Submitted:
03 March 2025
Posted:
04 March 2025
You are already at the latest version
Abstract
Strumal carcinoid tumors of the ovary are rare neoplasms composed of an intimate mixture of thyroid and carcinoid tissues. While various theories regarding their histogenesis have been proposed, direct evidence confirming the origin of the carcinoid component has been lacking. We report a case of a 40-year-old female with a left ovarian strumal carcinoid arising in a mature cystic teratoma. Morphological and immunohistochemical findings provide convincing evidence that the carcinoid component originates from thyroid follicular epithelium undergoing neuroendocrine differentiation. A single-cell invasion pattern was also identified, expanding the known histological spectrum of strumal carcinoids. Our case provides definitive immunohistochemical evidence for the histogenetic origin of strumal carcinoids, offering new insights into their pathogenesis. Recognizing these distinct staining and invasive patterns are critical for accurate diagnosis and differentiation from metastatic disease.
Keywords:
Ovary
; Strumal carcinoid
; Strumal ovarii
; Thyroid
; Single cell pattern
; TTF-1
; PAX-8
; CD56
; Synapthophysin
1. Introduction
Strumal carcinoid tumors of the ovary are exceedingly rare neoplasms that present a unique diagnostic and conceptual challenge. There has been debate whether strumal carcinoids are carcinoids with areas resembling thyroid or arise from bonafide thyroid tissue in struma. While thyroid nature has been proven by demonstrating positive TTF-1 in the struma component, evidence for the origin of the carcinoid component is sparse. Herein, we describe a case of strumal carcinoid and use a panel of markers to show definitive morphological and immunohistochemical evidence of the evolution of the neoplasm from struma ovarii to struma carcinoid within the same lesion. We also report a unique component of a more sinister single-cell pattern of invasion apart from the usual insular, trabecular, and mucinous patterns.
2. Case Presentation
The patient is a 40-year-old female with a history of chronic constipation who presented with abdominal and pelvic pain, fever, and episodes of hypotension. A computed tomography (CT) scan incidentally identified a left ovarian mass with solid and cystic components and ovarian enlargement. Subsequent MRI revealed a well-marginated, mixed solid and cystic 8.3 cm left ovarian mass with enhancement and diffusion restriction in the solid components, raising suspicion for malignancy, including sex cord-stromal or germ cell tumors (Figure 1). Tumor markers were within normal limits, including CA125 at 12.3 U/mL, carcinoembryonic antigen (CEA) at 1.3 ng/mL, CA19-9 at 7.7 U/mL, Inhibin B at 106 pg/mL, and alpha-fetoprotein (AFP) at 2.1 ng/mL, except for elevated lactate dehydrogenase (LDH) at 243 U/L. No evidence of metastatic disease was observed on contrast-enhanced MRI.
The patient was referred to gynecologic oncology and underwent a total laparoscopic hysterectomy, bilateral salpingo-oophorectomy, pelvic and para-aortic lymph node dissection, omentectomy, and staging biopsies.
Grossly, the left ovary weighed 155 g and measured 9.5 x 7.8 x 4.5 cm. Cross-sectioning revealed a round, yellow-tan, variegated, lobulated lesion with a focal cystic area filled with yellow-tan mucoid fluid, measuring 2.5 x 2.0 x 1.5 cm. Within this lesion, a well-circumscribed yellow-tan to brown-tan area was identified, containing necrotic cheesy material and hair. The right ovary exhibited a biloculated cyst measuring 3.4 x 2.8 x 1.4 cm, filled with yellow-tan fluid and lined by a smooth, unremarkable wall.
Microscopic analysis identified thyroid tissue consistent with struma ovarii, juxtaposed with a neuroendocrine neoplasm (carcinoid, Figure 3A) all arising in the background of a mature cystic teratoma. The strumal component had no features of papillary or follicular thyroid carcinoma. The carcinoid component predominated and showed foci with large islands of variable-sized nests and acini within the fibrous stroma (Figure 2A insular pattern) and other areas that show mixed trabecular and insular pattern (Figure 2B). Focal areas with mucinous patterns (Figure 2C) were also identified. Additionally, a pattern of single-cell invasion was identified at the ovarian surface, away from the main tumor (Figure 2D). These cells closely resembled luteinized ovarian stromal cells but stained positive for synaptophysin, like the carcinoid tumor (Figure 6).
Immunohistochemical stains performed with adequate controls show that the struma is strongly positive for CK-7, PAX-8, TTF-1, and CD56 (membranous, Figure 5) and negative for synaptophysin, chromogranin-A, CDX-2, and GATA-3. In contrast, the carcinoid was focally interspersed positive for TTF-1 (Figure 3B), patchy positive for CDX-2 and PAX-8 (Figure 3C), strongly positive for synaptophysin (Figure 3D) and CD56 (basal and cytoplasmic, Figure 5), and negative for GATA-3, calretinin, and chromogranin-A.
The interface between struma ovarii and carcinoid showed strong PAX-8 and uniform TTF-1 staining in the struma but gradual loss of TTF-1 (Figure 4B) with retained/weak PAX-8 staining (Figure 4C), moving away from the struma component and into the carcinoid. Synaptophysin was positive in the carcinoid component with few scattered cells staining in the strumal component (Figure 4D).
No metastatic lesions were identified in the four pelvic and paraaortic lymph nodes examined. At an 8-month postoperative follow-up, the patient showed no evidence of recurrence or metastasis.
3. Discussion and Literature Review
Strumal carcinoid tumors of the ovary are exceedingly rare ovarian germ cell tumors composed of an intimate mixture of thyroid and carcinoid tissues, and much of our current understanding derives from isolated case reports and small case series over the past five decades. Comprehensive large-scale analyses have remained scarce since the first documented case in 1970 (Scully 1970). For our review, we conducted a literature search using the keywords “ovarian strumal carcinoid” in PubMed and Google Scholar. We prioritized studies that investigated the tumor’s origin using immunohistochemical staining or ultrastructural methods. We also included studies that, while not directly addressing tumor origin, presented immunohistochemical findings that could indirectly support hypotheses regarding histogenesis. In total, 15 relevant articles (Table 1) were reviewed, including case reports, case series, research studies, and systematic case reviews.
Although studies such as those by Robboy and Scully (Robboy and Scully 1980), which examined 50 cases, and Theurer et al(Theurer, Ingenwerth et al. 2020), which evaluated 13 cases, have provided valuable insights into the histological characteristics of these tumors, the origin of strumal carcinoid tumors remains controversial. More recently, two systematic case reviews (Li, Wang et al. 2022, Turla, Zamparini et al. 2022) each encompassing over 100 cases, have provided further clinical and pathological data. However, debate persists regarding the tumor’s pathogenesis. One theory proposes that they arise from a common progenitor cell within strumal ovarii, while another posits that they reflect two distinct entities—an ovarian teratoma-derived thyroid component and a neuroendocrine tumor. Some researchers have questioned whether the carcinoid component might represent metastasis from the gastrointestinal tract. Several findings also suggest that the strumal carcinoid may represent a medullary carcinoma of thyroid within an ovarian teratoma. Over the years, various investigations have yielded different conclusions, and no definitive consensus has been reached regarding the pathogenesis of this rare tumor.
