
Submitted:
29 January 2025
Posted:
29 January 2025
You are already at the latest version
Abstract
Bioelectric membrane potentials regulate cellular growth, differentiation, and movement. Disruptions in bioelectric signaling are strongly linked to cancer development, particularly in breast cancer, where ion channel dysfunction and neuroreceptor-related pathways play significant roles in the cell cycle, epithelial-mesenchymal transition, angiogenesis, inflammation, the tumor microenvironment, and tumor progression. Neuroreceptors are critical not only in initiating and advancing cancer but also in conferring resistance to treatments. Advances in understanding these biological mechanisms could lead to more cost-effective and less invasive therapeutic strategies to treat tumors. This review explores the expanding evidence connecting bioelectric activity to breast cancer, focusing on neuroreceptor pharmacology as a transformative therapeutic approach. Investigating how neuroreceptor pharmacology-based modulation of bioelectricity affects breast cancer progression and integrating these insights into therapeutic development offers a promising path for addressing treatment challenges and improving precision in managing aggressive cancer subtypes.
Keywords:
bioelectric signalling
; neuroreceptor pharmacology
; breast cancer
; therapeutic strategies
1. Introduction
Cancer remains a major global health issue, causing millions of deaths each year and placing a substantial social and economic strain on communities worldwide. This deadly disease is characterized by the uncontrolled growth of abnormal cells that can invade nearby tissues and spread to other body parts, known as metastasis. In 2024, approximately 2,001,140 new cancer cases and 611,720 cancer-related deaths are anticipated in the U.S. The overall cancer mortality rate has been declining, reflecting advancements in early detection and treatment [1]. Recently, cancer treatment has shifted toward targeted therapies and immunotherapies, designed to attack cancer cells while sparing healthy tissue. These innovations have significantly improved survival rates and patients' quality of life [2]. According to the American Cancer Society's "Cancer Statistics, 2024," breast cancer (BC) is projected to be the most commonly diagnosed cancer in the United States, with an estimated 310,720 new cases in women and 2,790 in men. This underscores the critical need for effective prognostic biomarkers to improve patient outcomes [1]. BC is categorized into several subtypes, including hormone receptor-positive, HER2-positive, and triple-negative BC, each requiring specific treatment strategies. Ductal carcinoma, the most common type of BC, originates in the epithelial cells lining the breast's milk ducts [3,4]. This form of carcinoma can be categorized into ductal carcinoma in situ (DCIS), a non-invasive form where the cancer cells remain confined within the ducts, and invasive ductal carcinoma (IDC), where the cancer cells breach the ductal walls and invade surrounding breast tissue [5]. The relationship between breast carcinoma and cell physiology is deeply intertwined, as alterations in the normal cellular processes, such as cell proliferation, apoptosis, and differentiation, play a critical role in the development and progression of this cancer [6]. Membrane potential is the difference in electrical charge between the inside and outside of a cell, similar to a small battery that powers various cell functions. Membrane potential is generated by the differential distribution of sodium, potassium, calcium, and chloride ions on both sides of the cell [7]. In excitatory cells, like neurons, this potential is actively maintained and changes to transmit signals, while in non-excitatory cells, it helps regulate cell proliferation and apoptosis [8]. In cancer, alterations in membrane potential can disrupt normal cellular functions, promoting uncontrolled cell growth and metastasis [9,10,11]. Changes in membrane potential particularly membrane depolarization, ion channel activity, and signal transduction pathways can disrupt normal cell function, leading to uncontrolled cell growth and the potential for metastasis [12,13]. Understanding these physiological changes is crucial for developing targeted therapies that can correct or inhibit the abnormal cellular behaviors driving breast carcinoma. Neurotransmitters are chemicals released by nerve cells that regulate neuronal activity by interacting with specific receptors [14]. They are essential for maintaining the physiological functions of tissues and organs, and imbalances or disruptions in their activity are linked to various pathological conditions [15]. Neurotransmitters and their associated neuroreceptors play crucial roles in modulating membrane potentials in both excitable and non-excitable cells [16]. In excitable cells, such as neurons and muscle cells, neurotransmitters bind to specific neuroreceptors, triggering the opening of ion channels. This results in changes to the membrane potential, enabling the generation of action potentials and signal transmission [17,18]. In non-excitable cells, neurotransmitters influence intracellular signaling pathways by modulating ion fluxes, which affect processes such as secretion, migration, and metabolic regulation [19]. It is important to note that the activation of neuroreceptors by neurotransmitters always impacts membrane potential, whether in excitable or non-excitable cells. This ability to relay, amplify, and fine-tune electrical signals makes neurotransmitters essential for maintaining cellular communication and function across diverse systems. Despite advances in treatment, there remains an urgent need for fundamental and translational research to understand the underlying mechanisms of BC better, improve early detection, and develop more effective therapies to reduce the global health and economic burden of this disease. Investigating membrane electrical activities has emerged as a promising area of research, offering new insights into the role of neuroreceptors and membrane potential in cancer. For example, nanomaterials can modulate membrane potential and ion channel activity, thereby altering critical cellular behaviors such as migration and survival, which are essential processes in cancer progression [20]. Scientific review articles are crucial for synthesizing existing research, and providing researchers and clinicians with a comprehensive understanding of complex pathophysiological conditions. These reviews distill key findings, identify knowledge gaps, and highlight potential treatment strategies, ultimately guiding more informed and effective clinical decision-making. Unfortunately, there is currently no comprehensive review that specifically addresses the relationship between membrane potential, neuroreceptors, and cancer in breast cells. This lack of updated information leaves a significant gap in our understanding of how cellular electrophysiology influences cancer progression in these cells. Our review aims to fill this critical gap by synthesizing recent research on membrane potential, neuroreceptor pharmacology, and their roles in breast cell transformation and cancer development. This study offers essential insights that will inform future research and guide BC therapeutic approaches, benefiting foundational researchers and clinicians.
2. Bioelectric Membrane Potential in Breast Cancer
Changes in the resting membrane potential (RMP) and membrane electrical activities have been identified as key factors in breast cancer development [21,22]. Specific ion channels, such as potassium and sodium, contribute to cell proliferation and metastasis [23]. These channels modulate intracellular signaling pathways, including those involving calcium and neuroreceptors, linking bioelectricity to oncogenic processes. Furthermore, tumor cells exploit altered bioelectric signals to evade apoptosis and enhance invasive capabilities [24]. Membrane potential depolarization has been linked to cancer progression across various tissue types, including breast, liver, and ovarian cells [22]. Vm depolarization drives tumor progression and triggers DNA synthesis and mitosis [25]. The eukaryotic cell cycle consists of G1, S, G2, and M phases, with mitosis (M phase) typically followed by cytokinesis and DNA replication occurring during the S phase [26]. At the G1/S transition, Vm depolarization prepares cells to enter the M phase [22], and, quiescent cells in the G0 phase display increased mitotic activity following Vm depolarization, reinforcing its role in regulating cell division [22,27]. In metastasis, tumor cells lose adhesion, migrate, invade, and travel through vascular or lymphatic systems to form secondary tumors [28]. Vm plays a critical role in cell migration by regulating ion and water movement, crucial for metastatic progression [29]. Figure 1 provides a schematic depiction of how membrane potential fluctuates during the cell cycle. These variations are regulated by the synchronized opening and closing of specific ion channels. This coordination plays a vital role in enabling the progression from the G0/G1 phase to the S phase. During the S phase, the membrane potential usually becomes more depolarized. Similarly, mitosis is marked by additional depolarization, which continues until cell division concludes. Following this, the membrane potential reverts to a repolarized state typical of the G0/G1 phase. In BC cells, depolarization of the membrane potential is often associated with an increased rate of cell proliferation. This is partly due to the influence of membrane potential on the activity of cyclin-dependent kinases (CDKs) and other cell cycle regulators. Depolarized membrane potentials can also enhance the uptake of nutrients and growth factors, further promoting the proliferation of cancer cells [30]. For instance, the activity of sodium channels, which contribute to membrane depolarization, has been linked to increased cancer cell growth by activating various signaling pathways, including the MAPK and PI3K/Akt pathways [31]. Apoptosis, or programmed cell death, is a crucial mechanism for eliminating damaged or abnormal cells. In cancer, the evasion of apoptosis is a hallmark of disease progression. Membrane potential plays a critical role in regulating apoptosis, with alterations often leading to resistance to cell death in BC cells. Hyperpolarization and repolarization of the membrane potential are generally associated with pro-apoptotic signals, whereas depolarization can contribute to anti-apoptotic mechanisms [32].
Dysregulation of ion channels that regulate membrane potential in BC cells can inhibit apoptosis, enabling these cells to survive and proliferate despite treatment interventions [33]. Metastasis, the spread of cancer cells from the primary tumor to distant organs, remains a major cause of cancer-related deaths. Alterations in membrane potential are closely linked to the metastatic behavior of BC cells [22]. Depolarized membrane potentials are often associated with increased motility, invasiveness, and the ability to migrate through the extracellular matrix. The RMP in BC cells varies between ̶ 40 mV and ̶ 15 mV based on cell type and aggressiveness [22]. For triple-negative breast cancer cells (MDA-MB-231, MDA-MB-468, and MCF-7), the RMP ranges between ̶ 40 mV and ̶ 20 mV, reflecting distinct electrical properties when compared to normal cells [22,34]. In patient-derived breast cancer cells, the RMP is reported to be around ̶ 13 mV, which is significantly depolarized compared to normal mammary epithelial cells [35].
