Submitted:
13 February 2025
Posted:
14 February 2025
You are already at the latest version
Abstract
With the successful deployment of several mRNA vaccines against SARS-CoV2, an mRNA vaccine against RSV (respiratory syncytial virus) and a large pipeline of mRNA products against other infectious diseases, cancers and rare diseases, it is important to examine the whole product lifecycle. mRNA technology enables product design, testing and manufacturing systems to be rapidly developed, but these advantages can be lost if other factors that determine public access are not closely considered. This review analyzes key aspects of the mRNA product lifecycle including candidate design, manufacturing, quality systems and product safety and storage. Regulatory thinking is well advanced in some countries but not others, but more thought on regulation of mRNA vaccines outside of a pandemic situation as well as mRNA therapeutics including individual neoantigen therapies and rare disease treatments is needed. Consumer acceptance - the “social license to operate” around mRNA products - is critical for their uptake, particularly outside of a pandemic.
Keywords:
mRNA
; vaccine development
; regulation
; safety
; life cycle
; platform technology
1. Introduction
The development of mRNA vaccines and therapeutics has demonstrated a number of advantages in product research and development and in consistency of development processes and production that is readily scaled to suit the size of the patient cohort and product demand. The technology has proven broadly applicable to include both single protein products (e.g., as in monovalent COVID-19 vaccines or single enzyme replacement therapies), complex proteins (e.g., multiple sequences in CMV vaccines or individual neoantigen oncology therapies) or combinations of proteins (e.g., in seasonal influenza – COVID-19 vaccines). By being able to identify the appropriate antigen and/or most immunogenic epitopes in products as different as a vaccine for RSV or an individualized neoantigen therapy for melanoma, mRNA technology has demonstrated wide applicability and a high chance of technical success. Similarly, for monogenic rare diseases, identification of the mechanism of the disease where it can be attributed to a missing or malfunctioning enzyme or other protein in a metabolic pathway also enables the targeting of mRNA therapeutics.
Application of platform technology [1] has also facilitated product research and development and manufacture and promises to streamline regulatory review. There are a range of definitions of platform technology used internationally, and the concept is applied to a wider range of products outside mRNA vaccines and therapeutics. For example, the US Food Drug and Cosmetic Act defines platform technology as “a well-understood and reproducible technology, which may include a nucleic acid sequence, molecular structure, mechanism of action, delivery method, vector or a combination of any such technologies that FDA determines to be appropriate, where the sponsor demonstrates that the technology: is incorporated in or used by a drug/biological product and is essential to the structure or function of such drug/biological; can be adapted/incorporated/used by more than one drug or biological product sharing common structural elements; (and) facilitates the manufacture or development of more than one drug/biological product through a standardized … process”.
The development of mRNA vaccines and therapeutics is very similar for very different diseases and conditions, with similar mRNA sequence backbone and the same lipid nanoparticle technology utilized in different products within a therapeutic area, and the only significant change being in the antigen-encoding mRNA sequence. This enables the experience with manufacturing, quality controls/ analytical testing and preclinical testing (such as biodistribution and toxicology studies) to be adapted for other products [1]. Cell-free manufacturing of the mRNA sequence from a DNA template, the microgram doses of mRNA products (rather than gram-scale doses required for many monoclonal antibody therapeutics), and similarities in manufacturing processes between mRNA products for very different indications provides for fast, flexible and well-controlled manufacturing. mRNA manufacturing at a comparably modest physical scale has enabled the manufacture of billions of doses of COVID-19 vaccines and enables a move away from product-dedicated pharmaceutical and vaccine manufacturing plants that were a model for the pharma industry for some decades.
The focus of this review is on mRNA product development, regulation and deployment across the lifecycle. The authors are aware that the term “lifecycle” as applied to pharmaceuticals and vaccines can mean different things to different people. Taking a focus on manufacturing, in the case of mRNA products, lifecycle could be taken as the steps from DNA plasmid cloning, transformation, plasmid purification, linearization, mRNA transcription and modification, mRNA purification, encapsulation of mRNA in the LNP and the steps from drug substance purification through to drug product production [2]. In a commercial sense, pharmaceutical product lifecycles may begin with conceptualization of the unmet therapeutic need, research and development to establish intellectual capital, preclinical and clinical development, regulatory approval, reimbursement and marketing, through to loss of exclusivity of the innovator product, establishment of generic competition and potential withdrawal from the market. From a regulatory sense, the lifecycle can be seen more narrowly as the steps of drug discovery and development, preclinical research and clinical trials, regulatory review and post-market safety monitoring by the regulator. Others, such as the ICH (international Conference on Harmonisation) in their technical and regulatory considerations for product lifecycle management (e.g., in ICH guideline Q 12 [3]) focus specifically on post(regulatory)-approval changes to a product, specifically CMC (chemistry, manufacturing and controls) changes, and the requirements for pharmaceutical quality systems and change management processes. For chemical engineers, they may see product (manufacturing) lifecycles in terms of the synthesis, manufacture scale up and disposal of the active pharmaceutical ingredient (API) and intermediates. From a supply chain perspective, it can mean the planning of the end-to-end supply chain, purchasing of raw materials, manufacturing of intermediate and finished goods, distribution of all materials and reverse logistics of unused products.
In this review, we take a broader view, as well as highlighting some areas that have not been sufficiently explored with respect to mRNA vaccines and therapeutics. In particular, we focus on the critical aspect of mRNA product development that involves conceptualization through to population or patient use. We review aspects of the design of mRNA products, including some of the advances in mRNA design that have been enabled by use of AI technologies. We have separately reviewed aspects of the development, manufacturing and regulatory lifecycle particularly as they relate to preclinical and clinical development, manufacturing steps, quality assurance and platform technology aspects were reviewed recently [1]. It was concluded that while development and regulatory review can be supported by information obtained from preceding platform products, product-specific data will at least be required for:
- Cell banks for bacterial culture and plasmid amplification (where applicable), characterisation of plasmid DNA template for mRNA synthesis, bulk purified RNA and mRNA encapsulation into LNPs
- Identity testing of the sequence and expressed products
- Potency assurance of mRNA products during manufacture and at release
- Confirmatory stability data for the drug substance and the drug product
Clinical trials are a critical part of the mRNA product development lifecycle. While the platform approach can guide clinical development, with the exception of variants to existing vaccines, new product-specific clinical data is usually required for each product. Particular considerations for mRNA and contemporary regulatory challenges for both mRNA vaccines and therapeutics innovations across the mRNA products lifecycle are reviewed in this paper. As a comparatively new commercial technology, it is important that safety and consumer/patient considerations are also discussed.
This review focusses on vaccines and therapeutics developed from conventional mRNA and unmodified lipid nanoparticles. However, it is recognised that other “sub-platforms” involving self-amplifying mRNA (sa-mRNA, [4]), circular RNA [5], other LNP variants [6] and other mRNA technologies, involving delivery through other nanoparticles, dendritic cells or CAR-T cells are also among the other therapeutic technologies using mRNA [7,8].
2. Considerations for mRNA Product Design – the Beginning of the Lifecycle
Several other reviews [4,9,10] have described processes of optimization of mRNA sequences and structure for use in vaccines and other products, so they will only be summarized briefly here. mRNA sequences utilized in vaccines and therapeutics have five main structural elements: a 5′ cap which influences stability and translation efficiency; the 5′ untranslated region which acts as a binding site for ribosomes to initiate translation, the coding region that contains the sequence for the protein to be translated from the mRNA, a 3′ untranslated region that also affects mRNA transport, stability and translation and a poly-adenosine (A) tail, which protects the mRNA from degradation. In addition, modification, deletion or insertions of particular nucleosides in the mRNA sequence can be pursued to reduce stimulation of the innate immune system and to increase translation of the encoded protein sequence.
Some differences in mRNA sequence and structure are required for vaccines and therapeutics [11]. Prophylactic vaccines for infectious diseases require products that can ideally stimulate both B- and T- cell immunity, while mRNA oncology therapeutics are required to stimulate a significant cytotoxic cellular immune response so that cancer cells are eradicated. This can make antigen / epitope design for mRNA cancer therapeutics quite challenging, as T-cell receptor epitopes are generally less well understood [12]. In contrast, while mRNA vaccines and mRNA oncology therapeutics are assisted by the immunogenicity of the mRNA itself, in mRNAs for enzyme / protein replacement in rare diseases, activation of the innate immune system by the mRNA therapeutic is quite undesirable. This is reduced in these products through nucleoside modification to increase the durability of expression of the mRNA [13], although recent studies have shown that optimising or attenuating ribosome translational load along with optimizing codons leads to greatest mRNA stability [14]. Some software packages have been designed that optimize the design of therapeutic mRNAs [15]. While these context-specific considerations exist for the selection of the target protein to be expressed by the mRNA and in the design of the mRNA, common manufacturing elements, such as raw materials, unit operations, optimized process parameter setpoints, may be sharable in a platform-based approach even between mRNAs intended for highly diverse therapeutic applications.
The power of mRNA vaccine and therapeutic technologies also brings with it complexity. The ability to potentially design and translate an essentially unlimited number of amino acid variants in a protein sequence, the requirement to determine most effective codon choices for the amino acids in the protein sequence expressed by the mRNA, and the need to decide on particular codon modifications means that there are many thousands to millions of potentially feasible alternatives for each candidate mRNA. For example, due to the existence of synonymous codons alone, there are around 2.4 × 10632 candidate mRNA sequences for the codons encoding the 1273 amino acid SARS-CoV-2 spike protein [16]. Optimization of untranslated mRNA region can also be undertaken using AI and Machine learning approaches [17].
While the goal of exploring potential alternatives to mRNA sequences is clear – increasing the stability and expression of the mRNA and improved commercial manufacturability, it is not feasible to assess many of these alternatives through laboratory experimentation. An increasing number of research groups have reported the use of computational, bioinformatic and AI approaches for mRNA vaccine design [16,18,19,20,21,22], with commercial mRNA vaccine developers also extensively utilizing these approaches for mRNA vaccine and therapeutic design. Added to these are other modifications that can be investigated using AI aim to reduce toxicity or immunogenicity of sequences and their expressed proteins and potentially optimize biodistribution.
AI approaches can enhance several steps in the design and development of mRNA vaccines and therapeutics [19,22]. Where there are several potential protein antigen candidates for a vaccine, these can be ranked through AI and their immunogenicity predicted. Deep learning approaches supported by artificial neural networks can assess large databases of proteomic and genomic sequences to identify vaccine candidates, especially when a single dominant epitope has not been identified in earlier studies. This approach has in particular been applied to the design of mRNA vaccine candidates for infectious disease [17]. Potentially undesirable cross-reaction of vaccines with human proteins can also be predicted. Computational approaches to predict immunogenicity predate the application of AI but methods now used with mRNA vaccines enable much more extensive and more rapid investigation, and some newer models simulate both humoral and cellular immunogenicity.
A “LinearDesign AI tool” that increased mRNA sequence stability through creation of folded structures [16] resulted in significantly higher antibody responses in mice with candidate COVID-19 and varicella-zoster vaccines. Structural reconfiguration of the mRNA molecules was conducted by algorithmically determining the most stable configurations of nucleotide sequences, allowing the mRNA to loop back on itself and form intramolecular double-stranded structures. AI approaches have also been used to predict suitable epitopes in mRNA cancer vaccines, for example predicting the MHC presentation ability and immunogenicity of neoantigens [23,24,25] including in design of individualized neoantigen therapeutics and to design mRNA sequences and structures that optimize antigen presentation [26]. Identification of suitable LNP formulations (particularly the ionizable lipid component/s) is still largely conducted empirically through laboratory screening of candidates. However as the research and patent literature on LNP formulations increases, recently several groups have published machine learning approaches that interrogate this data source [27] and potentially to identify new ionizable lipid structures for use in LNPs [28] or to use machine learning to optimize composition of LNPs [29].
3. Clinical Trials of mRNA Products
An increasing number of mRNA products are moving from preclinical development into clinical trials; we [1] have recently reviewed those in late stage (phase 2 or 3) trials. mRNA products are highly amenable to the application of platform technology approaches for their pre-clinical development, manufacturing, controls and analytical methods, but clinical trials are typically required for each new product. There is the potential to use clinical trial results from related platform vaccines to determine possible doses, but only as a guide. Some conclusions about reactogenicity and safety based on impurities or concentrations of contaminants may also be possible. Exceptions to requiring full clinical data packages are mRNA vaccine to viral variants (e.g., for SARS-CoV-2), and it is expected that as mRNA vaccines for seasonal influenza become available annual strain updates should also be able to be made without a regulatory requirement for clinical data [1]. Pre-clinical data may be able to support a related platform product, such as pharmacokinetic and biodistribution studies and toxicology data as well as assays for, and information on, potential immune responses and reactogenicity. Some vaccine-specific data will still be needed.
The requirements for clinical trials for mRNA products are in general no different than for other drugs, although as for other vaccines, the numbers of participants enrolled in vaccine trials are typically somewhat larger than for therapeutics. Information from products with similar mRNA sequence design principles and secondary structures and LNP nature and composition can also provide useful platform information in summarizing pre-clinical development data, the
While several billion doses of mRNA vaccines have been administered globally, there may be some individuals who may have concerns about taking part in a clinical trial of an mRNA product. The informed consent information therefore should make it clear that the product in the active arm of the clinical trial is an mRNA product. Reactogenicity is a common but typically mild and transient adverse event of a number of mRNA products. It is recommended that trial participants are advised about the possibility of reactogenicity if appropriate. While advising trial participants of the importance of seeking urgent assistance for potentially serious adverse events that it is also important not to confuse common reactogenicity symptoms with more serious adverse events.
The COVID-19 pandemic demonstrated that highly-effective mRNA vaccines could be developed in a matter of months against a lethal viral pathogen of global concern. With 13.7 billion does of COVID-19 vaccines administered as of August 2024, a significant majority of them being mRNA vaccines, the SARS-CoV2 pandemic provides a real-world example of demonstration of vaccine safety and efficacy [30]. This experience can be utilised for other emerging diseases, and the ability of the technology to serve as a platform was amply demonstrated, meaning that now, and in the future, neither developers nor regulators would be required to start “from first principles” to develop new mRNA vaccines for other pathogens. Certain elements of mRNA medicines, such as mRNA design, LNP composition, and manufacturing processes and controls, which were established through the development of mRNA vaccines in the COVID-19 pandemic, should applied by developers, where appropriate, to deepen the evidence of product and process understanding provided in applications for new mRNA medicines. Similarly, this understanding can be employed by regulators to simultaneously provide additional rigor to their assessment and increase efficiency of their review for elements which are fixed between products.
mRNA as a platform technology can accelerate the development of vaccines for emerging and tropical diseases [31]. While highlighting the benefits that mRNA platform technology provides in rapid, scalable vaccine development, and the fact that the equipment used for mRNA-LNP products could be interchanged between products, including vaccines against different pathogens, the authors [31] described challenges for the development of vaccines against individual diseases. These include, for particular diseases, the lack of animal models, poorly established correlates of protection, clinical development challenged by sporadic and unpredictable outbreaks, variable antigenic diversity and challenges with antigen design and requirement for containment facilities for preclinical challenge studies. Human challenge studies may also not be feasible or ethical in certain cases.
In cases when an emerging disease affects populations sporadically, clinical trials for development of vaccines can pose a number of challenges. The sporadic or low rates of infection could mean that prohibitively large populations would need to be enrolled to demonstrated clinical efficacy. In these cases, correlates of protection (an immune function that correlates with and may be biologically responsible for efficacy) or surrogates of protection (an immune marker that can be used to predict efficacy when the actual correlate of protection has not been firmly established) can be used in a smaller population of healthy subjects. However, establishing immune biomarkers as adequate surrogates of clinical benefit is a challenge in itself [32]. Understanding the elements of the immune response that are involved in protective mechanisms is critical to develop reliable biomarkers that can help expedite the development process. Novel immune profiling tools will enable a more extensive characterization of the protective mechanisms and help identify those biomarkers).
Expedited regulatory pathways such as the US FDA’s Accelerated Approval pathway provide an option for faster approval of medicines that address a significant public health need ahead of the demonstration of clinical efficacy, provided that a surrogate marker reasonably likely to predict protection is identified, and that a clinical study to confirm efficacy is planned or underway [33].
