Submitted:
11 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Alzheimer's disease is the leading cause of dementia worldwide, with the number of patients expected to reach 131 million by 2050. Current treatments can only alleviate the symptoms of AD and are unable to halt the progression of the disease. Personalized immunotherapy shows great potential, as it can improve treatment efficacy and reduce side effects through precise targeting and early intervention. This paper emphasizes the importance of integrating genetic background with immune status, reviews the genetic and immune characteristics of AD, discusses multi-omics data integration methods, biomarker identification, patient stratification, and precision treatment strategies, as well as the current status and prospects of immunotherapy applications, thereby providing new directions for future AD treatments.
Keywords:
Alzheimer's disease
; personalized immunotherapy
; genetic-immune integration
; biomarker identification
1. Introduction
Alzheimer's Disease (AD) is the most common type of dementia, accounting for approximately 60% to 70% of all cases [1,2,3]. Currently, around 47 million people worldwide suffer from dementia, and this number is projected to increase to 131 million by 2050, primarily due to aging populations in North America and Europe[4,5]. AD not only exacerbates the burden on medical resources and social support services but also imposes significant economic pressure [6]. The core pathological features of AD include the deposition of amyloid-beta (Aβ), forming senile plaques in the brain, and the hyperphosphorylation of tau protein in neurofibrillary tangles [7]. These pathological changes lead to neuronal damage and brain atrophy[8]. Aβ is abnormally cleaved by β- and γ-secretases to produce Aβ40 and Aβ42 monomers, which further aggregate to form senile plaques. High concentrations of Aβ trigger the infiltration and activation of microglia, which, although aiding in the clearance of Aβ, exacerbate inflammation through an excessive immune response, thereby damaging neurons[9,10,11,12].
Currently, AD treatment primarily focuses on symptom management, with FDA-approved drugs including cholinesterase inhibitors and the NMDA receptor antagonist memantine[13]. These drugs work by inhibiting acetylcholinesterase, thereby reducing the breakdown of acetylcholine in the brain and enhancing central cholinergic neurotransmission to alleviate cognitive decline[14]. Studies have shown that these drugs can slow the progression of cognitive decline and improve patients' daily living abilities within the first year of treatment. However, these drugs cannot halt disease progression, and once discontinued, patients' cognitive functions deteriorate rapidly[15,16,17]. Additionally, the efficacy of these treatments varies significantly among different patients, and long-term use may be accompanied by various side effects such as nausea, diarrhea, and loss of appetite, further limiting their widespread and sustained clinical application[18,19,20].
Immunotherapy treats diseases by modulating the immune system and has achieved significant success in cancer treatment, such as immune checkpoint inhibitors enhancing the body's immune response against tumors and CAR-T cell therapy showing good efficacy in various cancers[21,22,23,24]. In AD, immunotherapy aims to activate the immune system to clear Aβ deposits in the brain, showing potential as a disease-modifying treatment[25]. Personalized immunotherapy in AD shows significant potential, particularly in precise targeting, early intervention, and reducing side effects[26]. By selecting the most suitable immunotherapy strategies based on the specific forms of Aβ deposition and tau protein status in patients, such as monoclonal antibodies targeting Aβ42, the effectiveness of treatment can be significantly improved[27,28,29]. Utilizing early diagnosis and biomarker detection to achieve early intervention can help prevent or delay neuronal damage and improve patient prognosis[30]. Additionally, optimizing treatment plans based on individual differences, such as adjusting dosages and treatment cycles, can optimize immune responses, reduce inflammation risks, thereby decreasing side effects and improving patient tolerance and compliance[31]. With a deeper understanding of the pathophysiological mechanisms of AD, personalized immunotherapy is expected to integrate multidisciplinary research findings from genomics, proteomics, and other fields to achieve more precise and effective disease management, becoming an important direction for future AD treatments [32].
2. Genetic Background and Immune System in AD
Apolipoprotein E ε4 (APOE ε4) is a major genetic risk factor for Alzheimer's Disease (AD), playing multiple roles in the disease's pathogenesis. The APOE4 protein encoded by APOE ε4 exhibits significant differences in lipid metabolism compared to APOE3, resulting in disrupted cholesterol transport and distribution in the brain. This disruption affects the stability and function of neuronal membranes [33]. APOE4 more readily binds to Aβ, promoting its aggregation and deposition to form amyloid plaques, which are hallmark pathological features of AD. Additionally, the interaction between APOE4 and mitochondria induces mitochondrial dysfunction, characterized by elevated mitochondrial calcium levels and increased reactive oxygen species production. These changes further exacerbate energy metabolism disorders and oxidative stress, thereby impairing neuronal survival[34]. In terms of immune response, APOE4 is more susceptible to proteolysis under stress conditions, generating products that promote the formation of neurofibrillary tangles. Moreover, APOE4 affects the function of immune cells such as microglia, reducing the clearance efficiency of Aβ, leading to chronic inflammatory responses, and thereby promoting the pathological progression of AD. Furthermore, APOE4 can translocate to the cell nucleus, regulating the expression of genes related to aging, production, inflammation, and apoptosis, thereby further exacerbating the pathological changes in AD[35,36,37,38,39].
Familial Alzheimer's Disease (FAD) is primarily caused by mutations in the APP, PSEN1, and PSEN2 genes, whose encoded proteins play critical roles in the production and clearance of Aβ [40,41]. Mutations in the APP gene result in the abnormal accumulation of Aβ following the cleavage of amyloid precursor protein (AβPP) by β- and γ-secretases on the cell membrane, thereby promoting the formation of amyloid plaques[42,43]. The PSEN1 and PSEN2 genes encode key components of the γ-secretase complex. Mutations in these genes lead to abnormal γ-secretase activity, increasing the production and deposition of Aβ, with PSEN1 gene mutations being the most common pathogenic factors in FAD (Figure 1)[44,45,46,47]. Although AD caused by PSEN2 mutations is relatively rare, its function is similar to that of PSEN1, also leading to the abnormal accumulation of Aβ.
Genetic background plays a crucial role in regulating immune responses. Genes influence the intensity and direction of immune responses by affecting the development, differentiation, and function of immune cells, as well as by modulating cellular signaling pathways[48,49,50]. Studies have shown that the expression of the TREM2 gene in microglia regulates their phagocytic activity and inflammatory responses, while mutations in the PSEN1 gene affect γ-secretase activity, thereby influencing Aβ production and immune cell activation[51,52,53,54]. Furthermore, the association between genetic variations and immune biomarkers provides new insights into the pathological mechanisms of AD. Specifically, certain genetic variations can lead to abnormal expression of immune biomarkers, triggering or exacerbating inflammatory responses. For instance, the APOE ε4 allele is closely associated with elevated levels of the inflammatory markers IL-6 and TNF-α, and mutations in the TREM2 gene affect the inflammatory responses of microglia, further promoting AD progression[55,56,57,58].
In the pathological process of AD, microglia and astrocytes play crucial roles, exhibiting dual functions. On one hand, these glial cells exert protective effects by clearing Aβ plaques and neurofibrillary tangles, secreting anti-inflammatory cytokines such as IL-10 and TGF-β, promoting tissue repair, and maintaining neural system homeostasis[59,60,61]. On the other hand, overactivated microglia and astrocytes can trigger chronic inflammatory responses, releasing large amounts of pro-inflammatory cytokines such as TNF-α and IL-1β[62,63,64]. These pro-inflammatory factors not only exacerbate neuroinflammation, leading to neuronal damage and death, but also promote the production of Aβ and the hyperphosphorylation of Tau protein by activating signaling pathways such as NF-κB, creating a vicious cycle that drives AD's pathological progression[65,66].
3. Integrated Analysis of Genetic and Immune Profiles
3.1. Integration Methods for Multi-Omics Data
In the study of AD, the integration of genomics, transcriptomics, and proteomics serves as crucial tools for revealing the intricate molecular mechanisms underlying the disease. Genomics, through genome-wide association studies (GWAS), identifies genetic variants related to AD, with studies demonstrating that the APOE ε4 gene is a primary genetic risk factor for AD. These gene variants not only influence the generation and clearance of Aβ but may also intensify neuroinflammation by affecting immune cell function[67,68,69,70]. Transcriptomics offers insights into dynamic alterations in gene expression. Utilizing single-cell RNA sequencing technology allows for detailed analysis of gene expression differences across various cell types during AD progression[71,72]. Relevant research has discovered that microglia in the brains of AD patients display specific transcriptional state alterations, which are closely associated with inflammatory responses and lipid metabolism. Proteomics complements genomics and transcriptomics data by examining protein expression and functionality, thereby uncovering the ultimate products of gene expression and their roles in the disease[73,74]. Proteome-wide association studies combine GWAS findings with proteomic data, enabling the identification of genes that elevate AD risk by influencing protein abundance. Bioinformatics tools and algorithms are essential for the integrative analysis of multi-omics datasets[75]. Weighted gene co-expression network analysis (WGCNA) is a frequently employed approach to identify gene modules related to AD and their pivotal hub genes. By constructing gene co-expression networks, researchers can pinpoint gene modules closely linked to disease progression and further elucidate their potential biological significance through functional annotation[76]. Furthermore, machine learning and artificial intelligence technologies are extensively utilized in the integration and analysis of multi-omics datasets[77]. Approaches like deep learning can autonomously discern underlying patterns and trends from complex multi-omics data, aiding in the identification of novel biomarkers and disease prediction (Figure 2)[78].