The predominant theory is that both the thyroid follicles and carcinoid components arise from a single precursor cell population. Multiple lines of evidence support this hypothesis. In their study of 50 cases of strumal carcinoid, Robboy and Scully (Robboy and Scully 1980) observed a close intermixture of thyroid-like follicles and carcinoid elements, with argentaffin (carcinoid) cells often lining thyroid follicles containing birefringent colloid crystals. These findings strongly suggest that both components derive from the same endodermal primordium rather than representing a coincidental “collision” of separate neoplasms or a metastatic process. A case review study of 13 ovarian strumal carcinoid tumors provided additional evidence. Electron microscopy revealed that thyroid follicular cells expressing thyroglobulin within the struma contained neuroendocrine granules resembling those of C cells (Snyder and Tavassoli 1986). However, these cells were negative for calcitonin, suggesting that thyroid follicular cells with C-cell–like features may give rise to the carcinoid component. Additionally, other earlier case studies (Takubo, Yasui et al. 1986, Tsubura and Sasaki 1986, Stagno, Petras et al. 1987) have reinforced the theory of multidirectional differentiation from an endodermal origin through ultrastructural examinations. Subsequent immunohistochemical studies have provided additional evidence not only supporting the unified origin theory but also raising the hypothesis that carcinoid components arise from thyroid follicular epithelium. In a series of 13 strumal carcinoid tumors (Theurer, Ingenwerth et al. 2020), both the strumal and carcinoid components expressed thyroglobulin, TTF-1, and neuroendocrine markers (chromogranin and synaptophysin), indicating a consistent follicular epithelial lineage. Other investigations (Greco, LiVolsi et al. 1979, Senterman, Cassidy et al. 1984, Snyder and Tavassoli 1986) corroborated these findings, reporting thyroglobulin expression in the strumal component and transitional zones where the thyroid follicles merged with nests of carcinoid cells. These studies provide indirect evidence supporting the hypothesis that the carcinoid component arises from bona fide thyroid tissue within the struma. Further evidence comes from Snyder and Tavassoli (Snyder and Tavassoli 1986), as well as Kimura et al(Kimura, Sasano et al. 1986) who identified hybrid cells exhibiting both thyroid and neuroendocrine features through immunohistochemical and ultrastructural studies, suggesting a transitional state between the two cell types. However, Hamazaki S et al (Hamazaki, Okino et al. 2002) observed that while the follicular cells were positive for TTF-1, the carcinoid component largely lacked TTF-1 expression, leading them to conclude that there is divergent differentiation from a common progenitor. These findings suggest that strumal carcinoid tumors originate from a single precursor cell population with mixed (amphicrine) differentiation potential, capable of developing into both thyroid follicular epithelial and neuroendocrine identities. The presence of hybrid cells exhibiting both thyroid and neuroendocrine features, combined with immunostaining results showing expression of thyroid differentiation markers (thyroglobulin and TTF-1) in the carcinoid component and in transitional areas, strongly indicates that the carcinoid component arises directly from the nearby thyroid follicular epithelium.
Another hypothesis suggests that the carcinoid component arises from parafollicular C cells within the thyroid tissue of struma ovarii, based on the detection of calcitonin in the carcinoid component. Blaustein (Blaustein 1979) reported a case of a strumal carcinoid tumor secreting calcitonin, with elevated serum calcitonin levels and immunohistochemical staining confirming calcitonin expression in the carcinoid areas. Similarly, several case studies (Greco, LiVolsi et al. 1979, Ulbright, Roth et al. 1982) observed calcitonin positivity in the carcinoid component, supporting the possibility of C-cell differentiation. Furthermore, a systematic literature review and pooled analysis (Turla, Zamparini et al. 2022) revealed that calcitonin was expressed in 52% of tumors (12/23), providing additional evidence for C-cell origin. These findings raise the potential relationship between strumal carcinoid tumors and medullary thyroid carcinoma, known for its C-cell origin and calcitonin secretion. However, calcitonin expression is not consistently observed across all cases. S. Theurer et al. (Theurer, Ingenwerth et al. 2020) failed to detect calcitonin in any of their 13 cases. Likewise, other investigators (Tsubura and Sasaki 1986) (Senterman, Cassidy et al. 1984, Hamazaki, Okino et al. 2002, Ciobanu Apostol, BuTureanu et al. 2017, Machalekova, Kolnikova et al. 2018) have also reported an absence of calcitonin staining in both the thyroid and carcinoid components of strumal carcinoid tumors. This inconsistency suggests that calcitonin production may not be a defining feature of these neoplasms. Additionally, the carcinoid component typically resembles a gastrointestinal carcinoid tumor rather than medullary thyroid carcinoma, which often exhibits amyloid deposition and distinct cytological features. Taken together, these observations weaken the argument for a direct C-cell origin and thus challenge the hypothesis that strumal carcinoids should be classified as medullary thyroid carcinoma-like lesions.
In contrast, another early theory proposes that strumal carcinoids are purely neuroendocrine tumors that resemble a follicular architecture, rather than incorporating true thyroid tissue. Ultrastructural studies (Hart and Regezi 1978, Sarcevic, Separovic et al. 1990) demonstrated that both the follicular and trabecular components contain numerous neurosecretory granules, which are characteristic of neuroendocrine cells. These observations suggest that the follicular structures are formed by neuroendocrine cells resembling the morphology of thyroid follicles. However, the thyroid nature of these tumors has been confirmed by demonstrating positive expression of TTF-1 and thyroglobulin in the struma component, thereby refuting the hypothesis that strumal carcinoids are purely neuroendocrine in origin.
Our case provides strong evidence that strumal carcinoid tumors arise from thyroid follicular epithelium within struma ovarii undergoing neuroendocrine differentiation. Immunohistochemical analysis reveals that the strumal component is strongly positive for CK7, PAX-8, and TTF-1, firmly establishing its thyroid follicular epithelial identity. The adjacent carcinoid component, arranged in insular and trabecular patterns, demonstrates robust expression of neuroendocrine markers such as synaptophysin and CD56. As one moves from the struma into the carcinoid areas, there is a gradual reduction in TTF-1 staining and a shift to weaker PAX-8 expression with strong synaptophysin expression. This continual immunophenotypic transition strongly suggests that the neuroendocrine component emerges directly from previously established thyroid follicular cells rather than metastasizing from another primary site such as the gastrointestinal tract or even native Mullerian tissue. Interestingly, the staining pattern of CD56 differs between the two components: in the strumal areas, CD56 shows strong membranous staining, consistent with its typical expression in thyroid follicular epithelium. However, in the carcinoid component and transitional zone, CD56 exhibits basal and cytoplasmic staining, reflecting the shift toward a neuroendocrine phenotype. This distinct staining pattern reinforces the notion that the carcinoid component arises directly from the thyroid follicular cells within the struma. Moreover, chromogranin-A staining was negative in the carcinoid component, which aligns with prior studies suggesting that ovarian carcinoid tumors often resemble gastrointestinal carcinoid tumors, where synaptophysin is intensely expressed but chromogranin expression is variable or absent (Shia, Tang et al. 2008, Jukic, Limani et al. 2012). The patchy positivity for CDX2 and the focal mucinous pattern observed in the carcinoid component further support its resemblance to gastrointestinal-type carcinoid tumors.
