Submitted:
04 March 2025
Posted:
04 March 2025
You are already at the latest version
Abstract
Background:
Cardiopulmonary resuscitation (CPR) is a vital intervention for managing cardiac arrest; however, enhancing survival rates remains a significant challenge. Recent advancements highlight the importance of integrating artificial intelligence (AI) to overcome existing prediction, intervention, and post-resuscitation care limitations.
Methods:
A thorough review of contemporary literature regarding AI applications in CPR was undertaken, explicitly examining its role in the early prediction of cardiac arrest, optimization of CPR quality, and enhancement of post-arrest outcomes. The analysis incorporated data from machine learning models, biosignal-responsive robotics, and advanced monitoring systems to showcase advancements and identify future challenges.
Results:
Innovations driven by AI have significantly transformed CPR practices across multiple areas. Predictive algorithms leveraging electronic health records and continuous electrocardiogram (ECG) monitoring facilitate the early identification of at-risk patients. Additionally, AI-enhanced feedback systems improve the accuracy of chest compressions and minimize variability in manual execution. Integrating AI with automated external defibrillators (AEDs) and real-time ECG analysis increases defibrillation precision and reduces interruptions during CPR. Emerging technologies, including wearable devices, immersive training simulators, and drone-delivered defibrillators, show considerable potential in addressing response time disparities during out-of-hospital cardiac arrests. Nevertheless, ethical considerations, particularly regarding data privacy and equitable access, pose significant challenges.
Conclusions:
Integrating AI into CPR practices can enhance prediction accuracy, procedural effectiveness, and survival rates. Addressing the ethical, legal, and technological barriers to successful implementation in clinical settings is crucial.
Keywords:
artificial intelligence
; cardiopulmonary resuscitation
; automated external defibrillators
; electrocardiogram
; defibrillators
; cardiac arrest
1. Introduction
Cardiac arrest (CA) is a significant global public health issue, leading to 15–20% of annual deaths and impacting 50–100 individuals per 100,000 people. Although emergency medicine has progressed, survival rates are still worryingly low, especially for out-of-hospital cardiac arrest (OHCA), which has an average survival rate of just 9%, in contrast to 18% for in-hospital cardiac arrest (IHCA). These unfavourable outcomes primarily result from delayed detection, inadequate cardiopulmonary resuscitation (CPR) initiation, and insufficient access to automated external defibrillators (AEDs). In the United States, over 290,000 IHCA cases arise each year, with survival rates varying from 0% to 36%, and only a limited number of these patients experience favourable neurological recovery [1,2]. Artificial intelligence (AI) innovations have transformed various healthcare sectors by facilitating early disease detection, tailored diagnostics, and immediate decision-making. Notably, AI applications in cardiac care have garnered considerable interest, especially in interpreting electrocardiograms (ECGs) and echocardiograms, where machine learning algorithms assist clinicians in pinpointing cardiac abnormalities with greater accuracy. Moreover, AI has shown promise in predicting cardiac arrests and dangerous arrhythmias through continuous ECG monitoring and evaluating post-arrest outcomes like neurological prognosis [1,3]. Incorporating AI into CPR protocols marks a significant change in cardiac arrest management by enabling real-time analysis of patient data, quicker identification of cardiac arrests, and improved CPR performance. AI-enhanced feedback devices help ensure compliance with evidence-based CPR standards by tracking essential parameters like compression depth, rate, and recoil while identifying rescuer fatigue to preserve CPR quality. Moreover, AI-fueled simulators and virtual reality (VR) training platforms offer engaging, high-fidelity learning experiences, boosting technical skills and increasing responder confidence [1,4].
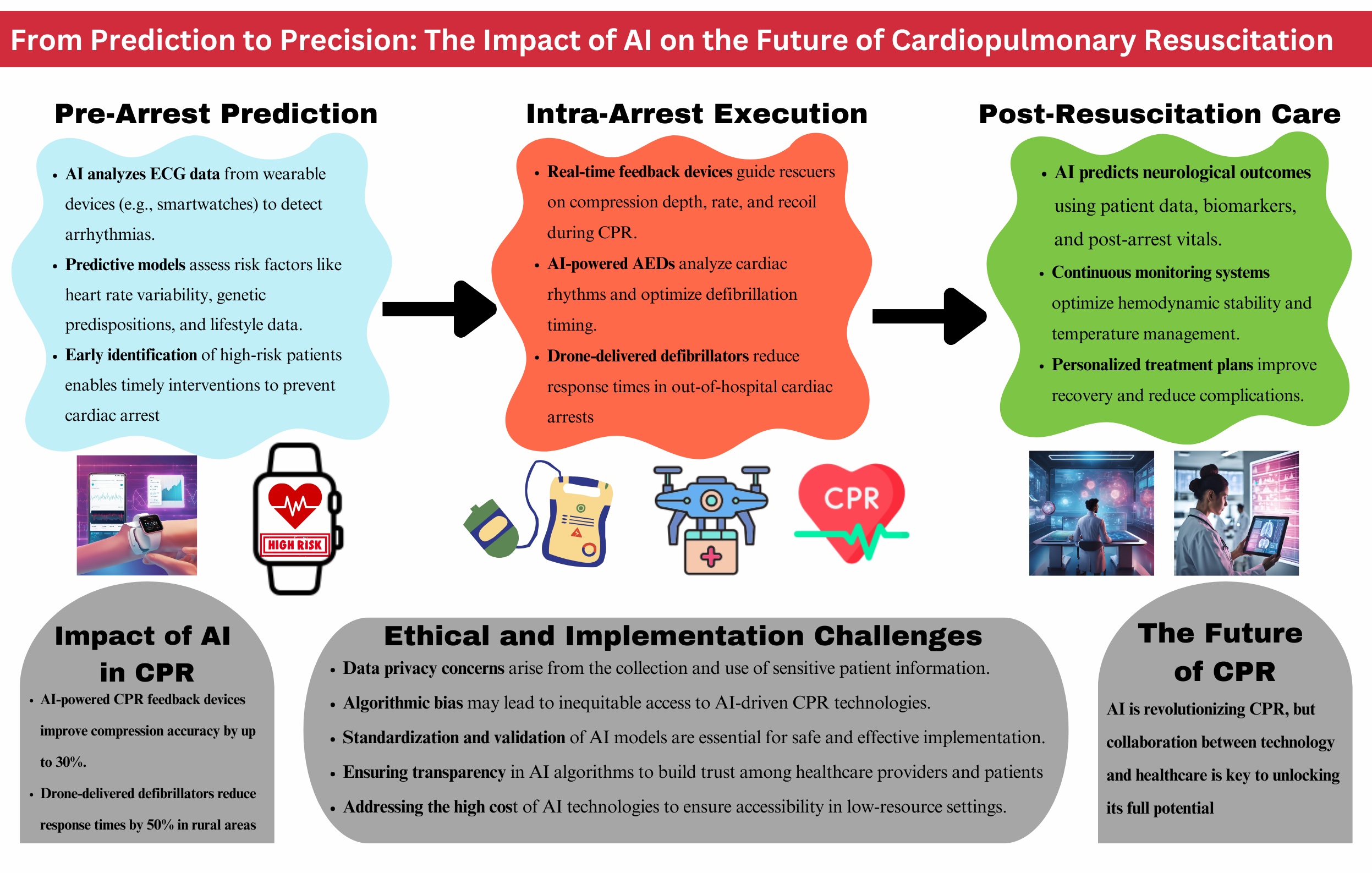
In addition to enhancing CPR techniques, AI innovations are revolutionizing public access to defibrillation and emergency response methods. Developments like AED tracking, connections with emergency medical services (EMS), and responder mobilization through smartphone apps have accelerated emergency responses and boosted survival rates. New technologies, such as drone-delivered AEDs and AI-assisted CPR coaching, highlight AI's capacity to address challenges in OHCA care [4,5]. Despite progress, Significant inequalities exist, especially in low-resource areas with restricted access to resuscitation technology. The International Liaison Committee on Resuscitation (ILCOR) and the Global Resuscitation Alliance (GRA) highlight the critical requirement for standardized guidelines, fair implementation strategies, and technological adjustments to address the disparities in cardiac arrest care [2]. This review analyzes the changing role of AI and new technologies in identifying cardiac arrest, enabling real-time responses, and improving CPR training, offering an in-depth look at their effects on survival rates. Examining the intersection of AI-driven automation and evidence-based resuscitation practices emphasizes the collaboration between technology and clinical expertise in transforming CPR methodologies. The results highlight that AI should be viewed not as a substitute but as a crucial enhancement to human judgment, defining the future of resuscitation research [1,3]. Figure 1 illustrates the integration of AI across the CPR continuum, from pre-arrest prediction to intra-arrest execution and post-resuscitation care, demonstrating its role in enhancing early risk detection, intervention precision, and patient outcomes.
