
Submitted:
05 January 2025
Posted:
06 January 2025
You are already at the latest version
Abstract
Background: In unresectable pleural mesothelioma, pemetrexed+cisplatin as first line is considered the standard of care, but novel treatments have been recently proposed. Methods: Our objective was to compare, albeit indirectly, the results of randomized controlled trials on overall survival (OS) The IPDfromKM method was employed for reconstruct individual patient data (IPD) from the graphs of Kaplan-Meier curves. Cox statistics was run to estimate hazard ratios (HRs). Results: After a literature search on Medline (via PubMed) and Scopus databases, six randomized controlled trials were identified in which five new treatments (nivolumab plus ipilimumab, bevacizumab plus pemetrexed plus cisplatin, chemotherapy plus pembrolizumab, ONCOS-102 plus pemetrexed plus cisplatin/carboplatin, cediranib plus pemetrexed+cisplatin with maintenance with cediranib) were evaluated. In 5 trials, pemetrexed plus cisplatin was the standard of care given to the control arms. Nivolumab plus ipilimumab, bevacizumab plus pemetrexed plus cisplatin, and chemotherapy plus pembrolizumab showed a significantly better OS compared with controls. ONCOS-102 plus pemetrexed plus cisplatin/carboplatin did not significantly improve OS. In contrast, OS worsened with cisplatin alone and with cediranib plus pemetrexed+cisplatin with maintenance with cediranib. Discussion: Our analysis indicates that, in patients with unresectable pleural mesothelioma, three of the five novel treatments provided a significant survival benefit compared with the standard of care. Further research is needed to confirm the OS benefit found in our analysis with some treatments, whereas cisplatin alone and cediranib plus pemetrexed+cisplatin with maintenance with cediranib do not seem to deserve further research.
Keywords:
pleural mesothelioma
; pemetrexed
; cisplatin
; nivolumab+ipilimumab
; bevacizumab+pemetrexed+cisplatin
; pembrolizumab
; durvalumab
; reconstruction of patient-level data
1. Introduction
Malignant pleural mesothelioma is a rare and aggressive carcinoma associated with a poor prognosis [1]. It is generally triggered by asbestos exposure [2], with a latency period ranging from 20 to 40 years [3]. The diagnosis of pleural mesothelioma is often delayed because of the silent and insidious onset of the disease, which contributes to the inauspicious outcome. In fact, the estimated 5-year survival probability in untreated patients is less than 5.0%, with an average of 4-12 months depending on the stage of disease, patients’ age, and histopathologic subtype [4,5].
From a pathophysiological perspective, malignant pleural mesothelioma originates from pleural mesothelial cells that rapidly spread to the diaphragm, pericardium and lungs [1]. Almost all pleural mesotheliomas are diffuse, and by the time of diagnosis, cancer cells have usually invaded many tissues [6]. For this reason, surgery is often impractical because of the metastatic nature of the carcinoma, as well as the high risks of complications and treatment failure [7].
The only treatment option in patients with unresectable pleural mesothelioma is chemotherapy, with pemetrexed+cisplatin administered first-line and considered the standard of care [8]. Indeed, some studies have demonstrated improved quality of life and favourable clinical outcomes, such as overall survival (OS) and progression-free survival (PFS) [9,10]. In patients without tumour progression, the treatment regimen should be continued for up to six cycles while, in subjects with unacceptable toxicity due to adverse events, pemetrexed+carboplatin could be a possible alternative [11].
In recent years, new treatments have been proposed for this clinical indication, representing a potential therapeutic advancement [12,13,14,15,16,17,18,19]. They include nivolumab plus ipilimumab, bevacizumab plus pemetrexed plus cisplatin, chemotherapy plus pembrolizumab, ONCOS-102 plus pemetrexed plus cisplatin/carboplatin, cediranib plus pemetrexed+cisplatin with maintenance with cediranib. However, there are no current studies aimed at summarizing the efficacy of the available therapeutic options or comparing these new combinations with the standard of care. In 2022, we conducted a preliminary analysis of the 4 published clinical trials [20] but, in the meantime, more studies have been conducted on the topic.
The aim of this paper was to summarise the current state of the art and provide new evidence on the clinical efficacy of available or proposal first-line treatment options for patients with unresectable pleural mesothelioma. In particular, we reconstructed individual patient data (IPD) from survival curves and then, performed indirect analyses among published clinical trials. For this purpose, we used an innovative artificial intelligence tool (the IPDfromKM or Shiny method [21,22]) published in 2021. From 2022 to 2024, this technique has been increasingly used especially, but not exclusively, in oncology and cardiology to generate new clinical evidence [23,24,25,26,27]. The reliability and validity of the IPDfromKM method were recently confirmed in the study by Rogula and co-workers, who demonstrated the overlap between the original and reconstructed Kaplan-Meier curves obtained with the artificial intelligence tool [28].
