Submitted:
18 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
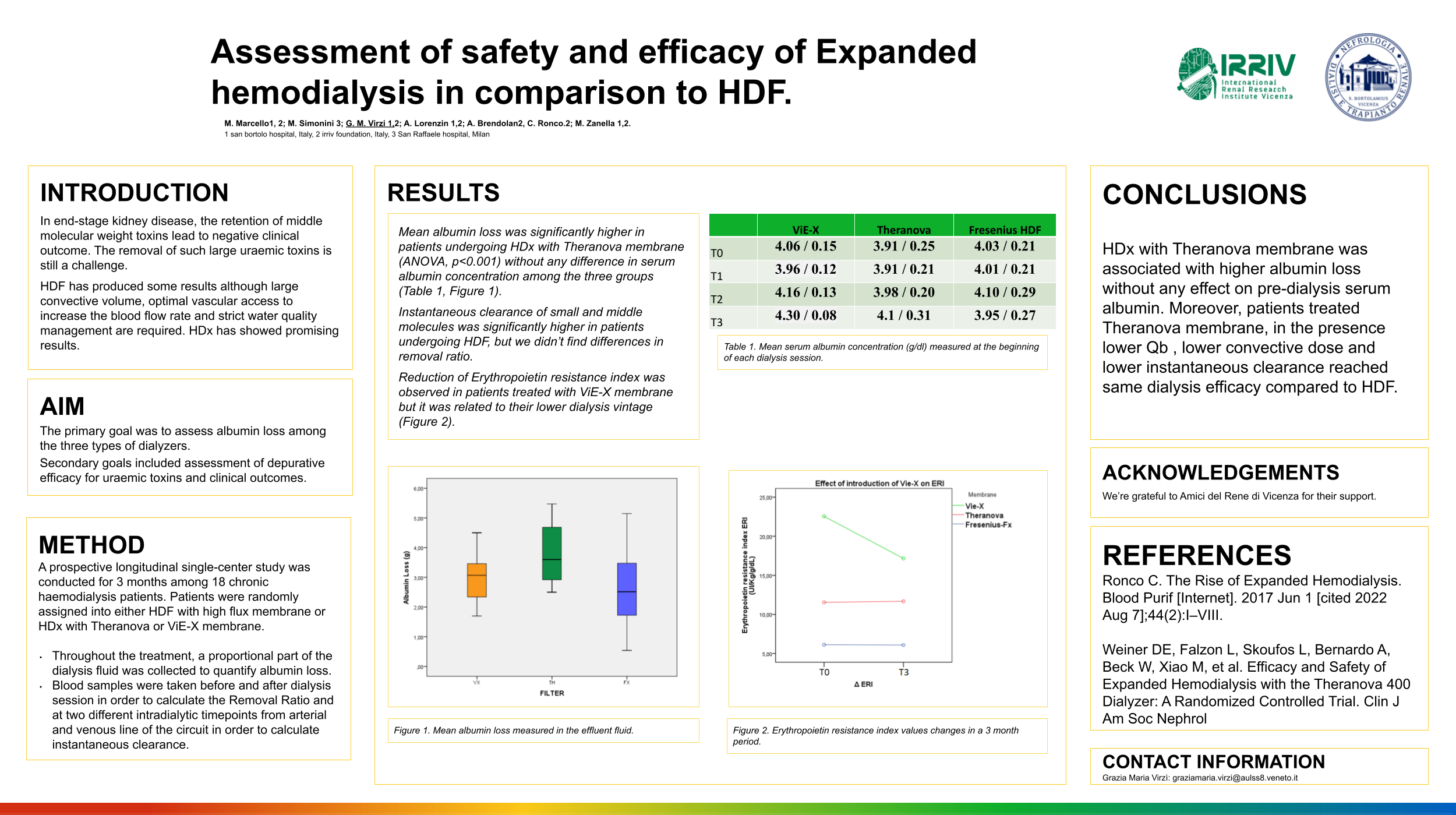
Background: Removal of large uraemic toxins is still a challenge. HDF has produced some results although large convective volume, optimal vascular access to increase the blood flow rate and strict water quality management are required. Medium Cut-Off, high Retention Onset membrane have been recently developed introducing the concept therapy called “expanded haemodialysis” (HDx). Furthermore, vitamin E-coated membrane has potential beneficial effects on inflammation and oxidative stress. Ma-terial and Methods: A prospective longitudinal multi-center study was conducted for 3 months among 24 chronic haemodialysis patients. Patients were randomly assigned into either HDF with high flux membrane or HDx with Theranova or ViE-X mem-brane. The primary goal was to assess albumin loss among the three types of dialyzers. Secondary goals included assessment of depurative efficacy for uraemic toxins and clinical outcomes. Results: Mean albumin loss was significantly higher in patients undergoing HDx with Theranova membrane (ANOVA, p< 0.001) without any differ-ence in serum albumin concentration among the three groups. Instantaneous clearance of small and middle molecules was significantly higher in patients undergoing HDF, but we didn’t find differences in removal ratio and Kt/V. Reduction of Erythropoietin resistance index was observed in patients treated with ViE-X membrane due to their lower dialysis vintage. Conclusion: The higher albumin loss during HDx has no effects on pre-dialysis serum albumin. HDx with Theranova® in presence of lower session length, lower Qb , lower convective dose and lower instantaneous clearance reached same dialysis efficacy compared to HDF.
Keywords:
Expanded hemodialysis
; Hemodiafiltration
; Medium Cut-off
; middle molecules
1. Introduction
Along with the retention of metabolic waste products, patients with advanced kidney disease typically experience a constellation of symptoms which lead to a reduced quality of life and increased morbidity and mortality. Complications of uraemia in patients with adequate urea kinetics and Kt/V have been correlated with uraemic toxins in the molecular range of 5000–50 000 Da not being adequately cleared by current dialysis techniques [1]. These molecules have been shown to have significant effects on the cardiovascular system, inflammation, and fibrosis [2]. Myoglobin (molecular weight 17 kDa) is involved in organ damage, oxidative stress and mitochondrial dysfunction [4]. Restless leg syndrome (RLS) is a neurological complication often seen in HD patients related to the accumulation of α1-Microglobulin, a middle molecule (molecular weight of 33 kDa)[5]. Patients with CKD have high plasma concentration of inflammatory markers such as C-reactive protein (CRP) and reactive oxygen species (ROS) [6]. Furthermore, the increased expression of proinflammatory cytokines such as IL-1, IL-6 and TNF-α lead to vascular calcification, oxidative stress, and endothelial dysfunction[7]. Increased oxidative stress, which is prominent in HD, has also been proposed as a significant link to uremic myopathy and fatigue in renal failure[8].
