Submitted:
07 February 2025
Posted:
10 February 2025
You are already at the latest version
Abstract
The article delves into the systemic inflammatory response syndrome (SIRS), thromboinflammation, and septic shock in fetuses and neonates, providing a comprehensive examination of their pathophysiology, diagnostic criteria, and clinical implications. It establishes SIRS as a hyper-reaction to external stress, disrupting the balance between inflammation and adaptive mechanisms, driven by cytokines like TNF-α and IL-1. The fetal inflammatory response syndrome (FIRS), a subset of SIRS, is highlighted for its role in adverse neonatal outcomes, including organ damage, inflammation, and long-term developmental disorders. The article outlines the extensive impact of FIRS on vital systems such as the blood, lungs, central nervous system, and kidneys. The paper underscores the challenges in diagnosing and managing septic shock in neonates, emphasizing the interplay between inflammation and hemostatic system. It highlights recent advancements like the convergent model of coagulation and emerging biomarkers such as microRNAs for early detection. Despite progress, gaps in understanding the molecular underpinnings of these conditions and effective therapeutic strategies are noted. This underscores the need for targeted research to mitigate the morbidity and mortality associated with septic shock in neonates.
Keywords:
systemic inflammatory response syndrome
; thromboinflammation
; septic shock
; fetal inflammatory response syndrome
1. Introduction
The phenomenon of Sanarelli-Schwartzman is a localized or generalized reaction of the body to endotoxins, which cause thrombosis and ultimately necrosis of affected tissues. In fact, the generalized reaction of Sanarelli-Schwartzman is a model of sepsis and septic shock. Conditions such as systemic inflammatory response syndrome (SIRS), septic shock, hemolytic-uremic syndrome, Waterhouse-Friderichsen syndrome can all be considered part of the Sanarelli-Schwartzman phenomenon. Activation of the clotting system is what occurs in this phenomenon, leading to consumption coagulopathy and intravascular clotting in the microcirculatory system. In 2020, the names of Grigory Schwartzman and Giuseppe Sanarelli once again became widely recognized in the scientific community in the context of the COVID-19 pandemic [1].
2. Systemic Inflammatory Response Syndrome, Thromboinflammation and Septic Shock in Fetuses and Neonates
2.1. Systemic Inflammatory Response Syndrome, SIRS
SIRS is a hyper-response of the body to an external stress factor, which may include inflammation due to an infectious process, surgical intervention, or malignancy [2]. Regulation of the body's response should effectively suppress the cause of inflammation, but in the development of SIRS, the balance between inflammation and the adaptive anti-inflammatory mechanism is disrupted [3].
2.1.1. Diagnostic Criteria for SIRS
2.1.2. The Pathogenesis of SIRS
The pathogenesis of SIRS is based on the production of pro-inflammatory cytokines, especially TNF-α, IL-1, IL-6, IL-8, IL-10, which spread to sites distant from the primary focus. In this case, TNF-α and IL-1, which stimulate the production of tissue factor (TF), play a major role in the development of endothelial dysfunction. As a result of systemic effects on the endothelium and changes in the balance between the coagulation system and fibrinolysis, the whole hemostasis system is disturbed, leading to the development of organ failure. Stimulation of the coagulation system and suppression of fibrinolysis results in increased thrombosis, impaired microcirculation and further organ damage. Cytokines also activate MAPK/NF-κB pathways within endothelial cells, leading to increased synthesis and release of procoagulant factors [5]
Over the past few years, more and more researches have highlighted the importance of SIRS in the development of serious pregnancy complications, including recurrent pregnancy loss, preterm delivery, placenta accreta, intrauterine growth restriction (IUGR) and preeclampsia [6].
2.2. Fetal Inflammatory Response Syndrome, FIRS
The syndrome of systemic inflammatory response in the fetus is known as fetal inflammatory response syndrome (FIRS), which is associated with infectious and inflammatory changes in the placenta. The diversity of microorganisms infecting the fetus and the need for different diagnostic modalities complicate pathogen identification, especially in high-risk neonates. Several studies demonstrated that the presence of intrauterine infection during pregnancy is associated with a high risk of serious long-term sequelae. These include exudative otitis media and neuroendocrine-immune dysfunction in the child. [7,8]. It is therefore of particular interest to consider the problem of intrauterine infection from the perspective of the FIRS. Despite the high morbidity and mortality, there is a lack of convincing data on the early diagnosis and effective treatment of this pathology.
The molecular mechanisms of FIRS are still far from being fully understood. However, it has been proposed to divide this syndrome into 2 types, depending on the nature of the inflammatory response. Type 1 FIRS is characterized by elevated levels of IL-6, IL-8, CXCL10 (a chemokine whose levels are increased in the amniotic fluid of patients with chronic chorioamnionitis), IL-1β and TNF-α compared with healthy newborns. There are also characteristic gene expression changes in FIRS type 1, resulting in suppression of T-cell immune regulation [9]. Thymic involution, often seen in newborns with acute inflammation, is one explanation for this response [10]. Straňák et al. after analyzing the cord blood of 100 preterm infants also found a correlation between the presence of FIRS and increased IL-6, CRP and procalcitonin levels. Maternal leukocytosis (P<0.001), premature rupture of membranes (P<0.001) and preterm uterine contractions (P<0.0001) were observed in the presence of FIRS type 1 [11]. There is no acute inflammatory response in FIRS type 2. However, upregulation of HLA-F, HLA-C and HLA-DRA genes and a significant increase in CXCL10 with normal proinflammatory cytokine levels were observed, resembling the mechanisms of graft rejection [12].
2.3. Multiple Organ Failure in FIRS
The basis of FIRS is the maternal inflammatory response (MIR), which encompasses acute subchorionitis, inflammation of the placenta and extraplacental membranes. The diagnostic criteria for FIRS include the fetal inflammatory reaction (FIR), acute inflammation of the placenta, extraplacental membranes, umbilical cord and chorionic vasculitis. It is possible that FIR and MIR may be absent in patients with FIRS type 2. However, this does not negate the likelihood of subsequent neonatal complications [13].
In the context of FIRS, the fetus exhibits indications of damage to a multitude of organs and body systems. The most frequently affected organs include the blood system, lungs, central nervous system, thymus, spleen, and kidneys.
Neutrophils represent a significant component of the innate immune system. Fetuses with FIRS were more likely to have neutrophil counts that exceeded the 95th percentile for gestational age (71% (30/42) vs. 35% (37/105); p<0,001) [14]. Granulocyte colony-stimulating factor (G-CSF) is a cytokine that stimulates the production of various cells, including neutrophils, macrophages, eosinophils, T-helper cells (Th1 and Th17), and cells of some tumors. The expression of this factor is enhanced by inflammatory mediators, including IL-1, IL-4, IL-6, and TNF-α, but can be inhibited by a number of cytokines, including IL-10, and interferon-gamma [15,16]. Additionally, G-CSF is known to facilitate the release of neutrophils in response to stressors, associated with infectious processes. Chaiworapongsa et al. demonstrated that G-CSF levels were significantly elevated in fetuses with FIRS in comparison to controls (p < 0.001). Furthermore, they identified that a fetal plasma G-CSF concentration of ≥134 pg/ml was a significant predictor of chorioamnionitis, infection, and cumulative neonatal morbidity and mortality [17]. An increased number of nucleated erythrocytes (immature forms) in neonates has been observed in cases of a prolonged rupture of fetal membranes (>24 hours), with a histological diagnosis of chorioamnionitis and neonatal sepsis presenting in early onset. These observations indicate an increase in erythropoiesis [18,19]. It is commonly assumed that circulating nucleated erythrocytes are a reliable indicator of hypoxia. However, in the case of by FIRS, no acidosis or hypoxemia was observed. Furthermore, the pH (-0.026 and -0.016), PaO(2) (0.25 mmHg and 5.9 mmHg) and BE (-2.4 and -2.6 mEq/L) values didn’t differ significantly between the fetuses without FIRS and those affected by it (p<0.05) [20].
Zaharie et al. examined the dynamics of plasma levels of the main pro-inflammatory cytokines on the first and third days of life. Their findings indicated a correlation between these levels and neonatal morbidity and mortality [21]. The study included 80 neonates. pH, oxygen saturation, fraction of inhaled oxygen (FiO2), gestational age at which premature rupture of the fetal membranes (PROM) occurred, and venous blood cytokine levels (CRP, IL-6, CXCL-5, IL-10, TNF-α) were assessed. The results of the study demonstrated that neonates born to mothers with PROM exhibited elevated levels of all cytokines. The symptoms of necrotizing enterocolitis (NEC) were associated with elevated levels of IL-6, while the development of cerebral intraventricular hemorrhage in neonates was correlated with high CXCL-5 (p=0.037) and sepsis was correlated with high IL-10 levels (p=0.02).
The lungs represent a crucial target organ in fetuses with FIRS. Elevated levels of IL-6 in cord blood were associated with an increased risk of bronchopulmonary dysplasia (BPD) in neonates. Kallapur et al., demonstrated that the administration of intra-amniotic endotoxin in vivo resulted in an enhanced inflammatory response and the occurrence of multiple increases in mRNA levels of IL-1, IL-6, IL-8 and TNF-α in subsequent bronchoalveolar lavage [22]. The administration of endotoxin in vivo results in an increase in surfactant synthesis and structural changes in the fetal lungs, including an enlarged alveolar diameter and thinned alveolar septa. These changes facilitate accelerated lung maturation and preparation for preterm labor [23,24]. Yoon et al. demonstrated the correlation between cord blood and amniotic fluid IL-6 levels and the subsequent development of BPD in 203 patients. The results demonstrated that 17% of the patients exhibited BPD symptoms. The results indicated that IL-6 levels in cord blood were significantly elevated in newborns with BPD (OR 4,2; 95% CI 1,6–11,2) [25]. Nevertheless, a meta-analysis by Jackson et al. revealed no correlation between BPD and chorioamnionitis, adjusted for gestational age (OR 0.99, Cl 0.76-1.3). Consequently, prospective studies will be required in order to ascertain the pathogenetic mechanisms underlying these pathologies [26]. Other complications of the perinatal period in children include respiratory distress syndrome (RDS), which is caused by increased cortisol secretion and surfactant deficiency, and persistent pulmonary hypertension. The symptom complex of neonatal RDS includes cyanosis, tachypnea, retraction of the pliable areas of the chest, and a characteristic wheeze that results from exhaled air entering the partially closed vocal tract during or shortly after birth [27]. In the study by Dessardo et al., the presence of FIRS was the most important risk factor for both chronic lung disease of prematurity (OR 31,05, 95% CI 10,7–87,75, p<0,001), and wheezing in infants (OR 5,63, 95% CI 2,42–13,05, р=0,01) [28].
A number of authors have proposed that fetal FIRS affects brain function and leads to neuroinflammation [29]. The pathogenetic mechanism of brain damage is not yet fully understood and is probably related to the ‘multiple hits’ theory. Chorioamnionitis causes diffuse damage to both white and grey matter neurons, most likely due to the direct damaging effects of pro-inflammatory cytokines (TNF-α, IL-1 and IL-6) [30,31,32]. Furthermore, inflammatory mediators can also affect the integrity of the blood-brain barrier (BBB), which contributes to increased permeability of the BBB to various proteins and exacerbates brain damage [33]. The activation of microglia, which represents the initial line of defense of nerve cells during inflammation, plays a pivotal role in the pathogenesis of brain disorders. When endotoxin was administered to animals, a profound activation of microglia was observed, accompanied by changes in immunoreactivity of myelin basic protein and apoptosis of oligodendrocytes [34]. In 2023, Giovannini et al. demonstrated that the primary and most life-threatening condition in the newborn following FIRS is cerebral hypoxia (CH) [35]. For this reason, it is recommended that these children undergo a GM ultrasound or GM MRI to detect focal and periventricular leukomalacia and cystic changes [36]. Consequences of GM hypoxia may be irreversible, including cerebral atrophy, which is characterized by decreased white matter volume and enlarged ventricles. Another significant complication of FIRS is neonatal encephalopathy (NE), which is characterized by altered consciousness, seizures, impaired muscle tone and the inability to initiate or maintain respiration. NE is associated with a high mortality rate and long-term disability, including cerebral palsy (CP), various cognitive impairments, and visual and hearing damage. In turn, CP is characterized by a variety of motor and sensory impairments, in addition to mental retardation, perceptual, behavioral and consciousness disorders [37].
