Submitted:
16 May 2025
Posted:
19 May 2025
You are already at the latest version
Abstract
Background/Objectives: It is essential that education in palliative care is accessible at all levels and adapted to various contexts. In Brazil, Palliative Care is starting to progress, but awareness in the public is still lacking. The Last Aid approach provides accessible ways for the general public to engage in discussions about serious illness, death, dying, and grief, while also suggesting practical actions to support. The present study aimed to investigate if Last Aid Courses (LAC) contribute to bringing knowledge and awareness of Palliative Care to different settings in Brazil. Methods: Participants of the LAC responded to a qualitative-quantitative questionnaire provided after the course, between March and November 2024. Results: 32 courses were offered, with 343 participants. The majority of the LAC participants came from the at the general public (53,2%), followed by health students (28.1%). 98.8% of all informants indicated they had acquired new knowledge. The qualitative analysis provided significant insights from participants, focusing on normalizing conversations about death and the emphasis on dignity during the dying process. Conclusions: The course implementation in Brazil showed positive results, indicating its potential to raise awareness about the topic, regardless of the context.
Keywords:
palliative care
; compassionate communities
; Last Aid Course
; public palliative care education
; Brazil
; end of life care
1. Introduction
Palliative care is a specialized form of medical care designed to provide relief from the symptoms, pain, and emotional distress associated with serious illnesses. It focuses on improving the quality of life for patients and their families and is applicable from the moment of diagnosis through the progression of the illness and up until the end of life. [1,2,3,4]. Although significant efforts are directed toward curative treatments in several countries, efforts focused on palliative care and end-of-life care remain limited. Furthermore, important disparities exist in the quality of palliative care services across different countries [1] leaving many seriously ill and dying people in need without adequate palliative and compassionate care around the end-of-life.
The results of the latest ranking published by The Economist on the quality of death in various countries showed the U.K., Australia, New Zealand, Ireland, Belgium, Taiwan, Germany, the Netherlands, the U.S. and France among the Top Ten. Brazil ranked 42nd among the 80 countries analyzed. To prepare this ranking, 20 quantitative and qualitative indicators were analyzed and categorized into five categories: the palliative and health environment, human resources, accessibility to care, care quality, and the level of community engagement. Furthermore, Brazil ranked third to last in terms of quality of death among 81 countries studied, ahead only of Lebanon and Paraguay, according to the international report published in the Journal of Pain and Symptom Management [1,5]
One possible explanation for this result is linked to a widespread culture of denying the reality of death and dying [2]. Thus, it is crucial to foster cultural changes that acknowledge the significance of palliative care, recognize death as a natural aspect of life, and emphasize the quality of life for patients throughout their entire life journey including serious illness and end of life, for both patients and their families [5].
In Brazil, palliative care has been progressing steadily, marked by the significant achievement of the National Palliative Care Policy published in 2024 [6]. This policy aims to enhance autonomy and quality of life for patients, focusing on symptom control to relieve suffering, the development of advanced care plans, and end of life care in the community. One major point of the policy is to promote awareness and education about palliative care throughout society [6]. Unfortunately, at present palliative care is widely unknown to the general public as well as to health professionals in Brazil [7].
Education is fundamental in palliative care. It is therefore essential that this education should be accessible at all levels and tailored to various contexts including public palliative care education (PPCE) [8,9]. This is particularly important in a country like Brazil, where some regions still face challenges in accessing essential services that contribute to quality of life, including healthcare, food, housing, income, education, and leisure [8,9,10] and adapts to different realities [4].
Among the strategies implemented, the Last Aid Course (LAC) is particularly noteworthy. The concept of Last Aid is founded on the idea that knowledge of palliative care should be included in public education as part of a so-called public knowledge approach [11,12]. The aim is to cultivate compassionate communities and to transform end-of-life care into a collective responsibility [11,12]. The Last Aid approach provides accessible ways for the general public to engage in discussions about serious illness, dying, death and grief, and it also suggests practical Last Aid measures to offer support in various contexts [12].
The concept was first described by Georg Bollig in 2008, and courses started in 2015 in Germany, Norway, and Denmark. Through a standardized curriculum and a slide set, the courses are held in 23 countries, including Germany, Australia, Scotland, Slovenia, Brazil, and Singapore [12,13,14,15].
In 2020, LAC were started in Brazil, utilizing an international curriculum and slide set. Since then, Last Aid Brazil has offered both face-to-face and online courses in various locations, including cultural centers, healthcare centers, nursing homes, universities, and compassionate communities [16]. The course duration usually is 4 hours (=240 min), including brakes.
