Submitted:
05 February 2025
Posted:
06 February 2025
You are already at the latest version
Abstract
Diquafosol is a purinergic P2Y2 receptor agonist that is garnering much interest for its potential therapeutic benefits in dry eye disease (DED) management and is used commonly in Asia. Diquafosol’s mechanism of action involves enhancing fluid secretion from conjunctival epithelial cells and promoting mucin secretion, thereby improving tear film stability and ocular surface lubrication. Clinical trials have demonstrated its efficacy in effectively targeting all three DED subtypes, aqueous-deficient, decreased-wettability, and evaporative dry eye, by increasing tear production leading to improvements in objective markers and reducing subjective symptoms of DED. Adverse effects are generally mild and transient, including ocular irritation and discomfort. This review explores future research directions including its efficacy in certain subtypes of DED yet to be thoroughly explored, inter-product superiority, creation of various formulations, recommended treatment duration and its potential combination therapies. Overall, this review seeks to provide an overview of the pharmacological properties, clinical efficacy, safety profile, clinical utility, long-term usage, and prospects of diquafosol in managing DED. Diquafosol represents a promising novel option in the armamentarium against DED to address the underlying pathophysiology of this common ocular condition.
Keywords:
dry eye
; diquafosol
; ocular surface disorders
; tear film-oriented therapy
; tear film oriented diagnosis
; topical non-steroidal immunosuppressants
; Ocular Graft versus Host Disease
; soft contact lens users
; LASIK
; post-cataract surgery
1. Introduction
Dry eye disease (DED) is a chronic, multifactorial ocular surface disease [1] and is particularly common in Asia, with a pooled prevalence of 21.7% among males and 16.4% among females [2]. In China alone, a meta-analysis estimated that symptomatic DED affects approximately 31.4% of the population, corresponding to 394 million individuals [3]. DED carries a significant symptomatic burden and is associated with reduced quality of life and vision [4]. Patients with severe DED have reported that loss in health utilities were comparable to patients on dialysis, experiencing severe angina or a disabling hip fracture [5]. At a population level, these issues translate into substantial economic costs, with estimated annual healthcare expenditures for DED reaching USD$104-167 billion in China and USD$55 billion in the United States respectively [6,7].
Several factors contribute to the development of DED, including systemic and ocular diseases, medication intake, genetic, environmental and lifestyle choices. The Tear Film and Ocular Surface Society Dry Eye Workshop II (TFOS DEWS II) defines DED as a multifactorial disease of the tear and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface [8]. It highlights tear film hyperosmolarity and inflammation as key drivers of epithelial damage. The Asia Dry Eye Society (ADES) defines DED as a multifactorial disease characterised by an unstable tear film causing a variety of symptoms or visual impairment, potentially accompanied by ocular surface damage [9]. In contrast to the TFOS DEWS II, ADES focuses on tear film instability as the primary mechanism of DED and suggests that inflammation occurs secondary to epithelial damage caused by an unstable tear film.
While perspectives on mechanisms leading to DED may differ, both highlight the critical role of tear film stability – the ability to maintain a smooth, continuous, and uniform layer over the corneal surface before breaking up [10]. Deficiencies in any of the key components of the tear film result in distinct DED subtypes, including aqueous-deficient, evaporative and decreased wettability, each characterised by variations in tear film dynamics and break-up patterns [10].
Diquafosol sodium, a first-in-class mucin secretagogue, has introduced a paradigm shift in the treatment of DED in Asia. Although primarily indicated to improve surface wettability, its effectiveness has been demonstrated across all DED sub-types. It is one of the few therapies that enhances lipid layer thickness (LLT) and goblet cell density while reducing conjunctival epithelial damage [11]. Diquafosol has reported superior efficacy over many tear-replacement solutions in improving tear production, ocular surface staining scores and tear film stability [12,13]. Emerging research highlights diquafosol’s effectiveness in managing an array of ocular surface disorders. This review aims to summarise its utility and provide recommendations for clinical use based on existing evidence, and offer insights into the future directions and innovations to optimise the management of ocular surface diseases.
2. Methods
A detailed search of the available literature was conducted in PubMed, EMBASE and COCHRANE from inception to September 2024. Key search terms included but were not limited to “dry eye”, “diquas”, “diquafosol”, “ocular surface disorders”, “tear film oriented therapy”, “tear film oriented diagnosis”, “tear-replacement solutions”, “topical corticosteroids”, “intense pulsed light”, “ocular graft versus host disease”, “soft contact lens users”, “LASIK”, “cataract surgery”. Both animal and human clinical studies were included in this review. Additionally, references were hand-searched for further relevant articles.
3. Pharmacologic Properties
3.1. Mechanism of Action
Diquafosol is a stable derivative of uridine 5’-triphosphate (UTP) and a potent P2Y2 receptor (P2Y2R) agonist that plays a significant role in regulating tear and mucin secretion. In the eye and ocular adnexae, P2Y2R are expressed by the corneal and conjunctival epithelium, goblet cells and meibomian glands [14]. Activation of P2Y2R elevates intracellular calcium ion concentrations and facilitates fluid transport from the serosal to mucosal side via chloride channel activation to enhance tear fluid secretion from conjunctival epithelial cells and mucin secretion from conjunctival goblet cells [15]. Diquafosol also augments gene expression of membrane-associated mucin 1 (MUC1), 4 (MUC4) and 16 (MUC16) in corneal epithelial cells and MUC1, MUC16 and membrane-associated mucin 5AC (MUC5AC) in conjunctival epithelial cells to stimulate mucin secretion [16]. Figure 1 summarises the action of diquafosol on various receptors in the ocular region to stabilise the tear film.
3.2. Commercially Available Formulations
Diquafosol 3% is presently available in two commercial formulations, a formulation containing chlorhexidine gluconate solution as a preservative (Diquas®) and a non-preservative, single vial formulation (Diquas®-S). Table 1 lists the active ingredients in Diquas® and Diquas®-S. When compared against Diquas®, administration of Diquas®-S has been reported to lead to greater improvements in dry eye symptoms, tear break-up time (TBUT) and meibomian gland function across parameters such as LLT, lid margin abnormalities, meibomian gland dysfunction stage, meibum expressibility and quality and meibomian gland dropout among post-cataract surgery patients after three months of usage [17]. However, Diquas®-S is presently available in a limited number of countries, with cost and logistical considerations likely limiting its commercial availability.
3.3. Adverse Effects
Diquafosol is a relatively safe medication with no serious adverse events associated with its usage reported across several major clinical trials [18,19,20,21,22,23,24]. A meta-analysis estimated the odds of developing adverse events from using topical diquafosol to be 1.7 times that of hyaluronic acid (odds ratio: 1.71, 95% confidence interval (CI): 1.08 to 2.71, p=0.02; I2=18%) [13]. Reported side effects, such as ocular irritation (6.3%), discharge (2.8%), foreign body sensation (2.8%), conjunctival hyperaemia (1.4%), pain (1.4%), and pruritus (1.4%) are generally mild and transient [19]. An observational study by Ohashi and coworkers reported an adverse drug reaction rate of 10.7%, primarily involving non-serious symptoms of eye discharge, irritation, pain, pruritus, foreign body sensation, with the highest incidence occurring during the first month of treatment [25]. A study by Nakamura and coworkers reported that symptoms of diquafosol-induced eye irritation and pain disappeared within seven days in about 50% of cases and within 28 days in 80% of cases following continued diquafosol instillation [11]. No studies till date have evaluated the mechanisms leading to a transient worsening of DED symptoms during diquafosol initiation. It is postulated that activation of P2Y2R in the acute phase induces a local pro-inflammatory state over the ocular surface [26]. Additionally, on compromised ocular surfaces with corneal epithelial erosions, diquafosol may bind to P2Y2R in nerve terminals and the purinergic pain receptor P2X3 to induce pain and discomfort [26]. Therefore, the authors recommend active management of ocular surface inflammation prior to commencement of topical diquafosol for DED. Additionally, patients ought to be primed regarding possible ocular discomfort and worsening dry eye symptoms upon commencement of diquafosol and encouraged to persist with treatment if minor side effects manifest.
Systemically, research has reported P2Y2R to worsen inflammation [26]. The activation of P2Y2R is reported to induce proinflammatory states in gastrointestinal, respiratory and neurological cells, and has also been implicated in cancer pathogenesis [27,28,29]. However, P2Y2R agonists have also been demonstrated to promote wound healing through recruitment of leukocytes to sites of tissue damage, facilitating differentiation and proliferation of structural cells [30]. Nevertheless, topical administration of diquafosol is unlikely to yield any systemic adverse reactions as it is rapidly metabolised at the ocular surface. Random sampling of 25 patients receiving topical diquafosol for six months showed no elevation of systemic concentration of derived metabolites relating to diquafosol [31]. Thus far, no studies have evaluated its safety during pregnancy.
3.4. Effects on Tear Stimulation
Diquafosol administration has been reported to increase tear fluid secretion in murine dry eye models. A study conducted on Goto-Kakizaki rats; a spontaneous murine model of type 2 diabetes with corneal neuropathy, which were exposed to constant airflow towards the face reported that diquafosol administration significantly increased Schirmer’s test after 15 minutes (p<0.01), reduced corneal fluorescein staining score at four (p<0.05) and six weeks (p<0.01) [32]. Exact values were not reported by the authors. This suggests the possible role of diquafosol in stimulating tear production, despite the presence of impaired corneal neuronal function. Another in-vivo murine study investigated the effect of diquafosol administration on corneal epithelial defects, with percentage of wound closure monitored via image analysis [33]. Rats were anesthetised followed by the creation of a 3 mm central corneal epithelial defect with a burr. Instillation of diquafosol facilitated earlier epithelial healing compared to control eyes at 12 and 24 hours respectively (percentage wound closure of diquafosol-treated eyes at 12 and 24 hours: 63.4±2.0% and 98.1±1.1%; percentage wound closure of control eyes at 12 and 24 hours: 42.7±2.5% and 82.3±3.2%). However, no mention of use of topical agents or vehicle in the control group was reported. This is further supported by in-vitro experiments demonstrating that diquafosol induces extracellular signal-regulated kinase cell proliferation, epithelial growth factor receptor phosphorylation and increased intracellular calcium, suggesting that the accelerated corneal epithelial healing process may be attributed to intracellular calcium-mediated epithelial growth factor receptor signalling pathways through the activation of P2Y2R [33].
Studies in human subjects have reported similar improvements in tear secretion. Administration of diquafosol in both healthy and DED patients demonstrated increased radius of curvature of the central lower tear meniscus for up to 30 minutes after instillation [34]. The radius of curvature of the lower tear meniscus shares a linear relationship with the cumulative tear volume over the ocular surface, serving as a surrogate measure of aqueous tear volume [35,36]. This was also observed in patients with aqueous deficient DED secondary to Sjögren’s syndrome, where instillation of diquafosol significantly increased the central lower tear meniscus radius curvature at 15 minutes [37]. These results suggest the role of diquafosol in promoting tear fluid secretion of conjunctival epithelial cells, independent of lacrimal gland function [33,37].