Chorioamnionitis is a significant risk factor for the development of retinopathy of prematurity (ROP). This condition is caused by various lesions that disrupt neurovascular growth in the immature retina, which may be a consequence of gestational maternal hypoxia. Elevated plasma IL-6 levels indicate the severity of ROP, which can be used as a prognostic factor in the development of the disease [38,39].
Gibson et al. analyzed the risk of developing various psychiatric disorders with a history of FIRS in nearly five thousand children [40]. The findings and statistical analyses confirmed that children with FIRS were more likely to be diagnosed with neuropsychiatric disorders (OR = 1.21, CI 95% [1.09, 1.35]): autism spectrum disorder (OR = 1.35, 95% CI [1.08, 1.67]), attention deficit hyperactivity disorder (ADHD) (OR = 1.27, 95% CI [1.07, 1.49]), conduct disorder (OR = 1.50, 95% CI [1.24, 1.81]), post-traumatic stress disorder (PTSD) (OR = 2.46. CI 95% [1.21, 5.04]). A seven-year period of observation was employed in this study in order to assess the long-term effects of FIRS on newborn infants. However, it is important that psychiatric disorders are not necessarily related to complications of the neonatal period.
Furthermore, the kidneys are frequently affected in fetus with FIRS. The relationship between the amniotic fluid index (AFI), which is dependent on renal function and fetal urination, and the presence of intra-amniotic infection was explored. A positive culture result and an increased concentration of matrix metalloproteinase-8 (>23 ng/ml), IL-6 and TNF-α were observed more frequently in patients with oligohydramnios (p < 0.05) [41,42]. Azpurua et al. demonstrated that children born to mothers with intra-amniotic inflammation exhibited elevated levels of IL-6 and urea nitrogen. However, there were no discernible alterations in renal vascular function as assessed by ultrasound Doppler ultrasonography [43]. In animal model studies, chorioamnionitis resulted in a reducing number of renal tubules (p < 0.05), but there was no significant difference in body weight or degree of inflammation in the kidneys [44,45]. However, Muk et al. demonstrated that inflammation within the amnion led to an increase in creatinine and microalbumin concentrations — markers of renal dysfunction. Moreover, elevated concentrations of biomarkers indicative of renal damage (e.g., LRG1, KIM1, NGLA, HIF1A, and CASP3) were observed in kidney tissue. Consequently, further research is warranted to elucidate the impact of FIRS on fetal immune activation and kidney function [46].
Furthermore, FIRS has a significant impact on the thymus, which is the most crucial organ in fetal immune defense. A study by Kuypers et al. observed a decrease in lymphocyte levels and a decrease in the cortico-medullary area of the thymus following intra-amniotic injection of endotoxin. Twenty-four hours after administration, the levels of IL-6, IL-17 mRNA and TLR4 mRNA were increased, indicating acute activation of the thymus [47]. In the context of inflammation, there is a notable shift in the composition of CD8+ T-lymphocytes, accompanied by an activation of CD4+ T-lymphocytes, as evidenced by an elevated expression of CD25 (p = 0.0001), HLA-DR and CD69 (p = 0.0003) [48,49].
Other organs and systems can also be affected in FIRS, including the spleen, liver, thyroid and intestine. In FIRS, there is an alteration in splenic blood flow and a significant increase in TNF-α and CD3 expression, indicating an inflammatory response [50,51,52]. Presumed mechanisms of bowel damage in FIRS involve increased TNF-α-mediated impairment of wall microcirculation and decreased expression of vascular endothelial growth factor (VEGF) [53,54]. Сhorioamnionitis also decrease the liver function. In animal models, administration of endotoxin resulted in impaired lipid and glucose metabolism, increased alanine aminotransferase and aspartate aminotransferase, and decreased total antioxidant status [55]. Furthermore, during endotoxin administration, the production of cytokines by Kupffer cells, such as TNF-α, IL-8 and IL-18 levels, increase, which precede intestinal inflammation. This indicates a possible influence of hepatic cytokines on the subsequent development of NEC [56].
Umbilical vessel funiculitis is a marker of FIRS, which occurs more frequently in preterm infants who have elevated serum levels of intercellular adhesion molecule-1 (sICAM-1) [57]. A correlation between FIRS and endothelial dysfunction has been proposed, as a reduction in the systemic inflammatory response in patients was accompanied by an increase in sICAM-1 levels and endothelial activation. Additionally, elevated sICAM-1 levels were observed in neonates with CNS depression syndrome. Further studies are required to ascertain the role of sICAM-1 as a predictor of the development of long-term consequences of FIRS [58,59].
There are only a few studies that have clearly defined the relationship between specific hemodynamic abnormalities and fetal intrauterine growth restriction syndrome (FIRS). Eloundou et al. evaluated the effect of intrauterine inflammation on hemodynamic and structural abnormalities of the placenta (vascular malperfusion) and fetal outcomes in vivo. Virchow's triad postulates that thrombus formation occurs when three conditions are present: hypercoagulability (as in pregnancy), vascular injury, and slow blood flow. Upon exposure of the mice to the infectious agent, the following observations were made: placental endotheliitis, thrombus formation as a result of decreased fibrinogen levels, and placental thinning. The third component of Virchow's triad, stasis of blood flow, may be caused by placental thinning in conjunction with damage to the vascular network. Furthermore, the fetuses exhibited the activation of fetal microglia, which is likely associated with impaired nutrient passage and toxin excretion through the placenta [60].
It is important that de novo synthesis of antiphospholipid antibodies (aPL) may be one of the responses to intra-amniotic inflammation, which is viewed from a "first-hit" perspective. As a consequence of inflammation during the perinatal period, there may be significant alterations in the composition of the peripheral regulatory T-cell population in umbilical cord blood. Maternal infections may therefore result in the reprogramming of the still immature innate and adaptive immune systems of the fetus [61]. The first three months of a newborn's life are characterized by the presence of maternal antibodies, which provide immunity. However, a year after birth, IgG and IgM levels reach 50% of the total adult level. This may explain the propensity for sepsis, septic shock and other life-threatening conditions in the neonatal period, especially in premature infants.
Preterm infants with abnormal immune system responses, combined with immaturity of most organs and systems (including the hemostasis system), are at greatest risk of high mortality and the development of complications associated with inflammation and thrombosis [61]. It is becoming increasingly evident that fetal immune shifts resulting from intrauterine infection and de novo aPL may play a significant role in the development of neonatal thrombosis [61].
FIRS in neonates has a higher risk of neonatal sepsis [62]. In a study by Nomiyama et al., neonates with FIRS and MIR/FIR had a higher prevalence of neonatal sepsis than neonates without FIRS and MIR/FIR (p <0,001) [13].
The major complications of the neonatal period and associated cytokines after undergoing FIRS are summarized in Figure 1.
2.4. Perinatal Aspects of Septic Shock
Shock is a state of organ hypoperfusion characterized by cellular dysfunction. The pathogenesis of shock is diverse and includes several development mechanisms: decrease in circulating blood volume, decreased cardiac output and vasodilation. Sepsis is a dangerous condition that develops during excessive response of the body's immune system to infection, which leads to organ dysfunction. The development of sepsis in newborn infants is the most dangerous condition, which correlates with increased mortality ([OR] 4.41, 95% CI 1.75-11.1) [63].
The development of sepsis can be attributed to a number of factors, which can be categorized into several groups. These include maternal and neonatal risk factors [64] (Table 2).
Septic shock in the newborn is a life-threatening complication of sepsis. It is characterized by a high mortality rate among patients. Inadequate treatment of sepsis or its late diagnosis can result in the spread of infection, which in turn causes the development of generalized endothelial inflammation and subsequently septic shock. Statistical data indicates that septic shock develops in 10-15% of children with sepsis [65]. The high mortality rate observed in patients with septic shock is attributed to the nonspecific clinical manifestations and the delayed diagnosis. Consequently, this condition demands particular attention from physicians.
The development of septic shock is a complex process involving cells of the immune system and the pathogen itself. Upon entering the bloodstream, the infectious agent is recognized by macrophages and monocytes through surface receptors, initiating the activation of secondary messengers and intracellular cascades that promote the release of cytokines and chemokines. Subsequently, generalized activation of the endothelium, lymphocytes, and complement function occurs, resulting in massive inflammation and shock [66].
The systemic spread of the pathogen and the generalized activation of the endothelium result in impaired microcirculation and the development of tissue hypoxia, acidosis, and hypotension. These factors determine the development of septic shock in newborns [67]. The clinical manifestations of septic shock in neonates include damage to the respiratory and cardiovascular systems, as well as some other non-specific symptoms, such as decreased muscle tone and skin discoloration [68].
The clinical features of septic shock are characterized by three distinct stages of development, each with its own set of clinical characteristics:
- 1)
- The initial phase, termed 'compensated shock', is characterized by the activation of neuroendocrine compensatory mechanisms [66]. The symptoms of stage 1 may include tachycardia, hypouresis, decreased tissue perfusion, and extremity coldness in the newborn.
- 2)
- The subsequent stage in the development of septic shock is uncompensated shock, which is characterized by symptoms of systemic hypotension and metabolic acidosis.
- 3)
- The final phase of septic shock development is irreversible shock, which is characterized by severe microcirculatory disorders and irreversible cellular damage, leading to necrosis and multi-organ failure.
In children, cold septic shock usually develops, which is characterized by a change in hemodynamics, an increase in systemic vascular resistance due to peripheral vasoconstriction. The symptom complex of cold septic shock includes decreased and weakened pulse, diuresis, and marbling of fingertips. The development of metabolic acidosis at the second stage of shock leads to increased pulmonary resistance, which is a key link in the formation of right ventricular failure.
2.5. Hemostasis in Newborns
The specific hemostatic characteristics of newborns contribute to the development of non-specific clinical features of septic shock and SIRS. The peculiarities of hemostasis in newborns include prolongation of aPTT, PT and delayed thrombin formation. The ability to produce thrombin in the plasma of a healthy newborn is markedly reduced and delayed in comparison to an adult [69]. The neonatal hemostasis system functions by maintaining a balance between factors that promote bleeding and those that lead to thrombosis. Factors that can induce bleeding include decreased platelet reactivity, pellet release, levels of II, VII, IX, X, XI, XII coagulation factors and increased levels of alpha-2-macroglobulin. Factors that may cause thrombosis in neonates include increased hematocrit, mean corpuscular volume (MCV), von Willebrand factor (vWF), and decreased protein S, protein C, heparin cofactor II. Additionally, thrombin production in neonates is equivalent to approximately 90% of that observed in adults, which is sufficient for hemostatic clot formation [70]. Furthermore, neonatal hemostasis exhibits a low buffer capacity, which increases the risk of thrombosis due to acquired risk factors. These include various comorbidities, reduced fibrinolytic capacity, resistance to heparin due to low antithrombin (AT) levels and higher clearance of unfractionated heparin (UFH). The rise in neonatal thrombosis may be attributed to improvements in the management of life-threatening neonatal conditions, as well as a reduction in mortality among preterm infants.
Platelet function and physiology are also age-dependent. The study demonstrated an increase in fetal platelet count by ~2 × 10^9/L for each week of gestation [71]. The mean platelet count in preterm infants was ≥200 × 10^9 /L, which is a normal level for adult patients. Platelet counts that are normal for newborn infants range from 150×10^3 to 450×10^3 /μL. However, there is an evidence that platelet counts in preterm infants may be lower than this value [72]. For this reason, preterm infants are more susceptible to developing hemorrhage, particularly in the brain. The reactivity of platelets in neonates increases with age. A decrease in the expression of membrane glycoproteins in preterm infants results in an increased platelet reactivity [73].
2.6. Alterations in Neonatal Hemostasis in Septic Shock
In patients with septic shock, there is a prevalence of pronounced disorders of hemostasis, which can occur in three distinct forms: chronic, subacute and acute (disseminated intravascular coagulation, DIC). The relationship between inflammation and hemostasis is considered from the perspective of an “amplification loop”, whereby inflammation triggers and supports coagulation processes, and coagulation products support and amplify inflammation [74] (Figure 2).
