
Submitted:
23 December 2024
Posted:
24 December 2024
You are already at the latest version
Abstract
Systemic lupus erythematosus (SLE) is a systemic autoimmune disease affecting all organ systems. The disease preferentially affects females of childbearing age. It runs a variable course. It may run a mild course which may never lead to severe disease and manifestations from critical organ systems. However, it may also run an undulating course with periods of mild and severe disease. It may run as a mild disease quickly deteriorating to severe disease affecting multiple organ systems. Various immune pathways related both to the innate and adaptive immune response are involved in the pathogenesis of SLE. Various drugs have been developed targeting cellular and mo-lecular targets in these pathways. Interferons are involved in the pathogenesis of SLE and various drugs have been developed to target this pathway. T and B lymphocytes are involved in the pathophysiology of SLE. Various treatment modalities targeting cellular targets are available for the treatment of SLE. These include biologic agents targeting B lymphocytes. However, some patients have disease refractory to these treatment modalities. For these patients cell-based therapies may be used. Hematopoietic stem cell transplantation involving autologous cells is an option in the treatment of refractory SLE. Mesenchymal stem cells are also applied in the treatment of SLE. Chi-meric antigen receptor (CAR)-T cell therapy is a novel treatment also used in SLE management. This novel treatment method holds major promise for the management of autoimmune diseases and in particular SLE. Major hurdles to be overcome are the logistics involved, as well as the need for specialized facilities. This review focuses on novel treatment modalities in SLE which are targeting cellular and molecular targets in the immune system.
Keywords:
systemic lupus erythematosus
; B lymphocyte
; stem cell transplantation
; mesenchymal cell transplantation
; CAR T – cell therapy
1. Introduction
Systemic lupus erythematosus (SLE) is the prototype of systemic autoimmune diseases. The disease affects all organ systems and runs a variable course. It may run as a mild disease with periods of exacerbation and remission. It may affect critical organ systems such as the kidneys and the central nervous system. The disease may also run a very mild course. In such cases the diagnosis and careful follow-up of the disease with the respective management is critical.
The exact etiology and pathophysiology of the disease remains elusive. It appears however that environmental agents act and induce the disease. Such factors are viruses and ultraviolet light. Such factors induce activation of the immune system and the development of an autoimmune response. Antibodies against intranuclear particles are formed, such as antinuclear antibodies, anti-ds DNA antibodies, anti-SSA (Ro), anti-SSA (La) antibodies and anti-Smith antibodies. Antibodies form complexes with the respective antigens and are deposited in the respective organ systems and cause disease. In lupus the clearance pathways of the organism are defective. Thus, apoptotic cells are not properly cleared. Antibody antigen complexes are not properly cleared. In patients with severe lupus disorders of hematopoietic progenitor cells have been described, including increased proliferation, differentiation activation of cytokines and chemokines leading to differentiation towards myeloid cells [1]. Increased risk of myelodysplastic syndrome has been observed in patients with autoimmune diseases including SLE [2], indicating shared genetic susceptibility between myelodysplastic syndrome and SLE. The disease was managed in the past by the administration of corticosteroids in various dose schedules. Various modes of treatment have been applied over the years in cases of severe SLE. As biological drugs emerged a biologic agent was applied in the management of SLE, namely belimumab. However, recently modes of treatment, applications of modern technology entered the field of SLE treatment (figure 1). These treatment modalities will be discussed in this paper. In particular, hematopoietic stem cell transplantation, mesenchymal stem cell transplantation and CAR-T-cell therapy will be discussed.
2. Stem Cell Transplantation
The application of modern disease modifying modes of treatment has significantly improved outcome in autoimmune diseases [3]. Despite these therapeutic improvements and innovations a fraction of patients is refractory to both conventional and innovative modes of treatment [4,5]. Cure or long-term disease remission is not common [6,7]. Hematopoietic stem cell transplantation has been applied in the management of autoimmune diseases since the last decade of the twentieth century [8,9,10,11,12,13]. Most of the cases in which it has been applied are cases of multiple sclerosis [9,14,15,16,17], systemic sclerosis [11,18,19], Crohn’s disease [20,21,22,23] and only a minority of the cases are cases of SLE [24,25,26,27,28]. It is thought that the conditioning regimen before the procedure and the subsequent infusion of the stem cells may reset the immune system as it is considered to eradicate autoreactive immune cells and allows the generation of a novel immune system which is self-tolerant [29,30]. Hematopoietic stem cell transplants, as shown in a review published in 2017, are mainly autologous [31], while allogeneic stem cell transplants are performed almost exclusively in pediatric patients. Almost two thirds of autologous stem cell transplants are delivered in patients with multiple sclerosis and systemic sclerosis. This trend is on the rise.
Hematopoietic stem cell transplantation is a form of cellular immunotherapy [27,32,33,34]. This treatment modality involves the transfusion of hematopoietic stem cells to the recipient in order to replace the patient’s hematopoietic stem cells. Stem cell transplantation has been effectively and successfully applied in the treatment of malignant diseases [35,36]. However, it has been also applied in the treatment of autoimmune conditions. Based on the fact that systemic lupus erythematosus is a disease characterized by disorders of stem cells [37], stem cell transplantation has been applied in the treatment of SLE in cases of severe or treatment refractory disease. Stem cell transplantation is a procedure performed in multiple steps. These steps include collection of the stem cells, conditioning of the recipient with a proper regimen followed by infusion of the stem cell transplant [38]. The aim is the creation of a novel hematopoietic and a novel immune system.
Hematopoietic stem cell transplantation has been applied in patients with hematologic diseases [35]. Early observations of remission of concurrent autoimmune disease in patients with hematologic diseases undergoing hematopoietic stem cell transplantation led to the application of hematopoietic stem cell transplantation in patients with severe autoimmune diseases [39,40,41]. Hematopoietic stem cell transplantation has been applied in patients with multiple sclerosis. It involves immunoablative treatment followed by autologous hematopoietic stem cell transplantation and has been found to have positive results [9]. Autologous hematopoietic stem cell transplantation has also been applied in patients with systemic sclerosis and has been found to improve lung function in patients with systemic sclerosis [42,43]. It has been suggested that autologous stem cell transplantation might be an option for progressive systemic sclerosis if major organ failure is imminent. Crohn’s disease has also been treated with autologous stem cell transplantation and it may be an option for treatment resistant disease [44].
Hematopoietic stem cell transplantation has been used in patients with SLE [24]. Patients with disease refractory to standard and biologic treatment are candidates for this form of treatment. In a review article published in 2017 the use of hematopoietic stem cell transplantation has been reviewed [31]. Hematopoietic stem cell transplantation had been applied in 279 patients with SLE, including 54 patients who also fulfilled the criteria of antiphospholipid syndrome. In the majority of the studies an improvement in disease control as assessed by SLEDAI or time free from disease was noted. In one of the studies included in the abovementioned review, no net benefit was found from hematopoietic stem cell transplantation as compared to immunosuppression. In five patients who also had antiphospholipid syndrome antiphospholipid antibodies were negative after stem cell transplantation while 73% of the patients with SLE and antiphospholipid syndrome were able to discontinue coagulation. Infections were observed in 30.8% of the patients who were subjected to hematopoietic stem cell transplantation, while 3 patients succumbed to the infection. An annual incidence of infections of 11.9% was observed in the SLE patients subjected to hematopoietic stem cell transplantation. Autologous hematopoietic stem cell transplantation has been complicated by the appearance of aplastic anemia [45]. Secondary autoimmune diseases may also complicate hematopoietic stem cell transplantation [46,47,48]. Infections are a major adverse effect of hematopoietic stem cell transplantation [49].
Allogeneic stem cell transplantion in SLE has been fraught with adverse effects and it may be reserved only for patients with concurrent malignant disease [26]. Autologous stem cell transplantation has been explored in a large trial with a group of 339 patients. In this trial a disease-free survival of 50-60% at 5 years was observed [50]. Relapse risk increased with longer follow-up. The conditioning regimen before transplantation has been shown to affect the rate of remission, as a conditioning regimen of cyclophosphamide, thymoglobulin and rituximab is related with a better remission rate [50].
Hematopoietic stem cell transplantation is an option in the treatment of SLE, in severe cases refractory to standard treatment regimens. However, the experience so far shows that there are major difficulties to be overcome before it enters widespread clinical practice. Hematopoietic stem cell transplantation is characterized by mortality related to the transplant procedure and in long-term follow-up with relapse of the underlying disease. In a study [51] hematopoietic stem cell transplantation was related with relapse in one-third of the recipients and mortality more than 10% related to the transplantation. In a study in which hematopoietic stem cell transplantation was performed to treat lupus nephritis a mortality of 5% was noted, the disease – free survival at 5 years was 53% and the rate of relapse was 27% [52]. As noted above, infections may occur including cytomegalovirus infection, bacterial and/or fungal infections, allergic reactions, bone pain and heart failure. Secondary emergence of autoimmune diseases is also a problem to be expected [48,53].
