Submitted:
19 December 2024
Posted:
19 December 2024
You are already at the latest version
Abstract
Alcohol is a substantial risk factor for trauma, accounting for 30-50% of cases with alcohol intoxication. Alcohol usage impairs wound healing in traumatic injuries by lowering immune function and leukocyte production. This review compares the outcomes and complications of trauma patients who have consumed alcohol to those who have not. Systematic and independent searches were carried out on PubMed, Google Scholar, Scopus, and Web of Science databases. Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were strictly followed. Data was gathered on the type of trauma, the type of operation, whether or not alcohol was used, the outcomes, and the complications. The study included 12 publications, all of which came to the same conclusion: trauma patients with alcohol intoxication spent more time on mechanical ventilators, had longer Intensive care unit, Length of stay, and had longer hospital stays.
Keywords:
alcohol
; trauma
; outcomes
; surgical complications
; anaesthetic complications hospital length of stay
; mechanical ventilation
; ICU stay
Introduction
Alcohol is the most often abused drug worldwide, causing substantial harm to individuals, families, and society. [9] Alcohol intoxication has a substantial impact on the outcomes of traumatic injuries, altering patient management, surgical treatments, and postoperative care. Several research have investigated the link between alcohol intoxication and various traumatic injuries, offering light on the challenges of treating individuals who have a history of alcohol use. Trauma includes both purposeful and unintentional injuries from car accidents, piercing or blunt violence, falls, firearms, poisons, and burns. [13] Epidemiology studies show that intoxication is becoming more common during trauma injuries, which can impair coordination and reaction times and has been linked to an increased risk of complications after surgery. [3]
Crutcher et al. (2014) investigated the effects of alcohol intoxication on traumatic spinal cord injury outcomes, focusing on the potential role of alcohol intake in the severity and recovery of such injuries. Similarly, Vartan et al. (2020) conducted a statewide examination of rib fractures in patients with alcohol use disorder, emphasizing the relationship between alcohol usage and specific injury patterns. These findings emphasize the need of managing alcohol intoxication as a contributing factor in trauma patients. [1,2] Klifto et al. (2020) conducted a systematic review and meta-analysis of the effects of nicotine/smoking, alcohol, and illegal substance use on burn patient outcomes and complications, emphasizing the multifaceted nature of substance abuse on burn injury management. [3] Hsieh et al. (2013) examined the intriguing question of whether alcohol intoxication could
Protect trauma patients from major harm and lower hospital mortality, demonstrating the intricate relationship between alcohol use, injury severity, and patient survival. [4] Furthermore, Puyana et al. (2021) investigated the effect of elevated blood alcohol levels on burn patient outcomes, providing insight into the difficulty of managing burn injuries in patients with alcohol-related comorbidities. [5] Jung et al. (2023) evaluated the effect of alcohol consumption prior to damage on functional and survival outcomes after catastrophic brain damage, emphasizing the need of considering pre-accident alcohol usage while treating traumatic brain injuries. [6]
This systematic evaluation of 12 studies compared the outcomes and repercussions of trauma patients referred to hospitals with and without alcohol intoxication. According to the data analysed, trauma patients who are drunk with alcohol, before hospitalization have worse outcomes and complications than those who are not.
Objectives
The primary objective of the review is to comparatively evaluate the use of mechanical ventilator post operatively and length of the hospital stay in alcohol intoxicated trauma patients to that of non-intoxicated patients. Secondary objective is to evaluate any anaesthetic complications such as intubation and coagulation in both the groups.
