
Submitted:
31 December 2024
Posted:
02 January 2025
You are already at the latest version
Abstract
Background/Objectives: Over the past 50 years, developing new vaccines has been pivotal in responding to emerging and re-emerging diseases globally. However, despite substantial partner support, introducing new vaccines in sub-Saharan Africa remains challenging. This systematic review documents the barriers to new vaccine introduction and proposes evidence-based solutions. Methods: A comprehensive electronic search was conducted across five databases for articles published in English or French on the challenges of new vaccine introduction in sub-Saharan Africa. Three reviewers screened articles independently based on titles and abstracts, with full-text assessments conducted for inclusion. Data were analyzed thematically and synthesized narratively. Results: A total of 796 articles were retrieved from the five databases. Following the screening, 33 articles were finally retained and included in the review. These articles concerned the introduction of eight new vaccines (malaria vaccine, COVID-19 vaccine, HPV vaccine, Ebola vaccine, cholera vaccine, hepatitis B vaccine, rotavirus vaccine and typhoid vaccine). The analyses revealed coordination and financing challenges for six vaccines in 17 countries, acceptability challenges for five vaccines in ten countries, logistical challenges for two vaccines in six countries and quality service delivery challenges for three vaccines in 13 countries. Conclusions: Addressing the challenges of introducing new vaccines in sub-Saharan Africa requires targeted, evidence-based strategies. Prioritizing political commitment, innovative funding, public education, workforce development, and infrastructure improvements will strengthen immunization systems and enable timely vaccine delivery. Collaborative efforts and a focus on local context can advance equitable health outcomes, safeguard public health, and support global immunization goals.
Keywords:
new vaccines
; immunization challenges
; implementation barriers
; sub-saharan Africa
; health systems strengthening
1. Introduction
Vaccination remains one of the most effective strategies for preventing and controlling infectious diseases, offering protection against over 20 potentially life-threatening conditions worldwide [1]. Over the past five decades, vaccination has been estimated to save more than 130 million lives, underscoring its critical role in global health [2]. Recognizing its importance, the World Health Assembly has recommended the introduction of new vaccines into national immunization programs, particularly to address emerging diseases of public health concern [3].
Technical and financial assistance has been pivotal to vaccine introduction for resource-limited settings, such as sub-Saharan Africa. Between 2000 and 2022, Gavi, the Vaccine Alliance, invested over 11 billion US dollars to improve access to vaccines across the African continent [4].
Specific initiatives, including the COVAX mechanism funded by the European Union, have supported the deployment of COVID-19 vaccines in 15 African countries [5]. Similarly, the AMVIRA initiative has facilitated malaria vaccine introduction in 19 African nations [6]. Supporting new vaccine rollout also encompasses research, clinical trials [7], and pilot phase implementation [8]. These efforts have led to measurable successes. In Botswana, for instance, introducing COVID-19 vaccines resulted in more than 50% population coverage [9], while the rollout of cholera vaccines successfully curtailed transmission during an outbreak in Lusaka, Zambia [10]. Despite such achievements, significant challenges have been identified in implementing new vaccines in sub-Saharan Africa [11]. First, many new vaccines require stringent storage and transportation conditions to maintain efficacy, which poses difficulties in keeping the cold chain in remote or resource-constrained regions [12]. Second, affordability and funding sustainability challenges threaten coverage rates, particularly in countries with fragile health systems and economies [13].
Additionally, new vaccine introduction frequently encounters resistance fueled by misinformation, mistrust, or entrenched cultural beliefs [14]. Operational challenges further compound these issues. Evaluations of vaccine introductions have highlighted inadequacies in adverse event monitoring systems and limitations in data infrastructure, impeding the comprehensive assessment of vaccine safety and coverage [15]. Furthermore, new vaccines necessitate additional training for healthcare workers, exacerbating workloads in health systems already strained by human resource shortages [16]. Logistical barriers are another key challenge, particularly in reaching remote and marginalized populations [17]. To better understand these challenges, identify effective solutions, and guide the introduction of new vaccines in sub-Saharan Africa, we systematically reviewed published articles examining barriers to vaccine rollout and their associated mitigation strategies in the region.
2. Materials and Methods
This systematic review followed the PRISMA 2020 Statement guidelines to ensure rigor and transparency in reporting [18]. A comprehensive search strategy, guided by the PICO approach, was developed to identify relevant quantitative and qualitative studies. Five electronic databases—PubMed, Scopus, CINAHL, Web of Science, and Embase—were queried, yielding 796 articles. The search period spanned January 2019 to December 2024. The detailed PubMed search strategy is provided in Appendix A1 (see Table A1). The review protocol was prospectively registered on the PROSPERO platform (registration number: 532857; registered on April 6, 2024) to enhance methodological transparency and reduce the potential for bias.
2.1. Inclusion/Exclusion Criteria
We restricted our search to articles published in English or French between January 2019 and July 2024, focusing on the challenges of introducing new vaccines in sub-Saharan Africa. Articles were excluded if they were: (i) dissertations or theses, (ii) press publications, (iii) editorials, (iv) editorial reports, (v) supplementary articles, (vi) newsletters, or (vii) studies not accessible in the university library.
