
Submitted:
22 December 2024
Posted:
23 December 2024
You are already at the latest version
Abstract
Cervical cancer causes 350,000 deaths annually, with 90% occurring in low and middle-income countries (LMICs), despite being largely preventable through vaccination and screening. This review examines innovative approaches to address screening coverage gaps worldwide, analysing both established programs in high-income countries and implementation strategies for LMICs. Self-sampling technologies demonstrate significant potential to increase screening participation by 1.5 to 2.5 times compared to traditional methods, particularly benefiting underserved populations across all healthcare settings. Vaginal brushes achieve the highest sensitivity (94.6%, 95% CI: 92.4-96.8) for HPV detection, while novel approaches like tampon sampling show promising acceptability and performance metrics. Implementation strategies vary by healthcare context, with high-income countries achieving success through integrated screening programs and digital solutions, while LMICs demonstrate effective adaptation through community-based distribution (20-35% uptake) and innovative delivery methods. In resource-limited settings, self-sampling increases participation through enhanced patient comfort and cultural acceptability, while reducing costs by 32-48%. Progress toward the WHO's cervical cancer elimination goals require careful consideration of local healthcare infrastructure, cultural contexts, and sustainable financing mechanisms. Future research priorities include optimising self-sampling technologies for sustainability and scalability, developing context-specific implementation strategies, and validating artificial intelligence applications to enhance screening efficiency across diverse healthcare settings.
Keywords:
Cervical Cancer (CC)
; Human Papillomavirus (HPV)
; Screening
; Self-Sampling
; Low- and middle-income countries (LMICs)
; FemTech
1. Introduction
FemTech represents a rapidly evolving sector of technology-driven solutions transforming cervical cancer prevention through Artificial Intelligence (AI) enabled diagnostics, smart self-sampling devices, and integrated digital platforms [1,2]. This review evaluates emerging self-sampling technologies and FemTech solutions for cervical cancer screening, analysing innovations and performance metrics, implementation strategies, and cost-effectiveness considerations for resource-limited settings.
Human Papillomavirus (HPV) infection is extremely common, with an estimated 80% of sexually active people acquiring at least one HPV type during their lifetime [3,4]. While most infections clear naturally within two years, persistent infection with high-risk HPV types causes 99.7% of cervical cancer cases, making HPV detection an important screening strategy [5,6]. In 2022, there were 660,000 new diagnoses and 350,000 from cervical cancer deaths globally [7,8].
This preventable disease disproportionately affects LMICs, which account for 90% of cervical cancer mortality [9,10,11]. The burden varies significantly by region, with age-standardised incidence rates ranging from 75 cases per 100,000 women in some African countries to less than 10 per 100,000 in many high-income countries [11]. The risk of persistent infection and progression to cancer is higher in people with compromised immune systems, particularly those living with HIV who are 6 times more likely to develop cervical cancer [12]. These disparities reflect inequitable access to both HPV vaccination and screening programmes [13,14].
The United Kingdom’s experience illustrates both progress and persistent challenges in cervical cancer control. While comprehensive screening programs contributed to a 25% decrease in incidence rates since the early 1990s, recent data show a 4% increase over the past decade suggesting evolving risk factors and potential gaps in screening coverage [15,16]. This trend has been exacerbated by the COVID-19 disruptions, with screening participation declining significantly. Some areas of London now report screening uptake rates as low as 48%, reflecting widespread disengagement with screening services [17,18].
Screening detects asymptomatic precancerous lesions which if undetected and untreated, can put women at risk of developing cervical cancer. In 2023, the NHS announced a plan for cervical cancer elimination by 2040 (defined as fewer than 4 cases per 100,000 women) which aligns with the World Health Organization (WHO) global 90-70-90 initiative, which aims for 90% HPV vaccination coverage, 70% screening coverage, and 90% treatment of precancerous lesions by 2030 [9,19]. Achieving this goal requires enhanced HPV vaccination coverage, increased screening participation, and innovative solutions adaptable to diverse healthcare settings [20,21,22,23,24]. Scotland demonstrates the potential success of comprehensive prevention strategies, achieving near elimination through high vaccination uptake and effective screening programmes [25]. The prevention of cervical cancer stands at a critical transition point. While HPV vaccination programmes are widespread in high income countries, their full impact on mortality rates will take decades to realise due to the extended latency between infection and cancer development [26,27]. Meanwhile, the evolution from traditional cytology to HPV-based screening (see Figure 1) offers enhanced detection capabilities, though implementation challenges persist, especially in resource-limited settings [28,29].
1.1. Prevention Strategies
1.1.1. Primary Prevention
HPV vaccination demonstrates exceptional efficacy, with the Swedish nationwide study (1.7 million women) showing a 90% reduction in cervical cancer incidence among girls vaccinated before age 17 over 2006-2017 [30]. Norwegian registry data showed 82% reduction in CIN2+ in girls vaccinated at an early age [31]. Effectiveness significantly decreases when vaccination is given after age 17 [32]. A systematic review from 2023 demonstrated vaccine effectiveness ranging from 74-93% for ages 9-14 versus 12-90% for ages 15-18, highlighting the critical importance of vaccination at an early age [33]. The implementation of WHO’s 90% vaccination coverage strategy poses significant challenges in LMICs due to infrastructure limitations and cost barriers [34,35]. Historical controversies surrounding vaccine trials and implementation programmes have created enduring trust issues in some regions, particularly in India and Sub-Saharan Africa [36]. These challenges underscore the importance of ethical implementation practices, community engagement, and cultural sensitivity in vaccination programmes.
1.1.2. Secondary Prevention
The evolution of screening methods marks a significant advancement in cervical cancer prevention, transitioning from traditional cytology to HPV-based approaches [37,38]. While high-income countries maintain screening coverage above 60%, LMICs struggle with rates as low as 20%, highlighting the need for resource-appropriate solutions [39]. Secondary prevention through HPV testing has emerged as superior to cytology for cervical screening; extensive research demonstrates enhanced sensitivity compared to cytology-based approaches [40,41].
1.1.3. Emerging Technologies
WHO’s 2021 guidelines recommended HPV DNA testing as the preferred screening method for women aged 30-49 years, with 5–10-year intervals [42]. Implementation success varies globally, requiring careful consideration of local healthcare infrastructure, resource availability, population-specific needs and healthcare system capacity [6,43].
Self-sampling represents a transformative approach to cervical cancer screening, particularly for underserved populations at elevated risk of HPV infection [44,45]. This review examines how innovative technologies and implementation strategies can bridge disparities in screening access. We analyse the potential of self-sampling and FemTech solutions to overcome traditional barriers, with particular focus on their application in resource-limited settings where conventional screening methods remain challenging to implement.
2. Understanding HPV and Cervical Carcinogenesis: A Foundation for Prevention
Understanding the relationship between HPV infection and cervical cancer development is crucial for developing effective prevention strategies and implementing appropriate screening programs [6,46,47]. Persistent infection with high-risk HPV is the primary causative agent of cervical cancer, with high-risk types 16 and 18 responsible for approximately 70% of cases globally, while types 31, 33, 45, 52, and 58 contribute another 20% [48,49]. The global prevalence of HPV16 and HPV18 in women with normal cytology is 3.2% and 1.4%, respectively [50,51].
HPV causes cervical cancer through persistent infection of epithelial cells, where continued expression of the viral oncoproteins E6 and E7 disrupt cell cycle regulation, leading to genomic instability and malignant transformation [52,53]. This process can result in precancerous lesions, graded as Cervical Intraepithelial Neoplasia (CIN1-3), with CIN2/3 requiring treatment to prevent progression to cancer [54,55]. Early detection through screening and colposcopy examination is crucial for identifying and managing CIN [56].
2.1. HPV Vaccination
Prophylactic HPV vaccines have demonstrated efficacy, achieving up to 90% reduction in vaccine-type HPV infections and 85% reduction in high-grade cervical lesions among vaccinated cohorts aged 13-24 years [57]. Evidence suggests extending screening intervals for vaccinated populations, with recommendations to start screening at age 30 instead of 25 for vaccinated women [58]. However, even the broadest 9-valent vaccine does not protect against all oncogenic HPV types, necessitating continued screening programs [59,60].While vaccination coverage is increasing globally, uptake remains suboptimal in many regions, and women aged 35 and older, who were not eligible for vaccination programs, remain at risk and require regular screening [61,62].
Recent evidence supports WHO’s simplified HPV vaccination schedules: one dose for ages 9-14 years, one or two doses for ages 15-20 years, and two doses for those over 21 years. This optimisation reduces costs by 30% while maintaining efficacy in younger age groups [63,64].
Global vaccination rates declined significantly, with studies showing coverage reductions of 42% in Italy and decreased uptake from 89.92% to 69.59% during the pandemic in US border communities [65]. These disruptions are projected to increase cases of cervical cancer and precancerous lesions over the coming decades, necessitating urgent recovery strategies [66].
2.2. Evolution of Cervical Cancer Screening Methods
The transition from traditional cytology to HPV-based screening represents a significant advancement in cervical cancer detection. HPV testing demonstrates superior detection of precancerous lesions with 98.1% sensitivity (95% CI: 96.3-96.7) for CIN3+, compared to cytology’s 48.5% sensitivity (95% CI: 44.0-53.0) [67]. While HPV testing shows slightly lower specificity (94.4%, 95% CI: 94.1-94.7) than cytology (97.9%, 95% CI: 97.8-98.1), new molecular technologies offer improved specificity without compromising sensitivity [67].
