Submitted:
29 January 2025
Posted:
31 January 2025
You are already at the latest version
Abstract
Recent years have seen a rapid expansion in research examining the relationship between homocysteine and stroke. In this study, we conducted a comprehensive bibliometric analysis of 233 articles related to homocysteine and stroke, published over the past 30 years in the Web of Science Core Collection. Our findings reveal a significant global increase in research on homocysteine and stroke, with China emerging as a leader, contributing 39.9% of total publications. Employing advanced methodologies such as co-citation analysis, bibliographic coupling, keyword co-occurrence, and citation burst analysis, we identified key research themes and emerging trends within the field. Notably, the results indicate a shift in focus from viewing homocysteine solely as a biomarker to recognizing its potential role in stroke prevention and management. These insights provide a valuable roadmap for future research directions and clinical strategies aimed at enhancing stroke prevention and improving patient outcomes.
Keywords:
Homocysteine
; Hyperhomocysteinemia
; Ischemic stroke
; Bibliometric analysis
; Research Trends
1. Introduction
Homocysteine is a sulfur-containing amino acid structurally related to cysteine and methionine. Unlike these amino acids, which are directly involved in protein synthesis, homocysteine primarily functions in one-carbon metabolism, a crucial process for cellular function. It undergoes processing via three main pathways: (i) remethylation to methionine, (ii) conversion to cysteine through the transsulfuration pathway, and (iii) formation of homocysteine thiolactone. These pathways depend on essential vitamins such as B6, B12, and B9 (folate) for their proper function [1]. Deficiencies in these vitamins, or genetic mutations, particularly in the methylenetetrahydrofolate reductase (MTHFR) enzyme, can impair homocysteine metabolism. This impairment can result in elevated homocysteine levels, which have been linked to vascular damage and other health complications [2].
In circulation, most homocysteine is bound to proteins, with a smaller fraction existing as dimers or free thiols. Normal fasting plasma homocysteine levels range from 5 to 15 μmol/L, but these levels increase with age and are generally higher in men. When plasma homocysteine exceeds 15 μmol/L, the condition is termed hyperhomocysteinemia. Elevated homocysteine has been identified as a significant risk factor for cardiovascular and cerebrovascular diseases. It is strongly associated with hypertension, smoking, and kidney dysfunction, which together exacerbate vascular damage and impair endothelial function [3]. This contributes to oxidative stress and inflammation, processes that play a central role in the development of stroke.
Stroke is a multifactorial disease, with numerous contributing risk factors, including hypertension, smoking, and kidney dysfunction [2]. Hyperhomocysteinemia further worsens these conditions by damaging the blood vessels, increasing oxidative stress, and promoting inflammation. For example, hypertension is aggravated by the endothelial dysfunction caused by elevated homocysteine, while smoking compounds vascular injury through mechanisms that accelerate atherosclerosis. Kidney dysfunction, which impairs the clearance of homocysteine, further increases its plasma levels, amplifying the risk of stroke. These interrelated mechanisms highlights the importance of controlling homocysteine levels as part of a strategy to mitigate stroke risk [1].
Despite the established association between hyperhomocysteinemia and stroke, several research gaps remain. Emerging research areas and trends, particularly those focusing on novel therapeutic approaches and mechanistic insights, are still underexplored. Bibliometric analysis provides a valuable tool for systematically evaluating the scientific literature, identifying research trends, and predicting future developments in this field [4]. This method can help uncover critical research hotspots, guiding future efforts to better understand how elevated homocysteine contributes to stroke risk. The present study employs bibliometric analysis to explore the relationship between hyperhomocysteinemia and stroke, aiming to identify key trends and emerging areas of research. These insights will contribute to the development of more effective prevention, diagnostic, and treatment strategies for stroke, particularly in individuals with elevated homocysteine levels.
2. Materials and Methods
2.1. Ethical Statement
No ethical approval was required as this study did not involve human participants or animals.
2.2. Data Source and Search Strategy
All data used in this study were retrieved from the publicly accessible Web of Science Core Collection (WoSCC) database and are fully detailed in the article and supplementary materials. No new datasets were generated as part of this research. Data are available upon request for further inquiry. A comprehensive literature search was conducted in the WoSCC using the search terms "homocysteine" and "stroke" in the title field (TI). This search, conducted as of September 23, 2024, identified 419 relevant studies. The search encompassed the full timespan of the database, from its inception to the specified date, ensuring a broad scope of historical and recent publications. To ensure a consistent dataset and avoid potential bias due to ongoing updates in the database, all records were extracted on September 23, 2024. The search results were restricted to English-language publications and excluded certain document types, including meeting abstracts (n=118), review articles (n=24), letters (n=17), proceedings papers (n=10), editorial materials (n=8), corrections (n=6), book chapters (n=1), and retracted publications (n=2). This filtering process resulted in a final dataset of 233 articles, which were used for the analysis (Figure S1).
2.3. Bibliometric Analyses
The Bibliometrix R package was employed to perform an extensive bibliometric analysis of the research landscape, focusing on the thematic structure of the literature and evaluating the academic impact of key researchers and journals. Bradford’s Law was applied to categorize journals by their productivity, identifying core journals that contribute the majority of the literature. Lotka’s Law was used to assess long-term trends in research output, focusing on the consistency of contributions over a 30-year period. Scientific mapping techniques were utilized to explore patterns and trends in homocysteine and stroke research. Tools such as VOSviewer (version 1.6.20) and CiteSpace (version 5.8) were applied to conduct various analyses, including bibliographic coupling, co-citation analysis, timeline analysis, burst analysis, and co-occurrence mapping. These methods allowed for the tracking of key term frequencies, identifying research hotspots, and predicting future research directions [4].
3. Results
3.1. Overview
This study provides a detailed analysis of the research landscape surrounding homocysteine and stroke, focusing on 233 articles published across 137 journals from 1995 to 2024, the period during which homocysteine was first linked to stroke in the scientific literature. The analysis reveals a steady annual growth rate of 5.32% in publications, reflecting increasing interest in this research area over nearly three decades. The average age of the documents analyzed was 11.4 years, with many foundational studies retaining relevance. The study involved contributions from approximately 1,500 authors, highlighting a collaborative approach in this field. Notably, only four of these authors contributed solo publications, emphasizing the importance of teamwork in advancing research on homocysteine and stroke. About 17% of the papers included in the dataset involved international collaborations, with an average of seven co-authors per paper, suggesting a global effort to address this important health issue (Supplemental Figure S2A). The research output peaked in 2017, with 16 publications in that year alone, marking a high point in scholarly attention to the topic (Supplemental Figure S2B). Despite this peak, citation trends have fluctuated over time. On average, each article received 39.94 citations, reflecting moderate academic influence and impact within the scientific community (Supplemental Figure S2A, S2C).
3.2. Scholarly Journal Influence and Collaboration Networks
The analysis of the most-cited journals in homocysteine and stroke research shows that Stroke has the highest m-index (0.67), with all top ten journals classified within Zone 1 of Bradford’s Law (Supplemental Table S1). The University of Western Australia leads in institutional output with 34 articles, and its most prolific author, Hankey, holds the highest h-index (10) and an m-index of 0.42 (Supplemental Tables S2A, S2B). According to Lotka’s Law, Hankey is also the most published author, while 88.5% of contributors authored only a single paper (Supplemental Table S2C). Hankey has maintained consistent publication activity over the past 30 years (Supplemental Figure S3). Collaboration networks, as illustrated in Supplemental S, highlight significant partnerships, with Australia collaborating with Canada on nine publications and China working with the USA on nine articles. These partnerships are among the most prolific in international research efforts. China leads in total publication volume with 331 articles but does not hold the top spot in citation impact, which belongs to the United Kingdom, averaging 224.30 citations per article (Supplemental Table S2D). Additionally, China exhibits a higher frequency of intra-country collaborations among corresponding authors compared to international partnerships, while Singapore and Australia demonstrate exclusively intra-country collaborations (Supplemental Figure S4B). In terms of citation impact, the article by Toole et al. [5] has the highest Normalized Global Citations (NGC) at 5.73 and Normalized Local Citations (NLC) at 3.91, though its NGC/NLC ratio is 1.28 (Table 1). In contrast, Perry et al. [6] holds the highest NGC/NLC ratio at 1.54, suggesting that its relative impact, based on global citations, is stronger compared to its local citation count (Table 1).