The activation of hemostasis in sepsis and septic shock occurs as a result of the damage to the vascular endothelium. This damage occurs by pathogenic microorganisms, activated immunocompetent blood cells, proinflammatory cytokines (especially IL-6 and TNF-α), with the subsequent production and release of tissue factor by monocyte, macrophages and endothelial cells. Furthermore, the TF-mediated generation of thrombin occurs, as well as the inhibition of protein C activity and fibrinolysis [75,76].
Another mechanism that suggests the presence of an “amplification loop” (Figure 2) is the interaction of protease-activated receptors (PARs) with coagulation factors, in particular TF-VIIa and factor Xa. This interaction results in the activation of intracellular signal transduction by endothelial cells, which also contributes to the amplification of the inflammatory response. Nevertheless, this mechanism has not yet been sufficiently studied in neonates [77].
The development of sepsis is associated with an increased release of plasminogen activator inhibitor type 1 (PAI-1) from endothelial cells, which inhibits the activity of plasmin. Bacteremia is associated with the early activation of fibrinolysis due to increased tissue-type plasminogen activator (tPA) levels, which in turn leads to a reciprocal release of PAI-1. However, the appearance of tPA is not the sole factor responsible for the increase in PAI-1 levels; the circulation of a number of cytokines (TNF-α, IL-6, etc.) affects this process. Elevated levels of TNF-α and PAI-1 in patients are directly correlated with the severity of DIC and sepsis. Furthermore, these levels are significantly associated with an unfavorable prognosis and a high risk of mortality. In a study of 107 children with sepsis, Green et al. examined the levels of TF and PAI-1 antigens. The results indicated that elevated TF and PAI-1 levels were associated with increased IL-6, cardiovascular and renal abnormalities, liver failure, coagulopathy and increased mortality (p < 0.05) [78].
Another crucial aspect of the hemostasis system is the thrombin-activated inhibitor of fibrinolysis (TAFI) [79,80,81]. The activated form of TAFI has the capacity to suppress fibrinolysis. This is achieved by the removal of the terminal lysine molecule in fibrin, thereby inhibiting the high-affinity binding site for plasmin [82]. The existing literature contains information on TAFI gene polymorphisms, but it is not yet known which gene variants are associated with a more severe disease course [83]. The role of TAFI in neonates is poorly understood. Emonts et al. observed a decrease in TAFI levels in patients with septic shock and an increase in TAFI activation peptide (TAFI-AP) in patients with the pediatric DIC [84].
The complement system plays a pivotal role in the immune response, and the effective neutralization of foreign agents depends on it. In sepsis, there is a failure of the complement system to respond adequately to infection, which results in the uncontrolled release of chemoattractants C3a and C5a that bind to receptors on the surface of macrophages and neutrophils [85]. Component C5a activates the wall coagulation system, namely factor XII and kallikrein, which is accompanied by thrombosis and development of DIC. New therapies targeting the complement system may be an effective way to combat septic shock and coagulation disorders in children [86].
In addition to the clinical manifestations of DIC, patients with septic shock may present with signs of thrombotic thrombocytopenic purpura (TTP). TTP is a pathology resulting from congenital or more commonly acquired deficiency of the metalloproteinase ADAMTS-13, whose main role is to cleave vWF multimers into monomeric fragments [87]. This deficiency results in microvascular obstruction, which in turn causes organ damage, particularly in the brain and kidneys. Additionally, thrombocytopenia and non-immune hemolytic anemia are observed [88]. In addition to overuse, thrombocytopenia (platelet count less than 100×109/l) in patients with sepsis may be due to either delayed platelet formation or spleen sequestration [89]. The formation of vWF multimers is stimulated by inflammatory mediators, including IL-8 and TNF-α, whereas the action of ADAMTS-13 is inhibited by IL-6 and antimicrobial peptides secreted by neutrophils [90]. Furthermore, during the inflammatory process, vWF and ADAMTS-13 are oxidized, which impairs the cleavage of vWF multimers by metalloproteinases [91].
A number of studies have reported that more than one-third of patients with sepsis have ADAMTS-13 levels 2 times lower than normal, and approximately 15% of patients have levels less than 10% of normal. A reduction in ADAMTS-13 levels is associated with an increased risk of mortality in patients with sepsis and septic shock [92,93,94,95]. Enzyme deficiency results in the accumulation and prolongation of vWF action, which is associated with an increased risk of mortality in patients due to the formation of prothrombotic status [96,97]. Papadogeorgou et al. demonstrated a significant decrease in ADAMTS-13 levels in neonates with sepsis during the acute phase of infection compared to controls (488.5 ± 75.4 ng/ml and 577.2 ± 113.6 ng/ml, p = 0.015) [98].
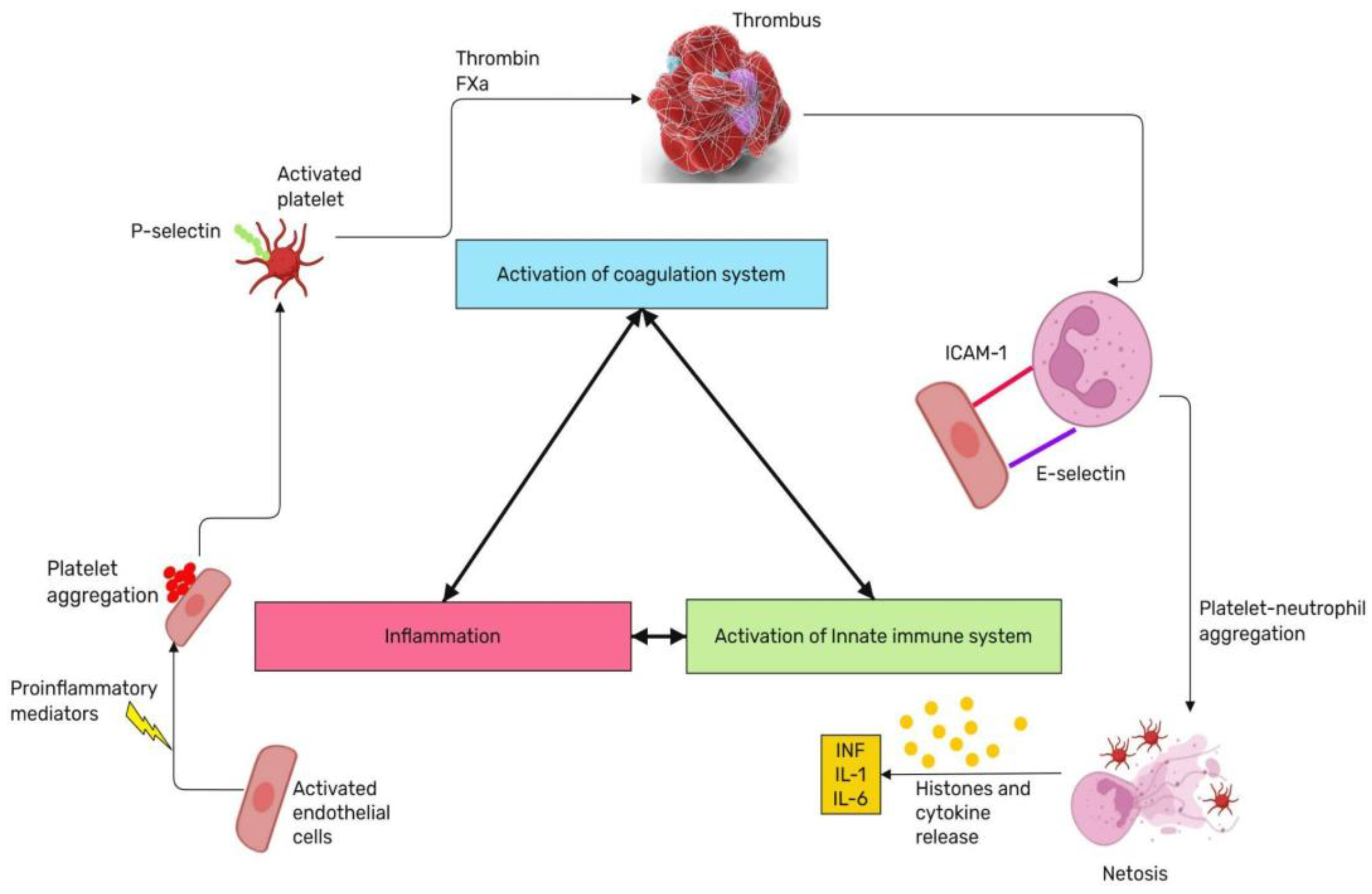
The role of platelets in the coagulopathy associated with sepsis is significant. During the inflammatory process, P-selectin (intercellular adhesion protein), is expressed on the platelet surface. P-selectin is located in α-granules of platelets and Weibel-Palade secretory granules of endothelial cells, and is involved in the primary interaction between polymorphonuclear neutrophils and endotheliocytes. In conjunction with cytokines, it is capable of regulating the synthesis of integrins [99]. Bacteria from the Staphylococcus and Escherichia coli families play a role in increasing GPIIb/IIIa receptor expression on activated platelet surfaces and activation of FcγRIIA [100]. Platelets also help to attract other cells of innate immunity such as granulocytes, monocytes and innate lymphoid cells (ICL) [101]. Consequently, platelets play a crucial role in the immunological response to bacterial invasion.
In patients with septic shock, thrombocytopenia is frequently accompanied by augmented platelet consumption for clot formation [102]. Neonatal thrombocytopenia more likely happens due to a reduction in the expression of platelet Toll-like receptor 4 (TLR-4), which is associated with an increased mortality rate [103]. A reduction in MyD88 expression on monocytes is also observed in neonates, which is associated with an increased incidence of severe bacterial infections and septicemia [104]. Also, preterm neonates with histologically confirmed chorioamnionitis had higher levels of CD40L expression in platelets compared to the control group (5.3 +/- 2.9% vs. 1.6+/-0.7%, p<0.05), indicating a significant involvement of platelets in the pathological process [105,106].
Recently, the role of neutrophils and the formation of neutrophil extracellular traps (NETs), or netosis, in the pathogenesis of sepsis has become increasingly significant. For a considerable period, neutrophils were regarded as a uniform population. However, recent studies demonstrated that the cells can be subdivided according to their density, expression of surface markers and stage of maturation [107]. NETs consist of modified chromatin and proteins of cytoplasm, nuclei, and granules of neutrophils with antimicrobial activity. NETs can be triggered not only by microorganisms, but also by platelets, immune complexes, proteins of the complement system, anti-inflammatory cytokines and other biologically active substances [108]. NETs form a framework for binding platelets, erythrocytes, and plasma proteins [109]. The formation of neutrophil extracellular traps (NETs) is reduced in neonates born preterm, which is associated with an elevated incidence of sepsis during the neonatal period [110]. Although the formation of NETs reduce the spread of infection, they are also associated with the development of DIC and microvascular damage [111], consequently, further research is required to elucidate the mechanism in children.
The damage to the endothelial glycocalyx can lead to sepsis in children. The glycocalyx plays a pivotal role in maintaining vascular homeostasis, controlling vascular permeability and microcirculation, preventing microvascular thrombosis and regulating leukocyte adhesion. The sympathoadrenal system can be hyperactivated in response to shock, which can subsequently lead to damage to endothelial cells and the glycocalyx. The anticoagulation system interacts with the endothelial glycocalyx system via several components, including antithrombin III and activated factors IX and X. The anticoagulant activity of antithrombin III is enhanced by binding to heparan sulphate — a structural link of the glycocalyx [112]. A potential marker of glycocalyx damage in neonatal sepsis is matrix metalloproteinases (MMP-8, MMP-9). Studies demonstrated a correlation of MMP-8 and MMP-9 levels with early onset of sepsis and increased risk of multi-organ failure in children [113,114].
MicroRNAs (miRNAs), small non-coding RNA molecules that regulate gene expression by binding to messenger RNA (mRNA) involve in immune and inflammatory responses as modulators of critical biological pathways and processes [115]. Dysregulated miRNA expression profiles have been identified in sepsis, suggesting their potential as both diagnostic and prognostic biomarkers. For instance, specific miRNAs such as miR-155-5p, miR-21, miR-223, miR-146a, and miR-125a have shown promise in detecting sepsis, with pooled sensitivities and specificities ranging from 0.67 to 0.85 and SROC values demonstrating their diagnostic accuracy [116,117].
