
Submitted:
31 December 2024
Posted:
31 December 2024
You are already at the latest version
Abstract
The extensive genetic diversity of HIV-1 represents a major challenge to public health interventions, treatment, and successful vaccine design. This challenge is particularly pronounced in the Middle East and North Africa (MENA) region, where limited data among other barriers preclude accurate characterization of HIV-1 genetic diversity. The objective of this review was to analyze studies conducted in the MENA region to delineate possible barriers that would hinder accurate depiction of HIV-1 genetic diversity in the MENA region. A systematic search of PubMed/MEDLINE and Google Scholar was conducted for published records on HIV-1 genetic diversity in English up till 1 October 2024 across 18 MENA countries. The pre-defined themes of challenges/barriers included limited sampling, data gaps, resource and infrastructure constraints, HIV-specific factors, and socio-cultural barriers. A total of 38 records were included in the final review, comprising original articles (55.3%), reviews (21.1%), and sequence notes (10.5%). Libya (15.8%), Morocco (13.2%), Saudi Arabia and MENA as a whole (10.5% for each) were the primary sources of the included records. Of the 23 records with original MENA HIV-1 sequences, the median number of sequences was 46 (range: 6–193). The identified barriers included (1) low sampling density; (2) limited clinical data (21.7% with no data, 60.9% partial data, and 17.4% with full data); (3) reliance solely on population sequencing and insufficient use of advanced sequencing technologies; (4) lack of comprehensive recombination analysis; (5) socio-cultural barriers including stigma with subsequent underreporting among at-risk groups. The barriers identified in this review can hinder the ability to map the genetic diversity of HIV-1 in the MENA. Poor characterization of HIV-1 genetic diversity in the MENA would hinder the efforts to optimize prevention strategies, monitor drug resistance, and develop MENA-specific treatment protocols. To overcome these challenges, investment in public health/research infrastructure, policy reforms to reduce stigma, and strengthened regional collaboration are recommended.
Keywords:
Molecular epidemiology
; phylogenetics
; under-reporting
; AIDS
; HIV infection
1. Introduction
The human immunodeficiency viruses (HIV) are rapidly evolving viruses characterized by extensive genetic diversity [1,2,3]. The extensive diversity of these retroviruses is reflected in its classification into two types: HIV-1 and HIV-2; and four major groups for HIV-1: M, N, O, and P [4]. Group M (major) of is responsible for the vast majority of HIV-1 infections globally and it is further divided into several subtypes (A, B, C, D, F, G, H, J, K), numerous circulating recombinant forms (CRFs), and a countless number of unique recombinant forms (URFs) [5,6,7,8,9].
The global distribution of HIV-1 group M subtypes/CRFs is shaped by historical factors and contemporary transmission dynamics, region-specific distribution of HIV genetic variants [3,4,10,11]. For example, subtype C of HIV-1, which accounts for over half of the global HIV-1 infections, predominates in sub-Saharan Africa (SSA) and India, whereas subtype B is more common in Europe, North America, and certain regions of South America [3,6,12,13]. In Southeast Asia, CRF01_AE is widespread with evidence indicating the role of sex tourism in its global spread [14,15]. In Russia and former Soviet Union countries, subtype A predominates [3,16], while in West and Central Africa, a mixture of HIV-1 and HIV-2 subtypes circulate with predominance of CRF02_AG [3,17,18].
The genetic diversity of HIV-1 is the result of its high evolutionary rate driven by high substitution rate and frequent occurrence of recombination [1,19,20]. The implications of extensive HIV-1 genetic diversity are profound since it contributes to virus virulence, disease progression, and the development of antiretroviral (ARV) drug resistance [19,21,22,23,24,25]. Specifically, variability in the viral envelope (env) gene that encode the HIV surface glycoproteins gp120 and gp41, is a major factor in evasion of humoral immune response [26,27]. Additionally, the swift evolution in the reverse transcriptase, protease, and integrase proteins —the primary targets of ARV drugs— can lead to ARV drug resistance, which would complicate successful management of HIV/AIDS [25,28].
The Middle East and North Africa (MENA) is a region with a complex HIV-1 epidemic [29]. The HIV-1 epidemic in the MENA is characterized by diverse transmission patterns and complex diversity of HIV-1 variants driven by unique socio-cultural factors in the regions [29,30,31,32]. However, accurate mapping of the MENA HIV-1 epidemic is complicated by limited epidemiological and virus sequence data [29,30,31,32,33,34]. Historically, the MENA has been considered as a region with a relatively low prevalence of HIV/AIDS [34,35]. Current estimates suggest that the overall adult HIV prevalence remains below 0.1% in the MENA region; however, certain countries and sub-populations exhibit much higher HIV prevalence rates [36,37,38,39]. Notably, the UNAIDS reported an increase in new HIV infections in the MENA by 116% between 2010 and 2023 [40]. Additionally, recent evidence suggested an accompanying rising trend in HIV prevalence in certain sub-populations [41]. In particular, this trend has been reported among most-at-risk groups such as men who have sex with men (MSM), injection drug users (IDUs), and female sex workers (FSWs) [42].
Regarding the genetic diversity of HIV-1 in the MENA region, a heterogeneous pattern of distribution of HIV-1 genetic variants in the MENA was reported based on the limited sequence data from the region [31,32]. This complex pattern of circulation of diverse range of HIV-1 genetic variants in the MENA likely reflects the region’s geographical location at the crossroads of Asia, Africa, and Europe with frequent population movement [12,32,43]. Therefore, a comprehensive understanding of the genetic diversity of HIV-1 in the MENA region is an important aspect of the regional response to tailor intervention and management measures [32,44,45].
Genetic characterization of HIV-1 through phylogeny-based studies provides valuable insights into the origins and spread of HIV-1, allowing the identification of networks of HIV-1 transmission and enable the tracking of cross-border transmissions [32,46,47,48]. Thus, phylogenetic inference methods can elucidate the role of travel and migration in shaping local HIV-1 epidemics [49,50,51,52]. In the MENA region, phylogenetic analysis revealed a considerable proportion of domestic spread of HIV-1 contrary to the previous notions [32]. The utility of genetic data analysis results in understanding HIV-1 transmission dynamics extends to involve the informing of targeted interventions [53]. However, the lack of systematic and comprehensive HIV-1 genetic surveillance across the MENA countries hinder the ability to map the region-specific HIV-1 dynamics comprehensively [54].
In addition to HIV transmission dynamics studies, genetic characterization of HIV-1 is important to address the challenges of ARV drug resistance [55,56,57,58]. The emergence of drug-resistant mutations poses a significant threat to the success of ARV therapy, particularly in regions with limited access to second-line treatment options [59,60]. In the MENA region, preliminary studies showed a range of resistance-associated mutations (RASs), albeit with varying prevalence across countries [61,62,63,64,65,66]. The variability in ARV drugs’ resistance patterns in the MENA highlights the continuous need for region-specific genetic HIV-1 data to guide the selection of first- and second-line ARV drugs regimens for successful management of the patients in the MENA [67].
Regarding the epidemiology of HIV-1 in the MENA, previous studies revealed country-specific patterns, with high-income countries of the Gulf Cooperation Council (GCC), such as Saudi Arabia and the United Arab Emirates, HIV cases have historically been lower, largely due to strict regulations and religious/cultural norms that traditionally discouraged or legally penalized high-risk behaviors [38,68]. By comparison, North African countries, such as Morocco, Libya, Tunisa, and Egypt, characterized concentrated epidemics among at-risk groups [29,69,70,71,72]. In Sudan, perinatal HIV transmission, especially in conflict-affected areas with limited access to healthcare has been reported [73].
Despite the increasing insights through cumulative HIV research in the MENA, the overall picture of HIV-1 genetic diversity in the MENA region remains fragmented. Challenges to accurate depiction of HIV-1 genetic diversity in the MENA is multifactorial and include limited number of sequence data, variable clinical and epidemiological data quality, and poor regional coordination in surveillance efforts [29,32,33,68,74].
On a related note, the efforts to map the genetic diversity of HIV-1 in the MENA region is hindered by additional challenges, including political instability, limited resources, and social stigma associated with HIV infection [29,75,76]. These factors contribute to the deficiency in robust HIV surveillance, with subsequent gaps in knowledge regarding the true scale of HIV-1 epidemic in the MENA region including its genetic diversity. Additionally, the MENA region is characterized by substantial heterogeneity in terms of health infrastructure and response capacity, ranging from high-income countries with advanced health systems to conflict-affected areas where healthcare access is severely limited [77,78,79,80].
The challenges that may negatively impact the elucidation of HIV-1 genetic diversity in the MENA region necessitate deeper understanding through a focused review of literature. Thus, the current review aimed to identify and describe the specific obstacles that could hinder HIV-1 genetic characterization efforts in the MENA. This description can help to propose actionable strategies to overcome these barriers. By identification of these barriers, we aimed to advance the level of understanding of HIV-1 challenges in the MENA, enhance regional and global public health responses, and contribute to the global efforts to reduce the burden of HIV/AIDS.
2. Materials and Methods
2.1. Review Design
This review was designed to comprehensively analyze the challenges in elucidating HIV-1 genetic diversity within the MENA region. To achieve this, we conducted a systematic search of PubMed/MEDLINE and Google Scholar for records published in English which focused on HIV-1 genetic diversity across 18 MENA countries, including the United Arab Emirates (UAE), Qatar, Bahrain, Oman, Saudi Arabia, Kuwait, Iraq, Syria, Lebanon, Palestine, Jordan, Egypt, Sudan, Libya, Tunisia, Algeria, and Morocco.
The 18 countries were selected based on their geographic and cultural inclusion in the MENA region, as well as their shared epidemiological characteristics, which justify a collective assessment. Conversely, we excluded Türkiye, Iran, Israel, Pakistan, Afghanistan, Djibouti, Somalia, South Sudan, and Mauritania, as previous studies have demonstrated distinct epidemic patterns in these countries that differ significantly from the broader MENA region and would therefore fall outside the scope of this review [81,82,83,84,85,86,87,88,89,90,91,92].
2.2. Search Strategy
The literature search was conducted by the first author (Malik Sallam) on 1 October 2024. The inclusion criteria included: (1) Published records; (2) Language of publication is English; and (3) Any type of publication (original article, review, sequence note, short communication, book, book chapter).
The exact PubMed/MEDLINE search strategy was ((HIV) AND ("Middle East" OR "North Africa" OR "MENA" OR "Arab" OR "United Arab Emirates" OR "UAE" OR "Saudi Arabia" OR "Qatar" OR "Bahrain" OR "Oman" OR "Yemen" OR "Kuwait" OR "Iraq" OR "Syria" OR "Palestine" OR "Jordan" OR "Egypt" OR "Sudan" OR "Libya" OR "Algeria" OR "Tunisia" OR "Morocco")) AND ("genetic diversity" OR "molecular epidemiology").
The Google Scholar search was conducted in Publish or Perish (Version 8) [93]. The exact search strategy was based on the keywords function with 10 hits: HIV molecular epidemiology “Country Name” and HIV genetic diversity “Country Name”.
2.3. Themes to be Extracted from Included Records
To identify the key challenges associated with HIV-1 genetic diversity research in the MENA region, a structured approach was used to establish a priori themes to be extracted from the included records. These themes were developed through a combination of literature review followed by a consensus between the first and senior authors based on these cited publications [94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114]. The process was further informed by barriers previously identified in the first author’s PhD thesis, "Phylogenetic Inference in the Epidemiologic and Evolutionary Investigation of HIV-1, HCV, and HBV," which included analysis of MENA HIV-1 sequences from the Los Alamos HIV Sequence Database [115,116].
Four common themes were identified which are summarized in (Figure 1).
The first theme identified was limited sampling and gaps in clinical and epidemiology data. This included insufficient sampling, poor representation of HIV-1 sequences, low HIV-1 sequencing density, and reliance on non-representative cross-sectional studies. Additionally, this theme included the gaps in clinical and epidemiologic data such as the sex of the patients, age, risk factors for HIV-1 acquisition, viral load, etc. These issues were deemed deficiencies in the genetic analysis approach to delineate HIV-1 genetic diversity.
The second theme identified was limited resources and infrastructure constraints. This issue highlights the reliance on older HIV-1 genetic sequencing methods, such as Sanger sequencing, and the limited use of advanced tools like next-generation sequencing (NGS). Restricted research funding and technical capacity were also included in this theme since these issue were considered as hindrances to progress in HIV-1 genetic diversity research.
The third identified theme was HIV-specific factors, which addressed the genetic complexity of HIV-1 due to high rates of mutation and recombination. A lack of full-genome sequencing and robust HIV-1 isolates’ recombination analysis can limited accurate subtyping and the characterization of CRFs/URFs and thus were deemed as a barrier to HIV-1 genetic characterization.
Finally, the fourth theme identified was the socio-cultural, religious issues, and legal barriers. Stigma, cultural taboos, and punitive laws can hinder access to HIV testing and care for key populations, such as MSM and IDUs. These barriers can cause underreporting and significant data gaps in the investigation of HIV-1 genetic diversity.
3. Results
3.1. Description of the Included Records
A total of 38 records were deemed eligible for inclusion in this review as shown in (Figure 2).
