
Submitted:
03 December 2024
Posted:
03 December 2024
You are already at the latest version
Abstract
The Eastern Mediterranean Region (EMR), with its diverse ecological zones, is currently experi-encing climate changes in temperature and precipitation at rates that surpass the global average. This heightened variability significantly increases the region's vulnerability to climate impacts. Using the Climate Risk Index (CRI) by Germanwatch and the Notre Dame Global Adaptation Initiative (ND-GAIN), we evaluated the susceptibility of EMR countries to these changes. Fur-thermore, we investigated the relationship between climate vulnerabilities and public health, focusing on climate-sensitive communicable diseases such as diarrheal diseases, cholera, malaria, and Crimean-Congo Haemorrhagic Fever (CCHF). We identified regional trends, progress, and preparedness gaps by recalibrating ranking data from both indices. Our findings reveal significant climate-induced shifts that challenge traditional economic classifications of EMR countries. No-tably, public health systems are increasingly burdened by climate-driven infectious diseases, highlighting the gravity of the situation. This study underscores the importance of urgent action for integrating climate adaptation measures into public health frameworks and fostering regional collaboration to mitigate the evolving threats of climate change.
Keywords:
Eastern Mediterranean Region
; Communicable Diseases
; Climate Risk Index
; ND-GAIN
; Climate Vulnerability
; Adaptation Strategies
; Climate Change
; Public Health Impacts
; Infectious Disease Trends
1. Introduction
The Eastern Mediterranean Region (EMR), with its unique blend of climates ranging from arid deserts to lush temperate zones, is experiencing warming at a rate significantly higher than the global average [1]. This accelerated warming, compounded by the region's intricate natural, societal, and economic systems, underscores its heightened vulnerability to the diverse impacts of climate change [2,3]. These vulnerabilities, transcending traditional economic classifications, are closely linked to the region's public health challenges, particularly the spread of climate-sensitive infectious diseases. The urgency of this research is underscored by the need for immediate action to mitigate these impacts.
Country-specific vulnerabilities to climate fluctuations within the EMR are often assessed using indices synthesizing environmental and socio-economic indicators. This study employs two such indices: the Climate Risk Index (CRI) by Germanwatch, which evaluates weather-related loss events such as storms, floods, and heatwaves with a focus on human rights and development, and the Notre Dame Global Adaptation Initiative (ND-GAIN), which combines 45 indicators across critical sectors like food, water, health, infrastructure, and ecosystem services to measure a country's vulnerability and readiness for resilience. These indices reveal shifting vulnerabilities that increasingly defy traditional economic groupings, suggesting direct implications for infectious diseases' incidence and geographic spread.
The complex climatic narrative of the EMR is intricately shaped by its proximity to significant bodies of water and unique geological structures. Influential phenomena such as the North Atlantic Oscillation (NAO), the Indian Ocean Dipole (IOD), and the El Niño-Southern Oscillation (ENSO) are potent forces that significantly influence the region's climate patterns. [4,5,6]. These patterns manifest in increased temperatures and a rise in hydrological extremes, such as floods and droughts, posing considerable challenges to the region's infrastructure, agriculture, and water resources [7,8]. The anticipated northward migration of jet streams and storm paths may increase precipitation in specific areas; however, the overarching trend points to a drying trajectory that has profound implications for river systems and the agricultural livelihoods they support [9,10,11,12].
The EMR's vulnerability to climate impacts extends to public health. In 2021, the region reported over 12 million COVID-19 cases and 194,245 deaths, with a case-fatality ratio of 1.8%. Additionally, 31 major outbreaks of infectious diseases were reported across 11 countries, including acute watery diarrhea, cholera, Crimean-Congo hemorrhagic fever (CCHF), dengue, extensively drug-resistant typhoid fever, hepatitis E, measles, and wild poliovirus. Seven countries experienced vaccine-derived poliovirus type 2 (VDPV2) outbreaks, while 17 sporadic MERS cases were reported in Saudi Arabia and the UAE. These outbreaks resulted in over 398,140 cases and 682 deaths, with WHO supporting detection and response efforts [13]. Figure 1 illustrates the distribution of infectious disease outbreaks across the EMR in 2021.