2. Materials and Methods
Study Design and Literature Search
We performed a systematic literature review by searching two databases (Medline, via Pubmed, and Scopus). The aim was to identify randomized controlled trials (RCTs), either phase II or phase III, that tested the efficacy of new agents ("novel treatments") when given as first-line in patients with unresectable pleural mesothelioma. The final search was conducted on December 5, 2024. The search term was constructed as follows: “mesothelioma[titl]” with filters on RCTs. Article selection was performed in accordance with the PRISMA algorithm [29].
Inclusion Criteria
Only RCTs conducted on previously untreated patients with unresectable mesothelioma, written in English, were eligible. We included all the RCTs that tested the effects of a combination or a single-agent treatment on OS, using a standard of care in the control group. Since the method of our analysis aimed at reconstructing IPD, another inclusion criterion was the availability of a Kaplan-Meier graph comparing the intervention and control groups based on the OS endpoint.
Data Analysis
We firstly selected OS as the endpoint of the statistical analysis and then performed an indirect comparison between each of the six intervention arms vs. the six control arms (pemetrexed+cisplatin or chemotherapy) pooled together. The hazard ratio (HR), with 95% confidence interval (CI), was the parameter for testing the superiority of each of the 6 experimental treatments vs. standard of care (pemetrexed+cisplatin). In addition, the six control arms of the included trials were subjected to an assessment of cross-trial heterogeneity, which was based on Wald’s test and the likelihood ratio test. To perform these analyses, we used three statistical packages ("survival," "survminer," "survRM2," and "readxl") of the R-platform (version 4.3.2) [30]. Finally, since the oldest of the six included trials compared pemetrexed+cisplatin vs. cisplatin alone, the arm treated with pemetrexed+cisplatin was pooled with the other 5 control arms given pemetrexed+cisplatin. Then, the arm treated with cisplatin alone was pooled with the experimental arms of the other 5 trials. This allowed us to determine the magnitude of the survival gain between the most effective treatment vs. cisplatin alone.
Reconstruction of Individual Patient Data from Kaplan-Meier Curves and Statistical Analysis
Our analysis, performed with the online version of the IPDfromKM method, included a first phase in which the graph of each Kaplan-Meier curve was digitized using Webplotdigitizer (version 4 online; https://apps.automeris.io/ accessed 10 August 2024), and a second phase in which the IPDfromKM algorithm [22] reconstructed individual patient data, separately for each curve, from the x-y coordinates deriving from the digitized KM curves (software version 1.2.3.0; https://www.trialdesign.org/one-page-shell.html#IPDfromKM, accessed 10 August 2024) . Once these databases of reconstructed patients were created, indirect comparisons were made between the experimental treatments and the standard of care, using the same statistical tests (e.g. HR estimated by Cox’s multiple regression model) as in clinical trials based on “real” patients.
3. Results
Six RCTs [12,13,14,15,16,17] were identified from the literature search. Figure 1 shows the selection process of the included trials according to the PRISMA algorithm. The characteristics of these 6 trials are presented in Table 1. The 6 treatments tested in these trials included: 1) nivolumab+ipilimumab; 2) bevacizumab+pemetrexed+cisplatin; 3) pembrolizumab+chemotherapy; 4) ONCOS-102 plus pemetrexed plus cisplatin/carboplatin; 5) cediranib plus pemetrexed+platinum; 6) cisplatin alone. In the control arms, the treatment was pemetrexed+cisplatin with the only exception of chemotherapy given to the controls in the trial by Chu et al. (2023) [14]. As described in the “Material and methods” section, the arm treated with pemetrexed+cisplatin in the study by Vogelzang et al. [17] was grouped with the arms treated with pemetrexed+cisplatin in the other 5 trials. Regarding the randomized trial by Ponce et al. [15], the treatment arm included ONCOS-102, which is an oncolytic adenovirus expressing granulocyte-macrophage colony-stimulating factor. Since the trial enrolled both pre-treated patients and treatment-naïve patients, only the latter group, consisting of a very small number of patients, met the inclusion criteria of our analysis.
To reconstruct individual patient data, the IPDfromKM technique was applied to the 12 Kaplan-Meier curves reported in these 6 trials (Table 1). The analysis of reconstructed OS curves was then carried out according to standard survival statistics; indirect comparisons between different treatments were evaluated according to HRs. The six experimental arms of these analyses are shown in Table 1. As control groups for our indirect comparisons, we considered the 5 arms treated with pemetrexed+platinum and the arm treated with chemotherapy from the trial by Chu et al. (2023) [14]; these 6 arms were pooled to generate a single Kaplan-Meier curve of 1,020 controls.
Among the six control arms (Figure 2), the level of cross-trial heterogeneity was significant (likelihood ratio test= 32.6 on 5 df, p<0.001; Wald test = 34.23 on 5 df, p<0.001). However, it should be noted that the first 4 trials reported in Table 1 (Peters et al., 2022 [12]; Zalcman et al., 2016 [13]; Chu et al., 2023 [14]; Ponce et al., 2023 [15]) showed no significant heterogeneity (data not shown). By contrast, the last 2 trials in Table 2 (Tsao et al., 2019 [16] and Vogelzang et al., 2003 [17]) were those determining the significant level of overall heterogeneity mentioned above. On the one hand, this can in part be explained by the fact that the trial by Vogelzang et al., 2003 [17], conducted more than 20 years ago, had a worse survival pattern compared with the first 4 trials, which are more recent; on the other hand, the performance of combining cediranib with other agents, studied in the trial by Tsao et al., (2019) [16], was particularly poor, as confirmed by the 47 controls shown in Figure 2.
