
Submitted:
10 December 2024
Posted:
11 December 2024
You are already at the latest version
Abstract
Dengue virus (DENV) infection is a significant global public health concern, with its burden pre-dominantly felt in tropical and subtropical regions. While commonly associated with febrile ill-ness and systemic complications, neurological manifestations beyond cerebrovascular disorders are increasingly recognized but remain underexplored. This scoping review aims to synthesize the current understanding of non-cerebrovascular neurological manifestations of DENV infec-tion, including encephalitis, encephalopathy, myelitis, Guillain-Barré syndrome, acute dissemi-nated encephalomyelitis (ADEM), and neuropathies. A narrative search of peer-reviewed litera-ture was conducted to identify studies reporting clinical presentations, pathophysiological mechanisms, diagnostic approaches, and treatment strategies for these manifestations. Findings suggest that neurological complications often arise from direct viral neuroinvasion, im-mune-mediated mechanisms, or systemic complications such as metabolic disturbances. Key symptoms include altered mental status, seizures, focal neurological deficits, and peripheral nerve involvement. Neuroimaging and cerebrospinal fluid analysis are essential tools for diag-nosis, though challenges remain in differentiating dengue-associated manifestations from other tropical infections. Management is primarily supportive, with corticosteroids and immunomod-ulators employed in immune-mediated conditions. This review underscores the need for height-ened clinical awareness and further research to improve diagnostic accuracy and therapeutic outcomes for dengue-related neurological disorders. Understanding these manifestations is cru-cial for reducing morbidity and improving patient care in endemic regions.
Keywords:
dengue
; dengue fever
; severe dengue
; dengue hemorrhagic fever
; dengue shock syndrome
; aedes aegypti
; neglected tropical disease
; neurology
; neuroimmunology
1. Introduction
Arboviruses are viral diseases transmitted mainly by mosquitoes and other hematophagous arthropods. Several arboviruses are transmitted by mosquitoes, such as Zika virus, dengue, malaria, yellow fever and chikungunya, accounting for millions of deaths each year, especially in third world countries with tropical climates [1]. Unfortunately, due to global warming, the prevalence of these viruses which was previously limited to tropical areas, has been rising significantly even in temperate nations due to unusually higher temperatures in those areas. In this context, arboviruses have posed significant challenges for health systems worldwide.
In 2023, there were more than five million individuals infected with dengue virus, and dengue-related deaths were reported in more than five thousand cases. Noteworthy, these numbers are likely under-reported because most individuals will have minor symptoms or be asymptomatic [2]. Furthermore, there are a rising number of reports of dengue worldwide, and some specialists believe that this can be related to climate changes, since the environmental factors can lead to expansion of the geographical area and population of the vectors [3].
There are four serotypes of the dengue virus (DENV 1–4), which share genetic similarity but are antigenically distinct [4]. Dengue syndrome can be caused by any of the four DENV serotypes. DENV is a member of the Flaviviridae family, which includes other notable arboviruses such as Zika, West Nile, and yellow fever viruses. It is a small, spherical virus approximately 50 nm in diameter. The virus is encased in a lipid bilayer envelope, which is derived from the host cell membrane during viral budding. Embedded in this envelope are the E (envelope) and M (membrane) proteins, which play crucial roles in viral entry into host cells and immune response evasion. DENV’s genome consists of approximately 10.7 kilobases of single-stranded, positive-sense RNA. This RNA encodes a single polyprotein, which is subsequently cleaved into three structural proteins—C (capsid), prM (precursor membrane), and E (envelope)—and seven non-structural proteins, including NS1, NS3, and NS5, which are critical for viral replication and immune modulation. The E protein, in particular, mediates host cell attachment and fusion, while the NS5 protein contains RNA-dependent RNA polymerase and methyltransferase activities essential for viral replication and capping of the RNA genome. This genetic organization allows efficient replication and adaptation in mosquito vectors and human hosts, contributing to the virus’s persistence and widespread transmission. The primary vector of dengue is the female Aedes aegypti mosquito, predominantly found in tropical and subtropical regions. However, due to climate changes associated with global warming, the Aedes albopictus mosquito, another potential vector, has increasingly been identified in temperate regions. [5].
The clinical manifestations caused by DENV infection vary greatly (Table 1). Some patients may only present with a flu-like syndrome also known as dengue fever (DF). However, dengue fever (DF) can sometimes progress to a life-threatening condition known as dengue hemorrhagic fever (DHF), characterized by plasma leakage, severe bleeding, and organ involvement. In severe cases, it may lead to dengue shock syndrome (DSS), marked by circulatory collapse, profound hypotension, and multi-organ failure. These complications result from an exaggerated immune response, increased vascular permeability, and disruption of the coagulation system [6]. Dengue fever typically presents with a sudden onset of acute fever accompanied by a variety of symptoms, including severe headaches, muscle pain (myalgia), joint pain (often referred to as “breakbone fever”), nausea, vomiting, abdominal pain, and skin rashes. Gastrointestinal symptoms such as diarrhea or loss of appetite may also occur. The characteristic rash often appears 2–5 days after the fever onset and can range from a maculopapular to a petechial rash, contributing to the disease’s diagnostic features [5]. Less than 5% of dengue patients develop severe, life-threatening manifestations, such as DHF or DSS. These severe outcomes are more commonly observed in individuals with prior exposure to a different DENV serotype, a phenomenon linked to antibody-dependent enhancement (ADE), where non-neutralizing antibodies from the previous infection facilitate increased viral replication [7]. The clinical outcome of dengue infection is influenced by a combination of factors involving the host (patient), the vector, and the virus. Patient-related factors include age, genetic predisposition, immune status, pre-existing conditions, and prior dengue infections, which may contribute to either protective immunity or severe disease through antibody-dependent enhancement (ADE). Vector-related factors, such as the mosquito species (Aedes aegypti or Aedes albopictus), mosquito density, and feeding behavior, affect the transmission efficiency. Viral factors include the infecting dengue serotype (DENV-1 to DENV-4), virulence, and the genetic diversity of the virus, which can impact replication rates and immune evasion. Together, these factors interact to determine the severity of the disease and clinical progression.
Interestingly, recent evidence has shown that DENV can also affect the central nervous system (CNS), leading to a wide range of neurological manifestations. These manifestations are variable, with reported incidence rates ranging from 0.5% to 21% across different studies. Neurological complications can include encephalitis, encephalopathy, seizures, Guillain-Barré syndrome, myelitis, and other peripheral neuropathies. The underlying mechanisms for these CNS involvement include direct viral invasion of neural tissues, immune-mediated responses, and metabolic disturbances associated with severe dengue. These neurological manifestations can complicate the clinical course and may result in long-term neurological deficits in some patients [8]. The most common DENV serotype associated with neurological disorders appears to be DENV-3. This serotype’s increased association with CNS involvement could be due to factors such as its ability to more effectively invade neural tissues or its propensity to trigger stronger immune responses that may lead to neuroinflammation. However, it is important to note that neurological manifestations can occur with any of the four dengue serotypes, with varying frequencies [9]. In this context, the hemorrhagic manifestations of dengue in the central nervous system (CNS) are among the most well-known and frequently reported neurological complications. These can include subarachnoid hemorrhage, intracerebral hemorrhage, and cerebral venous thrombosis, which are typically seen in severe cases of dengue, such as DHF. The bleeding within the CNS is thought to result from the increased vascular permeability and coagulation abnormalities associated with severe dengue infection. The presence of hemorrhagic manifestations in the CNS is a serious clinical concern and often correlates with poor outcomes, including neurological deficits or even death [10]. However, herein we will describe neurological manifestations that are not related with hemorrhagic or ischemic events.
2. Search Methods
We searched PubMed for articles published until December 2024 without language restriction. We used the term “dengue fever,” “myelitis,” “encephalitis,” “ADEM,” “new daily persistent headache,” “guillain barre syndrome,” “neurological complications.” In this review, we focus on clinical studies, case reports, systematic reviews (with or without meta-analysis), and relevant narrative reviews to examine neurological complications of dengue that are not associated with hemorrhagic or thromboembolic events (Table 2).
3. Discussion
Neurological events in dengue are relatively uncommon, but an increasing number of reports have emerged in recent years, highlighting the growing recognition of these complications. These neurological manifestations can range from mild symptoms such as headaches and dizziness to more severe conditions like encephalitis, encephalopathy, and Guillain-Barré syndrome. In a study conducted by Sahu et al., which enrolled 486 dengue fever patients, the incidence rate of neurological complications was found to be 9.26%. This study reported a variety of neurological manifestations, with the most common being seizures, altered mental status, and focal neurological deficits. The study also emphasized that these complications were more likely to occur in severe cases of dengue and in individuals with previous dengue exposure. The findings underscore the need for heightened clinical awareness and the importance of monitoring neurological symptoms in dengue-endemic areas, especially as more cases with neurological involvement are being reported globally [9]. Nonetheless, a prospective study involving 116 patients revealed a significantly higher incidence of neurological complications, with 79% of the patients presenting with neurological manifestations. Among these, 34% exhibited encephalitis or encephalopathy, characterized by altered mental status, confusion, or seizures, while 45% experienced muscular symptoms, including myalgia, muscle weakness, and even acute flaccid paralysis. This study highlights the broad spectrum of neurological involvement in dengue and underscores the importance of recognizing and managing these complications, particularly in severe cases [11]. Bhushan et al. identified that 4.86% of 1,627 patients DENV infection experienced immune-mediated neurological complications. These complications included conditions such as Guillain-Barré syndrome, acute disseminated encephalomyelitis (ADEM), and other peripheral neuropathies, suggesting that immune responses triggered by DENV infection can contribute to neurological damage. This study highlights the potential for immune-mediated mechanisms in the pathogenesis of neurological complications in dengue, emphasizing the need for early recognition and appropriate management to reduce long-term neurological sequelae [12]. In a study involving 71 confirmed cases of dengue in children, it was found that 28.17% of the patients had central nervous system (CNS) involvement [13]. For a complete understanding of the prevalence of neurological manifestations in patients with DENV infection, read Table 3.
The mechanisms by which dengue affects the central nervous system are yet to be elucidated [8]. Several potential mechanisms have been proposed, including direct viral invasion of neural tissues, immune-mediated damage, and systemic effects such as metabolic disturbances and hypoxia. The virus may enter the CNS via the bloodstream or through the olfactory nerves, potentially leading to encephalitis or encephalopathy. Immune responses triggered by dengue infection, such as antibody-dependent enhancement (ADE), may also contribute to neuroinflammation and neuronal injury. Additionally, alterations in the blood-brain barrier, resulting from increased vascular permeability during severe dengue, may facilitate viral entry into the CNS or exacerbate neurological damage. Further studies are needed to clarify these mechanisms and improve our understanding of how dengue leads to CNS involvement [7].
There are three main mechanisms to explain the neurological manifestations of dengue (Figure 1). The first is related to direct viral invasion of the CNS structures, which can be observed in encephalitis, meningitis, and myelitis. It has also been hypothesized that DENV may cause a systemic infection resulting in ultimately in encephalopathy and stroke. The third proposed mechanism is an immune-mediated infection, which likely results in acute disseminated encephalomyelitis, Guillain-Barre syndrome, and optic neuritis that present after DENV infection [17].
Experimental in vitro and in vivo studies suggest that glial cells and the innate immune response play a significant role in DENV infection of the CNS. Glial cells, including microglia and astrocytes, may serve as both targets and mediators of the immune response to DENV. These cells can become activated during infection, releasing pro-inflammatory cytokines and chemokines that contribute to neuroinflammation. The innate immune response, particularly the activation of pattern recognition receptors such as toll-like receptors (TLRs), can also trigger an inflammatory cascade that may lead to neuronal injury. Additionally, the activation of glial cells can influence the blood-brain barrier’s integrity, potentially facilitating viral entry into the CNS and exacerbating neurological damage. These findings highlight the complex interplay between viral infection, immune response, and glial cell function in the pathogenesis of dengue-related neurological complications [18]. In a study involving rhesus monkeys, no apparent brain histological alterations were observed; however, the study did report a series of virus-induced changes in astrocytes. Specifically, there was a decrease in the number of astrocytes, along with signs of their activation. These alterations suggest that while overt structural damage may not always be evident, DENV infection can still affect glial cell function, leading to a disruption in the normal homeostasis of the central nervous system. Astrocyte activation is often associated with neuroinflammation, which could contribute to the neurological complications observed in dengue infection [19]. There is also evidence of DENV presence in the CSF of infected patients. Studies have detected viral RNA or antigens in CSF samples from individuals with neurological complications associated with dengue infection, such as encephalitis and encephalopathy. The detection of the virus in CSF supports the hypothesis of direct viral invasion of the CNS, which may contribute to the development of neurological symptoms. However, the exact mechanism by which the virus crosses the blood-brain barrier remains unclear, and further research is needed to better understand how DENV affects the CNS [20].
Regarding the immune response, a study found similarities between the cytokine release in dengue infection and that of Japanese encephalitis virus. Several cytokines were detected in the CSF of dengue-infected patients, indicating that an inflammatory response is likely playing a key role in dengue’s CNS involvement. The accumulation of these cytokines in the CSF suggests that neuroinflammation is a significant feature of dengue-associated neurological complications, potentially contributing to the development of encephalitis, encephalopathy, and other CNS disorders. This immune response may exacerbate neuronal damage, highlighting the importance of managing inflammation in severe dengue cases [21]. In this context, Al-Shujairi et al. demonstrated that DENV induces the activation of TCD8 lymphocytes in the CNS of mice. The study also found that genes stimulated by interferon were upregulated, suggesting a virus-driven immune response. This immune activation, including the recruitment of TCD8 lymphocytes and the subsequent inflammatory response, highlights the role of the host’s immune system in contributing to the pathogenesis of neurological complications in dengue infection. The findings further support the notion that immune-mediated mechanisms, including the activation of cytotoxic T cells, play a significant role in dengue-related CNS inflammation [22].
Neurovirulence may be due to some molecular specificities of some subtypes of the DENV virus. The evidence demonstrated in the DENV strain 1 shows a correlation between the domain of helicase E and non-structural-3 (NS3), increasing the capacity for infection and neuronal replication [23]. There are also samples of replication of the DENV2 in neurons [24]. Another study in mice showed behavior similar to anxiety associated with increased inflammatory cytokines such as IL-6 and tumor necrosis factor-alpha (TNF) and neuronal loss in the hippocampus [25]. These findings are corroborated by another study, which found that DENV 3 induces meningoencephalitis and behavioral changes in mice [26].
3.1. Guillain-Barre Syndrome
Guillain-Barré syndrome (GBS), also known as acute idiopathic polyradiculoneuropathy, is an acute, inflammatory, demyelinating, and immune-mediated neurological disorder. The hallmark features of GBS include areflexia (loss of reflexes), ascending motor paralysis, and an elevated protein concentration in the CSF without an increase in white blood cells (pleocytosis), a phenomenon known as albuminocytological dissociation. This pattern is characteristic of GBS and reflects the disruption of the blood-nerve barrier and inflammatory changes in the peripheral nervous system. GBS is often triggered by infections, including viral infections like dengue, and the immune system’s response can damage peripheral nerves, leading to muscle weakness and, in severe cases, respiratory failure. Early diagnosis and prompt treatment, such as intravenous immunoglobulins or plasmapheresis, are crucial for improving outcomes [8]. In GBS, approximately 70% of cases are preceded by a respiratory or gastrointestinal infection, typically viral, occurring 1 to 3 weeks before the onset of neurological symptoms. The most common microbiological agents associated with GBS include Cytomegalovirus, Epstein-Barr virus, Campylobacter jejuni, Mycoplasma pneumoniae, and HIV. These infections are believed to trigger an immune response that mistakenly targets peripheral nerves, leading to the inflammatory and demyelinating effects characteristic of GBS. The immune response may involve molecular mimicry, where the immune system attacks nerves that share similar structures to those of the pathogen, contributing to the development of GBS [27]. A study from Mexico found 14.5 cases of GBS for every 10000 individuals diagnosed with dengue [28]. In Brazil, Matos et al. found a prevalence of 10% of dengue in individuals with GBS in an endemic area of dengue [29]. For a list of cases of GBS associated with DENV infection, read Table 4.
GBS and its variants account for 5% of neurological complications in pediatric patients with dengue fever (DF). The typical time between the onset of dengue symptoms and the development of GBS is approximately eleven days [32]. Acute motor and sensory axonal neuropathy (AMSAN) was the most common subtype of Guillain-Barré syndrome (GBS) in these patients with dengue fever. AMSAN is characterized by the damage to both motor and sensory axons, often leading to severe, rapidly progressing weakness, sensory loss, and respiratory complications. It typically involves the peripheral nervous system’s axonal structures, with an autoimmune response that damages the axonal membrane and disrupts nerve conduction. Following AMSAN, the next most common subtype was acute motor axonal neuropathy (AMAN), which primarily affects motor axons, leading to paralysis without significant sensory involvement. AMAN is often less severe than AMSAN but still results in considerable motor weakness and can involve respiratory muscles, requiring close monitoring. Acute inflammatory demyelinating polyradiculoneuropathy (AIDP) is the classic form of GBS and was also observed, though less frequently. AIDP involves the inflammatory destruction of the myelin sheath surrounding peripheral nerves, leading to muscle weakness and sensory disturbances, often in a symmetric and ascending pattern. It is more commonly associated with viral infections. Lastly, Miller Fisher syndrome (MFS), a rare variant of GBS, was also reported. MFS typically presents with ataxia, ophthalmoplegia, and areflexia. It is often considered a variant of GBS, though its pathophysiology may differ slightly, and it is more often associated with infections such as Campylobacter jejuni but can also occur with dengue [12]. Both GBS and MFS are associated with immune-mediated complications of DF [35]. Another variant of GBS reported in association with dengue fever is the pharyngeal-cervical-brachial variant. This variant primarily affects the muscles of the throat, neck, and upper limbs, leading to symptoms such as dysphagia (difficulty swallowing), respiratory distress, and weakness in the arms and shoulders. It is considered a rare but significant manifestation of GBS in dengue-infected patients, reflecting the diverse range of neurological complications that can arise from the infection [34].