Research findings indicate that the LAC is not only feasible and well-received, but also has significant potential to enhance palliative care education for the general public across various countries [11,13,17], including children and adolescents [18]. Brazil is the first country in South America that has started to implement LACs. So far a scientific evaluation of LAC in Brazil and South America is needed to evaluate the feasibility and acceptance in this part of the world with huge geographical distances and different ethnicities. Considering this, it is crucial to conduct a study on LAC in Brazil to better understand its potential, challenges, and the experiences involved in its implementation across the country. This phase is particularly important, as emphasized by Bollig and Bauer as research indicates that outcomes may vary depending on the location where LACs are implemented [19]. Furthermore, the LAC addresses a new demand arising from the National Palliative Care Policy in Brazil [6].
In addition to this, Brazil faces unique challenges, such as regional disparities in access to healthcare services. There is a need for better training of healthcare professionals, raising public awareness about palliative care, recognizing it as an integral part of patient care, and improving access to medications for pain relief and symptom management [20].
This study is also aligned with the needs outlined in the Global Atlas of Palliative Care, which highlighted the importance of strategies to promote education in palliative care and research on the topic, especially in low- and middle-income countries [21].
The aim of the present study was to investigate if LACs can contribute to bringing knowledge and awareness of Palliative Care to different settings in Brazil.
2. Materials and Methods
2.1. Study Design
The research design is a cross-sectional study, collecting data of the participants at a specific moment. It is based on a mixed-methods approach with a combination of quantitative and qualitative data from a questionnaire. It employed a descriptive analysis design to investigate the frequency of the quantitative data collected, and a qualitative research design to explore the perceptions and experiences of the participants. The analysis and presentation of the qualitative data was based on qualitative description [22,23].
2.2. Participants, Data Collection and Analysis
Between March and October 2024, all LAC participants were invited to participate in the study. All were given a brief explanation of the importance of evaluating the course to improve its efficiency, quality, and outcome. They were informed that participation in the study was voluntary. After providing informed consent to participate in the study the informants were asked to return a questionnaire with an included informed consent statement.
The informants were asked to return the questionnaire right away or in the next couple of days. The present study is a part of an ongoing larger research project that aims to analyze the understanding and impact of the LAC on the perception of finitude, care, mourning, death literacy, and breaking of taboos among the participants in Brazil.
The inclusion and exclusions criteria were as follows:
- o Inclusion criteria: all questionnaires from LAC participants from 18 years of age, who provided informed consent and completed all the answers of the questionnaires properly
- o Exclusion criteria: participants under 18 years of age were excluded
The data collection was conducted virtually through a webbasedquestionnaire created on the Google Forms platform, featuring both open and closed-ended questions. Data analysis regarding participant characteristics was performed using absolute and relative frequencies. The open-ended questions were grouped into thematic categories and counted after their inductive evaluation.
In order too protect the informants privacy, no personal data other than age, sex, and profession were collected.Participants could choose whether or not to provide this information.
The qualitative data presented are based on the answers provided by the participants in the questionnaires, which were translated into English. These transcriptions faithfully reflect the original responses given during the course, without any alteration of content, and were used for qualitative data analysis. The data were subsequently subjected to analysis based on qualitative content analysis [24] and qualitative description. [22,23]
The analysis was performed using the following steps:
- Pre-analysis, with floating reading and the establishment of information about the topic, through exhaustiveness, representativeness, homogeneity, and relevance to the research objectives
- exhaustive exploration of the material for coding, creation of context units, and categorization
- interpretation of the data and necessary inferences.
The study was conducted after approval from the ethics and research committee. Furthermore, all the ethical requirements necessary for conducting the research were properly respected. All informants provided informed consent before participating in the study. The study was conducted following the Declaration of Helsinki, and approved by the Ethics Committee of Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil (number 7.228.452 of 16.11.2024)
3. Results
3.1. Quantitative Data
In the study period from March to Okt 2024 32 LACs were offered in different settings in São Paulo, Rio de Janeiro and Online and 343 people attended.
Participants were divided according to the setting where they attended the course. People living in a favela, with courses offered in 3 favelas in Rio de Janeiro and São Paulo; University students from courses offered to medical, nursing and ergotherapy students; Community Health Worker (CHW) who attended courses offered at their Primary Care Unit (PCU) and the General Public who attended face-to-face courses offered at public places or online. Table 1 shows the characteristics of each setting.
A total of 246 participants completed the questionnaire, resulting in a response rate of 72%.
The participants´ age ranged from 19 to 82 years with an average of 39,6 years. The self-declared gender characteristics of these participants are outlined in Table 1.
| Women | Men | No Information provided | Participants | |
| Favela | 12 (92,3%) | 1 (7,7%) | 0 (0.0%) | 13 |
| University | 69 (19,8%) | 17 (19,8%) | 0 (0.0%) | 86 |
| PCU | 41 (100,0%) | 0 (0.0%) | 0 (0.0%) | 41 |
| Public Place | 66 (77,6%) | 17 (20,0%) | 2 (2,4%) | 85 |
| Online | 16 (80%) | 4 (20,0%) | 0 (0.0%) | 20 |
| Total | 204 (83,3%) | 39 (15,9%) | 2 (0,8%) | 245 |
| PCU: Primary Care Unit. | ||||
Table 2 shows the participant´s evaluation of the questions about learning new things during the course and a statement if they would recommend the course to others or not.
