Submitted:
12 February 2025
Posted:
13 February 2025
You are already at the latest version
Abstract
Minimal hepatic encephalopathy (MHE) is primarily a cognitive disorder linked to chronic liver disease that often remains underdiagnosed due to the subtlety of its clinical manifestations. These symptoms are frequently overlooked or dismissed as inconsequential in clinical practice, leading to many undiagnosed cases. The standard neurological examination is usually normal in indi-viduals with MHE. Regular and systematic screening for MHE is essential for early detection, which can improve cognitive outcomes and prevent progression to a more serious and debilitat-ing condition also known as overt hepatic encephalopathy. The pathophysiology of MHE is very complex and multifactorial, involving several interplaying mechanisms. Mainly, hyperammone-mia, system-wide inflammation, gut-derived neurotoxins, oxidative stress, and mitochondrial dysfunction are at its root. Any of these factors may interfere with the normal functioning of neu-rotransmitters, giving rise to the typical subtle cognitive impairments that are hallmarks of MHE. The Animal Naming Test and EncephalApp-Stroop tests are useful for screening for minimal en-cephalopathy in office or bedside settings. The role potentially played by emerging diagnostic technologies of advanced neuroimaging and biomarkers has been reviewed, underscoring its promise in improving early detection and diagnosis of MHE.
Keywords:
minimal hepatic encephalopathy
; hepatic encephalopathy
; minimal he
; chronic liver diseases
; driving impairment
; neurocognitive testing
; neuropsychological testing
; psychometric tests
; elec-troencephalography
; quality of life
1. Introduction
Chronic liver disease (CLD) and the resulting cirrhosis lead to around 1 million deaths annually. Beyond its clinical impact, CLD significantly affects health-related quality of life (HRQL) and imposes an economic burden. While there are various causes of liver disease, the four primary contributors to the burden associated with CLD are chronic hepatitis C virus (CHC), chronic hepatitis B virus (CHB), alcohol-related liver disease (ALD), and nonalcoholic fatty liver disease (NAFLD) [1]. Over 100 million people in the United States experience some form of liver disease. Approximately 4.5 million U.S. adults (1.8%) have received a liver disease diagnosis, but it is estimated that 80-100 million adults in the U.S. have fatty liver disease, with many unaware of their condition. In 2020, 51,642 adults in the U.S. died from liver disease [2]. Despite the availability of a highly effective vaccine and antiviral regimens for treatment and cure, the global burden of CLD continues to increase, most likely owing to the increasing rates of NAFLD and ALD [2].
CLD can manifest with nonspecific symptoms like fatigue, anorexia, and weight loss. However, the specific presentation depends on the complications the patient has developed. The major complications of CLD include portal hypertension (leading to esophageal varices and ascites), hepatocellular insufficiency (resulting in jaundice and Hepatic Encephalopathy [HE]), and hepatocellular carcinoma.
HE is a significant complication associated with severe acute or chronic liver insufficiency. HE is a condition characterized by brain dysfunction resulting from liver insufficiency or portal-systemic shunting [3]. It presents a wide range of neurological or psychiatric abnormalities, spanning from subtle subclinical changes to coma. Notably, this definition of HE does not consider the underlying cause of liver disease. However, various factors associated with CLDs, including ALD, non-alcoholic fatty liver disease, viral hepatitis, and primary biliary cholangitis, can independently impact brain function beyond the effects triggered by liver failure or dysfunction [4].
HE primarily manifests as alterations in personality, consciousness, cognition, and motor function. Traditionally, three types of HE have been identified based on their underlying causes: Type A occurs as an essential component of acute liver failure; type B arises due to portosystemic shunts in the absence of liver dysfunction; and type C presents in patients with liver cirrhosis and portosystemic bypass. There is ongoing discussion about whether HE in patients with acute-on-chronic liver failure should be classified separately (as type D), given its distinct clinical, pathophysiological, and prognostic features [5].
The West Haven criteria (WHC) are commonly used to grade HE. This system distinguishes four clinically presentation: Grade I: Patients exhibit a lack of attention and subtle personality changes, often noticeable to their relatives; Grade II: The most intriguing finding is disorientation for time, combined with inappropriate behavior and lethargy; Grade III: Patients are stuporous but respond to stimuli, they are also disoriented by place and situation and may exhibit bizarre behavior; Grade IV: Patients are in a coma. Additionally, a fifth grade was added for patients without clinical signs of HE: the so-called subclinical or minimal HE (MHE) [6] (Figure 1). The International Society for HE and Nitrogen Metabolism classifies Covert HE, also known as clinically undetectable HE. According to the West Haven Criteria, this category includes minimal and grade I disease categories. Patients falling into these categories are considered to have MHE [7].
MHE, previously known as subclinical HE, is the earliest and mildest HE form [8]. Importantly, it needs to be more recognized and often needs to be diagnosed. Patients with MHE do not display clinical evidence of cognitive changes; instead, they experience subtle alterations in psychomotor or neuropsychiatric functioning [3]. Up to 80% of patients with CLD are estimated to experience MHE [9]. While there is no definitive gold standard for diagnosing MHE, several validated testing methods have been developed to detect this neurocognitive complication. Additionally, some of these diagnostic tools can also predict the risk of progression to Overt Hepatic Encephalopathy (OHE) [10].
While recognizing MHE can be challenging, early detection is crucial due to its association with worse clinical outcomes. Patients with MHE face an increased risk of hospitalization and motor vehicle collisions [11]. Moreover, individuals with MHE are more likely to progress to OHE, experience impaired quality of life, and have higher overall mortality rates [12]. Therefore, this narrative review aims to provide an overview of the current literature on MHE, summarize its main features, and provide current perspectives, including diagnosis and management.
2. Pathophysiology
The pathophysiology of HE is complex, as it is multifactorial, encompassing ammonia toxicity, dysregulation of central nervous system (CNS) activity, and an excess of inflammatory cytokines. Ammonia plays a crucial role in the pathophysiology of HE. Ammonia is a small nitrogenous metabolite that results from the breakdown of proteins and amino acids. While the pathophysiology of HE involves multiple factors, extensive research has centered on accumulating this nitrogenous waste product in the blood and brain. Although hyperammonemia is not the sole mechanism in HE development, it significantly impacts cellular function (Figure 2).
2.1. Role of Ammonia
2.1.1. Ammonia Production
Ammonia is primarily produced in the small and large intestines (50%) and the kidneys (40%). In the intestine, there are two mechanisms: (1) urea from dietary protein is broken down into ammonia and carbon dioxide by urease-producing bacteria (such as Klebsiella and Proteus), mainly in the large intestine, and (2) glutamate is directly degraded into glutamate and free ammonia by glutaminase in enterocytes. This unionized ammonia can freely cross the intestinal epithelium and enter the portal circulation. The ionization of ammonia depends on the colonic luminal pH. A more acidic pH leads to protonation and trapping of ammonium (NH₄⁺) within the lumen. Additionally, nonabsorbable disaccharides like lactulose can lower colonic pH, reducing ammonia reabsorption [13].
While gut bacteria contribute significantly to ammonia production through protein breakdown, low-protein diets should be avoided in patients with HE. Protein malnutrition can lead to sarcopenia, which is associated with higher mortality and an increased risk of HE. Muscles play a crucial role in nitrogen metabolism for patients with cirrhosis. Additionally, increased fiber intake reduces bowel transit time and decreases ammonia absorption [14].
Renal ammoniagenesis occurs in the proximal tubular cells, in which these cells generate ammonia from glutamine, producing bicarbonate as a byproduct. Renal ammonia production is influenced by acid-base status and potassium balance. In metabolic acidosis or hypokalemia, glutamine helps with acid disposal or potassium recovery, leading to increased arterial ammonia levels [15]. Intravascular hypovolemia (e.g., due to gastrointestinal bleeding or over-diuresis) enhances renal ammonia production via angiotensin II. Volume expansion (e.g., stopping diuretics) benefits patients with worsening HE [16].
Muscles also have a minor contribution as they release ammonia through adenylic acid metabolism (part of the purine nucleotide cycle). Senescent red blood cells release glutamine, contributing to ammonia production [17].
2.1.2. Ammonia Excretion
The primary site of ammonia breakdown occurs in the liver through the urea cycle (also known as the Krebs-Henseleit cycle). In this process, two molecules of ammonia and one molecule of carbon dioxide combine to produce urea and water. Due to its small size, urea can easily cross membranes and return to the intestines and kidneys for excretion. Interestingly, the ammonia concentration in the portal vein is 5 to 10 times higher than in the systemic circulation. When liver function is compromised—either due to hepatocellular damage or shunting around the liver (such as from portal hypertension or portosystemic shunts)—ammonia accumulates in the systemic circulation [17].
The kidneys contribute to ammonia excretion by generating ammonium through parallel H1 and ammonia secretion in the collecting duct. Most urinary ammonia results from renal ammonia genesis. Factors like acid-base balance, potassium levels, protein intake, and glucocorticoid hormones influence the proportion of ammonia excreted in urine. Interestingly, renal venous ammonia exceeds arterial ammonia, indicating that the kidneys actually increase systemic ammonia [18]. In normal physiology, about 50% of ammonia is excreted in urine, while the rest returns to the systemic circulation via the renal vein. In acidosis, the kidneys excrete hydrogen ions and convert ammonia to ammonium. Conversely, alkalosis reduces renal ammonia excretion, and reduced renal perfusion (e.g., dehydration) also decreases ammonia excretion [17].
In patients with cirrhosis, skeletal muscles play a significant role in detoxifying ammonia by converting it into glutamine via glutamine synthetase (GS). Sarcopenia (muscle loss) is a risk factor for HE, so improving muscle mass is beneficial. Abnormal ratios of branched-chain amino acids (BCAAs) and aromatic amino acids in cirrhotic patients affect ammonia metabolism. BCAA supplementation has shown promise in treating HE, especially in non-responsive cases [19].
Therapeutic options such as L-Ornithine L-Aspartate (LOLA) enhance both ureagenesis and glutamine synthesis. L-ornithine plays a role in the urea cycle in periportal hepatocytes, while L-aspartate contributes to glutamate production via transamination in perivenous hepatocytes, skeletal muscle, and the brain. Intravenous LOLA has improved psychometric testing and postprandial venous ammonia levels in patients with persistent HE [20].
2.2. Ammonia Neurotoxicity
Under normal conditions, most ammonia exists in the weakly acidic NH₄⁺ form. Interestingly, this ion has a similar ionic radius and diffusion coefficient to potassium (K⁺). As a result, it can compete with and bind to various K⁺ channels and transporters. Ammonia can cross the blood-brain barrier through passive diffusion in its uncharged form and also via active transport using ion transporters in its NH₄⁺ form [21]. Some evidence suggests that specific mammalian ammonia transporters and aquaporin channels (such as aquaporin-8) are involved in this process [22].
2.2.1. Astrocyte Dysfunction Theory
Ammonia, when detoxified by astrocytes, leads to cellular changes that can alter brain function. These changes include pH shifts, membrane potential alterations, and impaired oxidative metabolism [23]. Glutamine synthetase (GS) plays a key role in detoxifying ammonia by converting it into glutamine. However, excessive ammonia can cause astrocyte swelling and dysfunction [24]. CLD results in mild swelling, while acute liver failure leads to significant swelling and increased intracranial pressure [25]. Additionally, hyponatremia can contribute to astrocyte swelling. Therefore, correcting electrolyte imbalances is crucial for preventing or treating HE [26].
In addition to astrocyte dysfunction, neuropathology studies have observed microglial cell activation [27]. This leads to a pro-inflammatory state, monocyte recruitment, and increased cytokine gene expression in the brain. PET imaging reveals heightened signal intensity in the anterior cingulate cortex, which is associated with attention control. Neuronal damage and death contribute to acquired hepatocerebral degeneration, post-shunt myelopathy, and direct cerebellar damage [28]. Liver failure can also cause neuronal death in Wernicke encephalopathy due to impaired thiamine synthesis. Mechanisms of neuronal damage include NMDA receptor-mediated excitotoxicity, lactic acidosis, oxidative stress, and proinflammatory cytokines. Despite ammonia’s role in HE, other factors play a significant role, and ammonia levels do not always correlate directly with HE severity. Neurotoxins, nutritional deficiencies, inflammation, and neurotransmission changes are major contributors to HE [29].
2.3. Role of Tumor Necrosis Factor-Alpha
Systemic inflammation plays a crucial role in HE. Cirrhotic patients often have elevated levels of tumor necrosis factor (TNF)-alpha. Common triggers include infection or direct hepatocellular injury, leading to the release of proinflammatory cytokines like TNF-alpha, interleukin (IL)-1B, and IL-6 [30]. Gut flora translocation contributes to increased TNF-alpha levels. Additionally, proton pump inhibitors (PPIs) may exacerbate bacterial translocation. TNF-alpha affects neurotransmission, astrocyte function, and blood-brain barrier permeability, emphasizing its role in HE [31].
2.4. Role of Gut Microbiota: Gut-Liver-Brain Axis
Changes in gut flora contribute to HE. Reduced bile acid production in liver disease leads to pathogenic bacteria (e.g., Enterobacteriaceae) proliferation and reduced protective commensals (e.g., Lachnospiraceae) [32]. Patients with HE exhibit dysbiosis, hyperammonemia, and systemic inflammation. Specific gut microbial changes correlate with inflammation and neuronal dysfunction. Probiotics may reduce ammonia and endotoxin levels, improving HE. Fecal microbiota transplant (FMT) shows promise in treating recurrent HE [33].
2.5. Neurotransmitters and Minerals Involved in the Pathophysiology of Hepatic Encephalopathy
2.5.1. Glutamate
In HE, glutamate, the brain’s main excitatory neurotransmitter, experiences reduced transmission. Elevated ammonia levels within the CNS lead to various changes in the glutamate system [34]. These include altered expression and activity of glutamate transporters in the synaptic cleft, reduced glutamate release from nerve terminals due to decreased synthesis from glutamine, prevention of action potential invasion in presynaptic terminals, and blockage of glutamate receptors [35]. These alterations contribute to the neurological symptoms observed in HE. Additionally, acute ammonia elevations lead to excessive NMDA receptor activation, resulting in significant neurotoxicity, although this effect is not seen with chronic hyperammonemia [36].
2.5.2. Monoamines: Histamine and Serotonin
The monoamine system, affected by ammonia, plays a role in HE. The activation of histaminergic systems contributes to symptoms like disturbances in the sleep cycle and altered motor functions. Studies have reported elevated histamine levels in plasma and the brain tissue, possibly due to changes in the brain’s neutral amino acid transporter system [37]. Additionally, increased concentrations of 5-hydroxyindoleacetic acid (5-HIAA), a serotonin (5-HT) metabolite, correlate with plasma ammonia levels. In patients with cirrhosis who died in hepatic comas, cerebrospinal fluid (CSF) 5-HIAA levels were elevated, suggesting increased 5-HT turnover and metabolism [38]. Mechanisms include stimulation of precursor L-tryptophan uptake, increased expression of monoamine oxidase A, and altered 5-HT storage and release from presynaptic terminals. These changes contribute to neuropsychiatric symptoms such as depression and disrupted sleep patterns [39].
2.5.3. Gamma-Aminobutyric Acid
GABA is the primary inhibitory neurotransmitter in the brain. Increased GABAergic transmission has been linked to HE [40]. Factors contributing to this include upregulation of the 18-kDa translator protein, which produces endogenous benzodiazepines (neurosteroids) that modulate GABA type A receptors. Additionally, increased peripheral benzodiazepine receptor concentrations in astrocyte mitochondria may alter energy metabolism. Clinical studies using benzodiazepine site antagonists like flumazenil have shown improvement in HE patients. The exact pathophysiology remains incompletely understood, but it involves gene expression changes, increased brain GABA agonists, and endogenous modulators [41]. Allopregnanolone, a neurosteroid activating GABA type A receptors, is elevated in advanced HE. The agent GR 3027, a neurosteroid-site antagonist, shows promise in symptom improvement [42].
2.5.4. Manganese
Manganese (Mn) is essential for physiological functions but can become a neurotoxin in end-stage liver disease. Elevated Mn levels due to CLD lead to CNS deposition, primarily in the basal ganglia [43]. Astrocytes are particularly affected. Mn disrupts oxidative phosphorylation by sequestering in mitochondria. Impaired glutamate transport and dopamine-D2 binding result in extrapyramidal symptoms similar to Parkinson’s disease. L-Dopa treatment may improve symptoms, and liver transplantation can resolve them in some patients [44].
2.6. Risk Factors Contributing to the Development of Minimal Hepatic Encephalopathy
In a multicenter, cross-sectional study, 1879 patients with confirmed cirrhosis were enrolled across 40 hospitals [45]. Researchers conducted both univariate and multivariate logistic analyses to explore risk factors for MHE in cirrhotic patients. The study focused on age, duration of education, etiology, and MELD-Na score. Age was identified as an independent risk factor (p < 0.001). A longer duration of education was associated with a reduced risk (p = 0.001). Etiology (p = 0.039) and MELD-Na score (p = 0.009) were also significant risk factors. For HBV-related cirrhosis, age (p = 0.001) and duration of education (p = 0.001) influenced MHE risk. For HCV-related cirrhosis, age (p = 0.009) and creatinine concentration (p = 0.042) were risk factors. No significant risk factors were found for ALD-related cirrhosis. In alcoholic cirrhosis, platelet count (p = 0.045) was associated with MHE risk.
On the other hand, risk factors for OHE in cirrhosis include MHE, prior history of OHE, sarcopenia, hyponatremia, epilepsy, type 2 diabetes mellitus, elevated creatinine levels, elevated bilirubin levels, low albumin levels, proton pump inhibitor (PPI) use, nonselective beta-blocker use, and statin use [46,47].
2.7. Mechanisms Underlying Cognitive Dysfunction in Minimal Hepatic Encephalopathy
Current understanding suggests that both hyperammonemia and inflammation play significant roles in causing cognitive impairment in MHE [48]. Consequently, it is not unexpected that certain diseases, which result in similar changes in ammonia levels and inflammatory factors akin to those seen in liver cirrhosis, may also lead to mild cognitive impairment affecting performance in similar psychometric tests [49].
Felipo et al. assessed cognitive function using the PHES battery of psychometric tests in patients with varying degrees of hyperammonemia and inflammation caused by different diseases, both with and without liver failure. It was noticed that all patient groups exhibit some level of inflammation [50]. However, the severity and nature of inflammation vary among different patient types, with distinct contributions from increased IL-6 and IL-18 levels. The findings indicate that mild cognitive impairment, as evaluated using the PHES battery, necessitates the simultaneous presence of moderate hyperammonemia and inflammation. While it remains possible that hyperammonemia or inflammation alone may affect other cognitive functions, impairment, specifically in the cognitive domains assessed by the PHES battery, appears to require a combination of both factors [51].
In rat models of MHE, impaired cognition is induced by reduced synthesis of cyclase guanylyl monophosphate (cGMP) through various mechanisms. This cognitive impairment is evident in the reduced learning ability observed during a Y-maze task. Neuroinflammation, characterized by increased extracellular GABA and hyperammonemia, which activates N-methyl-D-aspartate receptors, ultimately leads to decreased neuronal NO synthase activity, resulting in reduced cGMP synthesis [52].
2.8. Differences in Brain Activity Between Averted Hepatic Encephalopathy and Minimal Hepatic Encephalopathy
In addition to the common alterations in brain activity observed in patients with OHE and MHE, quantitative comparison analysis revealed that OHE patients exhibit reduced brain activity in regions associated with the default mode network (DMN) compared to MHE patients [53]. The DMN plays a role in various cognitive functions, including memory, visual and auditory attention, motor activity, and language processing. Specifically, the precuneus, a key component of the DMN, is closely linked to visuospatial information integration, episodic memory retrieval, and self-processing operations.
Consistent with these findings, a resting-state functional MRI (rs-fMRI) study demonstrated decreased functional connectivity within the DMN in patients with prior OHE compared to those with current MHE. These results suggest that resting-state brain activity in the DMN could serve as a noninvasive and sensitive neuroimaging biomarker for detecting the progression from MHE to OHE. Furthermore, OHE patients exhibited increased brain activity in specific regions, including the left olfactory cortex, left cerebellum (crus I), right superior temporal gyrus (STG), and right putamen, when compared to MHE patients. Such increased activity is often interpreted as a compensatory mechanism resulting from neural reorganization. Thus, the heightened brain activity in these regions among OHE patients may play a compensatory role as the severity of HE worsens. These findings suggest that rs-fMRI could be a valuable imaging technique for assessing HE severity in clinical practice [54].
3. Definition
Modern diagnostic methods enable the detection of functional abnormalities even before symptoms manifest. Identifying impairments early can help prevent or delay disease progression. This approach is essential for recognizing and modifying risk factors, such as hypercholesterolemia or arterial hypertension [55]. Neurologists, recognizing the significance of early Alzheimer’s disease diagnosis, coined the term “mild cognitive impairment” to identify patients in the initial stages of the disease—candidates who may benefit from available treatments. Similarly, early identification of HE patients can enhance their quality of life and prognosis.
The concept of “subclinical HE” was introduced to identify patients exhibiting subtle manifestations of HE that are challenging to recognize. This term underscores the importance of using complementary tests to diagnose brain dysfunction that might not be detectable through standard clinical examination [56].
Other researchers have preferred terms like “latent” or “early” to emphasize the potential progression to OHE [57,58]. However, once the impact on patients’ quality of life became evident, the term “subclinical” faced criticism. To prevent medical misunderstandings, alternative terms were suggested, avoiding the implications that the condition is insignificant [59]. The current consensus is to use the term “minimal hepatic encephalopathy” (MHE), as proposed by the Working Party commissioned by the XI World Congress of Gastroenterology [60]. The American Association for the Study of Liver Diseases (AASLD) defines MHE as the presence of test-dependent or clinical signs of brain dysfunction in cirrhotic patients who are not disoriented or displaying asterixis [3].
3.1. Clinical Manifestations
The International Society for HE and Nitrogen Metabolism (ISHEN) consensus delineated the symptoms and their grading into covert (MHE and grade I) and OHE (OHE; grades II-IV) in September 2014. Motor manifestations of stage I HE begin with impaired handwriting and incoordination. Stage II HE is characterized by asterixis. As encephalopathy progresses, flapping tremors weaken in stage III and disappear in stage IV. Later stages involve hyporeflexia, ataxia, hyperreflexia, clonus, and rigidity and may culminate in opisthotonus and coma [3].
MHE is often underrecognized, significantly impacting patients’ quality of life and their families. It is highly prevalent among cirrhotic patients, affecting up to 80% of this population. Despite normal clinical examination findings, patients with MHE exhibit abnormal psychometric test results. These subtle symptoms necessitate specialized neuropsychiatric diagnostic testing [61]. MHE primarily affects executive functioning, leading to deficits in vigilance, response inhibition, working memory, and orientation [62]. Importantly, MHE can impair daily functioning, including safe automobile operation [63]. The ISHEN consensus defines the onset of OHE as the appearance of disorientation or asterixis [64]. As awareness of MHE grows, early treatment may significantly enhance the quality of life for cirrhotic patients.
3.2. Clinical Significance
3.2.1. Effect of Minimal Hepatic Encephalopathy on Quality of Life
QOL encompasses physical, cognitive, emotional, and psychosocial well-being. It is assessed using various scales, such as the Nottingham Health Profile (NHP), the Sickness Impact Profile (SIP), and disease-specific questionnaires [65,66].
MHE negatively impacts health-related quality of life (HRQOL). Complex tasks requiring attention, information processing, and psychomotor skills are affected. Basic self-care functions remain preserved [67]. Patients with MHE show impaired scores across SIP scales, affecting social interaction, alertness, emotional behavior, sleep, work, and recreation [68].
3.2.2. Sleep and Health-Related Quality of Life
Sleep disturbances are common in cirrhosis patients, affecting 26–70% of cases. Patients with MHE experience more sleep disturbances than those without MHE. Homeostatic and circadian processes regulate sleep. MHE disrupts these processes. Unsatisfactory night sleep, delayed onset, and multiple awakenings lead to reduced sleep time and daytime sleepiness [71]. Excessive daytime sleepiness correlates with ammonia levels and increases HE-related hospitalization risk. Sleep disturbances can impair health-related quality of life (HRQOL) in MHE patients [72].