MiR-146a is known to modulate the immune response by targeting key signaling molecules such as TRAF6 and IRAK 1-5, which are involved in the NF-κB pathway. Its upregulation has been observed in septic patients, indicating its role in dampening excessive inflammatory responses. Similarly, miR-150 levels are significantly reduced in sepsis, correlating with disease severity and mortality. This miRNA affects the activation and function of immune cells, thus serving as a potential prognostic marker [115]. MiR-223, another miRNA of interest, regulates granulocyte function and inflammation by targeting various mRNAs involved in these processes. Its expression is dysregulated in septic shock, making it a viable candidate for both diagnostic and prognostic applications.
Compared to traditional diagnostic methods such as leukocytosis and fever monitoring, miRNAs offer a more specific and stable biomarker profile. Their presence in circulating blood makes them accessible for non-invasive testing, potentially leading to earlier and more accurate diagnosis of septic shock [118]. This novel approach not only aids in early detection but also provides insights into the molecular mechanisms underlying sepsis, paving the way for targeted therapeutic interventions.
2.7. The Role of Convergent Model of Coagulation in Septic Shock
The Convergent Model of Coagulation represents a paradigm shift in our understanding of hemostasis and thrombosis, integrating inflammation and innate immune activation as a unified response to vascular injury [119]. This model builds upon previous advancements in the knowledge in coagulation cascade, by incorporating the role of damage-associated molecular patterns (DAMPs) which facilitate interactions within and between systems to reinforce and resolve clot formation. The aim of this model is to extend the boundaries of coagulation to address novel diagnostics and therapeutics for contemporary medical challenges, highlighted by the COVID-19 pandemic and vaccine-induced immune thrombotic thrombocytopenia.
The Convergent Model of Coagulation describes the interaction between the coagulation pathways and the innate immune system during vascular injury, highlighting a collaborative mechanism essential for clot formation. Upon vascular injury, the coagulation cascade is initiated, leading to the activation of various immune cells such as platelets, monocytes/macrophages, and neutrophils. Platelets not only participate in clot formation but also release cytokines and chemokines that recruit additional immune cells to the site of injury, thereby reinforcing the immune response. Monocytes and macrophages contribute by expressing tissue factor (TF), a critical initiator of the extrinsic coagulation pathway, further bridging coagulation with immune activation. Neutrophils, another key component, release extracellular traps (NETs) that provide a scaffold for clot formation and capture pathogens, simultaneously enhancing both coagulation and immune defense. This integrated response underscores the complex yet coordinated interactions between the coagulation system and innate immunity in maintaining hemostasis and defending against infections [120].
Figure 3.
The concept of Coagulation Convergent Model.
3. The Early Diagnosis and Treatment of Septic Shock
In accordance with the recommendations of international guidelines, a systematic screening process for sepsis and septic shock is indicated when acute multiorgan failure is identified [121]. The timely identification of sepsis and septic shock allows for the administration of appropriate treatment. The diagnosis of sepsis is primarily based on the isolation of the pathogen in blood cultures. It is therefore necessary to isolate the pathogen before antibiotic therapy is initiated. Furthermore, it is essential to differentiate between septic shock and other forms of shock, which may exhibit similar symptoms. Lactate is a nonspecific marker of septic shock, reflecting the presence of tissue hypoperfusion. However, blood lactate measurement is not indicated according to international guidelines.
The treatment of septic shock encompasses a range of interventions, including cardiovascular and respiratory support. In the event of cardiovascular damage, infusion therapy or inotropic support is required [122]. If the neonate exhibits symptoms indicative of septic shock, including cyanosis, marbling, and a weakened pulse wave, it is recommended to start treatment with prostaglandins [123]. In 2020, Weiss et al. published the International Guidelines for the management of septic shock and organ dysfunction associated with sepsis in children. These guidelines include the following treatment steps [121]:
3.1. Antimicrobial Therapy
It is recommended that antibiotic therapy be initiated without delay in neonates presenting with the first signs of septic shock. Nevertheless, in children with multi-organ failure associated with sepsis but without symptoms of septic shock, antimicrobial therapy is also recommended. It is better to choose a broad-spectrum antibiotic with a wide therapeutic window to avoid the development of undesirable side effects. Cancellation of antibiotic therapy is possible in case of its ineffectiveness, development of side effects and absence of isolated pathogen. Intravascular access is not recommended, as catheters can act as an additional source of infection and may also complicate the course of septic shock, prolonging the recovery period [124]. The high mortality of neonates with septic shock is a consequence of inappropriate or delayed antibiotic therapy. The safest drugs should be prescribed, taking into account all pathological symptoms of the neonate and the risk-benefit ratio for each patient, based on the individuality of each case. Third-generation cephalosporins (ceftriaxone) may be employed as an initial therapeutic option for out-of-hospital sepsis. In the event of antibiotic resistance to cephalosporins, it is necessary to alter the approach to antibiotic therapy and prescribe a drug from the aminoglycoside group [125]. The greatest challenge in the clinical management of sepsis and other serious infections caused by antibiotic-resistant bacteria, such as Methicillin-resistant Staphylococcus aureus (MRSA), is the lack of effective therapeutic options. In such cases, vancomycin is often added to the treatment regimen to enhance its efficacy.
3.2. Infusion Therapy
Infusion therapy to correct the hypovolemia caused by septic shock is recommended as 40-60 ml/kg bolus (10-20 ml/kg bolus) during the first hour. Concurrently, both BP and pulse control should be carried out. If signs of fluid overload develop, infusion therapy should be discontinued. It is recommended that infusion therapy be replaced with crystalloids, as they have fewer side effects, rather than albumin and physiological solution. Starch (e.g., Hydroxyethyl Starch) is not recommended as a treatment for septic shock in children. In a study involving adult patients with septic shock, starch increased the risk of death, coagulopathy, and acute kidney injury [126]. The measurements of lactate levels are not recommended as a marker of septic shock in children. However, they can be used to assess the adequacy and effectiveness of infusion therapy [127]. Elevated lactate levels may indicate incomplete or inadequate hemodynamic resuscitation, which in turn necessitates the continuation of infusion therapy or an increase in the bolus fluid volume.
3.3. Vasoactive Drugs
International guidelines recommend the use of adrenaline or noradrenaline instead of dopamine as first-line therapy in children with septic shock. If the signs of impaired perfusion are observed following infusion therapy, the administration of vasoactive drugs via intravenous or intraosseous assesses (where available) should be initiated. A comparison of the efficacy of adrenaline and dopamine has demonstrated that adrenaline therapy has been shown to reduce mortality, in contrast to dopamine (OR, 0.63; 95% CI, 0.40-0.99) [128,129].
3.4. Corticosteroids
In accordance with international clinical guidelines, the use of glucocorticosteroids is acceptable if infusion therapy and therapy with vasoactive drugs is not effective. A study demonstrated the efficacy of glucocorticosteroid therapy in children. The administration of glucocorticosteroids resulted in earlier relief of septic shock (p=0,046) [130]. Furthermore, there are no more extensive or detailed studies in the pediatric population on the use of hydrocortisone in the therapy of septic shock.
3.5. Antipyretic Therapy
There is no consensus among healthcare professionals regarding the use of antipyretics in children. However, international guidelines do recommend their use in patients with septic shock.
Currently, there is no unambiguous and uniform protocol for the management of neonatal septic shock in neonates. Treatment depends on numerous factors, including the age and weight of the child, the presence or absence of nonspecific symptoms, comorbidities, and the genetically determined response to drug therapy. Primarily, therapy for septic shock should aim to save the patient's life, offset adverse symptoms of the underlying disease, and minimize undesirable side effects of drug therapy. International guidelines provide a general framework for the approach to therapy of septic shock.
4. Conclusions
The impact of FIRS and septic shock on the newborn organism is significant, affecting all systems. It is important to consider the changes occurring in the still immature hemostasis system. The nonspecific clinical features of septic shock, which is characterized by damage to various body systems (from cardiovascular to endocrine), represents a significant challenge for clinicians. The clinical manifestations of newborns differ significantly from adults due to the unique features of the organism. A deeper understanding of the underlying pathogenic mechanisms will facilitate the development of more effective therapeutic approaches and improve the prognosis for these children.
Author Contributions
Conceptualization, Victoria Bitsadze, Alexander Makatsariya; methodology, Alexander Vorobev, Arina Lazarchuk; data curation, Anna Karpova, Aleksei Mostovoi, Nart Kuneshko; software Maria Tretyakova, Armen Blbulyan, Kristina Grigoreva, Nilufar Gashimova; validation, Alena Tatarintseva, Natalia Makatsariya and Daredzhan Kapanadze; formal analysis, Grigoris Gerotziafas, Alexander Makatsariya; writing—original draft preparation, Jean-Christophe Gris, Ismail Elalamy, Marina Zainulina; visualization, Jamilya Khizroeva; All authors have read and agreed to the published version of the manuscript.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Linnikov V.I., Linnikov S.V., Makatsariya N.A. Sanarelli and Schwartzman, a historical background. Obstetrics, Gynecology and Reproduction. 2022;16(3):324-327. (In Russ.). [CrossRef]
- Chakraborty RK, Burns B. Systemic Inflammatory Response Syndrome. 2023 May 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449.
- Wang Y, Dong H, Dong T, Zhao L, Fan W, Zhang Y, Yao W. Treatment of cytokine release syndrome-induced vascular endothelial injury using mesenchymal stem cells. Mol Cell Biochem. 2024 May;479(5):1149-1164. Epub 2023 Jul 1. PMID: 37392343. [CrossRef]
- Beznoshchenko G.B. Sindrom sistemnogo vospalitel'nogo otveta v akusherskoj klinike: reshennye voprosy I nereshennye problemy // Rossijskij vestnik akushera-ginekologa. 2018. T.18, No4. S.6–10. [CrossRef]
- Sikora JP, Karawani J, Sobczak J. Neutrophils and the Systemic Inflammatory Response Syndrome (SIRS). Int J Mol Sci. 2023 Aug 30;24(17):13469. PMID: 37686271; PMCID: PMC10488036. [CrossRef]
- Medzidova MK, Tiutiunnik VL, Kan NE, Kurchakova TA, Kokoeva DN. The role of systemic inflammatory response syndrome in preterm labour development. Russian Journal of Human Reproduction. 2016;22(2):116-120. (In Russ.) https://doi.org/10.17116/repro2016222116-120.