An intriguing case report described two brothers who simultaneously developed the axonal variant of GBS following DENV infection [33]. Although neither of the two brothers exhibited typical symptoms of dengue fever, this case report supports the possibility of a genetic predisposition contributing to the development of GBS following DENV infection. The simultaneous onset of the axonal variant of GBS in both siblings suggests that genetic factors may play a role in their heightened susceptibility to immune-mediated complications associated with dengue. This raises the possibility that certain genetic markers or immune system variations could predispose individuals to develop GBS or other neurological manifestations when infected with the DENV.
Since most cases of GBS occur after the acute phase of dengue, it is widely believed that these manifestations have an immunological origin. The immune system’s response to the DENV, possibly involving mechanisms like molecular mimicry or the activation of autoreactive immune cells, is thought to contribute to the development of GBS. This delayed onset, typically one to three weeks after the initial infection, suggests that GBS is a post-infectious complication driven by the body’s immune response rather than direct viral invasion of the nervous system [35]. The evidence supporting the immunological origin of GBS following dengue infection is based on the involvement of similar pro-inflammatory substances in both conditions. These substances, including tumor necrosis factor (TNF), interleukins, and complement proteins, play key roles in the immune response against the DENV and in the pathogenesis of GBS. The immune response triggered by dengue may inadvertently cross-react with peripheral nerve tissues due to molecular mimicry, where antibodies or immune cells target components of the nervous system, such as myelin or peripheral nerve axons. This cross-reactivity may contribute to the development of GBS following dengue infection [31].
A common presentation of dengue and lower extremity weakness is related to hypokalemia, which was already reported in adults and pediatric individuals [42]. A basic metabolic panel should be obtained because they are usually misdiagnosed with GBS due to the symptoms of distal weakness and decreased reflexes. Hypokalemia is found in around 1.3 to 13.7% of the cases of dengue and severe dengue respectively [43,44].
3.2. Myopathy
Myalgia is a common symptom of dengue fever, with studies showing that up to 90% of patients report muscle pain as part of their illness. This widespread occurrence of myalgia is often considered one of the hallmark symptoms of dengue, along with fever, headaches, and joint pain. The muscle pain in dengue is typically intense and can be associated with general malaise, further contributing to the overall discomfort experienced by patients [45]. Muscular alterations were detected in biopsies from 12 out of 15 patients who did not report muscle weakness, suggesting that muscular changes can occur even in the absence of overt symptoms. This indicates that muscle involvement may be more widespread in dengue patients than previously recognized, and some individuals may experience subclinical or asymptomatic muscular alterations that do not manifest as weakness but may still contribute to the overall disease process [46]. For a full understanding of the cases of myopathy associated with DENV infection, read Table 5.
Myopathy is a common complication of dengue infection. In a study of 116 patients, 34 exhibited muscle weakness and elevated creatine kinase (CK) serum levels, highlighting the prevalence of muscle involvement in dengue cases. This suggests that muscle dysfunction, including weakness and increased CK levels, is a significant aspect of the disease’s clinical presentation [11]. In another study, 14 out of 30 patients with acute myopathy were diagnosed with dengue fever. Of these 14 patients, 9 had normokalemia, indicating that dengue-associated myopathy can occur regardless of potassium levels. The presence of normokalemia in a majority of the cases suggests that other factors, apart from electrolyte imbalances, may contribute to the development of myopathy in dengue fever [53].
The severity and clinical presentation of acute myopathy associated with dengue fever can vary widely, ranging from subclinical elevations in creatine kinase (CK) levels to severe muscle weakness. This variability underscores the diverse spectrum of muscle involvement in dengue infection, with some patients exhibiting only mild biochemical changes, while others experience significant muscular dysfunction that can severely impact mobility and overall health [50,52]. Rhabdomyolysis and myocarditis can occur simultaneously with dengue acute myopathy, further complicating the clinical picture. These serious complications can lead to severe muscle damage, electrolyte imbalances, and cardiac dysfunction, increasing the risk of organ failure. Prompt diagnosis and intervention are critical to managing these co-occurring conditions and preventing long-term damage [48]. Electromyography (EMG) studies, when performed in patients with dengue-related myopathy, typically do not reveal characteristics of inflammatory myositis. This suggests that, despite the presence of muscle weakness and elevated creatine kinase (CK) levels, the muscle dysfunction in dengue may not be primarily due to an inflammatory process. Instead, it may result from other mechanisms, such as viral-induced muscle injury or metabolic disturbances [51].
Myopathy associated with dengue is typically self-limited and does not result in long-term sequelae. Most patients experience a full recovery, with muscle weakness and elevated creatine kinase (CK) levels resolving within a few weeks. However, early recognition and appropriate management are essential to ensure a smooth recovery and prevent complications in severe cases [52]. In 2006, Finsterer and colleagues reported a case of a 38-year-old male who contracted dengue fever during a holiday in Thailand. He presented with fever, headache, and sore eyes, accompanied by intense myalgia rated 10/10 on a visual scale, which persisted for over 60 days. Electromyography revealed spontaneous activity in the subscapularis muscle. After three weeks of corticosteroid treatment, the myositis resolved, highlighting the potential for prolonged muscle pain and the need for corticosteroid therapy in severe cases of dengue myopathy [47].
It is worth mentioning that dengue can lead to GBS and also myositis, and sometimes the pattern of involvement is difficult to be isolated. Gulia et al. reported a case of a patient developing both GBS and myositis [59].
3.3. Encephalitis
Encephalopathy, as a manifestation of dengue fever, is more commonly secondary to multisystem complications caused by infectious factors such as shock, hepatitis, coagulation disturbances, and even concomitant bacterial infections. These systemic issues can exacerbate the effects of the virus on the central nervous system, leading to encephalopathy in some patients. This highlights the complex interplay between dengue and other complications that may contribute to neurological manifestations [60]. However, this mechanism is different when it comes to encephalitis (Table 6).
In the study by Bhushan et al., of the 79 patients with immune-mediated neurological complications, 9 developed acute disseminated encephalomyelitis (ADEM), 3 experienced isolated cerebellar demyelination, and 1 was diagnosed with limbic encephalitis [12]. Considering these three manifestations, it was found that 0.8% of patients with dengue fever developed encephalitis associated with DENV infection. This suggests that encephalitis, while rare, can occur as a complication of dengue infection. In a separate pediatric study, which had a smaller sample size of 71 patients, a higher incidence of 8% of children was reported to have encephalitis related to dengue fever. Tragically, 3 out of 4 children with dengue-related encephalitis in this study died, highlighting the severe and potentially fatal nature of encephalitis in the context of dengue infection, especially in younger patients. This increased mortality rate underscores the importance of early diagnosis and intervention in managing severe complications like encephalitis in dengue cases [13]. Fong et al. reported 10% of prevalence of DENV infections in patients with acute necrotising encephalopathy in the pediatric population from Malaysia [82].
Although rarer, dengue encephalitis is caused by direct neuronal infiltration of the DENV. The virus can induce neurological damage both through direct infection of the neurons and by triggering immunological mechanisms. The immune response to the virus can lead to inflammation and tissue damage in the brain, which may contribute to neurological symptoms such as altered mental status, seizures, and focal neurological deficits. The exact mechanisms of how the immune system contributes to this damage are not fully understood but likely involve an exaggerated inflammatory response or immune-mediated injury. This dual mechanism—direct viral invasion and immune-mediated damage—can lead to severe neurological complications in some patients [60]. While dengue is not traditionally classified as a neurotropic virus, meaning it does not typically target the nervous system, there is increasing evidence linking it to encephalitis. This neurological complication is distinct from encephalopathy (a general term for brain dysfunction), and it is not associated with the other common features of dengue, such as fever or rash. Dengue-related encephalitis is considered when CSF analysis reveals the presence of the DENV or dengue IgM antibodies, indicating direct involvement of the virus in the central nervous system. The detection of these markers helps differentiate dengue encephalitis from other neurological conditions and supports the diagnosis of viral encephalitis caused by dengue [61]. Encephalitis in dengue occurs during the viremic stage of the disease, when the virus is present in the bloodstream, whereas encephalopathy typically develops later, after the acute phase of the infection has subsided. Encephalitis is a direct consequence of the virus’s ability to invade the central nervous system, while encephalopathy is a more generalized brain dysfunction that may result from immune or metabolic factors related to the infection. Evidence suggests that DENV-2 and DENV-3, two of the four DENV serotypes, are the most commonly associated with neurotropism—the ability of the virus to infect and damage nervous tissue. These serotypes have been more frequently identified in cases of dengue-related encephalitis, indicating a stronger propensity to affect the brain compared to other serotypes [71]. There are anecdotal reports of DENV-4 found in the CSF in patients with encephalitis [83]. Also, some authors recommend performing nonstructural protein 1 (NS1) antigen in the CSF to differentiate dengue encephalitis from encephalopathy [84].
In cases where encephalitis is present, the manifestation typically includes headache, confusion, dizziness, disorientation, behavioral symptoms, and drowsiness. These symptoms reflect the neurological impact of the infection, which can range from mild cognitive disturbances to more severe alterations in consciousness and behavior [8]. Occasionally, patients with dengue-related encephalitis may also experience cranial nerve palsy, diminished deep tendon reflexes, hypotonia, and hemiparesis. Seizures are not commonly observed, but there have been reports of patients progressing to coma in severe cases. These additional neurological manifestations highlight the potential for varied and serious outcomes in individuals with dengue encephalitis [71]. Dengue-related encephalitis may be accompanied by typical dengue symptoms such as fever, arthralgia, myalgia, and vomiting. In addition to these, leukopenia, thrombocytopenia, and anemia are common findings, which are characteristic of the viral infection itself. These hematological abnormalities occur as a result of the virus’s impact on bone marrow function and immune system response, contributing to the overall clinical picture of severe dengue [71].
Diagnostic criteria for dengue-related encephalitis dictate the management approach. As established by Carod-Artal et al., the diagnosis requires the presence of clinical signs and symptoms of central nervous system (CNS) injury, along with confirmation of DENV involvement. This includes positive testing for DENV RNA, IgM, or NS1 antigen in cerebrospinal fluid (CSF), along with the presence of CSF lymphocytic pleocytosis (an elevated white blood cell count in the CSF, indicating inflammation). It is also essential that other neuroinvasive pathogens are ruled out, which is done by testing negative for other potential infectious diseases. These criteria help ensure an accurate diagnosis and appropriate treatment for patients with dengue-related encephalitis [8]. Following this assay, Cristiane and colleagues, in a supplementary study, defined dengue encephalitis as the presence of fever along with acute signs of cerebral involvement, such as confusion or altered consciousness. The diagnosis was further supported by the detection of reactive IgM antibodies, NS1 antigen, or positive dengue PCR in both serum and CSF. Additionally, the definition required the exclusion of other viral causes of encephalitis and encephalopathy to ensure that the symptoms were directly attributable to dengue. This approach helped refine the criteria for diagnosing dengue encephalitis, distinguishing it from other potential neurological complications [62].
Neuroimaging in DENV encephalitis usually shows no major abnormalities [64]. Vyas et al. reported normal brain MRI (magnetic resonance imaging) in only 30% of the individuals with dengue encephalitis, the other individuals had encephalitic and encephalopathic changes, and interestingly, around 15% had micro/macro-hemorrhages [85]. Once the affection is verifiable through MRI, dengue-related encephalitis is commonly demonstrated as abnormal multifocal hyperintensity on T2-weighted (T2W) and Fluid-Attenuated Inversion Recovery (FLAIR) sequences. These abnormalities are typically seen in both hemispheres, the periventricular zones, and the basal ganglia, areas of the brain involved in movement and coordination. These imaging findings reflect the inflammation and damage caused by the virus in the central nervous system [66]. Some distinctive patterns have been associated with dengue encephalitis on MRI, including the “double doughnut sign” and the “Jack-o’-lantern sign.” These patterns are related to the bilateral nature of the lesions seen in dengue-related encephalitis. The “double doughnut sign” refers to ring-like hyperintensities on T2W or FLAIR sequences, which are seen in the basal ganglia or periventricular areas. Similarly, the “Jack-o’-lantern sign” describes lesions that appear with a central area of hypointensity surrounded by a hyperintense rim, resembling a jack-o’-lantern shape. These patterns are not only characteristic of dengue encephalitis but also help in differentiating it from other causes of encephalitis [69]. In cases of dengue encephalitis, the thalamic double doughnut sign should be used to further specify the diagnosis, but there are no studies regarding the prevalence of this finding in cases of dengue encephalitis. Other areas reported to be affected in dengue-related encephalitis include the brainstem, cerebellum, corpus callosum, and bilateral thalami. In some patients, the lesions may involve both white and gray matter of the brain. These regions are critical for functions such as motor control, coordination, communication between brain hemispheres, and sensory processing. The involvement of both types of brain tissue suggests a widespread inflammatory response in the central nervous system, which can contribute to the diverse neurological symptoms observed in dengue encephalitis [64]. Noteworthy, tumefactive lesions were already observed with DENV encephalitis [86].
Regarding laboratory analysis, the dengue NS1 antigen test must be positive in serum to confirm the infection. CSF is typically described as colorless and transparent, with the presence of lymphocytic pleocytosis, indicating inflammation. Additionally, CSF testing should be negative for other infectious serologies, helping to rule out other potential causes of encephalitis. This combination of findings aids in diagnosing dengue-related encephalitis and differentiating it from other neurological infections [61]. IgM testing in the CSF using enzyme-linked immunosorbent assay (ELISA) for dengue antibodies is widely applied and reliable in diagnosing dengue-related encephalitis. This test has both high sensitivity (92%) and specificity (99%), making it a valuable tool in clinical practice. The presence of IgM antibodies in the CSF indicates recent DENV infection and supports the diagnosis of dengue encephalitis, particularly when other potential causes of encephalitis have been ruled out [71]. The gold standard for diagnosing dengue-related encephalitis would be isolating the virus in cell culture, followed by antibody identification through fluorescence. This method, while highly accurate, is rarely used in clinical practice due to its technical complexity and limited availability in many settings. As a result, other diagnostic tests, such as NS1 antigen detection and IgM antibody testing, are more commonly employed for practical and timely diagnosis [66].
It is equally important to test both the serum and CSF for other potential causes of encephalitis, including herpes simplex virus, Mycobacterium tuberculosis, cytomegalovirus, human T cell lymphotropic virus type-1, Epstein-Barr virus, and varicella-zoster virus. These tests help rule out other infectious agents that could be responsible for the neurological symptoms. Once the results for these viruses and pathogens are negative, it strengthens the diagnosis of dengue-related encephalitis, allowing for more targeted management [12].
Moreover, encephalitis must be distinguished from encephalopathy of other etiology. In such cases, detecting the DENV, NS1 antigen, or IgM dengue virus-specific antibodies in the CSF will support the diagnosis of dengue-related encephalitis. These diagnostic markers help differentiate between encephalitis caused by dengue and encephalopathy resulting from other underlying conditions, ensuring that appropriate treatment is administered [8]. The presence or absence of the Japanese encephalitis virus IgM is helpful to detect its presence which is one of the main differentials [70]. It is necessary for physicians to be aware of cross-reactivity and to consider the epidemiology context. The PCR exam can determine the concomitant infection of both viruses [67].
Although there is no specific antiviral agent for the DENV, treatments such as acyclovir, corticosteroids, and sodium valproate are occasionally used in the management of dengue encephalitis. Acyclovir may be used as an empirical treatment in cases where herpes simplex virus or other viral infections are suspected. Corticosteroids are sometimes employed to reduce inflammation in the central nervous system, while sodium valproate may be used to manage seizures, which can occur in severe cases of dengue encephalitis. However, the mainstay of management remains supportive care, as there is no proven antiviral therapy specifically for dengue-related encephalitis [71]. Supportive care is always necessary in the management of dengue encephalitis. This includes the use of antipyretic drugs to manage fever, analgesics for pain relief, and oral rehydration to prevent dehydration. These measures help alleviate symptoms and maintain hydration, which is crucial for patient recovery. On the other hand, the use of most non-steroidal anti-inflammatory drugs (NSAIDs), particularly acetylsalicylic acid (aspirin), is contraindicated in dengue cases. NSAIDs can increase the risk of bleeding, a common complication of dengue, and should be avoided to prevent worsening of this risk [8]. Mun et al. reported a case of encephalitis that was responsive to steroids [79], but there are reports of steroid-resistant dengue encephalitis [87].
Post-mortem analysis in patients with dengue-related encephalitis typically reveals non-specific edema lesions in the brain. These lesions are characterized by swelling of brain tissue, which is a common response to inflammation or injury. The edema observed is often diffuse and non-specific, meaning it does not point to a particular underlying cause or pattern of damage. This type of lesion reflects the generalized brain inflammation seen in severe cases of dengue encephalitis. However, further histological examination may reveal other subtle signs of viral infection or immune-mediated damage [8]. In cases where an autopsy was performed, the histopathological patterns observed in the brains of patients with dengue-related encephalitis included cerebral edema, vascular congestion, hemorrhage, perivascular lymphocyte infiltration, inflammation, and brain matter necrosis. These findings indicate significant damage to the brain tissue, with swelling, blood vessel changes, immune cell infiltration, and areas of tissue death, all of which are consistent with severe inflammation caused by the viral infection. These pathological features help confirm the diagnosis of dengue encephalitis and provide insight into the extent of the neurological damage [68]. Through immunoperoxidase staining, the presence of DENV antigens can be detected in brain tissue. This technique uses antibodies that specifically bind to DENV proteins, allowing for visualization of the virus within the brain tissue. Immunoperoxidase staining can help confirm the diagnosis of dengue encephalitis by identifying viral particles or antigens in the affected areas, such as neurons or inflammatory cells, and it plays a crucial role in understanding the pathogenesis of the disease [71].
