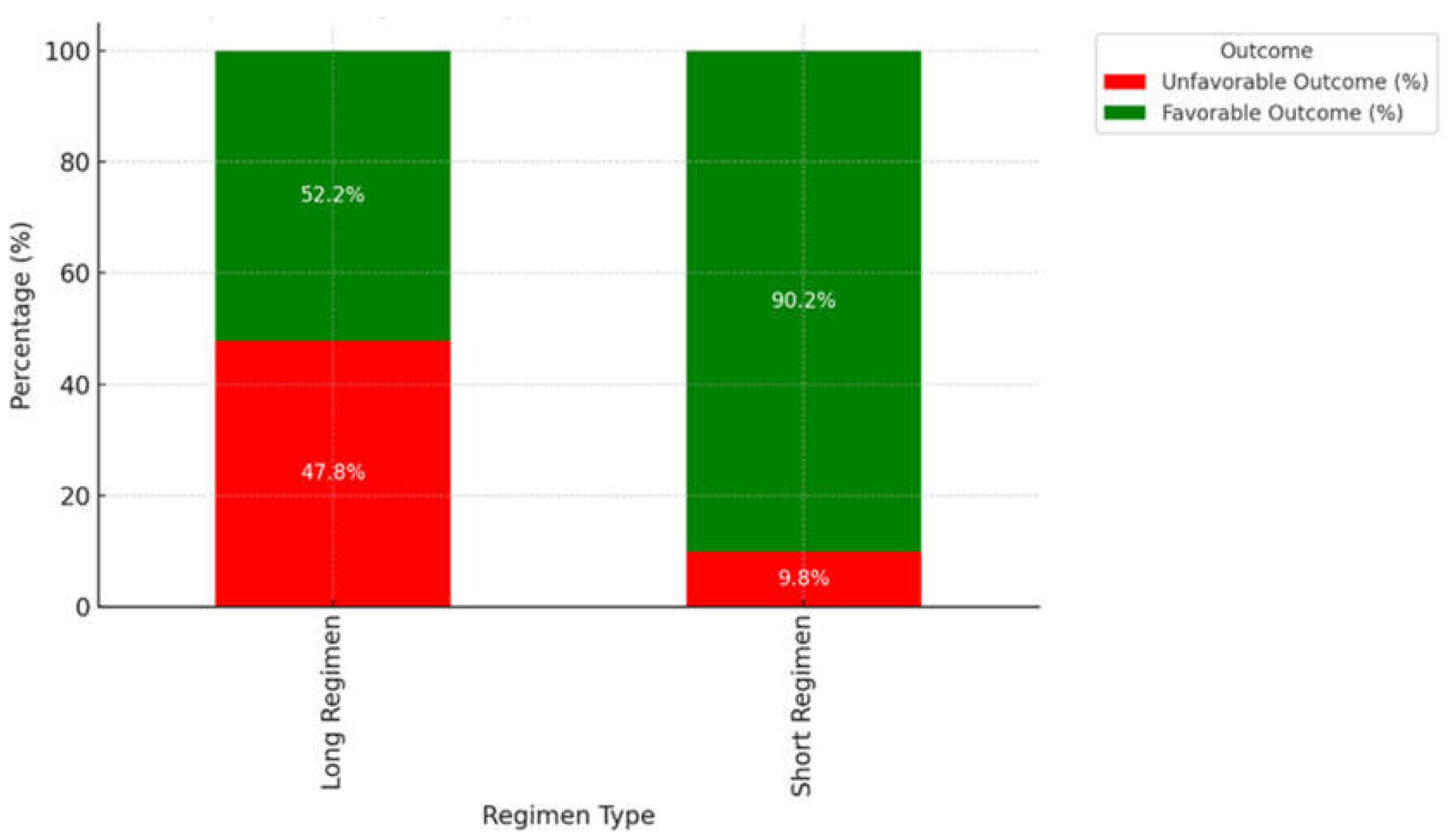
Figure 7.