3.2. Identification and Validation of Biomarkers
Genomic data play a crucial role in the discovery of biomarkers for AD. Utilizing high-throughput genomics technologies, researchers can identify genes associated with AD and analyze their expression patterns[79]. For instance, the strong association between the APOE ε4 genotype and Aβ pathology has been extensively studied. Moreover, the application of machine learning algorithms has significantly enhanced the efficiency and accuracy of gene data analysis. By employing algorithms such as support vector machines and random forests, predictive models can be constructed to distinguish AD patients from healthy control groups[80,81,82,83]. The immune system is integral to the pathological process of AD. Studies have found that inflammatory markers such as sTREM2 and YKL-40 are elevated in AD patients, serving as biomarkers for neuroinflammation[84]. Furthermore, the activation of immune cells like microglia is closely related to AD progression, and proteins involved in immune signaling pathways may also serve as potential biomarkers. By combining immuno-omics analysis with machine learning methods, these immune-related biomarkers can be more effectively screened and validated[85,86]. The discovery of novel biomarkers opens new possibilities for the early diagnosis and treatment monitoring of AD. Related studies have shown that plasma levels of p-tau181 exhibit high diagnostic accuracy in the early stages of AD[87,88]. Additionally, comprehensive models that integrate multiple biomarkers and clinical data can further enhance diagnostic sensitivity and specificity. This approach not only facilitates the early identification of AD patients but also provides a foundation for developing individualized treatment plans, thereby improving patient prognosis and quality of life[89,90].
3.3. Patient Stratification and Precision Therapeutics
Genetic variations play a crucial role in the onset and progression of Alzheimer's Disease (AD). The APOE ε4 allele stands out as one of the most significant genetic risk factors, with carriers exhibiting a higher incidence of AD and more rapid disease progression [91]. Moreover, other genetic mutations, such as those in APP, PSEN1, and PSEN2, are intimately linked to AD pathogenesis. Detecting these genetic mutations enables the categorization of patients into distinct genetic subtypes, thereby laying the foundation for personalized treatment approaches[92,93]. Beyond genetics, the immune system is pivotal in AD's pathological processes. Research indicates that inflammatory responses emerge early in AD and are closely associated with disease progression. By analyzing the types of immune cells and levels of inflammatory factors in patients, they can be classified into different immune subtypes[94]. For instance, elevated levels of pro-inflammatory factors like IL-1β and TNF-α suggest an active inflammatory state, whereas levels of anti-inflammatory factors such as IL-10 reflect the patients' immune regulatory status[95]. This stratification based on immune features aids in elucidating the mechanisms underlying inflammatory responses in AD and provides a basis for targeted immune regulation therapies.
Pathological changes in AD begin decades before clinical symptoms manifest. Therefore, the early identification of high-risk populations and timely interventions are essential for achieving precision treatment. For patients carrying high-risk genetic mutations, interventions such as lifestyle modifications and cognitive training can be implemented to delay disease onset and progression. The pathogenesis of AD is complex, involving multiple pathological processes, which is why single-treatment approaches often fall short of achieving optimal outcomes. Personalized treatment plans should comprehensively account for patients' genetic and immune characteristics, employing combination therapies that target multiple aspects of the disease[96]. For example, treatments may include β-secretase inhibitors to target Aβ deposition, tau aggregation inhibitors to address tau protein pathology, and non-steroidal anti-inflammatory drugs to mitigate neuroinflammation. Given the prolonged and intricate course of AD, patient conditions evolve over time[97]. Consequently, treatment plans should be dynamically adjusted in response to changes in patients' conditions. Regular monitoring of patients' genetic and immune biomarker levels allows for the assessment of treatment efficacy and disease progression, facilitating timely adjustments to treatment strategies[98]. Additionally, individual differences in drug metabolism and responses necessitate personalized treatment plans that determine appropriate drug dosages and administration methods based on patients' genetic profiles and drug metabolism capacities. Studies have shown that patients with mutations in drug-metabolizing enzyme genes may require dosage adjustments to prevent drug toxicity or enhance therapeutic efficacy[99].
4. Current Status and Future Prospects of Immunotherapy in AD
4.1. Types and Mechanisms of Immunotherapeutic Approaches
Passive immunotherapy involves the clearance of pathological proteins through the direct injection of specific monoclonal antibodies into patients. For example, Aducanumab, Lecanemab, and Donanemab have been approved by the United States Food and Drug Administration (FDA) for the treatment of early AD[100]. These antibodies bind to Aβ, promoting its clearance and thereby slowing cognitive decline. However, some side effects, such as brain edema and microhemorrhages, have been observed in clinical trials. Therefore, optimizing the structure of antibodies and their administration strategies to enhance safety and efficacy is an important direction for future research[101].
Active immunotherapy stimulates the body's immune response by injecting antigens or vaccines, thereby clearing pathological proteins. Early studies on Aβ vaccines demonstrated that vaccination could reduce Aβ deposition and improve cognitive function in animal models. However, early human clinical trials were terminated due to the occurrence of meningitis in some patients. In recent years, researchers have reduced the incidence of side effects by improving antigen design and adjuvant selection for vaccines[102]. Related studies have shown that using non-Aβ peptides folded into conformations similar to Aβ oligomers as antigens can effectively reduce Aβ deposition and improve cognitive function. Nevertheless, active immunotherapy still faces numerous challenges in clinical applications, such as individual differences in immune responses and the maintenance of long-term immune memory[103,104].
Cell therapy involves transplanting specific immune cells or stem cells into patients to enhance immune responses or repair damaged neural tissue. Some studies attempt to use patients' own stem cells differentiated into neurons or glial cells to replace damaged neural cells. Furthermore, genetically engineered T cells, such as CAR-T cells, are also being explored for the clearance of pathological proteins[105,106,107]. However, the clinical application of cell therapy is still in its early stages, and its safety and efficacy need further validation(Table 1).
4.2. Review and Analysis of Clinical Trials
The clinical evaluation of Aducanumab primarily encompasses two Phase III studies, EMERGE and ENGAGE. Both studies are randomized, double-blind, placebo-controlled, multicenter trials designed to assess the efficacy and safety of Aducanumab in patients with early AD. The EMERGE and ENGAGE trials enrolled thousands of patients with mild cognitive impairment and mild AD, lasted 78 weeks, and treated them with varying doses of Aducanumab, notably the high dose of 10 mg/kg[108]. In the EMERGE trial, the high-dose Aducanumab treatment group exhibited a 30% reduction in Clinical Dementia Rating-Sum of Boxes (CDR-SB) scores at 78 weeks, indicating significant alleviation of disease symptoms. However, in the ENGAGE trial, the difference in CDR-SB scores between the Aducanumab treatment group and the placebo group did not achieve statistical significance. This discrepancy in results may be attributed to differences in patients' baseline characteristics, stages of disease progression, and treatment doses[109]. The Phase III clinical trial of Lecanemab, Clarity AD, is a randomized, double-blind, placebo-controlled study that included approximately 2,000 patients with early AD. The trial aims to evaluate the impact of Lecanemab on cognitive function and Aβ deposition, lasts 18 months, and administers a fixed dose[110]. The results of the Clarity AD trial demonstrated that Lecanemab could slow the rate of cognitive and functional decline by 27% in patients and significantly reduce their Aβ levels. Additionally, Lecanemab showed statistically significant benefits on three secondary endpoints related to cognition and function. These findings indicate that Lecanemab has potential clinical benefits in delaying the progression of AD[111,112]. The success of Lecanemab is attributable to its precise target selection and optimized clinical trial design. The drug selectively neutralizes soluble and toxic Aβ aggregates, thereby reducing non-specific binding and side effects[113] . Furthermore, stringent patient selection and stratification strategies ensured the reliability of the trial results. These factors collectively contributed to the favorable performance of Lecanemab in clinical trials[114]. Although Aducanumab demonstrated significant efficacy in a subset of patients with high-dose treatment in the EMERGE trial, the failure of the ENGAGE trial underscores the importance of individualized therapy. The variability in ENGAGE trial results suggests that clinical trial designs must adequately consider patients' baseline characteristics and individual differences to prevent inconsistent efficacy due to population heterogeneity. Additionally, the selection of drug dosages and the optimization of administration protocols remain key focus areas for future research[115].
4.3. Strategies and Future Directions for Personalized Immunotherapy
Advances in genomics have enabled researchers to identify specific gene variations associated with AD, thereby designing targeted therapeutic strategies. By targeting gene variations of Aβ and tau proteins, specific small molecule drugs or monoclonal antibodies can be developed. Furthermore, gene editing technologies like CRISPR/Cas9 offer new possibilities for personalized gene therapy, allowing the direct repair or replacement of pathogenic genes. This approach not only enhances the specificity of treatment but also reduces damage to normal cells, providing patients with more precise therapeutic options[116,117,118,119]. Additionally, the development of immunomodulatory drugs is a crucial aspect of personalized immunotherapy. In recent years, drugs targeting immune checkpoints such as PD-1/PD-L1 and CTLA-4 inhibitors have achieved significant success in treating various diseases. In AD, modulating the immune system's response to Aβ and tau proteins can enhance the clearance of pathological proteins. Moreover, the design of personalized vaccines is continually advancing[120,121]. Studies indicate that personalized nano-vaccines developed using patients' own tumor cell membrane vesicles can activate immune responses targeting specific antigens, thereby enhancing the immunogenicity and specificity of vaccines and providing more effective therapeutic options[122,123,124]. Case studies on comprehensive personalized strategies demonstrate that multidisciplinary collaboration and data sharing are key to advancing personalized immunotherapies. For example, the International Alzheimer's Disease Neuroimaging Initiative database offers researchers worldwide a wealth of data resources. By integrating patients' genomic data, proteomic data, and clinical information, researchers can better understand the complexity of AD and develop personalized treatment plans[125,126]. The establishment of data-sharing platforms enables the sharing of clinical trial data, biomarker information, and treatment response data, thereby accelerating the development and validation of new therapies. This comprehensive strategy not only improves research efficiency but also provides patients with more comprehensive and precise treatment plans[127,128,129].
