
Submitted:
22 January 2025
Posted:
23 January 2025
You are already at the latest version
Abstract
Background/Objectives: Unanticipated difficult airways remain a significant challenge in anesthesia practice and are associated with increased severe complication risk. This study developed and validated a novel predictive tool for identifying unanticipated difficult airways. Methods: This retrospective case-control study analyzed data from 62,111 patients who underwent general anesthesia between 2015 and 2020. Among them, 98 unanticipated difficult airways were identified and matched in a 1:3 ratio with 294 controls. Multivariate logistic regression was utilized to determine key predictors for developing the CLAIR score, which integrates coagulopathy, hypocalcemia, laryngoscopic view, potential airway difficulty, and the presence of inexperienced residents. Results: The incidence of unanticipated difficult airways was 0.16%. The CLAIR score exhibited excellent discriminative performance, with an area under the receiver operating characteristic curve of 0.93. At an optimal cutoff of 4, the score achieved a sensitivity of 86% and a specificity of 90%. Patients were stratified into high (≥6), intermediate (1–5), and low (≤0) risk categories, facilitating tailored airway management strategies. A web-based risk calculator, accessible via a QR code, further enhances its utility in real-time clinical applications. Conclusions: Implementing the CLAIR score holds significant promise for enhancing preoperative risk assessment, optimizing resource allocation, and improving patient safety in diverse anesthesia settings. Future prospective studies and robust external validation are essential to establishing the generalizability of the CLAIR score and confirming its efficacy in reducing airway-related complications. This novel tool represents a paradigm shift in airway management, addressing a longstanding challenge in anesthesia practice with a practical and actionable solution.
Keywords:
patient safety
; preoperative assessment
; predictors
; unanticipated difficult airway
1. Introduction
Securing a patent airway is a fundamental requirement for safe anesthesia. Unanticipated difficult airways, reported in 1.5%–8.5% of cases, pose significant challenges and can result in life-threatening complications [1,2,3,4,5,6]. The 2015 Perioperative and Anesthetic Adverse Events in Thailand (PAAd Thai) study demonstrated a 2.3% incidence of unanticipated difficult intubation [7]. Ineffective management of such cases can lead to severe complications, including emergency surgical airway, airway trauma, hypoxic brain injury, and death due to oxygen deprivation [8,9].
Difficult airway scenarios are multifactorial, involving anatomical, patient history, and medication-related challenges. Comprehensive preoperative assessment, careful planning, and experienced anesthesiologists' management strategies are essential to mitigate risks and ensure patient safety [7,10,11]. Previous studies have primarily focused on the management of these difficulties; the variability in identified risk factors highlights the complexity of the issue [12,13,14,15]. This study aims to clarify the predictive factors associated with unanticipated airway difficulties during anesthesia to enhance patient safety and preparedness for critical situations.
2. Materials and Methods
This retrospective observational case-control study was conducted at an 858-bed tertiary care teaching hospital in southern Thailand from January 2015 to December 2020. All procedures adhered to relevant laws and institutional guidelines. The study protocol was approved by the institutional review board (approval number 63-560-8-1), which granted a waiver for informed consent due to the study’s retrospective nature design. The privacy rights of all participants were rigorously observed.
2.1. Patient Selection
The inclusion comprised patients undergoing general anesthesia with endotracheal intubation for elective or emergency surgeries who encountered difficult airway management, defined as requiring three or more intubation attempts by anesthesia providers. Patients who were already on preoperative mechanical ventilation or had anticipated difficult airways were excluded from the analysis.
2.2. Matching Procedure
A rigorous matching algorithm was implemented to minimize selection bias and control for potential confounding variables in the analysis. Cases of difficult airway management were matched with controls who underwent routine airway management, based on age (± 5 years), surgical type, and year, in a 1:3 ratio. For each difficult airway case, three controls were selected: one with a preoperatively anticipated difficult airway and two with normal airway assessments.
2.3. Potential Risk Factors and Confounding Variables
Potential predictors included patient, surgical, and anesthesia-related factors, such as sex, age, weight, height, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, preoperative airway assessment, history of difficult intubation and ventilation, comorbidities (e.g., medical conditions, congenital heart disease, obstructive sleep apnea, head and neck radiation, anatomical abnormalities due to infection, trauma, tumors, or burns, and abnormal laboratory values), type of surgery, laryngoscopic view grades, the clinician’s first intubation attempt, and intubation experience.
2.4. Sample Size Determination
A sample size calculation estimated that 70 unanticipated difficult airway cases and 280 controls were required to detect an odds ratio of 2.5, assuming a 15% prevalence of exposure among controls, with 80% power and a 0.05 significance level. Based on the institution’s annual incidence of 10–15 cases, a 6-year study period was required.
2.5. Statistical Analysis
Statistical analyses were performed using R version 4.3.1 (R Core Team). Descriptive statistics are reported as medians with interquartile ranges for continuous variables and as frequencies with percentages for categorical variables. Associations between categorical variables and difficult intubation were assessed using the chi-square or Fisher’s exact test, while continuous variables were evaluated with the Student’s t-tests or Mann–Whitney tests, depending on data distribution. Collinearity diagnostics and bivariate correlation matrices were evaluated for all variables. In cases of multicollinearity, only one variable was retained for multivariate analysis. Variables with a p-value < 0.25 in the univariate analysis were considered for inclusion in the initial multivariate logistic regression model. The final regression model was derived using backward selection, retaining all significant variables. The optimal cutoff point was identified using Youden’s index. Statistical significance was defined as a p-value < 0.05.