2. Methods
This review explores the incorporation of AI in CPR by analyzing pertinent clinical studies and technological developments. Studies that did not provide clinical data or were restricted to theoretical models were omitted. Figure 2 illustrates the systematic framework detailing AI applications in CPR. Since this review relies solely on published literature, ethical approval is unnecessary.
2.1. Systematic Literature Search and Study Selection:
We extensively searched relevant articles through PubMed, EMBASE, and Google Scholar, concentrating on studies investigating AI use in CPR (Table 2). Our search encompassed systematic reviews, clinical trials, randomized controlled trials, and meta-analyses accessible on these platforms. We also pursued additional studies that met our inclusion criteria.
A collection of abstracts was assembled, and each was independently evaluated against our predefined criteria before inclusion. These criteria involved examining AI-driven interventions in CPR, analyzing their effects on clinical outcomes, and excluding studies that lacked empirical evidence or concentrated solely on theoretical frameworks.
2.2. Inclusion and Exclusion Criteria:
We organized specific criteria for including and excluding participants to achieve our study goals. Our Criteria are summarized in Table 1.
3. Results:
Initially, 265,152 records were found in various databases and registers. After eliminating duplicate records (n = 292) and studies that did not satisfy the inclusion criteria (n = 240,892), 23,968 records were available for screening. During the screening phase, 22,211 records were discarded after reviewing titles and abstracts, along with 1,041 case reports and editorial letters. This resulted in 716 full-text articles being evaluated for eligibility. Ultimately, 704 studies were excluded due to a lack of adequate information, leading to the inclusion of 12 studies in this review (Figure 2).
3.1. Pathophysiology, Risk Factors, and Triggers of Sudden Cardiac Arrest
Sudden Cardiac Arrest (SCA) is a critical medical emergency marked by an unexpected stop in heart function, resulting in immediate loss of consciousness and, without intervention, swiftly leading to death. The underlying mechanisms of SCA mainly involve a disturbance in the heart's electrical system, often initiated by sustained ventricular tachycardia or ventricular fibrillation [6]. These arrhythmias hinder the heart’s capacity to circulate blood effectively, causing systemic hypoperfusion, vital organ ischemia, and potentially life-threatening issues like sepsis, hypovolemic shock, or acute heart failure. Coronary heart disease (CHD) is the most prevalent cause of SCA, characterized by the gradual buildup of atherosclerotic plaques in the coronary arteries. When these plaques rupture, it can lead to myocardial infarction, which sets the stage for dangerous arrhythmias. Additional factors include various cardiomyopathies (such as hypertrophic, dilated, or arrhythmogenic), congenital heart defects, electrolyte disturbances, Long QT syndrome, and urgent medical situations like anaphylaxis, airway obstructions, electrical injuries, or adverse drug reactions [7,8]. SCA risk factors can be divided into two main categories: modifiable and non-modifiable. Modifiable factors encompass tobacco use, lack of physical activity, and unhealthy eating habits, all of which are significantly associated with conditions like hypertension, obesity, and diabetes.
In contrast, non-modifiable factors include older age, male gender, ethnicity, and genetic factors. Additionally, specific triggers can provoke SCA in those at risk, such as intense physical activity, excessive consumption of alcohol or caffeine, use of stimulants like cocaine or amphetamines, high levels of emotional stress, and infections, including influenza, which can lead to life-threatening arrhythmias [9]. Comprehending these mechanisms, risk factors, and triggers is crucial for creating effective preventive strategies, enhancing early diagnosis, and optimizing management techniques for SCA.
3.2. Current Strategies for Predicting Sudden Cardiac Death
Due to the unpredictable nature of SCA, significant efforts have been dedicated to enhancing risk prediction for sudden cardiac death (SCD). Conventional methods concentrate on heart rate variability (HRV), a well-established indicator of autonomic dysfunction. Diminished HRV, which is characterized by reduced variations in interbeat intervals, indicates an imbalance between sympathetic and parasympathetic activities, often seen in diseased hearts with increased resting heart rates. Various HRV metrics, such as the standard deviation of interbeat intervals and power spectral density, are linked to declining cardiovascular health and a heightened risk of SCD. Nevertheless, these associations are too inconsistent for dependable risk stratification, as they fail to consider the complexities of arrhythmic substrates. Genetic susceptibility is crucial in assessing the risk of sudden cardiac death. Mutations in potassium and sodium channel genes lead to prolonged action potentials and QT interval irregularities, increasing the risk for arrhythmias like premature ventricular contractions (PVCs), ventricular tachycardia (VT), and Torsades de Pointes. Moreover, mutations in calcium receptors can result in calcium overload, which is a factor in catecholaminergic polymorphic ventricular tachycardia (CPVT). These genetic risks are further augmented by electrocardiographic (ECG) abnormalities, including long QT syndrome (LQTS) and short QT syndrome (SQTS), both characterized by prolonged or shortened QT intervals. Given the shortcomings of individual predictive markers, contemporary strategies merge HRV metrics, genetic information, and ECG irregularities to enhance risk stratification. However, a more holistic approach is necessary, including electrophysiological mapping and machine learning models to improve predictive accuracy [10,11].
