Submitted:
08 February 2025
Posted:
10 February 2025
You are already at the latest version
Abstract
A comprehensive literature review was conducted with the aim of describing the existing evidence and the most recent therapeutic advancements. The phenotype of hypertrophic cardiomyopathy is characterised by the development of concentric hypertrophy, which is variable but often asymmetric, primarily occurring in the left ventricle. The disease is marked by diastolic dysfunction, with a reduction in the intracavitary internal diameter, due to the disordered positioning of cardiomyocytes and the presence of collagen fibres, which thicken the myocardial tissue and impair relaxation. There is strong evidence of mutational components in the sarcomeric genes contributing to the development of the disease. The clinical signs are variable and are frequently associated with congestive heart failure and arterial thromboembolism. Diagnosis is determined through the combination of clinical, laboratory, and imaging tests, although there are still gaps that need further investigation. Therapeutic management aims to control clinical signs, disease progression, and to improve both quality of life and life expectancy.
Keywords:
cardiovascular
; cats
; heart failure
; hypertrophy
; physiology cardiovascular
1. Introduction
Currently, there has been an increase in the number of domestic animals, especially cats [1]. Thus, frequent changes in the lifestyle of these animals contribute to a greater demand for specialized services in the area [2]. In addition, a point to be considered is the increase in the life expectancy of felines, which may explain the greater occurrence of diseases [2]. Among the various illnesses to which cats may be subjected, cardiovascular diseases, owing to their frequency and severity, require special attention [2]. Feline cardiomyopathies, especially the hypertrophic phenotype, are considered one of the main causes of death in cats [3,4,5]. Hypertrophy cardiomyopathy is the most common feline heart disease, with evidence of genetic origin, and presents itself as left ventricular hypertrophy, with or without systemic complications [6,7,8,9].
Early diagnosis of feline hypertrophic cardiomyopathy (HCM) enables patient staging, monitoring and symptomatic management, as well as control of disease progression [10]. A few cats can present the asymptomatic form, making it difficult for both owners and veterinarian professionals to recognize it [2]. Furthermore, this underdiagnosis process implies a lack of recognition of the condition and a reduction in the patient's life expectancy [11]. Several diagnostic options are available to enable diagnosis and assist in associated clinical-therapeutic management [5]. This article aims to describe, update, and characterize feline hypertrophic cardiomyopathy and discuss available diagnostic tools and clinical therapeutic management, the guidelines (2020) established by the American College of Veterinary Internal Medicine (ACVIM) and new evidence after the publication of the consensus.
2. Feline Hypertrophic Cardiomyopathy Phenotype
Feline hypertrophic cardiomyopathy is a disease characterized by hypertrophy of the cardiac musculature and diastolic dysfunction that affects mainly the left ventricular chamber [5,12,13]. Hypertrophic cardiomyopathy can lead to hemodynamic consequences, depending on the severity of the condition (mild to severe) [5]. Initially, alterations in muscle thickness are observed in the left ventricular region, especially at the ventricular wall and papillary muscles, either completely or partially [5]. Thus, due to cardiac dysfunction caused by cardiac hypertrophy, the diastolic process is affected, which interferes with the proper functioning of the organ, leading to serious systemic complications [4,14,15]; therefore, echocardiographic examination can be useful in this assessment [16]. The occurrence of cardiomyopathies is not restricted to cats and has been described in other species [17]. However, in felines, HCM is considered the most common form [18,19]. In a study conducted by Argenta et al. [20], the prevalence of HCM was 78%, and HCM was the most commonly observed phenotype. The prevalence of HCM reported in the Cat Scan Study by Payne et al. [21] was 14.7% (95% CI; 12.3--17.4%), in contrast to the 37.4% (n=40/107) reported in the Cat Scan II study [22], and Matos et al. [23] reported a prevalence of 28.4% (n=29/102). HCM can be characterized by several cardiac and systemic changes, including increased density of the left ventricular (LV) wall, correlated cardiac morphofunctional changes and activation of compensatory mechanisms [4,5]. Recently, Seo et al. [24] reported a prevalence of 17.4% in cats with HCM, with a greater emphasis on the subclinical form.
HCMs can affect cats in general, although some breeds are predisposed, such as Maine Coon, Ragdolls, Persian, Sphynx, Birman, American and British short-haired, Scottish fold, Cornish Rex, Himalayan, Chartreux, Bengal and mixed breeds [3,25,26,27,28]. Some of these patients have hereditary diseases with an associated mutagenic component, such as Maine Coon (autosomal dominant) and Ragdoll [4,6,7,29]. According to Stern and Ueda [30], Maine Coon cats may manifest changes in echocardiographic findings during the early stages (premature form of HCM). HCM can occur aggressively and at an early age in other breeds, such as Ragdolls and Sphinxes [31,32]. In terms of age group, middle-aged and elderly cats are more predisposed, although this can occur at all ages [3,21,22,26,27,28,33]. According to Matos & Payne [16], age over 6 years is considered an independent predictive factor for HCM. The occurrence of HCM is more common in males than in females [19,23,34]. In a study conducted by Matos & Payne [16], the average diagnostic age for cats was 7.3 years, and 23 of the 40 positive animals were males. In the study by Seo et al. [24], the mean age was 4.0 years (3.2–5.3), which affected more male cats. A Figure 1 schematically summarises the phenotype of hypertrophic cardiomyopathy, including clinical manifestations, associated factors, and pathophysiology.
3. Genetic Influence
HCM has some similarities with human hypertrophic patterns [17,35]. According to Maron and Fox [17], “it is believed that no other animal species spontaneously develop HCM in such a closely aligned way with human HCM as cats”. Feline HCM was discovered in mid-1977 [36], and there was evidence of genetic involvement approximately years later, only in 1999 [33,37]. This mutagenic evidence demonstrates the existence of alterations in the formation process and sarcomeric composition [15], especially in the coding of amino acids (replacement by the exchange of nitrogenous base pairs) [8,33]. These modifications induce changes in the expression, function or formation of protein structures with the development of functional consequences [8]. The mutagenic component was identified in 2005 by Meurs et al. [6] in a study involving 16 Maine Coon cats with a family history of HCM and a control group of 100 cats of different breeds.
Owing to the reduction in the MYBPC3 concentration, there was a substitution in a base pair (codon 31 and exon 3). Therefore, there was an exchange of the amino acid alanine for proline, a mutation known as A31P (A31P; p.A31P; G91C; c.91G>C) [6,38]. The prevalence of A31P is believed to be between 22% and 42%, which is specific to Maine Coon cats [33,39]. In the study conducted by Stern et al. [38], most HCM-positive cats had the A31P variant. The genotypes of those affected by the A31P mutation did not show changes worthy of note for Meurs et al. [6]; however, for Longeri et al. [25] and Ontiveros et al. [40], homozygous cats are more affected by the disease, and the increase in penetrance is related to age. In agreement with the findings of Longeri et al. [25] and Ontiveros et al. [40], Stern et al. [38] reported that the penetrance of the A31P mutation was greater in cats with a homozygous genotype, and these cats more frequently developed HCM than heterozygotes did. New evidence suggests the benefit of using a loop-mediated isothermal amplification assay (LAMP) combined with a lateral flow dipstick (LFD) as a screening method for detecting A31P mutations [41].
In 2007, Meurs et al. [7] reported the presence of a second variant in the MYBPC3 gene known as R820W (c.2460C>T; R820W). This variant causes the substitution of the amino acid arginine for tryptophan in the region of codon 820 (p.R820W). In view of this, there are changes in sarcomeric nature and functionality. According to Kittleson et al. [33], the prevalence of this mutation is 27%, and it is exclusive to Ragdoll cats [25]. Regarding the pattern of occurrence, Borgeat et al. [42] reported that homozygous cats have a shorter life expectancy. However, in 2015, Borgeat et al. [32] did not observe differences in the occurrence of the disease between homozygous and heterozygous cats. Stern et al. [38] reported that crossing a heterozygous male with a homozygous female was able to generate offspring with more severe HCM with early manifestations of the disease.
New studies indicate the presence of other genes associated with the occurrence of HCM, including MYH7 and ALMS1. Meurs et al. [43] described the occurrence of a mutation in the ALMS1 gene, which is responsible for Alström syndrome, a familial systemic disease, in Sphynx cats. The G/C variation (g.92439157G>C) was found in exon 12 of the ALMS1 gene in a deleterious form (glycine to arginine) with changes in protein structure, in addition to muscle disorders and fibrosis in cats with HCM. Turba et al. [44] reported that, considering the g.92439157G > C mutation, the g.92439157 The C variant was well propagated (frequency > 0.50) in 136 Italian Sphynx cats, revealing studies that verified the frequency of the variant in relation to the occurrence of HCM. Furthermore, Akiyama et al. [45] studied the prevalence of the MYBPC3 and ALMS1 variants in a sample of cats in Japan. The authors observed cats with the MYBPC3-A31P and ALMS1 p.G3376R variants carrying HCM, which varied between breeds and genotypes. However, in a recent study by Seo et al. [46], the ALMS1 variant was present in 70.9% of cats but was not related to the occurrence of HCM. Mutations in the MYBPC3-A74T gene were found in Bengal cats, supporting the theory that the mutation is capable of promoting the development of HCM in homozygous cats, although for heterozygotes, there is a lack of evidence of the presence of the disease [47].
Sukumolanan & Petchdee [47] reported the prevalence of the MYBPC3-A31P (16.33%) and MYBPC-A74T (24.45%) mutations in 49 Maine Coon cats. Furthermore, the authors reported that HCM in cats with mutations increased in relation to epidemiological factors such as age and weight, as did heart rate and isovolumetric relaxation (IVRT) [20]. Therefore, the authors suspect that Maine Coon cats present the disease in a multifactorial way (genetics and underlying conditions) [10]. New evidence pointed to the causality of HCM in Maine Coons due to a mutation originating from the TNNT2 intronic variant c.95--108G>A. Thus, Schipper et al. [49] carried out a study to investigate the allelic frequencies of the variant in several countries and reported that it has no significance and does not guarantee a benefit for screening in breeding programs. Recently, Grzeczka et al. [50] reported that one of the main obstacles for cats with HCM is that the majority are mixed-breed; therefore, the detection of variants associated with the disease is difficult.
4. Pathophysiology of Feline Hypertrophic Cardiomyopathy
LV diastolic dysfunction initially damages blood ejection mechanisms, reducing the amount of circulating blood [5,51]. This dysfunction induces important hemodynamic changes that are easily compensated for when it occurs in healthy cats [5]. In cats with HCM, degenerated cardiomyocytes are replaced by fibrous tissue due to decreased myocardial blood supply and hypertrophy (collagen deposition due to structural breakdown) [32]. In a compensatory way, hypertrophy begins to develop with alterations in ventricular compliance capacity, leading to significant myocardial fibrosis [5].
Concentric hypertrophy reduces the size of the ventricular lumen so that compensatory tachycardia can develop as a way of maintaining adequate blood pressure and flow [30]. However, this tachycardia causes cardiac aggravation for a shorter time to fill the ventricular chamber [30]. It may be possible to observe serious regional and systemic complications such as myocardial and organic ischemia [30]. Diastolic dysfunction may increase the filling pressure (compensatory response) to the point at which the maximum ventricular compliance rate is reached [5]. Once this limit is exceeded, ventricular modification occurs due to increased pressure, and thus, the atria may be affected [5,16]. There may be changes with increases in pulmonary capillary pressure values (edema and/or pleural effusion) and impairment of systolic function [52]. There is a great possibility of right ventricular hypertrophy with the progression of the disease, clinical condition and presence of left hypertension [53,54]. It is common for cats affected by HCM to exhibit systolic anterior motion (SAM) with displacement of the caudal portion of the mitral leaflet toward the LV outflow tract, which is capable of promoting left ventricular outflow tract (LVOT) obstruction (LVOTO) [16]. SAM conditions are associated with mitral regurgitation due to changes in valve coaptation [28]. Figure 2A-D shows the macroscopic and histopathological alterations associated with hypertrophic cardiomyopathy.
According to Kittleson and Côté [5], the presence of mitral valve regurgitation and obstructive conditions in the LVOT can contribute to increases in atrioventricular pressure. Blood flow obstructions can occur in secondary cases of HCM due to several factors, such as LVOT obstruction, displacement of the mitral leaflet and increased pressure caused by the LVOT [55]. Patients with HCM may present changes in hypertrophic patterns, with certain regions of the septum exhibiting greater hypertrophy than others do, and LVOT obstruction may be caused by interventricular hypertrophy [5,55]. Studies have shown that the septal region close to the mitral leaflets hypertrophies more frequently than other areas [56]. Furthermore, new studies point to the role of new potential factors associated with the pathogenesis of HCM as well as the occurrence of fibrosis and remodelling. Joshua et al. [57] reported that some signalling pathways, such as RhoGDI-RhoGTPase, integrin, LXR/RXR, PPARα/RXRα, HIF1α and CXCR4, which have specific myocardial transcription patterns, seem to be associated with HCM.
This evidence indicates that differences in the gene activation process may be associated with the occurrence of HCM. Colpitts et al. [58] reported such differences in young and adult cats and in young and sick HCM patients, who presented elevated levels of interleukins (IL-6) and monocyte chemoattractant protein 1 (MCP-1) and increased expression of IL-6 under thrombotic conditions. Factors related to age, lifestyle and genetic transcription observed in adult cats may be associated with the occurrence of the remodelling process and thrombotic formation, which are related to the pathogenesis of the disease [58]. Furthermore, Rodríguez et al. [59] reported that cats with HCM have reduced microvasculature density, with an increase in interstitial edema, collagen and mononuclear cells. The presence of mostly resident macrophages as well as fibroblastic and/or vascular cells and interstitial cell groups of the CD34+ type are associated with the occurrence of the disease. Given the deleterious role of angiotensin II (ANG II) and angiotensin II-converting enzyme (ACE2) in the pathogenesis of cardiovascular disorders, Lean et al. [60] investigated the presence of the enzyme in healthy cats and those with HCM. The authors reported that ACE2 is overexpressed in cardiac tissue, which could partly explain the regional and systemic consequences of the disease [60]. Increased expression of ACE2 may be capable of inducing cardiovascular disorders [60].
5. Clinical Manifestations
The symptoms of HCM carriers vary and are often associated with factors such as severity, age and breed [4,5,17,22,26,55]. In general, affected cats can develop signs of congestive heart failure (CHF) to arterial thromboembolism (ATE) [4,17,22,26,30,54]. Some cats can carry the disease asymptomatically (15% healthy cats > 25% over 9 years), and the diagnosis of these animals is an impasse [24,35]. This may be associated with a low demand by owners for veterinary assistance, in addition to the fact that the absence of symptoms can make it difficult to diagnose [35]. Most symptoms are associated with cardiac and respiratory changes, depending on the condition [61]. These symptoms may include tachycardia, tachypnea, exercise intolerance, arrhythmias and, depending on the severity, dyspnea [5,35]. The presence of a gallop heart sound may indicate cardiac alterations that must be investigated but are not exclusive to HCM [28].
Cats with HCM associated with flow obstruction are more likely to develop heart failure, ATE and/or sudden death [3,27]. The occurrence of sudden death in Cat Scan II was 5.9% in 34 cats with HCM [22]. According to Follby et al. [62], cats with HCM have a shorter lifespan, with rates similar to those of noncardiac disorders. The presence of respiratory symptoms such as cough is less frequently observed, and the presence of pleural effusion can cause dyspnea [63,64]. In cases of pulmonary edema and pleural effusion [38], there may be muffled sounds on auscultation and the presence of crackles [9]. In cases of systemic vascular congestion, cyanotic mucosa may be observed due to reduced perfusion [17,20,26,30,65].
Approximately 20 to 60% of affected cats may experience murmurs of varying intensities and degrees, with an age-dependent increase [21,24,27]. The cause of these murmurs in these patients may be regurgitation in the atrioventricular region (mitral valve) or displacement of the mitral leaflet (SAM) associated with LVOT obstruction, among other factors [5,35]. In a study by Payne et al. [21], animals with SAM had more murmur events (42/45, 93.3%), and a third heart sound could be heard in patients with HCM. The presence of the third sound was observed in 40% (n=20/50) of the evaluated animals, and the animals presented an obstructive phenotype and SAM [66]. According to Payne et al. [21], if a cat has a high classification of murmur (III/IV or above), older individuals, males and a larger body size can be considered at risk for HCM. Compared with healthy cats (30–45%), approximately 80% of subclinical HCM patients may present with murmurs in the parasternal region [21,27,67,68]. Pellegrino [69] reported that “not every cat with a murmur has cardiomyopathy, and the absence of a murmur does not rule out HCM”. For Matos et al. [22], the presence of a murmur can be variable, and it is possible to observe a greater occurrence for those with HCM at the beginning of the evaluations with high ventricular thickness, a decrease in internal diastolic diameter and a shortening fraction compared with healthy individuals. For Tantitamtaworn et al. [70], the assessment of heart sounds and left atrium (LA) dimensions remains valuable in assisting in the diagnosis of HCM. If the cat is purring during auscultation, Vliegenthart & Szatmári [71] suggest that grasping the larynx ventrally with the hand allows better definition of the heart sound.
Owing to diastolic dysfunction with reduced cardiac output and flow, cats with HCM can often develop ATE [4,72,73], which is predictive of death [16]. The emergence of thromboembolic conditions is associated with the presence of endothelial lesions with activation of the coagulation cascade and a large number of clots [74,75]. According to Shaverdian & Li [72], Poredos & Jezovnik [73] and Holm et al. [76], ATE cases are derived from Virchow’s Triad, which is characterized by “blood stasis, hypercoagulable state and endothelial injury”. The pathophysiology of thrombi is associated with blood stasis, blood turbulence, and changes in ejection and/or endothelial injury [754]. The location of thrombi is variable; they are found in the aorta region (majority), renal, iliac, and femoral arteries, among others [77,78]. Most thrombi are considered secondary conditions to cardiac diseases [75]. Arterial thromboembolism induces significant vascular obstructions, depending on factors such as thrombus size, degree of obstruction, and location [75,78]. Furthermore, as they cause some vasoconstriction, they lead to reduced organ and/or tissue perfusion [75,79]. According to Fox et al. [27], the incidence of ATE in cats with HCM increases up to 10 years of age, with a reduction after this age. These can manifest according to intrinsic and extrinsic conditions such as the time of onset, location, shape, dimensions and degree of obstruction (partial/complete) [75]. Often, cats with ATE present mainly with hind limb paresis (uni- or bilateral), a reduced/absent femoral pulse, hypothermia and cyanosis of the pads [75]. ATE cases are often characterized by the presence of ischemic neuropathy originating from the obstruction with the presence of pain [75,80,81].