3. Mesenchymal Stem Cell Transplantation
Mesenchymal stem cells are adult stem cells which harbor the innate ability to self-renew and further differentiate into various types of cells. Mesenchymal stem cell treatment has been described as an option for the management of various diseases of autoimmune etiology. Such diseases amongst others are rheumatoid arthritis, type 1 diabetes mellitus and multiple sclerosis. [54]. The application of mesenchymal stem cell transplantations as a treatment for SLE has been investigated [55,56,57].
Sources for mesenchymal stem cells include the bone marrow, umbilical cord and adipose tissue. The procedure involves the isolation of mesenchymal stem cells, cell expansion and infusion In the patient. Prior chemotherapy is not required. The availability of stem cells, the low rejection rate as well as the absence of necessity for prior chemotherapy are advantages of this treatment modality for SLE patients refractory to standard treatment. Mesenchymal stem cells when transplanted regulate adaptive and immune response. The cells may downregulate inflammation and alleviate autoimmunity [58]. Findings from various studies suggest that mesenchymal stem cell transplantation is safe and has shown encouraging results as far as disease activity is concerned. However, it is not a curative option [59]. The procedure is performed with allogeneic mesenchymal stem cells and is not yet standardized.
4. CAR-T Cell Therapy
Chimeric antigen receptor T cell therapy is a form of technologically advanced treatment which has been applied successfully for the treatment of different types of B cell hematologic neoplasms. It was suggested that it might also be applied for the treatment of severe authoimmune disease. SLE is managed by the administration of various agents targeting B lymphocytes. However, cases of severe disease not responding to treatment or cases with severe adverse effects to this type of treatment exist. In these cases it was thought that chimeric antigen receptor T cell therapy might be applied.
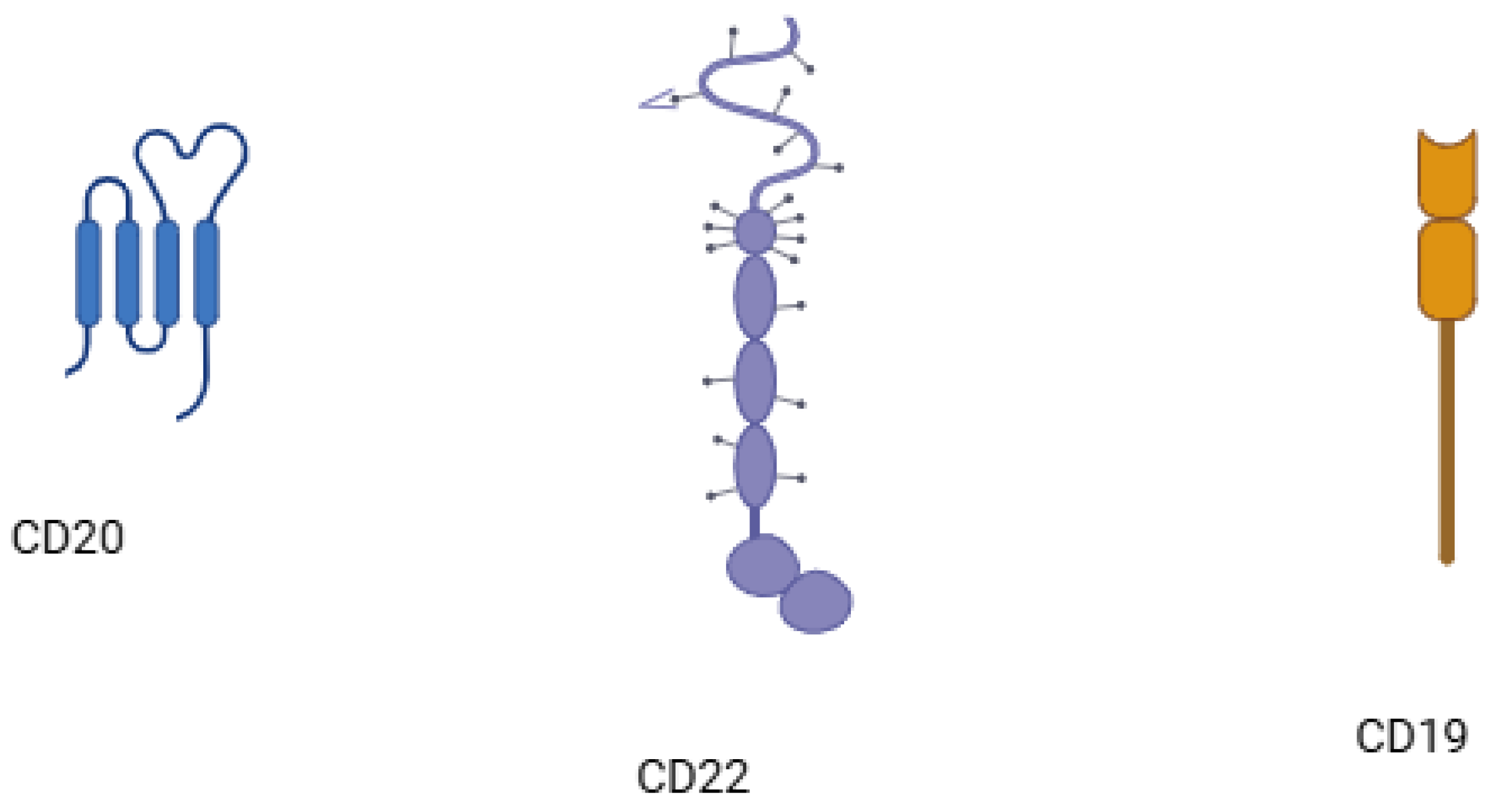
B cells are critical for the defense of the immune system against pathogens through various mechanisms, which include antibody production, handling of antigen presentation, T-cell activation and subsequent differentiation and the production of cytokines [60]. B lymphocytes have an antigen receptor, the B-cell receptor. Once the B-cell receptor recognizes an antigen the B-cell is activated and undergoes proliferation and subsequent differentiation leading to the secretion of specific antibodies [61]. B cells with autoreactive properties undergo a process of regulation during early development leading to central tolerance and a process of regulation during later stages of maturation in peripheral lymphoid organs leading to peripheral tolerance. A disorder in central tolerance leads to the development of autoimmune and some immunodeficiency disorders [61]. Cell surface markers such as CD19 and CD20 are expressed on B cells depending on the stage of maturation, CD19 observed on B cells from the stage of pre-B cell to plasmablast [60,62].
B lymphocytes are critically involved in SLE pathogenesis. Epstein-Barr virus has been implicated in the pathogenesis of SLE [63] and the virus infects B lymphocytes where its genome may persist as an episome and may shift between a latent and a lytic phase [64]. Hence, modes of treatment targeting B lymphocytes (figure 2) have shown beneficial effects in the treatment of SLE [65]. Modes of treatment targeting B cells utilize either inhibition of B cells via blockade of BAFF (B cell activating factor and APRIL (A-proliferation inducing ligand) [66] and B cells depletion through the application of monoclonal antibodies against B cell surface molecules, namely CD19, CD20 or CD22 [67,68]. Rituximab, an anti-CD20 monoclonal antibody, ocrelizumab, another anti-CD20 monoclonal antibody, obinutuzumab, a fully humanized anti-CD20 monoclonal antibody and epratuzumab, a recombinant humanized anti-CD22 monoclonal antibody have been used in lupus treatment with varied success. Rituximab induces B cell depletion via the CD20 molecule [69]. However, tissue resident B cells [70] as well as cells not expressing the CD20 molecule evade depletion, leading to incomplete response to treatment [71,72]. Ocrelizumab has been administered in lupus nephritis with partial success, however its administration led to serious infections [73]. Obinutuzumab has been administered to patients with lupus [74], renal and non-renal, unresponsive to second line rituximab, and to patients with lupus nephritis [75]. Epratuzumab, a recombinant monoclonal antibody targeting the CD22 molecule (figure 3) on B cells has also been administered to lupus patients [76]. Belimumab was the first biologic agent approved for the treatment of SLE [77]. It inhibits BAFF, which is important for B lymphocyte survival [78]. Belimumab improved disease activity, flare rates [79] and was effective in renal lupus [80]. Tabalumab and blisibimod, are BAFF inhibitors which have also been applied in lupus [81,82,83]. Atacicept, which aims to achieve the inhibition of both APRIL and BAFF, has also been applied in lupus cases with efficacy and no serious adverse effects [84,85,86]. Cases refractory to this type of treatment exist as well as cases which respond, exhibiting however, adverse effects.