2.6. Score Derivation and Validation
The risk prediction score system was developed using predictors derived from the multivariate logistic regression model. Risk scores were calculated by assigning weights to regression coefficients and scaling the total to 10.
In the final model, the total predictor score was used to estimate the likelihood of unanticipated difficult airways. Youden’s index determined the cutoff value that maximized specificity and sensitivity. The performance of the final model was reported as the area under the receiver operating characteristic curve (AUC), with an AUC greater than 80 indicating excellent predictive accuracy.
3. Results
Among 62,111 patients undergoing general anesthesia over 6 years, 168 cases of difficult airways were identified. After excluding 70 anticipated difficult airway cases, 98 unanticipated difficult airway cases, and 294 matched controls were analyzed (Figure 1), yielding an incidence of 0.16%. Patient demographics and perioperative characteristics are presented in Table 1. Notably, only 3.1% of patients in the unanticipated difficult airway group were preoperatively assessed as having a probable difficult airway, compared with 16% in the control group (p = 0.002). Most first-attempt intubations (66.1%) were performed by anesthesiology residents. The unanticipated difficult airway group exhibited significantly worse laryngoscopic view grades (p < 0.001).
3.1. Development of the CLAIR Risk Prediction Tool
The initial multivariate model included seven variables with p-values < 0.25: sex, preoperative assessment of probable difficult airway, overbite, coagulopathy, hypocalcemia, first-attempt intubation personnel, and laryngoscopic view. The final predictive model for unanticipated difficult airways (Table 2) identified four key variables, which are incorporated into the CLAIR risk score: coagulopathy and hypocalcemia (C), laryngoscopic view grades (L), potential airway difficulty (A), and first-attempt intubation by residents (inexperienced residents) (IR). The optimal risk score ranged from −4 to 7, with an interquartile range of 0–4; the AUC was 0.93 (Figure 2). A cutoff score of 4 provided 86% sensitivity and 90% specificity. The CLAIR scores were classified into high (≥ 6), intermediate (1–5), and low (≤ 0) risk groups, guiding the need for enhanced management of unanticipated difficult airways. The diagnostic performance of the risk-scoring model for predicting unanticipated difficult airways is presented in Table 3.
3.2. Web-Based Risk Calculator and Accessibility
The initial multivariate model included seven variables with p-values < 0.25: sex, preoperative assessment of probable difficult airway, overbite, coagulopathy, hypocalcemia, first-attempt intubation personnel, and laryngoscopic view. The final predictive model for unanticipated difficult airways (Table 2) identified four key variables, which are incorporated into the CLAIR risk score: coagulopathy and hypocalcemia (C), laryngoscopic view grades (L), potential airway difficulty (A), and first-attempt intubation by residents (inexperienced residents) (IR). The optimal risk score ranged from −4 to 7, with an interquartile range of 0–4; the AUC was 0.93 (Figure 2). A cutoff score of 4 provided 86% sensitivity and 90% specificity. The CLAIR scores were classified into high (≥ 6), intermediate (1–5), and low (≤ 0) risk groups, guiding the need for enhanced management of unanticipated difficult airways. The diagnostic performance of the risk-scoring model for predicting unanticipated difficult airways is presented in Table 3.
3.3. Web-Based Risk Calculator and Accessibility
The CLAIR score calculator, now a web-based tool, enables clinicians to quickly categorize patients into risk groups for tailored airway management. Accessible via a QR code (Figure 3), the tool supports real-time use during preoperative assessments or emergency scenarios, helping to swiftly identify at-risk patients, optimize resource allocation, and enhance airway management strategies, ultimately improving patient safety and outcomes.
4. Discussion
4.1. Key Findings
The CLAIR risk prediction tool represents a significant advancement in identifying unanticipated difficult airways, addressing a critical gap in anesthesia practice. Our study revealed an incidence of unanticipated difficult airways of 0.16%, significantly lower than the 2.3% reported in the 2015 PAAd Thai study [7]. This discrepancy may be due to the development of preoperative assessment techniques, increased awareness of airway difficulties, or differences in patient populations and clinical settings. However, it also underscores the persistent challenges in airway assessment and highlights the potential value of our novel approach.
4.2. Strengths and Limitations
Despite the considerable sample size of the present study and meticulous matching methods, its retrospective design and reliance on existing medical records introduce limitations, such as potential data variability and accuracy concerns. The single-center setting may limit the generalizability of the findings to other healthcare systems or patient populations.
4.3. Interpretation and Implications
3.1.1. CLAIR Score: A Paradigm Shift in Airway Risk Prediction
The CLAIR score demonstrated excellent predictive performance for unanticipated difficult airways, with an AUC of 0.93. Unlike traditional models that primarily focus on anatomical factors, CLAIR integrates patient, clinical, and procedural elements. This multifactorial approach aligns with evolving airway management guidelines, such as those from the ASA [16], emphasizing the importance of individual practitioner expertise, patient-specific considerations, and a well-developed airway management strategy. These guidelines support an adaptable framework that enhances patient safety and improves first-attempt success in difficult airway management. The CLAIR score incorporates four key factors:
- Coagulopathy and hypocalcemia
Coagulopathy increases the risk of bleeding during airway manipulation, whereas hypocalcemia increases neuromuscular excitability, potentially causing masseter spasms despite using muscle relaxants [17]. These conditions complicate airway management and increase the difficulty of intubation. Including this factor in the CLAIR score emphasizes the importance of a comprehensive preoperative evaluation that extends beyond traditional airway assessment.