Emerging molecular approaches such as mRNA-based tests specifically detect active HPV infections by identifying viral oncogene expression, reducing false positives from transient infections [68]. Next-generation sequencing platforms enable simultaneous detection of multiple biomarkers, allowing better risk stratification of HPV-positive women. These innovations help identify women most at risk of disease progression while reducing unnecessary referrals [69].
2.4. Innovative Vaccination and Screening Approaches in High-Income Countries
High-income countries have pioneered different approaches to implementing HPV-based screening and self-sampling programs, providing valuable insights for global cervical cancer prevention strategies. Australia and the UK demonstrate successful integration of vaccination and screening programs. Australia’s comprehensive approach, achieving 80% vaccination coverage and implementing primary HPV screening, projects cervical cancer elimination by 2028, with 92% reduction in high-grade abnormalities among women vaccinated before age 15 [26,70]. The UK’s strategy complements its screening programme, contributing to a 25% decrease in cervical cancer incidence since the 1990s [71].
European countries have led self-sampling innovations. The opt-in model in the Netherlands achieved 16% self-sampling uptake by 2020, while Sweden’s direct-mailing approach during COVID-19 increased coverage from 54% to 60% in one year, reaching Europe’s highest rate of 83% [72,73]. Both countries maintain sustained screening coverage above 70% through automated testing platforms and standardised protocols, particularly benefiting under-screened populations [72,73].
2.5. Prevention Strategies in Middle and Low-Income Countries
Middle-income countries have developed effective hybrid approaches to cervical cancer prevention, exemplified by Malaysia and Thailand’s integration of national vaccination programs with phased HPV-based screening implementation [74]. These programs achieve 85-90% vaccination coverage through school-based delivery systems while expanding screening access via public-private partnerships [75].
WHO’s pragmatic approach for LMICs focuses on high-precision HPV testing with two lifetime screens at ages 35 and 45, balancing effective coverage against resource constraints [76]. Rwanda’s successful implementation demonstrates the potential of this approach, achieving 93% HPV vaccination coverage among girls aged 11-12 and screening 329,000 women between 2013-2016, resulting in a 50% reduction in cervical cancer mortality [77].
Successful programs utilise community health worker networks, mobile clinics, and partnerships with local religious leaders while integrating self-sampling options to optimise resource utilisation [78]. This comprehensive approach enables LMICs to maximise precancerous lesion detection during peak risk periods while maintaining cost-effectiveness within resource-limited healthcare systems [74].
3. Implementation Barriers and Economic Impact of Cervical Screening in LMICs
The implementation of cervical cancer prevention programs in low- and middle-income countries faces significant systemic challenges that impact both healthcare delivery and economic outcomes. A WHO analysis (2022) of 45 African countries revealed only 15% have universal health coverage schemes for cervical cancer screening, resulting in significant out-of-pocket expenditure for families [79]. Screening rates in LMICs remain critically low at 5%, exemplified by Nigeria where only 8.7% of 60.9 million at-risk women undergo screening, with even lower rates in rural areas [80].
The economic implications are substantial yet promising: every dollar invested in cervical cancer prevention yields a $3.20 return through improved health outcomes and productivity gains [81]. HPV-based screening programs demonstrate high cost-effectiveness, with an incremental cost-effectiveness ratio of $569 per quality-adjusted life year gained [82].
3.1. Innovative Implementation Strategies in LMICs
Several countries have developed effective solutions to increase screening coverage through innovative integration with existing healthcare services and novel delivery approaches. Rwanda has successfully integrated cervical screening with HIV/AIDS care services, with studies showing increased screening rates among HIV-positive women through integrated services [77]. Ethiopia’s screening coverage remains very low at less than 2% nationally, while Zambia has achieved about 26% population-level coverage through HIV program integration [83,84]. Mobile screening units and task-shifting strategies have been implemented in Rwanda to reach women in remote areas, with the country screening nearly 95,000 women and achieving 91% treatment rates for those testing positive [85].
International support has been crucial, with Gavi, The Vaccine Alliance committing $600 million for HPV vaccination and the Global Fund reaching over 1 million women through integrated HIV-screening programmes [86]. While many LMICs currently rely on visual inspection methods – direct inspection of the cervix to identify macroscopic morphological abnormalities, with typically low specificity - (Visual inspection with acetic acid ((VIA))/Visual inspection with Lugol’s Iodine ((VILI))) due to resource constraints, these approaches offer advantages of immediate results and same-day treatment [87]. The emergence of HPV self-sampling technologies presents an opportunity to implement more sensitive molecular testing while maintaining community-based screening benefits, which in some setting will be followed up by VIA/VILI and in some contexts referral to colposcopy (depending on the infrastructure available, based on country).
4. Enhancing Screening Participation Through Self-Sampling: Evidence and Implementation
Self-sampling represents a transformative approach to cervical cancer screening, addressing traditional barriers while improving accessibility for underserved populations through patient-centred collection methods. Cervical screening coverage in England has declined, with only 69.9-71.2% of eligible women screened within the recommended interval [88,89]. Barriers to screening include discomfort, embarrassment, time constraints, and procedure-related anxiety [90]. Lower uptake is associated with younger age, ethnic minority background, and socioeconomic deprivation [91]. Women who have experienced sexual abuse are less likely to attend screening [92]. Studies show that transgender men and non-binary people have significantly lower cervical screening uptake, with only 58% of those eligible having been screened [93]. Research indicates that transgender men are 37% less likely to be current with cervical screening compared to cisgender patients, and are ten times more likely to have inadequate test results [94].
The YouScreen trial in London (n=8338) validated self-sampling’s effectiveness in increasing participation, achieving 56% uptake through GP practices compared to 13% via direct mailing. The approach showed particular success among ethnic minorities (64% coverage) and socioeconomically deprived populations (60% coverage)[95].
Implementation strategies for self-sampling vary in effectiveness, with community-based distribution through pharmacies and health centres achieving higher uptake (20-35%) compared to direct mailing methods (8-25%) [95]. The UK HPValidate study validated multiple device-test combinations (3 different collection devices: Evalyn Brush (Rovers Medical), Self-Vaginal Floqswabs (Copan) and Aptima Multitest (Hologic), demonstrating strong user preference (85%) for having self-sampling as an option alongside traditional screening [96].
Economic analyses demonstrate cost-effectiveness of self-sampling in low-resource settings. A 2023 study in Sikkim, India found that HPV self-testing cost US$15.3 per woman screened compared to US$19.2 for traditional screening, representing a significant cost reduction [97].
Successful implementation in LMICs requires tailored delivery approaches combining clinic-based and home-based methods. Community health workers facilitate education and sample collection through door-to-door visits, while trusted community leaders address health literacy through visual instructions [97]. Sample transport systems using swabs remain stable at room temperature for up to two weeks, eliminating cold-chain requirements [98]. Digital platforms enable result communication where infrastructure permits, as demonstrated by the PRESCRIP-TEC project across Bangladesh, India, Uganda and Slovakia [99].
Self-sampling is endorsed by WHO because of its potential to increase screening coverage among underserved populations, though success depends on standardised procedures, comprehensive follow-up protocols, and context-specific implementation strategies that consider local healthcare infrastructure and economic conditions [45].
5. Evolution and Performance of Self-Sampling Technologies in Cervical Screening
The development of self-sampling technologies represents a significant advancement in cervical cancer screening, with various collection methods demonstrating increasing accuracy and accessibility while addressing traditional barriers to participation [100]. Collection approaches have evolved to encompass vaginal swabs with soft, flexible tips made of cotton, polyester, or nylon fibres; brushes designed with flexible low-density polyethylene (LDPE) bristles for standardised sampling; and diagnostic tampons utilising absorbent materials to collect vaginal secretions [101,102]. Additional innovations include urine collection devices targeting first-void samples and menstrual fluid collection systems like Qvin-pad and the Papcup [103,104]. These diverse sampling methods offer specific advantages and performance characteristics suited to different healthcare settings and patient populations, enabling more inclusive screening options across varied contexts.
Performance metrics from meta-analyses show that self-collected samples have slightly lower detection rates compared to clinician collection, with sensitivity reduced by 14% (95% CI: 9-20%) and specificity by 11% (95% CI: 8-15%) [105]. However, newer PCR-based assays demonstrate comparable accuracy, particularly with lavage devices and brushes [105].
The integration of AI enhances screening precision through advanced image analysis capabilities. Recent studies demonstrate AI algorithms achieving sensitivity and specificity ranges of 0.22-0.93 and 0.67-0.95 respectively in classifying visual inspection images [106,107]. Wu et al. (2024) highlight how AI-assisted digital microscopy platforms like CytoBrain can analyse digitised cervical samples with up to 78% efficiency in cell classification, reducing reliance on specialised personnel while maintaining diagnostic accuracy [108]. While these technologies show particular promise for resource-limited settings, large-scale validation in real-world conditions remains crucial for establishing clinical feasibility.