There are some anecdotal reports in the literature of dengue fever presenting with psychosis and maniac episodes [88]. Several aspects including high fevers and even encephalitis by DENV can explain these findings that were already observed in the pediatric and adult population [89]. Clues for the diagnosis of this zoonose include the fact that the patient developed fever and coagulation abnormalities, but some patients may be challenging to diagnose especially in cases of mild fever and nonspecific pain [90].
Seizures
There are divergent reports in the literature regarding the prevalence of seizures associated with DENV infection [91]. Some authors describe that as a common finding and that the most frequent semiology is generalized tonic-clonic and epilepsia partialis continua [8]. Others describe that it is an uncommon finding affecting around three percent of the patients affected by DENV [92]. Though not specific, electroencephalogram (EEG) often demonstrates generalized slow waves in cases of encephalitis. These slow waves can be indicative of brain dysfunction, though they are not exclusive to encephalitis. Such changes are frequently attributed to factors like seizures, intracranial hemorrhage, or viral infection, all of which can contribute to altered brain activity. While EEG findings provide valuable insight into the neurological state of the patient, they must be interpreted in conjunction with other clinical and diagnostic information to confirm the underlying cause [71].
3.4. Myelitis
Spinal cord involvement, particularly transverse myelitis (TM), is not a common manifestation of DENV infection, but it should not be ignored. In a study by Sahu et al., out of 484 patients who developed neurological complications, 45 cases were identified, and 7 of those patients had myelitis, resulting in an incidence of 1.4%. While relatively rare, the occurrence of myelitis in dengue infection highlights the potential for serious neurological involvement beyond the more typical manifestations like encephalitis [9]. Additionally, in a study involving 1,627 patients, 79 presented with neurological immune-mediated syndromes. Among these, nine patients had acute disseminated encephalomyelitis, while five had myelitis alone. This further emphasizes that while neurological complications in dengue are relatively rare, they can present in a variety of forms, including both encephalitis and myelitis, highlighting the diverse impact the virus can have on the nervous system [12]. In a study by Sil et al., 5% of the pediatric patients with dengue infection were found to have myelitis as a neurological complication. This highlights that, although rare, myelitis can occur in children with dengue, further illustrating the diverse neurological manifestations of the infection in different age groups [13].

Table 7.
Myelitis associated with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Soares et al. (2006) [93] | Brazil | 13 | Thirteen patients, including ten females and three men aged 11 to 79 years, developed dengue fever during the 2002 epidemic in Rio de Janeiro and experienced neurological complications. Two of these patients developed myelitis with paraparesis and sphincter retention, although MRI results were abnormal in only one case. CSF analysis revealed that both patients had an elevated Albumin Quotient, suggesting blood-CSF barrier dysfunction, and one also had intrathecal synthesis of antibodies. Additionally, both patients showed high cell and protein levels in the CSF, which indicated direct viral invasion and acute inflammation. |
| Puccioni-Sohler et al. (2009) [94] | Brazil | 10 | This retrospective study examined ten patients, aged 22 to 74, who were seropositive for dengue IgM/IgG and presented with neurological symptoms. Among them, three were diagnosed with transverse myelitis, based on MRI findings of the spine and inflammatory changes in the cerebrospinal fluid (CSF). Additionally, one patient showed intrathecal synthesis of dengue antibodies in the CSF, suggesting a possible direct viral involvement in the spinal cord. The findings highlight the potential for DENV to cause neurological complications, including spinal cord involvement, even in patients without typical encephalitis symptoms. |
| Chanthamat et al. (2010) [95] | Thailand | 1 | A 61-year-old female developed acute paraplegia, sensory loss, and urinary retention six days after the onset of dengue fever. She was diagnosed with transverse myelitis (TM) and was promptly treated with immunomodulatory therapy. After one month of treatment, she made a full recovery. This case underscores the potential for dengue to cause neurological complications, even in the absence of typical encephalitis symptoms, and highlights the effectiveness of early intervention in managing such complications. |
| Larik et al. (2012) [96] | India | 1 | An adolescent male patient presented with high-intensity low back pain and was diagnosed with longitudinally extensive transverse myelitis (LETM) four weeks after the onset of dengue infection. This case illustrates the potential for severe neurological complications, such as LETM, to develop weeks after the initial viral infection, emphasizing the importance of early detection and management. |
| Tomar et al. (2015) [97] | India | 1 | A middle-aged male developed longitudinally extensive transverse myelitis (LETM) during the acute parainfectious phase of dengue fever. On the third day of fever, he began experiencing neurological symptoms, including lower limb weakness, urinary retention, and sensory impairment. Despite the typically poor prognosis associated with LETM, the patient responded well to intravenous corticosteroid treatment and made a full recovery, with no residual neurological deficits. This case highlights the potential for recovery even in severe cases of dengue-related myelitis when treated promptly. |
| Fong et al. (2016) [98] | Malaysia | 1 | A 12-year-old girl became the first reported pediatric case of longitudinally extensive transverse myelitis (LETM) associated with dengue fever. On the 8th day of infection, she developed flaccid quadriplegia. She was treated with pulse methylprednisolone, intravenous immunoglobulin, and plasmapheresis, eventually achieving near-complete recovery after six months, with only mild residual limb weakness. This case highlights both the severity of neurological complications in pediatric dengue patients and the potential for recovery when treated aggressively. |
| Patras et al. (2016) [99] | India | 1 | Transverse myelitis in an 8-month-old child. |
| Mota et al. (2017) [100] | Brazil | 1 | A 21-year-old male patient with dengue fever developed transverse myelitis (TM). This case indicates that the actual prevalence of dengue-associated TM may be significantly underestimated, suggesting the need for greater clinical vigilance and further research to better understand the neurological complications of dengue. |
| Badat et al. (2018) [101] | United Kingdom | Not applicable | Until 2017, there were 61 cases of dengue and myelitis in the literature. They represented 2.3% of the presentation of dengue. |
| Chaudhry et al. (2018) [102] | India | 1 | A 55-year-old female who tested positive for the dengue IgM antibody developed spontaneous subarachnoid hemorrhage and longitudinally extensive transverse myelitis (LETM). She was treated with pulse methylprednisolone therapy and physical rehabilitation. However, after a one-month follow-up, she showed minimal improvement, underscoring the severity and difficult prognosis of neurological complications related to dengue infection, despite appropriate treatment. |
| Lana-Peixoto et al. (2018) [103] | Brazil | 2 | Two patients diagnosed with neuromyelitis optica spectrum disorder (NMOSD) developed symptoms following dengue fever (DF) infection. Both patients tested positive for aquaporin-4 (AQP4) antibodies, a hallmark of NMOSD, indicating an autoimmune response triggered by the viral infection. In both cases, the patients experienced neurological complications typical of NMOSD, such as transverse myelitis and optic neuritis, after recovering from the acute phase of dengue. This suggests that dengue infection may potentially act as a trigger for NMOSD in predisposed individuals, highlighting the complex interplay between viral infections and autoimmune disorders. |
| Malik et al. (2018) [104] | India | 1 | An adolescent patient presented with symptoms of transverse myelitis (TM) four weeks after contracting dengue fever (DF). The authors discuss the distinction between the acute (parainfectious) and late (post-infectious) stages of dengue with neurological manifestations. They suggest that in the parainfectious phase, the DENV directly infects the spinal cord, leading to neurological symptoms. In contrast, the post-infectious phase is primarily characterized by immune-mediated reactions that contribute to the development of neurological complications such as TM. This distinction emphasizes the different mechanisms involved in dengue-related neurological damage at various stages of infection. |
| Landais et al. (2019) [105] | France | 1 | A 24-year-old female developed myelitis on the 7th day of dengue fever. Spinal MRI revealed diffuse hyperintense lesions in the spinal cord, suggesting acute inflammation. She was treated with intravenous pulse methylprednisolone, immunoglobulin plasmapheresis, and physiotherapy. After five months of treatment, she achieved almost complete recovery, with only mild residual symptoms. This case highlights the potential for significant neurological recovery with appropriate and timely treatment in dengue-related myelitis. |
| Singh et al. (2019) [106] | India | 1 | Patient improved with steroid course. |
| Tan et al. (2019) [107] | Malaysia | 1 | Longitudinal extensive myelitis. High-index of suspicion in endemic regions is needed. |
| Comtois et al. (2021) [108] | Canada | 1 | Positive aquaporin-4 IgG titer in individual with longitudinal extensive myelitis. |
| Karishma et al. (2024) [109] | Pakistan | 1 | Acute transverse myelitis with serology positive for immunoglobulin M to DENV and non-structural protein |
| Kumar et al. (2024) [109] | India | 1 | Dengue serology positive in the CSF |
| Mangudkar et al. (2024) [110] | India | 1 | IVIG and steroids IV and taper. |
| Shrestha et al. (2024) [111] | Nepal | 1 | Drastic improvement with steroid course. |
When transverse myelitis (TM) occurs, it can be associated with challenging clinical recovery, often leading to long-term disability. The severity of neurological damage and the extent of recovery can vary, but in many cases, the condition results in lasting impairments, such as weakness, sensory loss, or bladder dysfunction, which may require prolonged rehabilitation and management. Early diagnosis and treatment are crucial to improving outcomes, although complete recovery is not always achievable [96]. When a spinal injury involves more than three vertebral segments, it is classified as longitudinally extensive transverse myelitis (LETM), a rare and more severe form of myelitis. LETM can result in significant morbidity, including severe neurological impairments such as paralysis, sensory deficits, and bladder dysfunction. Due to the extensive involvement of the spinal cord, the condition often requires intensive treatment and rehabilitation, and recovery may be incomplete, leading to long-term disability in many cases [98].
Symptoms commonly associated with transverse myelitis (TM) include weakness or paralysis of the upper and lower limbs, urinary retention, and sensory alterations such as numbness or tingling. These symptoms result from inflammation of the spinal cord, which disrupts normal nerve function. Depending on the severity and extent of the inflammation, individuals may experience varying degrees of motor and sensory deficits, which can significantly impact daily functioning and quality of life [102]. It is suggested that temporal factors significantly influence the presentation of pathology in transverse myelitis (TM). During the acute phase, patients typically exhibit flaccid paralysis, which is associated with direct viral or inflammatory damage to the spinal cord. In contrast, during the post-infectious stage, which often begins 1-2 weeks after the initial symptoms, patients are more likely to present with spastic weakness, a condition that results from the spinal cord’s response to immune-mediated damage. This distinction highlights the evolving nature of TM and its varied clinical manifestations over time [97,104].
According to Mota et al., the initial signs of transverse myelitis (TM) associated with DF may arise in two phases. Initially, the symptoms can be attributed to the direct viral impact on the spinal cord. Subsequently, the progression of the disease is often influenced by an immune response, where the body’s immune system targets the spinal cord as a result of the dengue infection. This twofold mechanism emphasizes the complex interplay between viral infection and immune-mediated damage in the development of TM in dengue patients [100]. The diagnosis of direct viral invasion in cases of TM associated with dengue fever is supported by IgG and IgM tests, which detect antibodies specific to the DENV. Additionally, isolating the virus in CSF during the very early stages of infection can provide further evidence of direct viral invasion. These diagnostic methods help confirm the presence of the DENV in the central nervous system and distinguish it from other potential causes of neurological symptoms [95]. A retrospective study involving ten patients with neurological complications associated with DF revealed that seven of the patients tested positive for IgM antibodies, while nine tested positive for IgG antibodies specific to the DENV in CSF. This finding supports the presence of DENV in the central nervous system and highlights the importance of serological testing in diagnosing dengue-related neurological complications [94]. The detection of elevated protein and leukocyte levels in the CSF could also suggest an acute inflammatory process, likely resulting from the local effects of the viral infection. These abnormalities in the CSF are indicative of inflammation and may help differentiate dengue-related neurological complications from other conditions, providing valuable diagnostic insight into the nature and severity of the infection [93]. Diagnostic imaging methods, such as MRI, can also be utilized to detect signs of inflammation in the central nervous system and assist in the differential diagnosis of dengue-related neurological complications. MRI can reveal characteristic abnormalities, such as lesions or hyperintensities in areas like the spinal cord or brain, which are indicative of inflammation caused by the viral infection. These imaging findings are crucial for confirming the diagnosis and ruling out other potential causes of neurological symptoms [104].
A 2018 report described two patients with neuromyelitis optica spectrum disorder (NMOSD) who tested positive for aquaporin-4 antibodies and developed the condition concurrently with an acute dengue fever infection. This finding highlights the potential for dengue to trigger or exacerbate autoimmune disorders such as NMOSD, suggesting that dengue fever may be a possible precipitating factor in the onset of neurological diseases characterized by autoimmune-mediated damage to the central nervous system [103].
There are ongoing controversies regarding treatment decisions for TM. Even with appropriate therapy, many patients require months to regain neurological function, and some continue to experience residual symptoms. Currently, there is a lack of high-level evidence to definitively support the use of intravenous corticosteroids. Nevertheless, pulse therapy with methylprednisolone remains the primary treatment option for TM. In cases where the response is inadequate, therapeutic plasma exchange may be considered as a secondary treatment approach to help reduce inflammation and improve outcomes [104]. A case report of a 24-year-old female who tested positive for dengue IgM/IgG antibodies and developed acute myelitis showed that despite receiving treatment with intravenous pulse methylprednisolone, immunoglobulin plasmapheresis, and physiotherapy, she was unable to achieve complete recovery of her motor and sensory deficits after five months. This case highlights the challenging nature of dengue-related myelitis, where even with aggressive treatment, full recovery may not always be attainable, and patients may experience long-term neurological impairments [105]. Although myelitis is a rare complication of dengue fever (DF), clinicians must remain vigilant and consider it as a potential cause of neurological symptoms in patients with typical dengue symptoms. Early recognition and investigation of myelitis in such cases are crucial, as prompt diagnosis and appropriate treatment can help manage the condition and potentially improve outcomes, reducing the risk of long-term neurological impairments [97].
3.5. Acute Disseminated Encephalomyelitis
As previously discussed, myelitis and encephalitis can occur as separate entities within the spectrum of neurological complications associated with dengue fever. Another neurological complication linked to dengue fever is acute disseminated encephalomyelitis (ADEM), which presents with a combination of both encephalitis and myelitis symptoms. ADEM is an autoimmune-mediated disorder that can develop after a viral infection like dengue, leading to widespread inflammation in the brain and spinal cord, and may present with a range of neurological deficits depending on the extent and location of the damage (Table 8).
In their study, Bhushan et al. discovered that among patients suffering from dengue fever, 11% experienced immune-mediated neurological complications specifically identified as Acute Disseminated Encephalomyelitis (ADEM). This finding highlights a significant association between DENV infection and the onset of neurological disorders, emphasizing the need for heightened awareness and monitoring of such complications in patients with dengue fever [12]. In a different study, Sil et al. assessed a group of children and discovered that 5% of pediatric patients diagnosed with dengue fever had experienced ADEM [13]. A meta-analysis conducted in 2017 found that the prevalence of Acute Disseminated Encephalomyelitis (ADEM) among patients with dengue fever is approximately 0.4%. This finding suggests that a small yet significant percentage of individuals infected with dengue may experience this severe neurological condition. It emphasizes the importance of awareness regarding potential neurological complications in dengue patients, highlighting the necessity for careful monitoring and prompt intervention when neurological symptoms arise [113].
Neurological symptoms typically arise between 3 to 19 days after the initial signs of illness. Altered mental status is the most common, affecting 58% of patients and often presenting as confusion, disorientation, or changes in consciousness. Seizures and urinary issues were noted in 35% of cases, while visual disturbances, including blurred vision and difficulty focusing, affected 31%. Slurred speech was reported by 23%, indicating motor function disruptions. Additionally, walking difficulties impaired mobility and balance in 15% of individuals, and ataxia, characterized by uncoordinated muscle movements, was present in 12%. These findings underscore the wide-ranging neurological effects that can follow the onset of illness [113]. Also, the authors found that there is little information on the spinal MRI of the patients [113]. Still, nine patients with ADEM associated with DENV infection were reported. Of these, 7 had an LETM, as featured in the image study [12]. A different study that examined 22 cases indicates a similar conclusion, noting that the majority of patients experienced significant myelitis with a tendency towards the cervical and thoracic regions [114].
Recently, three unusual instances of ADEM linked to dengue fever have been reported. In the first case, an individual with a 5-day fever history was discovered in a state of diminished vitality by their sister and arrived at the emergency department with a Glasgow Coma Scale score of 5, requiring mechanical ventilation; they subsequently received treatment in the intensive care unit with steroids and made a recovery [115]. In the remaining two cases, there were two patients diagnosed with ADEM (Acute Disseminated Encephalomyelitis) associated with dengue fever. Their MRI scans exhibited patterns and lesions that closely resembled those typically seen in multiple sclerosis, highlighting the complexities of accurately diagnosing these conditions [112].
The therapies administered included intravenous immunoglobulin, steroids, plasma exchange, and various other forms of immunotherapy. Regarding prognosis, in the meta-analysis conducted by Kamel et al., out of 29 cases studied, three individuals passed away, seven experienced partial recovery, and sixteen achieved complete recovery. Those who fully recovered exhibited lower body temperatures compared to the groups with partial recovery and poor outcomes [113].
3.6. New Daily Persistent Headache
New daily persistent headache (NDPH) is a primary headache characterized by abrupt onset and daily occurrence without remission [119]. Some inciting events for NDPH have been described, such as viral infections, surgeries, and stress. However, the pathogenesis remains unclear (Table 9). Numerous studies have established a correlation between Epstein-Barr Virus (EBV) infection and the development of New Daily Persistent Headache (NDPH). Research indicates that individuals who contract EBV may experience a variety of neurological symptoms, among which NDPH is notably prevalent. This connection suggests that EBV infection could be a potential trigger for the onset of chronic headache disorders, highlighting the importance of investigating the underlying mechanisms linking viral infections to neurological conditions [112]. Notably, the connection between dengue and NDPH has been recently documented. Abreu et al. found that among 450 patients with dengue, 3 had NDPH, resulting in a prevalence rate of 0.67%, which surpasses the estimated prevalence of 0.03-0.1% found in the general population [120].