These records were mostly original articles 21/38 (55.3%), followed by reviews including systematic reviews 8/38 (21.1%), and sequence notes/dispatches 4/38 (10.5%). The most common source location for the included records was Libya 6/38 (15.8%), followed by Morocco 5/38 (13.2%), Saudi Arabia and MENA as a whole 4/38 (10.5%) for both, Egypt and Kuwait 3/38 (7.9%) for both (Figure 3 and Table 1).
3.2. Challenge of Limited Sampling and Limited Data
A summary of the included records with HIV-1 sequence and data availability is included in (Table 2).
For the studies where original HIV-1 sequences were originated (n = 23), the average number of sequences included was 62±50 (median: 46, IQR: 25 – 65, range: 6–193). Number of sequences per year is shown in Figure 4, which highlighted gaps in sequencing for HIV-1 in the MENA over two stretches of years (2002–2004) and (2009–2011).
Partial clinical data were available for 14 records (60.9%), and clinical data were totally absent in 5 records (21.7%), while full clinical data were present only in four records (17.4%).
In the included records, the following limitations in terms of limited sampling and limited data were identified: In Morocco, a systematic review by Kouyoumjian et al., reported insufficient data on MSM and IDUs, with reliance on convenience sampling and limited behavioral data often affected by self-report biases [128]. Modes of transmission mathematical model predictions in Morocco exhibited considerable uncertainty due to inadequate input data [129].
In the sole study which investigated domestic HIV-1 transmission in the MENA region as a single unit using the phylogenetic maximum likelihood and Bayesian approaches, eight of the 21 MENA countries lacked HIV-1 sequences, and among the 13 countries with available sequences, only seven countries had more than 50 unique sequences [32]. Many HIV-1 MENA sequences were derived from non-representative cross-sectional studies with low sampling density (<1%) [32].
In Libya, discrepancies were noted between government-reported infection rates and independent estimates as reported by Hamidi et al. [139]. In Saudi Arabia, data quality improved since 2011, but MSM populations remained underrepresented as reported by Al-Mozaini et al. [68]. In Jordan, available data were limited to individuals in HIV care who were willing to participate in research [141].
3.3. Challenge of Limited Resources
The results indicated that HIV surveillance in the MENA region remains limited, with only a small number of cases subtyped, primarily using Sanger sequencing rather than NGS for detecting minor variants as reported by Mumtaz et al. [30]. Only a single record reported using NGS for HIV-1 typing and resistance testing [141].
Challenge of accurate depiction of HIV genetic diversity in the MENA linked to limited resources were identified in Libya by Hamidi et al. [139]. In Libya, monitoring relies on mandatory screenings for certificates and hospital-reported cases, resulting in variable accuracy. In Jordan, limited access to HIV testing and care has been identified as a major factor contributing to late diagnoses, with subsequent increases in healthcare costs [141]. Additionally, in Jordan, contributory factors to late HIV diagnosis include limited access to HIV testing and care with subsequent higher healthcare costs.
On the positive side, Morocco made significant progress in addressing the HIV-1 epidemic and is likely the Arab country with the most advanced HIV-1 surveillance system, research capacity, and response framework as reported by Mumtaz et al. [129]. In Saudi Arabia, despite the progress made, Al-Mozaini et al. highlighted the need for establishing innovative testing services, improving medicine delivery systems which could enhance the understanding of HIV genetic diversity [68].
3.4. Challenge Posed by HIV-Specific Factors
In the majority of included records, HIV-1 subtyping results varied based on the methods employed, particularly for short sequences, which often lacked the resolution necessary for definitive subtype/CRF/URF assignment [32].
The scarcity of full-genome HIV sequences further complicated these challenges, as short sequences are less reliable for subtyping particularly to identify recombinant forms. Only a single record reported sequencing full HIV-1 genomes [126]. Several records relied on subtyping tools that may not account for the complexities of recombination, leading to potential misclassification or incomplete characterization of HIV-1 strains as highlighted in the study which analyzed HIV-1 sequences in the MENA region as a whole [32]. Based on these challenges mutation and recombination present significant obstacles to surveillance efforts.
3.5. Socio-Cultural and legal Issues
Socio-cultural and legal barriers can significantly hinder efforts to characterize HIV-1 genetic diversity in the MENA region, as reported in several included records and in the process shown in (Figure 5).
The groups of MSM was reported in a few records as a stigmatized and hidden HIV risk group, and these records reported that MSM face substantial obstacles to status disclosure and care [36,72]. Despite increasing epidemiological evidence on HIV-1 and risk behaviors among MSM, stigma and cultural norms in the MENA likely result in underreporting of male same-sex transmission in official case notifications [72]. Other high-risk groups, such as truck drivers and prisoners, remain underrepresented in research [33,36,42]. In Palestine, socio-cultural and religious barriers limit the identification of vulnerabilities among high-risk groups, with information gaps persisting on the role of transactional sex in HIV transmission [137]. In Libya, historical policies suppressed accurate HIV data which were considered as part of "national security," dismissing scientific evidence and attributing HIV-1 transmission solely to homosexuality [139]. Conspiratorial beliefs, including claims of clandestine HIV vaccine trials by foreign medical staff, have also been reported [125]. High levels of stigma associating HIV/AIDS with immoral behavior leads many individuals to avoid testing to protect personal and family reputations. In the included records, HIV infected individuals in the MENA were reported to experience severe social consequences, including family rejection, societal isolation, and restricted access to healthcare, education, and employment [137,139]. Women living with HIV were particularly reported to be vulnerable to violence, humiliation, and invasive practices such as virginity testing [139]. These socio-cultural and legal challenges can impede research efforts to delineate HIV-1 genetic diversity in the MENA through underreporting and subsequent gaps in data available for analysis.
4. Discussion
Identification and investigation of possible challenges that could negatively impact the accurate depiction of HIV-1 genetic diversity in the MENA is highly important. HIV-1 is characterized by swift evolutionary rate with subsequent extensive genetic diversity [145,146]. This rapid rate of HIV-1 evolution would in turn complicate HIV/AIDS management and prevention through compromised monitoring of ARV drug resistance and negative effects on vaccine design [147,148]. In the MENA region, the HIV-1 epidemic is characterized by distinct features that result from an interplay of unique socio-cultural, legal, and resource-related aspects [30,33,34,36,42]. Thus, it is important to understand the specific barriers and challenges that would compromise accurate depiction of HIV-1 genetic diversity in the region which in turn would help to develop effective region-specific responses to address the HIV epidemic in the region.
This review identified four key themes that represent barriers to accurate characterization of HIV-1 genetic diversity in the MENA region. These four themes were limited sampling and data gaps, resource and infrastructure constraints, HIV-specific factors, and socio-cultural and legal issues.
The first challenge of limited sampling and insufficient data can profoundly impact efforts to characterize HIV-1 genetic diversity in the MENA region. The molecular epidemiology of an epidemic including HIV-1 epidemics is operating at the population level of pathogens [149]. An important issue to be considered upon conducting genetic diversity investigation is the sampling approach since biased or non-representative sampling will give misleading results [150]. One of the challenging aspects to reconstruct the network of HIV-1 transmission is to obtain a complete sampling density for the population under study given the fraction of undiagnosed HIV-1 infections and the ongoing transmissions [107]. In addition, sampling density will affect the subsequent proportion of HIV-1 phylogenetic clustering indicative of domestic spread of the virus [108,109].
In this review, and across 23 records with HIV-1 sequences, the median number of sequences per record was only 46, with significant gaps in sequencing during two periods, 2002–2004 and 2009–2011. Additionally, as reported in an included record from Morocco, the mathematical models predicting modes of HIV transmission among MSM and IDUs were hampered by insufficient input data and reliance on convenience sampling [129]. Such gaps in data and samples often fail to represent hidden populations, subsequwntly compromising the reliability of transmission estimates [151]. In this review, a record from Libya identified discrepancies between government-reported and independent HIV prevalence rates, which further highlighted the MENA region data limitations aspects [139]. In Jordan, a recent study reported that data were restricted to individuals in HIV care willing to participate in research, creating additional selection bias which might be related to stigma as well [141,152].
The second barrier identified in this review was the challenge of limited resources. This barrier continues to impede HIV-1 genetic diversity research in the MENA region. HIV/AIDS surveillance efforts could also be constrained by traditional methods, with most sequence-based records included in this review relying on Sanger sequencing, which lacks the sensitivity to detect minor variants and recombinants [60,153]. Only one study from Jordan reported the use of NGS, an advanced tool used for robust genetic characterization [141]. Unsurprisingly, the study from Jordan, conducted in collaboration with the Center for Infectious Diseases Research at the Walter Reed Army Institute of Research, emphasize the critical role of international collaboration in addressing resource and capacity constraints faced by the MENA countries to address the topic of HIV-1 genetic diversity [141].
The consequences of health constraints identified in this review can be exemplified in Libya, where monitoring systems relied heavily on mandatory screenings for health certificates and hospital-reported cases [139]. In Jordan, the included study reported that limited access to HIV testing and care contributes to late diagnoses, further complicating health care costs and worsening patient outcomes [141]. These issues resonate with the broader global challenge of healthcare inequity, where underserved populations disproportionately suffer from preventable late-stage complications [154,155,156]. On the other hand, a few MENA countries such as Saudi Arabia and Morocco developed the region’s most advanced HIV surveillance system, demonstrating that resource constraints can be overcome with sustained investment and policy prioritization [68,129]. Saudi Arabia, though making progress, still requires innovative testing services and improved medicine delivery systems to address its unique challenges as reported by an included record in this review by Al-Mozaini et al. [68].
In this review, the third identified challenge was the HIV-specific factors, particularly the genetic complexity of the virus, which pose notable challenges to accurate subtyping and characterization of HIV-1 variants in the MENA region. For example, in HIV-1 molecular epidemiology studies, the choice of the genomic regions to be analyzed are of prime importance with conserved regions unable to resolve the true links compared to phylogenetic noise in hypervariable regions with random links [110,111,112]. Additionally, recombination in HIV is an evident biological phenomenon and can be viewed as means for production of new progeny with higher survival through sharp reduction of deleterious mutations or accumulation of advantageous mutations at a higher rate compared to their occurrence through nucleotide substitution by mutation [157,158]. Additionally, recombination can have adverse effect on molecular clock analysis comprising the validity of estimates of the most recent common ancestor for variant introduction into a region or country [159,160]. Furthermore, construction of phylogenetic trees can be complicated if parts of the nucleotide sequences undergoing analysis were the results of recombination events which implies that the sequences were generated by two viruses, each of which have a distinct evolutionary history [161]. Analysing HIV-1 sequences without excluding recombination will results in misleading findings of phylogenetic analysis [160].
The high mutation and recombination rates in HIV-1 demand advanced methodologies to capture its diversity, yet the majority of studies in the MENA region which were included in this study relied on short sequences that lack the resolution necessary for accurate subtype or recombinant form (CRF/URF) assignment [32,62,64,70,131,133]. Only one study reported sequencing full HIV-1 genomes, underscoring a critical gap in regional research capacity [126]. Additionally, reliance on subtyping tools other than the gold standard phylogenetic based approach with reference full-genome HIV-1 sequences often fail to account for the complexities of recombination, leading to potential misclassification and incomplete characterization of strains [162].
Finally, the socio-cultural and legal barriers remain among the most profound obstacles to understanding HIV-1 genetic diversity in the MENA region. Stigma, deeply rooted in cultural and religious norms in the region, casts a long shadow over public health efforts, particularly for marginalized groups such as MSM [45,163,164,165]. Despite growing epidemiological evidence on HIV-1 and risk behaviors among MSM, the MENA region societal attitudes may result in underreporting of MSM transmission, obscuring the true epidemiological picture of HIV-1 in the MENA [72]. This mirrors the global experience during the early years of the HIV epidemic in the United States, where stigma against MSM delayed effective responses and perpetuated transmission [166]. High-risk populations such as IDUs, FSWs, truck drivers and prisoners are similarly neglected in HIV research in the MENA, creating significant data gaps [29]. The consequences of these barriers are profound since HIV-infected individuals in the MENA region face family rejection, societal isolation, and restricted access to essential services [167]. Women, in particular, are subjected to violence, humiliation, and invasive practices such as virginity testing [139]. Addressing these challenges requires courageous policy reforms, culturally sensitive public health strategies, and a commitment to address stigma to foster transparency and equitable HIV/AIDS research efforts.
4.1. Recommendations
Based on the review findings, several recommendations can be proposed to address the identified barriers that may hinder the investigation of HIV-1 genetic diversity in the MENA. First, investment in infrastructure and research capacity is essential in the MENA region. This includes scaling up the use of advanced sequencing technologies such as NGS and increasing funding for HIV-1 molecular epidemiology studies.
Second, targeted policy reforms are needed to address the socio-cultural and legal barriers that impede access to HIV/AIDS testing and care, particularly among marginalized groups such as MSM, IDUs, and FSWs. Public health campaigns that aim to reduce stigma and promote inclusive policies can play a critical role in overcoming these challenges.
Third, regional and international collaborations should be strengthened to facilitate data sharing and capacity building. A unified regional database for HIV-1 sequences could improve the availability of comprehensive data and enhance cross-border efforts to monitor HIV-1 genetic diversity.
Fourth, increasing the representation of under-researched populations in HIV-1 studies is crucial. This includes prioritizing studies on high-risk groups, such as MSM, FSWs, IDUs, truck drivers, and prisoners, and addressing the gaps in behavioral data that hinder the development of effective interventions.