3. Neuroreceptors, Neurotransmitters, Membrane Potential, and Breast Cancer
Neurotransmitters and neuroreceptors are gaining recognition for their significant roles in cancer-related bioelectric signaling. These neuroreceptors modulate ion channels, leading to changes in membrane potential that drive signaling pathways promoting tumor growth and therapy resistance [22,27]. Research has focused on pharmacological strategies to modulate neuroreceptor activity to restore bioelectric function and suppress tumor progression. Promising approaches include peptide-based therapies and channel blockers targeting bioelectric and molecular mechanisms [36]. The connection between bioelectric membrane potentials and cancer, particularly breast cancer, highlights the potential of neuroreceptor-focused therapies. Figure 2 highlights the chemical structures of two neurotransmitters, gamma-aminobutyric acid (GABA) and acetylcholine, which alter the membrane potential in excitable and non-excitable cells. GABA is a simple amino acid neurotransmitter. Its structure includes a carboxylic acid group (-COOH) at one end and an amino group (-NH2) at the other, connected by a three-carbon backbone [37]. The carboxylic acid group, depicted on the left side of the molecule, features red oxygen atoms and a hydroxyl (-OH) group. The amino group on the opposite end includes a nitrogen atom bonded to two hydrogen atoms. This unique configuration underpins GABA's function as the primary inhibitory neurotransmitter in the central nervous system, where it helps regulate neural excitability and prevent overstimulation [38]. Acetylcholine, in contrast, has a more complex structure. It contains a quaternary ammonium group, where a positively charged nitrogen atom is bound to four organic groups. An acetyl group (-COOCH3) is linked through an ester bond, represented by red oxygen atoms connecting the acetyl group to the molecule [39]. Acetylcholine is vital for muscle activation and significantly functions in the autonomic nervous system, influencing various physiological processes [40]. The structural differences between these neurotransmitters illustrate their diverse biochemical roles. GABA’s linear structure, with both acidic and basic functional groups, allows it to act as a zwitterion under physiological conditions. Meanwhile, acetylcholine's positively charged quaternary ammonium group and ester group facilitate its role in rapid synaptic signaling. These variations underscore the structural diversity that enables distinct neurotransmitter functions.
Cell membrane receptors, such as ligand-gated ion channels and G protein-coupled receptors (GPCRs), play critical roles in regulating cellular processes by influencing membrane potential [41]. Ligand-gated ion Channels are integral membrane proteins that form ion channels spanning the plasma membrane [42]. These channels are composed of subunits that create a pore. When a specific ligand, such as a neurotransmitter, binds to the extracellular domain, the channel undergoes a conformational change, opening the pore. This allows ions such as sodium (Na⁺), calcium (Ca²⁺), potassium (K⁺), or chloride (Cl⁻) to pass through, following their electrochemical gradients. The movement of these ions alters the membrane potential. For example, the influx of Na⁺ or Ca²⁺ often causes depolarization (an increase in positive charge inside the cell), while the influx of Cl⁻ or efflux of K⁺ leads to hyperpolarization or repolarization, returning the cell to its resting potential [43]. GPCRs, on the other hand, are characterized by their seven-transmembrane domain structure. Upon ligand binding, the receptor undergoes a conformational change that activates associated intracellular G proteins. These G proteins, in turn, regulate various downstream signaling pathways, such as the production of cyclic AMP (cAMP) by adenylyl cyclase [44]. GPCR signaling can also modulate calcium ion channels, influencing intracellular calcium levels and contributing to depolarization [45]. Additionally, they activate protein kinases that regulate gene expression and other cellular responses. The two receptor types differ significantly in their effects on membrane potential. Ligand-gated ion channels directly and rapidly alter membrane potential by allowing immediate ion flux. GPCRs, however, produce indirect and slower effects by initiating complex intracellular signaling cascades that eventually modulate ion channel activity [46]. While ligand-gated ion channels are essential for fast synaptic transmission, GPCRs govern various physiological processes over a broader timescale. Figure 3 compares Ion Channel Receptors and G Protein-Coupled Receptors (GPCRs), highlighting two distinct cell signaling mechanisms through membrane receptors. On the left, ligand-gated ion channels enable the movement of ions (e.g., Na⁺, K⁺, Ca²⁺, Cl⁻) across the membrane, resulting in processes such as depolarization or repolarization. On the right, GPCRs are activated by ligand binding, triggering intracellular signaling pathways that involve G proteins, cAMP synthesis, kinase activation, and the regulation of Ca²⁺ ion channels. These pathways lead to effects like membrane depolarization and changes in gene expressions. Epinephrine (adrenaline) and norepinephrine (noradrenaline) are catecholamine neurotransmitters released during the fight-or-flight response, binding to adrenergic receptors [47]. Research indicates that breast cancer tissues often overexpress β-adrenergic receptors, linking these stress-related pathways to tumor progression [48]. For instance, temperature fluctuations (ranging from 22°C to 30°C) induce stress that activates β-adrenergic receptors, influencing the sensitivity of tumors to therapy in a murine model [49]. Local mammary tumor sympathetic innervation, which elevates norepinephrine turnover, appears to play a larger role in tumor growth than circulating norepinephrine. Activation of β2-adrenergic receptors promotes angiogenesis and tumor growth by upregulating vascular endothelial growth factor (VEGF) and matrix metalloproteases (MMP2, MMP9), facilitating metastatic processes [50]. Additionally, β2AR signaling may suppress p53-related apoptosis and cause DNA damage, further exacerbating cancer progression [51].
Epinephrine (adrenaline) and norepinephrine (noradrenaline) are catecholamine neurotransmitters released during the fight-or-flight response, binding to adrenergic receptors [47]. Research indicates that breast cancer tissues often overexpress β-adrenergic receptors, linking these stress-related pathways to tumor progression [48]. For instance, temperature fluctuations (ranging from 22°C to 30°C) induce stress that activates β-adrenergic receptors, influencing the sensitivity of tumors to therapy in a murine model [49]. Local mammary tumor sympathetic innervation, which elevates norepinephrine turnover, appears to play a larger role in tumor growth than circulating norepinephrine. Activation of β2-adrenergic receptors promotes angiogenesis and tumor growth by upregulating vascular endothelial growth factor (VEGF) and matrix metalloproteases (MMP2, MMP9), facilitating metastatic processes [50]. Additionally, β2AR signaling may suppress p53-related apoptosis and cause DNA damage, further exacerbating cancer progression [51]. Stress also increases the risk of cancer recurrence. Mechanisms involve the release of S100A8/A9 proteins via β2-adrenergic activation, triggering dormant cancer cells and promoting tumor reawakening [52]. In metastatic breast cancer, sympathetic nerve activation in bones enhances bone vascular density, creating a supportive environment for tumor cells [53]. Preclinical studies suggest beta-blockers may reduce breast cancer growth and metastasis, but clinical outcomes have been mixed [54]. A 2017 meta-analysis involving over 18,000 breast cancer patients found no significant impact of beta blockers on overall or cancer-specific mortality or recurrence rates [55]. However, the benefits for specific breast cancer subtypes remain unclear. Recent studies have also shown mixed results, with some suggesting a reduction in recurrence and metastasis in triple-negative breast cancer patients and others finding no improvement in overall survival or even worsened outcomes in HER2-positive advanced breast cancer [56]. Propranolol, a nonselective beta blocker, has demonstrated anti-tumor effects in preclinical and early clinical studies, including reduced tumor cell proliferation, increased immune cell infiltration, and enhanced apoptosis [57]. Combining beta blockers with other therapies, such as chemotherapy or non-chemotherapy agents like naltrexone, has shown promise in preclinical models [55]. These combinations may enhance treatment efficacy, inhibit angiogenesis, and improve survival rates. β2-adrenergic receptors may modulate resistance to trastuzumab, a common HER2-targeted therapy [58]. Dexmedetomidine, a commonly used anesthetic, has been reported to promote tumor growth, migration, and metastasis in certain breast cancer models by activating the α2B-adrenoceptor/ERK signaling pathway. However, these findings are model-specific and may not be universally applicable across all breast cancer types or experimental conditions [59]. Despite these findings, no conclusive evidence has emerged to discourage its clinical use. Conversely, tramadol, an opioid analgesic, has demonstrated the ability to inhibit breast cancer proliferation, migration, and invasion by blocking the α2-adrenoceptor signaling pathway, with potential benefits in combination therapy, especially for triple-negative breast cancer [60]. Similarly, the α2-adrenoceptor antagonist rauwolscine has shown anti-tumor effects in preclinical studies, including reduced tumor growth in models of human breast cancer, suggesting its promise as a therapeutic agent [55].
Acetylcholine (ACh) is a neurotransmitter in regulating cellular processes like proliferation, differentiation, and apoptosis [61]. Its receptors, acetylcholine receptors (AChRs), are divided into two types: muscarinic (mAChRs), which activate slowly via G protein-coupled mechanisms, and nicotinic (nAChRs), which act rapidly as ion channels [62]. In breast cancer, studies have shown that nicotine binding to nAChRs promotes pathways like EGFR and Src signaling, contributing to cancer progression [63]. High α9-nAChR expression is linked to advanced triple-negative breast tumors, and α7-nAChR is also implicated, suggesting that targeting specific AChR subtypes could be a promising therapeutic strategy [64]. Similarly, mAChRs are upregulated in breast tumors but absent in normal tissues, with evidence showing that mAChR agonists may suppress breast tumor growth effectively, even at low doses [65]. Serotonin (5-HT), synthesized from tryptophan, regulates various physiological processes, including epithelial homeostasis in the breast [66]. Research indicates that serotonin influences immune signaling and promotes the growth of breast cancer cells. Elevated expression of serotonin receptors, such as 5HTR2A and 5HTR3A, has been observed in breast tumor tissues compared to non-tumor tissues [67]. Serotonin also facilitates angiogenesis, proliferation, and invasion via receptors like 5-HT2A and 5-HT7, contributing to the mitogenic and oncogenic effects of 5-HT in breast cancer [68]. Tramadol, a pain medication, has shown anti-tumor effects, potentially by interacting with serotonin receptors and reducing breast cancer recurrence post-surgery [69]. Additionally, serotonin antagonists have demonstrated the ability to diminish breast cancer stem cell viability, suggesting serotonin production in tumors may correlate with poor prognosis [70]. The relationship between serotonin-raising medications, such as SSRIs, and breast cancer remains contentious. While some studies suggest increased breast cancer risk and mortality associated with SSRI use, others find no significant association. Preclinical research has also indicated the potential benefits of serotonin reuptake inhibition in reducing tumor growth [71]. These conflicting findings highlight the need for further investigation into serotonin's role in breast cancer progression and therapeutic potential. Breast cancer often overexpresses prolactin, a hormone linked to tumor growth, metastasis, and chemoresistance [72]. Dopamine, a neurotransmitter, regulates prolactin and may influence breast cancer outcomes [73]. While dopamine and its receptor agonists appear to inhibit tumor growth in various cancers, they do not consistently reduce proliferation or invasion in breast cancer cells [55]. The effectiveness of dopamine in suppressing tumors likely depends on factors such as tumor type, receptor expression, and dosage. One key mechanism of dopamine's anti-tumor effects is reduced angiogenesis. Activation of the DRD1/cGMP/PKG pathway has been shown to cause growth arrest and shrink tumors in breast cancer models [74]. Research has also explored dopamine receptor agonists like cabergoline, which inhibits prolactin secretion, but results have been inconclusive [75]. Additionally, phenothiazines, antipsychotic drugs, have shown promise by reducing the invasion and proliferation of triple-negative breast cancer cells and reducing tumor growth in animal models [76]. Despite these findings, ongoing research is needed to better understand the potential of dopaminergic drugs in breast cancer therapy, especially considering possible side effects.