2.2. Selection of Studies
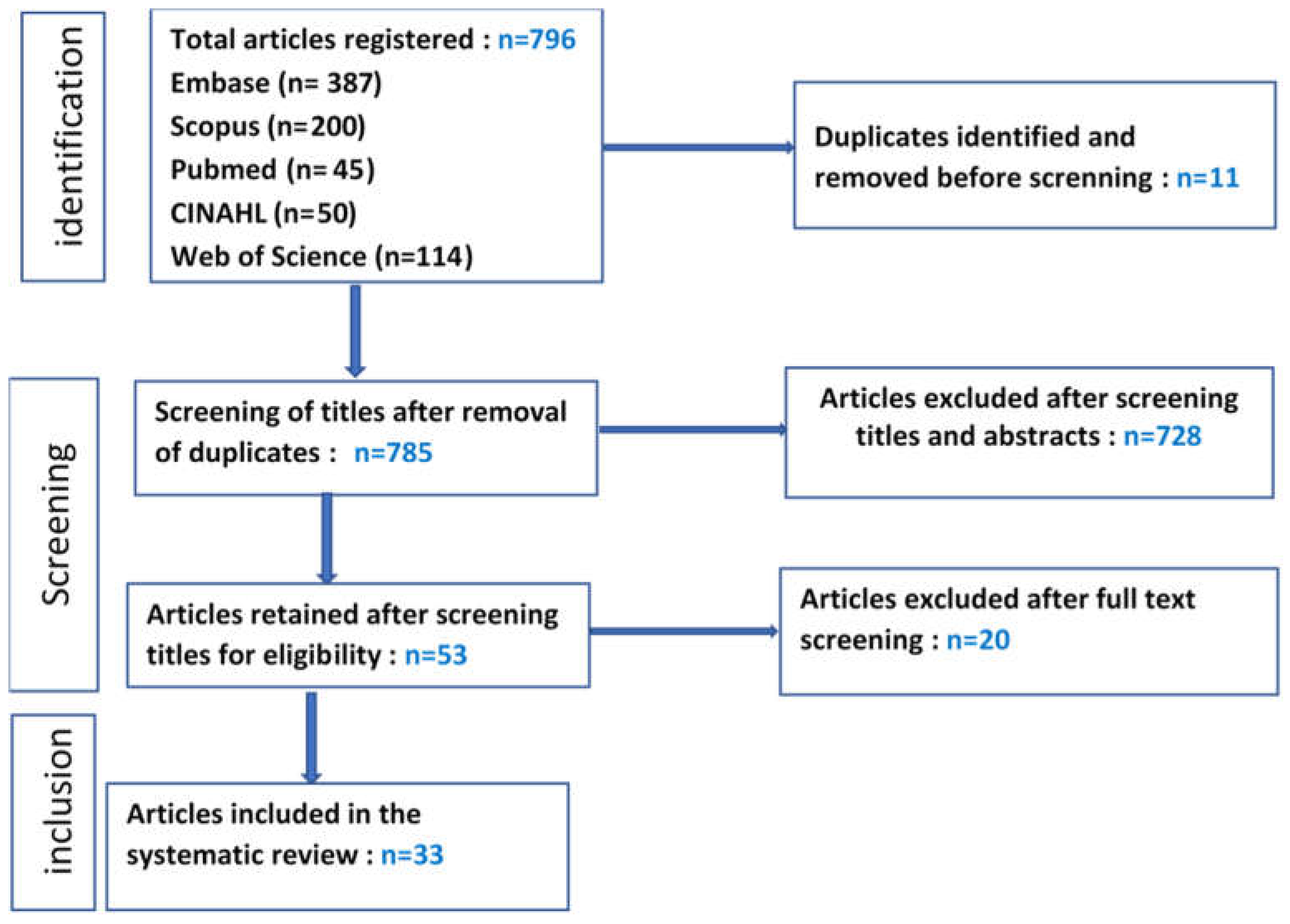
Articles retrieved were imported into Rayyan software for systematic screening. The selection process followed a stepwise approach based on our research question and inclusion criteria. Initially, articles were screened by title and abstract by the principal investigator and collaborators (SF, WSR, LTB, NMN). Of 796 articles identified, 11 duplicates and 732 articles not meeting the inclusion criteria were excluded. Fifty-three articles underwent full-text review, and 20 were excluded for the following reasons: insufficiently described or missing methodology (n=5), lack of specificity to new vaccines (n=4), not vaccine-related (n=1), not focused on African countries (n=2), prepublication articles not validated (n=2), results based on commentary rather than evidence (n=5), data dated beyond the eligibility window (n=1).
Disagreements on eligibility were resolved through consensus among reviewers, resulting in the inclusion of 33 studies. These comprised 26 quantitative studies, 4 qualitative studies, 2 mixed-methods studies, and 1 clinical trial.
2.3. Data Extraction and Analysis
Search results were uploaded to Rayyan for organization and deduplication. Initial selection by three reviewers (title and abstract) was followed by a full-text review based on the inclusion and exclusion criteria. A fourth reviewer resolved disagreements. Narrative synthesis was employed to thematically group challenges to introducing new vaccines. Extracted data included author and year of publication, study setting, participants and demographics, study design, vaccine type, study quality, main challenges reported
Challenges were categorized into four domains: acceptability, logistical challenges, service delivery, and coordination/financing.
2.4. Quality Assessment of Studies
The quality of the included studies was assessed using the Mixed Methods Appraisal Tool (MMAT), 2018 version. The MMAT was selected for its applicability to reviews involving qualitative, quantitative, and mixed-methods studies [19]. Each article was evaluated against five criteria, with a score of two points for "Yes" responses and zero for "No" or "Unknown" responses. Total scores were converted into percentages, ranging from 60% to 100%. Of the 33 studies, 12 scored 60%, 14 scored 80%, and 7 achieved 100%.
3. Results
The results of 33 articles concerned the introduction of eight (8) new vaccines. These vaccines include the malaria vaccine (MV), COVID-19 vaccine, human papillomavirus (HPV) vaccine, Ebola virus vaccine, cholera vaccine, hepatitis B vaccine (HBV), rotavirus vaccine and typhoid vaccine. The introduction of these vaccines has essentially revealed four types of challenges. These challenges are grouped into (1) acceptability, (2) immunization service logistics capacity, (3) quality service delivery, and (4) the challenges of coordinating and financing new vaccines.
Figure 1.
PRISMA flow diagram (PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only).