The median OS in the 1,020 controls pooled together was 14.6 months (95% CI, 13.6 to 15.6; n=1,020). In the 6 treatment groups, medians of OS were the following:
- -
- nivolumab plus ipilimumab: 18.29 months (95% CI, 17.63 to 21.9);
- -
- bevacizumab plus pemetrexed plus cisplatin: 19.13 months (95% CI, 17.15 to 23.1);
- -
- chemotherapy plus pembrolizumab: 18.26 months (95% CI, 15.01 to 22.1);
- -
- ONCOS-102 plus pemetrexed plus cisplatin or carboplatin: 21.27 months (95% CI, 11.19 to not computable);
- -
- cediranib plus cisplatin-pemetrexed: 11.58 months (95% CI, 8.24 to 17.1);
- -
- cisplatin alone: 9.67 months (95% CI, 8.25 to 11.2).
With the exceptions of cisplatin alone and cediranib plus pemetrexed+cisplatin, the remaining 4 experimental arms showed very similar values of median OS, around 18 to 21 months. This indicates that these treatments determine an improvement in OS of slightly more than 3 months.
4. Discussion
The main finding emerging from our analysis is that, in comparison with pemetrexed+ cisplatin, three of the novel treatments proposed as first-line (i.e., nivolumab plus ipilimumab, bevacizumab plus pemetrexed plus cisplatin, and chemotherapy plus pembrolizumab) provided a significant incremental benefit in OS compared with the standard of care (pemetrexed+cisplatin in 5 cases out of 6), even though the magnitude of this benefit was quite small (around 3 months). The role of the combination of ONCOS-102 with pemetrexed plus cisplatin or carboplatin as first-line remains uncertain due to the very small number of enrolled patients. By contrast, we found a negative survival outcome for the regimen based on cediranib, which was numerically inferior to the 6 control arms pooled together and significantly inferior to the three treatments mentioned above, which showed the best survival outcomes (detailed HR data not shown). Furthermore, our results confirmed the inferiority of cisplatin alone compared with pemetrexed plus cisplatin. Among the three best performing treatments given as first-line options, their limited incremental effectiveness aligns with the observations reported for second-line treatments in unresectable mesothelioma [15].
Our analysis has strengths and limitations. One strength is the excellent performance of the Shiny method in reconstructing individual patient data from published Kaplan-Meier curves, which is in line with findings from the most recent literature [12,16] . In our study, the quality of the reconstruction of individual patient data performed with the IPDfromKM method is confirmed by the agreement between the original HR values (Table 1) and those based on the reconstructed patient data (Table 2). Similarly, when examining all the Shiny analyses published thus far, especially in oncology [12], the median values and HRs estimated from the reconstructed curves of each clinical trial prove to be nearly identical to those originally determined from “real” patients. Another strength is that this strategy of evidence analysis enables the execution of indirect comparisons for new therapeutic questions which are suggested by the recent literature, particularly when direct comparisons based on “real” trials are not available.
As regards the limitations of our analysis, the most obvious one has already been mentioned and is the indirect nature of our comparisons. In fact, these indirect retrospective comparisons do not take into account the contribution of intrinsic differences in the patient cohorts from different studies. In contrast, when randomization is applied, it is well known that these characteristics can be balanced between the groups under comparison.
In summary, regarding novel first-line treatments for unresectable mesothelioma, our article has presented the current state of the art, in which three treatments are characterized by a significant survival advantage. Although the magnitude of their incremental survival benefit is quite small (about 3 months), these new treatments are likely to replace the current standard of pemetrexed plus cisplatin. On the other hand, further research into other combination treatments that may provide a more clinically relevant survival advantage is warranted.
Author Contributions
Conceptualization, S.T., A.M., and V.C.; methodology, E.P. and A.M.; software, E.P. and S.V.; investigation, E.P. and S.V.; data curation, E.P. and S.V.; writing—original draft preparation, E.P. and S.V.; writing—review and editing, E.P., S.V., S.T., A.M., and V.C.; supervision, A.M. and V.C.
Funding
Not applicable
Availability of Data and Materials
The files saved in the format of the IPDfromKM software are available from the corresponding author upon request.
Acknowledgments
We thank the Scientific Committee of SIFACT (Italian Society of Hospital Pharmacists) for their contribution to designing some projects in which the IPDfromKM method is applied to anti-neoplastic treatments.
