Submitted:
22 February 2025
Posted:
25 February 2025
You are already at the latest version
Abstract
With the intensification of population aging, the number of elderly cancer patients has increased dramatically in recent years. However, the treatment of aged cancer patients, particularly those who are not eligible for surgery, is still a challenge. Thus, in this study, we retrospectively summarized and analyzed the clinical effects of radiotherapy in 43 late-line patients with advanced bladder cancer, with an average age of 77.3 ± 5.1 years. All patients were pathologically diagnosed with transitional epithelial carcinoma of the bladder, persistent bleeding, no condition for surgery, and were not suitable for chemotherapy. After thorough communication, all patients were treated with radiotherapy. As a result, the degree of bleeding gradually decreased after 5 rounds of 10Gy radiotherapy. After 15 rounds of 30Gy radiotherapy, the gross hematuria disappeared, and the success rate of radiotherapy in preventing bleeding reached 100%. At the end of follow-up, 24 patients passed away, and 19 patients were alive. The median survival time (OS) was 14 months. Statistical analysis revealed that the survival time of patients significantly differed between radical and palliative radiotherapy. The survival time of patients with advanced cancer is usually less than 3 months in the clinic, whereas the OS of patients (14 months) in this study far exceeded that reported previously. Therefore, radiotherapy can not only stop bleeding and relieve symptoms but also prolong patient survival time, offering an option for elderly patients with advanced bladder cancer to control tumor progression and improve quality of life.
Keywords:
advanced bladder cancer
; late-line treatment
; radiotherapy
; hematuria
; survival time
1. Introduction
Bladder cancer is a common malignant tumor that occurs in the bladder mucosal epithelium; it is also the second most common malignant tumor in the urinary system, and its annual incidence rate is increasing annually [1,2]. The incidence rate of bladder cancer ranks 9th among malignant tumors worldwide [3,4,5]; among men, it ranks 7th (9.5 patients per 100,000 people), and among women, it ranks 10th (approximately 2.4 patients per 100,000 people). The mortality rate of bladder cancer ranks 13th among malignant tumors, and the mortality rate of men (3.2/100,000) is higher than that of women (0.9/100,000). Moreover, regional, racial and sex differences exist in bladder cancer. According to data released by the China Cancer Registration Center in 2019, in 2015, the incidence rate of bladder cancer in China ranked 13th among malignant tumors (5.80/100,000), and the incidence rates of men ranked 7th (8.83/100,000) and women ranked 17th (2.61/100,000); the total mortality rate ranked 13th (2.37/100,000), that of men ranked 11th (3.56/100,000), and that of women was 16th (1.11/100,000) [6].
The treatment of curable bladder cancer involves different methods depending on whether the tumor has invaded the bladder muscle layer [7]. The main surgical treatment for nonmuscle-invasive bladder cancer (NMlBC) is transurethral bladder tumor resection (TUR-BT), followed by postoperative bladder irrigation with a BCG vaccine and chemotherapy drugs. The main surgical treatment for muscle-invasive bladder cancer (NMIBC) is partial cystectomy or radical cystectomy. Radiotherapy is only used as an adjuvant treatment for the curable bladder cancer mentioned above. Moreover, radiotherapy is also recommended for patients with incurable bladder cancer, those who are unwilling to undergo surgery, or those who cannot tolerate surgery [8]. However, advancements in radiotherapy technology have played an important role in the treatment of bladder cancer. Radiotherapy for curable bladder cancer has achieved results comparable to those of surgical treatment [9]. In addition, for the treatment of late-line and aged cancer patients, particularly those who are not eligible for surgery, radiotherapy also has great potential. However, from the 2024 National Comprehensive Cancer Networks (NCCN) Clinical Practice Guidelines in Oncology (NCCN Guidelines®, https://www.nccn.org/patientresources/patient-resources/guidelines-for-patients), there is still no clear treatment guidance, especially for late-line elderly patients. To the best of our knowledge, there are no relevant studies or clinical reports on this topic. Thus, this study included patients with recurrence and progression after multiple methods or multiple lines of treatment in addition to radiotherapy, as well as patients who are elderly or have severe cardio-cerebral pulmonary complications and cannot tolerate surgery. They basically have no desire for anticancer treatment and are in the stage of hospice care. In the clinic, patients with malignant tumors whose expected survival time is less than 3 months enter hospice care. These patients went to the hospital due to obvious hematuria and/or urinary tract irritation and urinary tract obstruction caused by hematuria. After comprehensive evaluation, these patients were not suitable for antitumor drug (chemotherapy, targeted therapy, and immunotherapy) treatment, and hemostatic and symptomatic treatment was ineffective. With full communication with the patient and consent obtained, radiotherapy was applied to eliminate hematuria, control the tumor, and even cure the tumor and prolong the patient’s survival time.