3.3. Bibliographic Coupling
Bibliographic coupling, a method in which two works are linked by citing the same third source, was employed to reveal overlapping research areas and identify concurrent topics within homocysteine studies. This approach highlights the interconnections between different facets of homocysteine research, particularly the foundational studies that continue to inform current investigations. Analyzing 233 documents, 175 items were found to meet a citation threshold of at least five citations, forming a major cluster composed of six sub-clusters. This network contained 7,418 connections and achieved a Total Link Strength (TLS) of 15,448, providing a comprehensive view of the research landscape (Figure 1). In this network, the size of each node reflects its relevance, while the proximity of nodes indicates similarities in research focus. The lines connecting nodes represent the relationships between these topics.
A key advantage of this bibliographic mapping approach is its ability to identify documents with shared characteristics, often linked by common authors or research themes. A prominent example is the work by Toole et al. [5], which represents the largest node, centrally positioned in Figure 1 and colored blue. It is closely surrounded by related studies, such as those by Perry et al [6] and Casas et al [15]. Toole et al [5] holds the highest citation count, with 1,037 citations, underscoring its central role in the Vitamin Intervention for Stroke Prevention (VISP) trial. This pivotal study investigated whether high doses of folic acid, vitamin B6, and B12 could reduce homocysteine levels and thereby lower the risk of recurrent stroke among 3,680 patients with a history of cerebral infarction. Perry et al. [6] follows with 725 citations, further illustrating its influence within the field. This clustering of influential studies demonstrates the importance of bibliographic coupling in identifying key contributors and emerging research trends in homocysteine-related stroke research.
3.4. Co-Cited References
Co-citation analysis, which evaluates how often authors and publications are cited together, was employed to identify influential researchers and foundational papers in the field of homocysteine and stroke research. The frequency of co-citations highlights the importance of certain works in shaping the field, helping to pinpoint key studies and leading experts. Among the 4,507 cited references that met the minimum threshold of 20 citations, 26 articles were identified, forming three clusters interconnected by 308 links and a TLS of 1,907 (Figure 2). The ten most co-cited articles in homocysteine research are listed in Table 2, with eight of these being observational studies and two meta-analyses, each garnering over 25 citations.
The most co-cited article in this review is a 2004 clinical trial that demonstrated the efficacy of high doses of folic acid, vitamin B6, and vitamin B12 in significantly reducing homocysteine levels, thereby lowering the risk of recurrent stroke in patients with prior cerebral infarction. Specifically, a 3 µmol/L reduction in homocysteine levels among patients from the United States, Canada, and Scotland was associated with a 10% decrease in stroke risk, a 26% reduction in coronary heart disease events, and a 16% reduction in mortality in the low-dose group. Interestingly, the high-dose group exhibited minimal and statistically insignificant reductions in risk, suggesting that the benefits of homocysteine reduction may plateau at higher doses. Furthermore, moderate reductions in homocysteine showed no significant effect on vascular outcomes in patients with non-disabling cerebral infarction over a two-year follow-up period [5].
A follow-up meta-analysis reinforced the association between elevated homocysteine levels and increased risks of ischemic heart disease (IHD) and stroke, indicating that a 25% reduction in homocysteine could lower the risk of IHD by 11% and stroke by 19% [16]. Another pivotal study highlighted a strong correlation between elevated plasma homocysteine and ischemic stroke, particularly in both large-artery and small-vessel disease. Specifically, a 5 µmol/L increase in homocysteine was found to significantly raise the risk of stroke, highlighting the critical importance of monitoring and managing homocysteine levels, especially among high-risk populations in Australia [17]. The TOAST classification system also emerged as a crucial tool, enhancing diagnostic accuracy by categorizing ischemic strokes into five distinct subtypes. This system’s relevance in homocysteine research lies in its ability to enable more precise studies that examine how homocysteine interacts with different stroke etiologies [18].
Further supporting homocysteine’s role as a stroke risk factor, a study of middle-aged British men revealed significantly elevated homocysteine levels in stroke patients, independent of age and lifestyle factors [6]. Additionally, a comprehensive meta-analysis of 72 genetic studies and 20 prospective studies showed that a 3 µmol/L reduction in homocysteine, achievable through folic acid supplementation, could reduce the risk of ischemic heart disease, deep vein thrombosis, and stroke [20]. Long-term data from the Framingham Study echoed these findings, demonstrating that individuals with elevated non-fasting plasma homocysteine levels faced a significantly higher risk of stroke. Those in the highest quartile had notably more strokes compared to those in the lowest quartile in the U.S. [8]. Moreover, research on homocysteine levels during the acute and convalescent phases of stroke in Caucasians showed a significant increase in plasma homocysteine as the stroke progressed. This suggests that elevated homocysteine levels may not only contribute to stroke risk but could also be a consequence of the stroke itself [7].
Collectively, these studies highlight the importance of managing homocysteine levels to reduce the risks of stroke and cardiovascular disease. Although the evidence supports the preventive use of vitamin B supplementation, uncertainties remain regarding the optimal dosages and timing for intervention.
3.5. Thematic Structure, Thematic Evolution, Co-Words and Burst Analysis
Figure 3A presents a thematic map identifying the 10 most frequently used keyword clusters in homocysteine and stroke research, offering a visual representation of the main topics driving inquiry in this area. Figure 3B tracks how these keywords have evolved over the past 30 years, illustrating shifts in research focus and the increasing prominence of certain themes, such as the role of homocysteine in ischemic stroke. Figure 3C shows a co-word analysis, confirming the interconnectedness of these prominent terms and demonstrating how the research field has matured by linking previously distinct concepts. These figures collectively emphasize the dynamic nature of homocysteine and stroke research, highlighting its growing complexity and the ongoing refinement of key concepts over time.
Figure 3A classifies keywords into four quadrants: niche, emerging or declining, basic, and motor themes, based on their density and centrality. Keywords such as "aminothiols", "glutathione", and "meta-analysis" in the niche quadrant reflect highly specialized but narrowly focused topics. In contrast, terms such as "risk factor" and "hypertension" fall within the motor themes quadrant, indicating that they are not only central to the field but also have widespread relevance, particularly in stroke risk assessment and prevention strategies. However, keywords such as "cardiovascular disease" and "case-control study" show less centrality despite their relevance. The emerging themes quadrant reveals growing interest in terms such as "methylenetetrahydrofolate reductase" and "cerebral infarction". Similarly, "ischemic stroke" and "hyperhomocysteinemia," positioned in the lower-right quadrant, suggest areas that could evolve into key research directions with further exploration. Interestingly, terms such as "folate" and "folic acid" are positioned between emerging and basic themes, hinting at their transition into more foundational areas of study. Meanwhile, keyword emergence for terms such as "homocysteine" and "stroke" demonstrates their high centrality, as marked by a sudden increase in usage over a short period.
Since 2018, there has been a notable shift in research focus toward keywords such as "risk", "ischemic stroke", "death", "cardiovascular disease", "protein", and "health-care professional". (Figure 3B). This increasing prominence suggests a broader research emphasis on risk factors, clinical outcomes, and healthcare interventions. Moreover, co-word analysis further identified 106 keywords that met the citation threshold, forming six clusters with 2,443 links and a TLS of 6,723 (Figure 3C). Node size reflects the frequency of keyword co-occurrences, with larger nodes signifying more frequent occurrences. The color of the node's outer ring indicates the timing of these co-occurrences: cooler colors represent earlier years, while warmer colors signify more recent ones. Lines connecting the nodes depict the strength of the relationship. Among these nodes, the top five keywords, such as "homocysteine" (n=157), "stroke" (n=81), "plasma homocysteine" (n=68), "hyperhomocysteinemia" (n=54), and "risk" (n=53), were highlighted as the most influential topics in the field (Figure 3C, Supplemental Table S3).