Table 3 presents the paticipants evaluation of the LAC´s content on a five point scale ranking between very poor and very good.
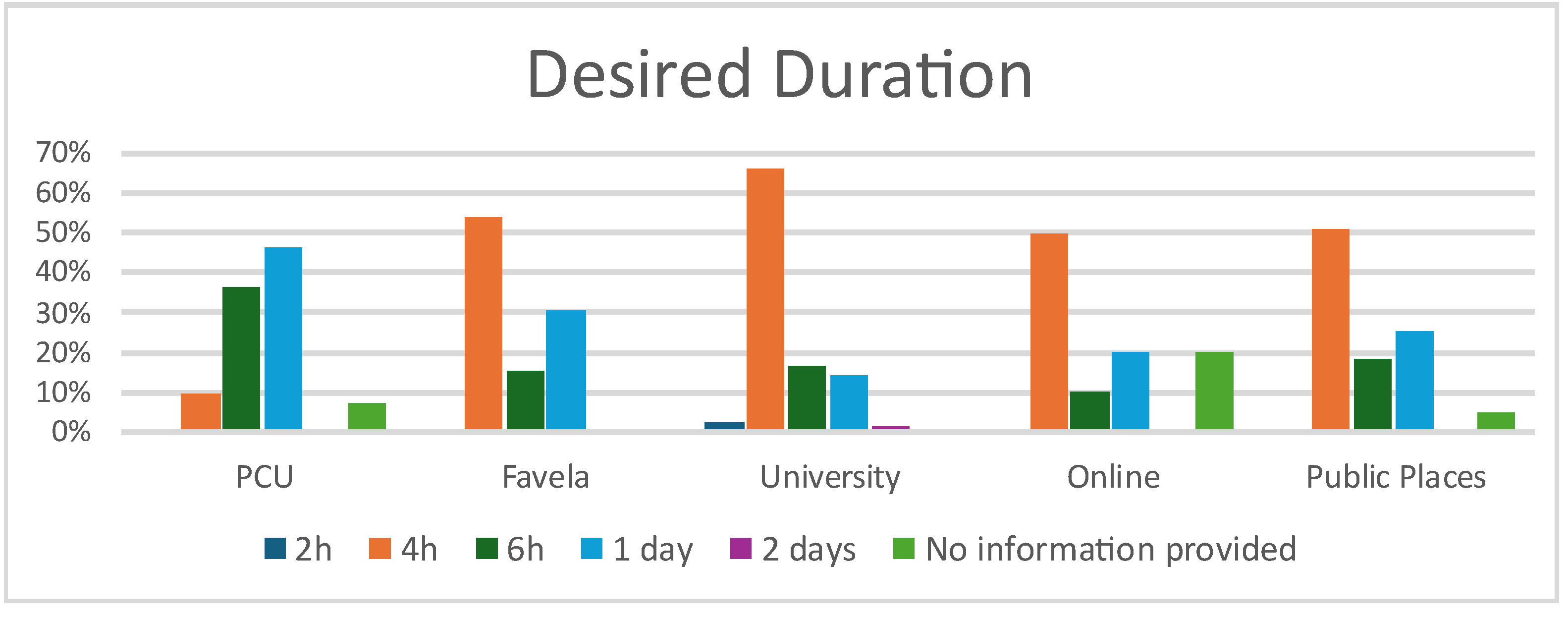
When asked about their preference for the duration of the LAC, participants suggestions for desiredlength of the LAC varied between 2h up to 2 days. Table 2 shows the answers according to the different settings.
Figure 1.
Participants’ suggestions for the desired duration of the Last Aid Course. CHW: Community Health Worker.
Figure 1.
Participants’ suggestions for the desired duration of the Last Aid Course. CHW: Community Health Worker.
3.2. Qualitative Data
Participants were asked about the most important message for them from the course. The responses were analyzed by qualitative content analysis and qualitative description. This process led to four main themes that are shown in figure 2 and which are described in more detail below:
Figure 2.
Themes from the qualitative data.