The therapeutic approaches applied so far suggest that targeting the B lymphocyte is a fruitful approach in the management of SLE. In addition, this approach so far has been fraught with the emergence of refractory cases as well as adverse effects. Thus, novel methods targeting the B lymphocyte in the treatment of SLE are investigated. The successful application of chimeric antigen receptor T lymphocytes in the treatment of B cell lymphomas has led to the observation that coexistent autoimmune diseases improved [87,88,89]. Thus, the application of chimeric antigen receptor T lymphocytes engineered to target the CD19 molecule on B lymphocytes was initiated. The aim was to target the CD19 molecule on the B lymphocyte in SLE patients and the subsequent depletion of B lymphocytes, suppression of the autoimmune process and disease remission. The application of anti-CD19 chimeric antigen receptor T lymphocytes in a murine model of SLE indicated that this treatment modality had a preventive as well as a therapeutic efficacy as far as SLE was concerned [90]. The anti-CD19 chimeric antigen receptor T cell treatment was administered to a female patient with active lupus nephritis refractory to treatment. The treatment led to seroconversion, i.e. anti-dsDNA antibodies were negative post-treatment and complement levels increased to normality [91]. Similar results were obtained by Taubmann et al [92]. In a larger trial involving 5 patients, 4 female and 1 male, with severe refractory SLE Mackensen et al [93] administered anti-CD19 chimeric antigen receptor T lymphocytes. B cell depletion occurred in all patients following treatment along with drug free remission in all eight patients. The B cell population re-emerged in the course of time following treatment. However, the re-emerging B cell population had a different non-pathogenic phenotype, indicating an immune system reset [93]. In another series of SLE patients the administration of chimeric antigen receptor T cell treatment led to disease remission [94]. A disease activity index (SLEDAI) of 0 was observed following treatment in the lupus cohort. Anti-CD19 chimeric antigen receptor T cell therapy was administered to a 15-year old female patient with lupus nephritis who was on haemodialysis [95]. The patient improved remarkably as creatinine levels decreased to normal, glomerular filtration rate increased, proteinuria improved and seroconversion was observed. The patient was not in need of hemodialysis following CAR-T cell treatment and anti-hypertensive treatment was withdrawn. A double-target CAR-T cell infusion harboring both BCMA and CD19 molecules on CD-19 B cells and plasma cells with BCMA surface antigen has been applied in patients with SLE and lupus nephritis in an open-label clinical trial [96]. The severity of lupus nephritis is related to increased expression of BCMA - B cell maturation antigen- in plasma cells with a long half-life [97,98]. Two patients suffering both from SLE and lymphoma achieved medication free remission [96]. A group of nine patients suffering from lupus nephritis had symptom and medication free remission with a follow-up post infusion of up to 46 months. Complement levels increased to normal, renal function and SLE disease activity index improved. Treatment was well tolerated and the cytokine release syndrome observed was mild. B cell receptor deep sequencing performed post infusion revealed a complete immune reset. By using specific molecular methods it has further been shown, that selective B cell depletion via CAR-T cell therapy reduces interferon signature in SLE [99]. CAAR-T cell therapy is a further adaptation of CAR-T cell therapy, which aims to deplete B cells producing specific sets of pathogenic antibodies and is now further tested in neuroimmunology [100]. CAR-T-cell therapy is accompanied by deep B cell depletion as the infused cells act autonomously, as opposed to monoclonal antibodies against B cells, which require natural killer cells, macrophages or the complement to achieve their goal [69]. CAR therapy with alternative cells such as natural killer cells or macrophages is being evaluated [101,102].
CAR T cell therapy is a novel method, initially applied successfully in patients with B cell lymphoma and leukemia [103,104,105,106]. The treatment is accompanied by toxicity, including cytokine release syndrome (CRS) alternatively cytokine associated cytotoxicity [107], immune effector-cell associated neurotoxicity syndrome (ICANS) [108], anemia, leukopenia, thrombocytopenia [109], immunogenicity leading to anaphylaxis [110], and oncogenesis [111]. CRS is an inflammatory response which results from the activation of T lymphocytes. It complicates CAR-T-cell therapy in a proportion of 42% to 93% of patients subjected to this type of treatment. It is an inflammatory response which is due to the activation of T lymphocytes and the release of IL-6 [107]. CRS is considered as a consequence of the efficacy of CAR T cell infusion, however, it may be associated with undesirable outcomes [112,113,114]. CRS may manifest itself in the initial 1 to 4 days of CAR-T-cell administration and may vary in severity. Severe episodes tend to occur earlier after the infusion. Levels of laboratory indicators of acute inflammatory response such as C-reactive protein and ferritin are elevated in parallel with cytokine levels, including IL-6 and IFN-γ [115]. CRS may vary in severity from mild, with only fever and myalgia, to severe manifesting with cardiorespiratory dysfunction [116]. CRS has been classified into five levels of severity [112]. CRS may need only symptomatic treatment. However, more severe cases may require the administration of tocilizumab to manage [117,118]. ICANS is another complication of CAR-T-cell therapy and may follow CRS, manifesting with delirium, seizures and aphasia. Its severity is not related to CRS severity. Corticosteroids is the best treatment modality for ICANS in the context of CAR-T-cell treatment [114]. Immunogenicity leading to allergic reactions may also be observed [110,119]. CAR-T-cells are generated by the genomic intregration of a viral vector into the genome of the recipient. Therefore, long-term oncogenicity is a concern leading to advice for long-term follow-up of the recipient for any malignancy. Secondary malignancies after CAR-T-cell treatment have been described [111,120].
CAR-T-cell therapy may be autologous or heterologous, meaning that the infused cell line may be derived from the patient’s own T lymphocytes or from the lymphocytes of an unrelated donor. Autologous CAR-T-cell therapy can avoid the adversity of immunological rejection, but it requires a lengthy production and this may be critical in severely ill patients. However, the adverse effects of host versus graft and graft versus host reaction may be avoided [121]. CAR-T-cell therapy involving a rapid manufacturing protocol has been applied successfully in patients with SLE [122,123]. Sequential lymph node biopsy performed before and after CD1-9 CAR T cell therapy in patients with autoimmune rheumatic diseases including a group of patients with SLE indicated complete B cell depletion in the lymph nodes, while T cells, macrophages and plasma cells remained intact [124].
Treatment with CAR T cells offers a possibility of lengthy sustained remission in cases of SLE refractory to conventional modes of treatment such as treatment with biological agents or monoclonal antibodies targeting B lymphocytes. This treatment modality is characterized by cumbersome logistics, requires specialized facilities and is accompanied by adverse effects such as cytokine release syndrome. In addition, CAR T cells are not readily available and require a quite lengthy period of production of about 4 weeks, as opposed to monocolonal antibodies or biological agents which are ready to be administered. It should be noted that protocols with shorter production period as well as allogeneic CAR T cell products are tested [125]. CAR T cell therapy is investigated as it holds the potential to be a one-stop therapeutic procedure to induce permanent remission in SLE patients, refractory to standard treatment modalities. Thus, CD-19 targeted CAR-T cells from a brave new world [126] may be the future in the treatment of refractory lupus [127].
5. Conclusions
The prototype systemic autoimmune disease SLE may be considered a stem cell disease and B lymphocytes are critically involved in its pathogenesis. Various drugs are available for the treatment of SLE. These include immunomodulating agents, corticosteroids, monoclonal antibodies targeting B lymphocytes and biological agents. However, cases refractory to these treatment modalities as well as adverse effects necessitated the evolution of alternative modes of treatment. Stem cell transplantation is an alternative treatment modality for SLE. Stem cell transplantation has been applied successfully in the treatment of cancer. During application in patients with cancer it was noted that stem cell transplantation may lead to remission a co-existing autoimmune condition. Thereafter, hematopoietic stem cell transplantation was applied in patients with SLE. Autologous hematopoietic stem cell transplantation has been the procedure of choice in patients with SLE, allogeneic stem cell transplantation being reserved only for pediatric cases. Remission and in some cases long-term remission has been achieved following stem cell transplantation. However, infections in some cases fatal, emerged. In addition, secondary autoimmune phenomena complicated the procedure. Mesenchymal cell transplantation is another stem cell procedure which has been tested in SLE. The procedure of choice was allogeneic mesenchymal cell transplantation. However, the procedure did not enter clinical practice successfully. CAR-T-cell therapy was applied successfully in patients with hematologic malignancies such as leukemia, lymphoma and myeloma. CAR-T cell therapy targeting CD19 on B lymphocytes proved successful in cases with hematologic malignancies. In addition, it was noted that autoimmune conditions went into remission. As B cell targeted monoclonal antibodies proved therapeutically successful, targeting the B lymphocyte with CD19 targeted CAR-T cells was a promising approach for the treatment of refractory to standard treatment SLE patients. The procedure had already been applied successfully for the treatment of multiple sclerosis. Thus, CD19 targeted CAR T-cell therapy was administered to patients with SLE. The procedure was followed by long-lasting remission and the adverse events such as cytokine release syndrome and immune effector-cell neurotoxicity syndrome were manageable. CAR-T cell therapy with alternative targets as well as CAR therapy with alternative cell types is being investigated. CAR-T cell therapy with preparations which are ready to be administered to the recipient is also under research. In conclusion, cell therapy is an option for refractory to standard treatment SLE. CAR-T-cell therapy holds major promise for the achievement of sustained remission over older methods such as hematopoietic stem cell transplantation or mesenchymal cell transplantation.