The keyword citation burst analysis using Citespace, with a five-year interval (Figure 3D), reveals key research hotspots and emerging trends in homocysteine studies. "Vascular disease" exhibited the highest burst strength (8.53), indicating its central importance in the research landscape, followed by "acute ischemic stroke" (6.00), "risk" (4.61), "population" (4.47), and "b-vitamins" (4.08). Notably, terms such as "vascular disease" and "b-vitamins" also maintained the longest burst durations, spanning up to 10 years, reflecting their sustained relevance in the field. In contrast, "population" was a focal point for a relatively shorter duration, from 2015 to 2019, suggesting more transient interest in demographic-related aspects. Likewise, emerging keywords such as "acute ischemic stroke" and "risk" have gained increasing attention. The prominence of these terms aligns with a growing emphasis on understanding stroke risk factors and interventions, suggesting that future studies may increasingly focus on the intersection of homocysteine levels, acute stroke management, and vascular disease prevention.
4. Discussion
4.1. Overview of Research Landscape
This project analyzed 233 research articles from the Web of Science Core Collection (WoSCC) database, covering the past 30 years, to identify key trends and future directions in homocysteine and stroke research. The findings provide valuable insights for further investigation. Publication volume reflects the field's productivity, while citation counts indicate the impact of individual studies. Before 2004, relatively few articles were published, suggesting that research on homocysteine and stroke was in its early stages. However, since 2005, the field has experienced substantial growth, despite occasional fluctuations. Over the past four years, research activity has intensified, with at least 10 articles published annually, except in 2024, which has already recorded 9 publications. This upward trend highlights a growing global interest in the role of homocysteine in stroke, and further expansion is anticipated in the coming years.
From a geographical perspective, China leads in this field, contributing 39.9% of the global publications on homocysteine and stroke. The country’s rapid growth over the past three decades highlights its strong research potential, particularly in domestic publications. Notably, Soochow University ranks eighth among the world's most productive institutions, and three of the top ten most-cited authors are affiliated with China. However, most of the top ten co-cited papers were authored by researchers from the USA [5,8,16,18], UK [6,19,20,21], Canada [17], and Sweden [7]. This indicates that while China generates a high volume of research, there is potential to enhance its global influence and research quality. Strengthening international collaboration, particularly between Chinese and global researchers, could help raise the quality and impact of future studies.
In terms of journal impact, Stroke holds the highest m-index and h-index, placing it in Zone 1 according to Bradford's Law, signifying its significant influence in homocysteine and stroke research. Current studies in this field are primarily published in journals focused on neurology, atherosclerosis, and multidisciplinary topics, with a strong emphasis on clinical trials [5,18] and observational studies [6,7,17]. However, there has been a relative lack of large-scale meta-analyses with comprehensive subgroup analyses of multi-populations in the past four years. Such studies could provide guidelines applicable to the general population, highlighting a critical gap and opportunity for further synthesis of existing evidence in this field.
From an authorial perspective, Hankey is the most prolific researcher, with the highest h-index, which reflect the broad impact of his work. His research primarily focuses on meta-analyses, randomized controlled trials, and risk factors for neurological diseases. Hankey and Eikelboom’s research in 1999 has laid a foundation for understanding the relationship between homocysteine and stroke [1]. Although Toole ranks lower in terms of productivity, his work has the highest normalized citation counts both globally and locally. Toole's VISP trial, ranked first among the top ten co-cited papers, demonstrated that high doses of folic acid, vitamin B6, and B12 significantly reduce recurrent stroke risk by lowering homocysteine levels. However, the trial also revealed that moderate homocysteine reduction did not affect vascular outcomes after cerebral infarction [5]. Several other scholars have also made substantial contributions, advancing knowledge of homocysteine’s role in stroke and shaping future prevention and treatment strategies [20,21].
4.2. Research Trend and Research Hotspots
Research on homocysteine and stroke has predominantly focused on elucidating the association between elevated homocysteine levels and stroke risk, along with investigating the role of vitamin supplementation in lowering homocysteine. Seminal studies, such as Toole’s VISP trial, have laid the groundwork for this field [5], with high citation counts emphasizing the importance of randomized controlled trials and meta-analyses. Recently, the research focus has expanded beyond stroke risk reduction to include broader cardiovascular outcomes linked to homocysteine management. The sections below explore the key research themes that have emerged.
4.2.1. Homocysteine and Vascular Disease
A major area of investigation has been the role of elevated homocysteine as an independent risk factor for stroke and cardiovascular diseases. This line of research highlights vascular disease as a prominent hotspot in homocysteine studies. First implicated in vascular disease by Kilmer McCully in the 1970s, homocysteine is now recognized as a crucial biomarker for cardiovascular disease [20], stroke [2], and conditions such as cognitive decline [23]. Elevated homocysteine levels, or known as hyperhomocysteinemia, are commonly attributed to factors such as B-vitamin deficiencies [2], oxidative stress, and disruptions in redox balance [24] rather than being a direct cause of these diseases. Hyperhomocysteinemia affects key metabolic pathways, especially remethylation and trans-sulfuration, leading to oxidative stress, endothelial dysfunction, and chronic inflammation, all of which contribute to atherosclerosis, stroke, and neurodegeneration [23,25]. The pathogenic role of hyperhomocysteinemia extends beyond elevated homocysteine levels. Mechanisms such as protein homocysteinylation [26], overactivation of N-methyl-D-aspartate receptors [27], and reduced nitric oxide bioavailability are implicated in vascular dysfunction and neuroinflammation [28]. These processes are particularly significant in acute ischemic stroke and cerebral infarction, where hyperhomocysteinemia exacerbates endothelial damage and vascular dysfunction [26,27]. Despite the established link between hyperhomocysteinemia and disease, clinical trials aimed at lowering homocysteine through B-vitamin supplementation have yielded mixed results, suggesting the complex role of homocysteine in disease prevention [5,29]. Moreover, elevated homocysteine levels have been associated with increased all-cause mortality, especially in patients with vascular disease. However, genetic studies have questioned the direct causality of hyperhomocysteinemia in stroke recurrence, suggesting that its role may be overstated [30]. This highlights the need for additional studies to unravel the complex interplay between homocysteine, vascular disease, and neurodegeneration, and to develop personalized approaches to managing elevated homocysteine in clinical practice.
4.2.2. Emerging Focus on Ischemic Stroke and Risk Factors
Recent keyword analyses highlight an increasing focus on the relationship between elevated homocysteine levels and ischemic stroke. Systematic reviews and meta-analyses have confirmed a dose-response relationship, with stroke risk rising significantly when homocysteine levels exceed 15 µmol/L. One prominent meta-analysis reported a 43% increase in stroke risk for every 5 µmol/L rise in homocysteine, indicating a nonlinear relationship that warrants further exploration to fully understand its clinical implications [31]. The interaction between hypertension and hyperhomocysteinemia is particularly critical in determining stroke risk. Patients with both conditions demonstrate a significantly higher risk of early cognitive impairment following their first ischemic stroke. Multivariate analyses have identified several independent predictors of cognitive decline, including elevated serum homocysteine levels, years of education, and Fazekas scale scores, underscoring the need for targeted interventions in these high-risk populations [32]. Elevated homocysteine levels have also been associated with poorer survival outcomes in acute ischemic stroke patients, with studies reporting significantly higher homocysteine levels in stroke patients compared to healthy controls [33]. In a large study from China involving over 3,000 participants, elevated homocysteine levels were found across all subtypes of ischemic stroke, according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification, reinforcing the role of homocysteine as a major risk factor [34]. Furthermore, a broader analysis of 51,426 participants confirmed that elevated plasma total homocysteine increases the risk of various stroke types, including ischemic, hemorrhagic, and recurrent strokes. These findings highlight the critical importance of routine homocysteine monitoring and early intervention to improve stroke outcomes [35]. Additionally, research has emphasized the need to address genetic predispositions and vitamin deficiencies, particularly in younger adults, as part of preventive strategies. Maintaining adequate folate levels has been shown to significantly reduce mortality and major disability in ischemic stroke patients [3,5], further reinforcing the significance of homocysteine management in stroke prevention.