Small molecules (<500 Da) are efficiently removed during the diffusion process while the removal of middle and large molecules (50–15,000 Da) is still a challenge[9]. HDF has been developed to efficiently remove middle molecules as well as small solutes. However, patients treated with HDF require large convective volume (>23 L/session)[10], optimal vascular access to increase the blood flow rate and strict water quality management [11]. Despite advanced technology and results achieved by HDF, clinical outcomes in dialysis are still suboptimal.
Recently, a new class of membranes called medium cut-off (MCO) dialyzers, have shown to provide a greater efficiency in the removal of larger solutes with molecular weight up to 45kD, with only marginal albumin loss[14]. These membranes, also called Medium Cut-off High Retention Onset, have a tight pore size distribution that was designed to have a steep sieving curve in order to minimize the molecular weight interval between the MWRO and the MWCO. In MCO membranes, the combination of hydraulic permeability and geometric structure of the fibres enhances the process of internal filtration and backfiltration[15]. The term Expanded Haemodialysis has been proposed to define a treatment where diffusion and convection are combined inside a hollow-fibre dialyzer equipped with a Medium Cut-off High Retention-onset membrane. The combination of increased pore size and pore density with an advanced sieving profile and increased internal filtration allows an enhanced clearance of large middle molecules [16].
The aim of this study was to evaluate safety and efficacy of Expanded Haemodialysis with the new membrane Vie-X®, comparing its performance with analogous Medium Cut-Off membrane and Hemodiafiltration with high-flux membrane. The primary goal was to assess albumin loss among the three types of dialyzers. Secondary goals included assessment of depurative efficacy for small and middle molecules and dilayzer’s effect on anemia.
2. Materials and Methods
Study design
The following, represent a prospective observational single-centre study involving 18 patients and conducted over a 3-months period in the Dialysis centre at San Bortolo Hospital in Vicenza, Italy.
Patients were assigned into three group (6 patients each):
Group 1, HDx with Asahi Kasei Medical ViE-X®
Group 2, HDx Baxter Theranova 400®
Group 3, HDF with Fresenius CorDiax Fx80®
ViE-X® is a polysulfone, vitamin E-interactive membrane with presumed a pore diameter of 48 Ä and hollow fibre with a length of about 300 mm and internal diameter of 185 μm allowing advanced sieving profiles and increased internal filtration.
Dialysis prescription wasn’t changed for Group 2 and Group 3, while Vie-X® was assigned to patients in Group 1 previously treated with high flux HD.
All patients in the study provided informed consent and the study was approved on 8th of June 2021 by the local Ethics Committee (n° 25/21) and was conducted according to the Declaration of Helsinki.
Patients’ selection
The study included all patients aged 18 years, with stage 5 CKD in hemodialysis who provided informed consent. Exclusion criteria were: liver disease, oncologic disease and lympho- or myeloproliferative disorders under chemotherapy, autoimmune disorders or immunosuppression state, pregnancy and denial to give written consent for participation. Dialysis vintage was not considered in the selection of patients because we assessed only short-term effect of dialyzer.
Dialysis buffer with bicarbonate and dialysate flow 500 mL/min were present for all patients. The anticoagulation used was unfractionated heparin. Net fluid removal was set individually, depending on the patient's clinical needs. Different dialysis monitors were used: Bellco Flexya, Baxter Artis Physio, Nikkiso DBB, Fresenius 5008 and 6008.
Laboratory sampling
We analyzed four early-week HD session, at the beginning of each month over a 3-months period:
T0. First HD session analyzed and first use of ViE-X dialyzer in Group 1.
T1. After one month from the first HD session
T2. After two months from the first HD session.
T3. After three months from the first HD session.
Throughout the treatment, a proportional part of the dialysis fluid was collected to quantify albumin loss.
Dialysis adequacy was assessed in terms of single pool Kt/V and Removal Ratio (RR) of Urea, Creatinine and Phosphate. We evaluated the removal of small and middle molecules as Removal Ratio and Instantaneous Clearance.
Laboratory measurements carried out at the beginning and at the end of the dialysis session included Blood Count, Urea, Creatinine, Phosphorus, Uric Acid, Phosphorus, Myoglobin, α1-microglobulin, β2-microglobulin and IL-6. Furthermore, blood samples were taken from arterial and venous lines of the extracorporeal circuit, in order to assay the instantaneous clearance (K) of small and middle molecules. Laboratory measurements for instantaneous clearance were divided into two intradialytic times-point:
Initial part of HD session (I), taken 15 minutes after the beginning of HD session
Final part of HD session (F), taken 15 minutes from the end of HD session
The gap between Initial and Final Clearance of solutes was indicated as ΔK.
All laboratory measurement on blood and effluent fluid have been performed at the Laboratory Medicine Department of San Bortolo Hospital in Vicenza, except for the dosage of α1-microglobulin, β2-microglobulin which were performed at the Clinical Chemistry Department of University Hospital of Padova. Laboratory dosage of IL-6 has been analyzed at Research Laboratory in Nephrology Department of San Bortolo Hospital, Vicenza.
Calculations
Albumin loss throughout the treatment was evaluated from the albumin concentration in the dialysate and the total volume of effluent fluid.
For mixed diffusive-convective treatment as hemodiafiltration or bicarbonate dialysis in the presence of ultrafiltration, instantaneous clearance of a determined solute was calculated as follow:
where Qpi is the effective plasmatic flow rate entering the dialyzer, Qpo is the plasmatic flow rate leaving the dialyzer calculated as the difference between Qpi and Qf (Qpo= Qpi – Qf). Qf is the total ultrafiltration rate equivalent to net Ultrafiltration volume during Bicarbonate Dialysis treatment and calculated as the sum of net Ultrafiltration volume and the total substitution fluid volume during HDF treatment. Cpi and Cpo are the plasma water concentrations in the arterial and venous line respectively.
K= [(Qpi x Cpi) – (Qpo x Cpo)] / Cpi
For the assessment of Urea instantaneous clearance blood flow Qb was used. For all other molecules, plasma water flow rate (Qp) was used, calculated as follows:
Qp= (1-Hct)xQb
The Δ Clearance was calculated as the difference between Final and Initial Clearance values.
Removal Ratio (RR) was calculated as follows:
where Cpre and Cpost are the plasma concentration of solutes measured prior and after the dialysis session, respectively.
RR= ((C_pre-C_post ))/C_pre
Dialyzers’ effects on anaemia and ESA dosage were evaluated with Erythropoietin resistance index (ERI). ERI is defined as average weekly erythropoietin (EPO) dose per kg body weight (wt) per average haemoglobin (Hgb), over a 3-month period (ERI = (EPO/wt)/Hgb).
