Submitted:
01 February 2025
Posted:
03 February 2025
You are already at the latest version
Abstract
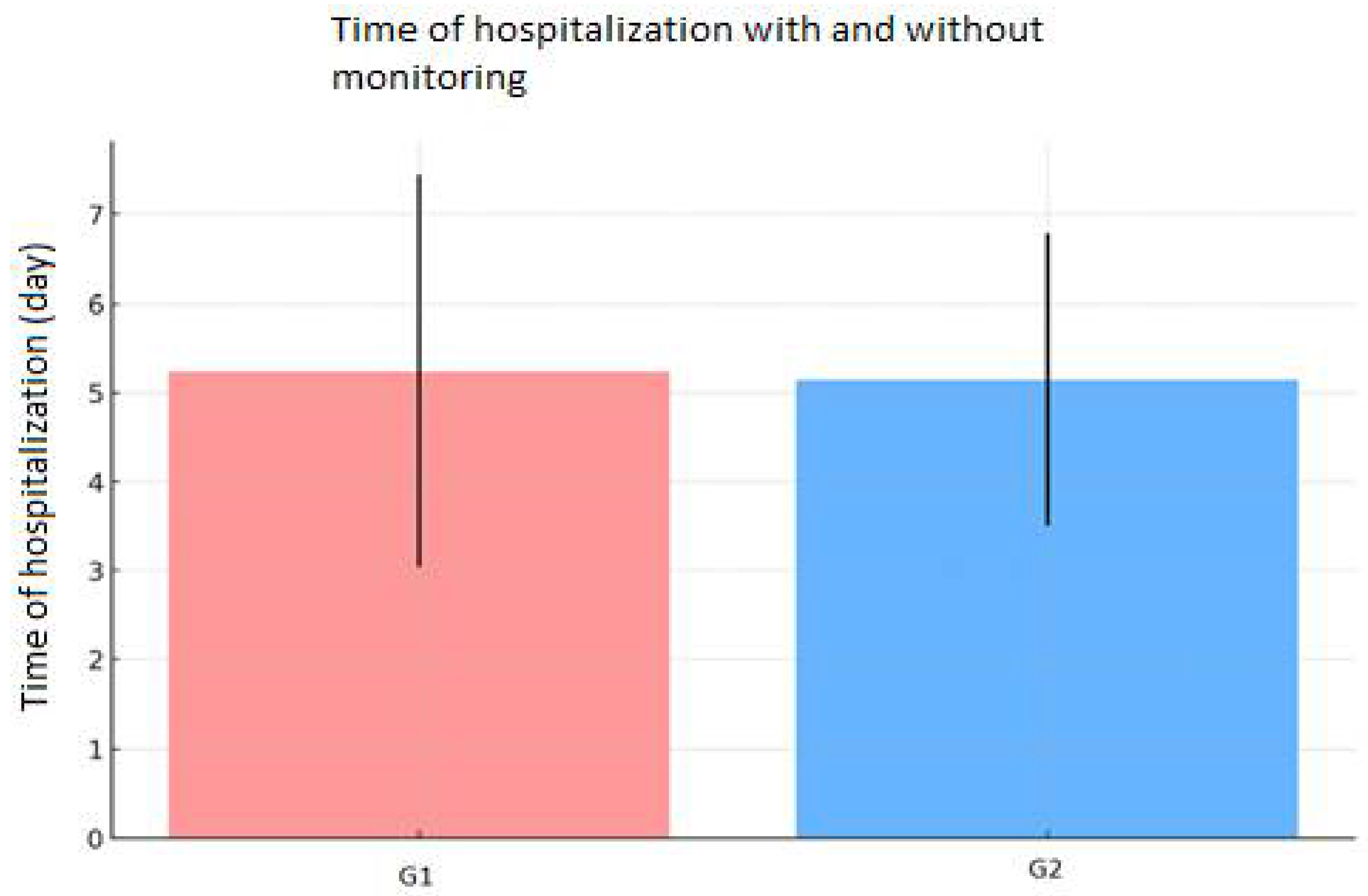
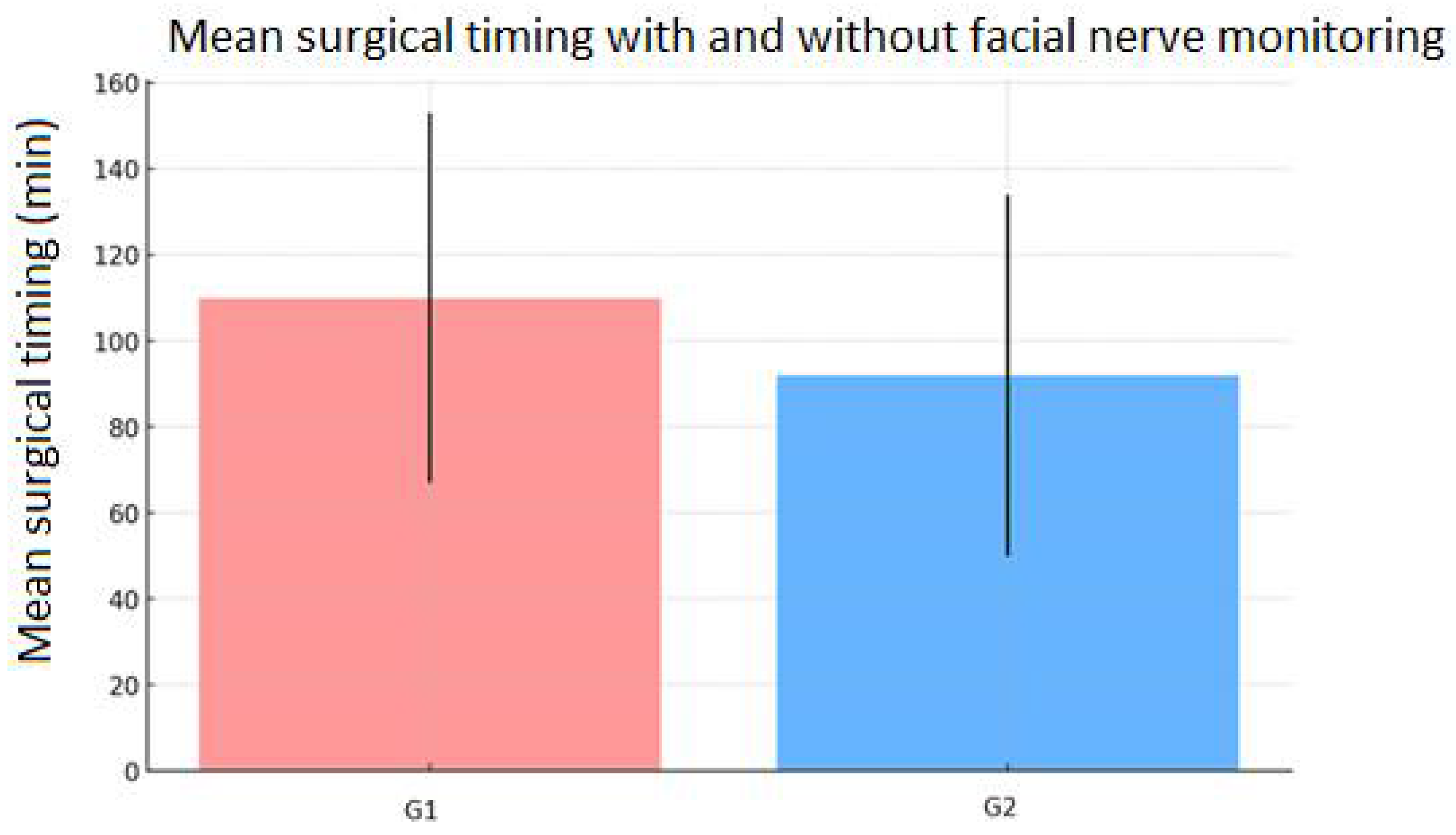
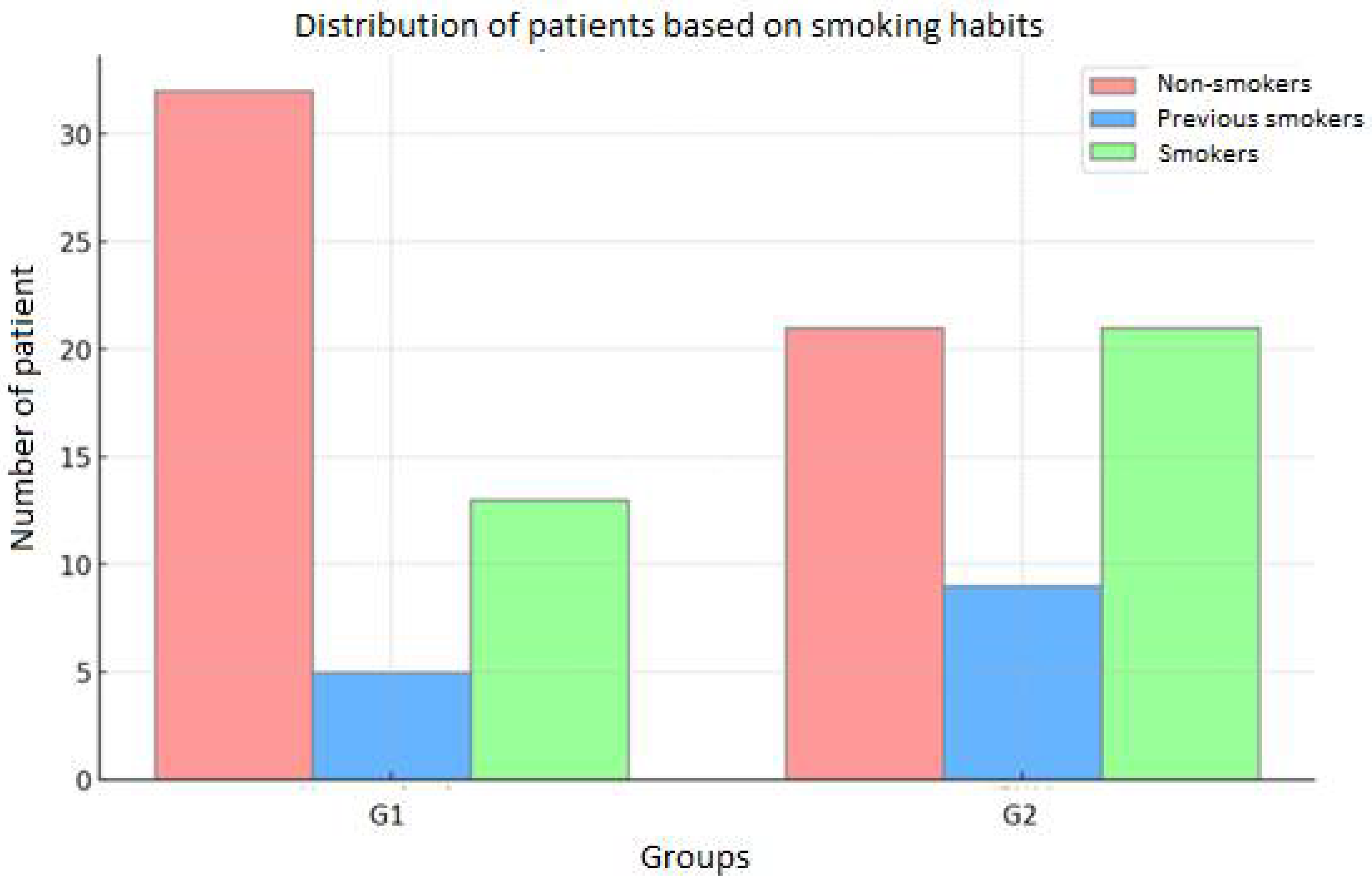
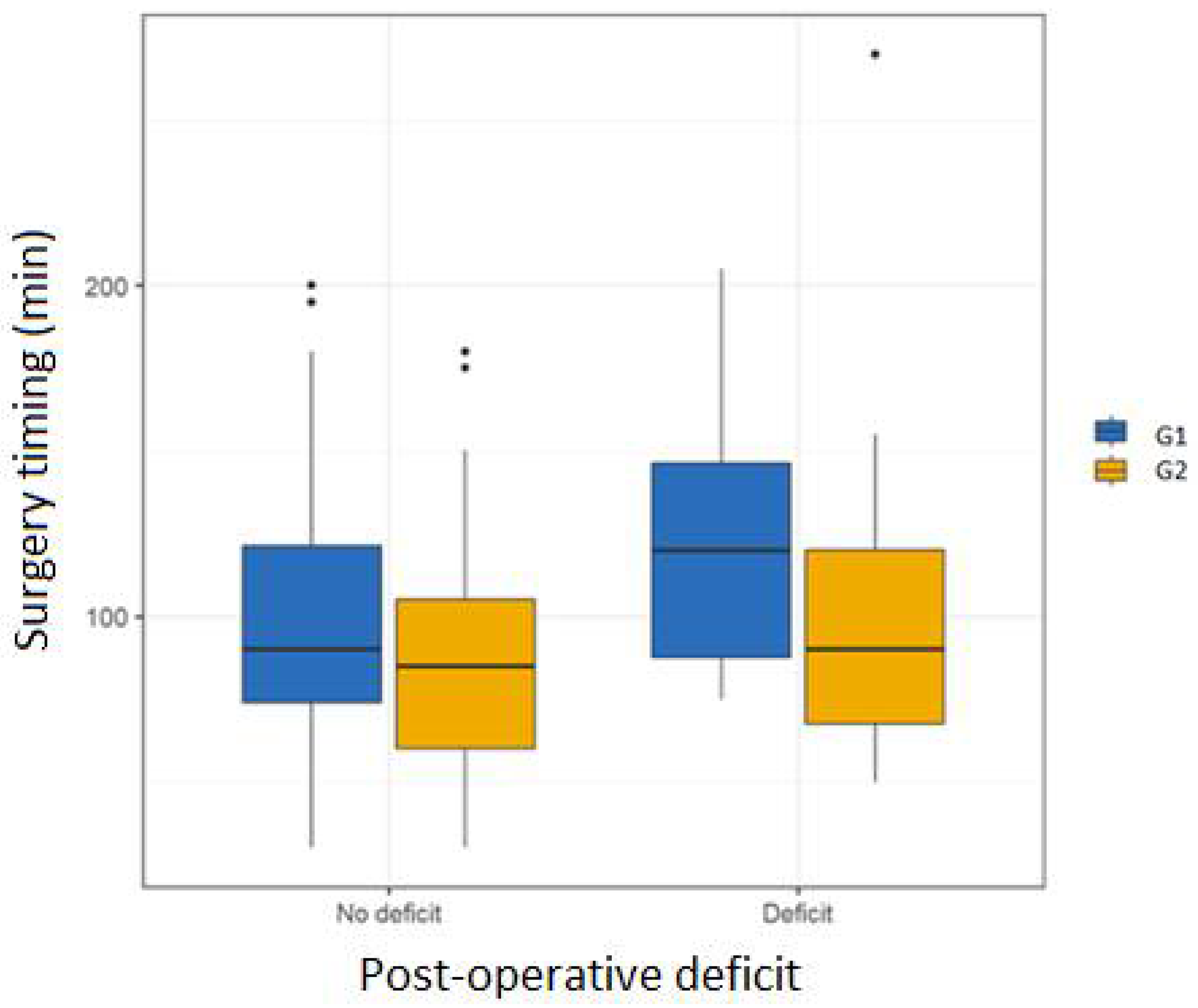
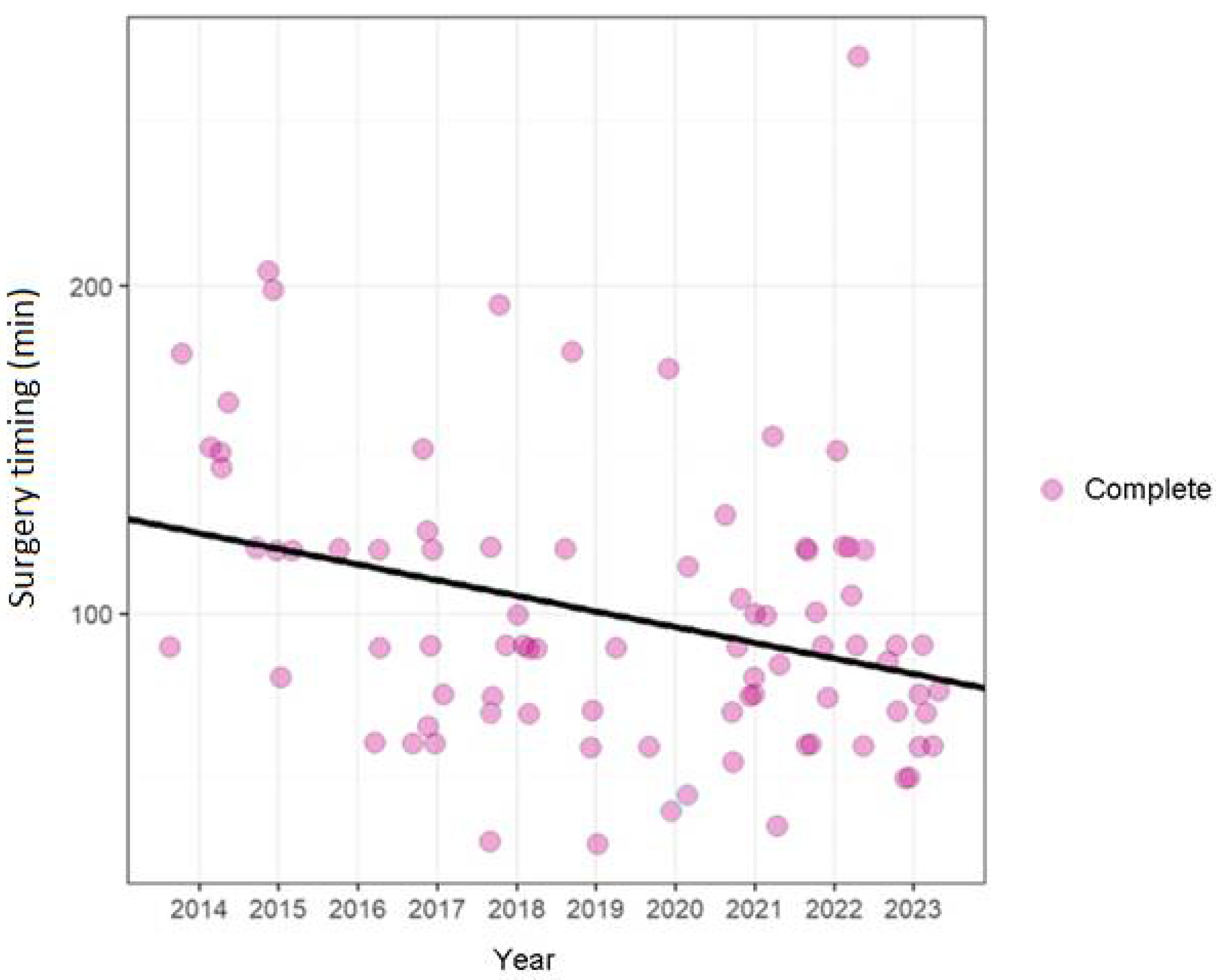
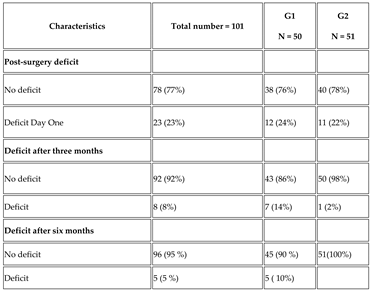
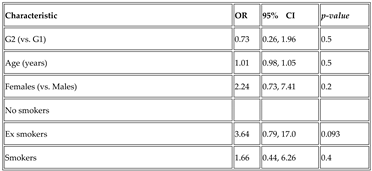
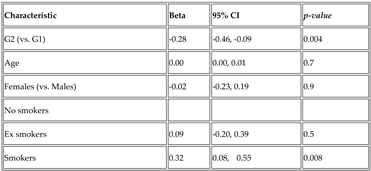
Background: The use of intraoperative facial nerve monitoring (IFNM) is becoming more and more frequent, an established intraoperative aid in parotid gland surgery. To date, there are no scientific studies in the literature on the post-operative outcomes of submandibular gland surgery, in particular on post-operative injury of the marginalis mandibulae branch (MMB) that represents the most frequent and feared complication of this surgery, with an incidence of 1-7% of cases. Objective: In this retrospective study, the authors evaluated the incidence of postoperative paralysis