Submitted:
12 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
Objectives: To examine the criteria used in return-to-play (RTP) decision-making following hip and groin injuries in soccer players. Design: Scoping review. Methods: A systematic search was conducted in PubMed, Scopus, and SPORTDiscus databases using keywords related to RTP and hip and groin injuries. Eligible studies included peer-reviewed articles in English that reported at least one RTP criterion for soccer players recovering from a hip and groin injury. Results: The search yielded 1,055 studies, of which eight met the inclusion criteria. Due to the heterogeneity of RTP criteria, we categorized them into three domains: clinical, functional, and sport-specific on-field criteria. Clinical criteria were reported in seven of the eight studies, with absence of pain being the most frequently described criterion. Functional criteria were present in six studies, with strength assessments being the most commonly used measure. Sport-specific or pitch-based criteria were reported in six studies, indicating a wide variation in testing approaches. Conclusions: This scoping review summarizes the current RTP criteria for soccer players recovering from hip and groin injuries, highlighting existing gaps in the literature and the need for further research. It provides practitioners with guidance on RTP decision-making and emphasizes the importance of using a combination of clinical, functional, and sport-specific criteria in RTP assessments.
Keywords:
Soccer
; rehabilitation
; hip
; RTP
; hip and groin injury
; sport-specific testing
; clinical assessment
What is Already Known
- Returning to sport after injury involves a complex decision-making process, where multiple stakeholders assess various criteria to minimize reinjury risk and optimize RTP.
- RTP decisions rely on clinical, biological, and functional criteria and no definitive evidence exists on the most effective criteria for hip and groin injuries in soccer.
What This Study Adds
- RTP assessments should include clinical, functional, and soccer-specific on-field criteria for a comprehensive evaluation.
- Sport-specific tests should complement clinical and functional measures to reflect match demands.
- Effective communication and interdisciplinary collaboration between medical, performance, and coaching staff is essential for objective RTP decisions.
Introduction
Hip and groin injuries are prevalent in high-intensity team sports, especially those that require acceleration, sudden changes in direction, and kicking. 10,26 These biomechanical demands place significant strain on muscles, tendons, and the pubic symphysis, making athletes more susceptible to both acute and overuse injuries. Injury incidence rates for hip and groin injuries in both elite 23 . and amateur 17 levels range from 1.5 to 1.9 injuries per 1000 hours of total exposure, with a recurrence rate of approximately 18 percent within two months 25 Epidemiological studies12 indicate that a professional soccer team consisting of 25 players can expect around four hip or groin injuries per season, highlighting the substantial burden these injuries place on teams and medical staff. A thorough understanding of injury incidence and recurrence rates is essential for designing effective rehabilitation protocols and injury prevention strategies.
The decision-making process regarding safe return-to-play is crucial, as premature return significantly increases the risk of reinjury, extends time-loss, and negatively affects performance. To ensure a safe and efficient return, a multidisciplinary approach that integrates input from medical professionals, performance specialists, and coaching staff is necessary. In recent years, scientific interest in return-to-play assessment has grown, largely due to persistently high reinjury rates,13,25 inconsistencies in return-to-play protocols, 5 and prolonged recovery durations. 13 Addressing these challenges requires a standardized and evidence-based approach to return-to-play decision-making, ensuring that players can resume competition safely and effectively. The Doha agreement provided a standardized, expert consensus-based classification system for groin pain terminology and definitions, significantly advancing our understanding of hip and groin injuries. 30This framework has proven invaluable in improving communication, diagnostic capabilities, and research efforts related to athletic groin pain. Despite these contributions, the agreement lacked consensus on the specifics of rehabilitation and failed to define criteria for safe return to play (RTP). The lack of standardized RTP protocols hinders clinicians, leading to subjective decisions and inconsistent rehabilitation strategies across various sports medicine settings. The first World Congress on Sports Physical Therapy produced a standardized set of consensus guidelines for RTP in sports to improve the consistency of decision-making processes. 3These guidelines, however, offered a generalized approach, failing to account for the nuances of specific injuries like groin pain. Although the framework established a foundation of scientific evidence for RTP after hip and groin injuries, its scope was restricted. The principal recommendation focused on hip adduction strength as the central, empirically supported criterion for RTP authorization, failing to consider other critical functional or sport-specific demands necessary for full recovery.
Recent studies suggest a need for a more encompassing and multi-faceted methodology in RTP. 2A Delphi study examined the refinement of return-to-play (RTP) criteria in the context of persistent adductor-related groin pain, incorporating a more comprehensive assessment. 29 In this study, the expert panel’s consensus was that hip adduction strength alone does not adequately determine readiness for return to participation. As an alternative, they recommended incorporating strength assessments, performance evaluations, and sport-specific testing to facilitate a safe and effective resumption of competitive play. The current findings emphasize the dynamic nature of RTP research, thereby necessitating the development of more individualized and objective assessment protocols that consider both functional recovery and the unique demands of the athlete’s sport. The high incidence of hip and groin injuries in soccer, coupled with a significant re-injury rate, underscores the absence of a universally accepted return-to-play (RTP) framework or standardized criteria. A lack of definitive guidelines may result in inconsistencies in rehabilitation practices, thus rendering return-to-play (RTP) decisions highly variable and subjective across various medical teams. Moreover, inadequate or unclear RTP data may negatively affect athlete recovery, resulting in frustration, unmet expectations, and heightened psychological barriers, including kinesiophobia. This uncertainty may also impair practitioners’ capacity to offer precise, evidence-based return-to-play (RTP) recommendations, potentially extending recovery periods and heightening the risk of re-injury.
The aim of this scoping review was to identify and analyze the RTP criteria reported in the existing literature for assessing soccer players’ readiness to return following a primary hip and groin injury. The absence of a globally accepted RTP framework suggests a significant research gap, necessitating a more rigorous and data-driven methodology. Through a mapping of current RTP criteria, this review aims to augment practitioners’ understanding of the field, illuminate existing practices, and expose critical deficiencies in RTP decision-making processes. Furthermore, this review will provide recommendations for future research to develop standardized, objective, and sport-specific return-to-play guidelines, thereby improving rehabilitation outcomes and minimizing reinjury rates in soccer players.