Yemen's severe cholera outbreak in 2017, with over 1.5 million suspected cases, highlights the urgent need to investigate how climate variability influences disease patterns [14]. Similarly, Djibouti experienced a surge in malaria cases due to the invasive Anopheles Stephensi mosquito. The outbreak worsened due to optimal urban breeding conditions, with malaria cases surging by 42.9 times from 2013 to 2021, reaching around 72,300 cases [15,16]. This increase has continued into 2023, posing a severe public health challenge. In 2022, Iraq experienced a significant outbreak of Crimean-Congo hemorrhagic Fever (CCHF), with 212 reported cases between January and May, including ninety-seven confirmed cases and 27 deaths, primarily in the Thiqar governorate [15]. The outbreak, transmitted through tick bites and contact with infected animal blood or tissues, strained Iraq's already challenged healthcare system.
Despite numerous studies on climate-related health impacts, a critical gap persists in the integration of qualitative assessments with quantitative indices, such as the Climate Risk Index (CRI) and the Notre Dame Global Adaptation Initiative (ND-GAIN), to comprehensively analyze the intersection of climate change and public health. This study bridges this gap by employing a mixed-methods approach to assess climate change vulnerabilities and their health impacts. By coupling climate indicators with trends in infectious diseases, this work provides a comprehensive overview of the region's emerging "communicable disease map," informing regional adaptation strategies and contributing to the global understanding of climate-health dynamics.
2. Materials and Methods
Study Objectives: This study critically assesses the health sector's vulnerability to climate change in Eastern Mediterranean Region (EMR) countries, spanning two decades from 1999 to 2022. By employing a mixed-methods approach, it integrates climate indicators with disease trends to offer a comprehensive perspective on emerging climate-related public health risks. The findings, which are important, are intended to inform targeted adaptation strategies and contribute to advancing the climate change and public health field.
Research Approach and Data Sources: The methodology integrates four analytical tracks to comprehensively address the intersection between climate change and health vulnerabilities from multiple perspectives. This integrated approach ensures a thorough analysis, identifying disparities, evaluating the concordance between climate vulnerability indices and public health challenges, and enhancing the depth of the study.
Track one. Global Vulnerability Indicators (CRI): The Climate Risk Index (CRI) quantifies exposure to climate-related disasters from 2000 to 2019, including mortality rates and economic losses [17,18]. This track provides a global perspective on exposure to climate-related disasters.
Track two. Health Vulnerability Indicators (ND-GAIN): The Notre Dame Global Adaptation Initiative (ND-GAIN) assesses vulnerability and readiness to adapt to climate change, focusing on the health sector [18,19].
Track three. Climatological Data Analysis: Surface air temperature and precipitation data for selected EMR countries were sourced from the NASA GISS Surface Temperature Analysis (GISTEMP) dataset. This data set provides comprehensive historical and projected climate data, enabling the evaluation of climatic trends and variability across the region [20].
Track four. Climate-Related Disease Patterns: This track investigates the relationship between climatic changes and regional patterns of climate-sensitive diseases, including diarrheal diseases, cholera, malaria, and Crimean-Congo hemorrhagic fever (CCHF), which were analyzed using publicly available datasets and literature.
Data Availability: All datasets used in this study, which are crucial for further research and policy development, are publicly available. The CRI data can be accessed at Germanwatch, ND-GAIN data at ND-GAIN.org, and climatological data at NASA GISS Surface Temperature Analysis (GISTEMP) dataset.
Ethical Considerations: No human or animal subjects were involved in this study, and no ethical approval was required.
3. Discussion
3.1. ND-Gain and CRI
The ND-GAIN Index assesses the country's preparedness to handle health-related climate challenges. It does so through a framework categorizing indicators into exposure, sensitivity, and adaptive capacity. Exposure indicators primarily forecast changes in disease patterns and mortality rates that could result from climate-induced health issues. On the other hand, sensitivity indicators highlight infrastructural weaknesses and societal capabilities to face health emergencies, revealing the underlying vulnerabilities within a health system. Adaptive capacity indicators evaluate the availability of critical health resources such as medical staff and sanitation facilities, providing a comprehensive picture of a country's resilience to health challenges posed by climate change [21].
The health vulnerability analysis in the Eastern Mediterranean Region (EMR) underscores the varying levels of preparedness and resilience among countries. Nations such as Afghanistan, Djibouti, Pakistan, Somalia, Sudan, and Yemen exhibit high vulnerability, with indices greater than 0.6. Among these, Afghanistan, Djibouti, and Pakistan have experienced an increase in health sector vulnerability over the past decade, while Somalia and Sudan have shown slight improvements.