- De Felice C, De Capua B, Costantini D, Martufi C, Toti P, Tonni G, Laurini R, Giannuzzi A, Latini G. Recurrent otitis media with effusion in preterm infants with histologic chorioamnionitis--a 3 years follow-up study. Early Hum Dev. 2008 Oct;84(10):667-71. Epub 2008 Aug 29. PMID: 18760552. [CrossRef]
- Karrow NA. Activation of the hypothalamic-pituitary-adrenal axis and autonomic nervous system during inflammation and altered programming of the neuroendocrine-immune axis during fetal and neonatal development: lessons learned from the model inflammagen, lipopolysaccharide. Brain Behav Immun. 2006 Mar;20(2):144-58. Epub 2005 Jul 14. PMID: 16023324. [CrossRef]
- Para R, Romero R, Miller D, Galaz J, Done B, Peyvandipour A, Gershater M, Tao L, Motomura K, Ruden DM, Isherwood J, Jung E, Kanninen T, Pique-Regi R, Tarca AL, Gomez-Lopez N. The Distinct Immune Nature of the Fetal Inflammatory Response Syndrome Type I and Type II. Immunohorizons. 2021 Sep 14;5(9):735-751. PMID: 34521696; PMCID: PMC9394103. [CrossRef]
- Glavina-Durdov M, Springer O, Capkun V, Saratlija-Novaković Z, Rozić D, Barle M. The grade of acute thymus involution in neonates correlates with the duration of acute illness and with the percentage of lymphocytes in peripheral blood smear. Pathological study. Biol Neonate. 2003;83(4):229-34. PMID: 12743450. [CrossRef]
- Straňák Zbyněk, Berka Ivan, Širc Jan, Urbánek Jan, Feyereisl Jaroslav, Korček Peter. Role of umbilical interleukin-6, procalcitonin and C-reactive protein measurement in the diagnosis of fetal inflammatory response syndrome. Ceska Gynekol. 2021;86(2):80-85. English. PMID: 34020553. [CrossRef]
- Persson G, Jørgensen N, Nilsson LL, Andersen LHJ, Hviid TVF. A role for both HLA-F and HLA-G in reproduction and during pregnancy? Hum Immunol. 2020 Apr;81(4):127-133. Epub 2019 Sep 24. PMID: 31558330. [CrossRef]
- Nomiyama M, Nakagawa T, Yamasaki F, Hisamoto N, Yamashita N, Harai A, Gondo K, Ikeda M, Tsuda S, Ishimatsu M, Oshima Y, Ono T, Kozuma Y, Tsumura K. Contribution of Fetal Inflammatory Response Syndrome (FIRS) with or without Maternal-Fetal Inflammation in The Placenta to Increased Risk of Respiratory and Other Complications in Preterm Neonates. Biomedicines. 2023 Feb 18;11(2):611. PMID: 36831147; PMCID: PMC9953376. [CrossRef]
- Romero R, Savasan ZA, Chaiworapongsa T, Berry SM, Kusanovic JP, Hassan SS, Yoon BH, Edwin S, Mazor M. Hematologic profile of the fetus with systemic inflammatory response syndrome. J Perinat Med. 2011 Sep 30;40(1):19-32. PMID: 21957997; PMCID: PMC3380620. [CrossRef]
- Ead JK, Armstrong DG. Granulocyte-macrophage colony-stimulating factor: Conductor of the wound healing orchestra? Int Wound J. 2023 Apr;20(4):1229-1234. Epub 2023 Jan 12. PMID: 36632762; PMCID: PMC10031218. [CrossRef]
- Zurochka A.V., Zurochka V.A., Dobrynina M.A., Gritsenko V.A. Immunobiological properties of granulocytemacrophage colony-stimulating factor and synthetic peptides of his active center. Medical Immunology (Russia). 2021;23(5):1031-1054. (In Russ.). [CrossRef]
- Chaiworapongsa T, Romero R, Berry SM, Hassan SS, Yoon BH, Edwin S, Mazor M. The role of granulocyte colony-stimulating factor in the neutrophilia observed in the fetal inflammatory response syndrome. J Perinat Med. 2011 Nov;39(6):653-66. Epub 2011 Jul 30. PMID: 21801092; PMCID: PMC3382056. [CrossRef]
- Leikin E, Garry D, Visintainer P, Verma U, Tejani N. Correlation of neonatal nucleated red blood cell counts in preterm infants with histologic chorioamnionitis. Am J Obstet Gynecol. 1997 Jul;177(1):27-30. PMID: 9240578. [CrossRef]
- Mandel D, Oron T, Mimouni GS, Littner Y, Dollberg S, Mimouni FB. The effect of prolonged rupture of membranes on circulating neonatal nucleated red blood cells. J Perinatol. 2005 Nov;25(11):690-3. PMID: 16222345. [CrossRef]
- Romero R, Soto E, Berry SM, Hassan SS, Kusanovic JP, Yoon BH, Edwin S, Mazor M, Chaiworapongsa T. Blood pH and gases in fetuses in preterm labor with and without systemic inflammatory response syndrome. J Matern Fetal Neonatal Med. 2012 Jul;25(7):1160-70. Epub 2011 Dec 20. PMID: 21988103; PMCID: PMC3383905. [CrossRef]
- Zaharie GC, Drugan T, Crivii C, Muresan D, Zaharie A, Hășmășanu MG, Zaharie F, Matyas M. Postpartum assessment of fetal inflammatory response syndrome in a preterm population with premature rupture of membranes: A Romanian study. Exp Ther Med. 2021 Dec;22(6):1427. Epub 2021 Oct 11. PMID: 34707708; PMCID: PMC8543235. [CrossRef]
- Kallapur SG, Willet KE, Jobe AH, Ikegami M, Bachurski CJ. Intra-amniotic endotoxin: chorioamnionitis precedes lung maturation in preterm lambs. Am J Physiol Lung Cell Mol Physiol. 2001 Mar;280(3):L527-36. PMID: 11159037. [CrossRef]
- Metcalfe A, Lisonkova S, Sabr Y, Stritzke A, Joseph KS. Neonatal respiratory morbidity following exposure to chorioamnionitis. BMC Pediatr. 2017 May 17;17(1):128. PMID: 28514958; PMCID: PMC5436447. [CrossRef]
- Plakkal N, Soraisham AS, Trevenen C, Freiheit EA, Sauve R. Histological chorioamnionitis and bronchopulmonary dysplasia: a retrospective cohort study. J Perinatol. 2013 Jun;33(6):441-5. Epub 2012 Dec 13. PMID: 23238570. [CrossRef]
- Yoon BH, Romero R, Kim KS, Park JS, Ki SH, Kim BI, Jun JK. A systemic fetal inflammatory response and the development of bronchopulmonary dysplasia. Am J Obstet Gynecol. 1999 Oct;181(4):773-9. PMID: 10521727. [CrossRef]
- Sarno L, Della Corte L, Saccone G, Sirico A, Raimondi F, Zullo F, Guida M, Martinelli P, Maruotti GM. Histological chorioamnionitis and risk of pulmonary complications in preterm births: a systematic review and Meta-analysis. J Matern Fetal Neonatal Med. 2021 Nov;34(22):3803-3812. Epub 2019 Nov 13. PMID: 31722581. [CrossRef]
- Wu J, Wang Y, Zhao A, Wang Z. Lung Ultrasound for the Diagnosis of Neonatal Respiratory Distress Syndrome: A Meta-analysis. Ultrasound Q. 2020 Jun;36(2):102-110. PMID: 32511203; PMCID: PMC7289125. [CrossRef]
- Dessardo NS, Dessardo S, Mustać E, Banac S, Petrović O, Peter B. Chronic lung disease of prematurity and early childhood wheezing: is foetal inflammatory response syndrome to blame? Early Hum Dev. 2014 Sep;90(9):493-9. Epub 2014 Jul 21. PMID: 25051540. [CrossRef]
- Yap V, Perlman JM. Mechanisms of brain injury in newborn infants associated with the fetal inflammatory response syndrome. Semin Fetal Neonatal Med. 2020 Aug;25(4):101110. Epub 2020 Apr 9. PMID: 32303463. [CrossRef]
- Muraskas JK, Kelly AF, Nash MS, Goodman JR, Morrison JC. The role of fetal inflammatory response syndrome and fetal anemia in nonpreventable term neonatal encephalopathy. J Perinatol. 2016 May;36(5):362-5. Epub 2016 Jan 21. PMID: 26796124. [CrossRef]
- Yoon BH, Romero R, Kim CJ, Koo JN, Choe G, Syn HC, Chi JG. High expression of tumor necrosis factor-alpha and interleukin-6 in periventricular leukomalacia. Am J Obstet Gynecol. 1997 Aug;177(2):406-11. PMID: 9290459. [CrossRef]
- Kadhim H, Tabarki B, Verellen G, De Prez C, Rona AM, Sébire G. Inflammatory cytokines in the pathogenesis of periventricular leukomalacia. Neurology. 2001 May 22;56(10):1278-84. PMID: 11376173. [CrossRef]
- Stolp HB, Dziegielewska KM, Ek CJ, Habgood MD, Lane MA, Potter AM, Saunders NR. Breakdown of the blood-brain barrier to proteins in white matter of the developing brain following systemic inflammation. Cell Tissue Res. 2005 Jun;320(3):369-78. Epub 2005 Apr 22. PMID: 15846513. [CrossRef]
- Zhang Z, Jyoti A, Balakrishnan B, Williams M, Singh S, Chugani DC, Kannan S. Trajectory of inflammatory and microglial activation markers in the postnatal rabbit brain following intrauterine endotoxin exposure. Neurobiol Dis. 2018 Mar;111:153-162. Epub 2017 Dec 21. PMID: 29274431; PMCID: PMC6082145. [CrossRef]
- Giovannini E, Bonasoni MP, Pascali JP, Giorgetti A, Pelletti G, Gargano G, Pelotti S, Fais P. Infection Induced Fetal Inflammatory Response Syndrome (FIRS): State-of- the-Art and Medico-Legal Implications—A Narrative Review. Microorganisms. 2023; 11(4):1010. [CrossRef]
- Goncalves LF, Cornejo P, Towbin R. Neuroimaging findings associated with the fetal inflammatory response syndrome. Semin Fetal Neonatal Med. 2020 Aug;25(4):101143. Epub 2020 Aug 3. PMID: 32800654. [CrossRef]
- Boog G. Asphyxie périnatale et infirmité motrice d’origine cérébrale (I- Le diagnostic). Gynécologie Obstétrique & Fertilité 2010; 38: 261–277.
- Song JS, Woo SJ, Park KH, Kim H, Lee KN, Kim YM. Association of inflammatory and angiogenic biomarkers in maternal plasma with retinopathy of prematurity in preterm infants. Eye (Lond). 2023 Jun;37(9):1802-1809. Epub 2022 Sep 15. PMID: 36109603; PMCID: PMC10275990. [CrossRef]
- Park YJ, Woo SJ, Kim YM, Hong S, Lee YE, Park KH. Immune and Inflammatory Proteins in Cord Blood as Predictive Biomarkers of Retinopathy of Prematurity in Preterm Infants. Invest Ophthalmol Vis Sci. 2019 Sep 3;60(12):3813-3820. PMID: 31525777. [CrossRef]
- Gibson B, Goodfriend E, Zhong Y, Melhem NM. Fetal inflammatory response and risk for psychiatric disorders. Transl Psychiatry. 2023 Jun 24;13(1):224. PMID: 37355708; PMCID: PMC10290670. [CrossRef]
- Yoon BH, Kim YA, Romero R, Kim JC, Park KH, Kim MH, Park JS. Association of oligohydramnios in women with preterm premature rupture of membranes with an inflammatory response in fetal, amniotic, and maternal compartments. Am J Obstet Gynecol. 1999 Oct;181(4):784-8. PMID: 10521729. [CrossRef]
- Lee SE, Romero R, Lee SM, Yoon BH. Amniotic fluid volume in intra-amniotic inflammation with and without culture-proven amniotic fluid infection in preterm premature rupture of membranes. J Perinat Med. 2010;38(1):39-44. PMID: 19708825; PMCID: PMC2887661. [CrossRef]
- Azpurua H, Dulay AT, Buhimschi IA, Bahtiyar MO, Funai E, Abdel-Razeq SS, Luo G, Bhandari V, Copel JA, Buhimschi CS. Fetal renal artery impedance as assessed by Doppler ultrasound in pregnancies complicated by intraamniotic inflammation and preterm birth. Am J Obstet Gynecol. 2009 Feb;200(2):203.e1-11. PMID: 19185102; PMCID: PMC3791328. [CrossRef]
- Galinsky R, Moss TJ, Gubhaju L, Hooper SB, Black MJ, Polglase GR. Effect of intra-amniotic lipopolysaccharide on nephron number in preterm fetal sheep. Am J Physiol Renal Physiol. 2011 Aug;301(2):F280-5. Epub 2011 May 18. PMID: 21593183. [CrossRef]
- Stantsidou A, Pagonopoulou O, Deftereou T. Effects of chorioamnionitis in fetal renal glomeruli. Hippokratia. 2021 Apr-Jun;25(2):98. PMID: 35937516; PMCID: PMC9347347.