- Laryngoscopic view grades
The inclusion of laryngoscopic view grades as a predictor in the CLAIR score may appear counterintuitive, as this factor is typically identified after intubation attempts. However, it reflects intraoperative challenges that may not be apparent preoperatively. To improve predictive accuracy, future studies could consider replacing this factor with preoperative airway ultrasonography, which has shown promise in predicting difficult airways. Recent studies have demonstrated that ultrasound-guided measurements, such as anterior neck soft tissue thickness, hyomental distance ratio, and epiglottis visibility, can reliably predict difficult laryngoscopy with high sensitivity and specificity, offering a more objective and reliable assessment compared to traditional methods [18,19,20]. Incorporating these ultrasound parameters into the CLAIR score could further enhance its accuracy and applicability across diverse clinical settings.
- Potential airway difficulty
The limited predictive value of conventional preoperative airway assessments, with an observed accuracy of only 3.1% in this study, aligns with findings by Roth et al. [21]. This underscores the need for a more comprehensive, multimodal approach to identifying risk factors for unanticipated difficult airways. The CLAIR score addresses this limitation by integrating multiple assessment criteria, thereby enhancing prediction accuracy, as evidenced by previous studies [22,23,24]. Despite routine screening, difficult airway scenarios may still arise unexpectedly, highlighting the importance of heightened vigilance and preparedness.
- Inexperienced residents
Our findings regarding the increased likelihood of unanticipated difficult airways among less experienced anesthesiology residents highlight the significance of ongoing training and supervision. These findings align with the previous studies examining the learning curve in airway management skills. Incorporating the CLAIR score into resident education programs could foster skill development and improve decision-making in airway management [25,26]. Simulation-based training utilizing the CLAIR score, coupled with frequent assessments, has been shown to significantly boost residents’ competency and confidence in anticipating and effectively managing challenging airway situations.
3.1.2. Clinical Implications in Anesthesia Practice
The CLAIR risk prediction tool offers a practical approach for enhancing preoperative risk stratification and airway management. Its implementation could optimize resource allocation, ensure the availability of advanced airway tools, and guide the use of specialized techniques, such as video laryngoscopy. The stratification of patients into high, intermediate, and low-risk categories enables tailored airway management strategies, potentially reducing adverse events and improving patient safety, especially in resource-limited settings or emergency scenarios where rapid, accurate risk assessment is essential.
4.4. Controversies4.5. Future Research Directions
Future research should prioritize the external validation of the CLAIR score, as well as the evaluation of its prospective outcomes. Integrating the CLAIR score into existing airway management protocols is another critical step. Additionally, developing CLAIR-based strategies for high-risk patients and assessing the economic impact of their implementation will be essential in refining the tool. These efforts will not only enhance the accuracy and reliability of the CLAIR score but also the practice of managing difficult airways. Ultimately, this could lead to a significant transformation in anesthesia practice, enhancing patient safety across a wide range of clinical settings.
5. Conclusions
The CLAIR risk prediction tool marks a significant advancement in the identification of unanticipated difficult airways, integrating multiple factors to achieve high predictive accuracy, with an AUC of 0.93, outperforming traditional models. Its web-based calculator and QR code enhance accessibility, making it a versatile tool across various clinical settings. By implementing the CLAIR score, anesthesia practice could see improvements in risk stratification, resource allocation, and patient safety. Overall, our findings affirm the CLAIR score as a valuable and user-friendly tool with the potential for transforming airway management. Nonetheless, future validation in diverse populations is essential to confirm its generalizability and to assess its impact on reducing airway-related complications.
Author Contributions
Chanatthee Kitsiripant: Data collection and preparation, draft of the manuscript, and final version approval. Wilasinee Jitpakdee: Data collection and preparation, drafting of the manuscript, and final version approved. Maliwan Oofuvong: Conceptualization and method design, statistical analysis and manuscript approval. Pannawit Benjawaleemas: Conceptualization and manuscript approval. Nussara Dilokrattanaphichit: Data collection and manuscript approval. Wipharat Juthasantikul: Data collection and manuscript approval. Pannipa Phakam: Data collection and manuscript approval. Qistina Yunuswangsa: Data collection and manuscript approval. Polathep Vichitkunakorn: Statistical analysis and manuscript approval.
Funding
This work was funded by the Faculty of Medicine, Prince of Songkla University.
Data Availability Statement
All the data created or analyzed during this work are available from the corresponding author upon reasonable request.
Acknowledgments
None.