Recent advancements in point-of-care (POC) HPV testing offer promising solutions for cervical cancer screening in resource-limited settings. These tests aim to provide rapid results with high sensitivity and specificity, addressing barriers in traditional cytology-based screening [109,110]. The careHPV test demonstrates good performance, with sensitivity and specificity around 88% and 84% for CIN2+ detection [111]. New technologies like isothermal amplification and lateral flow detection enable low-cost, sample-to-answer HPV testing suitable for decentralised screening [20]. HPV-based screen-and-treat approaches have shown effectiveness in reducing cervical disease and over-treatment compared to visual inspection methods [112]. A study in Papua New Guinea found high acceptability and safety of an integrated POC HPV self-sampling and same-day treatment strategy. POC innovations are transforming screening accessibility in resource-limited settings [113]. The Hemex Health Gazelle platform demonstrates the potential for rapid, affordable testing with high accuracy, achieving results within 8 minutes while maintaining laboratory-grade standards [114].
WHO has recently launched updated target product profiles for POC tests, emphasising the need for affordable, user-friendly devices suitable for low-resource settings [115]. These profiles aim to guide manufacturers in developing tests that meet specific performance and operational characteristics crucial for effective cervical cancer screening in diverse healthcare contexts [115].
5.1. Device Types and Clinical Performance
The Evalyn® Brush and FLOQSwabs™ (Copan) represent extensively validated self-sampling methods, with the Evalyn® Brush achieving 97% user acceptability through innovative features like depth indicators and click mechanisms [121,128]. FLOQSwabs™ use short nylon fibres arranged on a solid plastic shaft. The fibres are positioned perpendicularly to promote strong capillary action, allowing for rapid absorption of liquid samples. Also because it lacks an internal core, more than 90% of the collected sample can be easily released into testing media. While urine-based testing offers minimal invasiveness and potential integration with other screening programs, it demonstrates lower sensitivity (51-63%) compared to other self-sampling methods, limiting its current utility as a primary screening approach [129].
Table 1. provides a comprehensive comparison of current self-sampling devices, highlighting key features: [92,116–127].
The Daye Diagnostic Tampon (DT) shows promising performance with 82.9% sensitivity and 91.6% specificity, achieving the highest valid result rates (99.2%) compared to vaginal self-swabs (95.4%) and clinician-collected samples (90.8%) [123]. User acceptance is high, with 78.3% reporting high comfort pre-sampling and 74.5% finding it “very easy” to use [123,130]. When collected first in the sampling sequence, the DT achieves optimal performance (100% sensitivity, 96.8% specificity), with 70.5% of participants preferring this method [123].
Teal Health was granted Breakthrough Device Designation by FDA in 2024 [131]. It has integrated digital features, including visualisation capabilities and automated sample verification, achieving 94% sample adequacy rates and higher user satisfaction (Stanford Medicine Innovation Report, 2023). The Papcup system offers HPV detection from menstrual blood samples, providing results within 15 minutes and improving accessibility for younger women while maintaining functionality for post-menopausal women through traditional swab collection [132]. A novel approach using a modified menstrual pad (Q-Pad) for passive HPV sample collection showed high concordance (95-100%) with clinician-collected samples among HPV-positive women, offering potential for integration into cervical cancer prevention programs [125].
A collection of studies examined the effectiveness of self-sampling methods for HPV testing compared to clinician-taken cervical samples. Vaginal self-sampling using dry flocked swabs, wet dacron swabs, and urine samples showed similar sensitivity and specificity to clinician-taken samples for detecting high-grade cervical lesions [92,133,134]. Self-sampling methods were generally well-accepted by women, with urine collection being the easiest and most preferred option [92].
Digital health solutions demonstrate significant benefits in cervical cancer screening programmes, with electronic health interventions improving screening participation rates by 46% compared to usual care, with particularly strong impact in LMIC settings [135]. However, a critical limitation is the requirement for additional cytology visits following HPV-positive results, leading to 35-45% patient dropout rates during follow-up [136]. While newer devices attempt dual sample collection for both HPV and cytology testing, cytological examination from self-collected samples shows lower adequacy rates compared to clinician collection, primarily due to their inability to sample the cervical transformation zone where precancerous lesions typically originate [137]. Studies comparing self-sampling cytology to clinician collection show sensitivity ranges of 64.7-71.9% and specificity of 81.0-86.6% for detecting intraepithelial lesions [138]. Current self-sampling devices cannot access the endocervical cells in the transformation zone - a capability that requires speculum examination in a clinical setting - limiting their utility for comprehensive cervical screening [138,139].
5.2. Advancements in DNA Methylation Testing
Recent advancements in DNA methylation testing represent a significant breakthrough in cervical cancer screening strategies. Meta-analyses demonstrate that DNA methylation markers achieve 63% sensitivity and 76% specificity for CIN2+, and 71% sensitivity and 75% specificity for CIN3+ [140]. This approach effectively identifies women at higher risk of progression to cancer while reducing unnecessary referrals. The WID-qCIN test, which assesses methylation of DPP6, RALYL, and GSX1 genes, demonstrated improved performance over cytology in a large real-world cohort [141]. While methylation assays initially require higher investment in molecular infrastructure, their superior sensitivity (63-71% for CIN2+/CIN3+) and reduced need for specialised cytology expertise make them potentially cost-effective for LMICs in the long term [142]. There is the potential to repurpose Covid testing PCR equipment which is universally available, reducing investment costs in DNA methylationSelf-sampling in combination with DNA methylation testing presents a promising pathway for cervical cancer screening evolution, potentially streamlining the screening process by eliminating separate cytology testing and reducing reliance on clinical infrastructure while maintaining high diagnostic standards.
HPV genotyping provides another effective triage strategy, already implemented in countries like the Netherlands. This approach allows risk stratification of HPV-positive self-samples based on type-specific risk, though implementation in LMICs requires consideration of cost and laboratory infrastructure. Studies show that genotyping can effectively identify women requiring immediate colposcopy versus those suitable for routine screening intervals [143,144].
Successful implementation requires careful consideration of quality assurance, healthcare integration, and cost analysis. This innovative combination of self-sampling, methylation testing, and POC analysis represents a potentially transformative approach to cervical cancer screening, aligned with WHO’s elimination goals, and could significantly improve screening accessibility and effectiveness in low-resource settings while maintaining high diagnostic standards.
6. Conclusions
The landscape of cervical cancer prevention is transforming through emerging technologies and evolving healthcare strategies. While progress has been made, substantial disparities persist between high-income countries and LMICs, necessitating innovative solutions.
Self-sampling technologies, including novel approaches like the Diagnostic Tampon, and the Teal Wand, show promise for increasing screening accessibility. Meta-analyses demonstrate that self-sampling can increase participation by 1.5 to 2.5 times compared to traditional methods, particularly impacting underserved populations [145,146].
The integration of AI and molecular testing enhances screening precision, with AI algorithms demonstrating 95% accuracy in identifying cervical abnormalities [147]. POC testing, showing 93% sensitivity and 91% specificity, offers potential solutions for resource-limited settings [148].
Cost-effectiveness analyses indicate that integrated digital health solutions can reduce screening costs by 46% in low-resource settings while improving follow-up rates [135]. However, successful implementation requires careful consideration of quality assurance, follow-up pathways, healthcare infrastructure integration, and cultural acceptability.
As HPV vaccination coverage increases globally, screening protocols will require adjustment, with evidence suggesting extended intervals for vaccinated populations [58]. Critical knowledge gaps require focused research, including standardised quality metrics for sample adequacy and evidence-based risk-stratification algorithms. Research priorities vary by healthcare setting, with high-income countries focusing on AI integration and multi-cancer detection platforms, while LMICs require cost-effective sample transport systems and POC testing validation.
The goal of cervical cancer elimination appears increasingly achievable through these innovative approaches, but success depends on addressing implementation challenges, particularly in resource-limited settings.
Author Contributions
Conceptualisation, M.G., A.O., and A.G-M.; methodology, M.G., A.O., and A.G-M.; data curation, M.G. and E.P.; resources, M.G., E.P., A.O., and A.G-M.; writing—original draft preparation, M.G. A.O., and A.G-M; writing—review and editing, M.G., E.P., A.P., A.O., and A.G-M.; visualisation, M.G., A.O., and A.G-M.; supervision, M.G., A.P., A.O., and A.G-M.; project administration, M.G., A.O., and A.G-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. AGM is funded by EGA Institute for Women’s Health and MRC core funding (MC_UU_00004/01).
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authours.
Acknowledgments
The authors gratefully acknowledge Adeola Olaitan and Aleksandra Gentry-Maharaj for their invaluable guidance and scientific oversight throughout the manuscript development. We thank Dr. Karin Hellner (University of Oxford), Valentina Milanova (Daye), and Hannah McCulloch for their critical review and insightful comments that substantially improved the manuscript. Special thanks to Valentin Ivanov (Daye) for his technical expertise in figure production. The views expressed in this article are those of the authors and do not necessarily represent the views of their respective institutions.
