Submitted:
08 January 2025
Posted:
09 January 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Maintenance hemodialysis patients are at increased risk of cardiovascular complications and mortality following COVID-19 infection due to compromised immune function. This study aims to evaluate the effect of COVID-19 vaccination (CoronaVac) on cardiac function and survival in this population. Background/Objectives: This study aimed to evaluate the effects of CoronaVac on echocardiographic parameters, BNP levels, and survival rates in maintenance hemodialysis patients. By comparing vaccinated and unvaccinated patients, we sought to assess whether vaccination provides a protective effect on cardiac function and contributes to improved clinical outcomes in this population. Methods: We conducted a retrospective analysis of 531 maintenance hemodialysis patients, comprising 452 unvaccinated and 79 vaccinated with CoronaVac. We compared changes in echocardiographic parameters and BNP levels before and after COVID-19 infection between the vaccinated and unvaccinated groups and assessed their association with survival rates. Results: Vaccinated patients were younger (60.54 ± 13.51 vs. 65.21 ± 13.76 years, p=0.006), had shorter dialysis durations (56.04 ± 51.88 vs. 73.73 ± 64.79 months, p=0.022). The mortality rate was also significantly lower in the vaccinated group (6.33% vs. 14.38%, p=0.049). In the unvaccinated group, BNP levels and multiple echocardiographic parameters (IVSD, LVPWD, AO, LA, EF, FS) significantly deteriorated post-infection, whereas no significant changes were observed in the vaccinated group. Multivariate analysis identified age, CAD, Hs-CRP, and LVIDs abnormalities as independent predictors of mortality, indicating that the independent protective effect of vaccination requires further validation. Conclusions: CoronaVac is associated with lower mortality and stable cardiac function in maintenance hemodialysis patients. The vaccine may reduce infection severity, lower cardiac load, and improve prognosis.
Keywords:
COVID-19 vaccination
; maintenance hemodialysis
; cardiac function
; echocardiography
; BNP
; survival rate
1. Introduction
Since its initial outbreak in 2019, COVID-19 has rapidly spread, becoming a major global public health challenge. Hemodialysis patients, due to their immunocompromised status and multiple comorbidities, are particularly vulnerable to COVID-19 infection. An infection rate of 29.31% was reported among dialysis patients, primarily due to frequent interactions with healthcare facilities and increased exposure to high-risk environments [1]. Similarly, high infection rates in European dialysis centers have been linked to close contact within these facilities [2].
COVID-19 has significantly impacted dialysis patients, with mortality rates reaching 30.5%, as early lymphopenia and elevated lactate dehydrogenase were identified as predictors of poor outcomes [3]. Mortality in elderly dialysis patients was reported to be six times higher than in younger patients [4]. Additionally, mortality rates of 33.82% and 39.08% were documented in separate studies, highlighting the vulnerability of this population [5]. Frequent healthcare exposure and treatment interruptions, including disruptions in dialysis due to worsening conditions, have further complicated patient management during the pandemic. Risk factors such as chronic pulmonary and cardiovascular diseases, elevated C-reactive protein (CRP), and D-dimer levels have also been linked to poorer outcomes following COVID-19 infection [6].
Vaccination has been shown to provide substantial protection for dialysis patients, a highly vulnerable population. Two doses of the vaccine were reported to reduce hospitalization rates by 75% and mortality by 88% [7]. Additionally, vaccination offered significant defense against variants such as Omicron, demonstrating its efficacy even in the context of emerging viral strains [8]. However, concerns regarding vaccine safety in hemodialysis patients persist, given their immunocompromised status and multiple comorbidities. This population may be more prone to adverse effects or rare complications, including severe allergic reactions and localized infections. While the benefits of vaccination, such as reduced hospitalizations and mortality, are well-documented [8], addressing these safety concerns remains crucial to optimizing vaccine strategies in this high-risk group.
Cardiovascular disease is highly prevalent among dialysis patients, with incidence rates between 40% and 60%, making it a leading cause of mortality [9]. The mechanisms underlying impaired cardiac function include volume overload, metabolic disturbances and oxidative stress [10]. Routine assessments using echocardiography and biomarkers (e.g., BNP or NT-proBNP), along with optimized dialysis strategies, metabolic correction, and appropriate pharmacological intervention (e.g., ACE inhibitors or beta-blockers), can effectively improve prognosis [11]. Conditions like left ventricular hypertrophy and reduced ejection fraction are independent risk factors for cardiovascular events and all-cause mortality, emphasizing the critical importance of cardiac health in dialysis patients [12].
COVID-19 may also result in long-term cardiac sequelae. Studies have shown that 78% of recovered patients exhibit myocardial involvement, with 60% having persistent myocarditis [13]. Patients may experience arrhythmias and thrombosis due to systemic inflammation and hypercoagulability triggered by the virus [14]. Vaccination, in addition to reducing acute-phase infection risk, also lowers the incidence of long-term cardiovascular complications. Data suggest that patients receiving two vaccine doses had a 30% reduction in the risk of long-term cardiovascular complications [15]. Furthermore, vaccination reduced mortality and cardiovascular event rates by 91% among patients with underlying heart conditions, providing crucial protection for high-risk groups [16]. Vaccination also notably decreased the occurrence of post-COVID sequelae, such as hypertension and heart failure [17].
Studies specifically evaluating the effect of the CoronaVac vaccine on cardiac function in dialysis patients are limited. Akin et al. [18] reported that while immune response was weaker among hemodialysis patients receiving CoronaVac, antibody levels were still sufficient for protective immunity. Medina-Pestana et al. [19] showed that although breakthrough infection rates were relatively high among dialysis patients post-CoronaVac, hospitalization and mortality rates were significantly reduced. Ran et al. [20] documented a case of IgA nephropathy exacerbation leading to dialysis following CoronaVac vaccination, indicating the need for close renal function monitoring. Ihara et al. [21] observed that administration of the 23-valent pneumococcal polysaccharide vaccine significantly reduced cardiovascular events and improved survival among dialysis patients, especially when co-administered with the influenza vaccine.
During the Omicron variant outbreak, vaccination continued to demonstrate significant protective effects, reducing the hospitalization risk among dialysis patients who completed vaccination or received booster doses by 59%. Nevertheless, concerns persist regarding adverse reactions following vaccination, particularly related to cardiac function. Specifically, hypertensive patients were more likely to develop mild local or systemic reactions post-CoronaVac, although the overall safety profile remained favorable [22]. Additionally, comparative research has found that while inactivated vaccines have lower seroconversion rates compared to mRNA vaccines, they are better tolerated, especially in immunosuppressed individuals [23].
Direct studies on the impact of CoronaVac on cardiac function in dialysis patients are still lacking, and it remains unclear whether the vaccine exacerbates cardiac impairment or offers cardiovascular protection. More randomized controlled trials are needed to determine the specific impact of CoronaVac on cardiovascular outcomes in this population, thereby informing clinical practice.
2. Materials and Methods
2.1. Study Population
This retrospective study was conducted at the Hemodialysis Unit of Hangzhou Traditional Chinese Medicine Hospital in November 2022, following the Declaration of Helsinki and approved by the hospital’s Ethics Committee (approval number: 2023KLL027). Written informed consent was obtained from all participants. A total of 1,028 chronic maintenance hemodialysis patients were screened. Patients were excluded if they had died before the COVID-19 pandemic (n=3), transferred to other hospitals (n=383), transitioned to peritoneal dialysis (n=22), underwent renal transplant (n=13), experienced renal function recovery (n=20), or were lost to follow-up (n=37). This resulted in 587 eligible patients, of whom 56 were further excluded due to missing echocardiographic data, leaving 531 participants for analysis. Participants were categorized into vaccinated (CoronaVac, n=79) and unvaccinated groups (n=452). See Figure 1 for details.
2.2. Data Collection
Clinical data were retrieved from the Hospital Information System (HIS), including vaccination status (primary, booster, and secondary booster doses), demographic characteristics (age, gender, comorbidities), and COVID-19 outcomes (symptomatic infections, hospitalizations, COVID-19-related deaths, and all-cause mortality). Clinical indicators included echocardiographic parameters (e.g., interventricular septal thickness, left ventricular internal diameters in diastole and systole, posterior wall thickness, aortic root dimension, left atrial diameter, stroke volume, ejection fraction, fractional shortening), which were classified as normal or abnormal. Additional markers included brain natriuretic peptide (BNP; maximum and mean levels), biochemical markers (e.g., albumin, creatinine, blood urea nitrogen, lipid profiles, liver enzymes), hemoglobin, inflammatory markers (e.g., high-sensitivity CRP, ferritin), mineral metabolism indices (e.g., parathyroid hormone, calcium, phosphate), and dialysis adequacy metrics (e.g., KT/V, urea reduction ratio). Data were tracked longitudinally from November 2020 to November 2024 to evaluate trends and outcomes.
2.3. Statistical Methods
All analyses were conducted using SPSS version 26.0. Continuous variables were reported as mean ± standard deviation (SD) or median (Q1, Q3) depending on the data distribution, while categorical variables were expressed as frequencies and percentages. Group comparisons were conducted using appropriate statistical tests (e.g., t-test, Mann-Whitney U test, chi-square test). Survival analysis was performed using Cox proportional hazards models, with hazard ratios (HRs) and 95% confidence intervals (CIs) reported. A p-value <0.05 was considered statistically significant.
3. Results
3.1 Baseline Characteristics of the Study Population
The study included 531 maintenance hemodialysis patients, with a mean age of 64.51 ± 13.81 years. Most were male (62.90%), and the mean dialysis duration was 71.10 ± 63.30 months. Participants were divided into 452 unvaccinated and 79 vaccinated (CoronaVac) patients. The vaccinated group was younger (60.54 ± 13.51 vs. 65.21 ± 13.76 years, p = 0.006) and had a shorter dialysis duration (56.04 ± 51.88 vs. 73.73 ± 64.79 months, p = 0.022). Chronic glomerulonephritis (54.43%) and diabetic nephropathy (37.48%) were the most common primary diseases, while polycystic kidney disease (4.90%) and connective tissue disease (1.69%) were less frequent. Overall mortality was 13.18%, significantly lower in the vaccinated group (6.33% vs. 14.38%, p = 0.049). Hypertension (86.44%) and coronary artery disease (CAD) (26.18%) were prevalent, with a lower CAD rate in the vaccinated group (10.13% vs. 28.98%, p < 0.001). No significant differences were found in arrhythmia, heart failure, COVID-19 hospitalization, or severe COVID-19 rates. Details are presented in Table 1.