Conflicts of Interest
The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Abbreviations
The following abbreviations are used in this manuscript:
| PAAd Thai | Perioperative and Anesthetic Adverse Events in Thailand |
| BMI | body mass index |
| ASA | American Society of Anesthesiologists |
| AUC | area under the receiver operating characteristic curve |
References
- Koh, W.; Kim, H.; Kim, K.; Ro, Y.J.; Yang, H.S. Encountering unexpected difficult airway: relationship with the intubation difficulty scale. Korean J. Anesthesiol. 2016, 69, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Crosby, E.T.; Cooper, R.M.; Douglas, M.J.; Doyle, D.J.; Hung, O.R.; Labrecque, P.; Muir, H.; Murphy, M.F.; Preston, R.P.; Rose, D.K.; et al. The unanticipated difficult airway with recommendations for management. Can. J. Anaesth. 1998, 45, 757–776. [Google Scholar] [CrossRef] [PubMed]
- Benumof, J.L. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology. 1991, 75, 1087–1110. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Birkholz, T.; Irouschek, A.; Ackermann, A.; Schmidt, J. Incidences and predictors of difficult laryngoscopy in adult patients undergoing general anesthesia: a single-center analysis of 102,305 cases. J. Anesth. 2013, 27, 815–821. [Google Scholar] [CrossRef]
- Shah, P.N.; Sundaram, V. Incidence and predictors of difficult mask ventilation and intubation. J. Anaesthesiol. Clin. Pharmacol. 2012, 28, 451–455. [Google Scholar] [CrossRef]
- Jayaraj, A.K.; Siddiqui, N.; Abdelghany, S.M.O.; Balki, M. Management of difficult and failed intubation in the general surgical population: a historical cohort study in a tertiary care centre. Can. J. Anaesth. 2022, 69, 427–437. [Google Scholar] [CrossRef]
- Pipanmekaporn, T.; Punjasawadwong, Y.; Raksakietisak, M.; Sriraj, W.; Lekprasert, V.; Werawatganon, T. A study into perioperative anaesthetic adverse events in Thailand (PAAd Thai): an analysis of suspected emergence delirium. J. Perioper. Pract. 2018, 1750458918780117. [Google Scholar] [CrossRef]
- Joffe, A.M.; Aziz, M.F.; Posner, K.L.; Duggan, L.V.; Mincer, S.L.; Domino, K.B. Management of difficult tracheal intubation: A closed claims analysis. Anesthesiology. 2019, 131, 818–829. [Google Scholar] [CrossRef]
- Cook, T.M.; Woodall, N.; Harper, J.; Benger, J.; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: Intensive care and emergency departments. Br. J. Anaesth. 2011, 106, 632–642. [Google Scholar] [CrossRef]
- Leong, S.M.; Tiwari, A.; Chung, F.; Wong, D.T. Obstructive sleep apnea as a risk factor associated with difficult airway management - A narrative review. J. Clin. Anesth. 2018, 45, 63–68. [Google Scholar] [CrossRef]
- Crawley, S.M.; Dalton, A.J. Predicting the difficult airway. BJA Educ. 2015, 15, 253–258. [Google Scholar] [CrossRef]
- Honarmand, A.; Safavi, M.; Yaraghi, A.; Attari, M.; Khazaei, M.; Zamani, M. Comparison of five methods in predicting difficult laryngoscopy: neck circumference, neck circumference to thyromental distance ratio, the ratio of height to thyromental distance, upper lip bite test and Mallampati test. Adv. Biomed. Res. 2015, 4, 122. [Google Scholar] [CrossRef]
- Trambadia, D.N.; Yadav, P.; A, S. Preoperative assessment to predict difficult airway using multiple screening tests. Cureus. 2023, 15, e46868. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.H.; Lee, J.G.; Yu, S.B.; Kim, D.S.; Ryu, S.J.; Kim, K.H. Predictors of difficult intubation defined by the intubation difficulty scale (IDS): predictive value of 7 airway assessment factors. Korean J. Anesthesiol. 2012, 63, 491–497. [Google Scholar] [CrossRef]
- Vidhya, S.; Sharma, B.; Swain, B.P.; Singh, U.K. Comparison of sensitivity, specificity, and accuracy of Wilson’s score and intubation prediction score for prediction of difficult airway in an eastern Indian population-A prospective single-blind study. J. Family Med. Prim. Care. 2020, 9, 1436–1441. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice guidelines for management of the difficult airway. Anesthesiology. 2022, 136, 31–81. [Google Scholar] [CrossRef]
- Katiyar, S.; Srinivasan, S.; Jain, R.K. Hypocalcaemia leading to difficult airway in sepsis. J. Anaesthesiol. Clin. Pharmacol. 2011, 27, 123–124. [Google Scholar] [CrossRef]
- Carsetti, A.; Sorbello, M.; Adrario, E.; Donati, A.; Falcetta, S. Airway ultrasound as predictor of difficult direct laryngoscopy: A systematic review and meta-analysis. Anesth. Analg. 2022, 134, 740–750. [Google Scholar] [CrossRef]
- De Luis-Cabezón, N.; Ly-Liu, D.; Renedo-Corcostegui, P.; Santaolalla-Montoya, F.; Zabala-Lopez de Maturana, A.; Herrero-Herrero, J.C.; Martínez-Hurtado, E.; De Frutos-Parra, R.; Bilbao-Gonzalez, A.; Fernandez-Vaquero, M.A. A new score for airway assessment using clinical and ultrasound parameters. Front. Med. (Lausanne) 2024, 11, 1334595. [Google Scholar] [CrossRef]
- Fulkerson, J.S.; Moore, H.M.; Anderson, T.S.; Lowe, R.F. Jr. Ultrasonography in the preoperative difficult airway assessment. J. Clin. Monit. Comput. 2017, 31, 513–530. [Google Scholar] [CrossRef]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.M.; Arrich, J.; Herkner, H. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. Cochrane Database Syst. Rev. 2018, 5, CD008874. [Google Scholar] [CrossRef]
- Mallhi, A.I.; Abbas, N.; Naqvi, S.M.N.; Murtaza, G.; Rafique, M.; Alam, S.S. A comparison of Mallampati classification, thyromental distance and a combination of both to predict difficult intubation. Anaesth. Pain Intensive Care. 2018, 22, 468–473. [Google Scholar]
- Ambesh, S.P.; Singh, N.; Rao, P.B.; Gupta, D.; Singh, P.K.; Singh, U. A combination of the modified Mallampati score, thyromental distance, anatomical abnormality, and cervical mobility (M-TAC) predicts difficult laryngoscopy better than Mallampati classification. Acta Anaesthesiol. Taiwan. 2013, 51, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.Y.; Zhang, K.D.; Zhang, Z.H.; Zhang, D.X.; Wang, H.L.; Qi, F. Evaluation of the reliability of the upper lip bite test and the modified mallampati test in predicting difficult intubation under direct laryngoscopy in apparently normal patients: a prospective observational clinical study. BMC Anesthesiol. 2022, 22, 314. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, R.; Kasuya, Y.; Yogo, H.; Sessler, D.I.; Mascha, E.; Yang, D.; Ozaki, M. Learning curves for bag-and-mask ventilation and orotracheal intubation: an application of the cumulative sum method. Anesthesiology. 2010, 112, 1525–1531. [Google Scholar] [CrossRef]
- E J, S.K.; Purva, M.; Chander M, S.; Parameswari, A. Impact of repeated simulation on learning curve characteristics of residents exposed to rare life threatening situations. BMJ Simul. Technol. Enhanc. Learn. 2020, 6, 351–355. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of the study. GA, general anesthesia.