As a differential diagnosis, it is necessary that the differential evaluation for angioendotheliomatosis be performed in cats with symmetrical hypertrophy since it is capable of promoting a false diagnosis of HCM [82]. Other diseases, such as hyperthyroidism, may cause cardiac changes [24,83] that partially resemble the hypertrophic phenotype, and ruling out the presence of the disease by measuring total thyroxine T4 is interesting. Lee et al. [84] described the case of a Persian feline with signs of fatigue, tachycardia and tachypnea who was diagnosed with hyperthyroidism, although it was not constantly monitored. The patient underwent an echocardiographic examination, which revealed a hypertrophic phenotype pattern that responded to hyperthyroidism medication, resulting in regression of hypertrophy, highlighting the possibility of clinical similarities between the two diseases [84].
Given the variations between diseases, Janus et al. [83] compared histopathological findings between cats with hyperthyroidism and those with HCM. The authors reported that cats with hyperthyroidism had an increase in the transverse diameter of the heart, and in those with HCM, cardiomegaly, hypertrophy and an increase in the number of atrial appendages were observed in relation to the control. Furthermore, both patient groups exhibited cardiomyocyte degeneration, although cardiac fibre disorders and hypertrophy were more common only in the HCM group [83]. The authors reported that although there are similarities in the cardiac patterns of the two diseases, mainly with respect to tissue degeneration and cellular hypertrophy, the hypertrophy caused by hyperthyroidism is smaller than that in cats positive for the hypertrophic phenotype, which would help to differentiate the diagnosis.
6. HCM ACVIM Consensus
In 2020, the ACVIM proposed a classification system for feline heart disease [4]. The aim was to adapt the classification proposed by the European Society of Cardiology (ESC) [4,12]. The ESC classification has limitations for the authors, mainly because it does not include cases in which the phenotype changes throughout the progression of the disease [12]. The new classification proposed by ACVIM is based on structural/functional or phenotypic characteristics [4]. It is recommended not to classify cases according to the specific disease but rather according to phenotype [4]. The new classification categorizes cats according to the following phenotypes: hypertrophic cardiomyopathy (HCM), restrictive cardiomyopathy (RMC), dilated cardiomyopathy (DCM), arrhythmogenic cardiomyopathy (AMC), and a nonspecific phenotype that encompasses myocardial diseases that do not fit into the previous categories [4].
Given its clinical impact, ACVIM involves a categorization that allows cats to be placed into different categories according to the severity and presence of clinical signs [4]. In addition, it allows the follow-up and monitoring of cats at defined intervals to verify whether it is necessary to start treatment, the effectiveness of therapy, disease progression, and prognosis, among other factors [4]. The classification categorizes the animals into five classes: A (predisposed cats), B (asymptomatic cats, subcategorized into B1 and B2), C (symptomatic and responsive to treatment) and D (refractory to treatment) [4].
7. Diagnostic Tools for Feline HCM
7.1. Clinical-Laboratory Diagnosis
The In addition to the information obtained from anamnesis, such as history and data related to life habits and observed signs, a detailed clinical examination can provide indications for HCM [5]. Cardiovascular changes can subjectively indicate that something is wrong [9]. The presence of murmurs, noisy breathing, fatigue, tachypnea, tachycardia, cyanotic mucosa and limbs with cold extremities can be signs of cardiac changes [5,9,19,28]. In addition, it is important to consider associated comorbidities such as feline immunodeficiency virus and feline leukemia virus [85]. Laboratory tests are important, whether hematological or biochemical [86]. However, although it is important to acknowledge the systemic health of cats [86], they are not pathognomonic for diagnosing HCM. Although there is speculation about the role of the neutrophil/lymphocyte ratio (NLR) in sudden death, Fries et al. [87] investigated the association between the NLR and HCM in cats and reported that the NLR is elevated in patients with CHF; however, the NLR cannot be considered a prognostic marker for felines with HCM. Some conditions, such as hyperthyroidism and subaortic stenosis, can induce cardiac changes resulting from LV hypertrophy, which should be ruled out [14]. Pressure measurements should be performed to rule out other diseases [4], such as systemic hypertension and chronic kidney disease, although unfortunately, this is not a routine practice [88].
7.2. Imaging Diagnosis
7.2.1. Thoracic Radiographs
Thoracic radiographies are considered useful tests for evaluating cardiovascular structure [54,89]. Radiographs of two projections, laterolateral and ventrodorsal, are recommended to assist in the diagnosis [90]. According to Guglielmini & Diana [90], chest radiographs allow the characterization of the condition in general, as they allow the analysis of the heart and other regional organs. It may be possible to assess the consequences and repercussions of HCM in other organs, such as pulmonary edema/pleural effusion and bronchial compressions [90,91]. Some studies have shown that CHF caused by HCM induces more pulmonary edema than effusion [92]. However, the diagnosis of CHF via radiography still has several limitations [93]. Rho et al. [94] emphasized that the accuracy of radiography in diagnosing HCM is 70% and that studies based on automated assessment of residual architecture can be useful for improving the diagnosis of HCM. Notably, in view of the stress involved in handling and preparing patients, radiographs must be taken with the patient stabilized so that decompensated cats receive appropriate treatment before undergoing the examination [9,91].
Feline HCM is radiographically characterized by increases in cardiac dimensions, mainly at the left atrioventricular level [90,95]. According to Pellegrino [69], “the results of chest radiography vary, depending on the observed hypertrophy, the degree of myocardial dysfunction, the presence of increased cardiac cavities and the severity of circulatory congestion”. Cardiac hypertrophy can be suspected through direct observation or by using measurement strategies such as clock analogy and vertebral heart size (VHS) [90]. Notably, chest radiographs show suggestive signs of cardiac alteration, with or without complications [90]. In addition, it may be possible to visualize tortuosities and dilatations of pulmonary vessels, possibly associated with increases in atrial pressure and increased vascularization in the lungs [95].
Cardiomegaly associated with atrial enlargement may be observed [95], although other conditions may cause cardiac enlargement [90]. Cardiomegaly, or “Valentine heart shape”, is radiographically characterized by narrowing of the apex and widening of the cardiac base [96,97]. The clock analogy is based on the external contour of the organ, with identification of focal increases in the heart chambers; thus, the organ is divided into regions that correspond to the hands of a clock [90]. For mixed-breed cats, the normal VHS is 7.5 ± 0.3 vertebrae (maximum limit of 8) [98], and for Maine Coons, it is 7.61 ± 0.34 [99]. Breed and chest conformations can promote variations in mean values [89]. In the study by Diana et al. [97], it was observed that cats that present pulmonary edema may have evidence of cardiomegaly, dilation of pulmonary vessels, especially caudal vessels, and atrial enlargement, even if they have concomitant heart disease.
Kim et al. [93] carried out a study with the objective of analysing the clinical impact of chest radiographs in affected cats and characterizing predictive radiographic evidence for HCM and CHF in 78 animals (43 HCM). The authors reported that the VHS of cats with HCM was greater (8.57 ± 0.74) than that of healthy cats, although there were no differences in the incidence of CHF [93]. The VHS for CHF had a sensitivity of 76.19%, a specificity of 40.91%, a positive predictive value of 55.17% and a negative predictive value of 64.29% [93]. Radiographic evidence of an enlarged and bulging LA, as well as a bulging left auricle, has a significant effect on the left atrial and aorta diameter (LA/Ao) ratio [93]. The left atrium and bulging LA are larger in sick felines than in healthy felines and in those with concomitant CHF [93]. With respect to vertebral heart atrial size (VLAS), there were no differences between patients (CHF and/or HCM) and healthy animals [93]. The LA/Ao value was greater in sick cats, especially in those with concomitant CHF [93].
Affected felines present with cardiomegaly, atrial enlargement and dilation of the caudal pulmonary artery, with elevation of the carina capable of predicting left atrial enlargement (94.12% specificity; 17.5% sensitivity) [93]. Kim et al. [93] reported that caudal pulmonary vein dilation and atrial enlargement differed between CHF patients and HCM patients without CHF. Furthermore, for Kim et al. [93], “the distal side of the summated shadow made by the right caudal PV with the ninth rib in HCM cats with CHF was significantly larger than that in HCM cats without CHF and a cut-off value of 5.35 mm was drawn with 75% sensitivity and 100% specificity”. The results of this study demonstrated that in cats with HCM, radiographic changes can be useful for the clinical and imaging evaluation of potentially affected cats. Figure 3A-D shows the results of Kim’s study [93].
7.2.2. Electrocardiography
Cats may present changes in electrocardiographic patterns suggestive of HCM, although this is not conclusive [55]. Despite being useful, it is a test with reduced sensitivity because different cardiac alterations can present the same electrocardiographic results [55,95]. Patients with HCM may present ventricular tachyarrhythmia, ventricular preexcitation, wide QRS complexes, electrical conduction irregularities, increases in the amplitude of R waves, atrial fibrillation, and axis deviations, among other conditions [3,5,9,100,101,102,103]. Recently, Murphy & Nakamura [104] reported the alternation of ventricular preexcitation with doubtful preexcitation complexes in felines with HCM. Repolarization and depolarization disorders in cats are still rare, especially in relation to the hypertrophic phenotype [105]. The ST segment may be transiently elevated [106]. Figure 4 shows the electrocardiographic evaluation of a feline patient with stage B2 hypertrophic cardiomyopathy.
A strategy that can be adopted to research ventricular arrhythmias in cats with HCM was studied by Bastos et al. [105] when performing a study with the Tpeak–Tend (Tpte) measurement, comprising the period between the peak and the end of the T wave, as well as the relationship between Tpte and the Qt interval. The authors reported that the Tpte interval was greater in cats with HCM in leads II, aVR, aVL and aVF, and a Tpte interval greater than 27.5 ms in aVF may be able to identify HCM (83.3% accuracy). Felines with Tpte > 27.5 ms in aVR and aVF as well as > 26.5 ms in aVL are more likely to present HCM (1.28, 12 and 1.16x) [105]. Therefore, evaluating the Tpte period may assist in the diagnosis of hypertrophy. Bastos et al. [107] conducted a study with the objective of evaluating these indices and their applicability, especially for cats with HCM. The study included 40 healthy cats and 23 sick cats who underwent an electrocardiographic examination lasting 3–5 minutes [107]. Compared with healthy cats, sick cats presented short-term ventricular instability and prolonged QT and QRS intervals through QT intervals and corrected QT and QRS complexes. These findings suggest that they are potentially useful markers for screening HCM [107]. Notably, the possibility of bradyarrhythmia occurring after treatment with antiarrhythmics still needs to be further investigated [108]. Recently, Cofaru et al. [109] highlighted the importance of electrocardiography in the diagnosis of HCM but emphasized that 24-hour Holter monitoring would be the most ideal for evaluating electrical tracing over a longer period of time [110], but it is not yet in routine use.
7.2.3. Echocardiography
Considering that HCM is considered the gold standard exam for diagnostic determination [4,5,10,35,70], echocardiographic examination allows for the analysis of cardiac structures, verifying the presence of muscle hypertrophy (focal/regional) [28], especially in the left ventricular region [16], as well as observing the presence of mitral regurgitation with increased pressure [9,95]. It can be considered a very useful exam, although experience and training are needed [9,55,111]. Echocardiography can be performed in M mode, 2D mode, or both, although these methods have limitations [9,35,95]. Luis Fuentes et al. [4] and Wagner et al. [68] reported that among these obstacles, heterogeneous images (e.g., focal hypertrophies, probe cuts) and noninterchangeable values are obtained. It is necessary to pay attention to the type of image produced to avoid false diagnoses and changes in measured values [28]. Figure 5 shows the echocardiographic alterations in a feline patient with hypertrophic cardiomyopathy.
The ACVIM consensus states that for the LV, the M-mode is still the most commonly used mode for measurement, with short-axis images, although there may be erroneous assessments, especially due to heterogeneous hypertrophies [4,68]. The 2D mode makes it possible to measure the LV musculature in different regions with images of the short and long axes to assess the greatest thickness of each slice [4]. For long and short axes in 2D mode, measurements of at least 2 different points of the septal region and the wall are recommended, avoiding the papillary muscles [4,55]. The values between the two modes cannot be compared with each other, and the ideal would be to perform both [68]. It is expected that there will be an average value of echocardiographic measurements and that it is necessary to check for changes in myocardial motion [4,55]. For Fries et al. [28], isolated evidence of ventricular hypertrophy cannot be used as a decisive factor in the diagnosis of HCM, so in some cases, there may be a reversal, especially if it is of secondary origin. Furthermore, Stern et al. [38] reported that cats with a homozygous genotype more easily present preclinical signs of HCM than heterozygotes do, including ventricular and/or septal wall thickening and an increased AE/Ao ratio. LVOTO cases may be common in cats with HCM, especially due to regional obstructions in the ventricular outlet [38], and are associated with increased blood pressure, especially for animals with a wild-type genotype. However, Stern et al. [38] reported that the average incidence of obstruction was high in cats with A31P HCM.
According to Luis Fuentes et al. [4], LV hypertrophy can be categorized as follows: < 5 mm normal LV; 5–6 mm questionable; and > 6 mm hypertrophic LV. With respect to the LA, short-axis measurements can be obtained from the LA/Ao (left atrium/aorta) ratio in M and 2D modes at the end of ventricular systole/diastole [112,113], with differences between genotypes [38]. The long axis is measured at the end of systole, from the interventricular septum to the LA free wall [114]. It is necessary to evaluate and measure the shortening fraction (SF%) of the LA, the blood flow velocity of the ventricular atrial appendage (LAA), and the presence of spontaneous contrast and thrombi [18,91,115]. The LA measurements at the end of ventricular systole observed in a study were as follows: normal LA/Ao < 1.5; LA/Ao risk factor > 1.8; maximum distance LA 16 mm; LAA velocity < 0.25 m/s (blood stasis); and LA SF% < 12% (risk factor) [35]. In 2023, Matos et al. [116] reported that cats with advanced-stage HCM may present evidence of a thin and hypokinetic myocardial segment. The consensus does not describe measurements for echocardiographic variables. However, Luis Fuentes et al. [4] discussed echocardiographic protocols for cats suspected of having HCM. Fries et al. [28] recommended that Doppler echocardiographic examination be carried out to assess regions in which there is left hypertrophy, SAM and LVOTO, dysfunction in the diastolic process, atrial function and structure, and the presence of smoke and thrombi. Furthermore, it is essential to evaluate diastolic function in these cats via spectral/tissue Doppler, with tissue Doppler being the most appropriate for evaluation [28]. Recently, Colakoglu et al. [117] conducted a study to evaluate the relationship between smoke and LA dimensions. The authors reported that, with HCM and smoke, there was a reduction in the values of the SF% and fractional area, both of which are LA, which may be predictive markers for ATE.
In 2015, Payne et al. [21] conducted the Cat Scan study with 780 apparently healthy cats with the aim of screening the animals and analysing the predictive factors for the disease via echocardiography. Approximately 115 cats were considered positive for HCM, and only 5.8% had evidence of SAM; of the 45 animals with SAM, 41 (91.1%) had HCM. When cats were compared with those without SAM, they had greater median values of maximum left ventricular myocardial wall thickness, shortening fraction and atrial diameter. Exclusively in those with HCM and SAM, the median values were greater for the end-diastolic ventricular diameter and shortening fraction, although the left atrial diameter and LA/Ao ratio were not different. The authors observed associations between HCM and age, increased blood pressure, male sex, weight and body weight. For Seo et al. [118], the presence of baseline SAM was more strongly associated with disease progression than was the absence of baseline SAM.
In 2022, Matos et al. [22] conducted Cat Scan II, a multicenter study using data obtained from 107 cats from renowned centers in Europe. The authors monitored the cats for an average of 5.6 years and observed no changes in the thickness of the ventricular wall, although the atrial size and diastolic ventricular internal diameter increased [22]. The animals presented SAM during the study, with no change in the proportion of affected cats (33% of cats had SAM at the first assessment and 29% at the second assessment), focal ventricular wall thinning, atrial dilation, hypokinesia, or asymmetric hypertrophy [22]. Cat Scan II also revealed baseline predictive variables such as a reduction in the atrial ejection fraction (<25%), an increase in the ventricular ejection fraction, and a decrease in the internal diastolic ventricular volume in HCM patients [22]. Patients with an ejection fraction above 25% had a 91% reduction in the probability of HCM [Matos et al 2022]. Thus, the authors reported that an initial atrial ejection fraction less than 25%, increased ventricular fraction and high body weight were independently associated with the development of HCM [22].
In addition to the usual measures for diagnosing HCM, Seo et al. [119] conducted a study with the objective of evaluating the dimensions of the mitral valve leaflets and their relationship with the development of the disease. The authors reported that anterior mitral valve elongation can be considered a predictive marker for the development of HCM [118]. In the study by Velzen et al. [120], the size of the mitral leaflets was not considered a predictor of hypertrophy. Decreases in mitral and tricuspid annular plane systolic excursion values [121], hypokinesia and echo contrast may be associated with a worse outcome [92,116]. There is a lack of studies on whether diastolic dysfunction can be considered a predictive factor for HCM [122].