Material and Methods
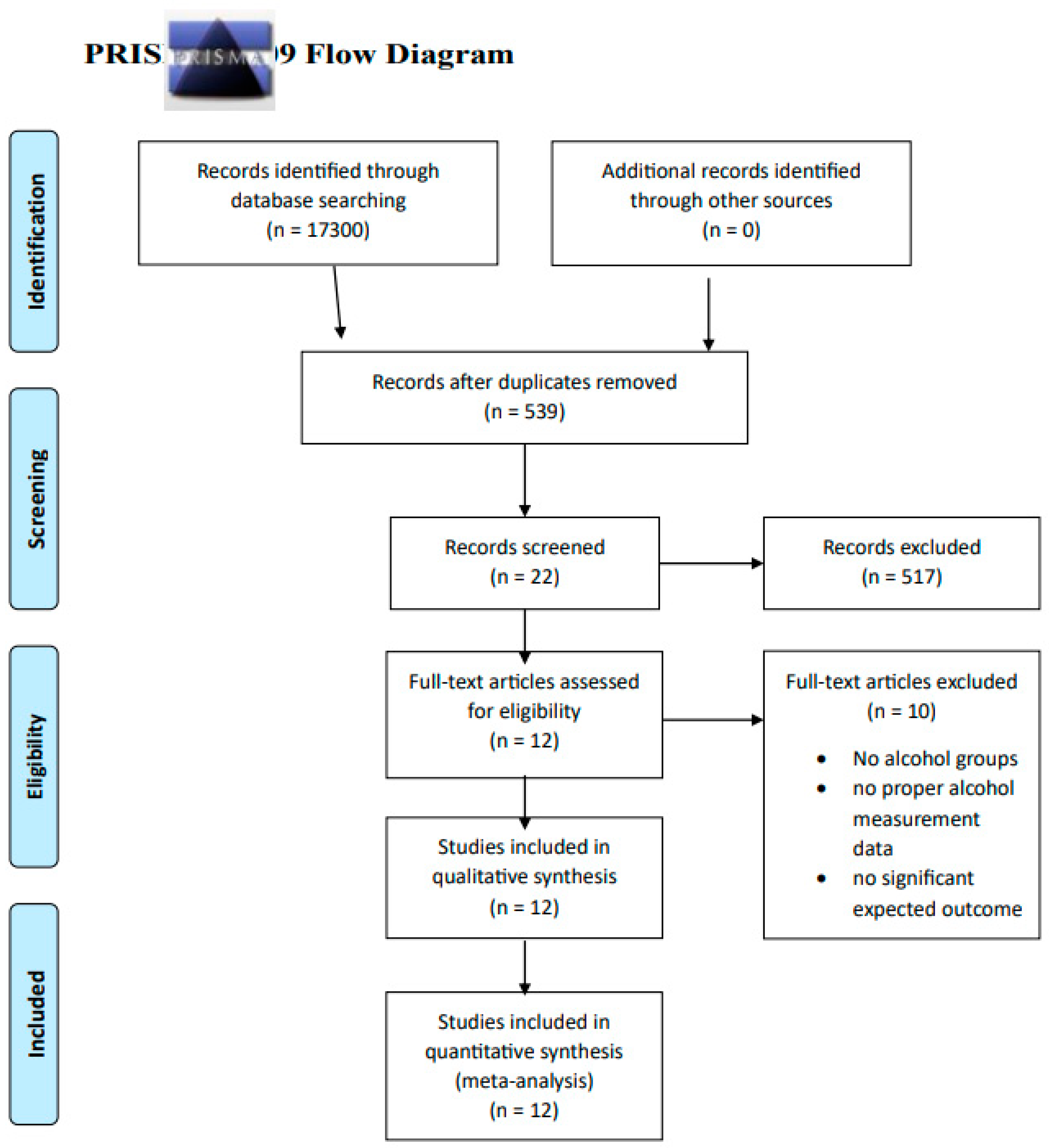
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines was followed in the literature search to create a framework for the review. Multiple search strings which included keywords like “alcohol”, “complications”, “trauma”, “outcomes”, “ICU stay” were built to rigorously search through different data bases (PubMed, Scopus, web of science, google scholar) to extract the required articles. 17300 articles were initially pulled out after the initial search. Both male and female patients of any age with any kind of trauma with alcohol intoxication before the trauma or with a habit of alcohol consumption admitted to the hospital were included in the study. Papers published in the last ten years were considered to narrow down the articles. After applying required filters, the articles were narrowed down to 539.Further specific papers were extracted using search string that included required outcomes like “length of hospital stay” and “use of mechanical ventilator”. Full article papers including review articles, observation prospective studies, retrospective studies, case studies from various parts of the world were extracted. The papers narrowed down to 22 out of which 12 relevant articles which had the expected outcomes were selected for the review.