Several organisations are developing – or have already developed- vaccines for highly infectious diseases which also have a high mortality rate. While the clinical trial considerations for mRNA vaccines for these diseases do not necessarily differ from other types of vaccines, it is worth outlining some considerations that may be relevant to clinical trials of these vaccines. Some mRNA candidate vaccines include those against Nipah virus [34,35,36], Ebola disease [37], rabies [38], Zika [39], mpox [40] and mRNA-encoded Chikungunya virus monoclonal antibodies [41].
Global regulators and the World Health Organization (WHO) have considered alternate approaches when the usual expectation of completion of phase 2/3 human trials of a product may be neither practical nor ethical, although demonstration of some form of clinical benefit in a randomized controlled interventional study remains the gold standard. The US FDA “animal rule” has been in place for over 20 years [42]. Related to this is the animal model qualification program which provides guidance on appropriate drug development tools, including animal biomarkers, and how they can potentially be reviewed and formally qualified by US FDA [43]. For a product to be eligible under the animal rule, the mechanism of action of the disease needs to be understood reasonably well. Animal studies may be required in more than one species and must be closely related to the desired benefit (protection/ immunity in humans) and data on the drug or vaccine pharmacokinetics and pharmacodynamics in animals and humans enable selection of an effective human dose. However, many viruses have very tight host species specificity and animal challenge models are not available for a human pathogen, creating difficulties for the interpretation of animal studies with related animal host-specific agents. There are also post-market requirements that FDA imposes for drugs and biologicals approved under the animal rule, in particular, the need for studies in humans if/when there is a disease outbreak.
The EMA also developed guidance around the animal rule [44]. There are some important policy differences to the US FDA with a greater focus on demonstrating safety and having strong pharmacovigilance systems in the presence of unclear efficacy. There is less of a focus on prescribing animal studies and their requirements and more on explaining the infeasibility of detailed human studies based on disease rarity or ethical reasons. Regional regulatory reliance involving leading reference agencies will also be important in supporting rapid regulatory review and deployment of mRNA vaccines against epidemic diseases of local importance [45].
4. CMC Life Cycle Considerations in mRNA Product Manufacturing and Deployment
With the need for rapid development and deployment of mRNA vaccines during the COVID-19 pandemic, manufacturers initially took a conservative approach to storage and shipping conditions for these products [46]. This was because it was well recognized that in aqueous solution, mRNA is inherently unstable, as both its single-stranded nature and the presence of a 2′ hydroxyl group can enable hydrolysis of neighbouring phosphodiester bonds, resulting in cleavage of the mRNA. Longer mRNA sequences can be less stable [47]. A number of approaches can be used to stabilize mRNA prior to encapsulation in an LNP, including the use of buffers and sucrose [48,49]. Design and modification of the mRNA sequence and its secondary structure is also important in increasing its stability, including nucleotide selection, modification of the 5′ cap and elongation of the poly-A tail [50,51]. LNP composition also directly affects storage stability of the mRNA as the mRNA forms a complex with ionized lipids. Encapsulation can protect mRNA from enzymatic degradation, but interactions with LNP components have been reported also to increase degradation risks. Drug product formulation processes can also affect stability. Changing the buffer composition of the latter product from a phosphate buffer to a Tris buffer increased the shelf life of the defrosted product [51].
Deployment of COVID-19 mRNA vaccines in some developing countries has been challenging, given the storage and shipping requirements [52]. As a result, a range of other approaches, such as the development of lyophilized candidate vaccines has been investigated. The stability of mRNA-LNPs was increased by lyophilization [53,54], with no loss in efficacy after 3-6 months at room temperature; although, some loss of efficacy has been seen in other studies [55]. An Indian lyophilized mRNA COVID-19 vaccine, GEMCOVAC-19 has received regulatory approval in that country. The mRNA is attached to the surface of a nano-emulsion, rather than being encapsulated in LNPs (https://gemcovac.com/). Sanofi’s current mRNA seasonal influenza candidate vaccine (SP0237) is also provided lyophilized, as is Moderna’s cytomegalovirus candidate vaccine (mRNA-1647 [56]).
While the long-term stability of lyophilized vaccines enables their manufacture and stockpiling ahead of an outbreak or regional epidemic [57] there are some disadvantages. Freeze-drying adds to manufacturing costs, while reconstitution of lyophilized vaccines can introduce particulates or aggregates and add to product handling and the risk of errors. To increase convenience, and avoid dosing errors, a prefilled syringe presentation can be developed. While syringes are shipped and supplied frozen, they are a convenient dose form, as they can be stored thawed in refrigerated conditions. Another way of increasing the stability of mRNA vaccines is by designing shorter antigens. While the ancestral mRNA-1273 vaccine encodes the full-length SARS-CoV-2 Spike (S) protein, mRNA-1283, a next generation vaccine intended to prevent disease caused by SARS-CoV-2, encodes only two regions of the S protein which contain major viral neutralization epitopes, together with a linker and a membrane anchor sequence. The shorter mRNA length of mRNA-1283 facilitates higher levels of protein expression as well as enabling longer storage at refrigerator temperatures [58].
5. Regulatory, Lifecycle and Deployment Considerations of mRNA Therapeutics
Rare genetic Diseases
The development of biomarkers or genetic tests that can identify relevant patient populations suffering from rare metabolic diseases establishes a path for drug development. Several of the newer approaches to treatment of these rare diseases, including mRNA therapies, address the root causes of the disease e.g., through the replacement of a deficient or mutated enzyme. Development is not straightforward though as the understanding of the epidemiology and natural history of many rare diseases can be quite poor [59].
Gene therapies for rare diseases focus on permanently modifying the defective gene. These approaches have had a longer history than mRNA therapies, which are currently at clinical trial stage. More than 10 gene therapies for non-cancer rare diseases have been approved by the US FDA. However, there are several limitations to the widespread use of these medicines. The gene therapy products have long manufacturing cycles and because they can require arduous preconditioning with chemotherapy drugs and in-or-outpatient infusions they may not be well tolerated by patients. Other potential limitations include the inability to reverse gene therapies, risk of incorporation of the target gene into the nucleus, and immunity to some viral vectors. Where they exist, treatment alternatives that can also help manage conditions such as haemophilia and may be preferred by affected patients.
mRNA treatments consist of an LNP-encapsulated mRNA encoding for the functional version of the defective protein, and therefore only produce transiently-expressed proteins and do not alter the patient’s nuclear DNA. These treatments offer an efficient alternative to gene therapy for those patients that may not be eligible for gene therapy or for which there is no treatment option. mRNA therapeutics are anticipated to have applicability to treat rare metabolic and other diseases, particularly those that are caused by a single gene (monogenic) and where the protein expressed by the defective gene requires restoration or replacement [60,61]. A feature of proteins encoded by therapeutic mRNAs is that they can be expressed in targeted organs, using features such as the composition of the lipid nanoparticles, and the route of administration, and in specific cellular compartments – secreted, transmembrane, within the cytosol or mitochondria - as determined by the signal peptide encoded by the mRNA.
A number of successful animal models have expressed exogenous mRNA from mRNA-LNP administration to treat three rare metabolic diseases: methylmalonic acidemia (targeting methylmalonyl-CoA [62,63,64], acute intermittent porphyria (targeting porphobilinogen deaminase [65]) and Fabry disease (targeting alpha-galactosidase A [62]). Other targets studied at the preclinical phase including hemophilia B (Factor IX), ornithine transcarbamylase deficiency [66], propionic acidemia [67], glycogen storage disease types 1a (glucose-6-phosphatase) and 3 (glycogen debranching enzyme), phenylketonuria (phenylalanine hydrolase),cystic fibrosis (transmembrane conductance regulator), maple syrup urine diseases (branched-chain alpha-keto acid dehydrogenase, BCKDH) dysfunction and arginosuccinyl aciduria (arginase) [68,69,70]. Several candidates have now moved into clinical trials [1], including for propionic acidaemia [71], methyl malonic acidemia, cystic fibrosis, ornithine transcarbamylase deficiency, phenylketonuria, propionic aciduria and primary ciliary dyskinesia.
New Approaches Will Be Needed to Keep Pace with Therapeutics Development for the Large Number of Rare Diseases
There are about 10,000 rare diseases identified [72] but only about 5 percent of rare diseases or conditions have US FDA-approved products available [73]. Using the current “one-disease, one-product-at a time” regulatory approach, it would take hundreds of years for therapeutics for each the currently known rare diseases to be developed and to receive regulatory approval.
Several approaches could improve the efficiency of development and regulatory review of new therapies for rare diseases. These include approaches such as basket clinical trials (designed to evaluate a single treatment intervention for multiple diseases that share a common molecular alteration) [74] or “N of 1” trials, which involve detailed longitudinal studies and use of historical controls [75,76]. One approach with great potential to improve development and regulatory licensure is the more systematic, standardized and controlled leverage of platform technology frameworks. It has been estimated that about 6500 rare diseases are caused by mutations in single genes [77] and these provide a readily addressable opportunity for new drug development using mRNA [78,79]. The platform technology approach has also been applied to development of gene therapies using a disease-agnostic approach and adeno-associated virus (AAV) vectors [80].
In addition, when there are several different but related genetic defects affecting a particular metabolic pathway, it may be possible to use the platform approach to further streamline evidence generation and regulatory review; an example are the rare diseases resulting from either propionyl-coenzyme A carboxylase or methyl malonyl coenzyme A mutase, which are successive enzymes in the same metabolic pathway and for which mRNA therapeutics are currently under clinical development [71]. As each of these therapies would consist of the same mRNA/LNP technology with only the encoded sequence being different, a potential model for accelerating the development and availability of these treatments would be to include several of these enzyme replacement treatments that belong to a same metabolic pathway under one marketing authorization.
Life Cycle Considerations for mRNA Rare Disease Therapies
Several considerations for the development of mRNA therapeutics for rare genetic disorders in addition to those contemplated for vaccine development need to be addressed [81,82,83,84]. While the quality and manufacturing/ CMC aspects of product development will often be largely similar to those for vaccines, the preclinical development program will not. With these therapies often requiring multiple doses given weeks apart during long periods, it is important to determine how durable the effects of the therapies are and thus the required frequency of repeat doses in clinical trials.
Studies on the biodistribution and accumulation of the relevant mRNA, translated protein (and its fragments) and LNP / LNP fragments are important, as are studies on the delivery to targeted organs. Most therapies are currently administered intravenously and circulate through the liver so are particularly useful when it is a liver enzyme that is in deficiency, but if distribution to other organs is required, alternate mRNA-LNP design strategies and/or administration routes may be necessary. Extensive preclinical safety studies are required, including assessment of inflammatory markers, liver function tests, and on the potential development of antibodies to the protein expressed by the mRNA. Efficacy studies may be required in several animal species especially if rodent models are of limited relevance to the particular human rare disease. In clinical studies, the duration of effect of the mRNA rare disease therapy will depend on the target protein and the organ system affected, and these will need to be established for each therapy individually. An understanding of the natural history of the disease should inform whether it is acceptable or desirable for the translated protein levels to drop back to baseline levels in the periods between treatments.
Oncology - Individualized Neoantigen Therapies (INT)
Tumor-specific neoantigens result from genetic alterations in cancers; they are recognized as foreign by the immune system and so are not subject to immune tolerance. The advent of next- generation sequencing and bioinformatic technologies has enabled these neoantigens to be targets for personalized cancer immunotherapies. mRNA, peptide and viral vector vaccines based on neoantigens rather than other tumor-associated antigens have several potential advantages [85,86,87,88] and have been applied to a rage of tumor types in preclinical models and in clinical trials. Neoantigens are exclusively expressed by tumor cells so the resulting T cell responses are tumor-specific and damage to healthy tissue is minimized. As neoantigens are derived from somatic mutations, T cell central tolerance of self-epitopes should be absent and a potentially robust immune response to the tumor could be induced. Finally, vaccine-boosted neoantigen-specific T cell responses could persist and could possibly provide long-term protection against disease recurrence.
A range of therapeutic approaches to the use of neoantigens in cancer vaccines have been developed [86], including adoptive cell therapies (T-cell receptor engineered-T cells, CAR-T); dendritic cell vaccines, bispecific antibodies, peptide-based neoantigen vaccines, and nucleic acid (RNA and DNA based) vaccines. mRNA therapeutics, however, have certain advantages over other approaches (Figure 1), including:
- simultaneous delivery of multiple tumor antigens, reducing risk of resistances or to antigen loss or change
- full-length antigens can be encoded if required, enabling multiple epitopes to be presented
- induction of a broad T-cell response
- manufacture is rapid and scalable compared with some of the other approaches
The identification, prediction and validation of suitable immunogenic neoantigen sequences is a critical part of the mRNA individualized neoantigen therapy development. Whole exome sequencing, RNA sequencing and proteomic data can be used, but identification of genome-expressed mutations and HLA typing of patients is required to best predict which neoantigens should be selected. Next generation sequencing data of normal and tumour tissues from the same patient are compared so that (somatic) mutant peptide sequences are able to be identified. In combination with HLA typing information, HLA binding of particular sequences can be predicted in silico to ensure that there is strong T-cell recognition of as many of the potential neoantigens as possible.
Personalized cancer immunotherapies encoding individual tumor mutations are being trialled in melanoma, adjuvant non-small cell lung cancer, gastrointestinal cancers, other solid tumors, colorectal cancers, triple negative breast cancer and pancreatic cancer, with or without an immune checkpoint inhibitor or another oncology drug [89,90]. Applications of INT have continued to expand, specifically for applications in tumor heterogeneity and/or low antigen burden. This includes preclinical models in a range of glioblastoma and medulloblastoma brain tumors where selective gene capture and enrichment has been used to develop mRNA therapies [87]. INT is also continuing to address challenges including increasing the rates of identification of neoantigen peptide sequences that will bind MHC with high affinity and be reliably recognised by patient T-cells; loss of neoantigens as the cancer evolves; immunosuppressive tumor microenvironments; insufficient production of neoantigen-specific T-cells and limited neoantigen-reactive T-cell repertoire [86]. As the understanding of neoantigens increases, this is leading to better identification of the most immunogenic ones using computational approaches [91].
mRNA technology is ideally suited to individualised neoantigen therapy as neoantigens can be identified and sequenced from an individual patient, corresponding codon- optimized mRNA sequences produced and manufactured into a mRNA-LNP for that patient within weeks. The approach brings with it technical, logistical and regulatory challenges. First, suitable neoantigens may be difficult to identify in certain patient tumors, and/or it is difficult to predict the most immunogenic neoantigen.
In the phase 2 trial of an INT mRNA vaccine under development by Moderna and Merck, the minimal number of target epitopes per patient was 9, and 91% of patients received mRNA encoding the full 34 epitopes [90]. The product being trialled by BioNTech for pancreatic ductal adenocarcinoma (in combination with atezolizumab and several chemotherapy agents) typically contained up to 20 target epitopes per patient [92]. Other personalized neoantigen mRNA treatments are in clinical trials –an sa-mRNA booster for metastatic colorectal cancer (Gritstone Bio) and a mRNA treatment for advanced solid tumors (Stemira Therapeutics) [21,93].
Second, the composition and predominance of different neoantigens evolves during the course of the disease and may have changed by the time the mRNA treatment is delivered to the patient. Manufacturing of large numbers of individualised vaccines will require simultaneous parallel end-to-end manufacturing at very small scale for dozens or hundreds of versions of the product under GMP conditions – effectively requiring “scale out”, rather than the typical “scale up” that occurs when a product is commercialized. Another consideration relevant for mRNA therapeutic development involves multi-dosing (e.g., nine doses of mRNA-4157 at three-weekly intervals). Therefore, more in-depth pre-clinical studies will be required, compared with mRNA vaccine development. On the other hand, compared to other oncology medicines, there is often a different approach to benefit-risk than for a prophylactic vaccine which is to be administered to large numbers of healthy adults and children.
It is anticipated that initial regulatory submissions for INTs will be made for potential approval against the particular cancer and disease paradigms that were the subject of the particular clinical trials (e.g., adjuvant or particular disease progression stages). However, having addressed the regulatory issues for the INT “platform technology within a platform technology”, development and regulatory review for similarly designed product against other indications could be facilitated. Because each product is unique for each patient to be treated, regulatory approaches will require adaptation to accommodate this.
Potential regulatory approaches to assess the manufacturing quality, and efficacy and safety of mRNA vaccines were discussed previously [1], noting that each individual neoantigen mRNA product is unique. Recently, Jonker et al. [94] reviewed the range of N-of-1 individualized therapies under development and noted that mRNA individual neoantigen therapies differ from other N-of-1 therapies in that they can be tested in clinical trials involving multiple patients with the same cancer type using the same endpoints. US FDA guidance [95] has indicated that each component of multiantigen vaccines may not be required to be individually evaluated, although it was emphasized that this would be on a case-by-case basis.