GABA, the brain's primary inhibitory neurotransmitter, has been shown to promote breast cancer cell proliferation and migration [77]. The GABAA receptor alpha3, normally found in the adult brain, is expressed in breast cancer tissue, and higher expression correlates with poorer survival outcomes [78]. This receptor activates the AKT pathway, enhancing breast cancer cell invasion and metastasis, as observed in mouse models [79]. Studies have also found that GABAA receptor activation increases brain metastasis in breast cancer patients, making it a potential therapeutic target. Propofol, a drug that activates GABAA receptors, has been linked to breast cancer cell migration [80]. Epidemiological studies suggest that benzodiazepine use may increase the risk of breast cancer in a dose-dependent manner [81]. GABA mimics, often used to alleviate chemotherapy-induced nerve pain, could potentially contribute to breast cancer metastasis, raising concerns about their impact [82]. Additionally, neurotensin, overexpressed in about a third of primary breast tumors, promotes cancer cell proliferation, migration, and resistance to apoptosis [83]. Neurotensin receptor antagonists may offer a treatment approach. Neuropeptide Y, which plays a role in angiogenesis, also supports breast cancer proliferation and metastasis, further suggesting potential therapeutic targets [83]. Histamine, a key neurotransmitter involved in allergic reactions, also plays a role in breast cancer growth [88]. Its effects are mediated through four G-protein-coupled receptor subtypes, with the H4 receptor being particularly significant in immune cells and breast cancer tissue [85]. Studies have shown that high levels of histamine decarboxylase correlate with better survival outcomes in breast cancer patients. In animal models, histamine administration reduced tumor growth and promoted apoptosis in triple-negative breast cancer cells (4T1 model). Research suggests that the H4 receptor may serve as a biomarker for predicting prognosis in triple-negative breast cancer [86]. Analysis from the Cancer Genome Atlas indicates that the H4 receptor is less expressed in basal-like/triple-negative breast cancers compared to other subtypes [87]. However, higher expression of this receptor in triple-negative breast cancer is associated with improved progression-free survival, fewer lymph node metastases, and better overall survival. These findings highlight the potential of the H4 receptor as a prognostic marker for breast cancer. In a study of 1,419 primary breast tumors, overexpression of neurotensin receptor-1 (NTS-1) was found in approximately one-third of the cases [55]. By activating this receptor, Neurotensin promotes tumor cell proliferation, invasion, and migration, and inhibits apoptosis. Antagonists of the neurotensin receptor may help treat tumors with NTS-1 overexpression. Estrogen upregulates neurotensin in normal epithelial breast cells, and in breast cancer, increased NTS-1 expression leads to enhanced migration and invasion [88]. High NTS-1 expression is linked to worse tumor grade, size, and higher metastatic lymph node count. Neuropeptide Y (NPY), a 36-amino-acid neuropeptide, is involved in various biological processes, including the regulation of bone metabolism [89]. Its receptors are overexpressed in breast cancer metastasis. NPY promotes breast cancer cell proliferation and metastasis, partly by facilitating angiogenesis through effects on vascular smooth muscle and VEGF [90]. Additionally, NPY and its receptors have been linked to both breast cancer and osteoporosis, with the Y1 receptor being suggested as a potential target for treatments combining stem cell therapy for both conditions. Immune checkpoint blockade therapy has become an important treatment for cancers like triple-negative breast cancer. Research is focused on enhancing the effectiveness of these therapies by modifying the tumor microenvironment, with neurotransmitters playing a significant role. Specifically, targeting tumor-associated macrophages to reduce their suppression of antitumor T-cell activity could improve immunotherapy outcomes in breast cancer [91]. Monoamine oxidase A (MAOA), an enzyme involved in regulating neurotransmitters like serotonin and dopamine, has been linked to cancer progression. Inhibitors of MAOA, which are FDA-approved for conditions like depression and Parkinson's disease, have shown potential in reducing tumor metastasis [92]. MAOA is known to promote epithelial-to-mesenchymal transition (EMT) and metastasis in cancers, including prostate cancer. Studies indicate that inhibiting MAOA may enhance antitumor immune responses, reduce immune suppression, and improve outcomes. Combining MAOA inhibitors with anti-PD-1 therapies has shown synergistic effects in preclinical models, suggesting that MAOIs could suppress tumor growth and metastasis in breast cancer. Table 1 presents a comprehensive list of various neuroreceptors, their corresponding neurotransmitters, and their effects on target cells and membrane potential.
4. Neuroreceptor Pharmacology and Therapeutic Advances
Venlafaxine, a serotonin-norepinephrine reuptake inhibitor (SNRI), has been extensively studied for its potential to alleviate hot flashes among breast cancer survivors [93]. This was notably explored in the NCT00198250 trial, completed in 2005 [55]. Similarly, solifenacin, a muscarinic acetylcholine receptor antagonist, is under investigation for its efficacy in managing hot flashes, compared with clonidine, although its study (NCT01530373) is ongoing but not recruiting participants [55]. Imipramine, a tricyclic antidepressant (TCA), is being assessed for its influence on biomarkers and cell proliferation in estrogen receptor-positive and triple-negative breast cancer (NCT03122444) [55]. Meanwhile, the ILIAD study (NCT02861859) demonstrated that olanzapine, an atypical antipsychotic, effectively reduces chemotherapy-induced nausea and relieves patients undergoing treatment [55]. Duloxetine, another SNRI, has shown promise in mitigating musculoskeletal pain and menopausal symptoms among patients using aromatase inhibitors, as evidenced by the NCT01028352 trial [55]. Beta-blockers like propranolol are also under investigation for their potential to influence tumor growth and immune responses (NCT02596867, NCT02013492). Dexmedetomidine, an alpha-2 adrenergic agonist, is being evaluated for its impact on breast cancer recurrence, metastasis, and postoperative outcomes in multiple studies (NCT03109990, NCT03108937, NCT04454515) [55]. Cabergoline, a dopamine agonist, has been shown to reduce prolactin levels and demonstrates promise in the treatment of metastatic breast cancer, as detailed in NCT01730729 [55].

Table 2.
List of Neuropharmacological Targets, Corresponding Neurotransmitters, and Their Effects on Target Cells and Membrane Potential. NCT: National Clinical Trial.
Table 2.
List of Neuropharmacological Targets, Corresponding Neurotransmitters, and Their Effects on Target Cells and Membrane Potential. NCT: National Clinical Trial.
| Neuropharmacological Identifier | Associated Neurotransmitters | Membrane Potential |
|---|---|---|
| NCT03108937, NCT04454515, NCT03109990, NCT02013492 | Norepinephrine and epinephrine | Depolarization |
| NCT01530373, NCT02312934 | Acetylcholine | Depolarization or Repolarization |
| NCT02312934 NCT03122444, NCT00198250 | Serotonin | Depolarization |
| NCT01730729, NCT02312934, NCT02861859 | Dopamine | Depolarization |
These studies reflect the dynamic approaches aimed at enhancing cancer care and improving patients’ quality of life by targeting the neurological pathways involved in disease progression and treatment side effects. Beyond these medications, advancements in understanding neurotransmitter signaling open new opportunities for drug repurposing. Beta-blockers, monoamine oxidase inhibitors, serotonin receptor antagonists, and other neuroactive agents offer promising avenues for combination therapies. Emerging research also supports integrating these pharmacological strategies with immunotherapies and conventional treatments to achieve synergistic effects. For example, leveraging the immune-modulating properties of beta blockers could complement immunotherapy in inhibiting tumor progression. Similarly, agents like duloxetine could provide symptomatic relief and potential tumor-modulating effects, broadening their clinical utility. Continued clinical and preclinical studies are critical to validating these innovative approaches. These efforts may redefine the role of neurotransmitter pathways in cancer therapy and further elucidate their impact on treatment resistance, disease recurrence, and overall survival outcomes.
5. Future Directions and Challenges
The future of investigating neurotransmitter-induced changes in membrane potential for breast cancer therapy lies in identifying specific bioelectric signatures, developing targeted ion channel modulators, and combining bioelectric therapies with traditional treatments. We can better understand how membrane potential affects cancer cell behavior and devise more precise and effective treatments through advanced imaging, multi-omics approaches, personalized medicine, animal models, and computational tools. Research into bioelectricity and cancer has seen rapid advancements, integrating nanotechnology and advanced imaging techniques providing new insights into bioelectric dynamics in real time. To further enhance our understanding, future studies should prioritize:
- Identifying bioelectric signatures for different breast cancer subtypes: Identifying bioelectric signatures in breast cancer subtypes can be improved using voltage-sensitive dyes for membrane potential monitoring, patch-clamp techniques for ion channel activity, and single-cell transcriptomics to link gene expression with bioelectric signaling. Combining these with imaging tools like fluorescence microscopy or optogenetics helps reveal bioelectricity's role in tumor behavior, offering insights into new therapeutic targets for personalized treatment strategies, and ultimately supporting personalized treatment strategies for different breast cancer subtypes.