of the MMB of the facial nerve (FN )in patients undergoing submandibular sialodenectomy for benign diseases, such as benign tumors and sialolithiasis, from 2014 to 2023, with particular attention to the role of IFNM in this context. Materials and Methods: The retrospective study was conducted at the Maxillo-Facial Department of Magna Graecia University of Catanzaro. The patients were divided into two groups: Group 1 (G1) consisted of subjects who underwent surgery without the use of IFNM and identification and clamping of facial vessels (1 January 2014 to 31 Dicember 2018); Group 2 (G2), consisted of subjects who underwent surgery with IFNM and without identification and clamping of facial vessels (1 January 2019 al 31 Dicember 2023). In G2 employed the Nerve Integrity Monitor (NIMR di Medtronic) and to classify the FN function we used the modified House-Brackmann classification. A descriptive analysis was performed, and univariate and multivariate logistic regression were used to examine the impact of IFNM on surgical timing and the association between deficit of G2 (vs. G1) adjusted for age, sex, smoking status for age, sex, smoking status. The level of statistical significance was set at p value<0.05. Results: A total of 101 patients were included in the study: 50 subjects were assigned to G1 (49.5%, comprising 24 female and 26 male, and 51 subjects were assigned to G2 (50.5%), comprising 21 men and 30 women, the mean age was 55 ± 16 years in the entire patient cohort. In 77% of the cases (n. 78, precisely 38 in G1 and 40 in G2), no facial nerve injury occurred. In 23% of the cases (n. 23, specifically 12 in G1 and 11 in G2), postoperative paralysis of MMB was observed. Of these subjects, nobody had permanent paralysis but only transient dysfuction (of the 12 patients of G1 four demonstrated grade I dysfunction while eight exhibited grade II dysfunction, of the 11 subjects of G2, eight exhibited grade I dysfunction, while three demonstrated grade II dysfunction). After six