3.5. Effects on Lipid Secretion
Diquafosol has also been demonstrated to stimulate holocrine-like lipid secretion from meibocytes via activation of P2Y2R. Tissue sections of meibomian gland specimens from superoxide dismutase-1 (Sod1) mice and wild-type (WT) mice were stained with Oil Red O stain and analysed digitally using an image processing software to quantify the number of pixels corresponding to lipid droplets [38]. Administration of diquafosol six times daily for two weeks increased the total number of lipid droplets (20±15 droplets pre-treatment to 100±80 droplets two weeks post-treatment, p<0.01 in Sod1 mice and 25±10 droplets pre-treatment to 60±100 droplets two weeks post-treatment, p<0.05 in WT mice), which was attributed to increased meibum secretion. There were also documented improvements in corneal fluorescein staining score, attributed by the authors to improved tear film stability and the impact of diquafosol on corneal epithelial healing. This was supported by an in-vitro study of cultivated rabbit meibomian gland cells, suggesting that diquafosol induced intracellular calcium signalling in a dose-dependent manner, increasing total cholesterol cellular release [39]. Clinically, administration of diquafosol in human eyes increased LLT and tear film stability. Interferometry measurements of tear film LLT in normal human eyes showed a statistically significant increase in mean thickness from 62.3±31.1 nm to 77.0±39.5 nm (p<0.001), 79.3±40.5 nm (p<0.001), and 77.7±43.6 nm (P=0.009) at the 15, 30 and 60 minute mark respectively [40]. A study among dry eye patients revealed similar improvements in LLT, from an initial 49.4±16.2 nm to 70.6±28.2 nm (p<0.001) and 63.9±30.0 nm (p=0.042) at 30 and 60 minutes after diquafosol instillation [41]. In comparison, instillation of artificial tears did not result in significant increase in LLT after treatment, with measurements reported at 52.9±22.8 nm, 52.3±20.3 nm and 50.3±19.8 nm at 30, 60 and 90 minutes, respectively (p>0.05 for all) [41].
3.6. Effects on Mucin Secretion
Diquafosol is primarily a mucin secretagogue that improves corneal wettability by stimulating expression of human epithelial mucins via intracellular extracellular signal-regulated kinase [16]. Mucins are categorised into two groups: membrane-associated mucins and goblet-cell secreted mucin. MUC1, MUC4, MUC16 are produced by both corneal and conjunctiva epithelia while MUC5AC is a secretory mucin produced by goblet cells [42]. Membrane-associated mucins form a dense protective glycocalyx barrier over the ocular surface epithelia, facilitating debris clearance and improves the lubricity effect of the tear film, thereby reducing friction generated between the eyelid and cornea interfaces [43,44]. Secretory mucins assist in clearing ocular surface pathogens and, improves surface lubricity by forming a highly hydrated mucus gel that reduces friction [44,45]. In a rabbit study comparing the effects of diquafosol, rebamipide and artificial tears, only diquafosol was found to increase MUC5AC levels in rabbits’ tears after 15 minutes (p<0.01) [46]. Similar observations in canine models have been documented with statistically significant increase in tear film MUC5AC concentrations at 300min (p=0.033) following administration of diquafosol, although neither Schirmer’s nor phenol red thread testing demonstrated any statistically significant differences [47]. Another study by Lee and coworkers demonstrated increased expression of MUC1 and MUC16 by human conjunctival epithelial cells following instillation of diquafosol [16]. These in-vivo and in-vitro studies support the efficacy of diquafosol in inducing secretion of membrane-associated and secretory mucins on the ocular surface.
4. Therapeutic Efficacy
4.1. Dry Eye Disease
Multiple studies have reported the efficacy of diquafosol in alleviating symptoms and signs of DED. Ohashi and coworkers report significant symptomatic improvements and reduction in Dry Eye-related Quality of Life Score (DEQS) values in patients receiving topical diquafosol for a duration of 12 months [25]. Randomised double-masked parallel-group trials also reported findings of greater improvement in foreign body sensation and eyelid heaviness among patients receiving diquafosol compared to placebo artificial tears [19,20]. A randomised controlled trial involving patients with DED reported comparable improvements in corneal fluorescein staining score (-2.1±1.5 in diquafosol, -2.0±1.3 in sodium hyaluronate at week four, 95% CI: -0.303 to 0.181) between patients who utilised diquafosol compared to sodium hyaluronate eyedrops (P>0.05) [21]. However, improvements in conjunctival rose bengal staining score was more significant among diquafosol users (-2.5±2.0 in diquafosol, -2.0±1.9 in sodium hyaluronate at week four, p=0.019). Both treatment groups experienced improvements in TBUT by 1.046±1.797 s and 0.832±1.775 s respectively with no statistically significant differences between findings [21]. Meta-analyses of randomised controlled trials exploring outcomes of diquafosol administration for the treatment of DED have reported its efficacy in alleviating subjective ocular symptoms and improving dry eye indices compared to artificial tears [13,48]. Sun and co-workers analysed nine randomised controlled trials that recruited patients with DED and reported significant improvements in Ocular Surface Disease Index (OSDI) (mean difference (MD): -3.59, 95% CI: -4.68 to -2.50, p<0.001; I2=6%), Schirmer’s test (MD: 1.08 mm, 95% CI: 0.41 to 1.76, p=0.002; I2=0%), TBUT (MD: 0.60 s, 95% CI: 0.20 to 0.99, p=0.003; I2=63%), corneal fluorescein staining score (MD: -0.20, 95% CI: -0.37 to -0.03, p=0.02; I2=58%), and rose bengal staining score (MD: -0.62, 95% CI: -0.88 to -0.35, p<0.001; I2=15%) [13].
Diquafosol has also been shown to inhibit nuclear factor-kappa B (NF-kB) signalling and other inflammatory factors induced by hyperosmotic stress in in-vitro studies using human corneal epithelial cells, suggesting its role in the management of inflammation in DED [49]. A study conducted on DED patients receiving cyclosporine 0.1%, cyclosporine 0.05% or diquafosol measured downregulation of tear proteomes (AFM, ALCAM, CFB, H1-4, PON1, RAP1B, and RBP4) across all three groups after 12 weeks of treatment, suggesting a reduction in inflammation [50]. Clinical parameters, including conjunctival fluorescein staining score and TBUT improved following administration of all medications compared to baseline. However, corneal fluorescein staining score improved more significantly in patients receiving cyclosporine compared to diquafosol from baseline to 12 weeks (cyclosporine 0.1%: 4.89±1.26 to 1.39±1.37, p< 0.001; cyclosporine 0.05%: 4.69±1.12 to 1.31±1.52, p<0.001 vs diquafosol: 4.31±0.93 to 2.15±1.42, p<0.001). A prospective non-randomised observational study of patients with DED comparing administration of only cyclosporine 0.1% once daily versus cyclosporine 0.1% once daily in combination with diquafosol six times daily reported that combination therapy led to a greater degree of improvement in TBUT compared to patients receiving only cyclosporine 0.1% (combination: 2.13±2.41 s vs 1.07±1.71 s; p=0.001) [51]. Therefore, administration of diquafosol and cyclosporine in combination appears to produce synergistic effects over the ocular surface. Thus far, evidence remains inconclusive on whether patients with poor response to artificial tears should be preferentially started on topical diquafosol or cyclosporine. A study exploring patients’ considerations and preferences around medications in DED management has reported that costs and side effect profiles are major attributing factors to choice of therapy [52]. While diquafosol offers a more favourable side effect profile, physicians should be mindful that initiation of diquafosol in the early phases, particularly in patients with significant inflammation, may exacerbate ocular surface symptoms. This benefit must be weighed carefully against diquafosol’s cost and the need for more frequent administration compared to cyclosporine.
4.2. Meibomian Gland Dysfunction
Meibomian gland dysfunction is a chronic process characterised by structural abnormalities of the meibomian gland, terminal duct obstruction and changes in meibum quality [53]. A reduction in meibum secretion and changes to both its viscosity and lipid composition disrupts the tear film lipid layer, contributing to increased evaporative loss.
Several studies have identified the potential of utilising diquafosol in the management of patients with meibomian gland dysfunction. A longitudinal study of patients with obstructive meibomian gland dysfunction receiving diquafosol four times daily for four months or more reported an improvement in measured mean meibomian gland area from 36.9±10.1% pre-treatment to 41.5±9.2% post-treatment (p<0.001) [54]. Ocular surface symptoms, lid margin abnormalities; such as plugging of meibomian orifices, and TBUT also improved after instillation of diquafosol. Moreover, diquafosol has been reported to significantly increase LLT [40]. A study analysing DED patients receiving either topical diquafosol, normal saline, sodium hyaluronate 0.1% or gatifloxacin 0.3% found that only diquafosol led to a significant increase in LLT (Mean change in LLT from baseline to 20 minutes after instillation of eyedrops: 12.6±2.0 nm for diquafosol (p<0.001), 1.2±2.2 nm for normal saline (p=0.301), 1.5±2.0 nm for sodium hyaluronate (p=0.495), and 0.5±3.2 nm for gatifloxacin (p=0.884)) [55]. These results suggest a possible therapeutic role for diquafosol in the treatment of evaporative DED.
4.3. Aqueous-Deficient Dry Eye Disease
Aqueous-deficient DED is a subtype of DED characterised by decreased tear production by the lacrimal and accessory glands, affecting up to one-third of patients diagnosed with DED [56]. Aqueous-deficient DED can arise due to a plethora of pathological mechanisms that can ultimately result in lacrimal gland damage. Donthineni and coworkers have suggested a classification comprising of four major groups: immune-mediated lacrimal gland inflammation (such as Sjogren’s syndrome), conjunctival cicatrisation (mucous membrane pemphigoid and Stevens-Johnson syndrome), neurogenic causes (for example diabetes mellitus) and lacrimal gland loss (arising from trauma, age, or congenital alacrima) [57].
Diquafosol has been shown to be effective in alleviating both subjective and objective clinical parameters of aqueous-deficient DED. A study recruiting patients with mild-to-moderate aqueous-deficiency DED reported that patients receiving diquafosol experienced significant improvements in subjective dry eye symptoms evaluated by the authors based on a composite severity scoring system (exact scores were not reported, p<0.01), corneal fluorescein staining score (4.1±1.8 to 1.1±1.1, p<0.01) and tear meniscus height (126±24 μm to 171±48 μm, p<0.01) with no major adverse reactions reported [58]. Usage of diquafosol has also been reported to improve the optical quality of the tear film, with higher-order aberrations used as a surrogate measurement in patients receiving diquafosol for four weeks. These patients experienced improvements in higher-order aberrations measured from a wavefront sensor at four weeks compared to baseline (0.180±0.06 μm to 0.148±0.039 μm, p=0.035), with improvements in subjective dry eye symptom scores (24.3±6.7 to 15.3±6.0, p<0.001), corneal fluorescein staining score (4.6±1.4 to 1.9±1.1, p<0.001) and TBUT (1.6±0.8 s to 3.1±0.8 s, p<0.001), although no significant improvements were demonstrated with conjunctival fluorescein staining score (5.3±1.3 to 4.8±1.1, p=0.078) and Schirmer’s test (1.7±2.0 mm to 1.2±1.8 mm, p=0.228) [59].
Patients with Sjogren’s syndrome also benefit from diquafosol, with its use associated with significant increase in central lower tear meniscus radius curvature 15 minutes after diquafosol instillation (0.16±0.07 mm to 0.21±0.08 mm, p<0.001), while no improvements were reported in patients receiving solely artificial tears [37]. Another observational study of female patients with Sjogren’s syndrome who were symptomatic despite treatment with artificial tears reported that addition of diquafosol to the existing treatment regimen resulted in improvements in both subjective symptoms, as well as objective parameters including tear meniscus radius (baseline vs 12 months: p<0.001), TBUT (baseline vs 12 months: p<0.05), corneal fluorescein staining score (baseline vs 12 months: p<0.001) and conjunctival fluorescein staining score (baseline vs 12 months: p<0.05) at regular intervals up till the 12th month of diquafosol treatment [60]. Importantly, all patients in the study who experienced symptomatic flares were also permitted to instil topical corticosteroids up to twice daily, which may have confounded these findings. However, the proportion of patients receiving topical corticosteroids was not reported.