3.2. Clinical and Biochemical Differences Between Survival and Death Groups
The clinical and biochemical profiles of 531 maintenance hemodialysis patients were compared between the survival group (n = 461) and the death group (n = 70). Patients in the death group were significantly older (75.67 ± 12.27 vs. 62.82 ± 13.24 years, p < 0.001) and exhibited lower serum albumin levels (33.60 ± 4.15 vs. 35.96 ± 3.88 g/dL, p < 0.001), creatinine concentrations (612.10 ± 223.19 vs. 774.00 ± 276.61 µmol/L, p < 0.001), and hemoglobin levels (104.77 ± 14.89 vs. 110.68 ± 13.38 g/dL, p < 0.001). Inflammatory markers, such as hs-CRP, were markedly higher in the death group (7.26 [3.17, 24.80] vs. 2.03 [0.97, 6.20] mg/L, p < 0.001), along with a prolonged prothrombin time (11.89 ± 1.68 vs. 11.20 ± 2.06 seconds, p = 0.016).Phosphate levels were significantly lower among patients in the death group (1.42 ± 0.46 vs. 1.64 ± 0.46 mg/dL, p < 0.001), as were uric acid levels (350.48 ± 112.04 vs. 410.32 ± 98.65 µmol/L, p < 0.001), potentially indicating nutritional and metabolic impairments. No significant differences were observed in alanine transaminase levels or parathyroid hormone concentrations. Dialysis duration, lipid profiles, and other biochemical markers also showed no notable variations between the groups.Details are presented in Table 2.
3.3. Echocardiographic and BNP Characteristics of the Study Population
Echocardiographic parameters and BNP levels were analyzed for 531 maintenance hemodialysis patients. BNP levels were significantly higher in the death group compared to the survival group (BNP Max: 1246.00 pg/mL vs. 401.50 pg/mL, p < 0.001; BNP Mean: 584.50 pg/mL vs. 247.00 pg/mL, p < 0.001).
Echocardiographic differences were limited. The interventricular septal thickness (IVSD) was slightly higher in the death group, but this was not statistically significant (p = 0.165). Among echocardiographic parameters, only abnormal left ventricular end-systolic diameter (LVIDs) showed a significant association with mortality (20.00% vs. 7.83%, p = 0.049). Coronary artery disease (67.14% vs. 19.96%, p < 0.001) and heart failure (11.43% vs. 3.47%, p = 0.007) were also more prevalent in the death group.
These findings suggest that elevated BNP levels and coronary artery disease are key predictors of mortality, with left ventricular dysfunction as a potential contributing factor. Details are presented in Table 3.
3.4. Multivariate Analysis of LVIDs and Related Factors
Multivariate Cox regression analysis was performed to explore the association between LVIDs and survival outcomes while adjusting for confounding variables. The results revealed that patients with abnormal LVIDs had significantly higher HRs for mortality compared to those with normal LVIDs (HR: 5.60, 95% CI: 1.34–23.34, p = 0.018). This suggests that abnormal LVIDs is an independent predictor of mortality in the maintenance hemodialysis population.
Among clinical parameters, age was identified as another significant predictor, with each one-year increase in age associated with a 10% higher risk of mortality (HR: 1.10, 95% CI: 1.02–1.18, p = 0.009). Elevated Hs-CRP was also independently associated with increased mortality risk (HR: 1.03, 95% CI: 1.01–1.05, p = 0.049), reflecting the role of systemic inflammation in adverse outcomes. Coronary artery disease (CAD) was a strong independent risk factor, with an HR of 4.20 (95% CI: 1.06–16.71, p = 0.041), indicating its significant impact on mortality.
Conversely, other variables such as albumin (ALB), serum creatinine (Cr), phosphate (PHOS), urea, prothrombin time (PT), prealbumin (PA), and heart failure (HF) did not reach statistical significance in the multivariate model. Interestingly, both BNP Max and BNP Mean, though significant in univariate analysis, were not independent predictors in the multivariate analysis after adjusting for other factors.
These findings emphasize the importance of echocardiographic parameters, particularly LVIDs, and the underlying systemic factors like age, inflammation, and CAD in predicting mortality in hemodialysis patients. This highlights the need for close monitoring and targeted interventions to address these risk factors in clinical practice.
3.5. Multivariate Cox Regression Analysis Across Different Models
To evaluate the relationship between echocardiographic parameters and mortality in hemodialysis patients, three Cox regression models were developed. Model 1 provided crude (unadjusted) HRs, while Model 2 accounted for hypertension (HTN), arrhythmia, CAD, and heart failure (HF). Model 3 further adjusted for age, HTN, arrhythmia, CAD, HF, albumin (ALB), and prealbumin (PA). The results demonstrated the significance of specific cardiac parameters in predicting mortality.
Among echocardiographic parameters, LVIDs1 was consistently identified as an independent predictor of mortality across all models. In the unadjusted analysis (Model 1), an abnormal LVIDs1 was associated with a twofold higher risk of mortality (HR: 2.66, 95% CI: 1.16–6.10, p = 0.021). After adjusting for additional variables in Model 2, the risk increased significantly (HR: 28.88, 95% CI: 3.47–240.13, p = 0.002). Model 3, which included demographic and nutritional variables, further amplified this association (HR: 1574.03, 95% CI: 3.30–750000.88, p = 0.019), underscoring the importance of LVIDs1 as a robust marker of poor prognosis.
Gender also emerged as a significant factor in the adjusted models. Women demonstrated a substantially reduced risk of mortality compared to men, with HRs of 0.15 (95% CI: 0.03–0.66, p = 0.013) and 0.01 (95% CI: 0.00–0.34, p = 0.011) in Models 2 and 3, respectively. Additionally, left ventricular end-diastolic diameter (LVIDd1) and ejection fraction (EF1) became significant predictors in Models 2 and 3, highlighting their importance in outcomes when confounding factors were considered.
Other parameters, including interventricular septal diameter (IVSD1), stroke volume (SV1), and aortic diameter (AO1), showed relevance in the adjusted models, reflecting their potential role in determining survival. However, some variables, such as left ventricular posterior wall diameter (LVPWD1) and fractional shortening (FS1), did not exhibit consistent significance across all models.
Overall, the findings highlight the critical role of echocardiographic parameters, particularly LVIDs1, in predicting mortality risk in the hemodialysis population. The strong associations observed after adjusting for clinical and demographic confounders emphasize the need for regular cardiac assessments and targeted interventions to improve patient outcomes (see Table 5).
3.6. BNP Levels and the Effect of Vaccination Pre- and Post-Infection in Hemodialysis Patients
This study evaluated the impact of COVID-19 infection on BNP levels in maintenance hemodialysis patients, focusing on the influence of vaccination. Among unvaccinated patients, BNP levels significantly increased post-infection, with BNP max showing a notable rise (p < 0.001) but only a moderate shift according to z-value analysis (p = 0.078). Similarly, BNP mean levels increased significantly (p < 0.001), though the z-value analysis indicated a less pronounced change (p = 0.119).In vaccinated patients, post-infection BNP max levels exhibited a decrease that was not statistically significant by Wilcoxon test (p = 0.3). However, z-value analysis revealed a significant reduction (p = 0.006). BNP mean levels also rose in the vaccinated group, but this increase was not significant (p = 0.098) in Wilcoxon test, while z-value analysis indicated a significant difference (p = 0.02).These findings suggest that vaccination may play a role in moderating changes in BNP levels following COVID-19 infection. Detailed data are presented in Table 6 and Figure 2.
3.7. Impact of Vaccination on Echocardiographic Parameters
This study investigated changes in echocardiographic parameters before and after COVID-19 infection in maintenance hemodialysis patients, comparing those vaccinated with CoronaVac to those who were unvaccinated. In the unvaccinated group, several parameters showed significant deterioration post-infection. Interventricular septal thickness (IVSD) and left ventricular posterior wall thickness (LVPWD) increased significantly (p < 0.001 and p = 0.001, respectively). Additionally, aortic root diameter (AO) decreased (p = 0.014), left atrial diameter (LA) enlarged (p = 0.013), ejection fraction (EF) declined (p = 0.002), and fractional shortening (FS) was reduced (p = 0.017). These findings reflect notable structural and functional cardiac changes following infection.In contrast, no significant changes were observed in the vaccinated group for these echocardiographic parameters (p > 0.05). For example, IVSD and LVPWD remained stable (p = 0.423 and p = 0.934), and EF and FS showed no significant decline (p = 0.971 and p = 0.810). These results suggest that vaccination may mitigate infection-induced cardiac damage, helping to preserve cardiac stability in this vulnerable population. Detailed data are presented in Table 7 and Figure 3.
4. Discussion
As shown in Table 1, significant differences were observed in the baseline characteristics of maintenance hemodialysis patients based on their COVID-19 vaccination status. Patients in the vaccinated group were younger (60.54 ± 13.51 vs. 65.21 ± 13.76 years, p = 0.006) and had shorter dialysis durations (56.04 ± 51.88 vs. 73.73 ± 64.79 months, p = 0.022). The prevalence of CAD was notably lower in vaccinated patients compared to those unvaccinated (10.13% vs. 28.98%, p < 0.001), and the mortality rate was also significantly reduced (6.33% vs. 14.38%, p = 0.049). These findings suggest that younger and healthier patients were more likely to receive the COVID-19 vaccine, potentially reflecting heightened health awareness in these individuals. While the vaccinated group demonstrated a lower prevalence of CAD, no significant differences were observed between the two groups regarding other comorbidities, such as arrhythmias and heart failure, or the rates of COVID-19-related hospitalization and severe illness (p > 0.05).This trend aligns with prior research, which indicates that younger and healthier individuals are generally more inclined to accept vaccination [24]. The lower CAD prevalence in the vaccinated group should not be interpreted as evidence of a direct protective effect of vaccination against CAD. Instead, it likely reflects a selection bias, where patients with preexisting cardiovascular conditions may have been less likely to receive vaccination due to concerns about their overall health status.In dialysis patients, vaccination appears to correlate with better overall health, characterized by lower systemic inflammation and stronger immune responses—factors associated with improved cardiovascular health [25]. The observed differences suggest that patients in better health are more likely to choose vaccination, a pattern consistent with previous findings [26]
Patients in the mortality group demonstrated significantly poorer performance in age, nutritional and metabolic markers (e.g., albumin, creatinine, hemoglobin, phosphorus, uric acid, prealbumin), and inflammatory markers (e.g., Hs-CRP) compared to the survival group (Table 2). Furthermore, the prevalence of cardiovascular complications, such as CAD and heart failure, was significantly higher in the mortality group. These findings are consistent with previous studies, which highlight the critical role of advanced age, malnutrition, and heightened inflammatory states in increasing mortality risk among dialysis patients [27,28,29]. Age emerged as a significant risk factor, with the mortality group being considerably older (75.67 ± 12.27 vs. 62.82 ± 13.24 years, p < 0.001). This finding aligns with the observation that older patients with CKD face elevated risks of cardiovascular events, malnutrition, and immunosuppression. Age is widely recognized as an independent predictor of increased mortality in this population [30]. In terms of nutritional and metabolic markers, the mortality group exhibited significantly lower levels of albumin (33.60 ± 4.15 vs. 35.96 ± 3.88 g/dL, p < 0.001), which is a well-established indicator of nutritional status and strongly correlates with mortality risk in CKD patients [27,31]. Similarly, creatinine levels were markedly reduced in the mortality group (612.10 ± 223.19 vs. 774.00 ± 276.61 µmol/L, p < 0.001), suggesting severe muscle wasting or malnutrition [32] Hemoglobin (104.77 ± 14.89 vs. 110.68 ± 13.38 g/dL, p < 0.001) and phosphorus levels (1.42 ± 0.46 vs. 1.64 ± 0.46 mmol/L, p < 0.001) were also significantly lower in the mortality group, further indicating inadequate protein intake and potential metabolic derangements [28] [33,34].Inflammatory markers also showed a stark contrast, with high-sensitivity Hs-CRP being significantly elevated in the mortality group (7.26 [3.17, 24.80] vs. 2.03 [0.97, 6.20] mg/L, p < 0.001), reflecting heightened systemic inflammation [28,35]. Hs-CRP is a sensitive biomarker of inflammation and is strongly associated with cardiovascular events and mortality [31,36]. Additionally, prothrombin time (PT) was prolonged in the mortality group (11.89 ± 1.68 vs. 11.20 ± 2.06 seconds, p = 0.016), potentially indicating impaired liver function, malnutrition, or comorbid conditions such as heart failure [33].The interplay between malnutrition and inflammation is well-documented in dialysis patients, often forming the “malnutrition-inflammation-atherosclerosis (MIA) syndrome.” This synergistic mechanism significantly elevates the risk of cardiovascular events and all-cause mortality [34,35]. These findings emphasize the need for early identification and management of malnutrition and inflammation to improve survival outcomes in this vulnerable population.