Furthermore, the patient’s history of chronic constipation raises the possibility of peptide YY (PYY) secretion by the carcinoid component, although the PYY expression was not directly evaluated. Several case studies (Motoyama, Katayama et al. 1992, Matsunami, Takagi et al. 2011, Noh, Kwon et al. 2017) previously identified a large number of PYY-secreting cells in strumal carcinoid tumors. PYY is known to inhibit intestinal motility, including gastric acid secretion, gastric emptying, and reduce jejunal and colonic movement. While PYY-producing neuroendocrine cells are typically derived from midgut or hindgut precursors, the patchy CDX2 expression observed in our case suggests a resemblance to gastrointestinal carcinoid tumors.
An important finding in our case was the presence of a single-cell pattern of invasion at the ovarian surface, away from the main tumor mass. This feature is significant because single-cell invasion must be carefully differentiated from luteinized stromal cells and metastatic carcinoma, which can be morphologically similar. Awareness of this pattern is imperative, especially on frozen sections, since an overcall can result in unnecessary staging in an otherwise mostly benign entity. While luteinized stromal cells are benign and associated with ovarian physiology, the invasive cells in our case were cytologically atypical and strongly positive for synaptophysin, confirming their neuroendocrine origin. The identification of these invasive cells emphasizes the importance of immunohistochemical analysis in distinguishing between benign stromal processes and malignant invasion. To our knowledge, this is the first report describing single-cell invasion in a strumal carcinoid tumor, highlighting a novel and potentially important feature of this rare neoplasm.
Our case thus aligns with the growing body of literature suggesting that strumal carcinoids represent a distinct ovarian neoplasm originating from a single histogenetic pathway. The presence of a transitional zone, which retains thyroid-specific characteristics while progressively adopting neuroendocrine traits, supports the hypothesis that the carcinoid component arises directly from thyroid follicular epithelium within struma ovarii.
4. Conclusions
We provide strong morphological and immunohistochemical evidence that strumal carcinoid likely develops from thyroid tissue undergoing neuroendocrine differentiation in struma ovarii. Specifically, retained/weak PAX-8 with interspersed TTF-1 in an adnexal carcinoid is a distinct pattern to be aware of when dealing with carcinoid tumors of unknown etiology, strongly favoring an ovarian primary (specifically, from struma ovarii) and not metastasis from the gastrointestinal tract or other Mullerian tissue. Recognizing this potential origin is crucial for the diagnosis, management, and understanding of the tumor's behavior. Lastly, the single-cell invasion pattern we have identified broadens the known morphological spectrum of strumal carcinoid tumors and is a significant feature to consider, especially in the context of metastases or intraoperative frozen sections.
Author Contributions
Ridin Balakrishnan and Yu Liu drafted the manuscript. Liz Yang and Asra Feroze collected clinical data. Ridin Balakrishnan revised the manuscript and is the author guarantor. All authors also revised the final manuscript.
Funding
No fundings.
Institutional Review Board Statement
This case report is exempt from Institutional Review Board approval.
Informed Consent Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal upon request.
Conflicts of Interest
The authors have nothing to disclose.
References
- Blaustein, A. Calcitonin secreting struma-carcinoid tumor of the ovary. Hum. Pathol. 1979, 10, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Apostol, D.G.C.; Buţureanu, T.A.; Socolov, D.G.; Scripcaru, D.C.; Rosin, O.L.; Lozneanu, L. Ovarian strumal carcinoid - case report. Rom J Morphol Embryol 2017, 58, 1035–1040. [Google Scholar]
- Greco, M.A.; Livolsi, V.A.; Pertschuk, L.P.; Bigelow, B. Strumal carcinoid of the ovary.An analysis of its components. Cancer 1979, 43, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Hamazaki, S.; Okino, T.; Tsukayama, C.; Okada, S. Expression of thyroid transcription factor-1 in strumal carcinoid and struma ovarii: An immunohistochemical study. Pathol. Int. 2002, 52, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Hart, W.R.; Regezi, J.A. Strumal Carcinoid of the Ovary: Ultrastructural Observations and Long-term Follow-up Study. Am. J. Clin. Pathol. 1978, 69, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Jukić, Z.; Limani, R.; Luci, L.G.; Nikić, V.; Mijić, A.; Tomas, D.; Krušlin, B. hGH and GHR expression in large cell neuroendocrine carcinoma of the colon and rectum. Anticancer Res. 2012, 32, 3377–81. [Google Scholar] [PubMed]
- Kimura, N.; Sasano, N.; Namiki, T. Evidence of Hybrid Cell of Thyroid Follicular Cell and Carcinoid Cell in Strumal Carcinoid. Int. J. Gynecol. Pathol. 1986, 5, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, X.; Sui, X.; Zhang, X.; Yin, M.; Yang, J. Clinical characteristics and survival outcomes in patients with ovarian strumal carcinoid. BMC Cancer 2022, 22, 1–9. [Google Scholar] [CrossRef]
- Macháleková, K.; Kolníková, G.; Redecha, M.; Žúbor, P.; Kajo, K. Strumal carcinoid of the ovary - report of two cases and review of literature. Ceska Gynekol. 2018, 83, 452–457. [Google Scholar] [PubMed]
- Matsunami, K.; Takagi, H.; Ichigo, S.; Murase, T.; Ikeda, T.; Imai, A. Peptide YY producing strumal carcinoid tumor of the ovary. Eur J Gynaecol Oncol. 2011, 32, 201–2. [Google Scholar] [PubMed]
- Motoyama, T.; Kafayama, Y.; Watanabe, H.; Okazaki, E.; Shibuya, H. Functioning ovarian carcinoids induce severe constipation. Cancer 1992, 70, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Noh, H.K.; Kwon, B.S.; Kim, Y.H.; Lee, N.K.; Choi, K.U.; Suh, D.S.; Lee, D.H.; Kim, K.H. Peptide YY producing strumal carcinoid tumor of the ovary in a postmenopausal woman: a rare cause of chronic constipation. Obstet. Gynecol. Sci. 2017, 60, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Robboy, S.J.; Scully, R.E. Strumal carcinoid of the ovary: An analysis of 50 cases of a distinctive tumor composed of thyroid tissue and carcinoid. Cancer 1980, 46, 2019–2034. [Google Scholar] [CrossRef] [PubMed]
- Sarcević, B.; Separović, V.; Sćukanec-Spoljar, M.; Pejsa, V. [Strumal carcinoid tumor of the ovary--histologic and electron microscopy characteristics of the tumor]. Lijec Vjesn. 1990, 112, 381–393. [Google Scholar] [PubMed]
- Scully, R.E. Recent progress in ovarian cancer. Hum. Pathol. 1970, 1, 73–98. [Google Scholar] [CrossRef] [PubMed]
- Senterman, M.K.; Cassidy, P.N.; Fenoglio, C.M.; Ferenczy, A. Histology, ultrastructure, and immunohistochemistry of strumal carcinoid: A case report. Int J Gynecol Pathol 1984, 3, 232–240. [Google Scholar] [PubMed]
- Shia, J., L. H. Tang, M. R. Weiser, B. Brenner, N. V. Adsay, E. B. Stelow, L. B. Saltz, J. Qin, R. Landmann, G. D. Leonard, D. Dhall, L. Temple, J. G. Guillem, P. B. Paty, D. Kelsen, W. D. Wong and D. S. Klimstra (2008). "Is nonsmall cell type high-grade neuroendocrine carcinoma of the tubular gastrointestinal tract a distinct disease entity?" Am J Surg Pathol 32(5): 719-731.
