Submitted:
07 February 2025
Posted:
08 February 2025
You are already at the latest version
Abstract
Healthcare organisations in the United Kingdom must comply with national standards for food and drink, including sustainable sourcing and minimisation, mitigation and management of food waste. Despite this, an estimated one in six plates of food served in hospitals are wasted daily, producing 12% of the UK food waste, equating to 6% of carbon dioxide emissions (CO2e) nationally, and a waste-management cost of £230m per annum. Within healthcare there is a move towards the implementation of “plant-based diets by default” to reduce the environmental impact, improve nutritional outcomes, and reduce costs. However, plant-based diets are often perceived as being difficult to prepare by caterers, less enjoyable and may result in more food waste. We conducted a scoping review to examine the influence of the social, medical, and physical environment on food intake during inpatient admission to a mental health hospital. Fourteen-studies were included. We identified five critical knowledge areas: i) food and socio-cultural environment, ii) evidence-based measures and strategies to reduce food waste, iii) economic food environment, iv) inevitability of weight gain and v) applications of theoretical models for behaviour-change. Future research should explore the development of a behaviour-change framework inclusive of training, education, and goal setting component for staff, patients, and visitors.
Keywords:
food waste
; sustainability
; greenhouse gas emissions
; plant-based diet
; severe mental illness
; obesity
; behaviour change
1. Introduction
The goal of the Paris Agreement (2015), a legally binding international treaty, is to limit global warming to well below 2oC compared with pre-industrial levels. Despite international commitment to the multilateral climate change process, it is anticipated that global temperatures will reach and exceed the 1.5°C threshold by 2030 and 2°C by 2050 [1]. Increasing global temperatures are predicted to have an irrevocable impact on the natural world as well as humankind. Rising temperatures are likely to lead to animal and plant extinctions, water and crop failures leading to rising food prices, poverty, famine, and extreme weather events resulting in mass displacement [2]. Greenhouse gas (GHG) emissions are responsible for global warming and climate change [3]. Estimates of GHG emissions by economic sectors indicate that electricity and heat production account for 25%, industry for 21%, agriculture, forestry, and other land use for 24%, transportation for 14%, buildings for 6%, and other sources for 10% [4,5,6,7]. The healthcare sector, despite its dedication to enhancing health outcomes, plays a considerable role in the climate crisis, contributing 4.4% of global net emissions and ranking as the fifth-largest annual emitter of GHGs [8], with the United States, China and the European Union/ UK comprising 56% of the total healthcare climate footprint [9]. The impact of climate change is impacting the most vulnerable societies including those in the Global South, where existing adaptations may he insufficient to cope with the effect of rising temperatures on, agriculture , water availability, leading to biodiversity loss and irrevocable changes to ecosystem structures [10,11]. The healthcare industry's overall influence on the climate emergency is complex and significant, with emissions arising from energy use, transportation, waste production, and the manufacturing of pharmaceuticals and medical devices [12]. The sector's dependence on fossil fuels and inadequate disposal practices for medications and medical waste further intensify environmental harm. Moreover, emissions from the global food system, food including medical nutrition ingredients, and medical supplies account for one-third of all human-generated GHG emissions, contributing to deforestation and loss of biodiversity, while chemical pollutants threaten water and soil quality [4,5,6,7].
Within the United Kingdom (UK) the health and social care sector represents 6.3% of the total national carbon dioxide emissions (CO2e) [13]. National Health Services (NHS) hospitals must comply with national standards for healthcare food and drink, which includes improving sustainable sourcing of foods, and reducing food waste [14]. Food waste is a significant contributor to GHG emissions, including CO2 and methane [15]. Food waste occurs at every level of the supply chain; all of the components associated with production (including water usage), processing, transportation, preparation and storage of discarded food are also wasted [16,17]. With one in six plates of hospital food wasted [18], approximately 50% of the total waste generated in a ward environment comes from food [16,17]. Despite the use of food and drink standards it is estimated the 1,297 NHS hospitals and 515 private hospitals produce 12% of the total food waste generated in the UK. This equates to 1.1 million tonnes of food waste per annum [19], producing 1,543ktCO2e, approximately 6% of total NHS annual emission per annum [18], with a NHS waste management cost of £230m per annum [19].
Numerous factors influence food consumption in hospitals, shaping both what is eaten and discarded. These factors include: i) food quality – encompassing aesthetic and sensory attributes such as texture, smell, color, taste, and temperature; ii) food quantity – the portion size of meals; iii) ordering/service model – including the ability to accommodate individual preferences, system automation, and the time between meal ordering and delivery; iv) quality assurance and control mechanisms – such as food waste audits; v) dining environment – factors related to where and how meals are consumed; vi) mealtime assistance – support available to patients during meals; and vii) staff knowledge and training – ensuring that healthcare staff are equipped to promote adequate food intake and minimize waste [20,21,22,23,24]. Meeting the dietary and nutritional needs of individuals requiring hospital care, visitors and staff is challenging [25], with the triple burden of malnutrition (i.e. over-, undernutrition and micronutrient deficieny) commonplace amongst those admitted to hospitals [25,26,27,28,29,30,31]. For individuals with severe mental illness, nutritional status may be affected further due to longer hospital admissions [29,30]. The average length of stay in a mental health bed is 39 days [32] compared with 8.3 days in an acute hospital bed (2022) [33]. This poses problems with menu fatigue, high levels of food waste, and poor compliance with healthy diet recommendations [34]. Healthcare professionals and staff working within these settings often feel they do not have sufficient knowledge and individuals admitted are resistant to engaging in healthy diet and physical activity programmes [30]. Changes to service provision including food is often met with resistance from staff, visitors, and patients [22,23].
The global expansion of Western diet [35,36] has contributed to climate change leading to unstainable agricultural practices [37,38], negatively impacting food systems, nutrient bioavailability and cost of food costs [38,39]. The International Panel on Climate Change [2], World Health Organisation, [40] and the United Nations Food and Agriculture Organisation [41] recognise the need to move towards plant-based diets. Currently, 65% of the worlds nitrous oxide emissions arise from animal agriculture. The expansion of plant-based diets would significantly reduce the impact of agriculture on GHG emissions [42]. In addition, plant-based agriculture is associated with improved individuals, populations and planetary health [43]. Compared with Western diet with high amounts of animal-protein, plant-based diets are more sustainably and reduce the risk of chronic diseases (i.e., cancer, dementia, cardiovascular disease), water conservation and reduce land use for agriculture including deforestation and reduced pollution (arising from less methane, nitrous oxide and carbon dioxide (CO2)) [43,44]. The EAT-Lancet Commission (2019) provided a definition for a ”planetary diet”, which they propose should be mainly composed of ‘vegetables, fruit, whole grains, legumes, nuts and unsaturated fats, limited amounts of fish and poultry, and low consumption of red meat, ultra processed foods [45] added sugars, refined cereals and starchy vegetables’ [46], and translated into a food based dietary guidelines [47]. The most affordable foods are typically high fat, salt, sugar ultra processed foods [52], with plant-based diets potentially a more nutritious alternative but slightly less affordable in some socio-economic settings [37,50,51]. Despite the increased cost compared to the ultra processed food diet, a plant-based diet is more affordable compared to an omnivorous diet (i.e. meat and dairy) [49], and would offer a large diversity of nutrients, be better for overall health, less obseogenic [48] and have a lower enviornmental impact [37]. Due to individual dietary habits, food cultures, and local environmental considerations, the promotion of plant-based diets requires context-specific solutions, especially as familiarity is a key factor driving individual acceptance of food related behaviour change. The use of local foods may result in higher levels of acceptability [53] and environmental benefits [37]. Although there is a move to implement plant-based diets by default within a hospital setting [54,55,56,57], factors associated with the success of this approach in mental health hospitals amongst patients with severe mental illness remain unknown, especially with regards to potential unintended consequence of nutritional inadequacy [37,58] and increased food waste.
As such, the objective of this scoping review was to examine the influence of the social, medical and physical environment on food during inpatient admissions to mental health hospitals, with the intention of identifying gaps in the existing evidence related to the default implementation of plant-based diets.
2. Methods
2.1. Preparing to Scope the Literature and Protocol Development
A scoping review was conducted to identify the key concepts within this area of research [59]. This design was chosen because it offers a framework to identify and synthesize a broad range of evidence. We considered literature about 1) changing body habitus on admission to a mental health hospital, 2) exploring food waste in mental health hospitals, and 3) knowledge and training needs of stakeholders for a plant-based diet to be implemented [60].
2.2. Identifying the Research Questions
1. What influence do social-, medical- and physical-environment factors have on food intake during hospitalization in a mental health facility?
An a priori scoping review protocol was developed and included 1) the research question 2) eligibility criteria of the studies be to included, 3) information sources to be searched, 4) description of a full electronic search strategy, 5) data charting process with data items included, 6) critical appraisal and synthesis of the data in order to answer the question posed [59,61]. This scoping review has been reported in line with PRISMA-ScR (Supplementary file 1).
2.3. Data Sources—Stage 1
Following the finalisation of the research question and objectives, a literature search was completed to identify studies in scope. A search strategy was devised for PubMed using key words from the grey literature and modified for additional electronic data bases using NHS Knowledge and Library Hub website (https://library.nhs.uk/knowledgehub/). A grey literature search was also conducted in OpenGrey to expand the scope in this subject. Forward and backward citation searching was completed on studies exploring the food waste in a psychiatric/ mental health hospital setting. A twenty-four-year time limit was set as 2000 until Septmeber 2024, to ensure the use of relevant contemporaneous evidence.