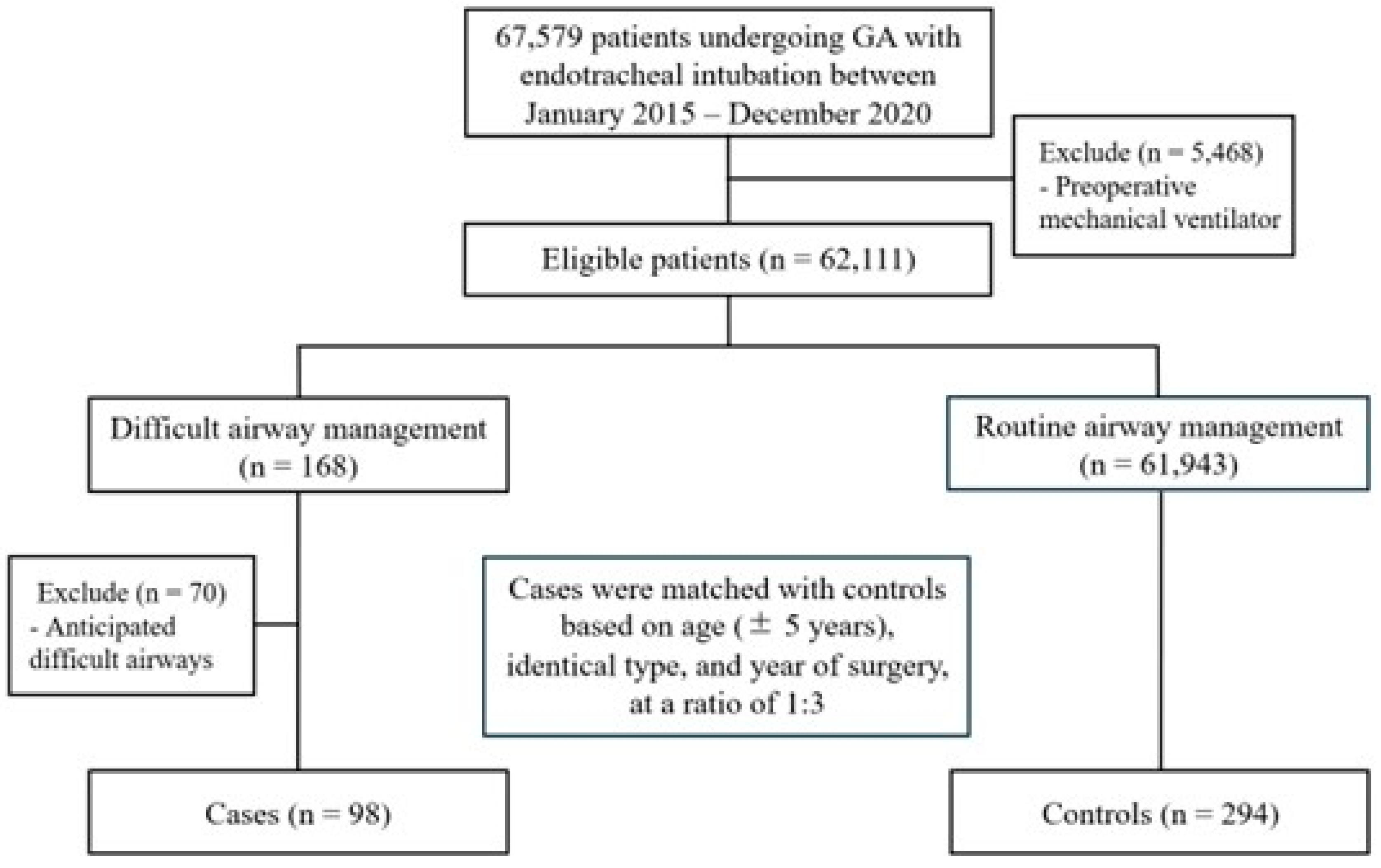
Figure 2.
Receiver operating characteristic (ROC) curve for the CLAIR score predictive model, demonstrating an area under the curve of 0.93. An optimal cutoff score of 4 yielded 86% sensitivity and 90% specificity. Risk stratification categories: high (≥ 6), intermediate (1–5), and low (≤ 0).
Figure 2.
Receiver operating characteristic (ROC) curve for the CLAIR score predictive model, demonstrating an area under the curve of 0.93. An optimal cutoff score of 4 yielded 86% sensitivity and 90% specificity. Risk stratification categories: high (≥ 6), intermediate (1–5), and low (≤ 0).