3.2.3. Memory and Learning Difficulties in Minimal Hepatic Encephalopathy
MHE involves subcortical dysfunction, including slowed mental processing, attention disturbances, executive disabilities, psychomotor slowing, and memory issues. MHE primarily affects short-term memory due to attention deficits, leading to encoding defects and learning impairments [73]. FDG PET studies reveal decreased glucose metabolism in the parieto-occipital region (related to visual perception) and preserved metabolism in the temporomesial area (associated with memory) [74]. Learning impairment in MHE may result from hyperammonemia, affecting cGMP levels. Pharmacological interventions may help [75].
3.2.4. Driving and Navigational Skills in Minimal Hepatic Encephalopathy
MHE patients show impaired driving performance in real road tests and driving simulators. The categories most affected include car handling, maneuvering, adaptation, and cautiousness [76]. The increased risk of accidents is attributed to cognitive decline in MHE patients. Difficulties in following maps and higher self-reported traffic violations are observed. Fatigue worsens driving performance over time. Navigation relies on working memory, attention, response inhibition, visuomotor coordination, and executive control [77]. MHE patients have navigation difficulties, leading to illegal turns and accidents. Rifaximin improves driving performance in MHE patients, correlating with cognitive improvement [11].
3.2.5. Falls in Minimal Hepatic Encephalopathy
MHE is linked to an elevated risk of falls, impacting patients’ quality of life. While only 12% of patients without MHE experience falls, nearly 40% of those with MHE suffer falls that often require hospitalization [78]. The risk is further heightened for patients taking psychoactive drugs. Impaired attention, visuomotor coordination, and slowed reaction time increase the fall risk in MHE patients [79]. Additionally, the higher incidence of falls in these patients can lead to osteoporosis-related fractures, surgeries, and associated morbidity, ultimately affecting both patients and their families [80].
3.2.6. Employment and Socioeconomic Burden of Minimal Hepatic Encephalopathy
3.2.7. Natural History and Survival in Minimal Hepatic Encephalopathy
Patients with MHE can experience improvement, stability, or deterioration over the long term. The frequency of MHE increases with the severity of liver dysfunction. MHE predicts the development of OHE and adversely affects survival [83]. Studies have shown that both abnormal psychometric scores for HE and the Child-Turcotte-Pugh (CTP) score independently correlate with survival. Additionally, covert HE is associated with worsened survival, increased hospitalization risk, and overted HE development [84].
4. Diagnosis and Available Tests
MHE is the mildest clinical manifestation of HE. It can impact as many as 80% of individuals with liver cirrhosis, varying depending on the specific population examined and the diagnostic method employed [85]. Thus, every patient who is at risk should undergo testing for this condition. This is because MHE is a significant health issue and, even in its mildest form, it is linked to carer burden, poor prognosis, increased risk of experiencing episodes of OHE, inability to drive, sleep disorders, falls, and ultimately, a impairment of the quality of life [86,87]. The most effective method for identifying MHE is still an ongoing issue. None of the offered strategies adequately address the intricate and diverse nature of cognitive impairment in MHE (Figure 3).
Additionally, suitable norms are frequently necessary, and MHE still needs to be recognized or underdiagnosed by most clinicians [88]. The diagnosis of MHE might frequently be missed due to various factors, including the fact that diagnosing MHE is challenging with objective neurological examination alone, hence requiring specific neuropsychological and neurophysiological studies, and cognitive impairment affects overall performance and psychomotor skills [9]. In contrast, verbal skills typically remain intact [85]. Certain tests can be costly and necessitate highly skilled personnel and specialized testing equipment [83]. The absence of diagnostic criteria and age- and education-adjusted normal distribution values is notable [85]. There is no singularly ideal approach to evaluating the existence of MHE, as none of the proposed tests comprehensively address all aspects of HE; each method investigates distinct brain functions [9].
4.1. Psychometric Testing
Psychometric testing is a cornerstone in diagnosing MHE, providing valuable insights into the often subtle cognitive impairments that accompany this condition. Sharma et al. reported that these tests assess a range of psychological functions frequently impacted by MHE, including attention, memory, and visuospatial abilities. Psychometric hepatic encephalopathy score (PHES), specifically designed and validated across numerous populations and clinical scenarios to detect and stage HE [89]. For a broader neuropsychological evaluation, the repeatable battery for the assessment of neuropsychological status (RBANS), also described in the table, can identify cognitive deficits, including those characteristic of MHE [90]. Even simpler tests like the animal naming test (ANT), measuring verbal fluency, a function often impaired in MHE, can be helpful [91]. Factors such as age, education level, and previous test experience can influence results, making it essential to interpret findings carefully and within the context of each patient's overall clinical picture.
Furthermore, the field is continuously evolving, with ongoing research refining existing tests and exploring innovative digital assessments, such as EncephalApp [92] and QuickStroop [93], for their potential advantages in accessibility and ease of administration. Ultimately, a comprehensive approach to diagnosing MHE often entails integrating findings from various psychometric tests with clinical observations and laboratory markers to gain a holistic understanding of each patient's condition [94]. A summary of diagnostic methods for the detection of MHE is presented in Table 1.
4.1.1. Psychometric Hepatic Encephalopathy Score (PHES)
The PHES, a set of psychometric test techniques, is currently recognized as the worldwide preferred and most reliable method for diagnosing MHE [96]. PHES was specifically designed for individuals with MHE and has been confirmed reliable and valid for MHE diagnosis. The PHES consists of five tests: number connection test A, number connection test B, serial dotting test, line tracing test, and digit symbol test. The PHES evaluates various cognitive functions, including motor speed, accuracy, concentration, attention, visual perception, visual-spatial orientation, visual construction, and memory [6].
A cohort of Thailand adults with cirrhosis assessed the efficacy of PHES in diagnosing MHE [134]. The authors described that a PHES threshold of ≤−5 points suggests MHE. MHE was detected in 26.6% of cirrhotic patients who did not exhibit OHE. However, some authors reported that test findings with a score (≤-2SD) were considered abnormal [6,95]. Furthermore, validation studies have been conducted in Italy [95], Spain [83], Germany [6], Korea [97], China [98], and India [89]. Standardizing these tests using a large control group must account for variations in mathematics, literacy, and language skills that may affect test outcomes [94]. The test findings are additionally impacted by factors such as age, gender, level of education, alcohol consumption, and visual abilities of the individual being tested [135]. While adjusting the findings based on age and education is possible, managing the impact of other variables is challenging. Another issue arises from the diminishing sensitivity of these tests due to many repetitions [136].
4.1.2. Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)
The RBANS has been confirmed by a working committee established by the International Society for HE and Nitrogen Metabolism (ISHEN) to evaluate the existing evidence on the neuropsychological evaluation of HE, and it is recommended for diagnosis [135]. ISHEN suggests conducting the RBANS test together with the PHES test. The RBANS assesses verbal and visual anterograde memory, working memory, cognitive processing speed, language, and visuospatial function [137]. It specifically evaluates cognitive skills that are not impacted by HE but are often affected [6]. The test battery was developed to evaluate dementia and identify cognitive impairment in other conditions. Thus far, the utilization of this method for identifying MHE has been limited [138]. The RBANS test has a low sensitivity of just 38% in accurately detecting OHE. Therefore, it is not recommended to utilize RBANS to diagnose MHE [108].
4.1.3. Animal Naming Test (ANT)
Campagna et al. confirmed the effectiveness of the ANT in assessing cognitive impairment in individuals diagnosed with cirrhosis [91]. This highly straightforward test requires the patient to enumerate as many species of animals as they can within 1 minute. Furthermore, a study revealed that the ANT is an effective, uncomplicated, and flexible instrument for assessing cognitive impairment. While the data does not directly establish a connection between the ANT and HE, it does indicate that the ANT identifies a group of individuals with low health status and higher rates of frailty and impairment. This suggests that further investigation is needed to understand the underlying causes of these conditions [139].
4.1.4. Continuous Response Time (CRT) Test
This test evaluates the motor response time by instructing the patient to press a button when they hear auditory stimuli through headphones. The CRT index is the most crucial test result as it quantifies the stability of reaction times. The test result can distinguish between organic and metabolic brain dysfunction. The test is unaffected by the patient's age or gender, and it does not have any impact on learning or fatigue [140].
4.1.5. Inhibitory Control Test (ICT)
ICT can be easily and quickly used to diagnose MHE in a clinical setting in just a few minutes [87]. The effectiveness of ICT in diagnosing MHE has been confirmed by multiple studies [141]. There was no disparity in ICT efficiency between patients with alcoholic cirrhosis and people with nonalcoholic cirrhosis [142]. These findings suggest that the various causes of liver cirrhosis do not influence the use of ICT for MHE diagnosis [143]. The findings of ICT are also not influenced by age in both cirrhotic patients and controls [144].
Moreover, the findings of ICT show improvement following lactulose therapy and deterioration after a transjugular intrahepatic portosystemic shunt. This suggests that ICT can be utilized to assess the psychometric changes caused by these treatments [143]. In clinical settings, the ICT, is widely recognized as a reliable diagnostic tool for MHE. Consequently, it enables clinicians to identify cirrhotic patients at a heightened risk of MHE accurately. These patients can then be recommended to undertake other neurophysiological and psychometric tests for further evaluation [109].
4.1.6. EncephalApp (Stroop App) and QuickStroop
It is available as a mobile application. The application has been accessible since 2013 [145]. Presently available for both iOS and Android devices. The program utilizes the Stroop effect to evaluate psychomotor speed and cognitive awareness. The objective for the patient is to determine the colors of the stimulus displayed on the screen. The comprehensive assessment comprises three steps. Initially, the patient selects the color in which a randomly chosen word is presented on the screen. In the second task, the patient must identify the color of the word that corresponds to its color definition, as indicated by its name. During the third phase, there is a discrepancy between the name of the color and the actual color of the word. The test result is promptly accessible upon completion [145]. A multicenter study comparing it to the PHES and ICT showed a high level of accuracy in detecting the condition and is effective in evaluating the likelihood of developing OHE with a favorable sensitivity (70-80%) for screening minimal MHE [146].
The Quick Stroop test is a version of the EncephalApp Stroop test and is a reliable substitute for the full EncephalApp Stroop and PHES. It can accurately and specifically detect cognitive impairment associated with rapid cognitive health evaluation in real-world scenarios [93]. Furthermore, a study by Kanagalingam et al. suggested that the QuickStroop test, which can be completed in about a minute and utilizes the early runs of the EncephalApp Stroop's "Off" stage, is a dependable method for diagnosing covert or MHE. CHE was linked to elevated odds of developing OHE and necessitating hospitalizations [147].
4.1.7. SCAN Test
The test is a computerized assessment that evaluates the patient's ability to accurately and quickly complete a task involving the recognition of digits. The task's difficulty increases as the test progresses [94,148]. The process involves randomly presenting a sequence of 72 ordered pairs of numbers on a computer screen for 3 seconds. Patients are directed to press the corresponding number on a keyboard if they recognize a familiar digit in the series of digits displayed. The study records the average reaction times and the proportion of errors and then evaluates the results by considering the reaction times in relation to the number of errors [149].
4.2. Electrophysiologic Tests
4.2.1. Electroencephalogram Monitoring
The EEG can serve as a valuable tool in the differential diagnosis of disoriented or comatose persons with liver insufficiency/shunt, particularly when the diagnosis of HE is uncertain. It can help guide the diagnosis toward alternative illnesses [150]. HE is defined by changes in the oscillatory characteristics of neural networks in the brain [151]. The EEG readily detects a broad range of irregularities, which have been conclusively linked to behavioral changes in HE. The EEG consists of two primary components: repetitive background activity and transients. Patients' HE sees a gradual decrease in the fundamental rhythmic activity of their EEG.
Furthermore, the waking EEG's responsiveness to opening the eyes diminishes and ultimately ceases. Transient phenomena, specifically called 'triphasic waves,' can be detected in the EEG of patients with moderate/severe HE. However, it is worth noting that these waves are not exclusive to this particular metabolic disorder [152]. It detects alterations in brain activity, even in uncooperative patients [9].
In individuals with MHE, quantitative electroencephalography (q-EEG) examination reveals an elevated proportion of theta wave activity and a reduced mean dominant frequency (MDF) in the posterior derivations. These alterations are associated with indicators of liver dysfunction and can predict the development of HE and death related to liver disease [153]. An EEG study conducted during sleep can benefit cirrhotic patients by detecting variations in mean dominant frequency (MDF) that early indicate brain dysfunction in individuals with MHE [118]. During this scenario, q-EEG reveals changes in the slow oscillatory activity, characterized by an elevated frequency of the prominent delta rhythm [85]. At first, the EEG does not show overall slowing but simply periods of theta activity. Quantitative EEG demonstrates no decrease in the average dominant frequency (MDF) of the EEG [154]. However, it does show an increase in theta activity, specifically in the posterior regions of the scalp [155]. A study discussed an early marker of EEG (alpha rhythm). The paper presents a new biophysical model called MHE-AWD-NCM, which includes communication dynamics between the cortical neuron population (CNP) and astrocyte population (AP). This model aims to comprehend the role of disrupted communication between astrocytes and neurons in developing alpha wave disturbances (AWD) in MHE [156].
4.2.2. Evoked Potentials
Electrical signals can be created by adequately stimulating excitable tissues using light (visual evoked potentials, [VEPs]), acoustic signals (brainstem auditory evoked potentials [AEPs]), or electrical stimulation of somatosensory nerves [123]. The latency of VEPs is determined by the passage of signals from the retina to the visual brain through several connections [157]. VEPs can be affected by several factors, such as optic nerve illnesses, demyelinating processes, disorders of subcortical or cortical neurons in the cerebral hemispheres, metabolic abnormalities, and the use of psychoactive medicines [158]. The latency of the P100 wave of pattern visual evoked potentials (pVEPs) has been utilized to monitor MHE [159]. VEPs measure the time delay between visual input and the corresponding brain activity; however, the outcomes can vary. The variability in the assessment of subclinical HE may be attributed to the utilization of an N3 instead of the commonly used P100 component in routine neurological examinations. Furthermore, the definition of subclinical HE varies across different studies, making it challenging to compare the results. Consequently, using VEPs in patients with MHE seems to have limited diagnostic significance [160].
The significant incidence (about 40%) of flash visual evoked potential abnormalities in cirrhotic patients with normal EEG and psychometric performance indicates that this approach is highly sensitive in diagnosing HE [124,161]. Brainstem AEPs (BAEPs) are generated by delivering rapid sequences of monaural auditory stimuli, typically consisting of 1000 to 2000 clicks. The stimulation of several regions inside the brainstem subsequently accompanies the activation of the auditory nerve. Healthy individuals can have a total of seven detectable positive and negative waves. Patients in HE stages 0-I do not exhibit any notable elongation of BAEP-peaks I-V or the interpeak delay I-V. BAEPs have an erratic reaction when subjected to HE testing [123].
4.2.3. Critical Flicker Frequency Testing
CFF is a widely recognized neurophysiological method that assesses the CNS's capacity to perceive rapid changes in light intensity. This measurement is directly impacted by cortical activity [162]. It involves presenting light pulses at progressively lower frequencies (starting at 60 Hz) and requiring the patient to touch a button as soon as the perception of steady light transitions to flickering light. Following a training period, the test is conducted on eight occasions, and the average value of these trials is computed as CFF, which serves as a metric for visual temporal resolution. The threshold value is between 38 and 39 Hz, and the duration is approximately 10 minutes [125]. CFF can identify a wide range of neuropsychological disorders, including issues with visual signal processing (retinal gliopathy) as well as cognitive functioning.
Furthermore, PHES investigates the interplay between visual perception, construction, visual/spatial orientation, motor speed, accuracy, focus, and attention. Therefore, the two ways could be mutually beneficial [163]. There has been a reported discrepancy between neurophysiological research, which primarily focuses on externally stimulated brain responses, and psychometric testing [164].
4.3. Biomarkers
Ammonia is a serum biomarker that 60-95% of clinicians in their medical practice use to diagnose HE [165]. However, if the blood ammonia level is within the normal range in a patient with OHE, it should arouse suspicion of a different diagnosis [136].
Hyperammonemia can cause cell death by activating N-methyl-D-aspartic acid (NMDA) receptors excessively through glutamate, as well as increasing the activity of GABAergic receptors, which can be temporarily reversed with flumazenil [166]. A research team in Valencia studied the harmful oxidant 3-nitro-tyrosine as a biomarker. The reason for this choice was the well-established fact that hyperammonemia can cause oxidative stress. Indeed, 3-nitro-tyrosine has been identified as a toxic substance that has a role in the development of HE. Their preliminary study demonstrated encouraging findings, indicating that 3-nitro-tyrosine levels above 14 nM exhibited about 90% sensitivity, specificity, positive predictive value, and negative predictive value for MHE [132]. Another study conducted in Egypt between 2016-2018 The quantification of 3-nitro-tyrosine in serum is an easy and efficient process that does not require a significant amount of time, and this would enable the expansion of the diagnostic of MHE to a wide range of clinical environments, facilitating the identification of patients with MHE. 3-nitro-tyrosine serum levels serve as a reliable indicator for the existence of MHE in individuals with liver cirrhosis. These levels exhibit a high sensitivity of 90% and a specificity of 93.33%. Additionally, the positive and negative predictive values at a cutoff of 14 ng are 93.1% and 90.3%, respectively [167].
Inflammation is another factor contributing to the development of HE. Indeed, chemokines, cytokines, and ammonia can stimulate microglia, leading to neuroinflammation and worsening cognitive performance. Preliminary investigations assessing the levels of IL-18, namely IL-6, demonstrated strong associations with the occurrence and intensity of HE [168]. A level of IL-6 higher than 11 pg/mL is a potentially effective threshold for identifying MHE [49]. Other studies have also examined the role of S100β as a biomarker in HE, specifically in the context of acute liver failure (ALF) [169]. During ALF, the concentration of S100β protein in the blood increased by up to three times upon admission and remained elevated for 72 hours [170]. However, there was no association between S100β levels and the severity of HE, the occurrence of brain herniation, or the final result [171]. Two smaller studies conducted in patients with CLD discovered that individuals without HE had normal levels of S100β. However, patients with HE had a two-fold rise in S100β levels. S100β levels higher than 0.13 µg/L can achieve 83% sensitivity and 64% specificity in detecting HE. The correlation between S100β and HE severity was not seen, indicating its inability to differentiate between OHE and MHE [172,173].
4.4. Evaluation for Precipitating Causes
Numerous studies have documented multiple risk factors, which can be categorized into two main groups: precipitating events and predisposing factors (Table 2).
Age, liver function, the existence of portal hypertension, medication, renal function, genetic predispositions, underlying medical conditions, and the pathophysiology of liver cirrhosis (alcoholic or nonalcoholic) are risk factors [12]. Common risk factors that might trigger or worsen the condition include problems associated with decompensated liver cirrhosis, such as acute-on-chronic liver failure, hepatorenal syndrome, and gastrointestinal hemorrhage [174]. Additional risk factors involve infection, hypokalemia, hyponatremia, constipation, disruption of the gut-liver axis, type 2 diabetes mellitus, malnutrition, and sarcopenia [88,175]. Certain pharmacological substances can worsen HE, such as opioids, proton pump inhibitors, benzodiazepines, and other sedative medications. Infection is the primary precipitating factor, while electrolyte imbalance is the secondary precipitating factor [176]. All patients diagnosed with HE who were admitted to the intensive care unit (ICU) had a minimum PF, and the majority had multiple PFs. Increased mortality was independently associated with PF or an infection [177].
Moreover, there is a direct relationship between the severity of portosystemic shunt and an increased likelihood of HE. A study discovered that individuals with cirrhosis with a total cross-sectional spontaneous portosystemic shunting area greater than 83 mm2 had a higher risk of experiencing HE [178]. In individuals with cirrhosis, some genetic risk factors, including single nucleotide polymorphisms of fucosyltransferase 2, toll-like receptor 9, solute carrier family one member 3, solute carrier family one member 5, and have been linked to an increased likelihood of developing HE. Moreover, these genetic risk variables have demonstrated the ability to estimate the intensity of HE [179]. Furthermore, patients carrying genetic variations in the promoter region of GLS1, which encodes kidney-type glutaminase, had a higher occurrence of HE [180]. This finding establishes a connection between specific genes and an elevated HE risk in patients who have experienced previous episodes [12].
4.5. Challenges in Diagnosing Minimal Hepatic Encephalopathy
In fact, there needs to be more comprehensive knowledge on how to combine different test methodologies and interpret the results effectively. Additionally, studies have often needed better agreement between different tests. Diagnosing HE poses challenges. Clinical scales have faced criticism because of their poor specificity and significant variability amongst operators, particularly regarding mild HE [181]. MHE remains a condition that is not diagnosed frequently enough. This might be attributed to the limited quantity of multicentre randomized studies, the need for definitive guidelines for suggested diagnostic methods, and a shortage of experienced professionals [182]. A wide range of variation is due to the absence of standardized research methodologies and the unique characteristics of the examined populations. Although patients with MHE may not exhibit clear clinical symptoms, it still significantly impacts their everyday functioning. At the same time, Individuals diagnosed with MHE experience a notable decline in their overall well-being and quality of life as it relates to their health [69]. The diagnosis of MHE can be ignored due to the predominant impairments in global cognitive functioning and motor skills, while linguistic abilities typically remain intact. A survey conducted among members of the American Association for the Study of the Liver revealed that while 84% of participants recognized the clinical significance of MHE, nearly 40% of respondents had never undergone testing for MHE [183].
5. Management
5.1. Pharmacological Management
The recommendation is that only OHE should be routinely treated [17]. The target of treating the first attack of OHE should be limiting the result, reducing the duration, and treating the cause (Table 3). After that, we should focus on limiting hospital stays, preventing recurrence, and improving quality of life [184,185]. Treatment targets decreasing ammonia production and stimulating its elimination [186]. However, preventing recurrence by focusing on the related factors should also be assessed.
Nondigestible lactitol, lactulose, and disaccharides are the first line of treatment. These substances are broken down into organic acids (of short chain) in the colon [5]. The acidity reduces the bacteria that produce ammonia, reducing the production of ammonia and converting ammonia into ammonium (nonabsorbable), thus decreasing the absorption of ammonia. Also, they increase osmolarity and thus lead to rapid intestinal transit and remove excess nitrogen from feces by the laxative role [184,185,186]. Lactose additionally increases zinc absorption [229]. Lactulose enema improves the electroencephalograms and asterixis by the same degree as neomycin tablets, but lactose enema additionally acidifies the pH of the stool, thus improving the number connection test [230]. It was proven that there was nearly no difference between lactulose and lactitol regarding efficacy and safety [231]. Gluud et al. found that nonabsorbable disaccharides play a role in HE treatment and mortality [232]. PEG or Polyethylene glycol 3350-electrolyte solution is an osmotic laxative that can be used instead of lactulose in the treatment of hospitalized HE patients [233,234].
Antibiotics targeting the reduction of the number of intestinal bacteria that produce ammonia can be used in therapy [186]. The first antibiotic to be used was neomycin, which reduced the concentration of colonic ammonia [235]. Rifaximin (non-absorbable antibiotic) inhibits RNA synthesis in gram-negative, gram-positive, anaerobic, and aerobic intestinal bacteria [184]. Rifaximin was proven to be as effective as neomycin and also as effective and safe as lactulose [236,237]. Also, studies proved that the use of rifaximin plus lactulose has a better response than lactulose alone in the treatment of HE and mortality reduction [238]. Rifaximin was found to have the same effect as nonabsorbable disaccharides or other antibiotics but with more safety in asterixis reduction and improving the mental state [239].
5.2. Nutritional Therapies and Dietary Modifications
Metabolic ammonia scavengers are substances that increase the excretion of ammonia in urine through an alternative pathway. One of the firstly used scavengers was sodium benzoate, which is conjugated in the liver with glycerin and then passed in urine as Hippurate [240]. It has proved to be as effective as nonabsorbable disaccharides in treating HE [241]. Glycerol phenylbutyrate also eliminates ammonia through excretion in the urinary tract, such as phenylacetylglutamine. Ammonia level with Glycerol phenylbutyrate was found to be lower than that with rifaximin and lactulose use [238]. Ornithine phenylacetate activates glutamine synthetase, inducing muscle trap of ammonia (as glutamine) followed by its conjugation with phenylacetic acid, forming phenylacetylglutamine and then excreted in urine [242]. Ornithine phenylacetate administration after GIT bleeding (upper tract) reduces ammonia levels in the plasma and appears to be safe [243].
