Submitted:
20 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
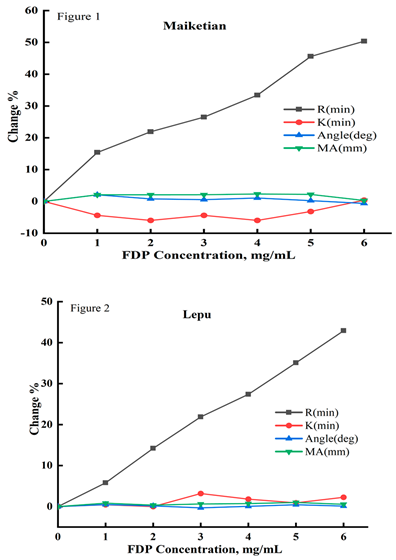
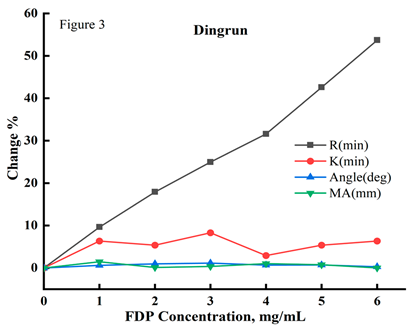
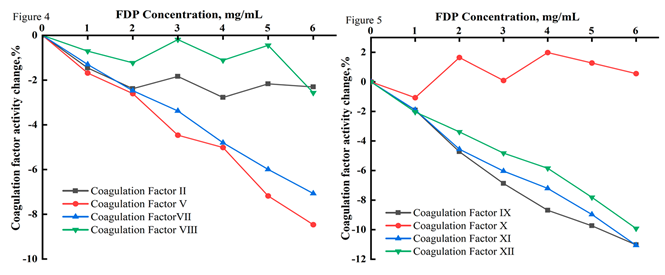
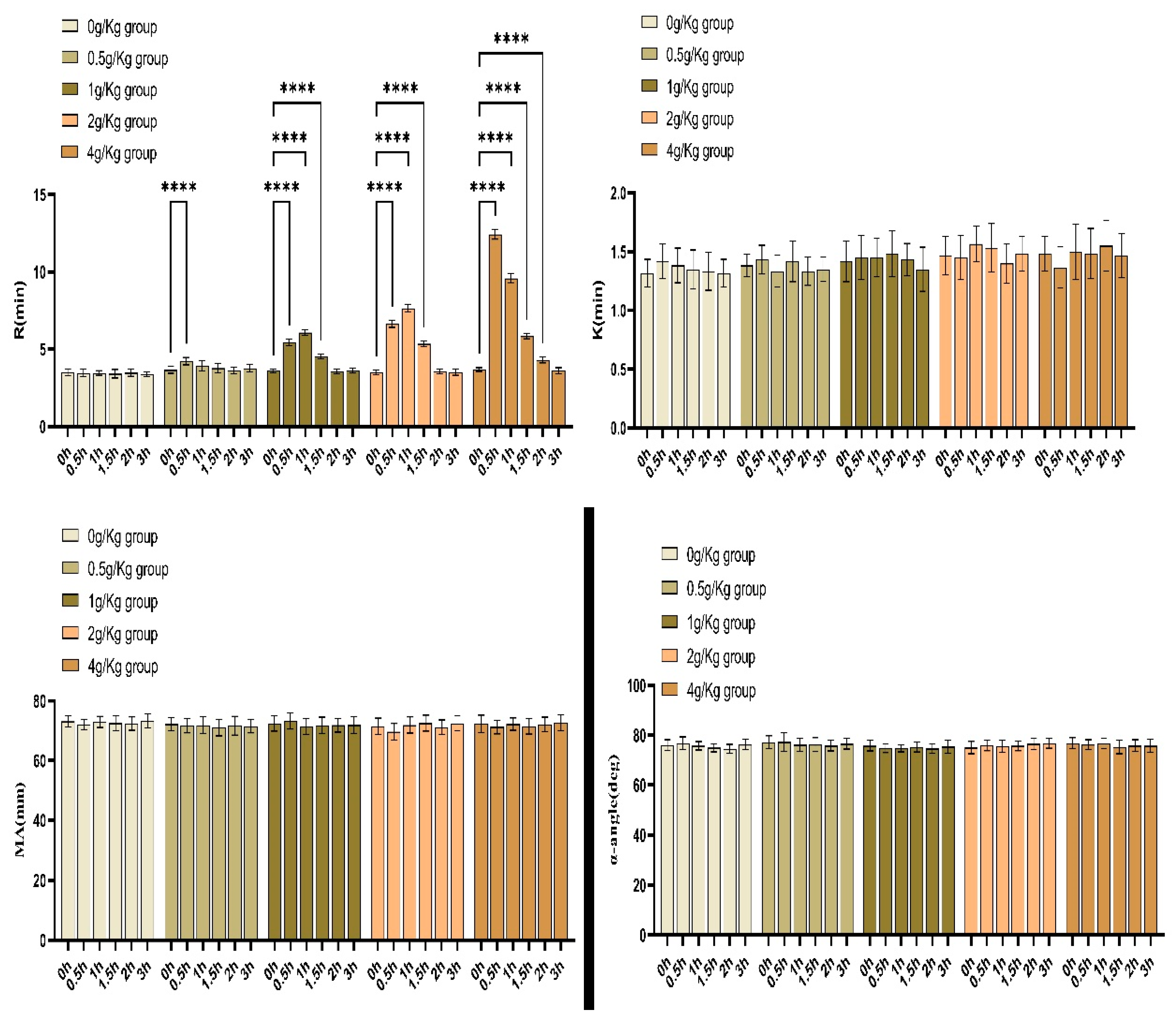
Objective To investigate the effects of sodium fructose diphosphate (FDP) on blood coagulation reaction time and plasma coagulation factor activity in vitro. Method The thromboelastogram detection system provided by three different manufacturers (Maiketian, Lepu, and Dingrun) was used to determine the blood coagulation reaction time (R) , clotting time (K), α-angle, and maximal amplitude (MA) of blood samples mixed with different concentrations FDP and the samples before dosing.The activities of coagulation factors II, V, VII, VIII, IX, X, XI and XII for plasma mixed with FDP were determined by automatic hemagglutination analysis system. The difference of test results between the experimental group with FDP and the control group without FDP was compared. The correlation between FDP concentration and the results of thrombologram or coagulation factor activity was analyzed by linear regression. New Zealand white rabbits were selected for the experiment on the effect of the drug on blood coagulation in vivo, and the changes of the thrombologram test results (R, K, α-angle, MA) at each time point after injection of FDP groups with the same dose were analyzed. According to the changes of the thrombologram test results before and after injection, statistical analysis was conducted to determine whether there were statistical differences in the effect of the drug on blood coagulation function. Result The results of thrombologram provided by three different manufacturers showed that the R value of blood sample