Submitted:
19 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Background Stress hyperglycemia may deteriorate stroke outcomes, but the effects of this condition on prognosis of mechanical thrombectomy remain undetermined. This study aimed to evaluate the impacts of stress hyperglycemia on in-hospital and 3-month outcomes of mechanical thrombectomy in stroke patients due to anterior circulation occlusion.
Methods A total of 415 patients undergoing mechanical thrombectomy in the anterior circulation were enrolled. Stress hyperglycemia ratio (SHR) was measured with fasting glucose/glycated hemoglobin ratio and grouped as tertiles (i.e., SHR1–3) to compare in-hospital and 3-month outcomes using multivariable regression models. The effect of SHR stratified by diabetes status and the added value of SHR on the Totaled Health Risks in Vascular Events (THRIVE)-c risk score were also explored.
Results The SHR3 group compared with the SHR1–2 group showed increased 24h symptomatic intracranial hemorrhage (adjusted odds ratio [aOR], 4.088; 95% confidence interval [CI], 1.551–10.772; P = 0.004), increased 72h early neurological deterioration (aOR, 3.505; 95% CI, 1.984–6.192; P < 0.001), and a similar incidence of post-stroke pneumonia (aOR, 1.379; 95% CI, 0.838–2.268; P = 0.206). At three months, patients in the SHR3 group had a worse distribution of modified Rankin scale (aOR, 2.261; 95% CI, 1.495–3.421; P < 0.001), and were at a higher risk of unfavorable functional outcome (adjusted hazard ratio [aHR], 1.629; 95% CI, 1.230–2.158; P = 0.001) and all-cause mortality (aHR, 1.986; 95% CI, 1.235–3.194; P = 0.005). The adverse effects of SHR were more often observed in non-diabetic patients, and including SHR significantly improved the accuracy of the THRIVE-c score for predicting poor stroke outcomes.
Conclusions Stress hyperglycemia is related to the risks of in-hospital and 3-month poor outcomes after receiving mechanical thrombectomy in the anterior circulation.
Keywords:
stress hyperglycemia
; ischemic stroke
; symptomatic intracranial hemorrhage
; early neurological deterioration
; post-stroke pneumonia
; modified Rankin scale
Background
Stress hyperglycemia is defined as hospital-related hyperglycemia without evidence of previous diabetes, or deterioration of glycemic control with pre-existing diabetes[1]. It is a frequent occurrence in response to acute illness, regardless of the diabetes status. Nearly half of patients (45.2%) suffered from stress hyperglycemia in the setting of acute ischemic stroke[2]. To assess the impact of stress-induced hyperglycemia for predicting ischemic stroke outcome, various indicators were tested, among which stress hyperglycemia ratio (SHR) has been recommended in preference to glycemic gap (i.e., absolute increase in glycemia) and concentrations of random or fasting blood glucose[3, 4]. SHR considers previous diabetes and corrects for baseline glycemia. It was calculated as acute blood glucose divided by background glucose levels, yet hitherto without a consensual standard.
Previous study calculated SHR as dividing fasting blood glucose (FBG) by glycated hemoglobin (HbA1c)[5]. FBG is a more reliable glycemic index with minimized effects of diet, and HbA1c could properly reflect the background glucose levels over a two- to three-month period. A few studies used random blood glucose levels at admission, representing the acute change of glucose at an earlier stage of stroke[6]. However, SHR measured by the FBG/HbA1c ratio showed a significant and independent association with poor functional outcomes in patients with acute ischemic stroke, while calculation based on admission random blood glucose did not reach significance[4]. Also, calculating SHR via estimated average glucose derived from HbA1c with the equation “Estimated average glucose = (1.59 × HbA1c) – 2.59” has been used in several studies[7,8,9,10]. According to a recent investigation, SHR defined by the FBG/HbA1c ratio showed a better predictive power for stroke outcomes than definitions drew on this equation [5].
Although mechanical thrombectomy has been established as the first-line treatment for ischemic stroke in the anterior circulation, more than half of the treated patients could not reach functional independence, and the mortality was one in four at 90 days[11]. Hence, a valid prediction model for outcomes following endovascular therapy is necessary to help risk stratification and inform decision-making. A recent systematic overview included 19 prediction models and suggested that The Totaled Health Risks in Vascular Events (THRIVE)-c score had a superior combination of discrimination and calibration in predicting functional outcomes for patients with anterior circulation large vessel occlusions who received endovascular treatment[12]. It was developed on a large cohort[13] and has been externally validated in patients from everyday clinical practice[14] and randomized clinical trials[12]. However, it remains uncertain whether including SHR could improve the predictive ability of THRIVE-c, in light of a prior meta-analysis indicating that higher SHR significantly increased the occurrence of poor outcomes, mortality, neurological deficit, hemorrhagic transformation, and infectious complications in stroke patients[15].
Therefore, this study was conducted in acute ischemic stroke patients receiving endovascular treatment for emergent anterior circulation occlusion to determine 1) the impact of different SHR levels on in-hospital outcomes, including symptomatic intracranial hemorrhage (ICH) at 24h, early neurological deterioration at 72h, and post-stroke pneumonia, 2) the influence of SHR on 3-month functional outcome and all-cause mortality, 3) if these effects were different between patients with and without diabetes, and 4) whether SHR integrated into the THRIVE-c prediction model could better stratify patients with poor outcomes to guide treatment decisions.
Methods
Study design
This retrospective observational study screened consecutive patients between May 2017 and December 2021 from the prospective database in the stroke registry of Nanjing First Hospital, Nanjing Medical University, a Demonstration Advanced Stroke Center certified by the China Stroke Prevention Project Committee, National Health Commission[16]. It was conducted in compliance with the principles of the Declaration of Helsinki and was approved by the research ethics committee of Nanjing First Hospital, Nanjing Medical University, with approval number 20211011-The written informed consent was waived by the committee in view of the retrospective nature of the study, the anonymized evaluation of the registry data, and the procedures being performed as part of the routine clinical care.