Ethical approval
Not applicable.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Schumann, S.O.; Kocher, G.; Minervini, F. Epidemiology, diagnosis and treatment of the malignant pleural mesothelioma, a narrative review of literature. J Thorac Dis. 2021, 13, 2510–2523. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Santos, C.; Dixe, M.D.A.; Sacadura-Leite, E.; Astoul, P.; Sousa-Uva, A. Asbestos Exposure and Malignant Pleural Mesothelioma: A Systematic Review of Literature. Port J Public Health 2023, 40, 188–202. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scherpereel, A.; Astoul, P.; Baas, P.; Berghmans, T.; Clayson, H.; de Vuyst, P.; Dienemann, H.; Galateau-Salle, F.; Hennequin, C.; Hillerdal, G.; Le Péchoux, C.; Mutti, L.; Pairon, J.C.; Stahel, R.; van Houtte, P.; van Meerbeeck, J.; Waller, D.; f Weder, W.; European Respiratory Society/European Society of Thoracic Surgeons Task Force. Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma. Eur Respir J. 2010, 35, 479–495. [Google Scholar] [CrossRef] [PubMed]
- Amin, W.; Linkov, F.; Landsittel, D.P.; Silverstein, J.C.; Bashara, W.; Gaudioso, C.; Feldman, M.D.; Pass, H.I.; Melamed, J.; Friedberg, J.S.; Becich, M.J. Factors influencing malignant mesothelioma survival: a retrospective review of the National Mesothelioma Virtual Bank cohort. F1000Res 2018, 7, 1184. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.D.; Bayes, H.K.; Bardgett, J.; Wedderburn, S.; Kerr, K.M.; Currie, G.P. Survival from malignant mesothelioma: where are we now? J R Coll Physicians Edinb. 2015, 45, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Marchevsky, A.M.; Khoor, A.; Walts, A.E.; Nicholson, A.G.; Zhang, Y.Z.; Roggli, V.; Carney, J.; Roden, A.C.; Tazelaar, H.D.; Larsen, B.T.; LeStang, N.; Chirieac, L.R.; Klebe, S.; Tsao, M.S.; De Perrot, M.; Pierre, A.; Hwang, D.M.; Hung, Y.P.; Mino-Kenudson, M.; Travis, W.; Sauter, J.; Beasley, M.B.; Galateau-Sallé, F. Localized malignant mesothelioma, an unusual and poorly characterized neoplasm of serosal origin: best current evidence from the literature and the International Mesothelioma Panel. Mod Pathol. 2020, 33, 281–296. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ricciardi, S.; Cardillo, G.; Zirafa, C.C.; Carleo, F.; Facciolo, F.; Fontanini, G.; Mutti, L.; Melfi, F. Surgery for malignant pleural mesothelioma: an international guidelines review. J Thorac Dis. 2018, 10 (Suppl. 2), S285–S292. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pezzicoli, G.; Rizzo, M.; Perrone, M.; Minei, S.; Mutti, L.; Porta, C. A Glimpse in the Future of Malignant Mesothelioma Treatment. Front Pharmacol 2021, 12, 809337. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, E.; Kijima, T.; Kuribayashi, K.; Negi, Y.; Kanemura, S.; Mikami, K.; Doi, H.; Kitajima, K.; Nakano, T. First-line chemotherapy with pemetrexed plus cisplatin for malignant peritoneal mesothelioma. Expert Rev Anticancer Ther. 2017, 17, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; O'Brien, M.E.; Stahel, R.A.; Nackaerts, K.; Baas, P.; Karthaus, M.; Eberhardt, W.; Paz-Ares, L.; Sundstrom, S.; Liu, Y.; Ripoche, V.; Blatter, J.; Visseren-Grul, C.M.; Manegold, C. Pemetrexed plus cisplatin or pemetrexed plus carboplatin for chemonaïve patients with malignant pleural mesothelioma: results of the International Expanded Access Program. J Thorac Oncol. 2008, 3, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Baas, P.; Faivre-Finn, C.; Girard, N.; Nicholson, A.G.; Nowak, A.K.; Opitz, I.; Scherpereel, A.; Reck, M.; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann Oncol. 2022, 33, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Scherpereel, A.; Cornelissen, R.; Oulkhouir, Y.; Greillier, L.; Kaplan, M.A.; et al. First-line nivolumab plus ipilimumab versus chemotherapy in patients with unresectable malignant pleural mesothelioma: 3-year outcomes from CheckMate-743. Ann Oncol. Epub ahead of print. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zalcman, G.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): a randomised, controlled, open-label, phase 3 trial. Lancet 2016, 387, 1405–1414. [Google Scholar] [CrossRef] [PubMed]
- Chu, Q.; Perrone, F.; Greillier, L.; Tu, W.; Piccirillo, M.C; Grosso, F.; et al. Pembrolizumab plus chemotherapy versus chemotherapy in untreated advanced pleural mesothelioma in Canada, Italy, and France: a phase 3, open-label, randomised controlled trial. Lancet 2023, 402, 2295–2306. [Google Scholar] [CrossRef]
- Ponce, S.; Cedrés, S.; Ricordel, C.; Isambert, N.; Viteri, S.; Herrera-Juarez, M.; et al. ONCOS-102 plus pemetrexed and platinum chemotherapy in malignant pleural mesothelioma: a randomized phase 2 study investigating clinical outcomes and the tumor microenvironment. J Immunother Cancer 2023, 11, e007552. [Google Scholar] [CrossRef]
- Tsao, A.S.; Miao, J.; Wistuba, II.; Vogelzang, N.J.; Heymach, J.V.; Fossella, F.V.; et al. Phase II Trial of Cediranib in Combination With Cisplatin and Pemetrexed in Chemotherapy-Naïve Patients With Unresectable Malignant Pleural Mesothelioma (SWOG S0905). J Clin Oncol. 2019, 37, 2537–2547. [Google Scholar] [CrossRef]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; et al. Phase III Study of Pemetrexed in Combination With Cisplatin Versus Cisplatin Alone in Patients With Malignant Pleural Mesothelioma. J Clin Oncol. 2003, 41, 2125–2133. [Google Scholar] [CrossRef]