was significantly correlated with the blood FDP concentration (P < 0.000), and the correlation coefficient r was 0.988 (Maiketian), 0.999 (Lepu) and 0.996 (Dingrun), respectively. There was no significant correlation between FDP concentration and K, α-angle , or MA (P > 0.05). The results of in vitro experiments showed that plasma coagulation factor V, VII, IX, XI and XII activities were significantly negatively correlated with plasma FDP concentrations (P < 0.000), and the correlation coefficients r were -0.995, -0.990, -0.989, 0.997, 0.995, respectively. The activities of II, VIII and X were not significantly affected by FDP (P > 0.05). In vivo experiments of New Zealand white rabbits showed that 0.5h after intravenous 0.5g/Kg FDP administration , 0.5h, 1h and 1.5h after 1g/Kg administration, 0.5h, 1h and 1.5h after 2g/Kg administration, and 0.5h, 1h, 1.5h and 2h after 4g/Kg administration, there were statistical differences in the R values of thrombologram compared with those before administration (P < 0.05), and the R values increased significantly after administration. That is, the blood coagulation reaction time is prolonged. Conclusion FDP can affect the results of blood coagulation test in vivo and vitro. It may really affect the function of our coagulation system.
Keywords:
Introduction
Results
Discussion
Methods
Authorship Contributions
Competing interest
Data availability statement
Acknowledgements
References
- Zhang CS. et al. Fructose-1,6-bisphosphate and aldolase mediate glucose sensing by AMPK. Nature. 548(7665):112-116(2017).
- Wang W, Liu M, You C, Li Z & Zhang YHP. ATP-free biosynthesis of a high energy phosphate metabolite fructose 1,6-diphosphate by in vitro metabolic engineering. Metab Eng. 42:168-174(2017).