Aortic annular plane systolic excursion is reduced in cats with HCM, which is a variable of diagnostic interest [123]. Bach et al. [124] emphasized the importance of measuring mitral annular displacement in association with tissue tracking via Doppler and M-modes as ways of evaluating CHF conditions. The authors reported a reduction in longitudinal displacement by M-mode derived mitral annular plane systolic excursion (MAPSE) and mitral annular plane excursion measured by color-coded tissue tracking (TT-LD) due to the presence of CHF [124]. The area under the curve was more sensitive for the use of TT-LD than MAPSE; therefore, the authors observed that the methods can be used with strong correlation, although they cannot be used interchangeably [124]. Matos et al. [23] carried out a study with the objective of evaluating septal thickening in nonreferenced cats and reported that elderly cats had greater myocardial free wall thickness than young cats did. Approximately 38% of the cats (n=11/29) had SAM, and the average thickness was 6.5 mm, with the majority having LA/Ao and normal atrial dimensions, with an FS% of 24%. The aortoseptal angle was 140 ±14.4° in cats with HCM Matos et al. [23]. Assessment of aortoseptal angulation may be a useful strategy for inclusion in echocardiographic examinations of cats with HCM [125].
Another diagnostic option using echocardiographic evaluation is strain. Strain is a tool for analysing cardiac deformation with the aim of mapping the cardiac region and transmitting the findings through graphic images at a selected moment during the cardiac cycle [28]. Spalla et al. [126] carried out a study with cats with HCM via strain and reported that subclinically ill felines presented deforming changes in the long and axial axes, which highlights the importance of the tool as a diagnostic method.
Saito et al. [127] carried out a study with the objective of evaluating the myocardial function of cats with HCM, with or without LVOTO, using a speckle tracking echocardiographic diagnostic tool. Cats with HCM showed reduced longitudinal (epicardium and endocardium) and circumferential (epicardium) left ventricular deformation, although there was no difference between patients with and without LVOTO [127]. However, the endocardial and entire circumferential portions showed reduced deformation in HCM cats with LVOTO [127]. Thus, the authors reported that left ventricular myocardial function was more affected in HCM cats with LVOTO. Recently, Hirose et al. [128] reported that the occurrence of LVOTO promotes changes in the intraventricular pressure gradient; however, it is obtained via the Euler’s formula and not via conventional echocardiography, which is a method that can be effective for evaluating cardiac function.
Suzuki et al. [129] studied the relationship between CHF and myocardial function via speckle tracking in healthy and sick cats. The authors reported an increase in the LA/Ao ratio and a reduction in the left ventricular apical circumference in patients with CHF, as well as an increase in the left ventricular internal dimension at the end of diastole and a decrease in the longitudinal strain of the right ventricle. Left atrial dilation and decreased left ventricular apical myocardial function can be used as predictive markers for CHF. Furthermore, the presence of left ventricular dilation and dysfunction may be causes of CHF in cats with asymptomatic disease.
7.3. Biomarkers and Other Diagnostic Options
Biomarkers are substances that can be measured through blood exams for analysis and assessment of cardiac function and/or damage [20,28,130], helping in the characterization steps and evaluation of the severity of the disease [86,130] in addition to being able to be used as indicators of disease progression and prognosis [32,86]. The availability, price and release of results can be obstacles that make it difficult to use [4,5,32,35].
Among the biomarkers available for cardiac evaluation are N-terminal pro-atrial natriuretic peptide (NT-proANP), atrial natriuretic peptide (ANP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), B-type natriuretic peptide (BNP) and cardiac troponin-I (cTnI) [9,32,35,55,86,131]. They can be classified into markers of injury (cTnI) and function (NT-proANP and NT-proBNP). NT-proANP and NT-proBNP are released into the blood in cases of cardiac overload and/or distension [32,86]. Heishima et al. [132] conducted a study with cats in a control group (n=78) and cardiomyopathy patients (n=83) regarding the efficacy of ANP and reported that ANP concentrations increase with disease progression in a group of patients with cardiomyopathy. Heishima et al. [132] reported that these data cannot be considered alone.
NT-proBNP, the most commonly used biomarker [28], can be used to differentiate dyspnea conditions because of its long half-life and stability [10,61,92,133]. NT-proBNP for felines is commercially available through the Feline SNAP test. According to Kittleson & Côté [5] and Lu et al. [134], ideally, the test should not be used as a screening tool for healthy patients, although Luis Fuentes & Wilkie [35] state that these tests are valid for cats at high risk for HCM. Fries et al. [28] emphasized that NT-proBNP is not exclusive to cardiac conditions and that more in-depth tests, such as echocardiogram and magnetic resonance imaging, must be used for final diagnosis. Several studies have indicated that cats with HCM have elevated NT-proBNP and NT-proANP concentrations [131,135,136]. High doses of NT-proBNP increase the risk of cardiac events [136]. In the study by Matos et al. [22], the average NT-proBNP value was 400 pmol/L. Stern et al. [38] reported that NT-proBNP concentrations were associated with the A31P mutation, LVOTO and positive HCM, with values being greater for homozygous cats.
For the assessment of cardiac injuries, cTnI can be measured to assess for cardiac damage [10], and its use is beneficial for HCM [28]. In addition, cTnI is considered a prognostic marker [42,138], so the higher its concentration is, the shorter the survival time is. Gavazza et al. [85] reported that increases are related to the severity of the cardiac alteration, although it is not possible to clearly determine the underlying cause of the cardiac damage. Hori et al. [138] reported that cTnI concentrations can determine its origin and severity, given that other causes are ruled out. Hanås et al. [139] reported that the concentration of cTnI in patients with HCM is positively associated with the thickness of the free wall and the left atrium/aortic root ratio and that concentrations are greater and greater in patients with HCM with atrial enlargement. For Stern et al. [38], cTnI values did not differ according to genotype. According to Seo et al. [140], NT-proBNP and cTnI levels were greater when associated with SAM. Endothelin concentration measurements may also be useful because they are peptides with high levels of vasoconstrictor action (in the endothelium and blood vessels), although their use is of moderate importance [141]. Another useful biomarker for cases of ATE is D-dimer, which is capable of assessing coagulation function, with cats with HCM presenting high concentrations, in addition to which proteomics has shown favourable regulation of the integrin alpha M subunit (ITGAM), elongin B (ELOB) and fibrillin 2 (FBN2) [142]. The study showed that such assessments can be useful for better understanding of the disease.
Genetic tests can be performed to identify mutations associated with HCM [6,8] but must be performed for each patient tested [28]. Samples for deoxyribonucleic acid‒DNA analysis and genetic sequencing can be obtained from blood or oral mucous [6,143]. Importantly, owing to the variety of mutations observed [8], a negative result does not eliminate the possibility of an animal having HCM [143]. Genetic mapping of these cats would be of interest, especially for predisposed breeds [6,8]. Research shows that 39.4% of Maine Coon cats and 27% of Ragdolls have mutations in the MYBPC3 gene [144]; therefore, the monitoring of animals of these breeds must be periodic [28].
New evidence suggests that remodelling mediators such as lumican, isoenzymes and isoforms of lysyl oxidase (LOX) and transforming growth factor beta (TGF-β), which are associated with hypertrophy and fibrosis, are involved [145]. The authors reported that all collagen and noncollagen components were superior in diseased patients, as was mononuclear cell infiltration [145]. HCM-positive cats presented increased concentrations of lumican, LOX, TGF-β1, and β2 [145]. Thus, the authors point out that there is a link between markers of remodelling and fibrosis and HCM conditions, with proof through the dosage of these substances being a possible strategy to be included in other studies with the aim of improving the characterization of the disease and the search for treatment tools. Furthermore, Kaplan et al. [146] emphasized that, depending on the situation, fibrosis is self-perpetuating, which is independent of the process of myocyte dysfunction and may be associated with an excess of pleiotropic events and thus with an increase in fibrosis markers.
A new potential biomarker for cardiac fibrosis, galectin-3, which is considered a beta-galactoside-binding lectin derived from macrophages, has been identified. Stack et al. [147] conducted a study with 80 cats, 56 of which were in the ACVIM B1 and C stages. The authors reported that galectin-3 levels were increased in sick cats compared with healthy cats, with no differences in concentration by stage and a significant correlation with left atrial dimensions, the LA/Ao ratio and extracellular volume [147]. Fries et al. [148] reported that cats with HCM have greater extracellular volume values, with signs of diastolic impairment and greater left atrial dimension. A study by Deemekul et al. [149] revealed that galectin is associated with fraud in the interventricular septum and shortening fraction values, although it may be a possible initial predictive indicator of HCM. Although the results are favourable for its use, further studies are still needed to understand the role of dosage in cats with HCM. New evidence, which still requires further investigation, shows that biomarkers such as the myocardial genes interleukin 18 (IL-18), insulin-like growth factor binding protein 2 (IGFBP-2), and WNT Family Member 5 A (WNT5A) may be increased in patients with clinical and subclinical HCM [150].
Because cats with HCM are prone to ATE due to blood stasis, Li et al. [151] evaluated the potential of neutrophil extracellular traps (NETs) as biomarkers by measuring cell-free DNA (cfDNA) and citrullinated histone H3 (citH3). The authors reported that cats with HCM ATE presented an increase in cfDNA, and citH3 was identified in 52% of the animals with the disease and at a lower concentration in those with ATE. Li et al. [151] and Li et al. [152] concluded that the use of NETs may be a potential method for evaluating the presence of thrombi in cats with HCM because of variability in the distribution of thrombi due to factors such as shear and neutrophilic apprehension. Recently, Shaverdian et al. [73] described a new technique for flow cytometry using procoagulant markers such as thrombin and colvuxin, which showed a greater precoagulant tendency for cats with HCM.
8. Treatment Strategies
In general, cats need to be treated according to the stage of the disease [4,5] because of the prevalence and mortality rates, and it is ideal that diagnostic and therapeutic management be effective [28]. The prognosis of the disease is variable and is based on the stage of the animal [28]. One of the main objectives of therapy is to determine which cats appear to have a greater chance of developing HCM, which may be worsened by comorbidities, and whether there is an imminent risk of death, among other points [16,146]. In addition, it is necessary to prioritize treatment to avoid stress in these cats [153]. Cats often experience stress during laboratory tests and physical and imaging exams, and the administration of medication, mainly orally, can be an aggravating factor [153]. Controlling the stress of these patients is necessary and important for preventing complications that may worsen or decompensate their clinical condition [91]. In this way, cat-friendly practices should be prioritized in these cases from the moment the cat arrives for a routine veterinary appointment [153].
The ACVIM consensus recommends different therapeutic strategies for different stages of the disease, although many of these strategies have a low level of scientific evidence [4]. Fries et al. [28] emphasized that the prognosis and therapeutic options to be used are individual and dependent on the characteristics of the disease found in that patient. Stage A cats are not treated because they have no symptoms and are predisposed [4]. Class B1 patients are also not treated because they are asymptomatic, but annual monitoring is recommended for disease assessment and progression [4,5]. Therapeutic management of B2 cats includes thromboprophylaxis and monitoring [53,72,154]. Thromboprophylaxis is recommended when there is a high risk of developing ATE [95,154], such as moderate to severe dilation and decreased SF% and LA appendage velocities [4]. In this case, the use of clopidogrel (18.75 mg/cat orally - PO q24h with food), alone or in combination with aspirin (25 mg/kg PO q48-72 h; 81 mg PO q72h or 5 mg/kg PO q48h), or factor Xa inhibitors, such as rivaroxaban (2.5-5 mg PO q24h), is recommended [4,72]. Recently, Kamp et al. [155] described a case of liver involvement due to the use of clopidrogrel, which is uncommon but likely to occur and requires further investigation. For ventricular arrhythmias or ventricular atrial fibrillation, the use of atenolol (6.25 mg/cat PO q12h) or sotalol (10–20 mg/cat PO q12h) is recommended [4,156]. Kortas & Szatmári [157] conducted a study evaluating the use of atenolol and reported that, of the 23 cats treated, there was a positive response to SAM in 47% of cases; however, in the long term, SAM remained absent in only 9% of cases when it was administered q12h. Approximately 26% of cats medicated with atenolol die from cardiac causes, and it is not known whether the animals that did not respond positively to the medication had HCM or congenital disorders [157]. The use of pimobendan [4], angiotensinogen-converting enzyme (ACE) inhibitors [158], and spironolactone is not advised [159]. Regular frequency monitoring is recommended [4].
For stage C cats with acute CHF, oxygen supplementation and minimal stress are recommended; if necessary, the use of butorphanol (0.2 mg/kg IV) is recommended [4,5,9]. Management also includes furosemide in continuous rate infusion (CRI) (0.6–1 mg/kg/h) or a bolus (1–2 mg/kg) even in the presence of azotemia [4,90]; thoracentesis, if necessary (e.g., pleural effusion) [91]; and pimobendan (0.625–1.25 mg/cat PO) after signs of low output, a cold wet pattern, and the absence of LVOT obstruction [4,91]. Dobutamine (5–15 μg/kg/minute IV) may be used if pimobendan is not effective [4]. The use of atenolol, transdermal nitroglycerin and ACE inhibitors is not recommended [4,91]. These cats should be discharged as soon as possible [91]. Renal function and respiratory rate were reassessed after approximately 3‒7 days (at home <30 breaths/minute – breaths/min) [4].
For stage C patients with chronic CHF, furosemide (edema/effusion) at doses of 0.5–2 mg/kg PO q12h (balancing the dose to obtain a resting respiratory rate < 30 breaths/min) is recommended, as are urea assessment, creatinine and electrolytes 3–7 days after starting treatment; intravenous administration in cats with respiratory distress [4]; and thromboprophylaxis (clopidogrel 18.75 mg/cat orally q24h with food) [79]. Pimobendan can be used at a dose of 0.625–1.25 mg/cat orally every 12 h if there is systolic dysfunction and in the absence of LVOT obstruction [160]. Routine monitoring and follow-up (attention to patient stress) with respiratory rate measurements were performed at home [4]. Some evidence points to the arrhythmic effects of oral pimobendan in healthy cats; thus, it has been speculated that intravenous administration may be able to increase occurrence; however, studies have shown that this medication does not appear to have an influence, but further research is needed [161].
With respect to the use of pimobendan, Oldach et al. [162] carried out a study with the objective of analysing the pharmacological effects and tolerance of single-dose medication in cats with HCM. The authors evaluated 21 cats before and 90 minutes after the administration of 1.25 mg of pimobendan and 7 cats in the control group. In cats with HCM, the medication was able to promote an acute increase in left atrial and ventricular systolic function, and there was an increase in the LVOT velocity, which was well tolerated and without adverse effects [162]. With respect to LA, the benefits of pimobendan still require further study [163].
Schober et al. [164] conducted a study with the aim of evaluating the effects of pimobendan on sick cats with CHF. The authors reported that approximately 32% of cats with nonobstructive HCM achieved successful results after using the medication, and considering the obstruction conditions, the success rate was 28.6%. The use of pimobendan within 180 days did not guarantee any benefit to patients with HCM and CHF [164]. Therefore, the use of medication for patients with obstructive/nonobstructive HCM should be better evaluated. For stage D cats, the following is recommended: torasemide at a dose of 0.1–0.2 mg/kg PO q24h, in cases where the dose of furosemide used is > 6 mg/kg/day PO [4]; spironolactone at 1–2 mg/kg PO q12–24 h [165]; and pimobendan (0.625–1.25 mg/cat PO q12h) in cases of global LV dysfunction [166]. The use of torasemide in a single dose in cats is capable of promoting an increase in the diuresis process and the functioning of the renin angiotensin system (RAS), which has high bioavailability without major adverse effects that contraindicate its use [167]. In addition, dietary supplementation with 250 mg of taurine orally q12h is recommended [168]. High-sodium diets were avoided, body weight was controlled, and cachexia patients were removed [91]. Constant monitoring, including electrolytes (if potassium decreased, supplementation was needed) [4,91]. Recently, evidence has suggested that the acylcarnitine/free carnitine ratio is lower in cats with HCM, suggesting myocardial metabolic alterations and early stages of the disease [169], but further investigations are needed.
In cases where ATE is used, the possibility of euthanasia should be evaluated [42]; pain control with the opioids fentanyl (2.5 μg/kg bolus | 4–10 μg/h/h CRI), hydromorphone (0.08–0.3 mg/kg SQ, IM, IV q2–6 h), and methadone (0.1–0.3 mg/kg q12h IV/IM) [4,9]; anticoagulant treatment with low-molecular-weight heparin (100–200 IU/kg SC q12–24 h or 1.0–1.5 mg/kg SC q12–24 h); unfractionated heparin (150–250 IU/kg SC q6–8 h; 250 U/kg SC q6h); or rivaroxaban (2.5–5 mg PO q24h), a factor Xa inhibitor [72,75]. Heparin can be substituted for a factor Xa inhibitor combined with clopidogrel [4]. Thrombolytic therapy is not recommended for cats with ATE [170,171,172,173]. Lo et al. [173] carried out a study with the aim of verifying adverse effects through the combined administration of clopidogrel (18.75 mg PO q24h) and rivaroxaban (2.5 mg PO q24h) in 32 cats. The authors administered the medication in events such as ATE, intracardiac thrombosis or smoke. Approximately 5 cats showed adverse clinical signs, such as epistaxis, hematemesis, hematochezia or hematuria, without major complications [173]. The median survival intervals were 257 days for all cats, 502 days for those with ATE in one or more limbs (725 days) and 301 days for ATE in one limb [173]. The recurrence rate of ATE during treatment was 16.7%, and none of the cats developed recent ATE between the dual protocols, showing beneficial results through combined use [173]. Lo et al. [174] carried out a new study with 9 cats to compare the effects of antithrombotic treatment with clopidogrel, rivaroxaban or a combination of both in cats. The authors reported that the pharmacological combination promoted a reduction in platelet activity, the response to agonists and the production of thrombin in a safer and more effective way than either agent alone [174]. Recently, Jaturanratsamee et al. [175] reported that therapeutic strategies involving 2.5 mg/kg rivaroxaban every 24 h or the combination of 1 mg/kg injectable enoxaparin with 3 mg/kg oral clopidogrel every 24 h for 2 months prevented thrombus formation in cats with HCM. New therapies such as platelet integrin αIIbβ3 antagonists (abciximab and eptifibatide) and NETs may be useful for thromboprophylaxis, although further studies are needed [72].
