Submitted:
04 January 2025
Posted:
07 January 2025
You are already at the latest version
Abstract
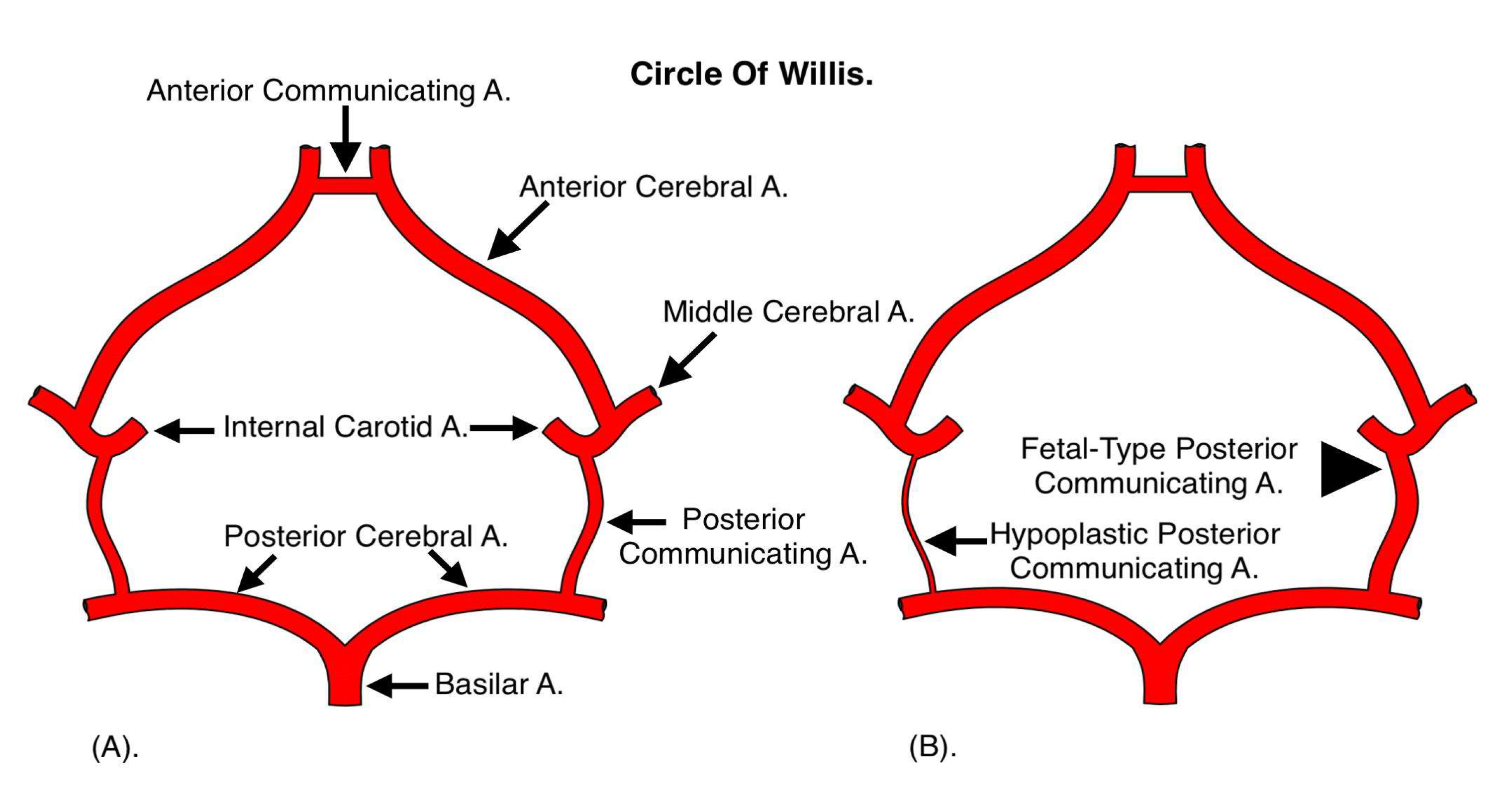
The fetal-type posterior communicating artery (PCoA) variant, present in approximately 17.5% of adults, has significant clinical and surgical implications, particularly in the management of cerebrovascular disorders such as aneurysms. This variant alters cerebral hemodynamics, increasing the risk of ischemic events and complicating neurosurgical interventions. Surgical management of aneurysms associated with fetal-type PCoA requires precise anatomical knowledge and advanced imaging to tailor the approach. Techniques such as pterional craniotomy and temporary clipping of the internal carotid artery facilitate safe dissection and aneurysm obliteration while preserving vascular integrity. This paper discusses the challenges posed by fetal-type PCoA anatomy, highlights tailored surgical techniques, and explores the role of endovascular alternatives. A case presentation demonstrates the successful management of a ruptured PCoA aneurysm, emphasizing the importance of individualized surgical strategies. Long-term follow-up is crucial to prevent complications such as recurrence or ischemic events, underscoring the need for a multidisciplinary approach to optimize patient outcomes.