Methods
This scoping review aimed to identify key concepts, categorize existing evidence, and highlight research gaps within the field of return-to-play following hip and groin injuries in male soccer players. Specifically, it provides an overview of the current research used to establish return-to-play criteria and evaluates the consistency and applicability of these criteria in clinical practice. The review follows the scoping review framework initially proposed by Arksey and O’Malley in 2005 4 and later by Levac et al.21 ensuring a systematic and transparent methodological approach. The primary research question was to describe the return-to-play criteria reported in the literature for assessing safe return after a primary hip and groin injury in soccer players (Table 1). The scoping review protocol was uploaded on the Open Science Framework on October 2, 2023, and the protocol is accessible through the following registration DOI: https://doi.org/10.17605/OSF.IO/XUCQV
Eligibility Criteria
This scoping review included studies published in peer-reviewed journals, as well as those classified as “in press” or “ahead of print.” Only English-language studies from 2003 onward were eligible for inclusion. The target population consisted of male and female soccer players at any competitive level, with no age restrictions. Studies involving disabled athletes or those participating in adapted sports were excluded. Eligible studies needed to describe and validate return-to-play criteria used to assess soccer players following a hip and groin injury. In accordance with the Doha agreement on groin pain 30 all recognized types of groin injuries were considered, including adductor-related, iliopsoas-related, inguinal-related, pubic-related, and hip-related groin pain. To be included, studies had to report at least one return-to-play criterion used to determine whether athletes were ready to resume soccer. Review studies were excluded from this scoping review.
Search, Extraction and Selection Process
The following electronic databases were searched: PubMed, Scopus, and SPORTDiscus. All databases were searched, and only papers in English were considered. Title and abstracts were checked to decide if they potentially met the inclusion criteria. The selected studies’ full text was subsequently assessed to decide on inclusion. Two blinded authors accessed the included articles (AK and PP). If an agreement was not reached, this was initially resolved between the two reviewers, and, if necessary, the two researchers would contact a third reviewer (MB) for a final decision. The online software “Rayyan – the intelligent systematic review” web app (www.rayyan.ai) was utilized to manage the searched studies. Duplicates were automatically deleted by the software. The keyword search was based on the MeSH subject headings. The PRISMA flowchart presents the results management (Figure 1). The primary search strategy is available in the Supplementary File 1.
Scoping reviews typically do not require a formal risk of bias assessment, as their primary objective is to map existing literature rather than critically evaluate or synthesize findings, as seen in systematic reviews or meta-analyses.14 Although a formal risk of bias tool was not applied, potential sources of bias were considered at multiple levels. A detailed list is provided as a Supplementary File 2. However, when the quality of evidence is a concern or when a review involves clinical decision-making, incorporating a risk of bias assessment can significantly enhance the credibility, transparency, and methodological rigor of the findings. To improve the methodological quality and consistency of scoping reviews, a 22-item Scoping Review Checklist was developed (Supplementary File 3) following rigorous, evidence-based recommendations8 This checklist provides a structured approach to ensure comprehensiveness, reduce bias, and improve reporting standards in scoping review methodology.
Results
Study Identification and Selection
A total of 1,066 records were imported into the Rayyan web application (www.rayyan.ai) for systematic review management. The software automatically removed 622 duplicate records, leaving 433 studies for title and abstract screening. Following this initial screening, 126 studies were deemed eligible for full-text review. However, 118 articles were excluded for the following reasons: absence of RTP criteria (n = 99), participants not being soccer players (n = 12), and unavailability of full text (n = 6). At the conclusion of the review process, eight studies met the inclusion criteria and were included in the final analysis.
RTP Criteria
Due to the heterogeneity of the criteria, we decided to group the criteria into three main domains: clinical, functional and sport-specific/on-field-based criteria. One criterion -time to RTP11- was considered as a clinical criterion. The Table 2 shows in detail the criteria grouped into the three domains. The studies and the RTP criteria included in this scoping review are summarized in Table 3.
The absence of pain was the most frequently utilized criterion in seven of the eight included studies, yet the methods used to assess pain varied significantly. Pain-free movement assessments were commonly employed, including full hip range of motion as a return-to-play (RTP) criterion. 1 Pain-free execution of the Copenhagen exercise was also identified as a significant marker of recovery, highlighting its role in functional rehabilitation. 7 Additional assessments included pain-free activities of daily living and unrestricted hip range of motion as indicators of RTP readiness. 11 Orthopedic testing, palpation, and functional exercise performance were also considered prerequisites for RTP clearance. 15 The assessment of pain during adductor muscle stretching, squeeze tests at multiple angles such as 0° and 60° of hip flexion, and straight-leg sit-ups further reinforced the importance of symptom resolution before clearance. 16 24 31 Moreover, only one study incorporated time 11 as a return-to-play criterion; however, a precise definition and explanation of the time measurement and its significance to the return-to-play process were absent.
Beyond pain assessment, additional clinical evaluations were integrated into RTP decision-making. Imaging modalities, such as MRI and ultrasound, were incorporated to assess tissue integrity and guide RTP progression. 1 However, the specific imaging markers necessary to determine RTP readiness were not clearly defined. Research has indicated that while MRI and ultrasound findings can help evaluate structural abnormalities, they do not always correlate with an athlete’s functional capacity to return to play. 6,27Additional assessments, including the Hip and Groin Outcome Score (HAGOS), initial medical examination, and osteopathic evaluations, were also used to inform RTP decisions, but the criteria for defining clearance thresholds remained inconsistent. 11,16 This inconsistency underscores the need for further research to standardize clinical RTP criteria and improve decision-making accuracy.
Functional RTP Criteria
A variety of functional return-to-play criteria were highlighted in the reviewed studies, emphasizing the importance of restoring strength, ensuring high-quality movement, and achieving optimal neuromuscular control. Adductor isometric strength asymmetry of less than 10% was frequently reported as a benchmark for RTP, ensuring adequate muscle balance between limbs (Abate et al., 2023).1 Isometric adductor strength was used as a fundamental measure to determine recovery, although specific assessment protocols varied across studies (Chiesa et al., 2023). 7Objective assessment of muscle function recovery and force production capacity before patient discharge was achieved by measuring maximal adductor muscle squeeze strength at hip flexion angles of 0°, 45°, and 90° (McAleer et al., 2017).24
According to Jardí et al. (2014),16 the ability to return to competitive play (RTP) hinges on achieving lumbo-pelvic stability, with their research indicating that a Level 4 stability rating is the minimum threshold necessary to ensure safe reintegration into competition. To strengthen the core muscles, a program of targeted concentric-eccentric exercises focusing on the rectus abdominis and obliques was prescribed, consisting of two sets of seven repetitions performed three times weekly. Eberbach et al. (2021)11employed the Functional Movement Screen (FMS) as a means of comprehensively evaluating the efficiency of movement patterns and identifying any underlying movement deficits that could negatively impact an individual’s performance following an injury, thereby contributing valuable insights into post-injury rehabilitation strategies. Researchers utilized pre-injury slide board skating scores as a comparative measure to evaluate the restoration of neuromuscular control and coordination in athletes, thereby assessing their suitability for unrestricted competition. 31
A primary return-to-play criterion emphasized in rehabilitation programs is the ability to perform exercises without experiencing pain, with at least one study highlighting pain-free strengthening exercises as a prerequisite for medical clearance to return to activity. 16 To ensure athletes could perform high-intensity functional tasks without experiencing any discomfort, asymptomatic performance during sport-specific movements and training drills was established as a necessary condition for a return to play (RTP). 15 Collectively, the studies show how strength, neuromuscular, and functional movement assessments can be used to determine when soccer players are ready to return to play (RTP) after experiencing groin injuries, providing valuable insights into the recovery process.