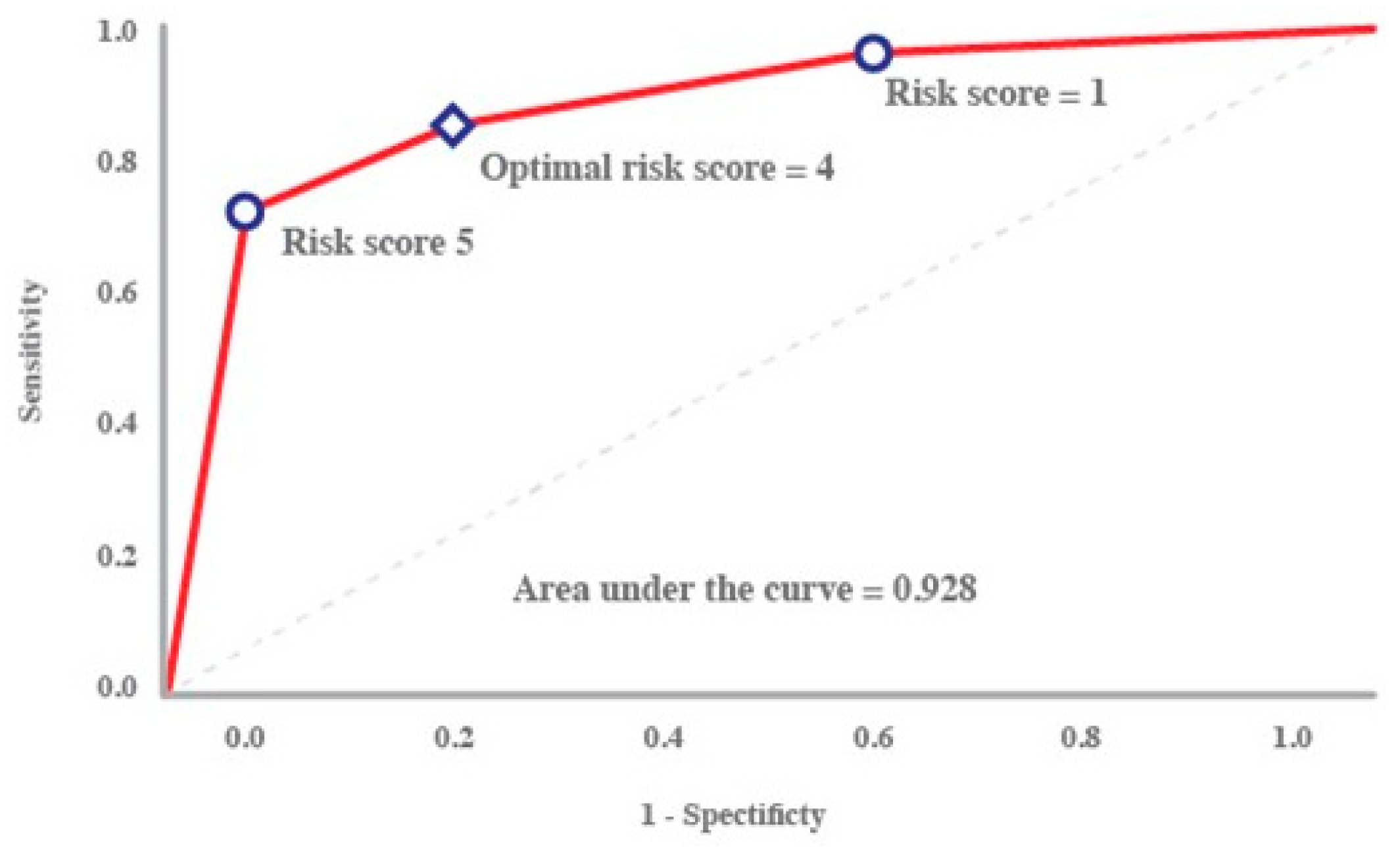
Figure 3.
QR code linking to the CLAIR Score Calculator, a web-based tool designed to predict unanticipated difficult airways.
Figure 3.
QR code linking to the CLAIR Score Calculator, a web-based tool designed to predict unanticipated difficult airways.


Table 1.
Patient demographics and perioperative characteristics.