4.2.3. Folic Acid and B-Vitamin Supplementation: Implications for Stroke
Research into the impact of vitamin supplementation on homocysteine levels remains a critical area of focus in stroke prevention. Folic acid, along with vitamins B6 and B12, plays a key role in homocysteine metabolism, which is directly linked to vascular health and the prevention of stroke recurrence. Folic acid provides essential methyl groups for the conversion of homocysteine into methionine, a process that requires vitamin B12 as a cofactor. Concurrently, vitamin B6 facilitates the breakdown of homocysteine into cysteine, which enhances antioxidant defenses through the production of glutathione [1]. Recent meta-analyses have produced mixed but valuable insights regarding the effects of B-vitamin supplementation on stroke risk. One major study found no overall association between B-vitamin supplementation and stroke risk reduction, but subgroup analyses revealed potential benefits in specific populations, such as those with a male-to-female ratio greater than 2 or individuals receiving folic acid doses below 1 mg [3]. Another meta-analysis indicated that B-vitamin supplementation significantly reduced stroke events, particularly among participants without chronic kidney disease and those with longer follow-up periods [36]. Additional evidence from meta-analyses suggests that combining folic acid with vitamins B6 and B12 not only reduces homocysteine levels but also lowers the risk of stroke recurrence and other vascular events [37,38,39]. These vitamins have also been associated with decreased stroke-related mortality. Despite the positive outcomes of B-vitamin supplementation in stroke prevention, its impact on major adverse cardiovascular events and overall mortality remains unclear [40].
4.2.4. Acute Stroke Phases and Homocysteine Dynamics
Research highlights the critical role of homocysteine level fluctuations during both the acute and convalescent phases of stroke. Elevated homocysteine levels in the acute phase are closely associated with increased oxidative stress, endothelial dysfunction, and the progression of lacunar stroke. Early intervention with folic acid or B-vitamins during this phase is essential to mitigate complications such as post-ischemic hyperperfusion, tissue damage, and delayed recovery, thereby improving patient outcomes [41]. Accurate measurement of homocysteine levels in the acute phase can help predict key outcomes, including the degree of reperfusion and the extent of ischemic damage [7,41,42]. SPECT imaging studies have shown that timely recanalization, combined with effective homocysteine management, can significantly reduce infarct size and accelerate recovery [42]. During the convalescent phase, continuous regulation of homocysteine levels remains essential to prevent further neurovascular damage and lower the risk of stroke recurrence or subsequent acute ischemic events [43,44]. Persistently elevated homocysteine levels in this phase exacerbate inflammation and oxidative stress, impeding the recovery process [45]. Therefore, sustained monitoring and targeted intervention throughout both the acute and recovery stages are crucial for optimizing long-term outcomes and minimizing the risk of recurrent strokes.
4.3. Limitations and Future Directions
Despite significant advancements in understanding homocysteine’s role in stroke pathogenesis, several key limitations continue to hinder the optimization of its clinical applications. One major challenge is the substantial variability in homocysteine levels, which are influenced by external factors such as diet, medication use, lifestyle, and genetic predispositions. This variability complicates efforts to establish a universal threshold for stroke risk, as inconsistent measurements undermine reliability. Future studies should be conducted to standardize homocysteine assessment, potentially through the incorporation of genetic markers and more precise biochemical testing, to enhance accuracy in clinical practice.
Another critical limitation is the inconsistent outcomes observed in clinical trials evaluating homocysteine-lowering interventions, such as folate and B-vitamin supplementation. Although some studies report modest reductions in stroke risk, others show minimal or no benefit, raising concerns about the generalizability of these interventions across diverse populations with different genetic, environmental, and lifestyle factors. Future research should focus on more rigorously controlled trials with broader population samples and explore patient-specific factors to develop more targeted and effective therapeutic approaches.
A further unresolved issue is the uncertainty regarding the optimal timing for homocysteine intervention in stroke treatment. Although early reduction of homocysteine has been associated with benefits, identifying the precise window for maximizing therapeutic efficacy remains challenging. This gap highlights the need for a deeper understanding of the temporal dynamics of homocysteine fluctuations during both the acute and recovery phases of stroke. Longitudinal studies that monitor homocysteine levels over time could help determine the most effective intervention periods and refine treatment protocols.
Moreover, existing research has primarily focused on the short-term effects of homocysteine-lowering strategies, with limited attention to long-term outcomes such as stroke recurrence and sustained recovery. This emphasis on immediate results overlooks the potential benefits of prolonged homocysteine management in reducing future stroke risk and improving post-stroke rehabilitation. Future studies should prioritize long-term follow-up to evaluate the impact of sustained interventions on stroke recurrence and the quality of life of stroke survivors over time.
A critical gap remains in understanding how demographic factors such as age, sex, and ethnicity influence homocysteine metabolism. These variables likely modulate both stroke risk and the effectiveness of homocysteine-lowering therapies, but they have been underexplored in research. Genetic polymorphisms that affect homocysteine metabolism, combined with lifestyle differences across demographic groups, could result in variable responses to treatment. Targeted research that accounts for these factors is essential to develop personalized interventions, improving therapeutic outcomes across diverse populations.
An additional limitation in this study is the oversight of key public health interventions, particularly the mandatory folic acid fortification of wheat flour introduced in countries such as the United Kingdom and Australia in the early 2000s. This fortification likely contributed to a general reduction in homocysteine levels during this period, potentially influencing the observed trends in stroke risk. Future studies should consider such public health measures to more accurately assess the relationship between homocysteine levels and stroke incidence in fortified versus non-fortified populations.
Hence, integrating advanced diagnostic tools, such as high-resolution imaging and multi-marker panels, into clinical practice will be crucial for improving the accuracy of homocysteine-related stroke risk assessments. These technologies may enable earlier detection and more tailored interventions, ultimately improving patient outcomes. Additionally, future research should investigate the interactions between homocysteine and other well-established stroke risk factors, such as hypertension, diabetes, and hyperlipidemia. By adopting a more comprehensive approach that accounts for the complex interplay of multiple risk factors, more refined and effective strategies for stroke prevention and management, especially in high-risk populations, can be developed.
5. Conclusions
In summary, this bibliometric analysis of 233 research articles over the past 30 years reveals substantial growth in the study of homocysteine and its role in stroke, with increasing global attention, particularly from China. However, strengthening its global influence will require enhanced international collaboration. Significant research gaps persist, particularly the need for large-scale meta-analyses to clarify homocysteine's impact on stroke risk and treatment efficacy. Studies on homocysteine fluctuations during the acute and convalescent phases of stroke emphasize the importance of timely intervention, with early reduction in homocysteine levels being critical for minimizing neurovascular damage and improving recovery outcomes. Moreover, managing homocysteine-related risks beyond the acute phase is crucial for preventing long-term complications and reducing stroke recurrence. Future research should prioritize standardizing homocysteine measurements, optimizing the timing of interventions, and further exploring the molecular mechanisms underlying homocysteine-induced damage. Additionally, developing personalized treatment strategies tailored to individual risk factors and specific stroke phases will be key to refining stroke care. Addressing these critical areas holds significant potential for improving patient outcomes and advancing stroke prevention and management on a global scale.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1. Overview of the bibliometric analysis; Figure S2. Overview of the study. (A): Main information. (B): Annual scientific production. (C): Average citations per year; Figure S3. Author’s productivity over 30 years period; Figure S4. Collaborative patterns among countries. (A): Country collaboration map. (B): Intra-country (SCP) and inter-country (MCP) collaboration indices; Table S1. Most cited journals for homocysteine and stroke; Table S2. (A) Prominent institutions published in homocysteine; (B) The most cited authors listed based on h-index; (C) Author productivity verify using Lotka Law; (D) Top 10 affiliated countries; Table S3. The top 5 co-words related to homocysteine and stroke.