It is recommended that cats start clopidogrel orally (initial dose of 75 mg orally, subsequent doses of 18.75 mg orally every 24 h) [4,68]. According to Matos & Payne [16], clopidogrel is the first-line medication for patients with ATE. According to Rishniw [176], in your viewpoint, clopidogrel reduces the risk of ATE by 3–4% for cats with moderately severe HCM; however, it is necessary to verify whether the benefit is advantageous because of factors such as difficulty in feline administration. In patients with CHF, the use of furosemide (1–2 mg/kg bolus | 0.6–1 mg/kg/h CRI) and oxygen supplementation are recommended if necessary [91]. Reassessments were made 3–7 days postdischarge and 1–2 weeks after the ATE event [4]. Variable monitoring, averaging 1–3 months, is used because of feline patient stress [4].
New therapeutic strategies have been developed with the aim of ensuring myocardial relaxation, reducing obstructive conditions and, to a certain extent, attenuating fibrotic events [146]. Currently, two medications considered small-molecule inhibitors, mavacamten and aficamten, which act on myosin ATPase and release energy for muscle contraction [146], have been studied. Mavacamten, after use in mouse models, prevented ventricular hypertrophy, disorganized cardiomyocytes and fibrotic events, and when it was used in mice with HCM, there was a decrease in ventricular thickness [146]. Compared with beta blockers and calcium channel blockers, mavacamten causes a decrease in the percentage of FS% without affecting heart rate [146]. In the case of aficamten, there is a decrease in pressure gradients and IVRT, with a beneficial diastolic effect [146].
In a study conducted by Sharpe et al. [177], 5 mixed-breed Maine Coon cats were treated with 2 mg/kg aficamten or placebo, and echocardiographic examinations were performed within 48 hours after administration. The authors reported that the administration of 2 mg/kg promoted a reduction in SF%, increased systolic ventricular dimensions and promoted a decrease in IVRT, indicating that smaller doses may be necessary and that new studies are needed to prove the ideal interval [177]. Sharpe et al. [178] carried out a dose reduction study (0.3 to 1 mg/kg) in 7 cats and reported that there was a dose-dependent reduction in left ventricular systolic function, IVRT and the pressure gradient in the LVOT. Furthermore, they emphasized that the most appropriate dose is in the range of 0.3-1 mg/kg, and studies are needed to evaluate the adverse effects of long-term administration [178]. Both medications are not used in cats, with aficamtem awaiting approval from the US Food and Drug Administration (FDA), and it is hypothesized that such drugs may offer benefits to cats with HCM [146].
Another substance that has been shown to potentially affect cats with HCM is rapamycin (the medication has completed all the technical phases required by the FDA for subclinical HCM, and the HALT HCM pivotal trial is ongoing; update as of 15th January 2025). Rapamycin is a macrolide produced by bacteria and is associated with the encoding of the TOR protein, which has a mammalian homologue, mTOR [179]. mTOR combines with various proteins and gives rise to multiprotein complexes known as mTORC1 and mTORC2, and sensitivity to rapamycin is variable [179]. mTORC1 is associated with positive regulation of protein and lipid synthesis and negative regulation of autophagy mechanisms, resulting in remodelling adaptation [179]. mTORC2 acts by regulating glucose and lipid metabolism, stabilizing cardiac physiology and ensuring the permanence of cardiomyocytes through changes in excess blood pressure [179]. Kaplan et al. [179] conducted a study with 43 cats with subclinical HCM in which rapamycin was administered at high and low doses in a randomized and placebo-controlled manner. The authors reported that the maximum ventricular thickness of cats after 180 days was lower for patients treated with low doses of rapamycin than for those treated with placebo, in addition to being well tolerated orally. However, studies are still needed to prove the preliminary effect of rapamycin in reducing ventricular thickness [179]. Recently, evidence points to the benefit of using CK-586, a cardiac myosin inhibitor, such that there is an improvement in LVOTO, an increase in the dimension of the ventricle in systole, a reduction in the SF% and ejection fraction without altering the frequency, with a therapeutic trend to be investigated [180].
9. Conclusions
Therefore, feline cardiomyopathies, especially those characterized by a hypertrophic phenotype, can induce serious changes. The associated symptoms range from mild to severe, which threatens the life expectancy of cats. There are still few studies dedicated to verifying the predictive factors associated with the occurrence of this disease. The pathophysiology of this disease involves mainly left ventricular dysfunction, which is characterized by concentric hypertrophy with a reduced lumen and associated hemodynamic changes. Genetic evidence has demonstrated the presence of an associated mutagenic component, mainly for some feline breeds. Early diagnosis and staging are essential for optimal therapeutic and nutritional management. In addition, monitoring these animals is necessary, as are routine check-ups to evaluate their condition. Treatment, despite being variable, aims to treat symptoms when present, prevent disease progression, ensure welfare and improve life expectancy. More studies are still needed to better understand the mutagenic behavior of this disease and to develop early diagnostic strategies and new forms of treatment.
Author Contributions
Conceptualization, F.G.d.S.; methodology, F.G.d.S.; validation, F.G.d.S., A.C.M., L.d.C. and S.B.; formal analysis, F.G.d.S., A.C.M., L.d.C. and S.B.; investigation, F.G.d.S., A.C.M., L.d.C. and S.B.; data curation, F.G.d.S. and A.C.M.; writing—original draft preparation, F.G.d.S., A.C.M.; writing—review and editing, F.G.d.S., A.C.M., L.d.C. and S.B.; visualization, F.G.d.S., A.C.M., L.d.C. and S.B.; supervision, S.B.; project administration, F.G.d.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
DMV MS Giovanni Canta for providing the echocardiography images.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| A31P | A31P mutation |
| ACE2 | angiotensin II-converting enzyme |
| ACVIM | American College of Veterinary Internal Medicine |
| ALMS1 | ALMS1 variant |
| AMC | arrhythmogenic cardiomyopathy |
| ANG II | angiotensin II |
| ANP | atrial natriuretic peptide |
| AO | aorta |
| ATE | arterial thromboembolism |
| BNP | B-type natriuretic peptide |
| cfDNA | cell-free DNA |
| CHF | chronic heart failure |
| citH3 | citrullinated histone H3 |
| CRI | continuous infusion |
| cTnI | cardiac troponin-I |
| DCM | dilated cardiomyopathy |
| ESC | European Society of Cardiology |
| FDA | Food and Drug Administration |
| HCM | hypertrophic cardiomyopathy |
| IL-6 | interleukin 6 |
| IV | intravenous |
| IVRT | isovolumetric relaxation |
| IVSd | interventricular septum in diastole |
| IVSs | interventricular septum in systole |
| LA | LA left atrium |
| LAA | left atrial appendage |
| LA/Ao | left atrium:aortic root ratio |
| LAMP | loop-mediated isothermal amplification assay |
| LFD | lateral flow dipstick |
| LOX | lysyl oxidase |
| LV | LV left ventricle |
| LVFW | left ventricle free wall thickness |
| LVFWd | left ventricle free wall thickness in diastole |
| LVFWs | left ventricle free wall thickness in systole |
| LVOT | left ventricular outflow tract |
| LVOTO | left ventricular outflow tract obstruction |
| MAPSE | mitral annular plane systolic excursion |
| MCP-1 | monocyte chemoattractant protein 1 |
| mTOR | mammalian homologue TOR protein |
| MYBPC3 | MYBPC3 gene |
| MYH7 | MYH7 gene |
| NETs | neutrophil extracellular traps |
| NLR | neutrophil/lymphocyte ratio |
| NTproANP | N-terminal pro-atrial natriuretic peptide |
| NTproBNP | N-terminal pro-B-type natriuretic peptide |
| PO | orally |
| PVF | pulmonary venous flow |
| R820W | R820W mutation |
| RA | right atrium |
| RAS | renin angiotensin system |
| RMC | restrictive cardiomyopathy |
| RV | right ventricle |
| RVOT | right ventricular outflow tract |
| SAM | systolic anterior movement |
| SF% | shortening fraction |
| SQ | subcutaneous |
| T4 | thyroxine |
| TGF-β | transforming growth factor beta |
| TNNT2 | TNNT2 intronic variant |
| TpTe | Tpeak–Tend |
| TT-LD | color-coded tissue tracking |
| VHS | vertebral heart size |
| VLAS | vertebral left atrial size |
References
- Garcia, R.C.M.; Amaku, M.; Biondo, A.W.; Ferreira, F. Dog and cat population dynamics in an urban area: evaluation of a birth control strategy. Pesq. Vet. Bras. 2018, 38, 511–518. [Google Scholar] [CrossRef]
- Reynolds, C.A.; Oyama, M.A.; Rush, J.E.; Rozanski, E.A.; Singletary, G.E.; Brown, D.C.; Cunningham, S.M.; Fox, P.R.; Bond, B.; Adin, D.B.; Williams, R.M.; MacDonald, K.A.; Malakoff, R.; Sleeper, M.M.; Schober, K.E.; Petrie, J.P.; Hogan, D.F. Perceptions of Quality of Life and Priorities of Owners of Cats with Heart Disease. J. Vet. Intern. Med. 2010, 24, 1421–1426. [Google Scholar] [CrossRef]
- Fox, P.R.; Keene, B.W.; Lamb, K.; Schober, K.A.; Chetboul, V.; Luis Fuentes, V.; Payne, J.R.; Wess, G.; Hogan, D.F.; Abbott, J.A.; Häggström, J.; Culshaw, G.; Fine-Ferreira, D.; Cote, E.; Trehiou-Sechi, E.; Motsinger-Reif, A.A.; Nakamura, R.K.; Singh, M.; Ware, W.A.; Riesen, S.C.; Borgarelli, M.; Rush, J.E.; Vollmar, A.; Lesser, M.B.; Van Israel, N.; Lee, P.M.; Bulmer, B.; Santilli, R.; Bossbaly, M.J.; Quick, N.; Bussadori, C.; Bright, J.; Estrada, A.H.; Ohad, D.G.; Del Palacio, M.J.F.; Brayley, J.L.; Schwartz, D.S.; Gordon, S.G.; Jung, S.; Bove, C.M.; Brambilla, P.G.; Moïse, N.S.; Stauthammer, C.D.; Stepien, R.L.; Quintavalla, C.; Amberger, C.; Manczur, F.; Hung, Y.W.; Lobetti, R.; De Swarte, M.; Tamborini, A.; Mooney, C.T.; Oyama, M.A.; Komolov, A.; Fujii, Y.; Pariaut, R.; Uechi, M.; Tachika Ohara, V.Y. International collaborative study to assess cardiovascular risk and evaluate long-term health in cats with preclinical hypertrophic cardiomyopathy and apparently healthy cats: The REVEAL Study. J. Vet. Intern. Med. 2018, 32, 930–943. [Google Scholar] [CrossRef]
- Luis Fuentes, V.; Abbott, J.; Chetboul, V.; Côté, E.; Fox, P.R.; Häggström, J.; Kittleson, M.D.; Schober, K.; Stern, J.A. ACVIM consensus statement guidelines for the classification, diagnosis, and management of cardiomyopathies in cats. J. Vet. Intern. Med. 2020, 34, 1–16. [Google Scholar] [CrossRef]
- Kittleson, M.D.; Côté, E. The feline cardiomyopathies 2. Hypertrophic cardiomyopathy. J. Feline Med. Surg. 2021, 23, 1028–1051. [Google Scholar] [CrossRef]
- Meurs, K.M.; Sanchez, X.; David, R.M.; Bowles, N.E.; Towbin, J.A.; Reiser, P.J.; Kittleson, J.A.; Munro, M.J.; Dryburgh, K.; Macdonald, K.A.; Kittleson, M.D. A cardiac myosin binding protein C mutation in the Maine Coon cat with familial hypertrophic cardiomyopathy. Hum. Mol. Genet. 2005, 14, 3587–3593. [Google Scholar] [CrossRef]
- Meurs, K.M.; Norgard, M.M.; Ederer, M.M.; Hendrix, K.P.; Kittleson, M.D. A substitution mutation in the myosin binding protein C gene in Ragdoll hypertrophic cardiomyopathy. Genomics. 2007, 90, 261–264. [Google Scholar] [CrossRef]
- Gil-Ortuño, C.; Sebastian-Marcos, P.; Sabater-Molina, M.; Nicolas-Rocamora, E.; Gimeno-Blanes, J.R.; Fernandez del Palacio, M.J. Genetics of feline hypertrophic cardiomyopathy. Clin. Genet. 2020, 98, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Kittleson, M.D.; Côté, E. The feline cardiomyopathies 1. General concepts. J. Feline Med. Surg. 2021, 23, 1009–1027. [Google Scholar] [CrossRef]
- Sukumolanan, P.; Petchdee, S. Feline hypertrophic cardiomyopathy: genetics, current diagnosis and management. Vet. Integr. Sci. 2020, 18, 61–73. [Google Scholar] [CrossRef]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef] [PubMed]
- Elliot, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; Monserrat, L.; Pankuweit, S.; Rapezzi, C.; Seferovic, P.; Tavazzi, L.; Keren, A. Classification of the cardiomyopathies: a position statement from the European society of cardiology working group on myocardial and pericardial diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef]
- Gersh, B.J.; Maron, B.J.; Bonow, R.O.; Dearani, J.A.; Fifer, M.A.; Link, M.S.; Naidu, S.S.; Nishimura, R.A.; Ommen, S.R.; Rakowski, H.; Seidman, C.E.; Towbin, J.A.; Udelson, J.E.; Yancy, C.W. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy. Circulation. 2011, 124, 2761–2796. [Google Scholar] [CrossRef]
- Barroso, C.D.N.; Caminotto, E.L.; Calahani, A.; Silveira, M.F. Sobrevida e características ecocardiográficas de gatos com e sem cardiomiopatias. R. Bras. Ci. Vet. 2020, 27, 175–182. [Google Scholar] [CrossRef]
- Rivas, V.N.; Stern, J.A.; Ueda, Y. The Role of Personalized Medicine in Companion Animal Cardiology. Vet. Clin. North Am. Small Anim. Pract. 2023, 53, 1255–1276. [Google Scholar] [CrossRef]
- Matos, J.N.; Payne, J.R. Predicting Development of Hypertrophic Cardiomyopathy and Disease Outcomes in Cats. Vet. Clin. North Am. Small Anim. Pract. 2023, 53, 1277–1292. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Fox, P.R. Hypertrophic cardiomyopathy in man and cats. J. Vet. Cardiol. 2015, 17, S6–S9. [Google Scholar] [CrossRef]
- Kiatsilapanan, A.; Surachetpong, S.D. Assessment of left atrial function in feline hypertrophic cardiomyopathy by using two-dimensional speckle tracking echocardiography. BMC Vet. Res. 2020, 16, 334. [Google Scholar] [CrossRef] [PubMed]