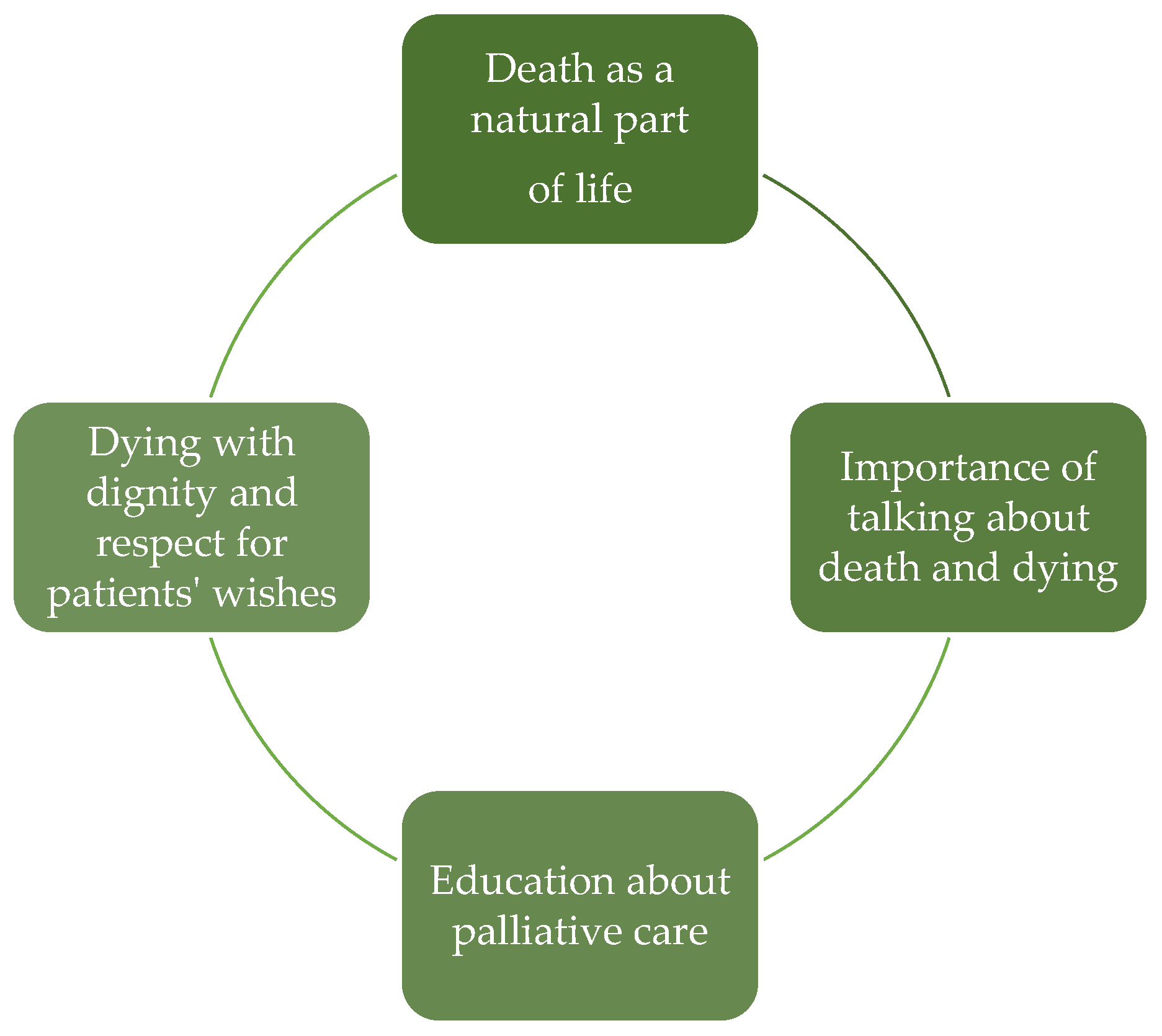
Theme 1: Death as a natural part of life
This theme reflects the widespread acknowledgment that death, is an inevitable part of life that requires preparation. Although this fact is known for everyone it is still a taboo to talk about it.
"Death is part of life, and there needs to be quality and humanity at this time as well." (General Public)
It emphasizes the importance of facing death with understanding and quality care, regardless of whether one feels ready for it. It is important to be prepare to say farewell.
"The only certainty in life is death, we need to be prepared for this moment of farewell." (Favela)
For many people it is paramount to be respected and to be able to die with dignity.
"The importance of dying with dignity." (Health Students)
Theme 2: Importance of talking about death and dying
The responses of the informants reinforce the broad consensus across all groups that talking about death is not harmful but rather helps to reduce fear, fostering a more supportive environment for everyone involved.
"Talking about death does not hasten death, that is, it does not attract death." (CHW)
"Talking about the process of dying is necessary and can be lighthearted." (Health Students)
Open communication about death, dying and grief allows individuals to express their thoughts, wishes, and fears, fostering an environment of respect.
"The importance of talking about death with our family, since death is inevitable. Maintaining a dialogue with loved ones is the best way to find out what they want, and also to make my wishes clear." (Favela)
Theme 3: Dying with dignity and respect for patients' wishes
It is important to talk about death and dying to support dying people in the best way possible and to respect their autonomy and their wishes for end of life care as far as possible. The responses of the informants underline the importance of respecting the wishes of individuals at the end of life, ensuring a dignified death by honoring the patient's decisions and preferences.