4.4. Ocular Graft-Versus-Host Disease (oGVHD)
Graft-versus-host disease (GVHD) is a complex immunological condition that arises from donor T-cell mediated responses towards recipient antigens, inciting tissue damage and cytokine-mediated activation of antigen-presenting cells [61]. Chronic GVHD involves additional processes such as thymic injury, B cell autoantibody synthesis, and the formation of profibrotic lesions [62]. oGVHD represents a significant complication of GVHD, with cicatrising changes and desiccation increasing the risk of corneal ulceration and perforation. oGVHD may affect all tear film components. Alloreactive T-cells promote myofibroblast proliferation which leads to fibrosis and destruction of lacrimal glands, with a consequent reduction in aqueous tear production [63]. T-cell infiltration, endothelial injury, neovascularisation and fibroblast activation have been observed in the meibomian glands of murine chronic GVHD models [64]. Another study reported that allogenic GVHD murine models had a significantly higher meibomian gland plugging score (1.5 vs 0, p<0.001) and more noticeable meibomian gland atrophy scored on the meiboscale (93% vs 47% atrophy) compared to the control group with no purified splenic T cells. These results suggest that meibomian gland changes occur with oGVHD which can reduce both the quantity and quality of meibum secretion in stabilising the lipid tear film layer [65]. Furthermore, mucin secretion is also impaired in oGVHD patients. Ogawa and coworkers suggest that epithelial mesenchymal transition, characterised by replacement of epithelial cell with mesenchymal markers incites basal epithelia secretion of abnormal collagen bundles contributing to conjunctival fibrosis that damages the mucin secretory function of goblet cells [66]. This is supported by findings in murine GVHD models in which a reduction in both the area and thickness of corneal glycocalyx has been reported [67]. Cicatrising changes that lead to eyelid abnormalities such as ectropion, entropion, lagophthalmos and trichiasis can further compromise the ocular surface [63].
Diquafosol has been studied as a treatment for oGVHD primarily for its mucin-secreting properties, but is also postulated to augment other components of the tear film. In a retrospective study of patients with mild to moderate chronic GVHD-induced DED using diquafosol for up to 17 months, marked improvements in corneal fluorescein staining score (5.9±0.6 to 1.3±1.1, p<0.001), corneal and conjunctival rose bengal staining score; an aggregate score of staining of the cornea, temporal and nasal conjunctiva (4.7±1.6 to 2.0±1.5, p=0.008), and TBUT (2.6±0.9 s to 4.6±1.6 s, p=0.009) were reported [68]. An anecdotal report of a 61-year-old lady with severe DED secondary to chronic GVHD showed that combination therapy of topical diquafosol six times daily with topical rebamipide four times daily resulted in a substantial reduction in an aggregated visual analogue score which measures 12 symptoms: asthenopia, pain, discharge, foreign body sensation, epiphora, burning, ocular itching, dull sensation, conjunctival injection, dullness, dryness, and photophobia from 33 points at baseline to 8.5 points. Improvements in objective clinical findings include corneal fluorescein staining score (4 to 1.5), cornea and conjunctiva rose bengal score, an aggregate of nasal, temporal conjunctiva and cornea (4 to 1), and TBUT (2.3 s to 10 s) [69]. However, no improvement on Schirmer’s test (3.0 mm to 3.0 mm) was identified compared to baseline. Further large-scale studies are required to ascertain its effectiveness in treating oGVHD.
4.5. Glaucoma Medication and Preservatives-Related Ocular Surface Disease
It has been reported that up to 59% of glaucoma patients experience ocular surface symptoms with 78% of patients in an examined cohort exhibiting signs of ocular surface disease [70]. The pathogenesis is multifactorial but has been significantly attributed to medicamentosa arising from the active ingredient, its excipients and associated preservatives [71]. Beta blocker formulations, particularly timolol maleate, have been reported to disrupt tear film stability, reduce tear secretions and incite cicatrising changes over the conjunctival epithelium [72,73,74,75,76]. Prostaglandin analogues induce obstructive meibomian gland dysfunction which exacerbates ocular surface disease and may contribute to poor compliance to glaucoma therapy [74,77]. Moreover, prostaglandin-associated periorbitopathy can induce periorbital and eyelid changes such as trichiasis, and periorbital fat loss that further alter and compromise the ocular surface [78]. Benzalkonium chloride (BAK) is a commonly used preservative that has been demonstrated to disrupt tear film homeostasis and alter corneal sensitivity in a dose-dependent manner [79,80]. A study examining corneal sensitivity in glaucoma patients using BAK-containing eyedrops reported a reduction in corneal sensitivity; measured with a Cochet-Bonnet esthesiometer, in a dose-dependent fashion. Findings of corneal sensitivity were 56.2±5.2 mm, 50.3±12.5 mm and 44.3±13.6 mm among those treated with none, one and two or more instillations of preserved eyedrops, respectively [81]. In-vivo confocal microscopy has also been applied, which demonstrates a significant reduction in sub-basal corneal nerve density among patients treated with BAK-containing medications as compared to BAK-free formulations [82]. BAK has also been shown to incite cornea, conjunctival, meibomian gland and trabecular meshwork cells toxicity [83,84,85]. A reduction in goblet cell density following brief exposure of the ocular surface to BAK containing formulations has been demonstrated using impression cytology [86]. In-vitro studies with human corneal-limbal epithelial cell cultures showed that prolonged exposure to 0.0025% and 0.01% BAK for an hour decreases the amount of functional mucin, eventually causing complete destruction of the mucous layer and diffuse damage to superficial corneal epithelial cells [87]. Instillation of BAK-preserved latanoprost upregulates tear inflammatory cytokines levels including IL-2, IL-5, IL-10, IL-12 (p70), IL-13, IL-15, IL-17, basic fibroblast growth factor, and platelet-derived growth factor compared to preservative-free formulations of latanoprost [88]. Several clinical studies have reported an association between BAK-containing medications and both worsening OSDI scores and poorer glaucoma filtering surgery outcomes [89,90]. It has been postulated that BAK induces conjunctival subepithelial inflammation and fibrosis [91], which aggravates the wound healing process in glaucoma filtering surgeries [92].
Diquafosol has been suggested to be useful in the management of glaucoma medication and preservative-related ocular surface symptoms due to its ability to promote tear and mucin secretion and stimulate meibomian gland function. Diquafosol contains chlorhexidine at a concentration of 0.0001-0.1% as a preservative, as detailed in the product insert. Chlorhexidine gluconate has been found to be safe and effective as an ocular surface antiseptic at concentrations between 0.05-0.1% [93]. While higher concentrations of chlorhexidine gluconate at 2-4% have been shown in rabbit studies to exhibit dose-dependent toxic effects such as corneal epithelial oedema, corneal de-epithelisation, conjunctival chemosis, bulbar conjunctival hyperaemia and anterior stromal oedema [94,95], application of concentrations of 1% or less did not result in delays in corneal re-epithelisation among experimental rabbit corneal abrasion models, with mild conjunctivitis as the only complication reported [96]. This suggests that diquafosol, even in its chlorhexidine gluconate preservative-containing formulation, is safe and produces minimal preservative-induced ocular surface complications. A clinical study recruited glaucoma patients suffering from DED and reported improvements in mean OSDI score (52.17±13.02 to 48.77±13.27, p=0.041), TBUT (3.79±1.94 s to 4.70±2.81 s, p=0.009) and Schirmer’s test (4.52±2.11 mm to 5.64±2.79 mm, p=0.001) up to 52 weeks following initiation of diquafosol [97]. Impression cytology demonstrated a sustained increase in goblet cell density which begun four weeks after commencing diquafosol, and lasting up to the 52 week mark (Baseline: 445.1±92.2 cells/mm2, 4 weeks: 511.0±110.8 cells/mm2, 12 weeks: 520.5±121.8 cells/mm2, 36 weeks: 504.8±160.3 cells/mm2, 52 weeks: 512.4±177.3 cells/mm2, p<0.05 for all). There was however no information provided regarding the type of anti-glaucoma medication used. Another study consisting of normal tension glaucoma patients who were either on a preservative-containing prostaglandin analogue, preservative-free prostaglandin analogue, or a combination of BAK-containing prostaglandin analogue (BAK-PGA) and diquafosol (BAK-PGA + DQS) suggested that diquafosol was protective against meibomian gland dropout that was associated with BAK-PGA [98]. In the BAK-PGA group, meibomian gland dropout increased significantly at nine and 12 months after initiation of topical therapy compared to baseline, while no statistically significant changes were observed among patients using solely BAK-free formulations or a BAK-PGA + DQS combination. Additionally, another study by Liu and coworkers on patients who underwent glaucoma surgery demonstrated that diquafosol administration in the early postoperative-period following trabeculectomy improved measured tear meniscus height (0.24±0.16 mm to 0.28±0.15 mm, p=0.025), TBUT (5.08±3.01 s to 9.02±3.20 s, p<0.05) and LLT (4.13±1.36 nm to 4.81±1.45 nm, p=0.007) at eight weeks postoperatively compared to baseline [99].
4.6. Cataract Surgery
Cataract surgery has been associated with a worsening of tear film parameters and increased dry eye symptoms postoperatively. A study examined patients three months after undergoing cataract surgery and demonstrated statistically significant deterioration of tear film parameters and increased dry eye symptoms [100]. Miyake and coworkers examined patients at one month after cataract surgery and reported that 31% of patients met the criteria for a diagnosis of DED [101]. This has been attributed to a range of factors, including medicamentosa, the surgical environment such as phototoxic effects from the operating microscope and surface desiccation and manipulation [102,103,104,105,106,107]. In patients with pre-existing ocular surface compromise, cataract surgery can alter meibum quality and exacerbate tear film instability and worsen symptoms [108,109].
In a study comparing patients receiving preservative-free diquafosol, preservative-containing diquafosol and preservative-free sodium hyaluronate commencing postoperatively from day one for three months, both groups of patients receiving diquafosol experienced significant improvements in measured TBUT at one month postoperatively compared to preoperative values (preservative-free: 4.6±2.2 s to 6.3±3.6 s, p<0.001, preservative-containing: 5.0±2.5 s to 7.0±2.8 s, p<0.001) [17]. These findings were compared to patients receiving sodium hyaluronate, where a decrease in TBUT from 4.6±1.8 s to 3.7±1.4 s (p=0.038) at one-month post-surgery was identified. At three months postoperatively, only patients receiving preservative-free diquafosol maintained significant improvements in TBUT compared to preoperative values (6.5±3.5 s vs 4.6±2.2 s, p=0.038) with significantly increased TBUT than patients receiving sodium hyaluronate (4.7±2.3 s vs 4.6±1.8 s, p=0.038). Similarly, OSDI and corneal fluorescein staining scores significantly improved in all patients receiving diquafosol compared to sodium hyaluronate. Schirmer’s test results remained unchanged across all groups throughout the study period. A study demonstrated that diquafosol administered six times daily postoperatively after cataract surgery resulted in significantly improved TBUT (4.88±2.52 s to 6.69±2.23 s at three months, p<0.001), corneal fluorescein staining score (values at three months were not reported, p=0.045), and conjunctival lissamine green staining score (1.55±1.19 to 0.36±0.76 at three months, p=0.001) compared to baseline [110].