2.4. Search Strategy—Stage 2
A search strategy was devised for PubMed using key words from food waste, sustainability, plant-based diets (including vegan and vegetarian), psychiatric/ mental health, obesity, behaviour change, and food systems and food waste modified for additional electronic data bases, and completed in September 2024 (Supplementary File: Table 1).
2.5. Study Selection—Stage 3
Titles and abstracts were screened (LVM, RM). Duplicates were deleted, full text articles were reviewed for eligibility. Inclusion criteria included; any study which used a qualitative or quantitative design, studies in English including published thesis and conference abstracts, those involving food waste, sustainability, plant-based diets, psychiatric/ mental health, obesity, behaviour change, food systems and food waste. Systematic reviews were not included, but the references of studies were hand searched for any references which may fulfil the inclusion criteria. Exclusion criteria were publications not in English language or those that did not relate to food systems within psychiatric/ mental health hospitals [61].
2.6. Data Extraction—Stage 4
Data extraction was completed using a two-stage process. A data extraction template (Microsoft Exel 2010, Redmond, WA) was created and used to capture the study design, results, and conclusions, followed by a content analysis.
2.7. Collating, Summarizing and Reporting the Results—Stage 5
Data synthesis was completed using an established content analysis approach [62], this method was chosen to report common themes within the data [63]. This approach captured descriptive aspects of the study, methodology, outcomes, and any key findings which were coded. A content analysis was completed by selecting, coding, and creating initial codes, sub-categories, and overarching themes to develop into a conceptual framework.
3. Results
3.1. Selection and Characteristics of Included Articles
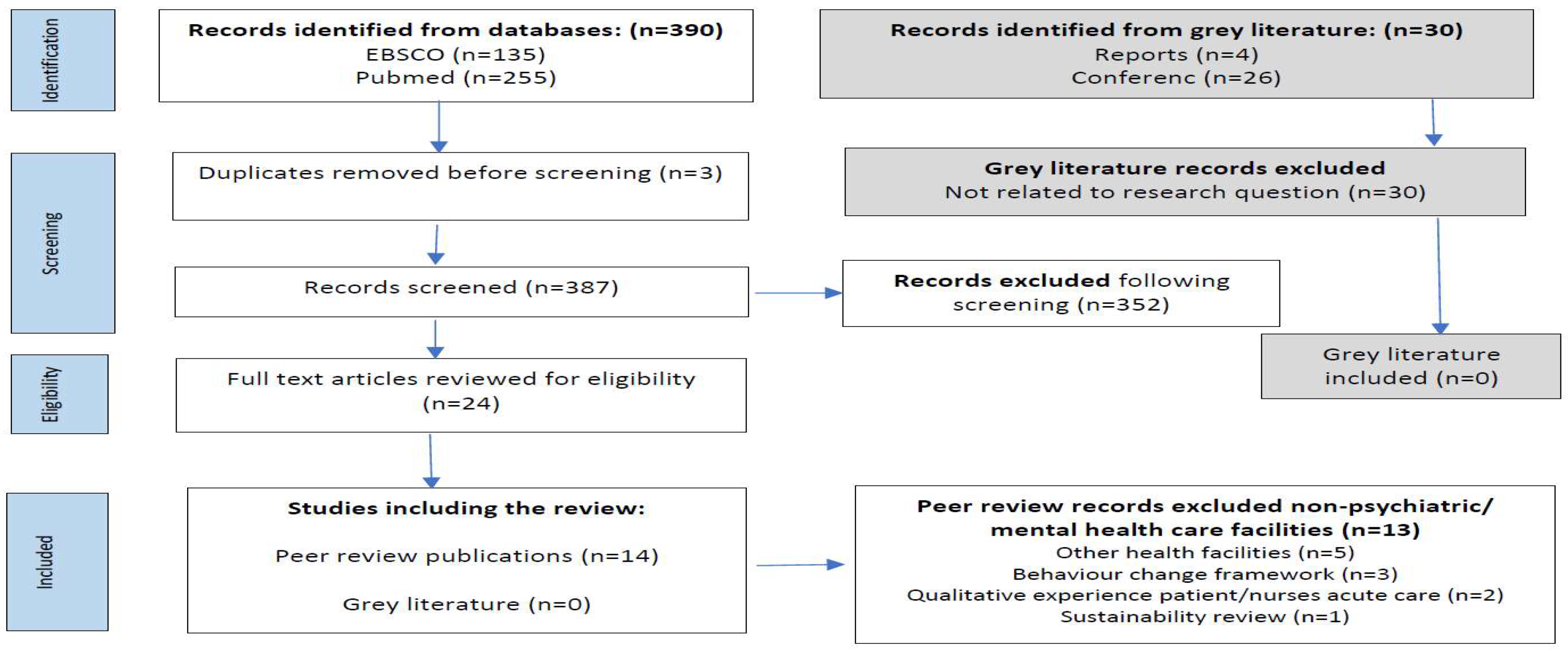
420 were identified. Following the removal of duplicate records, 411 titles and abstracts were screened for inclusion. The full text of 24 articles were reviewed for eligibility and 14 studies were included in the review (Figure 1).
3.2. Study Characteristics
The 14 included studies explored factors associated with food waste within a psychiatric/ mental health hospital setting including: ward environment [64,65,66,67,68,69,70], food environments [34,71], nurition knowledge, skills and eating beahaviours [72], theoretical framework of behaviour change [73], sustainable practices [74,75] and food waste [76]. Included in this scoping review are five qualitative studies [68,70,71,73,74], two audits [75,76] and seven quantitative studies [64,65,66,67,69,72,77] from years 2004 to 2024 from countries: Australia [73], Canada [76,78], Denmark [67], Switzerland [72,75], The Netherlands [71], the United Kingdom [64,65,68], and United States of America [66,69,70,74] (Table 2).
Figure 1.
Search results through to inclusion.
3.3. Content Analysis: Conceptual Framework and Overarching Themes
A content analysis identified 68 initial codes, 12 sub-categories and 5 overarching themes (Table 1), which were identified as:
- Food & socio-cultural environment; i) physical food environment, ii) political food environment, iii) medical ward culture
- Evidence-based measures to reduce food waste; i) sustainability initiatives, ii) ccommunication with staff and patients
- Economic food environment; i) quality & type of food, ii) food waste
- Inevitability of weight gain; i) factors associated with weight gain, ii) perception around weight gain
- Theoretical model for behaviour change; i) knowledge & training, ii) physical opportunity, iii) ability to change

Table 1.
Development of codes, sub-categories and overarching themes [34,64,65,66,67,68,69,70,71,72,73,74,75,76].
| Initial Coding (n=68) | Sub-Categories (n=12) | Overarching Themes/Categories (n=5) |
|---|---|---|
| Inadequacy of catered hospital food Food consumption - unmonitored Portion sizes too small or too big Vending machines – source of high calorie drinks/ snacks Water policy – health vs. safety Health promotion- healthy snacks, lower cost Limited choice of healthy options Buffet style – overeating, unhealthy choices Hoarding – milk, creamers, sugar Control over food – acting out Patients right to choose – wider choice Purchasing food close to hospital – lack of healthy options - takeaways Few opportunities to engage in physical activity Healthcare professional (HCP) respect for patient autonomy Staff dissatisfaction with catering HCP – not wishing to restrict choices of takeout food, portion sizes, number of servings at mealtimes, or purchases from food carts or vending machines HCP – not wishing to stop patients from eating food from other patients’ untouched trays Ward culture – not conducive to healthy eating Eating in silence and at speed – no social engagement Eating together – staff and patients Rule breaking around food – variation in staff practice Healthcare settings (acute vs. mental health) shaped socio-cultural environment Policies and procedures – top down |
Physical food environment Political food environment Ward culture |
Food & socio-cultural environment |
| Reduced portion sizes Selling surplus foods Collaboration with nutritionists Cook-to-order Regular monitoring Sustainable sourcing |
Sustainability initiatives Communication with staff and patients |
Evidence-based sustainable food practices |
| Environmental impact Evidence-based measures Ecological footprint of food waste Segregating food waste Weighing food Food waste - carbon footprint - carbon dioxide equivalent emissions per kg (CO2e/kg) Food waste water footprint – (i.e. total volume of freshwater use per kg of produced food waste (l/kg)) Food waste quantification Fish, Meat, and Protein – highest CO2e/kg Vegetables, salad, and fruits – highest water footprint (l/kg) Preparation method (i.e. bulk, cook-chill, plated) Food appearance & delivery method Reduced food waste High burden of food waste in forensic psychiatry, addictive disorders, and psychotic disorders Visual estimation of consumption / food waste Portion size (i.e. meal vs. snack) Meal occasion – greatest waste (e.g. lunch, afternoon snack) Healthy vs. unhealthy Dislike of vegetables |
Quality & type of food Food waste |
Economic food environment |
| Body habitus Lower or normal body weight admission – greater weight gain hospital Diagnosis associated weight gain – anti-psychotics Smokers Male vs. female Age at onset Duration of illness Inactivity – low levels of physical activity Co-morbidity – type 2 diabetes, heart disease, hypertension Length of hospital stay Staff who are obese |
Factors associated with weight gain Perception around weight gain |
Inevitability of weight gain |
| Knowledge, skills Environmental context and resource Social, professional role and identity, beliefs about capabilities Education Training Environmental restructuring Modelling Enablement |
Knowledge & training Physical opportunity Ability to change |
Theoretical model for behaviour change |
The five themes were used to explore interdependencies associated with social-, medical- and physical- -environments of food within a psychiatric/ mental health hospital setting (Figure 2).