Conflicts of Interest
M.G. and E.P. are employees of Daye, which owns intellectual property rights to the diagnostic tampon technology discussed in this review. M.G. and E.P. are employees of Daye, which owns intellectual property rights to the diagnostic tampon technology discussed in this review. AGM is a principal investigator on a study exploring acceptability of the diagnostic tampon in Tanzania, funded by the EPSRC IAA Innovation Challenge – Women’s Health Tech – 2024. The remaining authors declare no conflicts of interest. As employees of a company developing cervical screening technology, M.G. and E.P. acknowledge their position in relation to the research topic. To maintain objectivity, all performance metrics and study outcomes reported for the diagnostic tampon and other technologies were independently verified through peer-reviewed sources and validated by co-authors. The manuscript development process included rigorous review by independent academic collaborators to ensure balanced representation of all screening technologies and approaches.
References
- Chandra Sekar, P.K.; Thomas, S.M.; Veerabathiran, R. The future of cervical cancer prevention: advances in research and technology. Exploration of Medicine 2024, 384–400. [Google Scholar] [CrossRef]
- Accelerating the impact of technology and innovation for global cervical cancer prevention (Conference Presentation) | Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Accelerating-the-impact-of-technology-and-for-Ramanujam/28f74703b3992f143b2156d4aa9a994ff14f0b2d (accessed on 11 December 2024).
- Epidemiology and natural history of HPV. | Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Epidemiology-and-natural-history-of-HPV.-Cox/28f52ed799891e264adeafb6afb09823fa2c29e3 (accessed on 11 December 2024).
- Jensen, J.E.; Becker, G.L.; Jackson, J.B.; Rysavy, M.B. Human Papillomavirus and Associated Cancers: A Review. Viruses 2024, 16, 680. [Google Scholar] [CrossRef]
- Towards elimination of cervical cancer – human papillomavirus (HPV) vaccination and cervical cancer screening in Asian National Cancer Centers Alliance (ANCCA) member countries - PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10415801/ (accessed on 7 October 2024).
- Okunade, K.S. Human papillomavirus and cervical cancer. Journal of Obstetrics and Gynaecology 2020, 40, 602–608. [Google Scholar] [CrossRef]
- Singh, D.; Vignat, J.; Lorenzoni, V.; Eslahi, M.; Ginsburg, O.; Lauby-Secretan, B.; Arbyn, M.; Basu, P.; Bray, F.; Vaccarella, S. Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob Health 2022, 11, e197–e206. [Google Scholar] [CrossRef] [PubMed]
- Viveros-Carreño, D.; Fernandes, A.; Pareja, R. Updates on cervical cancer prevention. Int J Gynecol Cancer 2023, 33, 394–402. [Google Scholar] [CrossRef]
- Cervical Cancer Elimination Initiative. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed on 11 December 2024).
- Vaccarella, S.; Laversanne, M.; Ferlay, J.; Bray, F. Cervical cancer in A frica, L atin A merica and the C aribbean and A sia: Regional inequalities and changing trends. Intl Journal of Cancer 2017, 141, 1997–2001. [Google Scholar] [CrossRef] [PubMed]
- Hull, R.; Mbele, M.; Makhafola, T.; Hicks, C.; Wang, S.-M.; Reis, R.M.; Mehrotra, R.; Mkhize-Kwitshana, Z.; Kibiki, G.; Bates, D.O.; et al. Cervical cancer in low and middle-income countries. Oncol Lett 2020, 20, 2058–2074. [Google Scholar] [CrossRef] [PubMed]
- Cervical cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 11 December 2024).
- Spencer, J.C.; Brewer, N.T.; Coyne-Beasley, T.; Trogdon, J.G.; Weinberger, M.; Wheeler, S.B. Reducing Poverty-related Disparities in Cervical Cancer: The Role of HPV Vaccination. Cancer Epidemiol Biomarkers Prev 2021, 30, 1895–1903. [Google Scholar] [CrossRef]
- Falcaro, M.; Soldan, K.; Ndlela, B.; Sasieni, P. Effect of the HPV vaccination programme on incidence of cervical cancer and grade 3 cervical intraepithelial neoplasia by socioeconomic deprivation in England: population based observational study. BMJ 2024, 385, e077341. [Google Scholar] [CrossRef]
- NHS Cervical Screening Programme Audit of invasive cervical cancer: national report 1 April 2016 to 31 March 2019. Available online: https://www.gov.uk/government/publications/cervical-screening-invasive-cervical-cancer-audit-2016-to-2019/nhs-cervical-screening-programme-audit-of-invasive-cervical-cancer-national-report-1-april-2016-to-31-march-2019 (accessed on 11 December 2024).
- Choi, S.; Ismail, A.; Pappas-Gogos, G.; Boussios, S. HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK. Pathogens 2023, 12, 298. [Google Scholar] [CrossRef] [PubMed]
- Rajwinder K Hira, George Akomfrah.
- Cervical screening standards data report 2022 to 2023. Available online: https://www.gov.uk/government/publications/cervical-screening-standards-data-report-2022-to-2023/cervical-screening-standards-data-report-2022-to-2023 (accessed on 18 December 2024).
- England, N.H.S. NHS England » NHS sets ambition to eliminate cervical cancer by 2040. Available online: https://www.england.nhs.uk/2023/11/nhs-sets-ambition-to-eliminate-cervical-cancer-by-2040/ (accessed on 11 December 2024).
- Kundrod, K.A.; Jeronimo, J.; Vetter, B.; Maza, M.; Murenzi, G.; Phoolcharoen, N.; Castle, P.E. Toward 70% cervical cancer screening coverage: Technical challenges and opportunities to increase access to human papillomavirus (HPV) testing. PLOS Glob Public Health 2023, 3, e0001982. [Google Scholar] [CrossRef]
- Gravitt, P.E.; Silver, M.I.; Hussey, H.M.; Arrossi, S.; Huchko, M.; Jeronimo, J.; Kapambwe, S.; Kumar, S.; Meza, G.; Nervi, L.; et al. Achieving equity in cervical cancer screening in low- and middle-income countries (LMICs): Strengthening health systems using a systems thinking approach. Preventive Medicine 2021, 144, 106322. [Google Scholar] [CrossRef]
- eClinicalMedicine Global strategy to eliminate cervical cancer as a public health problem: are we on track? eClinicalMedicine 2023, 55, 101842. [CrossRef] [PubMed]
- Allanson, E.R.; Schmeler, K.M. Preventing Cervical Cancer Globally: Are We Making Progress? Cancer Prevention Research 2021, 14, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Canfell, K. Towards the global elimination of cervical cancer. Papillomavirus Research 2019, 8, 100170. [Google Scholar] [CrossRef]
- Palmer, T.J.; Kavanagh, K.; Cuschieri, K.; Cameron, R.; Graham, C.; Wilson, A.; Roy, K. Invasive cervical cancer incidence following bivalent human papillomavirus vaccination: a population-based observational study of age at immunization, dose, and deprivation. J Natl Cancer Inst 2024, 116, 857–865. [Google Scholar] [CrossRef]
- Hall, M.T.; Simms, K.T.; Lew, J.-B.; Smith, M.A.; Saville, M.; Canfell, K. Projected future impact of HPV vaccination and primary HPV screening on cervical cancer rates from 2017–2035: Example from Australia. PLoS ONE 2018, 13, e0185332. [Google Scholar] [CrossRef] [PubMed]
- Luckett, R.; Feldman, S. Impact of 2-, 4- and 9-valent HPV vaccines on morbidity and mortality from cervical cancer. Human Vaccines & Immunotherapeutics 2016, 12, 1332–1342. [Google Scholar] [CrossRef]
- Maver, P.J.; Poljak, M. Primary HPV-based cervical cancer screening in Europe: implementation status, challenges, and future plans. Clinical Microbiology and Infection 2020, 26, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Wentzensen, N.; Arbyn, M. HPV-based cervical cancer screening- facts, fiction, and misperceptions. Preventive Medicine 2017, 98, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N Engl J Med 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Orumaa, M.; Lahlum, E.J.; Gulla, M.; Tota, J.E.; Nygård, M.; Nygård, S. Quadrivalent HPV Vaccine Effectiveness Against Cervical Intraepithelial Lesion Grade 2 or Worse in Norway: A Registry-Based Study of 0.9 Million Norwegian Women. The Journal of Infectious Diseases 2024, jiae209. [Google Scholar] [CrossRef] [PubMed]
- Mikalsen, M.P.; Simonsen, G.S.; Sørbye, S.W. Impact of HPV Vaccination on the Incidence of High-Grade Cervical Intraepithelial Neoplasia (CIN2+) in Women Aged 20–25 in the Northern Part of Norway: A 15-Year Study. Vaccines 2024, 12, 421. [Google Scholar] [CrossRef]
- Ellingson, M.K.; Sheikha, H.; Nyhan, K.; Oliveira, C.R.; Niccolai, L.M. Human papillomavirus vaccine effectiveness by age at vaccination: A systematic review. Hum Vaccin Immunother 2023, 19, 2239085. [Google Scholar] [CrossRef]
- Tsu, V.D.; LaMontagne, D.S.; Atuhebwe, P.; Bloem, P.N.; Ndiaye, C. National implementation of HPV vaccination programs in low-resource countries: Lessons, challenges, and future prospects. Preventive Medicine 2021, 144, 106335. [Google Scholar] [CrossRef]
- Guignard, A.; Praet, N.; Jusot, V.; Bakker, M.; Baril, L. Introducing new vaccines in low- and middle-income countries: challenges and approaches. Expert Review of Vaccines 2019, 18, 119–131. [Google Scholar] [CrossRef]
- Kumar, S.; Butler, D. Calls in India for legal action against US charity. Nature 2013. [Google Scholar] [CrossRef]
- Swanson, A.A.; Pantanowitz, L. The evolution of cervical cancer screening. Journal of the American Society of Cytopathology 2024, 13, 10–15. [Google Scholar] [CrossRef]
- Chatterjee, P.B.; Hingway, S.R.; Hiwale, K.M. Evolution of Pathological Techniques for the Screening of Cervical Cancer: A Comprehensive Review. Cureus 2024. [Google Scholar] [CrossRef]
- Sharma, J.; Yennapu, M.; Priyanka, Y. Screening Guidelines and Programs for Cervical Cancer Control in Countries of Different Economic Groups: A Narrative Review. Cureus 2023. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Ronco, G.; Anttila, A.; Meijer, C.J.L.M.; Poljak, M.; Ogilvie, G.; Koliopoulos, G.; Naucler, P.; Sankaranarayanan, R.; Peto, J. Evidence Regarding Human Papillomavirus Testing in Secondary Prevention of Cervical Cancer. Vaccine 2012, 30, F88–F99. [Google Scholar] [CrossRef]
- Ogilvie, G.; Nakisige, C.; Huh, W.K.; Mehrotra, R.; Franco, E.L.; Jeronimo, J. Optimizing secondary prevention of cervical cancer: Recent advances and future challenges. Intl J Gynecology & Obste 2017, 138, 15–19. [Google Scholar] [CrossRef]
- WHO recommends DNA testing as a first-choice screening method for cervical cancer prevention. Available online: https://www.who.int/europe/news-room/11-09-2021-who-recommends-dna-testing-as-a-first-choice-screening-method-for-cervical-cancer-prevention (accessed on 13 December 2024).