Although multidisciplinary individualized precision treatment has achieved remarkable results, attention to the treatment of elderly patients with bladder cancer is lacking. In particular, aged patients with other heart, brain, and lung diseases are often afraid of surgery, easily miss the best treatment period, and suffer physical and mental pain, including but not limited to the fear of blood loss and pain during urination. In this work, we retrospectively summarized and analyzed the clinical effects and data of 43 late-line elderly patients with advanced bladder cancer who were diagnosed with and treated with radiotherapy at the Department of Oncology, Chongming Hospital Affiliated with Shanghai University of Medicine and Health Sciences, from January 2017 to June 2023. This study provides a reference treatment strategy for late-line and elderly patients with bladder cancer and low expectations for treatment and even for the clinical treatment of elderly patients with bladder cancer who are at an earlier stage and are in better physical condition.
2. Materials and Methods
2.1. Clinical Data
In this study, a total of 43 elderly patients with intermediate and advanced bladder cancer, including 37 males and 6 females, were treated with radiotherapy. The corresponding average age was 77.3 ± 5.1 years, and the median age was 82 years. The specific age distributions and corresponding ratios of patient numbers are shown in Figure 1. All patients were pathologically diagnosed with transitional epithelial carcinoma of the bladder. Two patients were in TNM stage ll, 31 patients were in stage lll, and 10 patients were in stage lV. Among them, 8 patients were initially treated, and 35 patients were retreated. All patients presented to the hospital with obvious symptoms of hematuria; 41 patients experienced pain; 37 patients experienced bladder irritation, such as urgency, frequency, and dysuria; 12 patients required continuous bladder irrigation due to blood clot obstruction; and 8 patients received blood component transfusions and red blood injection (2–8 U). The corresponding performance status (PS) scores were as follows: 11 cases with a score of 1, 19 cases with a score of 2, and 13 cases with a score of 3. The NRS score ranged from 0 to 3 points in 27 patients, 4 to 6 points in 11 patients, and 6 to 10 points in 5 patients. The patients who were initially treated were elderly, had comorbidities in other organs, and had poor PS scores. The retreated patients were all in stages lll to lV, and all had a history of intravesical chemotherapy with chemotherapy drugs. Thirteen patients had a history of intravenous chemotherapy, one patient had a history of intravenous chemotherapy and apparent diffusion coefficient (ADC) treatment, and 6 patients had a history of combined PD-1 inhibitor treatment. Twenty-eight patients had a history of cystoscopic electrocoagulation resection, of whom 11 patients had a history of interventional embolization to stop bleeding. None of the total 43 patients treated underwent partial or total cystectomy.
2.2. Clinical Treatment
All patients were unable to tolerate surgery and were not suitable for chemotherapy, or chemotherapy alone was ineffective due to advanced age, advanced tumor stage, and comorbidities. They were treated with palliative radiotherapy to stop bleeding and relieve pain and symptoms. Before radiotherapy, a 16-slice large-aperture spiral CT scan was used for the localization of the cancer lesion. The gross tumor volume (GTV) was recorded on the basis of the CT localization image, and the tumor was visible via cystoscopy and imaging. The clinical target volume CTV1 was the entire bladder, prostate, and regional lymph nodes. The tumor is visible on CTV2 entire bladder and CT images. CTV3 includes the GTV to ensure local increased-dose irradiation. The planned target area PTV1 is the small pelvic field, PTV2 is the full bladder field, and PTV3 is the planned target area for the increased dose to the tumor. The Monaco tumor radiotherapy planning system was used for plan design and evaluation, and radiotherapy was performed via a four-dimensional image-guided Infinity (Ruby) accelerator (Infinity™, Elekta, Sweden). The bladder of patients should be emptied before positioning and radiotherapy to reduce the bladder volume as much as possible. Using 6MV X-ray and IMRT technology, the prescribed doses were 96% PTV1 51Gy/30Fx/1.7Gy, 96% PTV2 54Gy/30Fx/1.8Gy, and 96% PTV3 64.5Gy/30Fx/2.15Gy, respectively. The tests were performed once a day for five days per week. Among them, 4 patients with bone metastases received radiotherapy at the same time. After 40 Gy, the treatment plan can be adjusted to radical radiotherapy depending on the patient’s physical condition and tolerance to radiation. During radiotherapy, concurrent chemotherapy can be applied to increase the degree of sensitization to radiotherapy. Fourteen patients were treated concurrently with weekly dose chemotherapy (gemcitabine + cisplatin, paclitaxel + cisplatin), and another 6 patients were treated with the addition of anlotinib. Radiotherapy was combined with antiangiogenic treatment in 7 patients, and 8 patients were treated with radiotherapy combined with PD-1 inhibitors. Moreover, routine blood tests, routine urine tests, liver function tests, and kidney function tests were repeated once a week.
2.3. Clinical Observation and Assessment Methods
The primary observation point was the disappearance of hematuria, and the secondary observation point was the patient’s overall survival time. Overall survival time refers to the time from the start of radiotherapy to death or the last follow-up (until June 2023).