Data Availability Statement
All data generated or analyzed are included in this published article.
Conflicts of Interest
The authors declare that they have no conflicts of interest in this work.
References
- G.J. Hankey, J.W. Eikelboom, Homocysteine and stroke, Curr. Opin. Neurol. 14 (2001) 95–102. [CrossRef]
- L.K. Wei, A. Au, S. Menon, S.H. Gan, L.R. Griffiths, Clinical relevance of MTHFR, eNOS, ACE, and ApoE gene polymorphisms and serum vitamin profile among Malay patients with ischemic stroke, J. Stroke Cerebrovasc. Dis. 24 (2015) 2017–2025. [CrossRef]
- C. Zhang, F.L. Chi, T.H. Xie, Y.H. Zhou, Effect of B-vitamin supplementation on stroke: A meta-analysis of randomized controlled trials, PLoS ONE 8 (2013) e81577. [CrossRef]
- L.K. Wei, H.S. Heidi, L.R. Griffiths, Epigenetics and ischemic stroke: A bibliometric analysis from 2014 to 2024, Epigenetics Insights (In press).
- J.F. Toole, M.R. Malinow, L.E. Chambless, J.D. Spence, L.C. Pettigrew, V.J. Howard,... G. Howard, Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: The Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial, JAMA 291 (2004) 565–575. [CrossRef]
- I.J. Perry, R.W. Morris, S.B. Ebrahim, A.G. Shaper, H. Refsum, P.M. Ueland, Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged British men, Lancet 346 (1995) 1395–1398. [CrossRef]
- Brattström, B. Norrving, B. Hultberg, A. Andersson, B.B. Johansson, Plasma homocysteine in the acute and convalescent phases after stroke, Stroke 26 (1995) 795–800. [CrossRef]
- A.G. Bostom, I.H. Rosenberg, H. Silbershatz, P.F. Jacques, J. Selhub, R.B. D’Agostino,... P.W. Wilson, Nonfasting plasma total homocysteine levels and stroke incidence in elderly persons: The Framingham Study, Ann. Intern. Med. 131 (1999) 352–355. [CrossRef]
- D.J. Meiklejohn, M.A. Vickers, R. Dijkhuisen, M. Greaves, Plasma homocysteine concentrations in the acute and convalescent periods of atherothrombotic stroke, Stroke 32 (2001) 57–62. [CrossRef]
- H. Iso, Y. Moriyama, S. Sato, A. Kitamura, T. Tanigawa, K. Yamagishi,... M. Konishi, Serum total homocysteine concentrations and risk of stroke and its subtypes in Japanese, Circulation 109 (2004) 2766–2772. [CrossRef]
- Z. Li, L. Sun, H. Zhang, Y. Liao, D. Wang, B. Zhao, et al., Elevated plasma homocysteine was associated with hemorrhagic and ischemic stroke, but methylenetetrahydrofolate reductase gene C677T polymorphism was a risk factor for thrombotic stroke, Stroke 34 (2003) 2085–2090. [CrossRef]
- M.L. Bots, L.J. Launer, J. Lindemans, A.W. Hoes, A. Hofman, J.C.M. Witteman, et al., Homocysteine and short-term risk of myocardial infarction and stroke in the elderly, Arch. Intern. Med. 159 (1999) 38–44. [CrossRef]
- Z. Shi, Y. Guan, Y.R. Huo, S. Liu, M. Zhang, H. Lu, et al., Elevated total homocysteine levels in acute ischemic stroke are associated with long-term mortality, Stroke 46 (2015) 2419–2425. [CrossRef]
- G. Saposnik, J.G. Ray, P. Sheridan, M. McQueen, E. Lonn, Homocysteine-lowering therapy and stroke risk, severity, and disability, Stroke 40 (2009) 1365–1372. [CrossRef]
- J.P. Casas, L.E. Bautista, L. Smeeth, P. Sharma, A.D. Hingorani, Homocysteine and stroke: evidence on a causal link from mendelian randomisation, Lancet 365 (2005) 224–232. [CrossRef]
- Homocysteine Studies Collaboration, Homocysteine and risk of ischemic heart disease and stroke, JAMA 288 (2002) 2015–2022. [CrossRef]
- J.W. Eikelboom, G.J. Hankey, S.S. Anand, E. Lofthouse, N. Staples, R.I. Baker, Association between high homocyst(e)ine and ischemic stroke due to large- and small-artery disease but not other etiologic subtypes of ischemic stroke, Stroke 31 (2000) 1069–1075. [CrossRef]
- H.P. Adams, B.H. Bendixen, L.J. Kappelle, J. Biller, B.B. Love, D.L. Gordon, et al., Classification of subtype of acute ischemic stroke: Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment, Stroke 24 (1993) 35–41. [CrossRef]
- I.M. Graham, L.E. Daly, H.M. Refsum, K. Robinson, L.E. Brattström, P.M. Ueland, et al., Plasma homocysteine as a risk factor for vascular disease, JAMA 277 (1997) 1775–1781. [CrossRef]
- D.S. Wald, Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis, BMJ 325 (2002) 1202–1206. [CrossRef]
- D.J. Meiklejohn, M.A. Vickers, R. Dijkhuisen, M. Greaves, Plasma homocysteine concentrations in the acute and convalescent periods of atherothrombotic stroke, Stroke 32 (2001) 57–62. [CrossRef]
- A.D. Smith, H. Refsum, Homocysteine – from disease biomarker to disease prevention, J. Intern. Med. 290 (2021) 826–854. [CrossRef]
- Y. Ma, Y. Chen, T. Yang, X. He, Y. Yang, J. Chen, et al., Blood biomarkers for post-stroke cognitive impairment: a systematic review and meta-analysis, J. Stroke Cerebrovasc. Dis. (2024) 107632. [CrossRef]
- M.Y. Maksimova, A.V. Ivanov, E.D. Virus, K.A. Nikiforova, F.R. Ochtova, E.T. Suanova, et al., Impact of glutathione on acute ischemic stroke severity and outcome: possible role of aminothiols redox status, Redox Rep. 26 (2021) 117–123. [CrossRef]