- Snyder, R. R. and F. A. Tavassoli (1986). "Ovarian strumal carcinoid: immunohistochemical, ultrastructural, and clinicopathologic observations." Int J Gynecol Pathol 5(3): 187-201.
- Stagno, P. A., R. E. Petras and W. R. Hart (1987). "Strumal carcinoids of the ovary. An immunohistologic and ultrastructural study." Arch Pathol Lab Med 111(5): 440-446.
- Takubo, K., H. Yasui and K. Toi (1986). "Strumal carcinoid of the ovary. A case report." Acta Pathol Jpn 36(5): 765-771.
- Theurer, S.; Ingenwerth, M.; Herold, T.; Herrmann, K.; Schmid, K.W. Immunohistochemical Profile and 47-Gene Next-Generation Sequencing (NGS) Solid Tumor Panel Analysis of a Series of 13 Strumal Carcinoids. Endocr. Pathol. 2020, 31, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Tsubura, A. and M. Sasaki (1986). "Strumal carcinoid of the ovary. Ultrastructural and immunohistochemical study." Acta Pathol Jpn 36(9): 1383-1390.
- Turla, A., M. Zamparini, M. Milione, S. Grisanti, V. Amoroso, R. Pedersini, D. Cosentini and A. Berruti (2022). "Ovarian Strumal Carcinoid: Case Report, Systematic Literature Review and Pooled Analysis." Front Endocrinol (Lausanne) 13: 871210.
- Ulbright, T.M.; Roth, L.M.; Ehrlich, C.E. Ovarian Strumal Carcinoid: An Immunocytochemical and Ultrastructural Study of Two Cases. Am. J. Clin. Pathol. 1982, 77, 622–631. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Abdominopelvic magnetic resonance imaging (MRI) shows an adnexal mass with enhancement.
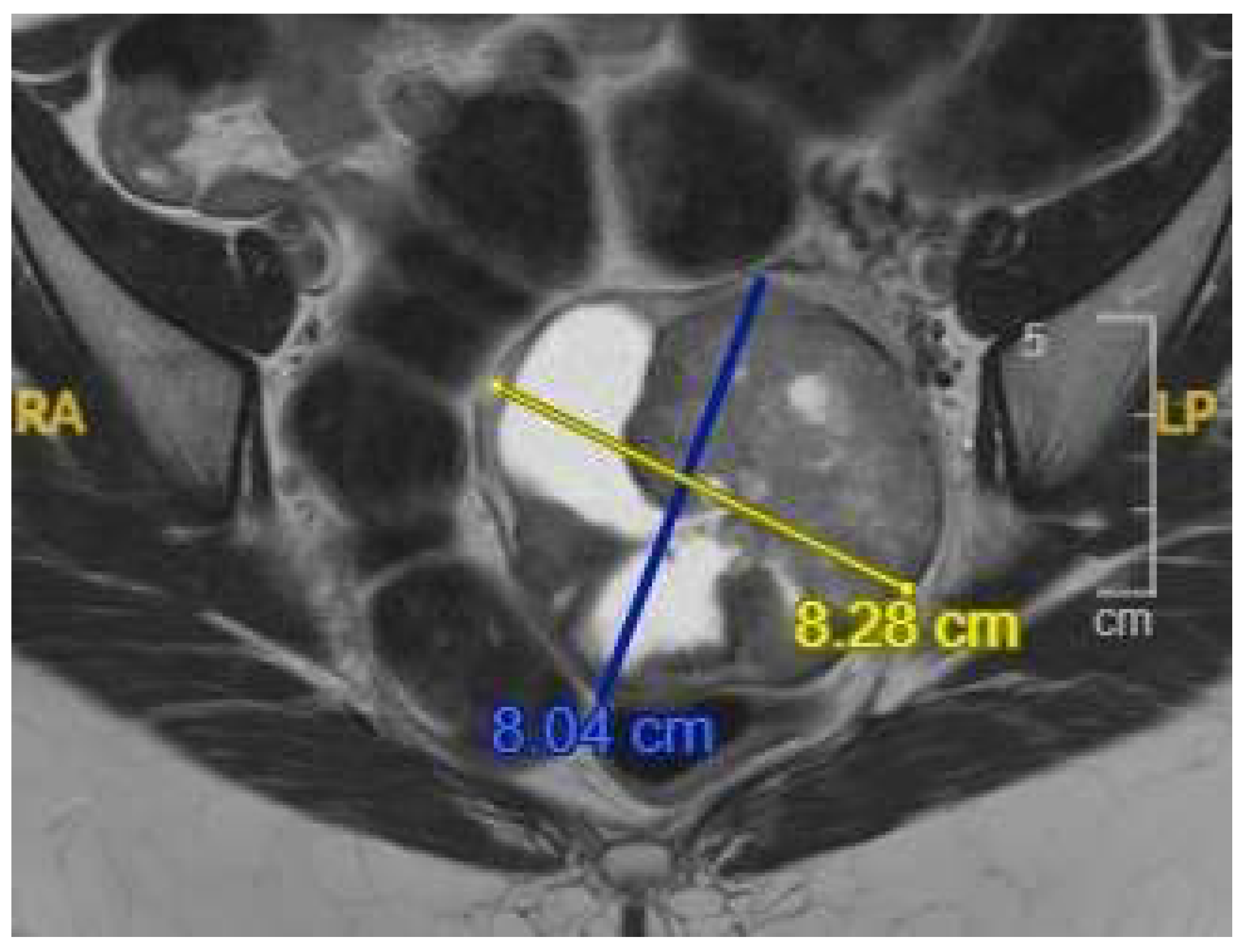
Figure 2.