Participants
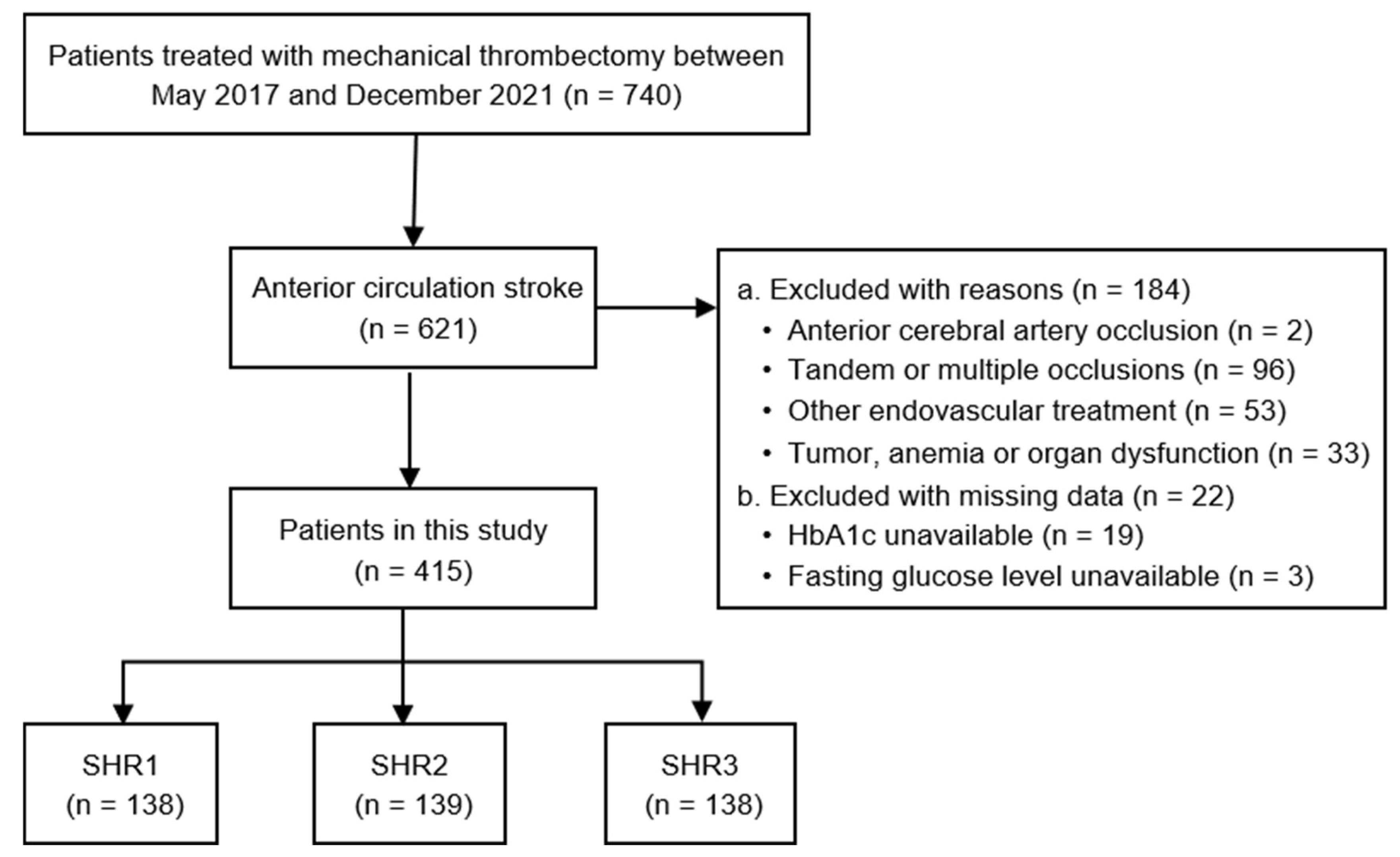
Patients were included if they: (1) were 18 years or older; (2) had an acute ischemic stroke due to large vessel occlusion in the anterior circulation (i.e., middle cerebral artery, MCA; or internal carotid artery, ICA) confirmed by computed tomography angiography or magnetic resonance angiography; (3) received mechanical thrombectomy in accordance with the national guideline. Patients were excluded if they: (1) had tandem or multiple occlusions; (2) had endovascular treatment aside from mechanical thrombectomy, e.g., emergent stent implantation; (3) malignancy, hemoglobin disorders, severe heart, hepatic or renal dysfunction, and (4) missing data on fasting blood glucose or HbA1c levels. A flow diagram of patient selection is provided in Fig. 1.
Figure.
Flow diagram of the study.
Baseline characteristics
Baseline information on demographics and comorbidities was extracted from the stroke registry[16]. The degree of previous functional disability was calculated based on the pre-stroke modified Rankin scale (mRS). The admission blood pressure and stroke severity (assessed by the National Institutes of Health Stroke Scale, NIHSS score) were recorded through face-to-face interviews by neurologists and stroke nurses as part of routine care. Stroke etiology was determined according to the Trial of Org 10,172 in Acute Stroke Treatment (TOAST) criteria. Serum levels of FBG, HbA1c, total cholesterol, triglyceride, low-density lipoprotein cholesterol, blood urea nitrogen (BUN), and estimated glomerular filtration rate (eGFR) were measured within 24 hours of admission at the hospital central laboratory by technicians who were blinded to clinical data. SHR was calculated as FBG (mmol/l)/HbA1c (%) ratio. For further comparisons, we stratified patients into three groups according to tertiles of SHR (i.e., SHR1–3), with the higher SHR indicating more severe stress hyperglycemia.
Reperfusion therapy
Patients eligible for intravenous thrombolysis were treated within a 4.5-hour time window after the onset of stroke symptoms. The indications for endovascular therapy were a target mismatch profile defined as an ischemic core volume of < 70 mL, a perfusion-diffusion mismatch ratio ≥ 1.8 and a mismatch volume ≥ 15 mL after the year 2018; until then, the procedure was performed within 6 h of witnessed stroke onset, and for patients admitted more than 6h of stroke onset, a perfusion-diffusion mismatch ratio ≥ 1.2 with an infarction involving < 1/3 MCA territory was required. The endovascular treatment was performed under conscious sedation and was conducted with stent retrievers or aspiration catheters alone or in combination at the discretion of each operator. The door-to-puncture time (DPT) was calculated. The recanalization status at the end of each procedure was graded using the modified Thrombolysis in Cerebral Infarction (mTICI) scale, with successful recanalization corresponding to a score of 2b-Two experienced neuroradiologists blinded to the clinical outcome reviewed the angiographic data.
Outcomes during hospitalization and 3-month follow-up
In-hospital outcomes included symptomatic ICH at 24h, early neurological deterioration within 72h, and post-stroke pneumonia. Symptomatic ICH was defined as any newly observed intracranial hemorrhage that led to an increase of 4 points or more in the NIHSS score or deterioration that led to death[17]. Early neurological deterioration was defined by an NIHSS increase of ≥ 2 points within 72 hours of hospitalization[18]. Post-stroke pneumonia was defined as the infection of the lower respiratory tract during the first 7 days of hospitalization after stroke onset, based on clinical symptoms, laboratory data, and confirmed with chest CT[19]. The 3-month follow-up outcomes were mRS scores of 3–6 and all-cause mortality during this follow-up period. The mRS is an ordinal scale that measures functional disability after a stroke, ranging from 0 (no symptoms) to 6 (death), of which a score between 3 and 6 indicated functional dependence. The mRS scores were documented within the registry program, as assessed by well-trained neurologists on scheduled interviews by telephone or face-to-face visits.
Statistical analysis
Statistical analyses were performed with SPSS (Version 26.0, IBM Corp., Armonk, NY) and R version 4.2.Baseline characteristics were compared across the three tertiles of SHR. Continuous variables were reported as median with interquartile ranges (IQR) and were compared using the Kruskal-Wallis test. Categorical variables were described as frequencies and percentages, with differences analyzed by the Chi-squared or Fisher exact test as appropriate.