- Franchini, A.; Abbott, J.A.; Lahmers, S.; Eriksson, A. Clinical characteristics of cats referred for evaluation of subclinical cardiac murmurs. J. Feline Med. Surg. 2021, 23, 708–714. [Google Scholar] [CrossRef]
- Argenta, F.F.; Mello, L.S.; Cony, F.G.; Pavarini, S.P.; Driemeier, D.; Sonne, L. Epidemiological and pathological aspects of cardiomiopatias in cats in southern Brazil. Pesq. Vet. Bras. 2020, 40, 389–398. [Google Scholar] [CrossRef]
- Payne, J.R.; Borgeat, K.; Brodbelt, D.C.; Connoly, D.J.; Luis Fuentes, V. Risk factors associated with sudden death vs. congestive heart failure or arterial thromboembolism in cats with hypertrophic cardiomyopathy. J. Vet. Cardiol. 2015, 17, S318–S328. [Google Scholar] [CrossRef] [PubMed]
- Matos, J.N.; Payne, J.R.; Seo, J.; Luis Fuentes, V. Natural history of hypertrophic cardiomyopathy in cats from rehoming centers: The CatScan II study. J. Vet. Intern. Med. 2022, 36, 1900–1912. [Google Scholar] [CrossRef] [PubMed]
- Matos, J.N.; Payne, J.R.; Mullins, J.; Luis Fuentes, V. Isolated discrete upper septal thickening in a nonreferral cat population of senior and young cats. J. Vet. Cardiol. 2023, 50, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Owen, R.; Hunt, H.; Luis Fuentes, V.; Connolly, D.J.; Munday, J.S. Prevalence of cardiomyopathy and cardiac mortality in a colony of nonpurebred cats in New Zealand. N. Z. Vet. J. 2025, 73, 1–9. [Google Scholar] [CrossRef]
- Longeri, M.; Ferrari, P.; Knafelz, P.; Mezzelani, A.; Marabotti, A.; Milanesi, L.; Pertica, G.; Polli, M.; Brambilla, P.G.; Kittleson, M.; Lyons, L.A.; Porciello, F. Myosin-Binding Protein C DNA Variants in Domestic Cats (A31P, A74T, R820W) and their Association with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2013, 27, 275–285. [Google Scholar] [CrossRef]
- Freeman, L.M.; Rush, J.E.; Stern, J.A.; Huggins, G.S.; Maron, M.S. Feline hypertrophic cardiomyopathy: a spontaneous large animal model of human HCM. Cardiol. Res. 2017, 8, 139–142. [Google Scholar] [CrossRef]
- Fox, P.R.; Keene, B.W.; Lamb, K.; Schober, K.A.; Chetboul, V.; Luis Fuentes, V.; Wess, G.; Payne, J.R.; Hogan, D.F.; Motsinger-Reif, A.; Häggström, J.; Trehiou-Sechi, E.; Fine-Ferreira, D.M.; Nakamura, R.K.; Lee, P.M.; Singh, M.K.; Ware, W.A.; Abbott, J.A.; Culshaw, G.; Riesen, S.; Borgarelli, M.; Lesser, M.B.; Van Israël, N.; Côté, E.; Rush, J.E.; Bulmer, B.; Santilli, R.A.; Vollmar, A.C.; Bossbaly, M.J.; Quick, N.; Bussadori, C.; Bright, J.M.; Estrada, A.H.; Ohad, D.G.; Fernández-Del Palacio, M.J.; Lunney Brayley, J.; Schwartz, D.S.; Bové, C.M.; Gordon, S.G.; Jung, S.W.; Brambilla, P.; Moïse, N.S.; Stauthammer, C.D.; Stepien, R.L.; Quintavalla, C.; Amberger, C.; Manczur, F.; Hung, Y.W.; Lobetti, R.; De Swarte, M.; Tamborini, A.; Mooney, C.T.; Oyama, M.A.; Komolov, A.; Fujii, Y.; Pariaut, R.; Uechi, M.; Tachika Ohara, V.Y. International collaborative study to assess cardiovascular risk and evaluate long-term health in cats with preclinical hypertrophic cardiomyopathy and apparently healthy cats: The REVEAL Study. J. Vet. Intern. Med. 2018, 32, 930–943. [Google Scholar] [CrossRef]
- Fries, R. Hypertrophic Cardiomyopathy-Advances in Imaging and Diagnostic Strategies. Vet. Clin. North Am. Small Anim. Pract. 2023, 53, 1325–1342. [Google Scholar] [CrossRef]
- Messer, A.E.; Chan, J.; Daley, A.; Copeland, O.; Marston, S.B.; Connoly, D.J. Investigations into the Sarcomeric Protein and Ca2+-Regulation Abnormalities Underlying Hypertrophic Cardiomyopathy in Cats (Felix catus). Front. Physiol. 2017, 8, 348. [Google Scholar] [CrossRef]
- Stern, J.A.; Ueda, Y. Inherited cardiomyopathies in veterinary medicine. Pflug. Arch. 2019, 471, 745–753. [Google Scholar] [CrossRef]
- Chetboul, V.; Petit, A.; Gouni, V.; Trehiou-Sechi, E.; Misbach, C.; Balouka, D.; Sampedrano, C.C.; Pouchelon, J.-L.; Tissier, R.; Abitbol, M. Prospective echocardiographic and tissue Doppler screening of a large Sphynx cat population: reference ranges, heart disease prevalence and genetic aspects. J. Vet. Cardiol. 2012, 14, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Borgeat, K. , Stern, J., Meurs, K.M., Fuentes, V.L., Connolly, D.J. The influence of clinical and genetic factors on left ventricular wall thickness in ragdoll cats. J. Vet. Cardiol. 2015, 17, S258–S267. [Google Scholar] [CrossRef]
- Kittleson, M.D.; Meurs, K.M.; Harris, S.P. The genetic basis of hypertrophic cardiomyopathy in cats and humans. J. Vet. Cardiol. 2015, 17, S53–S73. [Google Scholar] [CrossRef] [PubMed]
- Brizard, D.; Amberger, C.; Hartnack, S.; Doherr, M.G.; Lombard, C. Phenotypes and echocardiographic characteristics of a European population of domestic shorthair cats with idiopathic hypertrophic cardiomyopathy. Schweiz Arch. Tierheilkd. 2009, 151, 529–538. [Google Scholar] [CrossRef]
- Luis Fuentes, V.; Wilkie, L.J. Asymptomatic Hypertrophic Cardiomyopathy: Diagnosis and Therapy. Vet. Clin. Small. Anim. 2017, 47, 1041–1054. [Google Scholar] [CrossRef] [PubMed]
- Tilley, L.P.; Liu, S.K.; Gilbertson, S.R.; Wagner, B.M.; Lord, P.F. Primary myocardial disease in the cat: A model for human cardiomyopathy. Am. J. Pathol. 1977, 86, 493–522. [Google Scholar]
- Kittleson, M.D.; Meurs, K.M.; Munro, M.J.; Kittleson, J.A.; Liu, S.K.; Pion, P.D.; Towbin, J.A. Familial hypertrophic cardiomyopathy in Maine coon cats: an animal model of human disease. Circulation. 1999, 99, 3172–3180. [Google Scholar] [CrossRef]
- Stern, J.A.; Rivas, V.N.; Kaplan, J.L.; Ueda, Y.; Oldach, M.S.; Ontiveros, E.S.; Kooiker, K.B.; van Dijk, S.J.; Harris, S.P. Hypertrophic cardiomyopathy in purpose-bred cats with the A31P mutation in cardiac myosin binding protein-C. Sci. Rep. 2023, 13, 10319. [Google Scholar] [CrossRef]
- O'Donnell, K.; Adin, D.; Atkins, C.E.; DeFrancesco, T.; Keene, B.W.; Tou, S.; Meurs, K.M. Absence of known feline MYH7 and MYBPC3 variants in a diverse cohort of cats with hypertrophic cardiomyopathy. Anim. Genet. 2021, 52, 542–544. [Google Scholar] [CrossRef]
- Ontiveros, E.S.; Ueda, Y.; Harris, S.P.; Stern, J.A. Precision medicine validation: identifying the MYBPC3 A31P variant with whole-genome sequencing in two Maine Coon cats with hypertrophic cardiomyopathy. J. Feline Med. Surg. 2019, 21, 1086–1093. [Google Scholar] [CrossRef]
- Sukumolanan, P.; Demeekul, K.; Petchdee, S. Development of a Loop-Mediated Isothermal Amplification Assay Coupled with a Lateral Flow Dipstick Test for Detection of Myosin Binding Protein C3 A31P Mutation in Maine Coon Cats. Front. Vet. Sci. 2022, 9, 819694. [Google Scholar] [CrossRef] [PubMed]
- Borgeat, K.; Casamian-Sorrosal, D.; Helps, C.; Luis Fuentes, V.; Connolly, D.J. Association of the myosin binding protein C3 mutation (MYBPC3 R820W) with cardiac death in a survey of 236 ragdoll cats. J. Vet. Cardiol. 2014, 16, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Meurs, K.M.; Williams, B.G.; DeProspero, D.; Friedenberg, S.G.; Malarkey, D.E.; Ezzell, J.A.; Ezzell, J.A.; Keene, B.W.; Adin, D.B.; DeFrancesco, T.C.; Tou, S. A deleterious mutation in the ALMS1 gene in a naturally occurring model of hypertrophic cardiomyopathy in the Sphynx cat. Orphanet. J. Rare Dis. 2021, 16, 108. [Google Scholar] [CrossRef] [PubMed]
- Turba, M.E.; Ferrari, P.; Milanesi, R.; Gentilini, R.; Longeri, M. HCM-associated ALMS1 variant: Allele drop-out and frequency in Italian Sphynx cats. Anim. Genet. 2023, 54, 643–646. [Google Scholar] [CrossRef]
- Akiyama, N.; Suzuki, R.; Saito, T.; Yuchi, Y.; Ukawa, H.; Matsumoto, Y. Presence of known feline ALMS1 and MYBPC3 variants in a diverse cohort of cats with hypertrophic cardiomyopathy in Japan. PLoS ONE. 2023, 18, e0283433. [Google Scholar] [CrossRef]
- Seo, J.; Loh, Y.; Connolly, D.J.; Luis Fuentes, V.; Dutton, E.; Hunt, H.; Munday, J.S. Prevalence of Hypertrophic Cardiomyopathy and ALMS1 Variant in Sphynx Cats in New Zealand. Animals (Basel). 2024, 14, 2629. [Google Scholar] [CrossRef]
- Demeekul, K.; Sukumolanan, P.; Panprom, C.; Thaisakun, S.; Roytrakul, S.; Petchdee, S. Echocardiography and MALDI-TOF Identification of Myosin-Binding Protein C3 A74T Gene Mutations Involved Healthy and Mutated Bengal Cats. Animals (Basel). 2022, 12, 1782. [Google Scholar] [CrossRef] [PubMed]
- Sukumolanan, P.; Petchdee, S. Prevalence of cardiac myosin-binding protein C3 mutations in Maine Coon cats with hypertrophic cardiomyopathy. Vet. World. 2022, 15, 502–508. [Google Scholar] [CrossRef]
- Schipper, T.; Ohlsson, Å.; Longeri, M.; Hayward, J.J.; Mouttham, L.; Ferrari, P.; Smets, P.; Ljungvall, I.; Häggström, J.; Stern, J.A.; Lyons, L.A.; Peelman, L.J.; Broeckx, B.J.G. The TNNT2:c.95-108G>A variant is common in Maine Coons and shows no association with hypertrophic cardiomyopathy. Anim. Genet. 2022, 53, 526–529. [Google Scholar] [CrossRef]
- Grzeczka, A.; Graczyk, S.; Pasławski, R.; Pasławska, U. Genetic Basis of Hypertrophic Cardiomyopathy in Cats. Curr. Issues Mol. Biol. 2024, 46, 8752–8766. [Google Scholar] [CrossRef]
- Sciagrà, R. Positron-emission tomography myocardial blood flow quantification in hypertrophic cardiomyopathy. Q. J. Nucl. Med. Mol. Imaging. 2016, 60, 354–361. [Google Scholar] [PubMed]
- Patata, V.; Caivano, D.; Porciello, F.; Rishniw, M.; Domenech, O.; Marchesotti, F.; Marchesotti, F.; Giorgi, M.E.; Guglielmini, C.; Poser, H.; Spina, F.; Birettoni, F. Pulmonary vein to pulmonary artery ratio in healthy and cardiomyopathic cats. J. Vet. Cardiol. 2020, 27, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Schober, K.E.; Savino, S.I.; Yildiz, V. Right ventricular involvement in feline hypertrophic cardiomyopathy. J. Vet. Cardiol. 2016, 18, 297–309. [Google Scholar] [CrossRef]
- Visser, L.C.; Sloan, C.Q.; Stern, J.A. Echocardiographic assessment of right ventricular size and function in cats with hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2017, 31, 668–677. [Google Scholar] [CrossRef]
- Häggström, J.; Fuentes, L.V.; Wess, G. Screening for hypertrophic cardiomyopathy in cats. J. Vet. Cardiol. 2015, 17, 134–149. [Google Scholar] [CrossRef]
- Parato, V.M.; Antoncecchi, V.; Sozzi, F.; Marazia, S.; Zito, A.; Maiello, M.; Palmiero, P.; ISCU. Echocardiographic diagnosis of the different phenotypes of hypertrophic cardiomyopathy. Cardiovasc. Ultrasound. 2016, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Joshua, J.; Caswell, J.; O'Sullivan, M.L.; Wood, G.; Fonfara, S. Feline myocardial transcriptome in health and in hypertrophic cardiomyopathy-A translational animal model for human disease. PLoS One. 2023, 18, e0283244. [Google Scholar] [CrossRef] [PubMed]
- Colpitts, M.E.; Caswell, J.L.; Monteith, G.; Joshua, J.; O'Sullivan, M.L.; Raheb, S.; Fonfara, S. Cardiac gene activation varies between young and adult cats and in the presence of hypertrophic cardiomyopathy. Res. Vet. Sci. 2022, 152, 38–47. [Google Scholar] [CrossRef]
- Rodriguez, J.M.M.; Fonfara, S.; Hetzel, U.; Kipar, A. Feline hypertrophic cardiomyopathy: reduced microvascular density and involvement of CD34+ interstitial cells. Vet. Pathol. 2022, 59, 269–283. [Google Scholar] [CrossRef]
- Lean, F.Z.X.; Priestnall, S.L.; Vitores, A.G.; Suárez-Bonnet, A.; Brookes, S.M.; Núñez, A. Elevated angiotensin-converting enzyme 2 (ACE2) expression in cats with hypertrophic cardiomyopathy. Res. Vet. Sci. 2022, 152, 564–568. [Google Scholar] [CrossRef]
- Ward, J.L.; Lisciandro, G.R.; Ware, W.A.; Viall, A.K.; Aona, B.D.; Kurtz, K.A.; Reina-Doreste, Y.; DeFrancesco, T.C. Evaluation of point-of-care thoracic ultrasound and NT-proBNP for the diagnosis of congestive heart failure in cats with respiratory distress. J. Vet. Intern. Med. 2018, 32, 1530–1540. [Google Scholar] [CrossRef]
- Follby, A.; Pettersson, A.; Ljungvall, I.; Ohlsson, Å.; Häggström, J. A Questionnaire Survey on Long-Term Outcomes in Cats Breed-Screened for Feline Cardiomyopathy. Animals (Basel). 2022, 12, 2782. [Google Scholar] [CrossRef] [PubMed]
- Le Boedec, K.; Arnaud, C.; Chetboul, V.; Trehiou-Sechi, E.; Pouchelon, J.L.; Gouni, V.; Reynolds, B.S. Relationship between paradoxical breathing and pleural diseases in dyspneic dogs and cats: 389 cases (2001-2009). J. Am. Vet. Med. Assoc. 2012, 240, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D.; Little, C.J.L.; Harris, J.; Rishniw, M. Rapid assessment with physical examination in dyspnoeic cats: the RAPID CAT study. J. Small Anim. Pract. 2018, 59, 75–84. [Google Scholar] [CrossRef]
- Brugada-Terradellas, C.; Hellemans, A.; Brugada, P.; Smets, P. Sudden cardiac death: A comparative review of humans, dogs and cats. Vet. J. 2021, 274, 105696. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, V.; Mey, C.; Vonfeld, I.; Chamagne, A.; Alvarado, M.-P.; Cadoré, J.-L.; Chetboul, V.; Desquilbet, L. Systolic third sound associated with systolic anterior motion of the mitral valve in cats with obstructive hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2023, 37, 1679–1684. [Google Scholar] [CrossRef]
- Paige, C.F.; Abbott, J.A.; Elvinger, F.; Pyle, R.L. Prevalence of cardiomyopathy in apparently healthy cats. J. Am. Vet. Med. Assoc. 2009, 234, 1398–1403. [Google Scholar] [CrossRef]
- Wagner, T.; Luis Fuentes, V.; Payne, J.R.; McDermott, N.; Brodbelt, D. Comparison of auscultatory and echocardiographic findings in healthy adult cats. J. Vet. Cardiol. 2010, 12, 171–182. [Google Scholar] [CrossRef]
- Pellegrino, A. Cardiomiopatias em felinos. In Tratado de Cardiologia de Cães e Gatos, 1st ed.; Larsson, M.H.M.A., Ed. Interbook: São Paulo, Brazil, 2020: Volume 1, pp.