Histopathological patterns of the carcinoid tumor (HE, 200x). (A) Insular pattern displaying large nests and acini embedded within a fibrous. (B) Mixed trabecular and Insular pattern with interweaving trabeculae and large nests of tumor cells. (C) Focal mucinous pattern with tumor cells demonstrating intracellular and extracellular mucin accumulation. (D) Isolated single-cell invasion observed at the ovarian surface, away from the primary tumor mass.
Figure 2.
Histopathological patterns of the carcinoid tumor (HE, 200x). (A) Insular pattern displaying large nests and acini embedded within a fibrous. (B) Mixed trabecular and Insular pattern with interweaving trabeculae and large nests of tumor cells. (C) Focal mucinous pattern with tumor cells demonstrating intracellular and extracellular mucin accumulation. (D) Isolated single-cell invasion observed at the ovarian surface, away from the primary tumor mass.
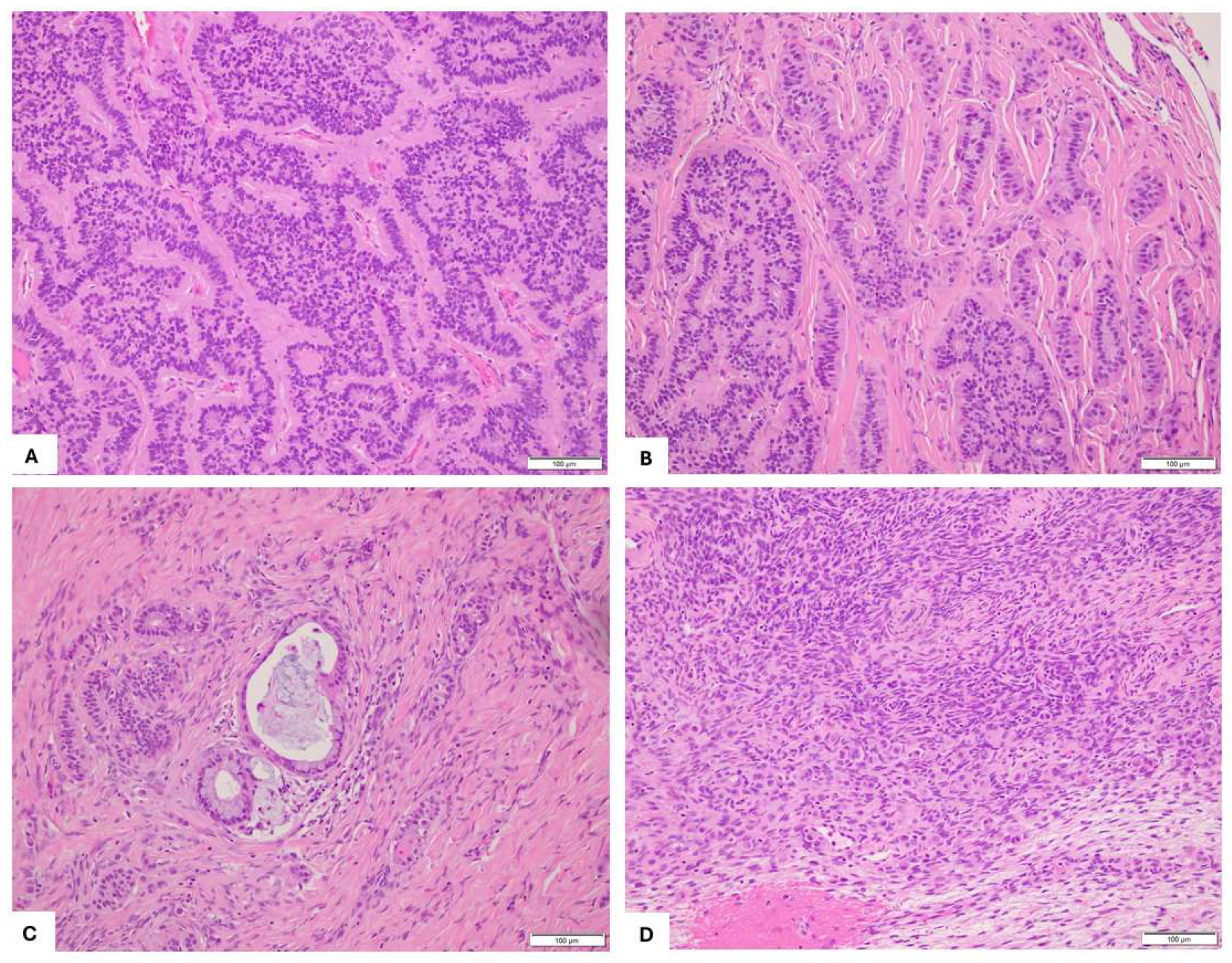
Figure 3.
Immunohistochemical staining of ovarian strumal carcinoid. (A) HE, 200×. (B) TTF-1: focal, interspersed positivity, 200×. (C) PAX8: weak but diffuse positivity, 200×. (D) Synaptophysin: strong, diffuse positivity (200×).
Figure 3.
Immunohistochemical staining of ovarian strumal carcinoid. (A) HE, 200×. (B) TTF-1: focal, interspersed positivity, 200×. (C) PAX8: weak but diffuse positivity, 200×. (D) Synaptophysin: strong, diffuse positivity (200×).