L-ornithine-L-aspartate converts ammonia into glutamine and urea, thus reducing the level of blood ammonia [185,186]. Oral L-ornithine-L-aspartate appears to have the same effect as lactulose in improving asterixis, mental state and reducing ammonia levels [244]. A Cochrane review proved that L-ornithine-L-aspartate has a beneficial effect on mortality and improves HE, but there still needs to be a clear recommendation for its use [245].
The liver synthesizes albumin protein, which modulates the antiinflammatory response and detoxification [5,184]. Studies have proven that using albumin with lactulose is more effective in treating HE and reducing mortality than using lactulose alone [246].
Probiotics are living microorganisms that, at a certain level, have a beneficial role in the host through modulating GIT immunity [247]. Some probiotics can reduce inflammation, restore microbiota, and prevent the translocation of bacteria by maintaining the integrity of the intestinal barrier [248]. VSL#3 was the most commonly used probiotic [249]. The use of fibers with probiotics appeared to reverse the minimal HE [250]. Studies have shown that using lactulose with probiotics can decrease the risk of unimprovement among HE patients [251].
The nutritional state, portosystemic shunt, and level of decompensation are very important and affect the response of the patient to diet. Studies found no difference between the effect of vegetable protein and psyllium Plantago in comparison with animal protein in patients with type 2 DM and HE [252]. The current recommendations suggest an intake of 35–40 kcal/kg of body weight and 1.2–1.5 g/kg of protein per day in case of the presence or absence of HE, and it is better to be vegetable and animal protein [253].
5.3. Role of Liver Transplant
Persistent HE, especially when liver function is not severely affected, suggests portocaval shunts (spontaneous). These patients can benefit from embolization in the form of a decrease in the number of HE attacks [254]. Also, shunt embolization was associated with better survival in these patients if MELD < 15 and did not have hepatocellular carcinoma [255]. Liver transplantation may be a treatment option in some HE patients [184].
Microbiota plays an important role in the pathogenesis of HE. A trial showed that patients using standard lines of therapy had a poorer response than those using transplanted fecal microbiota. Also, cognition was improved compared to the standard [256]. The neurological state also improved, and the hospitalization period decreased with it [33]. However, there is still no recommendation for its use [257].
Low zinc levels can increase the ammonia level in the blood by impairing enzyme sharing in the urea cycle and glutamine synthetase. Zinc supplements were associated with improvement in the number connection test but did not affect HE recurrence [258].
Lactulose plus rifaximin is considered the best prophylaxis against HE recurrence [259]. Studies have also proved that lactulose is a very strong prophylactic agent for preventing HE after variceal bleeding (acute attack)[260]. Also, using rifampicin can decrease the hospitalization rate in the long run [261]. Long-term use of albumin can also prevent HE recurrence and reduce the incidence of grades 3 and 4 of HE [262].
Patients with end-stage liver failure may suffer from HE and confusion. This is due to manganese accumulation in the pituitary gland, mesencephalon, and lentiform nucleus, which can be seen using MRI. After liver transplantation, these changes disappear due to the functioning of a new liver [263]. Some studies showed that the degree of HE before liver transplantation affects the degree of awareness after transplantation [264,265,266]. After transplantation, cases with fourth-stage HE need nearly five days for recovery [266,267]. Intraoperative brain ischemia, permanent Ischemia to the brain with or without persistent shunt before transplantation, can make HE irreversible after transplantation [268,269,270]. Studies proved that after liver transplantation, HE will show incomplete regression. So, it is necessary to develop different treatment plans after transplantation for complete HE recovery [271].
6. Interesting Points of Discussion
6.1. Prevalence and Incidence of Minimal Hepatic Encephalopathy
MHE, which is the mildest subtype of HE, is associated with psychomotor and cognitive affection with no clinical symptoms of HE [272]. Zeegen et al. first described MHE, in which it was found that many patients who underwent surgery for portal decompression had abnormal scores (in trail-making tests) [273]. After nearly eight years, the definition of subclinical HE appeared in the literature. The definition of OHE appeared to combine the first grade of HE with MHE [274].
The incidence of MHE ranges between 20 to 80 % among cirrhotic patients early or during the disease course. This wide range is due to different tests and different diagnostic symptoms [191,275]. HE prevalence is about 10 to 14 % at the time of cirrhosis diagnosis and about 16 to 21% in patients with decompensated cirrhosis. It reaches about 50% after intrahepatic portosystemic shunt. The risk for the first attack of HE within five years of cirrhosis diagnosis can reach about 25% [184].
6.2. Impact of Minimal Hepatic Encephalopathy on Quality of Life
Liver disease affects the patient's health and quality of life. The most affected activities are psychomotor skills, information processing, and those requiring attention. However, usual activities such as dressing, shopping, and maintaining personal hygiene are maintained [191]. Several mechanisms may impair the quality of life among cirrhotic patients. Impairment of physical performance forces these patients to limit their activities, especially in the late stages of the disease. Also, cirrhosis complications such as bleeding and ascites can impair quality of life. Marchesini et al. showed that cirrhosis symptoms such as muscle cramps and itching can strongly affect quality of life [276]. Disease severity, sleep disorders, and hospitalization can also affect the quality of life [277,278]. Also, Nardelli et al. showed that anxiety, alexithymia, and depression were common among cirrhotic subjects and widely affect HRQOL (health-related quality of life)[279]. MHE patients had a reduction in psychological sub-score, total score, physical subscore, and all 12 SIP scales. Groenweg et al. reported compared to those not having MHE. An analysis showed that MHE was associated with a low SIP scale in the areas of social interaction, work, recreation, and vigilance [67]. Schomerus et al. reported that about half of MHE patients could not work [280]. Also, loss of appetite and MHE among cirrhotic patients can negatively affect HRQOL [69].
The question now is whether a certain therapy for MHE could improve HRQOL or not [67,276,281]. The prevalence of sleep disorders among cirrhotic patients varies from 26% to 70%, which greatly affects the health and quality of life [72,282]. Also, sleep disorders can badly affect the liver function and cognitive level [283]. Melatonin clearance is decreased due to the affected liver (hepatic clearance), so the level increases daily. Also, defects in the circadian rhythm of melatonin with a delayed nocturnal peak in plasma can likely occur due to decreased sensitivity to light [71]. However, other mechanisms, such as thermoregulatory and neuromuscular alteration, may contribute to this [284].
Cirrhotic patients have a very high risk for falls [285]. The possible causes may be sleep problems, changes in body composition such as myosteatosis and sarcopenia, malnutrition, antidepressant medications, cognitive dysfunction, and endocrine disorders such as hypogonadism. These fractures usually lead to hospitalizations, fractures, high costs for health care, and thus bad HRQOL. The result is more serious among cirrhotic patients due to coagulopathy and the risk of operation [79].
Urios et al. reported that MHE patients have a higher risk for falls because of delayed movement onset, increased time for reaction, defective postural control, and decreased stability [286]. All these factors could contribute to bradykinesia among MHE patients [287]. Also, cirrhotic patients have very bad outcomes after accidents (traffic mainly) with long hospital stays, high costs for health care, and higher mortality rates [62]. Furthermore, the decreased ability to work among these patients puts an economic burden on them and their families, which may increase the indirect cost of this disease [77].
6.3. Continuum of Hepatic Encephalopathy from Minimal Hepatic Encephalopathy to Overted Hepatic Encephalopathy and Prognosis
MHE is a risk factor for OHE and also for mortality [288]. Within nearly three years, about 50% of patients suffer from OHE [275]. Hartmann et al. reported an increased risk of OHE among MHE patients after nearly 29 months and more attacks of OHE than those not having cognitive defects, with no difference in mortality risk between both groups [289]. Also, other studies proved that patients with MHE are at higher risk for developing OHE, especially those having high levels of ammonia and higher severity of the disease [163]. The incidence of OHE is higher among MHE patients with impaired function of the liver and those in the late stages of cirrhosis [275]. PHES of less than six and Child-Pugh score above seven were connected with higher mortality, as Dhiman et al. reported [89]. In multivariate analysis, Amodio et al. revealed that MHE had a prognostic effect on survival and disease severity [148].
6.4. Minimal Hepatic Encephalopathy Versus Hepatic Encephalopathy Stage I in Clinical Practice
HE is classified clinically into groups according to the West Haven criteria, which considers neuromuscular problems, changes in personality, and alteration in both intellectual function and consciousness [136]. Unfortunately, the diagnosis of grade 1 HE clinically according to this criteria is suggested to be operator-dependent; from this point, the expression of OHE appeared when at least flapping tremors or temporal disorientation occurred [136,290]. This flapping tremor is a negative myoclonus, not a true tremor. When grade 1 HE, in which the patient is symptomatic, is grouped with MHE, in which the patient has only abnormal tests with no clinical symptoms, the term Covert HE appears. However, this term made a huge debate as covert means hidden, although these patients are clinically symptomatic [181]. It was also noted that this condition has a different prognosis than MHE [291]. MHE diagnosis is very important as it is a very common condition and is associated with an increased risk of OHE and a worse prognosis [163,280]. In general, patients with both grade 1 HE and MHE are likely to have the worst prognosis among cirrhotic patients with no neuropsychiatric affection [292].
7. Future Perspectives and Current Trends
7.1. Development of Biomarkers
Identifying reliable biomarkers for MHE can significantly improve early diagnosis, intervention, and patient management. A study examined the role of S-100-beta and NSE in MHE patients undergoing treatment with L-ornithine-L-aspartate. However, these biomarkers did not significantly correlate with MHE severity [293]. Labenz et al. showed that higher serum levels of neurofilament light chains were independently associated with the presence of MHE, demonstrating reliable discriminative power for MHE detection [294].
Another promising biomarker for MHE is 3-nitro-tyrosine, which has high sensitivity and specificity in detecting MHE among cirrhotic patients [295]. Also, brain-derived neurotrophic factor (BDNF) serum results were twofold lower in liver cirrhosis compared to healthy subjects, its decrease due to a degree of liver insufficiency that may serve as a potential role as a diagnostic marker for MHE [296].
The progress of artificial intelligence in the field of medical imaging offers the opportunity to discover more efficient diagnostic biomarkers and enhance the predictive accuracy of MHE and, with a significant role of modern MRI techniques, have the potential to offer new perspectives for the future detection of MHE [297]. In addition, Luo et al. suggested that the intestinal microbiota compositions of MHE patients were shown to be changed, specifically in terms of the relative abundances of Salivarius and Veillonella. These changes were linked to sleep disorders, indicating that Salivarius and Veillonella could be used as diagnostic biomarkers [298]. Gairing et al. suggest that IL-6 could be useful for identifying individuals who should undergo further psychometric testing, thereby eliminating the necessity for such testing in around one-third of cases. Furthermore, when IL-6 serum levels reach or exceed seven pg/mL, it may be appropriate to consider starting anti-HE medication in patients unable to undertake psychometric testing [299]. Collectively, a variety of biomarkers are present, but the actual challenge is to ensure accuracy and reliability using larger population studies and making more effort to identify new biomarkers.
7.2. Development of Medical Calculators
Using the DFC-Dstrength metric, seven nodes were determined to be the most distinguishing characteristics for classifying MHE from the absence of HE (noHE). These nodes include the left inferior parietal lobule, left supramarginal gyrus, left calcarine, superior frontal gyrus, left cerebellum, right postcentral gyrus, and right insula. The distinguishing features of DFCs exhibit greater precision in accurately detecting MHE in patients with cirrhosis [300].
Another study suggests that cirrhotic individuals underwent eye testing with the OSCANN desk 100. The main features were derived from the memory-guided saccades, smooth pursuit, and antisaccades tests. An algorithm achieved a sensitivity of 93% and a specificity of 93%, exceeding the performance of the current gold standard, the PHES battery test [301].
7.3. Preventive Medicine
Based on the concept that HE refers to a range of cognitive and behavioral impairments that can occur as a complication of cirrhosis and have negative effects on outcomes. Ammonia is essential in its development. Rifaximin is a non-absorbable antibiotic that prevents the growth of bacteria that produce urease and decreases the intake of ammonia from food and bacteria. Rifaximin has the potential to both prevent and treat HE in individuals with cirrhosis. However, its efficacy is dependent on the specific state of the patient [302]. Furthermore, a combination of rifaximin and lactulose may be beneficial in preventing HE after TIPS placement, and most medications are ineffective alone [303].
Modern diagnostic tools such as PHES, CFF, and ANT are used to detect and grade MHE at the initial stages. This can help intervene in time and not let it go into the OHE stage. However, PHES is not usually used in clinical practice due to its time-consuming. Hence, it is necessary to create efficient diagnostic algorithms to advance screening and therapy [105]. In addition, Probiotics were more effective in reversing MHE and reducing serum ammonia levels in patients with MHE than placebo or no treatment. Still, they were less effective than lactulose or LOLA, considering highlighting their role in preventive treatment strategies [304]. Utilizing comprehensive strategies such as the ideal transitions of care model can successfully reduce the risk of readmission in patients suffering from MHE, facilitating a smooth transition to outpatient care. Ongoing research is focused on developing innovative approaches to reduce readmissions for patients with HE and enhancing their quality of life [305]. Expanding upon the integrated approach in the optimal transitions of care framework, advancements in digital and technology can result in additional enhancements in healthcare delivery. An example of such a method is the utilization of electronic medical record (EMR) alerts and electronic checklists. A quality improvement study examined the effectiveness of a paper checklist vs an electronic checklist in managing different decompensations of cirrhosis, with a specific focus on HE [12].
8. Conclusion
MHE is a major challenge in the management of chronic liver disease since it affects a large number of patients and is often unrecognized because of subtle clinical presentation. In the present review, some interrelationships between factors involved in the pathogenesis of MHE were shed, from the central role of hyperammonemia and its neurotoxic effects to complex systemic inflammation, gut dysbiosis, and altered neurotransmission. While no single diagnostic test perfectly captures the multifaceted nature of MHE, a combination of psychometric assessments (Psychometric HE Score, PHES) with neurophysiological tools (electroencephalography, EEG; critical flicker frequency, CFF) testing, as outlined in this review, contributes to accurate detection. The reduction strategies for the ammonia burden are based on the management of MHE with nonabsorbable disaccharides, such as lactulose, and antibiotics like rifaximin. These are usually combined with nutritional therapies and probiotics. In selected cases, treatments may include embolization of portosystemic shunts or even liver transplantation. Looking ahead, the development of dependable biomarkers, AI-driven diagnostic algorithms, and preventive strategies, including gut microbiome modulation, will bring about a future in which MHE is diagnosed early to enhance the quality of life and long-term outcomes for patients with chronic liver disease.
Author Contributions
J.P.R., R.S., I.K., A.M.K., H.H.S., A.A.C., and A.L.F.C. conceived and designed the methodology of the literature review. J.P.R., R.S., I.K., A.M.K., H.H.S., and A.A.C. extracted and collected the relevant information and drafted the manuscript. A.L.F.C. supervised the article selection and reviewed and edited the manuscript. J.P.R. and A.L.F.C. reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data created.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ALD | Alcohol-related liver disease |
| ANT | Animal Naming Test |
| AP | Astrocyte Population |
| AEPs | Auditory Evoked Potentials |
| BAEPs | Brainstem Auditory Evoked Potentials |
| BCAAs | Branched-Chain Amino Acids |
| BDNF | Brain-Derived Neurotrophic Factor |
| CFF | Critical Flicker Frequency |
| CNP | Cortical Neuron Population |
| CLD | Chronic Liver Disease |
| CHC | Chronic Hepatitis C Virus |
| CHB | Chronic Hepatitis B Virus |
| cGMP | Cyclase Guanylyl Monophosphate |
| CSF | Cerebrospinal Fluid |
| CNS | Central Nervous System |
| CTP | Child-Turcotte-Pugh |
| DFCs | Distinguishing Features of DFCs |
| DMN | Default Mode Network |
| EEG | Electroencephalography |
| HE | Hepatic Encephalopathy |
| HRQOL | Health-Related Quality of Life |
| ICT | Inhibitory Control Test |
| IL | Interleukin |
| ISHEN | International Society for Hepatic Encephalopathy and Nitrogen Metabolism |
| LOLA | L-Ornithine L-Aspartate |
| MHE | Minimal Hepatic Encephalopathy |
| MDF | Mean Dominant Frequency |
| Mn | Manganese |
| NAFLD | Nonalcoholic Fatty Liver Disease |
| NHP | Nottingham Health Profile |
| NOS | Newcastle-Ottawa Scale |
| NMDA | N-Methyl-D-Aspartic Acid |
| OHE | Overt Hepatic Encephalopathy |
| PHES | Psychometric Hepatic Encephalopathy Score |
| pVEPs | Pattern Visual Evoked Potentials |
| PPI | Proton Pump Inhibitors |
| RBANS | Repeatable Battery for the Assessment of Neuropsychological Status |
| SIP | Sickness Impact Profile |
| TNF-alpha | Tumor Necrosis Factor-alpha |