Figure 1.
PRISMA flow diagram (PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only).
3.1. Acceptability of New Vaccines
Challenges related to the acceptability of new vaccines were reported in 18 of the 33 studies and involved the introduction of five vaccines—against malaria, COVID-19, human papillomavirus (HPV), hepatitis B, and Ebola—in 10 African countries. Acceptability varied by vaccine type and country, ranging from strong adherence to marked reluctance (Table 1).
High vaccine acceptance rates (>90%) were noted for five vaccines across four countries. Key factors driving acceptance included perceived risks of target diseases, such as the Ebola virus in the Democratic Republic of Congo (DRC) [20], the severity of COVID-19 infection in Nigeria [21], the perceived sensitivity of hepatitis B (p<0.05) in Ghana [22], experiential attitudes toward HPV vaccination (p<0.01) in Nigeria [23] and population confidence in malaria vaccine in Sierra Leone [24].
Conversely, vaccine hesitancy emerged in at least eight countries. For COVID-19 vaccines, reluctance was driven by fear of adverse events following immunization (AEFI) in Ethiopia [25] and the DRC [26], lack of information in Senegal [27] and in Sudan [28], low awareness of vaccination in Ethiopia [29], concerns about safety in the DRC [30], religious considerations in Ghana [31] and perceived susceptibility (p<0.001) in Nigeria [32].
3.2. Logistic Challenges
Logistical barriers were reported in seven studies concerning introduction of malaria and HPV vaccines in six countries (Table 2). Challenges included vaccine availability, cold chain infrastructure gaps, and district and facility-level logistics shortfalls.
For the HPV vaccine, specific barriers were global vaccine shortages, delayed rollout in Senegal [34], vaccine unavailability at designated sites in Nigeria [37] and in public programs in South Africa [35], and inadequate cold chain storage in Uganda [36].
3.3. Challenges to Quality Service Delivery
Five studies identified immunization service delivery challenges for hepatitis B, malaria, and HPV vaccines across 13 countries (Table 3). Key issues included inadequate vaccination delivery strategies and healthcare workforce barriers.
For hepatitis B vaccination, inadequate provision of services contributed to a 32% non-vaccination rate across 12 countries [41]. Long waiting times and overburdened staff during malaria vaccine delivery were similarly noted in Ghana [42]. Furthermore, facility managers criticized extended malaria vaccination schedules for contributing to dropouts [40]. Ineffective HPV vaccine delivery strategies included difficulty tracking school-aged children transferred to other districts in Senegal [34] and in Uganda [36]. Challenges were exacerbated by workforce capacity deficits, particularly in Ghana for malaria vaccines [40] and in Senegal for HPV vaccines [34]. Recommendations included phased program scaling [39], stakeholder engagement [34], comprehensive training of healthcare providers [36], and sharing best practices to improve service delivery [40].
3.4. Challenges Associated with Coordinating and Financing New Vaccines
Fourteen studies reported coordination and financing challenges related to six vaccines—malaria, influenza, HPV, rotavirus, typhoid, and hepatitis B—across 17 African countries (Table 4).
Coordination issues included pilot site selection, eligibility criteria for target populations, and implementation planning. In Ghana, the exclusion of districts during malaria vaccine piloting led to dissatisfaction among health officials [40].
Implementation delays were similarly noted. In Senegal, the HPV vaccine rollout was postponed due to vaccine unavailability, insufficient funding, and an incomplete communication plan [43]. Financial resource mobilization challenges impacted the malaria vaccine rollout in Ghana [42].
Financing barriers centered on the high costs of vaccine introduction relative to WHO-recommended affordability thresholds, as observed with influenza vaccines in Kenya [44] and typhoid vaccines in Malawi [45].
Partner co-financing mitigated some costs, enabling HPV introduction in Senegal [46] and Zimbabwe [47] and rotavirus vaccine deployment in Niger [48]. However, cost variations persisted and were linked to differing proportions of co-financing [35].
Several countries adopted alternative strategies. Niger prioritized lower-cost rotavirus vaccines [48], Mozambique reduced HPV vaccine dosing regimens [49], and Malawi cut ancillary program costs [45]. Without subsidies, financial burdens fell to health services and vaccine beneficiaries, as documented with hepatitis B vaccines in 12 countries [41], HPV programs in Nigeria [35], HPV vaccine in Nigeria [37], and in Sierra Leone, where only 56% of respondents were willing to pay $0.69 for the HPV vaccine [38].
This review provides critical insights into the challenges of introducing new vaccines within sub-Saharan Africa’s national immunization programs. By categorizing these challenges into acceptability, logistical capacity, service delivery quality, and coordination and financing, the study identifies cross-cutting barriers that are context-dependent and vaccine-specific. These findings are pivotal for informing policymakers, program managers, and stakeholders to optimize vaccine introduction strategies and strengthen regional health interventions.
Our analysis underscores that vaccine acceptability is variable and context-specific, influenced by vaccine type, perceived risk, and sociocultural factors. High acceptance levels (>90%) were documented for Ebola and hepatitis B vaccines among healthcare workers and target populations in the DRC [20] and Ghana [50], respectively. This acceptance included heightened disease risk perceptions, community trust, and provider advocacy.
Conversely, vaccine hesitancy remains a significant barrier, particularly for COVID-19 and HPV vaccines. For COVID-19 vaccines, fear of adverse events following immunization (AEFI), limited information, and religious concerns contributed to reluctance in Ethiopia [51] and Senegal [27]. Similarly, parental education levels and infodemics drove HPV vaccine hesitancy in Uganda [52] and Senegal [34]. These findings mirror those from Latin America, where vaccine acceptability varied widely by country and target group: 95% among healthcare workers in Mexico but as low as 40% in Peru [53]. Such disparities emphasize the critical role of tailored communication strategies, trust-building interventions, and community engagement to mitigate misinformation and address population-specific barriers. Lessons from successful campaigns—such as Ebola vaccination in the DRC—highlight the importance of integrating risk communication and leveraging trusted local actors.