Alcohol usage in the articles was indicated by a positive blood alcohol concentration (BAC), urine toxicology report, drunkenness, or patient self-report on admission. [3] Injury severity score (ISS), Glassgow coma scale, PT, were measured to assess patient’s condition on arrival.
Outcomes measured in trauma cases (intoxicated and non-intoxicated patients) included comparative complications and severity of complications in both the groups like Mortality, Length of stay, Ventilator days Neurological complications, Pulmonary complications, Pneumonia complications, Renal complications, Haematological complications ,DVT/Reinfections complications ,UTI Ulcer/skin ,Wound complications, Alcohol withdrawal syndrome ,Delirium ,Pneumonia ,Sepsis ,ARDS, Unplanned intubation, myocardial infarction; hypotension and shock, gastroparesis, total parenteral nutrition use, acute respiratory failure, sepsis, central line associated blood stream infection, surgical site infection, , persistent postoperative fistula, postoperative gastrointestinal complication, and withdrawal from either alcohol or drugs, increased LOS. Out of all the mentioned complications, ones with p-value <0.05 were considered significant variables in both the groups. [1,2,3,4,5,6,7,8,9,10,11,12]
Figure 1.
PRISMA FLOW CHART SUMMARIZING THE SCREENING PROCESS AND FINAL ARTICLES SELECTION 5.
Findings and Results
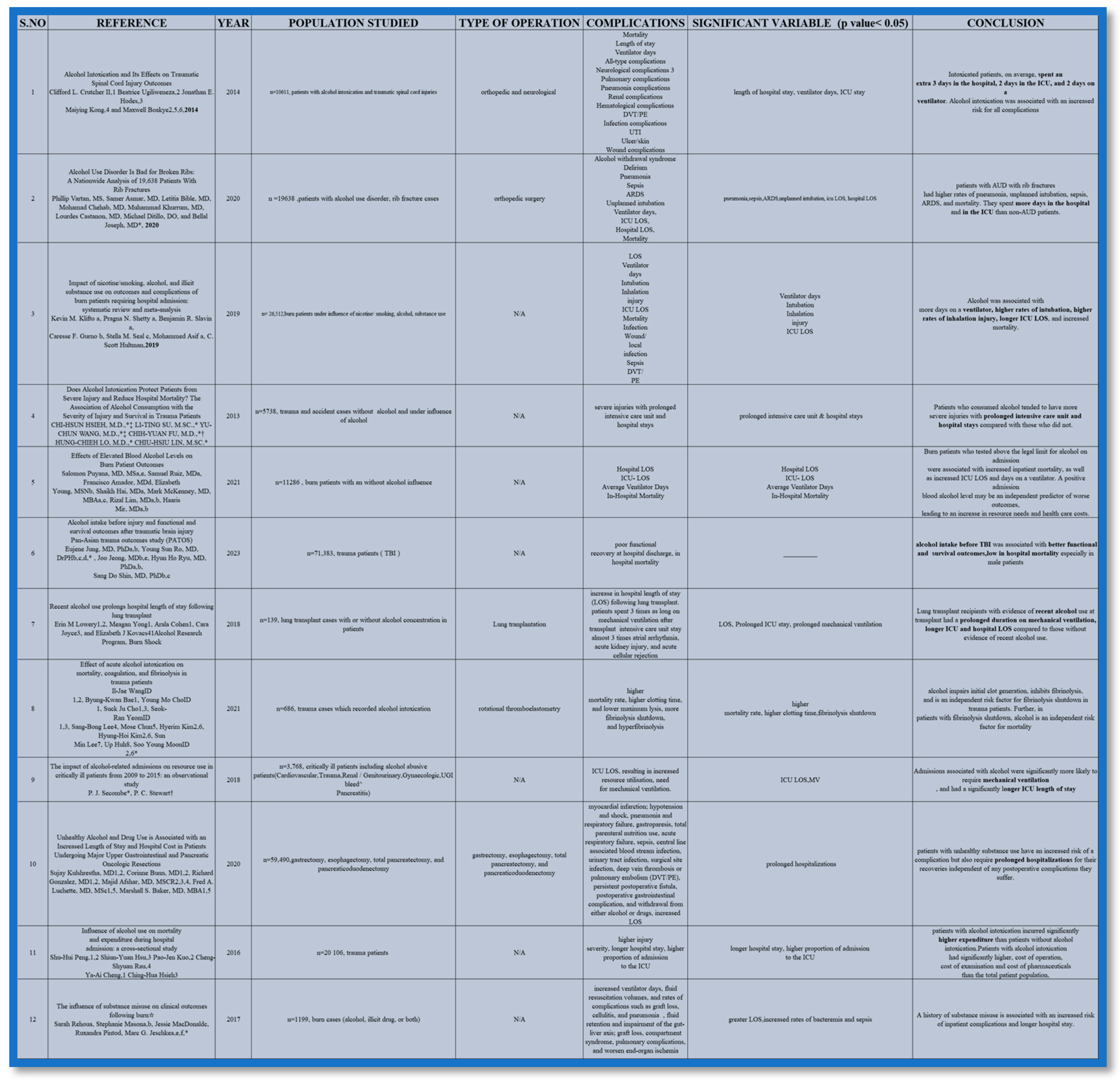
Upon reviewing the literature from different areas of the world made by various doctors, students and research professionals, a findings table (Table 1) was made which included the article being reviewed, year of publication, population studied, complications mentioned, significant variable complications and the conclusions given by each article.
The 12 articles included in the review were published from 2013 through 2023.Out of the 12 articles 11 papers had similar significant variables. A total of 2,30,556 patients were studied in the articles out of which 28,682 patients were intoxicated with alcohol before injury or at the time of arrival at the hospital. BAC>0.08% TO 