Figure 2.
Interdependencies associated with social, medical and physical food environment within a psychiatric/ mental health hospital setting [34,64,65,66,67,68,69,70,71,72,73,74,75,76].

3.3.1. Food & Socio-Cultural Environment
- (i)
- physical food environment,
Food (nutrition) is seen by healthcare professionals as an important component of recovery, pre-/ rehabilitation and prevention with compliance to nutrition standards an essential component of treatment [71]. Most hospitals have rigid structures for mealtimes [71], with three main meals and in-between meal snacks [68,71]. Food preparation varies considerably from cook-to-order, cook-chill or freeze systems, plated, tray- or self-service [71,74]. Physical food environments vary from household-like setting [71] to clinical institutionalized communal eating areas, impacting on the mealtime experience (i.e. staff and patients eating together with conversation or patients eating meals quickly, with little opportunity for relaxation or social interaction) [68,70]. Individual patients had the opportunity (with support) to cook their own meals once a week. Limited cooking facilities and equipment (e.g. blunt knives) may hamper skill acquisition, reducing patients’ ability to cook independently [68]. Patients appear to enjoy the creative experience of cooking, although this is seldom available to those in a secure environment, highlighting pressures around ward cohesion and skills development. Usings a systems-based approach to recognising the obesogenic nature of psychiatric inpatient stay, especially with regards to food available for very long stay patients [71], along with the environmental and economic impact of food waste may also be required [68,71].
- (ii)
- political food environment,
Organisation specific food policies play a pivotal role with regards to i) implementation of food policies, ii) improving food provision and meal ambience, iii) sustainable and healthier food choices, iv) knowledge and skills transfer for staff, visitors and patients and v) co-creation of food policy [71]. Interventions should also explore environments by type, i) physical – what is available, ii) economic – what are the costs, iii) political – what are the rules and iv) sociocultural – what are the attitudes and beliefs [70]. Within the budgeting process healthy and sustainable procurement often lacks priority [71].
- (iii)
- Medical ward culture,
Ward staff are role models and create the ‘family’ ambience within clinical environments bringing high fat, high calorie foods for their own consumption or celebrate ward activities [66,68,70]. This may create problems for patients, especially in environments where staff are also experiencing excess weight [66]. Vieweg et al. report 89% were overweight and of these 65% were obese, as a result staff may inadvertently model poor dietary habits [66]. Low staffing levels may impact on the quality of food and staff acquiescing to patient requests for additional food servings, creating tension between staff and patients. Purchasing takeaway foods to consume on wards within the NHS is common, with some wards having no constraints on orders with evening and weekend orders being popular [68,70]. Staff broadly support the right of patients to choose the type of food they wish to eat [70], although others are in favour of setting limits [71]. Initiatives such as staff, visitor and patient education were considered important to reduce unhealthy food consumed, as well as helping with skill development [70,71,72]. Inpatients would benefit from nutritional support that aims at improving their daily structure and social inclusion, using behavioural approaches related to meal planning and social eating [72].
3.3.2. Evidence-Based Sustainable Food Practices
- (i)
- sustainability initiatives,
Initiatives implemented to reduce food waste included i) communication of food waste reduction efforts to staff, patient and visitors, ii) sustainable sourcing for food procurement, iii) feedback loops where staff and patients provide input and rating on food quality and preference to minimize waste, iv) regular monitoring by staff along with staff sustainability champions, v) kitchen staff training in food preparation techniques to reduce waste, vi) cook-to-order reducing overproduction, vii) collaboration with a nutritionist to develop appropriate meal plans, educate staff and patients about nutrition, and address challenges regarding food waste, viii) selling surplus food in the employee cafeteria at reduced prices and ix) smaller portion sizes with the option of extra food for patients as required [74,75]. These initiatives led to significantly reduced food waste of 5.9% per kg, with 9% per patient, along with reductions in 22% environmental pollution points, 23% CO2e/kg emissions and 21% water usage (H2O – l/kg), respectively [75].
Increasing plant-based dishes may support environmental sustainability as well as providing healthier meals [71,74]. However, associated barriers to plant-based by default included patient preference for meat containing dishes, challenges around planning plant-based meals and difficulty in buying plant-based products. Associated facilitators of plant-based meals included taste testing recipes, young patients with plant-based preferences, reducing meat portion sizes compared to vegetables and blending plant and meat protein together [74] and staff, visitor and patient education [71].
- (ii)
- communication with staff and patients
For staff a ‘one size fits all’ approach fails to address individual patient needs, and efforts by some staff to curb patients eating patterns is ineffective as patients buy snacks and takeaways to supplement their intake [68]. Food is also used by staff to promote ward cohesion and build positive relationships with staff [68,71]. Effective communication, including education for visitors and patients, training ward and kitchen staff around food waste initiatives, led to healthier food choices and feedback loops [71,75].
3.3.3. Economic Food Environment
- (i)
- quality and type of food
The importance of food quality, taste and appearance is a central theme and despite the reliance of many hospitals on centralised food production, the poor quality of food served (e.g. lack of variety, small portion sizes, low food quality) often fails to meet patient requirements [68,70,71,75]. Dissatisfaction with catering services is often a long-standing concern amongst staff and patients [68,70]. For some patients within a low secure ward environment, trips outside the ward may be allowed, which often involve purchasing high fat, high calorie foods or meals (i.e. on-site hospital canteen for a cooked breakfast, visit to a fast-food outlet or supermarket). Healthier options, including lower fat options, should be made available in vending machines [70], and freshly cooked meals and fresh foods were perceived by staff and patients as the best option, providing an opportunity to tailor towards individual preference [71]. In addition, greater availability of water was considered helpful as an alternative to sugar rich beverages, although safety reasons relating to water intoxication were noted [70]. Patient food preparation was frequently associated with poor hygiene standards, with unhealthy meals eaten in large quantities negatively impacting on physical health outcomes [68].
- (ii)
- food waste
Food waste affects the environment and represents considerable economic loss [75]. Average plate waste has been described as being between 20 - 28% [75,76], with lunch meals having the greatest amount of waste at 31% and 45% of afternoon snacks. Delayed breakfast serving may impact on hunger at lunch [76]. Vegetables, salad and fruits made up the greatest proportion of food wasted (11.8%). Overproduction of meals contributed a relatively small amount at 5.7% of total waste [75].
3.3.4. Inevitability of Weight Gain
- (i)
- factors associated with weight gain
On admission to mental health hospitals patients who were overweight were significantly more likely to gain weight with body mass index (BMI) worsening to obesity during an inpatient stay [64,65,66,67,69] which was proportional to the duration of admission [64,67,69]. Weight gain of 1.8kg ± 6.0kg [69] or 0.03kg per day [64], with weight gain more common than weight loss [64,72] amongst patients admitted to a mental health hospital. Weight gain was often viewed as inevitable [68], with associated factors of medication (e.g. antipsychotics, mood stabilizers and anti-depressants) [64,65,66,69], gender (e.g. males), cigarette smoking, [64,69], duration of illness, length of hospital stay, age at disease onset (i.e. younger patients had the greatest risk) [65] and high fat, high calorie dietary intake [67]. In addition patients are often reported to show little interest in personal appearance with the ubiquitous presence of tracksuits with elasticated waist-bands, accommodating weight gain [68]. To reduce conflict patients may be permitted to skip breakfast, which was associated with the consumption of higher fat, higher calorie foods in between meals, reduced physical activity and missed appointments [70].
- (ii)
- perception around weight gain
Patients are assigned responsibility for maintaining a healthy weight or weight loss. However, this strategy suffers when there are high levels of overweight/ obesity amongst ward staff [66]. With an abundance of high-calorie snacks, beverages, and takeaways weight gain is perceived as inevitable [66,68,70].
3.3.5. Theoretical Model for Behaviour Change
- (i)
- Knowledge and training
The Behaviour Change Wheel (BCW) with theoretical components of capability (physical or psychological), opportunity (physical or social), and motivation (emotional or reflective), found the dominant COM-B constructs were psychological capability (knowledge, skills), physical opportunity (environmental context and resources), and reflective motivation (social/ professional role and identity beliefs about capabilities). Participants included those who worked in, or managed foodservices, reported food service staffs' lack of knowledge with regards to healthy eating, labour, time and hospitals avoiding the need to complete audits. Interventions which may have the greatest impact around the implementation of waste audits were education, training, environmental restructuring, modelling and enablement [73].
- (ii)
- physical opportunity,
There were limited opportunities to engage in sufficient physical activity to prevent weight gain particularly in a locked ward environment, with low levels of activity recorded [66,67,68]. Activities such as climbing stairs were rare, contributing to physical deconditioning [68] and weight gain [67,68,70]. For individuals with ward leave, visits to the on-site gym or walks around the hospital groups were possible but these were usually constrained by staff availability to accompany patients [68]. Dysregulated sleeping patterns and social deprivation may result in night eating and reduced social eating or activities during the day. This may be associated with higher calorie intake and increased risk of metabolic syndrome. Social aspects of eating are associated with feelings of inclusion and psychological well-being, and may lead to preferable food choices and healthier eating patterns [72].