3.3. Historical Development and Advances in CPR
Despite progress in predicting and preventing risks, SCA still represents a significant cause of global fatalities, highlighting the need for improved resuscitation methods. The evolution of CPR reflects a shift from basic life-saving practices to rigorously standardized, evidence-based protocols, which have markedly enhanced survival rates in cardiac arrest situations. The roots of CPR can be traced back to essential techniques like manual chest compressions and rescue breathing. An early recognized method, mouth-to-mouth resuscitation, was validated by the Paris Academy of Sciences 1740 as effective for reviving those with respiratory failure. However, it was not until 1960 that the American Heart Association (AHA) established a coherent CPR approach that integrated mouth-to-mouth ventilation with external chest compressions. This pivotal development set the stage for contemporary CPR practices and enabled the broad implementation of standardized training for healthcare professionals and laypersons [12]. Implementing standardized CPR guidelines by organizations like the AHA and the ILCOR signifies a crucial shift towards an evidence-driven approach. A significant advancement in modern resuscitation science is introducing the "Chain of Survival," a systematic model highlighting the importance of early detection, quality CPR, swift defibrillation, and care following resuscitation. Over the years, the enhancement of Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS) protocols has resulted in more effective CPR methods, merging chest compressions, ventilation techniques, and defibrillation into a well-organized resuscitation strategy. The 2021 European Resuscitation Council (ERC) guidelines embody these improvements by emphasizing ease of use and accessibility and encouraging public participation to boost global survival rates [12,13]. Technological innovations have transformed CPR, merging manual resuscitation methods with automated, data-centric interventions. The arrival of AEDs has changed bystander-initiated CPR, enabling quicker and more effective defibrillation in out-of-hospital scenarios. Real-time feedback devices for CPR continuously monitor compression depth and rate, ensuring compliance with evidence-based guidelines. Additionally, smartphone apps and dispatcher-assisted CPR systems have greatly improved emergency response coordination, enhancing bystander intervention effectiveness. Beyond standard CPR, advanced resuscitation technologies like extracorporeal CPR (ECPR) and point-of-care ultrasound (POCUS) have broadened diagnostic and therapeutic options, especially for patients in refractory cardiac arrest. New technologies, such as drone-delivered AEDs and wearable biosensors, showcase how AI and automation are integrated into resuscitation, improving survival rates before and during hospital care [12,13]. As CPR evolves, integrating technology and standardized protocols will play a vital role in enhancing global cardiac arrest survival rates.
4. Recent Advancements in CPR
4.1. Mechanical CPR Devices
Mechanical CPR devices, such as AutoPulse and Lund University Cardiopulmonary Assist System (LUCAS), are designed to provide consistent, high-quality chest compressions during cardiac arrest. These devices aim to address issues found with manual CPR, like inconsistencies in compression quality and rescuer fatigue. Nevertheless, studies assessing their effectiveness and safety relative to manual CPR have produced varied outcomes. A Bayesian network meta-analysis involving 12,908 cardiac arrest patients indicated that manual CPR outperformed AutoPulse regarding survival rates at 30 days or hospital discharge (OR: 1.40, 95% CI: 1.09–1.94) and neurological recovery (OR: 1.51, 95% CI: 1.06–2.39). However, no noteworthy differences were found in survival or neurological outcomes between manual CPR and LUCAS or between LUCAS and AutoPulse. Moreover, manual CPR was linked to fewer complications, showing a reduced risk of pneumothorax (OR: 0.56) and hematoma formation (OR: 0.15) compared to AutoPulse. At the same time, LUCAS had a decreased risk of hematoma formation compared to AutoPulse (OR: 0.07) [14]. A comprehensive umbrella review that assessed systematic reviews and additional data further confirmed that mechanical CPR devices do not consistently outperform manual CPR regarding return of spontaneous circulation (ROSC), survival to hospital admission, or survival to discharge.
However, mechanical devices might offer advantages in specific situations, such as prolonged resuscitation efforts or circumstances where manual CPR is impractical [15]. A meta-analysis of 24 studies with 111,681 cardiac arrest patients supported these findings, showing no statistically significant differences between mechanical and manual CPR in ROSC, short-term survival, or hospital discharge survival rates. However, manual CPR substantially improved post-resuscitation neurological outcomes (OR: 1.41, 95% CI: 1.07–1.84, P = 0.01). This indicates that manual compressions may benefit long-term neurological recovery even though mechanical CPR provides consistency [16]. While mechanical CPR devices lessen rescuer exhaustion and ensure continuous compressions, various challenges impede their widespread use. Deployment delays may disrupt CPR, risking patient outcomes and postponing crucial procedures like defibrillation.
Additionally, the likelihood of device-related complications, including rib fractures and internal injuries, has been noted, especially when compared to manual CPR [14]. The significant financial investment and specialized training needed for mechanical CPR devices further restrict their accessibility, especially in resource-limited settings. Moreover, differences in study methodologies, patient populations, and device protocols have led to inconsistent findings, hindering the establishment of clear clinical guidelines for optimal use [15]. Additional innovations and carefully designed clinical trials are crucial for thoroughly assessing the impact of mechanical CPR on cardiac arrest management and formulating evidence-based guidelines for its application [16].
4.2. Extracorporeal Cardiopulmonary Resuscitation (ECPR)
Extracorporeal cardiopulmonary resuscitation (ECPR) employs extracorporeal membrane oxygenation (ECMO) during cardiac arrest as a sophisticated method designed to restore circulation in patients experiencing refractory cardiac arrest when standard CPR falls short. By reinstating blood flow to essential organs before the ROSC, ECPR aims to enhance survival and neurological outcomes. Research indicates that ECPR boosts survival rates and functional recovery, mainly within well-coordinated healthcare systems, facilitating stabilization while addressing reversible factors contributing to cardiac arrest [17]. Randomized controlled trials have powerfully demonstrated the advantages of ECPR in cases of OHCA. A pivotal study that assessed early ECMO-assisted resuscitation against standard ACLS revealed a much higher survival rate of hospital discharge for the ECPR group (43%) versus the standard ACLS group (7%). This significant difference resulted in the early termination of the trial because of ECMO's apparent superiority [18]. A meta-analysis of randomized controlled trials further supported the role of ECPR, reporting significantly higher survival rates and better neurological outcomes, particularly in patients with shockable initial rhythms [19]. Patient selection is a critical factor in ECPR success, influenced by several determinants. Poor prognostic indicators include advanced age (over 65 years), prolonged low-flow times exceeding 40 minutes, non-shockable rhythms, and pre-existing life-limiting comorbidities, all of which are linked to higher mortality rates [20]. ECPR demonstrates the potential for hospital discharge survival in about 33.8% of instances. Still, complications like hemorrhage, renal failure, and neurological injury are common, highlighting the need for thorough risk assessment [21]. Oxygen management plays a vital role in ECPR, as too much oxygen can result in harmful effects. Patients undergoing ECPR experience extreme hyperoxia (PaO2 ≥300 mmHg) significantly more often than those undergoing conventional CPR, with a corresponding 2.52-fold rise in 30-day mortality. This underscores the importance of careful oxygen regulation [22]. Furthermore, incorporating percutaneous coronary intervention (PCI) during ECPR has been shown to enhance outcomes, mainly when cardiac arrest is caused by coronary artery disease, since it enables prompt revascularization [22]. While ECPR offers various benefits, it also poses logistical hurdles and demands significant healthcare resources. To implement it effectively, coordinated systems must enable swift ECMO deployment, highly trained staff, and strong post-resuscitation support. Research indicates that starting ECMO early is vital for securing positive outcomes, with survival rates ranging from 15% to 50%, contingent on patient selection and the clinical environment [23]. These findings collectively show that ECPR can significantly enhance survival and neurological outcomes in carefully chosen patients experiencing refractory cardiac arrest, especially when part of well-coordinated resuscitation efforts. Nonetheless, its effectiveness depends on the proper patient selection, prompt initiation, and efficient management of oxygen and complications.