The South Korean regulator (Ministry of Food and Drug Safety, MFDS) has released regulatory guidance specifically on individualised neoantigen therapies [96]. The guidance is principles-based and emphasises focus on the assessment of controls of design and manufacturing processes for the INTs in potential regulatory review, although the guidance is not specific to mRNA products.
These principles include:
- Ensuring that the biopsy of the tumor tissue taken for sequencing is representative
- Justification of the algorithms used to select neoantigen peptides
- Assessment of controls over automated parallel manufacturing processes
- Establishing the consistency of a test product across multiple batches based on agreed representative quality attributes
- Using pooled stability data from multiple batches
Very recently (February 2025), the UK Medicines and Healthcare products Regulatory Agency released “Draft guidance on individualised mRNA cancer immunotherapies” [97]. Unlike the South Korean document, the draft guidance is specific to mRNA-LNP therapies but also contains guidance on neoantigen identification and selection. However, there is more specific detail provided on proposed considerations around CMC/ product manufacturing, non-clinical and clinical aspects for mRNA INT. The draft guidance also emphasises the importance of having processes in place to effectively track and trace samples from patient biopsy stage through the design, manufacture, shipping and patient administration stages to ensure that the correct product is administered.
As the technology becomes more established, it is anticipated that representative batches would be used to assess the in vitro expression of test INT mRNA products, and to confirm that products remain immunogenic (given the necessary time lag between mutation sequencing and delivery of therapy). Similarly, it is anticipated that toxicology, immune induction in vitro and delivery efficacy in vivo would utilize representative batches. Apart from the use of representative batches, we anticipate that another potentially useful approach would be provision of regulatory data on products manufactured within certain bounds of total mRNA length and structure, and assessment of expression of sequences that encompass the extremes of potential INT products in the consideration of various CMC topics such as product specifications and shelf life. Regulators will also be required to adapt their manufacturing oversight to review facilities that conduct simultaneous, very small-scale manufacture of a product under GMP conditions.
Finally, both rare disease and INT mRNA therapies are by definition, low-volume individual products and will require the development of efficient distribution protocols (potentially different for those used for large scale vaccine distribution during the SARS-CoV-2 pandemic) so that they can reach affected patients in as timely a manner as possible. Customs and importation protocols will also need to be refined to avoid access delays, for example whether individual import licenses would be required for each INT product or whether they could also be considered a single product at the border. Import and distribution chains will also require alignment when two agents are involved, such as a checkpoint inhibitor (which can be stocked in bulk) and the patient-specific mRNA INT.
6. Emerging Regulatory Trends and Issues
Need for Greater International Alignment in Regulatory Pathways
A significant challenge for the commercialization of mRNA products is the lack of consistency in how different mRNA products are currently classified in a regulatory sense, both within and between regulatory agencies [81,98]. This can lead to differences in data requirements and regulatory submission dossier structure for different mRNA products even though they may be developed in the same facility using the same technology and have very similar structure and composition. There are also consequences that flow from regulator’s willingness to assess data in a platform manner or otherwise strictly on a product-by-product basis. In the absence of assessment of data using a platform approach, different evaluators within the one regulatory agency could potentially require different specifications or reach different shelf-life recommendations for products with very similar structure and composition. These differences in regulatory procedure also have implications as it can require a substantial effort to restructure a regulatory dossier from a medicines structure to a biologicals structure, so submission and therefore regulatory review and potential patient access is delayed.
The description of mRNA products, which do not alter the recipient’s genome, as “gene therapy” could lead to increased vaccine hesitancy among the public as it would be unrealistic to expect the patient to differentiate between gene therapies such as viral vector or DNA therapies and mRNA products. In the US FDA, mRNA products are regulated as biologicals by CBER (Center for Biologics Evaluation and Research). Within CBER, vaccines are reviewed by the Office of Vaccine Review and Research, while for therapeutics the mRNA platform is regulated by the OTP (Office of Therapeutic Products). There is still uncertainty regarding the classification of mRNA therapeutics by the FDA. Overall OTP has classified mRNA therapy as “gene therapy”, however there is some variation in how the FDA has applied gene therapy guidance requirements. This is important as the requirements for gene therapy products can be very different. Gene therapy products are typically excluded from ICH guideline S9, which requires a leaner pre-clinical package, and instead are likely subject to ICH guideline S12. The ICH guideline S12 requires full preclinical studies in US FDA Investigational New Drug (IND) submissions. These may include biodistribution and genotoxicity studies, safety pharmacology studies, long term carcinogenicity studies, and longer-term toxicology studies [99].
The potential consequences of mRNA being categorized as gene therapy could be very significant. For example, in a recent US FDA draft guidance [100], the agency recommends long-term safety monitoring for up to 15 years of follow-up for gene therapy products, to monitor potential delayed adverse events such as cancer or off-target effects, even though this is much more plausible with products such as viral vector therapies. In the EU, the classification is even more complex. mRNA vaccines against infectious diseases are reviewed as vaccines by the EMA as “immunological medicinal products”. In contrast, mRNA therapeutics are reviewed by the EMA as gene therapy medicinal products, a type of ATMP. A new definition of Gene Therapy Medicinal Products (GTMP) has been proposed by the European Commission (EC), subsequently amended by a draft of the European Parliament (EP). The revised draft definition provides a clear distinction between products that edit the host genome and those that do not, a differentiation agreed upon by both the EC and the EP. Additionally, the category of nucleic acid has been expanded to include both synthetic and biological origins [99].
The US FDA and EMA also apply differences to the definition of mRNA/ mRNA-LNP drug substance versus drug product, which creates further complexity in meeting regulatory data requirements during manufacturing and product analysis. There are also differences between the US FDA and EMA in how the lipids within the LNPs were treated, with differing classification as excipients or starting materials, affecting the level of safety and characterization data that was required to be submitted [101].
In some other countries such as Australia, both mRNA vaccines and therapeutics are regulated as medicines, rather than as biologicals. In Switzerland, products with defined nucleic acid sequences (including mRNA) are considered biologically active genetic material and regulated in a similar way to gene therapy products [102].
A final area of limited regulatory alignment between countries relates to the requirement in some countries for separate approvals (from a separate regulator) to manufacture and/or utilise particular mRNA products in clinical trials or commercial use which are deemed to be, or contain, genetically modified organisms (GMOs). For example, in Australia, while no approvals are required from the Australian Gene Technology Regulator for patient administration of conventional mRNA products, the initial manufacturing step in which plasmid DNA is expanded by fermentation in an E. coli host would be seen as a GMO step with the non-conjugative strains of E. coli containing the plasmid as the GMO and thus require a license from the regulator. However, for other mRNA vaccines and therapeutics, such as self-amplifying mRNA or ex vivo mRNA/CAR-T therapies, GMO licenses are also required for clinical trials.
Differing International Approaches to the Regulatory Application of Platform Technology
The WHO and several leading regulators have identified the development and regulatory advantages of treating mRNA as a platform technology, although some other regulators have not at this stage announced plans to development of specific platform guidance and have utilized the approach that “the platform concept can be treated as prior knowledge which is similar to any medicinal product development” [103].
Platform technology is most applicable to the Quality/CMC part of mRNA-LNP product development, although there are significant implications for non-clinical and clinical development too. Platforms can comprise:
- Starting materials: including DNA plasmids, enzymes, cell banks for expression systems
- mRNAs that encode antigens of interest
- mRNA-LNP control and testing of LNP size and mRNA encapsulation
- Unit operations throughout the manufacturing process
- Analytical techniques throughout the manufacturing process – identity, quantity, purity, integrity, characterization, potency and safety (contamination)
- Approaches to the validation of processes and methods used for manufacture and analysis
- Understanding of the degradation pathways and metabolism of mRNA and LNP components in consideration of non-clinical assessment and determination of shelf life
- Clinical experience justifying specification limits for certain shared attributes between products, such as particle size and product-related impurities
As outlined in our earlier review [1], non-clinical development of mRNA products can also extensively utilize the platform approach in dose-finding, pharmacokinetic, biodistribution, and toxicological studies. More specific to the individual product is the rationale for antigen selection/ epitope choice and studies on the extent and duration of immune response or persistence of the replaced protein in vivo.
There are several vaccine and therapeutic development strategies that can be considered as platforms and thus could utilize platform technology. Apart from mRNA vaccines and therapeutics, these include protein subunit and virus-like particle vaccines, viral vector vaccines and therapeutics, cell and gene therapies such as chimeric antigen receptor T-cell (CAR-T) therapies as well as monoclonal antibody and biosimilar products.
At this point, regulators internationally seem to be considering three broad pathways for the evaluation of mRNA products. These can loosely be categorized as relying only on “prior knowledge”, non-technology specific platform approaches and mRNA platform-specific approaches (potentially contemplating the development of platform technology master files). The long-established concept of regulatory prior knowledge, is for example, described as a platform approach in several ICH (International Conference on Harmonisation) guidelines. In the ICH Q11 guideline [104], platform manufacturing is defined as “the approach of developing a production strategy for a new drug starting from manufacturing processes similar to those used by the same applicant to manufacture other drugs of the same type” , while in the ICH Q14 guideline [105] a platform analytical procedure is defined as “a multi-product method suitable to test quality attributes of different products without significant change to its operational conditions, system suitability and reporting structure.… would apply to molecules that are sufficiently alike with respect to the attributes that the platform method is intended to measure”.
While the prior knowledge approach embraces elements of platform technology, it has its deficiencies. Without specific guidance there is a strong likelihood of evaluator-to-evaluator variability within an individual regulatory agency on how they utilise prior knowledge in product reviews, and there is no clarity for product developers on platform aspects. Thus, the prior knowledge approach may not lead to development or regulatory efficiencies nor a systematic utilization of learnings from the platform. The second group of platform technology approaches are “non technology-specific”. Examples from EMA and US FDA follow. The EMA guidance on biotechnology substances platform manufacturing [106] provides information for developers to support “a production strategy for a new drug starting from manufacturing processes similar to those used by the same applicant to manufacture other drugs of the same type….”
In early 2024, the US FDA undertook a public consultation on draft regulatory guidance on a proposed designation program for platform technologies [107]. Section 2503 of the US Omnibus Appropriations Act of 2023 required FDA to established a program for designation of platform technologies, so that sponsors may “reference or rely upon data and information” from a previous application for a drug or biological product that incorporates or uses the same platform technology. mRNA products were one example of the types of products in scope. The platform designation process aims to allow sponsors to “manufacture more than one product through a standardised process and provide predictability on product regulatory review”, by enabling information from a prior product to be re-used in subsequent application, including consideration of prior GMP inspection findings. Potential benefits from receiving a platform designation include early and continuous interactions by the developer with the FDA and potentially an expedited review. In order for platform technology to be used to its fullest potential, it would be best for designation to commence early, and for each of CMC, non-clinical and clinical uses of platform data to be in scope. As the extent of prior knowledge around mRNA products is already quite extensive, a major consideration is how that information will be provided by product developers to regulators and maintained in a coherent fashion. The FDA’s draft approach provides significant flexibility but lacks clarity on how the prior knowledge will be maintained.
The final group of platform technology guidances and approaches under consideration by regulatory agencies and related bodies are mRNA product-specific. In September 2022, the WHO Expert Committee on Biological Standardization developed a platform technology guidance for prophylactic mRNA vaccines [108] while in 2023, EMA consulted on development of a platform guideline on quality aspects of mRNA vaccines [109]. The EU Directorate for Quality of Medicines and Healthcare commenced a consultation on production and control of mRNA vaccines in May 2024, and in January 2025 announced that in July 2025 three new texts will be published in the European Pharmacopeia covering mRNA-LNP vaccines for human use; mRNA active substances used for vaccine manufacture and linear DNA templates used as starting materials [110].
mRNA Platform Master Files
To establish an efficient process for developing a regulatory dossier for a new mRNA product within a platform or supporting the evaluation of changes to a product as part of the mRNA platform, a sponsor could create a master comparability protocol for that product. The master comparability protocol would include specific tests, analytical procedures, and acceptance criteria for all specified changes expected over the lifecycle of the mRNA platform product. Boundaries for acceptance criteria can be based on process knowledge with different products using the same LNP (or potentially different LNPs with enough process knowledge), as well as the clinical experience generated with pre-licensure materials encompassing a range of values for the critical quality attributes.
Where changes are more significant in that there is a very different mRNA sequence targeting a new indication, comparability assessments could still streamline product development and regulatory review, and the concept of a master comparability protocol be suitably adapted. In the case of a new mRNA sequence based on an established mRNA platform, the only manufacturing-related change is the manufacture of the new DNA plasmid that is then used to manufacture the corresponding mRNA sequence. This portion of the manufacturing process could be described in a comparability assessment that would reference to the drug or active substance master file (DMF) for the mRNA platform manufacturing equipment, flow, and process, among other things. This assumes all mRNA-LNP products referencing this DMF are formulated with the same LNP and buffer components, excipients, and use the same equipment and process.
The master comparability protocol, together with other product- and sponsor-specific information on the product, particularly CMC information could be included in an “mRNA platform master file”. This platform master file would be a company-specific commercial-in-confidence document submitted to a regulator which would complement but not duplicate the development of public regulatory guidance which relates to mRNA platforms, rather than specific product families.
An important regulatory concept that is in use in some countries such as the US or Canada, is the Master File (MF). One MF covering a specific drug component can be used across several products that use the same component, alleviating the need to submit and review the same information repeatedly across products. In the case of mRNA products, the information on the lipid mixture used to produce the nanoparticle can be included in a separate master file that can be cross-referenced in any product file that contains it. This concept could be generalized to cover one or several platform technology building blocks such as the LNP itself.
EMA also have implemented veterinary vaccine platform technology master files (vPTMF) since January 2022 [111] and while these are for veterinary vaccines it is reasonable to expect they may guide future thinking at the EMA on human platform technology products. The guidance describes a platform technology master file as “a file that contains all data relative to the platform for which there is reasonable scientific certainty that they will remain unchanged regardless of the antigen(s)/gene(s) of interest added to the platform” (which) “aims to avoid the unnecessary re-submission and re-evaluation of data relating to a vaccine platform technology used in an authorised IVMP for the authorisation of subsequent vaccines”.
There are several analogies between this concept and the use of Drug or Active Substance Master files (DMF or ASMF) in regulatory submissions. DMFs have particularly been used to support regulatory submissions around the drug substances for generic medicines, although they are used more widely for a wider range of applications to enable the provision of confidential product information to regulators to support the applying sponsor’s application, without disclosing proprietary information. DMFs can provide detailed information about processes and facilities used in manufacturing as well as packaging and storage. They can also in some cases include pre-clinical information such as toxicology and clinical risk evaluation and mitigation strategy information.
It is proposed that an analogous approach to the development and use of mRNA platform master files be explored. While the intent of these master files could also be to protect confidential information for products that are licensed from an mRNA product manufacturer to a separate sponsor, the overarching purpose in most cases is to enable development of and sharing with regulatory agencies of a single set of manufacturing and analytical processes for a proprietary family of mRNA products.
mRNA Vaccine Laboratory Lot or Batch Release
In several countries vaccines are required to undergo individual lot or “batch” laboratory testing – depending on the local legislation, testing is conducted either by the manufacturer, the regulatory agency or a third-party laboratory network e.g., Official Control Authority Batch Release (OCABR) laboratory in Europe [112]. Lot release has been considered necessary because of concerns that there is a risk of greater batch to batch variation between manufacturing batches of vaccines than of other biologics and pharmaceuticals because of the greater molecular complexity of biological medicines than chemically-manufactured medicines. For this reason, regulators require testing of the final product for potency assurance (e.g., concentration and functionality of the active ingredient) and safety (typically of contaminants that could cause adverse reactions). The full set of analytical tests used for vaccine QA/QC are shared with the relevant regulatory agency and lot release specifications and characterisation tests will require agreement with them as part of the regulatory market authorisation process.
The EU has developed specific protocols for each type of vaccine for different antigenic targets [112] with some differences for different antigens across a given vaccine platform. They have recently updated their protocol for COVID-19 mRNA vaccines, with a new version in force from January 2024, but a general mRNA vaccine protocol is needed.