Bordini et al. reported two cases of new daily persistent headache (NDPH) following dengue fever infections. In the first case, a 23-year-old Caucasian male experienced daily bilateral headaches for two years, characterized by a severe pressure-like pain. His headaches were resistant to treatments like amitriptyline and valproic acid but showed temporary relief from nerve blockade. The second case involved a 42-year-old Caucasian female who developed a bilateral pressure-type headache shortly after her dengue fever diagnosis, confirmed by serological tests. Her headaches ranged from moderate to severe and were accompanied by nausea and sensitivity to light and sound, persisting for seven months. She finally found relief after a 10-day course of dexamethasone. These cases illustrate NDPH as a possible post-viral complication of dengue fever and the challenges in managing persistent headache disorders [121].
3.7. Acute Meningitis
Headaches are the most common symptom related to dengue fever. Some patients can develop acute meningitis signs with fever, headache, and nuchal rigidity. In an endemic area of dengue, around ten percent of the patients with acute viral meningitis had seropositivity in their CSF for dengue [122]. It is worth mentioning that meningeal contrast enhancement was already reported in individuals with acute viral meningitis due to dengue [123].
3.8. Movement Disorders
A review found that the movement disorders associated with dengue are ataxia, dystonia, parkinsonism, myoclonus, and stereotypy [124]. One of the most frequently observed associations are dystonia and parkinsonism, and less frequent is isolated parkinsonism. Batra et al. and Panda et al. reported cases of dengue-associated parkinsonism [125,126]. Interestingly, there are dengue-induced movement disorders in pediatric and adult individuals [127].
3.9. Others
The “other” neurological symptoms linked to dengue fever warrant a review because of the variety of disorders related to the virus found in the literature (Table 10). These atypical connections span from rapidly progressing dementia in an older patient to psychiatric conditions associated with dengue [128], as an Indian patient with maniac symptoms [129]. In a similar situation in Saudi Arabia, two additional patients experienced recurring migraine-like episodes accompanied by an intense fear of a near-death experience, along with symptoms of dysautonomia following viral meningitis caused by dengue [130].
In their research, Misra et al. discovered that 11% of individuals with dengue encephalitis experienced movement disorders [148]. There have been reports indicating that both adults and children with dengue may experience parkinsonism [132,133]. One of the neurological manifestations linked to DENV infection is the occurrence of opsoclonus-myoclonus. This condition is characterized by irregular, rapid eye movements known as opsoclonus, alongside sudden, involuntary muscle jerks or twitches referred to as myoclonus [135,139], cerebellar syndrome [136], and ocular flutter with truncal ataxia [137]. These symptoms can significantly affect a patient’s coordination and overall neurological function.
These diverse manifestations of the disease still encompass multiple motor neuropathy that responds to intravenous immunoglobulin [140], isolated cranial nerve paralysis [134,142], and neuralgic amyotrophy, which took 3 months for recovery in 2 out of 3 patients in a case series [131]. Additionally, there is an instance of immune-mediated cauda equina syndrome in a European patient following a trip to Brazil, with positive CSF for IgM antibodies to dengue, along with the presence of oligoclonal bands [141]. Moreover, there is a documented case of hemiconvulsion hemiplegia triggered by dengue infection [138], and two patients who were reported in the study by Bhushan and colleagues experienced painful retrobulbar optic neuritis [12]. Chang et al. reported increased risk of developing dementia after dengue fever [149].
4. Challenge
4.1. Challenges in Diagnosis
There is a significant increase of cases in developed countries due to traveling availability. It is always worth to ask regarding travelling history, and let the alerts for reminder to ask about travel history on. Kim et al. reply to the comment by readers as since dengue infection is not endemic and extremely rare in South Korea, the authors tested a wide range of possible infections [150].
4.2. Challenges for Prevention
Some of the main challenges in the development of vaccines for dengue is the fact they should cover the four serotypes of DENV. Also, they need to prevent cross-immunity. Currently, there are about seven vaccines and many ongoing clinical trials. The CYD-TDV (Dengvaxia®) was the first vaccine to be developed, and unfortunately the patient needs to have at least one episode of dengue before receiving vaccination. In the case of TAK-003 (Qdenga®) administration, it is independent of dengue serological status of the patient. And, interestingly the TV003 (TV005) is based on attenuated viruses [151]. It is worth mentioning that the current vaccines showed decreased cases of severe dengue in general, but there is no specific analysis of cases related to neurological manifestations. Furthermore, the CYD-TDV vaccine given to individuals with serological status negative for dengue more commonly developed severe dengue with neurological manifestations [152].
5. Limitations
This manuscript did not employ a systematic search methodology. Instead, all articles included in the study were sourced exclusively from the PubMed database. While this approach allowed for a broad exploration of available literature, the inclusion of diverse types of manuscripts introduces potential variability in the interpretation of the clinical neurological manifestations associated with DENV infection. The selected articles reflect a range of perspectives and methodologies, which may contribute to a more nuanced but less uniform understanding of the topic. This variability underscores the challenge of drawing definitive conclusions from heterogenous data.
Despite these limitations, the primary objective of this manuscript is to offer a comprehensive overview of the neuroinvasion characteristics of DENV, synthesizing current knowledge to better understand its neurological impacts. The manuscript also seeks to highlight critical gaps in the existing literature, providing a foundation for future research in this area. By summarizing diverse findings, it aims to inform clinicians and researchers about the spectrum of neurological complications linked to dengue. Additionally, this work underscores the importance of interdisciplinary approaches in studying viral neuroinvasion, as the mechanisms remain complex and multifactorial. Ultimately, this review hopes to contribute to a deeper understanding of how the DENV affects the central nervous system and to support the development of more targeted diagnostic and therapeutic strategies.
6. Conclusion
This scoping review highlights the diverse and significant neurological manifestations of DENV infection beyond cerebrovascular disorders. Dengue, a globally prevalent arboviral infection, has traditionally been associated with systemic and febrile illness. However, increasing evidence reveals its capacity to affect the central and peripheral nervous systems through direct viral invasion, immune-mediated mechanisms, and metabolic derangements. These manifestations encompass a wide spectrum, including encephalitis, myelitis, Guillain-Barré syndrome, transverse myelitis, and acute disseminated encephalomyelitis, among others. The variability in clinical presentations underscores the need for heightened clinical suspicion, particularly in endemic regions. Neurological complications can occur across all age groups and are often associated with more severe forms of the disease, such as dengue hemorrhagic fever and dengue shock syndrome. Timely recognition and intervention are crucial to mitigate long-term morbidity, which includes persistent cognitive, motor, and sensory deficits. However, diagnosis is often challenging due to overlapping symptoms with other tropical infections and the lack of specific neurological biomarkers. Our review identifies critical gaps in the understanding of the pathophysiological mechanisms underlying these complications. Additionally, there is a paucity of large-scale epidemiological studies that delineate the incidence, risk factors, and outcomes of neurological involvement in dengue. Addressing these gaps is essential for developing targeted diagnostic and therapeutic strategies. In conclusion, the neurological spectrum of dengue is broader than traditionally appreciated, warranting further research and a multidisciplinary approach to diagnosis and management. Clinicians, particularly in endemic areas, should maintain vigilance for neurological symptoms in dengue patients, ensuring prompt referral and comprehensive care. Enhanced awareness, along with public health measures to control the spread of dengue, will be pivotal in reducing the burden of these disabling complications.
Author Contributions
Conceptualization, J.P.R., V.V.B., and A.L.F.C.; methodology, A.L.F.C.; software, A.L.F.C.; validation, A.L.F.C., J.P.R. and V.V.B.; formal analysis, A.L.F.C.; investigation, A.L.F.C.; resources, A.L.F.C.; data curation, J.P.R.; writing—original draft preparation, J.P.R.; writing—review and editing, J.P.R.; visualization, V.V.B.; supervision, V.V.B.; project administration, V.V.B.; funding acquisition, J.P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data created.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hale, G.L. Flaviviruses and the Traveler: Around the World and to Your Stage. A Review of West Nile, Yellow Fever, Dengue, and Zika Viruses for the Practicing Pathologist. Mod Pathol 2023, 36, 100188. [CrossRef]
- Lessa, C.L.S.; Hodel, K.V.S.; Gonçalves, M. de S.; Machado, B.A.S. Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil. Trop Med Infect Dis 2023, 8. [CrossRef]
- Roberts, J.A.; Kapadia, R.K.; Pastula, D.M.; Thakur, K.T. Public Health Trends in Neurologically Relevant Infections: A Global Perspective. Ther Adv Infect Dis 2024, 11, 20499361241274206. [CrossRef]
- Muller, D.A.; Depelsenaire, A.C.I.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J Infect Dis 2017, 215, S89–S95. [CrossRef]
- Simon, O.; Billot, S.; Guyon, D.; Daures, M.; Descloux, E.; Gourinat, A.C.; Molko, N.; Dupont-Rouzeyrol, M. Early Guillain-Barré Syndrome Associated with Acute Dengue Fever. J Clin Virol 2016, 77, 29–31. [CrossRef]
- Guha-Sapir, D.; Schimmer, B. Dengue Fever: New Paradigms for a Changing Epidemiology. Emerg Themes Epidemiol 2005, 2, 1. [CrossRef]
- Estofolete, C.F.; de Oliveira Mota, M.T.; Bernardes Terzian, A.C.; de Aguiar Milhim, B.H.G.; Ribeiro, M.R.; Nunes, D.V.; Mourão, M.P.; Rossi, S.L.; Nogueira, M.L.; Vasilakis, N. Unusual Clinical Manifestations of Dengue Disease - Real or Imagined? Acta Trop 2019, 199, 105134. [CrossRef]
- Carod-Artal, F.J.; Wichmann, O.; Farrar, J.; Gascón, J. Neurological Complications of Dengue Virus Infection. Lancet Neurol 2013, 12, 906–919. [CrossRef]
- Sahu, R.; Verma, R.; Jain, A.; Garg, R.K.; Singh, M.K.; Malhotra, H.S.; Sharma, P.K.; Parihar, A. Neurologic Complications in Dengue Virus Infection: A Prospective Cohort Study. Neurology 2014, 83, 1601–1609. [CrossRef]
- Antônio Machado Schlindwein, M.; Pastor Bandeira, I.; Caroline Breis, L.; Machado Rickli, J.; César Demore, C.; Sordi Chara, B.; Henrique Melo, L.; Vinícius Magno Gonçalves, M. Dengue Fever and Neurology: Well Beyond Hemorrhage and Strokes. Preprints 2020. [CrossRef]
- Misra, U.K.; Kalita, J.; Mani, V.E.; Chauhan, P.S.; Kumar, P. Central Nervous System and Muscle Involvement in Dengue Patients: A Study from a Tertiary Care Center. J Clin Virol 2015, 72, 146–151. [CrossRef]
- Bhushan, B.; Sardana, V.; Maheshwari, D.; Ojha, P.; Mohan, S.; Moon, P.; Kamble, S.; Jain, N.; Sharma, S.K. Immune-Mediated Neurological Manifestations of Dengue Virus- a Study of Clinico-Investigational Variability, Predictors of Neuraxial Involvement, and Outcome with the Role of Immunomodulation. Neurol India 2018, 66, 1634–1643. [CrossRef]
- Sil, A.; Biswas, T.; Samanta, M.; Konar, M.C.; De, A.K.; Chaudhuri, J. Neurological Manifestations in Children with Dengue Fever: An Indian Perspective. Trop Doct 2017, 47, 145–149. [CrossRef]
- Bentes, A.A.; Maia De Castro Romanelli, R.; Crispim, A.P.C.; Marinho, P.E.S.; Loutfi, K.S.; Araujo, S.T.; Campos E Silva, L.M.; Guedes, I.; Martins Alvarenga, A.; Santos, M.A.; et al. Neurological Manifestations Due to Dengue Virus Infection in Children: Clinical Follow-Up. Pathog Glob Health 2021, 115, 476–482. [CrossRef]
- Suma, R.; Netravathi, M.; Gururaj, G.; Thomas, P.T.; Singh, B.; Solomon, T.; Desai, A.; Vasanthapuram, R.; Banandur, P.S. Profile of Acute Encephalitis Syndrome Patients from South India. J Glob Infect Dis 2023, 15, 156–165. [CrossRef]
- Khan, M.M.; Miah, M.A.H.; Alam, M.K.; Islam, M.A.; Rahman, M.A.; Noor, R.I.I.; Mondal, E.; Mamun, A.H.M.S.; Rasel, M.; Talukder, M.R.T.; et al. Clinico-Epidemiological Profiling of Dengue Patients in a Non-Endemic Region of Bangladesh. Trans R Soc Trop Med Hyg 2024, trae074. [CrossRef]
- Guzman, M.G.; Martinez, E. Central and Peripheral Nervous System Manifestations Associated with Dengue Illness. Viruses 2024, 16. [CrossRef]
- Jhan, M.-K.; Tsai, T.-T.; Chen, C.-L.; Tsai, C.-C.; Cheng, Y.-L.; Lee, Y.-C.; Ko, C.-Y.; Lin, Y.-S.; Chang, C.-P.; Lin, L.-T.; et al. Dengue Virus Infection Increases Microglial Cell Migration. Sci Rep 2017, 7, 91. [CrossRef]
- Lee, K.M.; Chiu, K.B.; Sansing, H.A.; Didier, P.J.; Lackner, A.A.; MacLean, A.G. The Flavivirus Dengue Induces Hypertrophy of White Matter Astrocytes. J Neurovirol 2016, 22, 831–839. [CrossRef]
- Araújo, F.M.C.; Araújo, M.S.; Nogueira, R.M.R.; Brilhante, R.S.N.; Oliveira, D.N.; Rocha, M.F.G.; Cordeiro, R.A.; Araújo, R.M.C.; Sidrim, J.J.C. Central Nervous System Involvement in Dengue: A Study in Fatal Cases from a Dengue Endemic Area. Neurology 2012, 78, 736–742. [CrossRef]
- Li, H.; Li, Y.; Wen, B.; Zhang, J.; Wang, C.; Song, Z.; Li, S.; Qu, X.; Huang, R.; Liu, W. Dengue Virus and Japanese Encephalitis Virus Infection of the Central Nervous System Share Similar Profiles of Cytokine Accumulation in Cerebrospinal Fluid. Cent Eur J Immunol 2017, 42, 218–222. [CrossRef]
- Al-Shujairi, W.H.; Clarke, J.N.; Davies, L.T.; Alsharifi, M.; Pitson, S.M.; Carr, J.M. Intracranial Injection of Dengue Virus Induces Interferon Stimulated Genes and CD8+ T Cell Infiltration by Sphingosine Kinase 1 Independent Pathways. PLoS One 2017, 12, e0169814. [CrossRef]
- Bordignon, J.; Strottmann, D.M.; Mosimann, A.L.P.; Probst, C.M.; Stella, V.; Noronha, L.; Zanata, S.M.; Dos Santos, C.N.D. Dengue Neurovirulence in Mice: Identification of Molecular Signatures in the E and NS3 Helicase Domains. J Med Virol 2007, 79, 1506–1517. [CrossRef]
- Salazar, M.I.; Pérez-García, M.; Terreros-Tinoco, M.; Castro-Mussot, M.E.; Diegopérez-Ramírez, J.; Ramírez-Reyes, A.G.; Aguilera, P.; Cedillo-Barrón, L.; García-Flores, M.M. Dengue Virus Type 2: Protein Binding and Active Replication in Human Central Nervous System Cells. ScientificWorldJournal 2013, 2013, 904067. [CrossRef]
- de Miranda, A.S.; Rodrigues, D.H.; Amaral, D.C.G.; de Lima Campos, R.D.; Cisalpino, D.; Vilela, M.C.; Lacerda-Queiroz, N.; de Souza, K.P.R.; Vago, J.P.; Campos, M.A.; et al. Dengue-3 Encephalitis Promotes Anxiety-like Behavior in Mice. Behav Brain Res 2012, 230, 237–242. [CrossRef]
- Amaral, D.C.G.; Rachid, M.A.; Vilela, M.C.; Campos, R.D.L.; Ferreira, G.P.; Rodrigues, D.H.; Lacerda-Queiroz, N.; Miranda, A.S.; Costa, V.V.; Campos, M.A.; et al. Intracerebral Infection with Dengue-3 Virus Induces Meningoencephalitis and Behavioral Changes That Precede Lethality in Mice. J Neuroinflammation 2011, 8, 23. [CrossRef]
- Dalugama, C.; Shelton, J.; Ekanayake, M.; Gawarammana, I.B. Dengue Fever Complicated with Guillain-Barré Syndrome: A Case Report and Review of the Literature. J Med Case Rep 2018, 12, 137. [CrossRef]
- Arriaga-Nieto, L.; Hernández-Bautista, P.F.; Vallejos-Parás, A.; Grajales-Muñiz, C.; Rojas-Mendoza, T.; Cabrera-Gaytán, D.A.; Grijalva-Otero, I.; Cacho-Díaz, B.; Jaimes-Betancourt, L.; Padilla-Velazquez, R.; et al. Predict the Incidence of Guillain Barré Syndrome and Arbovirus Infection in Mexico, 2014-2019. PLOS Glob Public Health 2022, 2, e0000137. [CrossRef]
- Matos, L.M. de; Borges, A.T.; Palmeira, A.B.; Lima, V.M.; Maciel, E.P.; Fernandez, R.N.M.; Mendes, J.P.L.; Romero, G.A.S. Frequency of Exposure to Arboviruses and Characterization of Guillain Barré Syndrome in a Clinical Cohort of Patients Treated at a Tertiary Referral Center in Brasília, Federal District. Rev Soc Bras Med Trop 2022, 55, e03062021. [CrossRef]