4.3. Feedback Mechanisms
Incorporating real-time feedback mechanisms into CPR training and clinical practice has greatly enhanced the quality and effectiveness of resuscitation efforts. Feedback devices offer continuous monitoring and corrective guidance on essential CPR metrics such as chest compression depth, rate, recoil, and ventilation performance. Numerous studies have examined the effectiveness of these devices across various populations, evaluating their influence on CPR quality, rescuer fatigue, and overall survival rates. Real-time feedback has improved CPR performance, especially regarding compression accuracy and ventilation quality. In a pediatric resuscitation simulation study, feedback devices boosted chest compression and ventilation performance; however, they also shifted the rescuer’s visual attention from the patient to the device, thereby increasing cognitive workload [24]. Similarly, paramedics using feedback devices observed greater adherence to recommended compression depth and rate than those performing standard CPR [25]. Integrating real-time visual feedback in CPR training for laypersons led to enhanced compression depth, full chest recoil, and better hand positioning, highlighting the importance of feedback-supported training in BLS courses [26]. Feedback mechanisms are essential for enhancing CPR performance in professional rescuers. Medical personnel often find it challenging to sustain the proper anatomical compression position, and feedback devices have proven effective in improving accuracy in positioning [27]. In simulated drowning rescues, lifeguards using the CPRMeter achieved notably better compression scores, highlighting the effectiveness of feedback in performance-intensive situations [28]. Moreover, feedback systems effectively uphold high-quality compressions over time and mitigate the decline in compression efficacy caused by fatigue, thus ensuring consistent CPR performance throughout extended resuscitation efforts [29].
Feedback devices influence not just training and simulation but also actual clinical resuscitations. Patients who received CPR using the Cardio First Angel™ feedback device experienced higher rates of ROSC and fewer rib fractures than those who received standard manual CPR [30]. Feedback devices have demonstrated their ability to enhance the ergonomic elements of CPR delivery. They help rescuers maintain steadier force output throughout extended compressions, which lowers physical strain and ensures the quality of compressions remains consistent [31]. In an emergency department, combining real-time feedback with post-event debriefing led to marked enhancements in compression depth and a higher percentage of compressions aligning with guideline recommendations [32]. Despite their demonstrated benefits, feedback mechanisms come with limitations. While they improve the quality of CPR, an increased cognitive burden has been noted, as rescuers may divert attention from patient monitoring to the feedback device, potentially compromising situational awareness in high-stress environments [24]. Additionally, the effectiveness of feedback-assisted CPR relies on the user's ability to interpret and apply the provided guidance, which requires adequate training in device usage [25]. The variation in feedback device designs and features further emphasizes the need for standardization and optimization to ensure smooth integration into various resuscitation settings [26].
5. Technological Innovations in CPR
Incorporating AI into CPR revolutionizes training and real-time resuscitation by increasing accuracy, effectiveness, and decision-making capabilities. AI-driven systems enhance various aspects of resuscitation, such as training simulations, ongoing performance assessment, cardiac arrest prediction, CPR automation, and follow-up care, leading to better survival rates. Machine learning (ML) and deep learning techniques are used more frequently to monitor compression quality, manage airways, assist dispatchers in CPR, and interpret physiological data, ensuring more dependable interventions. These technological innovations have demonstrated encouraging results in boosting compliance with CPR guidelines, reducing human errors, and enhancing resuscitation outcomes [33]. AI-powered CPR training has shown notable enhancements in accuracy by pinpointing frequent mistakes, such as improper compression depth, rate, hand placement, and ventilation methods. Feedback systems driven by machine learning offer real-time corrective advice, enabling rescuers to improve their techniques continuously. Sophisticated CPR trainers and VR simulation platforms provide engaging environments where healthcare professionals and laypeople can practice effective CPR with interactive, AI-supported guidance [34]. AI-powered multimodal training systems integrating motion tracking, electromyography (EMG), and AR have significantly enhanced compression precision and compliance with resuscitation protocols [35]. Neural network-based error detection models integrated into training manikins can independently identify and correct technique deficiencies without human instructors, enhancing training efficiency [36]. In addition to training, AI is essential for executing CPR in real time, guaranteeing high-quality chest compressions and effective ventilation (Figure 3). AI-powered airway monitoring models prevent misalignment during ventilation, enhancing oxygenation and minimizing human errors. Deep learning systems have reached nearly flawless accuracy in airway assessment, facilitating real-time adjustments in airway management [37]. AI-assisted CPR robots are engineered to provide mechanically optimized compressions, showcasing hemodynamic stability like traditional mechanical CPR devices (Figure 3). These autonomous systems adjust compression depth and rate dynamically based on real-time physiological feedback, offering a potential alternative to manual CPR [38]. AI-powered predictive models enhance the recognition and response to cardiac arrest by evaluating real-time physiological data from wearable sensors and electrocardiogram (ECG) readings. These models facilitate the early detection of cardiac arrest risk, aiding pre-hospital emergency response teams. AI-augmented ECG analysis demonstrates increased accuracy in identifying shockable rhythms, minimizing interruptions during CPR, and boosting defibrillation effectiveness [39]. Predictive analytics utilizing patient data have been created to evaluate the risk of SCA, facilitating early interventions and enhancing survival chances [40]. Additionally, deep learning-enhanced ultrasound imaging is now used to detect ROSC, minimize the need for manual pulse checks, and guarantee uninterrupted compressions [41]. AI-driven decision support systems have significantly improved dispatcher-assisted CPR (DA-CPR) by offering real-time coaching for bystanders. These AI-powered emergency dispatch platforms deliver step-by-step instructions to ensure correct compression techniques, enhancing survival rates in OHCA situations [1]. Neural networks integrated into survival prediction models help healthcare providers evaluate the chances of resuscitation success, aiding in clinical decision-making and end-of-life discussions [42]. Automated CPR monitoring systems assist emergency responders by ensuring adherence to CPR guidelines and notifying rescuers if quality decreases [33]. Combining AI with AEDs, the Internet of Medical Things (IoMT), and robotic CPR systems further improves emergency response capabilities (Figure 3). AI-assisted AEDs can independently assess cardiac rhythms, suggest shocks, and enhance defibrillation timing, minimizing delays and human error. AI-driven drones for AED deployment are being investigated as a method to swiftly supply defibrillators in remote or busy locations, greatly decreasing the time to defibrillation [33]. Wearable biosensors integrated with machine learning algorithms constantly assess cardiovascular function and CPR performance, delivering immediate feedback for tailored CPR enhancement [43]. The future of AI in CPR is anticipated to enhance automation, clinical decision support, and emergency response coordination. Autonomous resuscitation robots powered by AI, AEDs using deep learning, and tools for real-time physiological monitoring could transform cardiac arrest management by delivering consistent, high-quality interventions with limited human involvement. AI-based forecasting models are expected to boost survival rates by fine-tuning response protocols and offering personalized treatment plans. As AI becomes more embedded in healthcare, advancements in machine learning for resuscitation planning, automated defibrillation systems, and real-time dispatcher-integrated assistance will likely influence future cardiac arrest management guidelines [5]. Although AI holds transformative potential, its adoption in CPR faces challenges concerning ethical considerations, patient data privacy, and regulatory oversight (Figure 4). Key challenges to widespread adoption include bias in AI algorithms, interoperability issues, and the necessity for large-scale clinical trial validation. The effectiveness of AI-assisted CPR relies on its smooth integration into health systems, thorough validation processes, and continuous improvement of predictive algorithms to boost reliability and precision [36].