Many of the same platform considerations that have been applied to analytical testing to support CMC controls for mRNA vaccines should also be able to be applied to batch release considerations, and it will be important to specify this in future regulatory guidances. For example, the EU OCABR guidelines for COVID-19 mRNA vaccines specify that on at least 15 containers of each final lot official control laboratories should, apart from requiring documentation on production volumes, storage temperatures and time and expiry dates for intermediates and final product they should test for appearance, identity (for each antigen/strain, if it is a multi-strain vaccine) and integrity.
However, there is not international alignment on the processes or requirements for lot testing, and this can have implications for sponsors of imported mRNA vaccines. Further, the rationale for lot testing being required for vaccines derived from the origin of earlier vaccines as inactivated or killed cellular biological products. Given that mRNA vaccines are derived from in vitro translation of DNA, it could be questioned whether lot release testing should be required at all for mRNA vaccine products. Alternate approaches to manage safety and quality risks throughout the lifecycle could be considered for mRNA products, including some of the approaches proposed for individual neoantigen therapies in this review.
7. mRNA Product Safety
While critical for both vaccines and therapeutics, vaccine safety is appropriately closely scrutinized because most vaccines are administered to healthy people and to large numbers of children. While the mRNA COVID-19 vaccines were authorized for both children and adults, the majority of doses were administered to adults. Even so, initial trials were conducted with adult cohorts, and the initial regulatory approvals for the mRNA COVID-19 vaccines were for adults, before being extended to children following proper completion of clinical trials in pediatric age groups. Regulatory safety monitoring does not commence with post-market monitoring but rather is integral through the product development lifecycle [113]. Safety considerations are integrated into the design algorithms for many mRNA products, and toxicological studies are a major part of the preclinical development of all products, prior to any first-in-human clinical trials. As for any new product development, all clinical trial protocols closely evaluate safety, in first in human trials prior to introduction of a new treatment cohort as well as prior to approval for progression to subsequent trial phases involving more subjects.
Both clinical trials and real-world experience has shown that mRNA COVID-19 vaccines have a very good safety record; indeed, they became the mainstay after rare fatalities were associated with viral vector vaccines. The good safety record has also been observed in clinical trials of mRNA vaccines for indications other than COVID-19, and the first non-COVID-19 mRNA vaccines (targeting the respiratory syncytial virus pathogen) has now been approved in a number of countries, including in Europe and the USA [114].
Reactogenicity, which is due to an inflammatory response to vaccination, is a characteristic of many vaccines and was recognised well prior to the roll out of mRNA vaccines during the COVID-19 pandemic. It has been described as encompassing “injection-site pain, redness, swelling or induration (hardening of areas under the skin due to inflammation) at the injection site as well as symptomatic symptoms, such as fever, myalgia or headache” [115]. While reactogenicity effects are largely mild, short-term and self-resolving, they can lead to fear and loss of confidence in vaccination and vaccine hesitancy. Reactogenicity is due to an immune response to vaccine components, in the case of mRNA vaccines production of type 1 interferon. Both the mRNA and lipid nanoparticle components may contribute [116], with the LNP components particularly responsible [117,118,119]. The main reactogenicity symptoms were similar for the two main mRNA vaccines, BNT162b2 and mRNA-1273 [120].
While all vaccines can be reactogenic, the mRNA COVID-19 vaccines been associated with higher short-term reactogenicity than other COVID-19 vaccines. A systematic review which assessed 28 clinical trials of different COVID-19 vaccines as boosters [121] found that mRNA vaccines were the most reactogenic, compared to viral vector and protein subunit vaccines and inactivated vaccines the least reactogenic. Other than the ChAdOx viral vector vaccine early in the pandemic, the use of non-mRNA vaccines has been much more limited, however. In reports to the US CDC v-safe surveillance system, a smartphone-based active surveillance system in the US, about half to two-thirds of those who made reports reported reactogenicity, with higher proportions in females and those under 45 years. Local reactions were more common than systemic reactions, but new or worsening reactions were uncommon 2 weeks after vaccination, with fewer than 3 % of people reporting any reactions on day 14 [122]. It is important to note that there is a general correlation between efficacy and reactogenicity, emphasizing the importance of assessing the overall benefit-risk profile of a vaccine rather than solely its reactogenicity profile.
More serious adverse events often termed “adverse events of special interest (AESI)”, are quite rare but not unknown. A range of rare, serious adverse events were reported at low frequencies in mRNA vaccinated adults in clinical trials, including myocardial infarction, Bell’s palsy, cerebral venous sinus thrombosis, Guillain Barre syndrome, pulmonary embolism, stroke, thrombosis with thrombocytopenia, lymphadenopathy, appendicitis, herpes zoster reactivation, neurological complications and autoimmunity as well as myocarditis and pericarditis [123] but the frequency of many of these events were not different to that observed in the placebo arms of the trials [124].
The most significant AESI that has been clearly established for mRNA COVID-19 vaccines, myocarditis and pericarditis, are rare, occurring at only 1 or 2 cases per 100,000 people, and at much lower frequencies than in populations with SARS-CoV2 virus infection [125,126]. At such low frequencies these adverse events may not manifest in a clinical trial with 10,000 or 20,000 subjects in the vaccinated trial arm. The highest risk of myocarditis and pericarditis was in males under 40 years of age [127,128] although a review of safety outcomes following COVID-19 vaccination in 5.1 million English children emphasized that the overall safety profile was positive [127]. A recent study proposed a mechanism for myocarditis and pericarditis resulting from COVID-19 mRNA vaccines, identifying and inflammatory reaction in the cardiac tissue [129] with increases in circulating interleukins, chemokines and matrix metalloproteases. There was no evidence that antibodies to the virus spike protein were involved.
While some have proposed that myocarditis and/or myocarditis may be a class effect of mRNA vaccines, the evidence for this is mixed. For example, no myocarditis or pericarditis safety signals have been observed in the recently approved mRNA RSV vaccine or in other mRNA vaccines under development. Evaluation of the longer-term safety and effectiveness of mRNA-1273 (Moderna Inc.) in individuals enrolled in the original clinical trials [130] showed that the safety outcomes for boosters were similar to primary vaccination. One case of myocarditis was observed among over 16,000 people receiving the booster of the vaccine. There have been some deaths attributed to myocarditis following vaccination with mRNA COVID vaccines [131] but overall patients with myocarditis after COVID-19 vaccination do well, although some require medical care for several months. A recent study on the longer-term prognosis [132] using French national health data indicated that cardiovascular events after myocarditis following COVID-19 vaccination were less severe than after other causes of myocarditis.
Some studies have postulated possible mechanisms for myocarditis and pericarditis from mRNA COVID-19 vaccines, but there is no clear consensus and several confounding issues [133]. Possible mechanisms include that the immune system might detect the mRNA in the vaccine as an antigen, resulting in the activation of pro-inflammatory cascades and immunological pathways in the heart. This hypothesis is not supported by the lack of immune-related adverse effects in other organs. Molecular mimicry between the spike protein of SARS-CoV-2 and cardiac proteins is another possible mechanism. It has also been postulated that testosterone may have a role given the higher incidence of myocarditis in younger males. Additionally, Kadkhoda [134] postulated that circulating mRNA-LNPs could be endocytosed by cardiac tissue, with local production of spike protein on cardiac cells attracting neutrophils that also express ACE2 on their surfaces. Again, the question of why this was not observed with other organs was raised. Altman et al. [135] proposed that myocarditis may be caused by inflammatory cell infiltrates or by microvascular thrombosis. Buoninfante et al. [136] have recently reviewed possible mechanisms involving spike proteins, lipid nanoparticle pro-inflammatory responses, sex hormones and autoimmune and genetic factors but concluded that “there is still no clear understanding of the biological mechanism/s responsible”.
A wide range of different types of vaccines have been associated with myocarditis and pericarditis and include live attenuated and protein subunit vaccines such as vaccines for smallpox, anthrax, possibly influenza [135,137]. In addition, assessment of reports from the WHO VigiBase database demonstrated that the Novavax COVID protein vaccine has been associated with a similar frequency of myocarditis events than the mRNA COVID vaccines [138]. It is unclear, therefore whether rare myocarditis will be observed with other mRNA vaccines or therapeutics, and if it is, whether there would be a difference in frequency compared with other vaccines developed for the same disease.
In many countries, the largest numbers of adverse events were reported for COVID-19 vaccines, including mRNA vaccines, but this should be viewed against the massive numbers of vaccinations administered for COVID-19 and promotion by government and other health agencies for individuals to report adverse events, even if the reporting individual was unclear whether there was any potential association with vaccination. In addition, the majority of the reported adverse events were reactogenicity-related.
It is important to differentiate adverse events which have been reported from those that have been confirmed and attributed to vaccination including through in-depth population-based studies and statistical approaches. Studies of the background rates of particular conditions in the community, particularly assessed by age and sex are critical [139]. The WHO has published guidance on causality assessment of adverse events following vaccination [140]. Where there is at least a reasonable possibility that a vaccine could have caused a suspected side effect, regulatory agencies include this information in the product information document or label for the vaccine. The information is also summarised in the consumer package leaflet, e.g., by the European Medicines Agency [141,142]. Apart from myocarditis and pericarditis, both vaccines list other possible adverse events as
- Bell’s palsy (temporary one-sided facial drooping)
- swelling of the face
- severe allergic reaction
- extensive swelling of the vaccinated limb
- swelling of the face in patients who have had facial dermatological fillers
- a skin reaction (erythema multiforme)
- unusual (paraesthesia) or decreased sensation in the skin (hypoaesthesia)
- heavy menstrual bleeding
Extensive swelling of the vaccinated limb and skin rashes (mechanical urticaria and chronic urticaria) are also listed as possible adverse events in the EMA package leaflet for the Moderna vaccine to the SARS-Cov2 XBB.1.5 variant. A possible safety signal for acute disseminated encephalomyelitis (ADEM) and transverse myelitis for mRNA COVID-19 vaccines has been identified in a global study of 99 million vaccinated individuals [126] although a second study of 6.7 million people did not identify this signal [143]. In any event, the absolute risk of both forms of myelitis is low, being under 2 in a million doses. Regulators continually review safety signals to determine whether additional adverse events are identified.
Another claim that has been made by some groups is that the commercial mRNA COVID vaccines contained large levels of contamination of DNA fragments from the plasmid used for initial transcription of the mRNA [144,145]. However, these claims have been strongly rebutted by regulators (e.g., the Australian Therapeutic Goods Administration [146]), and scientific groups [147]. In these rebuttals it is noted that the fluorometric method used for DNA measurements in several of these studies provides significant over-estimates when RNA is present, that the samples tested were expired vaccine samples of unknown provenance and that the laboratories undertaking the testing appear not to have formal accreditation as an analytical facility. It is also emphasized that residual DNA, even if it were present at high levels, cannot alter human DNA. Moreover, the TGA has published laboratory lot testing data for the commercial mRNA vaccines indicating that residual DNA levels are very low and meet international regulatory requirements [148].
8. Social License to Operate for mRNA Products
The COVID-19 vaccines (including the mRNA vaccines) have been estimated as saving almost 20 million lives in their first years of administration [149]. However, their introduction and roll-out, particularly of the mRNA vaccines, also was accompanied by concerns in some parts of society. Surveys across many countries have revealed very significant differences in consumer preparedness to take new mRNA vaccines following their regulatory approval [150].
Some expressed concerns that the mRNA vaccines had been developed and approved by regulators quickly and with little supporting evidence, as well as a wider lack of trust in the science [151]. In countries such as the US, where emergency use authorizations rather than regulatory approvals were employed, this may have contributed to this view. In Australia and some other countries, the vaccines initially received provisional or conditional approvals, and the fact that these were “provisional” rather than full approvals also contributed to the same sentiments. Significant education and communication campaigns, including from the International Coalition of Medicines Regulatory Authorities attempted to address these issues [152].
Concerns around safety risks also contributed to vaccine hesitancy. Regulators globally published regular safety reports, but there was conflation by some sources of the reporting of adverse events with their actual causality. A recent French survey [153] identified that 62 % of those surveyed felt that there was “still a lot that we don’t know about the side effects of mRNA vaccines”, and the same percentage either agreed or did not know whether “mRNA vaccines modified the DNA of those vaccinated”. Mandatory vaccination requirements at the height of the pandemic in some countries for certain occupations was also divisive, with many seeing it as necessary to limit exposure to infection in vulnerable and high-risk groups [154], while others took the view that it was a violation of human rights.
Concerns about international equity, which included limited access to mRNA vaccines by certain developing countries in first 12-18 months of vaccine availability, obstacles to the use of the technologies in these countries such as cold chain access and lack of local manufacturing capacity were also factors in opposition by some to mRNA and other COVID-19 vaccines. WHO and the Medicines Patent Pool have implemented a global mRNA technology transfer program [155], establishing a global collaborative network with a hub in South Africa. Several Asian developing and middle-income countries are also establishing capacity for mRNA vaccine manufacture.
Vaccine hesitancy has been defined as “a state of indecisiveness regarding a vaccine decision” [156] rather than opposition to vaccination. An increase in hesitancy commenced well before the introduction of mRNA vaccines or the COVID pandemic and has been considered by the WHO as a top 10 global health threat following an increase in measles cases globally. There is some debate around the best approaches to reduce vaccine hesitancy. While most agree that it is important to respect that the decision whether to be vaccinated is an individual one, some argue that government can play a stronger facilitating role by facilitating low-cost or free access in communities, developing culturally-appropriate resources or investing in health systems especially those targeting marginalised groups [157]. There is evidence that hesitancy contributed to the severity of COVID-19 waves in some countries [158,159]. Over the last couple of years, the issue seems to be “vaccine fatigue” (a loss of interest in receiving a mRNA (or any) COVID vaccine), despite strong recommendations from health authorities that particularly the elderly and vulnerable should avail themselves of COVID-19 boosters. Several factors may be responsible including evidence that the more recent variants have lower mortality and morbidity than earlier ones as well as general desire to put COVID “in the rear vision mirror”.
The final issue relates to misinformation about the safety or other effects of mRNA vaccines [160]. There has been extensive information circulated, particularly through social media, for example that spike proteins and protein fragments encoded by the vaccines and LNPs are toxic, that mRNA or DNA copies of mRNA vaccines can somehow incorporate into the genomes of recipients of the vaccines, and that mRNA vaccination have led to significant increases in death rates in the populations, including of celebrities who have died suddenly. Other misinformation campaigns relate to mRNA vaccines being seen as a tool of control by governments or big pharma. Even more than four years after the first mRNA COVID-19 vaccinations, misinformation is rife. A recent survey of nearly 1500 US adults published in July 2024 [161] revealed that 28 % of Americans believe that COVID-19 vaccines have been responsible for thousands of deaths while 22 % believe that it is safer to get a COVID-19 infection than be vaccinated.
Several approaches have been proposed to increase confidence in COVID-19 mRNA vaccination. There is a role for genuine community engagement and empowerment to combat mis- and dis-information. Use of community organizations and leaders who have established trust has been successful [162]. Employers and healthcare providers and local governments that had strong community connections were also seen as trusted sources of vaccination advice [162,163]. Traditional communication strategies from government worldwide were often “one way”, and unresponsive to emerging community concerns, they missed opportunities to address misinformation early and insufficiently utilised social media platforms, despite this being the platform used to seek information by many in the community. Van der Linden [165] has made some valuable suggestions on how misinformation can be better managed.
The WHO Science Council has recently recommended that WHO utilises its reputation to address misinformation and disinformation around mRNA vaccines (although many of those who do not trust government also particularly distrust international institutions). Health care professionals, trusted community leaders and trusted friends and family may have a greater impact. Another approach may be “prebunking”, wherein organisations pre-emptively build resilience against anticipated exposure to misinformation”, including building consumer capacity to detect information manipulation and deliberate dissemination of false information [166].
The concept of the pharma industry, including sponsors of mRNA vaccines requiring a “social license to operate” will almost certainly gain momentum in the coming years (Figure 2). The term was initially coined in the 1990s by the forestry industry and related to the environmental “license” that they could achieve with society by demonstrating that their harvesting activities were responsible and environmentally sustainable [167]. It has since been used more widely by the mining industry [168] as well as in aquaculture but is increasingly being applied to banking, public policy and tourism, but in health is coming to the fore in the discussions on acceptable boundaries for health research and use of artificial intelligence and other approaches to mine sensitive personal health data [169]. Some jurisdictions, such as the USA and New Zealand, permit direct communication on vaccines between companies and consumers, while many OECD countries do not. While some studies have suggested that vaccine sale increased following direct to consumer advertising [170] other studies have shown that vaccine promotion requires greater nuance to encourage vaccine uptake [171]. Interestingly, the social license argument has been turned on its head to emphasis the social responsibility of parents deciding to have their children vaccinated, given the implications, if unvaccinated, of the spread of vaccine-preventable diseases to others [172].