Preoperative management of DED is important in ensuring accurate keratometry measurements, which can in-turn influence IOL calculations [111]. Trattler and coworkers reported that among patients scheduled for cataract surgery, 77% of eyes had evidence of corneal fluorescein staining while 63% of patients had a measured TBUT of five seconds or less, although the proportion of symptomatic patients was not reported [112]. Tear film instability can affect keratometric measurements. A study of dry eye patients scheduled for cataract surgery reported that IOL calculations may vary by as much as 0.5D between measurements across different visits [113]. Epitropoulos and coworkers have further reported that 8% of eyes with hyperosmolar tears had a difference of more than 0.50 D in measured mean keratometry values across two visits (p=0.049) and 17% of eyes had a vector astigmatism difference of more than 1.0 D (p=0.01). A multicentre prospective study of preoperative cataract surgery patients with DED found that administration of DQS-LX significantly improved the ocular surface and reliability of keratometry measurements [114]. In this study, patients were diagnosed using the Japanese version of the OSDI (J-OSDI) and underwent baseline biometry measurements and subsequently received DQS-LX thrice daily for four weeks. Post-treatment measurements demonstrated statistically significant improvements in TBUT (2.18±0.80 s pre-treatment to 4.29±1.14 s post-treatment, p<0.001) and corneal higher order of aberrations (0.30±0.03 µm pre-treatment to 0.25±0.03 µm post-treatment, p<0.001) after starting diquafosol. No statistically significant differences in measurements were seen in non-treated eyes across the measured time-points. Importantly, the duration between last dose of DQS-LX and keratometry measurements were not reported in this paper. Kobashi and coworkers have demonstrated improvements in mean intraocular scattering measured via the objective scattering index, a marker of optical quality, from 2.1±0.7 before treatment to 1.5±0.7 at two weeks (p<0.001), and 1.6±0.5 at four weeks (p<0.001), after treatment, measured at least two hours after the last instillation of diquafosol [115]. Instillation of diquafosol has also been associated with an increase in LLT and TBUT measured after at least 90 minutes following administration, in support of these findings [41]. Further research on the duration of onset of tear film changes following diquafosol administration will be useful in optimisation of keratometry measurements.
4.7. Contact Lens Wear
Contact lens wear compartmentalises the tear film into a pre- and post-lens tear film. This results in thinning of the tear film, which contributes to its instability and increased friction between the contact lens and the ocular surface [116]. Contact lens wear has also been associated with meibomian gland drop out, and is postulated to be related to either a reduction in volume of the pre-lens tear film or as a result of the direct mechanical effects of the contact lens [117]. These interactions can precipitate inflammation which contributes to further destabilisation of the tear film [116].
Diquafosol has been reported to create a statistically significant increase in pre- and post- (p<0.01 at 15 minutes and 30 minutes post-diquafosol instillation) lens tear film volumes in rabbit models of contact lens wear [118]. Topical application of diquafosol in soft contact lens users over a four week treatment period resulted in significant increase in fluorescein intensities of wheat germ agglutinin conjugate of fluorescein (F-WGA), which is used to quantify the presence of membrane-associated mucins (571.8±227.8 µg/ml to 794.6±219.4 µg/ml, p<0.001), while stable sialic acid and tear protein concentrations suggest that diquafosol increased mucin secretion. This study also reported significant improvement in subjective symptoms measured by DEQS (19.2±12.7 to 10.6±12.5, p=0.003), TBUT (3.6±2.2 s to 5.0±2.1 s, p=0.003), conjunctival fluorescein staining score (2.8±1.8 to 2.0±1.4, p=0.045), and corneal fluorescein staining score (0.7±1.0 to 0.3±0.6, p=0.021) [119]. Another study involving soft contact lens wearers on either a daily or fortnightly replacement schedule, reported that diquafosol significantly improved contrast sensitivity (p<0.05) following eight weeks of usage six times daily. In this study, both corneal fluorescein staining and conjunctival lissamine green staining scores decreased markedly in the diquafosol group (p=0.03 and p<0.001, respectively), with significantly lower conjunctival lissamine green staining score in the diquafosol group compared to soft contact lens wearers receiving artificial tears (p=0.02). Among contact lens users, Ogami and coworkers reported more significant improvement with diquafosol instillation for symptoms of dryness and blurred vision (p<0.01) compared to administration of artificial tears. This was postulated to be due to both good compliance to diquafosol and its ability to promote secretion of water and mucin, thereby stabilising the tear film [120].
Overnight orthokeratology lenses are an increasingly popular management modality for myopia control. However, 30-40% of patients experience ocular discomfort following lens insertion, which has been postulated to be due to tear film instability [121,122]. Similar to soft contact lenses, rigid gas permeable lenses can disrupt the tear film and induce meibomian gland atrophy [123,124]. A study by Xie and coworkers reported a significant increase in OSDI score following three months of orthokeratology lens usage compared to baseline (baseline: 4.13±4.21 vs third month: 7.26±4.52, p<0.05) [123]. A prospective study of paediatric orthokeratology lens wearers who were prescribed diquafosol four times daily for one month reported improved DEQS (5.54±3.25 to 3.85±2.98, p=0.00), tear meniscus height (0.20±0.05 mm to 0.21±0.05 mm, p=0.01) and TBUT (6.67±4.71 s to 10.32±6.19 s, p<0.001) compared to baseline [125]. Thus, diquafosol may help alleviate dry eye symptoms associated with paediatric orthokeratology lens wear and improve compliance, which is crucial for effective myopia management in children.
4.8. Keratorefractive Surgery
DED is the most common complication of keratorefractive surgery, with a reported prevalence of up to 75% of patients [126,127]. Pathogenesis of post-keratorefractive surgery dry eye is multifactorial, of which surgical transection of sub-basal corneal nerves; which reduces the cornea-blink reflex and disrupts the ocular surface-lacrimal gland neural loop, is a significant contributor [127]. This reduces the volume of tears secreted and induces tear film instability. Neurogenic inflammation, as evidenced by raised proinflammatory tear mediator levels (IL-6, MMP-9), neuropeptides (Substance P and calcitonin gene-related peptide) and neuromediators (nerve growth factor), also contribute to post-keratorefractive surgery dry eye [128]. Structures of the ocular surface, such as conjunctival goblet cells can inadvertently be damaged by surgical manipulation, such as during the application of suction devices in laser-assisted in situ keratomileusis (LASIK) and small incision lenticule extraction (SMILE) [129]. Other factors include administration of topical therapeutics which may induce a toxic effect on the conjunctiva and cornea [130] as well as central corneal flattening, which affects lid-globe apposition and may result in an abnormal distribution of the tear film and adversely affect meibomian gland function [131].
A prospective study of DED patients who underwent SMILE reported that cornea and conjunctival fluorescein staining score was lower in patients receiving diquafosol compared to sodium hyaluronate (1.20±1.06 vs 1.83±1.41 respectively, p=0.026) [132]. Additionally, the diquafosol group had better OSDI scores (12.98±7.29 vs 16.82±8.25, p=0.029), improved TBUT (5.83±2.02 s vs 4.24±0.94 s, p<0.001), and Schirmer’s test (7.75±3.92 mm vs 5.24±3.42 mm, p=0.003) three months post-surgery. A prospective study investigated the efficacy of diquafosol in treating patients experiencing persistent dry eye symptoms for over 12 months following LASIK [133]. This study compared the effects of diquafosol with those of artificial tears over a 12 week period. Results demonstrated that diquafosol significantly improved both subjective and objective parameters. Although Schirmer’s test was not significantly different after addition of diquafosol (7.4±5.1 mm pre-treatment vs 6.8±3.65 mm at 12 weeks post-treatment, p=0.48), TBUT improved from a baseline to one-week (p=0.007), four weeks (p=0.001), and 12 weeks (p<0.001), however, exact improvement in TBUT was not reported. Corneal fluorescein and conjunctival lissamine green staining scores improved within one week of initiating diquafosol treatment (p<0.001). Reported subjective symptoms; measured using a modified OSDI tool, demonstrated a reduction in fatigue, discomfort, dryness, grittiness, and difficulty reading (p<0.05).
In patients undergoing femtosecond LASIK (FS-LASIK), regardless whether dry eye was present, combining diquafosol six times a day and sodium hyaluronate four times a day postoperatively for a month significantly improved postoperative subjective symptoms, ocular surface status, and LLT compared to monotherapy with sodium hyaluronate therapy [134]. Additionally, all patients also received routine post-procedural eyedrops such as antibiotics and anti-inflammatory agents. The use of combination therapy significantly lowered OSDI scores (diquafosol and sodium hyaluronate: 17.55±15.70 to 16.97±9.96 vs sodium hyaluronate: 18.39±17.31 to 28.72±19.65, p=0.024) following FS-LASIK one month postoperatively. While there was no significant difference in corneal fluorescein staining score for the combination group between preoperative and postoperative visits, score increments were significantly lower for the combination group compared to the sodium hyaluronate group at one week (p=0.018) and was not statistically significant at one month after FS-LASIK. Furthermore, in patients without preoperative dry eye symptoms, addition of diquafosol resulted in better corneal sensitivity measured with a Cochet-Bonnet esthesiometer one month after FS-LASIK compared to patients who only used sodium hyaluronate (26.43 ± 20.80 mm vs 12.237 ± 14.86 mm, p=0.041). Confocal microscopic analysis of DED patients has suggested a possible role of diquafosol (administrated six times daily for three months) in increasing sub-basal corneal nerve density (Baseline: 829.6 ± 348.0 μm/mm2 vs three months: 1238.6 ± 410.1 μm/mm2, p=0.02) [135].
4.9. Long Acting Diquafosol (DQS-LX) Formulation
Diquafosol is usually prescribed up to six times daily for maximal efficacy. Compliance has however been identified as a challenge, with only 10.2% of participants reported to be compliant with the recommended administration frequency in a study [136]. A new long-acting diquafosol formulation which is administered thrice daily has recently been developed via the addition of polyvinylpyrrolidone (PVP). It confers several benefits including increased viscosity and higher levels of lipid-secretion more effectively compared to standard diquafosol formulation [137]. It is postulated that the increased viscosity reduces ocular surface irritation, improves tear fluid stability and reduces corneal and conjunctival epithelial damage. The lipid-increasing effect on the tear film may further minimise friction generated during lid-globe interactions and reduce evaporative loss. DQS-LX was dosed at three times daily as studies have shown that effects on corneal fluorescein staining score and TBUT were similar to when conventional diquafosol was used six times daily [138].
A randomised controlled trial of patients with aqueous deficient DED receiving DQS-LX were reported to experience improvements in corneal fluorescein staining (MD: -0.51, p<0.0001) and conjunctival lissamine green staining scores (MD: -0.33, p=0.0093) after four weeks of administration compared the vehicle control group [138]. Common adverse symptoms reported were eye irritation (3.6%) and discharge (1.8%) of mild severity.
Another study by Ishikawa and coworkers investigating compliance rates of patients using diquafosol reported that switching to a long-acting formulation improved adherence rates from 5.6% among those prescribed a conventional diquafosol formulation six times daily, to 88.9% in patients prescribed DQS-LX to be administered three times daily [139]. In this study, both formulations were found to be equally effective in improving TBUT.