| VEPs | Visual Evoked Potentials |
| WHC | West Haven Criteria |
References
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of Liver Diseases in the World. J Hepatol 2019, 70, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global Burden of Liver Disease: 2023 Update. J Hepatol 2023, 79, 516–537. [Google Scholar] [CrossRef] [PubMed]
- Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J Hepatol 2014, 61, 642–659. [CrossRef] [PubMed]
- Balzano, T.; Forteza, J.; Borreda, I.; Molina, P.; Giner, J.; Leone, P.; Urios, A.; Montoliu, C.; Felipo, V. Histological Features of Cerebellar Neuropathology in Patients With Alcoholic and Nonalcoholic Steatohepatitis. J Neuropathol Exp Neurol 2018, 77, 837–845. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Montagnese, S.; Jalan, R. Hepatic Encephalopathy in Patients with Acute Decompensation of Cirrhosis and Acute-on-Chronic Liver Failure. J Hepatol 2015, 62, 437–447. [Google Scholar] [CrossRef]
- Weissenborn, K.; Ennen, J.C.; Schomerus, H.; Rückert, N.; Hecker, H. Neuropsychological Characterization of Hepatic Encephalopathy. J Hepatol 2001, 34, 768–773. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Cordoba, J.; Mullen, K.D.; Amodio, P.; Shawcross, D.L.; Butterworth, R.F.; Morgan, M.Y. Review Article: The Design of Clinical Trials in Hepatic Encephalopathy--an International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) Consensus Statement. Aliment Pharmacol Ther 2011, 33, 739–747. [Google Scholar] [CrossRef]
- Amodio, P.; Montagnese, S.; Gatta, A.; Morgan, M.Y. Characteristics of Minimal Hepatic Encephalopathy. Metab Brain Dis 2004, 19, 253–267. [Google Scholar] [CrossRef]
- Ridola, L.; Cardinale, V.; Riggio, O. The Burden of Minimal Hepatic Encephalopathy: From Diagnosis to Therapeutic Strategies. Ann Gastroenterol 2018, 31, 151–164. [Google Scholar] [CrossRef]
- Lauridsen, M.M.; Schaffalitzky de Muckadell, O.B.; Vilstrup, H. Minimal Hepatic Encephalopathy Characterized by Parallel Use of the Continuous Reaction Time and Portosystemic Encephalopathy Tests. Metab Brain Dis 2015, 30, 1187–1192. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Thacker, L.R.; Heuman, D.M.; Gibson, D.P.; Sterling, R.K.; Stravitz, R.T.; Fuchs, M.; Sanyal, A.J.; Wade, J.B. Driving Simulation Can Improve Insight into Impaired Driving Skills in Cirrhosis. Dig Dis Sci 2012, 57, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Tapper, E.B.; Parikh, N.D.; Waljee, A.K.; Volk, M.; Carlozzi, N.E.; Lok, A.S.-F. Diagnosis of Minimal Hepatic Encephalopathy: A Systematic Review of Point-of-Care Diagnostic Tests. Am J Gastroenterol 2018, 113, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Córdoba, J.; López-Hellín, J.; Planas, M.; Sabín, P.; Sanpedro, F.; Castro, F.; Esteban, R.; Guardia, J. Normal Protein Diet for Episodic Hepatic Encephalopathy: Results of a Randomized Study. J Hepatol 2004, 41, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Meza-Junco, J.; Prado, C.M.M.; Lieffers, J.R.; Baracos, V.E.; Bain, V.G.; Sawyer, M.B. Muscle Wasting Is Associated with Mortality in Patients with Cirrhosis. Clin Gastroenterol Hepatol 2012, 10, 166–173, 173.e1. [Google Scholar] [CrossRef]
- Jalan, R.; Kapoor, D. Enhanced Renal Ammonia Excretion Following Volume Expansion in Patients with Well Compensated Cirrhosis of the Liver. Gut 2003, 52, 1041–1045. [Google Scholar] [CrossRef]
- Han, K.-H. Mechanisms of the Effects of Acidosis and Hypokalemia on Renal Ammonia Metabolism. Electrolyte Blood Press 2011, 9, 45–49. [Google Scholar] [CrossRef]
- Dasarathy, S.; Mookerjee, R.P.; Rackayova, V.; Rangroo Thrane, V.; Vairappan, B.; Ott, P.; Rose, C.F. Ammonia Toxicity: From Head to Toe? Metab Brain Dis 2017, 32, 529–538. [Google Scholar] [CrossRef]
- Weiner, I.D.; Mitch, W.E.; Sands, J.M. Urea and Ammonia Metabolism and the Control of Renal Nitrogen Excretion. Clin J Am Soc Nephrol 2015, 10, 1444–1458. [Google Scholar] [CrossRef]
- Jawaro, T.; Yang, A.; Dixit, D.; Bridgeman, M.B. Management of Hepatic Encephalopathy: A Primer. Ann Pharmacother 2016, 50, 569–577. [Google Scholar] [CrossRef]
- Kircheis, G.; Nilius, R.; Held, C.; Berndt, H.; Buchner, M.; Görtelmeyer, R.; Hendricks, R.; Krüger, B.; Kuklinski, B.; Meister, H.; et al. Therapeutic Efficacy of L-Ornithine-L-Aspartate Infusions in Patients with Cirrhosis and Hepatic Encephalopathy: Results of a Placebo-Controlled, Double-Blind Study. Hepatology 1997, 25, 1351–1360. [Google Scholar] [CrossRef]
- Bakouh, N.; Benjelloun, F.; Cherif-Zahar, B.; Planelles, G. The Challenge of Understanding Ammonium Homeostasis and the Role of the Rh Glycoproteins. Transfus Clin Biol 2006, 13, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Saparov, S.M.; Liu, K.; Agre, P.; Pohl, P. Fast and Selective Ammonia Transport by Aquaporin-8. J Biol Chem 2007, 282, 5296–5301. [Google Scholar] [CrossRef] [PubMed]
- Felipo, V.; Butterworth, R.F. Neurobiology of Ammonia. Prog Neurobiol 2002, 67, 259–279. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, J.; Norenberg, M.D. Glutamine: A Trojan Horse in Ammonia Neurotoxicity. Hepatology 2006, 44, 788–794. [Google Scholar] [CrossRef]
- Guevara, M.; Baccaro, M.E.; Ríos, J.; Martín-Llahí, M.; Uriz, J.; Ruiz del Arbol, L.; Planas, R.; Monescillo, A.; Guarner, C.; Crespo, J.; et al. Risk Factors for Hepatic Encephalopathy in Patients with Cirrhosis and Refractory Ascites: Relevance of Serum Sodium Concentration. Liver Int 2010, 30, 1137–1142. [Google Scholar] [CrossRef]
- Umapathy, S.; Dhiman, R.K.; Grover, S.; Duseja, A.; Chawla, Y.K. Persistence of Cognitive Impairment after Resolution of Overt Hepatic Encephalopathy. Am J Gastroenterol 2014, 109, 1011–1019. [Google Scholar] [CrossRef]
- Butterworth, R.F. Hepatic Encephalopathy in Cirrhosis: Pathology and Pathophysiology. Drugs 2019, 79, 17–21. [Google Scholar] [CrossRef]
- Butterworth, R.F. Neuronal Cell Death in Hepatic Encephalopathy. Metab Brain Dis 2007, 22, 309–320. [Google Scholar] [CrossRef]
- Ong, J.P.; Aggarwal, A.; Krieger, D.; Easley, K.A.; Karafa, M.T.; Van Lente, F.; Arroliga, A.C.; Mullen, K.D. Correlation between Ammonia Levels and the Severity of Hepatic Encephalopathy. Am J Med 2003, 114, 188–193. [Google Scholar] [CrossRef]
- Chao, C.C.; Hu, S. Tumor Necrosis Factor-Alpha Potentiates Glutamate Neurotoxicity in Human Fetal Brain Cell Cultures. Dev Neurosci 1994, 16, 172–179. [Google Scholar] [CrossRef]
- Merli, M.; Lucidi, C.; Pentassuglio, I.; Giannelli, V.; Giusto, M.; Di Gregorio, V.; Pasquale, C.; Nardelli, S.; Lattanzi, B.; Venditti, M.; et al. Increased Risk of Cognitive Impairment in Cirrhotic Patients with Bacterial Infections. J Hepatol 2013, 59, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Duan, Z.P.; Ha, D.K.; Bengmark, S.; Kurtovic, J.; Riordan, S.M. Synbiotic Modulation of Gut Flora: Effect on Minimal Hepatic Encephalopathy in Patients with Cirrhosis. Hepatology 2004, 39, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Fagan, A.; Gavis, E.A.; Kassam, Z.; Sikaroodi, M.; Gillevet, P.M. Long-Term Outcomes of Fecal Microbiota Transplantation in Patients With Cirrhosis. Gastroenterology 2019, 156, 1921–1923.e3. [Google Scholar] [CrossRef] [PubMed]
- Butterworth, R.F. Glutamate Transporters in Hyperammonemia. Neurochem Int 2002, 41, 81–85. [Google Scholar] [CrossRef]
- Fan, P.; Lavoie, J.; Lé, N.L.; Szerb, J.C.; Butterworth, R.F. Neurochemical and Electrophysiological Studies on the Inhibitory Effect of Ammonium Ions on Synaptic Transmission in Slices of Rat Hippocampus: Evidence for a Postsynaptic Action. Neuroscience 1990, 37, 327–334. [Google Scholar] [CrossRef]
- Palomero-Gallagher, N.; Zilles, K. Neurotransmitter Receptor Alterations in Hepatic Encephalopathy: A Review. Arch Biochem Biophys 2013, 536, 109–121. [Google Scholar] [CrossRef]
- Cascino, A.; Cangiano, C.; Fiaccadori, F.; Ghinelli, F.; Merli, M.; Pelosi, G.; Riggio, O.; Rossi Fanelli, F.; Sacchini, D.; Stortoni, M.; et al. Plasma and Cerebrospinal Fluid Amino Acid Patterns in Hepatic Encephalopathy. Dig Dis Sci 1982, 27, 828–832. [Google Scholar] [CrossRef]
- Erecińska, M.; Pastuszko, A.; Wilson, D.F.; Nelson, D. Ammonia-Induced Release of Neurotransmitters from Rat Brain Synaptosomes: Differences between the Effects on Amines and Amino Acids. J Neurochem 1987, 49, 1258–1265. [Google Scholar] [CrossRef]
- Dantzer, R.; O’Connor, J.C.; Lawson, M.A.; Kelley, K.W. Inflammation-Associated Depression: From Serotonin to Kynurenine. Psychoneuroendocrinology 2011, 36, 426–436. [Google Scholar] [CrossRef]
- Jones, E.A. Ammonia, the GABA Neurotransmitter System, and Hepatic Encephalopathy. Metab Brain Dis 2002, 17, 275–281. [Google Scholar] [CrossRef]
- Häussinger, D.; Sies, H. Hepatic Encephalopathy: Clinical Aspects and Pathogenetic Concept. Arch Biochem Biophys 2013, 536, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.; Agusti, A.; Llansola, M.; Montoliu, C.; Strömberg, J.; Malinina, E.; Ragagnin, G.; Doverskog, M.; Bäckström, T.; Felipo, V. GR3027 Antagonizes GABAA Receptor-Potentiating Neurosteroids and Restores Spatial Learning and Motor Coordination in Rats with Chronic Hyperammonemia and Hepatic Encephalopathy. Am J Physiol Gastrointest Liver Physiol 2015, 309, G400–409. [Google Scholar] [CrossRef] [PubMed]
- Normandin, L.; Hazell, A.S. Manganese Neurotoxicity: An Update of Pathophysiologic Mechanisms. Metab Brain Dis 2002, 17, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Bouabid, S.; Tinakoua, A.; Lakhdar-Ghazal, N.; Benazzouz, A. Manganese Neurotoxicity: Behavioral Disorders Associated with Dysfunctions in the Basal Ganglia and Neurochemical Transmission. J Neurochem 2016, 136, 677–691. [Google Scholar] [CrossRef]
- Li, X.; Liu, S.; Xiang, H.; Zhang, Q.; Guo, Y.; Zu, H.; Wang, J.; Lv, J.; Zhang, X.; Meng, F.; et al. Prevalence and Risk Factors for Minimal Hepatic Encephalopathy in Cirrhotic Patients with Different Etiologies. Portal Hypertension & Cirrhosis 2023, 2, 171–180. [Google Scholar] [CrossRef]
- Jepsen, P.; Christensen, J.; Weissenborn, K.; Watson, H.; Vilstrup, H. Epilepsy as a Risk Factor for Hepatic Encephalopathy in Patients with Cirrhosis: A Cohort Study. BMC Gastroenterol 2016, 16, 77. [Google Scholar] [CrossRef]
- Chang, K.-V.; Chen, J.-D.; Wu, W.-T.; Huang, K.-C.; Lin, H.-Y.; Han, D.-S. Is Sarcopenia Associated with Hepatic Encephalopathy in Liver Cirrhosis? A Systematic Review and Meta-Analysis. J Formos Med Assoc 2019, 118, 833–842. [Google Scholar] [CrossRef]
- Shawcross, D.L.; Wright, G.; Olde Damink, S.W.M.; Jalan, R. Role of Ammonia and Inflammation in Minimal Hepatic Encephalopathy. Metab Brain Dis 2007, 22, 125–138. [Google Scholar] [CrossRef]
- Montoliu, C.; Piedrafita, B.; Serra, M.A.; del Olmo, J.A.; Urios, A.; Rodrigo, J.M.; Felipo, V. IL-6 and IL-18 in Blood May Discriminate Cirrhotic Patients with and without Minimal Hepatic Encephalopathy. J Clin Gastroenterol 2009, 43, 272–279. [Google Scholar] [CrossRef]
- Felipo, V.; Urios, A.; Montesinos, E.; Molina, I.; Garcia-Torres, M.L.; Civera, M.; Olmo, J.A.D.; Ortega, J.; Martinez-Valls, J.; Serra, M.A.; et al. Contribution of Hyperammonemia and Inflammatory Factors to Cognitive Impairment in Minimal Hepatic Encephalopathy. Metab Brain Dis 2012, 27, 51–58. [Google Scholar] [CrossRef]
- López-Franco, Ó.; Morin, J.-P.; Cortés-Sol, A.; Molina-Jiménez, T.; Del Moral, D.I.; Flores-Muñoz, M.; Roldán-Roldán, G.; Juárez-Portilla, C.; Zepeda, R.C. Cognitive Impairment After Resolution of Hepatic Encephalopathy: A Systematic Review and Meta-Analysis. Front Neurosci 2021, 15, 579263. [Google Scholar] [CrossRef] [PubMed]
- Felipo, V. Hepatic Encephalopathy: Effects of Liver Failure on Brain Function. Nat Rev Neurosci 2013, 14, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Wu, B.; Chen, T.; Diao, W.; Jia, Z. Altered Intrinsic Brain Activity in Patients with Hepatic Encephalopathy. J Neurosci Res 2021, 99, 1337–1353. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-J.; Jiao, Y.; Zhu, X.-Q.; Zhang, H.-Y.; Liu, J.-C.; Wen, S.; Teng, G.-J. Brain Dysfunction Primarily Related to Previous Overt Hepatic Encephalopathy Compared with Minimal Hepatic Encephalopathy: Resting-State Functional MR Imaging Demonstration. Radiology 2013, 266, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical Characterization and Outcome. Arch Neurol 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Rikkers, L.; Jenko, P.; Rudman, D.; Freides, D. Subclinical Hepatic Encephalopathy: Detection, Prevalence, and Relationship to Nitrogen Metabolism. Gastroenterology 1978, 75, 462–469. [Google Scholar] [CrossRef]
- Schomerus, H.; Hamster, W.; Blunck, H.; Reinhard, U.; Mayer, K.; Dölle, W. Latent Portasystemic Encephalopathy. I. Nature of Cerebral Functional Defects and Their Effect on Fitness to Drive. Dig Dis Sci 1981, 26, 622–630. [Google Scholar] [CrossRef]
- Weissenborn, K.; Heidenreich, S.; Giewekemeyer, K.; Rückert, N.; Hecker, H. Memory Function in Early Hepatic Encephalopathy. J Hepatol 2003, 39, 320–325. [Google Scholar] [CrossRef]
- Lockwood, A.H. “What’s in a Name?” Improving the Care of Cirrhotics. J Hepatol 2000, 32, 859–861. [Google Scholar] [CrossRef]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic Encephalopathy--Definition, Nomenclature, Diagnosis, and Quantification: Final Report of the Working Party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef]
- Bass, N.M.; Mullen, K.D.; Sanyal, A.; Poordad, F.; Neff, G.; Leevy, C.B.; Sigal, S.; Sheikh, M.Y.; Beavers, K.; Frederick, T.; et al. Rifaximin Treatment in Hepatic Encephalopathy. N Engl J Med 2010, 362, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S. Minimal Hepatic Encephalopathy Matters in Daily Life. World J Gastroenterol 2008, 14, 3609–3615. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Saeian, K.; Schubert, C.M.; Hafeezullah, M.; Franco, J.; Varma, R.R.; Gibson, D.P.; Hoffmann, R.G.; Stravitz, R.T.; Heuman, D.M.; et al. Minimal Hepatic Encephalopathy Is Associated with Motor Vehicle Crashes: The Reality beyond the Driving Test. Hepatology 2009, 50, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Seyan, A.S.; Hughes, R.D.; Shawcross, D.L. Changing Face of Hepatic Encephalopathy: Role of Inflammation and Oxidative Stress. World J Gastroenterol 2010, 16, 3347–3357. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Hays, R.D.; Kilbourne, A.; Rosen, H.R.; Keeffe, E.B.; Artinian, L.; Kim, S.; Lazarovici, D.; Jensen, D.M.; Busuttil, R.W.; et al. Development and Evaluation of the Liver Disease Quality of Life Instrument in Persons with Advanced, Chronic Liver Disease--the LDQOL 1.0. Am J Gastroenterol 2000, 95, 3552–3565. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Guyatt, G.; Kiwi, M.; Boparai, N.; King, D. Development of a Disease Specific Questionnaire to Measure Health Related Quality of Life in Patients with Chronic Liver Disease. Gut 1999, 45, 295–300. [Google Scholar] [CrossRef]
- Groeneweg, M.; Quero, J.C.; De Bruijn, I.; Hartmann, I.J.; Essink-bot, M.L.; Hop, W.C.; Schalm, S.W. Subclinical Hepatic Encephalopathy Impairs Daily Functioning. Hepatology 1998, 28, 45–49. [Google Scholar] [CrossRef]
- Kim, W.R.; Lindor, K.D.; Malinchoc, M.; Petz, J.L.; Jorgensen, R.; Dickson, E.R. Reliability and Validity of the NIDDK-QA Instrument in the Assessment of Quality of Life in Ambulatory Patients with Cholestatic Liver Disease. Hepatology 2000, 32, 924–929. [Google Scholar] [CrossRef]
- Mina, A.; Moran, S.; Ortiz-Olvera, N.; Mera, R.; Uribe, M. Prevalence of Minimal Hepatic Encephalopathy and Quality of Life in Patients with Decompensated Cirrhosis. Hepatol Res 2014, 44, E92–99. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Wade, J.B.; Gibson, D.P.; Saeian, K.; Wegelin, J.A.; Hafeezullah, M.; Bell, D.E.; Sterling, R.K.; Stravitz, R.T.; et al. Rifaximin Improves Driving Simulator Performance in a Randomized Trial of Patients with Minimal Hepatic Encephalopathy. Gastroenterology 2011, 140, 478–487.e1. [Google Scholar] [CrossRef]
- Montagnese, S.; De Pittà, C.; De Rui, M.; Corrias, M.; Turco, M.; Merkel, C.; Amodio, P.; Costa, R.; Skene, D.J.; Gatta, A. Sleep-Wake Abnormalities in Patients with Cirrhosis. Hepatology 2014, 59, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; Middleton, B.; Skene, D.J.; Morgan, M.Y. Night-Time Sleep Disturbance Does Not Correlate with Neuropsychiatric Impairment in Patients with Cirrhosis. Liver Int 2009, 29, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.; Córdoba, J.; Jacas, C.; Flavià, M.; Esteban, R.; Guardia, J. Neuropsychological Abnormalities in Cirrhosis Include Learning Impairment. J Hepatol 2006, 44, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, A.H.; Weissenborn, K.; Bokemeyer, M.; Tietge, U.; Burchert, W. Correlations between Cerebral Glucose Metabolism and Neuropsychological Test Performance in Nonalcoholic Cirrhotics. Metab Brain Dis 2002, 17, 29–40. [Google Scholar] [CrossRef]
- Erceg, S.; Monfort, P.; Hernández-Viadel, M.; Rodrigo, R.; Montoliu, C.; Felipo, V. Oral Administration of Sildenafil Restores Learning Ability in Rats with Hyperammonemia and with Portacaval Shunts. Hepatology 2005, 41, 299–306. [Google Scholar] [CrossRef]
- Srivastava, A.; Mehta, R.; Rothke, S.P.; Rademaker, A.W.; Blei, A.T. Fitness to Drive in Patients with Cirrhosis and Portal-Systemic Shunting: A Pilot Study Evaluating Driving Performance. J Hepatol 1994, 21, 1023–1028. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Hafeezullah, M.; Hoffmann, R.G.; Varma, R.R.; Franco, J.; Binion, D.G.; Hammeke, T.A.; Saeian, K. Navigation Skill Impairment: Another Dimension of the Driving Difficulties in Minimal Hepatic Encephalopathy. Hepatology 2008, 47, 596–604. [Google Scholar] [CrossRef]
- Román, E.; Córdoba, J.; Torrens, M.; Torras, X.; Villanueva, C.; Vargas, V.; Guarner, C.; Soriano, G. Minimal Hepatic Encephalopathy Is Associated with Falls. Am J Gastroenterol 2011, 106, 476–482. [Google Scholar] [CrossRef]
- Soriano, G.; Román, E.; Córdoba, J.; Torrens, M.; Poca, M.; Torras, X.; Villanueva, C.; Gich, I.J.; Vargas, V.; Guarner, C. Cognitive Dysfunction in Cirrhosis Is Associated with Falls: A Prospective Study. Hepatology 2012, 55, 1922–1930. [Google Scholar] [CrossRef]
- Collier, J. Bone Disorders in Chronic Liver Disease. Hepatology 2007, 46, 1271–1278. [Google Scholar] [CrossRef]
- Groeneweg, M.; Moerland, W.; Quero, J.C.; Hop, W.C.; Krabbe, P.F.; Schalm, S.W. Screening of Subclinical Hepatic Encephalopathy. J Hepatol 2000, 32, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Poordad, F.F. Review Article: The Burden of Hepatic Encephalopathy. Aliment Pharmacol Ther 2007, 25 Suppl 1, 3–9. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Córdoba, J.; Jover, R.; del Olmo, J.A.; Ramírez, M.; Rey, R.; de Madaria, E.; Montoliu, C.; Nuñez, D.; Flavia, M.; et al. Value of the Critical Flicker Frequency in Patients with Minimal Hepatic Encephalopathy. Hepatology 2007, 45, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K.; Chawla, Y.K. Minimal Hepatic Encephalopathy. Indian J Gastroenterol 2009, 28, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Nardone, R.; Taylor, A.C.; Höller, Y.; Brigo, F.; Lochner, P.; Trinka, E. Minimal Hepatic Encephalopathy: A Review. Neurosci Res 2016, 111, 1–12. [Google Scholar] [CrossRef]
- Wein, C.; Koch, H.; Popp, B.; Oehler, G.; Schauder, P. Minimal Hepatic Encephalopathy Impairs Fitness to Drive. Hepatology 2004, 39, 739–745. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Wade, J.B.; Sanyal, A.J. Spectrum of Neurocognitive Impairment in Cirrhosis: Implications for the Assessment of Hepatic Encephalopathy. Hepatology 2009, 50, 2014–2021. [Google Scholar] [CrossRef]