9. Conclusions
mRNA vaccines have been among the most widely used therapeutic products globally in the last decade. Just under 2 billion doses of the two major mRNA COVID-19 vaccines (from Pfizer-BioNTech and Moderna) have been administered in the EU, US, Canada and Japan combined, in the period to 10 August 2024 [30]. While a wide range of mRNA products for infectious disease as well as rare disease and oncology were under development before the COVID pandemic, from the first global authorization of a COVID-19 mRNA vaccine it took about 3 ½ years until the first mRNA vaccine for another disease (Moderna’s RSV vaccine) to receive regulatory approval. However, based on the robust pipeline of late-stage clinical trials [1] a significant number of regulatory submissions for mRNA products is anticipated in 2025 and the following years for a wide range of indications.
In this review, I have examined several critical aspects of the lifecycle of mRNA vaccines and therapeutics. These include the design and optimization of the mRNA sequence, including through the application of AI approaches. CMC issues affect manufacturing and the stability of mRNA vaccines influencing storage and deployment approaches. Clinical trial considerations, including approaches for trialling vaccines against highly lethal diseases were also discussed, while the extensive global safety experience with mRNA vaccines was reviewed.
mRNA COVID-19 vaccines were rapidly developed and regulatory review and approvals undertaken efficiently without compromising product safety, quality or efficacy. Outside pandemic conditions it will be important to maintain development and regulatory efficiencies by finalizing the development of the range of mRNA platform technology regulatory guidelines that are currently under development and to ensure that there is international alignment between regulatory approaches to the extent possible. With several mRNA therapeutics in advanced development, it is critical to obtain clarity on the regulatory approaches to be used for evaluation of these products, in particular for individualized neoantigen oncology therapies, where the mRNA sequence in the drug product administered to each patient differs.
It is often said that “vaccination, not vaccines, prevent disease”. Therefore, incentives and barriers to vaccination are an important part of the life cycle considerations for mRNA products. We have reviewed some of the sources of hesitancy and resistance to vaccination, some of which are specific to mRNA products, and reviewed some proposed approaches to address hesitancy and resistance. While recognising the right of individual choice, we believe that for those facing a diagnosis of cancer or who are parents of a child with a serious rare metabolic disease, the considerations may be different. There will likely be a higher acceptance of mRNA therapeutics than for many healthy individuals considering vaccination against a disease that they may consider they only have a limited chance of contracting.
Author Contributions
The author shaped the structure and issues in the paper including conceptualization and also drafted the paper.
Funding
The author is a salaried part-time professor at the University of Melbourne, Australia.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article.
Acknowledgments
The author acknowledges the support of a working group which met several times in late 2023 and early 2024 and discussed several of the concepts in the review, with representation from Australian industry; University of Melbourne, Monash University, University of New South Wales, University of Western Australia; mRNA Victoria; Pharmaceutical Benefits Advisory Committee, Victorian and NSW State Governments, and Bellberry Limited. He is also grateful to AusBiotech Limited and the BioMelbourne Network for organising workshops at which he presented and discussed some of the concepts in the paper were discussed.
Conflicts of Interest
None.
References
- Skerritt, J.H.; Tucek-Szabo, C.; Sutton, B.; Nolan, T. The Platform Technology Approach to mRNA Product Development and Regulation. Vaccines 2024, 12, 528–556. [Google Scholar] [CrossRef] [PubMed]
- Webb, C.; Ip, S.; Bathula, N.V.; Popova, P.; Soriano, S.K.V.; Ly, H.H.; Eryilmaz, B.; Huu, V.A.N.; Broadhead, R.; Rabel, M.; et al. Current Status and Future Perspectives on MRNA Drug Manufacturing. Mol. Pharm. 2022, 19, 1047–1058. [Google Scholar] [CrossRef]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). Harmonised guideline technical and regulatory considerations for pharmaceutical product lifecycle management (Q12) November 2019. Available online: https://database.ich.org/sites/default/files/Q12_Guideline_Step4_2019_1119.pdf (accessed on 10 January 2025).
- Androsavich, J.R. Frameworks for the transformational breakthroughs in RNA-based medicines. Nature Rev. Drug Discov. 2024, 23, 412–444. [Google Scholar] [CrossRef] [PubMed]
- Niu, D.; Wu, Y.; Lian, J. Circular RNA vaccine in disease prevention and treatment. Sig Transduct. Target Ther, 2023, 8, 341. [Google Scholar] [CrossRef]
- Su, K.; Shi, L.; Sheng, T.; Yan, X.; Lin, L.; Meng, C.; Wu, S.; Chen, Y.; Zhang, Y.; Wang, C.; et al. Reformulating lipid nanoparticles for organ-targeted mRNA accumulation and translation. Nature Comm. 2024, 15, 5659. [Google Scholar] [CrossRef]
- Kon, E.; Ad-El, N.; Hazan-Halevy, I.; Stosky-Oterin, L.; Peer, D. Targeting cancer with mRNA-lipid nanoparticles: key considerations and future prospects. Nat Rev. Clin. Oncol. 2023, 20, 739–0754. [Google Scholar] [CrossRef]
- Cullis, P.R.; Feigner, P.L. The 60-year evolution of lipid nanoparticles for nucleic acid delivery. Nat. Rev. Drug Discov. 2024, 23, 709–722. [Google Scholar] [CrossRef]
- Kang, D.D.; Li, H.; Dong, Y. Advancements of in vitro transcribed mRNA (IVT mRNA) to enable translation into the clinics. Adv. Drug Deliv. Rev. 2023, 199, 114961. [Google Scholar] [CrossRef] [PubMed]
- Metkar, M.; Pepin, C.S.; Moore, M.J. Tailor made: the art of therapeutic mRNA design. Nature Rev. Drug Discov. 2024, 23, 67–83. [Google Scholar] [CrossRef]
- Wei, H.-H.; Zheng, L.; Wang, Z. mRNA therapeutics: new vaccination and beyond. Fundamental Res. 2023, 3, 749–759. [Google Scholar] [CrossRef]
- Brisse, M.; Vrba, S.M.; Kirk, N.; Liang, Y.; Ly, H. Emerging Concepts and Technologies in Vaccine Development. Front. Immunol. 2020, 11, 583077. [Google Scholar] [CrossRef] [PubMed]
- Roseman, D.S.; Khan, T.; Rajas, F.; Jun, L.S.; Asrani, K.H.; Isaacs, C.; Farelli, J.D.; Subramanian, R.R. G6PC mRNA therapy positively regulates fasting blood glucose and decreases liver abnormalities in a mouse model of glycogen storage disease 1a. Mol. Ther. 2018, 26, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Bicknell, A.A.; Reid, D.W.; Licata, M.C.; Jones, A.K.; Cheng, Y.M.; Li, M.; Hsiao, C.J.; Pepin, C.S.; Metkar, M.; Levdansky, Y.; et al. Attenuating ribosome load improves protein output from mRNA by limiting translation-dependent mRNA decay. Cell Reports. 2024, 43, 114098. [Google Scholar] [CrossRef]
- Vostrosablin, N.; Lim, S.; Gopal, P.; Brazdilova, K.; Parajuli, S.; Wei, X.; Gromek, A.; Prihoda, D.; Spale, M.; Muzdal, A.; et al. mRNAid, an open-source platform for therapeutic mRNA design and optimization strategies. NAR Genom. Bioinformat. 2024, 6, Iqae028. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, L.; Lin, A.; Xu. C.; Li. Z.; Liu, K.; Liu, B.; Ma, X.; Zhao, F.; Jiang, H. et.al. Algorithm for optimized mRNA design improves stability and immunogenicity. Nature 2023, 621, 396–403. [CrossRef] [PubMed]
- Lv, H.; Shi, l.; Berkenpas, J.W.; Dao, F-Y.; Zulfiqar, H.; Ding, H.; Zhang, Y.; Yang, L. Cao, R. Application of artificial intelligence and machine learning for COVID-19 drug discovery and vaccine design. Brief Bioinform. 2021, 22, bbab320.
- Leppek, K.; Byeon, G.W.; Kladwang, W.; Wayment-Steele, H.K.; Kerr, C.H.; Xu, A.F.; Kim, D.S.; Topkar, V.V.; Choe, C.; Rothschild, D.; et al. Combinatorial optimization of mRNA structure, stability, and translation for RNA-based therapeutics. Nature Commun. 2022, 13, 1536–1557. [Google Scholar] [CrossRef]
- McCaffrey, P. Artificial intelligence for vaccine design. Methods Mol. Biol. 2022, 2412, 3–13. [Google Scholar]
- Thomas, S.; Abraham, A.; Baldwin, J.; Piplani, S.; Petrovsky, N. Artificial intelligence in vaccine and drug design. Methods Mol. Biol. 2022, 2410, 131–146. [Google Scholar]
- Dolgin, E. Personalized cancer vaccines pass first major clinical test. Nat. Rev. Drug Discov. 2023, 22, 607–609. [Google Scholar] [CrossRef]
- Kim, Y-A.; Mousavi, K.; Yazdi, A.; Zwierzyna, M.; Cardinali, M.; Fox, D.; Peel, T.; Coller, J.; Aggarwal, K.; Maruggi, G. Computational design of mRNA vaccines. Vaccine, 2024, 42, 1831–1840.
- Xu, Z.; Wang, X.; Zeng, S.; Ren, X.; Yan, Y.; Gong, Z. Applying artificial intelligence for cancer immunotherapy. Acta Pharm. Sin. B, 2021, 11, 3393–3405. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.C.; Chai, S.; Washington, A.R.; et al. Machine-learning prediction of tumor antigen immunogenicity in the selection of therapeutic epitopes. Cancer Immunol. Res. 2019, 7, 1591–1604. [Google Scholar] [CrossRef]
- Shao, X.M.; Bhattacharya, R.; Huang, J.; Sivakumar, I.K.A.; Tolkheim, C.; Zheng, L.; Hirsch, D.; Kaminow, B.; Omdahl, A.; Bonsack, M.; et al. High-throughput prediction of MHC class I and II neoantigens with MHCnuggets. Cancer Immunol. Res. 2020, 8, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A. , Dixit, S., Srinivasan, K.M. D.; Vincent, P.M.D.R. Personalized cancer vaccine design using AI-powered technologies. Front. Immunol. 2024, 15, 1357217. [Google Scholar] [CrossRef]
- Lewis, M.M., Beck, T.J; Ghosh, D. Applying machine learning to identify ionizable lipids for nanoparticle-mediated delivery of mRNA. 2023, Preprint. [CrossRef]
- Xu, Y.; Ma, S.; Cui, H.; Chen, J.; Xu, S.; Gong, F.; Golubovic, A.; Zhou, M.; Wang, K.C.; Varley, A.; et al. AGILE platform: a deep learning powered approach to accelerate LNP development for mRNA delivery. Nature Comms. 2024, 15, 6305. [Google Scholar] [CrossRef]
- Van der Meel, R.; Grisoni, F.; Mulder, W.J.M. Lipid discovery for mRNA delivery guided by machine learning. Nature Materials, 2024, 23, 880–881. [Google Scholar] [CrossRef]
- Our World in Data, “COVID-19, vaccinations”. Available online: https://ourworldindata.org/grapher/cumulative-covid-vaccinations (accessed on December 22, 2024).
- Sparrow, E.; Hasso-Agopsowicz, M.; Kaslow, D.C.; Singh, K.; Rao, R.; Chibi, M.; Makubalo, L.E.; Reeder, J.C.; Kang, G. Karron, R.A.; et al. Leveraging mRNA Platform Technology to Accelerate Development of Vaccines for Some Emerging and Neglected Tropical Diseases Through Local Vaccine Production. Front. Trop. Dis., 2022, 3, 844039. [Google Scholar] [CrossRef]
- Van Tilbeurgh, M.; Lemdani, K.; Beignon, A.-S.; Chapon, C.; Tchitchek, N.; Cheraitia, l.; Lopez, E.M.; Pascal, Q.; Le Grand, R.; Maisonnasse, P.; et al. Predictive Markers of Immunogenicity and Efficacy for Human Vaccines. Vaccines 2021, 9, 579–615. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Expedited Program for Serious Conditions — Accelerated Approval of Drugs and Biologics Guidance for Industry. Draft Guidance December 2024. Available online: https://www.fda.gov/media/184120/download (accessed on 8 January 2025).
- Lo, M.K.; Spengler, J.R.; Welch, S.R.; Harmon, J.R.; Coleman-McCray, J.D.; Scholte, F.E.M.; Shrivastava-Ranjan, P.; Montgomery, J.M.; Nichol, S.T.; Weissman, D. et.al. Evaluation of a Single-Dose Nucleoside-Modified Messenger RNA Vaccine Encoding Hendra Virus-Soluble Glycoprotein Against Lethal Nipah virus Challenge in Syrian Hamsters. J Infect Dis. 2019, 221 (Suppl 4), S493–S498. [Google Scholar] [CrossRef]
- Loomis, R.J.; DiPiazza, A.T.; Falcone, S.; Ruckwardt, T.J.; Morabito, K.M.; Abiona, O.M.; Chang, L.A.; Caringal, R.T.; Presnyak, V.; Narayanan, E.; et al. Chimeric Fusion (F) and Attachment (G) Glycoprotein Antigen Delivery by mRNA as a Candidate Nipah Vaccine. Front. Immunol. 2021, 12, 772864. [Google Scholar] [CrossRef] [PubMed]
- Geisbert, T.W.; Bobb, K.; Borisevich, V.; Geisbert, J.B.; Agans, K.N.; Cross, R.W.; Prasad, A.N.; Fenton, K.A.; Yu, H. Fouts, T.R.; et al. A single dose investigational subunit vaccine for human use against Nipah virus and Hendra virus. Npj Vaccines, 2021, 6, 23. [Google Scholar] [CrossRef]
- Meyer, M.; Huang, E.; Yuzakov, O.; Ramanathan, P.; Ciaramella, G.; Bukreyev, A. Modified mRNA-based vaccines elicit robust immune responses and protect guinea pigs from Ebola virus disease. J. Infect. Dis. 2018, 217, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Alberer, M. Gand-Vogt, U.; Hong, H.S.; Mehr, K.T.; Backert, L.; Finak, G.; Gottardo, R.; Bica, M.A. Garofino, A.; Koch, S.D.; et al. Safety and immunogenicity of a mRNA rabies vaccine in healthy adults: an open-label, non-randomised, prospective, first-in-human phase 1 clinical trial. Lancet 2017, 390, 1511–1520. [Google Scholar] [PubMed]
- Richner, J. M.; Himansu, S.; Dowd, K.A.; Butler, S.L.; Salazar, V.; Fox, J.M.; Julander, J.G.; Tang, W.W.; Shresta, S.; Pierson, T.C.; et al. Modified mRNA vaccines protect against Zika virus infection. Cell 2017, 168, 1114–1125. [Google Scholar] [CrossRef]
- Mucker, E.M.; Freyn, A.W.; Bixler, S.L.; Cizmeci, D.; Atyeo, C.; Earl, P.L.; Natarajan, H.; Santos, G.; Frey, T.R.; Levin, R.H.; et al. Comparison of protection against mpox following mRNA or modified vaccinia Ankara vaccination in nonhuman primates. Cell 2024, 187, 5540–5553. [Google Scholar] [CrossRef]
- August, A. , Attarwala, H.Z., Himansu, S.; et al. A phase 1 trial of lipid-encapsulated mRNA encoding a monoclonal antibody with neutralizing activity against Chikungunya virus. Nat Med 2021, 27, 2224–2233. [Google Scholar] [CrossRef]
- US Food and Drug Administration. New drug and biological drug products: evidence needed to demonstrate effectiveness of new drug when human efficacy studies are not ethical or feasible, USFDA final rule, May 2002. Fed Register. 2002, 67, 37988–37998. [Google Scholar]
- US Food and Drug Administration. Product Development Under the Animal Rule Guidance for Industry, October 2015. Available online: www.fda.gov/media/88625/download. (accessed on 3 August 2024).