5. Conclusions and Perspectives
In recent years, the potential of personalized immunotherapy for AD treatment has increasingly garnered attention. Personalized immunotherapy involves designing individualized treatment plans by targeting patients' specific immune statuses and genetic backgrounds, thereby enhancing efficacy and reducing side effects. For instance, second-generation antibodies such as Lecanemab and Donanemab have demonstrated good blood-brain barrier permeability and effective Aβ clearance in clinical trials. The integration of genetic backgrounds and immune statuses is particularly important in AD treatment, as studies have shown that different genotypes can influence individuals' responses to immunotherapy. For example, carriers of the APOE ε4 allele, which plays a significant role in AD pathogenesis, may exhibit immune responses that differ markedly from non-carriers. Additionally, patients' immune statuses—such as levels of inflammatory factors and immune cell functions—also impact the efficacy of immunotherapy. Therefore, integrating genetic background and immune status information can more accurately predict patients' treatment responses, thereby optimizing treatment plans. Future research should further investigate the specific mechanisms and optimization strategies of personalized immunotherapy in AD. This includes a deep exploration of how different genotypes and immune statuses affect immunotherapy responses to better understand their underlying principles. Moreover, combining advanced bioinformatics technologies with artificial intelligence algorithms can aid in developing more precise patient stratification and treatment prediction models. Additionally, clinical trial designs should place greater emphasis on personalization, validating the safety and efficacy of personalized immunotherapy across different populations through multicenter, large-scale studies.
Author Contributions
Conceptualization, Data curation, Writing – original draft, C.H.; Writing – review & editing, Validation, Y.S.; Funding acquisition, Writing – review & editing, X.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Shenzhen Municipal Science and Technology Planning Project, grant number JCYJ20210324122210028.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
References
- Global Nutrition Target, C. Global, regional, and national progress towards the 2030 global nutrition targets and forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2025, 404, 2543–2583. [Google Scholar]
- Synnott, P.G.; Majda, T.; Lin, P.J.; Ollendorf, D.A.; Zhu, Y.; Kowal, S. Modeling the Population Equity of Alzheimer Disease Treatments in the US. JAMA Netw Open 2024, 7, e2442353. [Google Scholar] [CrossRef]
- Safiri, S.; Ghaffari Jolfayi, A.; Fazlollahi, A.; Morsali, S.; Sarkesh, A.; Daei Sorkhabi, A.; Golabi, B.; Aletaha, R.; Motlagh Asghari, K.; Hamidi, S.; Mousavi, S.E.; Jamalkhani, S.; Karamzad, N.; Shamekh, A.; Mohammadinasab, R.; Sullman, M.J.M.; Sahin, F.; Kolahi, A.A. Alzheimer's disease: a comprehensive review of epidemiology, risk factors, symptoms diagnosis, management, caregiving, advanced treatments and associated challenges. Front Med (Lausanne) 2024, 11, 1474043. [Google Scholar] [CrossRef]
- Lennon, M.J.; Lipnicki, D.M.; Lam, B.C.P.; Crawford, J.D.; Schutte, A.E.; Peters, R.; Rydberg-Sterner, T.; Najar, J.; Skoog, I.; Riedel-Heller, S.G.; Rohr, S.; Pabst, A.; Lobo, A.; De-la-Camara, C.; Lobo, E.; Lipton, R.B.; Katz, M.J.; Derby, C.A.; Kim, K.W.; Han, J.W.; Oh, D.J.; Rolandi, E.; Davin, A.; Rossi, M.; Scarmeas, N.; Yannakoulia, M.; Dardiotis, T.; Hendrie, H.C.; Gao, S.; Carriere, I.; Ritchie, K.; Anstey, K.J.; Cherbuin, N.; Xiao, S.; Yue, L.; Li, W.; Guerchet, M.; Preux, P.M.; Aboyans, V.; Haan, M.N.; Aiello, A.; Scazufca, M.; Sachdev, P.S.; as the Cohort Studies of Memory in an International Consortium, G. Blood Pressure, Antihypertensive Use, and Late-Life Alzheimer and Non-Alzheimer Dementia Risk: An Individual Participant Data Meta-Analysis. Neurology 2024, 103, e209715. [Google Scholar]
- Landeiro, F.; Harris, C.; Groves, D.; O'Neill, S.; Jandu, K.S.; Tacconi, E.M.C.; Field, S.; Patel, N.; Gopfert, A.; Hagson, H.; Leal, J.; Luengo-Fernandez, R. The economic burden of cancer, coronary heart disease, dementia, and stroke in England in 2018, with projection to 2050: an evaluation of two cohort studies. Lancet Healthy Longev 2024, 5, e514–e523. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.U.B. o. D. The burden of diseases, injuries, and risk factors by state in the USA, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 404, 2314–2340. [Google Scholar]
- Knecht, L.; Dalsbol, K.; Simonsen, A.H.; Pilchner, F.; Ross, J.A.; Winge, K.; Salvesen, L.; Bech, S.; Hejl, A.M.; Lokkegaard, A.; Hasselbalch, S.G.; Dodel, R.; Aznar, S.; Waldemar, G.; Brudek, T.; Folke, J. Autoantibody profiles in Alzheimer s, Parkinson s, and dementia with Lewy bodies: altered IgG affinity and IgG/IgM/IgA responses to alpha-synuclein, amyloid-beta, and tau in disease-specific pathological patterns. J Neuroinflammation 2024, 21, 317. [Google Scholar] [CrossRef] [PubMed]
- Mroke, P.; Goit, R.; Rizwan, M.; Tariq, S.; Rizwan, A.W.; Umer, M.; Nassar, F.F.; Torijano Sarria, A.J.; Singh, D.; Baig, I. Implications of the Gut Microbiome in Alzheimer's Disease: A Narrative Review. Cureus 2024, 16, e73681. [Google Scholar] [CrossRef]
- Zhang, Z.; Bai, J.; Zhang, S.; Wang, R.; Zhu, S.; Li, T.; Zhang, M. The Relationship Between Alzheimer's Disease and Pyroptosis and the Intervention Progress of Traditional Chinese Medicine. Int J Gen Med 2024, 17, 4723–4732. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Gong, Z.; Wang, Y.; Zhao, Y.; Lu, Y.; Sun, R.; Zhang, H.; Shang, J.; Zhang, J. Mutant NOTCH3ECD Triggers Defects in Mitochondrial Function and Mitophagy in CADASIL Cell Models. J Alzheimers Dis 2024, 100, 1299–1314. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Chen, N.; Wang, C. Frontiers and hotspots evolution in anti-inflammatory studies for Alzheimer's disease. Behav Brain Res 2024, 472, 115178. [Google Scholar] [CrossRef]
- Liu, P.P.; Liu, X.H.; Ren, M.J.; Liu, X.T.; Shi, X.Q.; Li, M.L.; Li, S.A.; Yang, Y.; Wang, D.D.; Wu, Y.; Yin, F.X.; Guo, Y.H.; Yang, R.Z.; Cheng, M.; Xin, Y.J.; Kang, J.S.; Huang, B.; Ren, K.D. Neuronal cathepsin S increases neuroinflammation and causes cognitive decline via CX3CL1-CX3CR1 axis and JAK2-STAT3 pathway in aging and Alzheimer's disease. Aging Cell 2024, e14393. [Google Scholar] [CrossRef] [PubMed]
- Gutierre, R.C.; Rocha, P.R.; Graciani, A.L.; Coppi, A.A.; Arida, R.M. Tau, amyloid, iron, oligodendrocytes ferroptosis, and inflammaging in the hippocampal formation of aged rats submitted to an aerobic exercise program. Brain Res 2024, 1850, 149419. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.W.; Khatib, L.A.; Heston, M.B.; Dilmore, A.H.; Labus, J.S.; Deming, Y.; Schimmel, L.; Blach, C.; McDonald, D.; Gonzalez, A.; Bryant, M.; Sanders, K.; Schwartz, A.; Ulland, T.K.; Johnson, S.C.; Asthana, S.; Carlsson, C.M.; Chin, N.A.; Blennow, K.; Zetterberg, H.; Rey, F.E.; Alzheimer Gut Microbiome Project, C.; Kaddurah-Daouk, R.; Knight, R.; Bendlin, B.B. Gut Microbiome Compositional and Functional Features Associate with Alzheimer's Disease Pathology. medRxiv 2024. [Google Scholar]
- Alfaro-Ruiz, R.; Martin-Belmonte, A.; Aguado, C.; Moreno-Martinez, A.E.; Fukazawa, Y.; Lujan, R. Selective disruption of synaptic NMDA receptors of the hippocampal trisynaptic circuit in Abeta pathology. Biol Res 2024, 57, 56. [Google Scholar] [CrossRef]
- Ali, J.; Choe, K.; Park, J.S.; Park, H.Y.; Kang, H.; Park, T.J.; Kim, M.O. The Interplay of Protein Aggregation, Genetics, and Oxidative Stress in Alzheimer's Disease: Role for Natural Antioxidants and Immunotherapeutics. Antioxidants (Basel) 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, W.; Wu, W.; Liu, Q.; You, M.; Liu, X.; Ye, C.; Chen, J.; Tan, Q.; Liu, G.; Du, Y. Effects of electroacupuncture on microglia phenotype and epigenetic modulation of C/EBPbeta in SAMP8 mice. Brain Res 2024, 1849, 149339. [Google Scholar] [CrossRef]