- Muk T, Jiang PP, Stensballe A, Skovgaard K, Sangild PT, Nguyen DN. Prenatal Endotoxin Exposure Induces Fetal and Neonatal Renal Inflammation via Innate and Th1 Immune Activation in Preterm Pigs. Front Immunol. 2020 Sep 30;11:565484. PMID: 33193334; PMCID: PMC7643587. [CrossRef]
- Kuypers E, Wolfs TG, Collins JJ, Jellema RK, Newnham JP, Kemp MW, Kallapur SG, Jobe AH, Kramer BW. Intraamniotic lipopolysaccharide exposure changes cell populations and structure of the ovine fetal thymus. Reprod Sci. 2013 Aug;20(8):946-56. Epub 2013 Jan 11. PMID: 23314960; PMCID: PMC3702021. [CrossRef]
- Luciano AA, Yu H, Jackson LW, Wolfe LA, Bernstein HB. Preterm labor and chorioamnionitis are associated with neonatal T cell activation. PLoS One. 2011 Feb 8;6(2):e16698. PMID: 21347427; PMCID: PMC3035646. [CrossRef]
- Melville JM, Bischof RJ, Meeusen EN, Westover AJ, Moss TJ. Changes in fetal thymic immune cell populations in a sheep model of intrauterine inflammation. Reprod Sci. 2012 Jul;19(7):740-7. Epub 2012 Mar 14. PMID: 22421448. [CrossRef]
- Kramer BW, Moss TJ, Willet KE, Newnham JP, Sly PD, Kallapur SG, Ikegami M, Jobe AH. Dose and time response after intraamniotic endotoxin in preterm lambs. Am J Respir Crit Care Med. 2001 Sep 15;164(6):982-8. PMID: 11587983. [CrossRef]
- Kuypers E, Willems MG, Jellema RK, Kemp MW, Newnham JP, Delhaas T, Kallapur SG, Jobe AH, Wolfs TG, Kramer BW. Responses of the spleen to intraamniotic lipopolysaccharide exposure in fetal sheep. Pediatr Res. 2015 Jan;77(1-1):29-35. Epub 2014 Oct 6. PMID: 25285474. [CrossRef]
- Musilova I, Kacerovsky M, Hornychova H, Kostal M, Jacobsson B. Pulsation of the fetal splenic vein--a potential ultrasound marker of histological chorioamnionitis and funisitis in women with preterm prelabor rupture of membranes. Acta Obstet Gynecol Scand. 2012 Sep;91(9):1119-23. PMID: 22574855. [CrossRef]
- Yan X, Managlia E, Tan XD, De Plaen IG. Prenatal inflammation impairs intestinal microvascular development through a TNF-dependent mechanism and predisposes newborn mice to necrotizing enterocolitis. Am J Physiol Gastrointest Liver Physiol. 2019 Jul 1;317(1):G57-G66. Epub 2019 May 24. PMID: 31125264; PMCID: PMC6689733. [CrossRef]
- Razak A, Malhotra A. Fetal inflammatory response spectrum: mapping its impact on severity of necrotising enterocolitis. Pediatr Res. 2024 Apr;95(5):1179-1180. Epub 2023 Dec 16. PMID: 38104186. [CrossRef]
- Bieghs V, Vlassaks E, Custers A, van Gorp PJ, Gijbels MJ, Bast A, Bekers O, Zimmermann LJ, Lütjohann D, Voncken JW, Gavilanes AW, Kramer BW, Shiri-Sverdlov R. Chorioamnionitis induced hepatic inflammation and disturbed lipid metabolism in fetal sheep. Pediatr Res. 2010 Dec;68(6):466-72. PMID: 20717072. [CrossRef]
- Heymans C, den Dulk M, Lenaerts K, Heij LR, de Lange IH, Hadfoune M, van Heugten C, Kramer BW, Jobe AH, Saito M, Kemp MW, Wolfs TGAM, van Gemert WG. Chorioamnionitis induces hepatic inflammation and time-dependent changes of the enterohepatic circulation in the ovine fetus. Sci Rep. 2021 May 14;11(1):10331. PMID: 33990635; PMCID: PMC8121927. [CrossRef]
- Sergeeva V.A., Shabalov N.P., Aleksandrovich Yu.S., and Nesterenko S.N. \"Predopredelyaet li fetal'nyj vospalitel'nyj otvet oslozhnyonnoe techenie rannego neonatal'nogo perioda?\" Bajkal'skij medicinskij zhurnal, vol. 93, no. 2, 2010, pp. 75-80.
- Watterberg KL, Demers LM, Scott SM, Murphy S. Chorioamnionitis and early lung inflammation in infants in whom bronchopulmonary dysplasia develops. Pediatrics. 1996 Feb;97(2):210-5. PMID: 8584379.
- Volpe JJ. Postnatal sepsis, necrotizing entercolitis, and the critical role of systemic inflammation in white matter injury in premature infants. J Pediatr. 2008 Aug;153(2):160-3. PMID: 18639727; PMCID: PMC2593633. [CrossRef]
- Eloundou SN, Lee J, Wu D, Lei J, Feller MC, Ozen M, Zhu Y, Hwang M, Jia B, Xie H, Clemens JL, McLane MW, AlSaggaf S, Nair N, Wills-Karp M, Wang X, Graham EM, Baschat A, Burd I. Placental malperfusion in response to intrauterine inflammation and its connection to fetal sequelae. PLoS One. 2019 Apr 3;14(4):e0214951. PMID: 30943260; PMCID: PMC6447225. [CrossRef]
- Luciano AA, Arbona-Ramirez IM, Ruiz R, Llorens-Bonilla BJ, Martinez-Lopez DG, Funderburg N, Dorsey MJ. Alterations in regulatory T cell subpopulations seen in preterm infants. PLoS One. 2014 May 5;9(5):e95867. PMID: 24796788; PMCID: PMC4010410. [CrossRef]
- Muraskas J, Astrug L, Amin S. FIRS: Neonatal considerations. Semin Fetal Neonatal Med. 2020 Aug;25(4):101142. Epub 2020 Aug 26. PMID: 32912755. [CrossRef]
- Agyeman PKA, Schlapbach LJ, Giannoni E, Stocker M, Posfay-Barbe KM, Heininger U, Schindler M, Korten I, Konetzny G, Niederer-Loher A, Kahlert CR, Donas A, Leone A, Hasters P, Relly C, Baer W, Kuehni CE, Aebi C, Berger C; Swiss Pediatric Sepsis Study. Epidemiology of blood culture-proven bacterial sepsis in children in Switzerland: a population-based cohort study. Lancet Child Adolesc Health. 2017 Oct;1(2):124-133. Epub 2017 Jul 21. PMID: 30169202. [CrossRef]
- Wynn JL, Wong HR. Pathophysiology and treatment of septic shock in neonates. Clin Perinatol. 2010 Jun;37(2):439-79. PMID: 20569817; PMCID: PMC2891980. [CrossRef]
- Samsygina G.A. \"Sepsis i septicheskij shok u novorozhdennyh detej\" Pediatriya. Zhurnal im. G. N. Speranskogo, vol. 87, no. 1, 2009, pp. 120-126.
- Spaggiari V, Passini E, Crestani S, Roversi MF, Bedetti L, Rossi K, Lucaccioni L, Baraldi C, Della Casa Muttini E, Lugli L, Iughetti L, Berardi A. Neonatal septic shock, a focus on first line interventions. Acta Biomed. 2022 Jul 1;93(3):e2022141. PMID: 35775767; PMCID: PMC9335427. [CrossRef]
- Schorr CA, Zanotti S, Dellinger RP. Severe sepsis and septic shock: management and performance improvement. Virulence. 2014 Jan 1;5(1):190-9. Epub 2013 Dec 11. PMID: 24335487; PMCID: PMC3916373. [CrossRef]
- Silveira Rde C, Giacomini C, Procianoy RS. Neonatal sepsis and septic shock: concepts update and review. Rev Bras Ter Intensiva. 2010 Sep;22(3):280-90. English, Portuguese. PMID: 25302436.
- Khizroeva J, Makatsariya A, Vorobev A, Bitsadze V, Elalamy I, Lazarchuk A, Salnikova P, Einullaeva S, Solopova A, Tretykova M, Antonova A, Mashkova T, Grigoreva K, Kvaratskheliia M, Yakubova F, Degtyareva N, Tsibizova V, Gashimova N, Blbulyan D. The Hemostatic System in Newborns and the Risk of Neonatal Thrombosis. Int J Mol Sci. 2023 Sep 8;24(18):13864. PMID: 37762167; PMCID: PMC10530883. [CrossRef]
- Andrew M, Vegh P, Johnston M, Bowker J, Ofosu F, Mitchell L. Maturation of the hemostatic system during childhood. Blood. 1992 Oct 15;80(8):1998-2005. PMID: 1391957. [CrossRef]
- Wiedmeier SE, Henry E, Sola-Visner MC, Christensen RD. Platelet reference ranges for neonates, defined using data from over 47,000 patients in a multihospital healthcare system. J Perinatol. 2009 Feb;29(2):130-6. Epub 2008 Sep 25. PMID: 18818663. [CrossRef]
- Sillers L, Van Slambrouck C, Lapping-Carr G. Neonatal Thrombocytopenia: Etiology and Diagnosis. Pediatr Ann. 2015 Jul;44(7):e175-80. PMID: 26171707; PMCID: PMC6107300. [CrossRef]
- Bednarek FJ, Bean S, Barnard MR, Frelinger AL, Michelson AD. The platelet hyporeactivity of extremely low birth weight neonates is age-dependent. Thromb Res. 2009 May;124(1):42-5. Epub 2008 Nov 20. PMID: 19026437. [CrossRef]
- Bitsadze V.O., Sukontseva T.A., Akinshina S.V., Sulina Ya.Yu., Khizroeva J.Kh., Tretyakova M.V., Sultangadzhieva Kh.G., Ungiadze J.Yu., Samburova N.V., Grigoreva K.N., Tsibizova V.I., Shkoda A.S., Blinov D.V., Makatsariya A.D. Septic shock. Obstetrics, Gynecology and Reproduction. 2020;14(3):314-326. (In Russ.). [CrossRef]
- Mal'ceva L.A., and Bazilenko D.V. \"Patogenez tyazhelogo sepsisa i septicheskogo shoka: analiz sovremennyh koncepcij\" Medicina neotlozhnyh sostoyanij, no. 7 (70), 2015, pp. 35-40.
- Bitsadze V.O., Khizroeva J.K., Makatsariya A.D., Slukhanchuk E.V., Tretyakova M.V., Rizzo G., Gris J.R., Elalamy I., Serov V.N., Shkoda A.S., Samburova N.V. COVID-19, septic shock and syndrome of disseminated intravascular coagulation syndrome. Part 1 // Annals of the Russian academy of medical sciences. - 2020. - Vol. 75. - N. 2. - P. 118-128. [CrossRef]
- Levi M, van der Poll T. Coagulation and sepsis. Thromb Res. 2017 Jan;149:38-44. Epub 2016 Nov 19. PMID: 27886531. [CrossRef]
- Green J, Doughty L, Kaplan SS, Sasser H, Carcillo JA. The tissue factor and plasminogen activator inhibitor type-1 response in pediatric sepsis-induced multiple organ failure. Thromb Haemost. 2002 Feb;87(2):218-23. PMID: 11858480.
- Asakura H, Ontachi Y, Mizutani T, Kato M, Ito T, Saito M, Morishita E, Yamazaki M, Suga Y, Miyamoto KI, Nakao S. Depressed plasma activity of plasminogen or alpha2 plasmin inhibitor is not due to consumption coagulopathy in septic patients with disseminated intravascular coagulation. Blood Coagul Fibrinolysis. 2001 Jun;12(4):275-81. PMID: 11460011. [CrossRef]
- Dempfle CE. Das TAFI-System. Die neue Rolle der Fibrinolyse [The TAFI system. The new role of fibrinolysis]. Hamostaseologie. 2007 Sep;27(4):278-81. German. PMID: 17938767.
- Stief TW, Ijagha O, Weiste B, Herzum I, Renz H, Max M. Analysis of hemostasis alterations in sepsis. Blood Coagul Fibrinolysis. 2007 Mar;18(2):179-86. PMID: 17287636. [CrossRef]
- Gando S. Role of fibrinolysis in sepsis. Semin Thromb Hemost. 2013 Jun;39(4):392-9. Epub 2013 Feb 27. PMID: 23446914. [CrossRef]
- Willemse JL, Heylen E, Nesheim ME, Hendriks DF. Carboxypeptidase U (TAFIa): a new drug target for fibrinolytic therapy? J Thromb Haemost. 2009 Dec;7(12):1962-71. Epub 2009 Aug 28. PMID: 19719827; PMCID: PMC3170991. [CrossRef]
- Emonts M, de Bruijne EL, Guimarães AH, Declerck PJ, Leebeek FW, de Maat MP, Rijken DC, Hazelzet JA, Gils A. Thrombin-activatable fibrinolysis inhibitor is associated with severity and outcome of severe meningococcal infection in children. J Thromb Haemost. 2008 Feb;6(2):268-76. Epub 2007 Nov 15. PMID: 18021301. [CrossRef]
- Prodeus A.P., Ustinova M.V., Korsunskiy A.A., Goncharov A.G. New aspects of sepsis and septic shock pathogenesis in children. The complement system as target for an effective therapy // Russian Journal of Infection and Immunity = Infektsiya i immunitet, 2018, vol. 8, no. 1, pp. 19–24. [CrossRef]
- Hazelzet JAde Groot R, van Mierlo G, Joosten KFM, van der Voort E, Eerenberg A, Suur MH, Hop WCJ, Hack CE. 1998. Complement Activation in Relation to Capillary Leakage in Children with Septic Shock and Purpura. Infect Immun 66: https://doi.org/10.1128/iai.66.11.5350-5356.1998.