- Gonçalves, E. Acute Inflammatory Demyelinating Polyradiculoneuropathy (Guillain-Barré Syndrome) Following Dengue Fever. Rev Inst Med Trop Sao Paulo 2011, 53, 223–225. [CrossRef]
- Ralapanawa, D.M.P.U.K.; Kularatne, S.A.M.; Jayalath, W.A.T.A. Guillain-Barre Syndrome Following Dengue Fever and Literature Review. BMC Res Notes 2015, 8, 729. [CrossRef]
- Fragoso, Y.D.; Gomes, S.; Brooks, J.B.B.; Matta, A.P. da C.; Ruocco, H.H.; Tauil, C.B.; Sousa, N.A. de C.; Spessotto, C.V.; Grippe, T. Guillain-Barré Syndrome and Dengue Fever: Report on Ten New Cases in Brazil. Arq Neuropsiquiatr 2016, 74, 1039–1040. [CrossRef]
- Pandey, S.; Garg, R.K.; Malhotra, H.S.; Kumar, N.; Uniyal, R. Simultaneous Occurrence of Axonal Guillain-Barré Syndrome in Two Siblings Following Dengue Infection. Ann Indian Acad Neurol 2018, 21, 315–317. [CrossRef]
- Pandey, R.K.; Jain, R.K.; Hussain, S.Z. Pharyngeal-Cervical-Brachial Variant of Guillain-Barré Syndrome Following Dengue Infection: A Rare Syndrome with Rare Association. Ann Indian Acad Neurol 2019, 22, 240–241. [CrossRef]
- de Silva, N.L.; Weeratunga, P.; Umapathi, T.; Malavige, N.; Chang, T. Miller Fisher Syndrome Developing as a Parainfectious Manifestation of Dengue Fever: A Case Report and Review of the Literature. J Med Case Rep 2019, 13, 120. [CrossRef]
- Pari, H.; Amalnath, S.D.; Dhodapkar, R. Guillain-Barre Syndrome and Antibodies to Arboviruses (Dengue, Chikungunya and Japanese Encephalitis): A Prospective Study of 95 Patients Form a Tertiary Care Centre in Southern India. Ann Indian Acad Neurol 2022, 25, 203–206. [CrossRef]
- Payus, A.O.; Ibrahim, A.; Liew Sat Lin, C.; Hui Jan, T. Sensory Predominant Guillain-Barré Syndrome Concomitant with Dengue Infection: A Case Report. Case Rep Neurol 2022, 14, 281–285. [CrossRef]
- Lim, C.S.; Kaisbain, N.; Lim, W.J. A Rare Combination: Dengue Fever Complicated With Guillain-Barre Syndrome. Cureus 2023, 15, e40957. [CrossRef]
- Rajurkar, R.D.; Patil, D.S.; Jagzape, M.V. Pediatric Physiotherapeutic Approach for Guillain-Barre Syndrome Associated With Dengue Fever: A Case Report. Cureus 2023, 15, e46488. [CrossRef]
- Mahashabde, M.L.; Kumar, L. Integrated Approach to Severe Dengue Complicated by Guillain-Barré Syndrome and Multi-Organ Failure. Cureus 2024, 16, e63939. [CrossRef]
- Rayamajhi, A.; Rayamajhi, S.; Agrawal, S.; Gautam, N. Unraveling the Neurological Intricacies: A Rare Case of Guillain-Barre Syndrome in Dengue Fever. Oxf Med Case Reports 2024, 2024, omae099. [CrossRef]
- Khan, A.B.; Ali, M.A.; Ur Rehman, S.; Siddiqe, U.; Ahmad, S. Dengue Fever-Induced Hypokalemic Paralysis in a Pregnant Patient: An Uncommon Presentation of a Common Disease. Cureus 2023, 15, e40174. [CrossRef]
- Garg, R.K.; Malhotra, H.S.; Verma, R.; Sharma, P.; Singh, M.K. Etiological Spectrum of Hypokalemic Paralysis: A Retrospective Analysis of 29 Patients. Ann Indian Acad Neurol 2013, 16, 365–370. [CrossRef]
- Kulkarni, R.; Pujari, S.; Gupta, D. Neurological Manifestations of Dengue Fever. Ann Indian Acad Neurol 2021, 24, 693–702. [CrossRef]
- Garg, R.K.; Malhotra, H.S.; Jain, A.; Malhotra, K.P. Dengue-Associated Neuromuscular Complications. Neurol India 2015, 63, 497–516. [CrossRef]
- Malheiros, S.M.; Oliveira, A.S.; Schmidt, B.; Lima, J.G.; Gabbai, A.A. Dengue. Muscle Biopsy Findings in 15 Patients. Arq Neuropsiquiatr 1993, 51, 159–164. [CrossRef]
- Finsterer, J.; Kongchan, K. Severe, Persisting, Steroid-Responsive Dengue Myositis. J Clin Virol 2006, 35, 426–428. [CrossRef]
- Acharya, S.; Shukla, S.; Mahajan, S.N.; Diwan, S.K. Acute Dengue Myositis with Rhabdomyolysis and Acute Renal Failure. Ann Indian Acad Neurol 2010, 13, 221–222. [CrossRef]
- Sangle, S.A.; Dasgupta, A.; Ratnalikar, S.D.; Kulkarni, R.V. Dengue Myositis and Myocarditis. Neurol India 2010, 58, 598–599. [CrossRef]
- Paliwal, V.K.; Garg, R.K.; Juyal, R.; Husain, N.; Verma, R.; Sharma, P.K.; Verma, R.; Singh, M.K. Acute Dengue Virus Myositis: A Report of Seven Patients of Varying Clinical Severity Including Two Cases with Severe Fulminant Myositis. J Neurol Sci 2011, 300, 14–18. [CrossRef]
- Kalita, J.; Misra, U.K.; Maurya, P.K.; Shankar, S.K.; Mahadevan, A. Quantitative Electromyography in Dengue-Associated Muscle Dysfunction. J Clin Neurophysiol 2012, 29, 468–471. [CrossRef]
- Misra, U.K.; Kalita, J.; Maurya, P.K.; Kumar, P.; Shankar, S.K.; Mahadevan, A. Dengue-Associated Transient Muscle Dysfunction: Clinical, Electromyography and Histopathological Changes. Infection 2012, 40, 125–130. [CrossRef]
- Verma, R.; Holla, V.V.; Kumar, V.; Jain, A.; Husain, N.; Malhotra, K.P.; Garg, R.K.; Malhotra, H.S.; Sharma, P.K.; Kumar, N. A Study of Acute Muscle Dysfunction with Particular Reference to Dengue Myopathy. Ann Indian Acad Neurol 2017, 20, 13–22. [CrossRef]
- Arif, A.; Abdul Razzaque, M.R.; Kogut, L.M.; Tebha, S.S.; Shahid, F.; Essar, M.Y. Expanded Dengue Syndrome Presented with Rhabdomyolysis, Compartment Syndrome, and Acute Kidney Injury: A Case Report. Medicine (Baltimore) 2022, 101, e28865. [CrossRef]
- Mekmangkonthong, A.; Amornvit, J.; Numkarunarunrote, N.; Veeravigrom, M.; Khaosut, P. Dengue Infection Triggered Immune Mediated Necrotizing Myopathy in Children: A Case Report and Literature Review. Pediatr Rheumatol Online J 2022, 20, 40. [CrossRef]
- Rashid, Z.; Hussain, T.; Abdullah, S.N.; Kumar, J. Case of Steroid Refractory Dengue Myositis Responsive to Intravenous Immunoglobulins. BMJ Case Rep 2022, 15. [CrossRef]
- Putri, A.; Arunsodsai, W.; Hattasingh, W.; Sirinam, S. DENV-1 Infection with Rhabdomyolysis in an Adolescent: A Case Report and Review of Challenge in Early Diagnosis and Treatment. Heliyon 2024, 10, e36379. [CrossRef]
- Samarasingha, P.; Karunatilake, H.; Jayanaga, A.; Jayawardhana, H.; Priyankara, D. Dengue Rhabdomyolysis Successfully Treated with Hemoperfusion Using CytoSorb® in Combination with Continuous Renal Replacement Therapy: A Case Report. J Med Case Rep 2024, 18, 329. [CrossRef]
- Gulia, M.; Dalal, P.; Gupta, M.; Kaur, D. Concurrent Guillain-Barré Syndrome and Myositis Complicating Dengue Fever. BMJ Case Rep 2020, 13. [CrossRef]
- Rao, S.; Kumar, M.; Ghosh, S.; Gadpayle, A.K. A Rare Case of Dengue Encephalitis. BMJ Case Rep 2013, 2013. [CrossRef]
- Borawake, K.; Prayag, P.; Wagh, A.; Dole, S. Dengue Encephalitis. Indian J Crit Care Med 2011, 15, 190–193. [CrossRef]
- Cristiane, S.; Marzia, P.-S. Diagnosis Criteria of Dengue Encephalitis. Arq Neuropsiquiatr 2014, 72, 263. [CrossRef]
- Withana, M.; Rodrigo, C.; Chang, T.; Karunanayake, P.; Rajapakse, S. Dengue Fever Presenting with Acute Cerebellitis: A Case Report. BMC Res Notes 2014, 7, 125. [CrossRef]
- Garg, R.K.; Rizvi, I.; Ingole, R.; Jain, A.; Malhotra, H.S.; Kumar, N.; Batra, D. Cortical Laminar Necrosis in Dengue Encephalitis-a Case Report. BMC Neurol 2017, 17, 79. [CrossRef]
- Kumar, A.S.; Mehta, S.; Singh, P.; Lal, V. Dengue Encephalitis: “Double Doughnut” Sign. Neurol India 2017, 65, 670–671. [CrossRef]
- Kutiyal, A.S.; Malik, C.; Hyanki, G. Dengue Haemorrhagic Encephalitis: Rare Case Report with Review of Literature. J Clin Diagn Res 2017, 11, OD10–OD12. [CrossRef]
- Sivamani, K.; Dhir, V.; Singh, S.; Sharma, A. Diagnostic Dilemma-Dengue or Japanese Encephalitis? Neurol India 2017, 65, 105–107. [CrossRef]
- Jois, D.; Moorchung, N.; Gupta, S.; Mutreja, D.; Patil, S. Autopsy in Dengue Encephalitis: An Analysis of Three Cases. Neurol India 2018, 66, 1721–1725. [CrossRef]
- Chatur, C.; Balani, A.; Kumar, A.; Alwala, S.; Giragani, S. “Double Doughnut” Sign - Could It Be a Diagnostic Marker for Dengue Encephalitis? Neurol India 2019, 67, 1360–1362. [CrossRef]
- Kyaw, A.K.; Ngwe Tun, M.M.; Nabeshima, T.; Buerano, C.C.; Ando, T.; Inoue, S.; Hayasaka, D.; Lim, C.-K.; Saijo, M.; Thu, H.M.; et al. Japanese Encephalitis- and Dengue-Associated Acute Encephalitis Syndrome Cases in Myanmar. Am J Trop Med Hyg 2019, 100, 643–646. [CrossRef]
- Weerasinghe, W.S.; Medagama, A. Dengue Hemorrhagic Fever Presenting as Encephalitis: A Case Report. J Med Case Rep 2019, 13, 278. [CrossRef]
- Pandeya, A.; Upadhyay, D.; Oli, B.; Parajuli, M.; Silwal, N.; Shrestha, A.; Gautam, N.; Gajurel, B.P. Dengue Encephalitis Featuring “Double-Doughnut” Sign - A Case Report. Ann Med Surg (Lond) 2022, 78, 103939. [CrossRef]
- Barron, S.; Han, V.X.; Gupta, J.; Lingappa, L.; Sankhyan, N.; Thomas, T. Dengue-Associated Acute Necrotizing Encephalopathy Is an Acute Necrotizing Encephalopathy Variant Rather than a Mimic: Evidence From a Systematic Review. Pediatr Neurol 2024, 161, 208–215. [CrossRef]
- Berdiñas Anfuso, M.; Gonzalez, M.V.; Schverdfinger, S.; Videla, C.G.; Ciarrocchi, N.M. [Dengue encephalitis in Argentina]. Medicina (B Aires) 2024, 84, 780–783.
- Gupta, N.; Acharya, V.; Amrutha, C.; Varma, M. Double Doughnut Sign in Dengue Encephalitis. QJM 2024, hcae162. [CrossRef]
- Harshani, H.B.C.; Ruwan, D.V.R.G.; Chathuranga, G.D.D.; Weligamage, D.C.U.D.; Abeynayake, J.I. Dengue Encephalitis: A Rare Manifestation of Dengue Fever. J Vector Borne Dis 2024, 61, 495–498. [CrossRef]
- Hussain, H.; Janaka, K.V.C.; Gunasekara, H.; Krishnan, M.; Perera, I. Acute Psychosis Presenting With Dengue Fever Complicated by Dengue Encephalitis. Cureus 2024, 16, e55628. [CrossRef]
- Khosla, S.; Chauhan, R.; Aggarwal, A.; Patel, N.B. Dengue Encephalitis - An Unusual Case Series. J Family Med Prim Care 2024, 13, 3420–3423. [CrossRef]
- Mun, Y.-J.; Shin, D.-H.; Cho, J.W.; Kim, H.-W. Steroid-Responsive Dengue Encephalitis Without Typical Dengue Symptoms. J Clin Neurol 2024, 20, 232–234. [CrossRef]
- Shah, S.A.; Chauhan, K.J.; Charan, B.D.; Garg, A.; Soneja, M. “Dual Double-Doughnut” Sign in Dengue Encephalitis. Ann Indian Acad Neurol 2024, 27, 569–570. [CrossRef]
- Verma, R.; Pandey, A.K.; Chakraborty, R.; Prakash, S.; Jain, A. Toll-Like Receptor 3 Genetic Polymorphism in Dengue Encephalitis. J Family Med Prim Care 2024, 13, 2397–2403. [CrossRef]
- Fong, C.Y.; Saw, M.T.; Li, L.; Lim, W.K.; Ong, L.C.; Gan, C.S. Malaysian Outcome of Acute Necrotising Encephalopathy of Childhood. Brain Dev 2021, 43, 538–547. [CrossRef]
- Domingues, R.B.; Kuster, G.W.; Onuki-Castro, F.L.; Souza, V.A.; Levi, J.E.; Pannuti, C.S. Involvement of the Central Nervous System in Patients with Dengue Virus Infection. J Neurol Sci 2008, 267, 36–40. [CrossRef]
- Prabhat, N.; Ray, S.; Chakravarty, K.; Kathuria, H.; Saravana, S.; Singh, D.; Rebello, A.; Lakhanpal, V.; Goyal, M.K.; Lal, V. Atypical Neurological Manifestations of Dengue Fever: A Case Series and Mini Review. Postgrad Med J 2020, 96, 759–765. [CrossRef]
- Vyas, S.; Ray, N.; Maralakunte, M.; Kumar, A.; Singh, P.; Modi, M.; Goyal, M.K.; Sankhyan, N.; Bhalla, A.; Sharma, N.; et al. Pattern Recognition Approach to Brain MRI Findings in Patients with Dengue Fever with Neurological Complications. Neurol India 2020, 68, 1038–1047. [CrossRef]
- Chayanopparat, S.; Jitprapaikulsan, J.; Ongphichetmetha, T. Catastrophic Tumefactive Acute Disseminated Encephalomyelitis in Patient with Dengue Virus: A Case Report. J Neurovirol 2024, 30, 202–207. [CrossRef]
- Varatharaj, A. Encephalitis in the Clinical Spectrum of Dengue Infection. Neurol India 2010, 58, 585–591. [CrossRef]
- Bokhari, S.A.; Alabrach, N.; Al Mansour, A.; Abulmagd, M. Manic Episode Following Dengue Fever: A Case Report. Cureus 2024, 16, e68630. [CrossRef]
- Elavia, Z.; Patra, S.S.; Kumar, S.; Inban, P.; Yousuf, M.A.; Thassu, I.; Chaudhry, H.A. Acute Psychosis and Mania: An Uncommon Complication of Dengue Fever. Cureus 2023, 15, e47425. [CrossRef]
- Moryś, J.M.; Jeżewska, M.; Korzeniewski, K. Neuropsychiatric Manifestations of Some Tropical Diseases. Int Marit Health 2015, 66, 30–35. [CrossRef]
- Biswas, H.K.; Ibu, K.T.I.; Biswas, R.; Ahmed, M.N.U. Posterior Reversible Encephalopathy Syndrome Associated with Dengue Fever Induced Intrauterine Death: A Case Report. Clin Case Rep 2024, 12, e8575. [CrossRef]
- Puccioni-Sohler, M.; Rosadas, C.; Cabral-Castro, M.J. Neurological Complications in Dengue Infection: A Review for Clinical Practice. Arq Neuropsiquiatr 2013, 71, 667–671. [CrossRef]
- Soares, C.N.; Faria, L.C.; Peralta, J.M.; de Freitas, M.R.G.; Puccioni-Sohler, M. Dengue Infection: Neurological Manifestations and Cerebrospinal Fluid (CSF) Analysis. J Neurol Sci 2006, 249, 19–24. [CrossRef]
- Puccioni-Sohler, M.; Soares, C.N.; Papaiz-Alvarenga, R.; Castro, M.J.C.; Faria, L.C.; Peralta, J.M. Neurologic Dengue Manifestations Associated with Intrathecal Specific Immune Response. Neurology 2009, 73, 1413–1417. [CrossRef]
- Chanthamat, N.; Sathirapanya, P. Acute Transverse Myelitis Associated with Dengue Viral Infection. J Spinal Cord Med 2010, 33, 425–427. [CrossRef]
- Larik, A.; Chiong, Y.; Lee, L.C.; Ng, Y.S. Longitudinally Extensive Transverse Myelitis Associated with Dengue Fever. BMJ Case Rep 2012, 2012. [CrossRef]
- Tomar, L.R.; Mannar, V.; Pruthi, S.; Aggarwal, A. An Unusual Presentation of Dengue Fever: Association with Longitudinal Extensive Transverse Myelitis. Perm J 2015, 19, e133-135. [CrossRef]
- Fong, C.Y.; Hlaing, C.S.; Tay, C.G.; Kadir, K.A.A.; Goh, K.J.; Ong, L.C. Longitudinal Extensive Transverse Myelitis with Cervical Epidural Haematoma Following Dengue Virus Infection. Eur J Paediatr Neurol 2016, 20, 449–453. [CrossRef]
- Patras, E.; Polagani, P.K.; Sural, A.; Parkhe, N.R. A Rare Case of an 8-Month-Old Child with Dengue Fever Complicated by Acute Diffuse Transverse Myelitis. J Pediatr Neurosci 2016, 11, 292–293. [CrossRef]
- Mota, M.T. de O.; Estofolete, C.F.; Zini, N.; Terzian, A.C.B.; Gongora, D.V.N.; Maia, I.L.; Nogueira, M.L. Transverse Myelitis as an Unusual Complication of Dengue Fever. Am J Trop Med Hyg 2017, 96, 380–381. [CrossRef]
- Badat, N.; Abdulhussein, D.; Oligbu, P.; Ojubolamo, O.; Oligbu, G. Risk of Transverse Myelitis Following Dengue Infection: A Systematic Review of the Literature. Pharmacy (Basel) 2018, 7. [CrossRef]
- Chaudhry, N.; Aswani, N.; Khwaja, G.A.; Rani, P. Association of Dengue with Longitudinally Extensive Transverse Myelitis and Subarachnoid Hemorrhage: An Unusual Presentation. Ann Indian Acad Neurol 2018, 21, 158–160. [CrossRef]
- Lana-Peixoto, M.A.; Pedrosa, D.; Talim, N.; Amaral, J.M.S.S.; Horta, A.; Kleinpaul, R. Neuromyelitis Optica Spectrum Disorder Associated with Dengue Virus Infection. J Neuroimmunol 2018, 318, 53–55. [CrossRef]
- Malik, S.; Saran, S.; Dubey, A.; Punj, A. Longitudinally Extensive Transverse Myelitis Following Dengue Virus Infection: A Rare Entity. Ann Afr Med 2018, 17, 86–89. [CrossRef]
- Landais, A.; Hartz, B.; Alhendi, R.; Lannuzel, A. Acute Myelitis Associated with Dengue Infection. Med Mal Infect 2019, 49, 270–274. [CrossRef]
- Singh, H.; Pannu, A.K.; Bhalla, A.; Suri, V.; Kumari, S. Dengue: Uncommon Neurological Presentations of a Common Tropical Illness. Indian J Crit Care Med 2019, 23, 274–275. [CrossRef]
- Tan, W.; Lim, C.T.S. Dengue-Related Longitudinally Extensive Transverse Myelitis. Neurol India 2019, 67, 1116–1117. [CrossRef]
- Comtois, J.; Camara-Lemarroy, C.R.; Mah, J.K.; Kuhn, S.; Curtis, C.; Braun, M.H.; Tellier, R.; Burton, J.M. Longitudinally Extensive Transverse Myelitis with Positive Aquaporin-4 IgG Associated with Dengue Infection: A Case Report and Systematic Review of Cases. Mult Scler Relat Disord 2021, 55, 103206. [CrossRef]
- Karishma, F.; Harsha, F.; Rani, S.; Siddique, S.; Kumari, K.; Mainka, F.; Nasir, H. Acute Transverse Myelitis as an Unusual Complication of Dengue Fever: A Case Report and Literature Review. Cureus 2024, 16, e54074. [CrossRef]
- Mangudkar, S.; Nimmala, S.G.; Mishra, M.P.; Giduturi, V.N. Post-Viral Longitudinally Extensive Transverse Myelitis: A Case Report. Cureus 2024, 16, e62033. [CrossRef]
- Shrestha, K.; Poudel, B.; Shrestha, S.; Rai, B.P.; Rajbhandari, P.; Mishra, D.K. An Unusual Case of Transverse Myelitis in Dengue Fever: A Case Report from Nepal. Clin Case Rep 2024, 12, e8461. [CrossRef]
- Viswanathan, S.; Botross, N.; Rusli, B.N.; Riad, A. Acute Disseminated Encephalomyelitis Complicating Dengue Infection with Neuroimaging Mimicking Multiple Sclerosis: A Report of Two Cases. Mult Scler Relat Disord 2016, 10, 112–115. [CrossRef]
- Kamel, M.G.; Nam, N.T.; Han, N.H.B.; El-Shabouny, A.-E.; Makram, A.-E.M.; Abd-Elhay, F.A.-E.; Dang, T.N.; Hieu, N.L.T.; Huong, V.T.Q.; Tung, T.H.; et al. Post-Dengue Acute Disseminated Encephalomyelitis: A Case Report and Meta-Analysis. PLoS Negl Trop Dis 2017, 11, e0005715. [CrossRef]
- Wan Sulaiman, W.A.; Inche Mat, L.N.; Hashim, H.Z.; Hoo, F.K.; Ching, S.M.; Vasudevan, R.; Mohamed, M.H.; Basri, H. Acute Disseminated Encephalomyelitis in Dengue Viral Infection. J Clin Neurosci 2017, 43, 25–31. [CrossRef]
- Rastogi, N.; Nayan, A.; Sethi, P.; Nischal, N.; Brijwal, M.; Kumar, A.; Wig, N. Dengue Fever with Acute Disseminated Encephalomyelitis : Sensorium Imbroglio. J Assoc Physicians India 2019, 67, 80–82.