Based on the data from this study, significant differences in BNP levels and echocardiographic parameters were observed between the survival and death groups of dialysis patients (Table 3). Specifically, the maximum and mean BNP levels in the death group were significantly higher than those in the survival group (p < 0.001), and the incidence of cardiovascular complications such as CAD and HF was markedly higher in the death group (p < 0.01). Additionally, the abnormality rate of LVIDs was significantly higher in the death group (p = 0.049), while no significant differences were observed in other echocardiographic parameters. These findings are supported and extended by previous studies. Palazzuoli [37] found that BNP levels were closely associated with left ventricular mass, volume, and function in dialysis patients, particularly in relation to left ventricular enlargement and diastolic dysfunction caused by volume overload in CKD patients. Zoccali [38]further emphasized that BNP levels are independent predictors of all-cause and cardiovascular mortality in dialysis patients, correlating with left ventricular mass and function, suggesting that BNP could be a valuable biomarker for predicting mortality risk in these patients. Harrison [39] identified BNP as a strong predictor of cardiovascular mortality in end-stage renal disease (ESRD) patients, with elevated BNP levels linked to an increased risk of cardiovascular death. It has also been reported that elevated BNP and NT-proBNP levels are associated with an increased risk of all-cause mortality in CKD patients, further reinforcing the role of BNP as a key predictor [40]. These results underscore the importance of monitoring BNP levels and assessing echocardiographic parameters for risk stratification in dialysis patients in clinical practice.
Using Cox regression analysis, LVIDs, age, high-sensitivity Hs-CRP, and CAD were identified as independent predictors of mortality in hemodialysis patients (Table 4). Specifically, abnormal LVIDs (HR = 5.60, p = 0.018), advancing age (HR = 1.10 per year, p = 0.009), elevated Hs-CRP (HR = 1.03, p = 0.049), and the presence of CAD (HR = 4.20, p = 0.041) were all significantly associated with increased mortality risk (Table 4). These findings underscore the critical role of LVIDs as a key marker of left ventricular function and its strong association with mortality in dialysis patients. Elevated LVIDs indicate more severe ventricular dilation and dysfunction, which are commonly observed in patients with CKD and ESRD. These changes are primarily driven by cardiac stress resulting from volume overload and hypertension. Previous studies have reported that increased LVIDs are significantly correlated with a heightened risk of adverse cardiovascular events in these populations [41]. Furthermore, LVIDs measurements are widely utilized to predict cardiovascular outcomes in dialysis patients, including heart failure and arrhythmias. The enlargement of LVIDs often results from long-term dialysis effects and persistent volume overload, leading to left ventricular hypertrophy and eventual dilation. A meta-analysis involving ESRD patients demonstrated that larger LVIDs are significant predictors of heart failure and overall mortality [42]. The modality of dialysis (e.g., hemodialysis versus peritoneal dialysis) may also influence LVIDs. Studies indicate that patients undergoing hemodialysis often exhibit more pronounced left ventricular dilation compared to those on peritoneal dialysis. This difference may be attributed to significant fluctuations in fluid balance and intravascular volume during hemodialysis sessions [43]. Monitoring and evaluating LVIDs are essential for guiding therapeutic strategies in dialysis patients. Early detection of significant increases in LVIDs allows for timely interventions aimed at controlling fluid overload, potentially mitigating the risk of heart failure. Some studies suggest that optimizing fluid management can prevent or slow the progression of left ventricular dilation in these patients [44]. These findings emphasize the importance of integrating LVIDs measurements into the routine clinical assessment and management of dialysis patients.
A stratified Cox regression analysis evaluated the association between echocardiographic parameters and mortality in hemodialysis patients (Table 5) using three sequential models. These models incorporated cardiovascular history (e.g., CAD, hypertension, heart failure) and demographic/nutritional factors (e.g., age, albumin) for comprehensive risk assessment. Abnormal LVIDs remained a significant independent predictor across all models (HR = 2.66, p = 0.021 in Model 1; p = 0.019 in Model 3). Female sex was identified as a protective factor, with lower mortality risk compared to males (p < 0.05). After further adjustments, left ventricular end-diastolic diameter (LVIDd) and ejection fraction (EF) also emerged as significant predictors, highlighting their relevance in specific clinical contexts.LVID abnormalities reflect severe ventricular dilation and dysfunction caused by volume overload and hypertension, conditions frequently observed in ESRD patients [38]. The observed sex differences in mortality risk are likely related to hormonal and physiological factors, with females often showing better survival outcomes [45]. Regular echocardiographic evaluation is essential for monitoring and addressing changes in left ventricular structure and function, with the potential to improve long-term prognosis [46].
This study evaluated the changes in BNP levels and echocardiographic parameters in maintenance hemodialysis patients before and after COVID-19 infection, with a particular focus on the impact of vaccination. Results showed that in patients who were not vaccinated, both the maximum (BNP Max) and mean (BNP Mean) BNP levels significantly increased after infection (p < 0.001) (Table 6, Figure 2). Additionally, echocardiographic parameters, such as interventricular septal thickness (IVSD) and left ventricular posterior wall thickness (LVPWD), worsened significantly (p < 0.001 and p = 0.001, respectively). In contrast, vaccinated patients did not show significant changes in BNP levels (BNP Max Wilcoxon test p = 0.3, z-value analysis p = 0.006; BNP Mean Wilcoxon test p = 0.098, z-value analysis p = 0.02), and no significant changes were observed in echocardiographic parameters (all p > 0.05) (Table 7, Figure 3).
The significant increase in BNP in unvaccinated patients post-infection reflects worsened myocardial workload and volume overload due to COVID-19 infection, leading to heart function deterioration. On the other hand, the absence of significant BNP changes in vaccinated patients suggests that vaccination may help reduce the severity of infection, decrease cardiac load, and lower the risk of heart failure, thus maintaining a relatively stable BNP level. These findings align with previous studies indicating that COVID-19 infection is closely linked to changes in BNP levels, particularly in severe cases where elevated BNP levels are associated with heart failure or cardiac injury [47]. Hemodialysis patients, in particular, face higher risks after COVID-19 infection, including increased cardiac load and organ failure, with significantly higher mortality and hospitalization rates [48]. Regarding vaccination, research shows that COVID-19 vaccines can reduce severe disease and mortality rates in dialysis patients, though some may exhibit lower immune responses, requiring additional monitoring and potential dose adjustments [49].
COVID-19 vaccines may protect heart function through several mechanisms. First, vaccination can mitigate the body’s immune response, particularly by reducing excessive immune reactions and the release of inflammatory cytokines, thus alleviating myocardial damage. This allows for a quicker clearance of the virus, shortening the course of the infection and reducing the sustained increase in viral load, which helps to prevent long-term damage to the heart and vascular system [50,51]. Additionally, in vaccinated patients, the vaccine may help control volume and hemodynamics, reducing the extra burden on the heart and thereby minimizing further cardiac injury [52,53].
Cardiovascular events play a crucial role in the mortality and complications of maintenance hemodialysis patients. This study suggests that vaccination not only reduces the overall risk of COVID-19 infection or mitigates its severity but may also help protect cardiac function, preventing or delaying myocardial structural and functional damage caused by the infection. Therefore, it is recommended that clinical practices actively promote vaccination among hemodialysis patients, particularly high-risk individuals who are unvaccinated or have insufficient vaccine protection, while enhancing cardiac function monitoring and management. However, this study has limitations: the sample size is relatively small, which may affect the generalizability of the results; the follow-up period is short, limiting the ability to assess long-term effects; and factors such as vaccine type and dosage were not analyzed in detail, which may influence the outcomes. Future large-scale, multi-center studies are needed to further validate and refine these findings.
5. Conclusions
In conclusion, this study indicates that COVID-19 vaccination (CoronaVac) is associated with reduced mortality and more stable cardiac function in maintenance hemodialysis patients. Vaccinated patients exhibited smaller changes in BNP levels and echocardiographic parameters following COVID-19 infection, suggesting that vaccination may enhance survival outcomes by alleviating infection severity and associated cardiac stress. However, due to the pre-existing prognostic advantages in age and CAD burden in the vaccinated group, further multi-variable analysis is required to confirm the independent protective effect of vaccination.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Xiao Tu and Lidan Hu; Data curation, Yayu Li; Formal analysis, Yayu Li; Funding acquisition, Yayu Li; Investigation, Bing Xu, Jiazhen Yin, Ye Li, Jinchi Gao, Peng Bi, Wanyue Xu and Rihong Hu; Methodology, Yayu Li; Project administration, Xiao Tu and Lidan Hu; Resources, Xiao Tu and Lidan Hu; Software, Yayu Li; Supervision, Xiao Tu and Lidan Hu; Validation, Jiazhen Yin, Ye Li, Jinchi Gao and Rihong Hu; Visualization, Yayu Li; Writing – original draft, Ye Li, Jinchi Gao and Yayu Li; Writing – review & editing, Tingfei He, Jiazhen Yin, Fangyu Yi and Rihong Hu.