- Alva N,Alva R & Carbonell T. Fructose 1,6-bisphosphate:A summary of its cytoprotective mechanism. Curr Med Chem. 23(39) :4396-4417(2016).
- Li TT, Xie JZ, Wang L,Gao YY & Jiang XH. Rational application of fructose-1, 6-diphosphate:From the perspective of pharmacokinetics. Acta Pharm. 65(2):147-157(2015).
- Donohoe PH, Fahlman CS, B ickler PE, etal. Neuroprotection and in-tracellular Ca2+ modulation w ith fructose-1, 6-bisphosphate during in vitro hypoxia-ischem ia involves phospholipaseC-dependent signaling[ J]. B rain Res, 917(2): 158 -166(2001).
- Lancé M D. A general review of major global coagulation assays: thrombelastography, thrombin generation test and clot waveform analysis[J]. Thrombosis journal, 13(1): 1(2015).
- Elliott, Andrea, Wetzel,Jeremy,et al. Thromboelastography in patients with acute ischemic stroke[J].International journal of stroke: official journal of the International Stroke Society. 10(2):194-201(2015).
- David WJ, James AD.TEG and ROTEM: technology and clinical applications[J]. Am J Hematol, 89(2):228-32(2014).
- Snorre BS, Jerard S, Joar S, etal. The use of thromboelastography (TEG) in massively bleeding patients at Haukeland University Hospital 2008-15[J]. Transfus Apher Sci, 58(1):117-121(2019).
- Kamal AH, Tefferi A, Pruthi RK. How to interpret and pursue an abnormal prothrombin time, activated partialthromboplastin time, and bleeding time in adults[J]. Mayo Clin Proc. 82(7):864-73(2007).
- Chen TQ, Duan Chen D , Lu Chen L, et al. The effects of fructose diphosphate on routine coagulation tests in vitro[J]. Sci Rep, 12(1):304(2022).

| FDP(mg/mL) | Maiketian | Lepu | Dingrun | |||||||||
| R(min) | K(min) | Angle(deg) | MA(mm) | R(min) | K(min) | Angle(deg) | MA(mm) | R(min) | K(min) | Angle(deg) | MA(mm) | |
| 0 | 5.66±0.49 | 2.52±0.27 | 67.35±2.76 | 63.51±2.28 | 6.90±0.46 | 2.20±0.26 | 68.14±2.53 | 63.8±2.62 | 6.65±0.36 | 2.05±0.27 | 69.37±2.51 | 64.14±2.43 |
| 1 | 6.53±0.50* | 2.41±0.31 | 68.75±2.73 | 64.83±3.07 | 7.30±0.31* | 2.21±0.26 | 68.47±2.00 | 64.33±2.85 | 7.29±0.49* | 2.18±0.28 | 69.81±2.31 | 65.08±2.67 |
| 2 | 6.9±0.51* | 2.37±0.28 | 67.89±2.48 | 64.84±2.88 | 7.88±0.38* | 2.20±0.30 | 68.25±2.45 | 64.03±2.88 | 7.84±0.59* | 2.16±0.27 | 70.05±2.44 | 64.23±2.52 |
| 3 | 7.16±0.55* | 2.41±0.26 | 67.72±2.42 | 64.85±2.79 | 8.41±0.45* | 2.27±0.27 | 67.93±2.27 | 64.20±2.53 | 8.31±0.61* | 2.22±0.30 | 70.18±2.58 | 64.38±2.43 |
| 4 | 7.55±0.43* | 2.37±0.20 | 68.08±1.78 | 65.00±2.73 | 8.79±0.47* | 2.24±0.32 | 68.18±2.22 | 64.26±2.85 | 8.75±0.63* | 2.11±0.25 | 69.84±2.14 | 64.81±2.48 |