References
- Grigoriou, M.; Banos, A.; Filia, A.; Pavlidis, P.; Giannouli, S.; Karali, V.; Nikolopoulos, D.; Pieta, A.; Bertsias, G.; Verginis, P.; et al. Transcriptome reprogramming and myeloid skewing in haematopoietic stem and progenitor cells in systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 79, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Boddu, P.C.; Zeidan, A.M. Myeloid disorders after autoimmune disease. Best Pr. Res. Clin. Haematol. 2019, 32, 74–88. [Google Scholar] [CrossRef] [PubMed]
- (Pdwp), O.B.O.T.E.A.D.W.P. (.A.P.D.W.P.; A Snowden, J.; Saccardi, R.; Allez, M.; Ardizzone, S.; Arnold, R.; Cervera, R.; Denton, C.; Hawkey, C.; Labopin, M.; et al. Haematopoietic SCT in severe autoimmune diseases: updated guidelines of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2011, 47, 770–790. [Google Scholar] [CrossRef]
- Vasconcelos, C.; Kallenberg, C.; Shoenfeld, Y. Refractory disease in autoimmune diseases. Autoimmun. Rev. 2011, 10, 653–654. [Google Scholar] [CrossRef]
- Marinho, A.; Alves, J.D.; Fortuna, J.; Faria, R.; Almeida, I.; Alves, G.; Correia, J.A.; Campar, A.; Brandão, M.; Crespo, J.; et al. Biological therapy in systemic lupus erythematosus, antiphospholipid syndrome, and Sjögren’s syndrome: evidence- and practice-based guidance. Front. Immunol. 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C.; Allaart, C.F.; Amoura, Z.; Bruce, I.N.; Cagnoli, P.C.; Chatham, W.W.; Clark, K.L.; Furie, R.; Groark, J.; Urowitz, M.B.; et al. Efficacy and safety of sequential therapy with subcutaneous belimumab and one cycle of rituximab in patients with systemic lupus erythematosus: the phase 3, randomised, placebo-controlled BLISS-BELIEVE study. Ann. Rheum. Dis. 2024, 83. [Google Scholar] [CrossRef]
- Nikolopoulos, D.; Lourenço, M.H.; Depascale, R.; Triantafyllias, K.; Parodis, I. Evolving Concepts in Treat-to-Target Strategies for Systemic Lupus Erythematosus. Mediterr. J. Rheumatol. 2024, 35, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.; Greco, R.; Snowden, J.A. Hematopoietic Stem Cell Transplantation for Autoimmune Disease. Annu. Rev. Med. 2021, 72, 215–228. [Google Scholar] [CrossRef]
- Muraro, P.A.; Martin, R.; Mancardi, G.L.; Nicholas, R.; Sormani, M.P.; Saccardi, R. Autologous haematopoietic stem cell transplantation for treatment of multiple sclerosis. Nat. Rev. Neurol. 2017, 13, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Balassa, K.; Danby, R.; Rocha, V. Haematopoietic stem cell transplants: principles and indications. Br. J. Hosp. Med. 2019, 80, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, A. Hematopoietic stem cell transplantation for autoimmune diseases: more than just prolonged immunosuppression. Curr. Opin. Hematol. 2018, 25, 433–440. [Google Scholar] [CrossRef]
- Malmegrim, K.C.R.; Lima-Júnior, J.R.; Arruda, L.C.M.; de Azevedo, J.T.C.; de Oliveira, G.L.V.; Oliveira, M.C. Autologous Hematopoietic Stem Cell Transplantation for Autoimmune Diseases: From Mechanistic Insights to Biomarkers. Front. Immunol. 2018, 9, 2602. [Google Scholar] [CrossRef]
- Atkins, H.L.; Muraro, P.A.; van Laar, J.M.; Pavletic, S.Z. Autologous Hematopoietic Stem Cell Transplantation for Autoimmune Disease—Is It Now Ready for Prime Time? Biol. Blood Marrow Transplant. 2012, 18, S177–S183. [Google Scholar] [CrossRef]
- Boffa, G.; Signori, A.; Massacesi, L.; Mariottini, A.; Sbragia, E.; Cottone, S.; Amato, M.P.; Gasperini, C.; Moiola, L.; Meletti, S.; et al. Hematopoietic Stem Cell Transplantation in People With Active Secondary Progressive Multiple Sclerosis. Neurology 2023, 100, e1109–e1122. [Google Scholar] [CrossRef]
- Boffa G, Inglese M, Mancardi GL. Hematopoietic stem cell transplantation for multiple sclerosis. Handb Clin Neurol. 2024;202:153-167. [CrossRef]
- Genc B, Bozan HR, Genc S, Genc K. Stem Cell Therapy for Multiple Sclerosis. Adv Exp Med Biol. 2019;1084:145-174. [CrossRef]
- Ross, L.A.; Stropp, L.M.; Cohen, J.A. Autologous Hematopoietic Stem Cell Transplantation to Treat Multiple Sclerosis. Neurol. Clin. 2023, 42, 165–184. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Ruscitti, P.; Cipriani, P.; Giacomelli, R. Haematopoietic stem cell transplantation in systemic sclerosis: Challenges and perspectives. 19, 1026; 62. [Google Scholar] [CrossRef]
- van Laar, J.M.; Farge, D.; Sont, J.K.; Naraghi, K.; Marjanovic, Z.; Larghero, J.; Schuerwegh, A.J.; Marijt, E.W.A.; Vonk, M.C.; Schattenberg, A.V.; et al. Autologous Hematopoietic Stem Cell Transplantation vs Intravenous Pulse Cyclophosphamide in Diffuse Cutaneous Systemic Sclerosis. JAMA 2014, 311, 2490–2498. [Google Scholar] [CrossRef] [PubMed]
- Reider, S.; Binder, L.; Fürst, S.; Hatzl, S.; Blesl, A. Hematopoietic Stem Cell Transplantation in Refractory Crohn’s Disease: Should It Be Considered? Cells 2022, 11, 3463. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Yao, Q.; Chen, W.; Gao, F.; Li, P.; Wu, J.; Yu, J.; Cao, H. Stem cell therapy for Crohn’s disease: systematic review and meta-analysis of preclinical and clinical studies. Stem Cell Res. Ther. 2021, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Hawkey, C. Hematopoietic Stem Cell Transplantation in Crohn's Disease: State-of-the-Art Treatment. Dig. Dis. 2017, 35, 107–114. [Google Scholar] [CrossRef]
- Ruiz, M.A.; Junior, R.L.K.; Piron-Ruiz, L.; Peña-Arciniegas, T.; Saran, P.S.; De Quadros, L.G. Hematopoietic stem cell transplantation for Crohn’s disease: Gaps, doubts and perspectives. World J. Stem Cells 2018, 10, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Radin, M.; Almarzooqi, A.M.; Al-Saleh, J.; Roccatello, D.; Sciascia, S.; Khamashta, M. Autologous hematopoietic stem cell transplantation in Systemic Lupus Erythematosus and antiphospholipid syndrome: A systematic review. Autoimmun. Rev. 2017, 16, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Sui, W.; Hou, X.; Che, W.; Chen, J.; Ou, M.; Xue, W.; Dai, Y. Hematopoietic and mesenchymal stem cell transplantation for severe and refractory systemic lupus erythematosus. Clin. Immunol. 2013, 148, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Champ, A.M.M.d.H. Hematopoietic Stem Cell Transplantation for Systemic Lupus Erythematosus. J. Immunol. Res. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Alexander, T.; Arnold, R.; Hiepe, F. Autologe hämatopoetische Stammzelltransplantation bei systemischem Lupus erythematodes. Z. fur Rheumatol. 2016, 75, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Askanase, A.; Khalili, L.; Tang, W.; Mertz, P.; Scherlinger, M.; Sebbag, E.; Chasset, F.; Felten, R.; Arnaud, L. New and future therapies: Changes in the therapeutic armamentarium for SLE. Best Pr. Res. Clin. Rheumatol. 2023, 101865. [Google Scholar] [CrossRef] [PubMed]