Funding
This work was supported by the Major Project of the Science and Technology Plan jointly estab-lished by the Department of Science and Technology of the National Administration of Tradi-tional Chinese Medicine and the Zhejiang Provincial Administration of Traditional Chinese Medicine (Grant No. GZY-ZJ-KJ-24041).
Institutional Review Board Statement
I The study was conducted in accordance with the Declaration of Helsinki and received approval from the Ethics Committee of Hangzhou Traditional Chinese Medicine Hospital (approval num-ber 2023KLL027). Written informed consent was obtained from all participants prior to their in-clusion in the study.
Informed Consent Statement
All subjects involved in the study have given their informed consent.
Data Availability Statement
The data supporting the reported results can be found.
Acknowledgments
The authors express great appreciation to all former and current members of the Department of Nephrology (Key Laboratory of Kidney Disease Prevention and Control Technology), Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University, for the insightful conversation and outstanding contributions to this research. We are also grateful to Lidan Hu for professional expertise in the experimental processes.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grujic N, Pešić S, Naumovic R: MO851 INCIDENCE AND MORTALITY OF CORONAVIRUS DISEASE (COVID 19) IN HEMODIALYSIS PATIENTS. Nephrology Dialysis Transplantation 2021, 36(Supplement_1):gfab098. 0043.
- Haarhaus M, Santos C, Haase M, Mota Veiga P, Lucas C, Macario F: Risk prediction of COVID-19 incidence and mortality in a large multi-national hemodialysis cohort: implications for management of the pandemic in outpatient hemodialysis settings. Clinical Kidney Journal 2021, 14(3):805-813.
- Goicoechea M, Cámara LAS, Macías N, de Morales AM, Rojas ÁG, Bascuñana A, Arroyo D, Vega A, Abad S, Verde E: COVID-19: clinical course and outcomes of 36 hemodialysis patients in Spain. Kidney international 2020, 98(1):27-34.
- Vergara A, Molina-Van den Bosch M, Toapanta N, Villegas A, Sánchez-Cámara L, Sequera Pd, Manrique J, Shabaka A, Aragoncillo I, Ruiz MC: The impact of age on mortality in chronic haemodialysis population with COVID-19. Journal of Clinical Medicine 2021, 10(14):3022.
- Tylicki L, Puchalska-Reglińska E, Tylicki P, Och A, Polewska K, Biedunkiewicz B, Parczewska A, Szabat K, Wolf J, Dębska-Ślizień A: Predictors of mortality in hemodialyzed patients after SARS-CoV-2 infection. Journal of Clinical Medicine 2022, 11(2):285.
- !!! INVALID CITATION !!! [5,6].
- Ashby DR, Caplin B, Corbett RW, Asgari E, Kumar N, Sarnowski A, Hull R, Makanjuola D, Cole N, Chen J: Severity of COVID-19 after vaccination among hemodialysis patients: an observational cohort study. Clinical Journal of the American Society of Nephrology 2022, 17(6):843-850.
- Wu C, Xie G, Chen J, Liu Q, Wang H, Tang Y: # 5019 MORTALITY FOR COVID-19 IN UNDERGOING MAINTENANCE DIALYSIS PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS. Nephrology Dialysis Transplantation 2023, 38(Supplement_1):gfad063c_5019.
- Cozzolino M, Mangano M, Stucchi A, Ciceri P, Conte F, Galassi A: Cardiovascular disease in dialysis patients. Nephrol Dial Transplant 2018, 33(suppl_3):iii28-iii34.
- !!! INVALID CITATION !!! [10].
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ: Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003, 108(17):2154-2169.
- Wang A, Montgomery D, Brinster DR, Gilon D, Upchurch Jr GR, Gleason TG, Estrera A, Isselbacher EM, Eagle KA, Hughes GC: Predicting in-hospital survival in acute type A aortic dissection medically treated. Journal of the American College of Cardiology 2020, 75(11):1360-1361.
- Puntmann VO, Carerj ML, Wieters I, Fahim M, Arendt C, Hoffmann J, Shchendrygina A, Escher F, Vasa-Nicotera M, Zeiher AM: Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA cardiology 2020, 5(11):1265-1273.
- Driggin E, Madhavan MV, Bikdeli B, Chuich T, Laracy J, Biondi-Zoccai G, Brown TS, Der Nigoghossian C, Zidar DA, Haythe J: Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. Journal of the American College of cardiology 2020, 75(18):2352-2371.
- Gao P, Liu J, Liu M: Effect of COVID-19 vaccines on reducing the risk of long COVID in the real world: a systematic review and meta-analysis. International Journal of Environmental Research and Public Health 2022, 19(19):12422.
- Feltes G, Romero R, Uribarri Gonzalez A, Nuñez Gil IJ, Raposeiras-Roubin S, Viana-Llamas MC, Alfonso E: Post-COVID-19 Symptoms and Heart Disease: Incidence, Prognostic Factors, Outcomes and Vaccination: Results from a Multi-Center International Prospective Registry (HOPE 2). 2023.
- Zisis SN, Durieux JC, Mouchati C, Perez JA, McComsey GA: The protective effect of coronavirus disease 2019 (COVID-19) vaccination on postacute sequelae of COVID-19: a multicenter study from a large national health research network. In: Open Forum Infectious Diseases: 2022: Oxford University Press; 2022: ofac228.
- Akin D, Ozmen S, Caliskan A, Sari T: Efficacy and safety of Sinovac vaccine administered in patients undergoing hemodialysis. The Journal of Infection in Developing Countries 2022, 16(12):1821-1825.
- Medina-Pestana J, Teixeira CM, Viana LA, Manfredi SR, Nakamura MR, Lucena EF, Amiratti AL, Tedesco-Silva H, Covas DT, Cristelli MP: Immunogenicity, reactogenicity and breakthrough infections after two doses of the inactivated CoronaVac vaccine among patients on dialysis: phase 4 study. Clinical Kidney Journal 2022, 15(4):816-817.
- Ran E, Wang M, Wang Y, Liu R, Yi Y, Liu Y: New-onset crescent IgA nephropathy following the CoronaVac vaccine: A case report. Medicine 2022, 101(33):e30066.
- Ihara H, Kikuchi K, Taniguchi H, Fujita S, Tsuruta Y, Kato M, Mitsuishi Y, Tajima K, Kodama Y, Takahashi F: 23-valent pneumococcal polysaccharide vaccine improves survival in dialysis patients by preventing cardiac events. Vaccine 2019, 37(43):6447-6453. [CrossRef]
- Zhang Q, Lu C, Chen H, Li M, Bai X, Chen J, Li D, Zhang Y, Lei N, He W: Effectiveness of vaccination in reducing hospitalization and mortality rates in dialysis patients with Omicron infection in China: A single-center study. Human Vaccines & Immunotherapeutics 2023, 19(2):2252257.
- Rincon-Arevalo H, Choi M, Stefanski A-L, Halleck F, Weber U, Szelinski F, Jahrsdörfer B, Schrezenmeier H, Ludwig C, Sattler A: Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Science immunology 2021, 6(61):eabj1031.
- Parker EP, Tazare J, Hulme WJ, Bates C, Carr EJ, Cockburn J, Curtis HJ, Fisher L, Green AC, Harper S et al.: Factors associated with COVID-19 vaccine uptake in people with kidney disease: an OpenSAFELY cohort study. BMJ Open 2023, 13(1):e066164. [CrossRef]
- Manley HJ, Li NC, Aweh GN, Hsu CM, Weiner DE, Miskulin D, Harford AM, Johnson D, Lacson E, Jr.: SARS-CoV-2 Vaccine Effectiveness and Breakthrough Infections Among Patients Receiving Maintenance Dialysis. Am J Kidney Dis 2023, 81(4):406-415.
- Speer C, Göth D, Benning L, Buylaert M, Schaier M, Grenz J, Nusshag C, Kälble F, Kreysing M, Reichel P et al.: Early Humoral Responses of Hemodialysis Patients after COVID-19 Vaccination with BNT162b2. Clin J Am Soc Nephrol 2021, 16(7):1073-1082. [CrossRef]
- Qureshi AR, Alvestrand A, Divino-Filho JC, Gutierrez A, Heimbürger O, Lindholm B, Bergström J: Inflammation, malnutrition, and cardiac disease as predictors of mortality in hemodialysis patients. J Am Soc Nephrol 2002, 13 Suppl 1:S28-36. [CrossRef]
- Selim G, Stojceva-Taneva O, Zafirovska K, Sikole A, Gelev S, Dzekova P, Stefanovski K, Koloska V, Polenakovic M: Inflammation predicts all-cause and cardiovascular mortality in haemodialysis patients. Prilozi 2006, 27(1):133-144.
- Jagadeswaran D, Indhumathi E, Hemamalini AJ, Sivakumar V, Soundararajan P, Jayakumar M: Inflammation and nutritional status assessment by malnutrition inflammation score and its outcome in pre-dialysis chronic kidney disease patients. Clin Nutr 2019, 38(1):341-347.
- de Mutsert R, Grootendorst DC, Axelsson J, Boeschoten EW, Krediet RT, Dekker FW: Excess mortality due to interaction between protein-energy wasting, inflammation and cardiovascular disease in chronic dialysis patients. Nephrol Dial Transplant 2008, 23(9):2957-2964.
- Wang AY, Wang M, Woo J, Lam CW, Lui SF, Li PK, Sanderson JE: Inflammation, residual kidney function, and cardiac hypertrophy are interrelated and combine adversely to enhance mortality and cardiovascular death risk of peritoneal dialysis patients. J Am Soc Nephrol 2004, 15(8):2186-2194. [CrossRef]
- Fernández-Reyes MJ, Alvarez-Ude F, Sánchez R, Mon C, Iglesias P, Díez JJ, Vázquez A: Inflammation and malnutrition as predictors of mortality in patients on hemodialysis. J Nephrol 2002, 15(2):136-143.
- Choi HY, Lee JE, Han SH, Yoo TH, Kim BS, Park HC, Kang SW, Choi KH, Ha SK, Lee HY et al.: Association of inflammation and protein-energy wasting with endothelial dysfunction in peritoneal dialysis patients. Nephrol Dial Transplant 2010, 25(4):1266-1271. [CrossRef]
- Brandão da Cunha Bandeira S, Cansanção K, Pereira de Paula T, Peres WAF: Evaluation of the prognostic significance of the malnutrition inflammation score in hemodialysis patients. Clin Nutr ESPEN 2020, 35:109-115.
- Liu Y, Coresh J, Eustace JA, Longenecker JC, Jaar B, Fink NE, Tracy RP, Powe NR, Klag MJ: Association between cholesterol level and mortality in dialysis patients: role of inflammation and malnutrition. Jama 2004, 291(4):451-459.