"Respect people's wishes." (CHW)
To know and understand the wishes of a person can also make decision-making and the whole dying process easier and might contribute to reduce conflichts.
"With understanding, I can make this process easier." (General Public)
One main theme that was emphasized as a key takeaway was need for compassion and empathy during the dying process.
"Respect the patient's decision because just a touch as a gesture of affection makes all the difference at this time." (Health Students)
Theme 4: Education about palliative care
As death literacy is low in the public and most people have a lack of knowledge about serios illness, dying, death and grief education about palliative care is urgently needed. Participants across various groups expressed the need for greater education on palliative care.
"The importance of breaking the taboo around death." (Health Students)
"We need to talk about Palliative Care." (General Public)
Many informants recognized the importance of discussing and understanding palliative care, which plays a crucial role in supporting both patients and their families during the end-of-life process.
“I learned about some ways to comfort, how to act and I learned about each religion and the importance of respecting the moment.” (General Public)
In summary the results from the qualitative data show that talking about death and dying should become more normal in the public and that talking about these themes is helpful. Communication about ones own wishes for decision-making is important to respect autonomy and patient wishes for end of life care. Thus the majority of participants highlight that education about death, dying, grief and palliative care is important and should be improved in the public space.
4. Discussion
The main results from the quantitative analysis of 32 courses that were held in various environments, attracting a total of 343 participants, were as follows:
Evaluations of the courses showed a high satisfaction rate, with 98.4% of participants expressing that they would recommend the course to others, and 98.8% indicating they had acquired new knowledge. Additionally, most attendees rated the course content as "very good" across all settings. This shows that the LAC is feasible and highly accepted by people in Brazil.,
Among all settings, the results from the analysis of the qualitative data highlight the importance of normalizing the conversations about death, raising awareness of palliative care and maintaining dignity during the dying process.
The implementation of the LAC in Brazil showed positive results, indicating its potential to raise awareness about the topic, regardless of the context. The high satisfaction rates and the recognition of the course's value among different participant groups, both in terms of local context and education, suggest that such initiatives can help break taboos surrounding death and improve the quality of end-of-life care. The findings of this study align with those from research conducted in other countries [11,13,18,25]. In a study conducted with 5,469 participants of LACs in Germany, Switzerland, and Austria, it was found that 99% found the course content easy to understand, and 99% would recommend the course to others. The overall course rating was 'very good’ [25]. These findings are similar to our resukts from Brazil.
The online course assessed in this study also received favorable feedback from participants, reinforcing the findings of the previously mentioned study in Germany and Scotland [17,27]. This format allows participation from individuals who are unable to attend in person, including caregivers of severely ill patients, as well as those living in locations with limited accessibility to the course [17].
The LAC was delivered to 42 CHWs, who are key in mediating between the population and the healthcare system. In addition to disseminating essential health information, they facilitate the referral of community needs to the Family Health Strategy. This approach is designed to address territorial, cultural, and social diversity, aligning with the principles of the Brazilian Unified Health System (SUS) [27].
Participants, in general, consider the four-hour duration to be sufficient. However, the CHWs showed greater interest in attending a longer course, indicating the need for more education and training for this profession. This finding is similar to findings from Germany that people from healthcare profeessions would prefer a slightly longer course lasting one day [28,29].
The quantitative and qualitative results indicate that the current LAC curriculum seems to meet the growing demand for educational strategies in end-of-life care, as outlined in the National Palliative Care Policy. (6) Furthermore, it helps to fill an important gap in strengthening knowledge and practices in this type of care, ensuring a more integrated approach to the needs and demands of end-of-life care [30].
The LAC was initiated in Brazil in 2020. In addition to community training, efforts were also made to offer courses aimed at training facilitators for the LAC. This initiative contributes to the dissemination of knowledge on this topic, not only for the training of future facilitators but also for the development of individuals across different states in Brazil [16].
As in other countries, the dissemination of LAC courses in Brazil has primarily occurred through word of mouth [13,16]. However, to expand its reach and impact, the course should be institutionally integrated into various settings.
Another promising initiative was the implementation of the LAC in favelas through partnerships with compassionate community projects [31]. The proposal contributes to enhancing the community's ability to support its members by mobilizing volunteers and expanding the health support network, integrated with primary care services, aiming to reduce disparities in access to palliative care [10,32]. Currently, established compassionate communities exist in Rio de Janeiro [10,32], Goiânia, São Paulo, and Belo Horizonte, with additional initiatives under development [10,32,33]. Thus the LAC can bee seen as the educational basis for public palliative care education of people in compassionate communities [11].