- Nowak, A.K.; Lesterhuis, W.J.; Kok, P.S.; Brown, C.; Hughes, B.G.; Karikios, D.J.; et al. Durvalumab with first-line chemotherapy in previously untreated malignant pleural mesothelioma (DREAM): a multicentre, single-arm, phase 2 trial with a safety run-in. Lancet Oncol. 2020, 21, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Messori, A.; Trippoli, S. Current treatments for inoperable mesothelioma: indirect comparisons based on individual patient data reconstructed retrospectively from 4 trials. J Chemother. 2023, 35, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2021, 21, 111. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Messori, A. Synthetizing Published Evidence on Survival by Reconstruction of Patient-Level Data and Generation of a Multi-Trial Kaplan-Meier Curve. Cureus 2021, 13, e19422. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Messori, A. Reconstruction of individual-patient data from the analysis of Kaplan-Meier curves: this method is widely used in oncology and cardiology – List of 53 studies in oncology and 61 in cardiology (preprint). Open Science Framework 2024. url https://osf.io/zcf4r, accessed 10 November 2024. [Google Scholar] [CrossRef]
- Piragine, E.; Veneziano, S.; Trippoli, S.; Messori, A.; Calderone, V. Efficacy and Safety of Cardioband in Patients with Tricuspid Regurgitation: Systematic Review and Meta-Analysis of Single-Arm Trials and Observational Studies. J Clin Med. 2024, 13, 6393. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cashman, K.D.; Ritz, C. Individual participant data (IPD)-level meta-analysis of randomised controlled trials among dark-skinned populations to estimate the dietary requirement for vitamin D. Syst Rev. 2019, 8, 128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wach, J.; Vychopen, M.; Güresir, A.; Guranda, A.; Nestler, U.; Güresir, E. A Long-Term Comparative Analysis of Endovascular Coiling and Clipping for Ruptured Cerebral Aneurysms: An Individual Patient-Level Meta-Analysis Assessing Rerupture Rates. J Clin Med. 2024, 13, 1778. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zoupas, I.; Manaki, V.; Tasoudis, P.T.; Karela, N.R.; Avgerinos, D.V.; Mylonas, K.S. Totally Endoscopic Coronary Artery Bypass Graft: Systematic Review and Meta-Analysis of Reconstructed Patient-Level Data. Innovations (Phila) 2024, 19, 616–625. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rogula, B.; Lozano-Ortega, G.; Johnston, K.M. A Method for Reconstructing Individual Patient Data From Kaplan-Meier Survival Curves That Incorporate Marked Censoring Times. MDM Policy Pract. 2022, 7, 23814683221077643. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Mohe, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/, 2023.
- Correale, P.; Pentimalli, F.; Nardone, V.; Giordano, A.; Mutti, L. CONFIRM trial: what is the real efficacy of second-line immunotherapy in mesothelioma? Lancet Oncol. 2022, 23, e13. [Google Scholar] [CrossRef] [PubMed]
- Ossato, A.; Damuzzo, V.; Baldo, P.; Mengato, D.; Chiumente, M.; Messori, A. Immune checkpoint inhibitors as first line in advanced melanoma: Evaluating progression-free survival based on reconstructed individual patient data. Cancer Med. 2023, 12, 2155–2165. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flowchart of the literature search. The keyword used for the initial search in the two databases was “mesothelioma [title]” combined with “randomized control trial” as selection term.
Figure 1.
PRISMA flowchart of the literature search. The keyword used for the initial search in the two databases was “mesothelioma [title]” combined with “randomized control trial” as selection term.

Figure 2.
Kaplan-Meier survival curves obtained by reconstructing individual patient data from 6 patient cohorts published in the included trials. The 6 curves refer to the 5 control arms treated with pemetrexed+cisplatinum and one control arm treated with chemotherapy alone in the trial by Chou et al., 2023 [14] (see Table 1).Figure 3 describes the results of our main analysis, in which each of the 6 experimental arms was compared with the 6 control arms pooled together. The HRs for the comparisons of each of the experimental treatment vs. the 6 control arms pooled together are shown in Table 2.
Figure 2.
Kaplan-Meier survival curves obtained by reconstructing individual patient data from 6 patient cohorts published in the included trials. The 6 curves refer to the 5 control arms treated with pemetrexed+cisplatinum and one control arm treated with chemotherapy alone in the trial by Chou et al., 2023 [14] (see Table 1).Figure 3 describes the results of our main analysis, in which each of the 6 experimental arms was compared with the 6 control arms pooled together. The HRs for the comparisons of each of the experimental treatment vs. the 6 control arms pooled together are shown in Table 2.