Sport-Specific on-Field RTP Criteria
Sport-specific or pitch-based criteria were described in six studies, emphasizing the necessity of replicating game-related demands during RTP assessments. The ability to complete soccer-specific activities without pain was consistently identified as an essential marker of RTP readiness. 1 Performance-based assessments included maximal ball strike velocity, the Yo-Yo Intermittent Recovery Test, and the Pro-Agility Test, which served as reliable indicators of an athlete’s ability to return to competition. 7
Agility-based assessments played a crucial role in RTP evaluations. The Agility T-Test was incorporated to assess movement efficiency and directional changes, critical components for soccer players recovering from groin injuries. 11 Meeting pre-injury pitch-based intensities and completing full-team training sessions without limitations were also considered essential markers of readiness for match participation. 16 The implementation of GPS tracking further refined RTP decision-making by ensuring that athletes met 95-100% of their pre-injury sprinting and movement patterns before receiving clearance for competitive play. 28
A progressive return-to-play approach was also documented, involving structured running programs designed to gradually reintroduce players to high-intensity efforts. Sprint-based assessments, such as the 20m shuttle run test, the 5m sprint, and the 20m sprint, were included to objectively evaluate an athlete’s ability to perform under game-like conditions. 31 Despite the widespread application of these sport-specific criteria, inconsistencies in testing protocols continue to present challenges in standardizing return-to-play assessments across different levels of play.
Discussion
The objectives of this review were conducted to determine and consolidate the criteria used by medical and performance specialists to make return-to-play (RTP) decisions for patients with hip and groin injuries. Moreover, the review analyzed gaps in the extant literature and offered recommendations for future research endeavors. Three primary domains—clinical, functional, and sport-specific on-field assessments—were used to categorize the identified RTP criteria. This structured classification guides practitioners through the rehabilitation continuum, integrating considerations of tissue demands, progressive loading, and sport-specific performance criteria for safe and effective return to competition. Nevertheless, in some instances, categorizing specific criteria presented a challenge owing to overlapping clinical, functional, and sport-specific evaluations. This underscores the intricate nature of RTP decision-making and necessitates the development of a more standardized and precise framework to ensure consistent assessment of athletes’ readiness for return to play.
This analysis predominantly utilizes Level 4 evidence, which consists of case series and uncontrolled observational studies. These studies offer substantial clinical understanding based on practical rehabilitation experience and objective functional assessments in the context of return-to-play decisions for groin injuries. However, the lack of control groups increases the likelihood of bias, limiting causal inferences and the generalizability of findings. While foundational to clinical practice, the lack of standardized RTP protocols hinders their practical implementation. To enhance the reliability and clinical applicability of return-to-play (RTP) frameworks and promote evidence-based clinical decision-making, future research should concentrate on large-scale, prospective, multicenter trials that utilize objective strength measurements and standardized RTP criteria.
Clinical Criteria
Pain was consistently reported as a primary criterion across all studies in this review. However, significant variability exists in how pain is assessed across studies. While some investigations rely on clinical evaluations, others incorporate functional and sport-specific assessments to determine RTP readiness. Evidence-based rehabilitation guidelines emphasize that athletes should achieve pain-free adductor squeeze tests at 0°, 45°, and 90° of hip flexion, in addition to demonstrating high Hip and Groin Outcome Scores (HAGOS), to be considered for RTP clearance. 19 Despite agreement on the importance of pain assessment,30 there remains considerable inconsistency in its application, leading to challenges in standardizing RTP criteria.
Assessing hip range of motion (ROM) has been widely adopted as a determinant of RTP, with full, pain-free ROM being considered an essential component of recovery. 1Successful, pain-free completion of high-demand rehabilitation exercises, including the Copenhagen exercise, serves as a valuable assessment metric, especially considering its emphasis on strengthening adductor muscles crucial for soccer performance. 7,16Moreover, unrestricted range of motion and the absence of pain during activities of daily living further corroborate an athlete’s capacity to tolerate progressively increased training loads without symptom exacerbation. 11Return-to-play (RTP) criteria now include additional assessments such as orthopedic examinations, palpation, and movement evaluations. Pain-free adductor muscle stretching, squeeze tests at various hip flexion angles, and straight-leg sit-ups are commonly employed to validate recovery.16
Three studies utilized integrated medical, orthopedic, and osteopathic assessments as further return-to-play determinants. The absence of a description of the specific components of the medical evaluations limits the clarity of their contribution to the assessment of musculoskeletal structures, pain tolerance, and tissue capacity. An Italian consensus statement concerning groin pain syndrome underscored the significance of comprehensive clinical assessment in return-to-play (RTP) determinations but omitted prioritization criteria for evaluation elements.29 The application of imaging techniques, including magnetic resonance imaging and ultrasound, in real-time treatment planning is a subject of ongoing debate. Certain rehabilitation protocols integrate imaging techniques to track tissue regeneration and evaluate structural soundness, frequently in conjunction with HAGOS scores. 1Currently, no definitive MRI or ultrasound findings conclusively indicate readiness for a return to athletic activity. Research evaluating the prognostic capacity of neuroimaging in RTP outcomes indicates that, although MRI and ultrasound can detect structural lesions, their utility in forecasting functional recovery remains constrained. 6Discrepancies between imaging findings and RTP timelines have generated contrasting viewpoints among experts. Some advocate for imaging in tracking rehabilitation progress, while others prioritize functional evaluations over radiological interpretations.29 Due to evidentiary inconsistencies, imaging modalities may offer supplementary support yet should not serve as the sole basis for return-to-play decisions.2,3