Logistical challenges emerged as central barriers, particularly the limitations of cold chain infrastructure and vaccine supply shortages. Insufficient cold chain capacity hampered HPV vaccine delivery in Uganda [52] and malaria vaccination in Ghana [55], consistent with observations from Latin America, where gaps in cold chain availability similarly undermined vaccine introduction efforts [56]. In addition to infrastructure gaps, recurrent vaccine shortages, notably for HPV [43] and malaria vaccines [38], disrupted program continuity and undermined population confidence. Comparable vaccine shortages in Asia and the Pacific highlight the global nature of organizational and funding constraints for vaccine distribution [57]. Cold chain strengthening and innovative logistical solutions, such as mobile storage units, must be prioritized to ensure vaccine potency and access in remote settings. Global partnerships, including Gavi and WHO support, remain critical to addressing supply disruptions and bridging logistical inequities across resource-limited contexts.
Shortcomings in immunization service delivery were widespread and included insufficient workforce capacity, poor customer care, and organizational inefficiencies. Long waiting times and provider negligence were reported during malaria vaccine delivery in Ghana [42] and hepatitis B vaccination across 12 countries [41]. Such findings align with studies on COVID-19 vaccination services in Egypt, where site overcrowding and disorganization were predominant challenges [54].
These barriers underscore the need to streamline service delivery processes, optimize workforce distribution, and strengthen training programs. Strategies to address inefficiencies include phased vaccine rollout approaches, stakeholder involvement, and monitoring frameworks to evaluate provider performance and client satisfaction.
Financing challenges remain a cornerstone barrier to vaccine introduction across Africa, where vaccine and operational costs often surpass available health budgets. For instance, the typhoid vaccine in Malawi [45] and influenza vaccines in Kenya [44] exceeded WHO-defined cost thresholds for health interventions. Unlike resource-constrained regions in Asia, such as Afghanistan, where HPV vaccination costs represented just 0.7% of GDP due to streamlined target cohorts [58], African countries contend with broader target populations and weaker financing mechanisms.
Co-financing agreements, such as Gavi-supported HPV vaccine programs in Senegal [46] and Zimbabwe [47], offer critical opportunities to offset costs. However, sustained government commitments, innovative financing strategies, and cost-effective program adaptations (e.g., reducing HPV vaccine doses [49]) are imperative to overcome long-term financial barriers and ensure equitable vaccine access.
This review is a comprehensive repository of challenges encountered in recent vaccine introductions across the African region. It highlights opportunities for strengthening health systems, aligning resources, and tailoring program interventions to overcome contextual barriers.
By addressing these interrelated challenges, countries can improve the efficiency, equity, and success of future vaccine introduction efforts, particularly in emerging diseases and global immunization goals.
Strengths and Limitations
This review offers a critical overview of vaccine introduction challenges across diverse African settings, providing practical insights to guide immunization program planning and execution. However, limitations must be acknowledged. First, while significant data were synthesized, insufficient evidence on political commitment—an essential determinant of vaccine program success—was available. Second, the exclusion of meta-analytical methods limited the quantitative exploration of results. Finally, contextual heterogeneity across countries warrants cautious interpretation when comparing findings. Variations in socio-economic, cultural, and health system factors may differentially influence vaccine-related challenges and solutions.
5. Conclusions
The successful introduction of new vaccines in sub-Saharan Africa is crucial for advancing immunization goals, but key challenges remain, including issues with coordination, financing, vaccine acceptability, service delivery quality, and logistical constraints. Overcoming these barriers requires evidence-driven approaches tailored to local contexts. Addressing financing gaps through political commitment, innovative funding, and global partnerships is essential, as is enhancing public awareness to combat misinformation and build vaccine trust. Investing in healthcare workforce capacity and strengthening cold and supply chain systems is also critical. By implementing these measures, resilient immunization systems can be built, enabling the introduction of new vaccines, reinforcing health systems, and ensuring equitable healthcare outcomes across Africa.
Author Contributions
PN supervise the study. SF drafted the manuscript and SF and developed the search strategy. SF, BAF and RWS selected the studies, and all auteurs extracted the data. SF, MNN, LBT and GMK synthesized the results. WSR, BAF, BS, MNN, SF, GMK, OS extensively reviewed the manuscript. All the authors read, provided feedback, and approved the final version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable.”.
Data Availability Statement
The original contributions presented in the study are included in this article further inquiries can be directed to the corresponding author.
Acknowledgments
We acknowledge all those who offered guidance and technical support during the writing of the manuscript, particularly Dr Patrice Ngangue.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
The following abbreviations are used in this manuscript:
| AMVIRA | Accelerating Malaria Vaccine Introduction and Rollout in Africa |
| COVAX | COVID-19 Vaccines Global Access |
| FVC | fully vaccination completed |
| HBV | Hepatitis B vaccine |
| HF | Healthcare facility |
| HPV | Human Papillomavirus |
| PRISMA | Preferred reporting items for systematic reviews and meta-analysis |
| MMAT | Mixed Methods Assessment Tool |
Appendix A
Appendix A.1

Table A1.