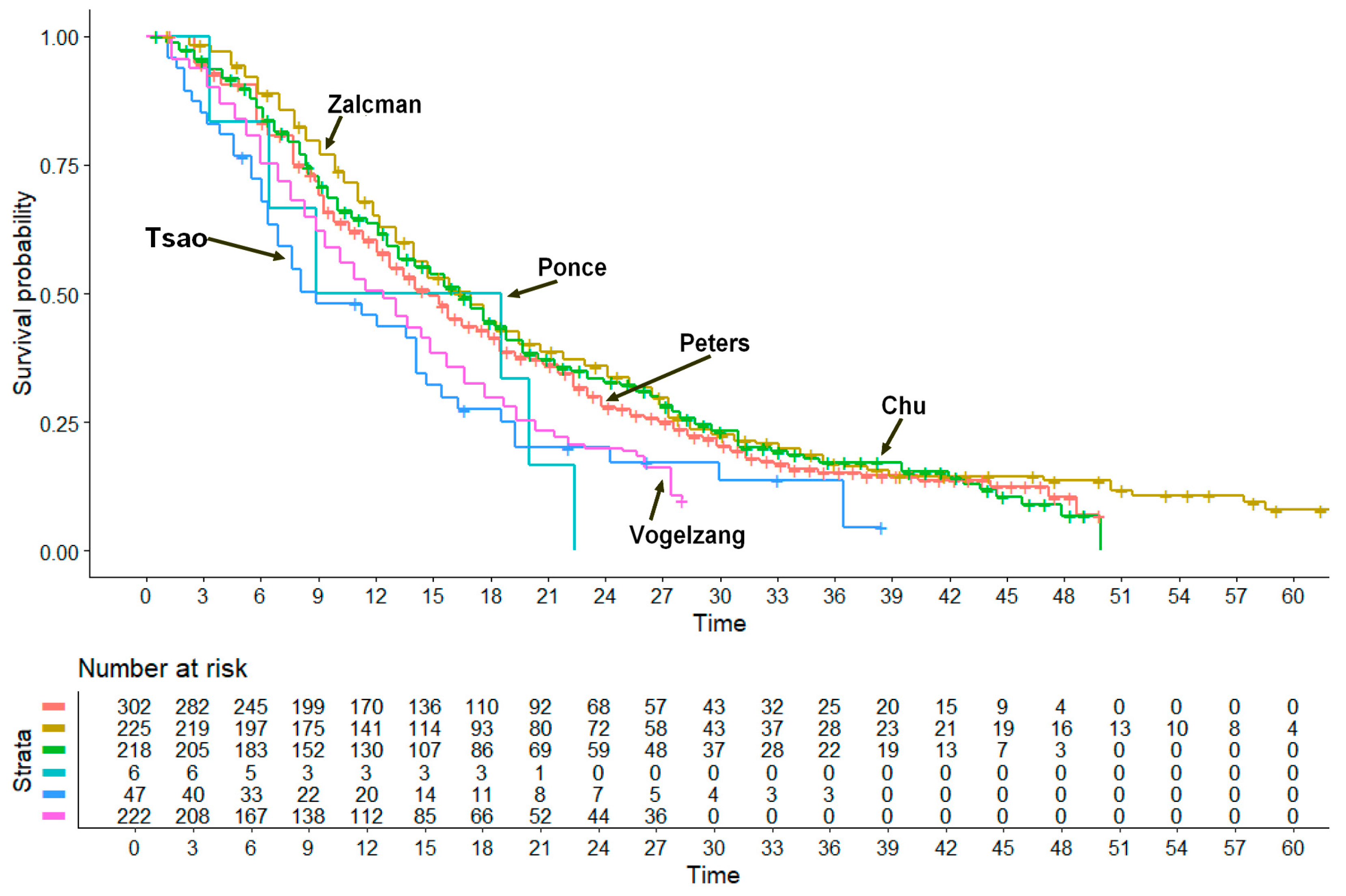
Figure 3.
Pooled Kaplan-Meier survival curves obtained by reconstructing individual patient data from 12 patient cohorts published in 6 trials. The curve for the 6 control arms pooled together (in orange) refers to 1,020 patients treated with pemetrexed + cisplatin in 5 phase III trials and with chemotherapy alone in the trial by Chu et al., 2023 [14]. The combination of ONCOS-102 with pem+pla did not show a significant improvement in OS (p>0.05). The other 5 curves refer to the 3 treatments (beva plus pem+cis, nivo+ipi, pem+chemo) that performed significantly better than standard of care (control) and to the 2 treatments (cisplatin alone or cedi+pem+plat) that performed significantly worse than the controls (see Table 2). Time is expressed in months. Trials are identified based on the first author. Abbreviations: beva, bevacizumab; cis, cisplatin; pem, pembrolizumab; plat, platinum agents; nivo, nivolumab; ipi, ipilimumab; cedi, cediranib.
Figure 3.