Basal-ERI was calculated in the three-month period preceding the study to evaluate the effect of introduction of the ViE-X dialyzer on anaemia. The gap between ERI and basal-ERI was called ΔERI
Statistical analysis
All statistical analysis was carried out using SPSS, version 23 (IBM Co., Armonk, NY, USA). Sample size was calculated as 18 patients, accepting a power of 80% and standard error α of 0.05 and effect size expressed as Cohen f=0.75, which allowed to assess the primary endpoint. The Kolmogorov–Smirnov test was used to analyse the variables’ distribution patterns. The baseline clinical characteristics are expressed as the means ± standard deviations, numbers (percentage, %) and median/IQR depending on the nature of the variables. Differences in biochemical parameters and albumin loss among different timepoints were analyzed using the repeated measures one-way analysis of variance. Differences in albumin loss, small and middle molecules’ clearances and removal ratio among different dialyzers were analyzed using ANOVA test. Correlation between clinical, anthropometric and biological parameters was carried out using Bivariate Correlation test.
3. Results
This prospective observational study was carried out in 18 patients (11 men, 7 Women), with a mean age of 67.7 ± 7 years (range 52 to 79 years) who were stable on a thrice-weekly haemodialysis (average dialysis vintage of 82 months, interval 1-437 months). Dialysis vintage was higher in patients undergoing HDF (p= 0.042). Underlying renal diseases were undiagnosed nephropathy in ten patients, chronic glomerulonephritis in five patients, obstructive nephropathy in two patients and polycystic kidney disease in one patient. All participants were either anuric or oliguric (<500 ml/24 h) except for three patients (two patients in Group 1, one in Group 2). Comorbidity was studied with Charlson index and incidence of Diabetes. Thirteen patients had Arteriovenous Fistula and five had Tunnelled Central Venous Catheter.
Baseline characteristics are summarized in Table 1.
We analysed four early-week HD session, at the beginning of each month over a 3-months period. Dialysis time was 210 minutes. Convective volume (Qf) during bicarbonate haemodialysis was calculated as the net Ultrafiltration volume. During HDF treatment convective volume was calculated as the sum of net Ultrafiltration volume and the total replacement volume. As shown in Table 1, Qb and Qf values differs between the three filters being higher in patients undergoing HDF (p<0.001).
Primary endpoint
In all 4 HD sessions analyzed, albumin loss was different among the three dialyzers (ANOVA p <0.001), even after correction for covariates (Univariate Analysis: Qb, Qf, BMI, Predialysis Serum Albumin). Patients in Group 2 had significantly higher albumin loss than those in Group 3 (ANOVA, post hoc test p<0.001) and those in Group 1 (ANOVA, post hoc test p=0.006). No significant differences among Group 1 and 3.
The introduction of Vie-X dialyzer in Group 1 lead to an initial fall followed by a progressive increase of pre-dialysis serum Albumin. No significant differences of Serum Albumin trend throughout different Timepoints were found among the three Groups (Analysis of Repeated Measures).
Mean albumin loss and pre-dialysis Serum Albumin values are summarized in Table 2.
Secondary endpoint
We found no differences in Kt/V between the three Groups (Group 1, 1.3 ± 0.16; Group 2, 1.27 ± 0.17; Group 3, 1.29 ± 0.1).
Initial instantaneous clearance (K) of Urea was different between the Groups (ANOVA p=0.003) being higher in Group 3. Patients in Group 3 had significantly higher Initial (I) instantaneous clearance of Creatinine than those in Group 1 (ANOVA, post hoc test p= 0.002) and those in Group 2 (ANOVA, post hoc test p=0.021). Patients in Group 1 had significantly lower Final (F) instantaneous clearance of Creatinine than those in Group 2 (p=0.014) and those in Group 3 (p<0.001). Patients in Group 3 had significantly higher Initial Instantaneous Clearance of Uric Acid than those in Group 1 (ANOVA, p=0.027) but not than Group 2. Patients in Group 3 had significantly higher Final Instantaneous Clearance of Uric Acid than those in Group 1 (ANOVA post hoc test, p=0.005) and Group 2 (p=0.014).
Initial and Final Instantaneous Clearance values, Δ Clearance as well as pre and post dialysis serum concentrations and Removal Ratios of small and middle molecules are shown in Table 3.
Both Initial and Final Instantaneous Clearance of middle molecules were higher in patients in Group 3. Phosphate instantaneous clearance was significantly lower in Group 1 compared to other groups. Δ Clearance of β2-microglobulin and α1-microglobulin were significantly higher Group 3.
We found no significant differences in the pre- and post-dialysis serum concentration as well as Removal Ratios of small molecules, phosphate, IL-6 and β2-microglobulin.
Initial α1-microglobulin serum concentration was significantly higher in Group 3 (ANOVA p<0.001). Final α1-microglobulin serum concentration in patients in Group 3 was significantly higher than those in Group 2 (post hoc test p=0.003). The RR α1-microglobulin in patients in Group 3 was significantly higher than those in Group 1 (ANOVA p=0.02) but not compared to Group 2.
Patients in Group 2 had Initial serum myoglobin significantly higher (ANOVA, p=0.005). No difference of final serum myoglobin was found among the Groups. The RR myoglobin was significantly higher in patients in Group 2 than those in Group 1 (ANOVA, p=0.04) and those in Group 3 (p=0.05).
We found no variation of Haemoglobin among different Groups and different timepoints (ANOVA). We found no differences on ERI and Basal-ERI and ΔERI value among the three Groups. Furthermore, we found a reduction in ERI value in patients in Group 1 but it was associated with their lower dialysis vintage (Bivariate Correlation p=0.009).
4. Discussion
In this prospective single-centre study, we made a cross-over comparison on 18 chronic haemodialysis patients undergoing either HDF or HDx. Patients were assigned into three group (6 patients each): bicarbonate dialysis with either VIE-X® (Asahi Kasei Medical) or Theranova 400® (Baxter) and hemodiafiltration HDF with Fresenius CorDiax Fx80®.
The present clinical trial examined the short-term effects of the newly developed MCO dialyzer Vie-X in terms of safety and efficacy comparing them with analogous MCO membrane Theranova, and high-flux membrane Fresenius-Fx in HDF modality.