PubMed Search Strategy.
| Search terms | Key-words | |
|---|---|---|
| Health workers, physicians, nurses, Decision makers, drug industry, | "Decision-makers “OR "Health Personnel"[Mesh] OR "Community Health Workers"[Mesh] OR "Allied Health Personnel"[Mesh] OR "Physicians"[Mesh] OR "nurses"[Mesh] OR "Societies, Pharmaceutical"[Mesh] OR "Drug Industry"[Mesh] OR "Drug and Narcotic Control"[Mesh] | |
| New vaccines | "New vaccines" OR "Ebola Vaccines"[Mesh] OR "West Nile Virus Vaccines"[Mesh] OR "AIDS Vaccines"[Mesh] OR "Cholera Vaccines"[Mesh] OR "Herpes Simplex Virus Vaccines"[Mesh] OR "Dengue Vaccines"[Mesh] OR "Cancer Vaccines"[Mesh] OR "Papillomavirus Vaccines"[Mesh] OR "Vaccines"[Mesh] OR "Rubella Vaccine"[Mesh] OR "Malaria Vaccines"[Mesh] OR "ChAdOx1 nCoV-19"[Mesh] OR "Poliovirus Vaccine, Inactivated"[Mesh] | |
| Challenges, Costs, impact | "Risk-Taking"[Mesh] OR "Challenge" OR "Health Impact Assessment"[Mesh] OR "Cost-Benefit Analysis"[Mesh] OR "Costs and Cost Analysis"[Mesh] OR "Costs" | |
| Low-and-middle income countries | "Angola" OR "Benin" OR "Botswana" OR "Burkina Faso" OR "Burundi" OR "Cabo Verde" OR "Cameroon" OR "Central African Republic" OR "Chad" OR "Comoros" OR "Congo" OR "Democratic Republic of Congo" OR "Cote d'Ivoire" OR "Equatorial Guinea" OR "Eritrea" OR "Eswatini" OR "Swaziland" OR "Ethiopia" OR "Gabon" OR "Gambia" OR "Ghana" OR "Guinea" OR "Guinea-Bissau" OR "Kenya" OR "Lesotho" OR "Liberia" OR "Madagascar" OR "Malawi" OR "Mali " OR "Mauritania" OR "Mauritius" OR "Mozambique" OR "Namibia" OR "Niger" OR "Nigeria" OR "Rwanda" OR "Sao Tome and Principe" OR "Senegal" OR "Seychelles" OR "Sierra Leone" OR "Somalia" OR "South Africa" OR "South Sudan" OR "Sudan" OR "Tanzania" OR "Togo" OR "Uganda" OR "Zambia" OR "Zimbabwe" | |
References
- OMS, « Vaccins et vaccination », 2024.
- UNICEF, « Les 10 chiffres clés de la vaccination des enfants dans le monde | UNICEF France », 2024.
- OMS, « World-health-assembly-resolution.pdf ». 2012.
- CDC Africa, « Africa CDC’s engage a soutenir la reconstitution des fonds Gavi à Paris – Africa CDC », 2024.
- OMS/AFRO, « Financement de l’Union européenne renforce la vaccination contre la COVID-19 en Afrique ». 2022.
- UNICEF, « La Sierra Leone introduit un vaccin contre le paludisme », 2024.
- Grantz et al, « Factors influencing participation in an Ebola vaccine trial among front-line workers in Guinea », Vaccine, vol. 37, no 48, p. 7165-7170, nov. 2019. [CrossRef]
- Baral et al, « Costs of continuing RTS,S/ASO1E malaria vaccination in the three malaria vaccine pilot implementation countries », PLOS ONE, vol. 16, no 1, p. e0244995, janv. 2021. [CrossRef]
- Hally, « Increasing COVID-19 vaccine uptake in Botswana through community outreach and door-to-door vaccination ». 2023.
- Poncin et al, « Implementation research: reactive mass vaccination with single-dose oral cholera vaccine, Zambia », Bull. World Health Organ., vol. 96, no 2, p. 86-93, févr. 2018. [CrossRef]
- USAID, « Goulots d’étranglement et avancées: », 2016.
- Bishai et al, « Defining the challenges in vaccine logistics and cold chain in developing countries. .pdf ». 2006.
- S. Ozawa et M. L. Stack, « Public trust and vaccine acceptance-international perspectives », Hum. Vaccines Immunother., vol. 9, no 8, p. 1774-1778, août 2013. [CrossRef]
- Larson et al, « Vaccine hesitancy and vaccine demand: Insights from low- and middle-income countries. Human Vaccines & Immunotherapeutics.pdf ». 2016.
- WHO, « Strengthening surveillance and evaluation frameworks for vaccine safety ». 2020.
- Lydon et al, « Health workforce challenges in the vaccine introduction era. Vaccine. » 2016.