Pooled Kaplan-Meier survival curves obtained by reconstructing individual patient data from 12 patient cohorts published in 6 trials. The curve for the 6 control arms pooled together (in orange) refers to 1,020 patients treated with pemetrexed + cisplatin in 5 phase III trials and with chemotherapy alone in the trial by Chu et al., 2023 [14]. The combination of ONCOS-102 with pem+pla did not show a significant improvement in OS (p>0.05). The other 5 curves refer to the 3 treatments (beva plus pem+cis, nivo+ipi, pem+chemo) that performed significantly better than standard of care (control) and to the 2 treatments (cisplatin alone or cedi+pem+plat) that performed significantly worse than the controls (see Table 2). Time is expressed in months. Trials are identified based on the first author. Abbreviations: beva, bevacizumab; cis, cisplatin; pem, pembrolizumab; plat, platinum agents; nivo, nivolumab; ipi, ipilimumab; cedi, cediranib.
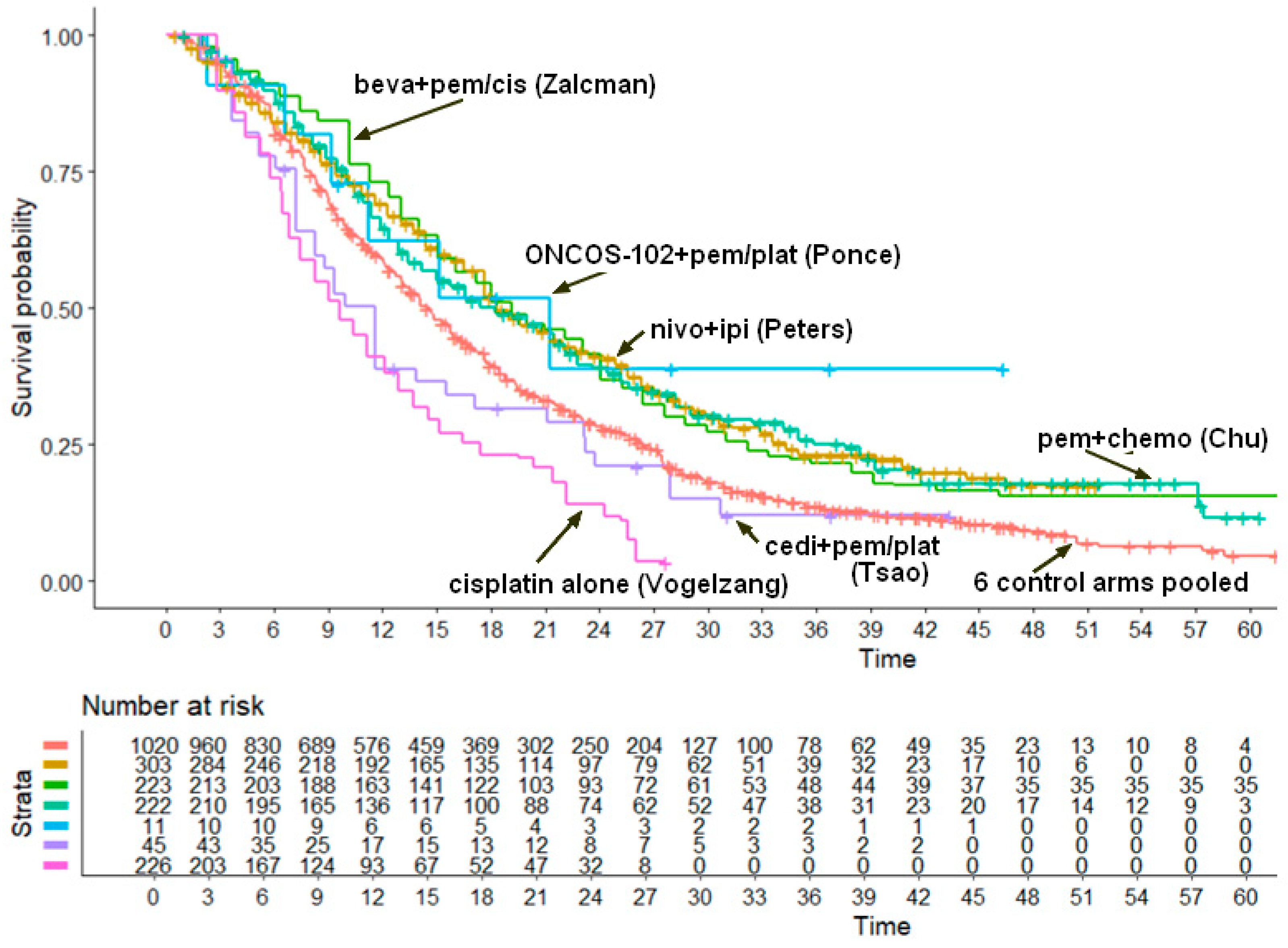

Table 1.
Unresectable pleural mesothelioma: information on first-line treatments reported in 6 RCT phase III trials. Endpoint: death for any cause.
Table 1.