- Kelwick R, Desanlis I, Wheeler GN, Edwards DR. The ADAMTS (A Disintegrin and Metalloproteinase with Thrombospondin motifs) family. Genome Biol. 2015 May 30;16(1):113. PMID: 26025392; PMCID: PMC4448532. [CrossRef]
- Levi M, Scully M, Singer M. The role of ADAMTS-13 in the coagulopathy of sepsis. J Thromb Haemost. 2018 Apr;16(4):646-651. Epub 2018 Feb 2. PMID: 29337416. [CrossRef]
- Levi M, Opal SM. Coagulation abnormalities in critically ill patients. Crit Care. 2006;10(4):222. PMID: 16879728; PMCID: PMC1750988. [CrossRef]
- Pillai VG, Bao J, Zander CB, McDaniel JK, Chetty PS, Seeholzer SH, Bdeir K, Cines DB, Zheng XL. Human neutrophil peptides inhibit cleavage of von Willebrand factor by ADAMTS13: a potential link of inflammation to TTP. Blood. 2016 Jul 7;128(1):110-9. Epub 2016 May 13. PMID: 27207796; PMCID: PMC4937355. [CrossRef]
- Chen J, Chung DW. Inflammation, von Willebrand factor, and ADAMTS13. Blood. 2018 Jul 12;132(2):141-147. Epub 2018 Jun 4. PMID: 29866815; PMCID: PMC6043979. [CrossRef]
- Peigne V, Azoulay E, Coquet I, Mariotte E, Darmon M, Legendre P, Adoui N, Marfaing-Koka A, Wolf M, Schlemmer B, Veyradier A. The prognostic value of ADAMTS13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13) deficiency in septic shock patients involves interleukin-6 and is not dependent on disseminated intravascular coagulation. Crit Care. 2013 Nov 18;17(6):R273. PMID: 24238574; PMCID: PMC4056532. [CrossRef]
- Habe K, Wada H, Ito-Habe N, Hatada T, Matsumoto T, Ohishi K, Maruyama K, Imai H, Mizutani H, Nobori T. Plasma ADAMTS13, von Willebrand factor (VWF) and VWF propeptide profiles in patients with DIC and related diseases. Thromb Res. 2012 May;129(5):598-602. Epub 2011 Nov 8. PMID: 22070827. [CrossRef]
- Ono T, Mimuro J, Madoiwa S, Soejima K, Kashiwakura Y, Ishiwata A, Takano K, Ohmori T, Sakata Y. Severe secondary deficiency of von Willebrand factor-cleaving protease (ADAMTS13) in patients with sepsis-induced disseminated intravascular coagulation: its correlation with development of renal failure. Blood. 2006 Jan 15;107(2):528-34. Epub 2005 Sep 27. PMID: 16189276. [CrossRef]
- Schwameis M, Schörgenhofer C, Assinger A, Steiner MM, Jilma B. VWF excess and ADAMTS13 deficiency: a unifying pathomechanism linking inflammation to thrombosis in DIC, malaria, and TTP. Thromb Haemost. 2015 Apr;113(4):708-18. Epub 2014 Dec 11. PMID: 25503977; PMCID: PMC4745134. [CrossRef]
- Emmer BT, Ginsburg D, Desch KC. Von Willebrand Factor and ADAMTS13: Too Much or Too Little of a Good Thing? Arterioscler Thromb Vasc Biol. 2016 Dec;36(12):2281-2282. PMID: 27879275; PMCID: PMC5127281. [CrossRef]
- Sonneveld MA, Franco OH, Ikram MA, Hofman A, Kavousi M, de Maat MP, Leebeek FW. Von Willebrand Factor, ADAMTS13, and the Risk of Mortality: The Rotterdam Study. Arterioscler Thromb Vasc Biol. 2016 Dec;36(12):2446-2451. Epub 2016 Oct 13. PMID: 27737864. [CrossRef]
- Papadogeorgou P, Boutsikou T, Boutsikou M, Pergantou E, Mantzou A, Papassotiriou I, Iliodromiti Z, Sokou R, Bouza E, Politou M, Iacovidou N, Valsami S. A Global Assessment of Coagulation Profile and a Novel Insight into Adamts-13 Implication in Neonatal Sepsis. Biology (Basel). 2023 Sep 26;12(10):1281. PMID: 37886991; PMCID: PMC10604288. [CrossRef]
- Kansas GS. Selectins and their ligands: current concepts and controversies. Blood. 1996 Nov 1;88(9):3259-87. PMID: 8896391. [CrossRef]
- Martinod K, Deppermann C. Immunothrombosis and thromboinflammation in host defense and disease. Platelets. 2021 Apr 3;32(3):314-324. Epub 2020 Sep 8. PMID: 32896192. [CrossRef]
- Rossaint J, Margraf A, Zarbock A. Role of Platelets in Leukocyte Recruitment and Resolution of Inflammation. Front Immunol. 2018 Nov 20;9:2712. PMID: 30515177; PMCID: PMC6255980. [CrossRef]
- Iba T, Levy JH. Inflammation and thrombosis: roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis. J Thromb Haemost. 2018 Feb;16(2):231-241. Epub 2017 Dec 21. PMID: 29193703. [CrossRef]
- Finkelstein Y, Shenkman B, Sirota L, Vishne TH, Dardik R, Varon D, Linder N. Whole blood platelet deposition on extracellular matrix under flow conditions in preterm neonatal sepsis. Eur J Pediatr. 2002 May;161(5):270-4. Epub 2002 Mar 16. PMID: 12012223. [CrossRef]
- Sadeghi K, Berger A, Langgartner M, Prusa AR, Hayde M, Herkner K, Pollak A, Spittler A, Forster-Waldl E. Immaturity of infection control in preterm and term newborns is associated with impaired toll-like receptor signaling. J Infect Dis. 2007 Jan 15;195(2):296-302. Epub 2006 Dec 1. PMID: 17191175. [CrossRef]
- Sitaru AG, Speer CP, Holzhauer S, Obergfell A, Walter U, Grossmann R. Chorioamnionitis is associated with increased CD40L expression on cord blood platelets. Thromb Haemost. 2005 Dec;94(6):1219-23. PMID: 16411397. [CrossRef]
- Aloui C, Prigent A, Sut C, Tariket S, Hamzeh-Cognasse H, Pozzetto B, Richard Y, Cognasse F, Laradi S, Garraud O. The signaling role of CD40 ligand in platelet biology and in platelet component transfusion. Int J Mol Sci. 2014 Dec 3;15(12):22342-64. PMID: 25479079; PMCID: PMC4284712. [CrossRef]
- Andryukov B.G., Bogdanova V.D., Lyapun I.N. PHENOTYPIC HETEROGENEITY OF NEUTROPHILS: NEW ANTIMICROBIC CHARACTERISTICS AND DIAGNOSTIC TECHNOLOGIES. Russian journal of hematology and transfusiology. 2019;64(2):211-221. (In Russ.). [CrossRef]
- Kaplan MJ, Radic M. Neutrophil extracellular traps: double-edged swords of innate immunity. J Immunol. 2012 Sep 15;189(6):2689-95. PMID: 22956760; PMCID: PMC3439169. [CrossRef]
- Fuchs TA, Brill A, Duerschmied D, Schatzberg D, Monestier M, Myers DD Jr, Wrobleski SK, Wakefield TW, Hartwig JH, Wagner DD. Extracellular DNA traps promote thrombosis. Proc Natl Acad Sci U S A. 2010 Sep 7;107(36):15880-5. Epub 2010 Aug 23. PMID: 20798043; PMCID: PMC2936604. [CrossRef]
- Hoppenbrouwers T, Boeddha NP, Ekinci E, Emonts M, Hazelzet JA, Driessen GJ, de Maat MP. Neutrophil Extracellular Traps in Children With Meningococcal Sepsis. Pediatr Crit Care Med. 2018 Jun;19(6):e286-e291. PMID: 29432403. [CrossRef]
- McDonald B, Davis RP, Kim SJ, Tse M, Esmon CT, Kolaczkowska E, Jenne CN. Platelets and neutrophil extracellular traps collaborate to promote intravascular coagulation during sepsis in mice. Blood. 2017 Mar 9;129(10):1357-1367. Epub 2017 Jan 10. Erratum in: Blood. 2022 Feb 10;139(6):952. doi: 10.1182/blood.2021014436. PMID: 28073784; PMCID: PMC5345735. [CrossRef]