- European Medicines Agency. Guideline on procedures for the granting of a marketing authorisation under exceptional circumstances, pursuant to article 14 (8) of Regulation (EC) No 726/2004. Available online: www.ema.europa.eu/en/documents/regulatory-procedural-guideline/guideline-procedures-granting-marketing-authorisation-under-exceptional-circumstances-pursuant/2004_en.pdf (accessed on 3 August 2024).
- Mukonzo, J.K.; Ndagije, H.B.; Sabbiah, G.T.; Mathenge, W.; Price, D.A.; Grasela, T.H. Expanding regulatory science: Regulatory complementarity and reliance. Clin. Trans. Sci. 2024, 17, e13683. [Google Scholar] [CrossRef]
- Schoenmaker, L.; Witzigmann, D.; Kulkarni, J.A.; Verbeke, R.; Kersten, G.; Jiskoot, W.; Crommelin, D.J.A. mRNA-lipid nanoparticle COVID-19 vaccines: structure and stability. Int J. Pharmaceutics. 2021, 601, 120586. [Google Scholar] [CrossRef]
- Demongeot, J.; Fougere, C. mRNA COVID-19 Vaccines—Facts and hypotheses on fragmentation and encapsulation. Vaccines 2023, 11, 40–65. [Google Scholar] [CrossRef]
- Cheng, F.; Wang, Y.; Bai, Y.; Liang, Z.; Mao, Q.; Liu, D.; Wu, X.; Xu, M. ; Research advances on the stability of mRNA vaccines. Viruses 2023, 15, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Chheda, U.; Pradeepan, S.; Esposito, E.; Strezsak, S.; Fernadez-Delgado, O.; Kranz, J. Factors affecting stability of RNA – Temperature, length, concentration, pH and buffering species. J. Pharm. Sci. 2024, 113, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Binzel, D.W. , Li X., Burns N., Khan E., Lee W., Chen L.-C., Ellipilli S., Miles W., Soon Ho Y., Guo P. Thermostability, tunability and tenacity of RNA as Rubbery Anionic Polymeric Materials in nanotechnology and nanomedicine—Specific cancer targeting with undetectable toxicity. Chem. Rev. 2021, 121, 1322–1335. [Google Scholar]
- Oude Blenke, E.; Ornskov, E.; Schoneich, C.; Nilsson, G.A.; Volkin, D.B.; Mastrobattista, E.; Almarsson, O.; Crommelin, D.J.A. The Storage and In-Use Stability of mRNA Vaccines and Therapeutics: Not A Cold Case. Pharm. Sci. 2023, 112, 386–403. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. Lancet. 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Ai, L.; Li, Y.; Zhou, L.; Yao, W.; Zhang, H.; Hu, Z.; Han, J.; Wang, W.; Wu, J.; Xu. P.; et al. Lyophilized mRNA-lipid nanoparticle vaccines with long-term stability and high antigenicity against SARS-CoV-2. Cell Discovery 2023, 9, 9–24. [Google Scholar] [CrossRef]
- Muramatsu, H.; Lam, K.; Bajusz, C.; Laczko, D.; Kariko, K.; Screiner, P.; Martin, A.; Lutwyche, P.; Heyes, J.; Pardi, N. Lyophilization provides long-term stability for a lipid nanoparticle-formulated nucleoside modified mRNA vaccine. Mol. Ther. 2022, 30, 1941–1962. [Google Scholar] [CrossRef]
- Zhao, P.; Hou, X.; Yan, J.; Du, S.; Xue, Y.; Li, W.; Xiang, G.; Dong, Y. Long-term storage of lipid-like nanoparticles for mRNA delivery. Bioact. Mater. 2020, 5, 358–363. [Google Scholar] [CrossRef]
- Panther, L.; Basnet, S.; Fierro, C.; Brune, D.; Legett, D.; Paterson, J.; Pickrell, P.; Lin, J.; Wu, K.; Lee, H.; et al. 2892. Safety and immunogenicity of mRNA-1647, an mRNA-based cytomegalovirus vaccine in healthy adults: Results of a phase 2, randomized, observer-blind, placebo-controlled, dose-finding trial. Open Forum Infect. Dis. 2023, 10 (suppl 2). [Google Scholar] [CrossRef]
- Zhai, J.; Cote, T.; Chen, Y. Challenges and advances in the stability of mRNA delivery therapeutics. Nucl. Acids Insights 2024, 1, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Stewart-Jones, G.B.E.; Elbashir, S.M.; Wu, K.; Lee, D.; Renzi, I.; Ying, B.; Kock, M.; Sein, C.E.; Choi, A.; Whitener, B.; et al. Domain-based mRNA vaccines encoding spike protein N-terminal and receptor binding domains confer protection against SARS-CoV-2. Sci. Transl. Med. 2023, 15, eadf4100. [Google Scholar] [CrossRef]
- Blin, O.; Lefebvre, N.; Rascol, O.; Micallef, J. Orphan drug clinical development. Therapies. 2020, 75, 141–147. [Google Scholar] [CrossRef]
- Berraondo, P.; Martini, P.G.V.; Avila, M.A.; Fontanellas, A. Messenger RNA therapy for rare genetic metabolic diseases. Gut 2019, 68, 1323–1330. [Google Scholar] [CrossRef]
- Córdoba, K.M.; Jericó, D.; Sampedro, A.; Jiang, L.; Iraburu, M.J.; Martini, P.G.V.; Berraondo, V.P.; Avila, M.A.; Fontanellas, A. Messenger RNA as a personalized therapy: The moment of truth for rare metabolic diseases. Int. Rev. Cell Mol. Biol. 2022, 372, 55–96. [Google Scholar] [PubMed]
- Martini, P.G.V.; Guey, L.T. A new era for rare genetic diseases: Messenger mRNA therapy. Human Gene Therapy, 2019, 30, 1180–1188. [Google Scholar] [CrossRef]
- An, D.; Schneller, D.L.; Frassetto, A.; Liang, S.; Zhu, X.; Park, J.S.; Theisen, M.; Hong, S.J.; Zhou, J.; Rajendran, R.; et al. Systemic messenger RNA therapy as a treatment for methylmalonic acidemia. Cell Rep. 2017, 21, 3548–3558. [Google Scholar] [CrossRef] [PubMed]
- An, D.; Frassetto, A.; Jacquinet, E.; Eybye, M.; Milano, J.; DeAntonis, C.; Nguyen, V.; Laureano, R.; Milton, J.; Sabnis, S.; Lukacs, C.M.; Guey, L.T. Long-term efficacy and safety of mRNA therapy in two murine models of methylmalonic acidemia. EBioMedicine 2019, 45, 519–528. [Google Scholar] [CrossRef]
- Jiang, L.; Berraondo, P.; Jerico, D.; Guey, L.T.; Sampedro, A.; Frassetto, A.; Benenato, K.E.; Burke, K.; Santamaria, E.; Alegre, M.; et al. Systemic messenger RNA as an etiological treatment for acute intermittent porphyria. Nat. Med. 2018, 24, 1899–1909. [Google Scholar] [CrossRef]
- Yu, H.; Brewer, E.; Shields, M.; Crowder, M.; Sacchetti, C.; Soontornniyomkij, B.; Dou, D.; Clemente, B.; Sablad, M.; Chivukula, P.; et al. Restoring ornithine transcarbamylase (OTC) activity in an OTC-deficient mouse model using LUNAR-OTC mRNA. Clin. Transl. Disc. 2022, 2, e33. [Google Scholar] [CrossRef]
- Jiang, L.; Park, J.-S. , Yin, L.; Laureano, R.; Jacquinet, E.; Yang, J.; Liang, S.; Frassetto, A.; Zhuo, J.; Yan, X.; et al. Dual mRNA therapy restores metabolic function in long-term studies in mice with propionic aciduria. Nat. Commun. 2020, 11, 5339–5348. [Google Scholar] [CrossRef]
- Truong, B. Allegri, G.; Liu, X.B.; Burke, K.E.; Zhu, X.; Cederbaum, S.D.; Häberle, J.; Martini, P.G.V.; Lipshutz, G.S.; et al. Lipid nanoparticle-targeted mRNA therapy as a treatment for the inherited metabolic liver disorder arginase deficiency. Proc. Natl. Acad. Sci. USA. 2019, 116, 21150–21159. [Google Scholar] [CrossRef]
- Khoja, S.; Liu, X.B.; Truong, B.; Nitzahn, M.; Lambert, J.; Eliav, A.; Nasser, E.; Randolph, E.; Burke, K.E.; White, R. et. al. Intermittent lipid nanoparticle mRNA administration prevents cortical dysmyelination associated with arginase deficiency. Mol. Ther. Nucleic Acids 2022, 28, 859–874. [Google Scholar] [CrossRef] [PubMed]
- Gurung, S.; Timmermand, O.V.; Perocheau, D.; Gil-Martinez, A.L.; Minnion, M.; Touramanidou, l.; Fang, S.; Messina, M.; Khalil, Y.; Spiewak, J.; et al. RNA therapy corrects defective glutathione metabolism and restores ureagenesis in preclinical argininosuccinic aciduria. Sci. Transl. Med. 2024, 16, 729. [Google Scholar] [CrossRef] [PubMed]
- Koeberl, D.; Schulze, A.; Sondheimer, N.; Lipschultz, G.S.; Geberhiwot, T.; Li, R.; Saini, R.; Luo, J.; Sikirica, V.; Jin, L.; et al. Interim analysis of a first in human phase 1/2 mRNA trial for propionic aciduria. Nature 2024, 628, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Haendel, M.; Vasilevsky, N.; Unni, D.; Bologa, C.; Harris, N.; Rehm, H.; Hamosh, A.; Baynam, G.; Groza, T.; McMurry, J.; et al. How many rare diseases are there? Nat Rev Drug Discov. 2020, 19, 77–78. [Google Scholar] [CrossRef]
- Fermaglich, L.J.; Miller, K.L. A comprehensive study of the rare diseases and conditions targeted by orphan drug designations and approvals over the forty years of the Orphan Drug Act. Orphanet J. Rare Dis. 2023, 18, 163–170. [Google Scholar] [CrossRef]
- Zanello, G.; Garrido-Estepa, M.; Crespo, A.; O’Connor, D.; Nabbout, R.; Waters, C.; Hall, A.; Taglialatela, M.; Chan, C.-H.; Pearce, D.A.; et al. Targeting shared molecular etiologies to accelerate drug development for rare diseases. EMBO Mol Med 2023, 1, e17159. [Google Scholar] [CrossRef]
- Muller, A.R.; Brands, M.M.M.G.; van de Ven, P.M.; Roes, K.C.B.; Cornel, M.C.; van Karnebeek, C.D.M.; Wijburg, F.A.; Daams, J.G.; Boot, E.; van Eeghen, A.M. Systematic Review of N-of-1 Studies in Rare Genetic Neurodevelopmental Disorders: The Power of 1. Neurology, 2021, 96, 529–540. [Google Scholar] [CrossRef]
- Zablin, M.A.; Novack, G. N-of-1 Clinical Trials: A Scientific Approach to Personalized Medicine for Patients with Rare Retinal Diseases Such as Retinitis Pigmentosa. J Ocul Pharmacol Ther. 2021, 37, 495–501. [Google Scholar]
- Lee, C.E.; Singleton, K.S.; Wallin, M.; Faundez, V. Rare Genetic Diseases: Nature’s Experiments on Human Development. iScience. 2020, 23, 101123. [Google Scholar] [CrossRef] [PubMed]
- Iyer, V.R.; Praveen, P.; Kaduskar, B.D.; Moharir, S.C.; Mishra, R.K. mRNA biotherapeutics landscape for rare genetic disorders. J. Biosci. 2024, 49, 33–60. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.; Liu, J.; Yang, H.; Xie, N.; Yang, Y. ; mRNA therapies: pioneering a new era in rare genetic disease treatment. J. Control. Rel. 2024, 369, 696–721. [Google Scholar] [CrossRef]
- Brooks, P.J.; Ottinger, E.A.; Portero, D.; Lomash, R.M.; Alimardanov, A.; Terse, P.; Xu, X.; Chandler, R.J.; Hauserman, J.G.; Esposito, E.; et al. The Platform Vector Gene Therapies Project: Increasing the Efficiency of Adeno-Associated Virus Gene Therapy Clinical Trial Startup. Hum. Gene Ther. 2020, 31, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Vervaeke, P.; Borgos, S.E.; Sanders, N.N.; Combes, F. ; Regulatory guidelines and preclinical tools to study the biodistribution of RNA therapeutics. Adv. Drug Deliv. Res. 2022, 184, 114236. [Google Scholar] [CrossRef]
- Qin, S.; Tang, X.; Chen, Y.; Chen, K.; Fan, N.; Xiao, W.; Zheng, Q.; Li, G.; Teng, Y.; Wu, M.; et al. mRNA-based therapeutics: Powerful and versatile tools to combat diseases. Signal Transduct. Target. Ther. 2022, 7, 166. [Google Scholar] [CrossRef]
- Rohner, E.; Yang, R.; Foo, K.S.; Goedel, A.; Chien, K.R. ; Unlocking the promise of mRNA therapeutics. Nat. Biotech 2022, 40, 1586–1600. [Google Scholar] [CrossRef]
- Parhiz, H.; Atochina-Vasserman, E.N.; Weissman, D. ; mRNA-based therapeutics: Looking beyond COVID-19 vaccines. Lancet 2024, 403, 1192–1204. [Google Scholar] [CrossRef]
- Blass, E.; Ott, P.A. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat Rev. Clin. Oncol. 2021, 18, 215–229. [Google Scholar] [CrossRef]
- Xie, N.; Shen, G.; Gao, W.; Huang, Z.; Huang, C.; Fu, Li. Neoantigens: promising targets for cancer therapy. Signal Transduct. Targeted Ther. 2023, 8, 9–46. [Google Scholar] [CrossRef]
- Trivedi, V.; Yang, C.; Klippel, K.; Yegorov, O.; von Roemeling, C.; Hoang-Minh, L.; Fenton, G.; Ogando-Rivas, E.; Castillo, P.; Moore, G.; et al. mRNA-based precision targeting of neoantigens and tumor-associated antigens in malignant brain tumors. Genome Med, 2024, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Wu, D-W. ; Jia, S-P.; Xing, S-J.; Ma, H-I.; Wang, X.; Tang Q-Y.; Li, Z-W.; Wu, Q.; Bai, M.; Zhang, X-Y.; et al. Personalized neoantigen cancer vaccines: current progression, challenges and a bright future. Clin. Exp. Med. 2024, 24, 229–239. [Google Scholar] [CrossRef]
- Cafri, G.; Gartner, J.J.; Zaks, T.; Hopson, K.; Levin, N.; Paria, B.C.; Parkhurst, M.R.; Yossef, R.; Lowery, F.J. Jafferji, M.S.; et al. mRNA vaccine–induced neoantigen-specific T cell immunity in patients with gastrointestinal cancer. J. Clin. Invest. 2020, 130, 5976–5988. [Google Scholar] [CrossRef]
- Weber, J.S.; Carlino, M.S.; Khattak, A.; Meniawy, T.; Ansstas, G.; Taylor, M.H.; Kim, K.B.; McKean, M.; Long, G.V.; Sullivan, R.J.; et al. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): A randomized, phase 2b study. Lancet 2024, 403, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Lang, F.; Schrors, B.; Lower, M.; Tureci, O.; Sahin, U. Identification of neoantigens for individualized therapeutic cancer vaccines. Nature Rev. Drug Discov. 2022, 21, 261–282. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.A.; Sethna, Z.; Soares, K.C.; Olcese, C.; Pang, N.; Patterson, E.; Lihm, J.; Ceglia, N.; Guasp, P.; Chu, A.; et al. Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer. Nature 2023, 618, 144–150. [Google Scholar] [CrossRef]
- May, M. How mRNA is powering a personalized vaccine revolution. Nature Med. 2024, 30, 2097–2098. [Google Scholar] [CrossRef]
- Jonker, A.H.; Taturu, E-A. ; Graessner, H.; Dimmock, D.; Jaffe, A.; Bayman, G.; Davies, J.; Mitkus, S.; Ilianch, O.; Horgan, R.; et al. The state-of-the-art of N-of-1 therapies and the IRDiRC N-of-1 development roadmap. Nat. Rev. Drug Discov. 2025, 24, 40–56. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Guidance for Industry: Clinical Considerations for Therapeutic Cancer Vaccines, October 201. Available online: www.fda.gov/media/82312/download. (accessed on August 3, 2024).