Modern RTP frameworks prioritize a balance between tissue repair and progressive loading, de-emphasizing exclusive reliance on imaging data. This perspective is in accordance with prevalent rehabilitation paradigms which prioritize functional performance as the primary indicator of RTP readiness.18 While a direct correlation between hip mobility and increased groin injury risk remains unestablished, maintaining sufficient range of motion, pain-free articulation, and balanced musculature is crucial for injury prevention by mitigating compensatory movement patterns .30 Persistent pain, limited range of motion, and impaired strength may suggest inadequate tissue healing, thereby increasing the risk of re-injury and delaying return to play. 6 The integration of objective strength and movement assessments is recommended for improved return-to-play (RTP) outcomes. This supports a paradigm shift towards functional criteria that reflect an athlete’s ability to meet the physical demands of soccer. 27 Subjective and objective metrics should both be included in a thorough RTP evaluation. Subjective pain reports necessitate corroboration through clinical evaluations, functional testing, and, when indicated, imaging studies. The implementation of standardized RTP protocols integrating diverse assessment methodologies is anticipated to improve decision-making accuracy, mitigate reinjury risk, and optimize long-term athletic performance. 29Future studies should prioritize the enhancement and validation of objective return-to-play criteria to ensure uniformity in clinical practice and improve rehabilitation approaches. Evidence-based, multifactorial approaches enable medical professionals to make more informed return-to-play (RTP) decisions, thereby mitigating reinjury risk and enhancing player safety and performance. 2,3
Functional Criteria
Strength was the most frequently reported return-to-play (RTP) criterion, mentioned in seven of the eight included studies (58.3%). Most studies assessed adductor muscle strength, with pre-injury strength levels commonly used as a benchmark for RTP clearance. Various strength assessment methods were identified, including absolute maximum isometric voluntary contractions,24 maximum squeeze scores at different hip angles, 24eccentric-to-concentric exercises,31 and inter-limb isometric strength symmetry.1 Strength plays a critical role in RTP decision-making, as it provides valuable insight into muscle tissue capacity and its ability to tolerate progressive loading. Research has shown that male soccer players with lower isometric hip adduction strength are at a higher risk of hip and groin injuries, reinforcing the importance of strength assessments in RTP protocols. 1Despite its widespread use in clinical practice, there is no clear consensus on the most effective contraction type for strength evaluation, nor agreement on which specific metric (symmetry, peak force, time to peak force, rate of force development, or impulse speed) best represents muscle function and recovery. Among the studies reviewed, the only tool identified for assessing isometric adductor strength was the handheld dynamomete. 1While this tool is widely used, it has limitations regarding standardization and inter-rater reliability, which may influence RTP decisions.
Lumbo-pelvic stability was also a commonly reported functional RTP criterion, particularly for athletes recovering from pubic-related groin injuries.16 The Wisbey-Roth Core Stability Grading System was employed to classify lumbo-pelvic stability and assess its impact on osteitis pubis. Athletes were only cleared to return to play upon reaching Level 5 on this grading system.16 Substantial evidence supports the association between lumbo-pelvic stability and hip and groin injuries, highlighting the necessity for rehabilitation strategies targeting core control. A recent prospective study indicated that muscular imbalances between the adductors and abductors could contribute to lumbo-pelvic dysfunction, particularly in sports involving high-intensity movements such as sudden direction changes, acceleration, and kicking. These biomechanical alterations increase the risk of recurrent groin injuries, emphasizing the importance of neuromuscular control in RTP decision-making.18 Moreover, deficits in core stability and pelvic alignment have been linked to poor movement efficiency and increased compensatory loading, further stressing the need for targeted rehabilitation before RTP.
Additionally, movement quality assessments were included in the RTP criteria of some studies. Eberbach et al. (2021)11 incorporated movement screening tools such as the Functional Movement Screen (FMS), the Square Hop Test (SHT), and the Y-Balance Test (YBT) to identify functional movement deficits, neuromuscular control impairments, and balance deficiencies. However, the literature presents conflicting findings on whether tests such as the YBT-LQ 20and FMS 22can accurately predict injury risk or identify correctable movement deficits. While these tools are used to screen for injury risk and assess movement efficiency, no clear evidence supports their use as RTP clearance criteria. Additionally, there is no consensus regarding the best movement assessment protocols for RTP, creating inconsistencies in clinical practice.
In the RTP decision-making process, it is essential to evaluate both the quantity and quality of movement. RTP test batteries should integrate both quantitative functional tests (e.g., strength assessments) and qualitative tests (e.g., movement efficiency assessments) to ensure comprehensive evaluation of an athlete’s ability to return to full training and competition. Functional criteria provide critical insights into an athlete’s ability to withstand progressive loading, guiding rehabilitation and performance monitoring throughout the RTP continuum. These tests track an athlete’s progression, offering valuable feedback to clinicians and coaches to optimize recovery timelines and reduce reinjury risk. 9Despite the widespread use of functional assessments, further research is needed to refine these criteria, ensuring standardization and reliability across different levels of play.
Sport-Specific on-Filed Criteria
A substantial majority (75%) of the reviewed studies integrated sport-specific, on-field assessments into their return-to-play (RTP) protocols. These criteria centered on evaluating physical performance preparedness using pre-determined capacity tests, specifically assessing aerobic endurance, 11 agility,28 sprinting,24 and running capabilities.31 Athletic participation was quantified in these tests by assessing an athlete’s capacity to complete a single full-squad training session 16or a sequence of three consecutive unrestricted training sessions. 7 Moreover, in the context of sport-specific return-to-play assessments, one study emphasized the importance of evaluating maximum ball strike velocity,7 underscoring the need for skill-based performance assessments when determining RTP readiness. A comprehensive series of tests, designed to replicate the physical stresses of soccer, forms the basis of the sport-specific on-field criteria, assessing an athlete’s ability to withstand the demands of competition. These assessments replicate the unique movement demands of soccer to ensure the athlete’s safe return to play. Despite the empirical basis for progressive on-field reintegration, a dearth of research exists concerning optimal assessment protocols for monitoring progress, GPS-based workload prescription, and return-to-play rehabilitation guidance.29 Furthermore, the limitations of current RTP protocols are evident in their failure to account for individual biomechanical and physiological differences, thereby obstructing the establishment of a universal gold standard for return-to-play readiness. Despite the proposition of progressive return-to-play guidelines in some studies, the effectiveness of these protocols in reducing re-injury rates remains ambiguous due to varying methodological approaches. Standardized, evidence-based return-to-play (RTP) guidelines would optimize decision-making, reduce re-injury risk, and ensure athletes’ full conditioning prior to resuming competition.