- Murewanhema, G.; Dzobo, M.; Moyo, E.; Moyo, P.; Mhizha, T.; Dzinamarira, T. Implementing HPV-DNA screening as primary cervical cancer screening modality in Zimbabwe: Challenges and recommendations. Scientific African 2023, 21, e01889. [Google Scholar] [CrossRef]
- Lozar, T.; Nagvekar, R.; Rohrer, C.; Dube Mandishora, R.S.; Ivanus, U.; Fitzpatrick, M.B. Cervical Cancer Screening Postpandemic: Self-Sampling Opportunities to Accelerate the Elimination of Cervical Cancer. Int J Womens Health 2021, 13, 841–859. [Google Scholar] [CrossRef] [PubMed]
- Serrano, B.; Ibáñez, R.; Robles, C.; Peremiquel-Trillas, P.; De Sanjosé, S.; Bruni, L. Worldwide use of HPV self-sampling for cervical cancer screening. Preventive Medicine 2022, 154, 106900. [Google Scholar] [CrossRef] [PubMed]
- Subramanya, D.; Grivas, P.D. HPV and Cervical Cancer: Updates on an Established Relationship. Postgraduate Medicine 2008, 120, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Barukčić, I. Human Papillomavirus—The Cause of Human Cervical Cancer. JBM 2018, 06, 106–125. [Google Scholar] [CrossRef]
- Cervical Cancer Causes, Risk Factors, and Prevention - NCI. Available online: https://www.cancer.gov/types/cervical/causes-risk-prevention (accessed on 13 December 2024).
- Lowy, D.R.; Solomon, D.; Hildesheim, A.; Schiller, J.T.; Schiffman, M. Human papillomavirus infection and the primary and secondary prevention of cervical cancer. Cancer 2008, 113, 1980–1993. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Barrionuevo-Rosas, L.; Herrero, R.; Bray, F.; Bosch, F.X.; de Sanjosé, S.; Castellsagué, X. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health 2016, 4, e453–463. [Google Scholar] [CrossRef] [PubMed]
- References Human papillomavirus vaccines: WHO position paper, May 2017 (References with abstracts cited in the position paper in the order of appearance.) SAGE guidance for the development of evidence-based vaccine-related recommendations. In 2017 [cited 2024 Dec 13]. Available from: https://www.semanticscholar.org/paper/References-Human-papillomavirus-vaccines%3A-WHO-May/7dc6c6b55657f911c80ea0427208cb1ff5aa913c.
- Chen, J.J. ; Department of Medicine, University of Massachusetts Medical School, Worcester, MA Genomic Instability Induced By Human Papillomavirus Oncogenes. N A J Med Sci 2010, 3, 043. [Google Scholar] [CrossRef]
- Korzeniewski, N.; Spardy, N.; Duensing, A.; Duensing, S. Genomic instability and cancer: Lessons learned from human papillomaviruses. Cancer Letters 2011, 305, 113–122. [Google Scholar] [CrossRef]
- Balasubramaniam, S.D.; Balakrishnan, V.; Oon, C.E.; Kaur, G. Key Molecular Events in Cervical Cancer Development. Medicina 2019, 55, 384. [Google Scholar] [CrossRef]
- Mello, V.; Sundstrom, R.K. Cervical Intraepithelial Neoplasia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Cooper, D.B.; Dunton, C.J. Colposcopy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Arbyn, M.; Xu, L. Efficacy and safety of prophylactic HPV vaccines. A Cochrane review of randomized trials. Expert Review of Vaccines 2018, 17, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Giorgi Rossi, P.; Carozzi, F.; Federici, A.; Ronco, G.; Zappa, M.; Franceschi, S.; Barca, A.; Barzon, L.; Baussano, I.; Berliri, C.; et al. Cervical cancer screening in women vaccinated against human papillomavirus infection: Recommendations from a consensus conference. Preventive Medicine 2017, 98, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Tumban, E. Gardasil-9: A global survey of projected efficacy. Antiviral Research 2016, 130, 101–109. [Google Scholar] [CrossRef]
- Signorelli, C.; Odone, A.; Ciorba, V.; Cella, P.; Audisio, R.A.; Lombardi, A.; Mariani, L.; Mennini, F.S.; Pecorelli, S.; Rezza, G.; et al. Human papillomavirus 9-valent vaccine for cancer prevention: a systematic review of the available evidence. Epidemiol. Infect. 2017, 145, 1962–1982. [Google Scholar] [CrossRef]
- Silver, M.I.; Kobrin, S. Exacerbating disparities?: Cervical cancer screening and HPV vaccination. Preventive Medicine 2020, 130, 105902. [Google Scholar] [CrossRef]
- Staley, H.; Shiraz, A.; Shreeve, N.; Bryant, A.; Martin-Hirsch, P.P.; Gajjar, K. Interventions targeted at women to encourage the uptake of cervical screening. Cochrane Database of Systematic Reviews 2021, 2021. [Google Scholar] [CrossRef]
- Stanley, M.; Schuind, A.; Muralidharan, K.K.; Guillaume, D.; Willens, V.; Borda, H.; Jurgensmeyer, M.; Limaye, R. Evidence for an HPV one-dose schedule. Vaccine 2024, 42, S16–S21. [Google Scholar] [CrossRef]
- PRIMAVERA Immunobridging Trial - NCI. Available online: https://dceg.cancer.gov/research/cancer-types/cervix/primavera (accessed on 15 December 2024).
- Rosa, A.D. Impact of the COVID-19 pandemic on HPV vaccination coverage in the general population and in PLWHs. European Review 2022.
- Castanon, A.; Rebolj, M.; Pesola, F.; Pearmain, P.; Stubbs, R. COVID-19 disruption to cervical cancer screening in England. J Med Screen 2022, 29, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, A.T.; Valls, J.; Baena, A.; Rojas, F.D.; Ramírez, K.; Álvarez, R.; Cristaldo, C.; Henríquez, O.; Moreno, A.; Reynaga, D.C.; et al. Performance of cervical cytology and HPV testing for primary cervical cancer screening in Latin America: an analysis within the ESTAMPA study. Lancet Reg Health Am 2023, 26, 100593. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, K.; Wentzensen, N. Human Papillomavirus mRNA and p16 Detection as Biomarkers for the Improved Diagnosis of Cervical Neoplasia. Cancer Epidemiology, Biomarkers & Prevention 2008, 17, 2536–2545. [Google Scholar] [CrossRef]
- Cuschieri, K.; Ronco, G.; Lorincz, A.; Smith, L.; Ogilvie, G.; Mirabello, L.; Carozzi, F.; Cubie, H.; Wentzensen, N.; Snijders, P.; et al. Eurogin roadmap 2017: Triage strategies for the management of HPV -positive women in cervical screening programs. Intl Journal of Cancer 2018, 143, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.T.; Simms, K.T.; Lew, J.-B.; Smith, M.A.; Brotherton, J.M.; Saville, M.; Frazer, I.H.; Canfell, K. The projected timeframe until cervical cancer elimination in Australia: a modelling study. The Lancet Public Health 2019, 4, e19–e27. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E. The impact of policy and screening on cervical cancer in England. Br J Nurs 2012, 21, S4–S10. [Google Scholar] [CrossRef]
- Arbyn, M.; Costa, S.; Latsuzbaia, A.; Kellen, E.; Girogi Rossi, P.; Cocuzza, C.E.; Basu, P.; Castle, P.E. HPV-based Cervical Cancer Screening on Self-samples in the Netherlands: Challenges to Reach Women and Test Performance Questions. Cancer Epidemiology, Biomarkers & Prevention 2023, 32, 159–163. [Google Scholar] [CrossRef]
- Elfström, M.; Gray, P.G.; Dillner, J. Cervical cancer screening improvements with self-sampling during the COVID-19 pandemic. eLife 2023, 12, e80905. [Google Scholar] [CrossRef]
- Integrating HPV vaccination programs with enhanced cervical cancer screening and treatment, a systematic review. | Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Integrating-HPV-vaccination-programs-with-enhanced-Wirtz-Mohamed/cea64a5bb058a357a4f17750bd4326202fdb9fcd (accessed on 19 December 2024).