Finally, integrating socio-cultural considerations into research design and public health strategies is important. Engaging community leaders and stakeholders can help foster acceptance and support for HIV-1 research and interventions, while culturally sensitive approaches can improve participation and data quality. By addressing these challenges, the MENA region can advance its understanding of HIV-1 genetic diversity, ultimately contributing to more effective public health strategies, improved drug resistance monitoring, and tailored treatment protocols in the region.
4.2. Limitations
This review has several limitations that must be acknowledged. First, the geographic and language constraints enforced in the search strategy may have inadvertently excluded relevant records. The focus on English-language publications inherently excludes studies published in Arabic or French, which are widely used in the MENA region especially in the Maghreb region.
Second, the exclusion of specific countries based on distinct epidemic patterns limits the generalizability of the findings. While these exclusions were justified by the review scope, this approach may have resulted in omitting valuable insights into regional HIV-1 genetic diversity. Similarly, the reliance on pre-defined country lists might exclude cross-border insights critical to understanding genetic diversity of HIV-1 in the MENA region characterized by significant population movement.
Third, the literature search relied on PubMed and Google Scholar, which may not fully capture gray literature or unpublished datasets of HIV-1 sequences. This may have lead to potential exclusion of valuable data, since relevant findings might exist in non-traditional repositories or institutional reports.
Fourth, the themes extracted for analysis were derived through consensus among authors and informed by the first author’s prior research. While this approach provides a structured framework, it introduces potential bias, as the thematic focus may overlook emerging challenges not previously documented or emphasized.
5. Conclusions
This review highlighted four key barriers that should be addressed for thorough investigation of HIV-1 genetic diversity in the MENA region. These challenges were limited sampling and data gaps, resource and infrastructure constraints, HIV-specific factors, and socio-cultural issues. Insufficient sampling, reliance on outdated sequencing methods, and a lack of comprehensive recombination analysis hinder accurate depiction of HIV-1 genetic diversity. Additionally, stigma, cultural taboos, and restrictive policies exacerbate HIV-1 underreporting, particularly among at-risk groups such as MSM and IDUs, leaving significant gaps in HIV-1 surveillance data. To overcome these challenges, it is essential to invest in health infrastructure, use advanced technologies, such as NSG, introduce policy reforms to reduce stigma and legal barriers, expand regional and international collaboration and data sharing. Addressing the barriers identified in this review can help in the efforts aiming to accurately map HIV-1 genetic diversity in the MENA region, which is crucial for effective public health strategies. Improved HIV/AIDS surveillance in the MENA would aid in monitoring ARV drug resistance, tailoring treatment protocols, and inform vaccine development efforts.
Author Contributions
Conceptualization, Malik Sallam; methodology, Malik Sallam, Arwa Omar Al-Khatib, Tarneem Sabra, Saja Al-Baidhani, Kholoud Al-Mahzoum, Maryam A. Aleigailly and Mohammed Sallam; software, Malik Sallam; validation, Malik Sallam and Mohammed Sallam; formal analysis, Malik Sallam, Arwa Omar Al-Khatib, Tarneem Sabra, Saja Al-Baidhani, Kholoud Al-Mahzoum, Maryam A. Aleigailly and Mohammed Sallam; investigation, Malik Sallam, Arwa Omar Al-Khatib, Tarneem Sabra, Saja Al-Baidhani, Kholoud Al-Mahzoum, Maryam A. Aleigailly and Mohammed Sallam; resources, Malik Sallam; data curation, Malik Sallam, Arwa Omar Al-Khatib, Tarneem Sabra, Saja Al-Baidhani, Kholoud Al-Mahzoum, Maryam A. Aleigailly and Mohammed Sallam; writing—original draft preparation, Malik Sallam; writing—review and editing, Malik Sallam, Arwa Omar Al-Khatib, Tarneem Sabra, Saja Al-Baidhani, Kholoud Al-Mahzoum, Maryam A. Aleigailly and Mohammed Sallam; visualization, Malik Sallam; supervision, Malik Sallam and Mohammed Sallam; project administration, Malik Sallam and Mohammed Sallam. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting this systematic review are available in the reference section. In addition, the analyzed data that were used during the current systematic review are available from the author on reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ARV | Antiretroviral |
| CRF | Circulating recombinant form |
| FSWs | Female sex workers |
| GCC | Gulf Cooperation Council |
| HIV | Human immunodeficiency viruses |
| HIV-1 | Human immunodeficiency virus type 1 |
| HIV-2 | Human immunodeficiency virus type 2 |
| IDUs | Injection drug users |
| MENA | The Middle East and North Africa |
| MSM | Men who have sex with men |
| NGS | Next-generation sequencing |
| RAS | Resistance-associated mutation |
| SSA | Sub-Saharan Africa |
| UAE | United Arab Emirates |
| UNAIDS | Joint United Nations Programme on HIV/AIDS |
| URF | Unique recombinant forms |
References
- Smyth, R.P.; Davenport, M.P.; Mak, J. The origin of genetic diversity in HIV-1. Virus Res 2012, 169, 415–429. [Google Scholar] [CrossRef]
- Gaschen, B.; Taylor, J.; Yusim, K.; Foley, B.; Gao, F.; Lang, D.; Novitsky, V.; Haynes, B.; Hahn, B.H.; Bhattacharya, T.; et al. Diversity considerations in HIV-1 vaccine selection. Science 2002, 296, 2354–2360. [Google Scholar] [CrossRef]
- Nair, M.; Gettins, L.; Fuller, M.; Kirtley, S.; Hemelaar, J. Global and regional genetic diversity of HIV-1 in 2010-21: systematic review and analysis of prevalence. Lancet Microbe 2024, 5, 100912. [Google Scholar] [CrossRef]
- Williams, A.; Menon, S.; Crowe, M.; Agarwal, N.; Biccler, J.; Bbosa, N.; Ssemwanga, D.; Adungo, F.; Moecklinghoff, C.; Macartney, M.; et al. Geographic and Population Distributions of Human Immunodeficiency Virus (HIV)-1 and HIV-2 Circulating Subtypes: A Systematic Literature Review and Meta-analysis (2010-2021). J Infect Dis 2023, 228, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Gouws, E.; Ghys, P.D.; Osmanov, S. Global and regional distribution of HIV-1 genetic subtypes and recombinants in 2004. Aids 2006, 20, W13–23. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Elangovan, R.; Yun, J.; Dickson-Tetteh, L.; Fleminger, I.; Kirtley, S.; Williams, B.; Gouws-Williams, E.; Ghys, P.D. Global and regional molecular epidemiology of HIV-1, 1990-2015: a systematic review, global survey, and trend analysis. Lancet Infect Dis 2019, 19, 143–155. [Google Scholar] [CrossRef]
- Eberle, J.; Gürtler, L. HIV types, groups, subtypes and recombinant forms: errors in replication, selection pressure and quasispecies. Intervirology 2012, 55, 79–83. [Google Scholar] [CrossRef]
- Hemelaar, J. The origin and diversity of the HIV-1 pandemic. Trends Mol Med 2012, 18, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Elangovan, R.; Yun, J.; Dickson-Tetteh, L.; Kirtley, S.; Gouws-Williams, E.; Ghys, P.D. Global and regional epidemiology of HIV-1 recombinants in 1990-2015: a systematic review and global survey. Lancet HIV 2020, 7, e772–e781. [Google Scholar] [CrossRef] [PubMed]
- Buonaguro, L.; Tornesello, M.L.; Buonaguro, F.M. Human immunodeficiency virus type 1 subtype distribution in the worldwide epidemic: pathogenetic and therapeutic implications. J Virol 2007, 81, 10209–10219. [Google Scholar] [CrossRef] [PubMed]
- Hemelaar, J.; Loganathan, S.; Elangovan, R.; Yun, J.; Dickson-Tetteh, L.; Kirtley, S. Country Level Diversity of the HIV-1 Pandemic between 1990 and 2015. J Virol 2020, 95. [Google Scholar] [CrossRef] [PubMed]
- Bbosa, N.; Kaleebu, P.; Ssemwanga, D. HIV subtype diversity worldwide. Curr Opin HIV AIDS 2019, 14, 153–160. [Google Scholar] [CrossRef]
- Novitsky, V.; Smith, U.R.; Gilbert, P.; McLane, M.F.; Chigwedere, P.; Williamson, C.; Ndung'u, T.; Klein, I.; Chang, S.Y.; Peter, T.; et al. Human immunodeficiency virus type 1 subtype C molecular phylogeny: consensus sequence for an AIDS vaccine design? J Virol 2002, 76, 5435–5451. [Google Scholar] [CrossRef] [PubMed]
- Angelis, K.; Albert, J.; Mamais, I.; Magiorkinis, G.; Hatzakis, A.; Hamouda, O.; Struck, D.; Vercauteren, J.; Wensing, A.M.; Alexiev, I.; et al. Global Dispersal Pattern of HIV Type 1 Subtype CRF01_AE: A Genetic Trace of Human Mobility Related to Heterosexual Sexual Activities Centralized in Southeast Asia. J Infect Dis 2015, 211, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- An, M.; Han, X.; Zhao, B.; English, S.; Frost, S.D.W.; Zhang, H.; Shang, H. Cross-Continental Dispersal of Major HIV-1 CRF01_AE Clusters in China. Front Microbiol 2020, 11, 61. [Google Scholar] [CrossRef]
- Aibekova, L.; Foley, B.; Hortelano, G.; Raees, M.; Abdraimov, S.; Toichuev, R.; Ali, S. Molecular epidemiology of HIV-1 subtype A in former Soviet Union countries. PLoS One 2018, 13, e0191891. [Google Scholar] [CrossRef]
- Giovanetti, M.; Ciccozzi, M.; Parolin, C.; Borsetti, A. Molecular Epidemiology of HIV-1 in African Countries: A Comprehensive Overview. Pathogens 2020, 9, 1072. [Google Scholar] [CrossRef] [PubMed]
- Njai, H.F.; Gali, Y.; Vanham, G.; Clybergh, C.; Jennes, W.; Vidal, N.; Butel, C.; Mpoudi-Ngolle, E.; Peeters, M.; Ariën, K.K. The predominance of Human Immunodeficiency Virus type 1 (HIV-1) circulating recombinant form 02 (CRF02_AG) in West Central Africa may be related to its replicative fitness. Retrovirology 2006, 3, 40. [Google Scholar] [CrossRef]
- Rambaut, A.; Posada, D.; Crandall, K.A.; Holmes, E.C. The causes and consequences of HIV evolution. Nature Reviews Genetics 2004, 5, 52–61. [Google Scholar] [CrossRef]
- Zhang, M.; Foley, B.; Schultz, A.K.; Macke, J.P.; Bulla, I.; Stanke, M.; Morgenstern, B.; Korber, B.; Leitner, T. The role of recombination in the emergence of a complex and dynamic HIV epidemic. Retrovirology 2010, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.F.; Soares, M.A. HIV Genetic Diversity and Drug Resistance. Viruses 2010, 2, 503–531. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Cajas, J.L.; Pant-Pai, N.; Klein, M.B.; Wainberg, M.A. Role of genetic diversity amongst HIV-1 non-B subtypes in drug resistance: a systematic review of virologic and biochemical evidence. AIDS Rev 2008, 10, 212–223. [Google Scholar]
- Bouman, J.A.; Venner, C.M.; Walker, C.; Arts, E.J.; Regoes, R.R. Per-pathogen virulence of HIV-1 subtypes A, C and D. Proc Biol Sci 2023, 290, 20222572. [Google Scholar] [CrossRef]
- Leda, A.R.; Hunter, J.; Castro de Oliveira, U.; Junqueira de Azevedo, I.; Kallas, E.G.; Araripe Sucupira, M.C.; Diaz, R.S. HIV-1 genetic diversity and divergence and its correlation with disease progression among antiretroviral naïve recently infected individuals. Virology 2020, 541, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Shi, B.; Kitchen, C.; Weiser, B.; Mayers, D.; Foley, B.; Kemal, K.; Anastos, K.; Suchard, M.; Parker, M.; Brunner, C.; et al. Evolution and recombination of genes encoding HIV-1 drug resistance and tropism during antiretroviral therapy. Virology 2010, 404, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Arrildt, K.T.; Joseph, S.B.; Swanstrom, R. The HIV-1 env protein: a coat of many colors. Curr HIV/AIDS Rep 2012, 9, 52–63. [Google Scholar] [CrossRef]
- Pérez-Yanes, S.; Pernas, M.; Marfil, S.; Cabrera-Rodríguez, R.; Ortiz, R.; Urrea, V.; Rovirosa, C.; Estévez-Herrera, J.; Olivares, I.; Casado, C.; et al. The Characteristics of the HIV-1 Env Glycoprotein Are Linked With Viral Pathogenesis. Front Microbiol 2022, 13, 763039. [Google Scholar] [CrossRef]
- Bure, D.; Makhdoomi, M.A.; Lodha, R.; Prakash, S.S.; Kumar, R.; Parray, H.A.; Singh, R.; Kabra, S.K.; Luthra, K. Mutations in the reverse transcriptase and protease genes of human immunodeficiency virus-1 from antiretroviral naïve and treated pediatric patients. Viruses 2015, 7, 590–603. [Google Scholar] [CrossRef]
- Karbasi, A.; Fordjuoh, J.; Abbas, M.; Iloegbu, C.; Patena, J.; Adenikinju, D.; Vieira, D.; Gyamfi, J.; Peprah, E. An Evolving HIV Epidemic in the Middle East and North Africa (MENA) Region: A Scoping Review. Int J Environ Res Public Health 2023, 20, 3844. [Google Scholar] [CrossRef]
- Mumtaz, G.; Hilmi, N.; Akala, F.A.; Semini, I.; Riedner, G.; Wilson, D.; Abu-Raddad, L.J. HIV-1 molecular epidemiology evidence and transmission patterns in the Middle East and North Africa. Sex Transm Infect 2011, 87, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Rolland, M.; Modjarrad, K. Multiple co-circulating HIV-1 subtypes in the Middle East and North Africa. Aids 2015, 29, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Şahin, G.; Ingman, M.; Widell, A.; Esbjörnsson, J.; Medstrand, P. Genetic characterization of human immunodeficiency virus type 1 transmission in the Middle East and North Africa. Heliyon 2017, 3, e00352. [Google Scholar] [CrossRef]
- Mumtaz, G.R.; Chemaitelly, H.; Abu-Raddad, L.J. The HIV Epidemic in the Middle East and North Africa: Key Lessons. In Handbook of Healthcare in the Arab World, Laher, I., Ed.; Springer International Publishing: Cham, 2021; pp. 3053–3079. [Google Scholar] [CrossRef]
- Gökengin, D.; Doroudi, F.; Tohme, J.; Collins, B.; Madani, N. HIV/AIDS: trends in the Middle East and North Africa region. Int J Infect Dis 2016, 44, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Shakiba, E.; Ramazani, U.; Mardani, E.; Rahimi, Z.; Nazar, Z.M.; Najafi, F.; Moradinazar, M. Epidemiological features of HIV/AIDS in the Middle East and North Africa from 1990 to 2017. Int J STD AIDS 2021, 32, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, G.R.; Riedner, G.; Abu-Raddad, L.J. The emerging face of the HIV epidemic in the Middle East and North Africa. Curr Opin HIV AIDS 2014, 9, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Kteily-Hawa, R.; Hawa, A.C.; Gogolishvili, D.; Al Akel, M.; Andruszkiewicz, N.; Vijayanathan, H.; Loutfy, M. Understanding the epidemiological HIV risk factors and underlying risk context for youth residing in or originating from the Middle East and North Africa (MENA) region: A scoping review of the literature. PLoS One 2022, 17, e0260935. [Google Scholar] [CrossRef]
- Awaidy, S.A.; Ghazy, R.M.; Mahomed, O. Progress of the Gulf Cooperation Council (GCC) Countries Towards Achieving the 95-95-95 UNAIDS Targets: A Review. J Epidemiol Glob Health 2023, 13, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Shawky, S.; Soliman, C.; Kassak, K.M.; Oraby, D.; El-Khoury, D.; Kabore, I. HIV surveillance and epidemic profile in the Middle East and North Africa. J Acquir Immune Defic Syndr 2009, 51 Suppl 3, S83–95. [Google Scholar] [CrossRef]
- UNAIDS. Middle East and North Africa regional profile — 2024 global AIDS update The Urgency of Now: AIDS at a Crossroads. Available online: https://www.unaids.org/en/resources/documents/2024/2024-unaids-global-aids-update-mena (accessed on 30 December 2024).