- Nonn, T.; Adisaisakundet, I.; Chairit, K.; Choksomngam, S.; Hunprasit, V.; Jeamsripong, S.; Surachetpong, S.D. Parameters related to diagnosing hypertrophic cardiomyopathy in cats. Open Vet. J. 2024, 14, 2407–2414. [Google Scholar] [CrossRef]
- Vliegenthart, T.; Szatmári, V. A New, Easy-to-Learn, Fear-Free Method to Stop Purring During Cardiac Auscultation in Cats. Animals (Basel). 2025, 15, 236. [Google Scholar] [CrossRef]
- Shaverdian, M.; Li, R.H.L. Preventing Cardiogenic Thromboembolism in Cats Literature Gaps, Rational Recommendations, and Future Therapies. Vet. Clin. North Am. Small Anim. Pract. 2023, 53, 1309–1323. [Google Scholar] [CrossRef] [PubMed]
- Shaverdian, M.; Nguyen, N.; Li, R.H.L. A novel technique to characterize procoagulant platelet formation and evaluate platelet procoagulant tendency in cats by flow cytometry. Front. Vet. Sci. 2024, 11, 1480756. [Google Scholar] [CrossRef] [PubMed]
- Poredos, P.; Jezovnik, M.K. Endothelial Dysfunction and Venous Thrombosis. Angiology 2017, 69, 564–567. [Google Scholar] [CrossRef]
- Hogan, D.F. Feline Cardiogenic Arterial Thromboembolism Prevention and Therapy. Vet. Clin. Small Anim. 2017, 47, 1065–1082. [Google Scholar] [CrossRef]
- Holm, J.K.; Kellett, J.G.; Jensen, N.H.; Hansen, S.N.; Jensen, K.; Brabrand, M. Prognostic value of infrared thermography in an emergency department. Eur. J. Emerg. Med. 2018, 25, 204–208. [Google Scholar] [CrossRef]
- Pavelková, E. Feline arterial thromboembolism. Companion animal, 2019, 24, 426–430. [Google Scholar] [CrossRef]
- Luis Fuentes, V. Arterial thromboembolism Risks, realities and a rational first-line approach. J. Feline Med. Surg. 2012, 14, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.F.; Fox, P.R.; Jacob, K.; Keene, B.; Laste, N.J.; Rosenthal, S.; Sederquist, K.; Weng, H.-Y. Secondary prevention of cardiogenic arterial thromboembolism in the cat: the double-blind, randomized, positive-controlled feline arterial thromboembolism; clopidogrel vs. aspirin trial (FAT CAT). J. Vet. Cardiol. 2015, 17, S306–S317. [Google Scholar] [CrossRef]
- Schaefer, G.C.; Veronezi, T.M.; Luz, C.G.; Gutierrez, L.G.; Scherer, S.; Pavarini, S.P.; Costa, F.V.A. Arterial thromboembolism of noncardiogenic origin in a domestic feline with ischemia and reperfusion syndrome. Semin. Cienc. Agrar. 2020, 41, 717–724. [Google Scholar] [CrossRef]
- Silva, D.M.; Caramalac, S.M.; Caramalac, S.M.; Gimelli, A.; Palumbo, M.I.P. Feline Aortic Thromboembolism Diagnosed by Thermography. Acta Vet. Sci. 2022, 50, 752. [Google Scholar] [CrossRef]
- Herrold, E.; Schober, K.; Miller, J.; Jennings, R. Systemic reactive angioendotheliomatosis mimicking hypertrophic cardiomyopathy in a domestic shorthair cat. J. Vet. Cardiol. 2024, 56, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Janus, I.; Noszczyk-Nowak, A.; Bubak, J.; Tursi, M.; Vercelli, C.; Nowak, M. Comparative cardiac macroscopic and microscopic study in cats with hyperthyroidism vs. cats with hypertrophic cardiomyopathy. Vet. Q. 2023, 43, 1–11. [Google Scholar] [CrossRef]
- Lee, H.; Lee, D.; Park, J.; Yun, T.; Koo, Y.; Chae, Y.; Kang, B.-T.; Yang, M.-P.; Kim, H. Heart failure in a cat due to hypertrophic cardiomyopathy phenotype caused by chronic uncontrolled hyperthyroidism. Acta Vet. Hung. 2023, 71, 96–100. [Google Scholar] [CrossRef]
- Little, S.; Levy, J.; Hartmann, K.; Hofmann-Lehmann, R.; Hosie, M.; Olah, G.; Hofmann-Lehmann, R.; Hosie, M.; Olah, G.; Denis, K.S. 2020 AAFP Feline Retrovirus Testing and Management Guidelines. J. Feline Med. Surg. 2020, 22, 5–30. [Google Scholar] [CrossRef]
- Gavazza, A.; Marchegiani, A.; Guerriero, L.; Turinelli, V.; Spaterna, A.; Mangiaterra, S.; Galosi, L.; Rossi, G.; Cerquetella, M. Updates on Laboratory Evaluation of Feline Cardiac Diseases. Vet. Sci. 2021, 8, 1–15. [Google Scholar] [CrossRef]
- Fries, R.C.; Kadotani, S.; Stack, J.P.; Kruckman, L.; Wallace, G. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Cats with Hypertrophic Cardiomyopathy. Front. Vet. Sci. 2022, 9, 813524. [Google Scholar] [CrossRef] [PubMed]
- Navarro, I.; Summers, S.; Rishniw, M.; Quimby, J. Cross-sectional survey of noninvasive indirect blood pressure measurement practices in cats by veterinarians. J. Feline Med. Surg. 2022, 2, 1–8. [Google Scholar] [CrossRef]
- Oura, T.J.; Young, A.N.; Keene, B.W.; Robertson, I.D.; Jennings, D.E.; Thrall, D.E. A Valentine-Shaped Cardiac Silhouette in Feline Thoracic Radiographs is Primarily due to Left Atrial Enlargement. Vet. Radiol. Ultrasound. 2015, 56, 245–250. [Google Scholar] [CrossRef]
- Guglielmini, C.; Diana, A. Thoracic radiography in the cat: Identification of cardiomegaly and congestive heart failure. J. Vet. Cardiol. 2015, 17, S87–S101. [Google Scholar] [CrossRef]
- Côtè, E. Feline Congestive Heart Failure Current Diagnosis and Management. Vet. Clin. Small Anim. 2017, 47, 1055–1064. [Google Scholar] [CrossRef]
- Payne, J.R.; Borgeat, K.; Connoly, D.J.; Boswood, A.; Dennis, S.; Wagner, T.; Menaut, P.; Maerz, I.; Evans, D.; Simons, V.E.; Brodbelt, D.C.; Luis Fuentes, V. Prognostic Indicators in Cats with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2013, 27, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, D.; Park, S.; Suh, G.H.; Choi, J. Radiographic findings of cardiopulmonary structures can predict hypertrophic cardiomyopathy and congestive heart failure in cats. Am. J. Vet. Res. 2023, 84, ajvr.23–01.0017. [Google Scholar] [CrossRef]
- Rho, J.; Shin, S.-M.; Jhang, K.; Lee, G.; Song, K.-H.; Shin, H. Deep learning-based diagnosis of feline hypertrophic cardiomyopathy. PLoS One. 2023, 18, e0280438. [Google Scholar] [CrossRef]
- Schober, K.E.; Zientek, J.; Li, X.; Luis Fuentes, V.; Bonagura, J.D. Effect of treatment with atenolol on 5-year survival in cats with preclinical (asymptomatic) hypertrophic cardiomyopathy. J. Vet. Cardiol. 2013, 15, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.D.; Giglio, R.F.; Berry, C.R.; Reese, D.J.; Maisenbacher, H.W.; Hernandez, J.A. Associations between 'valentine' heart shape, atrial enlargement and cardiomyopathy in cats. J. Feline Med. Surg. 2014, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Diana, A.; Perfetti, S.; Valente, C.; Toaldo, M.B.; Pey, P.; Cipone, M.; Poser, H.; Guglielmini, C. Radiographic features of cardiogenic pulmonary edema in cats with left-sided cardiac disease: 71 cases. J. Feline Med. Surg. 2022, 24, e568–579. [Google Scholar] [CrossRef]
- Litster, A.L.; Buchanan, W. Vertebral scale system to measure heart size in radiographs of cats. Am. Vet. Med. Assoc. 2000, 216, 210–214. [Google Scholar] [CrossRef]
- Jackson, B.L.; Lehmkuhl, L.B.; Adin, D.B. Heart rate and arrhythmia frequency of normal cats compared to cats with asymptomatic hypertrophic cardiomyopathy. J. Vet. Cardiol. 2014, 16, 215–225. [Google Scholar] [CrossRef]
- Oliveira, C.S.; Pinto, A.C.B.C.F.; Itikawa, P.H.; Júnior, F.F.L.; Goldfeder, G.T.; Larsson, M.H.M.A. Radiographic evaluation of cardiac silhouette in healthy Maine Coon cats. Semin: Ciênc. Agrar. 2014, 35, 2501–2506. [Google Scholar] [CrossRef]
- Hanås, S.; Tidholm, A.; Holst, B.S. Ambulatory electrocardiogram recordings in cats with primary asymptomatic hypertrophic cardiomyopathy. J. Feline Med. Surg. 2015, 19, 1–7. [Google Scholar] [CrossRef]
- Romito, G.; Gugliemini, C.; Mazzarella, M.O.; Cipone, M.; Diana, A.; Contiero, B.; Baron Toaldo, M. Diagnostic and prognostic utility of surface electrocardiography in cats with left ventricular hypertrophy. J Vet Cardiol 2018, 20, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Sidler, M.; Santarelli, G.; Kovacevic, A.; Matos, J.N.; Schreiber, N.; Toaldo, N.B. Ventricular preexcitation in cats: 17 cases. J. Vet. Cardiol. 2023, 47, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Murphy, L.A.; Nakamura, R.K. Pre-excitation alternans in a cat. J. Vet. Cardiol. 2025, 58, 13–16. [Google Scholar] [CrossRef]
- Bastos, R.F.; Tuleski, G.L.R.; Franco, L.F.C.; Sousa, M.G. Tpeak-Tend, a novel electrocardiographic marker in cats with hypertrophic cardiomyopathy-a brief communication. Vet. Res. Commun. 2023, 47, 559–565. [Google Scholar] [CrossRef]
- Seo, J.; Kurosawa, T.A.; Borgeat, K.; Novo Matos, J.; Hutchinson, J.C.; Arthurs, O.J.; Fuentes, V.L. Clinical signs associated with severe ST segment elevation in three cats with a hypertrophic cardiomyopathy phenotype. J. Vet. Cardiol. 2024, 54, 30–37. [Google Scholar] [CrossRef]
- Bastos, R.F.; Tuleski, G.L.R.; Sousa, M.G. QT interval instability and QRS interval dispersion in healthy cats and cats with a hypertrophic cardiomyopathy phenotype. J. Feline Med. Surg. 2023, 25, 1098612X231151479. [Google Scholar] [CrossRef]
- Oricco, S.; Quintavalla, C.; Apolloni, I.; Crosara, S. Bradyarrhythmia after treatment with atenolol and mirtazapine in a cat with hypertrophic cardiomyopathy. J. Vet. Cardiol. 2024, 53, 72–76. [Google Scholar] [CrossRef]
- Cofaru, A.; Murariu, R.; Popa, T.; Peștean, C.P.; Scurtu, I.C. The Unseen Side of Feline Hypertrophic Cardiomyopathy: Diagnostic and Prognostic Utility of Electrocardiography and Holter Monitoring. Animals (Basel). 2024, 14, 2165. [Google Scholar] [CrossRef] [PubMed]
- Bartoszuk U; Keene BW; Baron Toaldo M; Pereira N; Summerfield N; Novo Matos J; Glaus, T. M. Holter monitoring demonstrates that ventricular arrhythmias are common in cats with decompensated and compensated hypertrophic cardiomyopathy. Vet. J. 2019, 243, 21–25. [Google Scholar] [CrossRef]
- Tse, Y.C.; Rush, J.E.; Cunningham, S.M.; Bulmer, B.J.; Freeman, L.M.; Rozanski, E.A. Evaluation of a training course in focused echocardiography for noncardiology house officers. J. Vet. Emerg. Crit. Care. 2013, 23, 268–273. [Google Scholar] [CrossRef]
- Abbott, J.A.; MacLean, H.N. Two-Dimensional Echocardiographic Assessment of the Feline Left Atrium. J. Vet. Intern. Med. 2006, 20, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Chetboul, V.; Passavin, P.; Trehiou-Sechi, E.; Gouni, V.; Poissinnier, C.; Pouchelon, J.-L.; Desquilbet, L. Clinical, epidemiological and echocardiographic features and prognostic factors in cats with restrictive cardiomyopathy: A retrospective study of 92 cases (2001-2015). J. Vet. Intern. Med. 2019, 33, 1222–1231. [Google Scholar] [CrossRef]
- Maerz, I.; Schober, K.; Oechtering, G. Echocardiographic measurement of left atrial dimension in healthy cats and cats with left ventricular hypertrophy. Tieraerztl. Prax. Ausg. K. Kleintiere. Heimtiere. 2006, 34, 331. [Google Scholar]
- Schober, K.E.; Maerz, I. Assessment of left atrial appendage flow velocity and its relation to spontaneous echocardiographic contrast in 89 cats with myocardial disease. J. Vet. Intern. Med. 2006, 20, 120–130. [Google Scholar] [CrossRef]
- Matos, J.N.; Sargent, J.; Silva, J.; Payne, J.R.; Seo, J.; Spalla, I. Thin and hypokinetic myocardial segments in cats with cardiomyopathy. J. Vet. Cardiol. 2023, 46, 5–17. [Google Scholar] [CrossRef]
- Colakoglu, E.; Sevim, K.; Kaya, U. Short communication Assessment of left atrial size, left atrial volume and left ventricular function, and its relation to spontaneous echocardiographic contrast in cats with hypertrophic cardiomyopathy: A preliminary study. Pol. J. Vet. Sci, 2024, 27, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Novo Matos, J.; Munday, J.S.; Hunt, H.; Connolly, D.J.; Luis Fuentes, V. Longitudinal assessment of systolic anterior motion of the mitral valve in cats with hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2024, 38, 2982–2993. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Matos, J.M.; Payne, J.R.; Luis Fuentes, V.; Connolly, D.J. Anterior mitral valve leaflet length in cats with hypertrophic cardiomyopathy. J. Vet. Cardiol. 2021, 37, 62–70. [Google Scholar] [CrossRef]
- Velzen, H.G.; Schinkel, A.F.L.; Menting, M.E.; Bosch, A.E.V.D.; Michels, M. Prognostic significance of anterior mitral valve leaflet length in individuals with a hypertrophic cardiomyopathy gene mutation without hypertrophic changes. J. Ultrasound. 2018, 21, 217–224. [Google Scholar] [CrossRef]
- Spalla, I.; Payne, J.R.; Borgeat, K.; Pope, A.; Luis Fuentes, V.; Connoly, D.J. Mitral Annular Plane Systolic Excursion and Tricuspid Annular Plane Systolic Excursion in Cats with Hypertrophic Cardiomyopathy. J. Vet. Intern. Med. 2017, 31, 691–699. [Google Scholar] [CrossRef]
- Schober, K.E.; Chetboul, V. Echocardiographic evaluation of left ventricular diastolic function in cats: Hemodynamic determinants and pattern recognition. J. Vet. Cardiol. 2015, 17, S102–33. [Google Scholar] [CrossRef] [PubMed]
- Dutton, L.C.; Spalla, I.; Seo, J.; Silva, J.; Matos, J.N. Aortic annular plane systolic excursion in cats with hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2024, 38, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Bach, M.B.T.; Grevsen, J.R.; Kiely, M.A.B.; Willesen, J.L.; Koch, J. Detection of congestive heart failure by mitral annular displacement in cats with hypertrophic cardiomyopathy - concordance between tissue Doppler imaging-derived tissue tracking and M-mode. J. Vet. Cardiol. 2021, 36, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Crosara, S.; Allodi, G.; Guazzetti, S.; Oricco, S.; Borgarelli, M.; Corsini, A.; Quintavalla, C. Aorto-septal angle, isolated basal septal hypertrophy, and systolic murmur in 122 cats. J. Vet. Cardiol. 2023, 46, 30–39. [Google Scholar] [CrossRef]
- Spalla, I.; Boswood, A.; Connolly, D.J.; Luis Fuentes, V. Speckle tracking echocardiography in cats with preclinical hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2019, 33, 1232–1241. [Google Scholar] [CrossRef]
- Saito, T.; Suzuki, R.; Yuchi, Y.; Fukuoka, H.; Satomi, S.; Teshima, T.; Matsumoto, H. Comparative study of myocardial function in cases of feline hypertrophic cardiomyopathy with and without dynamic left-ventricular outflow-tract obstruction. Front. Vet. Sci. 2023, 10, 1191211. [Google Scholar] [CrossRef]
- Hirose, M.; Watanabe, M.; Takeuchi, A.; Yokoi, A.; Terai, K.; Matsuura, K.; Takahashi, K.; Tanaka, R. Differences in the Impact of Left Ventricular Outflow Tract Obstruction on Intraventricular Pressure Gradient in Feline Hypertrophic Cardiomyopathy. Animals (Basel). 2024, 14, 3320. [Google Scholar] [CrossRef]
- Suzuki, R.; Saito, T.; Yuchi, Y.; Kanno, H.; Teshima, T.; Matsumoto, H. Detection of Congestive Heart Failure and Myocardial Dysfunction in Cats With Cardiomyopathy by Using Two-Dimensional Speckle-Tracking Echocardiography. Front. Vet. Sci. 2021, 8, 771244. [Google Scholar] [CrossRef]
- Dhingra, R.; Vasan, R.S. Biomarkers in Cardiovascular Disease: Statistical Assessment and Section on Key Novel Heart Failure Biomarkers. Trends Cardiovasc. Med. 2017, 27, 123–133. [Google Scholar] [CrossRef]
- Machen, M.C.; Oyama, M.A.; Gordon, S.G.; Rush, J.E.; Achen, S.E.; Stepien, R.L.; Fox, P.F.; Saunders, A.B.; Cunningham, S.M.; Lee, P.M.; Kellihan, H.B. Multicentered investigation of a point-of-care NT-proBNP ELISA to detect moderate to severe occult (preclinical) feline heart disease in cats referred for cardiac evaluation. J. Ve.t Cardiol. 2014, 16, 245–255. [Google Scholar] [CrossRef]