Keywords:
1. Introduction

| Feature | Standard PCoA Anatomy | Fetal-Type PCoA Anatomy | Clinical Implications & Tratament |
|---|---|---|---|
| Origin | Posterior Cerebral Artery (PCA) | Internal Carotid Artery (ICA) | -Fetal-Type is a common congenital variation with altered blood flow |
| Hemodynamics | Normal flow dynamics | Abnormal flow due to ICA-PCA connection | -Increased risk of ischemia and aneurysm rupture. |
| Aneurysm Risk | Standard risk of formation | Higher risk due to altered hemodynamics | -Aneurysms more prone to rupture and difficult to treat. |
| Surgical Challenges | More straightforward dissection | Complex due to vascular fragility and abnormal anatomy | - Difficult access and higher risk of complications. |
| Surgical Approach | Standard clipping techniques | Requires tailored approach (Extra care not to obstruct the blood flow) | - Risk of obstructing the blood flow. Attention to the patency is crucial. Personalized surgical strategy for better outcomes. |
| Postoperative Monitoring | Routine follow-up | Extended follow-up for potential recurrence and ischemia. | -Regular imaging (Ct/MRI- Angio) and neurosurgical monitoring are critical. |
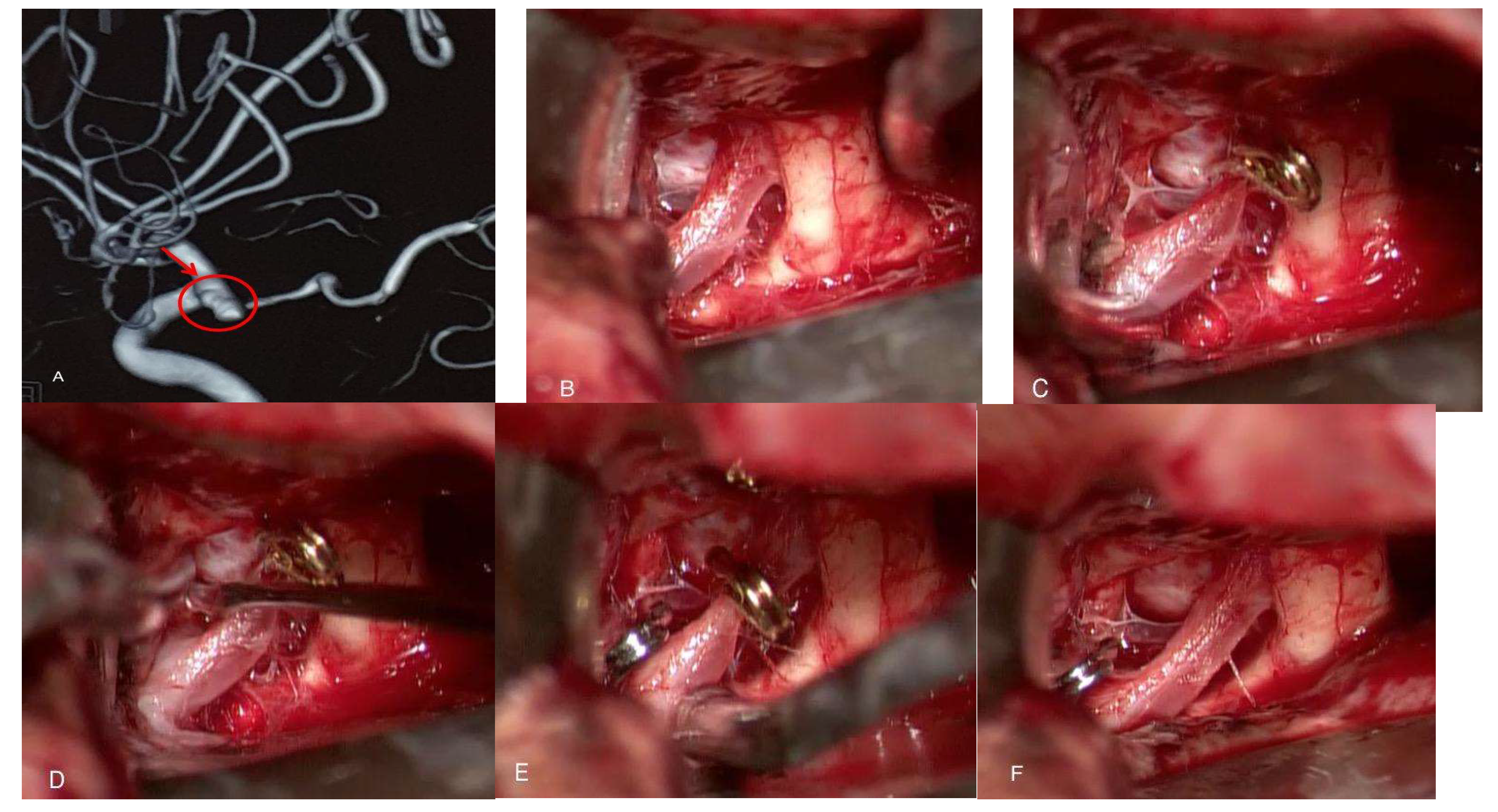
2. Case Presentation
3. Surgical Technique
4. Discussion
Anatomical Considerations and Challenges:
5. Conclusion
Author Contribution
Acknowledgement
References
- Mazzucchi, E., Casali, M., & Borsato, S. (2022). “Fetal-type posterior communicating artery and its implications in aneurysm surgery.” Journal of Neurosurgery, 15(2), 567–578.
- Chung, D., & Lee, J. (2023). “Challenges in managing fetal-type PCoA aneurysms: A review of surgical approaches.” Neurosurgical Review, 31(3), 233–240.
- Huang, Y., Zhang, L., & Liu, Y. (2021). “Anatomical and surgical considerations of fetal-type posterior communicating artery aneurysms.” Stroke Surgery and Neurointervention, 18(4), 1023–1030.
- Patel, R., & Goyal, M. (2022). “Preoperative imaging strategies in aneurysm surgery: Emphasis on PCoA variants.” Journal of Vascular and Interventional Radiology, 33(5), 1248–1255.
- Kumar, V., Prakash, R., & Malhotra, A. (2023). “Endovascular versus microsurgical treatment of posterior communicating artery aneurysms.” Neurointervention, 13(1), 29–36.
- Purkayastha, S., Singh, A., & Shah, S. (2006). “Fetal-type posterior communicating artery: Implications in ischemic stroke.” Stroke Research and Treatment, 12(1), 45–51.
- Boukili, M., Asser, M., Gupta, K., & Horio, N. (2021). “Advances in microsurgical techniques for PCoA aneurysms.” World Neurosurgery, 15(6), 789–805.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