Countries with moderate vulnerability, including Egypt, Iran, Iraq, Jordan, Lebanon, Libya, Morocco, and Syria, have indices ranging from 0.4 to 0.6. Jordan has significantly reduced its health sector vulnerability, decreasing from 0.41 to 0.36 over the past two decades, positioning it close to countries with lower vulnerability indices. Countries in the GCC, such as Bahrain, Kuwait, Qatar, Saudi Arabia, and the UAE, along with Tunisia, are categorized under low vulnerability, with indices below 0.4. Kuwait stands out for its consistently low vulnerability since 2000, showing a gradual decrease over the past decade. However, Oman's moderate vulnerability score indicates a pressing need for focused improvements in its health sector resilience. This underscores the urgency and importance of addressing health vulnerability in these regions. An overall summary of the dynamics of health vulnerability can be found in Table 1.
The Climate Risk Index (CRI), developed by Germanwatch, evaluates countries' and regions' vulnerability to climate-related disasters by examining both human and economic costs associated with extreme weather events. Using data from Munich Re NatCatSERVICE, one of the most comprehensive databases on natural catastrophes worldwide, the CRI calculates these metrics based on data from the past 20 years. By focusing on metrics such as number of deaths, death rates relative to population, financial losses, and the proportion of these losses relative to GDP, the CRI provides a comprehensive view of climate risk. It emphasizes the importance of normalization techniques, such as adjusting for population size and economic strength, for generating overall rankings based on scores in four weighted categories: death toll (1/6), deaths per 100,000 inhabitants (1/3), absolute losses in PPP (1/6), and losses per GDP unit (1/3) [17].
The CRI ranks countries based on how they have been affected by storms, floods, and heat waves, offering insights into their exposure and vulnerability. It evaluates absolute and relative impacts to generate an average ranking across four categories: number of deaths, deaths per 100,000 inhabitants, total losses in US dollars (adjusted for purchasing power parity, PPP), and losses as a percentage of GDP. The CRI provides critical data for policymakers and stakeholders to guide climate adaptation and mitigation strategies [17,18].
Countries ranking higher on the CRI typically experience more pronounced health impacts, such as higher mortality rates and disruptions to daily life, particularly straining healthcare systems in less developed countries [17]. Additionally, the CRI serves as a crucial warning system, alerting regions that may experience more frequent or severe extreme weather events due to ongoing climate change. The index highlights vulnerable areas, underlining the urgent need for governments to implement strategies that strengthen infrastructure, healthcare systems, and emergency responses [[18,22].
Figure 2 maps the average ranking of Eastern Mediterranean Region (EMR) countries according to the Climate Risk Index (CRI) over ten years. It shows the yearly ranking of countries in the Environmental and Monetary Risk (EMR) Index and the Climate Risk Index (CRI) over a substantial 20-year period from 1999 to 2019. The rankings demonstrate dramatic changes in some countries in the region from year to year. The long-term data, while revealing significant year-to-year fluctuations in rankings, is crucial for a reliable and accurate vulnerability assessment. It highlights persistent high vulnerability for specific countries, offering essential guidance for developing climate adaptation and risk management strategies [[17,23].
For example, Tunisia shifted from a ranking of 35 in 2018 to 130 in 2019. Afghanistan, for instance, ranked among the top twenty most vulnerable countries for 17 out of 20 years, reaching sixth globally in 2019. Similarly, Pakistan has consistently ranked among the top ten most vulnerable countries globally, reflecting its increased vulnerability to climate change.
Notably, the data challenges common assumptions about vulnerability to climate change and the economic strength of the countries, as seen in the case of Oman. Despite its higher GDP, Oman consistently maintained a vulnerability ranking within the top 20 to 30 throughout the two decades. This unexpected finding reinforces the fact that even economically stronger nations are not exempt from climate risks and underscores the multifaceted nature of vulnerability to climate change [17,18,22].
3.2. The Distinctive Climate Features of the EMR
The Eastern Mediterranean region has a diverse climate, including hot, arid deserts, semi-arid areas, and Mediterranean climates with hot, dry summers and mild, wet winters. Coastal areas experience more moderate temperatures and higher humidity, while inland areas, such as those in the Arabian Peninsula, are subject to extreme heat and minimal rainfall. The region is also prone to occasional droughts and has limited freshwater resources, exacerbating the challenges of water scarcity and significantly influencing agricultural and living conditions. These climatic features contribute to the overall environmental stress impacting public health and the prevalence of diseases, including diarrheal illnesses.