6. AI in Post-Cardiac Arrest Care
AI is transforming cardiac arrest care by improving prognostication, hemodynamic monitoring, automating ICU workflows, and enhancing ethical decision-making. Predictive AI-driven models enable more precise risk assessments, optimize resuscitation strategies, and lessen clinical workloads. Incorporating AI into post-resuscitation care facilitates timely interventions, boosts survival rates, and allows personalized treatment plans. AI-based prognostic models have greatly enhanced the ability to predict neurological outcomes and mortality following cardiac arrest. Machine learning algorithms that utilize real-time physiological data, patient histories, and post-resuscitation biomarkers show significantly greater accuracy than traditional scoring systems. Enhanced versions of the Cardiac Arrest Survival Post-Resuscitation In-hospital (CASPRI) score, developed with artificial neural networks (ANN), offer improved sensitivity and specificity in forecasting neurological recovery.
Additionally, ChatGPT-4-driven models have achieved performance levels comparable to established prognostic tools in predicting long-term survival and functional outcomes, thereby assisting clinicians with risk stratification and decisions regarding withdrawal of care [44,45,46,47]. Beyond prognostication, AI plays an essential role in real-time physiological monitoring. The integration of the AI-driven Hypotension Prediction Index (HPI) into Enhanced Recovery After Surgery (ERAS) protocols has proven effective in optimizing blood pressure stabilization and reducing the length of stay in intensive care units (ICUs). Additionally, AI-assisted targeted temperature management (TTM) facilitates patient-specific cooling and rewarming strategies, which have been shown to improve neurological outcomes following cardiac arrest. Moreover, AI-enhanced continuous ECG and hemodynamic monitoring enables the early detection of secondary cardiac arrest risks, thereby reducing recurrence rates and hospital readmissions [45,48,49]. In ICU environments, AI-driven workflow automation has significantly enhanced operational efficiency by providing real-time clinical decision support. These AI models continuously analyze multimodal patient data, facilitating automated ventilator adjustments, fluid resuscitation guidance, and early sepsis detection. Such advancements improve patient stabilization and alleviate the cognitive burden on clinicians, ensuring timely and precise interventions [46]. AI's ethical and socioeconomic implications in post-arrest care present opportunities and challenges. AI-driven disparity analysis has revealed significant racial and economic inequities in access to life-saving interventions for cardiac arrest patients, particularly those with cancer.
Additionally, AI-based cost-effectiveness models indicate that equitable resource distribution and expanded access to post-arrest interventions could improve patient outcomes while reducing healthcare costs [47]. AI is transforming post-cardiac arrest management by delivering precise, data-informed, and personalized treatment strategies to improve prognostication, optimize ICU efficiency, and address disparities in equitable care. However, to ensure their safe and effective integration into clinical practice, it is essential to tackle challenges related to clinical validation, ethical implementation, and the interpretability of AI models.
Institutional review board approval and ethics committee clearance
Not required.
Conflicts of Interest
None.
References
- Bednarz K, Goniewicz K, Al-Wathinani AM, Goniewicz M. Emergency Medicine Perspectives: The Importance of Bystanders and Their Impact on On-Site Resuscitation Measures and Immediate Outcomes of Out-of-Hospital Cardiac Arrest. JCM. 2023 Oct 28;12(21):6815.
- Zheng W, Zheng J, Wang C, Pan C, Zhang J, Liu R, et al. The development history, current state, challenges, and future directions of the BASIC-OHCA registry in China: A narrative review. Resusc Plus. 2024 Jun;18:100588.
- Kumari S, Kumari A, Asim R, Khan R. Multi-faceted role of artificial intelligence (AI) in cardiopulmonary resuscitation (CPR): a narrative review. AI Ethics [Internet]. 2024 Dec 5 [cited 2025 Feb 12]; Available from: https://link.springer.com/10. 1007.
- Levitt CV, Boone K, Tran QK, Pourmand A. Application of Technology in Cardiopulmonary Resuscitation, a Narrative Review. JCM. 2023 Nov 29;12(23):7383.
- Semeraro F, Schnaubelt S, Malta Hansen C, Bignami EG, Piazza O, Monsieurs KG. Cardiac arrest and cardiopulmonary resuscitation in the next decade: Predicting and shaping the impact of technological innovations. Resuscitation. 2024 Jul;200:110250.
- Waldmann V, Jouven X, Narayanan K, Piot O, Chugh SS, Albert CM, et al. Association Between Atrial Fibrillation and Sudden Cardiac Death: Pathophysiological and Epidemiological Insights. Circulation Research. 2020 Jul 3;127(2):301–9.
- Arzamendi D, Benito B, Tizon-Marcos H, Flores J, Tanguay JF, Ly H, et al. Increase in sudden death from coronary artery disease in young adults. American Heart Journal. 2011 Mar;161(3):574–80.
- Yang KC, Kyle JW, Makielski JC, Dudley SC. Mechanisms of Sudden Cardiac Death: Oxidants and Metabolism. Circulation Research. 2015 Jun 5;116(12):1937–55.
- Adabag AS, Luepker RV, Roger VL, Gersh BJ. Sudden cardiac death: epidemiology and risk factors. Nat Rev Cardiol. 2010 Apr;7(4):216–25.
- Kirchhof P, Breithardt G, Eckardt L. Primary prevention of sudden cardiac death. Heart. 2006 Dec 1;92(12):1873–8.
- Lerma C, Glass L. Predicting the risk of sudden cardiac death. The Journal of Physiology. 2016 May;594(9):2445–58.
- Perkins GD, Gräsner JT, Semeraro F, Olasveengen T, Soar J, Lott C, et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation. 2021 Apr;161:1–60.
- Kapoor, MC. The History and Evolution of Cardiopulmonary Resuscitation. Journal of Resuscitation. 2024 Dec;1(1):3.
- Khan SU, Lone AN, Talluri S, Khan MZ, Khan MU, Kaluski E. Efficacy and safety of mechanical versus manual compression in cardiac arrest – A Bayesian network meta-analysis. Resuscitation. 2018 Sep;130:182–8.
- El-Menyar A, Naduvilekandy M, Rizoli S, Di Somma S, Cander B, Galwankar S, et al. Mechanical versus manual cardiopulmonary resuscitation (CPR): an umbrella review of contemporary systematic reviews and more. Crit Care. 2024 Jul 30;28(1):259.
- Larik MO, Ahmed A, Shiraz MI, Shiraz SA, Anjum MU, Bhattarai P. Comparison of manual chest compression versus mechanical chest compression for out-of-hospital cardiac arrest: A systematic review and meta-analysis. Medicine. 2024 Feb 23;103(8):e37294.