2.4. Statistical Analysis
R4.2.3 software was used for data analysis. The “survival” package was used to calculate survival time analysis, and the “survminer” package was used to summarize and draw Kaplan–Meier (KM) survival curves. Age and patient survival time were analyzed via Pearson correlation analysis.
3. Results
3.1. Clinical Results
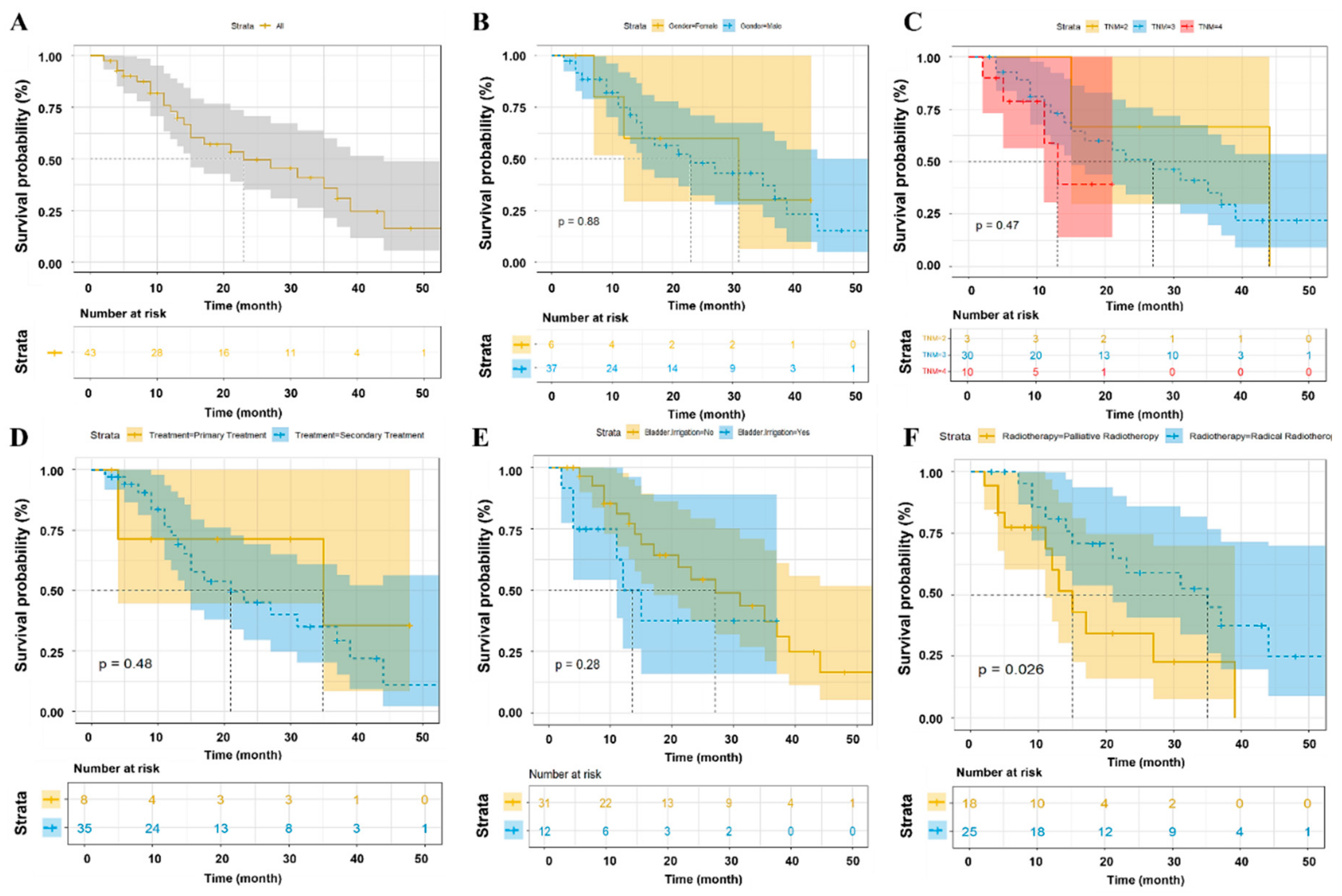
Among the 43 patients, 7 patients were treated with 36–40 Gy of radiotherapy, 11 patients were treated with 52–56 Gy of radiotherapy, and 25 patients were treated with 62–72 Gy of radiotherapy. After 5 rounds of radiotherapy at 10 Gy, the degree of bleeding gradually decreased. After 15 rounds of radiotherapy at 30 Gy, gross hematuria disappeared, and the pain was reduced or relieved. At the end of follow-up, 24 patients had died, and 19 patients had survived. Among the patients who died, 15 died from tumor progression, and 9 died from nonneoplastic diseases. The survival times of all patients after radiotherapy were as follows (Figure 2A): 34 patients at 6 months, 25 patients at 12 months, 17 patients at 18 months, 13 patients at 24 months, and 7 patients at more than 36 months; the corresponding survival rates were 79.1%, 58.1%, 39.5%, 30.2%, and 16.3%, respectively. The median survival time (OS) was 14 months, the shortest survival time was 2 months, and the longest survival time reached 53 months (i.e., more than 4 years). The results of the statistical analysis are shown in Figure 2. Notably, the survival time of patients significantly differed with radical or palliative RT (p=0.028, Figure 2F) but was not related to sex (p=0.88, Figure 2B), stage (p=0.47, Figure 2C), age (r=-0.064, p=0.684), initial treatment or retreatment (p=0.48, Figure 2D), or whether bladder bleeding requires flushing (p=0.28, Figure 2E).