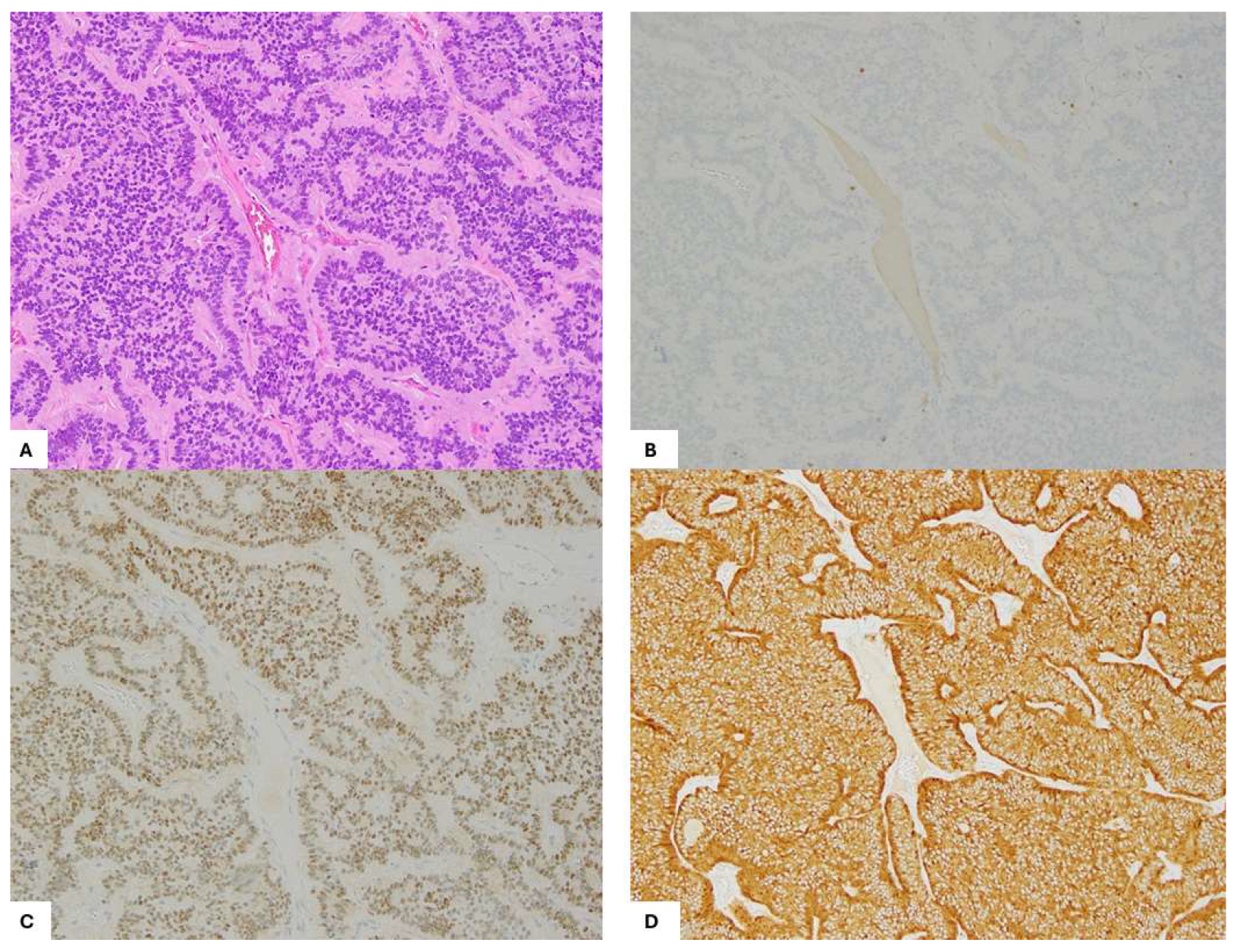
Figure 4.
Strumal carcinoid arising from struma ovarii. (A) H&E, 100x. Immunohistochemistry Staining (100x): gradual loss of TTF-1 (B) with retained/weak PAX8 (C) expression moving away from struma ovarii into carcinoid. Synaptophysin (D) is positive in the carcinoid component with few scattered cells staining in the struma component.
Figure 4.
Strumal carcinoid arising from struma ovarii. (A) H&E, 100x. Immunohistochemistry Staining (100x): gradual loss of TTF-1 (B) with retained/weak PAX8 (C) expression moving away from struma ovarii into carcinoid. Synaptophysin (D) is positive in the carcinoid component with few scattered cells staining in the struma component.
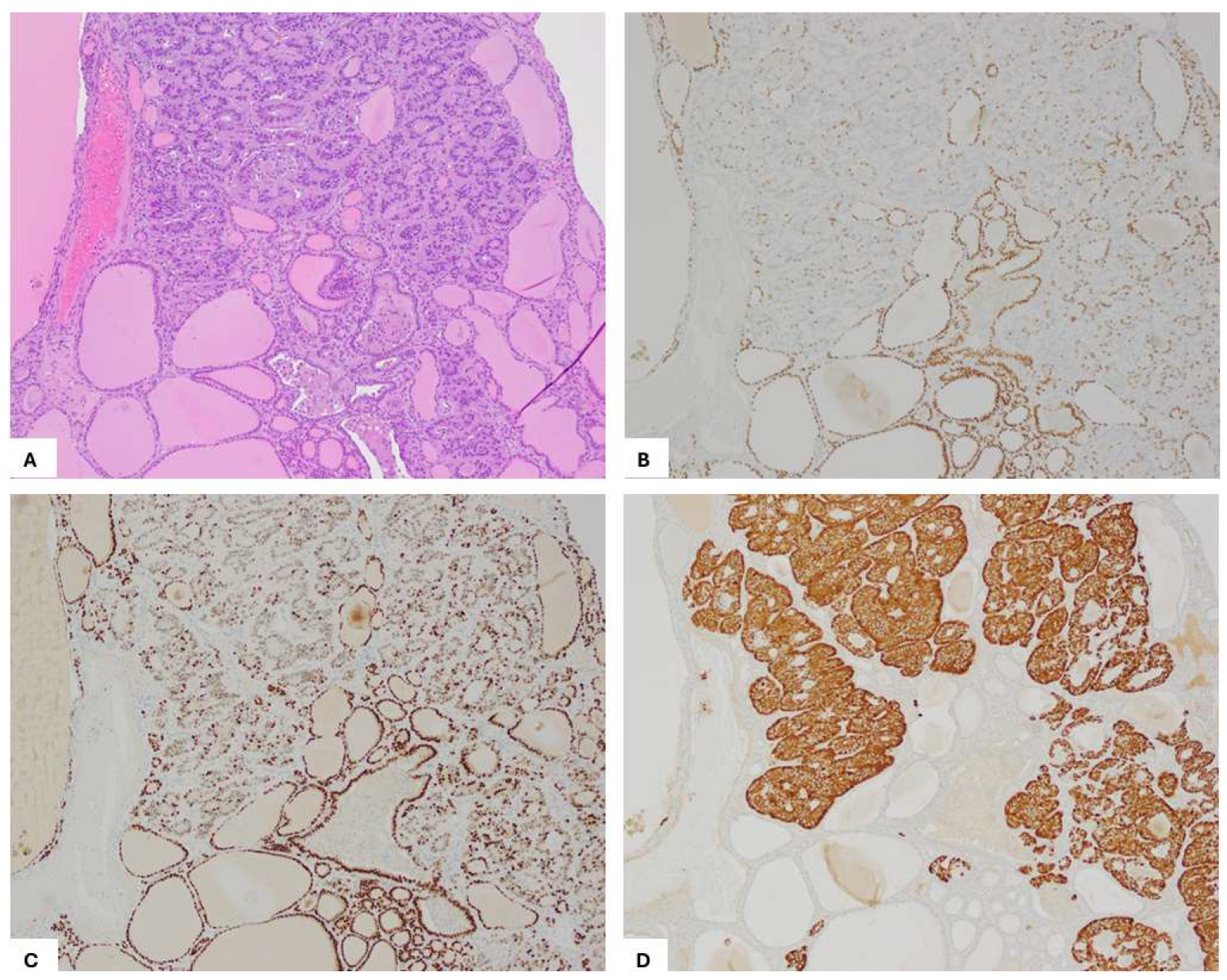
Figure 5.