- Ebrahimi, N.; Yousefi, Z.; Khosravi, G.; Malayeri, F.E.; Golabi, M.; Askarzadeh, M.; Shams, M.H.; Ghezelbash, B.; Eskandari, N. Human papillomavirus vaccination in low- and middle-income countries: progression, barriers, and future prospective. Front Immunol 2023, 14, 1150238. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Qiao, Y.; Keita, N. The Next Steps in Cervical Screening. Womens Health (Lond Engl) 2015, 11, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Binagwaho, A.; Wagner, C.; Gatera, M.; Karema, C.; Nutt, C.; Ngaboa, F. Achieving high coverage in Rwanda’s national human papillomavirus vaccination programme. Bull World Health Org 2012, 90, 623–628. [Google Scholar] [CrossRef]
- Poli, U.R.; Muwonge, R.; Bhoopal, T.; Lucas, E.; Basu, P. Feasibility, Acceptability, and Efficacy of a Community Health Worker–Driven Approach to Screen Hard-to-Reach Periurban Women Using Self-Sampled HPV Detection Test in India. JCO Global Oncology 2020, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Tracking Universal Health Coverage in the WHO African Region, 2022.
- Okolie, E.A.; Aluga, D.; Anjorin, S.; Ike, F.N.; Ani, E.M.; Nwadike, B.I. Addressing missed opportunities for cervical cancer screening in Nigeria: a nursing workforce approach. Ecancermedicalscience 2022, 16, 1373. [Google Scholar] [CrossRef]
- WHO CERVICAL CANCER ELIMINATION INITIATIVE: FROM CALL TO ACTION TO GLOBAL MOVEMENT.
- Goldhaber-Fiebert, J.D.; Stout, N.K.; Salomon, J.A.; Kuntz, K.M.; Goldie, S.J. Cost-Effectiveness of Cervical Cancer Screening With Human Papillomavirus DNA Testing and HPV-16,18 Vaccination. JNCI Journal of the National Cancer Institute 2008, 100, 308–320. [Google Scholar] [CrossRef]
- Zambia steps up cervical cancer screening with HPV testing | WHO | Regional Office for Africa. Available online: https://www.afro.who.int/countries/zambia/news/zambia-steps-cervical-cancer-screening-hpv-testing (accessed on 19 December 2024).
- Desta, A.A.; Alemu, F.T.; Gudeta, M.B.; Dirirsa, D.E.; Kebede, A.G. Willingness to utilize cervical cancer screening among Ethiopian women aged 30–65 years. Front. Glob. Womens Health 2022, 3. [Google Scholar] [CrossRef] [PubMed]
- Miller, S. Scaling up an effective model of care to prevent and treat cervical cancer in Rwanda. Available online: https://www.clintonhealthaccess.org/blog/scaling-up-an-effective-model-of-care-to-prevent-and-treat-cervical-cancer-in-rwanda/ (accessed on 19 December 2024).
- Wave of new commitments marks historic step towards the elimination of cervical cancer. Available online: https://www.gavi.org/news/media-room/wave-new-commitments-marks-historic-step-towards-elimination-cervical-cancer (accessed on 19 December 2024).
- Innovative approaches to cervical cancer screening in low- and middle-income countries | Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Innovative-approaches-to-cervical-cancer-screening-Toliman-Kaldor/12d6a2a977b943b7da0eb4a2322846ecb0ed2a33 (accessed on 19 December 2024).
- Davies-Oliveira, J.C.; Smith, M.A.; Grover, S.; Canfell, K.; Crosbie, E.J. Eliminating Cervical Cancer: Progress and Challenges for High-income Countries. Clinical Oncology 2021, 33, 550–559. [Google Scholar] [CrossRef]
- Ibrahim, A.; Simeen, N. 32P Cervical cancer: Barriers and smears to prevention. ESMO Open 2024, 9, 103532. [Google Scholar] [CrossRef]
- Waller, J.; Bartoszek, M.; Marlow, L.; Wardle, J. Barriers to cervical cancer screening attendance in England: a population-based survey. J Med Screen 2009, 16, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Marlow, L.; McBride, E.; Varnes, L.; Waller, J. Barriers to cervical screening among older women from hard-to-reach groups: a qualitative study in England. BMC Women’s Health 2019, 19, 38. [Google Scholar] [CrossRef] [PubMed]
- Cadman, L.; Waller, J.; Ashdown-Barr, L.; Szarewski, A. Barriers to cervical screening in women who have experienced sexual abuse: an exploratory study: Table 1. J Fam Plann Reprod Health Care 2012, 38, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Berner, A.M.; Connolly, D.J.; Pinnell, I.; Wolton, A.; MacNaughton, A.; Challen, C.; Nambiar, K.; Bayliss, J.; Barrett, J.; Richards, C. Attitudes of transgender men and non-binary people to cervical screening: a cross-sectional mixed-methods study in the UK. Br J Gen Pract 2021, 71, e614–e625. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, N.; Oliffe, J.L.; Kelly, M.T.; Krist, J. Bridging Barriers to Cervical Cancer Screening in Transgender Men: A Scoping Review. Am J Mens Health 2020, 14, 1557988320925691. [Google Scholar] [CrossRef]
- Lim, A.W.W.; Deats, K.; Gambell, J.; Lawrence, A.; Lei, J.; Lyons, M.; North, B.; Parmar, D.; Patel, H.; Waller, J.; et al. Opportunistic offering of self-sampling to non-attenders within the English cervical screening programme: a pragmatic, multicentre, implementation feasibility trial with randomly allocated cluster intervention start dates (YouScreen). eClinicalMedicine 2024, 73, 102672. [Google Scholar] [CrossRef] [PubMed]
- HPValidate: clinical validation of hrHPV test system using self-collected vaginal samples in NHS England commissioned laboratories providing cervical screening services.
- Hariprasad, R.; John, A.; Abdulkader, R.S. Challenges in the Implementation of Human Papillomavirus Self-Sampling for Cervical Cancer Screening in India: A Systematic Review. JCO Glob Oncol 2023, e2200401. [Google Scholar] [CrossRef] [PubMed]
- Woo, Y.L.; Gravitt, P.; Khor, S.K.; Ng, C.W.; Saville, M. Accelerating action on cervical screening in lower- and middle-income countries (LMICs) post COVID-19 era. Prev Med 2021, 144, 106294. [Google Scholar] [CrossRef] [PubMed]
- Feasibility of the WHO strategy to eliminate cervical cancer as a public health problem, lessons learned from the PRESCRIP-TEC project | Knowledge Action Portal on NCDs. Available online: https://www.knowledge-action-portal.com/en/content/feasibility-who-strategy-eliminate-cervical-cancer-public-health-problem-lessons-learned (accessed on 19 December 2024).
- Gupta, S.; Palmer, C.; Bik, E.M.; Cardenas, J.P.; Nuñez, H.; Kraal, L.; Bird, S.W.; Bowers, J.; Smith, A.; Walton, N.A.; et al. Self-Sampling for Human Papillomavirus Testing: Increased Cervical Cancer Screening Participation and Incorporation in International Screening Programs. Front. Public Health 2018, 6, 77. [Google Scholar] [CrossRef] [PubMed]
- Viviano, M.; Willame, A.; Cohen, M.; Benski, A.-C.; Catarino, R.; Wuillemin, C.; Tran, P.L.; Petignat, P.; Vassilakos, P. A comparison of cotton and flocked swabs for vaginal self-sample collection. Int J Womens Health 2018, 10, 229–236. [Google Scholar] [CrossRef] [PubMed]
- At-Home HPV Screen | Test Your Gynae Health. Available online: https://www.yourdaye.com/products/at-home-hpv-screening (accessed on 22 December 2024).
- Papcup | Cervical Screening. Available online: https://www.papcup.co.uk (accessed on 22 December 2024).
- QvinTM Introduces Q-PadTM: Transforming Women’s Health with FDA-Cleared Lab Testing using Menstrual Blood. Available online: https://www.biospace.com/qvin-introduces-q-pad-transforming-women-s-health-with-fda-cleared-lab-testing-using-menstrual-blood (accessed on 22 December 2024).
- Arbyn, M.; Smith, S.B.; Temin, S.; Sultana, F.; Castle, P. Detecting cervical precancer and reaching underscreened women by using HPV testing on self samples: updated meta-analyses. BMJ 2018, 363, k4823. [Google Scholar] [CrossRef]
- Viñals, R.; Jonnalagedda, M.; Petignat, P.; Thiran, J.-P.; Vassilakos, P. Artificial Intelligence-Based Cervical Cancer Screening on Images Taken during Visual Inspection with Acetic Acid: A Systematic Review. Diagnostics 2023, 13, 836. [Google Scholar] [CrossRef]
- Gupta, R.; Sarwar, A.; Sharma, V. Screening of Cervical Cancer by Artificial Intelligence based Analysis of Digitized Papanicolaou-Smear Images.; 2017.