3.2. Clinical Adverse Reactions
The primary objective of the treatment in this study was to provide palliative care to achieve hemostasis. Following 15 or more sessions of radiotherapy, if significant symptoms such as fatigue, anorexia, urinary tract irritation, or rectal irritation emerged—potentially attributable to radiotherapy-induced adverse effects—treatment was temporarily discontinued. Supportive and symptomatic management was administered during this suspension. Radiotherapy was resumed upon symptom resolution, or permanently discontinued based on the patient’s overall clinical status and tolerance. Notably, patients in this cohort did not experience any severe adverse reactions related to radiotherapy.
4. Discussion
Bladder cancer is a common malignancy of the urinary system, with a significant gender disparity in its incidence. Epidemiological data from the 2019 report by the Chinese Cancer Registry revealed that in 2015, bladder cancer ranked as the 13th most common malignancy in China, with an incidence rate of 5.80 per 100,000. Among males, it was the 7th most common malignancy (8.83 per 100,000), while among females, it ranked 17th (2.61 per 100,000), highlighting its relative rarity in women. Utilizing advanced statistical software, we conducted a comprehensive analysis of factors associated with bladder cancer, including gender-stratified analyses on six female patients. However, the unequal distribution of male and female cases limits the objectivity of assessing gender differences in treatment outcomes and precludes definitive conclusions regarding the comparative efficacy of therapeutic interventions. The study cohort comprised terminal-stage bladder cancer patients who were ineligible for surgery or chemotherapy and had discontinued other anticancer treatments. Most presented with gross hematuria, with some experiencing urinary retention due to urethral obstruction caused by blood clots. These symptoms, particularly persistent bleeding, caused substantial psychological distress for both patients and their families. Furthermore, many patients did not initially seek care from oncology or radiotherapy departments but were referred or incidentally directed there, complicating the process of case accumulation. Over six and a half years, only 37 cases were documented, underscoring the challenges of conducting research in this population and highlighting the need for larger, multi-center studies to enable more robust and generalizable findings.
The comprehensive multidisciplinary treatment of bladder cancer is a key treatment strategy that combines surgery, radiotherapy, and chemotherapy to control the recurrence and metastasis of local tumors. Surgical treatment plays an important role, and according to the degree of tumor infiltration into the muscle layer, different surgical treatment strategies can be used. The main surgical treatment for low-stage (Tis, T1) nonmuscle invasive bladder cancer is usually transurethral resection of bladder tumor (TUR-BT), which is supplemented with a BCG vaccine and chemotherapeutic drugs (mitomycin C, epirubicin, pirarubicin, gemcitabine, hydroxycamptothecin, and doxorubicin) for bladder lavage. The local recurrence rate after TUR-BT treatment is 50% to 80%, and the progression to invasive disease accounts for 15% to 23% of cases of recurrence [10]. Fewer than 5% of patients will also develop distant metastasis, and the mortality rate is approximately 9% [11]. Partial cystectomy or radical cystectomy is feasible for some NMIBC patients. The main surgical methods for treating muscle-invasive bladder cancer (MIBC) include radical cystectomy and pelvic lymph node dissection. Postoperative adjuvant local radiotherapy and systemic therapy are also needed. Systemic chemotherapy regimens for bladder cancer are mostly platinum-based combination chemotherapy regimens, such as cisplatin combined with gemcitabine/paclitaxel. This type of surgery is highly invasive and has many complications. The 5-year postoperative survival rate is 59% to 67%, and the recurrence-free survival rate is 56% to 71% [12,13]. Removal of the bladder may affect quality of life and reduce the recurrence-free survival rate. Recently, there have also been targeted therapies, especially antiangiogenic targeted therapies [14] and PD-1/PD-L1 immunotherapy [15].
The treatment of bladder cancer with radiotherapy could preserve the bladder for patients and has great advantages in improving patients’ quality of life. Radical radiotherapy provides a new treatment option for patients with muscle-invasive bladder cancer who are unable to undergo surgery or are unwilling to undergo surgery (NCCN Guidelines®). Duan et al. [16] reported that 963 patients were treated with radical radiotherapy. Patients with stage T1, T2, T3, and T4 tumors accounted for 20%, 32%, 40%, and 8%, respectively. After treatment with 55Gy/20F radiotherapy to the bladder, 65% of patients achieved CR, with 46% of patients having confirmed lesion disappearance via cystoscopy. The 5-year and 10-year survival rates after radiotherapy in the whole group were 30% and 18%, respectively, and the local recurrence rates were 47% and 53%, respectively.