CD56 immunohistochemistry staining in transitional zone from struma to carcinoid. (A) HE, 100x. (B, C) CD56 immunostaining showing membranous expression in the thyroid follicular epithelium of the struma and both membranous and basal expression in the tumor cells of the carcinoid component, shown at 100×(B) and 200× (C).
Figure 5.
CD56 immunohistochemistry staining in transitional zone from struma to carcinoid. (A) HE, 100x. (B, C) CD56 immunostaining showing membranous expression in the thyroid follicular epithelium of the struma and both membranous and basal expression in the tumor cells of the carcinoid component, shown at 100×(B) and 200× (C).
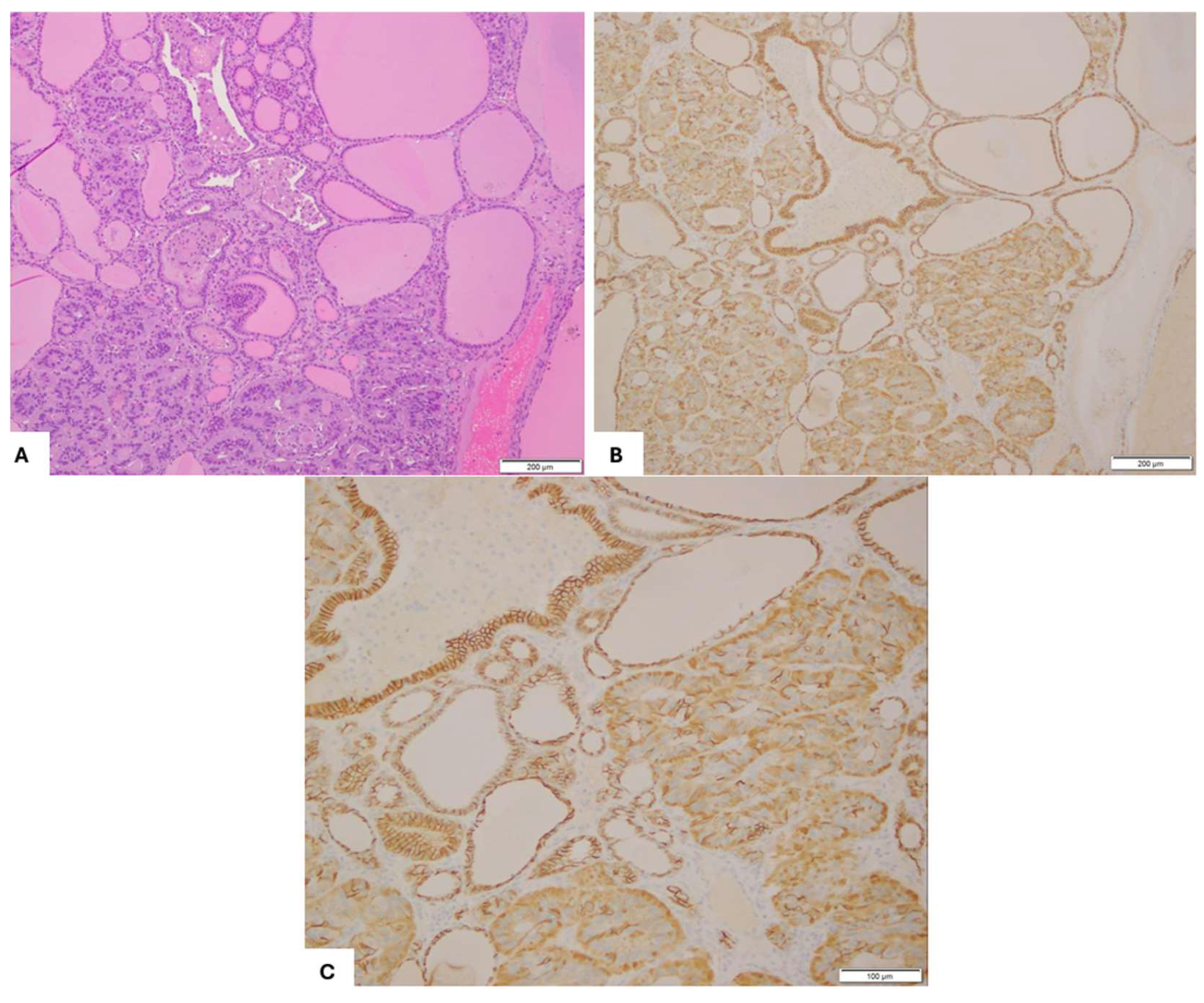
Figure 6.
Strumal Carcinoid with Single Cell Pattern of Invasion. (A) H&E, 200x. Immunohistochemistry Staining (200x) positive for Synaptophysin (B).
Figure 6.
Strumal Carcinoid with Single Cell Pattern of Invasion. (A) H&E, 200x. Immunohistochemistry Staining (200x) positive for Synaptophysin (B).
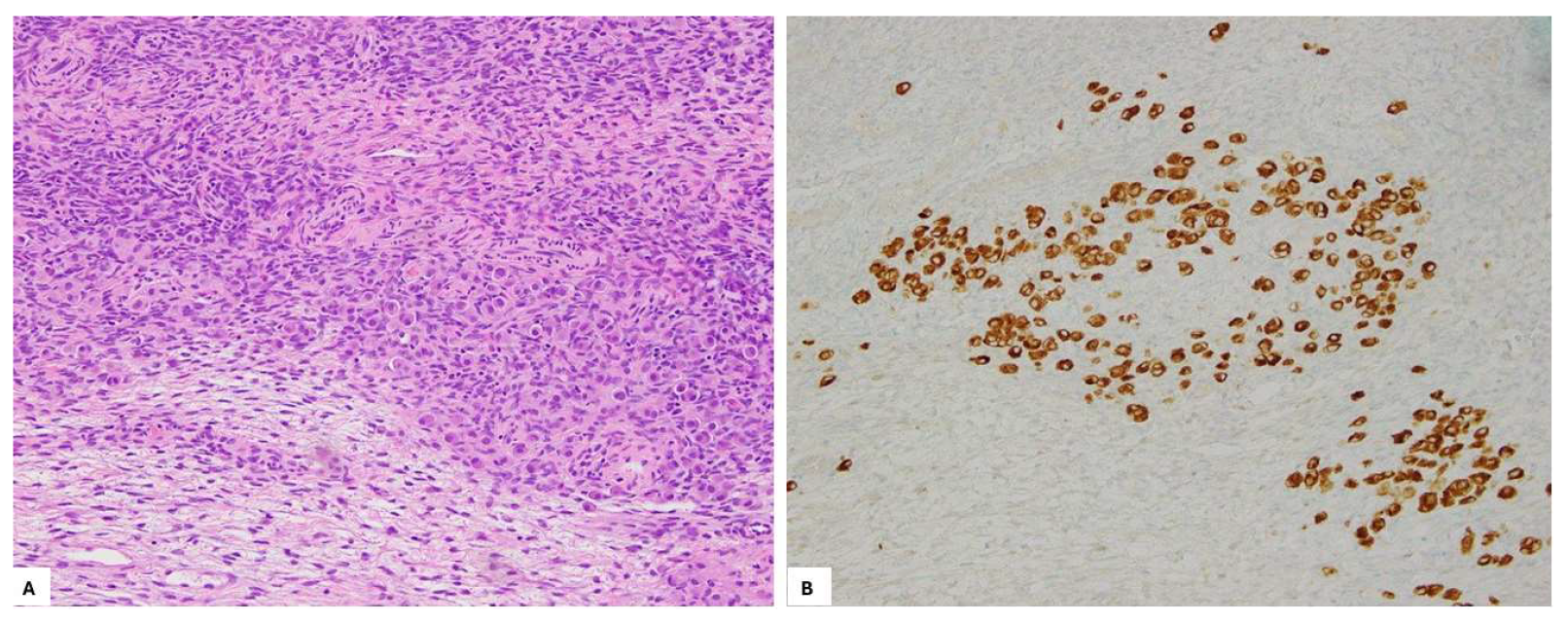

Table 1.