| 5 | 8.24±0.49* | 2.44±0.29 | 67.51±1.88 | 64.91±2.82 | 9.32±0.46* | 2.22±0.33 | 68.45±2.07 | 64.44±2.74 | 9.48±0.63* | 2.16±0.25 | 69.87±2.44 | 64.64±2.69 |
| 6 | 8.51±0.47* | 2.53±0.30 | 66.92±2.22 | 63.70±3.10 | 9.86±0.45* | 2.25±0.32 | 68.22±2.27 | 64.16±2.52 | 10.22±0.63* | 2.18±0.25 | 69.57±2.13 | 64.15±2.44 |
| r | 0.988 | 0.106 | -0.474 | 0.109 | 0.999 | 0.714 | 0.054 | 0.563 | 0.996 | 0.417 | 0.144 | -0.057 |
| Regression equation | Yresult=0.4507XFDP+ 5.8693 | Yresult=0.0032XFDP+2.4261 | Yresult=-0.1279XFDP+68.129 | Yresult=0.0318XFDP+64.425 | Yresult=0.4939XFDP+6.8696 | Yresult=0.0075XFDP+2.2046 | Yresult=0.0046XFDP+68.22 | Yresult=0.0546XFDP+64.01 | Yresult=0.5714XFDP+6.6486 | Yresult=0.0107XFDP+2.1193 | Yresult=0.0182XFDP+69.758 | Yresult=-0.0096XFDP+64.519 |
| P | 0.000 | 0.822 | 0.282 | 0.816 | 0.000 | 0.071 | 0.908 | 0.188 | 0.000 | 0.352 | 0.759 | 0.903 |
| FDP(mg/mL) | Coagulation factor activities(%) | |||||||
| Ⅴ | Ⅶ | Ⅸ | Ⅺ | Ⅻ | II | Ⅷ | Ⅹ | |
| 0 | 125.25±18.96 | 146.85±26.42 | 109.35±9.07 | 75.88±10.15 | 68.24±7.40 | 130.05±24.54 | 112.26±17.50 | 121.57±17.69 |
| 1 | 123.14±19.33* | 144.94±25.13* | 107.25±8.58* | 74.44±10.08* | 66.85±7.48* | 128.16±22.13 | 111.47±17.27 | 120.27±20.73 |
| 2 | 121.99±18.83* | 143.22±24.67* | 104.18±8.31* | 72.42±10.09* | 65.93±7.52* | 126.95±22.12 | 110.88±17.87 | 123.57±19.10 |
| 3 | 119.66±17.16* | 141.89±24.15* | 101.83±7.80* | 71.30±10.30* | 64.95±7.25* | 127.66±22.27 | 112.05±17.60 | 121.68±20.00 |
| 4 | 118.97±17.29* | 139.80±24.47* | 99.85±7.04* | 70.41±10.05* | 64.25±7.51* | 126.44±23.66 | 111.01±16.85 | 123.98±17.98 |
| 5 | 116.26±16.46* | 138.05±23.52* | 98.70±7.00* | 69.07±9.87* | 62.91±7.68* | 127.23±23.57 | 111.76±18.21 | 123.12±17.22 |
| 6 | 114.65±16.38* | 136.47±22.38* | 97.29±7.10* | 67.49±9.06* | 61.47±7.35* | 127.05±22.51 | 109.38±17.13 | 122.25±17.13 |
| r | -0.995 | -0.99 | -0.989 | -0.997 | -0.995 | -0.737 | -0.630 | 0.484 |
| Regression equation | Yresult=-1.735XFDP+125.19 | Yresult=-1.7264XFDP+146.78 | Yresult=-2.0575XFDP+108.81 | Yresult=-1.3543XFDP+75.636 | Yresult=-1.0668XFDP+68.143 | Yresult=-0.4061XFDP+128.87 | Yresult=-0.2832XFDP+112.11 | Yresult=0.2911XFDP+121.48 |
| P | <0.000 | <0.000 | <0.000 | <0.000 | <0.000 | 0.059 | 0.129 | 0.27 |
| time(h) | R(mim) | F | P | ||||
| 0g/Kg group | 0.5g/Kg group | 1g/Kg group | 2g/Kg group | 4g/Kg group | |||
| 0a | 3.52±0.21 | 3.67±0.23 | 3.62±0.12 | 3.50±0.14 | 3.67±0.12 | 1.38 | 0.26 |
| 0.5b | 3.47±0.23 | 4.23±0.23* | 5.45±0.21* | 6.65±0.23* | 12.43±0.32* | 1241.1 | 0.000 |