- (iii)
- Ability to change
Modelling of desired behaviours for staff and patients with regards to healthy diet and reducing food waste will be required to support behaviour change [70,73]. Some patients with severe mental illness may have difficulty translating nutrition knowledge into action requiring greater support [72].
Some food service staff do not see food or food-related waste audits as part of their role, and may have a lower willingness to implement new initiatives. This may be due to low levels of organisation interest or support from leadership teams. However, enablers for food service workers support is through coproduction/ codesign of initiatives along with the development of champion roles to model organisational responsibility of the wider food service teams [73] (Table 2).
Table 2.
Characteristics of studies describing of food environment within mental health hospitals.
| Author, Country | Title | Aim | Methods | Findings | Food Environment | Food Waste | Summary |
|---|---|---|---|---|---|---|---|
| Cook C et al. Australia, 2023 [73] | Applying the theoretical domains framework and behaviour change wheel to inform interventions for food and food related waste audits in hospital food services. | The aim of this study was to use the behaviour change theories and frameworks to 1) describe the drivers of behaviour to complete food and food related waste audits and 2) identify possible interventions that support the implementation and uptake of these audits. | Qualitative interviews of food service staff working in a variety of hospital settings, including mental health hospitals. | From the twenty interviews found the dominant COM-B constructs (theoretical domains framework) were psychological capability (knowledge, skills), physical opportunity (environmental context and resources), and reflective motivation (social/ professional role and identity beliefs about capabilities). Participants report foodservice staffs' lack of knowledge, labour, time and hospitals avoiding the need to complete audits. Interventions which may have the greatest impact around the implementation of waste audits were education, training, environmental restructuring, modelling and enablement. Suggested enablers were obtaining staff buy-in, reinforcing behaviour through incentives and establishing audit champions. | Food waste audits require education, training and environmental restructuring. | Using a behaviour change model may be beneficial for waste audits implementation strategies, including staff education, training and environmental restructuring. | |
| Faulkner G et al. United States, 2009 [70] | Psychiatric illness and obesity: recognizing the "obesogenic" nature of an inpatient psychiatric setting. | The aim of this study was to examine environmental factors that contribute to obesity in one psychiatric hospital in Canada. | Semi structured interviews were conducted with 25 key stakeholders from multiple professional disciplines at the hospital. | Factors contributing to obesity in this setting were related to increased energy intake, such as easy access to high-calorie snacks and beverages, and reduced energy expenditure, and lack of access to spaces to engage in physical activity. | Easy access to high-calorie foods and reduced levels of physical activity led to an obesogenic environment. | Psychiatric settings may contribute to the high prevalence of obesity among individuals with psychiatric illness and interventions considering environmental factors within an inpatient environment are required. | |
| Liwinski T et al. Switzerland, 2024 [75] | Sustainability initiatives in inpatient psychiatry: tackling food waste. | The aim of this paper was to explore sustainability initiatives within an inpatient psychiatric hospital. | Systematic food wastage audits were completed over three years (2020-2022) in May and June, for a four-week period. These audits collected costs associated with food, staff, infrastructure, and disposal. Environmental impact was assessed using environmental impact points and CO2e/kg emissions, alongside water usage l/kg. | Economic losses due to food wastage were substantial, primarily from untouched plates and partially consumed dinners, prompting meal planning adjustments. Despite a >3% increase in meals served, both food waste mass and costs decreased by nearly 6%. Environmental impact indicators showed a reduction >20%. Vegetables, salad, and fruits constituted a significant portion of waste. Overproduction minimally contributed to waste, validating portion control efficacy. Our study highlights significant economic and environmental losses due to hospital food waste, emphasizing the importance of resource efficiency. The strategies outlined offer promising avenues for enhanced efficiency. The decrease in food waste observed over the three-year period underscores the potential for improvement. | High economic losses arose from untouched meals. Evidence based strategies to minimise food waste included i) communication, ii) sustainable sourcing of food, iii) feedback loops for staff and patients to iterate meals, iv) regular food-waste audits, v) kitchen staff training, vi) cook-to-order, vii) collaboration with nutritionists, viii) selling surplus food to staff at low cost and ix) reduced portion sizes. | This study reports high economic and environmental loss arising from hospital food waste. Quality improvement strategies demonstrated reduction in food waste and increased satisfaction with catering services. | |
| Megna et al. USA, 2006 [69] | A retrospective study of weight changes and the contributing factors in short term adult psychiatric inpatients | The aim of this study was to explore e factors associated with significant weight gain during an acute psychiatric inpatient hospitalization for adults. | A retrospective chart review of all patients admitted to the psychiatric inpatient unit. | 535 charts were reviewed, and 96 patients met the inclusion criteria. Individuals with diagnoses of bipolar disorder and schizophrenia gained more compared to those diagnosed with major depressive disorder. Those prescribed atypical antipsychotics gained more weight compared to those who were not prescribed such medications. Smokers gained more weight than nonsmokers, and males gained more than females. There was an inverse relationship with weight at the time of the admission and the strongest predictors of weight gain. | Following admission patients on average gained 1.8 +/- 6.0kg. (p=0.005). Individuals with a lower body weight at admissions were associated with more weight gain. | Patients with a diagnosis of bipolar disorder and schizophrenia, prescribed atypical antipsychotics and overweight at the time of admission may be at risk of greater weight gain during an admission. | |
| Miller C et al. Canada, 2024 [76] | Something to Chew on; Plate-Waste at an Ontario Veteran's Centre. | The aim of this study was to explore food waste within a long-term mental health facility. | A 3-day waste-audit of food/beverage items provided explored factors associated with food waste. | 28% of items served to individuals were wasted. Lunch was the meal with the greatest waste at 31% and waste of solid items was 12% higher than that of liquids. There was a large variability in waste between and within individuals, with 15% of residents wasting more than >50% of items provided. | Food waste audits report lunch was the meal associated with the greatest waste, although there was a high variability in waste between individuals. | This study proposes individualized strategies to address waste. | |
| Mills S et al. England, 2024 [68] | What are the key influences and challenges around weight management faced by patients in UK adult secure mental health settings? A focused ethnographic approach. | The aim of this study was to identify the key influences and challenges around weight management in UK adult secure mental health settings. | Qualitative focused ethnography of 12 male patients within a low secure male mental health ward. | Within this study key themes i) highlighted the increased importance of food in secure settings, ii) the inadequacy of catered hospital food and shortcomings of alternative food options) limited physical activity opportunities and iv) a ward culture that did not support healthy behaviours. | The environment within secure mental healthcare is obesogenic increasing the risk of excessive weight gain and sedentary behaviour in patients. Excess weight gain is often perceived as inevitable. | Weight management within mental health services is a complex challenge. Whole setting-based interventions involving staff and patients are required to promote a culture of promoting weight management. The maintenance of a healthy weight should integrate physical and mental health strategies with sufficient staffing. | |
| Mötteli et al. Switzerland, 2023 [72] | Examining Nutrition Knowledge, Skills, and Eating Behaviours in People with Severe Mental Illness: A Cross-Sectional Comparison among Psychiatric Inpatients, Outpatients, and Healthy Adults | The aim of this study was to explore eating behaviours, dietary habits and motivation for healthy eating among psychiatric inpatients and outpatients with severe mental illness. | This prospective, cross-sectional study was based on semi-structured interview data and anthropometric measurements from people with severe mental illness treated at a psychiatric hospital including both inpatient (acute wards) and outpatient (day clinic) settings. | 65 inpatients, 67 outpatients, and 64 healthy controls were included in the study. The psychiatric patients had a higher BMI and waist to hip ratio and had an increased incidence of nutrition-related diseases and food intolerances versus healthy controls. Most patients with severe mental illness experienced weight changes in the previous three to six months, whereas the healthy controls had more stable weights. Psychiatric patients were also less likely to engage in healthy behaviours such as physical activity and not smoking. | Inpatients with severe mental illness were more likely to be overweight and have diabetes. They were also more likely to experience disordered eating habits and have unhealthy lifestyles. | Nutrition, knowledge, cooking and food skills, did not appear to be important barriers although they may be prerequisites for healthy eating. Inpatients with severe mental illness SMI would benefit from nutritional support that aims at improving their daily structure and social inclusion, using behavioural approaches related to meal planning and social eating. | |
| Pederson et al. Denmark, 2022 [67] | Hospitalisation time is associated with weight gain in forensic mental health patients with schizophrenia or bipolar disorder | The aim of this study was to explore the body habitus amongst inpatients within forensic mental health inpatients. | A retrospective cohort study including forensic mental health patients with schizophrenia or bipolar disorder. Patient characteristics and data on body weight was extracted from electronic medical records. The association between duration of hospital stay and weight change per year was analysed using linear regression. Proportional hospital duration was determined between each measurement as the total number of days hospitalized divided by the total number of days. Analyses were adjusted for gender, age, smoking, and antipsychotic medication. | 328 forensic mental health patients were included, of which 91% were diagnosed with schizophrenia. Compared to outpatients, inpatients underweight at the point of admission had the largest difference in weight gain (+18.0 kg/year, p=0.006), and the weight gain difference was smallest in patients who were obese (+2.3 kg/year, p=0.21) at the point of admission. | The duration of hospital stay in forensic mental health wards is associated the with the largest difference in weight gain. | Duration of length of hospital stay was associated with an estimated difference of +4.0 kg/year for forensic mental health inpatients, compared to individuals managed within an outpatient setting. | |