- Korenromp, E.L.; Sabin, K.; Stover, J.; Brown, T.; Johnson, L.F.; Martin-Hughes, R.; Ten Brink, D.; Teng, Y.; Stevens, O.; Silhol, R.; et al. New HIV Infections Among Key Populations and Their Partners in 2010 and 2022, by World Region: A Multisources Estimation. J Acquir Immune Defic Syndr 2024, 95, e34–e45. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, G.R.; Chemaitelly, H.; AlMukdad, S.; Osman, A.; Fahme, S.; Rizk, N.A.; El Feki, S.; Abu-Raddad, L.J. Status of the HIV epidemic in key populations in the Middle East and north Africa: knowns and unknowns. Lancet HIV 2022, 9, e506–e516. [Google Scholar] [CrossRef] [PubMed]
- Naujoks, D. Multilateral Approaches to Mobility in the Middle East and North Africa Region. International Development Policy | Revue internationale de politique de développement 2022, 14. [Google Scholar] [CrossRef]
- Kanki, P.J. HIV/AIDS Global Epidemichuman immunodeficiency virus (HIV)global epidemichuman immunodeficiency virus (HIV)Global Epidemic. In Encyclopedia of Sustainability Science and Technology; Meyers, R.A., Ed.; Springer New York: New York, NY, 2012; pp. 4996–5020. [Google Scholar] [CrossRef]
- McFarland, W.; Abu-Raddad, L.J.; Mahfoud, Z.; DeJong, J.; Riedner, G.; Forsyth, A.; Khoshnood, K. HIV/AIDS in the Middle East and North Africa: new study methods, results, and implications for prevention and care. Aids 2010, 24 Suppl 2, S1–4. [Google Scholar] [CrossRef]
- Hassan, A.S.; Pybus, O.G.; Sanders, E.J.; Albert, J.; Esbjörnsson, J. Defining HIV-1 transmission clusters based on sequence data. Aids 2017, 31, 1211–1222. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Jin, Y.; Yang, Y.; Duan, X.; Cao, Y.; Shan, D.; Cai, C.; Tang, H. Characterizing HIV-1 transmission by genetic cluster analysis among newly diagnosed patients in the China-Myanmar border region from 2020 to 2023. Emerg Microbes Infect 2024, 13, 2409319. [Google Scholar] [CrossRef] [PubMed]
- Ratmann, O.; Grabowski, M.K.; Hall, M.; Golubchik, T.; Wymant, C.; Abeler-Dörner, L.; Bonsall, D.; Hoppe, A.; Brown, A.L.; de Oliveira, T.; et al. Inferring HIV-1 transmission networks and sources of epidemic spread in Africa with deep-sequence phylogenetic analysis. Nature Communications 2019, 10, 1411. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.G.; Ibanescu, R.I.; Osman, N.; Cuadra-Foy, E.; Oliveira, M.; Chaillon, A.; Stephens, D.; Hardy, I.; Routy, J.P.; Thomas, R.; et al. The Role of Phylogenetics in Unravelling Patterns of HIV Transmission towards Epidemic Control: The Quebec Experience (2002-2020). Viruses 2021, 13, 1643. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.; Wainberg, M.A.; Roger, M. Phylogenetic inferences on HIV-1 transmission: implications for the design of prevention and treatment interventions. Aids 2013, 27, 1045–1057. [Google Scholar] [CrossRef]
- Dennis, A.M.; Hué, S.; Pasquale, D.; Napravnik, S.; Sebastian, J.; Miller, W.C.; Eron, J.J. HIV Transmission Patterns Among Immigrant Latinos Illuminated by the Integration of Phylogenetic and Migration Data. AIDS Res Hum Retroviruses 2015, 31, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yao, J.; Jiang, J.; Pan, X.; Luo, M.; Xia, Y.; Fan, Q.; Ding, X.; Ruan, J.; Handel, A.; et al. Migration interacts with the local transmission of HIV in developed trade areas: A molecular transmission network analysis in China. Infect Genet Evol 2020, 84, 104376. [Google Scholar] [CrossRef]
- Dong, Z.L.; Gao, G.F.; Lyu, F. Advances in research of HIV transmission networks. Chin Med J (Engl) 2020, 133, 2850–2858. [Google Scholar] [CrossRef] [PubMed]
- Bozicevic, I.; Riedner, G.; Calleja, J.M.G. HIV surveillance in MENA: recent developments and results. Sexually Transmitted Infections 2013, 89, iii11. [Google Scholar] [CrossRef] [PubMed]
- Sardashti, S.; Samaei, M.; Firouzeh, M.M.; Mirshahvalad, S.A.; Pahlaviani, F.G.; SeyedAlinaghi, S. Early initiation of antiretroviral treatment: Challenges in the Middle East and North Africa. World J Virol 2015, 4, 134–141. [Google Scholar] [CrossRef]
- Tang, M.W.; Shafer, R.W. HIV-1 antiretroviral resistance: scientific principles and clinical applications. Drugs 2012, 72, e1–25. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, C.; Sun, Y.; Fu, C.; Wei, S.; Zhang, X.; Ma, J.; Zhao, Q.; Huo, Y. Characteristics of drug resistance mutations in ART-experienced HIV-1 patients with low-level viremia in Zhengzhou City, China. Scientific Reports 2024, 14, 10620. [Google Scholar] [CrossRef] [PubMed]
- Bandera, A.; Gori, A.; Clerici, M.; Sironi, M. Phylogenies in ART: HIV reservoirs, HIV latency and drug resistance. Curr Opin Pharmacol 2019, 48, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Paydary, K.; Khaghani, P.; Emamzadeh-Fard, S.; Alinaghi, S.A.; Baesi, K. The emergence of drug resistant HIV variants and novel anti-retroviral therapy. Asian Pac J Trop Biomed 2013, 3, 515–522. [Google Scholar] [CrossRef]
- Apetroaei, M.M.; Velescu, B.; Nedea, M.I.I.; Dinu-Pîrvu, C.E.; Drăgănescu, D.; Fâcă, A.I.; Udeanu, D.I.; Arsene, A.L. The Phenomenon of Antiretroviral Drug Resistance in the Context of Human Immunodeficiency Virus Treatment: Dynamic and Ever Evolving Subject Matter. Biomedicines 2024, 12, 915. [Google Scholar] [CrossRef]
- Khan, S.; Zehra, F.; Zahid, M.; Ali, Z. Analysis of HIV-1 drug resistance in Gulf countries. Pathology 2014, 46, S111. [Google Scholar] [CrossRef]
- Chehadeh, W.; Albaksami, O.; Altawalah, H.; Ahmad, S.; Madi, N.; John, S.E.; Abraham, P.S.; Al-Nakib, W. Phylogenetic analysis of HIV-1 subtypes and drug resistance profile among treatment-naïve people in Kuwait. J Med Virol 2015, 87, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- Chehadeh, W.; Albaksami, O.; John, S.E.; Al-Nakib, W. Resistance-Associated Mutations and Polymorphisms among Integrase Inhibitor-Naïve HIV-1 Patients in Kuwait. Intervirology 2017, 60, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Chehadeh, W.; Albaksami, O.; John, S.E.; Al-Nakib, W. Drug Resistance-Associated Mutations in Antiretroviral Treatment-Experienced Patients in Kuwait. Medical Principles and Practice 2018, 27, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Gaballah, A.; Ghazal, A.; Metwally, D.; Emad, R.; Essam, G.; Attia, N.M.; Amer, A.N. Mutation patterns, Cross Resistance and Virological Failure Among HIV type-1 Patients in Alexandria, Egypt. Future Virology 2022, 17, 441–454. [Google Scholar] [CrossRef]
- Zaki, E.A.; El-Daly, M.M.; Abdulhaq, A.; Al-Subhi, T.L.; Hassan, A.M.; El-Kafrawy, S.A.; Alhazmi, M.M.; Darraj, M.A.; Azhar, E.I. Genotyping and antiretroviral drug resistance of human immunodeficiency Virus-1 in Jazan, Saudi Arabia. Medicine (Baltimore) 2020, 99, e23274. [Google Scholar] [CrossRef]
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infection, Genetics and Evolution 2016, 46, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Al-Mozaini, M.; Al-Rahabani, T.; Dirar, Q.; Alashgar, T.; Rabaan, A.A.; Murad, W.; Alotaibi, J.; Alrajhi, A. Human immunodeficiency virus in Saudi Arabia: Current and future challenges. J Infect Public Health 2023, 16, 1500–1509. [Google Scholar] [CrossRef] [PubMed]
- Daw, M.A.; Ahmed, M.O. Epidemiological characterization and geographic distribution of human immunodeficiency virus/acquired immunodeficiency syndrome infection in North African countries. World J Virol 2021, 10, 69–85. [Google Scholar] [CrossRef]
- Akrim, M.; Lemrabet, S.; Elharti, E.; Gray, R.R.; Tardy, J.C.; Cook, R.L.; Salemi, M.; Andre, P.; Azarian, T.; Aouad, R.E. HIV-1 Subtype distribution in morocco based on national sentinel surveillance data 2004-2005. AIDS Res Ther 2012, 9, 5. [Google Scholar] [CrossRef]
- Mumtaz, G.R.; Weiss, H.A.; Thomas, S.L.; Riome, S.; Setayesh, H.; Riedner, G.; Semini, I.; Tawil, O.; Akala, F.A.; Wilson, D.; et al. HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis. PLoS Med 2014, 11, e1001663. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, G.; Hilmi, N.; McFarland, W.; Kaplan, R.L.; Akala, F.A.; Semini, I.; Riedner, G.; Tawil, O.; Wilson, D.; Abu-Raddad, L.J. Are HIV epidemics among men who have sex with men emerging in the Middle East and North Africa?: a systematic review and data synthesis. PLoS Med 2010, 8, e1000444. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, B.A.; Mahfouz, M.S. Factors associated with HIV/AIDS in Sudan. Biomed Res Int 2013, 2013, 971203. [Google Scholar] [CrossRef]
- González-Alcaide, G.; Menchi-Elanzi, M.; Nacarapa, E.; Ramos-Rincón, J.-M. HIV/AIDS research in Africa and the Middle East: participation and equity in North-South collaborations and relationships. Globalization and Health 2020, 16, 83. [Google Scholar] [CrossRef]
- Al-Abri, S.; Mokhbat, J.E. HIV in the MENA Region: Cultural and Political Challenges. Int J Infect Dis 2016, 44, 64–65. [Google Scholar] [CrossRef]
- Ballouz, T.; Gebara, N.; Rizk, N. HIV-related stigma among health-care workers in the MENA region. Lancet HIV 2020, 7, e311–e313. [Google Scholar] [CrossRef] [PubMed]
- Mate, K.; Bryan, C.; Deen, N.; McCall, J. Review of Health Systems of the Middle East and North Africa Region. Reference Module in Biomedical Sciences 2014. [Google Scholar] [CrossRef]
- Katoue, M.G.; Cerda, A.A.; García, L.Y.; Jakovljevic, M. Healthcare system development in the Middle East and North Africa region: Challenges, endeavors and prospective opportunities. Front Public Health 2022, 10, 1045739. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yazbeck, A. Benchmarking Health Systems in Middle Eastern and North African Countries. Health Systems & Reform 2017, 3, 7–13. [Google Scholar] [CrossRef]