| 1b | 3.47±0.15 | 3.93±0.33 | 6.08±0.19* | 7.65±0.23* | 9.60±0.30* | 643.8 | 0.000 |
| 1.5b | 3.42±0.28 | 3.78±0.31 | 4.53±0.15* | 5.35±0.19* | 5.85±0.16* | 122.1 | 0.000 |
| 2b | 3.48±0.23 | 3.62±0.21 | 3.58±0.15 | 3.58±0.15 | 4.32±0.20* | 18.7 | 0.000 |
| 3b | 3.38±0.15 | 3.77±0.24 | 3.62±0.16 | 3.52±0.20 | 3.62±0.19 | 3.27 | 0.027 |
| time(h) | K(mim) | F | P | ||||
| 0g/Kg group | 0.5g/Kg group | 1g/Kg group | 2g/Kg group | 4g/Kg group | |||
| 0a | 1.32±0.12 | 1.38±0.10 | 1.42±0.17 | 1.47±0.16 | 1.48±0.15 | 1.33 | 0.286 |
| 0.5b | 1.42±0.15 | 1.43±0.12 | 1.45±0.19 | 1.46±0.20 | 1.37±0.18 | 0.27 | 0.893 |
| 1b | 1.38±0.15 | 1.33±0.14 | 1.45±0.16 | 1.57±0.14 | 1.50±0.24 | 1.75 | 0.171 |
| 1.5b | 1.38±0.16 | 1.42±0.17 | 1.48±0.19 | 1.53±0.21 | 1.48±0.21 | 0.83 | 0.518 |
| 2b | 1.33±0.16 | 1.33±0.12 | 1.43±0.14 | 1.40±0.17 | 1.55±0.22 | 1.78 | 0.165 |
| 3b | 1.32±0.12 | 1.35±0.10 | 1.35±0.19 | 1.48±0.15 | 1.47±0.19 | 1.49 | 0.234 |
| time(h) | α-angle(deg) | F | P | ||||
| 0g/Kg group | 0.5g/Kg group | 1g/Kg group | 2g/Kg group | 4g/Kg group | |||
| 0a | 76.05±2.14 | 77.18±2.57 | 75.82±2.12 | 75.08±2.47 | 76.83±2.22 | 0.78 | 0.547 |
| 0.5b | 76.82±2.54 | 77.35±0.23 | 74.83±1.83 | 75.97±2.15 | 76.30±1.91 | 0.86 | 0.504 |
| 1b | 75.78±1.65 | 76.17±2.53 | 74.80±1.38 | 75.58±2.40 | 76.72±2.13 | 0.71 | 0.592 |
| 1.5b | 75.02±1.60 | 76.27±2.81 | 75.32±2.04 | 75.77±1.95 | 75.38±2.73 | 0.27 | 0.896 |
| 2b | 74.55±1.81 | 75.88±2.15 | 74.67±1.91 | 76.63±2.26 | 75.85±2.34 | 1.06 | 0.394 |
| 3b | 76.28±2.07 | 76.63±2.20 | 75.43±2.54 | 76.88±2.17 | 75.78±2.68 | 0.32 | 0.863 |
| time(h) | MA(mm) | F | P | ||||
| 0g/Kg group | 0.5g/Kg group | 1g/Kg group | 2g/Kg group | 4g/Kg group | |||
| 0a | 73.13±1.92 | 72.22±2.27 | 75.52±2.61 | 71.47±2.76 | 72.35±2.91 | 0.34 | 0.849 |
| 0.5b | 72.10±1.64 | 71.70±2.40 | 73.27±2.68 | 69.67±2.79 | 72.27±2.28 | 1.81 | 0.159 |
| 1b | 72.95±1.86 | 71.85±2.85 | 71.43±2.75 | 71.92±2.71 | 72.23±2.09 | 0.31 | 0.868 |
| 1.5b | 72.57±2.46 | 71.07±2.80 | 71.85±2.72 | 72.57±2.63 | 71.51±2.60 | 0.37 | 0.826 |
| 2b | 72.40±2.26 | 71.72±3.13 | 71.87±2.31 | 71.22±2.40 | 72.12±2.44 | 0.19 | 0.943 |
| 3b | 73.35±2.37 | 71.53±2.25 | 71.95±2.78 | 72.50±2.54 | 72.75±2.67 | 0.46 | 0.761 |
| a: Before FDP injection; b:after FDP injection. P>0.05,No statistically significant difference between different dose groups at the same time point; P < 0.05, with statistically significant differences between the different dose groups at the same time point.*:P<0.01. | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