- Abrams D, MacLaren G, Lorusso R, Price S, Yannopoulos D, Vercaemst L, et al. Extracorporeal cardiopulmonary resuscitation in adults: evidence and implications. Intensive Care Med. 2022 Jan;48(1):1–15.
- Yannopoulos D, Bartos J, Raveendran G, Walser E, Connett J, Murray TA, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. The Lancet. 2020 Dec;396(10265):1807–16.
- Scquizzato T, Bonaccorso A, Swol J, Gamberini L, Scandroglio AM, Landoni G, et al. Refractory out-of-hospital cardiac arrest and extracorporeal cardiopulmonary resuscitation: A meta-analysis of randomized trials. Artificial Organs. 2023 May;47(5):806–16.
- Hashem A, Mohamed MS, Alabdullah K, Elkhapery A, Khalouf A, Saadi S, et al. Predictors of Mortality in Patients With Refractory Cardiac Arrest Supported With VA-ECMO: A Systematic Review and a Meta-Analysis. Current Problems in Cardiology. 2023 Jun;48(6):101658.
- Dalia AA, Lu SY, Villavicencio M, D’Alessandro D, Shelton K, Cudemus G, et al. Extracorporeal Cardiopulmonary Resuscitation: Outcomes and Complications at a Quaternary Referral Center. Journal of Cardiothoracic and Vascular Anesthesia. 2020 May;34(5):1191–4.
- Stoll SE, Paul E, Pilcher D, Udy A, Burrell A. Hyperoxia and mortality in conventional versus extracorporeal cardiopulmonary resuscitation. Journal of Critical Care. 2022 Jun;69:154001.
- Richardson A (Sacha) C, Tonna JE, Nanjayya V, Nixon P, Abrams DC, Raman L, et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. ASAIO Journal. 2021 Mar;67(3):221–8.
- Wagner M, Gröpel P, Eibensteiner F, Kessler L, Bibl K, Gross IT, et al. Visual attention during pediatric resuscitation with feedback devices: a randomized simulation study. Pediatr Res. 2022 Jun;91(7):1762–8.
- Jaskuła J, Stolarz-Skrzypek K, Jaros K, Wordliczek J, Cebula G, Kloch M. Improvement in chest compression quality performed by paramedics and evaluated with a real-time feedback device: Randomized trial. Kardiol Pol. 2023 Feb 28;81(2):177–9.
- Baldi E, Cornara S, Contri E, Epis F, Fina D, Zelaschi B, et al. Real-time visual feedback during training improves laypersons’ CPR quality: a randomized controlled manikin study. CJEM. 2017 Nov;19(06):480–7.
- Koyama Y, Matsuyama T, Kaino T, Hoshino T, Nakao J, Shimojo N, et al. Adequacy of compression positioning using the feedback device during chest compressions by medical staff in a simulation study. BMC Emerg Med. 2022 Dec;22(1):76.
- Iskrzycki L, Smereka J, Rodriguez-Nunez A, Barcala Furelos R, Abelarias Gomez C, Kaminska H, et al. The impact of the use of a CPRMeter monitor on quality of chest compressions: a prospective randomised trial, cross-simulation. Kardiol Pol. 2018 Mar 16;76(3):574–9.
- Wu C, You J, Liu S, Ying L, Gao Y, Li Y, et al. Effect of a feedback system on the quality of 2-minute chest compression-only cardiopulmonary resuscitation: a randomised crossover simulation study. J Int Med Res. 2020 Apr;48(4):0300060519894440.
- Vahedian-Azimi A, Hajiesmaeili M, Amirsavadkouhi A, Jamaati H, Izadi M, Madani SJ, et al. Effect of the Cardio First AngelTM device on CPR indices: a randomized controlled clinical trial. Crit Care. 2016 Dec;20(1):147.
- Kopacz K, Fronczek-Wojciechowska M, Jaźwińska A, Padula G, Nowak D, Gaszyński T. Influenece of the CPRmeter on angular position of elbows and generated forces during cardiopulmonary resuscitation. Int J Occup Med Environ Health [Internet]. 2017 Jul 6 [cited 2025 Feb 12]; Available from: http://www.journalssystem.com/ijomeh/Influenece-of-the-CPRmeter-on-angular-position-of-elbows-and-generated-forces-during-cardiopulmonary-resuscitation-,6 6857, 0, 2html.
- Crowe C, Bobrow BJ, Vadeboncoeur TF, Dameff C, Stolz U, Silver A, et al. Measuring and improving cardiopulmonary resuscitation quality inside the emergency department. Resuscitation. 2015 Aug;93:8–13.
- Viderman D, Abdildin Y, Batkuldinova K, Badenes R, Bilotta F. Artificial Intelligence in Resuscitation: A Scoping Review. JCM. 2023 Mar 14;12(6):2254.
- Ecker H, Adams NB, Schmitz M, Wetsch WA. Feasibility of real-time compression frequency and compression depth assessment in CPR using a “machine-learning” artificial intelligence tool. Resuscitation Plus. 2024 Dec;20:100825.
- Di Mitri D, Schneider J, Trebing K, Sopka S, Specht M, Drachsler H. Real-Time Multimodal Feedback with the CPR Tutor. In: Bittencourt II, Cukurova M, Muldner K, Luckin R, Millán E, editors. Artificial Intelligence in Education [Internet]. Cham: Springer International Publishing; 2020 [cited 2025 Feb 12]. p. 141–52. (Lecture Notes in Computer Science; vol. 12163). Available from: http://link.springer.com/10. 1007.
- Di Mitri D, Schneider J, Specht M, Drachsler H. Detecting Mistakes in CPR Training with Multimodal Data and Neural Networks. Sensors. 2019 Jul 13;19(14):3099.
- Marhamati M, Dorry B, Imannezhad S, Hussain MA, Neshat AA, Kalmishi A, et al. Patient’s airway monitoring during cardiopulmonary resuscitation using deep networks. Medical Engineering & Physics. 2024 Jul;129:104179.
- Kim T, Suh GJ, Kim KS, Kim H, Park H, Kwon WY, et al. Development of artificial intelligence-driven biosignal-sensitive cardiopulmonary resuscitation robot. Resuscitation. 2024 Sep;202:110354.
- Ahn S, Jung S, Park JH, Cho H, Moon S, Lee S. Artificial intelligence for predicting shockable rhythm during cardiopulmonary resuscitation: In-hospital setting. Resuscitation. 2024 Sep;202:110325.
- Aqel S, Syaj S, Al-Bzour A, Abuzanouneh F, Al-Bzour N, Ahmad J. Artificial Intelligence and Machine Learning Applications in Sudden Cardiac Arrest Prediction and Management: A Comprehensive Review. Curr Cardiol Rep. 2023 Nov;25(11):1391–6.
- Park S, Yoon H, Yeon Kang S, Joon Jo I, Heo S, Chang H, et al. Artificial intelligence-based evaluation of carotid artery compressibility via point-of-care ultrasound in determining the return of spontaneous circulation during cardiopulmonary resuscitation. Resuscitation. 2024 Sep;202:110302.