Univariable and multivariable backward stepwise logistic regression analyses were used to examine the associations between the highest tertile of SHR (SHR3) and in-hospital outcomes. The effect variable was the odds ratio (OR) and 95% confidence interval (CI). The effect of SHR3 compared to SHR1–2 on the distribution of the mRS scores at three months was calculated as an adjusted common OR by ordinal shift logistic regression. The comparison of 3-month follow-up data (i.e., mRS 3–6 and all-cause mortality rate) between SHR3 and SHR1–2 groups were assessed by using univariable and multivariable Cox proportional hazards regression models, with hazard ratio (HR) as the effect variable. The multivariable models were adjusted for factors and covariates that were clinically significant or had a significant univariate test, including age, sex, hypertension, diabetes mellitus (DM), atrial fibrillation (AF), pre-stroke mRS score, admission systolic blood pressure, baseline NIHSS, BUN, eGFR, successful recanalization, and door-to-puncture time. The variable of fasting blood glucose was not included as a covariate due to collinearity with SHR tertiles (Spearman correlation coefficient 0.786, P < 0.001).
In order to test the predictive value of SHR3 on the risk of unfavorable outcomes in stroke patients, receiver operating characteristic (ROC) curve analysis was done by adding 1 point of SHR3 or continuous SHR to the THRIVE-c risk score. The THRIVE-c score is calculated as the total sum of continuous age, continuous NIHSS score, and 1 point each for hypertension, DM, and AF[13]. The respective areas under the curve (AUCs) were compared between the SHR3-incorporated and the conventional THRIVE-c risk scores by the Delong test, and ΔAUC was calculated to evaluate the enhanced efficiency of risk prediction by SHRStatistical significance was thresholded for all analyses by a two-sided P value of < 0.05.
Results
Baseline characteristics
A total of 415 patients who underwent thrombectomy in the anterior circulation were included, with a median age of 72.0 (62.0–80.0) years, and 38.6% were women. Patients were grouped according to the SHR tertiles (Table 1). The baseline characteristics showed that older age (Kruskal-Wallis H = 19.110; P < 0.001), female sex (Pearson χ2 = 7.586; P = 0.023), and history of atrial fibrillation (Pearson χ2 = 8.595; P = 0.014) were most frequent in the highest SHR tertile. While other cardiovascular risk factors, including hypertension, diabetes mellitus, and previous stroke or transient ischemic attack, were similar among groups. The SHR3 group, compared to the other groups, had higher admission systolic blood pressure (Kruskal-Wallis H = 7.616; P = 0.022) and NIHSS score (Kruskal-Wallis H = 15.095; P < 0.001), equivalent HbA1c levels, higher FBG (Kruskal-Wallis H = 255.485; P < 0.001) and BUN (Kruskal-Wallis H = 10.726; P = 0.005), and worse eGFR (Kruskal-Wallis H = 12.191; P = 0.002). The use of intravenous alteplase, the occlusion site, and the door-to-puncture time were evenly distributed among the three SHR groups. Meanwhile, patients in the SHR3 group were less likely to achieve successful recanalization than the other two groups (Pearson χ2 = 7.883; P = 0.019).

Table.
Baseline characteristics according to different SHR tertiles.
| Characteristics | SHR tertiles | P | ||||
| SHR1 (≤0.940) | SHR2 (0.940–1.177) | SHR3 (≥1.177) | ||||
| n | 138 | 139 | 138 | |||
| Demography | ||||||
| Age (years) | 69.0 (60.0–76.0) | 71.0 (61.0–80.0) | 76.0 (67.0–82.0) | <0.001 | ||
| Sex (female) | 48 (34.8%) | 46 (33.1%) | 66 (47.8%) | 0.023 | ||
| Comorbidities | ||||||
| Hypertension | 99 (71.7%) | 108 (77.7%) | 98 (71.0%) | 0.384 | ||
| Diabetes mellitus | 42 (30.4) | 37 (26.6%) | 42 (30.4%) | 0.722 | ||
| Atrial fibrillation | 50 (36.2%) | 49 (35.3%) | 70 (50.7%) | 0.014 | ||
| Previous stroke/TIA | 38 (27.5%) | 33 (23.7%) | 30 (21.7%) | 0.522 | ||
| Pre-stroke mRS score ≤2 | 134 (97.1%) | 133 (96.4%) (n=138) | 132 (96.4%) (n=137) | 0.926 | ||
| Admission SBP | 133 (120–150) | 140 (123–157) | 144 (127–159) | 0.022 | ||
| Admission DBP | 83 (76–93) | 86 (76–95) | 86 (74–98) | 0.477 | ||
| Admission NIHSS score | 13 (8–17) | 13 (10–18) | 16 (12–19) | <0.001 | ||
| TOAST | 0.140 | |||||
| LAA | 65 (47.1%) | 68 (48.9%) | 50 (36.2%) | |||
| CE | 59 (42.8%) | 55 (39.6%) | 75 (54.3%) | |||
| Others | 14 (10.1%) | 16 (11.5%) | 13 (9.4%) | |||
| Blood test | ||||||
| FBG (mmol/l) | 4.8 (4.3–5.4) | 6.4 (5.7–6.9) | 8.5 (7.4–10.2) | <0.001 | ||
| HbA1c | 5.9 (5.6–6.8) | 5.9 (5.5–6.4) | 5.9 (5.5–6.6) | 0.495 | ||
| TC (mmol/l) | 4.0 (3.4–4.9) | 4.1 (3.4–4.9) (n=138) | 4.1 (3.5–4.9) (n=136) | 0.627 | ||
| TG | 1.0 (0.7–1.4) | 1.1 (0.8–1.5) (n=138) | 1.0 (0.7–1.5) (n=136) | 0.217 | ||
| LDL | 2.4 (1.9–3.1) | 2.4 (2.0–3.1) (n=138) | 2.4 (1.9–3.0) (n=136) | 0.944 | ||
| BUN (mmol/l) | 4.8 (4.3–5.4) | 6.4 (5.7–6.9) | 8.5 (7.4–10.2) | 0.005 | ||
| eGFR(ml/(min·1.73 m2)) | 78.7 (59.9–98.9) | 75.9 (55.4–105.6) | 65.4 (51.0–88.7) | 0.002 | ||
| Intravenous alteplase | 50 (36.2%) | 54 (38.8%) | 63 (45.7%) | 0.257 | ||
| Occlusion site | 0.496 | |||||
| Intracranial ICA | 42 (30.4%) | 48 (34.5%) | 54 (39.1%) | |||
| The first segment of MCA | 87 (63.0%) | 81 (58.3%) | 72 (52.2%) | |||
| The second segment of MCA | 9 (6.5%) | 10 (7.2%) | 12 (8.7%) | |||
| Mechanical thrombectomy procedure | ||||||
| Door-to-puncture time | 115.0 (88.0–145.0) (n=135) | 110.0 (85.0–135.0) (n=135) | 113.0 (85.0–148.3) (n=134) | 0.819 | ||
| Successful recanalization | 124 (89.9%) | 126 (90.6%) | 111 (80.4%) | 0.019 | ||
| Symptomatic ICH at 24 h | 5 (3.6%) | 4 (2.9%) | 12 (8.7%) | 0.056 | ||
| Early neurological deterioration | 18 (22.8%) | 19 (24.1%) | 42 (53.2%) | <0.001 | ||
| Post-stroke pneumonia | 70 (50.7%) | 89 (64.0%) | 99 (71.7%) | 0.001 | ||
| mRS 3–6 at 3 months | 64 (47.4%) (n=135) | 75 (55.1%) (n=136) | 107 (79.3%) (n=135) | <0.001 | ||
| Death within 3 months | 16 (11.9%) (n=135) | 23 (16.9%) (n=136) | 43 (31.9%) (n=135) | <0.001 | ||
SHR, stress hyperglycemia ratio, calculated as fasting serum glucose/HbA1C; SHR1, first SHR tertile, glucose to HbA1c ratio ≤ 0.940; SHR2, second SHR tertile, glucose to HbA1c ratio 0.940–1.177; SHR3, third SHR tertile, glucose to HbA1c ratio ≥ 1.177; TIA, transient ischemic attack; mRS, modified Rankin scale; SBP, systolic blood pressure; DBP, diastolic blood pressure; NIHSS, National Institute of Neurological Stroke Scale; TOAST, trial of Org 10172 in acute stroke treatment; LAA, large artery atherosclerosis; CE, cardioembolism; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; TC, total cholesterol; TG, triglyceride; LDL, low-density lipoprotein cholesterol; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; ICA, internal carotid artery; MCA, middle cerebral artery; ICH, intracranial hemorrhage.