- Stenvinkel P, Alvestrand A: Inflammation in end-stage renal disease: sources, consequences, and therapy. Semin Dial 2002, 15(5):329-337.
- Palazzuoli A, Gallotta M, Quatrini I, Nuti R: Natriuretic peptides (BNP and NT-proBNP): measurement and relevance in heart failure. Vasc Health Risk Manag 2010, 6:411-418.
- Zoccali C, Mallamaci F, Benedetto FA, Tripepi G, Parlongo S, Cataliotti A, Cutrupi S, Giacone G, Bellanuova I, Cottini E et al.: Cardiac natriuretic peptides are related to left ventricular mass and function and predict mortality in dialysis patients. J Am Soc Nephrol 2001, 12(7):1508-1515. [CrossRef]
- Harrison TG, Shukalek CB, Hemmelgarn BR, Zarnke KB, Ronksley PE, Iragorri N, Graham MM, James MT: Association of NT-proBNP and BNP With Future Clinical Outcomes in Patients With ESKD: A Systematic Review and Meta-analysis. American Journal of Kidney Diseases 2020, 76(2):233-247.
- Yuan L, Chen C, Feng Y, Yang XJ, Li Y, Wu Y, Hu F, Zhang M, Li X, Hu H et al.: High-sensitivity cardiac troponin, a cardiac marker predicting death in patients with kidney disease: a dose-response meta-analysis of cohort studies. Qjm 2023, 116(5):335-343.
- Zuo ML, Chen QY, Pu L, Shi L, Wu D, Li H, Luo X, Yin LX, Siu CW, Hong DQ et al.: Impact of Hemodialysis on Left Ventricular-Arterial Coupling in End-Stage Renal Disease Patients. Blood Purif 2023, 52(7-8):702-711. [CrossRef]
- McCullough PA, Chan CT, Weinhandl ED, Burkart JM, Bakris GL: Intensive Hemodialysis, Left Ventricular Hypertrophy, and Cardiovascular Disease. Am J Kidney Dis 2016, 68(5s1):S5-s14.
- Flythe JE, Chang TI, Gallagher MP, Lindley E, Madero M, Sarafidis PA, Unruh ML, Wang AY, Weiner DE, Cheung M et al.: Blood pressure and volume management in dialysis: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2020, 97(5):861-876. [CrossRef]
- Law MC, Kwan BC, Fung JS, Chow KM, Ng JKC, Pang WF, Cheng PM, Leung CB, Szeto CC: The efficacy of managing fluid overload in chronic peritoneal dialysis patients by a structured nurse-led intervention protocol. BMC Nephrol 2019, 20(1):454.
- Sturm G, Lamina C, Zitt E, Lhotta K, Lins F, Freistätter O, Neyer U, Kronenberg F: Sex-specific association of time-varying haemoglobin values with mortality in incident dialysis patients. Nephrol Dial Transplant 2010, 25(8):2715-2722.
- Zoccali C, Benedetto FA, Mallamaci F, Tripepi G, Giacone G, Stancanelli B, Cataliotti A, Malatino LS: Left ventricular mass monitoring in the follow-up of dialysis patients: prognostic value of left ventricular hypertrophy progression. Kidney Int 2004, 65(4):1492-1498.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X et al.: Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395(10223):497-506.
- Naga YS, El Keraie A, Abd ElHafeez SS, Zyada RS: Impact of COVID-19 pandemic on care of maintenance hemodialysis patients: a multicenter study. Clin Exp Nephrol 2024, 28(10):1040-1050.
- Natale P, Zhang J, Scholes-Robertson N, Cazzolli R, White D, Wong G, Guha C, Craig J, Strippoli G, Stallone G et al.: The Impact of the COVID-19 Pandemic on Patients With CKD: Systematic Review of Qualitative Studies. Am J Kidney Dis 2023, 82(4):395-409.e391. [CrossRef]
- Tobler DL, Pruzansky AJ, Naderi S, Ambrosy AP, Slade JJ: Long-Term Cardiovascular Effects of COVID-19: Emerging Data Relevant to the Cardiovascular Clinician. Curr Atheroscler Rep 2022, 24(7):563-570.
- Watanabe A, Iwagami M, Yasuhara J, Takagi H, Kuno T: Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41(11):1783-1790.
- Mercadé-Besora N, Li X, Kolde R, Trinh NT, Sanchez-Santos MT, Man WY, Roel E, Reyes C, Delmestri A, Nordeng HME et al.: The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications. Heart 2024, 110(9):635-643. [CrossRef]
- Boros LG, Kyriakopoulos AM, Brogna C, Piscopo M, McCullough PA, Seneff S: Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination. Pharmacol Res Perspect 2024, 12(3):e1218.
Figure 1.
Patient Selection Flowchart During the COVID-19 Pandemic.
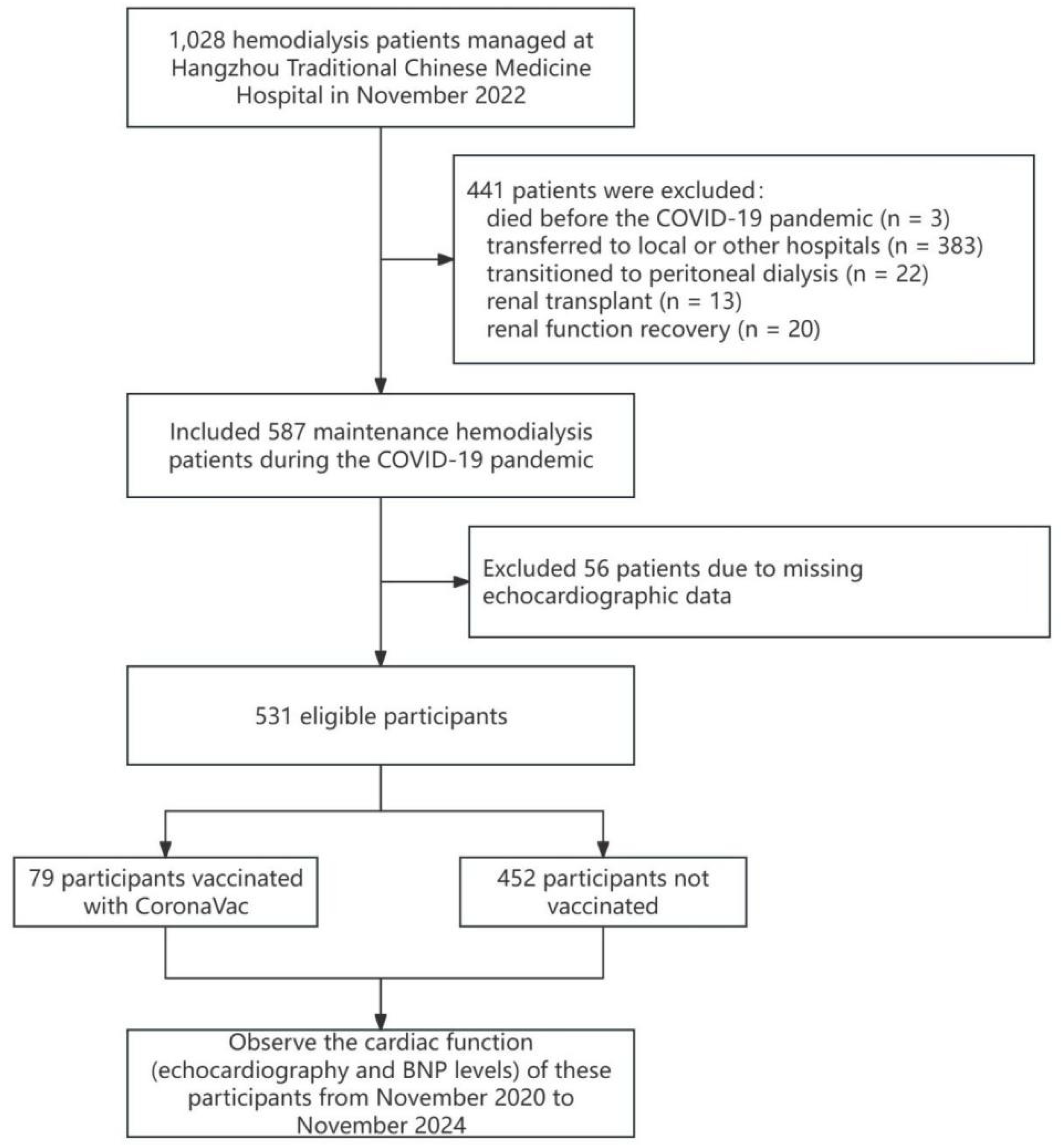
Figure 2.
Changes in BNP Levels Pre- and Post-Infection in Unvaccinated and Vaccinated Hemodialysis Patients.
Figure 2.
Changes in BNP Levels Pre- and Post-Infection in Unvaccinated and Vaccinated Hemodialysis Patients.
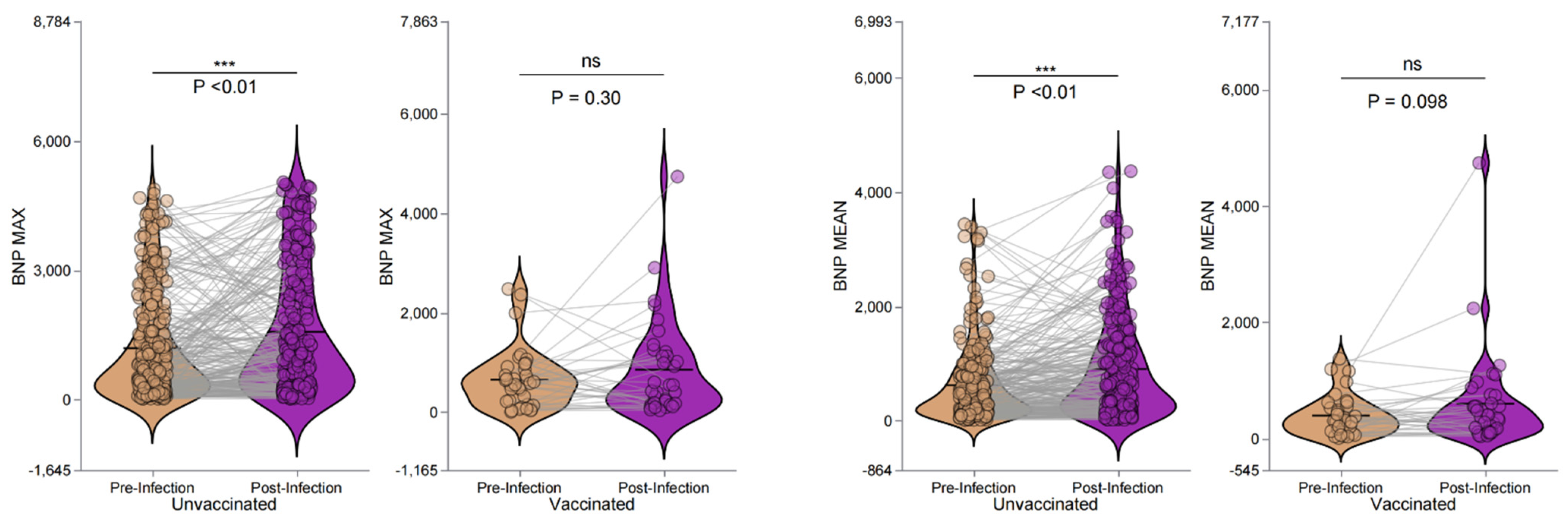
Figure 3.