months the dysfuction of grade II persisted only in five patients of G1. The results of univariate and multivariable linear regression demonstrated that the surgical timing was found to be 99 ± 44 minutes considering the entire cohort of patients, 110 ± 43 minutes for G1 and 92 ± 42 minutes for G2 (Beta = -19, 95% CI -37 to -0.16 and p = 0.048). A longer surgical timing was observed compared to non-smokers (always statistically significant with a p-value of 0.008), suggesting that smoking status may influence the duration of the intervention (Beta = -0,32, 95% CI -0,08 to -0.55 and p = 0.008). Discussion and Conclusions: MMB paralysis represents one of the most frequent complications that can occur also in submandibular gland surgery and IFNM offers to the surgeon a valuable support in identifying the MMB in submandibular sialadenectomy. The use of IFNM can be a valid aid, but its effectiveness always depends on the competence but its effectiveness always depends on the competence of the surgeon.
Keywords:
Introduction
2. Materials and Methods
2.1. Surgical Technique
Statistical Analysis
Results
Discussion
Conclusion
References
- Tirelli G.; Bergamini PR.; Scardoni A., Gatto A., Boscolo Nata F. and Marcuzzo AV., Intraoperative monitoring of marginal mandibular nerve during neck dissection. Head & neck, 2018. May;40(5):1016-1023. Epub 2018 Feb 1. [CrossRef]
- Savvas, E.; Hillmann, S.; Weiss, D.; Koopmann, M.; Rudack, C.; Alberty, J. Association Between Facial Nerve MonitoringWith Postoperative Facial Paralysis in Parotidectomy. JAMA Otolaryngol.–Head Neck Surg. 2016, 142, 828. [Google Scholar] [CrossRef] [PubMed]
- Cristofaro M.G., Colangeli W, Ferragina F, Tarallo G, Sottile AR, Ioppolo MG, Arrotta A, Barca I. Facial Nerve Injury after Extracapsular Dissection for Benign Parotid Tumors with and without Intraoperative Monitoring: A Retrospective Study of a Single Center. Diagnostics (Basel). 2024 Sep 12;14(18):2017. [CrossRef]
- Turhal, G.; Hepkarsi, S.; Ozturk, K. The potential applicability of facial nerve monitoring as a navigation tool in parotid gland surgery. Braz. J. Otorhinolaryngol. 2023, 89, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Duque, C.S.; Londoño, A.F.; Duque, A.M.; Zuleta, J.J.; Marulanda, M.; Otálvaro, L.M.; Agudelo, M.; Dueñas, J.P.; Palacio, M.F.; Dionigi, G. Facial nerve monitoring in parotid gland surgery: Design and feasibility assessment of a potential standardized technique. World J. Otorhinolaryngol.–Head Neck Surg. 2023, 9, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Cammaroto G., Vicini C., Montevecchi F. Bonsembiante G., Meccariello L., Bresciani L., Pelucchi S. and Capaccio P. Submandibular gland excision: From external surgery to robotic intraoral and extraoral approaches. Oral Dis 2020 Jul;26(5):853-857. [CrossRef]
- Righini C.A., Petrossi J. , E. Reyta E., Atallaha I. An original submandibular approach technique sparing the cervical branch of the facial nerve. Eur Ann Otorhinolaryngol, Head Neck Dis (2014) 131, 143—146.