- Ministry of Food and Drug Safety, South Korea. Considerations on the Development of Personalized Neoantigen-Targeted Therapy Products (Guidance for Industry), September 2024. Available online: www.mfds.go.kr/eng/brd/m_1127/list.do. (accessed on 12 November 2024).
- Medicines and Health products Regulatory Agency. Draft guideline on individualised mRNA cancer immunotherapies, February 2025. Available online: https://assets.publishing.service.gov.uk/media/6799ef4d9a6dc0352ab34225/Individualised_mRNA_cancer_immunotherapies_0.6.5.pdf (accessed on 10 February 2025).
- Guerriaud, M.; Kohli, E. RNA-based drugs and regulation: Toward a necessary evolution of the definitions issued from the European union legislation. Front. Med. 2022, 9, 1012497. [Google Scholar] [CrossRef]
- von Fritschen, M.; Haber, C.; Straus, W.; Schneider, C.K.; Janosz, E.; Jägle, U.; Mendila, M.; Blume, C. Defining Gene Therapy Medicinal Products in the EU: Scientific and Regulatory Perspectives. DIA Global Forum, March 2024. Available online: https://globalforum.diaglobal.org/issue/march-2024/defining-gene-therapy-medicinal-products-in-the-eu/ (accessed on 8 January 2025).
- US Food and Drug Administration. Frequently Asked Questions — Developing Potential Cellular and Gene Therapy Products Draft Guidance for Industry. Nov 2024. Available online: www.fda.gov/media/183631/download (accessed on 8 January 2025).
- Aust, A. Regulatory strategies for developing and manufacturing RNA-LNPs. Nucl. Acids Insights. 2024, 1, 139–145. [Google Scholar] [CrossRef]
- Djonova, J. Swiss regulatory aspects and evaluation considerations for ATMPs and other nucleic acid-based products such as mRNA vaccines. Vaccine Insights. 2024, 3, 91–95. [Google Scholar] [CrossRef]
- Wan, K-W. ; Galway, F. MHRA regulatory considerations in the quality of mRNA products. Nucl. Acids Insights, 2024, 1, 149–154.
- International Conference On Harmonisation Of Technical Requirements For Registration Of Pharmaceuticals For Human Use. Development and manufacture of drug substances (chemical entities and biotechnological/biological entities). Q11 guideline, May 2012. Available online: https://database.ich.org/sites/default/files/Q11%20Guideline.pdf (accessed on 14 November 2024).
- International Council For Harmonisation Of Technical Requirements For Pharmaceuticals For Human Use. ICH harmonised guideline analytical procedure development Q14 guideline, March 2022. Available online: https://database.ich.org/sites/default/files/ICH_Q14_Document_Step2_Guideline_2022_0324.pdf (accessed on 14 November 2024).
- European Medicines Agency. 20 April 1873.
- US Food and Drug Administration (Draft) Guidance Document: Platform Technology Designation Program for Drug Development, May 2024. Available online at: www.fda.gov/regulatory-information/search-fda-guidance-documents/platform-technology-designation-program-drug-development (accessed ). 3 August.
- World Health Organization. Evaluation of the Quality, Safety and Efficacy of Messenger RNA Vaccines for the Prevention of Infectious Diseases: Regulatory Considerations. World Health Organization Expert Committee on Biological Standardization 74th Report, 2022, Annex 3.Available online at: www.who.int/publications/m/item/evaluation-of-the-quality-safety-and-efficacy-of-messenger-rna-vaccines-for-the-prevention-of-infectious-diseases-regulatory-considerations. (accessed on 11 November 2024).
- European Medicines Agency. Concept Paper on the Development of a Guideline on the 5 Quality Aspects of mRNA Vaccines, May 2023. Available online at: www.ema.europa.eu/en/documents/scientific-guideline/concept-paper-development-guideline-quality-aspects-mrna-vaccines_en.pdf. (accessed on 26 March 2024).
- European Directorate for the Quality of Medicines and Healthcare. European Pharmacopoeia Commission adopts first three general texts on mRNA vaccines, January 2025. Available online at: www.edqm.eu/en/-/european-pharmacopoeia-commission-adopts-first-three-general-texts-on-mrna-vaccines. (accessed on 31 January 2025).
- European Medicines Agency. Procedural advice for vaccine platform technology master 5 file (vPTMF) certification. EMA Guidance EMA/CVMP/IWP/286631/2021, May 2022. Available online at: www.ema.europa.eu/en/documents/scientific-guideline/draft-procedural-advice-vaccine-platform-technology-master-file-vptmf-certification_en.pdf. (accessed on 3 August 2024).
- European Directorate for the Quality of Medicines and HealthCare, Human OCABR Guidelines, Available online at: www.edqm.eu/en/omcl/human-ocabr-guidelines (accessed ). 8 January.
- Ball, G.; Reblin, T.; Buchanan, J.; Hendrickson, B.A.; Lewis, E.; Schnell, P.M.; Rockhold, F.W. A framework for safety evaluation throughout the product development life-cycle. Therap. Innov. Reg. Sci. 2020, 54, 821–830. [Google Scholar] [CrossRef]
- Wilson, E.; Goswami, J.; Baqui, A.H.; Doreski, P.A.; Perez-Marc, G.; Zaman, K.; Monroy, J.; Duncan, C.J.A.; Ujiie, M.; Rämet, M.; et al. Efficacy and Safety of an mRNA-Based RSV PreF Vaccine in Older Adults. N Engl J Med. 2023, 389, 2233–2244. [Google Scholar] [CrossRef] [PubMed]
- Herve, C.; Laupeze, B.; Del Guidice, G.; Didierlaurent, A.M.; Da Silva, F.T. The how’s and what’s of vaccine reactogenicity. Npj Vaccines. 2019, 4, 39–49. [Google Scholar] [CrossRef]
- Lee, J.; Woodruff, M.C.; Kim, E.H.; Nam, J.-H. Knife’s edge: Balancing immunogenicity and reactogenicity in mRNA vaccines. Exp. Mol. Med. 2023, 55, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Kobiyama, K.; Ishii, K. J. Making innate sense of mRNA vaccine adjuvanticity. Nat. Immunol. 2022, 23, 474–476. [Google Scholar] [CrossRef]
- Ndeupen, S,; Qin, Z. ; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyártó, B.Z. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience, 2021, 24, 103479. [Google Scholar] [CrossRef]
- Alameh, M.G.; Tombacz, I.; Bettini, E.; Lederer, K.; Ndeupen, S.; Sittplangkoon, C.; Wilmore, J.R.; Gaudette, B.T.; Soliman, O.Y.; Pine, M.; et al. Lipid nanoparticles enhance the efficacy of mRNA and protein subunit vaccines by inducing robust T follicular helper cell and humoral responses. Immunity 2022, 55, 1136–1138. [Google Scholar] [CrossRef]
- Laurini, G.S.; Montanaro, N.; Broccoli, M.; Bonaldo, G.; Motola, D. Real-life safety profile of mRNA vaccines for COVID-19: An analysis of VAERS database. Vaccine 2023, 41, 2879–2886. [Google Scholar] [CrossRef]
- Ramos, A.S.F.; Sanchez, C.L.; Rose, T.B.; Smith, D.; Thorn, N.; Galiza, E.; Miah, T.; Pearce, J.; Hultin, C.; Cosgrove, C.; Hsia, Y.; Heath, P.T. Comparing reactogenicity of COVID-19 vaccine boosters: a systematic review and meta-analysis. Expert Rev. Vaccines. 2024, 23, 266–282. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Myers, T.; Gee, J.; Shay, D.K.; Marquez, P.; Baggs, J.; Zhang, B.; Licata, C.; Shimabukoro, T. Reactogenicity within 2 weeks after mRNA COVID-19 vaccines: Findings from the CDC v-safe surveillance system. Vaccine. 2021, 39, 7066–7073. [Google Scholar] [CrossRef] [PubMed]
- Fraiman, J.; Erviti, J.; Jones, M.; Greenland, S.; Whelan, P.; Kaplan, R.M.; Doshi, P. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine 2022, 40, 5798–5805. [Google Scholar] [CrossRef]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst Rev, 0154. [Google Scholar]
- Alami, A.; Krewski, D.; Farhat, N.; Mattison, D.; Wilson, K.; Gravel, C.A.; Farrell, P.J.; Crispo, J.A.G.; Haddad, N.; Perez-Lloret, S.; et al. Risk of myocarditis and pericarditis in mRNA COVID-19 vaccinated and unvaccinated populations: a systematic review and meta-analysis. BMJ Open 2023, 13, e065687. [Google Scholar] [CrossRef]
- Faksova, K.; Walsh, D.; Jiang, Y; Griffin, J. ; Phillips, A.; Gentile, A.; Kwong, J.C.; Macartney, K.; Naus, M.; Grange, Z.; et al. Covid-19 vaccines and adverse events of special interest: A multinational global vaccine data network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine, 2024, 42, 2200–2211. [Google Scholar] [CrossRef] [PubMed]
- Copland, E.; Patone, M.; Saatchi, D.; Handunnetthi, L.; Hirst, J.; Hunt, D.P.J.; Mills, N.L.; Moss, P.; Sheikh, A.; Coupland, C.A.A.; et al. Safety outcomes following COVID-19 vaccination and infection in 5.1 million children in England. Nature Comms. 2024, 15, 3822. [Google Scholar] [CrossRef]
- Xu, Y.; Li, H.; Santosa, A; Wettermark, B. ; Fall, T.; Bjork, J.; Borjesson, M.; Gisslen, M.; Nyberg, F. Cardiovascular events following coronavirus disease 2019 vaccination in adults: A nationwide Swedish study. Eur. Heart J. 2024, 30, ehae639. [Google Scholar]
- Barmada, A.; Klein, J.; Ranaswamy, A.; Brodsky, N.N.; Jaycox, J.R.; Sheikha, H.; Jones, K.M.; Habet, V.; Campbell, M.; Sumida, T.S.; et al. Cytokinopathy with aberrant cytotoxic lymphocytes and profibrotic myeloid response in SARS-CoV-2 mRNA vaccine-associated myocarditis. Sci. Immunol. 2023, 8, eadh3455. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Follmann, D.; Hachigian, G.; Strout, C.; Overcash, J.S.; Doblecki-Lewis, S.; Whitaker, J.A.; Anderson, E.J.; et al. Long-term safety and effectiveness of mRNA-1273 vaccine in adults: COVE trial open-label and booster phases. Nature Communications 2024, 15, 7469–7481. [Google Scholar] [CrossRef]
- Hulscher, N.; Hodgkinson, R.; Makis, W.; McCullough, P.A. Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis. ESC Heart Failure 2024. [Google Scholar] [CrossRef]
- Semenzato, L; Le Vu, S; Botton, J; Bertrand, M. ; Jabagi, M-J.; Drouin, J.; Cuenot, F.; Zores, F., Dray-Spira, R.; Weill, A.; et al. Long-term prognosis of patients with myocarditis attributed to covid-19 mRNA vaccination, SARS-CoV-2 infection of conventional etiologies. JAMA 2024, 332, 1367–1377. [Google Scholar] [CrossRef]
- Heymans, S; Cooper, L. T. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol. 2022, 19, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Kadkhoda, K. Post RNA-based COVID vaccines myocarditis: proposed mechanisms. Vaccine. 2022, 40, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Altman, N.L.; Berning, A.A.; Mann, S.C.; Quaife, R.A.; Gill, E.A.; Auerbach, S.R.; Campbell, T.B.; Bristow, M. Vaccination-Associated Myocarditis and Myocardial Injury. Circulation Res. 2023, 132, 1338–1357. [Google Scholar] [CrossRef] [PubMed]
- Buoninfante, A.; Andeweg, A.; Genov, G.; Cavaleri, M. Myocarditis associated with COVID-19 vaccination. Npj Vaccines 2024, 9, 122–129. [Google Scholar] [CrossRef]
- Ling, R.R.; Ramanathan, K.; Tan, F.L.; Tai, B.C.; Somani, J.; Fisher, D.; MacLaren, G. ; Myopericarditis following COVID-19 vaccination and non-COVID-19 vaccination: a systematic review and meta-analysis. Lancet Respir Med. 2022, 10, 679–688. [Google Scholar] [CrossRef]
- Saint-Gerons, D.M.; Ibarz, M.T.; Castro, J.L.; Fores-Martos, J.; Tabares-Seisdedsos, R. Myopericarditis associated with the Novavax COVID-19 vaccines (NVX-CoV2373): A retrospective analysis of individual case safety reports from VigiBase. Drugs- Real World Outcomes. 2023, 10, 263–270. [Google Scholar] [CrossRef]
- Ostropolets, A.; Makadia, R.; Shoaibi, A.; Rao, G.; Sena, A.G.; Martinez-Hernandez, E.; Delmestri, A.; Verhamme, K.; Rijnbeek, P.R.; Duarte-Salles, T.; Suchard, M.A.; Ryan, P.B.; Hripcsak, G.; Prieto-Alhambra, D. Characterising the background incidence rates of adverse events of special interest for covid-19 vaccines in eight countries: multinational network cohort study. BMJ. 2021, 373, n1435. [Google Scholar]
- World Health Organization. Causality assessment of an adverse event following immunization (AEFI). User manual for the revised WHO classification. Second edition WHO/HIS/EMP/SAV. Jan 2018. Available online at: https://iris.who.int/bitstream/handle/10665/259959/9789241513654-eng.pdf (accessed ). 14 November.
- European Medicines Agency (2023) Pfizer XBB 1.5 package leaflet, within Annex 1- Summary of Product Characteristics: Comirnaty, INN-tozinameran, tozinameran/famtozinameran, raxtozinameran, bretovameran. Available online at: www.ema.europa.eu/en/documents/product-information/comirnaty-epar-product-information_en.pdf (accessed ). 10 December.
- European Medicines Agency (2023) Moderna XBB 1.5 package leaflet, within Annex 1 – Summary of Product Characteristics: Spikevax, INN-elasomeran, elasomeran/imelasomeran, elasomeran/davesomeran, andusomeran. Available online at: - www.ema.europa.eu/en/documents/product-information/spikevax-epar-product-information_en.pdf (accessed ). 10 December.
- Morgan. H.J.; Clothier, H.J.; Kattan, G.S. Boyd, J.H., Buttery, J.P. Acute disseminated encephalomyelitis and transverse myelitis following COVID-18 vaccination – a self-controlled case series analysis. Vaccine, 2024, 42, 2212–2219. [Google Scholar] [CrossRef]
- Kammerer, U.; Schulz, V.; Steger, K. BioNtech RNA-based COVID-19 injections contain large amounts of residual DNA including an SV40 promoter/enhancer sequence. Sci Pub Health Policy Law. 2024, 5, 2019–2024. [Google Scholar]
- König, B.; Kirchner, J.O. Methodological Considerations Regarding the Quantification of DNA Impurities in the COVID-19 mRNA Vaccine Comirnaty®. Methods Protoc. 2024, 7, 41. [Google Scholar] [CrossRef] [PubMed]
- Therapeutic Goods Administration, Australia. Addressing misinformation about excessive DNA in the mRNA vaccines, Media Release . Available online at: www.tga.gov.au/news/media-releases/addressing-misinformation-about-excessive-dna-mrna-vaccines (accessed 14 November 2024). 18 October.
- Global vaccine data network. Debunking the DNA contamination claims in mRNA vaccines. Available online at: www.globalvaccinedatanetwork.org/news/plasmid-gate_debunking_the_DNA_contamination_claims_in_mRNA_vaccines (accessed ). 14 November.
- Therapeutic Goods Administration, Australia. Summary report of residual DNA and endotoxin on CoVID-19 mRNA vaccines conducted by TGA Laboratories, . Available online at: www.tga.gov.au/resources/publication/tga-laboratory-testing-reports/summary-report-residual-dna-and-endotoxin-covid-19-mrna-vaccines-conducted-tga-laboratories (accessed 14 November 2024). 11 November.
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- Larson, H.J. Understanding vaccine hesitancy: a call for more social science in RNA vaccine research. Vaccine insights.
- Leong, C.; Jin, L.; Kim, D.; Kim, J.; Teo, Y.Y.; Ho, T.-H. Assessing the impact of novelty and conformity on hesitancy towards COVID-19 vaccines using mRNA technology. Comms. Med, 2022, 2, 61. [Google Scholar] [CrossRef]
- European Medicines Agency. International regulators and WHO address need to boost COVID-19 vaccine confidence, June 2021. Available online at: www.ema.europa.eu/en/news/international-regulators-and-who-address-need-boost-covid-19-vaccine-confidence. (accessed ). 14 November.