- Developing ion channel modulators targeting cancer cells while minimizing off-target effects: Ion channel modulators show promise as breast cancer therapies by regulating cell functions such as proliferation and migration. For instance, Nav1.7 sodium channels contribute to metastasis, with inhibitors like tetrodotoxin being studied to limit cancer spread. TRPM7, involved in calcium and magnesium influx, is linked to poor prognosis, and inhibitors like NS8593 may slow tumor growth. Additionally, TPCs (TPC1 and TPC2) regulate calcium signaling and tumor progression, with modulators potentially reducing cell proliferation. While preclinical results are promising, further research is needed to evaluate their clinical effectiveness.
- Exploring the combination of bioelectric therapies with conventional treatments in clinical trials: Combining bioelectric therapies with conventional treatments like chemotherapy or immunotherapy is gaining attention in clinical trials. This approach aims to enhance treatment efficacy, overcome drug resistance, and minimize side effects. For example, ion channel modulators could sensitize cancer cells to chemotherapy, while bioelectric stimulation may boost immune response during immunotherapy. Ongoing trials are exploring how these combinations could provide synergistic benefits, leading to more effective and personalized cancer treatments.
While investigating the role of membrane potential in BC is an exciting and evolving area, challenges remain. Understanding the complex interactions among neuropharmacology, membrane potential, and cancer cell signaling is critical. Moreover, developing therapies that selectively modulate membrane potential in cancer cells without affecting normal cells poses a significant challenge. Future research should focus on deciphering how membrane potential influences BC, identifying novel ion channels and bioelectric targets, and translating these findings into effective therapies. Advances in bioelectric imaging and computational modeling may offer deeper insights into membrane potential's role in cancer biology:
- Advanced Imaging: New fluorescent probes and imaging techniques are needed to measure membrane potential and ion channel activity in real-time within live cells and tissues [94].
- Integrative Multi-Omics: Combining genomics, proteomics, and electrophysiology can provide comprehensive models of membrane potential modulation by neuroreceptors and ion channels [95].
- Personalized Medicine: Understanding individual responses to agonists and antagonists can help design personalized therapeutic strategies [96].
- Animal Models and Clinical Trials: Translating laboratory findings into animal models and clinical trials is essential for testing the efficacy of bioelectric-based therapies [97].
- Digital Twin and Computational Electrophysiology: Digital twin models, which replicate patients or biological systems, offer promising tools to address drug resistance in cancer by integrating clinical and multi-omics data to simulate disease progression and treatment outcomes. Initiatives like the PRIMUS project and NIH-funded INCEPTION have utilized digital twins to predict resistance mechanisms in cancers such as pancreatic, breast, and lung cancer. Combining these models with CRISPR screening enables genome-wide identification of resistance-related genes, like ABC transporters or MYC, and simulates their impact on tumor behavior. This approach refines therapeutic strategies, suggests combination therapies, and accelerates drug development by reducing preclinical costs while exploring immune escape mechanisms, paving the way for personalized cancer treatments. Digital twin models offer customized virtual representations of patients, enabling predictive modeling to optimize treatment strategies [98].
These approaches will provide essential tools to explore neurotransmitter-induced changes in membrane potential, aiding in the development of targeted breast cancer therapies.
6. Conclusions
In cancer cells, neurotransmitters influence intracellular signaling pathways by modulating ion fluxes, which affect processes such as secretion, migration, and metabolic regulation. In vivo studies using animal models have also provided insights into the role of neurotransmitters and their receptors in breast cancer progression. For instance, research has shown that sympathetic neurotransmitters, such as catecholamines and neuropeptides, can affect both cancer cell growth and tumor vascularization [99]. Additionally, high expression of nerve growth factor (NGF) and its receptors, TrkA and p75NTR, has been associated with lymph node metastasis in mouse models of breast cancer [100]. These findings suggest that neurotransmitter signaling can influence tumor growth and metastasis, highlighting potential therapeutic targets for breast cancer treatment. Certain drugs also influence neurotransmitters by altering their release, reuptake, or receptor binding, thereby affecting key signaling pathways essential for cell communication, survival, and apoptosis. For example, psychiatric medications, originally developed for mental health disorders, have shown promise in breast cancer models by disrupting tumor biology through mechanisms such as membrane potential alteration, ion channel modulation, and neuroreceptor signaling. For instance, antipsychotics like chlorpromazine promote apoptosis in breast cancer cells by modifying membrane potentials and calcium flux, while antidepressants like fluoxetine inhibit cell viability by disrupting serotonin signaling. Similarly, lithium, a mood stabilizer, suppresses tumor growth by modulating GSK-3β signaling and inducing apoptosis [101].
These observations underscore understanding the influence of neuroreceptor pharmacology on breast cancer is crucial for advancing our knowledge of breast cancer biology and developing innovative therapeutic strategies. This review emphasizes the intricate role of neuroreceptor pharmacology in breast cancer and the importance of integrating bioelectric membrane potential insights for future therapeutic advancements. By exploring the impacts of common medications and interventions on tumor biology, particularly about stress, exercise, and the gut microbiome, a more comprehensive understanding of breast cancer dynamics can be achieved. Targeting ion channels and neuroreceptor pathways offers a promising frontier in cancer therapy, particularly for aggressive subtypes like triple-negative breast cancer. Understanding how neuroreceptor pharmacology affects breast cancer biology is crucial for advancing therapeutic strategies. Specifically, exploring the impact of commonly used medications, such as beta-blockers, SSRIs, and MAOIs, as well as anesthesia protocols in breast cancer surgeries, is vital for understanding their potential influence—whether beneficial, harmful, or neutral—on cancer progression. Neuroreceptor signaling pathways, while adding complexity to breast cancer treatment and prevention strategies, also present promising therapeutic opportunities, particularly through their influence on the tumor microenvironment. These pathways regulate key processes such as cell proliferation, migration, and immune modulation, which can either promote or inhibit tumor progression depending on the context. For example, while exercise is a well-recommended preventive measure, it also triggers the release of adrenaline, which activates β2-adrenergic receptors. This signaling, associated with stress, can potentially worsen cancer progression. Researchers suggest, combining exercise with beta-blockers can mitigate the negative effects of adrenergic signaling on cancer progression by targeting complementary mechanisms. Adrenergic signaling, driven by stress hormones like adrenaline and noradrenaline, can promote tumor growth, metastasis, and angiogenesis by activating β-adrenergic receptors on cancer cells and within the tumor microenvironment. Beta-blockers inhibit these receptors, preventing the pro-tumor effects of adrenergic signaling. Psychological stress, driven by beta-adrenergic signaling, is also linked to poor prognosis, and interventions like cognitive behavioral therapy or meditation have demonstrated benefits by reducing inflammation and improving stress markers. Furthermore, the gut microbiome’s influence on neuroactive substances like dopamine and serotonin intersects with neuroreceptor pharmacology. This suggests that microbiota modulation could influence breast cancer outcomes and treatment side effects. Recent molecular experiments have identified that sensory neurons in TNBC tumors influence tumor cell migration through axon guidance molecules, underscoring the role of neuroreceptor signaling in metastasis. Integrating insights from bioelectric membrane potential changes in breast cancer cells with neuroreceptor pharmacology could significantly enhance therapeutic precision. In particular, understanding the unique bioelectric and molecular properties of TNBC may help improve treatment outcomes. Future research should focus on developing selective ion channel modulators to precisely target aggressive breast cancer subtypes and explore their clinical application.
This review represents a notable advancement over earlier works by incorporating recent findings on the interconnected roles of bioelectric membrane potentials, neuroreceptor pharmacology, and breast cancer. Unlike prior studies, which often examined these topics independently, the manuscript presents an integrated analysis of their influence on cancer progression, metastasis, and therapeutic resistance. It emphasizes innovative therapeutic strategies, including the development of neuroreceptor-targeted drugs and modulation of bioelectric signaling, which are poised to transform cancer treatment approaches. This study also explores emerging areas, such as the impact of stress-related adrenergic signaling and the application of digital twin technologies for personalized medicine. These aspects underscore its originality and contribution to advancing precision oncology. Additionally, it addresses aggressive breast cancer subtypes like triple-negative breast cancer, providing insights into targeted interventions for these challenging cases. By merging the concepts of bioelectricity and cancer biology, this review highlights how bioelectric signaling disruptions, such as membrane depolarization, drive key processes like proliferation, apoptosis, and metastasis. It also introduces novel connections between neurotransmitters, stress pathways, and the tumor microenvironment, offering a comprehensive understanding of their collective role in breast cancer dynamics. With its focus on cutting-edge research and emerging therapeutic tools, the manuscript provides a fresh perspective and fills critical gaps in the current literature.
The mitochondrial membrane potential (ΔΨm) has been increasingly recognized for its role in cancer progression. Mitochondria, as key regulators of energy metabolism, apoptosis, and redox balance, affect various pathways that support tumor growth and survival. Hyperpolarized ΔΨm, frequently observed in cancer cells, meets the heightened metabolic and biosynthetic demands of tumors by boosting ATP production through oxidative phosphorylation, facilitating rapid proliferation. Beyond energy production, changes in ΔΨm are associated with resistance to apoptosis. Additionally, mitochondrial membrane potential influences reactive oxygen species (ROS) generation, which, at moderate levels, can promote cancer by inducing genetic mutations, activating oncogenic pathways, and shaping the tumor microenvironment [102]. While ΔΨm is pivotal in cancer biology, this review focuses on the plasma membrane potential and its role in cancer progression. Mitochondrial potential has a minimal impact on plasma membrane potential due to their distinct functions and compartmentalization. Ion gradients primarily drive plasma membrane potential, whereas mitochondrial potential relates to energy generation. This targeted focus on plasma membrane potential highlights its unique contributions to cancer development and progression, separate from mitochondrial mechanisms.