- Diallo, A.; Dembele, Y.; Michaud, C.; Jean, M.; Niang, M.; Meliani, P.; Yaya, I.; Permal, S. Acute Disseminated Encephalomyelitis after Dengue. IDCases 2020, 21, e00862. [CrossRef]
- Farooque, U.; Pillai, B.; Karimi, S.; Cheema, A.Y.; Saleem, N. A Rare Case of Dengue Fever Presenting With Acute Disseminated Encephalomyelitis. Cureus 2020, 12, e10042. [CrossRef]
- Chakraborty, S.; Narayan, A.; Chakraborty, D.; Ukil, B.; Singh, S.N. Postdengue Acute Disseminated Encephalomyelitis. J Assoc Physicians India 2024, 72, 94–96. [CrossRef]
- Yamani, N.; Olesen, J. New Daily Persistent Headache: A Systematic Review on an Enigmatic Disorder. J Headache Pain 2019, 20, 80. [CrossRef]
- de Abreu, L.V.; Oliveira, C.B.; Bordini, C.A.; Valença, M.M. New Daily Persistent Headache Following Dengue Fever: Report of Three Cases and an Epidemiological Study. Headache 2020, 60, 265–268. [CrossRef]
- Bordini, C.A.; Valença, M.M. Post-Dengue New Daily Persistent Headache. Headache 2017, 57, 1449–1450. [CrossRef]
- Soares, C.N.; Cabral-Castro, M.J.; Peralta, J.M.; de Freitas, M.R.G.; Zalis, M.; Puccioni-Sohler, M. Review of the Etiologies of Viral Meningitis and Encephalitis in a Dengue Endemic Region. J Neurol Sci 2011, 303, 75–79. [CrossRef]
- Trivedi, S.; Chakravarty, A. Neurological Complications of Dengue Fever. Curr Neurol Neurosci Rep 2022, 22, 515–529. [CrossRef]
- Rissardo, J.P.; Caprara, A.L.F. Spectrum of Movement Disorders Associated with Dengue Encephalitis. MRIMS Journal of Health Sciences 2022, 10, 109. [CrossRef]
- Batra, P.; Dhiman, N.R.; Hussain, I.; Kumar, A.; Joshi, D. Movement Disorders in Dengue Encephalitis: A Case Report and Literature Review. Encephalitis 2024, 4, 83–86. [CrossRef]
- Panda, P.K.; Sharawat, I.K.; Bolia, R.; Shrivastava, Y. Case Report: Dengue Virus-Triggered Parkinsonism in an Adolescent. Am J Trop Med Hyg 2020, 103, 851–854. [CrossRef]
- Ganaraja, V.H.; Kamble, N.; Netravathi, M.; Holla, V.V.; Koti, N.; Pal, P.K. Stereotypy with Parkinsonism as a Rare Sequelae of Dengue Encephalitis: A Case Report and Literature Review. Tremor Other Hyperkinet Mov (N Y) 2021, 11, 22. [CrossRef]
- Mohammed, A.P.; Koraddi, A.; Prabhu, A.; Kotian, C.M.; Umakanth, S. Rapidly Progressive Dementia with Seizures: A Post-Dengue Complication. Trop Doct 2020, 50, 81–83. [CrossRef]
- Srivastava, S.; Bhatia, M.S.; Jhanjee, A. Organic Mania in Dengue. J Clin Diagn Res 2013, 7, 566–567. [CrossRef]
- Mamdouh, K.H.; Mroog, K.M.; Hani, N.H.; Nabil, E.M. Atypical Dengue Meningitis in Makkah, Saudi Arabia with Slow Resolving, Prominent Migraine like Headache, Phobia, and Arrhythmia. J Glob Infect Dis 2013, 5, 183–186. [CrossRef]
- Verma, R.; Sharma, P.; Khurana, N.; Sharma, L.N. Neuralgic Amyotrophy Associated with Dengue Fever: Case Series of Three Patients. J Postgrad Med 2011, 57, 329–331. [CrossRef]
- Azmin, S.; Sahathevan, R.; Suehazlyn, Z.; Law, Z.K.; Rabani, R.; Nafisah, W.Y.; Tan, H.J.; Norlinah, M.I. Post-Dengue Parkinsonism. BMC Infect Dis 2013, 13, 179. [CrossRef]
- Fong, C.Y.; Hlaing, C.S.; Tay, C.G.; Ong, L.C. Post-Dengue Encephalopathy and Parkinsonism. Pediatr Infect Dis J 2014, 33, 1092–1094. [CrossRef]
- Jaganathan, S.; Raman, R. Hypoglossal Nerve Palsy: A Rare Consequence of Dengue Fever. Neurol India 2014, 62, 567–568. [CrossRef]
- Tan, A.H.; Linn, K.; Ramli, N.M.; Hlaing, C.S.; Aye, A.M.M.; Sam, I.-C.; Ng, C.G.; Goh, K.J.; Tan, C.T.; Lim, S.-Y. Opsoclonus-Myoclonus-Ataxia Syndrome Associated with Dengue Virus Infection. Parkinsonism Relat Disord 2014, 20, 1309–1310. [CrossRef]
- Weeratunga, P.N.; Caldera, H.P.M.C.; Gooneratne, I.K.; Gamage, R.; Perera, W.S.P.; Ranasinghe, G.V.; Niraj, M. Spontaneously Resolving Cerebellar Syndrome as a Sequelae of Dengue Viral Infection: A Case Series from Sri Lanka. Pract Neurol 2014, 14, 176–178. [CrossRef]
- Mahale, R.R.; Mehta, A.; Buddaraju, K.; Srinivasa, R. Parainfectious Ocular Flutter and Truncal Ataxia in Association with Dengue Fever. J Pediatr Neurosci 2017, 12, 91–92. [CrossRef]
- Saini, L.; Chakrabarty, B.; Pastel, H.; Israni, A.; Kumar, A.; Gulati, S. Dengue Fever Triggering Hemiconvulsion Hemiplegia Epilepsy in a Child. Neurol India 2017, 65, 636–638. [CrossRef]
- Desai, S.D.; Gandhi, F.R.; Vaishnav, A. Opsoclonus Myoclonus Syndrome: A Rare Manifestation of Dengue Infection in a Child. J Pediatr Neurosci 2018, 13, 455–458. [CrossRef]
- Higgoda, R.; Perera, D.; Thirumavalavan, K. Multifocal Motor Neuropathy Presenting as a Post-Infectious Complication of Dengue: A CASE Report. BMC Infect Dis 2018, 18, 415. [CrossRef]
- Borrelli, S.; Sinzobahamvya, E.; Smetcoren, C.; Van Den Broucke, S.; Gille, M. Post-Dengue Sacral Radiculitis Presenting as a Cauda Equina Syndrome: A Case Report. Acta Neurol Belg 2019, 119, 127–128. [CrossRef]
- Sardana, V.; Bhattiprolu, R.K. Dengue Fever with Facial Palsy: A Rare Neurological Manifestation. Ann Indian Acad Neurol 2019, 22, 517–519. [CrossRef]
- Lau, Y.H.; Chinnasami, S. Emergence of Myasthenia Gravis in Dengue Infection-First Case Report. J Neurovirol 2021, 27, 183–185. [CrossRef]
- Martin, A.; Brown, D.A.; Wolfe, N. Dengue-Associated Postinfectious Meningoencephalomyelitis With Positive Anti-GFAP Antibody. Neurol Clin Pract 2021, 11, e926–e928. [CrossRef]
- Mathew, M.; Thomas, R.; S, V.; Pulicken, M. Severe Dengue with Rapid Onset Dementia, Apraxia of Speech and Reversible Splenial Lesion. J Neurosci Rural Pract 2021, 12, 608–610. [CrossRef]
- Arora, A.; Verma, S.; Khot, N.; Chalipat, S.; Agarkhedkar, S.; Kiruthiga, K.G. A Case Report on CNS Hemophagocytic Lymphohistiocytosis in an Infant With Dengue Hemorrhagic Fever. Cureus 2023, 15, e34773. [CrossRef]
- Kumar, A.; Hussain, I.; Singh, V.K.; Joshi, D. Dengue Fever Associated Opsoclonus Myoclonus Ataxia Syndrome. Mov Disord Clin Pract 2024, 11, 1053–1054. [CrossRef]
- Misra, U.K.; Kalita, J. Spectrum of Movement Disorders in Encephalitis. J Neurol 2010, 257, 2052–2058. [CrossRef]
- Chang, S.-H.; Chang, R.; Su, C.-S.; Wei, J.C.-C.; Yip, H.-T.; Yang, Y.-C.; Li, K.-Y.; Hung, Y.-M. Incidence of Dementia after Dengue Fever: Results of a Longitudinal Population-Based Study. Int J Clin Pract 2021, 75, e14318. [CrossRef]
- Kim, H.-W. Re: Comments on “Steroid-Responsive Dengue Encephalitis Without Typical Dengue Symptoms”: The Authors Respond. J Clin Neurol 2024, 20, 464–465. [CrossRef]
- Francelino, E. de O.; Puccioni-Sohler, M. Dengue and Severe Dengue with Neurological Complications: A Challenge for Prevention and Control. Arq Neuropsiquiatr 2024, 82, 1–6. [CrossRef]
- Hadinegoro, S.R.; Arredondo-García, J.L.; Capeding, M.R.; Deseda, C.; Chotpitayasunondh, T.; Dietze, R.; Muhammad Ismail, H.I.H.; Reynales, H.; Limkittikul, K.; Rivera-Medina, D.M.; et al. Efficacy and Long-Term Safety of a Dengue Vaccine in Regions of Endemic Disease. N Engl J Med 2015, 373, 1195–1206. [CrossRef]
Figure 1.
Neuropathogenesis of Dengue Virus: Flavivirus attacks neurons directly and causes in-flammation resulting in collateral damage. Blood brain barrier is damaged resulting in cytokine release which attracts lymphocytes. Lymphocytes kill infected neurons.
Figure 1.
Neuropathogenesis of Dengue Virus: Flavivirus attacks neurons directly and causes in-flammation resulting in collateral damage. Blood brain barrier is damaged resulting in cytokine release which attracts lymphocytes. Lymphocytes kill infected neurons.
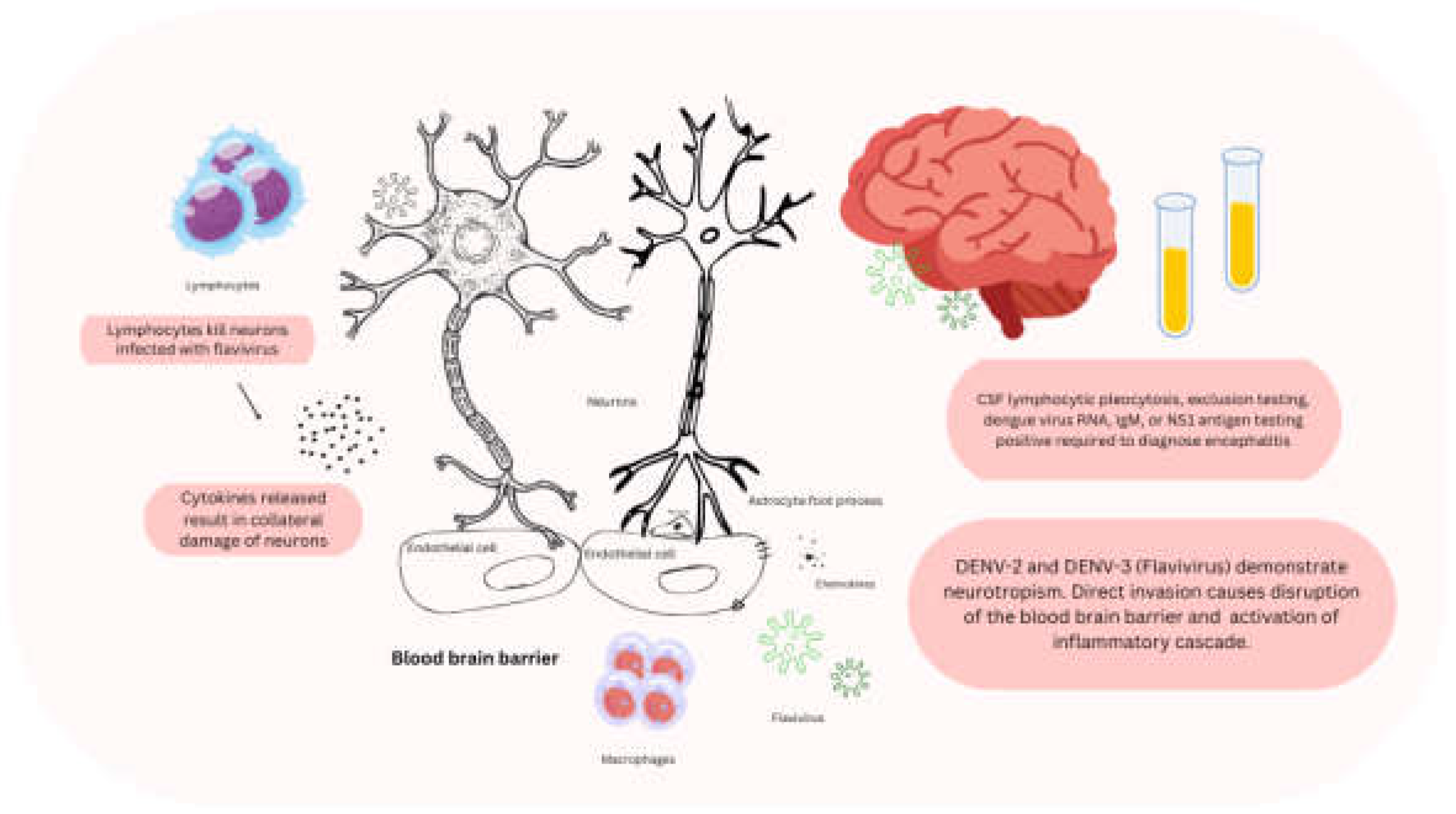
Table 1.