- Haessler, A.; Candlish, M.; Hefendehl, J.K.; Jung, N.; Windbergs, M. Mapping cellular stress and lipid dysregulation in Alzheimer-related progressive neurodegeneration using label-free Raman microscopy. Commun Biol 2024, 7, 1514. [Google Scholar] [CrossRef]
- Chilton, P.M.; Ghare, S.S.; Charpentier, B.T.; Myers, S.A.; Rao, A.V.; Petrosino, J.F.; Hoffman, K.L.; Greenwell, J.C.; Tyagi, N.; Behera, J.; Wang, Y.; Sloan, L.J.; Zhang, J.; Shields, C.B.; Cooper, G.E.; Gobejishvili, L.; Whittemore, S.R.; McClain, C.J.; Barve, S.S. Age-associated temporal decline in butyrate-producing bacteria plays a key pathogenic role in the onset and progression of neuropathology and memory deficits in 3xTg-AD mice. Gut Microbes 2024, 16, 2389319. [Google Scholar] [CrossRef]
- Qian, X.H.; Ding, G.Y.; Chen, S.Y.; Liu, X.L.; Zhang, M.; Tang, H.D. Blood Cathepsins on the Risk of Alzheimer's Disease and Related Pathological Biomarkers: Results from Observational Cohort and Mendelian Randomization Study. J Prev Alzheimers Dis 2024, 11, 1834–1842. [Google Scholar] [CrossRef]
- Vida, H.; Sahar, M.; Nikdouz, A.; Arezoo, H. Chemokines in neurodegenerative diseases. Immunol Cell Biol 2024. [Google Scholar]
- Luo, X.; Luo, B.; Fei, L.; Zhang, Q.; Liang, X.; Chen, Y.; Zhou, X. MS4A superfamily molecules in tumors, Alzheimer's and autoimmune diseases. Front Immunol 2024, 15, 1481494. [Google Scholar] [CrossRef]
- Hammers, D.B.; Eloyan, A.; Thangarajah, M.; Taurone, A.; Beckett, L.; Gao, S.; Polsinelli, A.J.; Kirby, K.; Dage, J.L.; Nudelman, K.; Aisen, P.; Reman, R.; La Joie, R.; Lagarde, J.; Atri, A.; Clark, D.; Day, G.S.; Duara, R.; Graff-Radford, N.R.; Honig, L.S.; Jones, D.T.; Masdeu, J.C.; Mendez, M.F.; Womack, K.; Musiek, E.; Onyike, C.U.; Riddle, M.; Grant, I.; Rogalski, E.; Johnson, E.C.B.; Salloway, S.; Sha, S.J.; Turner, R.S.; Wingo, T.S.; Wolk, D.A.; Carrillo, M.C.; Dickerson, B.C.; Rabinovici, G.D.; Apostolova, L.G.; Initiative, L.C. f. t. A. s. D. N. Differences in baseline cognitive performance between participants with early-onset and late-onset Alzheimer's disease: Comparison of LEADS and ADNI. Alzheimers Dement 2024. [Google Scholar] [CrossRef] [PubMed]
- Alqabandi, J.A.; David, R.; Abdel-Motal, U.M.; ElAbd, R.O.; Youcef-Toumi, K. An innovative cellular medicine approach via the utilization of novel nanotechnology-based biomechatronic platforms as a label-free biomarker for early melanoma diagnosis. Sci Rep 2024, 14, 30107. [Google Scholar] [PubMed]
- Hrybouski, S.; Das, S.R.; Xie, L.; Brown, C.A.; Flamporis, M.; Lane, J.; Nasrallah, I.M.; Detre, J.A.; Yushkevich, P.A.; Wolk, D.A. BOLD Amplitude Correlates of Preclinical Alzheimer's Disease. medRxiv 2024. [Google Scholar]
- Heneka, M.T.; Morgan, D.; Jessen, F. Passive anti-amyloid beta immunotherapy in Alzheimer's disease-opportunities and challenges. Lancet 2024, 404, 2198–2208. [Google Scholar] [CrossRef]
- Zou, Y.; Wang, C.; Li, H.; Zhong, M.; Lin, J.; Hu, Y.; Chen, Z.; Gan, C.L. Epileptic seizures induced by pentylenetetrazole kindling accelerate Alzheimer-like neuropathology in 5xFAD mice. Front Pharmacol 2024, 15, 1500105. [Google Scholar] [CrossRef]
- Chen, Y.; Qi, Y.; Hu, Y.; Qiu, X.; Qiu, T.; Li, S.; Liu, M.; Jia, Q.; Sun, B.; Liu, C.; Li, T.; Le, W.; Alzheimer's Disease Neuroimaging, I. Integrated cerebellar radiomic-network model for predicting mild cognitive impairment in Alzheimer's disease. Alzheimers Dement 2024. [Google Scholar] [CrossRef]
- Aisen, P.; Bateman, R.J.; Crowther, D.; Cummings, J.; Dwyer, J.; Iwatsubo, T.; Kosco-Vilbois, M.; McDade, E.; Mohs, R.; Scheltens, P.; Sperling, R.; Selkoe, D. The case for regulatory approval of amyloid-lowering immunotherapies in Alzheimer's disease based on clearcut biomarker evidence. Alzheimers Dement 2024. [Google Scholar] [CrossRef]
- Nosheny, R.L.; Miller, M.; Conti, C.; Flenniken, D.; Ashford, M.; Diaz, A.; Fockler, J.; Truran, D.; Kwang, W.; Kanoria, S.; Veitch, D.; Green, R.C.; Weiner, M.W.; Alzheimer's Disease Neuroimaging, I. The ADNI Administrative Core: Ensuring ADNI's success and informing future AD clinical trials. Alzheimers Dement 2024, 20, 9004–9013. [Google Scholar] [CrossRef] [PubMed]
- Menendez-Gonzalez, M. Therapeutic Challenges Derived from the Interaction Among Apolipoprotein E, Cholesterol, and Amyloid in Alzheimer's Disease. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Carracedo, S.; Launay, A.; Dechelle-Marquet, P.A.; Faivre, E.; Blum, D.; Delarasse, C.; Boue-Grabot, E. Purinergic-associated immune responses in neurodegenerative diseases. Prog Neurobiol 2024, 243, 102693. [Google Scholar] [CrossRef]
- Qu, L.; Xu, S.; Lan, Z.; Fang, S.; Xu, Y.; Zhu, X. Apolipoprotein E in Alzheimer's Disease: Focus on Synaptic Function and Therapeutic Strategy. Mol Neurobiol 2024. [Google Scholar] [CrossRef]
- Zhang, L.; Xia, Y.; Gui, Y. Neuronal ApoE4 in Alzheimer's disease and potential therapeutic targets. Front Aging Neurosci 2023, 15, 1199434. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.Y.; Wang, Z.; Huang, H.C. Roles of ApoE4 on the Pathogenesis in Alzheimer's Disease and the Potential Therapeutic Approaches. Cell Mol Neurobiol 2023, 43, 3115–3136. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.F. The problem of multiple adjustments in the assessment of minimal clinically important differences. Alzheimers Dement (N Y) 2025, 11, e70032. [Google Scholar] [CrossRef]
- Kannan, L.; Lelo de Larrea-Mancera, E.S.; Maniglia, M.; Vodyanyk, M.M.; Gallun, F.J.; Jaeggi, S.M.; Seitz, A.R. Multidimensional relationships between sensory perception and cognitive aging. Front Aging Neurosci 2024, 16, 1484494. [Google Scholar] [CrossRef]
- Sabouri, S.; Rostamirad, M.; Dempski, R.E. Unlocking the brain's zinc code: implications for cognitive function and disease. Front Biophys 2024, 2. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Liu, H.; Zhang, M.; Li, Y. Mapping the current trends and hotspots of extracellular vesicles in Alzheimer's disease: a bibliometric analysis. Front Aging Neurosci 2024, 16, 1485750. [Google Scholar] [CrossRef]
- Valdes, P.; Caldwell, A.B.; Liu, Q.; Fitzgerald, M.Q.; Ramachandran, S.; Karch, C.M.; Dominantly Inherited Alzheimer, N.; Galasko, D.R.; Yuan, S.H.; Wagner, S.L.; Subramaniam, S. Integrative multiomics reveals common endotypes across PSEN1, PSEN2, and APP mutations in familial Alzheimer's disease. Alzheimers Res Ther 2025, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Liu, H.; Liu, X.; Zhang, W.; Zhang, S.; Jiao, B. APP, PSEN1, and PSEN2 Variants in Alzheimer's Disease: Systematic Re-evaluation According to ACMG Guidelines. Front Aging Neurosci 2021, 13, 695808. [Google Scholar] [CrossRef] [PubMed]
- Mullan, M.; Crawford, F.; Buchanan, J. Technical feasibility of genetic testing for Alzheimer's disease. Alzheimer Dis Assoc Disord 1994, 8, 102–15. [Google Scholar] [CrossRef] [PubMed]
- Hutton, M.; Hardy, J. The presenilins and Alzheimer's disease. Hum Mol Genet 1997, 6, 1639–46. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Zhang, Y.; Sterling, K.; Song, W. Brain-derived neurotrophic factor in Alzheimer's disease and its pharmaceutical potential. Transl Neurodegener 2022, 11, 4. [Google Scholar] [CrossRef]
- Weninger, S.; Irizarry, M.C.; Fleisher, A.S.; Leon, T.; Maruff, P.; Miller, D.S.; Seleri, S.; Carrillo, M.C.; Weber, C.J. Alzheimer's disease drug development in an evolving therapeutic landscape. Alzheimers Dement (N Y) 2024, 10, e70015. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, U.; Briceno, E.; Sharma, U.; Bogati, U.; Sharma, A.; Shrestha, L.; Ghimire, D.; Mendes de Leon, C.F. Health care systems and policies for older adults in Nepal: new challenges for a low-middle income country. Discov Public Health 2024, 21, 256. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.K.S.; Udeh-Momoh, C.; Lim, M.A.; Gleerup, H.S.; Leifert, W.; Ajalo, C.; Ashton, N.; Zetterberg, H.; Rissman, R.A.; Winston, C.N.; S, O.B.; Jenkins, R.; Carro, E.; Orive, G.; Tamburin, S.; Olvera-Rojas, M.; Solis-Urra, P.; Esteban-Cornejo, I.; Santos, G.; Rajan, K.B.; Koh, D.; Simonsen, A.H.; Slowey, P.D.; et al. Guidelines for the standardization of pre-analytical variables for salivary biomarker studies in Alzheimer's disease research: An updated review and consensus of the Salivary Biomarkers for Dementia Research Working Group. Alzheimers Dement 2024. [Google Scholar] [CrossRef]