- Fatmi A, Saadi W, Beltrán-García J, García-Giménez JL, Pallardó FV. The Endothelial Glycocalyx and Neonatal Sepsis. Int J Mol Sci. 2022 Dec 26;24(1):364. PMID: 36613805; PMCID: PMC9820255. [CrossRef]
- Dreschers S, Platen C, Ludwig A, Gille C, Köstlin N, Orlikowsky TW. Metalloproteinases TACE and MMP-9 Differentially Regulate Death Factors on Adult and Neonatal Monocytes After Infection with Escherichia coli. Int J Mol Sci. 2019 Mar 20;20(6):1399. PMID: 30897723; PMCID: PMC6471605. [CrossRef]
- He Y, Du WX, Jiang HY, Ai Q, Feng J, Liu Z, Yu JL. Multiplex Cytokine Profiling Identifies Interleukin-27 as a Novel Biomarker For Neonatal Early Onset Sepsis. Shock. 2017 Feb;47(2):140-147. PMID: 27648693. [CrossRef]
- Formosa A, Turgeon P, Dos Santos CC. Role of miRNA dysregulation in sepsis. Mol Med. 2022 Aug 19;28(1):99. PMID: 35986237; PMCID: PMC9389495. [CrossRef]
- Bindayna K. MicroRNA as Sepsis Biomarkers: A Comprehensive Review. Int J Mol Sci. 2024 Jun 12;25(12):6476. PMID: 38928179; PMCID: PMC11204033. [CrossRef]
- Zheng X, Zhang Y, Lin S, Li Y, Hua Y, Zhou K. Diagnostic significance of microRNAs in sepsis. PLoS One. 2023 Feb 22;18(2):e0279726. PMID: 36812225; PMCID: PMC9946237. [CrossRef]
- Yao J, Lui KY, Hu X, Liu E, Zhang T, Tong L, Xu J, Huang F, Zhu Y, Lu M, Cai C. Circulating microRNAs as novel diagnostic biomarkers and prognostic predictors for septic patients. Infect Genet Evol. 2021 Nov;95:105082. Epub 2021 Sep 11. PMID: 34520874. [CrossRef]
- Yong J, Toh CH. The convergent model of coagulation. J Thromb Haemost. 2024 Aug;22(8):2140-2146. Epub 2024 May 28. PMID: 38815754. [CrossRef]
- Wilhelm G, Mertowska P, Mertowski S, Przysucha A, Strużyna J, Grywalska E, Torres K. The Crossroads of the Coagulation System and the Immune System: Interactions and Connections. Int J Mol Sci. 2023 Aug 8;24(16):12563. PMID: 37628744; PMCID: PMC10454528. [CrossRef]
- Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, Nadel S, Schlapbach LJ, Tasker RC, Argent AC, Brierley J, Carcillo J, Carrol ED, Carroll CL, Cheifetz IM, Choong K, Cies JJ, Cruz AT, De Luca D, Deep A, Faust SN, De Oliveira CF, Hall MW, Ishimine P, Javouhey E, Joosten KFM, Joshi P, Karam O, Kneyber MCJ, Lemson J, MacLaren G, Mehta NM, Møller MH, Newth CJL, Nguyen TC, Nishisaki A, Nunnally ME, Parker MM, Paul RM, Randolph AG, Ranjit S, Romer LH, Scott HF, Tume LN, Verger JT, Williams EA, Wolf J, Wong HR, Zimmerman JJ, Kissoon N, Tissieres P. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatr Crit Care Med. 2020 Feb;21(2):e52-e106. PMID: 32032273. [CrossRef]
- Haque KN. Defining common infections in children and neonates. J Hosp Infect. 2007 Jun;65 Suppl 2:110-4. PMID: 17540253. [CrossRef]
- McGovern M, Giannoni E, Kuester H, Turner MA, van den Hoogen A, Bliss JM, Koenig JM, Keij FM, Mazela J, Finnegan R, Degtyareva M, Simons SHP, de Boode WP, Strunk T, Reiss IKM, Wynn JL, Molloy EJ; Infection, Inflammation, Immunology and Immunisation (I4) section of the ESPR. Challenges in developing a consensus definition of neonatal sepsis. Pediatr Res. 2020 Jul;88(1):14-26. Epub 2020 Mar 3. PMID: 32126571. [CrossRef]
- Santhanam I, Sangareddi S, Venkataraman S, Kissoon N, Thiruvengadamudayan V, Kasthuri RK. A prospective randomized controlled study of two fluid regimens in the initial management of septic shock in the emergency department. Pediatr Emerg Care. 2008 Oct;24(10):647-55. PMID: 19242131. [CrossRef]
- Iroh Tam PY, Musicha P, Kawaza K, Cornick J, Denis B, Freyne B, Everett D, Dube Q, French N, Feasey N, Heyderman R. Emerging Resistance to Empiric Antimicrobial Regimens for Pediatric Bloodstream Infections in Malawi (1998-2017). Clin Infect Dis. 2019 Jun 18;69(1):61-68. PMID: 30277505; PMCID: PMC6579959. [CrossRef]
- Perner A, Haase N, Guttormsen AB, Tenhunen J, Klemenzson G, Åneman A, Madsen KR, Møller MH, Elkjær JM, Poulsen LM, Bendtsen A, Winding R, Steensen M, Berezowicz P, Søe-Jensen P, Bestle M, Strand K, Wiis J, White JO, Thornberg KJ, Quist L, Nielsen J, Andersen LH, Holst LB, Thormar K, Kjældgaard AL, Fabritius ML, Mondrup F, Pott FC, Møller TP, Winkel P, Wetterslev J; 6S Trial Group; Scandinavian Critical Care Trials Group. Hydroxyethyl starch 130/0.42 versus Ringer's acetate in severe sepsis. N Engl J Med. 2012 Jul 12;367(2):124-34. Epub 2012 Jun 27. Erratum in: N Engl J Med. 2012 Aug 2;367(5):481. PMID: 22738085. [CrossRef]
- Scott HF, Brou L, Deakyne SJ, Fairclough DL, Kempe A, Bajaj L. Lactate Clearance and Normalization and Prolonged Organ Dysfunction in Pediatric Sepsis. J Pediatr. 2016 Mar;170:149-55.e1-4. Epub 2015 Dec 19. PMID: 26711848. [CrossRef]
- Ventura AM, Shieh HH, Bousso A, Góes PF, de Cássia F O Fernandes I, de Souza DC, Paulo RL, Chagas F, Gilio AE. Double-Blind Prospective Randomized Controlled Trial of Dopamine Versus Epinephrine as First-Line Vasoactive Drugs in Pediatric Septic Shock. Crit Care Med. 2015 Nov;43(11):2292-302. PMID: 26323041. [CrossRef]
- Ramaswamy KN, Singhi S, Jayashree M, Bansal A, Nallasamy K. Double-Blind Randomized Clinical Trial Comparing Dopamine and Epinephrine in Pediatric Fluid-Refractory Hypotensive Septic Shock. Pediatr Crit Care Med. 2016 Nov;17(11):e502-e512. PMID: 27673385. [CrossRef]
- El-Nawawy A, Khater D, Omar H, Wali Y. Evaluation of Early Corticosteroid Therapy in Management of Pediatric Septic Shock in Pediatric Intensive Care Patients: A Randomized Clinical Study. Pediatr Infect Dis J. 2017 Feb;36(2):155-159. PMID: 27798546. [CrossRef]
Figure 1.
The major complications of the neonatal period and associated cytokines after undergoing FIRS.
Figure 1.
The major complications of the neonatal period and associated cytokines after undergoing FIRS.
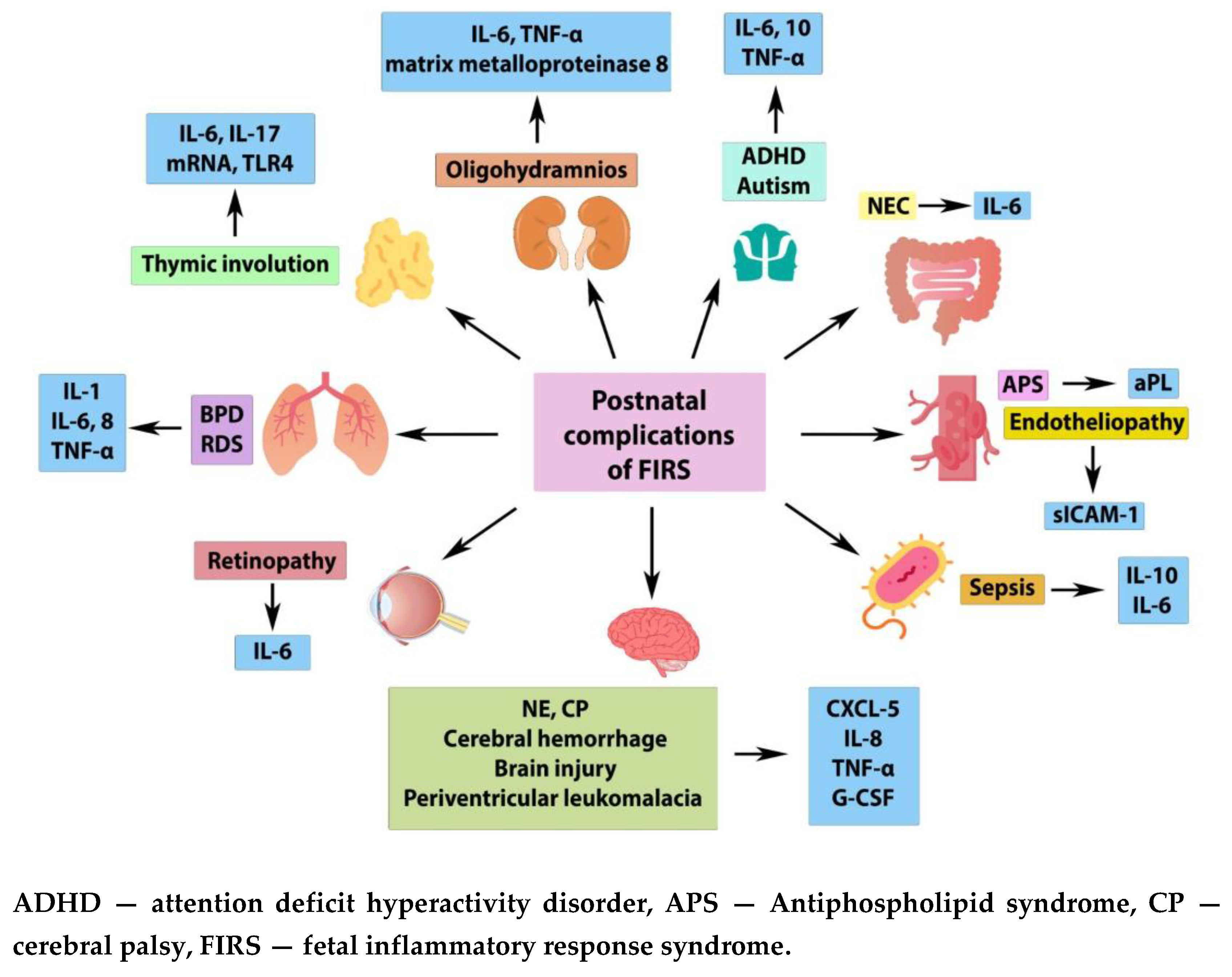
Figure 2.
The relationship between inflammation and hemostasis - “amplification loop”.
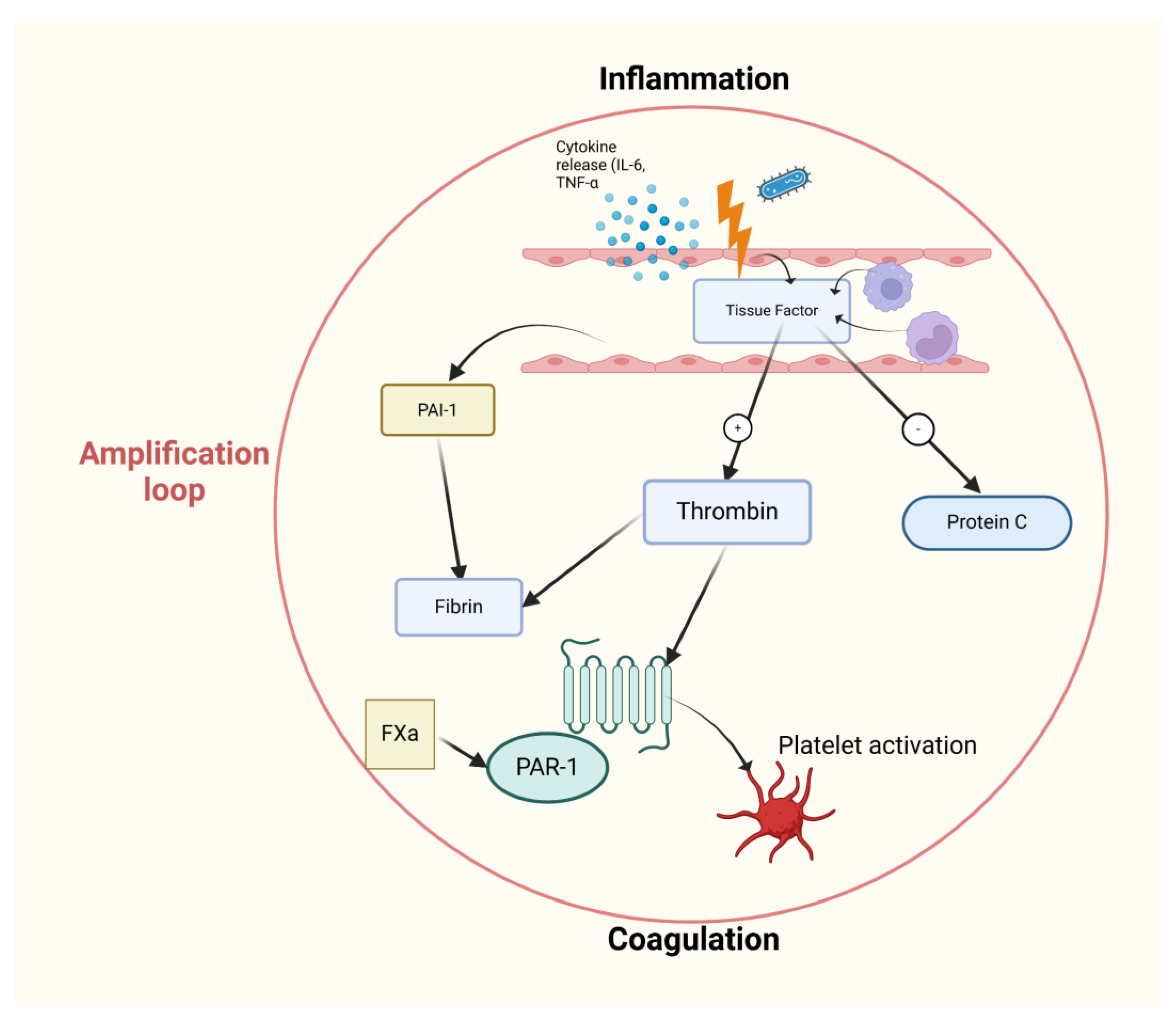

Table 1.
Diagnostic criteria for SIRS.
| Criterion | Value |
| Body temperature (rectal, oral) | >38.5°C or <36°C |
| Heart rate | Tachycardia ≥ 90/min, or bradycardia in children under 1 year of age below the 10th percentile |
| Respiratory rate | ≥ 20/min or hyperventilation with blood carbon dioxide ≤ 32 mmHg |
| White blood cell count | Leukocytosis or leukopenia or neutrophil left shift |
Table 2.
Potential risk factors for the development of sepsis.
| Maternal risk factors |
|
| Fetal risk factors |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