Clinical Implications
The objective of this scoping review was a comprehensive synthesis of the published literature on return-to-play (RTP) criteria after hip and groin injuries among soccer players. The heterogeneity of reported RTP assessments necessitated categorization into three distinct domains: clinical, functional, and sport-specific on-field criteria. While a scoping review does not evaluate the validity of individual studies, it offers valuable insights into prevalent methodologies and provides general guidance for practitioners. The study’s findings reveal a contribution from all three RTP assessment categories to both progression monitoring and decision-making. Nevertheless, a conclusive determination of the appropriate tests for each defined RTP stage lacks sufficient evidentiary support. A comprehensive evaluation necessitates a multidisciplinary approach, given the diversity of the tests, and requires the involvement of medical, performance, and coaching staff. The crucial role of functional testing lies in its ability to detect residual deficits that may compromise an athlete’s return to participation. Implementing objective functional assessments consistently allows practitioners to preemptively detect and manage impairments, thus mitigating the probability of recurrence. Throughout the rehabilitation process, ongoing evaluation is necessary to guarantee that advancements in strength, mobility, neuromuscular control, and sport-specific training align with safe return-to-play guidelines. Future investigations should concentrate on establishing standardized RTP testing frameworks and determining the optimal assessment tools for each stage of recovery, prioritizing reliability and validity.
Limitations and Future Directions
This review included a range of diagnoses falling under the umbrella term “groin pain,” and diverse rehabilitation approaches. The inherent variability and heterogeneity of hip and groin injuries may limit the RTP criteria’s overall specificity and applicability. In addition, this review considered only three of the six groin injury classifications outlined by the Doha Agreement. The incomplete nature of this coverage limits the extent to which the findings can be generalized to all groin pathologies. Furthermore, this review was confined to peer-reviewed English-language publications, which may have resulted in the exclusion of pertinent research from non-English-speaking areas. Given the prevalence of groin pain in sports involving multidirectional movement, return-to-play criteria have been studied extensively beyond the context of soccer. This review’s exclusive focus on soccer literature may have overlooked relevant findings from research on other high-impact sports, including ice hockey, Australian rules football, and rugby. Furthermore, this scoping review acknowledges the inherent methodological limitations; its primary purpose is to chart existing research, not to critically evaluate study quality or synthesize quantitative data. Subsequent research efforts should concentrate on validating RTP criteria for specific groin pain diagnoses, refining assessment protocols according to RTP stages, and evaluating the reliability and validity of diverse testing methodologies within the context of soccer-specific rehabilitation. Evidence-based recommendations could benefit from a systematic review or meta-analysis to achieve a more robust synthesis and critical appraisal.
Conclusions
This study employed a scoping review methodology to examine the established return-to-play (RTP) criteria following hip and groin injuries sustained by soccer athletes, with a focus on identifying critical clinical, functional, and sport-specific evaluation methods. Despite the identification of numerous return-to-play markers in current literature, there is no established consensus regarding the optimal selection and sequencing of these criteria during rehabilitation. This review integrates current RTP frameworks and underscores crucial research deficiencies. Clinicians should integrate clinical, functional, and sport-specific on-field criteria into RTP assessments for a comprehensive evaluation of an athlete’s recovery and readiness to return to performance. Comprehensive evaluations facilitate ongoing monitoring, thereby ensuring rehabilitation programs align with the unique physical and biomechanical requirements of soccer. The variability in reported criteria, however, indicates a need for enhanced standardization and validation of return-to-play protocols to optimize clinical decision-making and minimize the risk of reinjury. Future studies should prioritize the establishment of evidence-based return-to-play (RTP) timelines, the refinement of diagnosis-specific criteria, and an exploration of the reliability of functional and sport-specific assessments in determining RTP readiness. A standardized RTP framework would improve uniformity across clinical and performance settings, leading to safer and more effective return-to-play protocols for soccer athletes recovering from hip and groin injuries.
Funding
This research did not receive any specific grand from funding agencies in the public, commercial or not-for – profit sectors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Abate, M.; Sammarchi, L.; Calà, R.; Milesi, G.; Poerio, C.S.; Del Vescovo, R.; Corvino, A.; Pizzi, A.D.; Cocco, G.; Salini, V. Isolated adductor longus avulsion in a young semi-professional football player: Imaging contribution and therapeutic considerations. J. Clin. Ultrasound 2023, 51, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Bizzini, M.; Bahr, R. It is time for consensus on return to play after injury: five key questions. Br. J. Sports Med. 2015, 50, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Ardern CL, Glasgow P, Schneiders A, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med. 2016;50(14):853-864.
- Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology: Theory and Practice. 2005;8(1):19-32.
- Bisciotti GN, Corsini A, Volpi P. Return-to-Play after Lower Limb Muscle Injury in Football: The Italian Consensus Conference Guidelines. Return-to-Play after Lower Limb Muscle Injury in Football: The Italian Consensus Conference Guidelines. Published online 2021:1-165.
- Branci, S.; Thorborg, K.; Nielsen, M.B.; Hölmich, P. Radiological findings in symphyseal and adductor-related groin pain in athletes: a critical review of the literature. Br. J. Sports Med. 2013, 47, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, C.; Lopes, A.D.; Nolan, D. Functional Assessment and Treatment of Complex Pubic-Related and Adductor-Related Groin Pain in a Division I College Soccer Player: Case Report. JOSPT Cases 2023, 3, 134–143. [Google Scholar] [CrossRef]
- Cooper, S.; Cant, R.; Kelly, M.; Levett-Jones, T.; McKenna, L.; Seaton, P.; Bogossian, F. An Evidence-Based Checklist for Improving Scoping Review Quality. Clin. Nurs. Res. 2019, 30, 230–240. [Google Scholar] [CrossRef]
- Dunlop, G.; Ardern, C.L.; Andersen, T.E.; Lewin, C.; Dupont, G.; Ashworth, B.; O’driscoll, G.; Rolls, A.; Brown, S.; McCall, A. Return-to-Play Practices Following Hamstring Injury: A Worldwide Survey of 131 Premier League Football Teams. Sports Med. 2019, 50, 829–840. [Google Scholar] [CrossRef]
- Dupré, T.; Tryba, J.; Potthast, W. Muscle activity of cutting manoeuvres and soccer inside passing suggests an increased groin injury risk during these movements. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Eberbach, H.; Fürst-Meroth, D.; Kloos, F.; Leible, M.; Bohsung, V.; Bode, L.; Wenning, M.; Hagen, S.; Bode, G. Long-standing pubic-related groin pain in professional academy soccer players: a prospective cohort study on possible risk factors, rehabilitation and return to play. BMC Musculoskelet. Disord. 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef]
- Ekstrand, J.; Krutsch, W.; Spreco, A.; van Zoest, W.; Roberts, C.; Meyer, T.; Bengtsson, H. Time before return to play for the most common injuries in professional football: a 16-year follow-up of the UEFA Elite Club Injury Study. Br. J. Sports Med. 2019, 54, 421–426. [Google Scholar] [CrossRef]
- Giaume, L.; Lamblin, A.; Pinol, N.; Gignoux-Froment, F.; Trousselard, M. Evaluating cognitive bias in clinical ethics supports: a scoping review. BMC Med Ethic- 2025, 26, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Harmath, D.M.; Lejkowski, P.M. Pubic and adductor related groin pain in an athlete: A case report linking pathology to conservative care. J. Bodyw. Mov. Ther. 2021, 27, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Jardí, J. , Rodas G., Pedret C., et al. Osteitis pubis: can early return to elite competition be contemplated? Transl Med UniSa. 2014;10:52-58.