Patients with reduced tear film volume or moderate-severe dry eyes with meibomian gland dysfunction have been reported to prefer the long-acting formulation, while those with allergic findings such as conjunctival papillae expressed their preference for conventional diquafosol [137]. The study cited eye stickiness, discharge, itchiness, and irritation as reasons for reverting to conventional diquafosol. Notably, patients with papillary and follicular changes of the conjunctiva are more symptomatic regardless of the severity of dry eye symptoms [140]. The preference for conventional diquafosol may be attributable to PVP, which increases tear viscosity and prolongs allergen residence time on the ocular surface, exacerbating itch. Additionally, patients with allergic conjunctivitis have been described to experience impaired blink mechanisms which may affect the lacrimal pump mechanism and contribute to tear retention [141]. Likely explanations for this include changes in the palpebral conjunctival anatomy due to papillae formation, as well as persistent itching, which can disrupt normal blinking patterns.
5. Conclusions
Existing evidence suggests that diquafosol is a useful addition to our treatment armamentarium in managing a range of ocular surface conditions, though exact mechanisms underpinning its reported range of benefits have yet to be fully elucidated. Clinicians considering prescribing diquafosol for their patients should be aware of its potential side effects, particularly when initiating therapy. Future efforts ought to focus on conducting rigorous high-quality trials to evaluate the effectiveness of diquafosol across the spectrum of ocular surface diseases against and alongside other pharmacological and office-based interventions, and effects of long term cessation of diquafosol to optimise treatment outcomes for patients with ocular surface disorders.
Author Contributions
DW and CHLL conceived and designed the study. CQLT, DW, XYT, CHLL analysed and interpreted the data. CQLT, DW, XYT wrote the original draft of the manuscript. CQLT, DW, XYT, BXHL, KCS, LT, CHLL reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- D. Wu, L. Tong, A. Prasath, B. X. H. Lim, D. K. Lim, and C. H. L. Lim, “Novel therapeutics for dry eye disease,” (in eng), Ann Med, vol. 55, no. 1, pp. 1211-1212, Dec 2023. [CrossRef]
- Y. Cai, J. Wei, J. Zhou, and W. Zou, “Prevalence and Incidence of Dry Eye Disease in Asia: A Systematic Review and Meta-Analysis,” (in eng), Ophthalmic Res, vol. 65, no. 6, pp. 647-658, 2022. [CrossRef]
- P. Song et al., “Variations of dry eye disease prevalence by age, sex and geographic characteristics in China: a systematic review and meta-analysis,” (in eng), J Glob Health, vol. 8, no. 2, p. 020503, Dec 2018. [CrossRef]
- M. Uchino and D. A. Schaumberg, “Dry Eye Disease: Impact on Quality of Life and Vision,” (in eng), Curr Ophthalmol Rep, vol. 1, no. 2, pp. 51-57, Jun 2013. [CrossRef]
- P. Buchholz et al., “Utility assessment to measure the impact of dry eye disease,” (in eng), Ocul Surf, vol. 4, no. 3, pp. 155-61, Jul 2006. [CrossRef]
- W. Yang et al., “Estimated Annual Economic Burden of Dry Eye Disease Based on a Multi-Center Analysis in China: A Retrospective Study,” (in eng), Front Med (Lausanne), vol. 8, p. 771352, 2021. [CrossRef]
- J. Yu, C. V. Asche, and C. J. Fairchild, “The economic burden of dry eye disease in the United States: a decision tree analysis,” (in eng), Cornea, vol. 30, no. 4, pp. 379-87, Apr 2011. [CrossRef]
- J. P. Craig et al., “TFOS DEWS II Definition and Classification Report,” (in eng), Ocul Surf, vol. 15, no. 3, pp. 276-283, Jul 2017. [CrossRef]
- K. Tsubota et al., “A New Perspective on Dry Eye Classification: Proposal by the Asia Dry Eye Society,” (in eng), Eye Contact Lens, vol. 46 Suppl 1, no. 1, pp. S2-s13, Jan 2020. [CrossRef]
- N. Yokoi and G. A. Georgiev, “Tear Film-Oriented Diagnosis and Tear Film-Oriented Therapy for Dry Eye Based on Tear Film Dynamics,” (in eng), Invest Ophthalmol Vis Sci, vol. 59, no. 14, pp. Des13-des22, Nov 1 2018. [CrossRef]
- M. Nakamura, T. Imanaka, and A. Sakamoto, “Diquafosol ophthalmic solution for dry eye treatment,” (in eng), Adv Ther, vol. 29, no. 7, pp. 579-89, Jul 2012. [CrossRef]
- T. Kojima et al., “The Effects of High Molecular Weight Hyaluronic Acid Eye Drop Application in Environmental Dry Eye Stress Model Mice,” (in eng), Int J Mol Sci, vol. 21, no. 10, May 15 2020. [CrossRef]
- X. Sun, L. Liu, and C. Liu, “Topical diquafosol versus hyaluronic acid for the treatment of dry eye disease: a meta-analysis of randomized controlled trials,” (in eng), Graefes Arch Clin Exp Ophthalmol, vol. 261, no. 12, pp. 3355-3367, Dec 2023. [CrossRef]
- M. S. Cowlen, V. Z. Zhang, L. Warnock, C. F. Moyer, W. M. Peterson, and B. R. Yerxa, “Localization of ocular P2Y2 receptor gene expression by in situ hybridization,” (in eng), Exp Eye Res, vol. 77, no. 1, pp. 77-84, Jul 2003. [CrossRef]
- T. Murakami, T. Fujihara, Y. Horibe, and M. Nakamura, “Diquafosol elicits increases in net Cl- transport through P2Y2 receptor stimulation in rabbit conjunctiva,” (in eng), Ophthalmic Res, vol. 36, no. 2, pp. 89-93, Mar-Apr 2004. [CrossRef]
- H. J. Lee et al., “Diquafosol ophthalmic solution enhances mucin expression via ERK activation in human conjunctival epithelial cells with hyperosmotic stress,” (in eng), Mol Vis, vol. 28, pp. 114-123, 2022.
- I. Jun et al., “Effects of Preservative-free 3% Diquafosol in Patients with Pre-existing Dry Eye Disease after Cataract Surgery: A Randomized Clinical Trial,” (in eng), Sci Rep, vol. 9, no. 1, p. 12659, Sep 2 2019. [CrossRef]
- Y. Matsumoto, Y. Ohashi, H. Watanabe, and K. Tsubota, “Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial,” (in eng), Ophthalmology, vol. 119, no. 10, pp. 1954-60, Oct 2012. [CrossRef]
- E. Takamura, K. Tsubota, H. Watanabe, and Y. Ohashi, “A randomised, double-masked comparison study of diquafosol versus sodium hyaluronate ophthalmic solutions in dry eye patients,” (in eng), Br J Ophthalmol, vol. 96, no. 10, pp. 1310-5, Oct 2012. [CrossRef]
- J. Tauber et al., “Double-masked, placebo-controlled safety and efficacy trial of diquafosol tetrasodium (INS365) ophthalmic solution for the treatment of dry eye,” (in eng), Cornea, vol. 23, no. 8, pp. 784-92, Nov 2004. [CrossRef]
- L. Gong et al., “A randomised, parallel-group comparison study of diquafosol ophthalmic solution in patients with dry eye in China and Singapore,” (in eng), Br J Ophthalmol, vol. 99, no. 7, pp. 903-8, Jul 2015. [CrossRef]
- K. Kamiya et al., “Clinical evaluation of the additive effect of diquafosol tetrasodium on sodium hyaluronate monotherapy in patients with dry eye syndrome: a prospective, randomized, multicenter study,” (in eng), Eye (Lond), vol. 26, no. 10, pp. 1363-8, Oct 2012. [CrossRef]
- H. S. Hwang, Y. M. Sung, W. S. Lee, and E. C. Kim, “Additive Effect of preservative-free sodium hyaluronate 0.1% in treatment of dry eye syndrome with diquafosol 3% eye drops,” (in eng), Cornea, vol. 33, no. 9, pp. 935-41, Sep 2014. [CrossRef]
- S. Shimazaki-Den, H. Iseda, M. Dogru, and J. Shimazaki, “Effects of diquafosol sodium eye drops on tear film stability in short BUT type of dry eye,” (in eng), Cornea, vol. 32, no. 8, pp. 1120-5, Aug 2013. [CrossRef]
- Y. Ohashi et al., “Long-Term Safety and Effectiveness of Diquafosol for the Treatment of Dry Eye in a Real-World Setting: A Prospective Observational Study,” (in eng), Adv Ther, vol. 37, no. 2, pp. 707-717, Feb 2020. [CrossRef]
- M. Idzko, D. Ferrari, and H. K. Eltzschig, “Nucleotide signalling during inflammation,” (in eng), Nature, vol. 509, no. 7500, pp. 310-7, May 15 2014. [CrossRef]
- T. S. Peterson et al., “P2Y2 nucleotide receptor-mediated responses in brain cells,” (in eng), Mol Neurobiol, vol. 41, no. 2-3, pp. 356-66, Jun 2010. [CrossRef]
- Z. Kargarpour et al., “Blocking P2Y2 purinergic receptor prevents the development of lipopolysaccharide-induced acute respiratory distress syndrome,” (in eng), Front Immunol, vol. 14, p. 1310098, 2023. [CrossRef]
- S. D. Bellefeuille, C. M. Molle, and F. P. Gendron, “Reviewing the role of P2Y receptors in specific gastrointestinal cancers,” (in eng), Purinergic Signal, vol. 15, no. 4, pp. 451-463, Dec 2019. [CrossRef]
- M. R. Elliott et al., “Nucleotides released by apoptotic cells act as a find-me signal to promote phagocytic clearance,” (in eng), Nature, vol. 461, no. 7261, pp. 282-6, Sep 10 2009. [CrossRef]
- D. Bremond-Gignac, J. J. Gicquel, and F. Chiambaretta, “Pharmacokinetic evaluation of diquafosol tetrasodium for the treatment of Sjögren’s syndrome,” (in eng), Expert Opin Drug Metab Toxicol, vol. 10, no. 6, pp. 905-13, Jun 2014. [CrossRef]
- A. Dota, A. Sakamoto, T. Nagano, T. Murakami, and T. Matsugi, “Effect of Diquafosol Ophthalmic Solution on Airflow-Induced Ocular Surface Disorder in Diabetic Rats,” (in eng), Clin Ophthalmol, vol. 14, pp. 1019-1024, 2020. [CrossRef]
- Y. S. Byun et al., “Diquafosol promotes corneal epithelial healing via intracellular calcium-mediated ERK activation,” (in eng), Exp Eye Res, vol. 143, pp. 89-97, Feb 2016. [CrossRef]
- N. Yokoi, H. Kato, and S. Kinoshita, “Facilitation of tear fluid secretion by 3% diquafosol ophthalmic solution in normal human eyes,” (in eng), Am J Ophthalmol, vol. 157, no. 1, pp. 85-92.e1, Jan 2014. [CrossRef]
- H. Oguz, N. Yokoi, and S. Kinoshita, “The height and radius of the tear meniscus and methods for examining these parameters,” (in eng), Cornea, vol. 19, no. 4, pp. 497-500, Jul 2000. [CrossRef]
- N. Yokoi, A. J. Bron, J. M. Tiffany, and S. Kinoshita, “Reflective meniscometry: a new field of dry eye assessment,” (in eng), Cornea, vol. 19, no. 3 Suppl, pp. S37-43, May 2000. [CrossRef]
- N. Yokoi, H. Kato, and S. Kinoshita, “The increase of aqueous tear volume by diquafosol sodium in dry-eye patients with Sjögren’s syndrome: a pilot study,” (in eng), Eye (Lond), vol. 30, no. 6, pp. 857-64, Jun 2016. [CrossRef]
- K. Ikeda et al., “The effects of 3% diquafosol sodium eye drop application on meibomian gland and ocular surface alterations in the Cu, Zn-superoxide dismutase-1 (Sod1) knockout mice,” (in eng), Graefes Arch Clin Exp Ophthalmol, vol. 256, no. 4, pp. 739-750, Apr 2018. [CrossRef]
- K. I. Endo, A. Sakamoto, and K. Fujisawa, “Diquafosol tetrasodium elicits total cholesterol release from rabbit meibomian gland cells via P2Y(2) purinergic receptor signalling,” (in eng), Sci Rep, vol. 11, no. 1, p. 6989, Mar 26 2021. [CrossRef]
- S. Fukuoka and R. Arita, “Increase in tear film lipid layer thickness after instillation of 3% diquafosol ophthalmic solution in healthy human eyes,” (in eng), Ocul Surf, vol. 15, no. 4, pp. 730-735, Oct 2017. [CrossRef]
- S. Fukuoka and R. Arita, “Tear film lipid layer increase after diquafosol instillation in dry eye patients with meibomian gland dysfunction: a randomized clinical study,” (in eng), Sci Rep, vol. 9, no. 1, p. 9091, Jun 24 2019. [CrossRef]
- T. Inatomi, S. Spurr-Michaud, A. S. Tisdale, Q. Zhan, S. T. Feldman, and I. K. Gipson, “Expression of secretory mucin genes by human conjunctival epithelia,” (in eng), Invest Ophthalmol Vis Sci, vol. 37, no. 8, pp. 1684-92, Jul 1996.