- Silver NL., Chinn SB, Bradley PJ. and Weber RS. Surgery for Malignant Submandibular Gland Neoplasms. Adv Otorhinolaryngol 2016:78:104-12. [CrossRef]
- Kikuoka, Y.; Kawata, R.; Higashino, M.; Terada, T.; Haginomori, SI. Operative technique for benign submandibular gland mass without identifying the mandibular branch of the facial nerve. Auris Nasus Larynx 45 (2018) 1221–1226. [CrossRef] [PubMed]
- House, J.W.; Brackmann, D.E. Facial Nerve Grading System. Otolaryngol. Adv Otorhinolaryngol 2016:78:46-52. Epub 2016 Apr 12. [CrossRef]
- Sanfurgo De Carvalho; R. Aperecido Dedivitis; M.A. Ferrari De Castro.Submandibular gland excision. Ressecção da glândula submandibular Rev. Col. Bras. Cir. 2015; 42(1): 014-017.
- Wu C.W., Dionigi G., Barczynski M., Chiang F.Y., Dralle H., Schneider R., Al-Quaryshi Z., Angelos P., Brauckhoff K., Brooks J.A. International neuromonitoring study group guidelines 2018: Part II: Optimal recurrent laryngeal nerve management for invasive thyroid cancer—Incorporation of surgical, laryngeal, and neural electrophysiologic data. Laryngoscope. 2018;128:S18–S27. [CrossRef]
- Schneider, R. , Randolph G.W., Dionigi G., Wu C.W., Barczynski M., Chiang F.Y., Al-Quaryshi Z., Angelos P., Brauckhoff K., Cernea C.R. International neural monitoring study group guideline 2018 part I: Staging bilateral thyroid surgery with monitoring loss of signal. Laryngoscope. 2018;128:S1–S17. [CrossRef]
- Wilson L, Lin E, Lalwani A. Cost-effectiveness of intraoperative facial nerve monitoring in middle ear or mastoid surgery. Laryngoscope. 2003;113:1736-1745.
- Duque, C.S.; Londono, A.F.; Duque, A.M.; Zuleta, J.J.; Marulanda, M.; Otálvaro, L.M.; Agudelo, M.; Duenas, J.P.; Palacio, M.F.;Dionigi G. Facial nerve monitoring in parotid gland surgery: Design and feasibility assessment of a potential standardized technique. World J. Otorhinolaryngol.Head Neck Surg. 2023, 9, 280–287.
- Zieli ’ nski, M.; Sowa, P.; Adamczyk-Sowa, M.; Szl˛ezak, M.; Misiołek, M. Assessment of Intraoperative Facial Nerve Monitoring in Patients Undergoing Partial Parotidectomy. BioMed Res. Int. 2022, 2022, 3318175. [Google Scholar]
- Lin B., Lu X., Shan X., Zhigang L. and Cai Z. Preoperative percutaneous nerve mapping of the mandibular marginal branch of the facial nerve. J Craniofac Surg. 2015 Mar;26(2):411-4. [CrossRef]

| Grading | FN Function |
|---|---|
| I: Normal | No deficit. |
| II: Mild dysfunction | Slight facial weakness or other mild dysfunction, normal tone and symmetry at rest; complete closure of the eye without effort; slight asymmetry of the mouth when facial movements occur. |
| III: Moderate dysfunction | No facial weakness with synkinesis and complete eye closure and good forehead movement with effort. |
| IV: Moderate–severe dysfunction | Obvious facial weakness. Incomplete eye closure, no forehead movement, asymmetrical mouth movement, and synkinesis. |
| V: Severe dysfunction | Little to no ability to smile, frown, or make other facial expressions. The closure of the eye is incomplete, and there is no forehead movement. |
| VI: Complete paralysis | No facial motion. |
 |
 |
| DAY | G1 | No Facial Paralysis | G2 | No Facial Paralysis |
|---|---|---|---|---|
| Day 1 | Gr I: 4/12 Gr II: 8/12 |
38 | Gr I: 8/11 Gr II: 3/11 |
40 |
| Days 90 | (Gr II): 7/12 | 43 | Gr II: 1/11 | 50 |
| Days 180 | (Gr II): 5/12 | 45 | 51 |
 |
 |
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