- Qaqish, B.; Sallam, M.; Al-Khateeb, M.; Reisdorf, E.; Mahafzah, A. Assessment of COVID-19 Molecular Testing Capacity in Jordan: A Cross-Sectional Study at the Country Level. Diagnostics (Basel) 2022, 12, 909. [Google Scholar] [CrossRef]
- Sayan, M.; Sultanoglu, N.; Sanlidag, T. Dynamics of Rilpivirine Resistance-Associated Mutation: E138 in Reverse Transcriptase among Antiretroviral-Naive HIV-1-Infected Individuals in Turkey. AIDS Res Hum Retroviruses 2023, 39, 84–90. [Google Scholar] [CrossRef]
- Sayan, M.; Sargin, F.; Inan, D.; Sevgi, D.Y.; Celikbas, A.K.; Yasar, K.; Kaptan, F.; Kutlu, S.; Fisgin, N.T.; Inci, A.; et al. HIV-1 Transmitted Drug Resistance Mutations in Newly Diagnosed Antiretroviral-Naive Patients in Turkey. AIDS Res Hum Retroviruses 2016, 32, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Sayan, M.; Sargýn, F.; Inan, D.; Sevgi, D.Y.; Celikbas, A.K.; Yasar, K.; Kaptan, F.; Kutlu, S.S.; Fýsgýn, N.T.; Inci, A.; et al. Transmitted antiretroviral drug resistance mutations in newly diagnosed HIV-1 positive patients in Turkey. J Int AIDS Soc 2014, 17, 19750. [Google Scholar] [CrossRef] [PubMed]
- Jahanbakhsh, F.; Ibe, S.; Hattori, J.; Monavari, S.H.; Matsuda, M.; Maejima, M.; Iwatani, Y.; Memarnejadian, A.; Keyvani, H.; Azadmanesh, K.; et al. Molecular epidemiology of HIV type 1 infection in Iran: genomic evidence of CRF35_AD predominance and CRF01_AE infection among individuals associated with injection drug use. AIDS Res Hum Retroviruses 2013, 29, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Sanders-Buell, E.; Saad, M.D.; Abed, A.M.; Bose, M.; Todd, C.S.; Strathdee, S.A.; Botros, B.A.; Safi, N.; Earhart, K.C.; Scott, P.T.; et al. A nascent HIV type 1 epidemic among injecting drug users in Kabul, Afghanistan is dominated by complex AD recombinant strain, CRF35_AD. AIDS Res Hum Retroviruses 2007, 23, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Eybpoosh, S.; Bahrampour, A.; Karamouzian, M.; Azadmanesh, K.; Jahanbakhsh, F.; Mostafavi, E.; Zolala, F.; Haghdoost, A.A. Spatio-Temporal History of HIV-1 CRF35_AD in Afghanistan and Iran. PLoS One 2016, 11, e0156499. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Kang, L.; Yi, F.; Chu, Q.; Shah, S.A.; Mahmood, S.F.; Getaneh, Y.; Wei, M.; Chang, S.; Abidi, S.H.; et al. Human Immunodeficiency Virus Type-1 Genetic Diversity and Drugs Resistance Mutations among People Living with HIV in Karachi, Pakistan. Viruses 2024, 16, 962. [Google Scholar] [CrossRef] [PubMed]
- Grossman, Z.; Avidor, B.; Girshengoren, S.; Katchman, E.; Maldarelli, F.; Turner, D. Transmission Dynamics of HIV Subtype A in Tel Aviv, Israel: Implications for HIV Spread and Eradication. Open Forum Infect Dis 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Maslin, J.; Rogier, C.; Berger, F.; Khamil, M.A.; Mattera, D.; Grandadam, M.; Caron, M.; Nicand, E. Epidemiology and genetic characterization of HIV-1 isolates in the general population of Djibouti (Horn of Africa). J Acquir Immune Defic Syndr 2005, 39, 129–132. [Google Scholar] [PubMed]
- Kulane, A.; Owuor, J.O.A.; Sematimba, D.; Abdulahi, S.A.; Yusuf, H.M.; Mohamed, L.M. Access to HIV Care and Resilience in a Long-Term Conflict Setting: A Qualitative Assessment of the Experiences of Living with Diagnosed HIV in Mogadishu, Somali. Int J Environ Res Public Health 2017, 14, 721. [Google Scholar] [CrossRef] [PubMed]
- Jervase, A.; Tahir, H.; Modi, J.K.; Almobarak, A.O.; Mital, D.; Ahmed, M.H. HIV/AIDS in South Sudan past, present, and future: a model of resilience in a challenging context. Journal of Public Health and Emergency 2018, 2, 1–6. [Google Scholar] [CrossRef]
- Fall-Malick, F.Z.; Tchiakpé, E.; Ould Soufiane, S.; Diop-Ndiaye, H.; Mouhamedoune Baye, A.; Ould Horma Babana, A.; Touré Kane, C.; Lo, B.; Mboup, S. Drug resistance mutations and genetic diversity in adults treated for HIV type 1 infection in Mauritania. J Med Virol 2014, 86, 404–410. [Google Scholar] [CrossRef]
- Harzing, A.-W. Publish or Perish. Available online: https://harzing.com/resources/publish-or-perish (accessed on 1 October 2024).
- Mehta, S.R.; Schairer, C.; Little, S. Ethical issues in HIV phylogenetics and molecular epidemiology. Curr Opin HIV AIDS 2019, 14, 221–226. [Google Scholar] [CrossRef]
- Grabowski, M.K.; Herbeck, J.T.; Poon, A.F.Y. Genetic Cluster Analysis for HIV Prevention. Curr HIV/AIDS Rep 2018, 15, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Devlin, S.; Kerman, J.; Fujimoto, K.; Hirschhorn, L.R.; Phillips, G., 2nd; Schneider, J.; McNulty, M.C. Ending the HIV Epidemic: Identifying Barriers and Facilitators to Implement Molecular HIV Surveillance to Develop Real-Time Cluster Detection and Response Interventions for Local Communities. Int J Environ Res Public Health 2023, 20, 3269. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ouyang, F.; Liu, X.; Lu, J.; Hu, H.; Sun, Q.; Yang, H. A Sensitivity and Consistency Comparison Between Next-Generation Sequencing and Sanger Sequencing in HIV-1 Pretreatment Drug Resistance Testing. Viruses 2024, 16, 1713. [Google Scholar] [CrossRef]
- Ouyang, F.; Yuan, D.; Zhai, W.; Liu, S.; Zhou, Y.; Yang, H. HIV-1 Drug Resistance Detected by Next-Generation Sequencing among ART-Naïve Individuals: A Systematic Review and Meta-Analysis. Viruses 2024, 16, 239. [Google Scholar] [CrossRef] [PubMed]
- Molldrem, S.; Smith, A.K.J.; Subrahmanyam, V. Toward Consent in Molecular HIV Surveillance?: Perspectives of Critical Stakeholders. AJOB Empir Bioeth 2024, 15, 66–79. [Google Scholar] [CrossRef]
- Stojanovski, K.; Naja-Riese, G.; King, E.J.; Fuchs, J.D. A Systematic Review of the Social Network Strategy to Optimize HIV Testing in Key Populations to End the Epidemic in the United States. AIDS Behav 2021, 25, 2680–2698. [Google Scholar] [CrossRef] [PubMed]
- Rwabiyago, O.E.; Katale, A.; Bingham, T.; Grund, J.M.; Machangu, O.; Medley, A.; Nkomela, Z.M.; Kayange, A.; King'ori, G.N.; Juma, J.M.; et al. Social network strategy (SNS) for HIV testing: a new approach for identifying individuals with undiagnosed HIV infection in Tanzania. AIDS Care 2024, 36, 201–210. [Google Scholar] [CrossRef]
- Jamrozik, E.; Munung, N.S.; Abeler-Dorner, L.; Parker, M. Public health use of HIV phylogenetic data in sub-Saharan Africa: ethical issues. BMJ Glob Health 2023, 8. [Google Scholar] [CrossRef] [PubMed]
- Beamud, B.; Bracho, M.A.; González-Candelas, F. Characterization of New Recombinant Forms of HIV-1 From the Comunitat Valenciana (Spain) by Phylogenetic Incongruence. Front Microbiol 2019, 10, 1006. [Google Scholar] [CrossRef] [PubMed]
- Camacho, R. The significance of subtype-related genetic variability: controversies and unanswered questions. In Antiretroviral Resistance in Clinical Practice, Geretti, A.M., Ed.; Mediscript: London, 2006. [Google Scholar]
- Bouabida, K.; Chaves, B.G.; Anane, E. Challenges and barriers to HIV care engagement and care cascade: viewpoint. Front Reprod Health 2023, 5, 1201087. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.E.; Milloy, M.J.; Ogilvie, G.; Greene, S.; Nicholson, V.; Vonn, M.; Hogg, R.; Kaida, A. The impact of criminalization of HIV non-disclosure on the healthcare engagement of women living with HIV in Canada: a comprehensive review of the evidence. J Int AIDS Soc 2015, 18, 20572. [Google Scholar] [CrossRef] [PubMed]
- Giardina, F.; Romero-Severson, E.O.; Albert, J.; Britton, T.; Leitner, T. Inference of Transmission Network Structure from HIV Phylogenetic Trees. PLoS computational biology 2017, 13, e1005316. [Google Scholar] [CrossRef] [PubMed]
- Novitsky, V.; Moyo, S.; Lei, Q.; DeGruttola, V.; Essex, M. Impact of sampling density on the extent of HIV clustering. AIDS Res Hum Retroviruses 2014, 30, 1226–1235. [Google Scholar] [CrossRef]
- Slattery, M.L. The science and art of molecular epidemiology. Journal of epidemiology and community health 2002, 56, 728–729. [Google Scholar] [CrossRef] [PubMed]
- Hillis, D.M.; Huelsenbeck, J.P. Signal, noise, and reliability in molecular phylogenetic analyses. The Journal of heredity 1992, 83, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ratmann, O.; Hodcroft, E.B.; Pickles, M.; Cori, A.; Hall, M.; Lycett, S.; Colijn, C.; Dearlove, B.; Didelot, X.; Frost, S.; et al. Phylogenetic Tools for Generalized HIV-1 Epidemics: Findings from the PANGEA-HIV Methods Comparison. Molecular biology and evolution 2017, 34, 185–203. [Google Scholar] [CrossRef] [PubMed]
- Romero-Severson, E.O.; Bulla, I.; Leitner, T. Phylogenetically resolving epidemiologic linkage. Proceedings of the National Academy of Sciences of the United States of America 2016, 113, 2690–2695. [Google Scholar] [CrossRef] [PubMed]
- Romero-Severson, E.; Skar, H.; Bulla, I.; Albert, J.; Leitner, T. Timing and order of transmission events is not directly reflected in a pathogen phylogeny. Molecular biology and evolution 2014, 31, 2472–2482. [Google Scholar] [CrossRef] [PubMed]
- Resik, S.; Lemey, P.; Ping, L.H.; Kouri, V.; Joanes, J.; Perez, J.; Vandamme, A.M.; Swanstrom, R. Limitations to contact tracing and phylogenetic analysis in establishing HIV type 1 transmission networks in Cuba. AIDS Res Hum Retroviruses 2007, 23, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. Phylogenetic inference in the epidemiologic and evolutionary investigation of HIV-1, HCV and HBV. Lund University, Faculty of Medicine, Lund, 2017.