- Arruda, L.; Clave, E.; Moins-Teisserenc, H.; Douay, C.; Farge, D.; Toubert, A. Resetting the immune response after autologous hematopoietic stem cell transplantation for autoimmune diseases. Curr. Res. Transl. Med. 2016, 64, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Swart, J.F.; Lindemans, C.A.; van Royen, A.; Boelens, J.J.; Prakken, B.J.; Wulffraat, N. Changing winds in refractory autoimmune disease in children. Curr. Opin. Rheumatol. 2012, 24, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.A.; Badoglio, M.; Labopin, M.; Giebel, S.; McGrath, E.; Marjanovic, Z.; Burman, J.; Moore, J.; Rovira, M.; Wulffraat, N.M.; et al. Evolution, trends, outcomes, and economics of hematopoietic stem cell transplantation in severe autoimmune diseases. Blood Adv. 2017, 1, 2742–2755. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.; Badoglio, M.; Henes, J.; Heesen, C.; Arnold, R.; Radbruch, A.; Snowden, J.A.; Hiepe, F. Autologe hämatopoetische Stammzelltransplantation bei Autoimmunerkrankungen. Z. fur Rheumatol. 2020, 79, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, P.; Oliveira, M.-C.; Badoglio, M.; Sharrack, B.; Farge, D.; Snowden, J. Haematopoietic stem cell transplantation in autoimmune diseases: From basic science to clinical practice. Curr. Res. Transl. Med. 2016, 64, 71–82. [Google Scholar] [CrossRef]
- Doglio, M.; Alexander, T.; Del Papa, N.; Snowden, J.A.; Greco, R. New insights in systemic lupus erythematosus: From regulatory T cells to CAR-T-cell strategies. 150, 1289. [Google Scholar] [CrossRef]
- Snowden, J.A.; Sánchez-Ortega, I.; Corbacioglu, S.; Basak, G.W.; Chabannon, C.; de la Camara, R.; Dolstra, H.; Duarte, R.F.; Glass, B.; Greco, R.; et al. Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2022. Bone Marrow Transplant. 2022, 57, 1217–1239. [Google Scholar] [CrossRef]
- Faul, C.; Donnelly, M.; Merscher-Gomez, S.; Chang, Y.H.; Franz, S.; Delfgaauw, J.; Chang, J.-M.; Choi, H.Y.; Campbell, K.N.; Kim, K.; et al. The actin cytoskeleton of kidney podocytes is a direct target of the antiproteinuric effect of cyclosporine A. Nat. Med. 2008, 14, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.; Cui, M.; Kong, N.; Jing, J.; Xu, Y.; Liu, X.; Yang, F.; Xu, Z.; Yan, Y.; Zhao, D.; et al. Cytotoxic CD161−CD8+ TEMRA cells contribute to the pathogenesis of systemic lupus erythematosus. EBioMedicine 2023, 90, 104507. [Google Scholar] [CrossRef] [PubMed]
- Sureda, A.; Pereira, M.I.B.; Dreger, P. The role of hematopoietic stem cell transplantation in the treatment of relapsed/refractory Hodgkin's lymphoma. Curr. Opin. Oncol. 2012, 24, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Meloni, G.; Capria, S.; Vignetti, M.; Mandelli, F.; Modena, V. Blast Crisis of Chronic Myelogenous Leukemia in Long-Lasting Systemic Lupus Erythematosus: Regression of Both Diseases After Autologous Bone Marrow Transplantation. Blood 1997, 89, 4659–4659. [Google Scholar] [CrossRef] [PubMed]
- Lowenthal, R.M.; Cohen, M.L.; Atkinson, K.; Biggs, J.C. Apparent cure of rheumatoid arthritis by bone marrow transplantation. . 1993, 20, 137–40. [Google Scholar] [PubMed]
- A Yin, J.; Jowitt, S.N. Resolution of immune-mediated diseases following allogeneic bone marrow transplantation for leukaemia. . 1992, 9, 31–3. [Google Scholar] [PubMed]
- Milanetti, F.; Bucha, J.; Testori, A.; Burt, R.K. Autologous Hematopoietic Stem Cell Transplantation for Systemic Sclerosis. Curr. Stem Cell Res. Ther. 2011, 6, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Burt, R.K.; Han, X.; Quigley, K.; Arnautovic, I.; Shah, S.J.; Lee, D.C.; Freed, B.H.; Jovanovic, B.; Helenowski, I.B. Cardiac safe hematopoietic stem cell transplantation for systemic sclerosis with poor cardiac function: a pilot safety study that decreases neutropenic interval to 5 days. Bone Marrow Transplant. 2020, 56, 50–59. [Google Scholar] [CrossRef]
- Brierley, C.K.; Castilla-Llorente, C.; Labopin, M.; Badoglio, M.; Rovira, M.; Ricart, E.; Dierickx, D.; Vermeire, S.; Hasselblatt, P.; Finke, J.; et al. Autologous Haematopoietic Stem Cell Transplantation for Crohn’s Disease: A Retrospective Survey of Long-term Outcomes From the European Society for Blood and Marrow Transplantation. J. Crohn’s Colitis 2018, 12, 1097–1103. [Google Scholar] [CrossRef]
- Bregante, S.; Gualandi, F.; van Lint, M.T.; Schenone, A.; Bacigalupo, A.; Marmont, A.M. Sjögren’s syndrome associated chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) treated with autologous and subsequently allogeneic haematopoietic SCT (HSCT). Bone Marrow Transplant. 2013, 48, 1139–1140. [Google Scholar] [CrossRef] [PubMed]
- Loh, Y.; Oyama, Y.; Statkute, L.; Quigley, K.; Yaung, K.; Gonda, E.; Barr, W.; Jovanovic, B.; Craig, R.; Stefoski, D.; et al. Development of a secondary autoimmune disorder after hematopoietic stem cell transplantation for autoimmune diseases: role of conditioning regimen used. Blood 2006, 109, 2643–2548. [Google Scholar] [CrossRef] [PubMed]
- Bohgaki, T.; Atsumi, T.; Koike, T. Multiple Autoimmune Diseases after Autologous Stem-Cell Transplantation. New Engl. J. Med. 2007, 357, 2734–2736. [Google Scholar] [CrossRef] [PubMed]
- Daikeler, T.; Labopin, M.; Di Gioia, M.; Abinun, M.; Alexander, T.; Miniati, I.; Gualandi, F.; Fassas, A.; Martin, T.; Schwarze, C.P.; et al. Secondary autoimmune diseases occurring after HSCT for an autoimmune disease: a retrospective study of the EBMT Autoimmune Disease Working Party. Blood 2011, 118, 1693–1698. [Google Scholar] [CrossRef]
- He, J.; Li, Z. Dilemma of immunosuppression and infection risk in systemic lupus erythematosus. Rheumatology 2023, 62, i22–i29. [Google Scholar] [CrossRef]
- Burt, R.K.; Han, X.; Gozdziak, P.; Yaung, K.; Morgan, A.; Clendenan, A.M.; Henry, J.; Calvario, M.A.; Datta, S.K.; Helenowski, I.; et al. Five year follow-up after autologous peripheral blood hematopoietic stem cell transplantation for refractory, chronic, corticosteroid-dependent systemic lupus erythematosus: effect of conditioning regimen on outcome. Bone Marrow Transplant. 2018, 53, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.; Tyndall, A. Autologous stem cell transplantation for systemic lupus erythematosus. Lupus 2004, 13, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Chen, W.; Ren, G.; Zhao, L.; Guo, J.; Gong, D.; Zeng, C.; Hu, W.; Liu, Z. Autologous Hematopoietic Stem Cell Transplantation for Refractory Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2019, 14, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Daikeler, T.; Tichelli, A.; Passweg, J. Complications of autologous hematopoietic stem cell transplantation for patients with autoimmune diseases. Pediatr. Res. 2012, 71, 439–444. [Google Scholar] [CrossRef]