0.15% is considered a risky level of blood alcohol, therefore all the intoxicated patients were checked for BAC levels and also U-TOX level, ISS score, GCS score. The trauma patients in the papers included traumatic brain injury cases, burn cases, fracture cases, traumatic spinal cord injury cases, transplantation cases, critically ill patient cases post trauma. Out of all the complications recorded significant variables having a p-value <0.05 were taken into consideration. The significant variables in intoxicated patients included prolonged hospital LOS, longer ventilator days, elongated ICU LOS, higher clotting time which means more bleeding complications, sepsis or surgical site infections, unplanned intubation, inhalational injuries. [1,2,3,4,5,6,7,8,9,10,11,12]
Burn patients with alcohol intoxication had significantly higher in-hospital mortality rates (4.86% vs 3.91%) [4]. They also had increased ICU length of stay and total days on a ventilator [4]. Alcohol use was associated with increased morbidity and mortality in thermal injuries [4]. More than half (52.3%) of acute burn patients in one study were under the influence of alcohol at the time of injury. Out of all the trauma patients burn patients were severely impacted by alcohol consumption. [3,5,12]
Discussion and Conclusion
The articles mentioned proper comparison between patients who were under the influence of alcohol versus patients who were not .Clear results were obtained stating the complexity and severity of trauma patients who were intoxicated .11 out of 12 papers indicated prominent post operative complications in intoxicated patients like high percentage of hospital length of stay , increased mortality rates, , prolonged stay on mechanical ventilator , longer ICU LOS , sepsis and anesthetic complications observed were unplanned intubation , higher clotting time, inhalational injury .
In conclusion, this review suggests that trauma patients with alcohol intoxication had higher rate of post operative complications and anesthetic complications when compared to non-intoxicated trauma patients.