The primary aim of this study was to investigate the safety of different dialyzers, in terms of albumin loss. In the evaluation of safety, we found in both dialysis modality a mean albumin loss within 5 gram per HD session, a cut-off above which a membrane is considered not suitable for chronic haemodialysis[21]. Mean albumin loss was significantly higher in patients undergoing HDx with Theranova® membrane (ANOVA, p<0.001) while not significant differences were observed among the other two membranes. During dialysis, a certain degree of albumin leakage is acceptable in order to remove larger molecules and protein-bound uremic toxins, without incurring the risk of low serum albumin levels. A recent prospective randomized crossover trial comparing high-flux haemodialysis with Expanded Haemodialysis, showed a greater removal of large uremic toxins using Medium Cut-off dialyzer without excessive albumin leakage, which was in the mean 2.8 and 3.0 grams per treatment [14]. In our study, the higher albumin loss observed in Group 2 didn’t influence serum albumin concentration. Similar to our report, a multicentre, randomized, controlled trial comparing safety and efficacy of HDx with Theranova membrane and High-flux HD, showed an albumin loss of 4 grams per treatment although maintaining constant serum albumin level over a period of 24 weeks[22]. Low serum albumin represents a strong predictor of mortality in haemodialysis patients but only when associated with chronic inflammation and decreased synthesis in malnourished patients[23] while the consequences of increased albumin loss during dialysis remains unknown and its potential benefits due to the removal of protein-bound toxins are still under investigation[24]. In our study, as dialysis prescription wasn’t changed for Group 2 and Group 3, we didn’t expect to see any variation in serum albumin concentration during the 3-month observation period. In Group 1 with the introduction of MCO membrane, we observed an initial fall of serum albumin concentration, followed by a gradual increase. However, no significant differences in the trend of serum albumin through different Timepoints (Analysis of Repeated Measures) was found between the three dialyzers. In previous clinical trials conducted for three months or less, pre-dialysis albumin levels were reduced after application of medium cut-off dialyzers[25]. However, different multicentre trials conducted over a period of 6 months or more showed that in patients previously treated with High-flux dialysis, the application of medium cut-off dialyzers led to an initial decrease in pre-dialysis albumin level followed by a rise back to baseline[22,26]. This paradoxical behaviour usually observed in a time point between three to six months might be associated to the reduced inflammation and increased removal of uremic toxins that occurs during Expanded haemodialysis in comparison to High-flux haemodialysis.
Secondary endpoint of the study was dialysis efficacy in terms of removal of small and middle molecules. Instantaneous clearance of small solutes including Urea, Creatinine and Uric Acid was significantly higher in patients undergoing Hemodiafiltration. Similarly to previous study[14], we found no differences in the removal of small solutes evaluated as Reduction Ratio (RR). Furthermore, Kt/V values were above the minimum target of adequacy (Kt/V ≥ 1.2)[27] in all patients without significant differences among the three Groups.
The results from our analysis show that instantaneous clearance of both small and middle molecules is significantly higher in patients receiving hemodiafiltration.
Instantaneous clearance is strictly dependent on convective volume and thus on Ultrafiltration rate (Qf). In patients undergoing Expanded haemodialysis, the convective flux was equivalent to the net ultrafiltration rate set up according to interdialytic weight gain. In patients undergoing hemodiafiltration, the convective flux was calculated as the sum of net ultrafiltration rate plus the volume of substitution fluid, therefore in our study, ultrafiltration rate (Qf) was significantly higher in patients in Group 3 receiving HDF (ANOVA, p<0.001). This largely explain the significant difference in instantaneous clearance values. However, during HDx initial and final instantaneous clearance values of β2-microglobulin and α1-microglobulin were similar, while during HDF we observed a decrease of the instantaneous clearance throughout the dialysis session. Accordingly, we found the Δ clearance value of β2-microglobulin and α1-microglobulin significantly lower in patients undergoing HDF (ANOVA, β2mcg p=0.013, α1mcg p<0.001). This reduction in clearance value in Group 3 could be explained by the membrane fouling and concentration polarization occurring during HDF due to the higher Ultrafiltration rate [28], however the same pattern was not observed for other uremic toxins. A certain degree of convective flux independent from the net ultrafiltration rate usually take place inside the MCO-HRO membrane. This phenomenon, known as internal-filtration/backfiltration has been demonstrated for Theranova membrane by Lorenzin et al.[29] while it can be only hypothesized for Vie-X membrane. However, the main advantage of HDx is that the removal of middle molecules is dependent on the high Sieving Coefficient rather than the convective volume and therefore it can be used in patients with suboptimal vascular access and lower blood flow Qb. In our study, the majority of patients undergoing HDF (5 out of 6 patients) had an arteriovenous fistula as a vascular access and their Qb value was significantly higher compared to those receiving HDx (ANOVA, p<0.001), while half of patients undergoing HDx with Theranova membrane had a catheter as a vascular access. Blood flow Qb influence the performance of dialysis by increasing diffusive and convective dialysis dose and reducing the risk of coagulation with no additional costs[30]. A prospective single-center study by Maduell et al.[31] comparing safety and efficacy of HDx with high-flux HD and HDF in pre and post-dilution using a Qb of 250 ml/min shows that HDx achieve a better depurative performance than HD and pre-HDF but lower depuration than post-HDF. In another study by Maduell et al.[32] increasing the Qb to 400 ml/min was associated with increased solute removal in both HDx and HDF but the benefit was greater in HDF, probably because increasing the Qb facilitates the higher convective dose. In our study, even if instantaneous clearance values of middle molecules were higher in patients undergoing HDF, the removal ratio of myoglobin was significantly higher in patients receiving HDx with Theranova membrane. The same pattern was observed for β2-microglobulin, where the removal was higher with Theranova membrane, although no significant difference was found compared to HDF. Therefore, HDx with Theranova in presence of lower Qb and in the absence of high convective dose reached similar target of dialysis adequacy, lower instantaneous clearance of middle molecules but without differences in the serum concentration of uremic toxins ans RRs. The long term prognosis of HDx in comparison to HDF has been evaluated by the CARTOON study[33], a recent multicenter randomized controlled trial showing that HDx was not inferior to HDF in terms of cardiovascular risk.
Patients in the Group 3, treated with HDF had higher dialysis vintage compared to other groups. The only parameter assessed, that could have been influenced by dialysis vintage was pre-dialysis serum concentration of uremic toxins. However, we found significant differences only in the concentration of α1-microglobulin that was higher in Group 3.
Expanded haemodialysis with ViE-X dialyzer was associated to lower pre-dialysis Creatinine values, but this was probably related to the lower dialysis vintage of patients in Group 1 (ANOVA, p=0.042). Mean albumin loss was 2.9 g in patients receiving HDx with ViE-X® membrane with no significant differences compared to patients undergoing HDF. Moreover, the introduction of ViE-X® dialyzer in patients previously treated with high-flux HD was not associated to a decrease in pre-dialysis serum albumin. In the evaluation of the efficiency of Vie-X membrane, is necessary to take into account different features regarding patients in Group 1. The majority of patients in this group had arteriovenous fistula (5 out of 6 patients). Mean dialysis vintage was significantly lower compared to other groups, and only one patient receiving Vie-X membrane was anuric, however, blood flow (Qb) was significantly lower. Instantaneous clearance values were significantly lower compared to HDF but similar to those obtained with Theranova membrane. Even if Instantaneous clearance of phosphate was significantly lower in patients receiving HDx with VIE-X membrane, mean Removal Ratio of phosphate was similar to that achived with Theranova. Serum concentration of α1-microglobulin increased during the dialysis session in patients receiving ViE-X membrane, probably due to a low permeability of the dialyzer for this large middle molecule (MW 33KDa).