Clinical outcomes according to SHR tertiles
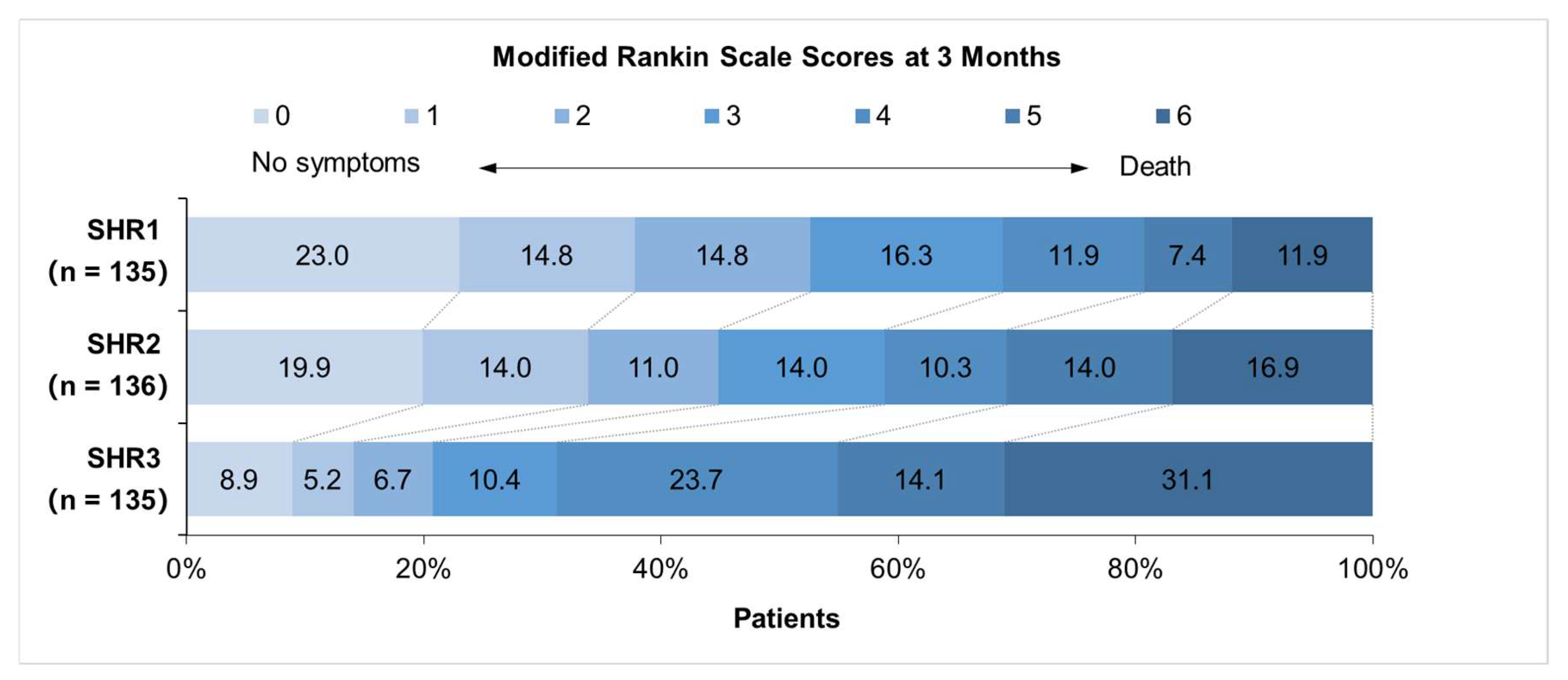
The symptomatic ICH at 24h after endovascular treatment was observed in 5.1% of patients, the rate of which was more predominant in the SHR3 group and reached borderline significance when compared among patients with different SHR tertiles (Pearson χ2 = 5.768; P = 0.056; Table 1). Early neurological deterioration at 72h was seen in 19.0% and post-stroke pneumonia in 62.2% of the total population; both outcomes were more likely to be seen in patients with higher tertiles of SHG (Pearson χ2 = 17.447 and 13.263 respectively; both P ≤ 0.001; Table 1). The SHR3 group when compared with the SHR1–2 group in the multivariable logistic regression model yielded an increased incidence of symptomatic ICH (adjusted OR, 4.088; 95% CI, 1.551–10.772; P = 0.004) and early neurological deterioration (adjusted OR, 3.505; 95% CI, 1.984–6.192; P < 0.001), but a similar incidence of post-stroke pneumonia (adjusted OR, 1.379; 95% CI, 0.838–2.268; P = 0.206; Table 2). A total of 406 patients (97.8%) had 3-month follow-up data, of whom 246 patients (60.6%) had an mRS of 3–6, and 82 all-cause deaths (20.2%) occurred over the follow-up period. Patients with different tertiles of SHG varied in the distribution of 3-month mRS scores. The SHR3 group compared to the SHR1–2 group was associated with higher odds of unfavorable outcomes at 3-month follow-up (adjusted common OR, 2.261; 95% CI, 1.495–3.421; P < 0.001) (Fig. 2). Patients who had higher tertiles of SHG were prone to having an mRS score of 4–6 and a higher proportion of death at 3-month follow-up (Pearson χ2 = 31.218 and 18.121 respectively; both P < 0.001; Table 1). Further multivariable Cox regression models suggested a 1.629-fold increase in the risk of 3-month unfavorable functional outcome (adjusted HR, 1.629; 95% CI, 1.230–2.158; P = 0.001) and a 1.986-fold increase in the risk of 3-month all-cause mortality (adjusted HR, 1.986; 95% CI, 1.235–3.194; P = 0.005) in the third SHR tertile group when compared with the SHR1–2 group (Table 3).