Radiotherapy has a significant effect on bleeding in bladder cancer patients. Liu et al. [17] reported that 23 patients with bladder cancer were treated with three-dimensional conformal radiation therapy, with 3–8 Gy of radiotherapy applied each time and once every other day, with a total dose of 48–66 Gy applied to the tumor lesion. After 3 months of treatment, reexamination revealed that the tumors had completely disappeared in 17 patients, the tumors had shrunk by more than 1/2 in 6 patients, and the hematuria had completely disappeared. The total effective rate of these treatments reached 100%. There were no serious complications during the treatment. Some patients had a mild urinary frequency, urgency, dysuria and slight abdominal discomfort, which were relieved by the oral administration of ciprofloxacin. For patients who are elderly, who are physically unable to accept or refuse cystectomy, or for whom chemotherapy alone is ineffective or intolerable, radiotherapy is a feasible and effective practical method. To a certain extent, radiotherapy could achieve equivalent results to those of surgery and could provide a better quality of life. Kotwali et al. [9] reported and analyzed 169 patients with bladder cancer, of whom 72 patients underwent radical bladder cancer resection and 97 underwent radical radiotherapy. Although the patients in the radiotherapy group were 7 years older than those in the surgery group were, the 5-year OS was similar; the OS rate was 34.6% in the radiotherapy group and 41.3% in the surgery group. Li et al. [18] reported the efficacy of radiotherapy in 53 cases of bladder cancer and reported that the 1-, 2-, and 5-year survival rates of patients were 75.6%, 51.1%, and 27.2%, respectively; the local recurrence rates were 14.8%, 40.6%, and 56.2%, respectively; and the median follow-up period was 24 months. The key factor affecting the effectiveness of radiotherapy is the clinical stage of the tumor. Single-factor analysis revealed that only the survival rates differed significantly across stages, and multifactor analysis revealed that T stage and N stage were statistically significantly associated with patient survival and local control of cancer.
In clinical practice, radiotherapy has demonstrated significant hemostatic efficacy in advanced bladder cancer, particularly in cases where urethral obstruction from bleeding renders continuous irrigation ineffective. At this critical stage, when surgical intervention is unfeasible and pharmacological treatments fail, radiotherapy stands out as the sole viable and effective option. Its administration, contingent upon stable vital signs, is generally accepted by patients and their families, often as a last resort, regardless of the eventual prognosis. At the initiation of this study in 2017, immunotherapy with PD-1/PD-L1 inhibitors had not yet become widely available, and even to date, neither immunotherapy alone nor in combination with single-agent chemotherapy has achieved significant success in managing advanced bladder cancer. Conversely, radiotherapy has consistently provided dual benefits by effectively controlling hematuria and prolonging survival, underscoring its critical role in patient care. Our analysis identified radiotherapy as the only treatment significantly associated with tumor control in terminal-stage bladder cancer, a finding corroborated by previous studies [11,12,13,14,15,16], which highlight radiotherapy’s comparable efficacy to surgery in early-stage bladder cancer while preserving bladder function. This dual advantage underscores radiotherapy’s potential as a compassionate and practical treatment strategy, especially for underserved and vulnerable patients. Despite this, current clinical guidelines and research place insufficient emphasis on the value of radiotherapy for such patients, representing a missed opportunity to enhance care. Raising awareness and integrating radiotherapy more prominently into treatment paradigms for advanced bladder cancer is imperative to improve outcomes and offer hope to this disadvantaged population.
In this group, elderly patients with advanced bladder cancer who presented with persistent bleeding and who were in poor physical condition were not eligible for surgery or chemotherapy. They are basically in the end-of-line hospice care stage and have low expectations for treatment. After thorough communication, the patients were treated with radiotherapy, and 4 patients with bone metastases were treated with radiotherapy at the same time as described in Section 2.2. The success rate of radiotherapy to stop bleeding was 100%, and the median survival time of patients reached 14 months. Initial palliative radiotherapy at a dose of approximately 30 Gy successfully stopped bleeding, after which patients and their families exhibited improved adherence to further treatment. This created opportunities to adjust treatment plans to curative-intent radiotherapy based on tumor stage and performance status (PS) scores. Additionally, the cessation of hematuria facilitated the initiation of systemic therapies, including chemotherapy, anti-angiogenic agents, and immunotherapy, which contributed to survival benefits in patients eligible for curative radiotherapy. However, the study did not stratify the effects of these pharmacological interventions, representing a limitation. Importantly, the therapeutic benefits observed were primarily attributed to radiotherapy, as achieving hemostasis was a prerequisite for subsequent treatments. Among the 35 patients treated, all had previously attempted drug therapies, but those experiencing terminal-stage hematuria were no longer eligible for further pharmacological interventions. Statistical analysis revealed that the survival time of patients significantly differed with radical or palliative RT (p=0.028) but was not related to sex, stage, age, initial treatment or retreatment, or whether bladder bleeding required flushing. The reason might be that the patients in this study were aged and late-line patients with poor physical condition; the expectation of treatment focused on stopping bleeding, which might affect compliance; and the number of patients included in this study was limited.