- Nardelli, S.; Gioia, S.; Faccioli, J.; Riggio, O.; Ridola, L. Sarcopenia and Cognitive Impairment in Liver Cirrhosis: A Viewpoint on the Clinical Impact of Minimal Hepatic Encephalopathy. World J Gastroenterol 2019, 25, 5257–5265. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Kurmi, R.; Thumburu, K.K.; Venkataramarao, S.H.; Agarwal, R.; Duseja, A.; Chawla, Y. Diagnosis and Prognostic Significance of Minimal Hepatic Encephalopathy in Patients with Cirrhosis of Liver. Dig Dis Sci 2010, 55, 2381–2390. [Google Scholar] [CrossRef]
- Duff, K.; Ramezani, A. Regression-Based Normative Formulae for the Repeatable Battery for the Assessment of Neuropsychological Status for Older Adults. Arch Clin Neuropsychol 2015, 30, 600–604. [Google Scholar] [CrossRef]
- Campagna, F.; Montagnese, S.; Ridola, L.; Senzolo, M.; Schiff, S.; De Rui, M.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Merkel, C.; et al. The Animal Naming Test: An Easy Tool for the Assessment of Hepatic Encephalopathy. Hepatology 2017, 66, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Heuman, D.M.; Sterling, R.K.; Sanyal, A.J.; Siddiqui, M.; Matherly, S.; Luketic, V.; Stravitz, R.T.; Fuchs, M.; Thacker, L.R.; et al. Validation of EncephalApp, Smartphone-Based Stroop Test, for the Diagnosis of Covert Hepatic Encephalopathy. Clin Gastroenterol Hepatol 2015, 13, 1828–1835.e1. [Google Scholar] [CrossRef] [PubMed]
- Acharya, C.; Shaw, J.; Duong, N.; Fagan, A.; McGeorge, S.; Wade, J.B.; Thacker, L.R.; Bajaj, J.S. QuickStroop, a Shortened Version of EncephalApp, Detects Covert Hepatic Encephalopathy With Similar Accuracy Within One Minute. Clin Gastroenterol Hepatol 2023, 21, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; Schiff, S.; De Rui, M.; Crossey, M.M.E.; Amodio, P.; Taylor-Robinson, S.D. Neuropsychological Tools in Hepatology: A Survival Guide for the Clinician. J Viral Hepat 2012, 19, 307–315. [Google Scholar] [CrossRef]
- Amodio, P.; Campagna, F.; Olianas, S.; Iannizzi, P.; Mapelli, D.; Penzo, M.; Angeli, P.; Gatta, A. Detection of Minimal Hepatic Encephalopathy: Normalization and Optimization of the Psychometric Hepatic Encephalopathy Score. A Neuropsychological and Quantified EEG Study. J Hepatol 2008, 49, 346–353. [Google Scholar] [CrossRef]
- Duarte-Rojo, A.; Estradas, J.; Hernández-Ramos, R.; Ponce-de-León, S.; Córdoba, J.; Torre, A. Validation of the Psychometric Hepatic Encephalopathy Score (PHES) for Identifying Patients with Minimal Hepatic Encephalopathy. Dig Dis Sci 2011, 56, 3014–3023. [Google Scholar] [CrossRef]
- Seo, Y.S.; Yim, S.Y.; Jung, J.Y.; Kim, C.H.; Kim, J.D.; Keum, B.; An, H.; Yim, H.J.; Lee, H.S.; Kim, C.D.; et al. Psychometric Hepatic Encephalopathy Score for the Detection of Minimal Hepatic Encephalopathy in Korean Patients with Liver Cirrhosis. J Gastroenterol Hepatol 2012, 27, 1695–1704. [Google Scholar] [CrossRef]
- Li, S.-W.; Wang, K.; Yu, Y.-Q.; Wang, H.-B.; Li, Y.-H.; Xu, J.-M. Psychometric Hepatic Encephalopathy Score for Diagnosis of Minimal Hepatic Encephalopathy in China. World J Gastroenterol 2013, 19, 8745–8751. [Google Scholar] [CrossRef]
- Schmitt, A.L.; Livingston, R.B.; Smernoff, E.N.; Reese, E.M.; Hafer, D.G.; Harris, J.B. Factor Analysis of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) in a Large Sample of Patients Suspected of Dementia. Appl Neuropsychol 2010, 17, 8–17. [Google Scholar] [CrossRef]
- Garcia, C.; Leahy, B.; Corradi, K.; Forchetti, C. Component Structure of the Repeatable Battery for the Assessment of Neuropsychological Status in Dementia. Arch Clin Neuropsychol 2008, 23, 63–72. [Google Scholar] [CrossRef]
- McKay, C.; Wertheimer, J.C.; Fichtenberg, N.L.; Casey, J.E. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Clinical Utility in a Traumatic Brain Injury Sample. Clin Neuropsychol 2008, 22, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Beul, L.; Toenges, G.; Schattenberg, J.M.; Nagel, M.; Sprinzl, M.F.; Nguyen-Tat, M.; Zimmermann, T.; Huber, Y.; Marquardt, J.U.; et al. Validation of the Simplified Animal Naming Test as Primary Screening Tool for the Diagnosis of Covert Hepatic Encephalopathy. Eur J Intern Med 2019, 60, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Taneja, S.; Chopra, M.; Duseja, A.; Dhiman, R.K. Animal Naming Test - a Simple and Accurate Test for Diagnosis of Minimal Hepatic Encephalopathy and Prediction of Overt Hepatic Encephalopathy. Clin Exp Hepatol 2020, 6, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Li, T.; Lin, C.; Liu, F.; Wu, S.; Wang, L.; Ye, Q. Animal Naming Test for the Assessment of Minimal Hepatic Encephalopathy in Asian Cirrhotic Populations. Clin Res Hepatol Gastroenterol 2021, 45, 101729. [Google Scholar] [CrossRef]
- Gairing, S.J.; Schleicher, E.M.; Galle, P.R.; Labenz, C. Prediction and Prevention of the First Episode of Overt Hepatic Encephalopathy in Patients with Cirrhosis. Hepatol Commun 2023, 7. [Google Scholar] [CrossRef]
- Lauridsen, M.M.; Mikkelsen, S.; Svensson, T.; Holm, J.; Klüver, C.; Gram, J.; Vilstrup, H.; Schaffalitzky de Muckadell, O.B. The Continuous Reaction Time Test for Minimal Hepatic Encephalopathy Validated by a Randomized Controlled Multi-Modal Intervention-A Pilot Study. PLoS One 2017, 12, e0185412. [Google Scholar] [CrossRef]
- Taneja, S.; Dhiman, R.K.; Khatri, A.; Goyal, S.; Thumbru, K.K.; Agarwal, R.; Duseja, A.; Chawla, Y. Inhibitory Control Test for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis of Liver. J Clin Exp Hepatol 2012, 2, 306–314. [Google Scholar] [CrossRef]
- Goldbecker, A.; Weissenborn, K.; Hamidi Shahrezaei, G.; Afshar, K.; Rümke, S.; Barg-Hock, H.; Strassburg, C.P.; Hecker, H.; Tryc, A.B. Comparison of the Most Favoured Methods for the Diagnosis of Hepatic Encephalopathy in Liver Transplantation Candidates. Gut 2013, 62, 1497–1504. [Google Scholar] [CrossRef]
- Gupta, D.; Ingle, M.; Shah, K.; Phadke, A.; Sawant, P. Prospective Comparative Study of Inhibitory Control Test and Psychometric Hepatic Encephalopathy Score for Diagnosis and Prognosis of Minimal Hepatic Encephalopathy in Cirrhotic Patients in the Indian Subcontinent. J Dig Dis 2015, 16, 400–407. [Google Scholar] [CrossRef]
- Luo, M.; Yu, X.-B.; Hu, S.-J.; Bai, F.-H. EncephalApp Stroop App Predicts Poor Sleep Quality in Patients with Minimal Hepatic Encephalopathy Due to Hepatitis B-Induced Liver Cirrhosis. Saudi J Gastroenterol 2020, 26, 120–128. [Google Scholar] [CrossRef]
- Cunha-Silva, M.; Neto, F.L.P.; de Araújo, P.S.; Pazinato, L.V.; Greca, R.D.; Secundo, T.M.L.; Imbrizi, M.R.; Monici, L.T.; Sevá-Pereira, T.; Mazo, D.F. EncephalApp Stroop Test Validation for the Screening of Minimal Hepatic Encephalopathy in Brazil. Ann Hepatol 2022, 27, 100543. [Google Scholar] [CrossRef] [PubMed]
- Lupescu, I.C.; Iacob, S.; Lupescu, I.G.; Pietrareanu, C.; Gheorghe, L. Assessment of Minimal Hepatic Encephalopathy with Brain MRI and EncephalApp Stroop Test. Maedica (Bucur) 2023, 18, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Nabi, E.; Thacker, L.R.; Wade, J.B.; Sterling, R.K.; Stravitz, R.T.; Fuchs, M.; Heuman, D.M.; Bouneva, I.; Sanyal, A.J.; Siddiqui, M.S.; et al. Diagnosis of Covert Hepatic Encephalopathy without Specialized Tests. Clin Gastroenterol Hepatol 2014, 12, 1384–1389.e2. [Google Scholar] [CrossRef]
- Maharshi, S.; Sharma, B.C.; Sachdeva, S.; Srivastava, S.; Sharma, P. Efficacy of Nutritional Therapy for Patients With Cirrhosis and Minimal Hepatic Encephalopathy in a Randomized Trial. Clin Gastroenterol Hepatol 2016, 14, 454–460.e3, quiz e33. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, M.M.; Jepsen, P.; Wernberg, C.W.; Schaffalitzky de Muckadell, O.B.; Bajaj, J.S.; Vilstrup, H. Validation of a Simple Quality-of-Life Score for Identification of Minimal and Prediction of Overt Hepatic Encephalopathy. Hepatol Commun 2020, 4, 1353–1361. [Google Scholar] [CrossRef]
- Luo, M.; Ma, P.; Li, L.; Cao, W.-K. Advances in Psychometric Tests for Screening Minimal Hepatic Encephalopathy: From Paper-and-Pencil to Computer-Aided Assessment. Turk J Gastroenterol 2019, 30, 398–407. [Google Scholar] [CrossRef]
- McLaughlin, T.J.; Koff, R.S. Feedback EEG in the Detection of Subclinical Hepatic Encephalopathy: A Preliminary Report. Int J Psychophysiol 1989, 8, 137–143. [Google Scholar] [CrossRef]
- Amodio, P.; Marchetti, P.; Del Piccolo, F.; de Tourtchaninoff, M.; Varghese, P.; Zuliani, C.; Campo, G.; Gatta, A.; Guérit, J.M. Spectral versus Visual EEG Analysis in Mild Hepatic Encephalopathy. Clin Neurophysiol 1999, 110, 1334–1344. [Google Scholar] [CrossRef]
- Amodio, P.; Pellegrini, A.; Ubiali, E.; Mathy, I.; Piccolo, F.D.; Orsato, R.; Gatta, A.; Guerit, J.M. The EEG Assessment of Low-Grade Hepatic Encephalopathy: Comparison of an Artificial Neural Network-Expert System (ANNES) Based Evaluation with Visual EEG Readings and EEG Spectral Analysis. Clin Neurophysiol 2006, 117, 2243–2251. [Google Scholar] [CrossRef]
- Pascoli, D.; Guérit, J.M.; Montagnese, S.; de Tourtchaninoff, M.; Minelli, T.; Pellegrini, A.; Del Piccolo, F.; Gatta, A.; Amodio, P. Analysis of EEG Tracings in Frequency and Time Domain in Hepatic Encephalopathy. Comput Methods Programs Biomed 2006, 81, 203–212. [Google Scholar] [CrossRef]
- Schiff, S.; Casa, M.; Di Caro, V.; Aprile, D.; Spinelli, G.; De Rui, M.; Angeli, P.; Amodio, P.; Montagnese, S. A Low-Cost, User-Friendly Electroencephalographic Recording System for the Assessment of Hepatic Encephalopathy. Hepatology 2016, 63, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Gatta, A. Neurophysiological Investigation of Hepatic Encephalopathy. Metab Brain Dis 2005, 20, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Kullmann, F.; Hollerbach, S.; Holstege, A.; Schölmerich, J. Subclinical Hepatic Encephalopathy: The Diagnostic Value of Evoked Potentials. J Hepatol 1995, 22, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Zeneroli, M.L.; Pinelli, G.; Gollini, G.; Penne, A.; Messori, E.; Zani, G.; Ventura, E. Visual Evoked Potential: A Diagnostic Tool for the Assessment of Hepatic Encephalopathy. Gut 1984, 25, 291–299. [Google Scholar] [CrossRef]
- Sharma, P.; Sharma, B.C.; Puri, V.; Sarin, S.K. Critical Flicker Frequency: Diagnostic Tool for Minimal Hepatic Encephalopathy. J Hepatol 2007, 47, 67–73. [Google Scholar] [CrossRef]
- Sharma, P.; Sharma, B.C.; Sarin, S.K. Critical Flicker Frequency for Diagnosis and Assessment of Recovery from Minimal Hepatic Encephalopathy in Patients with Cirrhosis. Hepatobiliary Pancreat Dis Int 2010, 9, 27–32. [Google Scholar]
- Lauridsen, M.M.; Jepsen, P.; Vilstrup, H. Critical Flicker Frequency and Continuous Reaction Times for the Diagnosis of Minimal Hepatic Encephalopathy: A Comparative Study of 154 Patients with Liver Disease. Metab Brain Dis 2011, 26, 135–139. [Google Scholar] [CrossRef]
- Barone, M.; Shahini, E.; Iannone, A.; Viggiani, M.T.; Corvace, V.; Principi, M.; Di Leo, A. Critical Flicker Frequency Test Predicts Overt Hepatic Encephalopathy and Survival in Patients with Liver Cirrhosis. Dig Liver Dis 2018, 50, 496–500. [Google Scholar] [CrossRef]
- Direkze, S.; Jalan, R. Diagnosis and Treatment of Low-Grade Hepatic Encephalopathy. Dig Dis 2015, 33, 562–569. [Google Scholar] [CrossRef]
- Suzuki, K.; Kuroda, H.; Sawara, K.; Yoshida, Y.; Kakisaka, K.; Suzuki, Y.; Suzuki, A.; Onodera, M.; Oikawa, T.; Tei, W. Predictive Biomarkers for Diagnosis of Minimal Hepatic Encephalopathy in Patients with Liver Cirrhosis: A Preliminary Result in a Single Center Study in Japan. Biomed Res Clin Prac 2016, 1. [Google Scholar] [CrossRef]
- Fiati Kenston, S.S.; Song, X.; Li, Z.; Zhao, J. Mechanistic Insight, Diagnosis, and Treatment of Ammonia-Induced Hepatic Encephalopathy. J Gastroenterol Hepatol 2019, 34, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Montoliu, C.; Cauli, O.; Urios, A.; ElMlili, N.; Serra, M.A.; Giner-Duran, R.; González-Lopez, O.; Del Olmo, J.A.; Wassel, A.; Rodrigo, J.M.; et al. 3-Nitro-Tyrosine as a Peripheral Biomarker of Minimal Hepatic Encephalopathy in Patients with Liver Cirrhosis. Am J Gastroenterol 2011, 106, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Salman, T.; Elsabaawy, M.; Omar, M.; Afify, M.; Elezawy, H.; Ghanem, S.; Abdelraouf, O.; Rewisha, E.; Shebl, N. Evaluation of Different Diagnostic Modalities of Minimal Hepatic Encephalopathy in Cirrhotic Patients: Case-Control Study. Clin Exp Hepatol 2021, 7, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Thanapirom, K.; Wongwandee, M.; Suksawatamnuay, S.; Thaimai, P.; Siripon, N.; Makhasen, W.; Treeprasertsuk, S.; Komolmit, P. Psychometric Hepatic Encephalopathy Score for the Diagnosis of Minimal Hepatic Encephalopathy in Thai Cirrhotic Patients. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Randolph, C.; Hilsabeck, R.; Kato, A.; Kharbanda, P.; Li, Y.-Y.; Mapelli, D.; Ravdin, L.D.; Romero-Gomez, M.; Stracciari, A.; Weissenborn, K. Neuropsychological Assessment of Hepatic Encephalopathy: ISHEN Practice Guidelines. Liver Int 2009, 29, 629–635. [Google Scholar] [CrossRef]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- Tarter, R.E.; Van Thiel, D.H.; Arria, A.M.; Carra, J.; Moss, H. Impact of Cirrhosis on the Neuropsychological Test Performance of Alcoholics. Alcohol Clin Exp Res 1988, 12, 619–621. [Google Scholar] [CrossRef]
- Sorrell, J.H.; Zolnikov, B.J.; Sharma, A.; Jinnai, I. Cognitive Impairment in People Diagnosed with End-Stage Liver Disease Evaluated for Liver Transplantation. Psychiatry Clin Neurosci 2006, 60, 174–181. [Google Scholar] [CrossRef]
- Louissaint, J.; Deutsch-Link, S.; Tapper, E.B. Changing Epidemiology of Cirrhosis and Hepatic Encephalopathy. Clin Gastroenterol Hepatol 2022, 20, S1–S8. [Google Scholar] [CrossRef]
- Lauridsen, M.M.; Grønbæk, H.; Næser, E.B.; Leth, S.T.; Vilstrup, H. Gender and Age Effects on the Continuous Reaction Times Method in Volunteers and Patients with Cirrhosis. Metab Brain Dis 2012, 27, 559–565. [Google Scholar] [CrossRef]
- Pawar, V.B.; Surude, R.G.; Sonthalia, N.; Zanwar, V.; Jain, S.; Contractor, Q.; Rathi, P.M. Minimal Hepatic Encephalopathy in Indians: Psychometric Hepatic Encephalopathy Score and Inhibitory Control Test for Diagnosis and Rifaximin or Lactulose for Its Reversal. J Clin Transl Hepatol 2019, 7, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Saeian, K.; Verber, M.D.; Hischke, D.; Hoffmann, R.G.; Franco, J.; Varma, R.R.; Rao, S.M. Inhibitory Control Test Is a Simple Method to Diagnose Minimal Hepatic Encephalopathy and Predict Development of Overt Hepatic Encephalopathy. Am J Gastroenterol 2007, 102, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Hafeezullah, M.; Franco, J.; Varma, R.R.; Hoffmann, R.G.; Knox, J.F.; Hischke, D.; Hammeke, T.A.; Pinkerton, S.D.; Saeian, K. Inhibitory Control Test for the Diagnosis of Minimal Hepatic Encephalopathy. Gastroenterology 2008, 135, 1591–1600.e1. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Ridola, L.; Schiff, S.; Montagnese, S.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Trezza, M.; Marzano, C.; Flaiban, C.; et al. Improving the Inhibitory Control Task to Detect Minimal Hepatic Encephalopathy. Gastroenterology 2010, 139, 510–518, 518.e1-2. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Thacker, L.R.; Heuman, D.M.; Fuchs, M.; Sterling, R.K.; Sanyal, A.J.; Puri, P.; Siddiqui, M.S.; Stravitz, R.T.; Bouneva, I.; et al. The Stroop Smartphone Application Is a Short and Valid Method to Screen for Minimal Hepatic Encephalopathy. Hepatology 2013, 58, 1122–1132. [Google Scholar] [CrossRef]
- Allampati, S.; Duarte-Rojo, A.; Thacker, L.R.; Patidar, K.R.; White, M.B.; Klair, J.S.; John, B.; Heuman, D.M.; Wade, J.B.; Flud, C.; et al. Diagnosis of Minimal Hepatic Encephalopathy Using Stroop EncephalApp: A Multicenter US-Based, Norm-Based Study. Am J Gastroenterol 2016, 111, 78–86. [Google Scholar] [CrossRef]
- Kanagalingam, G.; Park, D.; Badal, B.D.; Fagan, A.; Thacker, L.R.; Bajaj, J.S. QuickStroop Predicts Time to Development of Overt Hepatic Encephalopathy and Related Hospitalizations in Patients With Cirrhosis. Clin Gastroenterol Hepatol 2024, 22, 899–901.e2. [Google Scholar] [CrossRef]
- Amodio, P.; Del Piccolo, F.; Marchetti, P.; Angeli, P.; Iemmolo, R.; Caregaro, L.; Merkel, C.; Gerunda, G.; Gatta, A. Clinical Features and Survivial of Cirrhotic Patients with Subclinical Cognitive Alterations Detected by the Number Connection Test and Computerized Psychometric Tests. Hepatology 1999, 29, 1662–1667. [Google Scholar] [CrossRef]
- Amodio, P.; Marchetti, P.; Del Piccolo, F.; Rizzo, C.; Iemmolo, R.M.; Caregaro, L.; Gerunda, G.; Gatta, A. Study on the Sternberg Paradigm in Cirrhotic Patients without Overt Hepatic Encephalopathy. Metab Brain Dis 1998, 13, 159–172. [Google Scholar] [CrossRef]
- Kaplan, P.W. The EEG in Metabolic Encephalopathy and Coma. J Clin Neurophysiol 2004, 21, 307–318. [Google Scholar]
- Götz, T.; Huonker, R.; Kranczioch, C.; Reuken, P.; Witte, O.W.; Günther, A.; Debener, S. Impaired Evoked and Resting-State Brain Oscillations in Patients with Liver Cirrhosis as Revealed by Magnetoencephalography. Neuroimage Clin 2013, 2, 873–882. [Google Scholar] [CrossRef] [PubMed]
- PARSONS-SMITH, B.G.; SUMMERSKILL, W.H.; DAWSON, A.M.; SHERLOCK, S. The Electroencephalograph in Liver Disease. Lancet 1957, 273, 867–871. [Google Scholar] [CrossRef]
- Guerit, J.-M.; Amantini, A.; Fischer, C.; Kaplan, P.W.; Mecarelli, O.; Schnitzler, A.; Ubiali, E.; Amodio, P. Neurophysiological Investigations of Hepatic Encephalopathy: ISHEN Practice Guidelines. Liver Int 2009, 29, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Del Piccolo, F.; Pettenò, E.; Mapelli, D.; Angeli, P.; Iemmolo, R.; Muraca, M.; Musto, C.; Gerunda, G.; Rizzo, C.; et al. Prevalence and Prognostic Value of Quantified Electroencephalogram (EEG) Alterations in Cirrhotic Patients. J Hepatol 2001, 35, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, P.; D’Avanzo, C.; Orsato, R.; Montagnese, S.; Schiff, S.; Kaplan, P.W.; Piccione, F.; Merkel, C.; Gatta, A.; Sparacino, G.; et al. Electroencephalography in Patients with Cirrhosis. Gastroenterology 2011, 141, 1680–1689.e1. [Google Scholar] [CrossRef]
- Song, J.; Westover, M.B.; Zhang, R. A Neural Mass Model for Disturbance of Alpha Rhythm in the Minimal Hepatic Encephalopathy. Mol Cell Neurosci 2024, 128, 103918. [Google Scholar] [CrossRef]
- Córdoba, J.; Raguer, N.; Flavià, M.; Vargas, V.; Jacas, C.; Alonso, J.; Rovira, A. T2 Hyperintensity along the Cortico-Spinal Tract in Cirrhosis Relates to Functional Abnormalities. Hepatology 2003, 38, 1026–1033. [Google Scholar] [CrossRef]
- Oria, M.; Raguer, N.; Chatauret, N.; Bartolí, R.; Odena, G.; Planas, R.; Córdoba, J. Functional Abnormalities of the Motor Tract in the Rat after Portocaval Anastomosis and after Carbon Tetrachloride Induction of Cirrhosis. Metab Brain Dis 2006, 21, 297–308. [Google Scholar] [CrossRef]
- Sandford, N.L.; Saul, R.E. Assessment of Hepatic Encephalopathy with Visual Evoked Potentials Compared with Conventional Methods. Hepatology 1988, 8, 1094–1098. [Google Scholar] [CrossRef]
- Saxena, N.; Bhatia, M.; Joshi, Y.K.; Garg, P.K.; Dwivedi, S.N.; Tandon, R.K. Electrophysiological and Neuropsychological Tests for the Diagnosis of Subclinical Hepatic Encephalopathy and Prediction of Overt Encephalopathy. Liver 2002, 22, 190–197. [Google Scholar] [CrossRef]
- Davies, M.G.; Rowan, M.J.; MacMathuna, P.; Keeling, P.W.; Weir, D.G.; Feely, J. The Auditory P300 Event-Related Potential: An Objective Marker of the Encephalopathy of Chronic Liver Disease. Hepatology 1990, 12, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Curran, S.; Wattis, J. Critical Flicker Fusion Threshold: A Potentially Useful Measure for the Early Detection of Alzheimer’s Disease. Hum Psychopharmacol 2000, 15, 103–112. [Google Scholar] [CrossRef]