Different meta-analysis indicated that vitamin E-coated dialyzer can induce a reductions in serum CRP, IL-6, and thiobarbituric acid reactive substance levels in patients receiving haemodialysis[34,35]. This effect of Vitamin E-coated membrane seems to take place during the dialysis treatment but not during interdialytic interval [36]. In our study, even if there wasn’t significant difference of Clearance value of IL-6 between Group 1 and Group 2, mean values were higher in patients undergoing HDx with ViE-X® membrane. However, we found no significant difference of serum concentration or Δ IL-6 between the three groups. We also assessed the potential role of Vitamin E coated membrane in correcting anemia using ERI. We found that the introduction of ViE-X membrane was associated with a progressive reduction of ERI from basal value, in a 3 months therapy. Therefore, ΔERI was higher in comparison with other groups of patients, although it correlated significantly with dialysis vintage but was not influenced by the dialyzer.
One of the strengths of our study was the analysis of four dialysis session with each dialyzer. This allowed us to investigate the short-term performance as well as middle-term effects of three dialyzer and two different dialysis modalities.
A limitation of this study was the small sample size which could have influenced some of our results. Furthermore, dialysis vintage was significantly lower in the group of patients receiving the novel ViE-X membrane and this could have influenced some biological biomarkers. Furthermore, in this study, the comparison with standard High-flux haemodialysis was not performed..
5. Conclusions
To our knowledge, this is one of the few studies that provides data on short and middle-term outcome in patients receiving Expanded Haemodialysis compared to Hemodiafiltration. Using three dialyzers with no significant differences in dialysis adequacy we found that Expanded haemodialysis with Medium Cut-Off membranes without the use of high volume of substitution fluids for the convective dose, reaches dialysis efficacy in terms of in terms of middle-molecules removal and uremic toxins serum concentration. Furthermore, the present study indicates that even if albumin loss is higher during HDx compared to hemodiafiltration, it has no effects on pre-dialysis serum albumin. However, this data needs to be validated by more clinical trials with a larger sample size. Moreover, long-terms biological and clinical benefit of Expanded haemodialysis remains to be investigated.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authorship
Matteo Marcello: conception of the study, collection of data, statistical analysis, interpretation of data and drafting the article. Marco Simonini: statistical analysis and interpretation of data. Anna Lorenzin: collection of data. Grazia Maria Virzì, Valentina Corradi and Carlotta Caprara: laboratory analysis, Alessandra Brendolan, Claudio Ronco and Monica Zanella: providing intellectual content of critical importance to this work. All authors approved the final version of this paper.
Data Availability Statement
Such dataset may be requested from email to Correspondent Author
Acknowledgements
We express our gratefulness to the medical, nursing and secretarial staff from the Nephrology Department, St. Bortolo Hospital, Vicenza. We thank Associazione Amici del Rene Vicenza (A.A.R.VI) ONLUS
Ethical Approval
The protocol and consent form were approved by the Ethics Committee of San Bortolo Hospital (n. (n° 25/21). All patients were informed about the experimental protocol and the objectives of the study before providing informed consent and biological samples.
Conflicting Interest
the Authors declare that there is no conflict of interest. Prof. Claudio Ronco in the last three years has been consultant, medical advisor or part of the speaker bureau receiving fees from the following companies: Asahi Medical, Aferetica, Baxter, B.Braun, Biomerieux, Bioporto, Cytosorbents, ESTOR, Fresenius Medical Care, GE Healthcare, Kaneka, Medica, Medtronic- Bellco, Nipro, Spectral, Toray, Jafron.
References
- Locatelli F, Gauly A, Czekalski S, Hannedouche T, Jacobson SH, Loureiro A, et al. The MPO Study: just a European HEMO Study or something very different? Blood Purif [Internet]. 2008 Jan [cited 2022 Jul 31];26(1):100–4. Available from: https://pubmed.ncbi.nlm.nih.gov/18182806/.
- Kuragano T, Kida A, Furuta M, Nanami M, Otaki Y, Hasuike Y, et al. The impact of beta2-microglobulin clearance on the risk factors of cardiovascular disease in hemodialysis patients. ASAIO J [Internet]. 2010 Jul [cited 2022 Jul 31];56(4):326–32. Available from: https://pubmed.ncbi.nlm.nih.gov/20431482/.
- Nakano T, Matsui M, Inoue I, Awata T, Katayama S, Murakoshi T. Free immunoglobulin light chain: its biology and implications in diseases. Clin Chim Acta [Internet]. 2011 [cited 2022 Jul 31];412(11–12):843–9. Available from: https://pubmed.ncbi.nlm.nih.gov/21396928/.
- Ronco, C. The Rise of Expanded Hemodialysis. Blood Purif [Internet]. 2017 Jun 1 [cited 2022 Aug 7];44(2):I–VIII. Available from: https://www.karger.com/Article/FullText/476012.
- Sakurai, K. Biomarkers for evaluation of clinical outcomes of hemodiafiltration. Blood Purif [Internet]. 2013 Apr 24 [cited 2022 Aug 1];35 Suppl 1:64–8. Available from: https://pubmed.ncbi.nlm.nih.gov/23466382/.
- Scholze A, Jankowski J, Pedraza-Chaverri J, Evenepoel P. Oxidative Stress in Chronic Kidney Disease. Oxid Med Cell Longev [Internet]. 2016 [cited 2022 Aug 7];2016. Available from: https://pubmed.ncbi.nlm.nih.gov/27579156/.
- Lee BT, Ahmed FA, Lee Hamm L, Teran FJ, Chen CS, Liu Y, et al. Association of C-reactive protein, tumor necrosis factor-alpha, and interleukin-6 with chronic kidney disease. BMC Nephrol [Internet]. 2015 [cited 2022 Aug 30];16(1). Available from: /pmc/articles/PMC4449580/.
- Kaltsatou A, Sakkas GK, Poulianiti KP, Koutedakis Y, Tepetes K, Christodoulidis G, et al. Uremic myopathy: is oxidative stress implicated in muscle dysfunction in uremia? Front Physiol [Internet]. 2015 [cited 2022 Aug 7];6(MAR). Available from: https://pubmed.ncbi.nlm.nih.gov/25870564/.
- Aucella F, Gesuete A, Vigilante M, Prencipe M. Adsorption dialysis: from physical principles to clinical applications. Blood Purif [Internet]. 2013 May [cited 2022 Aug 7];35 Suppl 2(SUPPL.2):42–7. Available from: https://pubmed.ncbi.nlm.nih.gov/23676835/.