The demand for palliative care at home will increase in the coming years [11,21]. Additionally, it is important to highlight that there are unique realities in Brazil. Some areas are dominated by drug trafficking or militias and lack basic sanitation. There are regions where access to healthcare facilities is hindered, especially for individuals with mobility challenges and those who are seriously ill [34,10]. The disparities in the country are vast in access to healthcare services [35]. The disparities in access to healthcare services across the country are vast, and the growing need for home-based care further emphasizes the urgent need for initiatives and strategies focused on community education, such as the LAC.
In Brazil, in addition to insufficient care at the end of life, as shown in the international rankings [1,5], we face a challenge in the training process of healthcare professionals. Education on Palliative Care only became mandatory in the medical curriculum in 2023 [36]. Data collected in 2021 showed that only 44 out of 315 (14%) medical schools registered with the Ministry of Education and Culture offered any type of education on Palliative Care [37,38]. In other areas of healthcare professional education, this topic is not mandatory. Thus the LAC can contribute to educate the public about palliative care and to strengthen compassionate communities in their daily work. As first experiences with an extended Last Aid Course for healthcare professionals from Germany [29] are a future option could be to implement these courses in Brazil too.
5. Limitations
One of the main limitations of the course is the relatively small amount of data collected from certain settings. For example, in the favela and for the CHWs, only 4 and 2 courses were held, respectively. Additionally, all of the settings analyzed were located in the Southeast region of Brazil, which represents just one of the country's five major regions.
It is also worth noting that not all participants completed the questionnaire (72%), and other opinions could be lacking. On the other hand a response rate of 72% msay provide a valid representation of the group of informants for the current study.
6. Conclusions
The results of the current study indicate that using the standardized international LAC curriculum to discuss Palliative Care and end-of-life care can be effective in different settings and for participants with diverse backgrounds. This suggests that the LAC can serve as a simple and accessible tool to raise awareness of Palliative Care in different populations as shown for Brazil and many European countries.
The feedback from CHWs suggests that these professionals want more information about Palliative Care; benefit from a LAC and this may be an accessible tool to strengthen the National Palliative Care Policy, especially in Primary Health Care. In the future the implementation of the Last Aid Course professional might be a option for this special group.
As an innovative study, the findings show that the LAC model can be expanded and continued, offering significant potential for further implementation and impact in different regions and contexts of Brazil.
Author Contributions
“Conceptualization, Patricia Cury and Karin Schmid; methodology and data analysis, Patricia Cury, Karin Schmid, Marina Schmidt, Georg Bollig Janaina Nascimento; investigation, Karin Schmid; writing—original draft preparation, Karin Schmid.; writing—review and editing, Patricia Cury, Marina Schmidt, Georg Bollig and Janaina Nascimento; All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of UERJ (Parecer 7.228.452 of 16.11.2024)
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. Participation was voluntary, and the informants had the opportunity to end participation at any time without consequences for them.
Data Availability Statement
The data presented in this study are available in part on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Acknowledgments
We thank all participants of the Last Aid courses and workshops, all Last Aid instructors, all our network partners, supporters, and others who have contributed to or supported the project.
Conflicts of Interest
K.S. is the leader of Last Aid in Brazil. G.B. is the leader of Last Aid International and holds a trademark for Last Aid. The other authors have no conflicts of interest to declare.
References
- Finkelstein, E.A.; Bhadelia, A.; Goh, C.; Baid, D.; Singh, R.; Bhatnagar, S.; Connor, S.R. Cross Country Comparison of Expert Assessments of the Quality of Death and Dying 2021. Journal of Pain and Symptom Management 2022, 63, e419–e429. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.F.; da Silva, J.F.M.; Cabrera, M. Palliative care: pathway in primary health care in Brazil. Cad Saude Publica 2022, e00130222. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, J.M.G.; Johnson, F.R.; Finkelstein, E.A. What is a Good Death? A Choice Experiment on Care Indicators for Patients at End of Life. Journal of Pain and Symptom Management 2022, 457–467. [Google Scholar] [CrossRef]
- Borgstrom, E. What is a good death? A critical discourse policy analysis. BMJ Support Palliat Care. 2024, e2546–e2553. [Google Scholar] [CrossRef]
- The Economist Intelligence Unit, The 2015 Quality of Death Index Ranking palliative care across the world. London. 2015.
- Available online:. Available online: https://www.in.gov.br/web/dou/-/portaria-gm/ms-n-3.681-de-7-de-maio-de-2024-561223717 (accessed on 14 May 2025).