- Heishima, Y.; Hori, Y.; Nakamura, K.; Yamashita, Y.; Isayama, N.; Kanno, N.; Katagi, M.; Onodera, H.; Yamano, S.; Aramaki, Y. Diagnostic accuracy of plasma atrial natriuretic peptide concentrations in cats with and without cardiomyopathies. J. Vet. Cardiol. 2018, 20, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.F.; Quinn, R.L.; Rahilly, L.J. Biomarkers for differentiation of causes of respiratory distress in dogs and cats: Part 1-cardiac diseases and pulmonary hypertension. J. Vet. Emerg. Crit. Care. 2015, 25, 311–329. [Google Scholar] [CrossRef]
- Lu, T.-L.; Côté, E.; Kuo, Y.-W.; Wu, H.-H.; Wang, W.-Y.; Hung, Y.-H. Point-of-care N-terminal pro B-type natriuretic peptide assay to screen apparently healthy cats for cardiac disease in general practice. J. Vet. Intern. Med. 2021, 35, 1663–1672. [Google Scholar] [CrossRef]
- Mainville, C.A.; Clark, G.H.; Esty, K.J.; Foster, W.M.; Hanscom, J.; Hebert, K.J.; Lyons, H.R. Analytical validation of an immunoassay for the quantification of N-terminal pro–B-type natriuretic peptide in feline blood. J. Vet. Diagn. Invest. 2015, 27, 414–442. [Google Scholar] [CrossRef]
- Parzeniecka-Jaworska, M.; Garncarz, M.; Kluciński, W. ProANP as a screening biomarker for hypertrophic cardiomyopathy in Maine coon cats. Pol. J. Vet. Sci. 2016, 19, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Ironside, V.A.; Tricklebank, P.R.; Boswood, A. Risk indictors in cats with preclinical hypertrophic cardiomyopathy: a prospective cohort study. J. Feline Med. Surg. 2021, 23, 149–159. [Google Scholar] [CrossRef]
- Hori, Y.; Iguchi, M.; Heishima, Y.; Yamashita, Y.; Nakamura, K.; Hirakawa, A.; Kitade, A.; Ibaragi, T.; Katagi, M.; Sawada, T.; Yuki, M.; Kanno, N.; Inaba, H.; Isayama, N.; Onodera, H.; Iwasa, N.; Kino, M.; Narukawa, M.; Uchida, S. Diagnostic utility of cardiac troponin I in cats with hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2018, 32, 922–929. [Google Scholar] [CrossRef]
- Hanås, S.; Larsson, A.; Rydén, J.; Lilliehöök, I.; Häggström, J.; Tidholm, A.; Höglund, K.; Ljungvall, I.; Holst, B.S. Cardiac troponin I in healthy Norwegian Forest Cat, Birman and domestic shorthair cats, and in cats with hypertrophic cardiomyopathy. J. Feline Med. Surg. 2022, 24, e370–e379. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Payne, J.R.; Matos, J.N.; Fong, W.W.; Connolly, D.J.; Fuentes, V.L. Biomarker changes with systolic anterior motion of the mitral valve in cats with hypertrophic cardiomyopathy. J. Vet. Int. Med. 2020, 34, 1718–1727. [Google Scholar] [CrossRef]
- Prošek, R.; Sisson, D.; Oyama, M.A.; Biondo, A.W.; Solter, P.F. Measurements of Plasma Endothelin Immunoreactivity in Healthy Cats and Cats with Cardiomyopathy. J. Vet. Intern. Med. 2004, 18, 826–830. [Google Scholar] [CrossRef]
- Jiwaganont, P.; Roytrakul, S.; Thaisakun, S.; Sukumolanan, P.; Petchdee, S. Investigation of coagulation and proteomics profiles in symptomatic feline hypertrophic cardiomyopathy and healthy control cats. BMC Vet. Res. 2024, 20, 292. [Google Scholar] [CrossRef] [PubMed]
- Marsiglia, J.D.C.; Credidio, F.L.; Mimary de Oliveira, T.G.; Reis, R.F.; Antunes, M.O.; de Araujo, A.Q.; Pedrosa, R.P.; Barbosa-Ferreira, J.M.B.; Mady, C.; Krieger, J.E.; Arteaga-Fernandez, E.; Pereira, A.C. Clinical predictors of a positive genetic test in hypertrophic cardiomyopathy in the Brazilian population. BMC Cardiovascular Disorders 2014, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Casamian-Sorrosal, D.; Chong, S.K.; Fonfara, S.; Helps, C. Prevalence and demographics of the MYBPC3-mutations in ragdolls and Maine coons in the British Isles. J. Small Anim. Pract. 2014, 55, 269–273. [Google Scholar] [CrossRef]
- Cheng, W.-C.; Lawson, C.; Liu, H.-H.; Wilkie, L.; Dobromylskyj, M.; Luis Fuentes, V.; Dudhia, J.; Connolly, D.J. Exploration of mediators associated with myocardial remodelling in feline hypertrophic cardiomyopathy. Animals (Basel) 2023, 13, 2112. [Google Scholar] [CrossRef]
- Kaplan, J.L.; Rivas, V.N.; Connolly, D.J. Advancing treatments for feline hypertrophic cardiomyopathy: the role of animal models and targeted therapeutics. Vet. Clin. North. Am. Small Anim. Pract. 2023, 53, 1293–1308. [Google Scholar] [CrossRef]
- Stack, J.P.; Fries, R.C.; Kruckman, L.; Kadotani, S.; Wallace, G. Galectin-3 as a novel biomarker in cats with hypertrophic cardiomyopathy. J. Vet. Cardiol, 2023, 48, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Fries, R.C.; Kadotani, S.; Keating, S.C.J.; Stack, J.P. Cardiac extracellular volume fraction in cats with preclinical hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2021, 35, 812–822. [Google Scholar] [CrossRef]
- Demeekul, K.; Sukumolanan, P.; Petchdee, S. Evaluation of galectin-3 and titin in cats with a sarcomeric gene mutation associated with echocardiography. Vet. World. 2024, 17, 2407–2416. [Google Scholar] [CrossRef] [PubMed]
- Chong, A.; Joshua, J.; Raheb, S.; Pires, A.; Colpitts, M.; Caswell, J.L.; Fonfara, S. Evaluation of potential novel biomarkers for feline hypertrophic cardiomyopathy. Res. Vet. Sci. 2024, 180, 105430. [Google Scholar] [CrossRef]
- Li, R.H.L.; Nguyen, N.; Stern, J.A.; Duler, L.M. Neutrophil extracellular traps in feline cardiogenic arterial thrombi: a pilot study. J. Feline Med. Surg. 2022, 24, 580–586. [Google Scholar] [CrossRef]
- Li, R.H.L.; Fabella, A.; Nguyen, N.; Kaplan, J.L.; Ontiveros, E.; Stern, J.A. Circulating neutrophil extracellular traps in cats with hypertrophic cardiomyopathy and cardiogenic arterial thromboembolism. J. Vet. Intern. Med. 2023, 37, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Rodan, I.; Sundahl, E.; Carney, H.; Gagnon, A.-C.; Heath, S.; Landsberg, G.; Seksel, K.; Yin, S.; Association, A.A.H. AAFP and ISFM Feline-Friendly Handling Guidelines. J Feline Med Surg 2011, 13, 364–375. [Google Scholar] [CrossRef]
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Luis Fuentes, V.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Kamp, A.L.; Yousofzai, W.; Kooistra, H.S.; Santarelli, G.; van Geijlswijk, I.M. Suspected clopidogrel-associated hepatitis in a cat. J.F.M.S. Open Rep. 2024, 10, 20551169241278408. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.L.; Adin, D.B.; Lehmkuhl, L.B. Effect of atenolol on heart rate, arrhythmias, blood pressure, and dynamic left ventricular outflow tract obstruction in cats with subclinical hypertrophic cardiomyopathy. J. Vet. Cardiol. 2015, 17, S296–S305. [Google Scholar] [CrossRef]
- Kortas, M; Szatmári, V. Prevalence and prognosis of atenolol-responsive systolic anterior motion of the septal mitral valve leaflet in young cats with severe dynamic left ventricular outflow tract obstruction. Animals (Basel). 2022, 12, 3509. [Google Scholar] [CrossRef]
- King, J.N.; Martin, M.; Chetboul, V.; Ferasin, L.; French, A.T.; Strehlau, G.; Seewald, W.; Smith, S.G.W.; Swift, S.T.; Roberts, S.L.; Harvey, A.M.; Little, C.J.L.; Caney, S.M.A.; Simpson, K.E.; Sparkes, A.H.; Mardell, E.J.; Bomassi, E.; Muller, C.; Sauvage, J.P.; Diquélou, A.; Schneider, M.A.; Brown, L.J.; Clarke, D.D.; Rousselot, J.-F. Evaluation of benazepril in cats with heart disease in a prospective, randomized, blinded, placebo-controlled clinical trial. J. Vet. Intern. Med. 2019, 33, 2559–2571. [Google Scholar] [CrossRef]
- MacDonald, K.A.; Kittleson, M.D.; Kass, P.; White, S.D. Effect of spironolactone on diastolic function and left ventricular mass in Maine Coon cats with familial hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2008, 22, 335–341. [Google Scholar] [CrossRef]
- Reina-Doreste, Y.; Stern, J.A.; Keene, B.W.; Tou, S.P.; Atkins, C.E.; DeFrancesco, T.C.; Ames, M.K.; Hodge, T.E.; Meurs, K.M. Case-control study of the effects of pimobendan on survival time in cats with hypertrophic cardiomyopathy and congestive heart failure. J. Am. Vet. Med. Assoc. 2014, 245, 534–539. [Google Scholar] [CrossRef]
- Ishizaka, M.; Katagiri, K.; Ogawa, M.; Hsu, H.H.; Miyagawa, Y.; Takemura, N. A pilot study of the proarrhythmic effects of pimobendan injection in clinically healthy cats. Vet. Res. Commun. 2024, 48, 3177–3186. [Google Scholar] [CrossRef]
- Oldach, M.S.; Ueda, Y.; Ontiveros, E.S.; Fousse, S.L.; Visser, L.C.; Stern, J.A. Acute pharmacodynamic effects of pimobendan in client-owned cats with subclinical hypertrophic cardiomyopathy. BMC Vet. Res. 2021, 17, 89. [Google Scholar] [CrossRef] [PubMed]
- Kochie, S.L.; Schober, K.E.; Rhinehart, J.; Winter, R.L.; Bonagura, J.D.; Showers, A.; Yildez, V. Effects of pimobendan on left atrial transport function in cats. J. Vet. Intern. Med. 2021, 35, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Schober, K.E.; Rush, J.E.; Luis Fuentes, V.; Glaus, T.; Summerfield, N.J.; Wright, K.; Lehmkuhl, L.; Wess, G.; Sayer, M.P.; Loureiro, J.; MacGregor, J.; Mohren, N. Effects of pimobendan in cats with hypertrophic cardiomyopathy and recent congestive heart failure: results of a prospective, double-blind, randomized, nonpivotal, exploratory field study. J. Vet. Intern Med. 2021, 35, 789–800. [Google Scholar] [CrossRef]
- James, R.; Guillot, E.; Garelli-Paar, C.; Huxley, J.; Grassi, V.; Cobb, M. The SEISICAT study: a pilot study assessing efficacy and safety of spironolactone in cats with congestive heart failure secondary to cardiomyopathy. J. Vet. Cardiol. 2017, 20, 1–12. [Google Scholar] [CrossRef]
- Hambrook, L.E.; Bennett, P.F. Effect of pimobendan on the clinical outcome and survival of cats with nontaurine responsive dilated cardiomyopathy. J. Feline Med. Surg. 2012, 14, 233–239. [Google Scholar] [CrossRef]
- Roche-Catholy, M.; Paepe, D.; Devreese, M.; Broeckx, B.J.G.; Woehrlé, F.; Schneider, M.; Garcia de Salazar Alcala, A.; Hellemans, A.; Smets, P. Pharmacokinetic and pharmacodynamic properties of orally administered torasemide in healthy cats. J. Vet. Intern. Med. 2022, 36, 1782–1791. [Google Scholar] [CrossRef]
- Pion, P.D.; Kittleson, M.D.; Rogers, Q.R.; Morris, J.G. Myocardial failure in cats associated with low plasma taurine: a reversible cardiomyopathy. Science. 1987, 14, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Umezawa, M.; Aoki, T.; Niimi, S.; Takano, H.; Mamada, K.; Fujii, Y. A pilot study investigating serum carnitine profile of cats with preclinical hypertrophic cardiomyopathy. J. Vet. Med. Sci. 2025, 87, 75–79. [Google Scholar] [CrossRef]
- Moore, K.E.; Morris, N.; Dhupa, N.; Murtaugh, R.J.; Rush, J.E. Retrospective study of streptokinase administration in 46 cats with arterial thromboembolism. J. Vet. Emerg. Crit. Care 2000, 10, 245–257. [Google Scholar] [CrossRef]
- Welch, K.M.; Rozanski, E.A.; Freeman, L.M.; Rush, J.E. Prospective evaluation of tissue plasminogen activator in 11 cats with arterial thromboembolism. J Feline Med Surg 2010, 12, 122–128. [Google Scholar] [CrossRef]
- Guillaumin, J.; Gibson, R.M.B.; Goy-Thollot, I.; Bonagura, J.D. Thrombolysis with tissue plasminogen activator (TPA) in feline acute aortic thromboembolism: a retrospective study of 16 cases. J. Feline Med. Surg. 2018, 21, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.T.; Walker, A.L.; Georges, C.J.; Li, R.H.L.; Stern, J.A. Dual therapy with clopidogrel and rivaroxaban in cats with thromboembolic disease. J. Feline Med. Surg. 2022, 24, 277–283. [Google Scholar] [CrossRef]
- Lo, S.T.; Li, R.H.L.; Georges, C.J.; Nguyen, N.; Chen, C.K.; Stuhlmann, C.; Oldach, M.S.; Rivas, V.N.; Fousse, S.; Harris, S.P.; Stern, J.A. Synergistic inhibitory effects of clopidogrel and rivaroxaban on platelet function and platelet-dependent thrombin generation in cats. J. Vet. Intern. Med. 2023, 37, 1390–1400. [Google Scholar] [CrossRef] [PubMed]
- Jaturanratsamee, K.; Jiwaganont, P.; Panprom, C.; Petchdee, S. Rivaroxaban versus enoxaparin plus clopidogrel therapy for hypertrophic cardiomyopathy-associated thromboembolism in cats. Vet. World 2024, 17, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Rishniw, M. How much protection does clopidogrel provide to cats with hypertrophic cardiomyopathy? J. Am. Vet. Med. Assoc. 2024, 262, 1422–1424. [Google Scholar] [CrossRef]
- Sharpe, A.N.; Oldach, M.S.; Kaplan, J.L.; Rivas, V.; Kovacs, S.L.; Hwee, D.T.; Morgan, B.P.; Malik, F.I.; Harris, S.P.; Stern, J.A. Pharmacokinetics of a single dose of Aficamten (CK-274) on cardiac contractility in an A31P MYBPC3 hypertrophic cardiomyopathy cat model. J. Vet. Pharmacol. Therap. 2023, 46, 52–61. [Google Scholar] [CrossRef]
- Sharpe, A.N.; Oldach, M.S.; Rivas, V.N.; Kaplan, J.L.; Walker, A.L.; Kovacs, S.L.; Hwee, D.T.; Cremin, P.; Morgan, B.P.; Malik, F.I.; Harris, S.P.; Stern, J.A. Effects of Aficamten on cardiac contractility in a feline translational model of hypertrophic cardiomyopathy. Sci. Rep. 2023, 13, 32. [Google Scholar] [CrossRef]
- Kaplan, J.L.; Rivas, V.N.; Walker, A.L.; Grubb, L.; Farrell, A.; Fitzgerald, S.; Kennedy, S.; Jauregui, C.E.; Crofton, A.E.; McLaughlin, C.; Van Zile, R.; DeFrancesco, T.C.; Meurs, K.M.; Stern, J.A. Delayed-release rapamycin halts progression of left ventricular hypertrophy in subclinical feline hypertrophic cardiomyopathy: results of the RAPACAT trial. J. Am. Vet. Med. Assoc. 2023, 261, 1–10. [Google Scholar] [CrossRef]
- Rivas, V.N.; Crofton, E.A.; Jauregui, C.E.; Wouters, J.R.; Yang, B.S.; Wittenburg, L.A.; Kaplan, J.L.; Hwee, D.T.; Murphy, A.N.; Morgan, B.P.; Malik, F.I.; Harris, S.P.; Stern, J.A. Cardiac myosin inhibitor, CK-586, minimally reduces systolic function and ameliorates obstruction in feline hypertrophic cardiomyopathy. Sci. Rep. 2024, 14, 12038. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of the phenotype of feline hypertrophic cardiomyopathy (HCM), including genetic, clinical, and pathophysiological factors associated with the development and progression of the disease. BioRender (https://www.biorender.com/).
Figure 1.
Schematic representation of the phenotype of feline hypertrophic cardiomyopathy (HCM), including genetic, clinical, and pathophysiological factors associated with the development and progression of the disease. BioRender (https://www.biorender.com/).
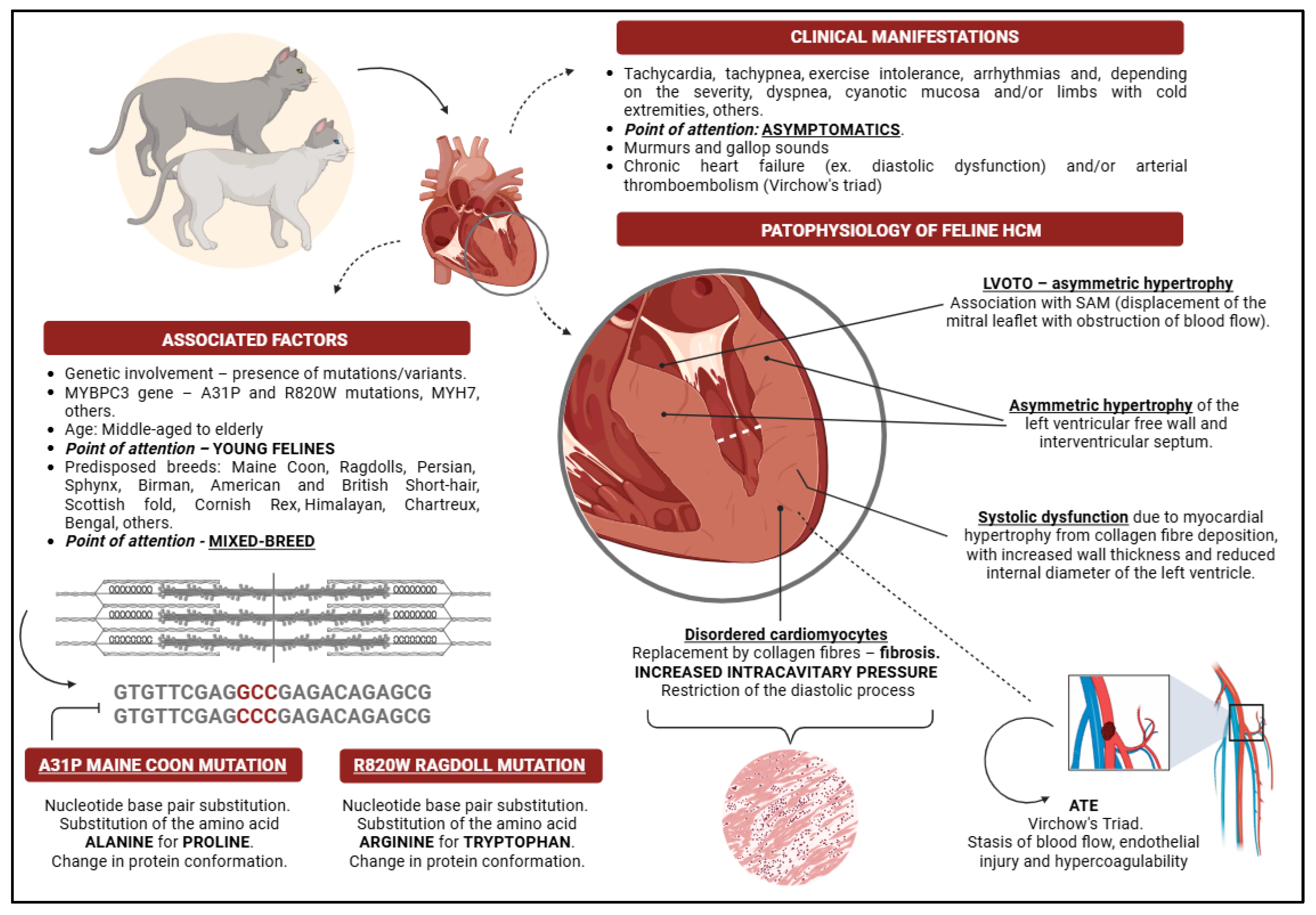
Figure 2.
Macroscopic and histopathological changes in feline patients with hypertrophic cardiomyopathy. (A) The sectioned heart showing varying levels of hypertrophy of the left free ventricular wall and interventricular septum (yellow line); in the atrial region, it is possible to observe the presence of a thrombus (star). (B) Various levels of myocardial hypertrophy, characteristic of heterogeneous hypertrophic conditions (blue lines), and septal hypertrophy at the level of the left ventricular outflow tract, which is a frequent finding in patients with outflow tract obstruction (star), were observed. (C) Cross-sectioned heart showing areas of cardiac fibrosis (arrows). (D) Histopathological evaluation of myocardial tissue showing muscle disarray and the presence of collagen fibre characteristic of a fibrotic process (dashed line). Images available in the Davis-Thompson Foundation database (Noah's archive; https://davisthomsfoundationdavisthomsfoundation.org).