- Ebell, MH. Artificial neural networks for predicting failure to survive following in-hospital cardiopulmonary resuscitation. J Fam Pract. 1993 Mar;36(3):297–303.
- Yammouri G, Ait Lahcen A. AI-Reinforced Wearable Sensors and Intelligent Point-of-Care Tests. JPM. 2024 Nov 1;14(11):1088.
- Johnsson J, Björnsson O, Andersson P, Jakobsson A, Cronberg T, Lilja G, et al. Artificial neural networks improve early outcome prediction and risk classification in out-of-hospital cardiac arrest patients admitted to intensive care. Crit Care. 2020 Dec;24(1):474.
- Amacher SA, Arpagaus A, Sahmer C, Becker C, Gross S, Urben T, et al. Prediction of outcomes after cardiac arrest by a generative artificial intelligence model. Resuscitation Plus. 2024 Jun;18:100587.
- Okada Y, Mertens M, Liu N, Lam SSW, Ong MEH. AI and machine learning in resuscitation: Ongoing research, new concepts, and key challenges. Resuscitation Plus. 2023 Sep;15:100435.
- Khawar MM, Abdus Saboor H, Eric R, Arain NR, Bano S, Mohamed Abaker MB, et al. Role of artificial intelligence in predicting neurological outcomes in postcardiac resuscitation. Annals of Medicine & Surgery. 2024 Dec;86(12):7202–11.
- Reddy VS, Stout DM, Fletcher R, Barksdale A, Parikshak M, Johns C, et al. Advanced artificial intelligence–guided hemodynamic management within cardiac enhanced recovery after surgery pathways: A multi-institution review. JTCVS Open. 2023 Dec;16:480–9.
- Nedadur R, Bhatt N, Liu T, Chu MWA, McCarthy PM, Kline A. The Emerging and Important Role of Artificial Intelligence in Cardiac Surgery. Canadian Journal of Cardiology. 2024 Oct;40(10):1865–79.
Figure 1.
Graphical abstract illustrating artificial intelligence's impact on cardiopulmonary resuscitation's future.
Figure 1.
Graphical abstract illustrating artificial intelligence's impact on cardiopulmonary resuscitation's future.
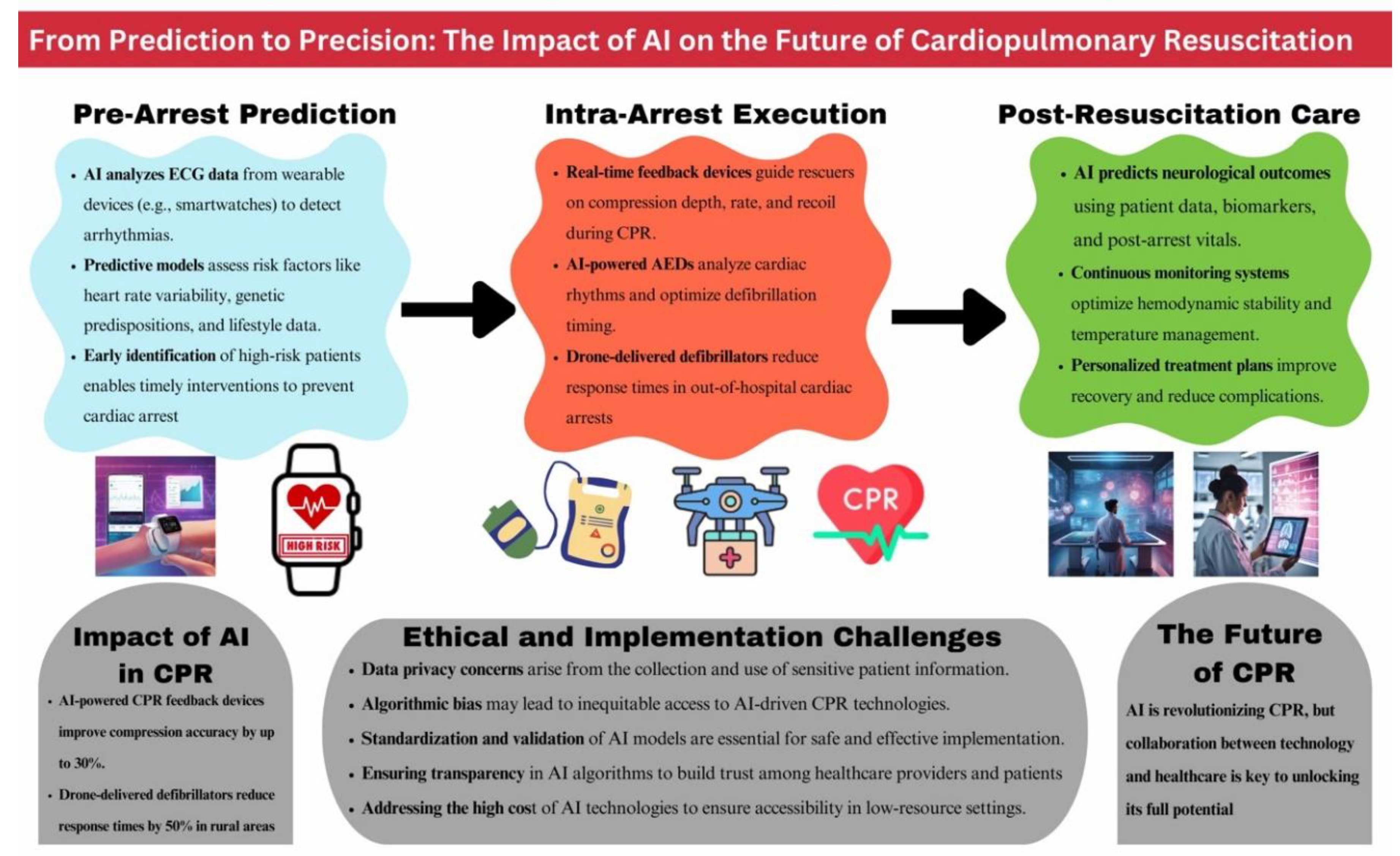
Figure 2.
PRISMA Flow Diagram of the Studies included in the review.