- Kekelekis, A.; Clemente, F.M.; Kellis, E. Muscle injury characteristics and incidence rates in men’s amateur soccer: A one season prospective study. Res. Sports Med. 2022, 32, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Kekelekis, A.; Musa, R.M.; Nikolaidis, P.T.; Clemente, F.M.; Kellis, E. Hip Muscle Strength Ratios Predicting Groin Injury in Male Soccer Players Using Machine Learning and Multivariate Analysis—A Prospective Cohort Study. Muscles 2024, 3, 297–309. [Google Scholar] [CrossRef]
- King, E.; Franklyn-Miller, A.; Richter, C.; O’reilly, E.; Doolan, M.; Moran, K.; Strike, S.; Falvey, É. Clinical and biomechanical outcomes of rehabilitation targeting intersegmental control in athletic groin pain: prospective cohort of 205 patients. Br. J. Sports Med. 2018, 52, 1054–1062. [Google Scholar] [CrossRef]
- Lai, W.C.; Wang, D.; Chen, J.B.; Vail, J.; Rugg, C.M.; Hame, S.L. Lower Quarter Y-Balance Test Scores and Lower Extremity Injury in NCAA Division I Athletes. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O'Brien, K.K. Scoping studies: advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Lisman, P.; Nadelen, M.; Hildebrand, E.; Leppert, K.; de la Motte, S. Functional movement screen and Y-Balance test scores across levels of American football players. Biol. Sport 2018, 35, 253–260. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gomez, J.A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 711–718. [Google Scholar] [CrossRef]
- McAleer, S.S.; Lippie, E.; Norman, D.; Riepenhof, H. Nonoperative Management, Rehabilitation, and Functional and Clinical Progression of Osteitis Pubis/Pubic Bone Stress in Professional Soccer Players: A Case Series. J. Orthop. Sports Phys. Ther. 2017, 47, 683–690. [Google Scholar] [CrossRef]
- Mosler, A.B.; Weir, A.; Eirale, C.; Farooq, A.; Thorborg, K.; Whiteley, R.J.; Hӧlmich, P.; Crossley, K.M. Epidemiology of time loss groin injuries in a men’s professional football league: a 2-year prospective study of 17 clubs and 606 players. Br. J. Sports Med. 2017, 52, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Serner, A.; Mosler, A.B.; Tol, J.L.; Bahr, R.; Weir, A. Mechanisms of acute adductor longus injuries in male football players: a systematic visual video analysis. Br. J. Sports Med. 2018, 53, 158–164. [Google Scholar] [CrossRef]
- Serner, A.; Weir, A.; Tol, J.L.; Thorborg, K.; Yamashiro, E.; Guermazi, A.; Roemer, F.W.; Hölmich, P. Associations Between Initial Clinical Examination and Imaging Findings and Return-to-Sport in Male Athletes With Acute Adductor Injuries: A Prospective Cohort Study. Am. J. Sports Med. 2020, 48, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Pereira, A.; Rodrigues-Gomes, S.; Lopes, T.R. An Unlikely Cause of Groin Pain: Obturator Externus Tear in a Professional Soccer Player. Cureus 2023, 15, e44612. [Google Scholar] [CrossRef]
- Vergani, L.; Cuniberti, M.; Zanovello, M.; Maffei, D.; Farooq, A.; Eirale, C. Return to Play in Long-Standing Adductor-Related Groin Pain: A Delphi Study Among Experts. Sports Med. - Open 2022, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Weir A, Brukner P, Delahunt E, et al. Doha agreement meeting on terminology and de fi nitions in groin pain in athletes. Published online 2015:768-774.
- Wollin, M.; Lovell, G. Osteitis pubis in four young football players: A case series demonstrating successful rehabilitation. Phys. Ther. Sport 2006, 7, 153–160. [Google Scholar] [CrossRef]
Figure 1.
Scoping review PRISMA flowchart.