- Canaud B, Barbieri C, Marcelli D, Bellocchio F, Bowry S, Mari F, et al. Optimal convection volume for improving patient outcomes in an international incident dialysis cohort treated with online hemodiafiltration. Kidney Int [Internet]. 2015 Nov 1 [cited 2022 Aug 8];88(5):1108–16. Available from: https://pubmed.ncbi.nlm.nih.gov/25945407/.
- Tattersall JE, Ward RA. Online haemodiafiltration: definition, dose quantification and safety revisited. Nephrol Dial Transplant [Internet]. 2013 Mar [cited 2022 Aug 10];28(3):542–50. Available from: https://pubmed.ncbi.nlm.nih.gov/23345621/.
- Bradbury BD, Fissell RB, Albert JM, Anthony MS, Critchlow CW, Pisoni RL, et al. Predictors of early mortality among incident US hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol [Internet]. 2007 Jan [cited 2022 Aug 10];2(1):89–99. Available from: https://pubmed.ncbi.nlm.nih.gov/17699392/.
- Smith JR, Zimmer N, Bell E, Francq BG, McConnachie A, Mactier R. A Randomized, Single-Blind, Crossover Trial of Recovery Time in High-Flux Hemodialysis and Hemodiafiltration. Am J Kidney Dis [Internet]. 2017 Jun 1 [cited 2022 Aug 29];69(6):762–70. Available from: http://www.ajkd.org/article/S0272638616306357/fulltext.
- Kirsch AH, Lyko R, Nilsson LG, Beck W, Amdahl M, Lechner P, et al. Performance of hemodialysis with novel medium cut-off dialyzers. Nephrol Dial Transplant [Internet]. 2017 [cited 2022 Aug 19];32(1):165–72. Available from: https://pubmed.ncbi.nlm.nih.gov/27587605/.
- Fiore GB, Ronco C. Principles and practice of internal hemodiafiltration. Contrib Nephrol [Internet]. 2007 Aug 8 [cited 2022 Aug 28];158:177–84. Available from: https://pubmed.ncbi.nlm.nih.gov/17684356/.
- Ronco C, Marchionna N, Brendolan A, Neri M, Lorenzin A, Martínez Rueda AJ. Expanded haemodialysis: from operational mechanism to clinical results. Nephrol Dial Transplant [Internet]. 2018 Oct 1 [cited 2022 Aug 28];33(suppl_3):iii41–7. Available from: https://pubmed.ncbi.nlm.nih.gov/30281134/.
- Leypoldt JK, Cheung AK, Deeter RB. Single compartment models for evaluating beta 2-microglobulin clearance during hemodialysis. ASAIO J [Internet]. 1997 [cited 2022 Aug 15];43(6):904–9. Available from: https://pubmed.ncbi.nlm.nih.gov/9386841/.
- Bergström J, Wehle B. No change in corrected beta 2-microglobulin concentration after cuprophane haemodialysis. Lancet (London, England) [Internet]. 1987 Mar 14 [cited 2022 Aug 15];1(8533):628–9. Available from: https://pubmed.ncbi.nlm.nih.gov/2881162/.
- Chait Y, Kalim S, Horowitz J, Hollot C V., Ankers ED, Germain MJ, et al. The greatly misunderstood erythropoietin resistance index and the case for a new responsiveness measure. Hemodial Int [Internet]. 2016 Jul 1 [cited 2022 Aug 7];20(3):392–8. Available from: https://pubmed.ncbi.nlm.nih.gov/26843352/.
- Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE open Med [Internet]. 2016 Jan 1 [cited 2022 Aug 17];4:205031211667172. Available from: https://pubmed.ncbi.nlm.nih.gov/27757230/.
- Maduell, F. Hemodiafiltration versus conventional hemodialysis: Should “conventional” be redefined? Semin Dial [Internet]. 2018 Nov 1 [cited 2022 Aug 29];31(6):625–32. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/sdi.12715.
- Weiner DE, Falzon L, Skoufos L, Bernardo A, Beck W, Xiao M, et al. Efficacy and Safety of Expanded Hemodialysis with the Theranova 400 Dialyzer: A Randomized Controlled Trial. Clin J Am Soc Nephrol [Internet]. 2020 Sep 7 [cited 2022 Sep 11];15(9):1310–9. Available from: https://pubmed.ncbi.nlm.nih.gov/32843372/.
- Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis [Internet]. 1990 [cited 2022 Sep 11];15(5):458–82. Available from: https://pubmed.ncbi.nlm.nih.gov/2333868/.
- Van Gelder MK, Abrahams AC, Joles JA, Kaysen GA, Gerritsen KGF. Albumin handling in different hemodialysis modalities. Nephrol Dial Transplant [Internet]. 2018 Jun 1 [cited 2022 Sep 11];33(6):906–13. Available from: https://pubmed.ncbi.nlm.nih.gov/29106652/.
- Cozzolino M, Magagnoli L, Ciceri P, Conte F, Galassi A. Effects of a medium cut-off (Theranova®) dialyser on haemodialysis patients: a prospective, cross-over study. Clin Kidney J [Internet]. 2021 Feb 3 [cited 2022 Sep 11];14(1):382–9. Available from: https://academic.oup.com/ckj/article/14/1/382/5621471.
- Krishnasamy R, Hawley CM, Jardine MJ, Roberts MA, Cho Y, Wong M, et al. A tRial Evaluating Mid Cut-Off Value Membrane Clearance of Albumin and Light Chains in HemoDialysis Patients: A Safety Device Study. Blood Purif [Internet]. 2020 Jul 1 [cited 2022 Sep 11];49(4):468–78. Available from: https://pubmed.ncbi.nlm.nih.gov/31968346/.
- Rocco M, Daugirdas JT, Depner TA, Inrig J, Mehrotra R, Rocco M V., et al. KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 Update. Am J Kidney Dis [Internet]. 2015 Nov 1 [cited 2022 Sep 11];66(5):884–930. Available from: http://www.ajkd.org/article/S0272638615010197/fulltext.
- Pstras L, Ronco C, Tattersall J. Basic physics of hemodiafiltration. Semin Dial [Internet]. 2022 [cited 2022 Sep 14]; Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/sdi.13111.
- Lorenzin A, Neri M, Lupi A, Todesco M, Santimaria M, Alghisi A, et al. Quantification of Internal Filtration in Hollow Fiber Hemodialyzers with Medium Cut-Off Membrane. Blood Purif [Internet]. 2018 Jul 1 [cited 2022 Aug 28];46(3):196–204. Available from: https://pubmed.ncbi.nlm.nih.gov/29886489/.