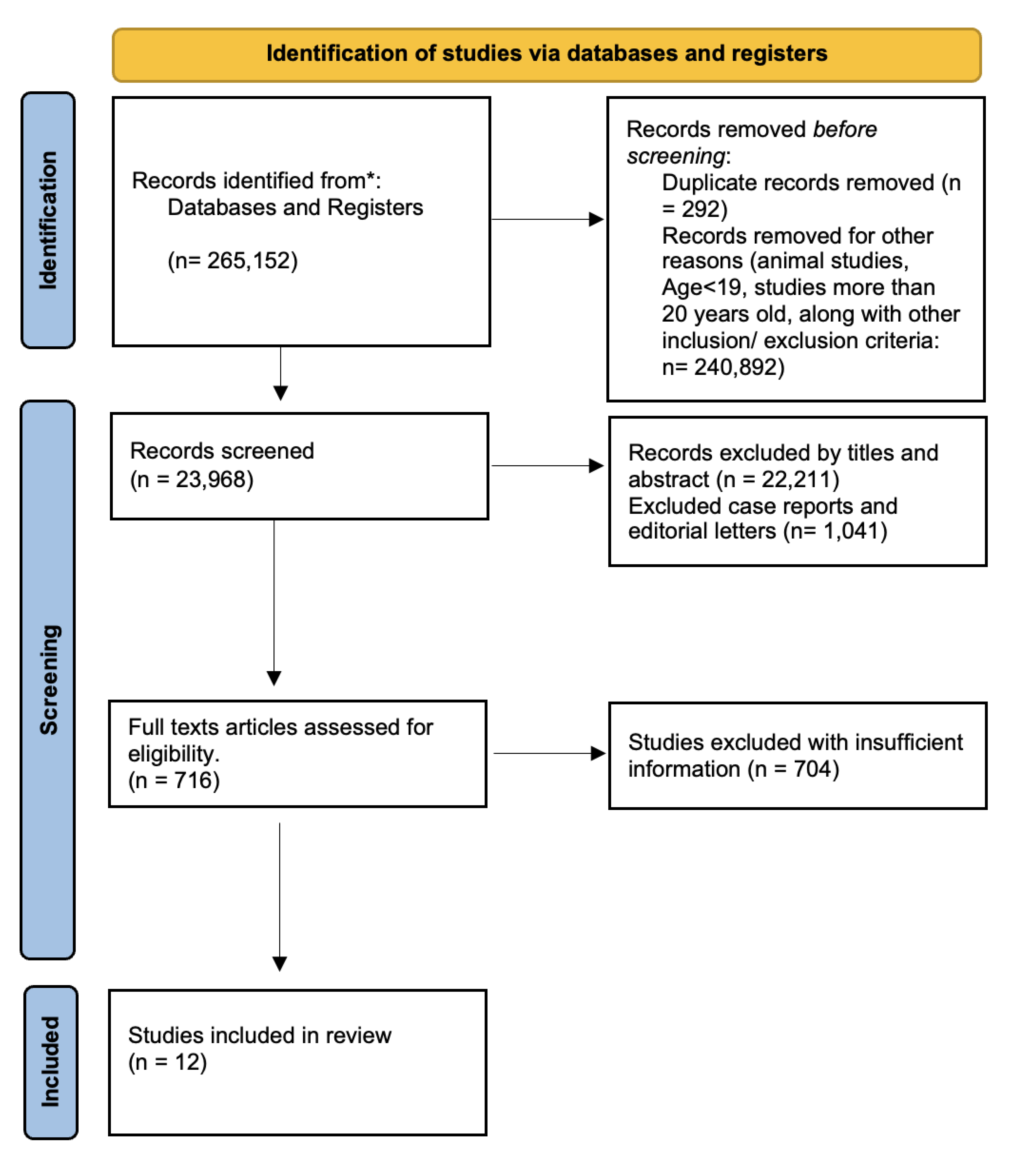
Figure 3.
Innovative Uses of AI in CPR Enhancement.

Figure 4.
Ethical & Implementation Challenges in AI-Driven Resuscitation.
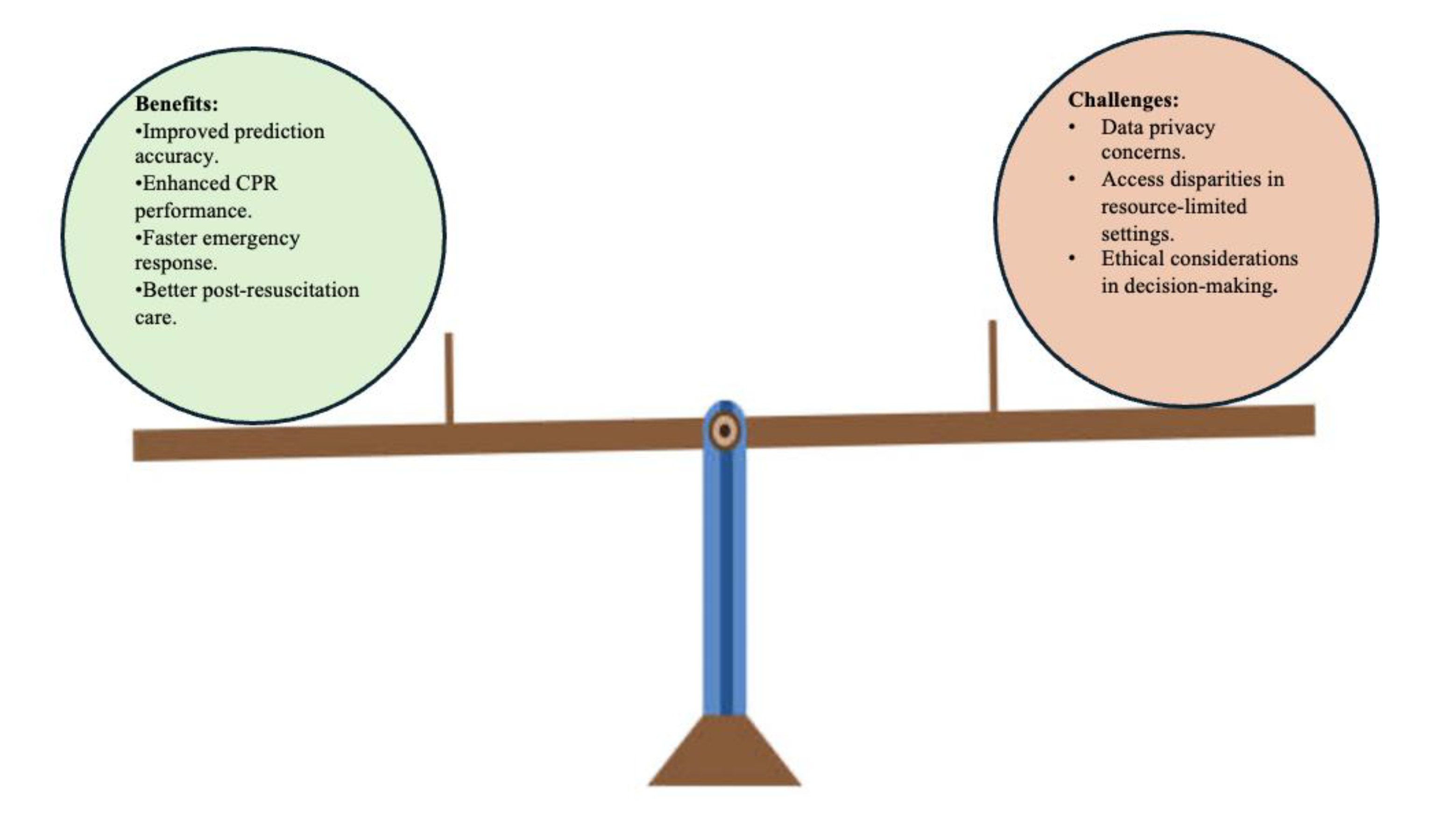

Table 1.
Inclusion and Exclusion criteria adopted during the search process.
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
|
b) Non-English text |
|
c) Animal studies |
|
d) Age: below 19 years of age |
|
e) Paid studies and studies that are not free full - text |
| f)Free full papers |
Table 2.
Shows the search strategy, the search engines used, and the number of results.
| Database | Search strategy | Search results |
|---|---|---|
|
PubMed/ EMBASE: |
|
22,808 |
| Google scholar: |
|
1,160 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