| Shin J et al. England, 2012 [64] | Weight changes and characteristics of patients associated with weight gain during inpatient psychiatric treatment. | The aim of this study was to investigate weight changes of patients in a public psychiatric hospital. | A retrospective chart review of weight changes during an inpatient admission was conducted on a multi-racial population admitted for psychiatric inpatient treatment. | 400 patient records were included, with 59% males and an average BMI of 27.6±6.3 on admission. Patients gained an average of 2.45kg during psychiatric hospitalization. Patients with normal weight at admission were significantly more likely to gain weight compared to overweight or obese patients. Black patients showed the greatest weight gain, while Asian patients showed the smallest weight gain. | Patients with normal weight at the point of admission were significantly more likely to gain weight compared to overweight or obese patients. | Patients were likely to gain weight during an inpatient admission. | |
| Vieweg W et al. United States, 2004 [66] | Patient and direct-care staff body mass index in a state mental hospital: implications for management. | The aim of this study was to explore the body habitus amongst inpatients within a mental health hospital. | BMI of chronically psychotic patients on admission to a mental hospital and in follow-up, along with staff BMI. | At admission, patient BMI (26.4 +/- 5.8 kg/m2) was in the overweight range. Patients BMI (29.1 +/- 5.8 kg/m2) significantly increased (p< 0.0001) on follow-up to the level of obesity. Staff BMI (35.1 +/- 8.6 kg/m2) was in the obese range with 65% meeting criteria of obesity and 30% meeting criteria of morbid obesity. African American women made up 85% of clinical-care staff and constitute the race-sex mix most vulnerable to obesity in the US. Morbid obesity (BMI > or = 40 kg/m2) was five times more common among these African American female clinical-care staff than among African American women in the general US population. These findings may have treatment implications for chronically psychotic patients at risk for obesity. | Patients gained a significant amount of weight on admission. Most of the clinical staff working on the wards had excess weight. | Patients experienced significant weight gain following a hospital admission. Weight gain may be exacerbated further by a culture that normalises excess weight. | |
| Wang P et al. England, 2014 [65] | The use of psychiatric drugs and worsening body mass index among inpatients with schizophrenia. | The aim of this study was to investigate the relationship between psychotropic agents and overweight to obese inpatients with schizophrenia. | Retrospective chart review. | A total of 138 patients with schizophrenia were recruited in this retrospective study comparing characteristics of those who gained weight from overweight to obesity (n=23) compared to those who did not (n=115). Of the 138 patients, 60.9% were men. The mean age of patients 47.2±9.7 years, mean age of onset of disease 32.2±10.4 years, and the mean length of illness 15.0±6.5 years. Valproic acid was found to have a significant impact on the worsening of BMI from overweight to obesity (p<0.05). Age at onset of disease, length of illness, and duration of hospitalization were not associated significantly with worsening of BMI from overweight to obesity. | Valproic acid in patients with schizophrenia was associated with increased weight gain. | Psychotropic medication in individuals with severe mental illness is associated with significant weight gain. | |
| Wierda J et al. The Netherlands. 2024 [71] | Characterizing food environments of hospitals and long-term care facilities in the Netherlands: a mixed methods approach. | The aim of this study was to characterize the physical, socio-cultural, political and economic dimensions of the food environment for staff, patients and visitors within long term mental health care facilities. | Semi-structured interviews were held with staff members (n = 46) representing 11 hospitals and 26 long-term care facilities (rehabilitation centres, nursing homes, institutions for people with intellectual disabilities and mental healthcare institutions). In sub-study 2, staff members audited the food environment in hospitals (n = 28) and long-term care facilities (n = 36) using a predefined checklist. | The type of healthcare shaped the socio-cultural food environment, with acute hospitals emphasising nutrition for fast recovery, while long term care facilities using food more of an instrument to structure the day. Study participants highlighted the importance of organisational and food policies for regulating and improving the feed environment. Economic aspects associated with food budgets and contracts with external providers shaped the food associated within all healthcare settings. | Sustainability and healthiness should be prioritised. | Research in the future should investigate the underlying mechanisms of the healthcare environment for staff, visitors and patients whilst prioritising sustainability alongside healthiness. | |
| Williams B et al. USA, 2024 [74] | A qualitative exploration of barriers, facilitators and best practices for implementing environmental sustainability standards and reducing food waste in veterans’ affairs hospitals. | The aim of this study was to explore barriers, facilitators and best practices for implementing environmental sustainability standards in food service in mental health hospitals. | Online survey with hospital food service directors and qualitative interviews. The survey assessed self-reported motivators around five standards with regards to initiating sustainability standards and implementation, i) increasing plant-forward dishes, ii) procuring and serving sustainable foods that meet organic/fair trade and other certifications, iii) procuring and serving locally produced foods, iv) reducing food waste and v) reducing energy consumption. | The top three motivators cited were i) reducing food waste, ii) serving healthier foods and iii) increasing efficiency or cost savings. Barriers were reported as i) patient preferences, ii) contractual difficulties and iii) costs related to reducing waste. Facilitators included i) taste testing new recipes that include more sustainable food options and ii) easy access to sustainable products from the main supplier. Best practices included i) making familiar dishes plant-forward and ii) plate waste studies to prevent overproduction. | Food waste audits are central to better understanding which dishes need to be changed, and where overproduction may be contributing to food waste. | Although there were many barriers to implementation, directors of food service offered solutions for overcoming challenges and implementing food service sustainability standards, many of which included involving staff, visitors and patients with regards to taste testing familiar dishes made with plant-based alternatives. | |
| Wilson E et al. Canada. 2011 [77] | Going green in food services: Can health care adopt environmentally friendly practices? | The aim of this study was to examine reported environmentally friendly practices being implemented in the food service industry and consider ways in which health care or hospital food services can adopt some of these programs. | A review article | Suggestions are made for small changes to start the green initiative in each of these areas. A health care food service department is a large consumer of resources, and therefore food service workers, managers, dietitians, and administrators can make a significant difference by supporting and adopting environmentally friendly practices. | Knowledge mobilisation with regards to small changes towards sustainable practices. | Further studies are needed to determine which practices are currently being implemented in health care facilities, as well as perceived facilitators and barriers to these practices in the food service area. |
4. Discussion
The results of this scoping review highlight a lack of research considering the use of plant-based diets by default within mental health hospitals and how this would improve nutrition outcomes for inpatients as well as reducing the ecological impact of animal-protein based diets and food waste. This review identified five overarching themes requiring further investigation i) the food and socio-cultural environment, ii) evidence-based measures to reduce food waste, iii) the economic food environment, iv) inevitability of weight gain and v) theoretical model for behaviour change [34,64,65,66,67,68,69,70,71,72,73,74,75,76]. Most mental health hospitals use contract caterers to provide food for staff, visitors and patients typically offering animal-protein /meat-dominated menu by default, with plant-based meals (vegetarian or vegan) as single menu options often only available on request, decreasing uptake [79]. Although there are compelling arguments for plant-based by default diets [80,81] there is a paucity of evidence regarding components associated with the successful implementation of plant-based by default within mental health hospitals. Insights from other healthcare settings, where such approaches have been successfully adopted [54,55,56,57] may offer valuable guidance. This includes understanding the impact on important physical and mental health outcomes, financial costs, GHG emissions, and the role of behaviour change models in supporting transitions. In secure mental health wards restricted physical activities and deprivation of liberty further exacerbate these challenges [82,83]. Nutrition, knowledge, cooking and food skills, did not appear to be important barriers although they may be prerequisites for healthy eating [72]. Staff may lack various resourcces or will to implement the much needed changes [64,65,66,67,68,69,70], resulting in mealtime environments unconducive for pleasant eating experiences [34,71]. Inpatients with severe mental illness would benefit from nutritional support that aims at improving their daily structure and social inclusion, using behavioural approaches related to meal planning and social eating [72], as an admission to a mental health hospital for treatment of severe mental illness has a deleterious impact on body habitus, with an increased risk of obesity [64,65,66,67,68,69,70].
Interventions targeting food waste and dietary changes rely on education, training, environmental restructuring, modelling, and enablement [73]. Using behavioural change frameworks such as the COM-B model, [84,85] has indicated positive results by emphasising and obtaining staff buy-in, incentivising participation and behaviours, and establishing audit champions to support waste reduction [70,73]. A novel approach to engaging hospitalised patients in their nutritional care was described by Roberts et al. [86] using technology such as Nutri-Tec intervention deployed in a tertiary teaching hospital, Queensland, Australia. This complex intervention is underpinned by theoretical frameworks, concepts (e.g. knowledge exchange and patient participation in care) and an established evidence base. Nutri-Tec provides patient participation through i) patient education and training and ii) directed goal setting and patient-generated dietary intake tracking [87]. This patient centred approach enhances collaboration between patients and staff, providing a structured framework for change. The first aspect of the Nutri-Tec intervention includes brief education and impactful education on the significance of meeting energy and protein requirements during a hospital stay, guidance on how the hospitals electronic food service system works and how to access it via a bedside computer screen. The second aspect provides patients the opportunity to record their food intake after each meal on the bedside computer which helps track their intake relative to their individual nutrition goals. This in turn is supported by brief, daily goal setting with a healthcare professional to reinforce accountability and engagement.