Unresectable pleural mesothelioma: information on first-line treatments reported in 6 RCT phase III trials. Endpoint: death for any cause.
| Study (First author, year and reference) |
Study design | Histology (number of patients) | Intervention vs. control | Follow-up (months) |
HR (95% CI)* | Total number of events/patients (n/N) |
|
|---|---|---|---|---|---|---|---|
| Treatment group | Control group |
||||||
| Peters et al. (2022) [12] | RCT | Epithelioid, n=455; non-epithelioid, n=150 |
Nivolumab plus ipilimumab vs. pemetrexed plus cisplatin |
54 | HR=0.73 (95% CI, 0.61 to 0.87) § | 212/303 | 234/302 |
| Zalcman et al. (2016) [13] | RCT | Epithelioid, n=179 (80%); non-epithelioid, n=44 (20%) |
Bevacizumab plus pemetrexed plus cisplatin vs. pemetrexed plus cisplatin |
80 | HR=0.77 (95% CI, 0.62 to 0.95) |
164/223 | 178/225 |
| Chu et al. (2023) [14] | RCT | Epithelioid, n=349 (79%); other, n=91 (21%) |
Chemotherapy† plus pembrolizumab vs. chemotherapy† | 60 | HR=0·79 (95% CI, 0.64 to 0.98) |
167/222 | 175/218 |
| Ponce et al. (2023) [15] | RCT §§ | Epithelioid, n=24 (77.4%); other, n=7 (22.6%) |
ONCOS-102** plus pemetrexed plus cisplatin/carboplatin vs. pemetrexed plus cisplatin/carboplatin | 33 | NR | 6/11 | 6/6 |
| Tsao et al. (2019) [16] | RCT | Epithelioid, n=69 (75%); other, n=23 (25%) |
Cediranib plus pemetrexed+cisplatin (with maintenance with cediranib) vs. placebo plus pemetrexed+cisplatin (with maintenance with placebo) | 40 |
HR=0.88 (80% CI, 0.65 to 1.17) |
39/45 | 41/47 |
| Vogelzang et al. (2003) [17] | RCT | Epithelioid, n=306 (68.3%); other, n=142 (31.7%) |
Pemetrexed plus cisplatin vs. cisplatin alone | 30 | HR=0.77Median OS, 12.1 vs. 9.3 months | NR/226 | NR/222 |
| *These values of HR are those reported by the authors in the original article. †The chemotherapy in this trial consisted in most cases of pemtrexed plus platinum. ** ONCOS-102 is an oncolytic adenovirus expressing granulocyte-macrophage colony-stimulating factor. § The paper by Peters et al. [12] did not explicitly report the number of deaths in the two patient groups; this information was therefore estimated from the number of deaths from 0 to 39 months previously reported in the article published by Baas et al. in 2021 [19] (200 and 219 deaths in the two groups, respectively) and by counting the deaths from 40 to 54 months (12 and 15 in the two groups, respectively) according to individual downward steps appearing in the Kaplan-Meier graph published by Peters et al. in 2022 [12]. §§ While the paper by Ponce et al. [15] included 20 patients in the treatment group vs. 6 in the control group, our analysis included only the subgroup of chemo-naïve patients who were 11 in the treatment group and 6 in the control group. Abbreviations: CI, confidence interval; HR, hazard ratio; RCT, randomized controlled trial; OS, overall survival; NR, not reported. | |||||||
Table 2.
Values of HR estimated in our main analysis.
| First author, year and reference | Treatment given to the experimental arm | Treatment given to the control arm | HR (with 95% CI) estimated from reconstrcucted patients |
|---|---|---|---|
| Peters et al. (2022) [12] | Nivolumab plus ipilimumab |
Pemetrexed plus cisplatin | HR=0.7149 (95% CI, 0.6139 to 0.8326; p<0.001) |
| Zalcman et al. (2016) [13] | Bevacizumab plus pemetrexed plus cisplatin |
Pemetrexed plus cisplatin | HR=0.7063 (95% CI, 0.6020 to 0.8288; p<0.001) |
| Chu et al. (2023) [14] | Chemotherapy plus pembrolizumab | Chemotherapy | HR=0.7297 (95% CI, 0.6170 to 0.8631; p<0.001) |
| Ponce et al. (2023) [15] | ONCO-102 plus pemetrexed plus cisplatin or carboplatin | Pemetrexed plus cisplatin | HR=0.5853 (95% CI, 0.2622 to 1.3067; p= 0.191165) |
| Tsao et al. (2019) [16] | Cediranib pluspemetrexed+cisplatin (with maintenance with cediranib) | Pemetrexed plus cisplatin | HR=1.2196 (95% CI, 0.8774 to 1.6953; p= 0.237475) § |
| Vogelzang et al. (2003) [17] | Cisplatin alone | Pemetrexed plus cisplatin | HR=1.7657 (95% CI, 1.5192 to 2.0523; p<0.001) §§ |
|
§ The reciprocal of this HR is 0.8199 (95% CI, 0.5899 to 1.1397). §§ The reciprocal of this HR is 0.5663 (95% CI, 0.483 to 0.6582). Abbreviations: CI, confidence interval; HR, hazard ratio. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