This study did not include a negative control group to assess the natural survival time of untreated patients, nor did it have sufficient data for direct comparative analysis. Clinically, patients with advanced-stage cancer in palliative care typically have an estimated survival time of less than three months. However, the observed median survival time of 14 months in this study significantly exceeds this expectation. Radiotherapy effectively achieved hemostasis, alleviated symptoms, improved patients’ quality of life, and extended survival. Persistent bleeding is well-recognized as a severe physiological burden that can lead to circulatory shock and death. Additionally, complications such as urethral obstruction caused by blood clots can result in urinary retention and postrenal kidney failure, often leading to mortality within a week if left untreated. Ethical constraints in modern medicine preclude the design of studies comparing radiotherapy to no treatment in patients with bladder cancer and severe bleeding, as withholding a potentially lifesaving intervention would be inhumane and ethically unacceptable. As such, the absence of a control group is an inherent limitation. Nonetheless, in scenarios where radiotherapy is the sole viable option, both patients and clinicians are inclined to proceed, even under challenging circumstances. The findings demonstrate that radiotherapy not only reliably achieves hemostasis but also avoids treatment-related mortality, reinforcing its safety and efficacy. The distinction between palliative and curative radiotherapy observed in practice serves as a de facto comparison, further highlighting its critical role in managing advanced bladder cancer with bleeding and its substantial impact on survival outcomes.
5. Conclusion and Outlook
In real-world clinical practice, cancer treatment is influenced not only by the stage of the disease but also by factors such as comorbidities, patient age, and the level of family support and care. As the population ages and fertility decline, elderly cancer patients receive less care, and some patients delay cancer treatment for various reasons. Bleeding symptoms are a serious cause of harm to patients’ body and mind, as is the case in this group of patients. These patients were treated for obvious bleeding, which is not suitable for surgery or chemotherapy. All the patients who received radiotherapy achieved hemostasis, eliminated the patient’s fear of bleeding, gained spiritual comfort, and improved their quality of life. After the bleeding was controlled and the physical condition of some patients improved, their condition was re-evaluated, and the prescribed dosage was changed from palliative radiotherapy to radical radiotherapy combined with chemotherapy, antiangiogenic therapy, and immunotherapy to prolong the survival time of patients. Notably, palliative treatment for cancer can relieve patients’ symptoms and pain, which is also an important way for patients to prolong their survival time. Therefore, radiotherapy is a feasible option to stop bleeding and relieve symptoms in elderly patients with advanced bladder cancer and persistent bleeding, and it is also possible to control the progression of bladder tumors.
However, this study has several limitations, including but not limited to the fact that the patients in this study were aged and were essentially in the end stage when available cancer treatment methods were exhausted, and radiotherapy was also a tentative treatment; the number of cases was small, and the stratification was rough; and some patients refused further radiotherapy after bleeding stopped, with only 25 patients who completed radical radiotherapy with more than 62 Gy. Thus, it is still necessary to accumulate more cases in the future and conduct more refined stratified analyses to provide a more accurate treatment basis and reference for this type of patient and even for elderly patients with earlier stages.
With the advancement of biomedical technology and improvements in clinical treatment, an increasing number of treatment methods and strategies have been developed [15,16,19,20]. Like combining radiotherapy with immune drugs, targeted and other high-efficiency and low-toxicity drugs have made it possible for some hospice care patients with poor physical conditions to receive treatment and achieved good therapeutic effects. Therefore, tumor treatment is a comprehensive and personalized treatment process that can be adjusted according to the individual differences among patients. For the special groups in this study, end-line elderly patients with advanced bladder cancer without surgery who were treated with radiotherapy exhibited good therapeutic effects, which not only alleviated the physical and mental pain caused by the disease but also extended the patients’ lifespan and improved their quality of life. These findings provide new opportunities for the treatment of this type of patient and make it possible to allow them to live with quality and dignity.
Conflicts of Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Ethics Approval and Consent to Participate
This study was approved by the Ethical Committee of Xinhua Hospital Affiliated with Shanghai Jiao Tong University School of Medicine Chongming Branch (No. 2019YA29). Meanwhile, written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Consent for Publication
Informed written consent was obtained from all patients included in this study. All the authors approved the publication of this paper.
Author Contributions
The study design was designed by all the authors, and all the authors were involved in the writing process and revisions of the initial drafts of the paper. J. Xu and Y. Huang: data collection and analysis, data acquisition, and case collection. G. Ni, Y. Huang, Q. Qian, X. Liang, Y. Ni, H. Xie, and Z. Yue: material preparation, data collection and analysis, and patient consent for publication. Z. Yang and H. Liu provided the idea, supervision, project management, and funding.