- Maduell, F. Hemodiafiltration versus conventional hemodialysis: Should “conventional” be redefined? Semin Dial [Internet]. 2018 Nov 1 [cited 2022 Sep 13];31(6):625–32. Available from: https://pubmed.ncbi.nlm.nih.gov/29813181/.
- Maduell F, Broseta JJ, Rodas L, Montagud-Marrahi E, Rodriguez-Espinosa D, Hermida E, et al. Comparison of Solute Removal Properties Between High-Efficient Dialysis Modalities in Low Blood Flow Rate. Ther Apher Dial [Internet]. 2020 Aug 1 [cited 2022 Sep 13];24(4):387–92. Available from: https://pubmed.ncbi.nlm.nih.gov/31583845/.
- Maduell F, Broseta JJ, Gómez M, Racionero P, Montagud-Marrahi E, Rodas L, et al. Determining factors for hemodiafiltration to equal or exceed the performance of expanded hemodialysis. Artif Organs [Internet]. 2020 Oct 1 [cited 2022 Sep 13];44(10):E448–58. Available from: https://pubmed.ncbi.nlm.nih.gov/32279348/.
- Lee Y, Jang M jin, Jeon J, Lee JE, Huh W, Choi BS, et al. Cardiovascular Risk Comparison between Expanded Hemodialysis Using Theranova and Online Hemodiafiltration (CARTOON): A Multicenter Randomized Controlled Trial. Sci Rep [Internet]. 2021 Dec 1 [cited 2022 Aug 28];11(1). Available from: https://pubmed.ncbi.nlm.nih.gov/34031503/.
- Yang SK, Xiao L, Xu B, Xu XX, Liu FY, Sun L. Effects of vitamin E-coated dialyzer on oxidative stress and inflammation status in hemodialysis patients: a systematic review and meta-analysis. Ren Fail [Internet]. 2014 [cited 2022 Sep 12];36(5):722–31. Available from: https://www.ncbi.nlm.nih.gov/books/NBK231773/.
- Rodríguez-Ribera L, Corredor Z, Silva I, Díaz JM, Ballarín J, Marcos R, et al. Vitamin E-coated dialysis membranes reduce the levels of oxidative genetic damage in hemodialysis patients. Mutat Res Genet Toxicol Environ Mutagen [Internet]. 2017 Mar 1 [cited 2022 Sep 12];815:16–21. Available from: https://pubmed.ncbi.nlm.nih.gov/28283088/.
- Girndt M, Lengler S, Kaul H, Sester U, Sester M, Köhler H. Prospective crossover trial of the influence of vitamin E-coated dialyzer membranes on T-cell activation and cytokine induction. Am J Kidney Dis [Internet]. 2000 Jan 1 [cited 2022 Aug 29];35(1):95–104. Available from: http://www.ajkd.org/article/S0272638600703076/fulltext.
- Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol [Internet]. 2001 [cited 2022 Aug 29];12(12):2797–806. Available from: https://pubmed.ncbi.nlm.nih.gov/11729250/.
- Ikizler TA, Cano NJ, Franch H, Fouque D, Himmelfarb J, Kalantar-Zadeh K, et al. Prevention and treatment of protein energy wasting in chronic kidney disease patients: a consensus statement by the International Society of Renal Nutrition and Metabolism. Kidney Int [Internet]. 2013 [cited 2022 Aug 29];84(6):1096–107. Available from: https://pubmed.ncbi.nlm.nih.gov/23698226/.
- Mazairac AHA, de Wit GA, Grooteman MPC, Penne EL, van der Weerd NC, den Hoedt CH, et al. Effect of Hemodiafiltration on Quality of Life over Time. Clin J Am Soc Nephrol [Internet]. 2013 Jan 1 [cited 2022 Aug 29];8(1):82–9. Available from: https://cjasn.asnjournals.org/content/8/1/82.
- Alarcon JC, Bunch A, Ardila F, Zuñiga E, Vesga JI, Rivera A, et al. Impact of Medium Cut-Off Dialyzers on Patient-Reported Outcomes: COREXH Registry. Blood Purif [Internet]. 2021 Jan 1 [cited 2022 Aug 29];50(1):110–8. Available from: https://www.karger.com/Article/FullText/508803.

Table 1.
Descriptive analysis.
| HDx | HDF | p-value | |||
| Group | 1 | 2 | 3 | ||
| Filter | VIEX | THERANOVA | Fresenius Cordiax | ||
| Nr of patients (n/%) | 6 /25 | 6 / 25 | 6 / 25 | ||
| AGE (mean ± SD) | 67.6 ± 4.1 | 65.17 ± 7.73 | 70.33 ± 10.1 | ns | |
| SEX (male) (n/ %) | 4 / 66.7 | 4 / 66.7 | 3 / 50 | ns | |
| BMI (mean ± SD) | 27.3 ± 4.3 | 24.67 ± 5.68 | 22.82 ± 1.64 | ns | |
| URINE OUTPUT (n/%) | ns | ||||
| <100 ml | 1 / 16.7 | 1 / 16.7 | 5 / 83.3 | ||
| < 500 ml | 3 / 50 | 4 / 66.7 | 1 / 16.7 | ||
| >500 ml | 2 / 33.3 | 1 / 16.7 | 0 | ||
| DIABETES (n/ %) | 2 / 33.3 | 1 / 16.7 | 3 / 50 | ns | |
| CHARLSON > 6 (n/%) | 3 / 50 | 2 / 33.3 | 3 / 50 | ns | |
| CHARLSON (mean ± SD) | 7.1 ± 0.9 | 5.67 ± 2.16 | 6.83 ± 2.99 | ns | |
| CKD CAUSE (n/%) | ns | ||||
| UNKNOWN | 4/ 66.7 | 1 / 16.7 | 5 / 83.3 | ||
| GLOMERULAR | 2/33.3 | 3 / 50 | 0 | ||
| OBSTRUCTIVE | 0 | 1 / 16.7 | 1 / 16.7 | ||
| ADPKD | 0 | 1 / 16.7 | 0 | ||
| DIALISYS VINTAGE (months) (median/IQR) | 15 [2.5-42.5] | 91 [18.5-113.2] | 149.8 [37-100] | .042 | |
| VASCULAR ACCES (n/%) | ns | ||||
| AVF | 5 / 83.3 | 3 / 50 | 5 / 83.3 | ||
| CVC | 1 / 16.7 | 3 / 50 | 1 / 16.7 | ||
|
Qb (ml/min) (median/IQR) |
290 [281-300] | 300 [287-300] | 300 [300-350] | <0.001 | |
|
Qf (ml/min) (median/IQR) |
13.15 [12.3-14] | 11,8 [7,9-14,3] | 99,1 [85,9-108,2] | <0.001 | |
Table 2.