- Romero-Gómez, M.; Boza, F.; García-Valdecasas, M.S.; García, E.; Aguilar-Reina, J. Subclinical Hepatic Encephalopathy Predicts the Development of Overt Hepatic Encephalopathy. Am J Gastroenterol 2001, 96, 2718–2723. [Google Scholar] [CrossRef] [PubMed]
- Jover, R.; Compañy, L.; Gutiérrez, A.; Lorente, M.; Zapater, P.; Poveda, M.J.; Such, J.; Pascual, S.; Palazón, J.M.; Carnicer, F.; et al. Clinical Significance of Extrapyramidal Signs in Patients with Cirrhosis. J Hepatol 2005, 42, 659–665. [Google Scholar] [CrossRef]
- Kumral, D.; Qayyum, R.; Roseff, S.; Sterling, R.K.; Siddiqui, M.S. Adherence to Recommended Inpatient Hepatic Encephalopathy Workup. J Hosp Med 2019, 14, 157–160. [Google Scholar] [CrossRef]
- Cauli, O.; Rodrigo, R.; Llansola, M.; Montoliu, C.; Monfort, P.; Piedrafita, B.; El Mlili, N.; Boix, J.; Agustí, A.; Felipo, V. Glutamatergic and Gabaergic Neurotransmission and Neuronal Circuits in Hepatic Encephalopathy. Metab Brain Dis 2009, 24, 69–80. [Google Scholar] [CrossRef]
- Awad, E.A.; Mohammed, M.N.; Sayyed, M.M.; El-Khayal, A.E.-S.; Ahmed, M.A.S. 3-Nitro-Tyrosine as a Biomarker of Minimal Hepatic Encephalopathy in Patients with Liver Cirrhosis. The Egyptian Journal of Hospital Medicine 2018, 72, 5647+. [Google Scholar] [CrossRef]
- Genesca, J.; Gonzalez, A.; Segura, R.; Catalan, R.; Marti, R.; Varela, E.; Cadelina, G.; Martinez, M.; Lopez-Talavera, J.C.; Esteban, R.; et al. Interleukin-6, Nitric Oxide, and the Clinical and Hemodynamic Alterations of Patients with Liver Cirrhosis. Am J Gastroenterol 1999, 94, 169–177. [Google Scholar] [CrossRef]
- Strauss, G.I.; Christiansen, M.; Møller, K.; Clemmesen, J.O.; Larsen, F.S.; Knudsen, G.M. S-100b and Neuron-Specific Enolase in Patients with Fulminant Hepatic Failure. Liver Transpl 2001, 7, 964–970. [Google Scholar] [CrossRef]
- Vaquero, J.; Jordano, Q.; Lee, W.M.; Blei, A.T. Serum Protein S-100b in Acute Liver Failure: Results of the US Acute Liver Failure Study Group. Liver Transpl 2003, 9, 887–888. [Google Scholar] [CrossRef]
- Isobe-Harima, Y.; Terai, S.; Segawa, M.; Uchida, K.; Yamasaki, T.; Sakaida, I. Serum S100b (Astrocyte-Specific Protein) Is a Useful Marker of Hepatic Encephalopathy in Patients with Fulminant Hepatitis. Liver Int 2008, 28, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Rojo, A.; Ruiz-Margáin, A.; Macias-Rodriguez, R.U.; Cubero, F.J.; Estradas-Trujillo, J.; Muñoz-Fuentes, R.M.; Torre, A. Clinical Scenarios for the Use of S100β as a Marker of Hepatic Encephalopathy. World J Gastroenterol 2016, 22, 4397–4402. [Google Scholar] [CrossRef] [PubMed]
- Wiltfang, J.; Nolte, W.; Otto, M.; Wildberg, J.; Bahn, E.; Figulla, H.R.; Pralle, L.; Hartmann, H.; Rüther, E.; Ramadori, G. Elevated Serum Levels of Astroglial S100beta in Patients with Liver Cirrhosis Indicate Early and Subclinical Portal-Systemic Encephalopathy. Metab Brain Dis 1999, 14, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Guevara, M.; Baccaro, M.E.; Torre, A.; Gómez-Ansón, B.; Ríos, J.; Torres, F.; Rami, L.; Monté-Rubio, G.C.; Martín-Llahí, M.; Arroyo, V.; et al. Hyponatremia Is a Risk Factor of Hepatic Encephalopathy in Patients with Cirrhosis: A Prospective Study with Time-Dependent Analysis. Am J Gastroenterol 2009, 104, 1382–1389. [Google Scholar] [CrossRef]
- Jepsen, P.; Watson, H.; Andersen, P.K.; Vilstrup, H. Diabetes as a Risk Factor for Hepatic Encephalopathy in Cirrhosis Patients. J Hepatol 2015, 63, 1133–1138. [Google Scholar] [CrossRef]
- Poudyal, N.S.; Chaudhary, S.; Kc, S.; Paudel, B.N.; Basnet, B.K.; Mandal, A.; Kafle, P.; Chaulagai, B.; Mojahedi, A.; Paudel, M.S.; et al. Precipitating Factors and Treatment Outcomes of Hepatic Encephalopathy in Liver Cirrhosis. Cureus 2019, 11, e4363. [Google Scholar] [CrossRef]
- Marie, M.S.; Shousha, H.I.; Abdelrazek, W.; Hassany, M.; Dabees, H.; Abdelghafour, R.; Aboganob, W. mosaad; Said, M. Prediction of Hepatic Decompensation and Hepatocellular Carcinoma after Direct-Acting Antiviral Therapy in Patients with Hepatitis C-Related Liver Cirrhosis: A Cohort Study. Egyptian Liver Journal 2023, 13, 12. [Google Scholar] [CrossRef]
- Praktiknjo, M.; Simón-Talero, M.; Römer, J.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Llop, E.; Maurer, M.H.; et al. Total Area of Spontaneous Portosystemic Shunts Independently Predicts Hepatic Encephalopathy and Mortality in Liver Cirrhosis. J Hepatol 2020, 72, 1140–1150. [Google Scholar] [CrossRef]
- Gil-Gómez, A.; Ampuero, J.; Rojas, Á.; Gallego-Durán, R.; Muñoz-Hernández, R.; Rico, M.C.; Millán, R.; García-Lozano, R.; Francés, R.; Soriano, G.; et al. Development and Validation of a Clinical-Genetic Risk Score to Predict Hepatic Encephalopathy in Patients With Liver Cirrhosis. Am J Gastroenterol 2021, 116, 1238–1247. [Google Scholar] [CrossRef]
- Qi, X.; Tian, Y.; Zhang, W.; Yang, Z.; Guo, X. Covered versus Bare Stents for Transjugular Intrahepatic Portosystemic Shunt: An Updated Meta-Analysis of Randomized Controlled Trials. Therap Adv Gastroenterol 2017, 10, 32–41. [Google Scholar] [CrossRef]
- Montagnese, S.; Balistreri, E.; Schiff, S.; De Rui, M.; Angeli, P.; Zanus, G.; Cillo, U.; Bombonato, G.; Bolognesi, M.; Sacerdoti, D.; et al. Covert Hepatic Encephalopathy: Agreement and Predictive Validity of Different Indices. World J Gastroenterol 2014, 20, 15756–15762. [Google Scholar] [CrossRef] [PubMed]
- Pisarek, W. Minimal Hepatic Encephalopathy - Diagnosis and Treatment. Prz Gastroenterol 2021, 16, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Etemadian, A.; Hafeezullah, M.; Saeian, K. Testing for Minimal Hepatic Encephalopathy in the United States: An AASLD Survey. Hepatology 2007, 45, 833–834. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.F.; Amodio, P.; Bajaj, J.S.; Dhiman, R.K.; Montagnese, S.; Taylor-Robinson, S.D.; Vilstrup, H.; Jalan, R. Hepatic Encephalopathy: Novel Insights into Classification, Pathophysiology and Therapy. J Hepatol 2020, 73, 1526–1547. [Google Scholar] [CrossRef]
- Patidar, K.R.; Bajaj, J.S. Covert and Overt Hepatic Encephalopathy: Diagnosis and Management. Clin Gastroenterol Hepatol 2015, 13, 2048–2061. [Google Scholar] [CrossRef]
- Bass, N.M. Review Article: The Current Pharmacological Therapies for Hepatic Encephalopathy. Aliment Pharmacol Ther 2007, 25 Suppl 1, 23–31. [Google Scholar] [CrossRef]
- Morgan, M.Y.; Alonso, M.; Stanger, L.C. Lactitol and Lactulose for the Treatment of Subclinical Hepatic Encephalopathy in Cirrhotic Patients. A Randomised, Cross-over Study. J Hepatol 1989, 8, 208–217. [Google Scholar] [CrossRef]
- Horsmans, Y.; Solbreux, P.M.; Daenens, C.; Desager, J.P.; Geubel, A.P. Lactulose Improves Psychometric Testing in Cirrhotic Patients with Subclinical Encephalopathy. Aliment Pharmacol Ther 1997, 11, 165–170. [Google Scholar] [CrossRef]
- Watanabe, A.; Sakai, T.; Sato, S.; Imai, F.; Ohto, M.; Arakawa, Y.; Toda, G.; Kobayashi, K.; Muto, Y.; Tsujii, T.; et al. Clinical Efficacy of Lactulose in Cirrhotic Patients with and without Subclinical Hepatic Encephalopathy. Hepatology 1997, 26, 1410–1414. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Sawhney, M.S.; Chawla, Y.K.; Das, G.; Ram, S.; Dilawari, J.B. Efficacy of Lactulose in Cirrhotic Patients with Subclinical Hepatic Encephalopathy. Dig Dis Sci 2000, 45, 1549–1552. [Google Scholar] [CrossRef]
- Prasad, S.; Dhiman, R.K.; Duseja, A.; Chawla, Y.K.; Sharma, A.; Agarwal, R. Lactulose Improves Cognitive Functions and Health-Related Quality of Life in Patients with Cirrhosis Who Have Minimal Hepatic Encephalopathy. Hepatology 2007, 45, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Gillevet, P.M.; Patel, N.R.; Ahluwalia, V.; Ridlon, J.M.; Kettenmann, B.; Schubert, C.M.; Sikaroodi, M.; Heuman, D.M.; Crossey, M.M.E.; et al. A Longitudinal Systems Biology Analysis of Lactulose Withdrawal in Hepatic Encephalopathy. Metab Brain Dis 2012, 27, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Sharma, B.C.; Agrawal, A.; Sarin, S.K. Primary Prophylaxis of Overt Hepatic Encephalopathy in Patients with Cirrhosis: An Open Labeled Randomized Controlled Trial of Lactulose versus No Lactulose. J Gastroenterol Hepatol 2012, 27, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Ziada, D.H.; Soliman, H.H.; El Yamany, S.A.; Hamisa, M.F.; Hasan, A.M. Can Lactobacillus Acidophilus Improve Minimal Hepatic Encephalopathy? A Neurometabolite Study Using Magnetic Resonance Spectroscopy. Arab J Gastroenterol 2013, 14, 116–122. [Google Scholar] [CrossRef]
- Pratap Mouli, V.; Benjamin, J.; Bhushan Singh, M.; Mani, K.; Garg, S.K.; Saraya, A.; Joshi, Y.K. Effect of Probiotic VSL#3 in the Treatment of Minimal Hepatic Encephalopathy: A Non-Inferiority Randomized Controlled Trial. Hepatol Res 2015, 45, 880–889. [Google Scholar] [CrossRef]
- Sidhu, S.S.; Goyal, O.; Parker, R.A.; Kishore, H.; Sood, A. Rifaximin vs. Lactulose in Treatment of Minimal Hepatic Encephalopathy. Liver Int 2016, 36, 378–385. [Google Scholar] [CrossRef]
- Wang, J.Y.; Bajaj, J.S.; Wang, J.B.; Shang, J.; Zhou, X.M.; Guo, X.L.; Zhu, X.; Meng, L.N.; Jiang, H.X.; Mi, Y.Q.; et al. Lactulose Improves Cognition, Quality of Life, and Gut Microbiota in Minimal Hepatic Encephalopathy: A Multicenter, Randomized Controlled Trial. J Dig Dis 2019, 20, 547–556. [Google Scholar] [CrossRef]
- Wang, M.-W.; Ma, W.-J.; Wang, Y.; Ma, X.-H.; Xue, Y.-F.; Guan, J.; Chen, X. Comparison of the Effects of Probiotics, Rifaximin, and Lactulose in the Treatment of Minimal Hepatic Encephalopathy and Gut Microbiota. Front Microbiol 2023, 14, 1091167. [Google Scholar] [CrossRef]
- Sidhu, S.S.; Goyal, O.; Mishra, B.P.; Sood, A.; Chhina, R.S.; Soni, R.K. Rifaximin Improves Psychometric Performance and Health-Related Quality of Life in Patients with Minimal Hepatic Encephalopathy (the RIME Trial). Am J Gastroenterol 2011, 106, 307–316. [Google Scholar] [CrossRef]
- Ballester, M.-P.; Gallego, J.-J.; Fiorillo, A.; Casanova-Ferrer, F.; Giménez-Garzó, C.; Escudero-García, D.; Tosca, J.; Ríos, M.-P.; Montón, C.; Durbán, L.; et al. Metabolic Syndrome Is Associated with Poor Response to Rifaximin in Minimal Hepatic Encephalopathy. Sci Rep 2022, 12, 2463. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Sanyal, A.J.; Hylemon, P.B.; Sterling, R.K.; Stravitz, R.T.; Fuchs, M.; Ridlon, J.M.; Daita, K.; Monteith, P.; et al. Modulation of the Metabiome by Rifaximin in Patients with Cirrhosis and Minimal Hepatic Encephalopathy. PLoS One 2013, 8, e60042. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, V.; Wade, J.B.; Heuman, D.M.; Hammeke, T.A.; Sanyal, A.J.; Sterling, R.K.; Stravitz, R.T.; Luketic, V.; Siddiqui, M.S.; Puri, P.; et al. Enhancement of Functional Connectivity, Working Memory and Inhibitory Control on Multi-Modal Brain MR Imaging with Rifaximin in Cirrhosis: Implications for the Gut-Liver-Brain Axis. Metab Brain Dis 2014, 29, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Feng, Y.; Cao, B.; Tian, Q. Effects of SIBO and Rifaximin Therapy on MHE Caused by Hepatic Cirrhosis. Int J Clin Exp Med 2015, 8, 2954–2957. [Google Scholar] [PubMed]
- Goyal, O.; Sidhu, S.S.; Kishore, H. Minimal Hepatic Encephalopathy in Cirrhosis- How Long to Treat? Ann Hepatol 2017, 16, 115–122. [Google Scholar] [CrossRef]
- Bakulin, I.G.; Ivanova, K.N.; Eremina, E.Y.; Marchenko, N.V. Comparative Analysis of the Efficacy of Different Regimens of 12 Months Rifaximin-Alfa Therapy in Patients with Liver Cirrhosis and Minimal Hepatic Encephalopathy. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef]
- Fiorillo, A.; Gallego, J.J.; Casanova-Ferrer, F.; Urios, A.; Ballester, M.-P.; San Miguel, T.; Megías, J.; Kosenko, E.; Tosca, J.; Rios, M.-P.; et al. Neurofilament Light Chain Protein in Plasma and Extracellular Vesicles Is Associated with Minimal Hepatic Encephalopathy and Responses to Rifaximin Treatment in Cirrhotic Patients. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Casanova-Ferrer, F.; Gallego, J.-J.; Fiorillo, A.; Urios, A.; Ríos, M.-P.; León, J.L.; Ballester, M.-P.; Escudero-García, D.; Kosenko, E.; Belloch, V.; et al. Improved Cognition after Rifaximin Treatment Is Associated with Changes in Intra- and Inter-Brain Network Functional Connectivity. J Transl Med 2024, 22, 49. [Google Scholar] [CrossRef]
- Egberts, E.H.; Schomerus, H.; Hamster, W.; Jürgens, P. Branched Chain Amino Acids in the Treatment of Latent Portosystemic Encephalopathy. A Double-Blind Placebo-Controlled Crossover Study. Gastroenterology 1985, 88, 887–895. [Google Scholar] [CrossRef]
- Plauth, M.; Egberts, E.H.; Hamster, W.; Török, M.; Müller, P.H.; Brand, O.; Fürst, P.; Dölle, W. Long-Term Treatment of Latent Portosystemic Encephalopathy with Branched-Chain Amino Acids. A Double-Blind Placebo-Controlled Crossover Study. J Hepatol 1993, 17, 308–314. [Google Scholar] [CrossRef]
- Marchesini, G.; Bianchi, G.; Merli, M.; Amodio, P.; Panella, C.; Loguercio, C.; Rossi Fanelli, F.; Abbiati, R. Nutritional Supplementation with Branched-Chain Amino Acids in Advanced Cirrhosis: A Double-Blind, Randomized Trial. Gastroenterology 2003, 124, 1792–1801. [Google Scholar] [CrossRef]
- Les, I.; Doval, E.; García-Martínez, R.; Planas, M.; Cárdenas, G.; Gómez, P.; Flavià, M.; Jacas, C.; Mínguez, B.; Vergara, M.; et al. Effects of Branched-Chain Amino Acids Supplementation in Patients with Cirrhosis and a Previous Episode of Hepatic Encephalopathy: A Randomized Study. Am J Gastroenterol 2011, 106, 1081–1088. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Greco, F.; Barone, G.; Gargante, M.P.; Malaguarnera, M.; Toscano, M.A. Bifidobacterium Longum with Fructo-Oligosaccharide (FOS) Treatment in Minimal Hepatic Encephalopathy: A Randomized, Double-Blind, Placebo-Controlled Study. Dig Dis Sci 2007, 52, 3259–3265. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Saeian, K.; Christensen, K.M.; Hafeezullah, M.; Varma, R.R.; Franco, J.; Pleuss, J.A.; Krakower, G.; Hoffmann, R.G.; Binion, D.G. Probiotic Yogurt for the Treatment of Minimal Hepatic Encephalopathy. Am J Gastroenterol 2008, 103, 1707–1715. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Sharma, B.C.; Puri, V.; Sarin, S.K. An Open-Label Randomized Controlled Trial of Lactulose and Probiotics in the Treatment of Minimal Hepatic Encephalopathy. Eur J Gastroenterol Hepatol 2008, 20, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.V.; Sharma, B.C.; Sharma, P.; Sarin, S.K. A Randomized Controlled Trial Comparing Lactulose, Probiotics, and L-Ornithine L-Aspartate in Treatment of Minimal Hepatic Encephalopathy. Eur J Gastroenterol Hepatol 2011, 23, 725–732. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; Puri, P.; Sterling, R.K.; Luketic, V.; Stravitz, R.T.; Siddiqui, M.S.; Fuchs, M.; et al. Randomised Clinical Trial: Lactobacillus GG Modulates Gut Microbiome, Metabolome and Endotoxemia in Patients with Cirrhosis. Aliment Pharmacol Ther 2014, 39, 1113–1125. [Google Scholar] [CrossRef]
- Lunia, M.K.; Sharma, B.C.; Sharma, P.; Sachdeva, S.; Srivastava, S. Probiotics Prevent Hepatic Encephalopathy in Patients with Cirrhosis: A Randomized Controlled Trial. Clin Gastroenterol Hepatol 2014, 12, 1003–1008.e1. [Google Scholar] [CrossRef]
- Sharma, K.; Pant, S.; Misra, S.; Dwivedi, M.; Misra, A.; Narang, S.; Tewari, R.; Bhadoria, A.S. Effect of Rifaximin, Probiotics, and l-Ornithine l-Aspartate on Minimal Hepatic Encephalopathy: A Randomized Controlled Trial. Saudi J Gastroenterol 2014, 20, 225–232. [Google Scholar] [CrossRef]
- Xia, X.; Chen, J.; Xia, J.; Wang, B.; Liu, H.; Yang, L.; Wang, Y.; Ling, Z. Role of Probiotics in the Treatment of Minimal Hepatic Encephalopathy in Patients with HBV-Induced Liver Cirrhosis. J Int Med Res 2018, 46, 3596–3604. [Google Scholar] [CrossRef]
- Ndraha, S.; Hasan, I.; Simadibrata, M. The Effect of L-Ornithine L-Aspartate and Branch Chain Amino Acids on Encephalopathy and Nutritional Status in Liver Cirrhosis with Malnutrition. Acta Med Indones 2011, 43, 18–22. [Google Scholar]
- Kato, A.; Tanaka, H.; Kawaguchi, T.; Kanazawa, H.; Iwasa, M.; Sakaida, I.; Moriwaki, H.; Murawaki, Y.; Suzuki, K.; Okita, K. Nutritional Management Contributes to Improvement in Minimal Hepatic Encephalopathy and Quality of Life in Patients with Liver Cirrhosis: A Preliminary, Prospective, Open-Label Study. Hepatol Res 2013, 43, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Rai, R.; Ahuja, C.K.; Agrawal, S.; Kalra, N.; Duseja, A.; Khandelwal, N.; Chawla, Y.; Dhiman, R.K. Reversal of Low-Grade Cerebral Edema After Lactulose/Rifaximin Therapy in Patients with Cirrhosis and Minimal Hepatic Encephalopathy. Clin Transl Gastroenterol 2015, 6, e111. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Li, F. Clinical Study of Probiotics Combined with Lactulose for Minimal Hepatic Encephalopathy Treatment. Eur J Gastroenterol Hepatol 2023, 35, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, M.; Gargante, M.P.; Cristaldi, E.; Vacante, M.; Risino, C.; Cammalleri, L.; Pennisi, G.; Rampello, L. Acetyl-L-Carnitine Treatment in Minimal Hepatic Encephalopathy. Dig Dis Sci 2008, 53, 3018–3025. [Google Scholar] [CrossRef]
- Agrawal, A.; Gupta, A.; Chandra, M.; Koowar, S. Role of Helicobacter Pylori Infection in the Pathogenesis of Minimal Hepatic Encephalopathy and Effect of Its Eradication. Indian J Gastroenterol 2011, 30, 29–32. [Google Scholar] [CrossRef]
- Burkard, T.; Biedermann, A.; Herold, C.; Dietlein, M.; Rauch, M.; Diefenbach, M. Treatment with a Potassium-Iron-Phosphate-Citrate Complex Improves PSE Scores and Quality of Life in Patients with Minimal Hepatic Encephalopathy: A Multicenter, Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Eur J Gastroenterol Hepatol 2013, 25, 352–358. [Google Scholar] [CrossRef]
- Janyajirawong, R.; Vilaichone, R.-K.; Sethasine, S. Efficacy of Zinc Supplement in Minimal Hepatic Encephalopathy: A Prospective, Randomized Controlled Study (Zinc-MHE Trial). Asian Pac J Cancer Prev 2021, 22, 2879–2887. [Google Scholar] [CrossRef]
- Sharma, B.C.; Maharshi, S.; Sachdeva, S.; Mahajan, B.; Sharma, A.; Bara, S.; Srivastava, S.; Kumar, A.; Dalal, A.; Sonika, U. Nutritional Therapy for Persistent Cognitive Impairment after Resolution of Overt Hepatic Encephalopathy in Patients with Cirrhosis: A Double-Blind Randomized Controlled Trial. J Gastroenterol Hepatol 2023, 38, 1917–1925. [Google Scholar] [CrossRef]
- Uribe, M.; Campollo, O.; Coté, C. Effect of Lactulose on the Metabolism of Short-Chain Fatty Acids. Hepatology 1990, 12, 1251–1252. [Google Scholar] [CrossRef]
- Uribe, M.; Berthier, J.M.; Lewis, H.; Mata, J.M.; Sierra, J.G.; García-Ramos, G.; Ramírez Acosta, J.; Dehesa, M. Lactose Enemas plus Placebo Tablets vs. Neomycin Tablets plus Starch Enemas in Acute Portal Systemic Encephalopathy. A Double-Blind Randomized Controlled Study. Gastroenterology 1981, 81, 101–106. [Google Scholar] [CrossRef]
- Uribe, M.; Toledo, H.; Perez, F.; Vargas, F.; Gil, S.; Garcia-Ramos, G.; Ravelli, G.P.; Guevara, L. Lactitol, a Second-Generation Disaccharide for Treatment of Chronic Portal-Systemic Encephalopathy. A Double-Blind, Crossover, Randomized Clinical Trial. Dig Dis Sci 1987, 32, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Gluud, L.L.; Vilstrup, H.; Morgan, M.Y. Non-Absorbable Disaccharides versus Placebo/No Intervention and Lactulose versus Lactitol for the Prevention and Treatment of Hepatic Encephalopathy in People with Cirrhosis. Cochrane Database Syst Rev 2016, 4, CD003044. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, R.S.; Singal, A.G.; Cuthbert, J.A.; Rockey, D.C. Lactulose vs Polyethylene Glycol 3350--Electrolyte Solution for Treatment of Overt Hepatic Encephalopathy: The HELP Randomized Clinical Trial. JAMA Intern Med 2014, 174, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Cevallos, P.; Chávez-Tapia, N.C.; Uribe, M. Current Approaches to Hepatic Encephalopathy. Ann Hepatol 2022, 27, 100757. [Google Scholar] [CrossRef]