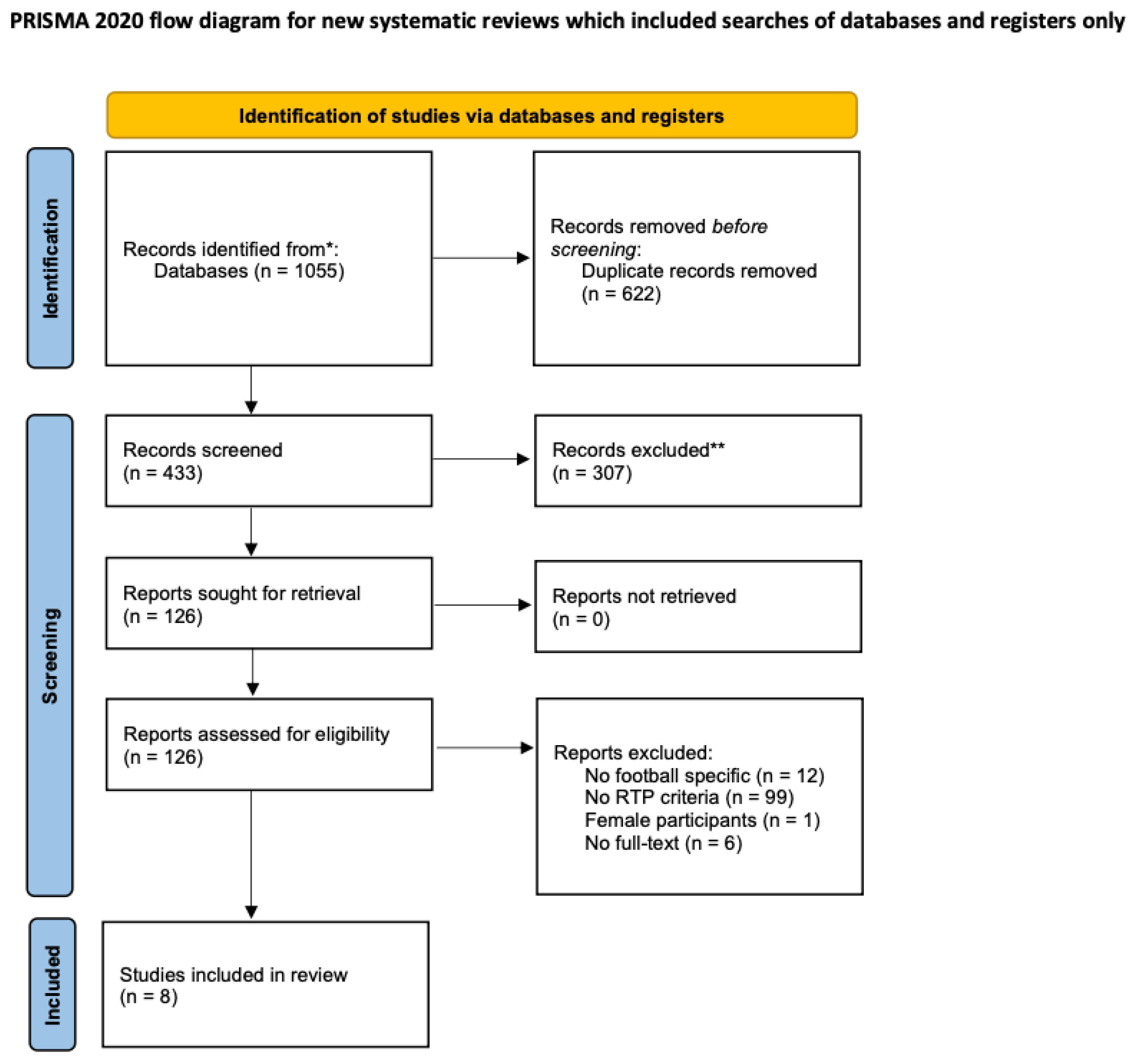

Table 1.
Scoping review framework as described by Askley and O'Malley4, and modified by Levac et al.21
Table 1.
Scoping review framework as described by Askley and O'Malley4, and modified by Levac et al.21
| 1 | identifying the research question | Investigating the criteria determined the RTP decisions after hip and groin injury in male and female soccer players. |
| 2 | Identifying of relevant studies | Search in electrinic databases PubMed, Scopus and SPORTDiscu and their reference lists for research studies published after 2003 in english language |
| 3 | Study selection | PubMed, Scopus and SPORTDiscus search for RTP criteria applied to soccer players after a hip and groin injury as defined by Weir et al. The search yielded 8 studies for inclusion |
| 4 | Charting the data | Evaluating relevant studies to determine criteria for RTP decisions following a hip and groin injury. |
| 5 | Collating, summarizing and reporting results | Clinical, functional and soccer specific on-filed criteria determine RTP decisions in male soccer. |
Table 2.
Categorization of Return to play Criteria. GPS = Global positioning system, HAGOS = Hip And Groin Outcome Score, MRI = Magnetic resonance imaging, ROM = Range of Movement, RTP = Return to Play, US = Ultrasound, VAS = Visual Analogue Scale, Yo-Yo IRT = Intermittent Recovery Test.
Table 2.
Categorization of Return to play Criteria. GPS = Global positioning system, HAGOS = Hip And Groin Outcome Score, MRI = Magnetic resonance imaging, ROM = Range of Movement, RTP = Return to Play, US = Ultrasound, VAS = Visual Analogue Scale, Yo-Yo IRT = Intermittent Recovery Test.
| clinical | functional | sport-specific on-fied | ||||
|---|---|---|---|---|---|---|
| Outcomes | Reference | Outcomes | Reference | Outcomes | Reference | |
| 1 | Pain-free full hip ROM | Abateet al. | < 10% Adductor isometric strength Asymmetry | Abateet al. | Pain-free football-specific activities | Abateet al. |
| 2 | US | Isometric adductors strength | Chiesaet al. | Maximal Ball strike velocity | Chiesaet al. | |
| 3 | MRI | FMS score | Eberbachet al. | Pro-Agility test | ||
| 4 | HAGOS scores | Asymptomatic exercise performance | Harmath & Lejkowski | Yo-Yo IRT | ||
| 5 | pain free Copenhagen exercises | Chiesaet al. | Pain free strengthening exercises | jardiet al. | Full squad training sessions for two weeks at 3 and 4 stages | jardi |
| 6 | Time to RTP | Eberbachet al. | Lumbo-pelvic stability at Level 4 | Pre-injury times and intensities (aerobic tests ) | ||
| 7 | Asymptomatic orthopaedic testing | Harmath & Lejkowski | Concentric-eccentric work of Rectus Abdominis and Obliques (2 sets of 7 repetitions 3/week) | Symptoms free full game | ||
| 8 | Pain free Palpation | Maximum adductor Squeeze scores at 0 | McAleeret al. | Successful completion of a running program | Wollin & Lovell | |
| 9 | Negative osteopathic assessment | jardiet al. | Maximum adductor squees scores at 45 | 20m shuttle run test | ||
| 10 | Negative squeeze test for at least a month | Maximum adductor squeeze scores at 90 | 5m sprint test | |||
| 11 | Pain free Pubic palpation | Adductor strength exercises | Wollin & Lovell | 20m sprint test | ||
| 12 | Negative squeeze test for at least a month | Pre-injury slide board skating scores | Pain free technical skills | Silvaet al. | ||
| 13 | Pain VAS with adductor squeeze at 45 | McAleeret al. | Pain free Change of Direction | |||
| 14 | Pain VAS with straight-leg-sit-up | Pain free maximum speed | ||||
| 15 | Negative Pubis Symphysis stress test | 95-100 pre-injury GPS values | ||||
| 16 | Pain free squeeze test at 0 | Wollin & Lovell | 3 compete training sessions with no limitations | |||
| 17 | Pain free squeeze test at 60 | |||||
| 18 | Pain free pubic palpation | |||||
Table 3.