Author Contributions
Conceptualization, C.M, J.G, C.B., and M.P; methodology, C.M.; software, C.M.; validation, C.M, J.G, C.B., and M.P; formal analysis, C.M.; investigation, C.M, J.G, C.B., and M.P.; resources, C.M, J.G, C.B., and M.P.; data curation, C.M.; writing—original draft preparation, C.M.; writing—review and editing, C.M, J.G, C.B., and M.P.; visualization, C.M.; supervision, C.M, J.G, C.B., and M.P.; project administration, C.M, J.G, C.B., and M.P.; funding acquisition, J.G, C.B., and M.P.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Siegel, Rebecca L., Angela N. Giaquinto, and Ahmedin Jemal. "Cancer statistics, 2024." CA: a cancer journal for clinicians 74, no. 1 (2024): 12-49. [CrossRef]
- Neri, Dario, and Paul M. Sondel. "Immunocytokines for cancer treatment: past, present and future." Current opinion in immunology 40 (2016): 96-102. [CrossRef]
- Kumar, Pankaj, and Rupali Aggarwal. "An overview of triple-negative breast cancer." Archives of gynecology and obstetrics 293 (2016): 247-269. [CrossRef]
- Mir, Manzoor Ahmad, and Hina Qayoom. "Introduction to breast cancer." In Therapeutic potential of cell cycle kinases in breast cancer, pp. 1-22. Singapore: Springer Nature Singapore, 2023.
- Lanyi, Marton. "Malignant and Benign Lobular and Ductal Lesions with Perifocal Reactions." In Mammography: Diagnosis and Pathological Analysis, pp. 145-212. Berlin, Heidelberg: Springer Berlin Heidelberg, 2003. [CrossRef]
- Feng, Yixiao, Mia Spezia, Shifeng Huang, Chengfu Yuan, Zongyue Zeng, Linghuan Zhang, Xiaojuan Ji et al. "Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis." Genes & diseases 5, no. 2 (2018): 77-106. [CrossRef]
- Mahapatra, Chitaranjan, and Ravinder Kumar. "Biophysical Mechanisms of Vaginal Smooth Muscle Contraction: The Role of the Membrane Potential and Ion Channels." Pathophysiology 31, no. 2 (2024): 225-243. [CrossRef]
- An, Qimin, Gengyu Yue, Xiaoxu Yang, Jun Lou, Weixi Shan, Jianhong Ding, Zhe Jin et al. "Pathophysiological role of purinergic P2X receptors in digestive system diseases." Frontiers in Physiology 12 (2021): 781069. [CrossRef]
- Sundelacruz, Sarah, Michael Levin, and David L. Kaplan. "Role of membrane potential in the regulation of cell proliferation and differentiation." Stem cell reviews and reports 5 (2009): 231-246. [CrossRef]
- Déliot, Nadine, and Bruno Constantin. "Plasma membrane calcium channels in cancer: Alterations and consequences for cell proliferation and migration." Biochimica et Biophysica Acta (BBA)-Biomembranes 1848, no. 10 (2015): 2512-2522. [CrossRef]
- Rao, Vidhya R., Mathew Perez-Neut, Simon Kaja, and Saverio Gentile. "Voltage-gated ion channels in cancer cell proliferation." Cancers 7, no. 2 (2015): 849-875. [CrossRef]
- Kunzelmann, Karl. "Ion channels and cancer." The Journal of membrane biology 205 (2005): 159-173. [CrossRef]
- Prevarskaya, Natalia, Roman Skryma, and Yaroslav Shuba. "Ion channels in cancer: are cancer hallmarks oncochannelopathies?." Physiological reviews 98, no. 2 (2018): 559-621. [CrossRef]
- Lauder, Jean M. "Neurotransmitters as growth regulatory signals: role of receptors and second messengers." Trends in neurosciences 16, no. 6 (1993): 233-240. [CrossRef]
- Hnasko, Thomas S., and Robert H. Edwards. "Neurotransmitter corelease: mechanism and physiological role." Annual review of physiology 74, no. 1 (2012): 225-243. [CrossRef]
- Ständer, Sonja, and Thomas A. Luger. "Neuroreceptors and neuromediators." Pruritus (2010): 7-15. [CrossRef]
- Rahmann, Hinrich. "Calcium-ganglioside interactions and modulation of neuronal functions." Current Aspects of the Neurosciences: Volume 4 (1992): 87-125. [CrossRef]
- Brown, A. G., and A. G. Brown. "The Postsynaptic Neuron I: Actions of Neurotransmitters." Nerve Cells and Nervous Systems: An Introduction to Neuroscience (2001): 87-100. [CrossRef]
- Mahaut-Smith, Martyn P., Kirk A. Taylor, and Richard J. Evans. "Calcium Signalling through ligand-gated ion channels such as P2X1 receptors in the platelet and other non-excitable cells." Calcium Entry Pathways in Non-excitable Cells (2016): 305-329. [CrossRef]
- Moreddu, Rosalia. "Nanotechnology and Cancer Bioelectricity: Bridging the Gap Between Biology and Translational Medicine." Advanced Science 11, no. 1 (2024): 2304110. [CrossRef]
- Marino, Andrew A., Ilko G. Iliev, Michael A. Schwalke, Enrique Gonzalez, Kevin C. Marler, and Carol A. Flanagan. "Association between cell membrane potential and breast cancer." Tumor Biology 15, no. 2 (1994): 82-89. [CrossRef]
- Yang, Ming, and William J. Brackenbury. "Membrane potential and cancer progression." Frontiers in physiology 4 (2013): 185. [CrossRef]
- Dai, Jiapei. "The Continuous Relative Deficiency of Intracellular Potassium Is a Core Mechanism for the Occurrence and Metastasis of Tumor Cancer Cells." Natural Science 14, no. 11 (2022): 492-496. [CrossRef]
- Robinson, Andie J., Akhil Jain, Harry G. Sherman, Richard JM Hague, Ruman Rahman, Paola Sanjuan-Alberte, and Frankie J. Rawson. "Toward hijacking bioelectricity in cancer to develop new bioelectronic medicine." Advanced Therapeutics 4, no. 3 (2021): 2000248. [CrossRef]
- Sheth, Maulee, and Leyla Esfandiari. "Bioelectric dysregulation in cancer initiation, promotion, and progression." Frontiers in Oncology 12 (2022): 846917. [CrossRef]
- Wang, Zhixiang. "Cell cycle progression and synchronization: an overview." Cell-Cycle Synchronization: Methods and Protocols (2022): 3-23. [CrossRef]
- Wang, Shiyi, Zaroui Melkoumian, Karen A. Woodfork, Carrie Cather, Ann G. Davidson, William F. Wonderlin, and Jeannine S. Strobl. "Evidence for an early G1 ionic event necessary for cell cycle progression and survival in the MCF-7 human breast carcinoma cell line." Journal of cellular physiology 176, no. 3 (1998): 456-464. [CrossRef]
- Guan, Xiangming. "Cancer metastases: challenges and opportunities." Acta pharmaceutica sinica B 5, no. 5 (2015): 402-418. [CrossRef]
- Fnu, Gulimirerouzi, and Georg F. Weber. "Alterations of ion homeostasis in cancer metastasis: Implications for treatment." Frontiers in Oncology 11 (2021): 765329. [CrossRef]
- Garbern, Jessica C., and Richard T. Lee. "Mitochondria and metabolic transitions in cardiomyocytes: lessons from development for stem cell-derived cardiomyocytes." Stem Cell Research & Therapy 12 (2021): 1-25. [CrossRef]
- Iorio, Jessica, Giulia Petroni, Claudia Duranti, and Elena Lastraioli. "Potassium and sodium channels and the Warburg effect: Biophysical regulation of cancer metabolism." Bioelectricity 1, no. 3 (2019): 188-200. [CrossRef]
- Wang, L., P. Zhou, R. W. Craig, and L. Lu. "Protection from cell death by mcl-1 is mediated by membrane hyperpolarization induced by K+ channel activation." The Journal of membrane biology 172 (1999): 113-120. [CrossRef]
- Tajbakhsh, Amir, Alireza Pasdar, Mehdi Rezaee, Mostafa Fazeli, Saman Soleimanpour, Seyed Mahdi Hassanian, Zahra FarshchiyanYazdi, Tayebe Younesi Rad, Gordon A. Ferns, and Amir Avan. "The current status and perspectives regarding the clinical implication of intracellular calcium in breast cancer." Journal of Cellular Physiology 233, no. 8 (2018): 5623-5641. [CrossRef]
- Quicke, Peter, Yilin Sun, Mar Arias-Garcia, Melina Beykou, Corey D. Acker, Mustafa BA Djamgoz, Chris Bakal, and Amanda J. Foust. "Voltage imaging reveals the dynamic electrical signatures of human breast cancer cells." Communications Biology 5, no. 1 (2022): 1178. [CrossRef]
- Berzingi, Seher, Mackenzie Newman, and Han-Gang Yu. "Altering bioelectricity on inhibition of human breast cancer cells." Cancer cell international 16 (2016): 1-9. [CrossRef]
- Stevens, Edward B., and Gary J. Stephens. "Ion channels as targets in drug discovery: outlook and perspectives." In Ion Channels as Targets in Drug Discovery, pp. 1-34. Cham: Springer International Publishing, 2024. [CrossRef]
- Dugas, Hermann, Christopher Penney, Hermann Dugas, and Christopher Penney. "Bioorganic chemistry of the amino acids." Bioorganic Chemistry: A Chemical Approach to Enzyme Action (1981): 13-92. [CrossRef]
- Akyuz, Enes, Ayse Kristina Polat, Ece Eroglu, Irem Kullu, Efthalia Angelopoulou, and Yam Nath Paudel. "Revisiting the role of neurotransmitters in epilepsy: An updated review." Life sciences 265 (2021): 118826. ttps://doi.org/10.1016/j.lfs.2020.118826.
- Malinak, David, Jan Korabecny, Ondrej Soukup, Lukas Gorecki, Eugenie Nepovimova, Miroslav Psotka, Rafael Dolezal et al. "A review of the synthesis of quaternary acetylcholinesterase reactivators." Current Organic Chemistry 22, no. 16 (2018): 1619-1648. [CrossRef]
- Berntson, Gary G., John T. Cacioppo, and Karen S. Quigley. "Respiratory sinus arrhythmia: Autonomic origins, physiological mechanisms, and psychophysiological implications." Psychophysiology 30, no. 2 (1993): 183-196. [CrossRef]
- Nantel, Francois, and Michel Bouvier. "Receptor regulation." In New Comprehensive Biochemistry, vol. 24, pp. 99-109. Elsevier, 1993.