Changes in echocardiographic parameters before and after COVID-19 infection in maintenance hemodialysis patients, comparing vaccinated (CoronaVac) and unvaccinated groups. The panels show changes in interventricular septal thickness (IVSD, a), left ventricular posterior wall thickness (LVPWD, b), aortic root diameter (AO, c), left atrial diameter (LA, d), ejection fraction (EF, e), and fractional shortening (FS, f). Green indicates pre-infection, and purple indicates post-infection. Left panels represent the unvaccinated group, and right panels the vaccinated group. Statistical significance is denoted by *p < 0.05, **p < 0.01, ***p < 0.001, and ns (not significant).
Figure 3.
Changes in echocardiographic parameters before and after COVID-19 infection in maintenance hemodialysis patients, comparing vaccinated (CoronaVac) and unvaccinated groups. The panels show changes in interventricular septal thickness (IVSD, a), left ventricular posterior wall thickness (LVPWD, b), aortic root diameter (AO, c), left atrial diameter (LA, d), ejection fraction (EF, e), and fractional shortening (FS, f). Green indicates pre-infection, and purple indicates post-infection. Left panels represent the unvaccinated group, and right panels the vaccinated group. Statistical significance is denoted by *p < 0.05, **p < 0.01, ***p < 0.001, and ns (not significant).
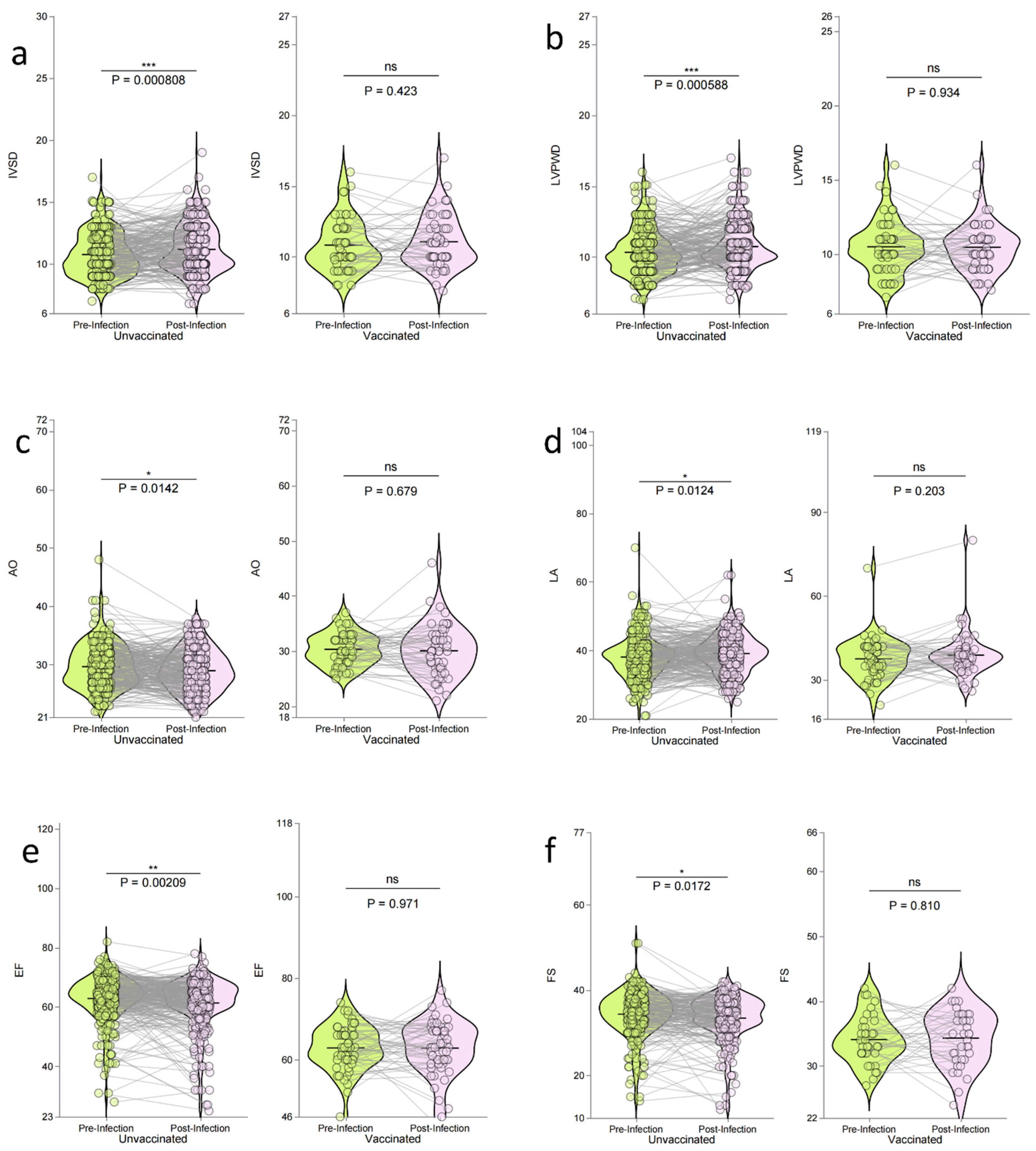

Table 1.
Baseline Demographic and Clinical Characteristics of Hemodialysis Patients by CoronaVac Status.
Table 1.
Baseline Demographic and Clinical Characteristics of Hemodialysis Patients by CoronaVac Status.
| Variable | Total (n = 531) |
Unvaccinated (n = 452) |
Vaccinated (n = 79) | t/χ2 | P-value |
|---|---|---|---|---|---|
| Age (years) | 64.51 ± 13.81 | 65.21 ± 13.76 | 60.54 ± 13.51 | t = 2.79 | 0.006 ** |
| Dialysis Duration (months) | 71.10 ± 63.30 | 73.73 ± 64.79 | 56.04 ± 51.88 | t = 2.30 | 0.022 * |
| Gender, n (%) | χ2 = 1.18 | 0.277 | |||
| Male | 334 (62.90) | 280 (61.95) | 54 (68.35) | ||
| Female | 197 (37.10) | 172 (38.05) | 25 (31.65) | ||
| Primary Disease, n (%) | 0.243 | ||||
| PKD | 26 (4.90) | 20 (4.42) | 6 (7.59) | ||
| CTD | 9 (1.69) | 8 (1.77) | 1 (1.27) | ||
| CGN | 289 (54.43) | 240 (53.10) | 49 (62.03) | ||
| DN | 199 (37.48) | 177 (39.16) | 22 (27.85) | ||
| Others | 8 (1.51) | 7 (1.55) | 1 (1.27) | ||
| Death, n (%) | χ2 = 3.98 | 0.049 * | |||
| 0 | 461 (86.82) | 387 (85.62) | 74 (93.67) | ||
| 1 | 70 (13.18) | 65 (14.38) | 5 (6.33) | ||
| HTN, n (%)* | χ2 = 0.01 | 0.918 | |||
| 0 | 72 (13.56) | 61 (13.50) | 11 (13.92) | ||
| 1 | 459 (86.44) | 391 (86.50) | 68 (86.08) | ||
| Arrhythmia, n (%) | χ2 = 3.33 | 0.068 | |||
| 0 | 491 (92.47) | 414 (91.59) | 77 (97.47) | ||
| 1 | 40 (7.53) | 38 (8.41) | 2 (2.53) | ||
| CAD, n (%) | χ2 = 12.37 | <0.001** | |||
| 0 | 392 (73.82) | 321 (71.02) | 71 (89.87) | ||
| 1 | 139 (26.18) | 131 (28.98) | 8 (10.13) | ||
| HF, n (%) | χ2 = 1.48 | 0.224 | |||
| 0 | 507 (95.48) | 429 (94.91) | 78 (98.73) | ||
| 1 | 24 (4.52) | 23 (5.09) | 1 (1.27) | ||
| COVID-19 Hospitalization, n (%) | χ2 = 0.02 | 0.898 | |||
| 0 | 452 (85.28) | 385 (85.37) | 67 (84.81) | ||
| 1 | 78 (14.72) | 66 (14.63) | 12 (15.19) | ||
| Severe COVID-19, n (%) | χ2 = 0.20 | 0.658 | |||
| 0 | 512 (96.42) | 437 (96.68) | 75 (94.94) | ||
| 1 | 19 (3.58) | 15 (3.32) | 4 (5.06) |
Abbreviations: PKD, Polycystic Kidney Disease; CTD, Connective Tissue Disease; CGN, Chronic Glomerulonephritis; DN, Diabetic Nephropathy; HTN, hypertension; CAD, coronary artery disease; HF, heart failure. *p < 0.05, ** p < 0.01.
Table 2.
Comparison of Clinical and Biochemical Characteristics Between Survival and Death Groups of Hemodialysis Patients.
Table 2.