| Characteristics | Unanticipated difficult airway (n = 98) |
Non-difficult airway (n = 294) |
Total (n = 392) |
p-value |
|---|---|---|---|---|
| Sex | 0.243 | |||
| Male | 56 (57.1) | 146 (49.7) | 202 (51.5) | |
| Female | 42 (42.9) | 148 (50.3) | 190 (48.5) | |
| Age (years), median (IQR) | 55 (38.0, 65.8) | 56 (36.2, 64.0) | 56 (37.8, 64.0) | 0.790 |
| Age (years) | match | |||
| ≤7 | 12 (12.2) | 34 (11.6) | 46 (11.7) | |
| 8–20 | 3 (3.1) | 14 (4.8) | 17 (4.3) | |
| 21–64 | 56 (57.1) | 180 (61.2) | 236 (60.2) | |
| ≥ 65 | 27 (27.6) | 66 (22.4) | 93 (23.7) | |
| Weight (kg), median (IQR) | 58.8 (49.1, 70.0) | 59.5 (48.4, 69.0) | 59.5 (48.5, 69.2) | 0.980 |
| Height (cm), median (IQR) | 160 (152.2,165.9) | 158.5 (150,165) | 159 (151,165) | 0.346 |
| BMI (kg/m2) median (IQR) | 23.3 (19,25.9) | 22.7 (19.2,26) | 22.9 (19.2,26) | 0.494 |
| BMI (kg/m2) | 0.286 | |||
| < 15 | 8 (8.2) | 21 (7.1) | 29 (7.4) | |
| 15–29 | 82 (83.7) | 231 (78.6) | 313 (79.8) | |
| ≥30 | 8 (8.2) | 42 (14.3) | 50 (12.8) | |
| ASA classification | 0.798 | |||
| I | 2 (2) | 13 (4.4) | 15 (3.8) | |
| II | 52 (53.1) | 155 (52.7) | 207 (52.8) | |
| III | 43 (43.9) | 123 (41.8) | 166 (42.3) | |
| IV | 1 (1) | 3 (1) | 4 (1) | |
| Preoperative probable difficult airway | 0.002 | |||
| No | 95 (96.9) | 247 (84) | 342 (87.2) | |
| Yes | 3 (3.1) | 47 (16) | 50 (12.8) | |
| Modified Mallampati classification | 0.911 | |||
| 1–2 | 79 (80.6) | 239 (81.3) | 318 (81.1) | |
| 3–4 | 10 (10.2) | 26 (8.8) | 36 (9.2) | |
| unknown | 9 (9.2) | 29 (9.9) | 38 (9.7) | |
| Thyromental distance | 0.832 | |||
| < 3 finger breaths | 3 (3.1) | 8 (2.7) | 11 (2.8) | |
| 3 finger breaths | 64 (65.3) | 181 (61.6) | 245 (62.5) | |
| > 3 finger breaths | 22 (22.4) | 80 (27.2) | 102 (26) | |
| unknown | 9 (9.2) | 25 (8.5) | 34 (8.7) | |
| Inter-incisor gap | 0.824 | |||
| 1–2 cm | 7 (7.1) | 16 (5.4) | 23 (5.9) | |
| 3–4 cm | 82 (83.7) | 251 (85.4) | 333 (84.9) | |
| unknown | 9 (9.2) | 27 (9.2) | 36 (9.2) | |
| Limited neck flexion and extension | 1 | |||
| No | 94 (95.9) | 284 (96.6) | 378 (96.4) | |
| Yes | 3 (3.1) | 8 (2.7) | 11 (2.8) | |
| Cannot evaluate | 1 (1) | 2 (0.7) | 3 (0.8) | |
| Upper lip bite test classification | 0.681 | |||
| 1 | 53 (54.1) | 175 (59.5) | 288 (58.2) | |
| 2 | 26 (26.5) | 75 (25.5) | 101 (25.8) | |
| 3 | 1 (1) | 3 (1) | 4 (1) | |
| unknown | 18 (18.4) | 41 (13.9) | 59 (15.1) | |
| Facial appearance or syndrome | 0.418 | |||
| Normal | 95 (96.9) | 289 (98.3) | 384 (98) | |
| Abnormal | 3 (3.1) | 5 (1.7) | 8 (2) | |
| Edentulous | 0.840 | |||
| No | 88 (89.8) | 268 (91.2) | 356 (90.8) | |
| Yes | 10 (10.2) | 26 (8.8) | 36 (9.2) | |
| Overbite | 0.250 | |||
| No | 97 (99) | 294 (100) | 391 (99.7) | |
| Yes | 1 (1) | 0 (0) | 1 (0.3) | |
| Previous history of difficult intubation and ventilation | 1 | |||
| No | 98 (100) | 293 (99.7) | 391 (99.7) | |
| Yes | 0 (0) | 1 (0.3) | 1 (0.3) | |
| Medical conditions | 1 | |||
| No | 93 (94.9) | 278 (94.9) | 371 (94.6) | |
| Yes | 5 (5.1) | 16 (5.4) | 21 (5.4) | |
| Congenital heart disease | 0.770 | |||
| No | 95 (96.9) | 281 (95.6) | 376 (95.9) | |
| Yes | 3 (3.1) | 13 (4.4) | 16 (4.1) | |
| Airway/neck/oral deformity | 0.639 | |||
| No | 90 (91.8) | 276 (93.9) | 366 (93.4) | |
| Yes | 8 (8.2) | 18 (6.1) | 26 (6.6) | |
| Foreign body aspiration | 0.438 | |||
| No | 97 (99) | 293 (99.7) | 390 (99.5) | |
| Yes | 1 (1) | 1 (0.3) | 2 (0.5) | |
| Infection: retropharyngeal abscess, epiglottitis, supraglottitis | 1 | |||
| No | 97 (99) | 292 (99.3) | 389 (99.2) | |
| Yes | 1 (1) | 2 (0.7) | 3 (0.8) | |
| Post-surgical procedure: thyroid, cervical vertebrae | 0.504 | |||
| No | 94 (95.9) | 286 (97.3) | 380 (96.9) | |
| Yes | 4 (4.1) | 8 (2.7) | 12 (3.1) | |
| OSA/Snoring | 0.875 | |||
| No | 83 (84.7) | 245 (83.3) | 328 (83.7) | |
| Yes | 15 (15.3) | 49 (16.7) | 100 (16.3) | |
| Tumors: thyroid, pharynx, larynx and tracheobronchus, esophagus | 0.634 | |||