- Peretti-Watel, P.; Verger, P.; Ward, J.K. To understand mRNA vaccine hesitancy, stop calling the public anti-science. Nature Med. 2024, 30, 923–924. [Google Scholar] [CrossRef] [PubMed]
- Attwell, K.; Rizzi, M.; McKenzie, L.; Carlson, S.J.; Roberts, L.; Tomkinson, S.; Blyth, C.C. COVID-19 vaccine Mandates: An Australian attitudinal study. Vaccine, 2021, 40, 7360–7369. [Google Scholar] [CrossRef]
- Medicines Patent Pool. mRNA Technology transfer programme. Available online at: https://medicinespatentpool. 14 November.
- Bussink-Voorend, D.; Hautvast, J.L.A.; Vandenberg, L.; Visser, O.; Hulscher, M.E.J.L. A systematic literature review to clarify the concept of vaccine hesitancy. Nat. Hum. Behav. 2022, 6, 1634–1648. [Google Scholar] [CrossRef] [PubMed]
- Attwell, K.; Hannah, A.; Leask, J. COVID-19: talk of ’vaccine hesitancy’ lets governments off the hook. Nature, 2022, 602, 574–577. [Google Scholar] [CrossRef]
- de Miguel-Arribas, A.; Aleta, A.; Moreno, Y. Impact of vaccine hesitancy on secondary COVID-19 outbreaks in the US: an age-structured SIR model. BMC Infect Dis. 2022, 22, 511. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Leigh, J.P.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 12, 3801. [Google Scholar] [CrossRef]
- Romer, D.; Winneg, K.M.; Jamieson, P.E.; Brensinger, C.; Jamieson, K.H. Misinformation about vaccine safety and uptake of COVID-19 vaccines among adults and 5-11 year olds in the United States. Vaccine, 2022, 40, 6463–6470. [Google Scholar] [CrossRef]
- Jamieson, K.H.; Winneg, K.; Patterson, S.Jr.; Gibson, L.A.; Jamieson, P.E. Annenberg Science and Public Health Monitor – Summer 2024. University of Pennsylvania, Philadelphia, PA USA (https://cdn.annenbergpublicpolicycenter.org/wp-content/uploads/2024/08/asaph-report-summer-2024.
- Ashfield, S.; Donelle, L.; Uppal, G.; Bauer, M.A.; Kothari, A. Community organization perspectives on COVID-19 vaccine hesitancy and how they increased COVID-19 vaccine confidence: a Canadian Immunization Research Network, social sciences and humanities network study. Front. Publ. Health. 2023, 11, 1258742. [Google Scholar] [CrossRef]
- Shiman, L.J.; Diallo, F.; Nieves, C.I.; Brooks, B.; Dannefer, R.; Dorvil, S.; Lejano, M.; Pierre, J. “Be honest and gain trust”: a population health study to understand the factors associated with building trust in three historically disinvested neighbourhoods in New York City. Front. Publ. Health. 2023, 11, 1285152. [Google Scholar] [CrossRef]
- Iqbal, S.M.; Rosen, A.M.; Edwards, D.; Bolio, A.; Larson, H.J.; Servin, M.; Rudowitz, M.; Carfi, A.; Ceddia, F. Opportunities and challenges to implementing mRNA-based vaccines and medicines: lessons from COVOD-19. Front Publ. Health. 2024, 12, 1429265. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, S. Misinformation: susceptibility, spread, and interventions to immunize the public. Nature Med. 2022, 28, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Roozenbeek. J.; van der Linden, S.; Goldberg, B.; Rathje, S.; Lewandowsky, S.. Psychological inoculation improves resilience against misinformation on social media, Science Advances 2024, 8.
- Moffat, K.; Lacey, J.; Zhang, A.; Leipold, S. The social licence to operate: a critical review. Forestry: Int. J. Forest Res. 2016, 89, 477–488. [Google Scholar] [CrossRef]
- Kamenopoulos, S.; Agioutantis, Z. The importance of the social license to operate at the investment and operations stage of coal mining projects: application using a decision support system. Extr. Ind. Soc. 2020, 8, 100740. [Google Scholar] [CrossRef]
- Muller SHA; Kalkman, S. ; van Thiel, G.J.M.W.; Mostert, M.; van Delden, J.J.M. The social licence for data-intensive health research: towards co-creation, public value and trust. BMC Med Ethics, 2021, 22, 110–118. [Google Scholar] [CrossRef]
- Churchill, B.F.; Henkhaus, L.E.; Lawler, E.C. Effect of vaccine recommendations on consumer and firm behavior, J Policy Analysis Management, 2024, 44, 125–150. 44.
- Brewer, N.T. What Works to Increase Vaccination Uptake. Acta Pediatr. 2021, 21(4S), s9–s16. [Google Scholar] [CrossRef]
- Sergi, C.M.; Leung, A.K.C. Vaccination: a question of social responsibility. J Prev Med Hyg. 2021, 62, E46–E47. [Google Scholar]
Figure 1.
Development and administration of mRNA individual neoantigen therapies.
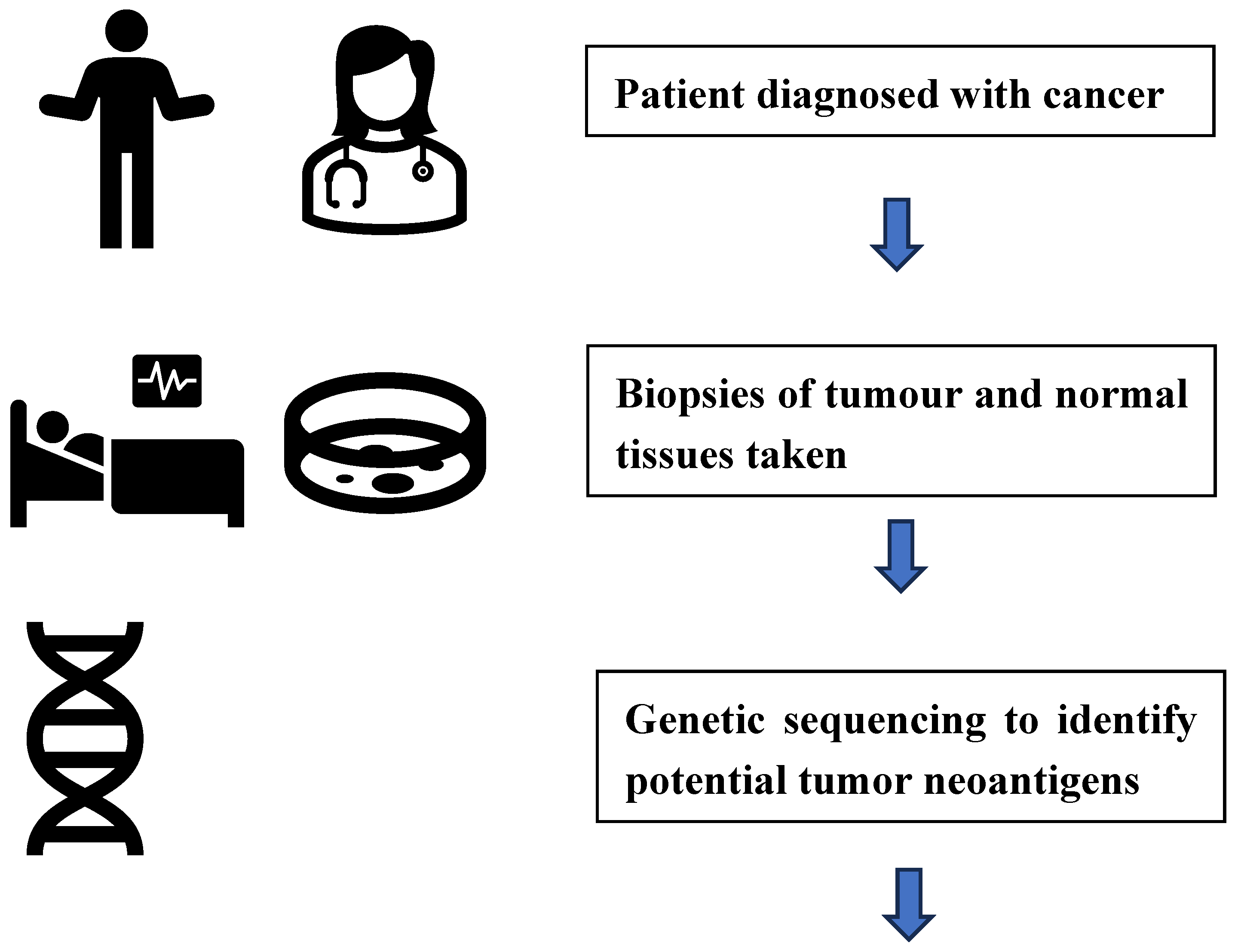
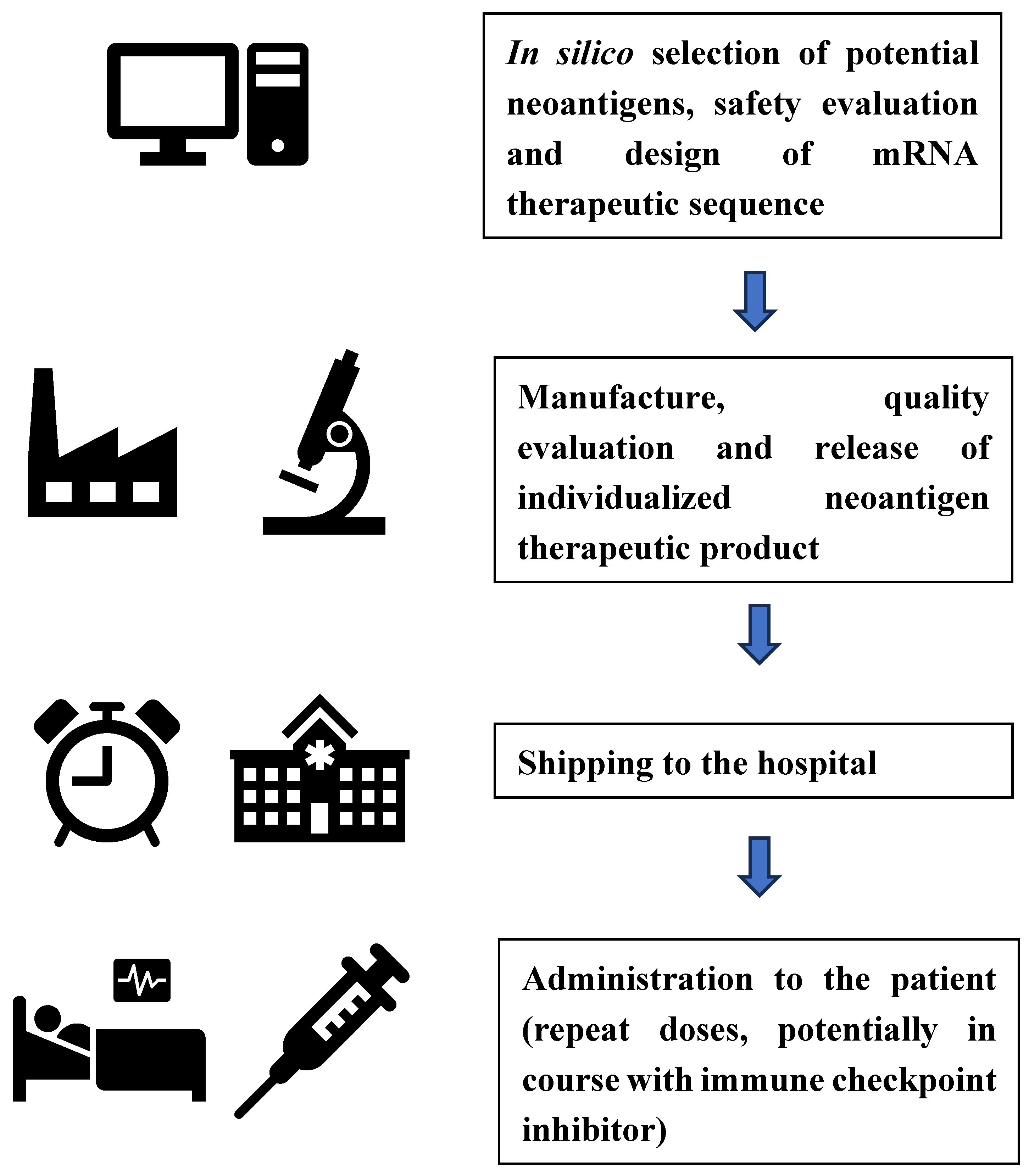
Figure 2.
Factors influencing the “Social license to operate” for mRNA vaccines.
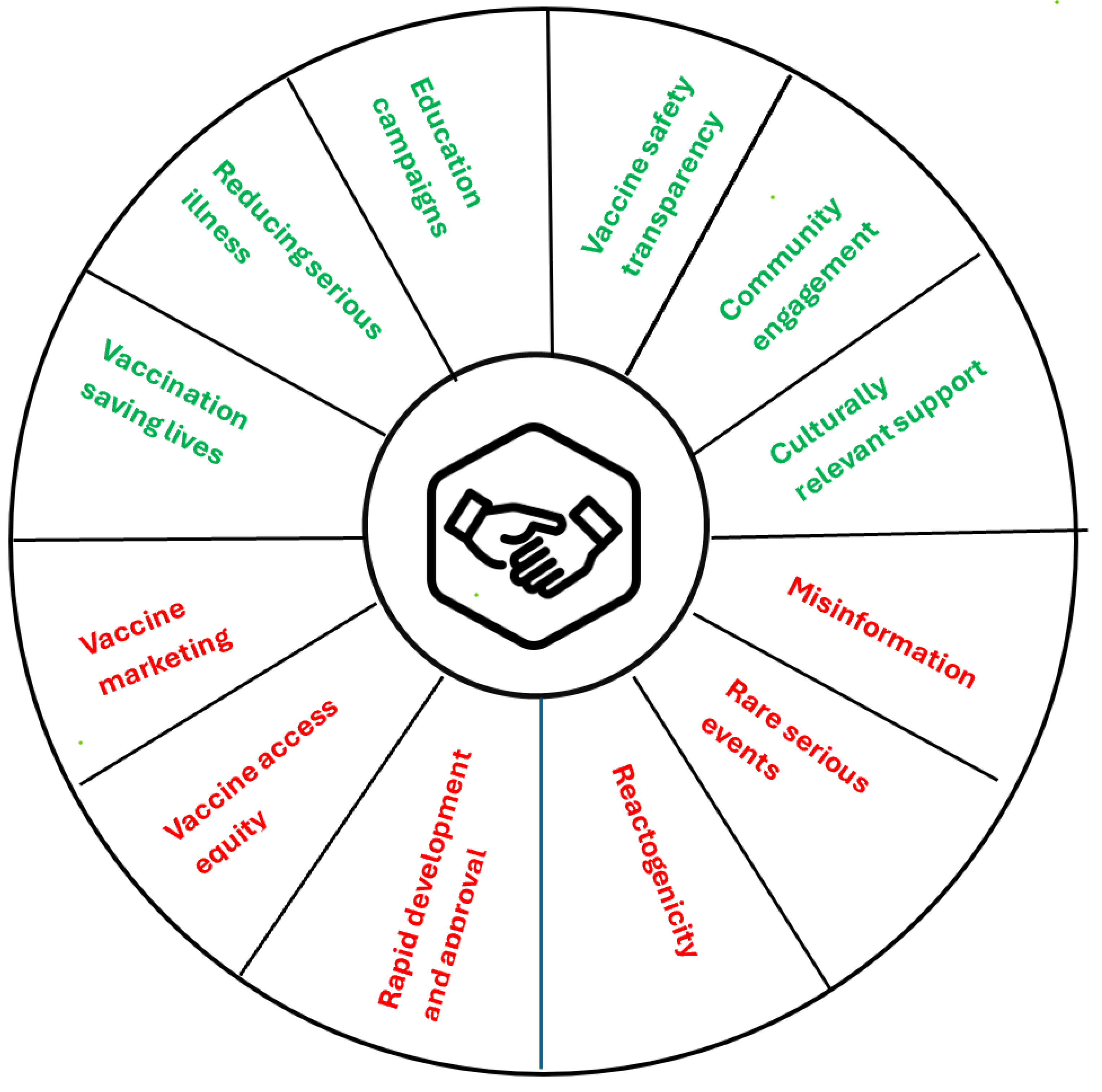
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