- Zgorzynska, E. TREM2 in Alzheimer's disease: Structure, function, therapeutic prospects, and activation challenges. Mol Cell Neurosci 2024, 128, 103917. [Google Scholar] [CrossRef]
- Wijesinghe, P.; Li, H.R.; Ai, Z.; Campbell, M.; Chen, S.X.; Xi, J.; Pham, W.; Matsubara, J.A. Apolipoprotein E dysfunction in Alzheimer's disease: a study on miRNA regulation, glial markers, and amyloid pathology. Front Aging Neurosci 2024, 16, 1495615. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xi, J.; Zhang, M.; Wang, J. Identification of potential therapeutic targets for Alzheimer's disease from the proteomes of plasma and cerebrospinal fluid in a multicenter Mendelian randomization study. Int J Biol Macromol 2025, 139394. [Google Scholar] [CrossRef]
- Roveta, F.; Bonino, L.; Piella, E.M.; Rainero, I.; Rubino, E. Neuroinflammatory Biomarkers in Alzheimer's Disease: From Pathophysiology to Clinical Implications. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Guo, Q.; Tian, J.; Liu, W.; Wang, X. TREM2 bridges microglia and extracellular microenvironment: Mechanistic landscape and therapeutical prospects on Alzheimer's disease. Ageing Res Rev 2025, 103, 102596. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.Y.; Liu, J.; Liu, Z.H.; Liu, X.Y.; Tuo, J.M.; Li, J.H.; Tu, Y.F.; Tan, Q.; Ma, Y.Y.; Bai, Y.D.; Xin, J.Y.; Huang, S.; Zeng, G.H.; Shi, A.Y.; Wang, J.; Liu, Y.H.; Bu, X.L.; Ye, L.L.; Wan, Y.; Liu, T.F.; Chen, X.W.; Qiu, Z.L.; Gao, C.Y.; Wang, Y.J. Roles of blood monocytes carrying TREM2(R47H) mutation in pathogenesis of Alzheimer's disease and its therapeutic potential in APP/PS1 mice. Alzheimers Dement 2024. [Google Scholar]
- Beydoun, M.A.; Beydoun, H.A.; Li, Z.; Hu, Y.H.; Noren Hooten, N.; Ding, J.; Hossain, S.; Maino Vieytes, C.A.; Launer, L.J.; Evans, M.K.; Zonderman, A.B. Alzheimer's Disease polygenic risk, the plasma proteome, and dementia incidence among UK older adults. Geroscience 2024. [Google Scholar] [CrossRef] [PubMed]
- Bagyinszky, E.; An, S.S.A. Haploinsufficiency and Alzheimer's Disease: The Possible Pathogenic and Protective Genetic Factors. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Baligacs, N.; Albertini, G.; Borrie, S.C.; Serneels, L.; Pridans, C.; Balusu, S.; De Strooper, B. Homeostatic microglia initially seed and activated microglia later reshape amyloid plaques in Alzheimer's Disease. Nat Commun 2024, 15, 10634. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Huang, L.Y.; Guo, H.H.; Liu, M.; Zhang, Y.Y.; Zhang, Z.Q.; Hao, Q.; Tan, C.C.; Tan, L. Higher CSF sTREM2 attenuates APOE epsilon4-related risk for amyloid pathology in cognitively intact adults: The CABLE study. J Neurochem 2025, 169, e16273. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Miller, G.W.; Vardarajan, B.N.; Baccarelli, A.A.; Guo, Z.; Liu, Z. Deciphering proteins in Alzheimer's disease: A new Mendelian randomization method integrated with AlphaFold3 for 3D structure prediction. Cell Genom 2024, 4, 100700. [Google Scholar] [CrossRef]
- Guenoun, D.; Blaise, N.; Sellam, A.; Roupret-Serzec, J.; Jacquens, A.; Steenwinckel, J.V.; Gressens, P.; Bokobza, C. Microglial Depletion, a New Tool in Neuroinflammatory Disorders: Comparison of Pharmacological Inhibitors of the CSF-1R. Glia 2024. [Google Scholar] [CrossRef]
- Weinstock, M. Therapeutic agents for Alzheimer's disease: a critical appraisal. Front Aging Neurosci 2024, 16, 1484615. [Google Scholar] [CrossRef]
- Song, X.; Wang, C.; Ding, Q.; Li, P.; Sun, S.; Wei, W.; Zhang, J.; Sun, R.; Yin, L.; Liu, S.; Pu, Y. Modulation of beta secretase and neuroinflammation by biomimetic nanodelivery system for Alzheimer's disease therapy. J Control Release 2024, 378, 735–749. [Google Scholar] [CrossRef] [PubMed]
- Gonul, C.P.; Kiser, C.; Yaka, E.C.; Oz, D.; Hunerli, D.; Yerlikaya, D.; Olcum, M.; Keskinoglu, P.; Yener, G.; Genc, S. Microglia-like cells from patient monocytes demonstrate increased phagocytic activity in probable Alzheimer's disease. Mol Cell Neurosci 2024, 132, 103990. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Gu, T.; Yu, P.; Zhang, Z.; Wei, Z. The role of microglia in Neuroinflammation associated with cardiopulmonary bypass. Front Cell Neurosci 2024, 18, 1496520. [Google Scholar] [CrossRef] [PubMed]
- Flury, A.; Aljayousi, L.; Park, H.J.; Khakpour, M.; Mechler, J.; Aziz, S.; McGrath, J.D.; Deme, P.; Sandberg, C.; Gonzalez Ibanez, F.; Braniff, O.; Ngo, T.; Smith, S.; Velez, M.; Ramirez, D.M.; Avnon-Klein, D.; Murray, J.W.; Liu, J.; Parent, M.; Mingote, S.; Haughey, N.J.; Werneburg, S.; Tremblay, M.E.; Ayata, P. A neurodegenerative cellular stress response linked to dark microglia and toxic lipid secretion. Neuron 2024. [Google Scholar] [CrossRef] [PubMed]
- Haessler, A.; Gier, S.; Jung, N.; Windbergs, M. The Abeta(42):Abeta(40) ratio modulates aggregation in beta-amyloid oligomers and drives metabolic changes and cellular dysfunction. Front Cell Neurosci 2024, 18, 1516093. [Google Scholar] [CrossRef] [PubMed]
- Vasilopoulou, F.; Piers, T.M.; Wei, J.; Hardy, J.; Pocock, J.M. Amelioration of signaling deficits underlying metabolic shortfall in TREM2(R47H) human iPSC-derived microglia. FEBS J 2024. [Google Scholar] [CrossRef] [PubMed]
- Bello-Corral, L.; Seco-Calvo, J.; Molina Fresno, A.; Gonzalez, A.I.; Llorente, A.; Fernandez-Lazaro, D.; Sanchez-Valdeon, L. Prevalence of ApoE Alleles in a Spanish Population of Patients with a Clinical Diagnosis of Alzheimer's Disease: An Observational Case-Control Study. Medicina (Kaunas) 2024, 60. [Google Scholar] [CrossRef]
- Grau-Jurado, P.; Mostafaei, S.; Xu, H.; Mo, M.; Petek, B.; Kalar, I.; Naia, L.; Kele, J.; Maioli, S.; Pereira, J.B.; Eriksdotter, M.; Chatterjee, S.; Garcia-Ptacek, S. Medications and cognitive decline in Alzheimer's disease: Cohort cluster analysis of 15,428 patients. J Alzheimers Dis 2025, 13872877241307870. [Google Scholar] [CrossRef] [PubMed]
- Visscher, P.M.; Gyngell, C.; Yengo, L.; Savulescu, J. Heritable polygenic editing: the next frontier in genomic medicine? Nature 2025. [Google Scholar] [CrossRef]
- Graham, A.C.; Bellou, E.; Harwood, J.C.; Yaman, U.; Celikag, M.; Magusali, N.; Rambarack, N.; Botia, J.A.; Sala Frigerio, C.; Hardy, J.; Escott-Price, V.; Salih, D.A. Human longevity and Alzheimer's disease variants act via microglia and oligodendrocyte gene networks. Brain 2025. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhu, H.; Deng, L.; Xu, S.; Xie, W.; Li, M.; Wang, R.; Tie, L.; Zhan, L.; Yu, G. Spatial Transcriptomics: Biotechnologies, Computational Tools, and Neuroscience Applications. Small Methods 2025, e2401107. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.N.; Jayadev, S.; Prater, K.E. Microglial Responses to Alzheimer's Disease Pathology: Insights From "Omics" Studies. Glia 2025. [Google Scholar] [CrossRef]
- Shwab, E.K.; Man, Z.; Gingerich, D.C.; Gamache, J.; Garrett, M.E.; Serrano, G.E.; Beach, T.G.; Crawford, G.E.; Ashley-Koch, A.E.; Chiba-Falek, O. Comparative mapping of single-cell transcriptomic landscapes in neurodegenerative diseases. bioRxiv 2024. [Google Scholar]
- He, Y.; Lu, W.; Zhou, X.; Mu, J.; Shen, W. Unraveling Alzheimer's disease: insights from single-cell sequencing and spatial transcriptomic. Front Neurol 2024, 15, 1515981. [Google Scholar] [CrossRef]
- Azargoonjahromi, A.; Alzheimer's Disease Neuroimaging, I. Serotonin enhances neurogenesis biomarkers, hippocampal volumes, and cognitive functions in Alzheimer's disease. Mol Brain 2024, 17, 93. [Google Scholar] [CrossRef]