- Lemoine, Damien, Ruotian Jiang, Antoine Taly, Thierry Chataigneau, Alexandre Specht, and Thomas Grutter. "Ligand-gated ion channels: new insights into neurological disorders and ligand recognition." Chemical reviews 112, no. 12 (2012): 6285-6318. [CrossRef]
- Mahapatra, Chitaranjan, Keith L. Brain, and Rohit Manchanda. "A biophysically constrained computational model of the action potential of mouse urinary bladder smooth muscle." PloS one 13, no. 7 (2018): e0200712. [CrossRef]
- Insel, Paul A., and Rennolds S. Ostrom. "Forskolin as a tool for examining adenylyl cyclase expression, regulation, and G protein signaling." Cellular and molecular neurobiology 23 (2003): 305-314. [CrossRef]
- Striessnig, Jörg, and Nadine J. Ortner. "Ca2+ channel blockers." In Encyclopedia of Molecular Pharmacology, pp. 375-383. Cham: Springer International Publishing, 2022. [CrossRef]
- Di Resta, Chiara, and Andrea Becchetti. "Introduction to ion channels." Integrins and Ion Channels: Molecular Complexes and Signaling (2010): 9-21.
- Ubuka, Takayoshi. "Noradrenaline/adrenaline." In Handbook of Hormones, pp. 1041-1044. Academic Press, 2021.
- Silva, Dany, Clara Quintas, Jorge Gonçalves, and Paula Fresco. "Contribution of adrenergic mechanisms for the stress-induced breast cancer carcinogenesis." Journal of Cellular Physiology 237, no. 4 (2022): 2107-2127. [CrossRef]
- Eng, Jason W-L., Chelsey B. Reed, Kathleen M. Kokolus, Rosemarie Pitoniak, Adam Utley, Mark J. Bucsek, Wen Wee Ma, Elizabeth A. Repasky, and Bonnie L. Hylander. "Housing temperature-induced stress drives therapeutic resistance in murine tumour models through β2-adrenergic receptor activation." Nature communications 6, no. 1 (2015): 6426. [CrossRef]
- quốc Lu’o’ng, Khanh vinh, and Lan Thi Hoàng Nguyễn. "The roles of beta-adrenergic receptors in tumorigenesis and the possible use of beta-adrenergic blockers for cancer treatment: possible genetic and cell-signaling mechanisms." Cancer management and research (2012): 431-445. [CrossRef]
- Strous, Ger J., and Julia A. Schantl. "β-arrestin and Mdm2, unsuspected partners in signaling from the cell surface." Science's STKE 2001, no. 110 (2001): pe41-pe41. [CrossRef]
- Yan, Man, Minying Zheng, Rui Niu, Xiaohui Yang, Shifeng Tian, Linlin Fan, Yuwei Li, and Shiwu Zhang. "Roles of tumor-associated neutrophils in tumor metastasis and its clinical applications." Frontiers in Cell and Developmental Biology 10 (2022): 938289. [CrossRef]
- Conceição, Francisco, Daniela M. Sousa, Joana Paredes, and Meriem Lamghari. "Sympathetic activity in breast cancer and metastasis: partners in crime." Bone research 9, no. 1 (2021): 9. [CrossRef]
- Alicia Luthy, Isabel, Ariana Bruzzone, and Cecilia Perez Pinero. "Adrenergic action in breast cancer." Current Cancer Therapy Reviews 8, no. 2 (2012): 90-99. [CrossRef]
- Jayachandran, Priya, Francesca Battaglin, Carly Strelez, Annika Lenz, Sandra Algaze, Shivani Soni, Jae Ho Lo et al. "Breast cancer and neurotransmitters: emerging insights on mechanisms and therapeutic directions." Oncogene 42, no. 9 (2023): 627-637. [CrossRef]
- Johnston, Stephen RD. "The role of chemotherapy and targeted agents in patients with metastatic breast cancer." European journal of cancer 47 (2011): S38-S47. [CrossRef]
- Pantziarka, Pan, Gauthier Bouche, Vidula Sukhatme, Lydie Meheus, Ilse Rooman, and Vikas P. Sukhatme. "Repurposing Drugs in Oncology (ReDO)—Propranolol as an anti-cancer agent." ecancermedicalscience 10 (2016).
- Liu, D., Z. Yang, T. Wang, H. Chen, Y. Hu, C. Hu, L. Guo et al. "β2-AR signaling controls trastuzumab resistance-dependent pathway." Oncogene 35, no. 1 (2016): 47-58. [CrossRef]
- Xia, M., N. N. Ji, M. L. Duan, J. H. Tong, J. G. Xu, Y. M. Zhang, and S. H. Wang. "Dexmedetomidine regulate the malignancy of breast cancer cells by activating α2-adrenoceptor/ERK signaling pathway." Eur Rev Med Pharmacol Sci 20, no. 16 (2016): 3500-3506.
- Kim, Myoung H., Ju E. Oh, Seho Park, Joo H. Kim, Ki Y. Lee, Sun J. Bai, Hyunjik Song, Hye J. Hwang, Dong W. Kim, and Young C. Yoo. "Tramadol use is associated with enhanced postoperative outcomes in breast cancer patients: a retrospective clinical study with in vitro confirmation." British journal of anaesthesia 123, no. 6 (2019): 865-876. [CrossRef]
- Resende, Rodrigo R., and Avishek Adhikari. "Cholinergic receptor pathways involved in apoptosis, cell proliferation and neuronal differentiation." Cell Communication and Signaling 7 (2009): 1-20. [CrossRef]
- Bertrand, Daniel, and Tanya L. Wallace. "A review of the cholinergic system and therapeutic approaches to treat brain disorders." Behavioral Pharmacology of the Cholinergic System (2020): 1-28. [CrossRef]
- Khodabandeh, Zhila, Mohammad Valilo, Kobra Velaei, and Abbas Pirpour Tazehkand. "The potential role of nicotine in breast cancer initiation, development, angiogenesis, invasion, metastasis, and resistance to therapy." Breast Cancer 29, no. 5 (2022): 778-789.
- Ochirbat, Sonjid, Tzu-Chun Kan, Chun-Chun Hsu, Tzu-Hsuan Huang, Kuo-Hsiang Chuang, Michael Chen, Chun-Chia Cheng, Chun-Chao Chang, Sri Rahayu, and Jungshan Chang. "The angiogenic role of the alpha 9-nicotinic acetylcholine receptor in triple-negative breast cancers." Angiogenesis 27, no. 4 (2024): 827-843. [CrossRef]
- Español, Alejandro, Agustina Salem, Yamila Sanchez, and María Elena Sales. "Breast cancer: Muscarinic receptors as new targets for tumor therapy." World Journal of Clinical Oncology 12, no. 6 (2021): 404. [CrossRef]
- Stull, Malinda A., Vaibhav Pai, Archie J. Vomachka, Aaron M. Marshall, George A. Jacob, and Nelson D. Horseman. "Mammary gland homeostasis employs serotonergic regulation of epithelial tight junctions." Proceedings of the National Academy of Sciences 104, no. 42 (2007): 16708-16713. [CrossRef]
- Olfati, Zahra, Garshasb Rigi, Hajar Vaseghi, Zahra Zamanzadeh, Mojtaba Sohrabi, and Seyed Hesamaldin Hejazi. "Evaluation of serotonin receptors (5HTR2A and 5HTR3A) mRNA expression changes in tumor of breast cancer patients." Medical Journal of the Islamic Republic of Iran 34 (2020): 99. [CrossRef]
- Sarrouilhe, Denis, Jonathan Clarhaut, Norah Defamie, and Marc Mesnil. "Serotonin and cancer: what is the link?." Current molecular medicine 15, no. 1 (2015): 62-77. [CrossRef]
- Bala Bhaskar, S., and M. Manjuladevi. "Drugs, Fluids and Cancer." Textbook of Onco-Anesthesiology (2021): 103-116.
- Chen, Lulu, Shuting Huang, Xiaoxue Wu, Weiling He, and Mei Song. "Serotonin signalling in cancer: Emerging mechanisms and therapeutic opportunities." Clinical and Translational Medicine 14, no. 7 (2024): e1750. [CrossRef]
- Antoszczak, Michał, Anna Markowska, Janina Markowska, and Adam Huczyński. "Antidepressants and antipsychotic agents as repurposable oncological drug candidates." Current medicinal chemistry 28, no. 11 (2021): 2137-2174. [CrossRef]
- Liby, Karen, Bonnie Neltner, Lisa Mohamet, Lindsey Menchen, and Nira Ben-Jonathan. "Prolactin overexpression by MDA-MB-435 human breast cancer cells accelerates tumor growth." Breast cancer research and treatment 79 (2003): 241-252. [CrossRef]
- Ben-Jonathan, Nira, and Robert Hnasko. "Dopamine as a prolactin (PRL) inhibitor." Endocrine reviews 22, no. 6 (2001): 724-763. [CrossRef]
- Jiang, Shu-Heng, Li-Peng Hu, Xu Wang, Jun Li, and Zhi-Gang Zhang. "Neurotransmitters: emerging targets in cancer." Oncogene 39, no. 3 (2020): 503-515. [CrossRef]
- Souteiro, P., and N. Karavitaki. "Dopamine agonist resistant prolactinomas: any alternative medical treatment?." Pituitary 23, no. 1 (2020): 27-37. [CrossRef]
- Feng, Zhanzhan, Yong Xia, Tiantao Gao, Fuyan Xu, Qian Lei, Cuiting Peng, Yufei Yang et al. "The antipsychotic agent trifluoperazine hydrochloride suppresses triple-negative breast cancer tumor growth and brain metastasis by inducing G0/G1 arrest and apoptosis." Cell death & disease 9, no. 10 (2018): 1006.