Summary of Studies on the Origin of Strumal Carcinoid Tumors of the Ovary.
| Reference | Number of Cases | Immunostaining/Ultrastructural Findings in strumal component | Immunostaining/Ultrastructural Findings in Carcinoid Component | Proposed Carcinoid Origin Hypothesis |
|---|---|---|---|---|
| S Robboy, et al 1980 (Robboy and Scully 1980) | 50 | -Calcium oxalate crystals present in half cases -Cells with argentaffin granules lined thyroid follicles -Positive for TG (n=2/50) |
-Argentaffin granules and electron-dense granules are present | Support unified Origin |
| Takubo K, et al 1986 (Takubo, Yasui et al. 1986) | 1 | -Neurosecretory-type granules in the cytoplasm of thyroid follicular -Positive for TG |
-Neurosecretory-type granules in the cytoplasm of carcinoid | Support unified origin |
| Tsubura A 1986 (Tsubura and Sasaki 1986) | 1 | -Positive for TG | -Carcinoid cells expanding toward the inner layer of the follicles -Negative for CAL and amyloid |
Support unified origin Not support origin from C cell |
| Stagno P, et al 1987 (Stagno, Petras et al. 1987) | 6 | -Positive for TG (6/6) -Thyroid follicular epithelium lined by non-neuroendocrine cells |
-Positive for CGA (5/6) and CAL (1/6) -Carcinoid cells progressively replace thyroid epithelial cells |
Support origin from thyroid tissue in strumal ovarii |
| S. Theurer, et al 2020 (Theurer, Ingenwerth et al. 2020) |
13 | -Positive for TG (100%), TTF-1(84.6%), CGA (76.9%), SYN (7.7%) -Negative for CDX2, CAL SSTR2a, and SSTR5 |
-Positive for TG (100%), TTF-1(84.6%), CGA (92.3%), SYN (100%), SSTR2a (92.3%), SSTR5 (46.1%) -Negative for CDX2 and CAL |
Support origin from thyroid tissue in strumal ovarii Not support origin from C cells |
| L. Greco, et al 1979 (Greco, LiVolsi et al. 1979) | 1 | -Positive for TG in thyroid follicles and transitional zone | -Negative for TG -Positive for CAL |
Support origin from thyroid tissue in strumal ovarii |
| M Senterman,et al 1984 (Senterman, Cassidy et al. 1984) | 1 | -Positive for TG in thyroid follicles and transitional zone -Negative for CAL |
-Negative for TG and CAL |
Support origin from thyroid tissue in strumal ovarii Not support origin from C cell |
| R. Snyder, et al 1986 (Snyder and Tavassoli 1986) | 13 | -Positive for TG in thyroid follicles and transitional zone (12/12) - NE granules in thyroid follicles (6/6) |
-Negative for TG and CAL (12/12) - NE granules in carcinoid (6/6) |
Support origin from thyroid tissue in strumal ovarii Not support origin from C cell |
| Kimura N, et al 1986 (Kimura, Sasano et al. 1986) | 1 | - Strong positive for TG - Intensive argyrophilia - Abundant neurosecretory granules, microfilaments, colloid-like droplets in thyroid follicles |
- Weak positive for TG - Intensive argyrophilia - Abundant neurosecretory granules, microfilaments, colloid-like droplets in carcinoid |
Support origin from hybrid cells having both thyroid and neuroendocrine features |
| S Hamazaki, et al 2002 (Hamazaki, Okino et al. 2002) | 2 | -Positive for TTF-1, TG -Negative for CGA, SYN, PAP, CAL |
-Positive for CGA, SYN, PAP -Negative for TTF-1, TG, CAL |
Divergent differentiation from a common progenitor Not support origin from C cell |
| K Macháleková 2018 (Machalekova, Kolnikova et al. 2018) | 2 | -Positive for TTF-1, TG -Negative for CAL, CEA |
-Positive for CGA, SYN -Negative for CAL, CEA |
Not support origin from C cell |
| C Apostol ,et al 2017 (Ciobanu Apostol, BuTureanu et al. 2017) | 1 | -Positive for TTF-1, TG, CD56. CK7, CK19 -Negative for CAL, HBME1, GFAP |
-Positive for SYN, CGA, CD56 -Negative for CK7, CAL, GFAP |
Not support origin from C cell |
| Blaustein, A 1979 (Blaustein 1979) | 1 | N/A | -Positive for CAL and 5-HA - Ultrastructural similarity to medullary carcinoma |
Support origin from C cell |
| Ulbright T, et al 1982(Ulbright, Roth et al. 1982) | 2 | -Granule-containing cells replaced some follicular epithelial cells |
-Positive for CAL in transitional zone and carcinoid | Support origin from C cell |
| A.Turla, et al 2022(Turla, Zamparini et al. 2022) | 117 | -Positive for TG (41/45), TTF-1(22/25) |
-Positive for CGA (39/39), SYN (31/31), CD56 (16/16), NSE (13/13), CAL (12/23) | Support origin from C cells |
TG: Thyroglobulin; TTF-1: Thyroid Transcription Factor-; CGA: Chromogranin A; SYN: Synaptophysin; CAL: Calcitonin; SSTR2a: Somatostatin Receptor 2a; SSTR5: Somatostatin Receptor 5; CEA: Carcinoembryonic Antigen; CK7: Cytokeratin 7; CK19: Cytokeratin 19; CD56: Neural Cell Adhesion Molecule; NSE: Neuron-Specific Enolase; 5-HA: 5-Hydroxytryptamine (Serotonin).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