- Hu, R.T.; Yu, Q.; Zhou, S.D.; Yin, Y.X.; Hu, R.G.; Lu, H.P.; Hu, B.L. Co-expression Network Analysis Reveals Novel Genes Underlying Alzheimer's Disease Pathogenesis. Front Aging Neurosci 2020, 12, 605961. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Liu, X.; Zuo, F.; Shi, H.; Jing, J. Artificial intelligence-based multi-omics analysis fuels cancer precision medicine. Semin Cancer Biol 2023, 88, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Ballard, J.L.; Wang, Z.; Li, W.; Shen, L.; Long, Q. Deep learning-based approaches for multi-omics data integration and analysis. BioData Min 2024, 17, 38. [Google Scholar] [CrossRef]
- Bolivar, D.A.; Mosquera-Heredia, M.I.; Vidal, O.M.; Barcelo, E.; Allegri, R.; Morales, L.C.; Silvera-Redondo, C.; Arcos-Burgos, M.; Garavito-Galofre, P.; Velez, J.I. Exosomal mRNA Signatures as Predictive Biomarkers for Risk and Age of Onset in Alzheimer's Disease. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Ibanez, L.; Liu, M.; Beric, A.; Timsina, J.; Kholfeld, P.; Bergmann, K.; Lowery, J.; Sykora, N.; Sanchez-Montejo, B.; Brock, W.; Budde, J.P.; Bateman, R.J.; Barthelemy, N.; Schindler, S.E.; Holtzman, D.M.; Benzinger, T.L.S.; Xiong, C.; Tarawneh, R.; Moulder, K.; Morris, J.C.; Sung, Y.J.; Cruchaga, C. Benchmarking of a multi-biomarker low-volume panel for Alzheimer's Disease and related dementia research. medRxiv 2024. [Google Scholar] [CrossRef]
- Mastenbroek, S.E.; Sala, A.; Vallez Garcia, D.; Shekari, M.; Salvado, G.; Lorenzini, L.; Pieperhoff, L.; Wink, A.M.; Lopes Alves, I.; Wolz, R.; Ritchie, C.; Boada, M.; Visser, P.J.; Bucci, M.; Farrar, G.; Hansson, O.; Nordberg, A.K.; Ossenkoppele, R.; Barkhof, F.; Gispert, J.D.; Rodriguez-Vieitez, E.; Collij, L.E.; et al. Continuous beta-Amyloid CSF/PET Imbalance Model to Capture Alzheimer Disease Heterogeneity. Neurology 2024, 103, e209419. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Xie, Q.; Xie, J.; Ni, M.; Wang, J.; Gao, Y.; Wang, Y.; Tang, Q. Cerebrospinal Fluid Proteomics Identifies Potential Biomarkers for Early-Onset Alzheimer's Disease. J Alzheimers Dis 2024, 100, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Tosun, D.; Hausle, Z.; Iwaki, H.; Thropp, P.; Lamoureux, J.; Lee, E.B.; MacLeod, K.; McEvoy, S.; Nalls, M.; Perrin, R.J.; Saykin, A.J.; Shaw, L.M.; Singleton, A.B.; Lebovitz, R.; Weiner, M.W.; Blauwendraat, C.; Alzheimer's Disease Neuroimaging, I. A cross-sectional study of alpha-synuclein seed amplification assay in Alzheimer's disease neuroimaging initiative: Prevalence and associations with Alzheimer's disease biomarkers and cognitive function. Alzheimers Dement 2024, 20, 5114–5131. [Google Scholar] [CrossRef]
- Salvado, G.; Horie, K.; Barthelemy, N.R.; Vogel, J.W.; Pichet Binette, A.; Chen, C.D.; Aschenbrenner, A.J.; Gordon, B.A.; Benzinger, T.L.S.; Holtzman, D.M.; Morris, J.C.; Palmqvist, S.; Stomrud, E.; Janelidze, S.; Ossenkoppele, R.; Schindler, S.E.; Bateman, R.J.; Hansson, O. Disease staging of Alzheimer's disease using a CSF-based biomarker model. Nat Aging 2024, 4, 694–708. [Google Scholar] [CrossRef]
- Huang, X.; Li, Y.; Fowler, C.; Doecke, J.D.; Lim, Y.Y.; Drysdale, C.; Zhang, V.; Park, K.; Trounson, B.; Pertile, K.; Rumble, R.; Pickering, J.W.; Rissman, R.A.; Sarsoza, F.; Abdel-Latif, S.; Lin, Y.; Dore, V.; Villemagne, V.; Rowe, C.C.; Fripp, J.; Martins, R.; Wiley, J.S.; Maruff, P.; Mintzer, J.E.; Masters, C.L.; Gu, B.J. Leukocyte surface biomarkers implicate deficits of innate immunity in sporadic Alzheimer's disease. Alzheimers Dement 2023, 19, 2084–2094. [Google Scholar] [CrossRef]
- Howe, M.D.; Britton, K.J.; Joyce, H.E.; Menard, W.; Emrani, S.; Kunicki, Z.J.; Faust, M.A.; Dawson, B.C.; Riddle, M.C.; Huey, E.D.; Janelidze, S.; Hansson, O.; Salloway, S.P. Clinical application of plasma P-tau217 to assess eligibility for amyloid-lowering immunotherapy in memory clinic patients with early Alzheimer's disease. Alzheimers Res Ther 2024, 16, 154. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, M.; Cabrera-Pastor, A. Emerging Role of Extracellular Vesicles as Biomarkers in Neurodegenerative Diseases and Their Clinical and Therapeutic Potential in Central Nervous System Pathologies. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Gotze, K.; Vrillon, A.; Dumurgier, J.; Indart, S.; Sanchez-Ortiz, M.; Slimi, H.; Raynaud-Simon, A.; Cognat, E.; Martinet, M.; Zetterberg, H.; Blennow, K.; Hourregue, C.; Bouaziz-Amar, E.; Paquet, C.; Lilamand, M. Plasma neurofilament light chain as prognostic marker of cognitive decline in neurodegenerative diseases, a clinical setting study. Alzheimers Res Ther 2024, 16, 231. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Gabelli, C.; Puthenparampil, M.; Cosma, C.; Cagnin, A.; Gallo, P.; Soraru, G.; Pegoraro, E.; Zaninotto, M.; Antonini, A.; Moz, S.; Zambon, C.F.; Plebani, M.; Corbetta, M.; Basso, D. Blood biomarkers for Alzheimer's disease with the Lumipulse automated platform: Age-effect and clinical value interpretation. Clin Chim Acta 2025, 565, 120014. [Google Scholar] [CrossRef]
- Liampas, I.; Kyriakoulopoulou, P.; Karakoida, V.; Kavvoura, P.A.; Sgantzos, M.; Bogdanos, D.P.; Stamati, P.; Dardiotis, E.; Siokas, V. Blood-Based Biomarkers in Frontotemporal Dementia: A Narrative Review. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Huda, T.I.; Diaz, M.J.; Gozlan, E.C.; Chobrutskiy, A.; Chobrutskiy, B.I.; Blanck, G. Immunogenomics Parameters for Patient Stratification in Alzheimer's Disease. J Alzheimers Dis 2022, 88, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Higgins, I.A.; Wang, J.; Kennedy, I.A.; Iaccarino, L.; Burnham, S.C.; Pontecorvo, M.J.; Shcherbinin, S. Predicting regional tau accumulation with machine learning-based tau-PET and advanced radiomics. Alzheimers Dement (N Y) 2024, 10, e70005. [Google Scholar] [CrossRef]
- Smits, L.L.; Pijnenburg, Y.A.; Koedam, E.L.; van der Vlies, A.E.; Reuling, I.E.; Koene, T.; Teunissen, C.E.; Scheltens, P.; van der Flier, W.M. Early onset Alzheimer's disease is associated with a distinct neuropsychological profile. J Alzheimers Dis 2012, 30, 101–8. [Google Scholar] [CrossRef]
- Calvo-Rodriguez, M.; Garcia-Rodriguez, C.; Villalobos, C.; Nunez, L. Role of Toll Like Receptor 4 in Alzheimer's Disease. Front Immunol 2020, 11, 1588. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Yang, G.; Luo, Y.; Jiang, L.; Chi, H.; Tian, G. Neuroinflammation in Alzheimer's disease: insights from peripheral immune cells. Immun Ageing 2024, 21, 38. [Google Scholar] [CrossRef]
- Rochon, E.A.; Sy, M.; Phillips, M.; Anderson, E.; Plys, E.; Ritchie, C.; Vranceanu, A.M. Bio-Experiential Technology to Support Persons With Dementia and Care Partners at Home (TEND): Protocol for an Intervention Development Study. JMIR Res Protoc 2023, 12, e52799. [Google Scholar] [CrossRef]
- Murfield, J.; Moyle, W.; O'Donovan, A. Planning and designing a self-compassion intervention for family carers of people living with dementia: a person-based and co-design approach. BMC Geriatr 2022, 22, 53. [Google Scholar] [CrossRef]
- Navathe, A.S.; Volpp, K.G.; Caldarella, K.L.; Bond, A.; Troxel, A.B.; Zhu, J.; Matloubieh, S.; Lyon, Z.; Mishra Meza, A.; Sacks, L.; Nelson, C.; Patel, P.; Shea, J.; Calcagno, D.; Vittore, S.; Sokol, K.; Weng, K.; McDowald, N.; Crawford, P.; Small, D.; Emanuel, E.J. Effect of Financial Bonus Size, Loss Aversion, and Increased Social Pressure on Physician Pay-for-Performance: A Randomized Clinical Trial and Cohort Study. JAMA Netw Open 2019, 2, e187950. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.D.; Catalano, R.F.; Miller, J.Y. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull 1992, 112, 64–105. [Google Scholar] [CrossRef]
- Schreiner, T.G.; Croitoru, C.G.; Hodorog, D.N.; Cuciureanu, D.I. Passive Anti-Amyloid Beta Immunotherapies in Alzheimer's Disease: From Mechanisms to Therapeutic Impact. Biomedicines 2024, 12. [Google Scholar] [CrossRef]
- Yi, L.X.; Tan, E.K.; Zhou, Z.D. Passive immunotherapy for Alzheimer's disease: challenges & future directions. J Transl Med 2024, 22, 430. [Google Scholar]