- Guo, Shenghao, Yanni Gu, Jiayin Qu, and Anne Le. "Bridging the metabolic parallels between neurological diseases and cancer." The Heterogeneity of Cancer Metabolism (2021): 229.
- Gumireddy, Kiranmai, Anping Li, Andrew V. Kossenkov, Masayuki Sakurai, Jinchun Yan, Yan Li, Hua Xu et al. "The mRNA-edited form of GABRA3 suppresses GABRA3-mediated Akt activation and breast cancer metastasis." Nature communications 7, no. 1 (2016): 10715.
- Carnero, Amancio, and Jesus M. Paramio. "The PTEN/PI3K/AKT pathway in vivo, cancer mouse models." Frontiers in oncology 4 (2014): 252.
- Garib, V., K. Lang, B. Niggemann, K. S. Zänker, L. Brandt, and T. Dittmar. "Propofol-induced calcium signalling and actin reorganization within breast carcinoma cells." European journal of anaesthesiology 22, no. 8 (2005): 609-615. [CrossRef]
- Hardwick, Matthew, Djamil Fertikh, Martine Culty, Hua Li, Branislav Vidic, and Vassilios Papadopoulos. "Peripheral-type benzodiazepine receptor (PBR) in human breast cancer: correlation of breast cancer cell aggressive phenotype with PBR expression, nuclear localization, and PBR-mediated cell proliferation and nuclear transport of cholesterol." Cancer research 59, no. 4 (1999): 831-842.
- Marwah, Harneet, Janmejay Pant, Jiten Yadav, Kamal Shah, and Hitesh K. Dewangan. "Biosensor Detection of COVID-19 in Lung Cancer: Hedgehog and Mucin Signaling Insights." Current Pharmaceutical Design 29, no. 43 (2023): 3442-3457. [CrossRef]
- Liberati, Sonia, Maria Beatrice Morelli, Massimo Nabissi, Matteo Santoni, and Giorgio Santoni. "Oncogenic and anti-oncogenic effects of transient receptor potential channels." Current topics in medicinal chemistry 13, no. 3 (2013): 344-366. [CrossRef]
- Medina, Vanina, Máximo Croci, Ernesto Crescenti, Nora Mohamad, Francisca Sanchez-Jiménez, Noelia Massari, Mariel Nuñez et al. "The role of histamine in human mammary carcinogenesis: H3 and H4 receptors as potential therapeutic targets for breast cancer treatment." Cancer biology & therapy 7, no. 1 (2008): 28-35. [CrossRef]
- Sterle, Helena A., Melisa B. Nicoud, Noelia A. Massari, Monica A. Taquez Delgado, María V. Herrero Ducloux, Graciela A. Cremaschi, and Vanina A. Medina. "Immunomodulatory role of histamine H4 receptor in breast cancer." British journal of cancer 120, no. 1 (2019): 128-138. [CrossRef]
- Wang, Ling, Chao Yang, Xin-bo Liu, Li Wang, and Fu-biao Kang. "B7-H4 overexpression contributes to poor prognosis and drug-resistance in triple-negative breast cancer." Cancer Cell International 18 (2018): 1-12. [CrossRef]
- Ospital, Ignacio A., Mónica A. Táquez Delgado, Melisa B. Nicoud, Michelle F. Corrêa, Gustavo A. Borges Fernandes, Isabela W. Andrade, Paolo Lauretta et al. "Therapeutic potential of LINS01 histamine H3 receptor antagonists as antineoplastic agents for triple negative breast cancer." Biomedicine & Pharmacotherapy 174 (2024): 116527. [CrossRef]
- Souazé, Frédérique, Sandra Dupouy, Véronique Viardot-Foucault, Erik Bruyneel, Samir Attoub, Christian Gespach, Anne Gompel, and Patricia Forgez. "Expression of neurotensin and NT1 receptor in human breast cancer: a potential role in tumor progression." Cancer research 66, no. 12 (2006): 6243-6249. [CrossRef]
- Wang, Xiaoyu, Jia Xu, and Qinglin Kang. "Neuromodulation of bone: Role of different peptides and their interactions." Molecular Medicine Reports 23, no. 1 (2021): 1-1. [CrossRef]
- Pouya, F. Danesh, Y. Rasmi, and E. Roshani Asl. "Role of neurotransmitters and neuropeptides in breast cancer metastasis." Biochemistry (Moscow), Supplement Series A: Membrane and Cell Biology 14 (2020): 107-116. [CrossRef]
- Tariq, Muhammad, Jieqiong Zhang, Guikai Liang, Ling Ding, Qiaojun He, and Bo Yang. "Macrophage polarization: anti-cancer strategies to target tumor-associated macrophage in breast cancer." Journal of cellular biochemistry 118, no. 9 (2017): 2484-2501. [CrossRef]
- Arnoux, Alizée, and Luc Dupuis. "Serotonin in Amyotrophic and the Lateral 5-HT2B Sclerosis Receptor." 5-HT2B Receptors: From Molecular Biology to Clinical Applications 35 (2021): 367.
- Joffe, Hadine, Ann Partridge, Anita Giobbie-Hurder, Xiaochun Li, Karleen Habin, Paul Goss, Eric Winer, and Judy Garber. "Augmentation of venlafaxine and selective serotonin reuptake inhibitors with zolpidem improves sleep and quality of life in breast cancer patients with hot flashes: a randomized, double-blind, placebo-controlled trial." Menopause 17, no. 5 (2010): 908-916.
- Przybylo, Magda, Tomasz Borowik, and Marek Langner. "Fluorescence techniques for determination of the membrane potentials in high throughput screening." Journal of fluorescence 20, no. 6 (2010): 1139-1157. [CrossRef]
- Tetzlaff, Svenja K., Ekin Reyhan, Nikolas Layer, C. Peter Bengtson, Alina Heuer, Julian Schroers, Anton J. Faymonville et al. "Characterizing and targeting glioblastoma neuron-tumor networks with retrograde tracing." Cell (2024).
- Yin, Ting, Jingsi Duan, Dong Xu, Mengying Huang, and Deling Yin. "Precision individualized medication strategies and challenges for cardiovascular diseases." Precision Medication 1, no. 1 (2024): 7-15. [CrossRef]
- Velikic, Gordana, Dusan M. Maric, Dusica L. Maric, Gordana Supic, Miljan Puletic, Oliver Dulic, and Danilo Vojvodic. "Harnessing the stem cell niche in regenerative medicine: innovative avenue to combat neurodegenerative diseases." International journal of molecular sciences 25, no. 2 (2024): 993. [CrossRef]
- de Oliveira El-Warrak, Leonardo, and Claudio Miceli de Farias. "Could digital twins be the next revolution in healthcare?." European Journal of Public Health (2024): ckae191. [CrossRef]
- Tilan, Jason, and Joanna Kitlinska. "Sympathetic neurotransmitters and tumor angiogenesis—link between stress and cancer progression." Journal of oncology 2010, no. 1 (2010): 539706. [CrossRef]
- Kuol, Nyanbol, Lily Stojanovska, Vasso Apostolopoulos, and Kulmira Nurgali. "Role of the nervous system in cancer metastasis." Journal of Experimental & Clinical Cancer Research 37 (2018): 1-12.
- Li, Ruo Qi, Xiao Hong Zhao, Qin Zhu, Tao Liu, Hubert Hondermarck, Rick F. Thorne, Xu Dong Zhang, and Jin Nan Gao. "Exploring neurotransmitters and their receptors for breast cancer prevention and treatment." Theranostics 13, no. 3 (2023): 1109. [CrossRef]
- Singh, Tashvinder, Kangan Sharma, Laxmipriya Jena, Prabhsimran Kaur, Sandeep Singh, and Anjana Munshi. "Mitochondrial bioenergetics of breast cancer." Mitochondrion (2024): 101951. [CrossRef]
Figure 1.
It illustrates the dynamic fluctuations in membrane potential throughout the eukaryotic cell cycle, including the G0, G1, S, G2, and M phases. During the G0 phase, cells are in a quiescent state with a stable membrane potential. In the G1 phase, preparation for DNA synthesis begins, followed by the S phase, where hyperpolarization facilitates DNA replication. The G2 phase involves further preparation for mitosis, with depolarization often marking the transition into the M phase. In the M phase, mitosis occurs, typically followed by cytokinesis, completing the cycle.
Figure 1.
It illustrates the dynamic fluctuations in membrane potential throughout the eukaryotic cell cycle, including the G0, G1, S, G2, and M phases. During the G0 phase, cells are in a quiescent state with a stable membrane potential. In the G1 phase, preparation for DNA synthesis begins, followed by the S phase, where hyperpolarization facilitates DNA replication. The G2 phase involves further preparation for mitosis, with depolarization often marking the transition into the M phase. In the M phase, mitosis occurs, typically followed by cytokinesis, completing the cycle.