Clinical classification of dengue.
| Dengue without warning sign (presumptive diagnosis) | Dengue with warning signs | Severe dengue |
|---|---|---|
| Fever, and two or more symptoms Vomiting, nausea Rash Body pains Leukopenia Petechiae or tourniquet test Neighbourhood dengue, history of travel to dengue endemic area |
Abdominal pain or tenderness Persistent vomiting Clinical fluid accumulation Mucosal bleed Lethargy and restlessness Liver enlargement > 2 cm Laboratory: increase in hematocrit concurrent with rapid decrease in platelet count |
Shock Fluid accumulation with respiratory distress Severe bleeding as evaluated by clinician Severe organ involvement with liver (AST/ALT ≥ 1000) or central nervous system infection |
Table 2.
FreeText and MeSH search terms in the US National Library of Medicine.
| Query | Search Terms | Results |
|---|---|---|
| dengue fever | “dengue”[MeSH Terms] OR “dengue”[All Fields] OR (“dengue”[All Fields] AND “fever”[All Fields]) OR “dengue fever”[All Fields] | 32120 |
| dengue (and) myelitis | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND (“myelitis”[MeSH Terms] OR “myelitis”[All Fields] OR “myelitides”[All Fields]) | 111 |
| dengue (and) encephalitis | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND (“encephalities”[All Fields] OR “encephalitis”[MeSH Terms] OR “encephalitis”[All Fields]) | 2615 |
| dengue (and) ADEM | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND “ADEM”[All Fields] | 28 |
| dengue (and) new daily persistent headache | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND “new”[All Fields] AND (“dailies”[All Fields] OR “daily”[All Fields]) AND (“persist”[All Fields] OR “persistance”[All Fields] OR “persistant”[All Fields] OR “persisted”[All Fields] OR “persistence”[All Fields] OR “persistences”[All Fields] OR “persistencies”[All Fields] OR “persistency”[All Fields] OR “persistent”[All Fields] OR “persistently”[All Fields] OR “persistents”[All Fields] OR “persister”[All Fields] OR “persisters”[All Fields] OR “persisting”[All Fields] OR “persists”[All Fields]) AND (“headache”[MeSH Terms] OR “headache”[All Fields] OR “headaches”[All Fields] OR “headache s”[All Fields]) | 3 |
| dengue (and) Guillain-Barré syndrome | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND (“guillain barre syndrome”[MeSH Terms] OR (“guillain barre”[All Fields] AND “syndrome”[All Fields]) OR “guillain barre syndrome”[All Fields] OR (“guillain”[All Fields] AND “barre”[All Fields] AND “syndrome”[All Fields]) OR “guillain barre syndrome”[All Fields]) | 341 |
| dengue (and) neurological complications | (“dengue”[MeSH Terms] OR “dengue”[All Fields] OR “dengue s”[All Fields]) AND (“neurologic”[All Fields] OR “neurological”[All Fields] OR “neurologically”[All Fields]) AND (“complicances”[All Fields] OR “complicate”[All Fields] OR “complicated”[All Fields] OR “complicates”[All Fields] OR “complicating”[All Fields] OR “complication”[All Fields] OR “complication s”[All Fields] OR “complications”[MeSH Subheading] OR “complications”[All Fields]) | 441 |
Table 3.
Prevalence of neurological manifestations in patients with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Sil et al. (2017) [13] | India | 71 | A descriptive, observational, cross-sectional study analyzed 71 children aged 1–12 years with confirmed dengue infection. The study found that 28% of the children had neurological involvement. The most common neurological presentations included encephalopathy (40%), encephalitis (30%), pyramidal motor weakness (15%), transverse myelitis (TM) (5%), acute disseminated encephalomyelitis (ADEM) (5%), and Guillain-Barré syndrome (GBS) (5%). These findings highlight the diverse range of neurological complications that can occur in pediatric dengue patients and emphasize the need for careful monitoring and timely intervention to manage these potentially severe manifestations. |
| Bhushan et al. (2018) [12] | India | 1627 | A cross-sectional observational study involving 1,627 laboratory-confirmed dengue fever (DF) cases found that 14.6% of patients presented with neurological complications. Among these, 4.86% (79 patients) had immune-mediated neurological complications (IMNC). The spectrum of IMNC included Guillain-Barré syndrome (GBS), Miller Fisher syndrome (MFS), acute disseminated encephalomyelitis (ADEM), myelitis, and polyneuritis cranialis, with the majority of cases developing in a subacute period (7-30 days post-infection). Specifically, GBS was detected in 32 patients, with the acute motor and sensory axonal neuropathy (AMSAN) subtype being the most prevalent, affecting 18 patients. Additionally, three cases of MFS were identified. Of the 32 GBS patients, 25 fully recovered following treatment, which included immunoglobulins, plasmapheresis, and methylprednisolone, highlighting the effectiveness of these therapies in promoting recovery from severe neurological complications. |
| Bentes et al. (2021) [14] | Brazil | 56 | Pediatric individuals with dengue taht were hospitalized. Up to 40% complained of at least one neurological manifestation. Almost 20% was discharged with an antiseizure medication, and 10% developed a motor issue, including paresis, ataxia, weakness, and ambulation difficulty. |
| Suma et al. (2023) [15] | India | 101 | Patients diagnosed with acute encephalitis syndrome related to dengue, presented with seizures (70.3%), headache (42.6%), and vomiting (27.7%). |
| Khan et al. (2024) [16] | Bangladesh | 805 | Non-endemic area. Neurological complains were reported in 25% of the patients, but only 3% were severe. Among the individuals with severe neurological symptoms, 16% reported encephalitis symptoms. |
Table 4.
Guillain Barre syndrome associated with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Gonçalves et al. (2011) [30] | Brazil | 1 | A six-year-old girl who developed Guillain-Barré syndrome (GBS) 20 days after being diagnosed with dengue fever (DF) provides an example of the potential link between the two conditions. The similarity in the immune response observed in DF and GBS may be attributed to the role of immune-mediated mechanisms in both diseases. In dengue, the immune system can be activated by the virus, leading to inflammation and, in some cases, autoimmune responses. Similarly, in GBS, an autoimmune response, often triggered by an infection like dengue, leads to the attack on peripheral nerves, causing demyelination and ascending paralysis. In this case, the immune response to the DENV likely triggered the development of GBS, which is characterized by the activation of the immune system and the production of antibodies that mistakenly target the peripheral nervous system. This delayed onset of GBS after dengue suggests the possibility of a post-infectious immune-mediated complication. |
| Ralapanawa et al. (2015) [31] | Sri Lanka | 1 | A 34-year-old male who developed Guillain-Barré syndrome (GBS) 10 days after being diagnosed with dengue fever (DF) provides another example of how dengue can trigger immune-mediated conditions. In this case, the pro-inflammatory immune response induced by dengue likely played a key role in the development of GBS. During DF, the immune system is activated in response to the virus, leading to the release of pro-inflammatory cytokines and immune cells. In some cases, this response can become dysregulated, leading to autoimmune conditions like GBS. The mechanism is thought to involve molecular mimicry, where the immune system mistakenly targets the peripheral nervous system due to similarities between viral proteins and nerve tissue. This results in inflammation and demyelination of the peripheral nerves. Plasmapheresis, used in this case, helps to remove the antibodies and inflammatory mediators from the blood, facilitating recovery. This example illustrates how dengue infection can induce a pro-inflammatory response that contributes to immune-mediated conditions such as GBS. Similar immune-mediated complications, including acute disseminated encephalomyelitis (ADEM) and other neuropathies, can also arise from this inflammatory response triggered by dengue. |
| Simon et al. (2016) [5] | France | 3 | Early GBS and dengue fever. Contrary to most cases, a serum diagnosis of dengue within one week was observed. It is considered a post-infectious disease. |
| Fragoso et al. (2016) [32] | Brazil | 10 | In all cases of Guillain-Barré syndrome (GBS) following dengue fever (DF), acute motor-sensory axonal neuropathy (AMSAN) was identified as the predominant subtype. The average time between the onset of DF and the development of GBS was eleven days. All patients received the same treatment regimen, consisting of intravenous immunoglobulin (IVIG), which is commonly used to modulate the immune response and reduce inflammation in GBS. Recovery varied among patients, with full recovery occurring within a range of nine days to one year. This variability in recovery time underscores the complex nature of GBS and its potential long-term effects, even with appropriate treatment. The development of AMSAN, characterized by motor and sensory axonal damage, in these patients highlights the severe nature of the neurological complications that can arise after dengue infection. |
| Dalugama et al. (2018) [27] | Sri Lanka | 1 | In hyperendemic regions, screening for dengue in patients presenting with acute flaccid paralysis may be essential. One potential mechanism is molecular mimicry, where the cell-mediated immune response to foreign antigens inadvertently targets the host’s nerve tissue. Another possibility is that pro-inflammatory cytokines, such as TNF, complement proteins, and interleukins, which are involved in the immune response to dengue fever, may play a significant role in the development of neurological complications. |
| Pandey et al. (2018) [33] | India | 2 | The case of two brothers presenting simultaneously with the axonal variant of Guillain-Barré syndrome (GBS), both associated with mild dengue fever, suggests the possibility of a genetic predisposition to GBS following dengue infection. Genetic factors may influence the immune response to the virus, potentially making certain individuals more susceptible to developing GBS. For example, genetic variations in immune-related genes, such as those involved in the cytokine response (e.g., TNF, IL-6), or genes related to the function of the peripheral nervous system, may increase the likelihood of an exaggerated immune response, leading to autoimmune damage to the nerves. Additionally, variations in the major histocompatibility complex (MHC) genes, which play a critical role in immune recognition, could predispose individuals to develop autoimmune conditions like GBS following viral infections, including dengue. This case highlights the potential for genetic mechanisms to contribute to the development of GBS in response to dengue fever, though further studies are needed to identify specific genetic markers associated with this risk. |
| Pandey et al. (2019) [34] | India | 1 | A case report of a pharyngeal-cervical-brachial variant of GBS associated with dengue fever infection. |
| Silva et al. (2019) [35] | Sri Lanka | 1 | Guillain-Barré syndrome (GBS) and its variants typically develop one or more weeks after the acute infection, indicating an underlying immunological mechanism. The DENV has a potential neurotropism for peripheral nerves, which contributes to the development of neurological complications. In this case, Miller Fisher syndrome (MFS) was considered a parainfectious manifestation rather than a postinfectious one. |
| Pari et al. (2022) [36] | India | 5 | From 5 patients with GBS associated with dengue and positive serum serology for dengue, only one had positivity to dengue in the CSF. |
| Payus et al. (2022) [37] | Malaysia | 1 | Sensory only, and improved with IVIG. |
| Lim et al. (2023) [38] | Malaysia | 1 | Patient improved without specific management. |
| Rajurkar et al. (2023) [39] | India | 1 | Pediatric patient with GBS associated with DENV infection, and patient was managed with physiotherapy. |
| Mahashabde et al. (2024) [40] | India | 1 | Diagnosed with acute motor axonal neuropathy. IVIG was started with full improvement. |
| Rayamajhi et al. (2024) [41] | Nepal | 1 | No electromyography was performed. Patient received plasmapheresis with full improvement. |
Table 5.
Myopathy associated with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Malheiros et al. (1993) [46] | Brazil | 15 | Perivascular infiltrates were observed in 12 out of 15 patients with classic dengue fever, although there was no evidence of myositis. None of the patients displayed abnormalities on neurological examination, and only three had elevated creatine kinase (CK) levels in their serum. These findings suggest that while muscular involvement, such as perivascular inflammation, can occur in dengue fever, it may not always lead to overt muscle damage or clinical symptoms like weakness or myositis. The absence of significant neurological findings further indicates that these muscular changes may not be linked to overt neurological complications in most patients. |
| Finsterer et al. (2006) [47] | Austria | 1 | A 38-year-old male developed severe headaches and fever while vacationing in Thailand, followed by intense myalgia rated 10/10. After 36 days, his myalgia persisted at a level of 6/10, and electromyography revealed spontaneous electrical activity in the subscapularis muscle. Sixty-two days after the onset of symptoms, he was treated with dexamethasone for three weeks, which successfully resolved the pain. |
| Acharya et al. (2010) [48] | India | 1 | A 40-year-old male initially presented with fever, myalgia, muscle tenderness, and pain on movement, but with normal muscle strength. The following day, he developed flaccid quadriparesis, which progressed to pharyngeal muscle weakness, head drop, respiratory insufficiency, and rhabdomyolysis. A muscle biopsy revealed perifascicular myonecrosis. |
| Sangle et al. (2010) [49] | India | 1 | A 16-year-old girl was diagnosed with both myositis and myocarditis following a dengue infection. She initially presented with the typical symptoms of dengue, including fever, headache, and muscle pain. However, her condition progressed to include significant muscle inflammation (myositis), leading to muscle weakness and tenderness. Additionally, she developed myocarditis, an inflammation of the heart muscle, which resulted in chest pain, tachycardia, and difficulty breathing. These complications are relatively rare but have been reported in severe cases of dengue infection. Both myositis and myocarditis can lead to long-term complications if not promptly managed. In this case, appropriate treatment and close monitoring helped manage her symptoms, although the recovery process required careful follow-up. |
| Paliwal et al. (2011) [50] | India | 7 | Dengue myositis can present with a wide range of clinical manifestations, from mild, asymmetric muscle weakness to severe cases. In some instances, such as in three reported patients, the condition progressed to fulminant myositis, characterized by rapid onset of muscle inflammation, severe pain, and significant muscle weakness. These severe cases often require urgent medical intervention due to the potential for complications like rhabdomyolysis, respiratory failure, or cardiac involvement. The wide spectrum of severity underscores the need for careful monitoring and management in patients with suspected dengue myositis. |
| Kalita et al. (2012) [51] | India | 13 | Thirteen patients with dengue myopathy underwent electromyography (EMG) and were followed for one month. The muscle weakness was more pronounced in the proximal muscles, particularly in the lower limbs. Interestingly, there was no significant difference in the EMG findings between the severe and mild cases. None of the patients exhibited signs of inflammatory myopathies, suggesting that the myopathy associated with dengue is not primarily inflammatory in nature, even though it can cause significant weakness, particularly in the proximal muscles. |
| Misra et al. (2012) [52] | India | 39 | In a study of sixteen patients, eight exhibited severe muscle weakness accompanied by elevated creatine kinase (CK) levels, while fifteen patients only had elevated CK levels without muscle weakness. Among the patients with muscle weakness, five presented with hypotonia and hyporeflexia. Remarkably, all patients had a full recovery within two weeks. Electromyography (EMG) did not reveal characteristics of inflammatory myopathy, and the three patients who underwent muscle biopsy showed no signs of myositis. These findings suggest that while muscle weakness and elevated CK levels are common in dengue myopathy, the condition may not involve significant inflammatory changes in muscle tissue. |
| Misra et al. (2015) [11] | India | 116 | In this prospective study, 79% of the 116 patients analyzed developed neurological complications. Of these, 34% presented with encephalopathy or encephalitis, while 45% experienced muscle dysfunction. Among the 34 patients with muscle dysfunction, all had muscle weakness accompanied by elevated creatine kinase (CK) levels. Additionally, 97% of patients with muscle weakness reported myalgia. The muscle weakness was severe in 20 patients, and 16 of these patients exhibited hyporeflexia. These findings highlight the significant prevalence of muscle-related complications in dengue patients, with a notable association between muscle weakness and elevated CK levels. |
| Verma et al. (2017) [53] | India | 30 | In this observational study, 14 out of 30 patients with elevated creatine kinase (CK) levels were found to have dengue infection as the underlying cause. Among these patients, 5 had hypokalemia, while 9 had normokalemia. Notably, the patients with normokalemia were more likely to have CK levels that were 10 times higher than the average value, compared to those in the hypokalemic group. This suggests that normokalemia may be associated with more severe muscle damage, as reflected by significantly elevated CK levels in dengue patients. |
| Arif et al. (2022) [54] | Pakistan | 1 | Rhabdomyolysis and compartment syndrome. |
| Mekmangkonthong et al. (2022) [55] | Thailand | 1 | He received IVIG, and steroid taper followed by methotrexate. |
| Rashid et al. (2022) [56] | Pakistan | 1 | Her myositis did not improve with steroids, and required IVIG. |
| Putri et al. (2024) [57] | Thailand | 1 | Cautious with patients with comorbidities that may contribute to a worse prognosis. |
| Samarasingha et al. (2024) [58] | Sri Lanka | 1 | Treated with hemoperfusion using CytoSorb® in combination with continuous renal replacement therapy. |
Table 6.