Table.
Associations between SHR3 and in-hospital clinical outcomes.
| SHR1–2 | SHR3 | P | Univariable analysis | Multivariable analysis* | ||||
| OR (95% CI) | P | OR (95% CI) | P | |||||
| Total population | n=277 | n=138 | ||||||
| sICH at 24h | 9 (3.2%) | 12 (8.7%) | 0.017 | 2.836 (1.165–6.905) | 0.022 | 4.088 (1.551–10.772) | 0.004 | |
| END at 72h | 37 (13.4%) | 42 (30.4%) | <0.001 | 2.838 (1.719–4.685) | <0.001 | 3.505 (1.984–6.192) | <0.001 | |
| post-stroke pneumonia | 159 (57.4%) | 99 (71.7%) | 0.005 | 1.884 (1.213–2.927) | 0.005 | 1.379 (0.838–2.268) | 0.206 | |
| DM | n=79 | n=42 | ||||||
| sICH at 24h | 2 (2.5%) | 5 (11.9%) | 0.048 | |||||
| END at 72h | 10 (12.7%) | 10 (23.8%) | 0.116 | 2.156 (0.816–5.697) | 0.121 | 2.533 (0.810–7.920) | 0.110 | |
| post-stroke pneumonia | 49 (62.0%) | 27 (64.3%) | 0.807 | 1.102 (0.506–2.399) | 0.807 | 1.018 (0.424–2.444) | 0.968 | |
| Non-DM | n=198 | n=96 | ||||||
| sICH at 24h | 7 (3.5%) | 7 (7.3%) | 0.240 | |||||
| END at 72h | 27 (13.6%) | 32 (33.3%) | <0.001 | 3.167 (1.760–5.697) | <0.001 | 5.313 (2.332–12.104) | <0.001 | |
| post-stroke pneumonia | 110 (55.6%) | 72 (75.0%) | 0.001 | 2.400 (1.398–4.120) | 0.001 | 4.089 (2.071–8.074) | <0.001 | |
SHR, stress hyperglycemia ratio; OR, odds ratio; CI confidence interval; sICH, symptomatic intracranial hemorrhage; END, early neurological deterioration; PSP, post-stroke pneumonia; DM, diabetes mellitus; Non-DM, non-diabetes mellitus. *Adjusted for age, sex, hypertension, diabetes mellitus, atrial fibrillation, pre-stroke mRS score, admission systolic blood pressure, baseline NIHSS, blood urea nitrogen, estimated glomerular filtration rate, successful recanalization, and door-to-puncture time.
Table.
Associations between SHR3 and 3 months clinical outcomes.
| SHR1–2 | SHR3 | P | Univariable analysis | Multivariable analysis | ||||
| HR (95% CI) | P | HR (95% CI) | P | |||||
| Total population | n=271 | n=135 | ||||||
| mRS 3–6 at 3 months | 139 (51.3%) | 107 (79.3%) | <0.001 | 1.799 (1.393–2.324) | <0.001 | 1.629 (1.230–2.158) | 0.001 | |
| Death within 3 months | 39 (14.4%) | 43 (31.9%) | <0.001 | 2.460 (1.573–3.848) | <0.001 | 1.986 (1.235–3.194) | 0.005 | |
| DM | n=75 | n=42 | ||||||
| mRS 3–6 at 3 months | 49 (65.3%) | 32 (76.2%) | 0.222 | 1.518 (0.962–2.395) | 0.073 | 1.587 (0.989–2.547) | 0.056 | |
| Death within 3 months | 11 (14.7%) | 13 (31.0%) | 0.036 | 2.492 (1.076–5.770) | 0.033 | 3.020 (1.219–7.484) | 0.017 | |
| Non-DM | n=196 | n=93 | ||||||
| mRS 3–6 at 3 months | 90 (45.9%) | 75 (80.6%) | <0.001 | 1.937 (1.419–2.645) | <0.001 | 1.600 (1.128–2.270) | 0.008 | |
| Death within 3 months | 28 (14.3%) | 30 (32.3%) | <0.001 | 2.346 (1.376–4.001) | 0.002 | 1.795 (1.007–3.200) | 0.047 | |
SHR, stress hyperglycemia ratio; HR, hazard ratio; CI confidence interval; mRS, modified Rankin scale; DM, diabetes mellitus; Non-DM, non-diabetes mellitus. *Adjusted for age, sex, hypertension, diabetes mellitus, atrial fibrillation, pre-stroke mRS score, admission systolic blood pressure, baseline NIHSS, blood urea nitrogen, estimated glomerular filtration rate, successful recanalization, and door-to-puncture time.
Impact of diabetes status on the association between SHR tertiles and outcomes
Interestingly, in patients with known diabetes, a higher SHR level did not pose a significantly higher risk of either early neurological deterioration (adjusted OR, 2.533; 95% CI, 0.810–7.920; P = 0.110) or post-stroke pneumonia (adjusted OR, 1.018; 95% CI, 0.424–2.444; P = 0.968). However, significantly higher risks of SHR3 were shown in those without diabetes, both for early neurological deterioration (adjusted OR, 5.313; 95% CI, 2.332–12.104; P < 0.001) and post-stroke pneumonia (adjusted OR, 4.089; 95% CI, 2.071–8.074; P < 0.001). Due to the small sample size of subgroups, the results for the impact of diabetes status on symptomatic ICH were lacking. Further to this, the follow-up findings showed that the association between SHR3 and the 3-month unfavorable outcome reached only borderline significance in diabetes patients (adjusted HR, 1.587; 95% CI, 0.989–2.547; P = 0.056) but was statistically significant in non-diabetic patients (adjusted HR, 1.600; 95% CI, 1.128–2.270; P = 0.008). Meanwhile, the independently significant correlations between SHR3 and 3-month all-cause mortality were consistently observed in diabetic (adjusted HR, 3.020; 95% CI, 1.219–7.484; P = 0.017) and non-diabetic patients (adjusted HR, 1.795; 95% CI, 1.007–3.200; P = 0.047).
Added predictive value of SHR for outcomes during hospitalization and 3-month follow-up
The THRIVE-c score is a simple tool for predicting prognosis after endovascular treatment in stroke patients. In the ROC analysis, the AUC of the THRIVE-c risk score was 0.564 for symptomatic ICH, 0.525 for early neurological deterioration, 0.669 for post-stroke pneumonia, 0.744 for the 3-month unfavorable outcome, and 0.690 for all-cause death at 3-month follow-up (Table 4). When SHR was included in the risk score with a value of 1 point for SHR3 or continuous SHR, the AUC estimated by the Delong test improved significantly compared to the original THRIVE-c score for symptomatic ICH (including SHR3: ∆AUC 0.011; P = 0.040; including continuous SHR: ∆AUC 0.072; P = 0.020), early neurological deterioration (including SHR3: ∆AUC 0.005; P = 0.001; including continuous SHR: ∆AUC 0.042; P < 0.001), but non-significantly for post-stroke pneumonia (including SHR3: ∆AUC 0.007; P = 0.311; including continuous SHR: ∆AUC 0.018; P = 0.195). SHR also enhanced predictive value of THRIVE-c for unfavorable outcome (including SHR3: ∆AUC 0.007; P = 0.001; including continuous SHR: ∆AUC 0.022; P = 0.040) and all-cause mortality (including SHR3: ∆AUC 0.006; P = 0.005; including continuous SHR: ∆AUC 0.041; P = 0.007) at 3-month follow-up (Table 4).