Rate of treatment outcomes stratified by type of regimen.
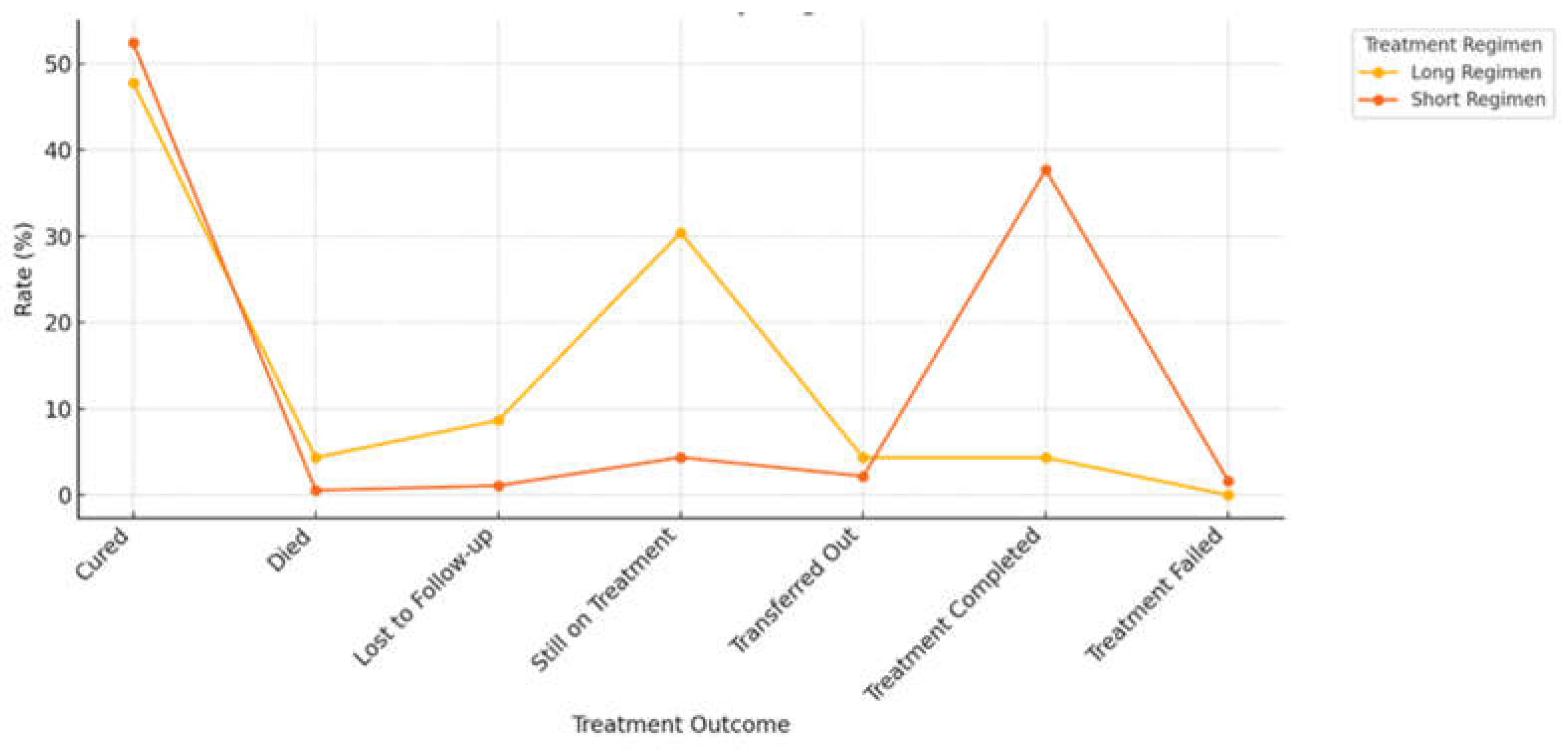
Figure 8.
Interaction of age, HIV status and comorbidities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