Comparison of Clinical and Biochemical Characteristics Between Survival and Death Groups of Hemodialysis Patients.
| Variables, Units | Total (n = 531) |
Survival (n = 461) |
Death (n = 70) | t/Z | P-value |
|---|---|---|---|---|---|
| Age, years | 64.51 ± 13.81 | 62.82 ± 13.24 | 75.67 ± 12.27 | t = -7.64 | <0.001** |
| Dialysis Duration, months | 48.00 (26.00, 96.50) | 49.00 (27.00, 97.00) | 45.38 (18.66, 94.21) | Z = -1.05 | 0.292 |
| URR, % | 68.55 ± 30.37 | 68.57 ± 32.12 | 68.37 ± 8.49 | t = 0.04 | 0.97 |
| ALB, g/dL | 35.62 ± 4.00 | 35.96 ± 3.88 | 33.60 ± 4.15 | t = 4.42 | <0.001** |
| ALT, U/L | 14.07 ± 8.47 | 14.11 ± 8.18 | 13.81 ± 10.06 | t = 0.26 | 0.794 |
| LDL-C, mg/dL | 2.19 ± 0.82 | 2.21 ± 0.84 | 2.06 ± 0.68 | t = 1.35 | 0.178 |
| Ca, mg/dL | 2.22 ± 0.20 | 2.22 ± 0.20 | 2.20 ± 0.17 | t = 0.86 | 0.389 |
| TG, mg/dL | 1.84 ± 1.48 | 1.86 ± 1.53 | 1.71 ± 1.11 | t = 0.73 | 0.468 |
| HDL-C, mg/dL | 0.97 ± 0.24 | 0.97 ± 0.24 | 0.92 ± 0.25 | t = 1.64 | 0.102 |
| Cr, µmol/L | 750.93 ± 275.31 | 774.00 ± 276.61 | 612.10 ± 223.19 | t = 5.14 | <0.001** |
| PTH, pg/mL | 226.10 (117.12, 437.43) | 224.40 (117.85, 418.15) | 273.90 (108.10, 504.00) | Z = -0.65 | 0.514 |
| K, mEq/L | 4.66 ± 0.66 | 4.68 ± 0.66 | 4.56 ± 0.65 | t = 1.40 | 0.162 |
| PHOS, mg/dL | 1.61 ± 0.46 | 1.64 ± 0.46 | 1.42 ± 0.46 | t = 3.66 | <0.001** |
| Na, mEq/L | 138.03 ± 3.16 | 138.12 ± 3.18 | 137.43 ± 2.96 | t = 1.70 | 0.090* |
| Urea, µmol/L | 21.80 ± 6.52 | 22.20 ± 6.25 | 19.40 ± 7.56 | t = 3.19 | 0.002** |
| PT, seconds | 11.30 ± 2.02 | 11.20 ± 2.06 | 11.89 ± 1.68 | t = -2.42 | 0.016* |
| PA, mg/dL | 313.06 ± 80.97 | 318.20 ± 78.71 | 275.05 ± 88.09 | t = 3.25 | 0.001** |
| AST, U/L | 18.86 ± 8.75 | 18.27 ± 7.79 | 22.24 ± 12.50 | t = -2.44 | 0.017* |
| Hb, g/dL | 109.90 ± 13.72 | 110.68 ± 13.38 | 104.77 ± 14.89 | t = 3.37 | <0.001** |
| UA, µmol/L | 401.74 ± 102.71 | 410.32 ± 98.65 | 350.48 ± 112.04 | t = 4.37 | <0.001** |
| TCH, mg/dL | 3.89 ± 1.11 | 3.93 ± 1.13 | 3.63 ± 0.95 | t = 1.96 | 0.051 |
| Hs-CRP, mg/L | 2.44 (1.11, 7.32) | 2.03 (0.97, 6.20) | 7.26 (3.17, 24.80) | Z = -6.30 | <0.001** |
| Ferritin, ng/mL | 80.75 (39.30, 160.82) | 74.30 (39.30, 157.10) | 120.70 (47.10, 221.90) | Z = -1.88 | 0.06 |
Abbreviations:URR: Urea Reduction Ratio,ALB: Albumin, ALT: Alanine Transaminase, LDL-C: Low-Density Lipoprotein Cholesterol, Ca: Calcium, TG: Triglycerides, HDL-C: High-Density Lipoprotein Cholesterol, Cr: Creatinine, PTH: Parathyroid Hormone, K: Potassium, PHOS: Phosphate, Na: Sodium, Urea: Urea, PT: Prothrombin Time, PA: Prealbumin, AST: Aspartate Transaminase, Hb: Hemoglobin, UA: Uric Acid, TCH: Total Cholesterol, Hs-CRP: High-sensitivity C-reactive Protein. *p < 0.05, ** p < 0.01.
Table 3.
Echocardiographic Parameters and BNP Levels in Relation to Mortality Among Maintenance Hemodialysis Patients.
Table 3.
Echocardiographic Parameters and BNP Levels in Relation to Mortality Among Maintenance Hemodialysis Patients.
| Variables, Units | Total (n = 531) | Survival (n = 461) | Death (n = 70) | Z/χ2 | P-value |
|---|---|---|---|---|---|
| BNP Max, pg/mL | 462.50 (98.75, 1216.50) | 401.50 (86.75, 999.75) | 1246.00 (387.75, 2456.50) | Z = -4.77 | <0.001** |
| BNP Mean, pg/mL | 283.00 (84.75, 679.75) | 247.00 (70.75, 612.25) | 584.50 (181.50, 992.00) | Z = -3.52 | <0.001** |
| IVSD, mm | 10.20 (9.00, 12.00) | 10.00 (9.00, 12.00) | 11.00 (10.00, 12.00) | Z = -1.39 | 0.165 |
| LVIDd, mm | 49.00 (46.00, 53.00) | 49.00 (46.00, 53.00) | 49.00 (46.02, 53.00) | Z = -0.08 | 0.938 |
| LVIDs, mm | 32.00 (30.00, 35.00) | 32.00 (30.00, 35.00) | 33.00 (30.00, 36.40) | Z = -0.99 | 0.321 |
| LVPWD, mm | 10.00 (9.00, 11.00) | 10.00 (9.00, 11.00) | 10.00 (9.57, 11.65) | Z = -1.53 | 0.127 |
| AO, mm | 29.00 (27.00, 32.00) | 29.00 (27.00, 32.00) | 29.00 (27.00, 32.00) | Z = -0.36 | 0.718 |
| LA, mm | 38.00 (34.00, 41.00) | 38.00 (34.00, 41.00) | 39.00 (34.25, 42.00) | Z = -1.14 | 0.254 |
| SV, mL | 72.00 (63.50, 85.00) | 72.00 (63.00, 85.00) | 73.00 (65.00, 81.00) | Z = -0.12 | 0.906 |
| EF, % | 64.00 (60.00, 68.00) | 64.00 (60.00, 68.00) | 64.00 (58.00, 66.75) | Z = -1.46 | 0.144 |
| FS, % | 35.00 (32.00, 38.00) | 35.00 (32.00, 38.00) | 35.00 (31.25, 37.00) | Z = -1.04 | 0.299 |
| Arrhythmia | χ2 = 3.28 | 0.07 | |||
| Normal | 491 (92.47) | 430 (93.28) | 61 (87.14) | ||
| Abnormal | 40 (7.53) | 31 (6.72) | 9 (12.86) | ||
| Coronary Artery Disease (CAD) | χ2 = 70.02 | <0.001** | |||
| Normal | 392 (73.82) | 369 (80.04) | 23 (32.86) | ||
| Abnormal | 139 (26.18) | 92 (19.96) | 47 (67.14) | ||
| Heart Failure | χ2 = 7.17 | 0.007** | |||
| Normal | 507 (95.48) | 445 (96.53) | 62 (88.57) | ||
| Abnormal | 24 (4.52) | 16 (3.47) | 8 (11.43) | ||
| IVSD Status | χ2 = 1.07 | 0.301 | |||
| Normal | 212 (39.92) | 188 (40.78) | 24 (34.29) | ||
| Abnormal | 319 (60.08) | 273 (59.22) | 46 (65.71) | ||
| LVIDd Status | χ2 = 1.50 | 0.221 | |||
| Normal | 464 (87.38) | 406 (88.07) | 58 (82.86) | ||
| Abnormal | 67 (12.62) | 55 (11.93) | 12 (17.14) | ||
| LVIDs Status | χ2 = 3.86 | 0.049* | |||
| Normal | 228 (90.48) | 200 (92.17) | 28 (80.00) | ||
| Abnormal | 24 (9.52) | 17 (7.83) | 7 (20.00) | ||
| LVPWDStatus | χ2 = 1.71 | 0.191 | |||
| Normal | 251 (47.27) | 223 (48.37) | 28 (40.00) | ||
| Abnormal | 280 (52.73) | 238 (51.63) | 42 (60.00) | ||
| AO Status | χ2 = 0.00 | 1 | |||
| Normal | 517 (97.36) | 449 (97.40) | 68 (97.14) | ||
| Abnormal | 14 (2.64) | 12 (2.60) | 2 (2.86) | ||
| LA Status | χ2 = 0.67 | 0.412 | |||
| Normal | 385 (72.64) | 337 (73.26) | 48 (68.57) | ||
| Abnormal | 145 (27.36) | 123 (26.74) | 22 (31.43) | ||
| SV Status | χ2 = 0.04 | 0.846 | |||
| Normal | 355 (90.79) | 306 (90.53) | 49 (92.45) | ||
| Abnormal | 36 (9.21) | 32 (9.47) | 4 (7.55) | ||
| EF Status | χ2 = 1.18 | 0.278 | |||
| Normal | 486 (91.87) | 424 (92.37) | 62 (88.57) | ||
| Abnormal | 43 (8.13) | 35 (7.63) | 8 (11.43) | ||
| FS Status | χ2 = 0.30 | 0.586 | |||
| Normal | 381 (93.38) | 332 (93.79) | 49 (90.74) | ||
| Abnormal | 27 (6.62) | 22 (6.21) | 5 (9.26) |
Abbreviations: BNP Max: Maximum Brain Natriuretic Peptide, BNP Mean: Mean Brain Natriuretic Peptide, IVSD: Interventricular Septal Thickness in Diastole, LVIDd: Left Ventricular Internal Diameter in Diastole, LVIDs: Left Ventricular Internal Diameter in Systole, LVPWD: Left Ventricular Posterior Wall Thickness in Diastole, AO: Aortic Root Diameter, LA: Left Atrium Diameter, SV: Stroke Volume, EF: Ejection Fraction, FS: Fractional Shortening, Arrhythmia: Abnormal Heart Rhythm. *p < 0.05, ** p < 0.01.
Table 4.
Multivariate Cox Regression Analysis of Predictors of Mortality in Maintenance Hemodialysis Patients.
Table 4.