Summary of RPT criteria in studies on Hip and Groin injuries in soccer players.Clinical RTP criteria.
Table 3.
Summary of RPT criteria in studies on Hip and Groin injuries in soccer players.Clinical RTP criteria.
| Author (year) | Type of groin pain injury | Study | level of | Aims of the study | Methodology | follow up period | Outcome Measures | Important Results | time to RTP |
|---|---|---|---|---|---|---|---|---|---|
| location | Population | Evidence | |||||||
| Abate et al. | Adductor related groin injury | 1 | Level 4 | (a) to describe a rare medical case, | case report study | NA | Pain-free full hip ROM | (a) MRI and US may assist in rehabilitation and RTP decisions | 146 days |
| 2023 | (adductor longus avulsion) | semi professional | (b) to evaluate the contribution of imaging and strength measurements to monitor healing process | Pain-free football-specific activities | (b) A HHD could be utilized for strength assessment | ||||
| Italy | < 10% Adductor isometric strength Asymmetry | (c) Resume full activity before RTP | |||||||
| US | |||||||||
| MRI | |||||||||
| HAGOS scores | |||||||||
| Chiesa et al. | Pubic and Adductor related groin pain | 1 | Level 4 | (a) to describe the rehabilitation program | case report study | NA | Isometric adductors strength | (a) a unique measurement was applied. The velocity of a maximal effort ball strike | not clearly stated |
| 2023 | collegiate player | (b) to describe the objective and functional assessments applied for RTP | pain free Copenhagen exercises | (d) a multifactorial rehabilitation and RTP strategy were suggested | |||||
| USA | Maximal Ball strike velocity | (c) RTP functional assessment lacking categorization, clinical feasibility, fitness and soccer-specific skill requirements | |||||||
| Pro-Agility test | |||||||||
| Yo-Yo IRT | |||||||||
| Eberbach et al. | Pubic related Groin pain | 14 | Level 4 | (a) to evaluate the effect of age/position and FMS score | Prospective Clinical Trial | 24 months | (a) Time to RTP | (a) Training load monitoring prevents from overuse injuries | 135.3±83.9 days |
| 2021 | elite academy players | (b) to implement a standardized nonsurgical therapeutic protocol and prospectively evaluate the outcome | (DRKS00016510) | (b) FMS score | (b) Limited recurrent symptoms were reported | ||||
| Germany | (c) A criteria-based rehabilitation program was followed | ||||||||
| (d) Age provided no effect on RTP timing | |||||||||
| Harmath & Lejkowski | Pubic and Adductor related groin pain | 1 | Level 4 | (a) to describe the successful management utilizing a comprehensive conservative evidence-based approach | case report study | 6 months | (a) Asymptomatic orthopaedic testing | (a) incorporate plyometric exercises, CoD and sprinting in the final stages of RTP | 70 days |
| 2021 | amateur player | (b) Pain free Palpation | (b) SWT or MT paired with sport specific rehabilitation program have shown to shorten RTP time | ||||||
| Canada | (c) Asymptomatic exercise performance | (c) emphasis should be placed on exercise technique and movement quality during the RTP process | |||||||
| Jardi et al. | Pubic related groin pain | 2 | Level 4 | (a) to report the duration of each rehabilitation stage | Retrospective case studies | 24 months | (a) Negative squeeze test for at least a month | (a) Clinical assessment and level of lumbo-pelvic stability (Wibsey-Roth Core Stability grading system) were incorporate in RTP decisions | 96.5 (72-121) days |
| 2014 | elite players | (b) Pain free Pubic palpation | (b) An individualized rehabilitation approach was preferred | ||||||
| Spain | (c) Adductors pain free reports during all contractions (isometric, concentric and eccentric) | (c) RTP decisions were significantly impacted by the level of Lumbo-pelvic stability. | |||||||
| (d) Negative osteopathic assessment | |||||||||
| (e) Pain free strengthening exercises | |||||||||
| (f) Lumbo-pelvic stability at Level 4 | |||||||||
| (g) Concentric-eccentric work of Rectus Abdominis and Obliques (2 sets of 7 repetitions 3/week) | |||||||||
| (h) Pre-injury times and intensities (aerobic tests ) | |||||||||
| (i) Full squad training sessions for two weeks at 3 and 4 stages | |||||||||
| (j) Symptoms free full game | |||||||||
| McAleer et al. | Pubic related groin pain | 5 | Level 4 | (a) to describe the objective and functional markers that to guide progressively the rehabilitation management | A case report series | 29,6 (16-33) months | (a) Pain VAS with adductor squeeze at 45 | (a) Criteria based early, middle and late pitch-based rehabilitation phases were introduced. | 49.4 (38 - 72) days |
| UK | professional and academy | (b) Pain VAS with straight-leg-sit-up | |||||||
| 2017 | soccer players | (c) Maximum adductor Squeeze scores at 0 | |||||||
| (d) Maximum adductor squees scores at 45 | |||||||||
| (e) Maximum adductor squeeze scores at 90 | |||||||||
| (f) Negative Pubis Symphysis stress test | |||||||||
| Wollin & Lovell | Pubic related groin pain | 4 | Level 4 | (a) to describe the successful nonsurgical management in 4 soccer players diagnosed with Osteitis pubis | a retrospective study | NA | (a) Pain free squeeze test at 0 | (a) clinical outcomes: Pain free adduction, No pubic symphysis tenderness by palpation over the bone and adductor complex | 92.7 (70 -112) days |
| Australia | elite youth soccer players | (b) Pain free squeeze test at 60 | (b) functional outcomes: pain free individualized running program | ||||||
| 2006 | (c) Pain free pubic palpation | (c) Performance markers: 20m sprint running to evaluate RTP readiness | |||||||
| (d) Adductor strength exercises | |||||||||
| (e) Pre-injury slide board skating scores | |||||||||
| (f) Successful completion of a running program | |||||||||
| (g) 20m shuttle run test | |||||||||
| (e) 5m sprint test | |||||||||
| (f) 20m sprint test | |||||||||
| Silva et al. | Hip related groin pain | 1 | Level 4 | (a) to describe a rare clinical case from the moment of injury to RTP | a case report study | NA | (a) Pain free technical skills | (a) The MRI accurately determined the injured tissues and the extent of damage. | 23 days |
| Portugal | (b) Pain free Change of Direction | ||||||||
| 2023 | (c) Pain free maximum speed | ||||||||
| (d) 95-100 pre-injury GPS values | |||||||||
| (e) 3 compete training sessions with no limitations | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