- I. K. Gipson, “Distribution of mucins at the ocular surface,” (in eng), Exp Eye Res, vol. 78, no. 3, pp. 379-88, Mar 2004. [CrossRef]
- F. Mantelli and P. Argüeso, “Functions of ocular surface mucins in health and disease,” (in eng), Curr Opin Allergy Clin Immunol, vol. 8, no. 5, pp. 477-83, Oct 2008. [CrossRef]
- Y. Jin, K. Y. Seo, and S. W. Kim, “Comparing two mucin secretagogues for the treatment of dry eye disease: a prospective randomized crossover trial,” Scientific Reports, vol. 14, no. 1, p. 13306, 2024/06/10 2024. [CrossRef]
- Y. Hori, T. Kageyama, A. Sakamoto, T. Shiba, M. Nakamura, and T. Maeno, “Comparison of Short-Term Effects of Diquafosol and Rebamipide on Mucin 5AC Level on the Rabbit Ocular Surface,” (in eng), J Ocul Pharmacol Ther, vol. 33, no. 6, pp. 493-497, Jul/Aug 2017. [CrossRef]
- K. Terakado et al., “Conjunctival expression of the P2Y2 receptor and the effects of 3% diquafosol ophthalmic solution in dogs,” (in eng), Vet J, vol. 202, no. 1, pp. 48-52, Oct 2014. [CrossRef]
- S. Liu, G. Yang, Q. Li, and S. Tang, “Safety and efficacy of topical diquafosol for the treatment of dry eye disease: An updated meta-analysis of randomized controlled trials,” (in eng), Indian J Ophthalmol, vol. 71, no. 4, pp. 1304-1315, Apr 2023. [CrossRef]
- Y. H. Kim et al., “Effect of Diquafosol on Hyperosmotic Stress-induced Tumor Necrosis Factor-α and Interleukin-6 Expression in Human Corneal Epithelial Cells,” (in eng), Korean J Ophthalmol, vol. 34, no. 1, pp. 1-10, Feb 2020. [CrossRef]
- G. T. Jung et al., “Proteomic analysis of tears in dry eye disease: A prospective, double-blind multicenter study,” (in eng), Ocul Surf, vol. 29, pp. 68-76, Jul 2023. [CrossRef]
- Y. Eom, J. S. Song, and H. M. Kim, “Effectiveness of Topical Cyclosporin A 0.1%, Diquafosol Tetrasodium 3%, and Their Combination, in Dry Eye Disease,” (in eng), J Ocul Pharmacol Ther, vol. 38, no. 10, pp. 682-694, Dec 2022. [CrossRef]
- S. Ozdemir, S. W. J. Yeo, J. J. Lee, A. Bhaskar, E. Finkelstein, and L. Tong, “Patient Medication Preferences for Managing Dry Eye Disease: The Importance of Medication Side Effects,” (in eng), Patient, vol. 15, no. 6, pp. 679-690, Nov 2022. [CrossRef]
- J. D. Sheppard and K. K. Nichols, “Dry Eye Disease Associated with Meibomian Gland Dysfunction: Focus on Tear Film Characteristics and the Therapeutic Landscape,” (in eng), Ophthalmol Ther, vol. 12, no. 3, pp. 1397-1418, Jun 2023. [CrossRef]
- R. Arita et al., “Topical diquafosol for patients with obstructive meibomian gland dysfunction,” (in eng), Br J Ophthalmol, vol. 97, no. 6, pp. 725-9, Jun 2013. [CrossRef]
- D. H. Kang et al., “Changes of tear film lipid layer thickness by 3% diquafosol ophthalmic solutions in patients with dry eye syndrome,” (in eng), Int J Ophthalmol, vol. 12, no. 10, pp. 1555-1560, 2019. [CrossRef]
- P. R. Donthineni, P. Kammari, S. S. Shanbhag, V. Singh, A. V. Das, and S. Basu, “Incidence, demographics, types and risk factors of dry eye disease in India: Electronic medical records driven big data analytics report I,” (in eng), Ocul Surf, vol. 17, no. 2, pp. 250-256, Apr 2019. [CrossRef]
- P. R. Donthineni et al., “Aqueous-deficient dry eye disease: Preferred practice pattern guidelines on clinical approach, diagnosis, and management,” (in eng), Indian J Ophthalmol, vol. 71, no. 4, pp. 1332-1347, Apr 2023. [CrossRef]
- S. Koh, C. Ikeda, Y. Takai, H. Watanabe, N. Maeda, and K. Nishida, “Long-term results of treatment with diquafosol ophthalmic solution for aqueous-deficient dry eye,” (in eng), Jpn J Ophthalmol, vol. 57, no. 5, pp. 440-6, Sep 2013. [CrossRef]
- S. Koh et al., “Effect of diquafosol ophthalmic solution on the optical quality of the eyes in patients with aqueous-deficient dry eye,” (in eng), Acta Ophthalmol, vol. 92, no. 8, pp. e671-5, Dec 2014. [CrossRef]
- N. Yokoi, Y. Sonomura, H. Kato, A. Komuro, and S. Kinoshita, “Three percent diquafosol ophthalmic solution as an additional therapy to existing artificial tears with steroids for dry-eye patients with Sjögren’s syndrome,” (in eng), Eye (Lond), vol. 29, no. 9, pp. 1204-12, Sep 2015. [CrossRef]
- F. Malard, E. Holler, B. M. Sandmaier, H. Huang, and M. Mohty, “Acute graft-versus-host disease,” (in eng), Nat Rev Dis Primers, vol. 9, no. 1, p. 27, Jun 8 2023. [CrossRef]
- Y. Sakoda et al., “Donor-derived thymic-dependent T cells cause chronic graft-versus-host disease,” (in eng), Blood, vol. 109, no. 4, pp. 1756-64, Feb 15 2007. [CrossRef]
- P. L. Surico and Z. K. Luo, “Understanding Ocular Graft-versus-Host Disease to Facilitate an Integrated Multidisciplinary Approach,” (in eng), Transplant Cell Ther, vol. 30, no. 9s, pp. S570-s584, Sep 2024. [CrossRef]
- F. Yang et al., “Eyelid blood vessel and meibomian gland changes in a sclerodermatous chronic GVHD mouse model,” (in eng), Ocul Surf, vol. 26, pp. 328-341, Oct 2022. [CrossRef]
- V. L. Perez et al., “Meibomian Gland Dysfunction: A Route of Ocular Graft-Versus-Host Disease Progression That Drives a Vicious Cycle of Ocular Surface Inflammatory Damage,” (in eng), Am J Ophthalmol, vol. 247, pp. 42-60, Mar 2023. [CrossRef]
- Y. Ogawa, S. Shimmura, T. Kawakita, S. Yoshida, Y. Kawakami, and K. Tsubota, “Epithelial mesenchymal transition in human ocular chronic graft-versus-host disease,” (in eng), Am J Pathol, vol. 175, no. 6, pp. 2372-81, Dec 2009. [CrossRef]
- K. Shamloo, A. Barbarino, S. Alfuraih, and A. Sharma, “Graft Versus Host Disease-Associated Dry Eye: Role of Ocular Surface Mucins and the Effect of Rebamipide, a Mucin Secretagogue,” (in eng), Invest Ophthalmol Vis Sci, vol. 60, no. 14, pp. 4511-4519, Nov 1 2019. [CrossRef]
- M. Yamane et al., “Long-Term Topical Diquafosol Tetrasodium Treatment of Dry Eye Disease Caused by Chronic Graft-Versus-Host Disease: A Retrospective Study,” (in eng), Eye Contact Lens, vol. 44 Suppl 2, pp. S215-s220, Nov 2018. [CrossRef]
- M. Yamane et al., “Long-term rebamipide and diquafosol in two cases of immune-mediated dry eye,” (in eng), Optom Vis Sci, vol. 92, no. 4 Suppl 1, pp. S25-32, Apr 2015. [CrossRef]
- M. Kolko et al., “Impact of glaucoma medications on the ocular surface and how ocular surface disease can influence glaucoma treatment,” (in eng), Ocul Surf, vol. 29, pp. 456-468, Jul 2023. [CrossRef]
- X. Zhang, S. Vadoothker, W. M. Munir, and O. Saeedi, “Ocular Surface Disease and Glaucoma Medications: A Clinical Approach,” (in eng), Eye Contact Lens, vol. 45, no. 1, pp. 11-18, Jan 2019. [CrossRef]
- R. L. Coakes, I. A. Mackie, and D. V. Seal, “Effects of long-term treatment with timolol on lacrimal gland function,” (in eng), Br J Ophthalmol, vol. 65, no. 9, pp. 603-5, Sep 1981. [CrossRef]
- E. V. Kuppens, C. A. de Jong, T. R. Stolwijk, R. J. de Keizer, and J. A. van Best, “Effect of timolol with and without preservative on the basal tear turnover in glaucoma,” (in eng), Br J Ophthalmol, vol. 79, no. 4, pp. 339-42, Apr 1995. [CrossRef]
- Y. Zhang, W. R. Kam, Y. Liu, X. Chen, and D. A. Sullivan, “Influence of Pilocarpine and Timolol on Human Meibomian Gland Epithelial Cells,” (in eng), Cornea, vol. 36, no. 6, pp. 719-724, Jun 2017. [CrossRef]
- S. Aydin Kurna, S. Acikgoz, A. Altun, N. Ozbay, T. Sengor, and O. O. Olcaysu, “The effects of topical antiglaucoma drugs as monotherapy on the ocular surface: a prospective study,” (in eng), J Ophthalmol, vol. 2014, p. 460483, 2014. [CrossRef]
- L. M. Nijm, L. De Benito-Llopis, G. C. Rossi, T. S. Vajaranant, and M. T. Coroneo, “Understanding the Dual Dilemma of Dry Eye and Glaucoma: An International Review,” (in eng), Asia Pac J Ophthalmol (Phila), vol. 9, no. 6, pp. 481-490, Dec 2020. [CrossRef]
- M. C. Mocan, E. Uzunosmanoglu, S. Kocabeyoglu, J. Karakaya, and M. Irkec, “The Association of Chronic Topical Prostaglandin Analog Use With Meibomian Gland Dysfunction,” (in eng), J Glaucoma, vol. 25, no. 9, pp. 770-4, Sep 2016. [CrossRef]
- M. P. Rabinowitz et al., “Unilateral Prostaglandin-Associated Periorbitopathy: A Syndrome Involving Upper Eyelid Retraction Distinguishable From the Aging Sunken Eyelid,” (in eng), Ophthalmic Plast Reconstr Surg, vol. 31, no. 5, pp. 373-8, Sep-Oct 2015. [CrossRef]
- M. A. Vitoux et al., “Benzalkonium chloride-induced direct and indirect toxicity on corneal epithelial and trigeminal neuronal cells: proinflammatory and apoptotic responses in vitro,” (in eng), Toxicol Lett, vol. 319, pp. 74-84, Feb 1 2020. [CrossRef]
- E. Ivakhnitskaia et al., “Benzalkonium chloride, a common ophthalmic preservative, compromises rat corneal cold sensitive nerve activity,” (in eng), Ocul Surf, vol. 26, pp. 88-96, Oct 2022. [CrossRef]
- C. Van Went et al., “[Corneal sensitivity in patients treated medically for glaucoma or ocular hypertension],” (in fre), J Fr Ophtalmol, vol. 34, no. 10, pp. 684-90, Dec 2011. [CrossRef]
- G. Martone et al., “An in vivo confocal microscopy analysis of effects of topical antiglaucoma therapy with preservative on corneal innervation and morphology,” (in eng), Am J Ophthalmol, vol. 147, no. 4, pp. 725-735.e1, Apr 2009. [CrossRef]
- D. A. Ammar, R. J. Noecker, and M. Y. Kahook, “Effects of benzalkonium chloride-preserved, polyquad-preserved, and sofZia-preserved topical glaucoma medications on human ocular epithelial cells,” (in eng), Adv Ther, vol. 27, no. 11, pp. 837-45, Nov 2010. [CrossRef]
- H. Liang, F. Brignole-Baudouin, L. Riancho, and C. Baudouin, “Reduced in vivo ocular surface toxicity with polyquad-preserved travoprost versus benzalkonium-preserved travoprost or latanoprost ophthalmic solutions,” (in eng), Ophthalmic Res, vol. 48, no. 2, pp. 89-101, 2012. [CrossRef]
- M. Y. Kahook, C. J. Rapuano, E. M. Messmer, N. M. Radcliffe, A. Galor, and C. Baudouin, “Preservatives and ocular surface disease: A review,” (in eng), Ocul Surf, vol. 34, pp. 213-224, Aug 3 2024. [CrossRef]
- J. M. Herreras, J. C. Pastor, M. Calonge, and V. M. Asensio, “Ocular surface alteration after long-term treatment with an antiglaucomatous drug,” (in eng), Ophthalmology, vol. 99, no. 7, pp. 1082-8, Jul 1992. [CrossRef]
- S. H. Chung et al., “Impact of short-term exposure of commercial eyedrops preserved with benzalkonium chloride on precorneal mucin,” (in eng), Mol Vis, vol. 12, pp. 415-21, Apr 26 2006.