This person/ patient centred approaches to staff and patient participation may help to support individualised approaches to improving patient engagement in achieving their nutrition goals [86] and support behaviour change [73]. Patients within a secure environment may also lack psychological or functional capacity to make better food choices [70], and coupled with staff not having sufficient knowledge or experience around motivating behaviour change with regards to food choices and achieving or maintaining a healthy weight [68], as there may be considerable resistance to change [22,23,73]. However, a technology approach with regards to engaging patients with regards to tailoring choice and education may work well with a mental health hospital; particularly as staff often feel conflicted around further encroaching on patients’ autonomy with regards unhealthy foods choices (i.e. takeaways), portion sizes and number of servings at mealtimes, along with purchase from food carts or vending machines, or eating food from other patients untouched trays. At the same time, staff have expressed a feeling of responsibility to restrict and control access to unhealthy food [68,70]. The development of technology-driven solutions in mental health hospitals could support person-centered participation, enabling patients and staff to actively engage in dietary changes and monitor progress to reinforce the adoption of plant-based diets long term, but would require further research with regards to accessibility of information in this format, especially with regards to digital literacy and skills [88,89,90] and functional ability [91,92].
An Independent Review of NHS Hospital Food [93] concentrated on local and seasonal (i.e. vegetable and fruit) food procurement and waste, rather than the need to reduce animal-protein/meat consumption and promote plant-based menu cycles [81]. However, there is a move to flip this model offering plant-based meals by default, with the option for animal-based meals on request. This approach may help to prevent the obesogenic impact of an inpatient admissions to a mental health hospital [64,65,66,67,68,69,70], and reduce the risk of chronic diseases (e.g., diabetes) [94], simultaneously decreasing the environmental impact and economic consequences of food waste [54]. Smith et al. [54] suggest plant-based diets by default is a more sustainable way of providing food for staff, visitors and patients, and behaviour change techniques may help people to be healthier and may be more ‘inclusive of all cultural, traditional, religious, and ethical preferences and can be free of common allergens’. Greener By Default, a movement supported by eleven hospitals in New York City have implemented plant-based meals for staff, visitors and patients by default reporting after two years more than 50% of patients chose plant-based meals, with a 36% reduction in greenhouse gas emissions, in addition to cost savings of 59 cents (46 pence) per meal [95]. Berardy et al. [96] explored the impact of plant-based diets offered to all patients in the first 24-hours of admission to an acute hospital setting. A limited 7-day study suggested plant-based meals were associated with significantly reduced food waste compared with meat-based meals within this setting. Although the others are clear their findings may not be generalisable, and the mechanism leading to the reduction in food waste is unclear.
Average plate waste has been described as between 6 - 65% [75,76,81,97], with food making up 50% of the total waste generated within the ward environment [16,17]. Common components of aspects contributing to food waste in hospitals include large portion sizes, vegetables, salad and fruit [75,76,81]. Food waste has significant environmental and economic implications and in order to implement sustainable practices [74,75] whilst reducing food waste, a multi-system implementation framework is needed, spanning from farm to fork [76]. Sustainability initiatives may support this, such as i) communication food waste reduction efforts to staff, patient and visitors, ii) feedback loops where staff and patients provide input and rating on food quality and preference to minimize waste, iii) kitchen staff training in food preparation techniques to reduce waste, v) collaboration with a nutritionist to develop appropriate meal plans, portion sizes, education for staff and patients about nutrition, and address challenges regarding food waste [74,75]. These initiatives can lead to significantly reduced food waste of -5.9% per kg, with 9% per patient, along with reductions in 22% environmental pollution points, 23% CO2e/kg emissions and 21% water usage (H2O – l/kg) respectively [75]. However, this assumption would need to be explored in addition to the impact on nutritional status of using plant-based diets [37,58] within a mental health setting.
5. Research Limitations
There are several limitations to this work relating to the paucity of evidence around the use of plant-based diets by default within mental health, as well as reducing the environmental impact of food waste and animal protein based diets. The quality of the evidence within the studies examined varied, with some small cohort sizes, however this was not formally assessed. This scoping review identified a numer of overarching themes associated with, the i) nutrition implications of plant-based diets, ii) acceptability and feasibility from staff, patients and visitors as plant-based meals choices by default, iii) training needs of staff, visitor and patients around the benefits of plant-based diets and healthier food choices for maintaining of sustaining a healthy weight, iv) the broader impact of food waste reduction and v) environmental and sustainability considerations aligngin with frameworks such as One Health [40]. Future research should address these limitations by incorporating larger, more representative samples and robust methodologies to evaluate the impact of plant-based diets in these and other healthcare settings. This includes their potential to improve nutrition outcomes for patients, reduce the environmental impact of food waste and animal-protein based diets, and lower the risk of chronic diseases associated with unhealthy eating behaviors in a secure mental health setting. Additionally, a holistic perspective is needed to integrate traditional knowledge with evidence-based innovations, ensuring the cultural acceptability, nutritional adequacy, and operational feasibility of plant-based diets in mental health hospitals across diverse settings.
6. Conclusions
Inpatient wards within mental health hospitals are obesogenic environments, with limited opportunity for meaningful engagement with physical activity, food choices which may not be tailored to individual preferences, and unrestricted access to nutritiously poor, high fat, high calorie foods from vending machines or takeaways resulting in high levels of food waste. The use of plant-based diets may provide an opportunity to reduce waste management costs associated with food waste, reduce the enviromental impact of animal-based protein diets and offer a healthier less obesogenic diet for patients and staff. However, patient and staff engagement using a behaviour change framework should underpin interventions aimed at addressing these challenges, incorporating training, education and goal-setting components for staff, patients and visitors to foster more nutritious dietary choices within an improved food environment. Future efforts should also consider integrating cullturally appropriate and evidence-based innovations to enhance the feasibility and acceptability of such interventions within diverse inpatient settings.
Supplementary Materials
None.
Author Contributions
Conceptualization, LVM; methodology, LVM; formal analysis, LVM, RM.; investigation, LVM; data extraction and curation LVM, RM; writing—original draft preparation, LVM; writing—review and editing, JVEB, SV, RM; project administration, LVM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No data is available.
Acknowledgments
None to note.
Conflicts of Interest
Luise Marino has received honorarium to give lectures for Abbott Laboratories, Danone and Nestle, who had no role in role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. None of the other authors have note any conflicts of interest to declare.
References
- The Paris Agreement | UNFCCC [Internet]. Available online: https://unfccc.int/process-and-meetings/the-paris-agreement/the-paris-agreement (accessed on 21 December 2022).
- lena. CCARDESA. 2019. IPCC Special Report: Global Warming of 1.5 oC - Summary for Policymakers. Available online: https://www.ccardesa.org/knowledge-products/ipcc-special-report-global-warming-15-%C2%BAc-summary-policymakers (accessed on 21 December 2022).
- How do greenhouse gases actually warm the planet? [Internet]. 2022. Available online: https://www.unep.org/news-and-stories/story/how-do-greenhouse-gases-actually-warm-planet (accessed on 25 January 2025).
- Chen, Z.; Wang, X.; Xia, Y. A review of the energy consumption and greenhouse gas emissions of hospitals in China. Renewable and Sustainable Energy Reviews 2022, 109838. [Google Scholar]
- Climate change and health [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health (accessed on 21 December 2022).
- Erol, A.; Karahan, H. Energy consumption and emission factors of a hospital in Turkey. Journal of Cleaner Production 2018, 207, 384–393. [Google Scholar]
- Health-care waste [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 16 December 2023).
- Health Care without Harm. The role of the health care sector in climate change mitigation. In London; 2022. Available online: https://saludsindanio.org/sites/default/files/documents-files/7347/2022_AnnualReport_HCWH.pdf (accessed on 16 December 2023).
- Health care climate footprint report | Health Care Without Harm (Global) [Internet]. Available online: https://global.noharm.org/resources/health-care-climate-footprint-report (accessed on 29 January 2025).
- Ngcamu, B.S. Climate change effects on vulnerable populations in the Global South: a systematic review. Nat Hazards 2023, 118, 977–991. [Google Scholar] [CrossRef]
- Abbass, K.; Qasim, M.Z.; Song, H.; Murshed, M.; Mahmood, H.; Younis, I. A review of the global climate change impacts, adaptation, and sustainable mitigation measures. Environ Sci Pollut Res Int. 2022, 29, 42539–42559. [Google Scholar] [CrossRef]
- Tennison, I.; Roschnik, S.; Ashby, B.; Boyd, R.; Hamilton, I.; Oreszczyn, T.; et al. Health care’s response to climate change: a carbon footprint assessment of the NHS in England. Lancet Planet Health 2021, 5, e84–e92. [Google Scholar] [CrossRef]
- Wooldridge, G.; Murthy, S. Pediatric Critical Care and the Climate Emergency: Our Responsibilities and a Call for Change. Front Pediatr. 2020, 8, 472. [Google Scholar] [CrossRef] [PubMed]
- England NHS. NHS England » National standards for healthcare food and drink [Internet]. 2022. Available online: https://www.england.nhs.uk/publication/national-standards-for-healthcare-food-and-drink/ (accessed on 16 January 2025).
- From Farm to Kitchen: The Environmental Impacts of U.S. Food Waste.
- Alam, M.M.; Sujauddin, M.; Iqbal, G.M.A.; Huda, S.M.S. Report: Healthcare waste characterization in Chittagong Medical College Hospital, Bangladesh. Waste Manag Res. 2008, 26, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Mattoso, V.D.; Schalch, V. Hospital waste management in Brazil: a case study. Waste Manag Res. 2001, 19, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Nutrition-and-Hydration-Digest-3rd-edition.pdf [Internet]. Available online: https://www.bda.uk.com/static/176907a2-f2d8-45bb-8213c581d3ccd7ba/06c5eecf-fa85-4472-948806c5165ed5d9/Nutrition-and-Hydration-Digest-3rd-edition.pdf (accessed on 12 August 2024).