References
- Crutcher, C. L., 2nd, Ugiliweneza, B., Hodes, J. E., Kong, M., & Boakye, M. (2014). Alcohol intoxication and its effects on traumatic spinal cord injury outcomes. Journal of neurotrauma, 31(9), 798–802. [CrossRef]
- Vartan, P., Asmar, S., Bible, L., Chehab, M., Khurrum, M., Castanon, L., Ditillo, M., & Joseph, B. (2020). Alcohol Use Disorder Is Bad for Broken Ribs: A Nationwide Analysis of 19,638 Patients with Rib Fractures. The Journal of surgical research, 255, 556–564. [CrossRef]
- Klifto, K. M., Shetty, P. N., Slavin, B. R., Gurno, C. F., Seal, S. M., Asif, M., & Hultman, C. S. (2020). Impact of nicotine/smoking, alcohol, and illicit substance use on outcomes and complications of burn patients requiring hospital admission: systematic review and meta-analysis. Burns: journal of the International Society for Burn Injuries, 46(7), 1498–1524. [CrossRef]
- Hsieh, C.H.; Su, L.T.; Wang, Y.C.; Fu, C.Y.; Lo, H.C.; Lin, C.H. Does alcohol intoxication protect patients from severe injury and reduce hospital mortality? The association of alcohol consumption with the severity of injury and survival in trauma patients. The American surgeon 2013, 79, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Puyana, S., Ruiz, S., Amador, F., Young, E., Hai, S., Mckenney, M., Lim, R., & Mir, H. (2021). Effects of Elevated Blood Alcohol Levels on Burn Patient Outcomes. Eplasty, 21, e8.
- Jung, E., Ro, Y. S., Jeong, J., Ryu, H. H., & Shin, S. D. (2023). Alcohol intake before injury and functional and survival outcomes after traumatic brain injury: Pan-Asian trauma outcomes study (PATOS). Medicine, 102(34), e34560. [CrossRef]
- Lowery, E. M., Yong, M., Cohen, A., Joyce, C., & Kovacs, E. J. (2018). Recent alcohol use prolongs hospital length of stay following lung transplant. Clinical transplantation, 32(6), e13250. [CrossRef]
- Wang, I. J., Bae, B. K., Cho, Y. M., Cho, S. J., Yeom, S. R., Lee, S. B., Chun, M., Kim, H., Kim, H. H., Lee, S. M., Huh, U., & Moon, S. Y. (2021). Effect of acute alcohol intoxication on mortality, coagulation, and fibrinolysis in trauma patients. PloS one, 16(3), e0248810. [CrossRef]
- Secombe, P. J., & Stewart, P. C. (2018). The impact of alcohol-related admissions on resource use in critically ill patients from 2009 to 2015: an observational study. Anaesthesia and intensive care, 46(1), 58–66. [CrossRef]
- Kulshrestha, S., Bunn, C., Gonzalez, R., Afshar, M., Luchette, F. A., & Baker, M. S. (2021). Unhealthy alcohol and drug use is associated with an increased length of stay and hospital cost in patients undergoing major upper gastrointestinal and pancreatic oncologic resections. Surgery, 169(3), 636–643. [CrossRef]
- Peng, S. H., Hsu, S. Y., Kuo, P. J., Rau, C. S., Cheng, Y. A., & Hsieh, C. H. (2016). Influence of alcohol use on mortality and expenditure during hospital admission: a cross-sectional study. BMJ open, 6(11), e013176. [CrossRef]
- Rehou, S., Mason, S., MacDonald, J., Pinto, R., & Jeschke, M. G. (2017). The influence of substance misuse on clinical outcomes following burn. Burns: journal of the International Society for Burn Injuries, 43(7), 1493–1498. [CrossRef]
- Prin, M., & Li, G. (2016). Complications and in-hospital mortality in trauma patients treated in intensive care units in the United States, 2013. Injury epidemiology, 3(1), 18. [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