- Winblad, B.; Graf, A.; Riviere, M.E.; Andreasen, N.; Ryan, J.M. Active immunotherapy options for Alzheimer's disease. Alzheimers Res Ther 2014, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Lacosta, A.M.; Pascual-Lucas, M.; Pesini, P.; Casabona, D.; Perez-Grijalba, V.; Marcos-Campos, I.; Sarasa, L.; Canudas, J.; Badi, H.; Monleon, I.; San-Jose, I.; Munuera, J.; Rodriguez-Gomez, O.; Abdelnour, C.; Lafuente, A.; Buendia, M.; Boada, M.; Tarraga, L.; Ruiz, A.; Sarasa, M. Safety, tolerability and immunogenicity of an active anti-Abeta(40) vaccine (ABvac40) in patients with Alzheimer's disease: a randomised, double-blind, placebo-controlled, phase I trial. Alzheimers Res Ther 2018, 10, 12. [Google Scholar] [CrossRef]
- Lambracht-Washington, D.; Rosenberg, R.N. Active DNA Abeta42 vaccination as immunotherapy for Alzheimer disease. Transl Neurosci 2012, 3, 307–313. [Google Scholar] [CrossRef]
- Ou, C.M.; Xue, W.W.; Liu, D.; Ma, L.; Xie, H.T.; Ning, K. Stem cell therapy in Alzheimer's disease: current status and perspectives. Front Neurosci 2024, 18, 1440334. [Google Scholar] [CrossRef]
- Cao, Z.; Kong, F.; Ding, J.; Chen, C.; He, F.; Deng, W. Promoting Alzheimer's disease research and therapy with stem cell technology. Stem Cell Res Ther 2024, 15, 136. [Google Scholar] [CrossRef] [PubMed]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; Garcia-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; Vina, J.; Gomez-Cabrera, M.C. Physical exercise in the prevention and treatment of Alzheimer's disease. J Sport Health Sci 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Mallinckrodt, C.; Tian, Y.; Aisen, P.S.; Barkhof, F.; Cohen, S.; Dent, G.; Hansson, O.; Harrison, K.; Iwatsubo, T.; Mummery, C.J.; Muralidharan, K.K.; Nestorov, I.; Nisenbaum, L.; Rajagovindan, R.; von Hehn, C.; van Dyck, C.H.; Vellas, B.; Wu, S.; Zhu, Y.; Sandrock, A.; Chen, T.; Budd Haeberlein, S. Investigating Partially Discordant Results in Phase 3 Studies of Aducanumab. J Prev Alzheimers Dis 2023, 10, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Budd Haeberlein, S.; Aisen, P.S.; Barkhof, F.; Chalkias, S.; Chen, T.; Cohen, S.; Dent, G.; Hansson, O.; Harrison, K.; von Hehn, C.; Iwatsubo, T.; Mallinckrodt, C.; Mummery, C.J.; Muralidharan, K.K.; Nestorov, I.; Nisenbaum, L.; Rajagovindan, R.; Skordos, L.; Tian, Y.; van Dyck, C.H.; Vellas, B.; Wu, S.; Zhu, Y.; Sandrock, A. Two Randomized Phase 3 Studies of Aducanumab in Early Alzheimer's Disease. J Prev Alzheimers Dis 2022, 9, 197–210. [Google Scholar] [CrossRef]
- Tarawneh, R.; Pankratz, V.S. The search for clarity regarding "clinically meaningful outcomes" in Alzheimer disease clinical trials: CLARITY-AD and Beyond. Alzheimers Res Ther 2024, 16, 37. [Google Scholar] [CrossRef]
- Honig, L.S.; Sabbagh, M.N.; van Dyck, C.H.; Sperling, R.A.; Hersch, S.; Matta, A.; Giorgi, L.; Gee, M.; Kanekiyo, M.; Li, D.; Purcell, D.; Dhadda, S.; Irizarry, M.; Kramer, L. Correction: Updated safety results from phase 3 lecanemab study in early Alzheimer's disease. Alzheimers Res Ther 2024, 16, 159. [Google Scholar] [CrossRef]
- Honig, L.S.; Sabbagh, M.N.; van Dyck, C.H.; Sperling, R.A.; Hersch, S.; Matta, A.; Giorgi, L.; Gee, M.; Kanekiyo, M.; Li, D.; Purcell, D.; Dhadda, S.; Irizarry, M.; Kramer, L. Updated safety results from phase 3 lecanemab study in early Alzheimer's disease. Alzheimers Res Ther 2024, 16, 105. [Google Scholar] [CrossRef] [PubMed]
- McDade, E.; Cummings, J.L.; Dhadda, S.; Swanson, C.J.; Reyderman, L.; Kanekiyo, M.; Koyama, A.; Irizarry, M.; Kramer, L.D.; Bateman, R.J. Lecanemab in patients with early Alzheimer's disease: detailed results on biomarker, cognitive, and clinical effects from the randomized and open-label extension of the phase 2 proof-of-concept study. Alzheimers Res Ther 2022, 14, 191. [Google Scholar] [CrossRef]
- Tampi, R.R.; Forester, B.P.; Agronin, M. Aducanumab: evidence from clinical trial data and controversies. Drugs Context 2021, 10. [Google Scholar] [CrossRef]
- Kuller, L.H.; Lopez, O.L. ENGAGE and EMERGE: Truth and consequences? Alzheimers Dement 2021, 17, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Ritchie, M.D. Is the Relationship Between Cardiovascular Disease and Alzheimer's Disease Genetic? A Scoping Review. Genes (Basel) 2024, 15. [Google Scholar] [CrossRef]
- Pettigrew, C.; Nazarovs, J.; Soldan, A.; Singh, V.; Wang, J.; Hohman, T.; Dumitrescu, L.; Libby, J.; Kunkle, B.; Gross, A.L.; Johnson, S.; Lu, Q.; Engelman, C.; Masters, C.L.; Maruff, P.; Laws, S.M.; Morris, J.C.; Hassenstab, J.; Cruchaga, C.; Resnick, S.M.; Kitner-Triolo, M.H.; An, Y.; Albert, M. Alzheimer's disease genetic risk and cognitive reserve in relationship to long-term cognitive trajectories among cognitively normal individuals. Alzheimers Res Ther 2023, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- Feldner, A.C.; Turner, A.K.; Simpson, J.F.; Estus, S. Skipping of FCER1G Exon 2 Is Common in Human Brain But Not Associated with the Alzheimer's Disease Genetic Risk Factor rs2070902. J Alzheimers Dis Rep 2023, 7, 1313–1322. [Google Scholar] [CrossRef]
- Whitson, H.E.; Potter, G.G.; Feld, J.A.; Plassman, B.L.; Reynolds, K.; Sloane, R.; Welsh-Bohmer, K.A. Dual-Task Gait and Alzheimer's Disease Genetic Risk in Cognitively Normal Adults: A Pilot Study. J Alzheimers Dis 2018, 64, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Suzuki, H.; Yoshiyama, T. Vanutide cridificar and the QS-21 adjuvant in Japanese subjects with mild to moderate Alzheimer's disease: results from two phase 2 studies. Curr Alzheimer Res 2015, 12, 242–54. [Google Scholar] [CrossRef]
- Chmatalova, Z.; Skoumalova, A. [Some aspects of the immune system in the pathogenesis of Alzehimers disease]. Epidemiol Mikrobiol Imunol 2016, 65, 79–84. [Google Scholar]
- Morgan, D.; Landreth, G.; Bickford, P. The promise and perils of an Alzheimer disease vaccine: a video debate. J Neuroimmune Pharmacol 2009, 4, 1–3. [Google Scholar] [CrossRef]
- Sterner, R.M.; Takahashi, P.Y.; Yu Ballard, A.C. Active Vaccines for Alzheimer Disease Treatment. J Am Med Dir Assoc 2016, 17, 862 e11-5. [Google Scholar] [CrossRef] [PubMed]
- Kwan, P.; Konno, H.; Chan, K.Y.; Baum, L. Rationale for the development of an Alzheimer's disease vaccine. Hum Vaccin Immunother 2020, 16, 645–653. [Google Scholar] [CrossRef]
- Xue, D.; Blue, E.E.; Conomos, M.P.; Fohner, A.E. The power of representation: Statistical analysis of diversity in US Alzheimer's disease genetics data. Alzheimers Dement (N Y) 2024, 10, e12462. [Google Scholar] [CrossRef]
- Ray, N.R.; Kumar, A.; Zaman, A.; Del Rosario, P.; Mena, P.R.; Manoochehri, M.; Stein, C.; De Vito, A.N.; Sweet, R.A.; Hohman, T.J.; Cuccaro, M.L.; Beecham, G.W.; Huey, E.D.; Reitz, C. Disentangling the genetic underpinnings of neuropsychiatric symptoms in Alzheimer's disease in the Alzheimer's Disease Sequencing Project: Study design and methodology. Alzheimers Dement (Amst) 2024, 16, e70000. [Google Scholar] [CrossRef] [PubMed]
- Greenfest-Allen, E.; Valladares, O.; Kuksa, P.P.; Gangadharan, P.; Lee, W.P.; Cifello, J.; Katanic, Z.; Kuzma, A.B.; Wheeler, N.; Bush, W.S.; Leung, Y.Y.; Schellenberg, G.; Stoeckert, C.J., Jr.; Wang, L.S. NIAGADS Alzheimer's GenomicsDB: A resource for exploring Alzheimer's disease genetic and genomic knowledge. Alzheimers Dement 2024, 20, 1123–1136. [Google Scholar] [CrossRef]
- Toga, A.W.; Phatak, M.; Pappas, I.; Thompson, S.; McHugh, C.P.; Clement, M.H.S.; Bauermeister, S.; Maruyama, T.; Gallacher, J. The pursuit of approaches to federate data to accelerate Alzheimer's disease and related dementia research: GAAIN, DPUK, and ADDI. Front Neuroinform 2023, 17, 1175689. [Google Scholar] [CrossRef]
- Hao, X.; Li, X.; Zhang, G.Q.; Tao, C.; Schulz, P.E.; Alzheimer's Disease Neuroimaging, I.; Cui, L. An ontology-based approach for harmonization and cross-cohort query of Alzheimer's disease data resources. BMC Med Inform Decis Mak 2023, 23 (Suppl 1), 151. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The APOEε4 allele disrupts lipid metabolism, promotes Aβ aggregation, impairs mitochondrial function, alters immune responses, and regulates gene expression. These changes lead to amyloid plaque formation, oxidative stress, energy metabolism impairment, chronic inflammation, and neuronal damage. Mutations in APP, PSEN1, and PSEN2 genes result in abnormal Aβ production and γ-secretase activity, further driving amyloid plaque formation and neurodegeneration.