- Kuiken, C.; Korber, B.; Shafer, R.W. HIV sequence databases. AIDS Rev 2003, 5, 52–61. [Google Scholar] [PubMed]
- Pieniazek, D.; Baggs, J.; Hu, D.J.; Matar, G.M.; Abdelnoor, A.M.; Mokhbat, J.E.; Uwaydah, M.; Bizri, A.R.; Ramos, A.; Janini, L.M.; et al. Introduction of HIV-2 and multiple HIV-1 subtypes to Lebanon. Emerg Infect Dis 1998, 4, 649–656. [Google Scholar] [CrossRef]
- El Sayed, N.M.; Gomatos, P.J.; Beck-Sagué, C.M.; Dietrich, U.; von Briesen, H.; Osmanov, S.; Esparza, J.; Arthur, R.R.; Wahdan, M.H.; Jarvis, W.R. Epidemic transmission of human immunodeficiency virus in renal dialysis centers in Egypt. J Infect Dis 2000, 181, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Ben Halima, M.; Pasquier, C.; Slim, A.; Ben Chaabane, T.; Arrouji, Z.; Puel, J.; Ben Redjeb, S.; Izopet, J. First molecular characterization of HIV-1 Tunisian strains. J Acquir Immune Defic Syndr 2001, 28, 94–96. [Google Scholar] [CrossRef]
- Elharti, E.; Alami, M.; Khattabi, H.; Bennani, A.; Zidouh, A.; Benjouad, A.; El Aouad, R. Some characteristics of the HIV epidemic in Morocco. East Mediterr Health J 2002, 8, 819–825. [Google Scholar] [CrossRef]
- Saad, M.D.; Al-Jaufy, A.; Grahan, R.R.; Nadai, Y.; Earhart, K.C.; Sanchez, J.L.; Carr, J.K. HIV type 1 strains common in Europe, Africa, and Asia cocirculate in Yemen. AIDS Res Hum Retroviruses 2005, 21, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Bouzeghoub, S.; Jauvin, V.; Recordon-Pinson, P.; Garrigue, I.; Amrane, A.; Belabbes el, H.; Fleury, H.J. High diversity of HIV type 1 in Algeria. AIDS Res Hum Retroviruses 2006, 22, 367–372. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, T.; Pybus, O.G.; Rambaut, A.; Salemi, M.; Cassol, S.; Ciccozzi, M.; Rezza, G.; Gattinara, G.C.; D'Arrigo, R.; Amicosante, M.; et al. Molecular epidemiology: HIV-1 and HCV sequences from Libyan outbreak. Nature 2006, 444, 836–837. [Google Scholar] [CrossRef] [PubMed]
- Badreddine, S.; Smith, K.; van Zyl, H.; Bodelle, P.; Yamaguchi, J.; Swanson, P.; Devare, S.G.; Brennan, C.A. Identification and characterization of HIV type 1 subtypes present in the Kingdom of Saudi Arabia: high level of genetic diversity found. AIDS Res Hum Retroviruses 2007, 23, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Bagasra, O.; Alsayari, M.; Bullard-Dillard, R.; Daw, M.A. The Libyan HIV Outbreak How do we find the truth? Libyan J Med 2007, 2, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, J.; Badreddine, S.; Swanson, P.; Bodelle, P.; Devare, S.G.; Brennan, C.A. Identification of new CRF43_02G and CRF25_cpx in Saudi Arabia based on full genome sequence analysis of six HIV type 1 isolates. AIDS Res Hum Retroviruses 2008, 24, 1327–1335. [Google Scholar] [CrossRef]
- Mumtaz, G.; Abu-Raddad, L. HIV Molecular Epidemiology in the Middle East and North Africa: Understanding the Virus Transmission Patterns. 2011, 2011. [CrossRef]
- Kouyoumjian, S.P.; Mumtaz, G.R.; Hilmi, N.; Zidouh, A.; El Rhilani, H.; Alami, K.; Bennani, A.; Gouws, E.; Ghys, P.D.; Abu-Raddad, L.J. The epidemiology of HIV infection in Morocco: systematic review and data synthesis. Int J STD AIDS 2013, 24, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, G.R.; Kouyoumjian, S.P.; Hilmi, N.; Zidouh, A.; El Rhilani, H.; Alami, K.; Bennani, A.; Gouws, E.; Ghys, P.D.; Abu-Raddad, L.J. The distribution of new HIV infections by mode of exposure in Morocco. Sex Transm Infect 2013, 89 Suppl 3, iii49–56. [Google Scholar] [CrossRef]
- Mokhbat, J.M.; Melhem, N.M.; El-Khatib, Z.; Zalloua, P. Screening for antiretroviral drug resistance among treatment-naive human immunodeficiency virus type 1-infected individuals in Lebanon. J Infect Dev Ctries 2014, 8, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Abdellaziz, A.; Papuchon, J.; Khaled, S.; Ouerdane, D.; Fleury, H.; Recordon-Pinson, P. Predominance of CRF06_cpx and Transmitted HIV Resistance in Algeria: Update 2013-2014. AIDS Res Hum Retroviruses 2016, 32, 370–372. [Google Scholar] [CrossRef]
- Daw, M.A.; El-Bouzedi, A.; Ahmed, M.O.; Dau, A.A. Molecular and epidemiological characterization of HIV-1 subtypes among Libyan patients. BMC Res Notes 2017, 10, 170. [Google Scholar] [CrossRef] [PubMed]
- El Moussi, A.; Thomson, M.M.; Delgado, E.; Cuevas, M.T.; Nasr, M.; Abid, S.; Ben Hadj Kacem, M.A.; Benaissa Tiouiri, H.; Letaief, A.; Chakroun, M.; et al. Genetic Diversity of HIV-1 in Tunisia. AIDS Res Hum Retroviruses 2017, 33, 77–81. [Google Scholar] [CrossRef]
- Khamis, F.; Al Noamani, J.; Al Naamani, H.; Al-Zakwani, I. Epidemiological and Clinical Characteristics of HIV Infected Patients at a Tertiary Care Hospital in Oman. Oman Med J 2018, 33, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Alaoui, N.; El Alaoui, M.A.; El Annaz, H.; Farissi, F.Z.; Alaoui, A.S.; El Fahime, E.; Mrani, S. HIV-1 Integrase Resistance among Highly Antiretroviral Experienced Patients from Morocco. Intervirology 2019, 62, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Daw, M.A.; Daw, A.M.; Sifennasr, N.E.M.; Draha, A.M.; Daw, A.A.; Daw, A.A.; Ahmed, M.O.; Mokhtar, E.S.; El-Bouzedi, A.H.; Daw, I.M.; et al. Spatiotemporal analysis and epidemiological characterization of the human immunodeficiency virus (HIV) in Libya within a twenty five year period: 1993-2017. AIDS Res Ther 2019, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- Hamarsheh, O. HIV/AIDS in Palestine: A growing concern. Int J Infect Dis 2020, 90, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Amer, A.N.; Gaballah, A.; Emad, R.; Ghazal, A.; Attia, N. Molecular Epidemiology of HIV-1 Virus in Egypt: A Major Change in the Circulating Subtypes. Curr HIV Res 2021, 19, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, A.; Regmi, P.R.; van Teijlingen, E. HIV Epidemic in Libya: Identifying Gaps. J Int Assoc Provid AIDS Care 2021, 20, 23259582211053964. [Google Scholar] [CrossRef]
- Al- Qassab, H.S.; Utba, N. Human Immunodeficiency Virus Genotyping in Baghdad, Iraq. Indian Journal of Ecology 2022, 49, 318–323. [Google Scholar]
- Bakri, F.G.; Mukattash, H.H.; Esmeiran, H.; Schluck, G.; Storme, C.K.; Broach, E.; Mebrahtu, T.; Alhawarat, M.; Valencia-Ruiz, A.; M'Hamdi, O.; et al. Clinical, molecular, and drug resistance epidemiology of HIV in Jordan, 2019-2021: A national study. Int J Infect Dis 2024, 145, 107079. [Google Scholar] [CrossRef]
- El-Daly, M.M.; Zaher, K.A.; Zaki, E.A.; Bajrai, L.H.; Alhazmi, M.M.; Abdulhaq, A.; Azhar, E.I. Immunological and molecular assessment of HIV-1 mutations for antiretroviral drug resistance in Saudi Arabia. PLoS One 2024, 19, e0304408. [Google Scholar] [CrossRef]
- Shalaka, N. Retrospective study of the prevalence of acquired drug resistance after failed antiretroviral therapy in Libya. East Mediterr Health J 2024, 30, 470–480. [Google Scholar] [CrossRef]
- CDC. Emerging Infectious Diseases Article Types. Available online: https://wwwnc.cdc.gov/eid/article-types (accessed on 29 December 2024).
- Santoro, M.M.; Perno, C.F. HIV-1 Genetic Variability and Clinical Implications. ISRN Microbiol 2013, 2013, 481314. [Google Scholar] [CrossRef]
- Korber, B.; Gaschen, B.; Yusim, K.; Thakallapally, R.; Kesmir, C.; Detours, V. Evolutionary and immunological implications of contemporary HIV-1 variation. Br Med Bull 2001, 58, 19–42. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Hellmann, N.; Levy, J.A.; DeCock, K.; Lange, J. The spread, treatment, and prevention of HIV-1: evolution of a global pandemic. J Clin Invest 2008, 118, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- De Cock, K.M.; Jaffe, H.W.; Curran, J.W. The evolving epidemiology of HIV/AIDS. Aids 2012, 26, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Redondo, R.; Ozer, E.A.; Achenbach, C.J.; D'Aquila, R.T.; Hultquist, J.F. Molecular epidemiology in the HIV and SARS-CoV-2 pandemics. Curr Opin HIV AIDS 2021, 16, 11–24. [Google Scholar] [CrossRef]
- Layan, M.; Müller, N.F.; Dellicour, S.; De Maio, N.; Bourhy, H.; Cauchemez, S.; Baele, G. Impact and mitigation of sampling bias to determine viral spread: Evaluating discrete phylogeography through CTMC modeling and structured coalescent model approximations. Virus Evol 2023, 9, vead010. [Google Scholar] [CrossRef] [PubMed]
- Case, K.K.; Ghys, P.D.; Gouws, E.; Eaton, J.W.; Borquez, A.; Stover, J.; Cuchi, P.; Abu-Raddad, L.J.; Garnett, G.P.; Hallett, T.B. Understanding the modes of transmission model of new HIV infection and its use in prevention planning. Bull World Health Organ 2012, 90, 831–838a. [Google Scholar] [CrossRef]
- Sallam, M.; Alabbadi, A.M.; Abdel-Razeq, S.; Battah, K.; Malkawi, L.; Al-Abbadi, M.A.; Mahafzah, A. HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Quiñones-Mateu, M.E.; Avila, S.; Reyes-Teran, G.; Martinez, M.A. Deep sequencing: becoming a critical tool in clinical virology. J Clin Virol 2014, 61, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.C.; Kumar, S. Health inequalities and infectious disease epidemics: a challenge for global health security. Biosecur Bioterror 2014, 12, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Pellowski, J.A.; Kalichman, S.C.; Matthews, K.A.; Adler, N. A pandemic of the poor: social disadvantage and the U.S. HIV epidemic. Am Psychol 2013, 68, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Simms, C. Sub-Saharan Africa's HIV pandemic. Am Psychol 2014, 69, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Immonen, T.T.; Conway, J.M.; Romero-Severson, E.O.; Perelson, A.S.; Leitner, T. Recombination Enhances HIV-1 Envelope Diversity by Facilitating the Survival of Latent Genomic Fragments in the Plasma Virus Population. PLoS computational biology 2015, 11, e1004625. [Google Scholar] [CrossRef] [PubMed]
- Smyth, R.P.; Schlub, T.E.; Grimm, A.J.; Waugh, C.; Ellenberg, P.; Chopra, A.; Mallal, S.; Cromer, D.; Mak, J.; Davenport, M.P. Identifying recombination hot spots in the HIV-1 genome. J Virol 2014, 88, 2891–2902. [Google Scholar] [CrossRef] [PubMed]
- Schierup, M.H.; Hein, J. Consequences of recombination on traditional phylogenetic analysis. Genetics 2000, 156, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Posada, D.; Crandall, K.A. The effect of recombination on the accuracy of phylogeny estimation. Journal of molecular evolution 2002, 54, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; Posada, D. The effect of recombination on the reconstruction of ancestral sequences. Genetics 2010, 184, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Peña, A.C.; Faria, N.R.; Imbrechts, S.; Libin, P.; Abecasis, A.B.; Deforche, K.; Gómez-López, A.; Camacho, R.J.; de Oliveira, T.; Vandamme, A.M. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: performance evaluation of the new REGA version 3 and seven other tools. Infect Genet Evol 2013, 19, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Alageel, S.; Alsadhan, N.M.; Alkhaldi, G.; Alkasabi, R.; Alomair, N. Public perceptions of HIV/AIDS awareness in the Gulf Council Cooperation countries: a qualitative study. International Journal for Equity in Health 2024, 23, 269. [Google Scholar] [CrossRef]
- Delabre, R.M.; Moussa, A.B.; Villes, V.; Elkhammas, M.; Ouarsas, L.; Castro Rojas Castro, D.; Karkouri, M. Fear of stigma from health professionals and family/neighbours and healthcare avoidance among PLHIV in Morocco: results from the Stigma Index survey Morocco. BMC Public Health 2022, 22, 1705. [Google Scholar] [CrossRef]
- Abboud, S.; Seal, D.W.; Pachankis, J.E.; Khoshnood, K.; Khouri, D.; Fouad, F.M.; Heimer, R. Experiences of stigma, mental health, and coping strategies in Lebanon among Lebanese and displaced Syrian men who have sex with men: A qualitative study. Social Science & Medicine 2023, 335, 116248. [Google Scholar] [CrossRef]
- Mahajan, A.P.; Sayles, J.N.; Patel, V.A.; Remien, R.H.; Sawires, S.R.; Ortiz, D.J.; Szekeres, G.; Coates, T.J. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. Aids 2008, 22 Suppl 2, S67–79. [Google Scholar] [CrossRef]
- Kontomanolis, E.N.; Michalopoulos, S.; Gkasdaris, G.; Fasoulakis, Z. The social stigma of HIV-AIDS: society's role. HIV AIDS (Auckl) 2017, 9, 111–118. [Google Scholar] [CrossRef]
Figure 1.