Effect of different treatment on Albumin loss and Serum Albumin.
|
ALBUMIN LOSS (G) (MEAN/SD) | |
| VIE-X | 2.9/ 0.7 |
| THERANOVA | 3.7/ 0.9 |
| FRESENIUS-FX | 2.5/ 1.1 |
|
SERUM ALBUMIN (G/DL) (MEAN±SD) | |
| VIE-X | |
| T0 | 4.06 / 0.15 |
| T1 | 3.96 / 0.12 |
| T2 | 4.16 / 0.13 |
| T3 | 4.30 / 0.08 |
| THERANOVA | |
| T0 | 3.91 / 0.25 |
| T1 | 3.91 / 0.21 |
| T2 | 3.98 / 0.20 |
| T3 | 4.1 / 0.31 |
| FRESENIUS-FX | |
| T0 | 4.03 / 0.21 |
| T1 | 4.01 / 0.21 |
| T2 | 4.10 / 0.29 |
| T3 | 3.95 / 0.27 |
Table 3.
Kinetics of uremic toxins.
| Vie-X | Theranova | FreseniusFx | p-value | ||
| K Urea (Mean±SD) | I | 258 ± 16 | 258± 15 | 277± 29 | 0.003 |
| F | 212 ± 10 | 199 ± 32 | 222 ± 501 | ns | |
| Δ | 45.6 ± 14.8 | 58.3 ± 34 | 54.5 ± 56.7 | ns | |
| Pre | 60.3 ± 9.6 | 58.0 ± 16.8 | 65.2 ± 14.2 | ns | |
| Post | 15.8 ± 4.9 | 16.2 ± 6.1 | 16.5 ± 5.8 | ns | |
| RR | 72.9 ± 5.1 | 72.1 ± 6.2 | 75.0 ± 4.4 | ns | |
| K Creatinine (Mean±SD) | I | 140 ± 17 | 144 ± 14 | 156 ± 20 | 0.007 |
| F | 133 ± 15 | 145 ± 13 | 151 ± 20 | 0.001 | |
| Δ | 7.3 ± 8.2 | -0.6 ± 11 | 5.4 ± 13.2 | 0.040 | |
| Pre | 8.6 ± 1.5 | 10.0 ± 1.3 | 9.1 ± 1.9 | 0.010 | |
| Post | 3.0 ± 0.7 | 3.4 ± 0.8 | 3.0 ± 0.6 | ns | |
| RR | 65.5 ± 6.3 | 66.3 ± 6.3 | 66.9 ± 5.1 | ns | |
| K Uric Acid (Mean±SD) | I | 132.6 ± 12.5 | 143.7 ± 11 | 157.9 ± 25.7 | ns |
| F | 127.8 ± 6.0 | 133.9 ± 10 | 159.3 ± 26.0 | 0.010 | |
| Δ | 4.8 ± 8.1 | 10.7 ± 8.3 | -1.4 ± 11.8 | ns | |
|
K Phosphate (Mean±SD) |
I | 164.8 ± 12.6 | 174.5± 12.8 | 178.6 ± 13.8 | 0.002 |
| F | 154.1 ± 14.1 | 165.1 ± 11.8 | 169.5 ± 20.2 | 0.004 | |
| Δ | 10.6 ± 10.9 | 9.4 ± 4.1 | 9.0 ± 14.9 | ns | |
| Pre | 4.67 ± 0.7 | 4.69 ± 1.21 | 4.88 ± 0.85 | ns | |
| Post | 1.96 ± 0.95 | 2.03 ± 0.5 | 1.93 ± 0.45 | ns | |
| RR | 58.2 ± 11.2 | 56.1 ± 9.4 | 60.2 ± 7.3 | ns | |
|
K IL-6 (Mean±SD) |
I | 23.1 ± 17.4 | 12.8 ± 8 | 107.0 ± 28.1 | < 0.001 |
| F | 21.4 ± 19.7 | 10.4 ± 6.5 | 107.9 ± 26.0 | < 0.001 | |
| Δ | 1.7 ± 5.5 | 2.3 ± 8.8 | -0.9 ± 4.2 | ns | |
| Pre | 6,93 ± 0.15 | 6.96 ± 0.17 | 6.88 ± 0.16 | ns | |
| Post | 6.86 ± 0.28 | 6.90 ± 0.17 | 6.88 ± 0.07 | ns | |
| RR | 0.9 ± 3.7 | 0.9 ± 2.6 | - 0.05 ± 2.9 | ns | |
|
K β2-microglobulin (Mean±SD) |
I | 75.4 ± 12.6 | 86.9 ±10.1 | 128.5 ± 32.4 | < 0.001 |
| F | 82.0 ± 11.3 | 82.2 ± 14.2 | 110.7 ± 34.6 | < 0.001 | |
| Δ | -6.5 ± 14.1 | 4.2 ± 16.5 | 11.4± 26.8 | 0.013 | |
| Pre | 13.7 ± 2.8 | 16.0 ± 2.9 | 16.5 ± 3.6 | ns | |
| Post | 6.9 ± 1.1 | 7.2 ± 2.2 | 7.5 ± 1.8 | ns | |
| RR | 48.2 ± 8.9 | 55.9 ± 9.3 | 55.7 ± 13.2 | ns | |
|
Kα1-microglobulin (Mean±SD) |
I | 8.8 ± 5.3 | 8.0 ± 7.3 | 101.6 ± 42.1 | < 0.001 |
| F | 9.1 ± 12.3 | 10.9 ± 16.3 | 61.9 ± 36.3 | < 0.001 | |
| Δ | -0.3 ± 13.7 | -2.3 ± 12.6 | 33.0 ± 39.0 | <0.001 | |
| Pre | 222.4 ± 54.1 | 212.7 ± 25.0 | 264.5 ± 22.0 | < 0.001 | |
| Post | 232.4 ± 57.9 | 211.7 ± 33.1 | 254.0 ± 46.8 | 0.012 | |
| RR | - 4.5 ± 5.8 | 0.7 ± 13.2 | 4.5 ± 12.9 | 0.024 | |
|
K Myoglobin (Mean±SD) |
I | 58.3 ± 9.8 | 69.7 ± 11.9 | 94.5 ± 46.1 | < 0.001 |
| F | 45.0 ± 10.5 | 51.6 ± 7.3 | 73.4 ± 30.9 | < 0.001 | |
| Δ | 13.2 ± 12.0 | 18.1 ± 13.6 | 21.1 ± 38.9 | ns | |
| Pre | 196.4 ± 86.2 | 266.6 ± 121 | 198.2 ± 73.8 | 0.005 | |
| Post | 118.9 ± 46.5 | 135.2 ± 47.1 | 123.2 ± 73.5 | ns | |
| RR | 38.1 ± 8.6 | 47.1 ± 9 | 38.6 ± 23.1 | 0.07 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