- Bruni et al, « Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis », Lancet Glob. Health, vol. 4, no 7, p. e453-e463, juill. 2016. [CrossRef]
- Page, « The PRISMA 2020 statement: an updated guideline for reporting systematic reviews », BMJ, p. n71, mars 2021. [CrossRef]
- Hong et al, « Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study », J. Clin. Epidemiol., vol. 111, p. 49-59.e1, juill. 2019. [CrossRef]
- Doshi et al, « Ebola vaccine uptake and attitudes among healthcare workers in North Kivu, Democratic Republic of Congo, 2021 », Front. Public Health, vol. 11, p. 1080700, juill. 2023. [CrossRef]
- A. S. Azees et al., « Vaccine Safety: Assessing the Prevalence and Severity of Adverse Events Following COVID-19 Vaccination amongst Healthcare Workers in Tertiary Health Facilities in Nigeria », Niger. Postgrad. Med. J., vol. 31, no 1, p. 1-7, janv. 2024. [CrossRef]
- S. Tagbor, L. A. Ohene, C. A. Adjei, et J. Kyei, « Perceptions and Cues to Action as Predictors of Nurses’ Vaccination Intentions at Two Primary Health Care Facilities in Ghana », Am. J. Trop. Med. Hyg., vol. 108, no 2, p. 433-440, févr. 2023. [CrossRef]
- Balogun et al, « Parental intention to vaccinate adolescents with HPV vaccine in selected communities in Ibadan, Southwest Nigeria: an application of Integrated Behavioral Model », Hum. Vaccines Immunother., vol. 18, no 5, p. 2069959, nov. 2022. [CrossRef]
- K. D. McCoy et al., « Are malaria transmission-blocking vaccines acceptable to high burden communities? Results from a mixed methods study in Bo, Sierra Leone », Malar. J., vol. 20, no 1, p. 183, avr. 2021. [CrossRef]
- Ayele et al, « Acceptance of COVID-19 vaccine and associated factors among health professionals working in Hospitals of South Gondar Zone, Northwest Ethiopia », Hum. Vaccines Immunother., vol. 17, no 12, p. 4925-4933, mars 2024. [CrossRef]
- Garbern et al, « COVID-19 Vaccine Perceptions among Ebola-Affected Communities in North Kivu, Democratic Republic of Congo, 2021 », Vaccines, vol. 11, no 5, p. 973, mai 2023. [CrossRef]
- Ridde et al, « Participating in a vaccine trial for COVID-19 in Senegal: trust and information », Hum. Vaccines Immunother., vol. 17, no 11, p. 3907-3912, nov. 2021. [CrossRef]
- Elbadawi et al, « Beliefs and barriers of COVID-19 vaccination hesitancy among Sudanese healthcare workers in Sudan: A cross-sectional study », Hum. Vaccines Immunother., vol. 18, no 6, p. 2132082, nov. 2022. [CrossRef]
- Niguse et al, « Assessment of COVID-19 vaccine take-up and its predictors among healthcare professionals in public hospitals, Addis Ababa, Ethiopia: Facility-based cross-sectional study », Hum. Vaccines Immunother., vol. 19, no 1, p. 2171181, janv. 2023. [CrossRef]
- Barrall et al, « Hesitancy to receive the novel coronavirus vaccine and potential influences on vaccination among a cohort of healthcare workers in the Democratic Republic of the Congo », Vaccine, vol. 40, no 34, p. 4998-5009, août 2022. [CrossRef]
- Addo et al, « Guarding against COVID-19 vaccine hesitance in Ghana: analytic view of personal health engagement and vaccine related attitude », Hum. Vaccines Immunother., vol. 17, no 12, p. 5063-5068, mars 2024. [CrossRef]
- Chinawa et al, « Maternal level of awareness and predictors of willingness to vaccinate children against COVID 19; A multi-center study », Hum. Vaccines Immunother., vol. 17, no 11, p. 3982-3988, nov. 2021. [CrossRef]
- Chekol et al, « Evaluation and comparison of post-vaccination adverse effects among Janssen and Oxford-AstraZeneca vaccinated adult individuals in Debre Tabor Town: A cross- sectional survey in Northwest Ethiopia », Hum. Vaccines Immunother., vol. 18, no 6, p. 2104059, nov. 2022. [CrossRef]
- Casey et al, « National introduction of HPV vaccination in Senegal—Successes, challenges, and lessons learned », Vaccine, vol. 40, p. A10-A16, mars 2022. [CrossRef]
- Islam et al, « Health Care Provider Perceptions of Facilitators and Barriers to Human Papillomavirus Vaccination Delivery in Five Countries », Sex. Transm. Dis., vol. 48, no 8, p. 557-564, août 2021. [CrossRef]
- Rujumba et al, « Why don’t adolescent girls in a rural Uganda district initiate or complete routine 2-dose HPV vaccine series: Perspectives of adolescent girls, their caregivers, healthcare workers, community health workers and teachers », PLOS ONE, vol. 16, no 6, p. e0253735, juin 2021. [CrossRef]
- Nguyen et al, « Identifying Perceived Barriers to Human Papillomavirus Vaccination as a Preventative Strategy for Cervical Cancer in Nigeria », Ann. Glob. Health, vol. 86, no 1, p. 118, sept. 2020. [CrossRef]
- McCoy et al, « Are malaria transmission-blocking vaccines acceptable to high burden communities? Results from a mixed methods study in Bo, Sierra Leone », Malar. J., vol. 20, no 1, p. 183, avr. 2021. [CrossRef]
- Adjei et al, « Post introduction evaluation of the malaria vaccine implementation programme in Ghana, 2021 », BMC Public Health, vol. 23, no 1, p. 586, mars 2023. [CrossRef]
- Grant et al, « Challenges and lessons learned during the planning and early implementation of the RTS,S/AS01E malaria vaccine in three regions of Ghana: a qualitative study », Malar. J., vol. 21, no 1, p. 147, déc. 2022. [CrossRef]
- Shah et al, « Hepatitis B Awareness and Vaccination Patterns among Healthcare Workers in Africa », Am. J. Trop. Med. Hyg., vol. 103, no 6, p. 2460-2468, déc. 2020. [CrossRef]
- Adjei et al, « Post introduction evaluation of the malaria vaccine implementation programme in Ghana, 2021 », BMC Public Health, vol. 23, no 1, p. 586, mars 2023. [CrossRef]
- Casey et al, « National introduction of HPV vaccination in Senegal—Successes, challenges, and lessons learned », Vaccine, vol. 40, p. A10-A16, mars 2022. [CrossRef]
- Waterlow et al, « Potential health and economic impact of paediatric vaccination using next-generation influenza vaccines in Kenya: a modelling study », BMC Med., vol. 21, no 1, p. 106, mars 2023. [CrossRef]