Multivariate Cox Regression Analysis of Predictors of Mortality in Maintenance Hemodialysis Patients.
| Univariate | Multivariate | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | S.E | Z | P-value | HR (95% CI) | Variables | β | S.E | Z | P-value |
| Age | 0.07 | 0.01 | 7.23 | <0.001** | 1.08 (1.06–1.10) | 0.1 | 0.04 | 2.6 | 0.009** | 1.10 (1.02–1.18) |
| ALB | -0.11 | 0.02 | -4.48 | <0.001** | 0.90 (0.85–0.94) | 0.13 | 0.12 | 1.05 | 0.294 | 1.14 (0.89–1.45) |
| Cr | -0.01 | 0 | -4.3 | <0.001** | 0.99 (0.99–0.99) | 0 | 0 | 0.12 | 0.906 | 1.00 (1.00–1.00) |
| PHOS | -1.16 | 0.3 | -3.86 | <0.001** | 0.31 (0.17–0.57) | -0.56 | 0.93 | -0.6 | 0.547 | 0.57 (0.09–3.54) |
| Urea | -0.07 | 0.02 | -3.34 | <0.001** | 0.93 (0.89–0.97) | -0.09 | 0.07 | -1.3 | 0.195 | 0.91 (0.79–1.05) |
| PT | 0.06 | 0.03 | 2.2 | 0.028* | 1.07 (1.01–1.13) | -0.03 | 0.17 | -0.16 | 0.869 | 0.97 (0.69–1.37) |
| PA | -0.01 | 0 | -3.29 | <0.001** | 0.99 (0.99–0.99) | 0 | 0.01 | 0.01 | 0.989 | 1.00 (0.99–1.00) |
| AST | 0.04 | 0.01 | 3.54 | <0.001** | 1.04 (1.02–1.06) | 0.03 | 0.02 | 1.43 | 0.154 | 1.03 (0.99–1.08) |
| Hb | -0.03 | 0.01 | -3.5 | <0.001** | 0.97 (0.96–0.99) | -0.04 | 0.03 | -1.34 | 0.18 | 0.96 (0.90–1.02) |
| UA | -0.01 | 0 | -4.52 | <0.001** | 0.99 (0.99–0.99) | 0 | 0 | 0.55 | 0.584 | 1.00 (0.99–1.01) |
| Hs-CRP | 0.01 | 0 | 4.84 | <0.001** | 1.01 (1.01–1.02) | 0.03 | 0.01 | 1.97 | 0.049* | 1.03 (1.01–1.05) |
| BNP Max | 0.01 | 0 | 4.93 | <0.001** | 1.01 (1.01–1.01) | 0 | 0 | -0.19 | 0.847 | 1.00 (1.00–1.00) |
| BNPMean | 0.01 | 0 | 2.1 | 0.036* | 1.01 (1.01–1.01) | 0 | 0 | -0.66 | 0.506 | 1.00 (1.00–1.00) |
| HTN | -0.81 | 0.28 | -2.92 | 0.004** | 0.44 (0.26–0.77) | -0.63 | 0.73 | -0.86 | 0.388 | 0.53 (0.13–2.23) |
| CAD | 1.93 | 0.25 | 7.57 | <0.001** | 6.88 (4.18–11.34) | 1.44 | 0.7 | 2.04 | 0.041* | 4.20 (1.06–16.71) |
| HF | 1.17 | 0.38 | 3.12 | 0.002** | 3.22 (1.54–6.74) | -0.18 | 1.37 | -0.13 | 0.896 | 0.84 (0.06–12.34) |
Abbreviations: ALB: Albumin, Cr: Creatinine,PHOS: Phosphate, Urea: Urea Nitrogen,PT: Prothrombin Time, PA: Prealbumin, AST: Aspartate Transaminase, Hb: Hemoglobin, UA: Uric Acid, Hs-CRP: High-sensitivity, BNP Max: Brain Natriuretic Peptide Maximum, BNP Mean: Brain Natriuretic Peptide Mean, HTN: Hypertension,CAD: Coronary Artery Disease, HF: Heart FailureHR: Hazard Ratio,CI: Confidence Interval, S.E: Standard Erro. *p < 0.05, ** p < 0.01.
Table 5.
Multivariate Cox Regression Analysis of Echocardiographic and Clinical Parameters Across Different Models.
Table 5.
Multivariate Cox Regression Analysis of Echocardiographic and Clinical Parameters Across Different Models.
| Variables | Model 1 HR (95% CI), p | Model 2 HR (95% CI), p | Model 3 HR (95% CI), p |
|---|---|---|---|
| LVIDd | 1.46 (0.78–2.71), 0.235 | 1.03 (0.28–3.76), 0.959 | 2.85 (0.18–45.72), 0.460 |
| LVPWD | 1.36 (0.84–2.19), 0.207 | 1.19 (0.25–5.68), 0.824 | 1.58 (0.05–48.08), 0.793 |
| AO | 1.06 (0.26–4.33), 0.934 | 0.00 (0.00–Inf), 0.997 | 0.00 (0.00–Inf), 0.999 |
| LA | 1.25 (0.75–2.06), 0.394 | 1.17 (0.29–4.65), 0.828 | 0.12 (0.01–1.96), 0.135 |
| IVSD | 1.28 (0.78–2.10), 0.326 | 5.94 (1.04–33.77), 0.045* | 49.88 (0.85–2938.25), 0.060* |
| SV | 0.81 (0.29–2.23), 0.679 | 1.12 (0.25–5.14), 0.879 | 0.41 (0.02–10.64), 0.593 |
| EF | 1.49 (0.71–3.11), 0.289 | 0.10 (0.01–1.14), 0.064 | 0.00 (0.00–74.96), 0.259 |
| FS | 1.49 (0.59–3.73), 0.398 | 0.57 (0.05–6.22), 0.649 | 97.62 (0.02–562248.02), 0.300 |
| LVIDs | 2.66 (1.16–6.10), 0.021* | 28.88 (3.47–240.13), 0.002** | 1574.03 (3.30–750000.88), 0.019* |
| Gender (Female) | 1.00 (0.61–1.62), 0.988 | 0.15 (0.03–0.66), 0.013* | 0.01 (0.00–0.34), 0.011* |
| LVIDd (Abnormals) | 0.99 (0.96–1.03), 0.779 | 0.86 (0.74–0.99), 0.046* | 0.78 (0.57–1.08), 0.139 |
| LVIDs (Abnormal) | 1.02 (0.97–1.08), 0.434 | 0.87 (0.75–1.01), 0.074 | 0.72 (0.51–0.99), 0.050 |
| SV (Abnormal) | 1.00 (0.99–1.01), 0.914 | 1.04 (1.01–1.07), 0.037* | 1.08 (1.01–1.16), 0.023* |
| EF (Abnormal) | 0.98 (0.95–1.00), 0.089 | 0.87 (0.76–0.98), 0.027* | 0.71 (0.52–0.96), 0.025* |
| AO (Abnormal) | 1.00 (0.94–1.07), 0.888 | 0.93 (0.81–1.06), 0.288 | 0.65 (0.45–0.95), 0.027* |
Abbreviations: HR: Hazard Ratio,CI: Confidence Interval,Model 1: Crude analysis,Model 2: Adjusted for HTN, arrhythmia, CAD, and HF, Model 3: Adjusted for age, HTN, arrhythmia, CAD, HF, ALB, and PA. *p < 0.05, ** p < 0.01.
Table 6.
Changes in BNP Levels Pre- and Post-Infection in Unvaccinated and Vaccinated Hemodialysis Patients.
Table 6.
Changes in BNP Levels Pre- and Post-Infection in Unvaccinated and Vaccinated Hemodialysis Patients.
| Group | Pre-Infection (n=283) | Post-Infection (n=283) | z | p-value | z-value | z p-value |
|---|---|---|---|---|---|---|
| BNP Max, pg/mL | ||||||
| Unvaccinated | 652.00 (234.00, 1765.50) | 1059.00 (312.00, 2486.50) | 10629.5 | <0.001** | -1.76 | 0.078 |
| Vaccinated | 573.50 (205.50, 882.50) | 489.50 (161.25, 1152.75) | 266 | 0.3 | -2.78 | 0.006** |
| BNP Mean, pg/mL | ||||||
| Unvaccinated | 398.00 (158.50, 833.00) | 619.00 (226.50, 1291.50) | 8658 | < 0.001** | -1.56 | 0.119 |
| Vaccinated | 311.00 (121.50, 535.25) | 389.50 (155.75, 640.50) | 227 | 0.098 | -2.33 | 0.02* |
*p < 0.05, ** p < 0.01.
Table 7.
Changes in Echocardiographic Parameters Before and After COVID-19 Infection in Vaccinated and Unvaccinated Maintenance Hemodialysis Patients.
Table 7.
Changes in Echocardiographic Parameters Before and After COVID-19 Infection in Vaccinated and Unvaccinated Maintenance Hemodialysis Patients.
| Group | Pre-Infection (n=348) | Post-Infection (n=348) | t-value | p-value | |
|---|---|---|---|---|---|
| IVSD, mm | Unvaccinated | 10.76 ± 1.73 | 11.18 ± 1.95 | -3.39 | <0.001** |
| Vaccinated | 10.84 ± 1.81 | 11.07 ± 1.86 | -0.81 | 0.423 | |
| LVIDd, mm | Unvaccinated | 49.48 ± 5.65 | 49.79 ± 5.33 | -0.82 | 0.411 |
| Vaccinated | 49.71 ± 5.64 | 49.59 ± 5.35 | 0.13 | 0.897 | |
| LVIDS, mm | Unvaccinated | 33.52 ± 6.01 | 33.61 ± 5.81 | 0.15 | 0.883 |
| Vaccinated | 32.80 ± 3.36 | 32.23 ± 4.30 | 1.3 | 0.206 | |
| LVPWD, mm | Unvaccinated | 10.34 ± 1.58 | 10.96 ± 3.12 | -3.2 | 0.001** |
| Vaccinated | 10.50 ± 1.78 | 10.48 ± 1.57 | 0.08 | 0.934 | |
| AO, mm | Unvaccinated | 29.68 ± 3.73 | 28.92 ± 3.95 | 2.62 | 0.014* |
| Vaccinated | 30.35 ± 2.83 | 29.53 ± 5.98 | 0.95 | 0.679 | |
| LA, mm | Unvaccinated | 38.15 ± 6.06 | 39.20 ± 5.73 | -2.51 | 0.013* |
| Vaccinated | 37.58 ± 7.33 | 38.91 ± 7.82 | -1.29 | 0.203 | |
| SV, mL | Unvaccinated | 74.95 ± 16.79 | 75.99 ± 17.05 | -0.35 | 0.727 |
| Vaccinated | 81.57 ± 32.12 | 78.55 ± 13.44 | 0.63 | 0.531 | |
| EF, % | Unvaccinated | 62.89 ± 7.64 | 61.39 ± 8.59 | 3.11 | 0.002** |
| Vaccinated | 63.30 ± 5.08 | 63.13 ± 6.27 | 0.27 | 0.971 | |
| FS, % | Unvaccinated | 34.37 ± 5.44 | 33.32 ± 5.58 | 2.37 | 0.017* |
| Vaccinated | 34.11 ± 3.72 | 34.44 ± 4.38 | -0.24 | 0.810 |
Abbreviations: Data are presented as mean ± standard deviation, IVSD: Interventricular Septal Thickness in Diastole, LVIDd: Left Ventricular Internal Diameter in Diastole, LVIDS: Left Ventricular Internal Diameter in Systole, LVPWD: Left Ventricular Posterior Wall Thickness in Diastole, AO: Aortic Root Diameter, LA: Left Atrium Diameter, SV: Stroke Volume, EF: Ejection Fraction,FS: Fractional Shortening. *p < 0.05, ** p < 0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