Major challenges in HIV genetic diversity research in the Middle East and North Africa (MENA) region.
Figure 1.
Major challenges in HIV genetic diversity research in the Middle East and North Africa (MENA) region.
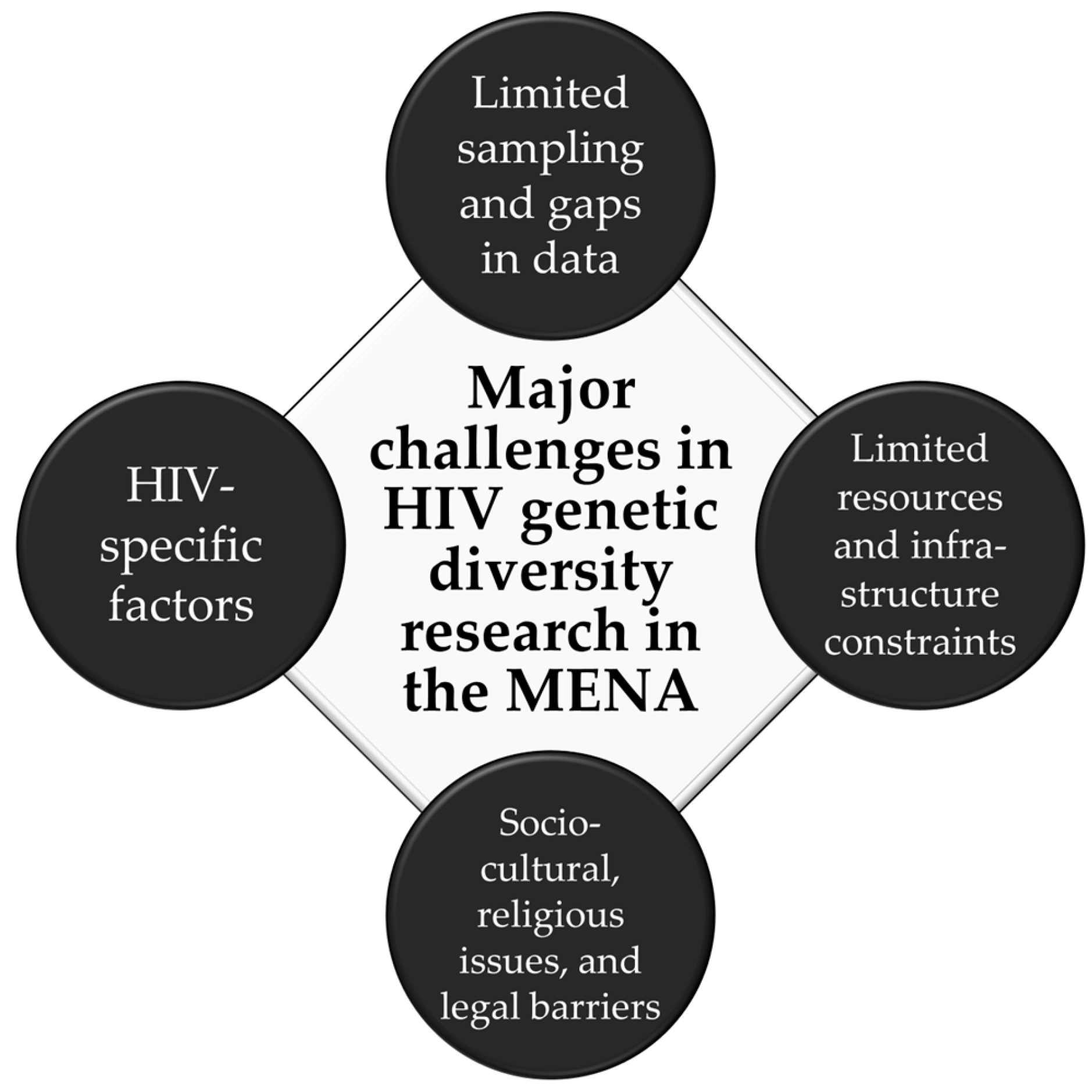
Figure 2.
Flow diagram on the record selection process for the review of HIV-1 genetic diversity research challenges in the Middle East and North Africa (MENA) region.
Figure 2.
Flow diagram on the record selection process for the review of HIV-1 genetic diversity research challenges in the Middle East and North Africa (MENA) region.
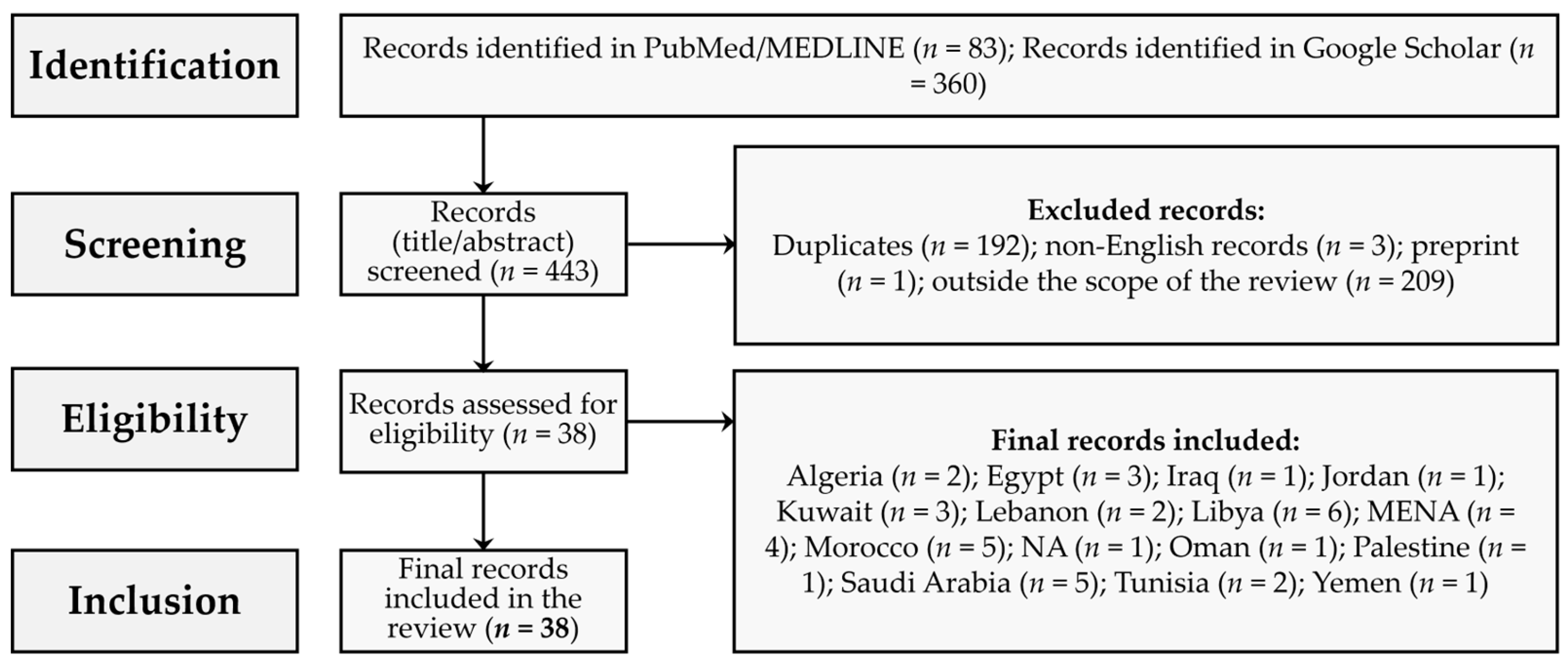
Figure 3.
Geographical distribution of the included records on HIV-1 genetic diversity challenges in the MENA region. The map was generated in Microsoft Excel, powered by Bing, © GeoNames, Microsoft, Navinfo, TomTom, Wikipedia. We are neutral with regard to jurisdictional claims in this map.
Figure 3.
Geographical distribution of the included records on HIV-1 genetic diversity challenges in the MENA region. The map was generated in Microsoft Excel, powered by Bing, © GeoNames, Microsoft, Navinfo, TomTom, Wikipedia. We are neutral with regard to jurisdictional claims in this map.
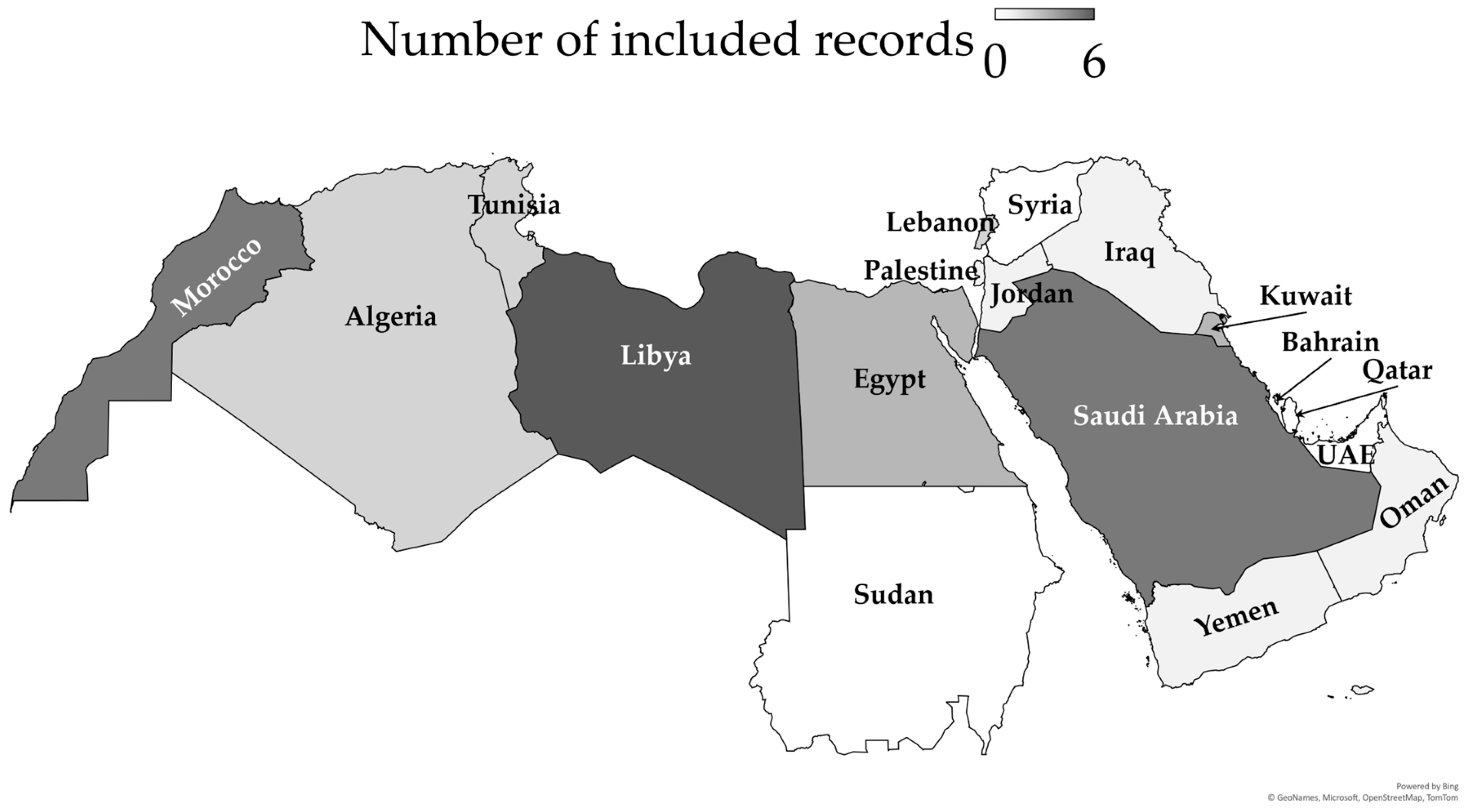
Figure 4.
Annual distribution of HIV-1 sequences in the included records in the Middle East and North Africa (MENA) region from 1998 to 2024.
Figure 4.
Annual distribution of HIV-1 sequences in the included records in the Middle East and North Africa (MENA) region from 1998 to 2024.