- Debellut et al, « Projecting the cost of introducing typhoid conjugate vaccine (TCV) in the national immunization program in Malawi using a standardized costing framework », Vaccine, vol. 40, no 12, p. 1741-1746, mars 2022. [CrossRef]
- Brennan et al, « Cost of human papillomavirus vaccine delivery in a single-age cohort, routine-based vaccination program in Senegal », Vaccine, vol. 40, p. A77-A84, mars 2022. [CrossRef]
- Hidle et al, « Cost of human papillomavirus vaccine delivery at district and health facility levels in Zimbabwe: A school-based vaccination program targeting multiple cohorts », Vaccine, vol. 40, p. A67-A76, mars 2022. [CrossRef]
- Debellut et al, « Impact and cost-effectiveness of rotavirus vaccination in Niger: a modelling study evaluating alternative rotavirus vaccines », BMJ Open, vol. 12, no 10, p. e061673, oct. 2022. [CrossRef]
- Alonso et al, « Costs associated with delivering HPV vaccination in the context of the first year demonstration programme in southern Mozambique », BMC Public Health, vol. 19, no 1, p. 1031, déc. 2019. [CrossRef]
- Tagbor et al, « Perceptions and Cues to Action as Predictors of Nurses’ Vaccination Intentions at Two Primary Health Care Facilities in Ghana », Am. J. Trop. Med. Hyg., vol. 108, no 2, p. 433-440, févr. 2023. [CrossRef]
- Ayele et al, « Acceptance of COVID-19 vaccine and associated factors among health professionals working in Hospitals of South Gondar Zone, Northwest Ethiopia », Hum. Vaccines Immunother., vol. 17, no 12, p. 4925-4933, mars 2024. [CrossRef]
- Rujumba et al, « Why don’t adolescent girls in a rural Uganda district initiate or complete routine 2-dose HPV vaccine series: Perspectives of adolescent girls, their caregivers, healthcare workers, community health workers and teachers », PLOS ONE, vol. 16, no 6, p. e0253735, juin 2021. [CrossRef]
- Alarcón-Braga et al, « Acceptance towards COVID-19 vaccination in Latin America and the Caribbean: A systematic review and meta-analysis », Travel Med. Infect. Dis., vol. 49, p. 102369, sept. 2022. [CrossRef]
- Kandeel et al, « COVID-19 vaccination coverage in Egypt: a large-scale national survey – to help achieving vaccination target, March-May, 2022 », BMC Public Health, vol. 23, no 1, p. 397, févr. 2023. [CrossRef]
- Grant et al, « Challenges and lessons learned during the planning and early implementation of the RTS,S/AS01E malaria vaccine in three regions of Ghana: a qualitative study », Malar. J., vol. 21, no 1, p. 147, déc. 2022. [CrossRef]
- Guzman-Holst et al, « Barriers to vaccination in Latin America: A systematic literature review », Vaccine, vol. 38, no 3, p. 470-481, janv. 2020. [CrossRef]
- Ong et al, « Towards elimination of cervical cancer – human papillomavirus (HPV) vaccination and cervical cancer screening in Asian National Cancer Centers Alliance (ANCCA) member countries », Lancet Reg. Health - West. Pac., vol. 39, p. 100860, oct. 2023. [CrossRef]
- Anwari et al, « Potential health impact and cost-effectiveness of bivalent human papillomavirus (HPV) vaccination in Afghanistan », Vaccine, vol. 38, no 6, p. 1352-1362, févr. 2020. [CrossRef]
Table 1.
Results on the acceptability of new vaccines.
| Author, year | Country | Vaccine | Participants | Acceptability |
|---|---|---|---|---|
| Articles describing high acceptability of new vaccines (adherence >80%) | ||||
| Doshi et al, 2023 | DRC | Ebola vaccine | 588 healthcare professionals | 99.0% self-reported vaccine acceptance and 70.2% acceptance of the first offer. |
| Tagbor et al., 2023 | Ghana | Hepatitis B vaccine (HBV) | 190 Nurses | 98.8% were willing to receive the vaccine, |
| Balogun et al, 2022 | Nigeria | HPV vaccine | 678 Parents of teenagers | 96.8% of parents intended to have their teenagers vaccinated with HPV |
| McCoy et al, 2021 | Sierra Leone | Malaria vaccine | 615 inhabitants of Bo | 95% of participants were ready to receive the vaccine, and 99% were ready to have their children vaccinated |
| Azees et al., 2024 | Nigeria | COVID-19 vaccine | 2130 Health workers | 92.8% of agents recommend the vaccine despite MAPI |
| Elbadawi et al, 2022 | Sudan | COVID-19 vaccine | 930 Healthcare professionals | 88.0% of participants agreed to be vaccinated. |
| Articles describing reluctance and refusal towards new vaccines | ||||
| Chekol et al, 2022 | Ethiopia | HPV vaccine | 366 Schoolgirls | 75.7% believe they will take the vaccine if they feel at risk. |
| Niguse et al., 2023 | Ethiopia | COVID-19 vaccine | 403 Healthcare professionals | 71% of participants vaccinated against COVID-19 at least once |
| Grantz et al., 2019 | Guinea | Ebola vaccine | 110 front-line health workers | 67% agreed to take part in the vaccine trial |
| Barrall et al., 2022 | DRC | COVID-19 vaccine | 588 Healthcare professionals | 52.0% reluctant to vaccinate |
| Ayele et al, 2024 | Ethiopia | COVID-19 vaccine | 422 Healthcare professionals | 45.3% of healthcare professionals accepted the COVID-19 vaccine. |
| Islam et al, 2021 | South Africa and 4 countries | HPV vaccine | 151 Vaccine suppliers | 13% of service providers report non-completion of doses (2nd and 3rd) |
| Garbern et al, 2023 | DRC | COVID-19 vaccine | 631 Healthcare professionals and community members | 26.5% of healthcare professionals are reluctant to vaccinate, and 32.4% refuse outright |
| Ridde et al, 2021 | Senegal | COVID-19 vaccine | 607 Adults | 18.4% do not wish to be vaccinated, 41.5% have not been vaccinated, and 25% have been vaccinated incorrectly |
| Addo et al., 2024 | Ghana | COVID-19 vaccine | 1768 Ghanaian adults | 12.7% say their religion does not allow vaccination |
| Chinawa et al, 2021 | Nigeria | COVID-19 vaccine | 577 Mothers and children | 6.9% of mothers intend to receive the vaccine |
| Casey et al, 2022 | Senegal | HPV vaccine | 10 of stakeholders | Reluctance and refusal to take the HPV vaccine, according to key informants. |
| Rujumba et al, 2021 | Uganda | HPV vaccine | 40 Health workers, teachers, girls' parents | Reluctance on the part of some parents (according to teachers) |
Table 2.