- L.K. Wei, H. Sutherland, A. Au, E. Camilleri, L.M. Haupt, S.H. Gan, et al., A potential epigenetic marker mediating serum folate and vitamin B12 levels contributes to the risk of ischemic stroke, Biomed. Res. Int. 2015 (2015) 1–4. [CrossRef]
- M. Sikora, E. Bretes, J. Perła-Kaján, O. Utyro, K. Borowczyk, J. Piechocka, et al., Homocysteine thiolactone and other sulfur-containing amino acid metabolites are associated with fibrin clot properties and the risk of ischemic stroke, Sci. Rep. 14 (2024). [CrossRef]
- A.R. Mathew, G. Di Matteo, P. La Rosa, S.A. Barbati, L. Mannina, S. Moreno, et al., Vitamin B12 deficiency and the nervous system: Beyond metabolic decompensation—Comparing biological models and gaining new insights into molecular and cellular mechanisms, Int. J. Mol. Sci. 25 (2024) 590. [CrossRef]
- Z.J. Yang, S.Y. Huang, K.Y. Zhong, W.G. Huang, Z.H. Huang, T.T. He, et al., Betaine alleviates cognitive impairment induced by homocysteine through attenuating NLRP3-mediated microglial pyroptosis in an m6A-YTHDF2-dependent manner, Redox Biol. 69 (2024) 103026. [CrossRef]
- N. Zhang, Z. Zhou, X. Chi, F. Fan, S. Li, Y. Song, et al., Folic acid supplementation for stroke prevention: a systematic review and meta-analysis of 21 randomized clinical trials worldwide, Clin. Nutr. 43 (2024) 1706–1716. [CrossRef]
- Q. Zhou, Z. Xu, Y. Duan, H. Tang, H. Zhang, H. Liu, MTHFR C677T, hyperhomocysteinemia, and their interactions with traditional risk factors in early neurological deterioration in Chinese patients with ischemic stroke, Heliyon 10 (2024) e31003. [CrossRef]
- M. Holmen, A.M. Hvas, J.F.H. Arendt, Hyperhomocysteinemia and ischemic stroke: A potential dose-response association—A systematic review and meta-analysis, TH Open 5 (2021) e420–437. [CrossRef]
- Z.H. Lu, J. Li, X.L. Li, M. Ding, C.J. Mao, X.Y. Zhu, et al., Hypertension with hyperhomocysteinemia increases the risk of early cognitive impairment after first-ever ischemic stroke, Eur. Neurol. 82 (2019) 75–85. [CrossRef]
- S. Huang, J. Cai, Y. Tian, The prognostic value of homocysteine in acute ischemic stroke patients: A systematic review and meta-analysis, Front. Syst. Neurosci. 14 (2021). [CrossRef]
- T. Zhang, Y. Jiang, S. Zhang, T. Tie, Y. Cheng, X. Su, et al., The association between homocysteine and ischemic stroke subtypes in Chinese, Med. 99 (2020) e19467. [CrossRef]
- H. Li, L. Shu, Q. Dai, T. Wu, Association between plasma total homocysteine (tHcy) and strokes: A meta-analysis, Pteridines 33 (2022) 58–68. [CrossRef]
- Y. Ji, S. Tan, Y. Xu, A. Chandra, C. Shi, B. Song, et al., Vitamin B supplementation, homocysteine levels, and the risk of cerebrovascular disease, Neurol. 81 (2013) 1298–1307. [CrossRef]
- S. Tripathi, M. Nath, S. Misra, P. Kumar, From A to E: Uniting vitamins against stroke risk—A systematic review and network meta‐analysis, Eur. J. Clin. Invest. 54 (2024). [CrossRef]
- N. Kataria, P. Yadav, R. Kumar, N. Kumar, M. Singh, R. Kant, et al., Effect of vitamin B6, B9, and B12 supplementation on homocysteine level and cardiovascular outcomes in stroke patients: A meta-analysis of randomized controlled trials, Cureus (2021). [CrossRef]
- N. Zhang, Z. Wu, X. Bai, Y. Song, P. Li, X. Lu, et al., Dosage exploration of combined B-vitamin supplementation in stroke prevention: A meta-analysis and systematic review, Am. J. Clin. Nutr. 119 (2024) 821–828. [CrossRef]
- J.D. Spence, G.J. Hankey, Problem in the recent American Heart Association guideline on secondary stroke prevention: B vitamins to lower homocysteine do prevent stroke, Stroke 53 (2022) 2702–2708. [CrossRef]
- W.C. Dong, J.L. Guo, L. Xu, X.H. Jiang, C.H. Chang, Y. Jiang, et al., Impact of homocysteine on acute ischemic stroke severity: Possible role of aminothiols redox status, BMC Neurol. 24 (2024). [CrossRef]
- Y. Wang, R. Hou, Y. Liu, Plasma homocysteine (Hcy) concentration functions as a predictive biomarker of SPECT-evaluated post-ischemic hyperperfusion in acute ischemic stroke, Pharmacogenomics Pers. Med. 16 (2023) 481–489. [CrossRef]
- Žitňanová, P. Šiarnik, B. Kollár, M. Chomová, P. Pazderová, L. Andrezálová, et al., Oxidative stress markers and their dynamic changes in patients after acute ischemic stroke, Oxid. Med. Cell Longev. 2016 (2016) 1–7. [CrossRef]
- M.Y. Maksimova, A.V. Ivanov, E.D. Virus, K.A. Nikiforova, F.R. Ochtova, E.T. Suanova, et al., Impact of glutathione on acute ischemic stroke severity and outcome: Possible role of aminothiols redox status, Redox Rep. 26 (2021) 117–123. [CrossRef]
- F.Z. Kamal, R. Lefter, H. Jaber, I.M. Balmus, A. Ciobica, A.C. Iordache, The role of potential oxidative biomarkers in the prognosis of acute ischemic stroke and the exploration of antioxidants as possible preventive and treatment options, Int. J. Mol. Sci. 24 (2023) 6389. [CrossRef]
Figure 1.
Bibliographic coupling analysis with network visualization.
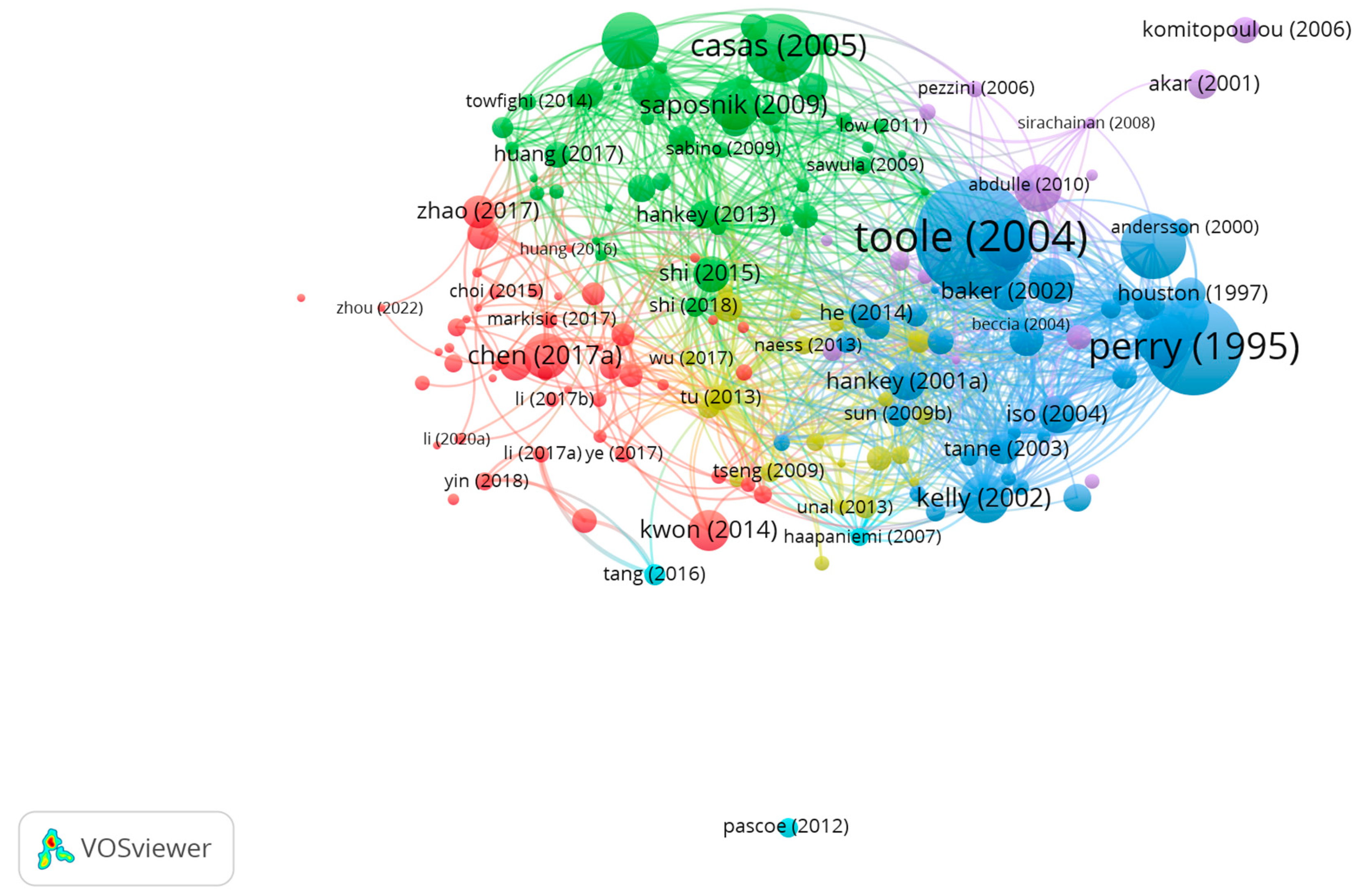
Figure 2.