Figure 2.
Macroscopic and histopathological changes in feline patients with hypertrophic cardiomyopathy. (A) The sectioned heart showing varying levels of hypertrophy of the left free ventricular wall and interventricular septum (yellow line); in the atrial region, it is possible to observe the presence of a thrombus (star). (B) Various levels of myocardial hypertrophy, characteristic of heterogeneous hypertrophic conditions (blue lines), and septal hypertrophy at the level of the left ventricular outflow tract, which is a frequent finding in patients with outflow tract obstruction (star), were observed. (C) Cross-sectioned heart showing areas of cardiac fibrosis (arrows). (D) Histopathological evaluation of myocardial tissue showing muscle disarray and the presence of collagen fibre characteristic of a fibrotic process (dashed line). Images available in the Davis-Thompson Foundation database (Noah's archive; https://davisthomsfoundationdavisthomsfoundation.org).
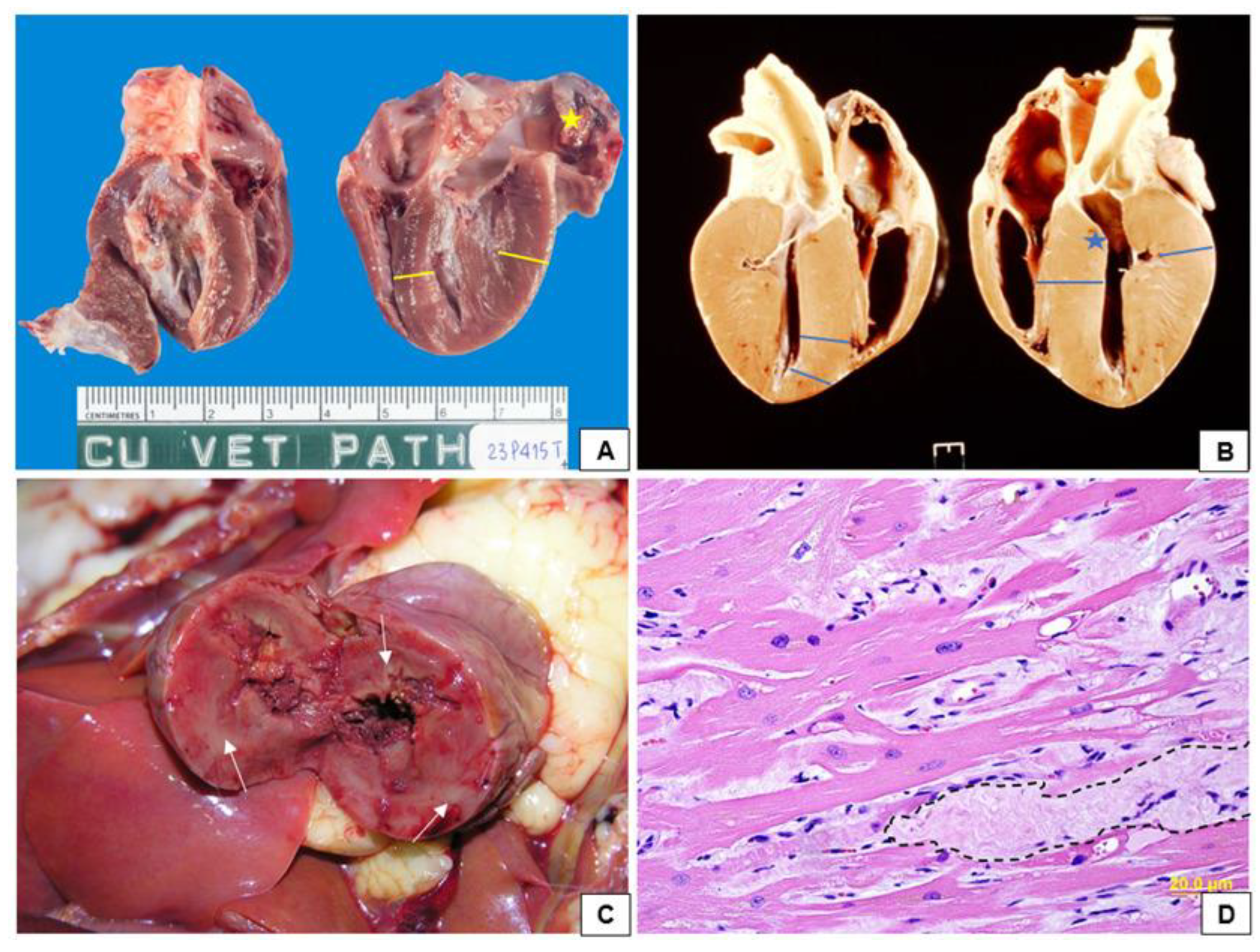
Figure 3.
Radiographic images of cats with hypertrophic cardiomyopathy obtained in the study by Kim et al. [93]. (A) and (B) Lateral projection images and (C) and (D) ventrodorsal projection images. (A) and (B) Note the atrial enlargement (dashed line) and the parallelism of the trachea (line), showing tracheal displacement (A). (C) and (D) Atrial and ventricular enlargement with changes in the normal cardiac structure.
Figure 3.
Radiographic images of cats with hypertrophic cardiomyopathy obtained in the study by Kim et al. [93]. (A) and (B) Lateral projection images and (C) and (D) ventrodorsal projection images. (A) and (B) Note the atrial enlargement (dashed line) and the parallelism of the trachea (line), showing tracheal displacement (A). (C) and (D) Atrial and ventricular enlargement with changes in the normal cardiac structure.
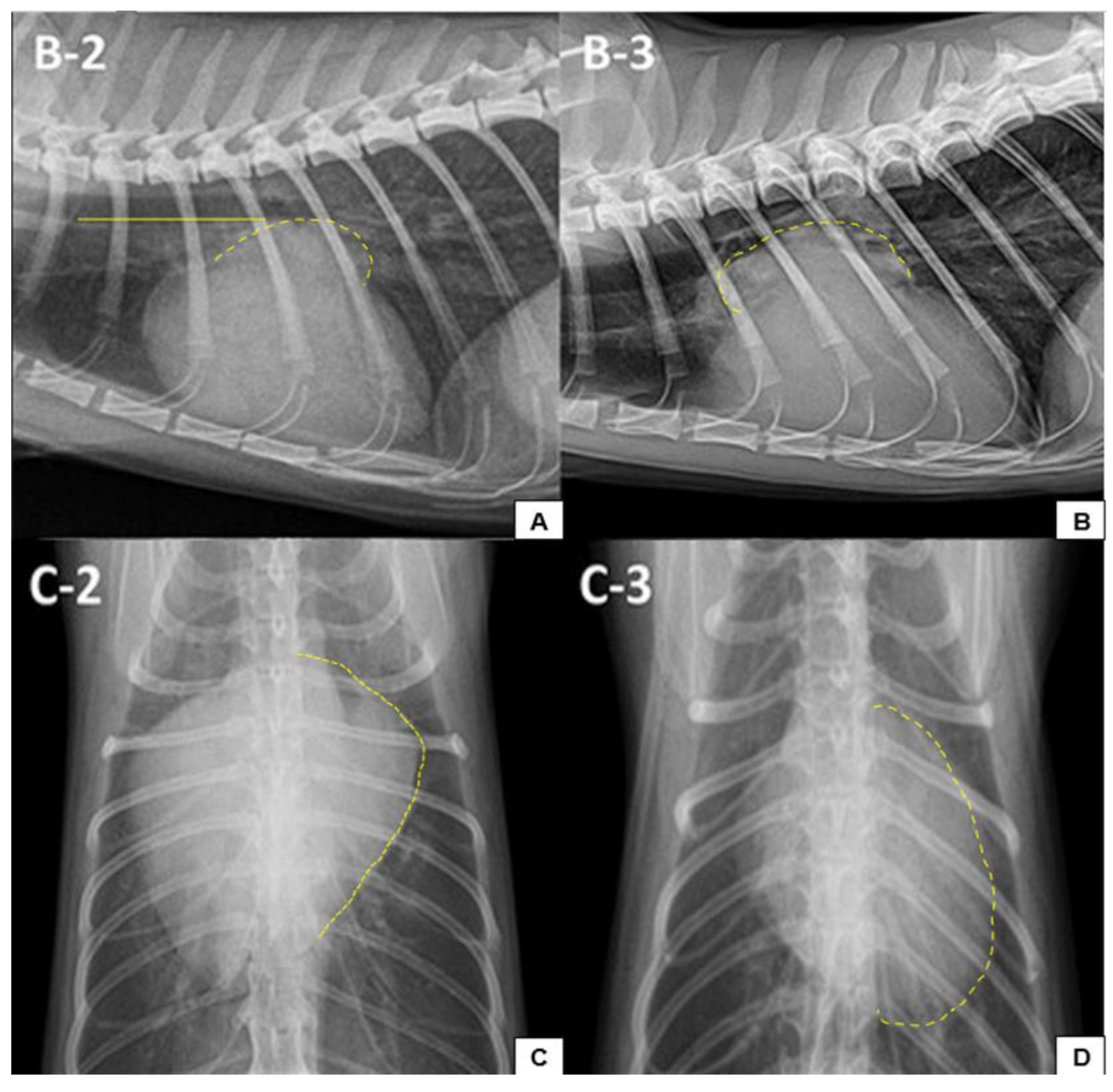
Figure 4.
An electrocardiographic examination of a 10-year-old female mixed breed feline patient diagnosed with stage B2 hypertrophic cardiomyopathy was performed. Note the presence of premature ventricular complex and right bundle branch blocks in the DII derivation.
Figure 4.
An electrocardiographic examination of a 10-year-old female mixed breed feline patient diagnosed with stage B2 hypertrophic cardiomyopathy was performed. Note the presence of premature ventricular complex and right bundle branch blocks in the DII derivation.
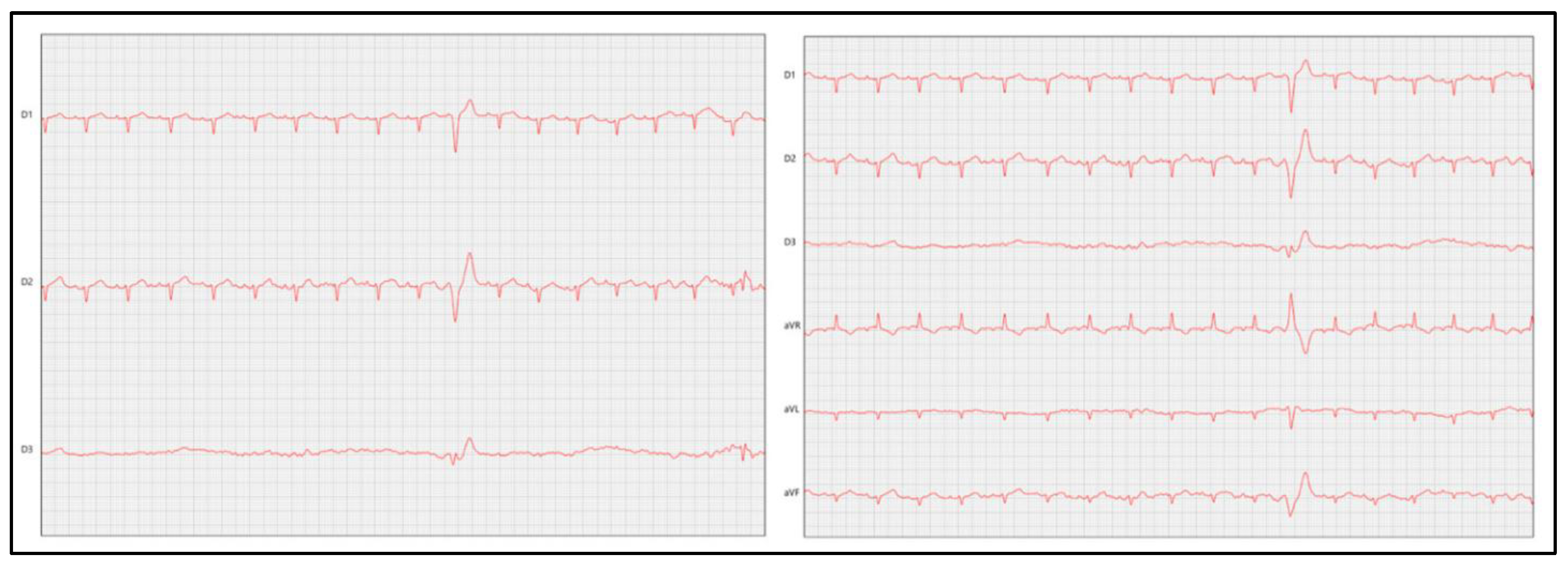
Figure 5.
Echocardiographic examination showing right parasternal longitudinal section 4 and 5 chambers in a feline patient diagnosed with hypertrophic cardiomyopathy. The images point to characteristics frequently observed in felines affected by the disease. There is evident left atrial dilation (dashed line), hypertrophy with a heterogeneous appearance in the region of the left ventricular free wall and interventricular septum (line), a reduction in the size of the left ventricular cavity (dashed line), an obstruction of the ventricular outflow tract to the left and the presence of smoke (star). Consider: RA, right atrium; RV, right ventricle; LV, left ventricle; RV, right ventricle; AO, aorta; IVS, interventricular septum; LVFW, left ventricle free wall.
Figure 5.
Echocardiographic examination showing right parasternal longitudinal section 4 and 5 chambers in a feline patient diagnosed with hypertrophic cardiomyopathy. The images point to characteristics frequently observed in felines affected by the disease. There is evident left atrial dilation (dashed line), hypertrophy with a heterogeneous appearance in the region of the left ventricular free wall and interventricular septum (line), a reduction in the size of the left ventricular cavity (dashed line), an obstruction of the ventricular outflow tract to the left and the presence of smoke (star). Consider: RA, right atrium; RV, right ventricle; LV, left ventricle; RV, right ventricle; AO, aorta; IVS, interventricular septum; LVFW, left ventricle free wall.
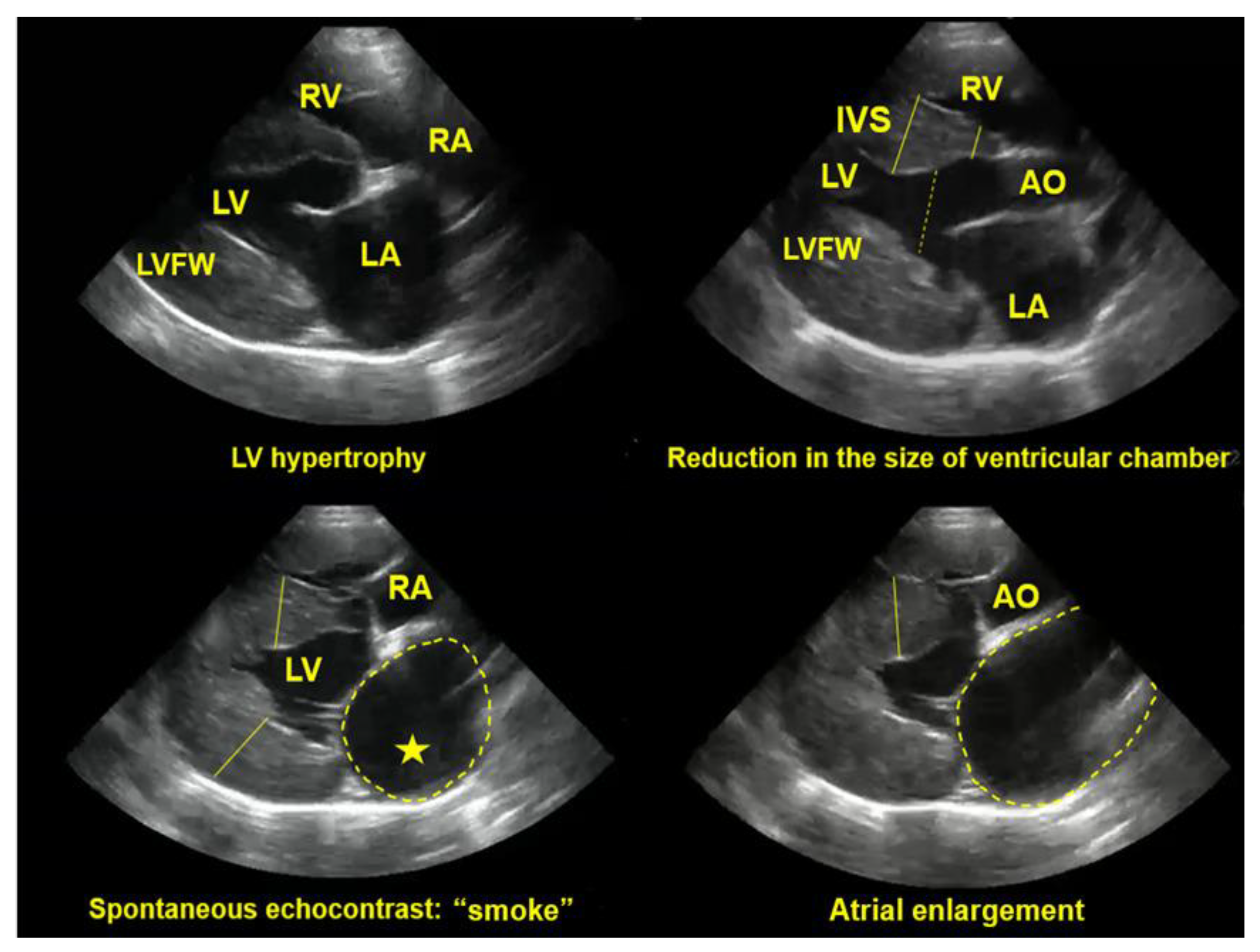
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