- J. M. Martinez-de-la-Casa et al., “Tear cytokine profile of glaucoma patients treated with preservative-free or preserved latanoprost,” (in eng), Ocul Surf, vol. 15, no. 4, pp. 723-729, Oct 2017. [CrossRef]
- C. Boimer and C. M. Birt, “Preservative exposure and surgical outcomes in glaucoma patients: The PESO study,” (in eng), J Glaucoma, vol. 22, no. 9, pp. 730-5, Dec 2013. [CrossRef]
- M. Tomić, S. Kaštelan, K. M. Soldo, and J. Salopek-Rabatić, “Influence of BAK-preserved prostaglandin analog treatment on the ocular surface health in patients with newly diagnosed primary open-angle glaucoma,” (in eng), Biomed Res Int, vol. 2013, p. 603782, 2013. [CrossRef]
- C. Huang et al., “Benzalkonium chloride induces subconjunctival fibrosis through the COX-2-modulated activation of a TGF-β1/Smad3 signaling pathway,” (in eng), Invest Ophthalmol Vis Sci, vol. 55, no. 12, pp. 8111-22, Nov 18 2014. [CrossRef]
- D. C. Broadway, I. Grierson, C. O’Brien, and R. A. Hitchings, “Adverse effects of topical antiglaucoma medication. II. The outcome of filtration surgery,” (in eng), Arch Ophthalmol, vol. 112, no. 11, pp. 1446-54, Nov 1994. [CrossRef]
- R. Merani et al., “Aqueous Chlorhexidine for Intravitreal Injection Antisepsis: A Case Series and Review of the Literature,” (in eng), Ophthalmology, vol. 123, no. 12, pp. 2588-2594, Dec 2016. [CrossRef]
- N. E. Epstein, “Review: Perspective on ocular toxicity of presurgical skin preparations utilizing Chlorhexidine Gluconate/Hibiclens/Chloraprep,” (in eng), Surg Neurol Int, vol. 12, p. 335, 2021. [CrossRef]
- K. Green, V. Livingston, K. Bowman, and D. S. Hull, “Chlorhexidine Effects on Corneal Epithelium and Endothelium,” Archives of Ophthalmology, vol. 98, no. 7, pp. 1273-1278, 1980. [CrossRef]
- M. B. Hamill, M. S. Osato, and K. R. Wilhelmus, “Experimental evaluation of chlorhexidine gluconate for ocular antisepsis,” (in eng), Antimicrob Agents Chemother, vol. 26, no. 6, pp. 793-6, Dec 1984. [CrossRef]
- S. W. Jin and J. S. Min, “Clinical evaluation of the effect of diquafosol ophthalmic solution in glaucoma patients with dry eye syndrome,” (in eng), Jpn J Ophthalmol, vol. 60, no. 3, pp. 150-5, May 2016. [CrossRef]
- Y. Guo, J. Y. Ha, H. L. Piao, M. S. Sung, and S. W. Park, “The protective effect of 3% diquafosol on meibomian gland morphology in glaucoma patients treated with prostaglandin analogs: a 12-month follow-up study,” (in eng), BMC Ophthalmol, vol. 20, no. 1, p. 277, Jul 10 2020. [CrossRef]
- Q. Liu et al., “Evaluation of effects of 3% diquafosol ophthalmic solution on preocular tear film stability after trabeculectomy,” (in eng), Int Ophthalmol, vol. 43, no. 6, pp. 1903-1910, Jun 2023. [CrossRef]
- S. Dasgupta, “The course of dry eye following phacoemulsification and manual - SICS: a prospective study based on Indian scenario,” International eye science, vol. 16, pp. 1789-1794, 07/12 2016. [CrossRef]
- K. Miyake and N. Yokoi, “Influence on ocular surface after cataract surgery and effect of topical diquafosol on postoperative dry eye: a multicenter prospective randomized study,” (in eng), Clin Ophthalmol, vol. 11, pp. 529-540, 2017. [CrossRef]
- K. Kato et al., “Conjunctival Goblet Cell Density Following Cataract Surgery With Diclofenac Versus Diclofenac and Rebamipide: A Randomized Trial,” (in eng), Am J Ophthalmol, vol. 181, pp. 26-36, Sep 2017. [CrossRef]
- T. Oh, Y. Jung, D. Chang, J. Kim, and H. Kim, “Changes in the tear film and ocular surface after cataract surgery,” (in eng), Jpn J Ophthalmol, vol. 56, no. 2, pp. 113-8, Mar 2012. [CrossRef]
- R. Yanai et al., “Evaluation of povidone-iodine as a disinfectant solution for contact lenses: antimicrobial activity and cytotoxicity for corneal epithelial cells,” (in eng), Cont Lens Anterior Eye, vol. 29, no. 2, pp. 85-91, May 2006. [CrossRef]
- S. P. Epstein, M. Ahdoot, E. Marcus, and P. A. Asbell, “Comparative toxicity of preservatives on immortalized corneal and conjunctival epithelial cells,” (in eng), J Ocul Pharmacol Ther, vol. 25, no. 2, pp. 113-9, Apr 2009. [CrossRef]
- H. B. Hwang and H. S. Kim, “Phototoxic effects of an operating microscope on the ocular surface and tear film,” (in eng), Cornea, vol. 33, no. 1, pp. 82-90, Jan 2014. [CrossRef]
- T. Ipek, M. P. Hanga, A. Hartwig, J. Wolffsohn, and C. O’Donnell, “Dry eye following cataract surgery: The effect of light exposure using an in-vitro model,” (in eng), Cont Lens Anterior Eye, vol. 41, no. 1, pp. 128-131, Feb 2018. [CrossRef]
- K. E. Han et al., “Evaluation of dry eye and meibomian gland dysfunction after cataract surgery,” (in eng), Am J Ophthalmol, vol. 157, no. 6, pp. 1144-1150.e1, Jun 2014. [CrossRef]
- J. Ram, A. Gupta, G. Brar, S. Kaushik, and A. Gupta, “Outcomes of phacoemulsification in patients with dry eye,” (in eng), J Cataract Refract Surg, vol. 28, no. 8, pp. 1386-9, Aug 2002. [CrossRef]
- D. H. Park, J. K. Chung, D. R. Seo, and S. J. Lee, “Clinical Effects and Safety of 3% Diquafosol Ophthalmic Solution for Patients With Dry Eye After Cataract Surgery: A Randomized Controlled Trial,” (in eng), Am J Ophthalmol, vol. 163, pp. 122-131.e2, Mar 2016. [CrossRef]
- P. Kim, S. Plugfelder, and A. R. Slomovic, “Top 5 pearls to consider when implanting advanced-technology IOLs in patients with ocular surface disease,” (in eng), Int Ophthalmol Clin, vol. 52, no. 2, pp. 51-8, Spring 2012. [CrossRef]
- W. B. Trattler, P. A. Majmudar, E. D. Donnenfeld, M. B. McDonald, K. G. Stonecipher, and D. F. Goldberg, “The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye,” (in eng), Clin Ophthalmol, vol. 11, pp. 1423-1430, 2017. [CrossRef]
- A. T. Epitropoulos, C. Matossian, G. J. Berdy, R. P. Malhotra, and R. Potvin, “Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning,” (in eng), J Cataract Refract Surg, vol. 41, no. 8, pp. 1672-7, Aug 2015. [CrossRef]
- T. Teshigawara et al., “Effect of Long-Acting Diquafosol Sodium on Astigmatism Measurement Repeatability in Preoperative Cataract Cases with Dry Eyes: A Multicenter Prospective Study,” (in eng), Ophthalmol Ther, vol. 13, no. 6, pp. 1743-1755, Jun 2024. [CrossRef]
- H. Kobashi, K. Kamiya, A. Igarashi, T. Miyake, and K. Shimizu, “Intraocular Scattering after Instillation of Diquafosol Ophthalmic Solution,” (in eng), Optom Vis Sci, vol. 92, no. 9, pp. e303-9, Sep 2015. [CrossRef]