Table.
The added predictive value of SHR on THRIVE-c risk score for stroke outcomes.
| AUC (95% CI) | ΔAUC | P | |
| Symptomatic ICH at 24h | |||
| THRIVE-c | 0.564 (0.465–0.663) | - | - |
| THRIVE-c + SHR3 | 0.575 (0.460–0.690) | 0.011 | 0.040 |
| THRIVE-c + SHR-c | 0.636 (0.510–0.763) | 0.072 | 0.020 |
| Early neurological deterioration at 72h | |||
| THRIVE-c | 0.525 (0.453–0.596) | - | - |
| THRIVE-c + SHR3 | 0.530 (0.462–0.598) | 0.005 | 0.001 |
| THRIVE-c + SHR-c | 0.572 (0.497–0.678) | 0.042 | <0.001 |
| Post-stroke pneumonia | |||
| THRIVE-c | 0.669 (0.617–0.721) | - | - |
| THRIVE-c + SHR3 | 0.676 (0.622–0.729) | 0.007 | 0.311 |
| THRIVE-c + SHR-c | 0.687 (0.635–0.740) | 0.018 | 0.195 |
| mRS 3–6 at 3 months | |||
| THRIVE-c | 0.744 (0.697–0.791) | - | - |
| THRIVE-c + SHR3 | 0.751 (0.703–0.799) | 0.007 | 0.001 |
| THRIVE-c + SHR-c | 0.766 (0.720–0.813) | 0.022 | 0.040 |
| Death within 3 months | |||
| THRIVE-c | 0.690 (0.631–0.750) | - | - |
| THRIVE-c + SHR3 | 0.696 (0.635–0.758) | 0.006 | 0.005 |
| THRIVE-c + SHR-c | 0.731 (0.671–0.792) | 0.041 | 0.007 |
DeLong's test for two correlated ROC curves. SHR, stress hyperglycemia ratio; THRIVE-c, the Totaled Health Risks in Vascular Events (THRIVE)-c risk score; AUC, area under the curve; ICH, intracranial hemorrhage; mRS, modified Rankin scale.
Figure.
Distribution of 3-month mRS stratified by SHR tertiles.
Discussion
This study indicated that patients in the highest tertile of SHR were more likely to suffer from symptomatic ICH at 24h and early neurological deterioration at 72h, meanwhile having less functional independence and a higher risk of mortality within three months of follow-up. Subgroup analyses showed that stress hyperglycemia was significantly associated with adverse outcomes of early neurological deterioration, post-stroke pneumonia, and poor functional outcome at 3-month in non-diabetic patients but not in diabetic patients; in contrast, the relationship between SHR and 3-month all-cause mortality existed regardless of the presence or absence of diabetes. Including SHR significantly improved the predictive accuracy of the THRIVE-c score for symptomatic ICH at 24h, early neurological deterioration within 72h, and the functional outcome and all-cause mortality during the 3-month follow-up period.
The acute rise in blood glucose levels is an evolutionarily adaptive response to stress and injury. It is caused by activating the hypothalamic-pituitary-adrenal axis and the sympathoadrenal system, which raises circulating glucose levels via enhanced gluconeogenesis, glycogenolysis, and insulin resistance[20]. The transient increase in glucose can serve as a ready energy source for the brain and immune system[20]. However, it may also promote platelet hyperactivity, coagulopathy, and endothelial dysfunction, favoring thrombotic and inflammatory processes, thus leading to an exacerbated neurovascular injury[21]. Stress hyperglycemia has widely been proven to be a strong predictor of a poor prognosis in acute ischemic stroke patients[2–10, 22–32], even in those who received first-line therapy of intravenous thrombolysis[4–6, 29] and mechanical thrombectomy[2, 7–9, 24–27].
The present study first explored the relation between stress hyperglycemia and adverse events during hospitalization in patients with anterior circulation ischemic stroke who received mechanical thrombectomy. Our findings suggested that a higher SHR could pose a significant risk for symptomatic ICH and early neurological deterioration. Consistently, an increased risk for symptomatic ICH due to stress hyperglycemia has been reported in recent work which recruited stroke patients admitted within seven days of onset[31], patients after endovascular therapy in the anterior[24, 27] and posterior[9] circulation, as well as those receiving intravenous thrombolysis[5]. Meanwhile, the relationship between SHR and early neurological deterioration was similarly observed in strokes due to large vessel occlusion[26] or a single subcortical infarction[10]. Furthermore, there was a clear trend that patients with higher SHR levels were more likely to experience post-stroke pneumonia; however, it did not reach statistical significance after adjustment, though a previous report indicated that SHR was independently related to post-stroke pneumonia[30].
Next, this study evaluated the effect of SHR on the functional outcome and mortality within 3-month of follow-up in patients with anterior circulation stroke after mechanical thrombectomy. Our data exhibited that high levels of SHR were independently correlated with poor 3-month functional outcomes. In line with our results, prior investigations have highlighted SHR as a risk factor for 3-month poor mRS in stroke patients undergoing mechanical thrombectomy in the anterior[2, 7, 25, 27] and posterior[9, 24, 26] circulation, in those receiving thrombolysis[4], and in patients with single subcortical infarction[10]. Besides, we found that severe stress hyperglycemia significantly increased risks of 3-months all-cause mortality in this cohort of patients. Our study concurred with all recent studies, implying that SHR can be a valid predictor for 3-month mortality among patients receiving mechanical thrombectomy[8, 24, 27]. However, conclusions were controversial for patients treated with intravenous thrombolysis, and more research is needed on whether SHR was an independent contributor to 3-month mortality in these patients[4, 5].
Both non-diabetic and diabetic patients suffering an acute stroke may develop stress hyperglycemia, with high incidences ranging from 8% to 63% for non-diabetic patients, and from 39% to 83% for diabetic patients[33]. Notably, our results showed that the effects of SHR varied according to the premorbid diabetic status; that is, non-diabetic patients who had stress hyperglycemia were facing worse consequences. Likewise, SHR has been linked to adverse post-stroke outcomes in the non-diabetic subgroup rather than the diabetic subgroup in patients with vertebrobasilar artery occlusion who received endovascular treatment[9]. One possible reason is that in diabetes patients, the diabetes medications (e.g., pioglitazone) have a protective effect against stroke[34]. However, others argued that stress hyperglycemia was an epiphenomenon of most severe strokes and rather the severity of the stroke that led to worse outcomes[35]. Meanwhile, another study showed no interactions between SHR and diabetes status to predict 3-month functional recovery and all-cause mortality after thrombectomy for anterior circulation stroke[27]. Hence, future prospective studies are warranted to determine the interactive effect of comorbid diabetes and SHR on stroke prognosis, and if prior diabetes carries an effect of neuroprotection in the setting of post-stroke stress hyperglycemia.