- Ghisleni, R.C.; Valandro, C.G.; Saavedra, L.P. Avaliação do conhecimento em cuidados paliativos entre médicos de família e comunidade. Rev Bras Med Fam Comunidade 2023, 45, 3871. [Google Scholar] [CrossRef]
- Torres, L.F.; de Oliveira, N.M.S. Programa educacional em cuidados paliativos para os profissionais de saúde: uma revisão sistemática. Research Society and Development 2022, e18011628885. [Google Scholar] [CrossRef]
- Zamarchi, G.; Leitão, B. Estratégias educativas em cuidados paliativos para profissionais da saúde. Revista Bioética 2023, 11. [CrossRef]
- Mesquita, M.G.D.R.; Silva, A.E.; Pereira, L.C.; Martins, M.R.; de Souza, T.; Trotte, L.A.C. Slum compassionate community: expanding access to palliative care in Brazil. Revista de Escola de Enfermagem da USP 2023, e20220432. [Google Scholar] [CrossRef]
- Bollig, G.; Brandt, F.; Ciurlionis, M.; Knopf, B. Last Aid Course. An Education For All Citizens and an Ingredient of Compassionate Communities. Healthcare (Basel) 2019, 7, 19. [Google Scholar] [CrossRef]
- Mills, J.; Rosenberg, J.P.; Bollig, G.; Haberecht, J. Last Aid and Public Health Palliative Care: Towards the development of personal skills and strengthened community action. Progress in Palliative Care 2020, 28, 343–345. [Google Scholar] [CrossRef]
- Bollig, G.; Neylon, S.; Niedermann, E.; Zelko, E. The Last Aid Course as Measure for Public Palliative Care Education: Lessons Learned from the Implementation Process in Four Different Countries. Palliative Care - Current Practice and Future Perspectives IntechOpen 2024. [CrossRef]
- Bollig, G.; Heller, A. A Simple and Effective Concept to Teach the Public about Palliative Care and to Enhance the Public Discussion about Death and Dying. Austin Palliative Care 2016, 1, 1010. [Google Scholar]
- Bollig, G. Palliative Care für alte und demente Menschen lernen und lehren, LIT Verlag: Berlin, Germany, 2010, ISBN: 978-364-390-058-6.
- Schmid, K. Implantação dos Cursos de Últimos Socorros no Brasil (CDUS) – Relato de Experiência. Presented at the X Congresso Brasileiro de Cuidados Paliativos, Fortaleza, Brazil, 13-16 Nov 2024.
- Bollig, G.; Meyer, S.; Knopf, B.; Schmidt, M.; Bauer, E.H. First Experiences with Online Last Aid Courses for Public Palliative Care Education during the COVID-19 Pandemic. Healthcare 2021, 9, 172. [Google Scholar] [CrossRef]
- Bollig, G.; Graef, K.; Gruna, H.; Drexler, D.; Pothmann, R. “We Want to Talk about Death, Dying and Grief and to Learn about End-of-Life Care”—Lessons Learned from a Multi-Center Mixed-Methods Study on Last Aid Courses for Kids and Teens. Children 2024, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Bollig, G.; Bauer, E.H. Last Aid Courses as measure for public palliative care education for adults and children—a narrative review. Annals of palliative medicine 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Guirro, U.B.d.P.; Castilho, R.K.; Crispim, D.; de Lucena, N.C. Atlas dos Cuidados Paliativos no Brasil, 1st ed.; ANCP: Brazil, 2022. [Google Scholar]
- Connor, S.; Morris, C.; Jaramillo, E.; Harding, R.; Cleary, J.; Haste, B.; Knaul, F.; de Lima, L.; Krakauer, E.; Bhadelia, A.; et al. Global atlas of palliative care at the end of life, 2nd ed.; Connor, S., Ed.; Alliance WHO&WHPC: London, UK 2020; ISBN 978-0-9928277-2-4. [Google Scholar]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description–the poor cousin of health research?, BMC Med. Res. Methodol 2009, 9, 52. [Google Scholar] [CrossRef]
- Sandelowski, M. What’s in a name? Qualitative description revisited. Res. Nurs. Health 2010, 33, 77–84. [Google Scholar] [CrossRef]
- Bardin, L. Análise do Conteúdo, 1st ed.; Edições 70ª: São Paulo, Brazil, 2016; ISBN 978-85-62938-04-7. [Google Scholar]
- Bollig, G.; Kristensen, F.; Wolff, L. Citizens appreciate talking about death and learning end-of-life care – a mixed-methods study on views and experiences of 5469 Last Aid Course participants. Progress in Palliative Care 2021, 29, 140–148. [Google Scholar] [CrossRef]