- Wu, T.; Lucas, E.; Zhao, F.; Basu, P.; Qiao, Y. Artificial intelligence strengthens cervical cancer screening – present and future. Cancer Biol Med 2024, 21, 864–879. [Google Scholar] [CrossRef]
- Gupta, R.; Gupta, S. Point-of-care tests for human papillomavirus detection in uterine cervical samples: A review of advances in resource-constrained settings. Indian Journal of Medical Research 2023, 158, 509–521. [Google Scholar] [CrossRef]
- Seely, S.; Zingg, J.-M.; Joshi, P.; Slomovitz, B.; Schlumbrecht, M.; Kobetz, E.; Deo, S.; Daunert, S. Point-of-Care Molecular Test for the Detection of 14 High-Risk Genotypes of Human Papillomavirus in a Single Tube. Anal. Chem. 2023, 95, 13488–13496. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.; Mayaud, P.; Segondy, M.; Pant Pai, N.; Peeling, R.W. A systematic review and meta-analysis of studies evaluating the performance of point-of-care tests for human papillomavirus screening. Sex Transm Infect 2017, 93, S36–S45. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, L.; Denny, L. The time is now to implement HPV testing for primary screening in low resource settings. Preventive Medicine 2017, 98, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Vallely, A.J.B.; Saville, M.; Badman, S.G.; Gabuzzi, J.; Bolnga, J.; Mola, G.D.L.; Kuk, J.; Wai, M.; Munnull, G.; Garland, S.M.; et al. Point-of-care HPV DNA testing of self-collected specimens and same-day thermal ablation for the early detection and treatment of cervical pre-cancer in women in Papua New Guinea: a prospective, single-arm intervention trial (HPV-STAT). The Lancet Global Health 2022, 10, e1336–e1346. [Google Scholar] [CrossRef]
- Shrivas, S.; Patel, M.; Kumar, R.; Gwal, A.; Uikey, R.; Tiwari, S.K.; Verma, A.K.; Thota, P.; Das, A.; Bharti, P.K.; et al. Evaluation of Microchip-Based Point-Of-Care Device “Gazelle” for Diagnosis of Sickle Cell Disease in India. Front. Med. 2021, 8, 639208. [Google Scholar] [CrossRef] [PubMed]
- Target product profiles for human papillomavirus screening tests to detect cervical pre-cancer and cancer. Available online: https://www.who.int/publications/i/item/9789240100275 (accessed on 19 December 2024).
- Agency for Drugs and Technologies in Health. (2017). Health Technology Update: Issue 18. https://www.cda-amc.ca/sites/default/files/pdf/Health_Technology_Update_Issue_18.pdf 8/1055-9965.EPI-20-1226.
- Chakravarti, P.; Maheshwari, A.; Tahlan, S.; Kadam, P.; Bagal, S.; Gore, S.; Panse, N.; Deodhar, K.; Chaturvedi, P.; Dikshit, R.; et al. Diagnostic accuracy of menstrual blood for human papillomavirus detection in cervical cancer screening: a systematic review. Ecancermedicalscience 2022, 16, 1427. [Google Scholar] [CrossRef] [PubMed]
- Arias, M.; Jang, D.; Gilchrist, J.; Luinstra, K.; Li, J.; Smieja, M.; Chernesky, M.A. Ease, Comfort, and Performance of the HerSwab Vaginal Self-Sampling Device for the Detection of Chlamydia trachomatis and Neisseria gonorrhoeae. Sex Transm Dis 2016, 43, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.C.; Sargent, A.; Pinggera, E.; Carter, S.; Gilham, C.; Sasieni, P.; Crosbie, E.J. Urine high-risk human papillomavirus testing as an alternative to routine cervical screening: A comparative diagnostic accuracy study of two urine collection devices using a randomised study design trial. BJOG 2024, 131, 1456–1464. [Google Scholar] [CrossRef]
- Jentschke, M.; Chen, K.; Arbyn, M.; Hertel, B.; Noskowicz, M.; Soergel, P.; Hillemanns, P. Direct comparison of two vaginal self-sampling devices for the detection of human papillomavirus infections. J Clin Virol 2016, 82, 46–50. [Google Scholar] [CrossRef]
- Leinonen, M.K.; Schee, K.; Jonassen, C.M.; Lie, A.K.; Nystrand, C.F.; Rangberg, A.; Furre, I.E.; Johansson, M.J.; Tropé, A.; Sjøborg, K.D.; et al. Safety and acceptability of human papillomavirus testing of self-collected specimens: A methodologic study of the impact of collection devices and HPV assays on sensitivity for cervical cancer and high-grade lesions. Journal of Clinical Virology 2018, 99–100, 22–30. [Google Scholar] [CrossRef]
- Martinelli, M.; Giubbi, C.; Di Meo, M.L.; Perdoni, F.; Musumeci, R.; Leone, B.E.; Fruscio, R.; Landoni, F.; Cocuzza, C.E. Accuracy of Human Papillomavirus (HPV) Testing on Urine and Vaginal Self-Samples Compared to Clinician-Collected Cervical Sample in Women Referred to Colposcopy. Viruses 2023, 15, 1889. [Google Scholar] [CrossRef] [PubMed]
- Milanova, V.; Gomes, M.; Mihaylova, K.; Twelves, J.L.; Multmeier, J.; McMahon, H.; McCulloch, H.; Cuschieri, K. Diagnostic Accuracy of the Daye Diagnostic Tampon Compared to Clinician-Collected and Self-Collected Vaginal Swabs for Detecting HPV: A Comparative Study 2024, 2024. 12.02.2431 8200. [CrossRef]
- National Institute for Health and Care Excellence (NICE). The technology [Internet]. Available from: https://www.nice.org.uk/advice/mib273/chapter/The-technology.
- Naseri, S.; Young, S.; Cruz, G.; Blumenthal, P.D. Screening for High-Risk Human Papillomavirus Using Passive, Self-Collected Menstrual Blood. Obstet Gynecol 2022, 140, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Nilyanimit, P.; Chaithongwongwatthana, S.; Oranratanaphan, S.; Poudyal, N.; Excler, J.-L.; Lynch, J.; Vongpunsawad, S.; Poovorawan, Y. Comparable detection of HPV using real-time PCR in paired cervical samples and concentrated first-stream urine collected with Colli-Pee device. Diagn Microbiol Infect Dis 2024, 108, 116160. [Google Scholar] [CrossRef] [PubMed]
- Sechi, I.; Muresu, N.; Puci, M.V.; Saderi, L.; Del Rio, A.; Cossu, A.; Muroni, M.R.; Castriciano, S.; Martinelli, M.; Cocuzza, C.E.; et al. Preliminary Results of Feasibility and Acceptability of Self-Collection for Cervical Screening in Italian Women. Pathogens 2023, 12, 1169. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi, N.P.C.; Termini, L.; Longatto Filho, A.; Tacla, M.; De Aguiar, L.M.; Beldi, M.C.; Ferreira-Filho, E.S.; Baracat, E.C.; Soares-Júnior, J.M. Age-related acceptability of vaginal self-sampling in cervical cancer screening at two university hospitals: a pilot cross-sectional study. BMC Public Health 2019, 19, 963. [Google Scholar] [CrossRef] [PubMed]
- Sabeena, S.; Kuriakose, S.; Binesh, D.; Abdulmajeed, J.; Dsouza, G.; Ramachandran, A.; Vijaykumar, B.; Aswathyraj, S.; Devadiga, S.; Ravishankar, N.; et al. The Utility of Urine-Based Sampling for Cervical Cancer Screening in Low-Resource Settings. Asian Pac J Cancer Prev 2019, 20, 2409–2413. [Google Scholar] [CrossRef] [PubMed]
- Turner, F.; Drury, J.; Hapangama, D.K.; Tempest, N. Menstrual Tampons Are Reliable and Acceptable Tools to Self-Collect Vaginal Microbiome Samples. International Journal of Molecular Sciences 2023, 24, 14121. [Google Scholar] [CrossRef]
- FDA Puts Teal Health on an Accelerated Path to Market for our At-Home Cervical Cancer Screening. Available online: https://www.getteal.com/post/fda-puts-teal-health-on-an-accelerated-path-to-market-for-our-at-home-cervical-cancer-screening (accessed on 20 December 2024).
- Shafaghmotlagh, S. Papcup: Could this at-home HPV test make cervical screening easier? Available online: https://news.cancerresearchuk.org/2024/09/04/papcup-at-home-hpv-test-to-make-cervical-screening-smear-test-easier/ (accessed on 20 December 2024).
- Vaginal and Urine Self-sampling Compared to Cervical Sampling for HPV-testing with the Cobas 4800 HPV Test. AR 2017, 37. [CrossRef]
- [PDF] Clinical performance and acceptability of self-collected vaginal and urine samples compared with clinician-taken cervical samples for HPV testing among women referred for colposcopy. A cross-sectional study | Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Clinical-performance-and-acceptability-of-vaginal-A-%C3%98rnskov-Jochumsen/08d58fd35f8974135928df67f200fbf3fb39aa99 (accessed on 19 December 2024).