| No | 86 (87.8) | 265 (90.1) | 528 (87.7) | |
| Yes | 12 (12.2) | 29 (9.9) | 74 (12.3) | |
| Trauma: face, neck | 0.643 | |||
| No | 96 (98) | 290 (98.6) | 386 (98.5) | |
| Yes | 2 (2) | 4 (1.4) | 6 (1.5) | |
| Burns (head, neck, face), smoke inhalation, massive burn | 0.261 | |||
| No | 96 (98) | 292 (99.3) | 388 (99) | |
| Yes | 2 (2) | 2 (0.7) | 4 (1) | |
| History radiation of head, neck | 0.697 | |||
| No | 95 (96.9) | 288 (98) | 383 (97.7) | |
| Yes | 3 (3.1) | 6 (2) | 9 (2.3) | |
| Laryngeal edema: angioedema, allergic, post rigid bronchoscopy | 1 | |||
| No | 97 (99) | 292 (99.3) | 389 (99.2) | |
| Yes | 1 (1) | 2 (0.7) | 3 (0.8) | |
| Coagulopathy and hypocalcemia | 0.102 | |||
| No | 95 (96.9) | 292 (99.3) | 387 (98.7) | |
| Yes | 3 (3.1) | 2 (0.7) | 5 (1.3) | |
| Type of surgery | match | |||
| Remote | 14 (14.3) | 41 (13.9) | 55 (14) | |
| Neuro/Orthopedic | 6 (6.1) | 18 (6.1) | 24 (6.1) | |
| Eye/superficial | 12 (12.2) | 40 (13.6) | 52 (13.3) | |
| ENT | 31 (31.6) | 90 (30.6) | 121 (30.0) | |
| Thoracic/Vascular | 12 (12.2) | 34 (11.6) | 46 (11.7) | |
| Abdomen | 23 (23.5) | 71 (24.1) | 94 (24) | |
| First-attempt intubation personnel | 0.152 | |||
| Anesthesia instructors | 9 (9.2) | 31 (10.5) | 40 (10.2) | |
| Anesthesiology residents | 72 (73.5) | 187 (63.6) | 259 (66.1) | 0.096 |
| Certified registered nurse anesthetists | 3 (3.1) | 28 (9.5) | 31 (7.9) | |
| Nurse anesthetist students | 14 (14.3) | 48 (16.3) | 62 (15.8) | |
| Intubation experience (years) | 0.837 | |||
| < 5 | 93 (94.9) | 275 (93.5) | 368 (93.9) | |
| 5–10 | 3 (3.1) | 13 (4.4) | 16 (4.1) | |
| 11–20 | 2 (2) | 4 (1.4) | 6 (1.5) | |
| > 20 | 0 (0) | 2 (0.7) | 2 (0.5) | |
| Laryngoscopic view | < 0.001 | |||
| Grade 1 | 10 (10.2) | 227 (77.2) | 237 (60.5) | |
| Grade 2 | 14 (14.3) | 49 (16.7) | 63 (16.1) | |
| Grade 3 | 43 (43.9) | 14 (4.8) | 57 (14.5) | |
| Grade 4 | 30 (30.6) | 0 (0) | 30 (7.7) | |
| Unknown | 1 (1) | 4 (1.4) | 5 (1.3) |
Data are presented as numbers (%) unless otherwise indicated. IQR = interquartile range, BMI = body mass index, ASA = American Society of Anesthesiologists, OSA = obstructive sleep apnea, ENT = ear, nose, and throat.
Table 2.
Multivariate logistic regression of predictive factors of unanticipated difficult airway (CLAIR score).
Table 2.
Multivariate logistic regression of predictive factors of unanticipated difficult airway (CLAIR score).
| Predictive factors | Coefficient | Adjusted OR (95% CI) | p-value | Risk score |
|---|---|---|---|---|
| C: Coagulopathy and hypoCalcemia | 2.36 | 10.57 (0.67, 167.55) | 0.094 | 3 |
|
L: Laryngoscopic view (Ref: grade 1) Grade 2 Grade 3 Grade 4 |
2.14 4.85 5.36 |
8.52 (3.45, 21.04) 128.15 (45.66, 359.67) 212.4 (56.66, 796.25) |
< 0.001 < 0.001 < 0.001 |
3 6 7 |
| A: potential Airway difficulty | -2.97 | 0.05 (0.01, 0.23) | < 0.001 | -4 |
| IR: Inexperienced Residents | 0.96 | 2.61 (1.17, 5.81) | 0.019 | 1 |
OR = odds ratio, CI = confident interval.
Table 3.
Diagnostic performance of the CLAIR score for predicting unanticipated difficult airway.
| Score | Sensitivity | Specificity | PPV | NPV | Accuracy | +LR | -LR |
|---|---|---|---|---|---|---|---|
| 3 | 100.00 | 2.38 | 25.45 | 100.00 | 51.19 | 1.02 | 0 |
| 4 | 98.98 | 9.18 | 26.65 | 96.43 | 54.08 | 1.09 | 0.11 |
| 5 | 97.96 | 15.65 | 27.91 | 95.83 | 56.80 | 1.16 | 0.13 |
| 6 | 96.94 | 15.65 | 27.70 | 93.88 | 56.29 | 1.15 | 0.2 |
| 7 | 79.59 | 22.45 | 25.49 | 76.74 | 51.02 | 1.03 | 0.91 |
| 8 | 35.71 | 55.44 | 21.08 | 72.12 | 45.58 | 0.8 | 1.16 |
| 9 | 2.04 | 99.66 | 66.67 | 75.32 | 50.85 | 6 | 0.98 |
| 10 | 1.02 | 99.66 | 50.00 | 75.13 | 50.34 | 3 | 0.99 |
| 11 | 0.00 | 99.66 | 0 | 74.94 | 49.83 | 0 | 1 |
PPV = positive predictive value, NPV = negative predictive value, +LR = positive likelihood ratio, -LR = negative likelihood ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