- Macaden, L.; Broadfoot, K.; Carolan, C.; Muirhead, K.; Neylon, S.; Keen, J. Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland. Healthcare 2022, 10, 918. [Google Scholar] [CrossRef]
- de Oliveira, F.F.; de Almeida, M.T.P.; Ferreira, M.G.; Pinto, I.C.; Amaral, G.G. Importância do agente comunitário de saúde nas ações da Estratégia Saúde da Família: Revisão integrativa. Revista Baiana de Saúde Pública 2022, 46, 291-313. [CrossRef]
- Mueller, E.; Bollig, G.; Becker, G.; Boehlke, C. Lessons Learned from Introducing Last Aid Courses at a University Hospital in Germany. Healthcare 2021, 9, 906. [Google Scholar] [CrossRef]
- Bollig, G.; Schmidt, M.; Aumann, D.; Knopf, B. Der Letzte Hilfe Kurs professionell – Erste Erfahrungen mit einem eintägigen niedrigschwelligen Palliative Care Fortbildungsangebot für Personal aus dem Gesundheitswesen. Zeitschrift für Palliativmedizin 2023, 24, 31 – 39. [CrossRef]
- Salman, M.S.M.; Cassavia, M.F.d.C.; Salman, C.S.; Salman, A.A.; Bryan, L.; de Oliveira, C. National Palliative Care Policy: Challenges of Professional Qualification in Palliative. Rev. Bras. Cancerol 2024, 70, e–044753. [Google Scholar] [CrossRef]
- Kellehear, A Compassionate communities: end-of-life care as everyone’s responsibility, QJM: An International Journal of Medicine 2013, 106, 1071–1075. [CrossRef]
- Silva, E.; Prates, C.M.; Couto, L.D.S.; Oliveira, L.O. Compassionate Community of the Slums of Rocinha and Vidigal: Strategy to Help in Cancer Control. Rev. Bras. Cancerol 2024, 70, e–104714. [Google Scholar] [CrossRef]
- Collucci, C. Profissionais da saúde e moradores levam cuidados paliativos a doentes em favelas. Available online: https://www1.folha.uol.com.br/equilibrioesaude/2023/08/profissionais-da-saude-e-moradores-levam-cuidados-paliativos-a-doentes-em-favelas.shtml (accessed on 14 May 2025).
- Minayo, M.C.D.S.; Constantino, P.; Mangas, R.M.d.N.; Pereira, T.F.d.S. Experiências de agentes comunitários de saúde com pessoas idosas dependentes e vulneráveis. Revista Pesquisa Qualitativa 2024, 12, 570–590. [Google Scholar] [CrossRef]
- Coube, M.; Nikoloski, Z.; Mrejen, M.; Mossialos, E. Inequalities in unmet need for health care services and medications in Brazil: a decomposition analysis. Lancet Reg Health Am. 2023, 19, 100426. [Google Scholar] [CrossRef] [PubMed]
- Available online:. Available online: http://portal.mec.gov.br/docman/marco-2022-pdf/238001-pces265-22/file (accessed on 14 May 2025).
- Castro, A.; Taquette, S.; Marques, N. Cuidados paliativos: inserção do ensino nas escolas médicas do Brasil. Revista Brasileira de Educação Médica 2021, 45, 1-7. [CrossRef]
- Castro, A.A.; Mendonça, A.V.P.D.M.; Terzi, C.; Martin, E.Z.; de Oliveira, J.R.; Figueiredo, M.D.G.M.C.D.A.; Cury, P.M.; Almeida, P.O.D.A. Compartilhando Experiências: Do Ensino de Cuidados Paliativos na Medicina; ANCP: Brazil, 2023. [Google Scholar]

Table 1.
Settings and Participants of the LACs.
| nº of courses | Participants | |
| Favela | 4 (12.5%) | 32 (9.3%) |
| University | 9 (28.1%) | 105 (30.6%) |
| PCU | 2 (6.25%) | 42 (12.2%) |
| Public Place | 10 (31.25%) | 121 (35.3%) |
| Online | 7 (21.9%) | 43 (12.5%) |
| Total | 32 | 343 |
PCU: Primary Care Unit.
Table 2.
Participants´ evaluation of the importance and relevance of the course.
| Yes | No | No Information Provided | |
| I will recommend the course to others | 242 (98.4%) | 4 (1.6%) | 0 (0.0%) |
| I learned new things | 243 (98.8%) | 2 (0.8%) | 1 (0.4%) |
Table 3.
Participants´ rating of the Last Aid course.
|
Participant Type |
Very Poor (n, %) |
Poor (n, %) |
Neither Poor Nor Good (n, %) |
Good (n, %) |
Very Good (n, %) |
No Information Provided (n, %) |
Total Responses |
| PCU | 1 (2.4%) | 0 | 0 | 1 (2.4%) | 38 (92.7%) | 1 (2.4%) | 41 |
| Favela | 0 | 0 | 0 | 0 | 13 (100%) | 0 | 13 |
| University | 0 | 0 | 0 | 4 (4.7%) | 81 (94.2%) | 1 (1.2%) | 86 |
| Online | 0 | 0 | 0 | 3 (15.0%) | 17 (85.0%) | 0 | 20 |
| Public Places | 0 | 0 | 0 | 11 (12.8%) | 72 (83.7%) | 3 (3.5%) | 86 |
PCU: Primary Care Unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