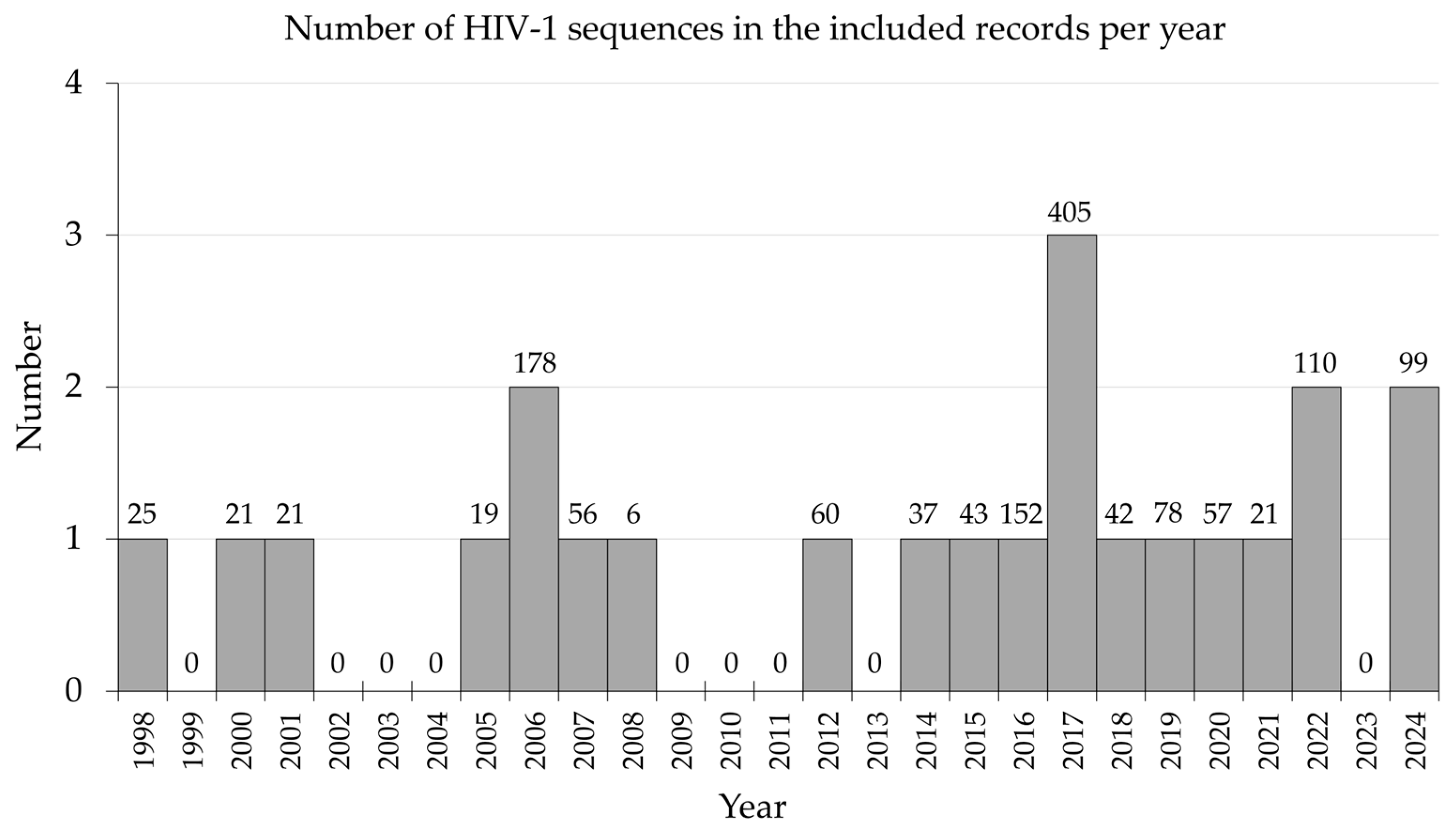
Figure 5.
The process of socio-cultural barriers impact on assessment of HIV-1 genetic diversity in the Middle East and North Africa (MENA) region. MSM: Men who have sex with men; FSWs: Female sex workers; IDUs: Injection drug users.
Figure 5.
The process of socio-cultural barriers impact on assessment of HIV-1 genetic diversity in the Middle East and North Africa (MENA) region. MSM: Men who have sex with men; FSWs: Female sex workers; IDUs: Injection drug users.
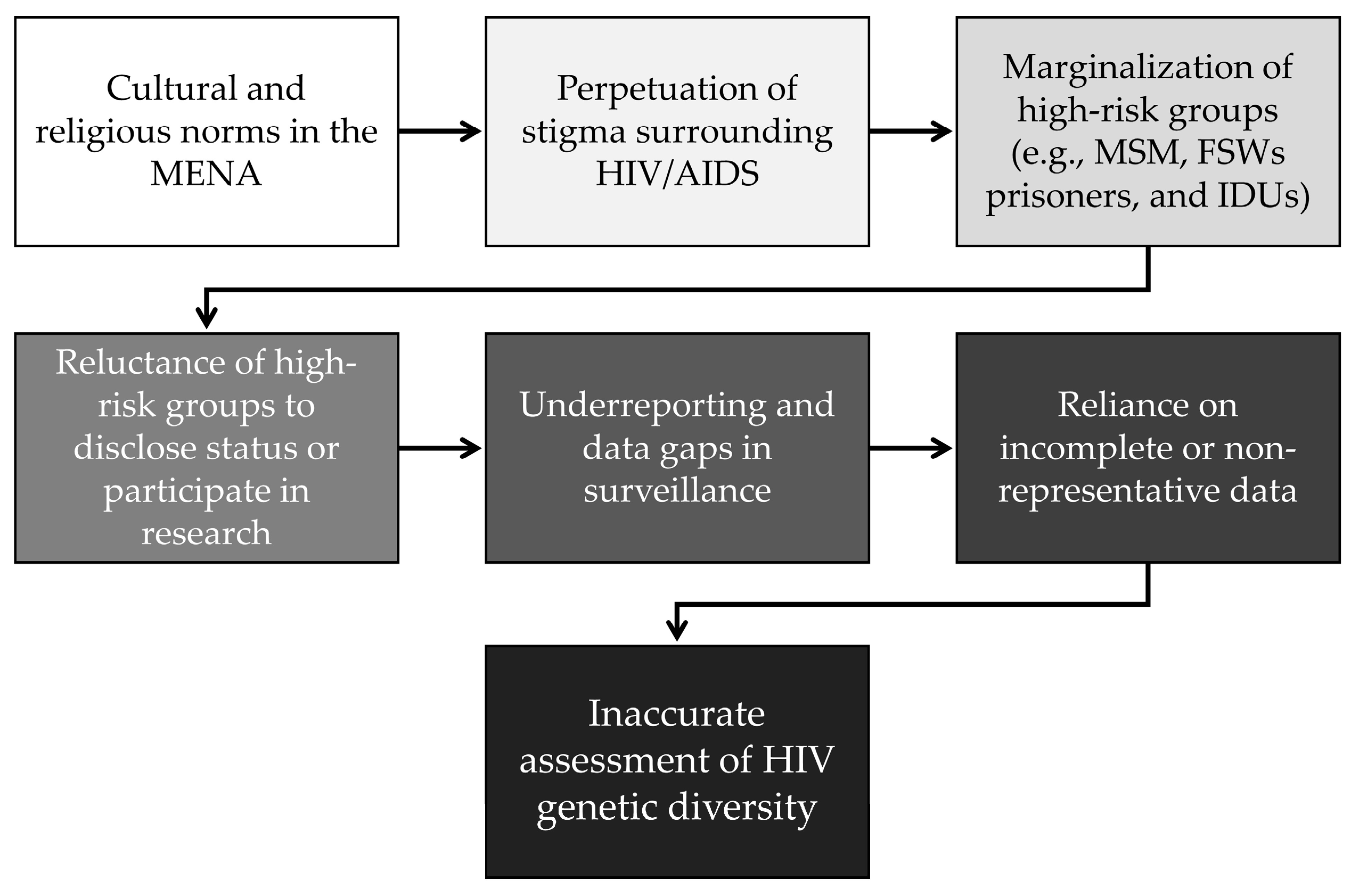

Table 1.
Summary of the included records (n = 38).
| Author(s), Year | Country/Region | Type of article |
|---|---|---|
| Pieniazek et al., 1998 [117] | Lebanon | Dispatch 2 |
| El Sayed et al., 2000 [118] | Egypt | Original article |
| Ben Halima et al., 2001 [119] | Tunisia | Brief Report |
| Elharti et al., 2002 [120] | Morocco | Review |
| Saad et al., 2005 [121] | Yemen | Sequence note |
| Bouzeghoub et al., 2006 [122] | Algeria | Sequence note |
| de Oliveira et al., 2006 [123] | Libya | Brief communication |
| Badreddine et al., 2007 [124] | Saudi Arabia | Original article |
| Bagasra et al., 2007 [125] | Libya | Reply |
| Yamaguchi et al., 2008 [126] | Saudi Arabia | Other |
| Mumtaz et al., 2010 [72] | MENA 1 | Systematic review |
| Mumtaz & Abu-Raddad, 2011 [127] | MENA | Review |
| Mumtaz et al., 2011 [30] | MENA | Systematic review |
| Akrim et al., 2012 [70] | Morocco | Original article |
| Kouyoumjian et al., 2013 [128] | Morocco | Systematic review |
| Mumtaz et al., 2013 [129] | Morocco | Original article |
| Mokhbat et al., 2014 [130] | Lebanon | Original article |
| Chehadeh et al., 2015 [62] | Kuwait | Original article |
| Abdellaziz et al., 2016 [131] | Algeria | Sequence note |
| Chehadeh et al., 2017 [63] | Kuwait | Original article |
| Daw et al., 2017 [132] | Libya | Original article |
| El Moussi et al., 2017 [133] | Tunisia | Original article |
| Sallam et al., 2017 [32] | MENA | Original article |
| Chehadeh et al., 2018 [64] | Kuwait | Original article |
| Khamis et al., 2018 [134] | Oman | Original article |
| Alaoui et al., 2019 [135] | Morocco | Original article |
| Daw et al., 2019 [136] | Libya | Original article |
| Giovanetti et al., 2020 [17] | North Africa | Review |
| Zaki et al., 2020 [66] | Jazan, Saudi Arabia | Observational Study |
| Hamarsheh, 2020 [137] | Palestine | Short communication |
| Amer et al., 2021 [138] | Egypt | Original article |
| Hamidi et al., 2021 [139] | Libya | Review |
| Al- Qassab & Utba, 2022 [140] | Iraq | Original article |
| Gaballah et al., 2022 [65] | Egypt | Original article |
| Al-Mozaini et al., 2023 [68] | Saudi Arabia | Review |
| Bakri et al., 2024 [141] | Jordan | Original article |
| El-Daly et al., 2024 [142] | Saudi Arabia | Original article |
| Shalaka, 2024 [143] | Libya | Original article |
1 MENA: Middle East and North Africa; 2 Dispatch: “updates on infectious disease trends and research that include descriptions of new methods for detecting, characterizing, or subtyping new or reemerging pathogens.” [144].
Table 2.
The MENA records which analyzed HIV-1 molecular sequences, sequencing technique, and the clinical data availability.
Table 2.
The MENA records which analyzed HIV-1 molecular sequences, sequencing technique, and the clinical data availability.
| Author(s) | YEAR | Country/Region | Sample size of HIV-1 sequences | Clinical data | Sequencing technique |
|---|---|---|---|---|---|
| El Moussi et al., 2017 [133] | 2017 | Tunisia | 193 | Partial data were available | Sanger dideoxy sequencing |
| Daw et al., 2017 [132] | 2017 | Libya | 159 | Partial data were available | Not mentioned |
| Abdellaziz et al., 2016 [131] | 2016 | Algeria | 152 | Data were absent | Sanger dideoxy sequencing |
| Bouzeghoub et al., 2006 [122] | 2006 | Algeria | 134 | Data were absent | Not mentioned |
| Alaoui et al., 2019 [135] | 2019 | Morocco | 78 | Partial data were available | Sanger dideoxy sequencing |
| Al- Qassab & Utba, 2022 [140] | 2022 | Iraq | 65 | Partial data were available | Sanger dideoxy sequencing |
| Akrim et al., 2012 [70] | 2012 | Morocco | 60 | Full data were available | Sanger dideoxy sequencing |
| Zaki et al., 2020 [66] | 2020 | Jazan, Saudi Arabia | 57 | Partial data were available | Sanger dideoxy sequencing |
| Badreddine et al., 2007 [124] | 2007 | Saudi Arabia | 56 | Full data were available | Sanger dideoxy sequencing |
| El-Daly et al., 2024 [142] | 2024 | Saudi Arabia | 56 | Partial data were available | Sanger dideoxy sequencing |
| Chehadeh et al., 2017 [63] | 2017 | Kuwait | 53 | Data were absent | Sanger dideoxy sequencing |
| Gaballah et al., 2022 [65] | 2022 | Alexandria, Egypt | 45 | Data were absent | Sanger dideoxy sequencing |
| de Oliveira et al., 2006 [123] | 2006 | Libya | 44 | Partial data were available | Sanger dideoxy sequencing |
| Chehadeh et al., 2015 [62] | 2015 | Kuwait | 43 | Partial data were available | Sanger dideoxy sequencing |
| Bakri et al., 2024 [141] | 2024 | Jordan | 43 | Partial data were available | Next-generation sequencing |
| Chehadeh et al., 2018 [64] | 2018 | Kuwait | 42 | Partial data were available | Sanger dideoxy sequencing |
| Mokhbat et al., 2014 [130] | 2014 | Lebanon | 37 | Partial data were available | Sanger dideoxy sequencing |
| Pieniazek et al., 1998 [117] | 1998 | Lebanon | 25 | Full data were available | Sanger dideoxy sequencing |
| El Sayed et al., 2000 [118] | 2000 | Egypt | 21 | Full data were available | Sanger dideoxy sequencing |
| Ben Halima et al., 2001 [119] | 2001 | Tunisia | 21 | Partial data were available | Sanger dideoxy sequencing |
| Amer et al., 2021 [138] | 2021 | Egypt | 21 | Partial data were available | Sanger dideoxy sequencing |
| Saad et al., 2005 [121] | 2005 | Yemen | 19 | Partial data were available | Sanger dideoxy sequencing |
| Yamaguchi et al., 2008 [126] | 2008 | Saudi Arabia | 6 | Data were absent | Sanger dideoxy sequencing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