results of studies on the logistical challenges of new vaccines.
| Author, Year | Country | Vaccine | Targets | Logistics description |
|---|---|---|---|---|
| Islam et al, 2021 | South Africa | HPV vaccine | 151 Service providers | Vaccine not available to the public |
| Adjei et al, 2023 | Ghana | Malaria vaccine | 54 facilities and 94 carers | Out of stock in the previous six months in 24% (13/54) HF |
| McCoy et al, 2021 | Sierra Leonne | Malaria vaccine | 615 inhabitants of Bo | Supply shortages during vaccination campaigns |
| Nguyen et al, 2020 | Nigeria | HPV vaccine | 137 health agents | Barriers to vaccination: availability of vaccine (39%), lack of CDF (4%), support (1%) |
| Casey et al. 2022 | Senegal | HPV vaccine | 10 of stakeholders | Vaccine shortages leading to postponements and restrictions on targets |
| Rujumba et al, 2021 | Uganda | HPV vaccine | 40 keys informants | Lack of refrigerators in some |
| Grant et al, 2022 | Ghana | Malaria vaccine | 21 healthcare managers and staff | Insufficient refrigerators and vaccine carriers in HF |
| Lack of vehicles in the districts and motorbikes in the HF |
Table 3.
Results related to the logistical challenges of new vaccines.
| Author, Year | Country | Vaccine | Targets | Delivery challenge |
|---|---|---|---|---|
| Shah et al, 2020 | 12 African countries | HBV | 1044 Healthcare personnel | Customer reception problems 32% of reasons for not vaccinating targets |
| Adjei et al, 2023 | Ghana | Malaria vaccine | 54 ESS, 94 carers | Customer reception problems: busy carers (50/54), long waiting times (44/54) |
| Casey et al, 2022 | Senegal | HPV vaccine | 10 of stakeholders | Unsuitable strategy (focused solely on schools) |
| Shortage of qualified staff: lack of information and consistency of services | ||||
| Rujumba et al, 2021 | Uganda | HPV vaccine | 40 Health workers, teachers, girls' parents | Insufficient vaccination staff |
| Lack of strategies for those not attending school | ||||
| Non-payment of staff allowances and teacher motivation | ||||
| Grant et al, 2022 | Ghana | Malaria vaccine | 21 SSE managers | Lack of training for volunteers responsible for raising community awareness |
| Unsuitable timetable: gap (15 months) between the 3rd and 4th doses, leading to dropouts |
Table 4.
Results related to the coordination and financial challenges of new vaccines.
| Author, Year | Country | Vaccine | Targets | Coordination and financial challenges |
|---|---|---|---|---|
| Waterlow et al, 2023 | Kenya | Flu vaccines | Patients hospitalised in 5 hospitals | Median cost per DALY averted above WHO threshold (USD 100) |
| Debellut et al, 2022 | Malawi | Typhoid vaccine | 4 districts and 6 establishments | High cost of introduction (4% of total EPI budget, i.e., $29,814,969) |
| Shah et al, 2020 | 12 African countries | HBV | 1044 healthcare staff | High cost of the vaccine, the most frequently cited reason for non-vaccination (46% of participants) |
| Islam et al, 2021 | South Africa and 4 countries | HPV vaccine | 151 providers authorised to administer vaccines | High cost of the vaccine for customers is a barrier to vaccination for 30% of interviewers, including 16% of South Africans. |
| Baral et al, 2021 | Ghana, Kenya and Malawi) | Malaria vaccine | Nourishing SSEs in pilot areas | Financial cost per FVC* multiplied by 3 if the government pays for the vaccine in full. Economic costs 3 and 5 times higher |
| Debellut et al, 2022 | Niger | Rotavirus Vaccine | 391 children under the age of 5 | High cost of the programme, varying according to the vaccine: USD 46.7 million with ROTAVAC, USD 61.8 million, ROTASIIL Government co-funding |
| Adjei et al, 2023 | Ghana | Malaria vaccine | 54 establishments and 94 carers | Lack of funds forced 90% of establishments to cancel activities |
| McCoy et al, 2021 | Sierra Leone | Malaria vaccine | 615 inhabitants of Bo | Cost of barrier vaccine: 56% prepared to pay USD 0.69 for the vaccine |
| Hidle et al, 2022 | Zimbabwe | HPV vaccine | 30 districts and 60 health facilities | MOHCC co-funding 77% High additional cost: US$7.79 economic cost per dose. |
| Nguyen et al, 2020 | Nigeria | HPV vaccine | 137 Health agents | The cost of vaccine is seen as an obstacle to vaccination by 13% of respondents |
| Casey et al 2022 | Senegal | HPV vaccine | 10 of stakeholders | Delay in the availability of national funds Introduction delayed until Gavi support Communication plan not finalised |
| Alonso et al, 2019 | Mozambique | HPV vaccine | 13 keys informants | The budget constraint for 3 doses: economic cost per FIG, 3 doses ($52.29) and alternative cost at a reduced dose ($31.14) |
| Grant et al, 2022 | Ghana | Malaria vaccine | 21 health service managers | The pilot district selection process is unknown or contested |
| Criteria for eligibility of targets for vaccination open to criticism | ||||
| Brennan et al, 2022 | Senegal | HPV vaccine | 77 Health establishments | High operational costs: service provision (57%; US$4.28 per dose), training (18%; US$1.36 per dose). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