Funding
The authors acknowledge funding support from the Shanghai Municipal Health Commission (Grant Nos. 201940274) and the Key Disciplines of Chongming District Health Commission.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
- R.L. Siegel, K.D. Miller, A. Jemal, Cancer statistics, 2018, CA: A Cancer Journal for Clinicians 68(1) (2018) 7-30.
- J. Dobruch, M. Oszczudłowski, Bladder Cancer: Current Challenges and Future Directions, 57(8) (2021) 749.
- C. Xia, X. Dong, H. Li, M. Cao, D. Sun, S. He, F. Yang, X. Yan, S. Zhang, N. Li, W. Chen, Cancer statistics in China and United States, 2022: profiles, trends, and determinants, 135(5) (2022) 584-590.
- W. Chen, R. Zheng, P.D. Baade, S. Zhang, H. Zeng, F. Bray, A. Jemal, X.Q. Yu, J. He, Cancer statistics in China, 2015, CA Cancer J Clin 66(2) (2016) 115-32.
- M. Cao, C. Ding, C. Xia, H. Li, D. Sun, S. He, W. Chen, Attributable deaths of liver cancer in China, Chinese journal of cancer research Chung-kuo yen cheng yen chiu 33(4) (2021) 480-489.
- Q. Huang, H. Zi, L. Luo, X. Li, C. Zhu, X. Zeng, Secular trends of morbidity and mortality of prostate, bladder, and kidney cancers in China, 1990 to 2019 and their predictions to 2030, BMC Cancer 22(1) (2022) 1164.
- U.N. Joensen, S.L. Maibom, A.M. Poulsen, Surgical Management of Muscle Invasive Bladder Cancer: A Review of Current Recommendations, Seminars in oncology nursing 37(1) (2021) 151104.
- N.P. Omorphos, J.C.P. Piedad, N. Vasdev, Guideline of guidelines: Muscle-invasive bladder cancer, Turkish journal of urology 47(Supp. 1) (2021) S71-s78.
- S. Kotwal, A. Choudhury, C. Johnston, A.B. Paul, P. Whelan, A.E. Kiltie, Similar treatment outcomes for radical cystectomy and radical radiotherapy in invasive bladder cancer treated at a United Kingdom specialist treatment center, International journal of radiation oncology, biology, physics 70(2) (2008) 456-63.
- Z. Petrovich, G. Jozsef, L.W. Brady, Radiotherapy for carcinoma of the bladder: a review, American journal of clinical oncology 24(1) (2001) 1-9.
- G. Kovács, D. Hebbinghaus, P. Dennert, P. Kohr, R. Wilhelm, B. Kimmig, Conformal treatment planning for interstitial brachytherapy, Strahlentherapie und Onkologie : Organ der Deutschen Rontgengesellschaft [J] 172(9) (1996) 469-74.
- T. Lin, X. Fan, C. Zhang, K. Xu, H. Liu, J. Zhang, C. Jiang, H. Huang, J. Han, Y. Yao, W. Xie, W. Dong, L. Bi, J. Huang, A prospective randomized controlled trial of laparoscopic vs open radical cystectomy for bladder cancer: perioperative and oncologic outcomes with 5-year follow-upT Lin et al., British journal of cancer 110(4) (2014) 842-9.
- S. Madersbacher, W.W. Hochreiter, F.C. Burkhard, G.N. Thalmann, H. Danuser, R. Markwalder, U.E.J.J.o.c.o.o.j.o.t.A.S.o.C.O. Studer, Radical cystectomy for bladder cancer today--a homogeneous series without neoadjuvant therapy, 21 4 (2003) 690-6.
- J.Z. Cao, W. Wu, J.F. Pan, H.W. Wang, J.H. Jiang, Q. Ma, Case Report: Anlotinib Combined With Sintilimab as Third-Line Treatment in a Metastatic Urothelial Bladder Carcinoma Patient With FGFR3 Mutation, Frontiers in oncology 11 (2021) 643413.
- F.C. de Jong, V.C. Rutten, T.C.M. Zuiverloon, D. Theodorescu, Improving Anti-PD-1/PD-L1 Therapy for Localized Bladder Cancer, Int J Mol Sci 22(6) (2021).
- W. Duncan, P.M. Quilty, The results of a series of 963 patients with transitional cell carcinoma of the urinary bladder primarily treated by radical megavoltage X-ray therapy, Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 7(4) (1986) 299-310.
- J.T. Liu zhi-hui, Zhong shou-bin, et al., Three dimensional conformal radiotherapy for bladder cancer:Analysis of 23 cases, Practical Journal of Medicine Pharmacy 23(2006-08) (2006).
- F.Y. LI Yunhai, WANG Honglin, Radiotherapy of 53 patients with bladder cancer, Journal of Practical Oncology 19(2) 5.