The THRIVE-c risk score is a recently validated tool that is accurate and patient-specific for outcome prediction in endovascular stroke treatment[12]. We compared the original THRIVE-c prediction score with a new score that either included the continuous SHR or the SHR3 as a value of 1 point; both showed better stratification of patients with symptomatic ICH, early neurological deterioration, 3-month poor functional outcome and all-cause mortality. The detrimental effects triggered by stress hyperglycemia in stroke patients might have several explanations. Firstly, the aggravated risk of hemorrhagic transformation by high levels of SHR may be attributable to mitochondrial dysfunction[36] and oxidative stress[37] in endothelial cells, resulting in endothelial dysfunction, hyperpermeability, apoptosis, and inflammatory infiltration[31]. Secondly, the increased risk of early neurological deterioration in stroke patients who had high-stress hyperglycemia can be explained by an exacerbation of anaerobic metabolism, neurovascular injury, and thrombo-inflammation in hyperglycemic patients[21], promoting infarct growth, collateral failure, and hemorrhagic transformation[26]. Lastly, the effect of SHR on the outcomes at 3-month follow-up not merely shared the mechanisms underlying the in-hospital complications, but also stress hyperglycemia played a causative role in atherosclerotic plaque progression[38] and had a higher hazard of subsequent stroke despite dual antiplatelet therapy[39], contributing to the decreased likelihood of favorable outcomes and increased likelihood of mortality at follow-up.
Several limitations should be considered in the interpretation of our findings. First, our retrospective design may be subject to selection bias, and uncontrolled confounders are possible. Hence, the study results need replication in settings with prospective designs. Second, the duration of follow-up was restricted to the first three months after the event. However, this is the most critical period for functional recovery. Further long-term follow-up studies are required to verify our results. Third, as SHR is an indicator of stress response, we only focused on SHR at the acute stage of stroke; whether dynamic changes of SHR at a 3-month follow-up period will affect stroke prognosis warrants further investigation. Fourth, the protective effects of anti-diabetic drugs against stress hyperglycemia were not assessed due to the incomplete data on the medication history in these patients. Finally, given the exploratory nature of our observational study and the conflicting results of strict glucose control[40], the optimal management of stress hyperglycemia and target range of glycemic control remained to be elucidated.
Conclusions
This study adds to the growing body of evidence that stress hyperglycemia is associated with poor outcomes in the setting of ischemic stroke. SHR included in the risk prediction model had improved accuracy for adverse events during hospitalization and at 3-month follow-up for stroke patients receiving mechanical thrombectomy in the anterior circulation. Further studies are required to develop a tailored intervention for SHR and facilitate a mechanistic understanding both for nondiabetic and diabetic stroke patients to achieve enhanced functional recovery.
Author Contributions
Conceptualization: G.X., J.G. and X.C.; Methodology: J.G., Q.H., and M.G.; Formal analysis and investigation: J.G., X.C. and Q.H.; Validation: Q.H. and Y.H.; Writing - original draft preparation: J.G., X.C. and Q.H.; Writing - review and editing: All; Funding acquisition: X.C. and G.X.; Supervision: G.X.
Funding
This study was supported by the Medical Science and Technology Program of Nanjing to X.C. (JQX20007) and the National Natural Science Foundation of China to G.X. (82171330).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. It is approved by the research ethics committee of Nanjing First Hospital, Nanjing Medical University, with approval number 20211011-05.
Informed Consent Statement
The written informed consent was waived by the committee in view of the retrospective nature of the study, the anonymized evaluation of the registry data, and the procedures being performed as part of the routine clinical care.
Data Availability Statement
The anonymized data analyzed during this study are available from the corresponding authors upon reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare that they have no competing interests.
List of abbreviations
AF atrial fibrillation
AUCs areas under the curve
BUN blood urea nitrogen
CI confidence interval
DM diabetes mellitus
DPT door-to-puncture time
eGFR estimated glomerular filtration rate
FBG fasting blood glucose
HbA1c glycated hemoglobin
HR hazard ratio
ICA internal carotid artery
ICH intracranial hemorrhage
IQR interquartile ranges
OR odds ratio
MCA middle cerebral artery
mRS modified Rankin scale
mTICI the modified Thrombolysis in Cerebral Infarction
NIHSS the National Institutes of Health Stroke Scale
ROC receiver operating characteristic
SHR stress hyperglycemia ratio
THRIVE Totaled Health Risks in Vascular Events
TOAST the Trial of Org 10,172 in Acute Stroke Treatment
References
- Dungan K, Braithwaite S, Preiser J. Stress hyperglycaemia. Lancet. 2009;373:1798–807.
- Sun Y, Guo Y, Ji Y, Wu K, Wang H, Yuan L, et al. New stress-induced hyperglycaemia markers predict prognosis in patients after mechanical thrombectomy. BMC Neurol. 2023;23:132. [CrossRef]
- Roberts G, Sires J, Chen A, Thynne T, Sullivan C, Quinn S, et al. A comparison of the stress hyperglycemia ratio, glycemic gap, and glucose to assess the impact of stress-induced hyperglycemia on ischemic stroke outcome. J Diabetes. 2021;13:1034–42.
- Chen G, Ren J, Huang H, Shen J, Yang C, Hu J, et al. Admission random blood glucose, fasting blood glucose, stress hyperglycemia ratio, and functional outcomes in patients with acute ischemic stroke treated with intravenous thrombolysis. Front Aging Neurosci. 2022;14:782282. [CrossRef]
- Shen C, Xia N, Wang H, Zhang W. Association of stress hyperglycemia ratio with acute ischemic stroke outcomes post-thrombolysis. Front Neurol. 2021;12:785428. [CrossRef]
- Li G, Wang C, Wang S, Hao Y, Xiong Y, Zhao X. Clinical significance of stress hyperglycemic ratio and glycemic gap in ischemic stroke patients treated with intravenous thrombolysis. Clin Interv Aging. 2022;17:1841–9. [CrossRef]
- Chen X, Liu Z, Miao J, Zheng W, Yang Q, Ye X, et al. High stress hyperglycemia ratio predicts poor outcome after mechanical thrombectomy for ischemic stroke. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc. 2019;28:1668–73. [CrossRef]
- Wang L, Zhou Z, Tian X, Wang H, Yang D, Hao Y, et al. Impact of relative blood glucose changes on mortality risk of patient with acute ischemic stroke and treated with mechanical thrombectomy. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc. 2019;28:213–9. [CrossRef]
- Gu M, Fan J, Xu P, Xiao L, Wang J, Li M, et al. Effects of perioperative glycemic indicators on outcomes of endovascular treatment for vertebrobasilar artery occlusion. Front Endocrinol. 2022;13:1000030. [CrossRef]
- Liu H, Yao Y, Zhang K, Zong C, Yang H, Li S, et al. Stress hyperglycemia predicts early neurological deterioration and poor outcomes in patients with single subcortical infarct. Diabetes Res Clin Pract. 2023;200:110689. [CrossRef]
- Zi W, Wang H, Yang D, Hao Y, Zhang M, Geng Y, et al. Clinical effectiveness and safety outcomes of endovascular treatment for acute anterior circulation ischemic stroke in China. Cerebrovasc Dis. 2017;44:248–58. [CrossRef]
- Kremers F, Venema E, Duvekot M, Yo L, Bokkers R, Lycklama À. Nijeholt G, et al. Outcome prediction models for endovascular treatment of ischemic stroke: systematic review and external validation. Stroke. 2022;53:825–36.