- Food-surplus-and-waste-in-the-UK-key-facts-Jan-2020.pdf [Internet]. Available online: https://www.wrap.ngo/sites/default/files/2020-11/Food-surplus-and-waste-in-the-UK-key-facts-Jan-2020.pdf (accessed on 13 August 2024).
- Chatzipavlou, M.; Karayiannis, D.; Chaloulakou, S.; Georgakopoulou, E.; Poulia, K.A. Implementation of sustainable food service systems in hospitals to achieve current sustainability goals: A scoping review. Clin Nutr ESPEN 2024, 61, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.; Collins, J.; Goodwin, D.; Porter, J. A systematic review of food waste audit methods in hospital foodservices: development of a consensus pathway food waste audit tool. J Hum Nutr Diet 2022, 35, 68–80. [Google Scholar] [CrossRef]
- Cook, N.; Collins, J.; Goodwin, D.; Porter, J. Factors influencing implementation of food and food-related waste audits in hospital foodservices. Front Nutr. 2022, 9, 1062619. [Google Scholar] [CrossRef]
- Cook, N.; Porter, J.; Goodwin, D.; Collins, J. Diverting Food Waste From Landfill in Exemplar Hospital Foodservices: A Qualitative Study. J Acad Nutr Diet 2023, S2212-2672(23)01763-X. [Google Scholar] [CrossRef]
- Mahmoudifar, K.; Raeesi, A.; Kiani, B.; Rezaie, M. Food waste in hospitals: implications and strategies for reduction: a systematic review. Management of Environmental Quality: An International Journal 2024. [Google Scholar] [CrossRef]
- Baumgartner, A.; Kägi-Braun, N.; Tribolet, P.; Gomes, F.; Stanga, Z.; Schuetz, P. Individualised nutritional support in medical inpatients - a practical guideline. Swiss Med Wkly. 2020, 150, w20204. [Google Scholar] [CrossRef] [PubMed]
- Cristancho, C.; Mogensen, K.M.; Robinson, MK. Malnutrition in patients with obesity: An overview perspective. Nutr Clin Pract. 2024, 39, 1300–1316. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Long, Y.; Peng, R.; He, P.; Luo, Y.; Zhang, Y.; et al. Epidemiology, Controversies, and Dilemmas of Perioperative Nutritional Risk/Malnutrition: A Narrative Literature Review. Risk Management and Healthcare Policy 2025, 18, 143–162. [Google Scholar] [CrossRef]
- Wunderle, C.; Gomes, F.; Schuetz, P.; Stumpf, F.; Austin, P.; Ballesteros-Pomar, M.D.; et al. ESPEN practical guideline: Nutritional support for polymorbid medical inpatients. Clin Nutr. 2024, 43, 674–691. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Palomo, A.; Gomes-da-Costa, S.; Borràs, R.; Pons-Cabrera, M.T.; Doncel-Moriano, A.; Arbelo, N.; et al. Effects of malnutrition on length of stay in patients hospitalized in an acute psychiatric ward. Acta Psychiatr Scand. 2023, 148, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Day, M.; Moholkar, R.; Gilluley, P.; Goyder, E. Tackling obesity in mental health secure units: a mixed method synthesis of available evidence. BJPsych Open 2018, 4, 294–301. [Google Scholar] [CrossRef]
- Smith, J.; Ker, S.; Archer, D.; Gilbody, S.; Peckham, E.; Hardman, C.A. Food insecurity and severe mental illness: understanding the hidden problem and how to ask about food access during routine healthcare. BJPsych Advances 2023, 29, 204–212. [Google Scholar] [CrossRef]
- The King’s Fund [Internet]. Mental Health 360 | Acute Care For Adults. Available online: https://www.kingsfund.org.uk/insight-and-analysis/long-reads/mental-health-360-acute-mental-health-care-adults (accessed on 13 August 2024).
- Longer hospital stays and fewer admissions - The Health Foundation [Internet]. Available online: https://www.health.org.uk/publications/long-reads/longer-hospital-stays-and-fewer-admissions (accessed on 13 August 2024).
- Porter, J.; Collins, J. Nutritional intake and foodservice satisfaction of adults receiving specialist inpatient mental health services. Nutr Diet 2022, 79, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D. Defining a healthy diet globally: The good, the bad, and the ugly. The American Journal of Clinical Nutrition 2024, 120, 1003–1004. [Google Scholar] [CrossRef]
- Fanzo, J.; Rudie, C.; Sigman, I.; Grinspoon, S.; Benton, T.G.; Brown, M.E.; et al. Sustainable food systems and nutrition in the 21st century: a report from the 22nd annual Harvard Nutrition Obesity Symposium. Am J Clin Nutr. 2021, 115, 18–33. [Google Scholar] [CrossRef]
- Viroli, G.; Kalmpourtzidou, A.; Cena, H. Exploring Benefits and Barriers of Plant-Based Diets: Health, Environmental Impact, Food Accessibility and Acceptability. Nutrients 2023, 15, 4723. [Google Scholar] [CrossRef] [PubMed]
- Owino, V.; Kumwenda, C.; Ekesa, B.; Parker, M.E.; Ewoldt, L.; Roos, N.; et al. The impact of climate change on food systems, diet quality, nutrition, and health outcomes: A narrative review. Front Clim [Internet]. 2022 Aug 16. Available online: https://www.frontiersin.org/journals/climate/articles/10.3389/fclim.2022.941842/full (accessed on 5 February 2025).
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Redondo-Flórez, L.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Global Impacts of Western Diet and Its Effects on Metabolism and Health: A Narrative Review. Nutrients 2023, 15, 2749. [Google Scholar] [CrossRef] [PubMed]
- One health [Internet]. Available online: https://www.who.int/health-topics/one-health (accessed on 26 January 2025).
- Food security and nutrition and sustainable agriculture | Department of Economic and Social Affairs [Internet]. Available online: https://sdgs.un.org/topics/food-security-and-nutrition-and-sustainable-agriculture (accessed on 27 January 2025).
- Xu, X.; Sharma, P.; Shu, S.; Lin, T.S.; Ciais, P.; Tubiello, F.N.; et al. Global greenhouse gas emissions from animal-based foods are twice those of plant-based foods. Nat Food 2021, 2, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Advances in Nutrition 2019, 10, S275–S283. [Google Scholar] [CrossRef]
- Gibbs, J.; Cappuccio, F.P. Plant-Based Dietary Patterns for Human and Planetary Health. Nutrients 2022, 14, 1614. [Google Scholar] [CrossRef] [PubMed]
- redazione. Food Compliance Solutions. 2021 ULTRA-PROCESSED FOODS: NOVA CLASSIFICATION. Available online: https://regulatory.mxns.com/en/ultra-processed-foods-nova-classification (accessed on 29 January 2025).
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- EAT [Internet]. EAT-Lancet Commission Brief for Everyone. Available online: https://eatforum.org/lancet-commission/eatinghealthyandsustainable/ (accessed on 4 February 2025).
- Plant-based and sustainable diet: A systematic review of its impact on obesity - Mambrini - Obesity Reviews - Wiley Online Library [Internet]. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/obr.13901?msockid=12382da5a90f6ceb15f838b7ad0f67c3 (accessed on 2 February 2025).
- Pais, D.F.; Marques, A.C.; Fuinhas, J.A. The cost of healthier and more sustainable food choices: Do plant-based consumers spend more on food? Agric Food Econ. 2022, 10, 18. [Google Scholar] [CrossRef]
- Drewnowski, A. Analysing the affordability of the EAT–Lancet diet. The Lancet Global Health 2020, 8, e6–e7. [Google Scholar] [CrossRef] [PubMed]
- Hirvonen, K.; Bai, Y.; Headey, D.; Masters, W.A. Affordability of the EAT-Lancet reference diet: a global analysis. Lancet Glob Health 2020, 8, e59–e66. [Google Scholar] [CrossRef] [PubMed]
- Hoenink, J.C.; Garrott, K.; Jones, N.R.V.; Conklin, A.I.; Monsivais, P.; Adams, J. Changes in UK price disparities between healthy and less healthy foods over 10 years: An updated analysis with insights in the context of inflationary increases in the cost-of-living from 2021. Appetite 2024, 197, 107290. [Google Scholar] [CrossRef] [PubMed]
- Onwezen, M.C.; Bouwman, E.P.; Reinders, M.J.; Dagevos, H. A systematic review on consumer acceptance of alternative proteins: Pulses, algae, insects, plant-based meat alternatives, and cultured meat. Appetite 2021, 159, 105058. [Google Scholar] [CrossRef] [PubMed]
- Plants First Healthcare; Normalising plant-based meals in healthcare. By Dr. Laura-Jane Smith and Dr. Shireen Kassam – The official blog of BMJ Leader [Internet]. 2024. Available online: https://blogs.bmj.com/bmjleader/2024/10/01/plants-first-healthcare-normalising-plant-based-meals-in-healthcare-by-dr-laura-jane-smith-and-dr-shireen-kassam/ (accessed on 16 January 2025).