- Swales, J.D.; Wrong, O.M. Ammonia Production in the Human Colon. N Engl J Med 1971, 284, 216–217. [Google Scholar] [CrossRef]
- Miglio, F.; Valpiani, D.; Rossellini, S.R.; Ferrieri, A. Rifaximin, a Non-Absorbable Rifamycin, for the Treatment of Hepatic Encephalopathy. A Double-Blind, Randomised Trial. Curr Med Res Opin 1997, 13, 593–601. [Google Scholar] [CrossRef]
- Paik, Y.H.; Lee, K.S.; Han, K.H.; Song, K.H.; Kim, M.H.; Moon, B.S.; Ahn, S.H.; Lee, S.J.; Park, H.J.; Lee, D.K.; et al. Comparison of Rifaximin and Lactulose for the Treatment of Hepatic Encephalopathy: A Prospective Randomized Study. Yonsei Med J 2005, 46, 399–407. [Google Scholar] [CrossRef]
- Sharma, B.C.; Sharma, P.; Lunia, M.K.; Srivastava, S.; Goyal, R.; Sarin, S.K. A Randomized, Double-Blind, Controlled Trial Comparing Rifaximin plus Lactulose with Lactulose Alone in Treatment of Overt Hepatic Encephalopathy. Am J Gastroenterol 2013, 108, 1458–1463. [Google Scholar] [CrossRef]
- Eltawil, K.M.; Laryea, M.; Peltekian, K.; Molinari, M. Rifaximin vs. Conventional Oral Therapy for Hepatic Encephalopathy: A Meta-Analysis. World J Gastroenterol 2012, 18, 767–777. [Google Scholar] [CrossRef]
- Poo, J.; Cervera, E.; De Hoyos, A.; Gil, S.; Cadena, M.; Uribe, M. Benzoato de Sodio. Fundamentos Para Su Uso Clinico En Hepatologia. Rev Invest Clin 1990, 42, 101. [Google Scholar]
- Uribe, M.; Bosques, F.; Marín, E.; Cervera, E.; Gil, S.; Luis Poo, J.; Garcia Compeán, D.; Santoyo, R.; Huerta, E.; García-Ramos, G.; et al. [Sodium benzoate in portal-systemic-encephalopathy-induced blood ammonia normalization and clinical improvement. Interim report of a double-blind multicenter trial]. Rev Invest Clin 1990, 42, 149–154. [Google Scholar] [PubMed]
- Rahimi, R.S.; Safadi, R.; Thabut, D.; Bhamidimarri, K.R.; Pyrsopoulos, N.; Potthoff, A.; Bukofzer, S.; Bajaj, J.S. Efficacy and Safety of Ornithine Phenylacetate for Treating Overt Hepatic Encephalopathy in a Randomized Trial. Clin Gastroenterol Hepatol 2021, 19, 2626–2635.e7. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Cots, M.; Arranz, J.A.; Simón-Talero, M.; Torrens, M.; Blanco, A.; Riudor, E.; Fuentes, I.; Suñé, P.; Soriano, G.; Córdoba, J. Safety of Ornithine Phenylacetate in Cirrhotic Decompensated Patients: An Open-Label, Dose-Escalating, Single-Cohort Study. J Clin Gastroenterol 2013, 47, 881–887. [Google Scholar] [CrossRef]
- Poo, J.L.; Góngora, J.; Sánchez-Avila, F.; Aguilar-Castillo, S.; García-Ramos, G.; Fernández-Zertuche, M.; Rodríguez-Fragoso, L.; Uribe, M. Efficacy of Oral L-Ornithine-L-Aspartate in Cirrhotic Patients with Hyperammonemic Hepatic Encephalopathy. Results of a Randomized, Lactulose-Controlled Study. Ann Hepatol 2006, 5, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Goh, E.T.; Stokes, C.S.; Sidhu, S.S.; Vilstrup, H.; Gluud, L.L.; Morgan, M.Y. L-Ornithine L-Aspartate for Prevention and Treatment of Hepatic Encephalopathy in People with Cirrhosis. Cochrane Database Syst Rev 2018, 5, CD012410. [Google Scholar] [CrossRef]
- Sharma, B.C.; Singh, J.; Srivastava, S.; Sangam, A.; Mantri, A.K.; Trehanpati, N.; Sarin, S.K. Randomized Controlled Trial Comparing Lactulose plus Albumin versus Lactulose Alone for Treatment of Hepatic Encephalopathy. J Gastroenterol Hepatol 2017, 32, 1234–1239. [Google Scholar] [CrossRef]
- Rivera-Flores, R.; Morán-Villota, S.; Cervantes-Barragán, L.; López-Macias, C.; Uribe, M. Manipulation of Microbiota with Probiotics as an Alternative for Treatment of Hepatic Encephalopathy. Nutrition 2020, 73, 110693. [Google Scholar] [CrossRef]
- Altamirano-Barrera, A.; Uribe, M.; Chávez-Tapia, N.C.; Nuño-Lámbarri, N. The Role of the Gut Microbiota in the Pathology and Prevention of Liver Disease. J Nutr Biochem 2018, 60, 1–8. [Google Scholar] [CrossRef]
- Dalal, R.; McGee, R.G.; Riordan, S.M.; Webster, A.C. Probiotics for People with Hepatic Encephalopathy. Cochrane Database Syst Rev 2017, 2, CD008716. [Google Scholar] [CrossRef]
- Chávez-Tapia, N.C.; González-Rodríguez, L.; Jeong, M.; López-Ramírez, Y.; Barbero-Becerra, V.; Juárez-Hernández, E.; Romero-Flores, J.L.; Arrese, M.; Méndez-Sánchez, N.; Uribe, M. Current Evidence on the Use of Probiotics in Liver Diseases. Journal of Functional Foods 2015, 17, 137–151. [Google Scholar] [CrossRef]
- Shukla, S.; Shukla, A.; Mehboob, S.; Guha, S. Meta-Analysis: The Effects of Gut Flora Modulation Using Prebiotics, Probiotics and Synbiotics on Minimal Hepatic Encephalopathy. Aliment Pharmacol Ther 2011, 33, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Uribe, M.; Dibildox, M.; Malpica, S.; Guillermo, E.; Villallobos, A.; Nieto, L.; Vargas, F.; Garcia Ramos, G. Beneficial Effect of Vegetable Protein Diet Supplemented with Psyllium Plantago in Patients with Hepatic Encephalopathy and Diabetes Mellitus. Gastroenterology 1985, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The Nutritional Management of Hepatic Encephalopathy in Patients with Cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Laleman, W.; Simon-Talero, M.; Maleux, G.; Perez, M.; Ameloot, K.; Soriano, G.; Villalba, J.; Garcia-Pagan, J.-C.; Barrufet, M.; Jalan, R.; et al. Embolization of Large Spontaneous Portosystemic Shunts for Refractory Hepatic Encephalopathy: A Multicenter Survey on Safety and Efficacy. Hepatology 2013, 57, 2448–2457. [Google Scholar] [CrossRef]
- An, J.; Kim, K.W.; Han, S.; Lee, J.; Lim, Y.-S. Improvement in Survival Associated with Embolisation of Spontaneous Portosystemic Shunt in Patients with Recurrent Hepatic Encephalopathy. Aliment Pharmacol Ther 2014, 39, 1418–1426. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Kassam, Z.; Fagan, A.; Gavis, E.A.; Liu, E.; Cox, I.J.; Kheradman, R.; Heuman, D.; Wang, J.; Gurry, T.; et al. Fecal Microbiota Transplant from a Rational Stool Donor Improves Hepatic Encephalopathy: A Randomized Clinical Trial. Hepatology 2017, 66, 1727–1738. [Google Scholar] [CrossRef]
- Madsen, M.; Kimer, N.; Bendtsen, F.; Petersen, A.M. Fecal Microbiota Transplantation in Hepatic Encephalopathy: A Systematic Review. Scand J Gastroenterol 2021, 56, 560–569. [Google Scholar] [CrossRef]
- Chavez-Tapia, N.C.; Cesar-Arce, A.; Barrientos-Gutiérrez, T.; Villegas-López, F.A.; Méndez-Sanchez, N.; Uribe, M. A Systematic Review and Meta-Analysis of the Use of Oral Zinc in the Treatment of Hepatic Encephalopathy. Nutr J 2013, 12, 74. [Google Scholar] [CrossRef]
- Sharma, B.C.; Sharma, P.; Agrawal, A.; Sarin, S.K. Secondary Prophylaxis of Hepatic Encephalopathy: An Open-Label Randomized Controlled Trial of Lactulose versus Placebo. Gastroenterology 2009, 137, 885–891, 891.e1. [Google Scholar] [CrossRef]
- Sharma, P.; Agrawal, A.; Sharma, B.C.; Sarin, S.K. Prophylaxis of Hepatic Encephalopathy in Acute Variceal Bleed: A Randomized Controlled Trial of Lactulose versus No Lactulose. J Gastroenterol Hepatol 2011, 26, 996–1003. [Google Scholar] [CrossRef]
- Mullen, K.D.; Sanyal, A.J.; Bass, N.M.; Poordad, F.F.; Sheikh, M.Y.; Frederick, R.T.; Bortey, E.; Forbes, W.P. Rifaximin Is Safe and Well Tolerated for Long-Term Maintenance of Remission from Overt Hepatic Encephalopathy. Clin Gastroenterol Hepatol 2014, 12, 1390–1397.e2. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-Term Albumin Administration in Decompensated Cirrhosis (ANSWER): An Open-Label Randomised Trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef] [PubMed]
- Dietemann, J.L.; Reimund, J.M.; Diniz, R.L.; Reis, M.J.; Baumann, R.; Neugroschl, C.; Von Söhsten, S.; Warter, J.M. High Signal in the Adenohypophysis on T1-Weighted Images Presumably Due to Manganese Deposits in Patients on Long-Term Parenteral Nutrition. Neuroradiology 1998, 40, 793–796. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-H.; Hwang, S.; Jung, B.-H.; Park, Y.-H.; Park, C.-S.; Namgoong, J.-M.; Song, G.-W.; Jung, D.-H.; Ahn, C.-S.; Kim, K.-H.; et al. Post-Transplant Assessment of Consciousness in Acute-on-Chronic Liver Failure Patients Undergoing Liver Transplantation Using Bispectral Index Monitoring. Transplant Proc 2013, 45, 3069–3071. [Google Scholar] [CrossRef]
- Hwang, S.; Lee, S.-G.; Park, J.-I.; Song, G.-W.; Ryu, J.-H.; Jung, D.-H.; Hwang, G.-S.; Jeong, S.-M.; Song, J.-G.; Hong, S.-K.; et al. Continuous Peritransplant Assessment of Consciousness Using Bispectral Index Monitoring for Patients with Fulminant Hepatic Failure Undergoing Urgent Liver Transplantation. Clin Transplant 2010, 24, 91–97. [Google Scholar] [CrossRef]
- Kim, K.M.; Kim, G.S.; Ko, J.S.; Gwak, M.S.; Lee, S.-K.; Son, M.G. Factors Associated with Consciousness Recovery Time after Liver Transplantation in Recipients with Hepatic Encephalopathy. Transplant Proc 2014, 46, 712–715. [Google Scholar] [CrossRef]
- Kao, T.-L.; Wang, C.-C. Conscious Recovery Response in Post-Hepatic Transplant as a Function of Time-Related Acute Hepatic Encephalopathy. Transplant Proc 2012, 44, 421–423. [Google Scholar] [CrossRef]
- Sotil, E.U.; Gottstein, J.; Ayala, E.; Randolph, C.; Blei, A.T. Impact of Preoperative Overt Hepatic Encephalopathy on Neurocognitive Function after Liver Transplantation. Liver Transpl 2009, 15, 184–192. [Google Scholar] [CrossRef]
- Dhar, R.; Young, G.B.; Marotta, P. Perioperative Neurological Complications after Liver Transplantation Are Best Predicted by Pre-Transplant Hepatic Encephalopathy. Neurocrit Care 2008, 8, 253–258. [Google Scholar] [CrossRef]
- Herrero, J.I.; Bilbao, J.I.; Diaz, M.L.; Alegre, F.; Inarrairaegui, M.; Pardo, F.; Quiroga, J. Hepatic Encephalopathy after Liver Transplantation in a Patient with a Normally Functioning Graft: Treatment with Embolization of Portosystemic Collaterals. Liver Transpl 2009, 15, 111–114. [Google Scholar] [CrossRef]
- Saritaş, S.; Tarlaci, S.; Bulbuloglu, S.; Guneş, H. Investigation of Post-Transplant Mental Well-Being in Liver Transplant Recipients with Hepatic Encephalopathy. J Clin Med 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Umapathy, S.; Dhiman, R.K. Minimal Hepatic Encephalopathy Impairs Quality of Life. J Clin Exp Hepatol 2015, 5, S42–48. [Google Scholar] [CrossRef] [PubMed]
- Zeegen, R.; Drinkwater, J.E.; Dawson, A.M. Method for Measuring Cerebral Dysfunction in Patients with Liver Disease. Br Med J 1970, 2, 633–636. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines on the Management of Hepatic Encephalopathy. J Hepatol 2022, 77, 807–824. [CrossRef] [PubMed]
- Das, A.; Dhiman, R.K.; Saraswat, V.A.; Verma, M.; Naik, S.R. Prevalence and Natural History of Subclinical Hepatic Encephalopathy in Cirrhosis. J Gastroenterol Hepatol 2001, 16, 531–535. [Google Scholar] [CrossRef]
- Marchesini, G.; Bianchi, G.; Amodio, P.; Salerno, F.; Merli, M.; Panella, C.; Loguercio, C.; Apolone, G.; Niero, M.; Abbiati, R. Factors Associated with Poor Health-Related Quality of Life of Patients with Cirrhosis. Gastroenterology 2001, 120, 170–178. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Boparai, N.; Price, L.L.; Kiwi, M.L.; McCormick, M.; Guyatt, G. Health-Related Quality of Life in Chronic Liver Disease: The Impact of Type and Severity of Disease. Am J Gastroenterol 2001, 96, 2199–2205. [Google Scholar] [CrossRef]
- Labenz, C.; Baron, J.S.; Toenges, G.; Schattenberg, J.M.; Nagel, M.; Sprinzl, M.F.; Nguyen-Tat, M.; Zimmermann, T.; Huber, Y.; Marquardt, J.U.; et al. Prospective Evaluation of the Impact of Covert Hepatic Encephalopathy on Quality of Life and Sleep in Cirrhotic Patients. Aliment Pharmacol Ther 2018, 48, 313–321. [Google Scholar] [CrossRef]
- Nardelli, S.; Pentassuglio, I.; Pasquale, C.; Ridola, L.; Moscucci, F.; Merli, M.; Mina, C.; Marianetti, M.; Fratino, M.; Izzo, C.; et al. Depression, Anxiety and Alexithymia Symptoms Are Major Determinants of Health Related Quality of Life (HRQoL) in Cirrhotic Patients. Metab Brain Dis 2013, 28, 239–243. [Google Scholar] [CrossRef]
- Schomerus, H.; Hamster, W. Quality of Life in Cirrhotics with Minimal Hepatic Encephalopathy. Metab Brain Dis 2001, 16, 37–41. [Google Scholar] [CrossRef]
- Arguedas, M.R.; DeLawrence, T.G.; McGuire, B.M. Influence of Hepatic Encephalopathy on Health-Related Quality of Life in Patients with Cirrhosis. Dig Dis Sci 2003, 48, 1622–1626. [Google Scholar] [CrossRef] [PubMed]
- Samanta, J.; Dhiman, R.K.; Khatri, A.; Thumburu, K.K.; Grover, S.; Duseja, A.; Chawla, Y. Correlation between Degree and Quality of Sleep Disturbance and the Level of Neuropsychiatric Impairment in Patients with Liver Cirrhosis. Metab Brain Dis 2013, 28, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Marjot, T.; Ray, D.W.; Williams, F.R.; Tomlinson, J.W.; Armstrong, M.J. Sleep and Liver Disease: A Bidirectional Relationship. Lancet Gastroenterol Hepatol 2021, 6, 850–863. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O.; Ridola, L. Minimal Hepatic Encephalopathy Affects Daily Life of Cirrhotic Patients: A Viewpoint on Clinical Consequences and Therapeutic Opportunities. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Román, E.; Córdoba, J.; Torrens, M.; Guarner, C.; Soriano, G. Falls and Cognitive Dysfunction Impair Health-Related Quality of Life in Patients with Cirrhosis. Eur J Gastroenterol Hepatol 2013, 25, 77–84. [Google Scholar] [CrossRef]
- Urios, A.; Mangas-Losada, A.; Gimenez-Garzó, C.; González-López, O.; Giner-Durán, R.; Serra, M.A.; Noe, E.; Felipo, V.; Montoliu, C. Altered Postural Control and Stability in Cirrhotic Patients with Minimal Hepatic Encephalopathy Correlate with Cognitive Deficits. Liver Int 2017, 37, 1013–1022. [Google Scholar] [CrossRef]
- Joebges, E.M.; Heidemann, M.; Schimke, N.; Hecker, H.; Ennen, J.C.; Weissenborn, K. Bradykinesia in Minimal Hepatic Encephalopathy Is Due to Disturbances in Movement Initiation. J Hepatol 2003, 38, 273–280. [Google Scholar] [CrossRef]
- Riggio, O.; Amodio, P.; Farcomeni, A.; Merli, M.; Nardelli, S.; Pasquale, C.; Pentassuglio, I.; Gioia, S.; Onori, E.; Piazza, N.; et al. A Model for Predicting Development of Overt Hepatic Encephalopathy in Patients With Cirrhosis. Clin Gastroenterol Hepatol 2015, 13, 1346–1352. [Google Scholar] [CrossRef]
- Hartmann, I.J.; Groeneweg, M.; Quero, J.C.; Beijeman, S.J.; de Man, R.A.; Hop, W.C.; Schalm, S.W. The Prognostic Significance of Subclinical Hepatic Encephalopathy. Am J Gastroenterol 2000, 95, 2029–2034. [Google Scholar] [CrossRef]
- Montagnese, S.; Russo, F.P.; Amodio, P.; Burra, P.; Gasbarrini, A.; Loguercio, C.; Marchesini, G.; Merli, M.; Ponziani, F.R.; Riggio, O.; et al. Hepatic Encephalopathy 2018: A Clinical Practice Guideline by the Italian Association for the Study of the Liver (AISF). Dig Liver Dis 2019, 51, 190–205. [Google Scholar] [CrossRef]
- Thomsen, K.L.; Macnaughtan, J.; Tritto, G.; Mookerjee, R.P.; Jalan, R. Clinical and Pathophysiological Characteristics of Cirrhotic Patients with Grade 1 and Minimal Hepatic Encephalopathy. PLoS One 2016, 11, e0146076. [Google Scholar] [CrossRef] [PubMed]
- Kircheis, G.; Knoche, A.; Hilger, N.; Manhart, F.; Schnitzler, A.; Schulze, H.; Häussinger, D. Hepatic Encephalopathy and Fitness to Drive. Gastroenterology 2009, 137, 1706–1715.e1-9. [Google Scholar] [CrossRef] [PubMed]
- Strebel, H.; Haller, B.; Sohn, M.; Schepp, W.; Gundling, F. Role of Brain Biomarkers S-100-Beta and Neuron-Specific Enolase for Detection and Follow-Up of Hepatic Encephalopathy in Cirrhosis before, during and after Treatment with L-Ornithine-L-Aspartate. GE Port J Gastroenterol 2020, 27, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Nagel, M.; Kämper, P.; Engel, S.; Bittner, S.; Kaps, L.; Galle, P.R.; Schattenberg, J.M.; Wörns, M.-A.; Lüssi, F. Association Between Serum Levels of Neurofilament Light Chains and Minimal Hepatic Encephalopathy in Patients With Liver Cirrhosis. Clin Transl Gastroenterol 2021, 12, e00419. [Google Scholar] [CrossRef]
- Awad, E.A.; Mohammed, M.N.; Sayyed, M.M.; Elkhayal, A.E.; Ahmed, M.A.S. 3-Nitro-Tyrosine as a Biomarker of Minimal Hepatic Encephalopathy in Patients with Liver Cirrhosis. QJM: An International Journal of Medicine 2020, 113, hcaa052.027. [Google Scholar] [CrossRef]
- Stawicka, A.; Świderska, M.; Zbrzeźniak, J.; Sołowianowicz, N.; Woszczenko, A.; Flisiak, R.; Jaroszewicz, J. Brain-Derived Neurotrophic Factor as a Potential Diagnostic Marker in Minimal Hepatic Encephalopathy. Clin Exp Hepatol 2021, 7, 117–124. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, L.; Shang, Y.; Huang, Y.; Ju, C.; Zheng, H.; Zhao, W.; Liu, J. Identifying Minimal Hepatic Encephalopathy: A New Perspective from Magnetic Resonance Imaging. J Magn Reson Imaging 2023. [Google Scholar] [CrossRef]
- Luo, M.; Hu, F.-R.; Xin, R.-J.; Yao, L.; Hu, S.-J.; Bai, F.-H. Altered Gut Microbiota Is Associated with Sleep Disturbances in Patients with Minimal Hepatic Encephalopathy Caused by Hepatitis B-Related Liver Cirrhosis. Expert Rev Gastroenterol Hepatol 2022, 16, 797–807. [Google Scholar] [CrossRef]
- Gairing, S.J.; Anders, J.; Kaps, L.; Nagel, M.; Michel, M.; Kremer, W.M.; Hilscher, M.; Galle, P.R.; Schattenberg, J.M.; Wörns, M.-A.; et al. Evaluation of IL-6 for Stepwise Diagnosis of Minimal Hepatic Encephalopathy in Patients With Liver Cirrhosis. Hepatol Commun 2022, 6, 1113–1122. [Google Scholar] [CrossRef]
- Cheng, Y.; Zhang, G.; Zhang, X.; Li, Y.; Li, J.; Zhou, J.; Huang, L.; Xie, S.; Shen, W. Identification of Minimal Hepatic Encephalopathy Based on Dynamic Functional Connectivity. Brain Imaging Behav 2021, 15, 2637–2645. [Google Scholar] [CrossRef]
- Calvo Córdoba, A.; García Cena, C.E.; Montoliu, C. Automatic Video-Oculography System for Detection of Minimal Hepatic Encephalopathy Using Machine Learning Tools. Sensors (Basel) 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, H.D.; Kamel, F.; Tan, J.; Kimer, N.; Gluud, L.L.; Morgan, M.Y. Rifaximin for Prevention and Treatment of Hepatic Encephalopathy in People with Cirrhosis. Cochrane Database Syst Rev 2023, 7, CD011585. [Google Scholar] [CrossRef] [PubMed]
- Liang, A.; Brar, S.; Almaghrabi, M.; Khan, M.Q.; Qumosani, K.; Teriaky, A. Primary Prevention of Hepatic Encephalopathy Post-TIPS: A Systematic Review and Meta-Analysis. Medicine (Baltimore) 2023, 102, e35266. [Google Scholar] [CrossRef] [PubMed]
- Wibawa, I.D.N.; Mariadi, I.K.; Shalim, C.P.; Sindhughosa, D.A. Efficacy of Probiotics in the Treatment of Minimal Hepatic Encephalopathy: A Systematic Review and Meta-Analysis. Clin Exp Hepatol 2023, 9, 146–153. [Google Scholar] [CrossRef]
- Rosenstengle, C.; Kripalani, S.; Rahimi, R.S. Hepatic Encephalopathy and Strategies to Prevent Readmission from Inadequate Transitions of Care. J Hosp Med 2022, 17 Suppl 1, S17–S23. [Google Scholar] [CrossRef]
Figure 1.
Grades of hepatic encephalopathy (HE). These grades started with MHE, in which there are psychometric or neuropsychological alterations of tests without evidence of any mental changes, and ended with coma.
Figure 1.
Grades of hepatic encephalopathy (HE). These grades started with MHE, in which there are psychometric or neuropsychological alterations of tests without evidence of any mental changes, and ended with coma.
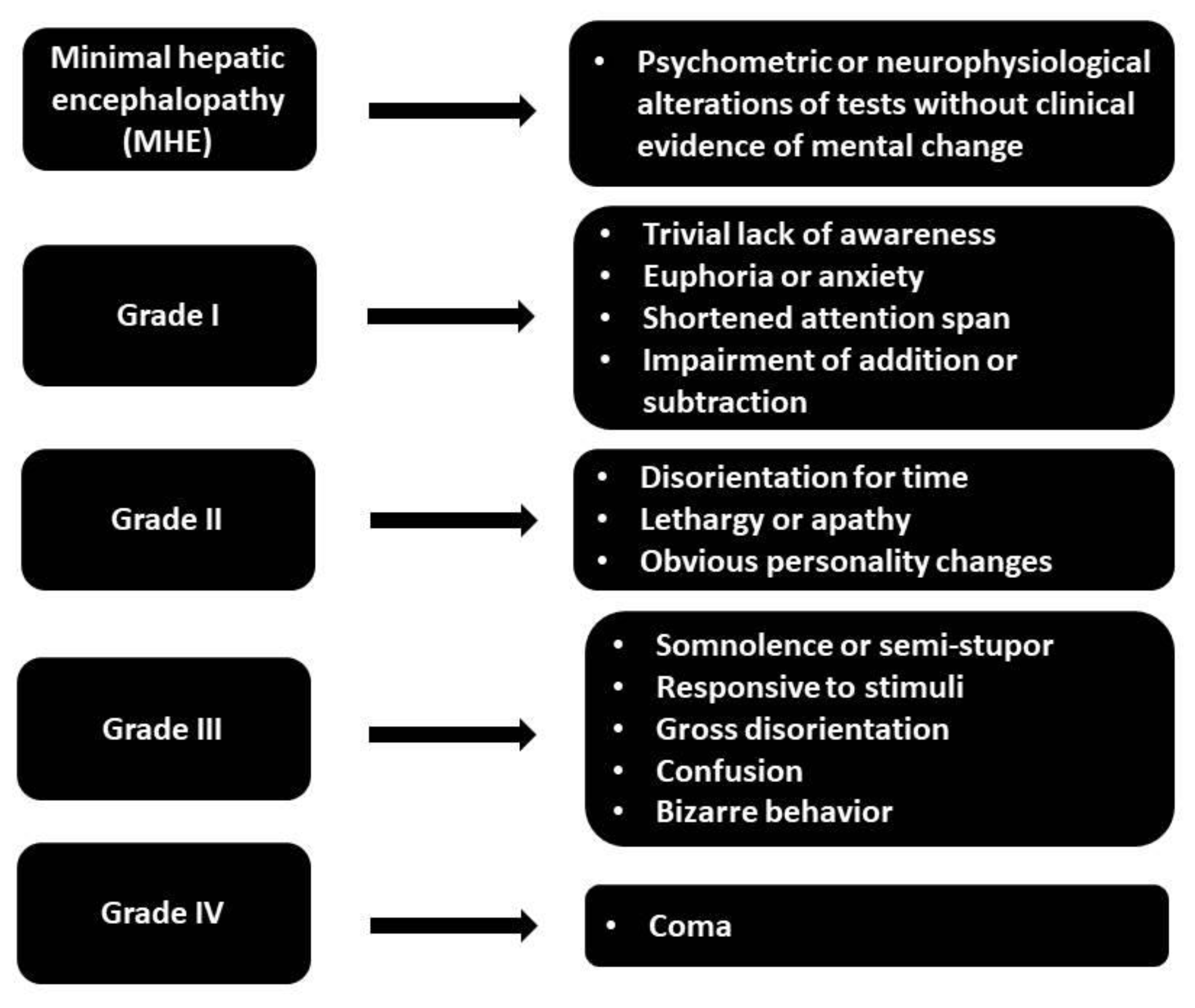
Figure 2.
Role of ammonia in the pathophysiology of hepatic encephalopathy (HE). Ammonia plays a central role in the pathophysiology of HE. Its accumulation due to liver dysfunction leads to a cascade of events in the brain, ultimately resulting in the neuropsychiatric symptoms characteristic of HE.
Figure 2.
Role of ammonia in the pathophysiology of hepatic encephalopathy (HE). Ammonia plays a central role in the pathophysiology of HE. Its accumulation due to liver dysfunction leads to a cascade of events in the brain, ultimately resulting in the neuropsychiatric symptoms characteristic of HE.