- Liu, X.; Ning, L.; Fan, W.; Jia, C.; Ge, L. Electronic Health Interventions and Cervical Cancer Screening: Systematic Review and Meta-Analysis. J Med Internet Res 2024, 26, e58066. [Google Scholar] [CrossRef] [PubMed]
- Olthof, E.M.G.; Aitken, C.A.; Siebers, A.G.; Van Kemenade, F.J.; De Kok, I.M.C.M. The impact of loss to follow-up in the Dutch organised HPV-based cervical cancer screening programme. Intl Journal of Cancer 2024, 154, 2132–2141. [Google Scholar] [CrossRef]
- Manley, K.; Patel, A.; Pawade, J.; Glew, S.; Hunt, K.; Villeneuve, N.; Mukonoweshuro, P.; Thompson, S.; Hoskins, H.; López-Bernal, A.; et al. The use of biomarkers and HPV genotyping to improve diagnostic accuracy in women with a transformation zone type 3. Br J Cancer 2022, 126, 91–99. [Google Scholar] [CrossRef]
- Gibert, M.J.; Sánchez-Contador, C.; Artigues, G. Validity and acceptance of self vs conventional sampling for the analysis of human papillomavirus and Pap smear. Sci Rep 2023, 13, 2809. [Google Scholar] [CrossRef] [PubMed]
- Othman, N.H.; Zaki, F.H.M.; Hussain, N.H.N.; Yusoff, W.Z.W.; Ismail, P. SelfSampling Versus Physicians’ Sampling for Cervical Cancer Screening Agreement of Cytological Diagnoses. Asian Pac J Cancer Prev 2016, 17, 3489–3494. [Google Scholar]
- Kelly, H.; Benavente, Y.; Pavon, M.A.; De Sanjose, S.; Mayaud, P.; Lorincz, A.T. Performance of DNA methylation assays for detection of high-grade cervical intraepithelial neoplasia (CIN2+): a systematic review and meta-analysis. Br J Cancer 2019, 121, 954–965. [Google Scholar] [CrossRef]
- Schreiberhuber, L.; Barrett, J.E.; Wang, J.; Redl, E.; Herzog, C.; Vavourakis, C.D.; Sundström, K.; Dillner, J.; Widschwendter, M. Cervical cancer screening using DNA methylation triage in a real-world population. Nat Med 2024, 30, 2251–2257. [Google Scholar] [CrossRef]
- Zhang, L.; Tan, W.; Yang, H.; Zhang, S.; Dai, Y. Detection of Host Cell Gene/HPV DNA Methylation Markers: A Promising Triage Approach for Cervical Cancer. Front. Oncol. 2022, 12, 831949. [Google Scholar] [CrossRef] [PubMed]
- Chatzistamatiou, K.; Tsertanidou, A.; Moysiadis, T.; Mouchtaropoulou, E.; Pasentsis, K.; Skenderi, A.; Stamatopoulos, K.; Agorastos, T. Comparison of different strategies for the triage to colposcopy of women tested high-risk HPV positive on self-collected cervicovaginal samples. Gynecol Oncol 2021, 162, 560–568. [Google Scholar] [CrossRef]
- Song, F.; Du, H.; Wang, C.; Huang, X.; Wu, R. ; CHIMUST team The effectiveness of HPV16 and HPV18 genotyping and cytology with different thresholds for the triage of human papillomavirus-based screening on self-collected samples. PLoS ONE 2020, 15, e0234518. [Google Scholar] [CrossRef] [PubMed]
- Verdoodt, F.; Dehlendorff, C.; Kjaer, S.K. Dose-related Effectiveness of Quadrivalent Human Papillomavirus Vaccine Against Cervical Intraepithelial Neoplasia: A Danish Nationwide Cohort Study. Clin Infect Dis 2020, 70, 608–614. [Google Scholar] [CrossRef]
- Yeh, P.T.; Kennedy, C.E.; De Vuyst, H.; Narasimhan, M. Self-sampling for human papillomavirus (HPV) testing: a systematic review and meta-analysis. BMJ Glob Health 2019, 4, e001351. [Google Scholar] [CrossRef]
- Ouh, Y.-T.; Kim, T.J.; Ju, W.; Kim, S.W.; Jeon, S.; Kim, S.-N.; Kim, K.G.; Lee, J.-K. Development and validation of artificial intelligence-based analysis software to support screening system of cervical intraepithelial neoplasia. Sci Rep 2024, 14, 1957. [Google Scholar] [CrossRef] [PubMed]
- Holmström, O.; Linder, N.; Kaingu, H.; Mbuuko, N.; Mbete, J.; Kinyua, F.; Törnquist, S.; Muinde, M.; Krogerus, L.; Lundin, M.; et al. Point-of-care digital cytology with artificial intelligence for cervical cancer screening at a peripheral clinic in Kenya. 2020. [CrossRef]
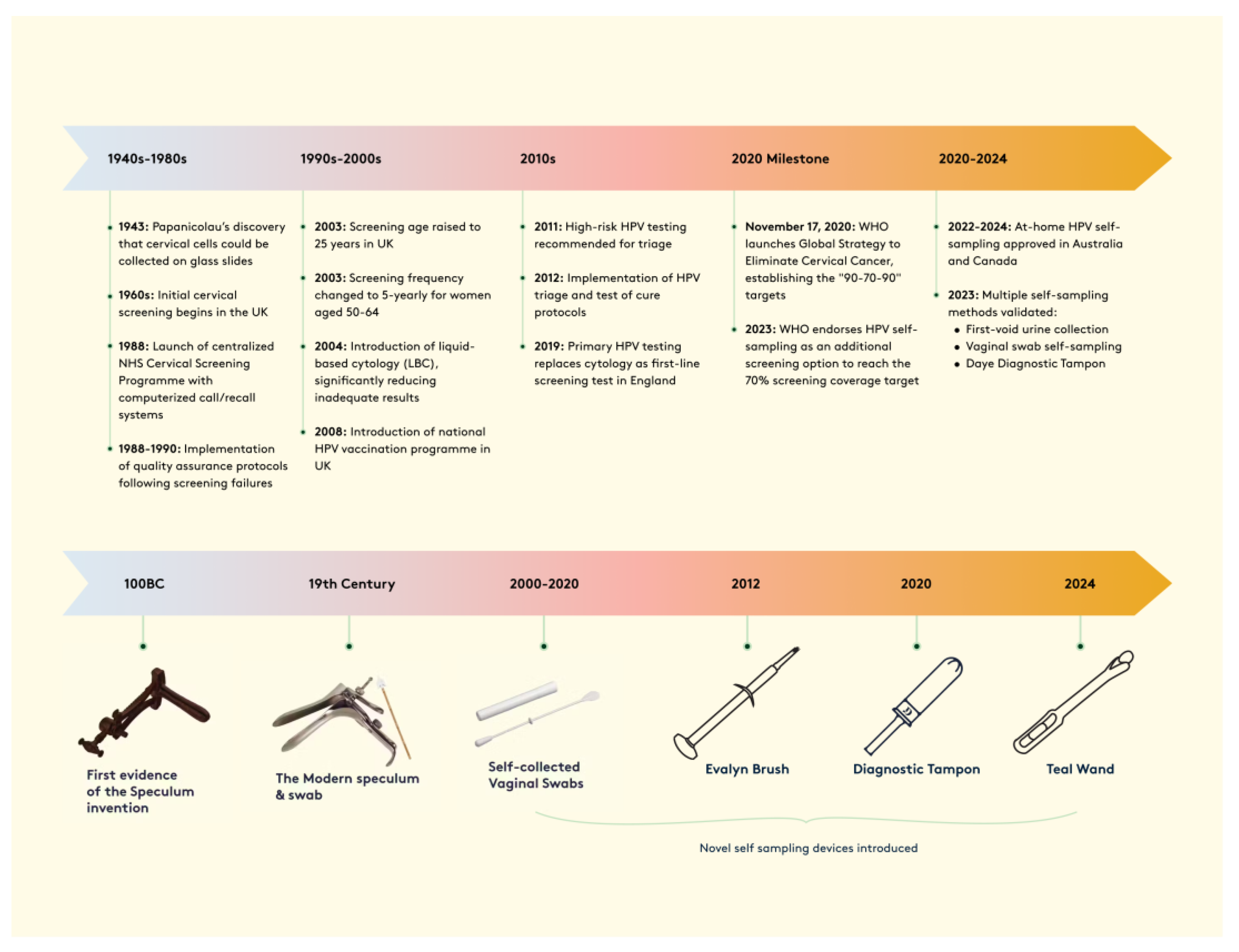
Figure 1.
Timeline of cervical cancer screening evolution, 1940s-2024. The upper panel shows key policy and technological developments in cervical screening programs, highlighting major milestones in the UK and globally. The lower panel illustrates the progression of screening devices from ancient speculums to modern self-sampling methods, demonstrating the advancement toward patient-centered screening approaches.
Figure 1.
Timeline of cervical cancer screening evolution, 1940s-2024. The upper panel shows key policy and technological developments in cervical screening programs, highlighting major milestones in the UK and globally. The lower panel illustrates the progression of screening devices from ancient speculums to modern self-sampling methods, demonstrating the advancement toward patient-centered screening approaches.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