- Jasim, S.A.; Yumashev, A.V.; Abdelbasset, W.K.; Margiana, R.; Markov, A.; Suksatan, W.; Pineda, B.; Thangavelu, L.; Ahmadi, S.H. Shining the light on clinical application of mesenchymal stem cell therapy in autoimmune diseases. Stem Cell Res. Ther. 2022, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Akiyama, K.; Zhang, H.; Yamaza, T.; Hou, Y.; Zhao, S.; Xu, T.; Le, A.; Shi, S. Mesenchymal Stem Cell Transplantation Reverses Multiorgan Dysfunction in Systemic Lupus Erythematosus Mice and Humans. STEM CELLS 2009, 27, 1421–1432. [Google Scholar] [CrossRef]
- Liang, J.; Zhang, H.; Hua, B.; Wang, H.; Lu, L.; Shi, S.; Hou, Y.; Zeng, X.; Gilkeson, G.S.; Sun, L. Allogenic mesenchymal stem cells transplantation in refractory systemic lupus erythematosus: a pilot clinical study. Ann. Rheum. Dis. 2010, 69, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, D.; Liang, J.; Zhang, H.; Feng, X.; Wang, H.; Hua, B.; Liu, B.; Ye, S.; Hu, X.; et al. Umbilical cord mesenchymal stem cell transplantation in severe and refractory systemic lupus erythematosus. Arthritis Rheum. 2010, 62, 2467–2475. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Guo, F.; Pan, Q.; Chen, S.; Chen, J.; Liu, H.-F.; Pan, Q. Mesenchymal Stem Cell Therapy: Hope for Patients With Systemic Lupus Erythematosus. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
- Xia, Y.; Ye, H.; Li, K.; Shi, B.; Sun, X.; Wu, J. Efficacy of Mesenchymal Stem Cell Therapy on Lupus Nephritis and Renal Function in Systemic Lupus Erythematosus: A Meta-Analysis. Clin. Investig. Med. 2023, 46, E24–35. [Google Scholar] [CrossRef]
- Oh, S.; Payne, A.S. Engineering Cell Therapies for Autoimmune Diseases: From Preclinical to Clinical Proof of Concept. Immune Netw. 2022, 22, e37. [Google Scholar] [CrossRef]
- Nemazee, D. Mechanisms of central tolerance for B cells. Nat. Rev. Immunol. 2017, 17, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Kochenderfer, J.N.; Rosenberg, S.A. Treating B-cell cancer with T cells expressing anti-CD19 chimeric antigen receptors. Nat. Rev. Clin. Oncol. 2013, 10, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Draborg, A.H.; Duus, K.; Houen, G. Epstein-Barr Virus and Systemic Lupus Erythematosus. J. Immunol. Res. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.R. Epstein-Barr virus (EBV) reactivation and therapeutic inhibitors. J. Clin. Pathol. 2019, 72, 651–658. [Google Scholar] [CrossRef]
- Nashi, E.; Wang, Y.; Diamond, B. The role of B cells in lupus pathogenesis. Int. J. Biochem. Cell Biol. 2009, 42, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Samy, E.; Wax, S.; Huard, B.; Hess, H.; Schneider, P. Targeting BAFF and APRIL in systemic lupus erythematosus and other antibody-associated diseases. Int. Rev. Immunol. 2017, 36, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Amengual, O. B cells targeting therapy in the management of systemic lupus erythematosus. Immunol. Med. 2019, 43, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.W.; Rojas, O.L.; Gommerman, J.L. B cell depletion therapies in autoimmune disease: advances and mechanistic insights. Nat. Rev. Drug Discov. 2020, 20, 179–199. [Google Scholar] [CrossRef] [PubMed]
- Weiner, G.J. Rituximab: Mechanism of Action. Semin. Hematol. 2010, 47, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Anolik, J.H.; Barnard, J.; Owen, T.; Zheng, B.; Kemshetti, S.; Looney, R.J.; Sanz, I. Delayed memory B cell recovery in peripheral blood and lymphoid tissue in systemic lupus erythematosus after B cell depletion therapy. Arthritis Rheum. 2007, 56, 3044–3056. [Google Scholar] [CrossRef] [PubMed]
- Forsthuber, T.G.; Cimbora, D.M.; Ratchford, J.N.; Katz, E.; Stüve, O. B cell-based therapies in CNS autoimmunity: differentiating CD19 and CD20 as therapeutic targets. Ther. Adv. Neurol. Disord. 2018, 11. [Google Scholar] [CrossRef]
- Merrill, J.T.; Neuwelt, C.M.; Wallace, D.J.; Shanahan, J.C.; Latinis, K.M.; Oates, J.C.; Utset, T.O.; Gordon, C.; Isenberg, D.A.; Hsieh, H.; et al. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: The randomized, double-blind, phase ii/iii systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2009, 62, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Mysler, E.F.; Spindler, A.J.; Guzman, R.; Bijl, M.; Jayne, D.; Furie, R.A.; Houssiau, F.A.; Drappa, J.; Close, D.; Maciuca, R.; et al. Efficacy and Safety of Ocrelizumab in Active Proliferative Lupus Nephritis: Results From a Randomized, Double-Blind, Phase III Study. Arthritis Rheum. 2013, 65, 2368–2379. [Google Scholar] [CrossRef]
- Arnold, J.; Dass, S.; Twigg, S.; Jones, C.H.; Rhodes, B.; Hewins, P.; Chakravorty, M.; Courtney, P.; Ehrenstein, M.; Yusof, Y.M.; et al. Efficacy and safety of obinutuzumab in systemic lupus erythematosus patients with secondary non-response to rituximab. Rheumatology 2022, 61, 4905–4909. [Google Scholar] [CrossRef]
- A Furie, R.; Aroca, G.; Cascino, M.D.; Garg, J.P.; Rovin, B.H.; Alvarez, A.; Fragoso-Loyo, H.; Zuta-Santillan, E.; Schindler, T.; Brunetta, P.; et al. B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2021, 81, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Clowse, M.E.B.; Wallace, D.J.; Furie, R.A.; Petri, M.A.; Pike, M.C.; Leszczyński, P.; Neuwelt, C.M.; Hobbs, K.; Keiserman, M.; Duca, L.; et al. Efficacy and Safety of Epratuzumab in Moderately to Severely Active Systemic Lupus Erythematosus: Results From Two Phase III Randomized, Double-Blind, Placebo-Controlled Trials. Arthritis Rheumatol. 2016, 69, 362–375. [Google Scholar] [CrossRef] [PubMed]
- Dubey, A.K.; Handu, S.S.; Dubey, S.; Sharma, P.; Sharma, K.K.; Ahmed, Q.M. Belimumab: First targeted biological treatment for systemic lupus erythematosus. J. Pharmacol. Pharmacother. 2011, 2, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.J.; Ginzler, E.M.; Merrill, J.T.; Furie, R.A.; Stohl, W.; Chatham, W.W.; Weinstein, A.; McKay, J.D.; McCune, W.J.; Petri, M.; et al. Safety and Efficacy of Belimumab Plus Standard Therapy for Up to Thirteen Years in Patients With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1125–1134. [Google Scholar] [CrossRef]
- Manzi, S.; Sánchez-Guerrero, J.; Merrill, J.T.; Furie, R.; Gladman, D.; Navarra, S.V.; Ginzler, E.M.; D'Cruz, D.P.; Doria, A.; Cooper, S.; et al. Effects of belimumab, a B lymphocyte stimulator-specific inhibitor, on disease activity across multiple organ domains in patients with systemic lupus erythematosus: combined results from two phase III trials. Ann. Rheum. Dis. 2012, 71, 1833–1838. [Google Scholar] [CrossRef]