- Nikshoar, M.S., Khayamian, M.A., Ansaryan, S. et al. Metas-Chip precisely identifies presence of micrometastasis in live biopsy samples by label free approach. Nat Commun 8, 2175 (2017).
- Khayamian MA, Baniassadi M, Abdolahad M. Monitoring the effect of sonoporation on the cells using electrochemical approach. Ultrason Sonochem. 2018 Mar;41:619-625.
Figure 1.
Age distributions and corresponding ratios of patient numbers in this study and average ages.
Figure 1.
Age distributions and corresponding ratios of patient numbers in this study and average ages.
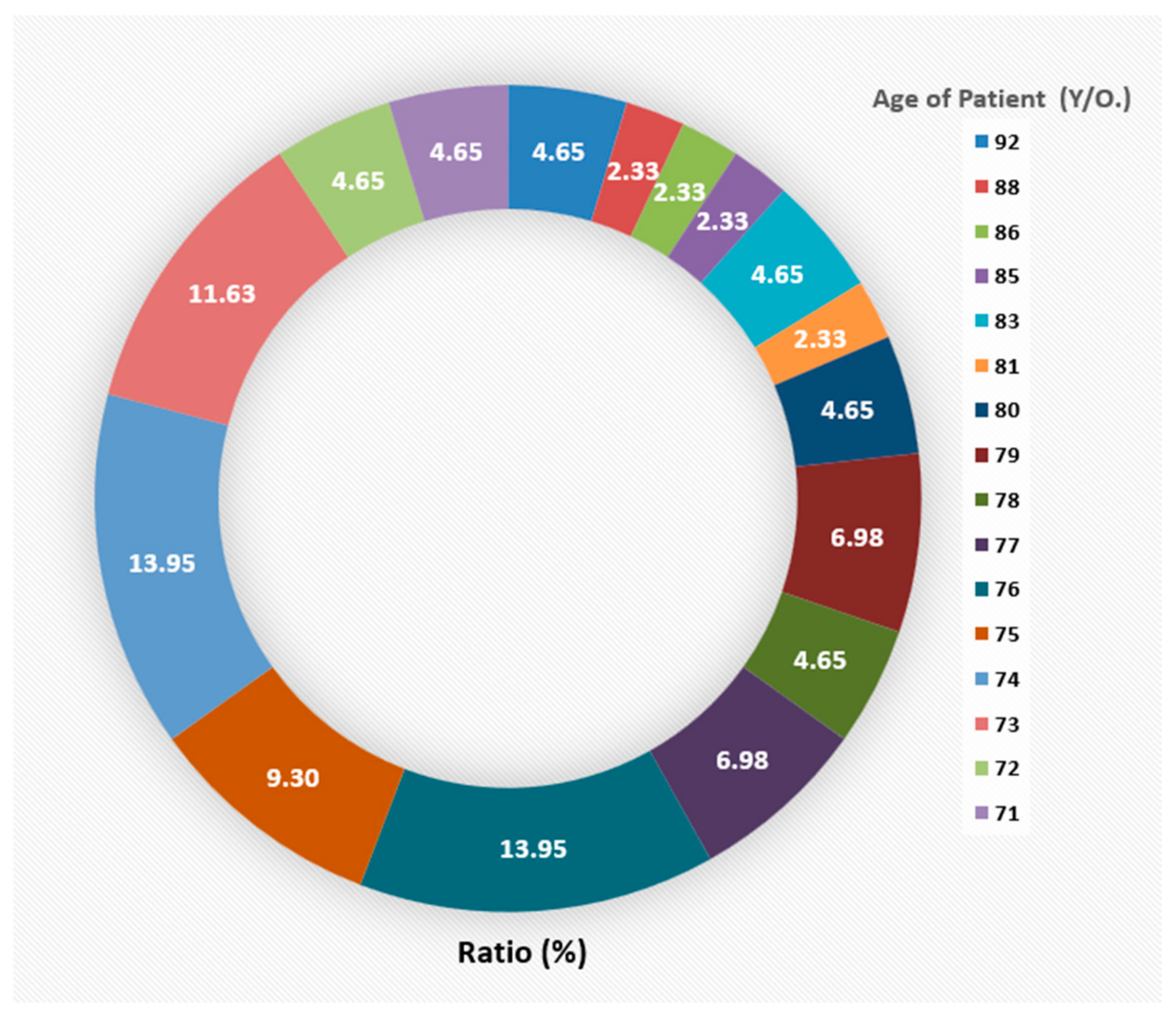
Figure 2.
(A) Survival curves of all patients after radiotherapy and survival curves according to sex (B), TNM stage (C), initial treatment or retreatment (D), whether bladder bleeding requires flushing (E), and treatment with radical or palliative radiotherapy (F).
Figure 2.
(A) Survival curves of all patients after radiotherapy and survival curves according to sex (B), TNM stage (C), initial treatment or retreatment (D), whether bladder bleeding requires flushing (E), and treatment with radical or palliative radiotherapy (F).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