Figure 1.
The APOEε4 allele disrupts lipid metabolism, promotes Aβ aggregation, impairs mitochondrial function, alters immune responses, and regulates gene expression. These changes lead to amyloid plaque formation, oxidative stress, energy metabolism impairment, chronic inflammation, and neuronal damage. Mutations in APP, PSEN1, and PSEN2 genes result in abnormal Aβ production and γ-secretase activity, further driving amyloid plaque formation and neurodegeneration.
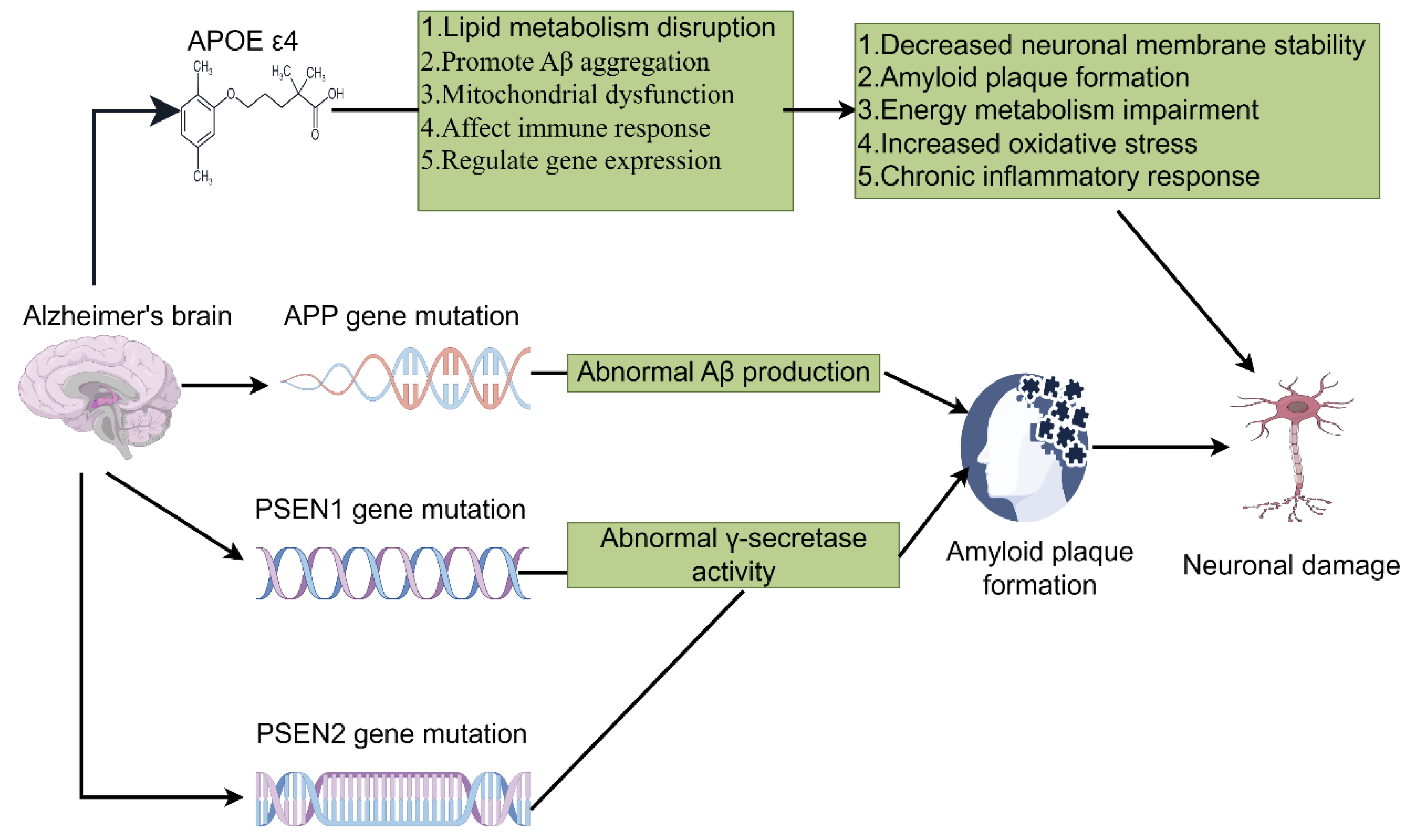
Figure 2.
This figure integrates genomics, transcriptomics, and proteomics to investigate Alzheimer’s disease. Genomics identifies genetic variations, transcriptomics reveals gene expression differences, and proteomics detects protein abundance changes. Bioinformatics analysis connects these data to identify key gene modules and predict disease progression.
Figure 2.
This figure integrates genomics, transcriptomics, and proteomics to investigate Alzheimer’s disease. Genomics identifies genetic variations, transcriptomics reveals gene expression differences, and proteomics detects protein abundance changes. Bioinformatics analysis connects these data to identify key gene modules and predict disease progression.
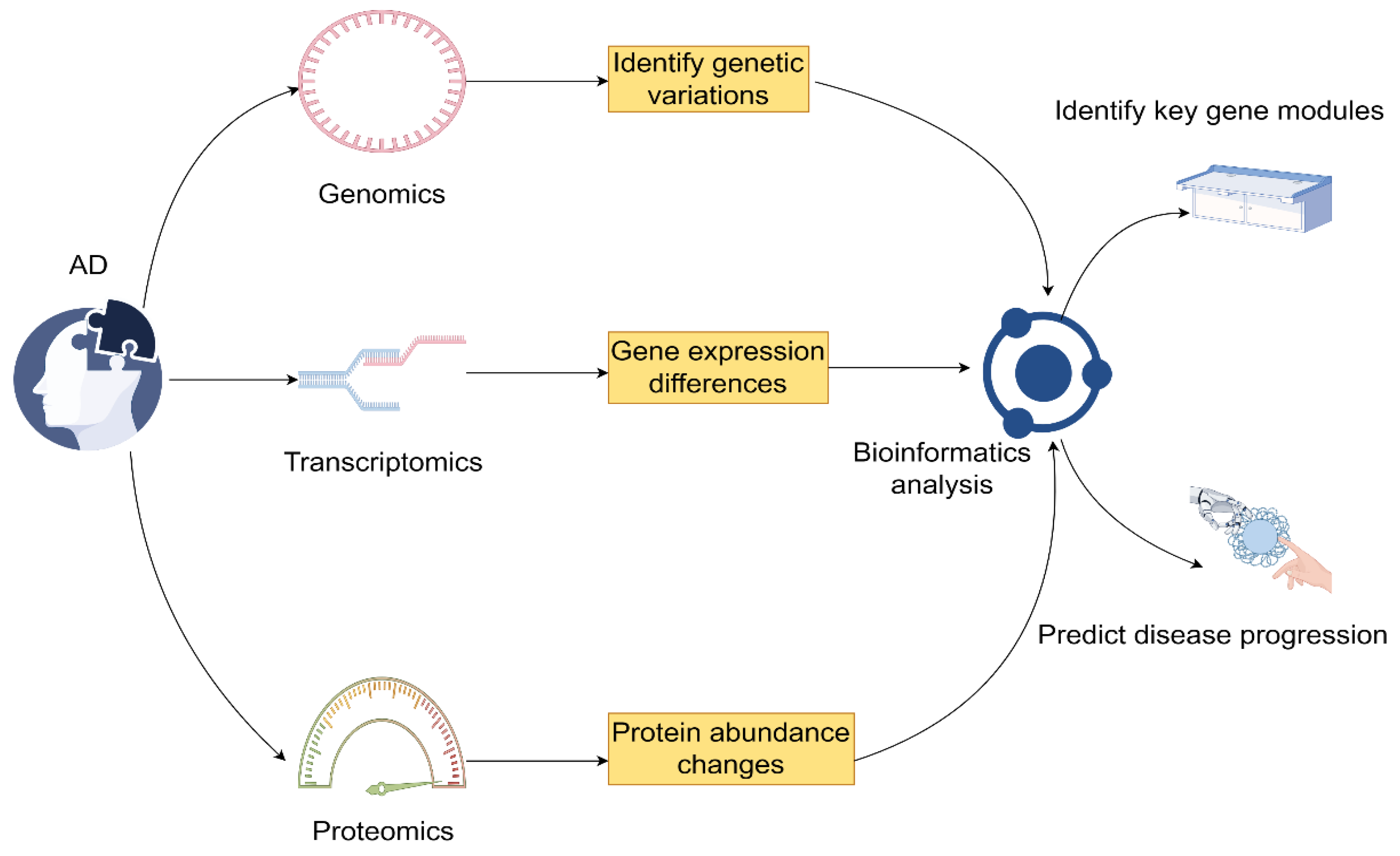

Table 1.
Therapeutic strategies for Alzheimer's disease.
| Therapy Type | Mechanism Description |
Clinical Application and Challenges | Reference |
|---|---|---|---|
| Passive immunotherapy |
Injection of monoclonal antibodies to clear pathological proteins. |
Approved for early AD treatment, optimization needed for safety. |
[100] |
| Active immunotherapy (Vaccine) |
Injection of antigens or vaccines to stimulate immune response. |
Improved to reduce side effects, individual differencesand immune memory maintenance are still challenges. |
[102] |
| Cell therapy | Transplantation of immune cells or stem cells to repair neural tissue. |
In early stages, further validation of safety and efficacy is required. |
[105] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