Co-citation analysis of cited references with network visualization.
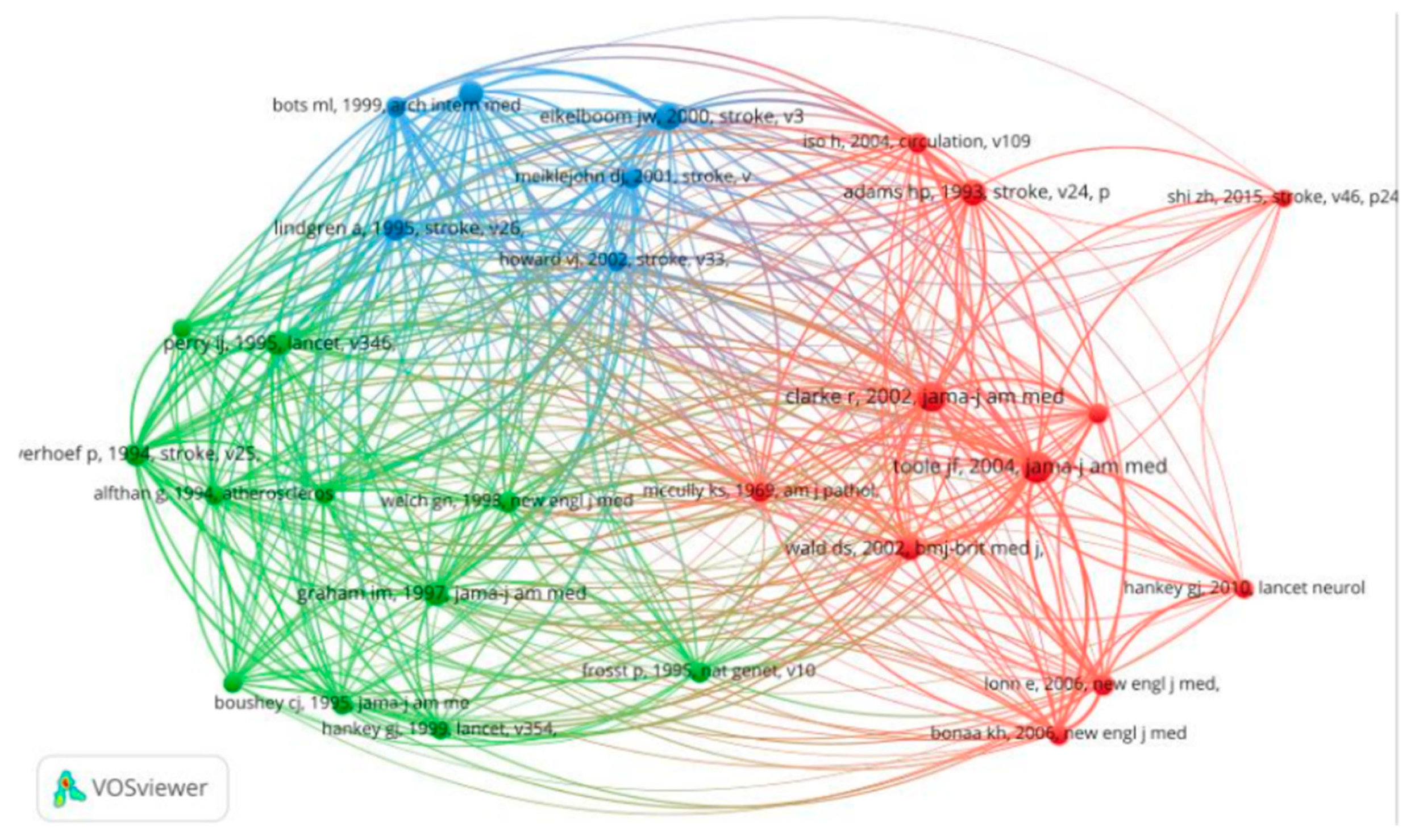
Figure 3.
Research hotspots and future trends. (A) Thematic analysis. (B) Thematic evolution analysis. (C) Co-words analysis. (D) Citation burst analysis.
Figure 3.
Research hotspots and future trends. (A) Thematic analysis. (B) Thematic evolution analysis. (C) Co-words analysis. (D) Citation burst analysis.
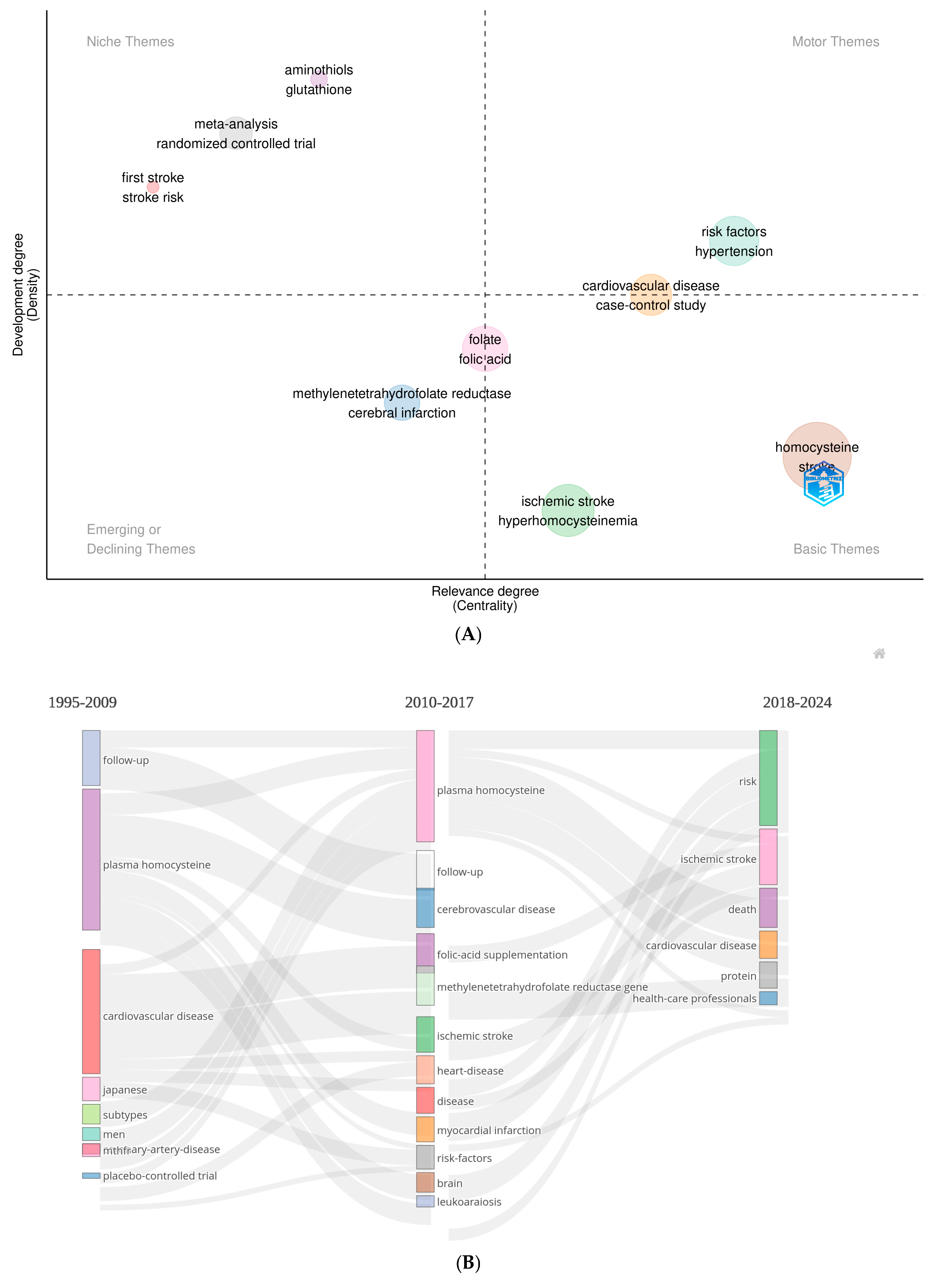
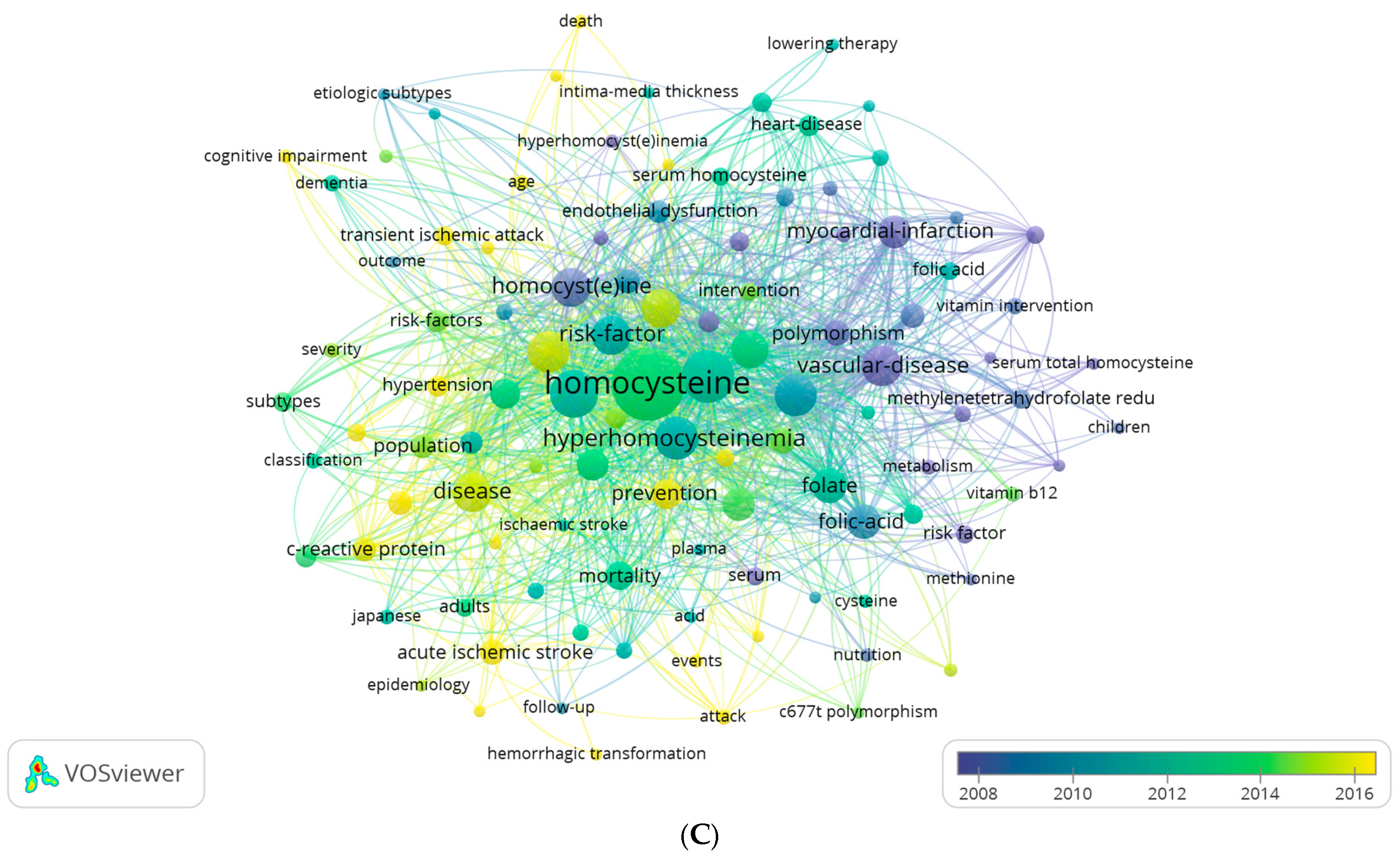

Table 1.
Impact measure for the most cited documents.
| Rank | DOI, [Reference] | Normalized Global Citations (NGC) |
Normalized Local Citations (NLC) |
NGC/NLC Ratio |
|---|---|---|---|---|
| 1 | 10.1001/jama.291.5.565 [5] | 5.00 | 3.91 | 1.28 |
| 2 | 10.1016/S0140-6736(95)92407-8 [6] | 1.59 | 1.03 | 1.54 |
| 3 | 10.1161/01.STR.26.5.795 [7] | 0.41 | 0.97 | 0.42 |
| 4 | 10.7326/0003-4819-131-5-199909070-00006 [8] | 2.22 | 2.18 | 1.02 |
| 5 | 10.1161/01.STR.32.1.57 [9] | 1.26 | 3.48 | 0.36 |
| 6 | 10.1161/01.CIR.0000131942.77635.2D [10] | 0.56 | 1.70 | 0.33 |
| 7 | 10.1161/01.STR.0000086753.00555.0D [11] | 2.09 | 2.45 | 0.85 |
| 8 | 10.1001/archinte.159.1.38 [12] | 1.40 | 1.54 | 0.91 |