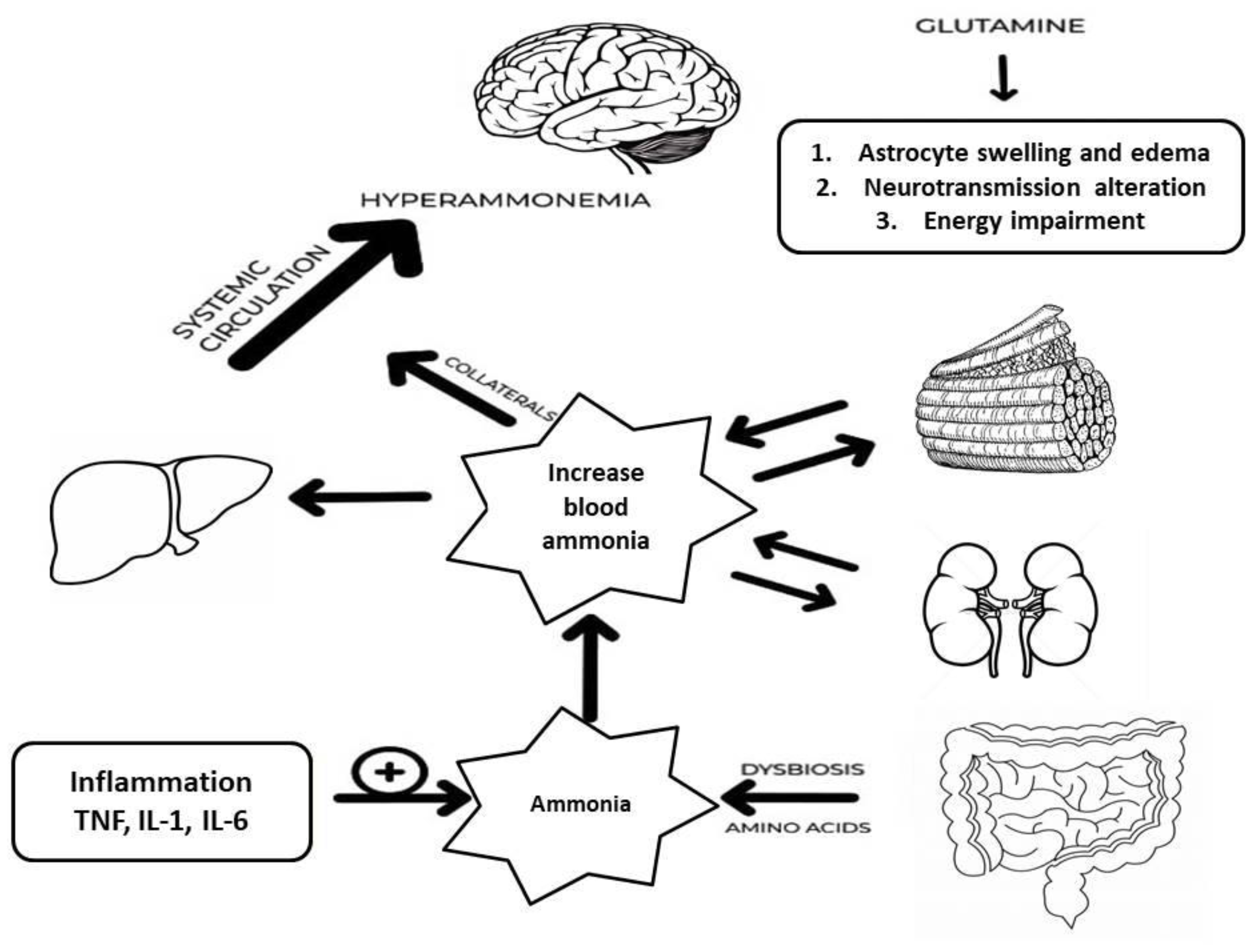
Figure 3.
The Algorithm for arriving at the diagnostically appropriate diagnosis of MHE starts with the patient’s history, clinical examination, and exclusion of other causes of encephalopathy. Then, neuropsychological tests and appropriate tools are performed. Finally, the diagnosis is reached through the interpretation of the data from the previous steps.
Figure 3.
The Algorithm for arriving at the diagnostically appropriate diagnosis of MHE starts with the patient’s history, clinical examination, and exclusion of other causes of encephalopathy. Then, neuropsychological tests and appropriate tools are performed. Finally, the diagnosis is reached through the interpretation of the data from the previous steps.


Table 1.
Diagnostic methods for the detection of MHE.
| Method | Advantages | Disadvantages | References |
| Psychometric testing | |||
| PHES |
-Validation across many populations and a wide range of therapeutic instances -Assists in diagnosing MHE and predicting the developing OHE. -High sensitivity and specificity when diagnosing MHE |
-Insufficient localization -Age and education levels greatly affect scores, requiring adjustment and complicating interpretation -Repeated use may provide practice effects when patients do better owing to familiarity with the tests rather than cognitive progress |
Amodio et al. (2008) [95] Dhiman et al. (2010) [89] Duarte-Rojo et al. (2011) [96] Seo et al. (2012) [97] Li et al. (2013) [98] |
| RBANS |
-Time-limitation to be performed in the clinical setting (30 minutes) -Efficacy in evaluating cognitive deficiencies in a variety of conditions -Initial diagnosis and monitoring of cognitive changes over time |
-Certain factor configurations may be more suitable for specific populations -Demographic characteristics can impact performance -May not evaluate some specific cognitive areas, such as executive function |
Duff et al. (2015) [90] Schmitt et al. (2010) [99] Garcia et al. (2008) [100] McKay et al. (2008) [101] |
|
ANT |
-Convenient for regular screenings -Do not require equipment or considerable training -Correlation with other diagnostic instruments, such as the PHES and EEG |
-Demographic characteristics can impact performance -Restrictive data on cognitive function requiring more extensive neuropsychological assessments -Dependence on verbal fluency might create bias, especially for those with speech or language difficulties, who may not adequately represent their cognitive capabilities |
Campagna et al. (2017) [91] Labenz et al. (2019) [102] Agarwal et al. (2020) [103] Qu et al. (2021) [104] Gairing et al. (2023) [105] |
| CRT |
-Treatment-response evaluation -Assess the consistency of reaction times -Unaffected by age and gender |
-Less stable than CFF -There was no correlation between CRT and laboratory tests -Long duration, requiring around 10 minutes to be performed |
Lauridsen et al. (2015) [10] Lauridsen et al. (2017) [106] |
| ICT |
-Notable level of sensitivity (88-90%) and specificity (up to 90%) in the diagnosis of MHE -Goog prediction for the onset of OHE -Strong test-retest reliability |
-Weak correlation between ICT results and the severity of liver disease (Child-Turcotte-Pugh or MELD scores) -ICT may have lower diagnosis accuracy than alternative approaches like the PHES |
Taneja et al. (2012) [107] Goldbecker et al. (2013) [108] Gupta et al. (2015) [109] |
| EncephalApp (Stroop test) |
-Accessible in clinical and non-clinical environments -Strong test-retest reliability -Weakly affected by demographic factors -Correlation of scores with sleep disruptions in patients with cirrhosis |
-Learning effect with repeated testing -Affected by age, education level, and smartphone experience -The ideal threshold values for detecting MHE using EncephalApp exhibit significant variation among different studies |
Bajaj et al. (2015) [92] Luo et al. (2020) [110] Cunha-Silva et al. (2022) [111] Lupescu et al. (2023) [112] |
| QuickStroop |
-High accuracy and specificity to detect MHE -Can be performed within 40 seconds, potentially enhancing CHE testing and treatment |
-Disadvantages are similar to the EncephalApp | Acharya et al. (2023) [93] |
| SIP-CHE |
-High level of sensitivity (80%) and specificity (79%) in identifying MHE -Does not require specific equipment or substantial training -Useful for monitoring the progress of HRQOL and cognitive function |
-Clinicometric features verified in specific populations, but their use in many cultural contexts is limited -Primarily a screening tool and does not thoroughly evaluate cognitive function (additional tests are usually necessary) |
Nabi et al. (2014) [113] Maharshi et al. (2016) [114] Lauridsen et al. (2020) [115] |
| SCAN test |
-Detects varying levels of hepatic encephalopathy by monitoring reaction times corresponding to the condition’s seriousness -High sensitivity and specificity in differentiating between different HE degrees -Impartial assessments of response times, minimizing the subjectivity |
-Influenced by the patient's cooperation level and cognitive condition -The absence of established standards for the administration and interpretation in various healthcare settings leads to variations and inconsistencies in the diagnosis of MHE |
Montagnese et al. (2012) [94] Luo et al. (2019) [116] |
| Electrophysiologic tests | |||
| EEG monitoring |
-Objective data, quantifiable parameters connected with mental state -Minor alterations in brain activity can be identified that may not be evident only by clinical assessment -EEG can be performed in various clinical environments, including those with minimal resources |
-Results interpretation can be subjective (high interrater variability) -The association between EEG alterations and clinical and psychometric findings regarding MHE can sometimes be variable -Standardized signal amplification, filtration, and spectral analysis techniques are necessary for precise EEG analysis |
McLaughlin et al. (1989) [117] Amodio et al. (1999) [118] Amodio et al. (2006) [119] Pascoli et al. (2006) [120] Schiff et al. (2016) [121] |
| Evoked potentials |
-Minimally invasive, uncomplicated, and can be readily conducted, even in intensive care units -Useful for patients with different levels of consciousness because they do not rely much on patient cooperation -Specific patterns have a strong correlation with cognitive deficits and psychometric test outcomes |
-Advanced equipment and specialized knowledge needed -Standardized methods for recording and interpretation are necessary |
Amodio et al. (2005) [122] Kullmann et al. (1995) [123] Zeneroli et al. (1984) [124] |
|
CFF |
-High level of sensitivity (96%) and specificity (77%) in diagnosing MHE -Unaffected by the patient's age or literacy level -Predict the risk of progression to OHE |
-Patient's state and the severity of liver disease can impact outcomes -There is usually no significant correlation between CFF and other psychometric tests |
Sharma et al. (2007) [125] Sharma et al. (2010) [126] Lauridsen et al. (2011) [127] Barone et al. (2018) [128] Romero-Gomez et al. (2007) [83] |
| Laboratory tests | |||
| Biomarkers |
-Ammonia is reliable for evaluating the occurrence of HE -Unbiased biomarker that minimizes the subjective inconsistencies in psychometric assessments and identifies the risk of OHE -There is a correlation between ammonia levels and cognitive impairment in MHE |
-Ammonia levels alone have limited clinical value in identifying MHE, and a comprehensive diagnostic strategy is recommended. | Direkze et al. (2015) [129] Suzuki et al. (2016) [130] Fiati et al. (2019) [131] |
|
-3-NT is a reliable biomarker with high sensitivity (90%) and specificity (93.33%) -Superior diagnostic accuracy of 3-NT compared to other markers like plasma ammonia |
-Specialized technology and experience are necessary for detecting 3-NT -It is advisable to utilize this tool alongside other diagnostic instruments to improve precision. |
Montoliu et al. (2011) [132] Salman et al. (2021) [133] |
|
Abbreviations: ANT, animal naming test; CFF, critical flicker frequency testing; CHE, covert hepatic encephalopathy; CRT, continuous response time test; EEG, electroencephalography; HRQOL, health-related quality of life; ICT, inhibitory control test; MHE, minimal hepatic encephalopathy; PHES, psychometric hepatic encephalopathy score; RBANS, repeatable battery for the assessment of neuropsychological status; SIP, Sickness Impact Profile; 3-NT, 3-nitrotyrosine.
Table 2.
Precipitating factors diagnosis and management.
| Precipitant factor | Diagnosis | Management |
| Alcohol and drugs |
Anamnesis |
Alcohol consumption counseling and discontinuation of hepatotoxic drugs |
| Constipation | More than 24 hours without passing stool or demonstration of significant fecal retention in the colon | Oral laxatives and/or cathartics, bowel enemas |
| Dehydration | Any sign of dehydration (skin and mucosal dryness, confused state) in a suitable context (patient with vomiting, diarrhea, diuretics abuse), as well as sodium, creatinine, and hematocrit increase | Correct dehydration (fluid therapy, stop diuretics) |
| Portosystemic shunt (spontaneous and TIPS) | Evidence of SPSS at radiologic imaging. Anamnesis and/or evidence of TIPS at radiologic imaging | Radiological shunt obliteration (BRTO, CARTO, PARTO) in case of recurrent/persistent HE |
| Electrolyte disorder | Hyponatremia (sodium < 130 mEq/L) | Hypovolemic hyponatremia: administration of normal saline. Hypervolemic hyponatremia: fluid restriction (<1000 mL/day); consider hypertonic saline or albumin administration. |
| Hypokalemia (potassium < 3 mEq/L) | Administer oral or IV potassium supplementation | |
| Malnutrition | Non-instrumental tools: BMI, food diary, objective examination, biochemical parameters, anthropometric measurements, creatinine-to-weight ratio, subjective global assessment questionnaire. Instrumental tools: bioimpedance test, handgrip strength test, DEXA, computed tomography scan | Dietary consult and advice for a correct supply of nutrients. Physical exercise to improve muscle tropism based on the patient’s potential |
| Gastrointestinal bleeding |
-Any evidence of upper GI tract bleeding (hematemesis or melena) |
Variceal bleeding: stabilize the patient if unstable, start vasoactive drugs and antibiotic prophylaxis, and perform an upper endoscopy. Consider TIPS placement in selected cases. Non-Variceal Bleeding: stabilize the patient if unstable, start PPI IV at high dosage, perform upper endoscopy within 24 h (<12 h if high-risk patient), and endoscopic hemostasis if indicated. |
Abbreviations: BRTO, Balloon-Occluded Transvenous Retrograde Obliteration; CARTO, Coil-Assisted Retrograde Transvenous Obliteration; PARTO, Plug-assisted BRTO.
Table 3.
Published studies on the management of minimal hepatic encephalopathy.
| Reference | Population | Intervention | Comparison | Outcomes |
| Lactulose therapy | ||||
| Morgan et al. (1989) [187] | 14/ 14 | Lactulose | Lactitol | No differences between treatments in a median change in psychometric time or scores |
| Horsmans et al. (1997) [188] | 7/ 7 | Lactulose | Lactose as placebo |
Improvement in time on Psychometric test on lactulose group with respect to basal values. Rate of improvement NCT: 5/7 (71.42%) vs 1/7 (14.28%); NNT:2 |
| Watanabe et al. (1997) [189] | 22/36 |
Lactulose |
No treatment | MHE had disappeared in 10 (50%) of the 20 treated patients at week 8, but it persisted in 11 (85%) of the untreated 13 patients |
| Dhiman et al. (2000) [190] | 14/ 12 | Lactulose | No lactulose |
Improvement in 8/10 (80.0%) vs 0/8 (0.0%), P < 0.001) |
| Prasad et al. (2007) [191] | 31/ 30 | Lactulose | No treatment |
ITT analysis: Improvement in 20/31 (64.5%) vs 2/30 (6.7%); NNT:2 |
| Bajaj et al. (2012) [192] | 1000 | Lactulose | Rifaximin |
Suggestions: MHE diagnosis with ICT and treatment with lactulose |
| Sharma et al. (2012) [193] |
105/ 55 |
Lactulose | No lactulose |
Improvement of MHE in 21/32 (66%) vs. 9/36 (25%) |
| Ziada et al. (2013) [194] | 24/ 26 | Lactulose or Probiotic | No treatment | Normalization of psychometry in half of treated patients (13/24 vs. 14/26 vs. 3/25). Reduction of OHE risk development |
| Pratap et al. (2015) [195] | 40/ 33 | Lactulose or probiotic | No treatment | Psychometric improvement in 23/33 and in 25/40. Improvement in MHE correlated with a reduction of ammonia levels. |
| Sidhu et al. (2016) [196] | 55/ 57 | Lactulose | Rifaximin | MHE reversal in 38/55 and in 42/57; HRQoL was significantly improved in both groups |
| Wang et al. (2019) [197] | 67/ 31 | Lactulose | No lactulose |
ITT analysis: 43/67 (64.2%) vs 7/31 (22.6%); NNT: 3PPS: 41/59 (69.5%) vs 6/28 (21.4%); NNT: 2 |
| Wang et al. (2023) [198] | 52 (Pro, n = 34) , (Rif, n = 11) , (Lac, n = 7) |
Probiotics, Rifaximin , Lactulose | Baseline before Probiotics, Rifaximin , Lactulose |
MHE Recovery Rates: Probiotics: 58.8% (20/34) Rifaximin: 45.5% (5/11) Lactulose: 57.1% (4/7) No significant difference in efficacy between the three groups (p = 0.843). |
| Rifaximin therapy | ||||
| Sidhu et al. (2011) [199] | 49/ 45 | Rifaximin | Placebo | Reversal at 2 wk: 57% vs 18% (NNT: 3)At 8 wk: Reversal of 75.5% vs 20% (NNT: 2) |
| Ballester et al. (2022) [200] | 32 | Rifaximin | Patients without metabolic syndrome manifestations | Mean PHES in responders (21 patients 66 %) was − 7.3 ± 0.7, − 3.2 ± 0.3, and − 3.3 ± 0.6 at study initiation and at 3 and 6 months of rifaximin, respectively |
| Bajaj et al. (2013) [201] | 20 | Rifaximin | Baseline (before Rifaximin) |
Significant improvement in cognitive performance (6/7 psychometric tests) |
| Ahluwalia et al. (2014) [202] | 20 | Rifaximin |
Baseline (before Rifaximin) | Changes in ICT, improvement of 12% respect to baseline, indicating a better cognition |
| Zhang et al. (2015) [203] | 26 | Rifaximin | Baseline (before Rifaximin) |
MHE reversal in 15/26; reduction in SIBO and ammonia levels |
| Goyal et al. (2017) [204] | 42/ 38 | Rifaximin | Lactulose | Still free of MHE: Rifaximin 42.8% vs lactulose 50.0% (NNT: 14) |
| Bakulin et al. (2023) [205] | 258 | Rifaximin | Cyclic therapy | Continuous rifaximin-alfa therapy significantly improves cognitive function and quality of life in patients with liver cirrhosis and MHE compared to cyclic therapy |
| Fiorillo et al. (2023) [206] | 31 | Rifaximin | Patients without MHE, controls, baseline (before Rifaximin) | NFL levels in MHE patients who responded to the treatment significantly decreased 16.1 ± 2.7 to 11.9 ± 1.8 |
| Casanova-Ferrer et al. (2024) [207] | 18/ 57 | Rifaximin | No treatment | Rifaximin treatment improved cognitive functions, as evidenced by better scores on the PPHES, OSDMT, and Stroop tests. |
| l-Ornithine l-Aspartate (LOLA) | ||||
| Kircheis et al. (1997) [20] | 26/ 27 | LOLA infusion | Placebo | Improvement in the mean time to respond NCT-A from baseline (29% vs. 9.73%) |
| Branched-chain amino acid (BCAA) therapy | ||||
| Egberts et al. (1985) [208] | 11/ 11 | BCAA | Placebo | Improvement in the psychometric test from 0 to 13.63% with respect to basal values in DST |
| Plauth et al. (1993) [209] | 17 | BCAA | Placebo | BCAA is superior to placebo in Psychometry and driving ability |
| Marchesini et al. (2003) [210] | 174 patients with advanced cirrhosis | 12-month BCAA supplementation | Lactoalbumin or maltodextrins | BCAA significantly reduced the combined event rate (death or deterioration) compared to lactoalbumin. BCAA group had fewer hospital admissions and improved nutritional parameters, liver function, anorexia, and quality of life. |
| Les et al. (2011) [211] | 116 patients with cirrhosis and prior HE episode | 56-week supplementation with 30g BCAA | Maltodextrin | There was no significant difference in HE-free survival. The BCAA group showed better performance on two neuropsychological tests and increased mid-arm muscle circumference. |
| Probiotic therapy | ||||
| Liu et al. (2004) [32] | 40 patients with cirrhosis and MHE. 15 healthy volunteers (controls). |
Probiotic, Prebiotic | Baseline (before synbiotic administration) Healthy controls |
MHE Reversal: Synbiotic group: 50% (20/40) showed significant improvement in psychometric test scores. No significant changes in the placebo group. Blood Ammonia: Significant reduction in arterial and venous ammonia levels in the synbiotic group (p < 0.01). No significant change in the placebo group. Endotoxemia: Significant reduction in plasma endotoxin levels in the synbiotic group (p < 0.01). No significant change in the placebo group. |
| Malaguarnera et al. (2007) [212] | 30/ 30 | Bifidobacterium longum + FOS | Placebo |
No statistical or clinical change was found with respect to basal values at 30, 60, 90, and 120 d |
| Bajaj et al. (2008) [213] | 17/ 8 | Probiotic yogurt | No treatment |
ITT analysis: Reversal in 12/17 (70.58%) vs 0/7 (0%) |
| Sharma et al. (2008) [214] | 31/ 31 | Lactulose or probiotic or lactulose + probiotic | No treatment | Normalization of all parameters in half of the treated patients (17/31, 16/31, and 17/30, respectively) |
| Mittal et al. (2011) [215] | 40/ 40/ 40/ 40 | Lactulose/ VSL#3, LOLA | No treatment | ITT analysis: Reversal of 4 (10%) in no treatment group, 19 (47.5%), 14 (35%) and 14 (35%) |
| Bajaj et al. (2014) [216] | 14 | Probiotics | Placebo | Reduction in endotoxin and TNF-α but not in cytokines. No effects on psychometric performance |
| Lunia et al. (2014) [217] | 86/74 | Probiotic | No treatment | Probiotics prevented HE. Reduced arterial ammonia, SIBO, OCTT; increased PHES and CFF thresholds compared to control. |
| Sharma et al. (2014) [218] | 32/ 31/ 31/ 30 | Probiotics | LOLA, rifaximin, placebo | All three treatments were better than placebo in improving CFF and abnormal neuropsychiatric test results. Rifaximin and LOLA significantly improved CFF compared to placebo. |
| Pratap Mouli et al. (2015) [195] | 33/ 40 | Probiotic | Lactulose | Probiotics non-inferior to lactulose in improving MHE. Improvement in both groups correlated with a reduction in ammonia levels. |
| Xia et al. (2018) [219] | 30/ 37 | Probiotic | No treatment | Improved cognition, enriched Clostridium cluster I and Bifidobacterium, decreased Enterococcus and Enterobacteriaceae. Reduced venous ammonia and improved intestinal mucosal barrier parameters. |
| Combined therapy | ||||
| Liu et al. (2004) [32] | 20/ 20/ 15 | Symbiotics + fermentable fibers | Fermentable fibers/ placebo |
Reversal of 50% in the symbiotic group, 50% in the fermentable fibers group, and 13% in the placebo. Not statistically significant until compression of treatment groups vs placebo (P = 0.03) |
| Ndraha et al. (2011) [220] | 17/ 17 | BCAAs + LOLA | BCAAs | Improvement in CFF 7.0% and 1.96% values (Hz), with respect to baseline |
| Kato et al. (2013) [221] | 19 |
30-35 Kcal + 1.0-1.5 g/kg of protein/d |
baseline (before treatment) |
11/19 (57.8%) recovered at 4 wk, and 13/19 (68.4%) at 8 wk |
| Rai et al. (2015) [222] | 7 |
Lactulose and Rifaximin |
Controls, NMHE group, baseline (before treatment) |
Psychometric improvement (P=0.044); reversal of low-grade cerebral edema |
| Shi et al. (2023) [223] | 44/ 44 | Combination of probiotics and lactulose. | Lactulose alone. | A combination of probiotics and lactulose is more effective than lactulose alone in improving cognitive function and quality of life in patients with MHE |
| Others | ||||
| Malaguarnera et al. (2008) [224] | 60/ 55 | Acetyl-L-carnitine | Placebo | Changes of mean values in at least 20.71% to 32.79% with respect to basal values |
| Agrawal et al. (2011) [225] | 35 | For patients with MHE and H. pylori infection, Clarithromycin, lansoprazole, tinidazole | Relationship between H. pylori and MHE, rather than directly contrasting different treatment approaches. | Improvement in 12.7%, 13.3%, and 18.7% with respect to basal mean time in NCT, FCT, and LTT |
| Bajaj et al. (2014) [216] | 18/ 19 | Lactobacillus GG | Placebo | Improvement from 1.02% to 15.89% from baseline values |
| Burkard et al. (2013) [226] | 25 | Potassium–iron–phosphate–citrate | baseline (before treatment) |
Normalization of psychometry in 72% vs. 26.9%. QoL improvement. |
| Maharshi et al. (2016) [114] | 60/ 60 | Nutritional education |
No nutritional therapy |
27/38 (71.1%) vs 8/35 (22.8%); 27/60 (45%) vs 8/60 (13.3%) when considering PPS and ITT analysis. |
| Janyajirawong et al. (2021) [227] | 34/ 32 | Zinc supplementation | Placebo | A 12-week course of zinc supplementation significantly improved psychomotor performance in cirrhotic patients with MHE. Patients receiving zinc performed better in neuropsychiatric tests (NCT-A, NCT-B, SDT, DST) than placebo patients. |
| Sharma et al. (2023) [228] | 75/ 75 | Nutritional therapy | No nutritional therapy | Nutritional therapy is effective in treating MHE and is associated with improving nutritional status, HRQOL, ammonia, endotoxins, inflammatory markers, and myostatin levels. |
Abbreviations: BCAA, branched-chain amino acids; BDT, block design test; CFF, critical flicker frequency; CEP, cognitive evoked potentials; DST, digit symbol test; EEG, electroencephalogram; FOS, fructooligosaccharide; HRQoL, health-related quality of life; ICT, inhibitory control test; LTT, line tracing test; MHE, minimal hepatic encephalopathy; NCT-A, number connection test-A; NCT-B, number connection test-B; NfL, Neurofilament light; OHE, overt hepatic encephalopathy; PHES, psychometric hepatic encephalopathy score; SDT, serial dotting test; SIBO, small intestinal bacterial overgrowth.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