- Furie, R.; Petri, M.; Zamani, O.; Cervera, R.; Wallace, D.J.; Tegzová, D.; Sanchez-Guerrero, J.; Schwarting, A.; Merrill, J.T.; Chatham, W.W.; et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011, 63, 3918–3930. [Google Scholar] [CrossRef] [PubMed]
- Merrill, J.T.; van Vollenhoven, R.F.; Buyon, J.P.; A Furie, R.; Stohl, W.; Morgan-Cox, M.; Dickson, C.; Anderson, P.W.; Lee, C.; Berclaz, P.-Y.; et al. Efficacy and safety of subcutaneous tabalumab, a monoclonal antibody to B-cell activating factor, in patients with systemic lupus erythematosus: results from ILLUMINATE-2, a 52-week, phase III, multicentre, randomised, double-blind, placebo-controlled study. Ann. Rheum. Dis. 2015, 75, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Merrill, J.T.; Shanahan, W.R.; Scheinberg, M.; Kalunian, K.C.; Wofsy, D.; Martin, R.S. Phase III trial results with blisibimod, a selective inhibitor of B-cell activating factor, in subjects with systemic lupus erythematosus (SLE): results from a randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2018, 77, 883–889. [Google Scholar] [CrossRef] [PubMed]
- A Petri, M.; Martin, R.S.; A Scheinberg, M.; A Furie, R. Assessments of fatigue and disease activity in patients with systemic lupus erythematosus enrolled in the Phase 2 clinical trial with blisibimod. Lupus 2016, 26, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Isenberg, D.; Gordon, C.; Licu, D.; Copt, S.; Rossi, C.P.; Wofsy, D. Efficacy and safety of atacicept for prevention of flares in patients with moderate-to-severe systemic lupus erythematosus (SLE): 52-week data (APRIL-SLE randomised trial). Ann. Rheum. Dis. 2014, 74, 2006–2015. [Google Scholar] [CrossRef] [PubMed]
- Merrill, J.T.; Wallace, D.J.; Wax, S.; Kao, A.; Fraser, P.A.; Chang, P.; Isenberg, D. ; on behalf of the ADDRESS II Investigators Efficacy and Safety of Atacicept in Patients With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2017, 70, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.J.; A Isenberg, D.; Morand, E.F.; Vazquez–Mateo, C.; Kao, A.H.; Aydemir, A.; Pudota, K.; Ona, V.; Aranow, C.; Merrill, J.T. Safety and clinical activity of atacicept in the long-term extension of the phase 2b ADDRESS II study in systemic lupus erythematosus. Rheumatology 2021, 60, 5379–5389. [Google Scholar] [CrossRef] [PubMed]
- Bachanova, V.; Nachman, P.H. Two for one? CAR-T therapy for lymphoma benefits concurrent autoimmune disorders. Bone Marrow Transplant. 2023, 58, 1175–1176. [Google Scholar] [CrossRef]
- Sheng, L.; Zhang, Y.; Song, Q.; Jiang, X.; Cao, W.; Li, L.; Yi, H.; Weng, X.; Chen, S.; Wang, Z.; et al. Concurrent remission of lymphoma and Sjögren’s disease following anti-CD19 chimeric antigen receptor-T cell therapy for diffuse large B-cell lymphoma: a case report. Front. Immunol. 2023, 14, 1298815. [Google Scholar] [CrossRef]
- Wang, J.; Alkrekshi, A.; Dasari, S.; Lin, H.-T.C.; Elantably, D.; Al Armashi, A.R. CD19-targeted chimeric antigen receptor T-cell therapy in patients with concurrent B-cell Non-Hodgkin lymphoma and rheumatic autoimmune diseases: a propensity score matching study. Bone Marrow Transplant. 2023, 58, 1223–1228. [Google Scholar] [CrossRef]
- Jin, X.; Xu, Q.; Pu, C.; Zhu, K.; Lu, C.; Jiang, Y.; Xiao, L.; Han, Y.; Lu, L. Therapeutic efficacy of anti-CD19 CAR-T cells in a mouse model of systemic lupus erythematosus. Cell. Mol. Immunol. 2020, 18, 1896–1903. [Google Scholar] [CrossRef] [PubMed]
- Mougiakakos, D.; Krönke, G.; Völkl, S.; Kretschmann, S.; Aigner, M.; Kharboutli, S.; Böltz, S.; Manger, B.; Mackensen, A.; Schett, G. CD19-Targeted CAR T Cells in Refractory Systemic Lupus Erythematosus. New Engl. J. Med. 2021, 385, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Taubmann, J.; Müller, F.; Mutlu, M.Y.; Völkl, S.; Aigner, M.; Bozec, A.; Mackensen, A.; Grieshaber-Bouyer, R.; Schett, G. CD19 Chimeric Antigen Receptor T Cell Treatment: Unraveling the Role of B Cells in Systemic Lupus Erythematosus. Arthritis Rheumatol. 2024, 76, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Mackensen, A.; Mackensen, A.; Müller, F.; Müller, F.; Mougiakakos, D.; Mougiakakos, D.; Böltz, S.; Böltz, S.; Wilhelm, A.; Wilhelm, A.; et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nat. Med. 2022, 28, 2124–2132. [Google Scholar] [CrossRef]
- Müller, F.; Taubmann, J.; Bucci, L.; Wilhelm, A.; Bergmann, C.; Völkl, S.; Aigner, M.; Rothe, T.; Minopoulou, I.; Tur, C.; et al. CD19 CAR T-Cell Therapy in Autoimmune Disease — A Case Series with Follow-up. New Engl. J. Med. 2024, 390, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Krickau, T.; Naumann-Bartsch, N.; Aigner, M.; Kharboutli, S.; Kretschmann, S.; Spoerl, S.; Vasova, I.; Völkl, S.; Woelfle, J.; Mackensen, A.; et al. CAR T-cell therapy rescues adolescent with rapidly progressive lupus nephritis from haemodialysis. Lancet 2024, 403, 1627–1630. [Google Scholar] [CrossRef]
- Wang, W.; He, S.; Zhang, W.; Zhang, H.; DeStefano, V.M.; Wada, M.; Pinz, K.; Deener, G.; Shah, D.; Hagag, N.; et al. BCMA-CD19 compound CAR T cells for systemic lupus erythematosus: a phase 1 open-label clinical trial. Ann. Rheum. Dis. 2024, 83, 1304–1314. [Google Scholar] [CrossRef]
- Salazar-Camarena, D.C.; Palafox-Sánchez, C.A.; Cruz, A.; Marín-Rosales, M.; Muñoz-Valle, J.F. Analysis of the receptor BCMA as a biomarker in systemic lupus erythematosus patients. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Cheng, Q.; Laurent, S.A.; Thaler, F.S.; Beenken, A.E.; Meinl, E.; Krönke, G.; Hiepe, F.; Alexander, T. B-Cell Maturation Antigen (BCMA) as a Biomarker and Potential Treatment Target in Systemic Lupus Erythematosus. Int. J. Mol. Sci. 2024, 25, 10845. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, A.; Chambers, D.; Müller, F.; Bozec, A.; Grieshaber-Bouyer, R.; Winkler, T.; Mougiakakos, D.; Mackensen, A.; Schett, G.; Krönke, G. Selective CAR T cell–mediated B cell depletion suppresses IFN signature in SLE. J. Clin. Investig. 2024, 9. [Google Scholar] [CrossRef] [PubMed]