| 9 | 10.1161/STROKEAHA.115.009136 [13] | 3.18 | 3.48 | 0.91 |
| 10 | 10.1161/STROKEAHA.108.529503 [14] | 4.81 | 5.02 | 0.96 |
NA: Not applicable. The document is cited only in global contexts.
Table 2.
The top 10 co-cited references related to homocysteine and stroke.
| Rank | DOI, [Reference] | First Author [Country] |
Co-cited (n) |
Year | TLS |
|---|---|---|---|---|---|
| 1 | *[10.1001/jama.291.5.565] [5] |
Toole JF [USA] |
59 | 2004 | 239 |
| 2 | [10.1001/jama.288.16.2015] [16] |
Clarke R [USA] |
55 | 2002 | 246 |
| 3 | [10.1161/01.str.31.5.1069] [17] |
Eikelboom JW [Canada] |
43 | 2000 | 193 |
| 4 | [10.1161/01.str.24.1.35] [18] |
Adams HP [USA] |
42 | 1993 | 159 |
| 5 | [10.1001/jama.277.22.1775] [19] |
Graham IM [UK] |
34 | 1997 | 162 |
| 6 | *[10.1016/S0140-6736(95)92407-8] [6] | Perry IJ [UK] |
34 | 1995 | 202 |
| 7 | [10.1136/bmj.325.7374.1202] [20] |
Wald DS [UK] |
33 | 1995 | 161 |
| 8 | *[10.1161/01.STR.26.5.795] [7] |
Lindgren A [Sweden] |
32 | 2002 | 168 |
| 9 | *[10.7326/0003-4819-131-5-199909070-00006] [8] |
Bostom AG [USA] |
31 | 1995 | 174 |
| 10 | [10.1161/01.str.32.1.57] [21] |
Meiklejohn DJ [UK] |
29 | 1999 | 165 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