- T. Kojima, “Contact Lens-Associated Dry Eye Disease: Recent Advances Worldwide and in Japan,” (in eng), Invest Ophthalmol Vis Sci, vol. 59, no. 14, pp. Des102-des108, Nov 1 2018. [CrossRef]
- R. Arita, K. Itoh, K. Inoue, A. Kuchiba, T. Yamaguchi, and S. Amano, “Contact lens wear is associated with decrease of meibomian glands,” (in eng), Ophthalmology, vol. 116, no. 3, pp. 379-84, Mar 2009. [CrossRef]
- Y. Nagahara et al., “Diquafosol Ophthalmic Solution Increases Pre- and Postlens Tear Film During Contact Lens Wear in Rabbit Eyes,” (in eng), Eye Contact Lens, vol. 43, no. 6, pp. 378-382, Nov 2017. [CrossRef]
- C. Shigeyasu, M. Yamada, Y. Akune, and M. Fukui, “Diquafosol for Soft Contact Lens Dryness: Clinical Evaluation and Tear Analysis,” (in eng), Optom Vis Sci, vol. 93, no. 8, pp. 973-8, Aug 2016. [CrossRef]
- T. Ogami, H. Asano, T. Hiraoka, Y. Yamada, and T. Oshika, “The Effect of Diquafosol Ophthalmic Solution on Clinical Parameters and Visual Function in Soft Contact Lens-Related Dry Eye,” (in eng), Adv Ther, vol. 38, no. 11, pp. 5534-5547, Nov 2021. [CrossRef]
- B. Yang, X. Ma, L. Liu, and P. Cho, “Vision-related quality of life of Chinese children undergoing orthokeratology treatment compared to single vision spectacles,” (in eng), Cont Lens Anterior Eye, vol. 44, no. 4, p. 101350, Aug 2021. [CrossRef]
- M. D. P. Willcox et al., “TFOS DEWS II Tear Film Report,” (in eng), Ocul Surf, vol. 15, no. 3, pp. 366-403, Jul 2017. [CrossRef]
- C. Xie and R. Wei, “Long-term changes in the ocular surface during orthokeratology lens wear and their correlations with ocular discomfort symptoms,” (in eng), Cont Lens Anterior Eye, vol. 46, no. 1, p. 101757, Feb 2023. [CrossRef]
- C. X. Miao, X. Y. Xu, and H. Zhang, “[Analysis of corneal complications in children wearing orthokeratology lenses at night],” (in chi), Zhonghua Yan Ke Za Zhi, vol. 53, no. 3, pp. 198-202, Mar 11 2017. [CrossRef]
- Y. Yang et al., “Short-term application of diquafosol ophthalmic solution benefits children with dry eye wearing orthokeratology lens,” (in eng), Front Med (Lausanne), vol. 10, p. 1130117, 2023. [CrossRef]
- C. S. De Paiva et al., “The incidence and risk factors for developing dry eye after myopic LASIK,” (in eng), Am J Ophthalmol, vol. 141, no. 3, pp. 438-45, Mar 2006. [CrossRef]
- S. Nair, M. Kaur, N. Sharma, and J. S. Titiyal, “Refractive surgery and dry eye - An update,” (in eng), Indian J Ophthalmol, vol. 71, no. 4, pp. 1105-1114, Apr 2023. [CrossRef]
- Y. C. Liu et al., “Comparison of tear proteomic and neuromediator profiles changes between small incision lenticule extraction (SMILE) and femtosecond laser-assisted in-situ keratomileusis (LASIK),” (in eng), J Adv Res, vol. 29, pp. 67-81, Mar 2021. [CrossRef]
- K. Konomi et al., “Preoperative characteristics and a potential mechanism of chronic dry eye after LASIK,” (in eng), Invest Ophthalmol Vis Sci, vol. 49, no. 1, pp. 168-74, Jan 2008. [CrossRef]
- E. Cohen and O. Spierer, “Dry Eye Post-Laser-Assisted In Situ Keratomileusis: Major Review and Latest Updates,” (in eng), J Ophthalmol, vol. 2018, p. 4903831, 2018. [CrossRef]
- J. W. Jung, J. Y. Kim, H. S. Chin, Y. J. Suh, T. I. Kim, and K. Y. Seo, “Assessment of meibomian glands and tear film in post-refractive surgery patients,” (in eng), Clin Exp Ophthalmol, vol. 45, no. 9, pp. 857-866, Dec 2017. [CrossRef]
- Y. Liu et al., “Combination Therapy With Diquafosol Sodium and Sodium Hyaluronate in Eyes With Dry Eye Disease After Small Incision Lenticule Extraction,” (in eng), In Vivo, vol. 37, no. 6, pp. 2829-2834, Nov-Dec 2023. [CrossRef]
- Y. Mori et al., “Effect of diquafosol tetrasodium eye drop for persistent dry eye after laser in situ keratomileusis,” (in eng), Cornea, vol. 33, no. 7, pp. 659-62, Jul 2014. [CrossRef]
- T. Wang, Y. Di, and Y. Li, “Combination therapy with 3% diquafosol tetrasodium ophthalmic solution and sodium hyaluronate: an effective therapy for patients with dry eye after femtosecond laser-assisted in situ keratomileusis,” (in eng), Front Med (Lausanne), vol. 10, p. 1160499, 2023. [CrossRef]
- Y. Matsumoto, O. M. A. Ibrahim, T. Kojima, M. Dogru, J. Shimazaki, and K. Tsubota, “Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome,” (in eng), Diagnostics (Basel), vol. 10, no. 7, Jul 20 2020. [CrossRef]
- M. Uchino, N. Yokoi, J. Shimazaki, Y. Hori, K. Tsubota, and S. On Behalf Of The Japan Dry Eye, “Adherence to Eye Drops Usage in Dry Eye Patients and Reasons for Non-Compliance: A Web-Based Survey,” (in eng), J Clin Med, vol. 11, no. 2, Jan 12 2022. [CrossRef]
- R. Arita, S. Fukuoka, and M. Kaido, “Tolerability of Diquas LX on tear film and meibomian glands findings in a real clinical scenario,” (in eng), PLoS One, vol. 19, no. 9, p. e0305020, 2024. [CrossRef]
- Y. Hori, K. Oka, and M. Inai, “Efficacy and Safety of the Long-Acting Diquafosol Ophthalmic Solution DE-089C in Patients with Dry Eye: A Randomized, Double-Masked, Placebo-Controlled Phase 3 Study,” (in eng), Adv Ther, vol. 39, no. 8, pp. 3654-3667, Aug 2022. [CrossRef]
- S. Ishikawa, T. Sasaki, T. Maruyama, K. Murayama, and K. Shinoda, “Effectiveness and Adherence of Dry Eye Patients Who Switched from Short- to Long-Acting Diquafosol Ophthalmic Solution,” (in eng), J Clin Med, vol. 12, no. 13, Jul 5 2023. [CrossRef]
- C. H. Y. Teo, H. S. Ong, Y. C. Liu, and L. Tong, “Meibomian gland dysfunction is the primary determinant of dry eye symptoms: Analysis of 2346 patients,” (in eng), Ocul Surf, vol. 18, no. 4, pp. 604-612, Oct 2020. [CrossRef]
- B. Yang et al., “Quantitative evaluation of lipid layer thickness and blinking in children with allergic conjunctivitis,” (in eng), Graefes Arch Clin Exp Ophthalmol, vol. 259, no. 9, pp. 2795-2805, Sep 2021. [CrossRef]
Figure 1.
Mechanism of action of diquafosol.
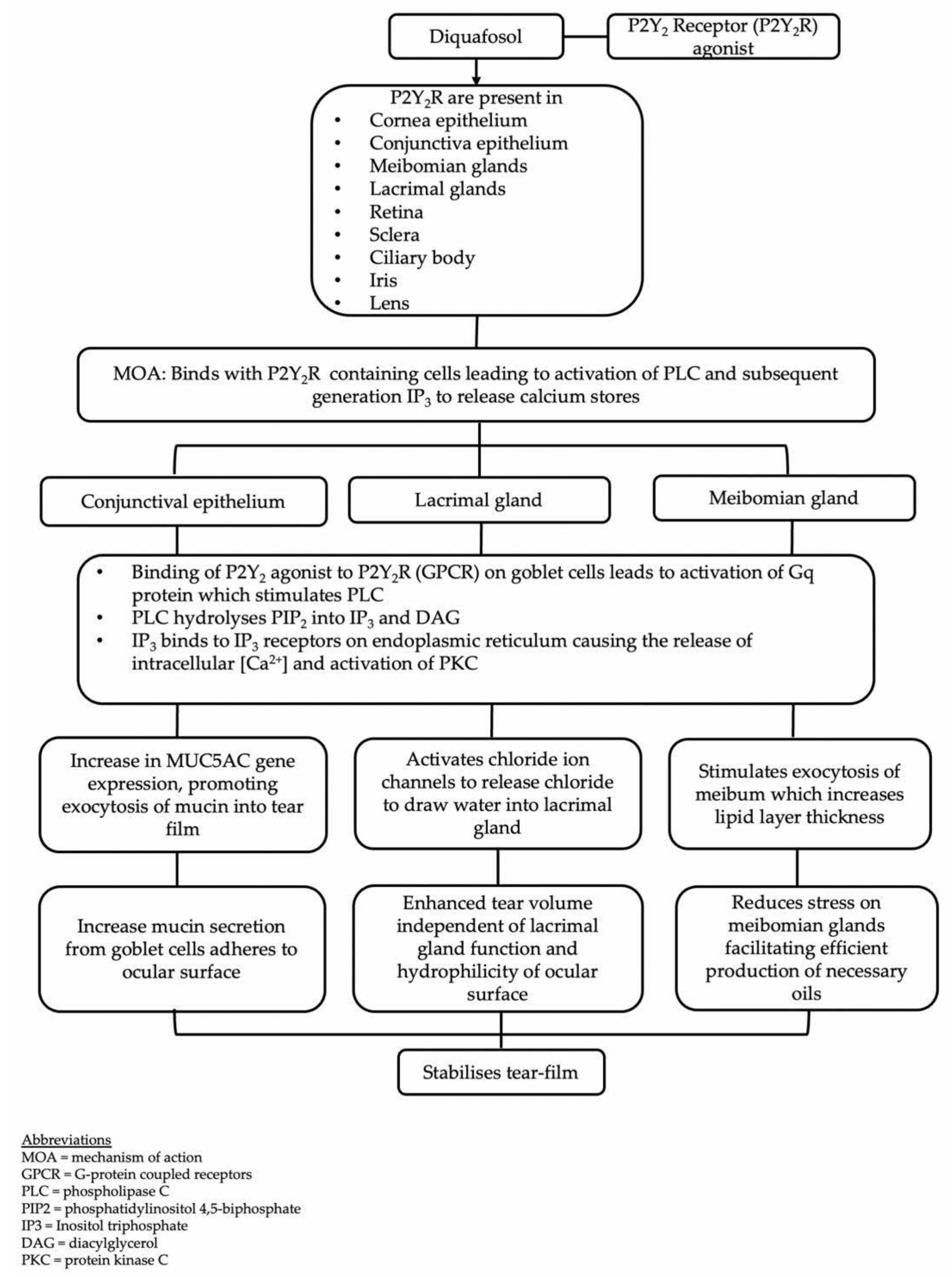

Table 1.
Composition of Diquas® and Diquas®-S.
| Diquas® | Diquas®-S |
|---|---|
| Chlorhexidine gluconate (preservative) Dibasic sodium phosphate hydrate Disodium edetate hydrate Sodium chloride Potassium chloride Sodium hydroxide Dilute hydrochloric acid |
Dibasic sodium phosphate hydrate Disodium edetate hydrate Sodium chloride Potassium chloride Hydrochloric acid Sodium hydroxide |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