Dengue virus encephalitis.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Borawake et al. (2011) [61] | India | 1 | DENV-associated encephalitis |
| Rao et al. (2013) [60] | India | 1 | DENV-associated encephalitis is characterized by the presence of DENV antibodies and antigen in the cerebrospinal fluid (CSF) of affected patients. This finding supports the diagnosis of encephalitis directly linked to the DENV, distinguishing it from other complications such as encephalopathy, which may arise from systemic issues. The detection of these markers in the CSF indicates a direct involvement of the virus in the central nervous system, leading to neurological manifestations. Such cases, while less common, highlight the need for careful evaluation and monitoring of patients with dengue fever, especially those exhibiting neurological symptoms. Prompt identification can be critical for management and treatment to mitigate potential long-term effects. |
| Cristiane et al. (2014) [62] | Brazil | Not applicable | Revised proposal for the definition of dengue encephalitis: (1) presence of fever; (2) acute symptoms of brain involvement, including altered consciousness or personality changes, seizures, and neurological abnormalities; (3) detection of reactive IgM dengue antibodies, NS1 antigen, or positive dengue PCR in serum and cerebrospinal fluid, based on the onset time; (4) elimination of other possible causes of viral encephalitis and encephalopathy. |
| Withana et al. (2014) [63] | Sri-Lanka | 1 | A notable case of acute cerebellitis has been linked to dengue fever. Furthermore, research indicates that dengue antigens can be identified in the brains of patients suffering from dengue encephalitis. |
| Garg et al. (2017) [64] | India | 1 | The brainstem, cerebellum, corpus callosum, and thalamus play crucial roles in the pathology of dengue encephalitis. This condition is characterized by the presence of multifocal hyperintensities observed in bilateral periventricular zones, which notably include the basal ganglia. These abnormalities are particularly evident on T2-weighted (T2W) and Fluid-Attenuated Inversion Recovery (FLAIR) imaging sequences, highlighting the impact of the disease on specific areas of the brain. |
| Kumar et al. (2017) [65] | India | 1 | A 22-year-old female, who is experiencing her first pregnancy, was diagnosed with encephalitis linked to dengue fever (DF). Upon examination using magnetic resonance imaging (MRI), distinct lesions were observed in her brain, resembling a “double doughnut” sign—characterized by a central area of low intensity surrounded by a ring of higher intensity, presenting a striking visual pattern indicative of her condition. |
| Kutiyal et al. (2017) [66] | India | 1 | The brain MRI, utilizing T2-weighted and FLAIR sequences, reveals areas of hyperintensity in the bilateral ganglio-thalamic complex, as well as in the periventricular and peritrigonal white matter. These findings are indicative of changes associated with Dengue encephalitis. |
| Sivamani et al. (2017) [67] | India | 1 | A patient diagnosed with encephalitis exhibited positive serology results for both DENV and Japanese encephalitis virus. However, the authors understood the necessity of conducting polymerase chain reaction (PCR) testing to determine whether the patient was truly experiencing a dual infection or if the positive serology results were simply due to cross-reactivity between the two viruses. |
| Jois et al. (2018) [68] | India | 3 | Dengue fever (DF) can exhibit viral neurotropism, leading to direct damage to neuronal tissues and potentially resulting in viral encephalitis. Autopsy examinations revealed significant cerebral edema, characterized by the obliteration of the brain’s sulci and a notable flattening of the gyri. The dura mater displayed elevated tension, and numerous hemorrhagic foci were observed throughout the brain, indicating severe vascular compromise. On a microscopic level, the predominant findings included pronounced cerebral edema, a marked inflammatory response, and evidence of hemorrhage. Notably, all three patients involved in this case study tested positive for the NS-1 dengue antigen, further confirming the viral involvement in their neurological symptoms. |
| Singh et al. (2018) [67] | India | 1 | In a patient who succumbed to dengue encephalitis on the seventh day of their illness, a distinctive Jack-o’-lantern sign was observed. This particular sign, often characterized by its appearance, highlighted the severe complications associated with the disease. |
| Chatur et al. (2019) [69] | India | 2 | In two documented cases of dengue encephalitis, the patients exhibited a distinctive radiological feature known as the “double doughnut sign.” This sign is characterized by a symmetrical pattern of involvement affecting the bilateral central nervous system (CNS) parenchyma, highlighting the unique bilateral nature of the neurological impact associated with this viral infection. |
| Kyaw et al. (2019) [70] | Myanmar | 123 | The study aimed to assess the prevalence and impact of the Japanese encephalitis virus and DENV in children under the age of 13 in Myanmar. Among the 123 pediatric patients evaluated, researchers identified a single case of dengue fever, highlighting the relative rarity of this virus in the population sampled. |
| Weerasinghe et al. (2019) [71] | Sri-Lanka | 1 | A detailed case report describes an 18-year-old patient who was diagnosed with encephalitis in conjunction with dengue hemorrhagic fever (DHF). This individual presented with neurological symptoms alongside the typical manifestations of DHF, such as high fever, bleeding tendencies, and thrombocytopenia. The medical team closely monitored the patient’s condition, considering the potential complications arising from the co-occurrence of these two serious illnesses. |
| Pandeya et al. (2022) [72] | Nepal | 1 | “double-doughnut” sign |
| Barron et al. (2024) [73] | United Kingdom | 162 | Systematic review of dengue-associated acute necrotizing encephalopathy, which has a worst prognosis when compared to other types of encephalopathy. |
| Berdiñas Anfuso et al. (2024) [74] | Argentina | 3 | Patients experienced refractory status epilepticus and minor disorientation, and in all three cases the neuroimaging was normal. |
| Gupta et al. (2024) [75] | India | 1 | Bilateral thalamic hyperintensities with central diffusion restriction. |
| Harshani et al. (2024) [76] | Sri Lanka | 1 | Post-mortem analysis of myocardial tissue revealed inflammation and findings concerning for viral myocarditis. No brain tissue was assessed. |
| Hussain et al. (2024) [77] | Sri Lanka | 1 | Patient presenting with acute psychosis reported as agitation and aggressive behavior. |
| Khosla et al. (2024) [78] | India | 4 | Authors stated the significance of a broad differential diagnosis including malaria, tuberculosis, herpes encephalitis, and bacterial meningitis in cases concerning for dengue encephalitis. |
| Mun et al. (2024) [79] | Korea | 1 | Dengue encephalitis responsive to short course of high-dose steroid therapy. His symptoms were mainly characterized by motr aphasia and cognitive dysfunction. |
| Shah et al. (2024) [80] | India | 1 | Double-doughnut is a sign not pathognomonic of dengue encephalitis. Other virus of Flaviridae family were already associated with this finding. |
| Verma et al. (2024) [81] | India | 29 | TLR3 Leu412Phe polymorphism for the mutant genotype Phe/Phe (TT) demonstrated increased association with dengue encephalitis. |
Table 8.
Acute disseminated encephalomyelitis associated with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Viswanathan et al. (2016) [112] | Malaysia | 2 | Two cases of acute disseminated encephalomyelitis (ADEM) associated with dengue fever (DF) have been reported that mimicked multiple sclerosis (MS) on neuroimaging. In these cases, the neuroimaging findings showed lesions in the brain and spinal cord that were similar to those seen in MS, leading to an initial misdiagnosis. However, the presence of dengue fever and the clinical progression of the disease helped differentiate ADEM from MS. These cases highlight the importance of considering ADEM as a potential diagnosis in patients with dengue fever who present with neurological symptoms, especially when neuroimaging resembles MS. |
| Kamel et al. (2017) [113] | Meta-analysis | 29 | In this meta-analysis, the authors found a 0.4% prevalence of acute disseminated encephalomyelitis (ADEM) among patients with dengue fever, accounting for 6.8% of all neurological complications associated with dengue. This indicates that while ADEM is a rare complication of dengue fever, it represents a significant portion of the neurological disorders that can occur in these patients, underlining the importance of early diagnosis and management. |
| Wan Sulaiman et al. (2017) [114] | Review | 22 | This narrative review provides a comprehensive summary of 22 reported cases of Acute Disseminated Encephalomyelitis (ADEM) that have been associated with dengue fever. The review highlights the clinical presentations, diagnostic challenges, underlying mechanisms, and outcomes observed in these cases, aiming to enhance understanding of the relationship between dengue infection and ADEM. It synthesizes findings from various studies to illustrate the clinical spectrum and implications for diagnosis and treatment in affected patients. |
| Rastogi et al. (2019) [115] | India | 1 | This case report presents the clinical progression of a male patient who received a diagnosis of Acute Disseminated Encephalomyelitis (ADEM) subsequent to an episode of dengue fever. The patient experienced a rapid deterioration in his condition, culminating in respiratory failure that required intervention through mechanical ventilation. Notably, he exhibited a favorable response to corticosteroid treatment, underscoring the potential efficacy of this therapeutic approach in comparable clinical scenarios. |
| Diallo et al. (2020) [116] | France | 1 | Authors reported that dengue PCR negative in teh CSF does not exclude the possibility of being dengue as the primary cause. |
| Farooque et al. (2020) [117] | Pakistan | 1 | The patient showed significant improvement following a brief regimen of high-dose corticosteroids, which effectively reduced inflammation and alleviated symptoms. The treatment was carefully monitored, and the positive response was evident in both clinical evaluation and patient-reported outcomes within a few days. |
| Chakraborty et al. (2024) [118] | India | 1 | Brain and spine MRIs with multiple demyelinating lesions, and they occurred after the fever improvement. |
| Chayanopparat et al. (2024) [86] | Thailand | 1 | No biopsy, but patient was diagnosed with tumefactive acute disseminated encephalomyelitis. |
Table 9.
New Daily Persistent Headache associated with dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Bordini et al. (2017) [121] | Brazil | 2 | A 23-year-old Caucasian male reports a two-year struggle with debilitating bilateral headaches that feel like severe pressure. These headaches have not responded to various treatments, including amitriptyline, divalproex, and topiramate. He experienced temporary relief that lasted two weeks following a nerve blockade. In contrast, a 42-year-old Caucasian female deals with moderate to severe bilateral pressure headaches that sometimes come with nausea, as well as heightened sensitivity to light and sound (photophobia and phonophobia). She experienced significant relief after a 10-day course of dexamethasone, demonstrating the effectiveness of corticosteroids in alleviating her symptoms. |
| Abreu et al. (2020) [120] | Brazil | 450 | Among the total of 600 reported cases of dengue fever, the authors successfully made contact with 450 of those individuals. Out of the 450 patients reached, three cases were confirmed to have NDPH, which corresponds to a prevalence rate of 0.67% (or approximately 1 in every 150 individuals) of NDPH specifically associated with dengue fever infections. |
Table 10.
Other neurological manifestations of dengue virus infection.
| Reference | Country | N | Commentary |
|---|---|---|---|
| Verma et al. (2011) [131] | India | 3 | In a detailed case series examining patients who experienced neuralgic amyotrophy linked to dengue infection, it was observed that two of these individuals demonstrated a remarkable and complete restoration of muscle strength by the third month of follow-up. This recovery highlights the potential for significant improvement in this specific patient population after the onset of the illness. |
| Azmin et al. (2013) [132] | Malaysia | 1 | An 18-year-old male presented with a complex neurological condition characterized by parkinsonism-related cerebellar ataxia, which resulted in an unsteady gait and difficulties with coordination. In addition to these symptoms, he exhibited multiple cranial neuropathies, which manifested as weaknesses and sensory changes in the cranial nerve distribution. Furthermore, he developed brachial plexopathy, leading to significant muscle denervation that was confirmed through electromyography after one month from the onset of his symptoms. Remarkably, this array of neurological issues emerged following a recent infection with dengue fever, highlighting a potential post-viral complication. |
| Mamdouh et al. (2013) [130] | Saudi Arabia | 2 | In two reported cases of atypical meningitis caused by the DENV, the patients experienced recurrent episodes resembling severe migraine attacks. Alongside these debilitating headaches, they exhibited intense phobias characterized by an overwhelming sense of impending doom, as if they were on the brink of death. Additionally, both individuals displayed symptoms indicative of cardiac dysautonomia, suggesting disruptions in their autonomic nervous system that affected heart function and regulation. |
| Srivastava et al. (2013) [129] | India | 1 | This is a detailed case report focusing on a 21-year-old individual who, despite having no significant family history of mental health issues or any identifiable risk factors, exhibited pronounced manic symptoms following an episode of dengue fever infection. |
| Fong et al. (2014) [133] | Malaysia | 1 | A remarkable case of pediatric post-dengue encephalopathy parkinsonism was observed in a 6-year-old patient. After experiencing the debilitating effects of the illness, it took approximately 7 weeks for the child to recover and regain normal neurological function. Throughout this challenging period, the child’s resilience was evident as they navigated through the symptoms and ultimately returned to their usual activities. |
| Jaganathan et al. (2014) [134] | India | 1 | This is a detailed case report highlighting an isolated paralysis of the hypoglossal nerve that occurred in a patient infected with the DENV. The report aims to explore the unique presentation and implications of this neurological complication arising from the viral infection. |
| Tan et al. (2014) [135] | Malaysia and Myanmar | 2 | Two reports of opsoclonus-myoclonus have been reported in patients with dengue fever. The first case involved a 30-year-old male who exhibited patchy enhancement of the leptomeninges. The second case was observed in a 10-year-old child whose EEG and computed tomography results were normal; an MRI was not conducted in this situation. |
| Weeratunga et al. (2014) [136] | Sri Lanka | 3 | The authors presented a detailed analysis of three specific cases of cerebellar syndrome that were associated with DENV infection. In each case, laboratory tests identified the presence of IgM antibodies against the DENV in the cerebrospinal fluid (CSF) of the affected patients. This finding suggests a direct link between the dengue infection and the neurological symptoms observed, highlighting the potential for dengue to impact the central nervous system. The clinical implications of these cases underscore the need for increased awareness of neurological complications among patients diagnosed with dengue. |
| Mahale et al. (2017) [137] | India | 1 | This case report focuses on a 14-year-old boy who presented with a combination of ocular flutter and truncal ataxia, in conjunction with a dengue fever infection. Ocular flutter, characterized by involuntary, rapid eye movements, along with truncal ataxia, which affected his balance and coordination, were significant concerns. The boy received a treatment regimen that included corticosteroids, and notably, both his ocular flutter and ataxia showed marked improvement following the intervention. This case highlights the importance of addressing neurological symptoms in the context of viral infections. |
| Saini et al. (2017) [138] | India | 1 | This is a case study of hemiconvulsion-hemiplegia epilepsy, which was triggered by an infection with the DENV. In this particular instance, the patient experienced a series of severe convulsive episodes affecting one side of the body, alongside significant weakness or paralysis on the same side. The onset of these neurological symptoms followed a confirmed DENV infection, indicating a potential link between the viral illness and the development of this rare form of epilepsy. Further examination and monitoring were conducted to manage the patient’s condition and assess the long-term implications of the virus on neurological health. |
| Desai et al. (2018) [139] | India | 1 | This is a case report detailing the experience of a 14-year-old boy who was diagnosed with dengue fever. Remarkably, he developed rare neurological symptoms characterized by opsoclonus-myoclonus, which are involuntary eye movements and muscle jerks. Fortunately, these symptoms exhibited a spontaneous resolution within a two-week period, highlighting the transient nature of his condition amidst the dengue infection. |
| Higgoda et al. (2018) [140] | Sri Lanka | 1 | This is a case report involving a patient who developed multiple motor neuropathy as a complication of dengue fever infection. The patient’s neurological symptoms, characterized by muscle weakness and impaired motor function, emerged during the course of the viral illness. Following a thorough assessment, the treatment approach included the administration of immunoglobulin therapy, which has been shown to provide supportive care in similar neurological manifestations. Fortunately, the patient responded positively to this intervention, exhibiting significant improvement in motor function and a gradual recovery from the neuropathic symptoms associated with the dengue infection. This case highlights the potential for effective treatment of motor neuropathy linked to dengue through the use of immunoglobulin therapy. |
| Borrelli et al. (2019) [141] | Belgium | 1 | A case report involving a 35-year-old female patient who experienced fever, muscle pain, eye discomfort, and joint pain following a trip to Brazil. Two months later, she developed cauda equina syndrome and was diagnosed with immune-mediated sacral radiculitis linked to dengue fever. In her cerebrospinal fluid, she tested positive for IgM antibodies for dengue, along with the presence of oligoclonal IgG bands. |
| Sardana et al. (2019) [142] | India | 1 | This report discusses a clinical case involving a patient who developed facial nerve palsy in conjunction with a dengue fever infection. The patient’s medical history includes typical symptoms of dengue, such as high fever, severe headaches, joint and muscle pain, rash, and fatigue. However, the patient also presented with neurological complications, specifically facial nerve palsy, which manifested as weakness or paralysis of the facial muscles on one side of the face. This condition raised concerns about the potential complications of DENV beyond its usual hematological implications. Further investigations revealed that the facial nerve palsy likely resulted from viral infection and inflammation affecting the nervous system. The case emphasizes the need for awareness of such neurological manifestations in patients diagnosed with dengue fever. |
| Mohammed et al. (2020) [128] | India | 1 | A 64-year-old female presented with rapidly advancing dementia linked to focal epilepsy, which began one month after she had an uncomplicated dengue infection. Investigations for autoimmune disorders yielded negative results, and her MRI was normal. She was treated with intravenous corticosteroids and showed gradual improvement within four weeks. |
| Lau et al. (2021) [143] | Malaysia | 1 | Myasthenia gravis like presentation with bilateral ptosis and dysphagia. |
| Martin et al. (2021) [144] | Australia | 1 | Anti-glial fibrillary acidic protein positive. Travel to the Philippines. |
| Mathew et al. (2021) [145] | India | 1 | Sudden onset dementia, speech apraxia, and a reversible splenial lesion. The lesion located in the corpus callosum is connected to cytotoxic edema and is typically linked to mild cognitive impairment that occurs in isolation. |
| Arora et al. (2023) [146] | India | 1 | Pediatric individual with dengue that had CNS hemophagocytic lymphohistiocytosis. |
| Biswas et al. (2024) [91] | Bangladesh | 1 | Intrauterine death in a pregnant patient that developed posterior reverisble encephalopathy likely associated with dengue fever. |
| Kumar et al. (2024) [147] | India | 1 | Dengue Fever Associated Opsoclonus Myoclonus Ataxia Syndrome |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