- Saldivar, B.; Al-Turk, B.; Brown, M.; Aggarwal, M. Successful Incorporation of a Plant-Based Menu Into a Large Academic Hospital. Am J Lifestyle Med. 2021, 16, 311–317. [Google Scholar] [CrossRef]
- Morgenstern, S.; Redwood, M.; Herby, A. An Innovative Program for Hospital Nutrition. Am J Lifestyle Med. 2024, 15598276241283158. [Google Scholar] [CrossRef]
- Roland. Hayek Hospital, The very 1st Hospital in the world to serve exclusively plant-based vegan food! – Hayek Hospital [Internet]. 2021. Available online: https://hayekhospital.org/2021/06/14/hayek-hospital-the-very-1st-hospital-in-the-world-to-serve-exclusively-plant-based-vegan-food/ (accessed on 26 January 2025).
- Tso, R.; Forde, C.G. Unintended Consequences: Nutritional Impact and Potential Pitfalls of Switching from Animal- to Plant-Based Foods. Nutrients 2021, 13, 2527. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]
- Shin, J.K.; Barron, C.T.; Chiu, Y.L.; Jang, S.H.; Touhid, S.; Bang, H. Weight changes and characteristics of patients associated with weight gain during inpatient psychiatric treatment. Issues Ment Health Nurs. 2012; 33, 505–512. [Google Scholar] [CrossRef]
- Wang, P.S.; Wu, S.L.; Ching, H.Y. The use of psychiatric drugs and worsening body mass index among inpatients with schizophrenia. Int Clin Psychopharmacol. 2014, 29, 235–238. [Google Scholar] [CrossRef]
- Vieweg, W.V.; Thomas, M.; Janisko, M.; Booth, M.; Fernandez, A.; Pandurangi, A.; et al. Patient and direct-care staff body mass index in a state mental hospital: implications for management. Acta Psychiatr Scand. 2004, 110, 69–72. [Google Scholar] [CrossRef]
- Pedersen, A.L.W.; Gildberg, F.A.; Hjorth, P.; Højlund, M.; Andersen, K. Hospitalisation time is associated with weight gain in forensic mental health patients with schizophrenia or bipolar disorder. Nordic Journal of Psychiatry 2023, 77, 46–54. [Google Scholar] [CrossRef]
- Mills, S.; Kaner, E.F.S.; Ramsay, S.E.; McKinnon, I. What are the key influences and challenges around weight management faced by patients in UK adult secure mental health settings? A focused ethnographic approach. BMJ Open 2024, 14, e079406. [Google Scholar] [CrossRef] [PubMed]
- Megna, J.L.; Raj Kunwar, A.; Wade, M.J. A retrospective study of weight changes and the contributing factors in short term adult psychiatric inpatients. Ann Clin Psychiatry 2006, 18, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, G.E.; Gorczynski, P.F.; Cohn, T.A. Psychiatric illness and obesity: recognizing the “obesogenic” nature of an inpatient psychiatric setting. Psychiatr Serv. 2009, 60, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Wierda, J.J.; de Vet, E.; Troost, E.; Poelman, M.P. Characterizing food environments of hospitals and long-term care facilities in the Netherlands: a mixed methods approach. BMC Health Services Research 2024, 24, 31. [Google Scholar] [CrossRef] [PubMed]
- Mötteli, S.; Provaznikova, B.; Vetter, S.; Jäger, M.; Seifritz, E.; Hotzy, F. Examining Nutrition Knowledge, Skills, and Eating Behaviours in People with Severe Mental Illness: A Cross-Sectional Comparison among Psychiatric Inpatients, Outpatients, and Healthy Adults. Nutrients 2023, 15, 2136. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.; Collins, J.; Porter, J.; Goodwin, D. Applying the theoretical domains framework and behavior change wheel to inform interventions for food and food-related waste audits in hospital foodservices. Front Nutr. 2023, 10, 1204980. [Google Scholar] [CrossRef]
- Williams, B.D.; Pitts, S.J.; Onufrak, S.J.; Sirois, E.; Utech, A.; Wood, M.; et al. A qualitative exploration of barriers, facilitators and best practices for implementing environmental sustainability standards and reducing food waste in veterans affairs hospitals. J Hum Nutr Diet [Internet]. 2024 [cited 8AD Jan 1]. Available online: https://pubmed.ncbi.nlm.nih.gov/39099188/.
- Liwinski, T.; Bocek, I.; Schmidt, A.; Kowalinski, E.; Dechent, F.; Rabenschlag, F.; et al. Sustainability initiatives in inpatient psychiatry: tackling food waste. Front Psychiatry 2024, 15, 1374788. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; MHSc, R.; Taylor, J.R.D.; Tong, R.; PMDip, *!!! REPLACE !!!*; Thompson, S.R.D.; Thomson, E.R.D.; Robertson, A.R.D.; et al. Something to Chew on; Plate-Waste at an Ontario Veteran’s Centre. Can J Diet Pract Res. 2024, 85, 106–110. [Google Scholar] [CrossRef]
- Wilson, E.D.; Garcia, A.C. “Going green” in food services: Can health care adopt environmentally friendly practices? Can J Diet Pract Res. 2011, 72, 43–47. [Google Scholar] [CrossRef]
- Wilson, E.D.; Garcia, A.C. Environmentally friendly health care food services: a survey of beliefs, behaviours, and attitudes. Can J Diet Pract Res. 2011, 72, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Meis-Harris, J.; Rramani-Dervishi, Q.; Seffen, A.E.; Dohle, S. Food for future: The impact of menu design on vegetarian food choice and menu satisfaction in a hypothetical hospital setting. Journal of Environmental Psychology 2024, 97, 102348. [Google Scholar] [CrossRef]
- Beavan, S.; Baker, R.; Sadler, H.; Collinson, A. Improving the nutritional intake of hospital patients: how far have we come? A re-audit. J Hum Nutr Diet 2019, 32, 372–384. [Google Scholar] [CrossRef]
- Moody, S.C. Enhancing food sustainability in the acute hospital setting - a nurse-led study of patient food. Br J Nurs. 2024, 33, S8–S17. [Google Scholar] [CrossRef]
- Rogers, E.; Papathomas, A.; Kinnafick, F.E. Inpatient perspectives on physical activity in a secure mental health setting. Psychology of Sport and Exercise 2021, 52, 101827. [Google Scholar] [CrossRef]
- Barriers to using physical exercise as an intervention within inpatient mental health settings: A systematic review - McKenna - 2024 - International Journal of Mental Health Nursing - Wiley Online Library [Internet]. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/inm.13302?msockid=12382da5a90f6ceb15f838b7ad0f67c3 (accessed on 30 January 2025).
- West, R.; Michie, S. A brief introduction to the COM-B Model of behaviour and the PRIME Theory of motivation. Qeios [Internet]. 2020 Apr 7. Available online: https://www.qeios.com/read/WW04E6 (accessed on 30 January 2025).
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.; Hopper, Z.; Chaboyer, W.; Gonzalez, R.; Banks, M.; Desbrow, B.; et al. Engaging hospitalised patients in their nutrition care using technology: development of the NUTRI-TEC intervention. BMC Health Services Research 2020, 20, 148. [Google Scholar] [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, P.; Wadman, R.; Walker, L.; Heron, P.; Mathers, A.; Baker, J.; et al. Measuring the digital divide among people with severe mental ill health using the essential digital skills framework. Perspect Public Health 2024, 144, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.A.; Blease, C.; Faurholt-Jepsen, M.; Firth, J.; Van Daele, T.; Moreno, C.; et al. Digital mental health: challenges and next steps. BMJ Ment Health 2023, 26, e300670. [Google Scholar] [CrossRef] [PubMed]
- Stein, O.A.; Prost, A. Exploring the societal implications of digital mental health technologies: A critical review. SSM - Mental Health 2024, 6, 100373. [Google Scholar] [CrossRef]
- Jameel, L.; Valmaggia, L.; Barnes, G.; Cella, M. mHealth technology to assess, monitor and treat daily functioning difficulties in people with severe mental illness: A systematic review. J Psychiatr Res. 2021, 145, 35–49. [Google Scholar] [CrossRef]
- Carpenter-Song, E.; Noel, V.A.; Acquilano, S.C.; Drake, R.E. Real-World Technology Use Among People With Mental Illnesses: Qualitative Study. JMIR Mental Health 2018, 5, e10652. [Google Scholar] [CrossRef]
- GOV.UK [Internet]. Independent review of NHS hospital food. Available online: https://www.gov.uk/government/publications/independent-review-of-nhs-hospital-food (accessed on 16 January 2025).
- Holt, R.I.G.; Mitchell, A.J. Diabetes mellitus and severe mental illness: mechanisms and clinical implications. Nat Rev Endocrinol. 2015, 11, 79–89. [Google Scholar] [CrossRef] [PubMed]
- NYC Health + Hospitals [Internet]. NYC Health + Hospitals Celebrates 1.2 Million Plant-Based Meals Served. Available online: https://www.nychealthandhospitals.org/pressrelease/nyc-health-hospitals-celebrates-1-2-million-plant-based-meals-served/ (accessed on 16 January 2025).
- Berardy, A.J.; Rubín-García, M.; Sabaté, J. A Scoping Review of the Environmental Impacts and Nutrient Composition of Plant-Based Milks. Adv Nutr. 2022, 13, 2559–2572. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Walton, K. Plate waste in hospitals and strategies for change. e-SPEN, the European e-Journal of Clinical Nutrition and Metabolism 2011, 6, e235–e241. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