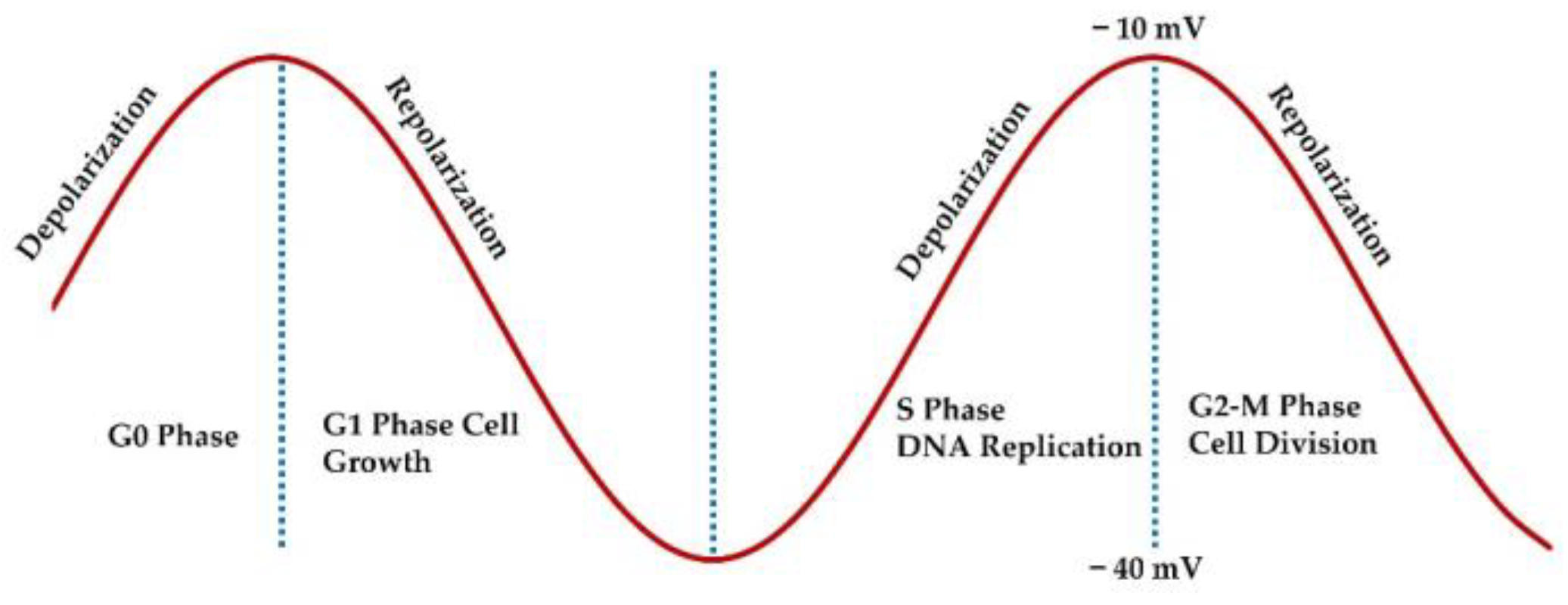
Figure 2.
Structural Comparison of GABA and Acetylcholine Neurotransmitters This figure depicts the molecular structures of two key neurotransmitters, GABA (Gamma-Aminobutyric Acid) and Acetylcholine, highlighting their chemical features and structural differences.
Figure 2.
Structural Comparison of GABA and Acetylcholine Neurotransmitters This figure depicts the molecular structures of two key neurotransmitters, GABA (Gamma-Aminobutyric Acid) and Acetylcholine, highlighting their chemical features and structural differences.

Figure 3.
Comparison of Ion Channel Receptors and G Protein-Coupled Receptors (GPCRs) The figure illustrates two mechanisms of cell signaling through membrane receptors: ion channel receptors and G protein-coupled receptors. On the left, ligand-gated ion channels allow the flow of ions (e.g., Na⁺, K⁺, Ca²⁺, Cl⁻) across the membrane, triggering depolarization or repolarization. On the right, GPCR activation by a ligand initiates intracellular signaling cascades involving G proteins, cAMP production, kinase activation, and modulation of Ca²⁺ ion channels, leading to membrane depolarization and gene regulations.
Figure 3.
Comparison of Ion Channel Receptors and G Protein-Coupled Receptors (GPCRs) The figure illustrates two mechanisms of cell signaling through membrane receptors: ion channel receptors and G protein-coupled receptors. On the left, ligand-gated ion channels allow the flow of ions (e.g., Na⁺, K⁺, Ca²⁺, Cl⁻) across the membrane, triggering depolarization or repolarization. On the right, GPCR activation by a ligand initiates intracellular signaling cascades involving G proteins, cAMP production, kinase activation, and modulation of Ca²⁺ ion channels, leading to membrane depolarization and gene regulations.
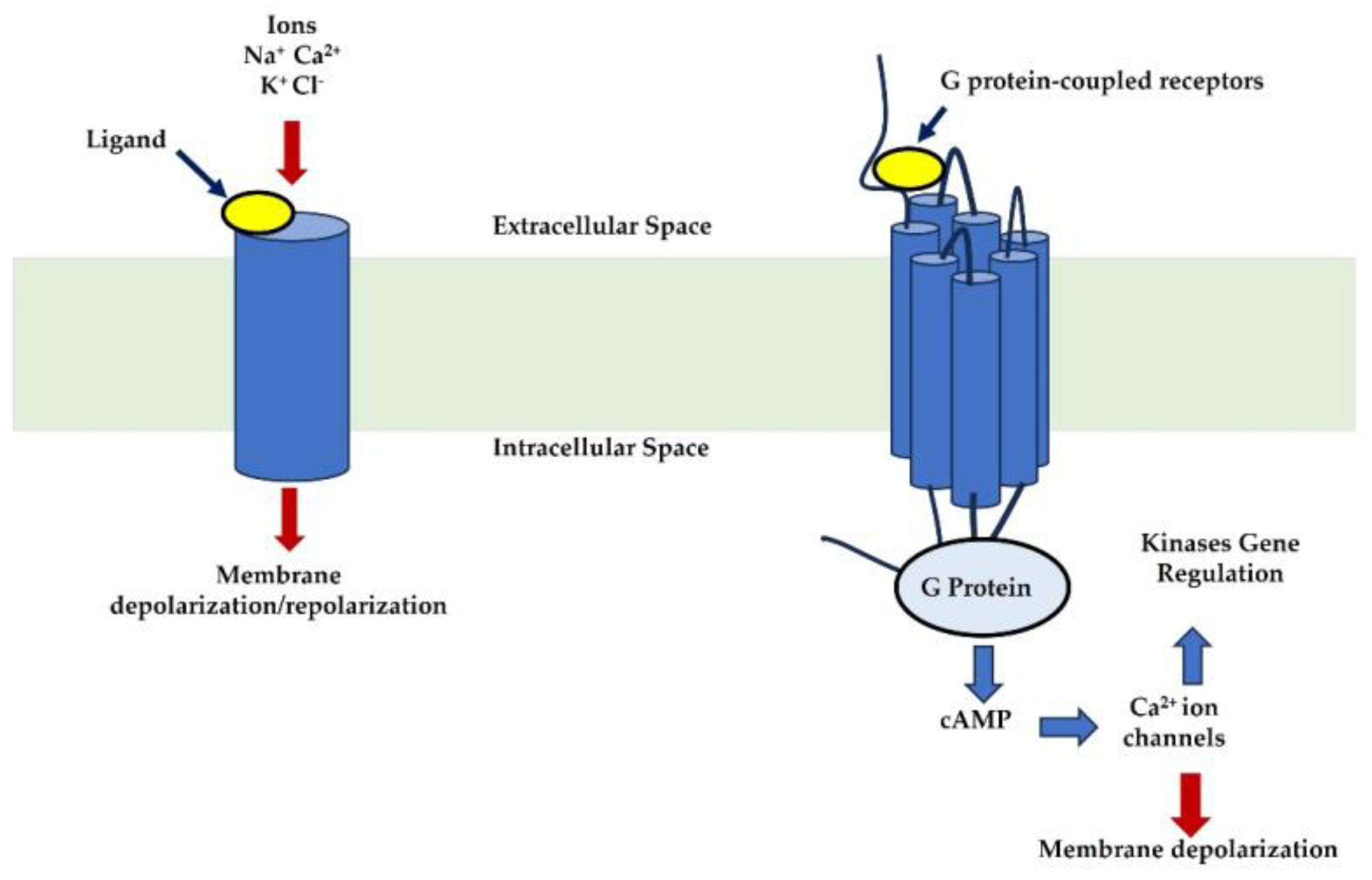
Table 1.
Table of Neuroreceptors, Corresponding Neurotransmitters, and Their Effects on Breast Cancer Cells and Membrane Potential. 5-HT: 5-hydroxytryptamine, GABA: Gamma-Aminobutyric Acid, AKT: Protein Kinase B.
Table 1.
Table of Neuroreceptors, Corresponding Neurotransmitters, and Their Effects on Breast Cancer Cells and Membrane Potential. 5-HT: 5-hydroxytryptamine, GABA: Gamma-Aminobutyric Acid, AKT: Protein Kinase B.
| Neuroreceptor | Associated Neurotransmitters | Expression in Breast Cancer | Functional Role in Breast Cancer | Impact on Membrane Potential | References |
|---|---|---|---|---|---|
| ß-adrenergic receptors | Norepinephrine and epinephrine | Overexpressed in breast cancer tissues | Promotes proliferation, migration, invasion, angiogenesis, and anti-apoptosis | Depolarization | [48,49,50] |
| Nicotinic (nAChRs) and Muscarinic (mAChRs) receptors | Acetylcholine | α9-nAChR and α7-nAChR are highly expressed in triple-negative and advanced breast tumors mAChRs are upregulated in breast tumors but absent in normal breast tissues |
nAChRs enhance epithelial-to-mesenchymal transition, invasion, migration, and stemness mAChRs inhibit tumor growth and promote anti-proliferative effects |
Depolarization or Repolarization | [63,64,65] |
| 5-HT receptors | Serotonin | 5HTR2A and 5HTR3A are overexpressed in breast cancer tissues | Facilitates angiogenesis, proliferation, invasion, and autophagy | Depolarization | [67,68] |
| Dopamine receptors | Dopamine | Variable expression; some subtypes linked to tumor suppression while others promote progression | Modulates proliferation, invasion, and angiogenesis; influences prolactin secretion |
Depolarization | [74,76] |
| GABA receptors | GABA | GABAA receptor α3 is overexpressed in breast cancer, particularly in invasive and metastatic cases | Promotes proliferation, migration, invasion, and activation of the AKT pathway | Repolarization | [78,79] |
| Histamine H4 Receptor | Histamine | High expression correlates with better prognosis in triple-negative breast cancer | Reduces tumor growth, enhances apoptosis, and improves survival | Depolarization or Repolarization | [84,85] |
| Neurotensin Receptor (NTS-1) | Neurotensin | Overexpressed in approximately one-third of primary breast cancers | Promotes proliferation, invasion, migration, and resistance to apoptosis | Depolarization | [88,90] |
| Neuropeptide Y (NPY) Receptors | Neuropeptide Y | Overexpressed in metastatic breast cancer tissues | Stimulates angiogenesis, proliferation, and metastasis | Depolarization | [89,90] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