- Flint A, Rao V, Chan S, Cullen S, Faigeles B, Smith W, et al. Improved ischemic stroke outcome prediction using model estimation of outcome probability: the THRIVE-c calculation. Int J Stroke. 2015;10:815–21.
- Kastrup A, Brunner F, Hildebrandt H, Roth C, Winterhalter M, Gießing C, et al. THRIVE score predicts clinical and radiological outcome after endovascular therapy or thrombolysis in patients with anterior circulation stroke in everyday clinical practice. Eur J Neurol. 2017;24:1032–9. [CrossRef]
- Huang Y, Yin X, Li Z. Association of the stress hyperglycemia ratio and clinical outcomes in patients with stroke: A systematic review and meta-analysis. Front Neurol. 2022;13:999536.
- Shen Y, Chao B, Cao L, Tu W, Wang L. Stroke center care and outcome: results from the CSPPC Stroke Program. Transl Stroke Res. 2020;11:377–86.
- Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–29. [CrossRef]
- Siegler J, Martin-Schild S. Early neurological deterioration (END) after Stroke: The END depends on the definition. Int J Stroke. 2011;6:211–2.
- Smith C, Kishore A, Vail A, Chamorro A, Garau J, Hopkins S, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46:2335–40.
- Sharma K, Akre S, Chakole S, Wanjari M. Stress-induced diabetes: a review. Cureus. 14:e29142. [CrossRef]
- Ferrari F, Moretti A, Villa R. Hyperglycemia in acute ischemic stroke: physiopathological and therapeutic complexity. Neural Regen Res. 2021;17:292–9.
- Pan Y, Cai X, Jing J, Meng X, Li H, Wang Y, et al. Stress hyperglycemia and prognosis of minor ischemic stroke and transient ischemic attack: the CHANCE study (Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events). Stroke. 2017;48:3006–11.
- Tziomalos K, Dimitriou P, Bouziana S, Spanou M, Kostaki S, Angelopoulou S, et al. Stress hyperglycemia and acute ischemic stroke in-hospital outcome. Metabolism. 2017;67:99–105. [CrossRef]
- Merlino G, Pez S, Gigli GL, Sponza M, Lorenzut S, Surcinelli A, et al. Stress hyperglycemia in patients with acute ischemic stroke due to large vessel occlusion undergoing mechanical thrombectomy. Front Neurol. 2021;12:725002.
- Peng Z, Song J, Li L, Guo C, Yang J, Kong W, et al. Association between stress hyperglycemia and outcomes in patients with acute ischemic stroke due to large vessel occlusion. CNS Neurosci Ther. [CrossRef]
- Dai Z, Cao H, Wang F, Li L, Guo H, Zhang X, et al. Impacts of stress hyperglycemia ratio on early neurological deterioration and functional outcome after endovascular treatment in patients with acute ischemic stroke. Front Endocrinol. 2023;14:1094353. [CrossRef]
- Zhang J, Dong D, Zeng Y, Yang B, Li F, Chen X, et al. The association between stress hyperglycemia and unfavorable outcomes in patients with anterior circulation stroke after mechanical thrombectomy. Front Aging Neurosci. 2022;14:1071377.
- Wang Y, Fan H, Duan W, Ren Z, Liu X, Liu T, et al. Elevated stress hyperglycemia and the presence of intracranial artery stenosis increase the risk of recurrent stroke. Front Endocrinol. 2022;13:954916. [CrossRef]
- Wang L, Cheng Q, Hu T, Wang N, Wei X, Wu T, et al. Impact of stress hyperglycemia on early neurological deterioration in acute ischemic stroke patients treated with intravenous thrombolysis. Front Neurol. 2022;13.
- Tao J, Hu Z, Lou F, Wu J, Wu Z, Yang S, et al. Higher stress hyperglycemia ratio is associated with a higher risk of stroke-associated pneumonia. Front Nutr. 2022;9:784114.
- Yuan C, Chen S, Ruan Y, Liu Y, Cheng H, Zeng Y, et al. The stress hyperglycemia ratio is associated with hemorrhagic transformation in patients with acute ischemic stroke. Clin Interv Aging. 2021;16:431–42. [CrossRef]
- Yang C, Liao W, Wang J, Tsai C, Lee J, Peng G, et al. Usefulness of glycated hemoglobin A1c-based adjusted glycemic variables in diabetic patients presenting with acute ischemic stroke. Am J Emerg Med. 2017;35:1240–6.
- Capes S, Hunt D, Malmberg K, Pathak P, Gerstein H. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients. Stroke. 2001;32:2426–32. [CrossRef]
- Mosenzon O, Cheng A, Rabinstein A, Sacco S. Diabetes and stroke: what are the connections? J Stroke. 2023;25:26–38.
- Muscari A, Falcone R, Recinella G, Faccioli L, Forti P, Pastore Trossello M, et al. Prognostic significance of diabetes and stress hyperglycemia in acute stroke patients. Diabetol Metab Syndr. 2022;14:126.
- Qu K, Yan F, Qin X, Zhang K, He W, Dong M, et al. Mitochondrial dysfunction in vascular endothelial cells and its role in atherosclerosis. Front Physiol. 2022;13:1084604. [CrossRef]
- González P, Lozano P, Ros G, Solano F. Hyperglycemia and oxidative stress: an integral, updated and critical overview of their metabolic interconnections. Int J Mol Sci. 2023;24:9352.
- Mastrogiacomo L, Ballagh R, Venegas-Pino DE, Kaur H, Shi P, Werstuck GH. The effects of hyperglycemia on early endothelial activation and the initiation of atherosclerosis. Am J Pathol. 2023;193:121–33.
- Mac Grory B, Piccini J, Yaghi S, Poli S, De Havenon A, Rostanski S, et al. Hyperglycemia, risk of subsequent stroke, and efficacy of dual antiplatelet therapy: a post hoc analysis of the POINT trial. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. 2022;11:e023223.
- Johnston K, Bruno A, Pauls Q, Hall C, Barrett K, Barsan W, et al. Intensive vs standard treatment of hyperglycemia and functional outcome in patients with acute ischemic stroke: the SHINE randomized clinical trial. JAMA. 2019;322:326–35.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