- Haghikia, A.; Schett, G.; Mougiakakos, D. B cell-targeting chimeric antigen receptor T cells as an emerging therapy in neuroimmunological diseases. Lancet Neurol. 2024, 23, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Maalej, K.M.; Merhi, M.; Inchakalody, V.P.; Mestiri, S.; Alam, M.; Maccalli, C.; Cherif, H.; Uddin, S.; Steinhoff, M.; Marincola, F.M.; et al. CAR-cell therapy in the era of solid tumor treatment: current challenges and emerging therapeutic advances. Mol. Cancer 2023, 22, 1–54. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.; Farrukh, H.; Chittepu, V.C.S.R.; Xu, H.; Pan, C.-X.; Zhu, Z. CAR race to cancer immunotherapy: from CAR T, CAR NK to CAR macrophage therapy. J. Exp. Clin. Cancer Res. 2022, 41, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Denlinger, N.; Bond, D.; Jaglowski, S. CAR T-cell therapy for B-cell lymphoma. Curr. Probl. Cancer 2022, 46, 100826. [Google Scholar] [CrossRef]
- Westin, J.R.; Sehn, L.H. CAR T cells as a second-line therapy for large B-cell lymphoma: a paradigm shift? Blood 2022, 139, 2737–2746. [Google Scholar] [CrossRef]
- Haslauer, T.; Greil, R.; Zaborsky, N.; Geisberger, R. CAR T-Cell Therapy in Hematological Malignancies. Int. J. Mol. Sci. 2021, 22, 8996. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.R.; Dorris, C.S.; Makambi, K.H.; Luo, Y.; Munshi, P.N.; Donato, M.; Rowley, S.D.; Saad, A.; Goy, A.; Dunleavy, K.; et al. Toxicity and efficacy of CAR T-cell therapy in primary and secondary CNS lymphoma: a meta-analysis of 128 patients. Blood Adv. 2023, 7, 32–39. [Google Scholar] [CrossRef]
- Maude, S.L.; Barrett, D.; Teachey, D.T.; Grupp, S.A. Managing Cytokine Release Syndrome Associated With Novel T Cell-Engaging Therapies. Cancer J. 2014, 20, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.D.; Smith, M.; Shah, N.N. How I Treat Refractory CRS and ICANS Following CAR T-cell Therapy. Blood 2023, 141, 2430–2442. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Hao, H.; Yang, G.; Zhang, Y.; Fu, Y. Immunotherapy with CAR-Modified T Cells: Toxicities and Overcoming Strategies. J. Immunol. Res. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Maus, M.V.; Haas, A.R.; Beatty, G.L.; Albelda, S.M.; Levine, B.L.; Liu, X.; Zhao, Y.; Kalos, M.; June, C.H. T Cells Expressing Chimeric Antigen Receptors Can Cause Anaphylaxis in Humans. Cancer Immunol. Res. 2013, 1, 26–31. [Google Scholar] [CrossRef]
- Verdun, N.; Marks, P. Secondary Cancers after Chimeric Antigen Receptor T-Cell Therapy. New Engl. J. Med. 2024, 390, 584–586. [Google Scholar] [CrossRef]
- Lee, D.W.; Gardner, R.; Porter, D.L.; Louis, C.U.; Ahmed, N.; Jensen, M.; Grupp, S.A.; Mackall, C.L. Current concepts in the diagnosis and management of cytokine release syndrome. Blood 2014, 124, 188–195. [Google Scholar] [CrossRef]
- Hay, K.A. Cytokine release syndrome and neurotoxicity afterCD19 chimeric antigen receptor-modified (CAR-) T cell therapy. Br. J. Haematol. 2018, 183, 364–374. [Google Scholar] [CrossRef]
- Maude, S.L.; Frey, N.; Shaw, P.A.; Aplenc, R.; Barrett, D.M.; Bunin, N.J.; Chew, A.; Gonzalez, V.E.; Zheng, Z.; Lacey, S.F.; et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 2014, 371, 1507–1517. [Google Scholar] [CrossRef]
- Zhao, J.L.; Ma, C.; O’connell, R.M.; Mehta, A.; DiLoreto, R.; Heath, J.R.; Baltimore, D. Conversion of Danger Signals into Cytokine Signals by Hematopoietic Stem and Progenitor Cells for Regulation of Stress-Induced Hematopoiesis. Cell Stem Cell 2014, 14, 445–459. [Google Scholar] [CrossRef] [PubMed]
- Brentjens, R.; Yeh, R.; Bernal, Y.; Riviere, I.; Sadelain, M. Treatment of Chronic Lymphocytic Leukemia With Genetically Targeted Autologous T Cells: Case Report of an Unforeseen Adverse Event in a Phase I Clinical Trial. Mol. Ther. 2010, 18, 666–668. [Google Scholar] [CrossRef]
- Kotch, C.; Barrett, D.; Teachey, D.T. Tocilizumab for the treatment of chimeric antigen receptor T cell-induced cytokine release syndrome. Expert Rev. Clin. Immunol. 2019, 15, 813–822. [Google Scholar] [CrossRef]
- Frey, N.; Porter, D. Cytokine Release Syndrome with Chimeric Antigen Receptor T Cell Therapy. Biol. Blood Marrow Transplant. 2018, 25, e123–e127. [Google Scholar] [CrossRef]
- Lamers, C.H.J.; Willemsen, R.; van Elzakker, P.; van Steenbergen-Langeveld, S.; Broertjes, M.; Oosterwijk-Wakka, J.; Oosterwijk, E.; Sleijfer, S.; Debets, R.; Gratama, J.W. Immune responses to transgene and retroviral vector in patients treated with ex vivo–engineered T cells. Blood 2011, 117, 72–82. [Google Scholar] [CrossRef]
- Levine, B.L.; Pasquini, M.C.; Connolly, J.E.; Porter, D.L.; Gustafson, M.P.; Boelens, J.J.; Horwitz, E.M.; Grupp, S.A.; Maus, M.V.; Locke, F.L.; et al. Unanswered questions following reports of secondary malignancies after CAR-T cell therapy. Nat. Med. 2024, 30, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, V.; Yazdanpanah, N.; Rezaei, N. The immunologic aspects of cytokine release syndrome and graft versus host disease following CAR T cell therapy. Int. Rev. Immunol. 2021, 41, 649–668. [Google Scholar] [CrossRef]
- Ghassemi, S.; Durgin, J.S.; Nunez-Cruz, S.; Patel, J.; Leferovich, J.; Pinzone, M.; Shen, F.; Cummins, K.D.; Plesa, G.; Cantu, V.A.; et al. Rapid manufacturing of non-activated potent CAR T cells. Nat. Biomed. Eng. 2022, 6, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, M.J.; Barba, P.; Jäger, U.; Shah, N.N.; Blaise, D.; Briones, J.; Shune, L.; Boissel, N.; Bondanza, A.; Mariconti, L.; et al. A Novel Autologous CAR-T Therapy, YTB323, with Preserved T-cell Stemness Shows Enhanced CAR T-cell Efficacy in Preclinical and Early Clinical Development. Cancer Discov. 2023, 13, 1982–1997. [Google Scholar] [CrossRef] [PubMed]
- Tur, C.; Eckstein, M.; Velden, J.; Rauber, S.; Bergmann, C.; Auth, J.; Bucci, L.; Corte, G.; Hagen, M.; Wirsching, A.; et al. CD19-CAR T-cell therapy induces deep tissue depletion of B cells. Ann. Rheum. Dis. 2024. [Google Scholar] [CrossRef] [PubMed]
- Mougiakakos, D.; Sengupta, R.; Gold, R.; Schroers, R.; Haghikia, A.; Lorente, M.; Pendleton, M.; Register, A.; Heesen, C.; Kröger, N.; et al. Successful generation of fully human, second generation, anti-CD19 CAR T cells for clinical use in patients with diverse autoimmune disorders. Cytotherapy 2024. [Google Scholar] [CrossRef] [PubMed]
- van Leuven SI, Duivenvoorden R. CAR-T cell therapy in systemic lupus erythematosus and beyond: a brave new world? Rheumatology (Oxford). 2024:1192-1194. vol. 5.
- Kambayana, G.; Rini, S.S. Autologous CD19-Targeted Chimeric Antigen Receptor (CAR)T-Cells as the Future of Systemic Lupus Erythematosus Treatment. Curr. Rheumatol. Rev. 2023, 19, 260–269. [Google Scholar] [CrossRef]
Figure 1.
Cell based treatment modalities for treatment refractory systemic lupus erythematosus.
Figure 2.
B cell targeted treatment modalities in systemic lupus erythematosus.
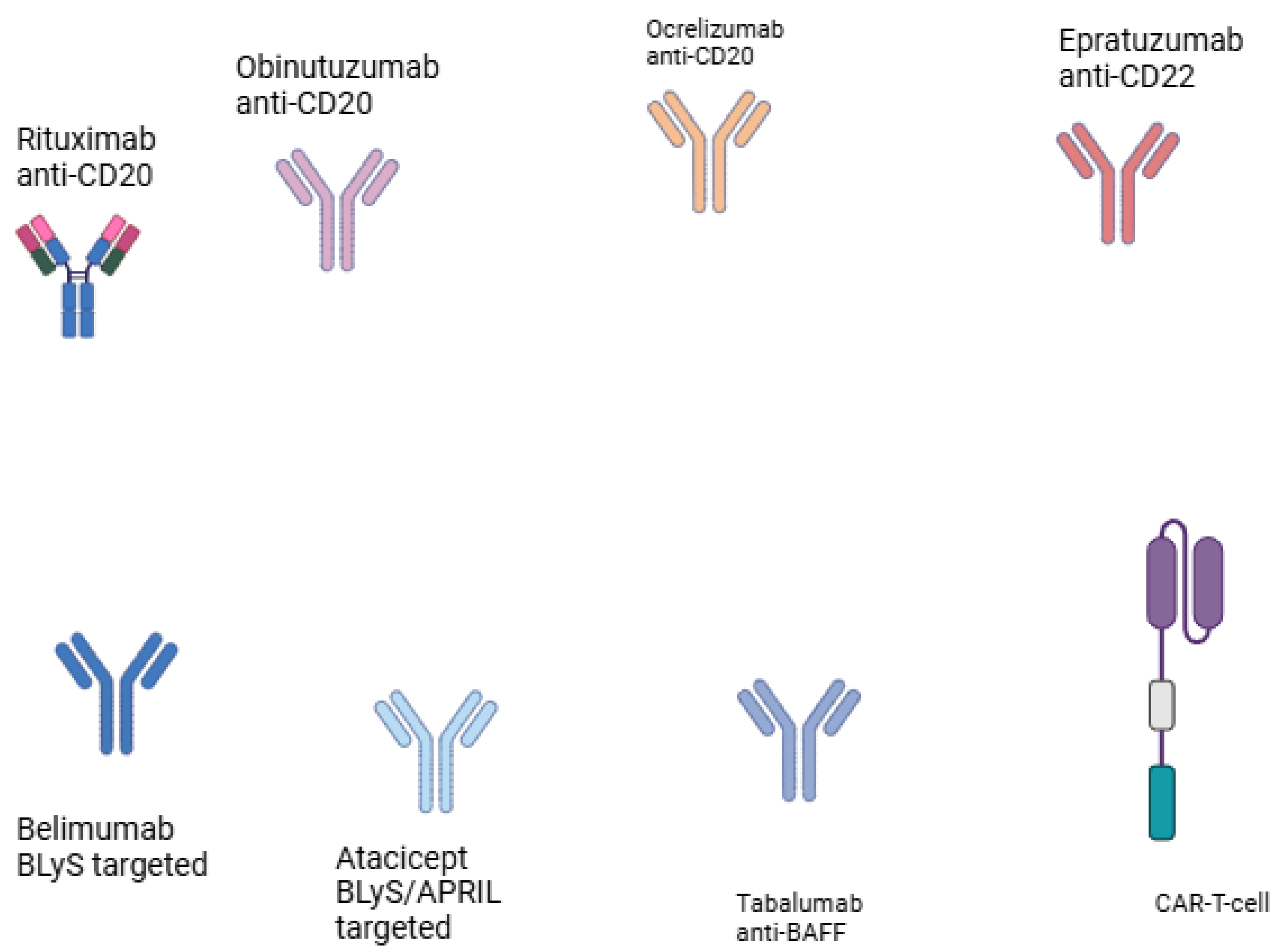
Figure 3.
Molecular targets on B lymphocytes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