3.2.1. Temperature Patterns and Trends
The EMR temperature anomaly trends follow a natural geographical subregional pattern. The EMR can be divided geographically into five subregions: North Africa (Egypt, Libya, Morocco, and Tunisia), Sham Area (Syria, Lebanon, and oPT), Southern Region (Djibouti, Somalia, Sudan, and Yemen), The Gulf Cooperation Council (GCC) (Bahrain, KSA, Kuwait, Oman, UAE, and Qatar), and the Eastern Sub-Region (Afghanistan, Iran, and Pakistan).
Trends of temperature anomalies in the Eastern Mediterranean Region (EMR) compared to global trends from 1940 to the present are presented in Figure 3. Over the decades, the EMR has experienced more significant fluctuations in temperature anomalies compared to the global average, with particularly deep troughs and sharp peaks. Notably, the EMR's temperature anomalies have occasionally dipped below -2.5°C and surged above 1.5°C, diverging markedly from the more stable global trend. Since the early 2000s, the EMR and the global average have shown an upward trend. However, a notable exponential rise of the regional anomaly during the past two decades, almost 0.4 °C compared with the global one, underscores the EMR's heightened sensitivity to climate variability and its significant deviation from the global temperature behaviour [2]. This emphasizes the urgency for a deep understanding of the climatic drives in the region and the region-specific needs.
The graph of subregional temperature anomalies in the Eastern Mediterranean Region (EMR) from 1940 to the present displays distinct climatic behaviours across its five subregions—North Africa, Sham Area, Southern Region, Gulf Cooperation Council (GCC), and Eastern Sub-Region. North Africa shows stable but changing climate patterns with less fluctuation, while the Sham Area and Southern Region exhibit high variability with sharp temperature peaks, indicating extreme climate events. The GCC demonstrates moderate variability with notable recent peaks, reflecting sensitivity to climatic shifts. The Eastern Sub-Region experiences the most dramatic fluctuations, suggesting significant climatic extremes. Overall, recent years show a trend of rising temperature anomalies across the subregions, underscoring the need for region-specific climate adaptation strategies.
3.2.2. Rainfall and Extreme Weather Events
While temperature monitoring and data are widely available, precipitation data with a period that allows a regional or country analysis are scarce. Published data showed contrasting cumulative regional and sub-regional annual, seasonal, and monthly rainfall trends. The results show a mix of statistically significant negative and positive annual rainfall trends over the EMR The negative trends are primarily found in the northern parts of the Sham sub-region, while the positive trends are mostly located in the Arabian Peninsula sub-region. The trends in the seasonal patterns of early, mid, and late annual rainfall onset and cessation, as well as the duration of the dry and wet seasons, were also calculated [24].
Extreme precipitation events can vary between increases in floods and extended droughts, even within country borders. One of the ways to express the possible impact of a shifting pattern of rainfall can be presented by monitoring the population exposed to flooding and droughts. Recent studies [25] pointed out that much of the region surrounding the Mediterranean Sea showed an expected decrease (down -30% from historical values), yet for the Arabian Peninsula, there is an expected increase in precipitation (up +50% from historical values). The stretch of countries from the Horn of Africa to the United Arab Emirates should expect increased precipitation. Extreme weather events such as flooding, and droughts directly affect many communicable diseases. Many countries in the region have been experiencing a rise in the number of populations affected by these events. As seen in Figure 4, some of the countries in the region, such as Djibouti and Afghanistan, are witnessing an increase in both extremes. Meteorological patterns of increasing temperature and extreme events, such as flooding and droughts, are crucial factors in controlling many communicable disease patterns, particularly those related to vectors and environmental factors.
3.3. Climate-Related Disease Patterns in the EMR
The Eastern Mediterranean region faces various public health challenges, including those related to communicable diseases, with certain diseases being particularly influenced by climate factors such as diarrheal diseases and vector-borne diseases. Here is an overview of the regional profile with emphasis on these issues:
3.3.1. Diarrheal Diseases
Diarrheal diseases are a significant public health concern in the Eastern Mediterranean region, particularly in areas with inadequate sanitation, poor hygiene practices, and limited access to safe drinking water. Climate factors such as increased temperatures and changes in precipitation patterns can explicitly define the risk of disease spread by providing a favourable environment for the survival of the disease vehicle or by affecting water quality and sanitation infrastructure [26]. For instance, high and low-temperature extremes affect illness rates and years of life lost in regions across various income levels, including low-, middle-, and high-income areas [27].
The systematic review and meta-analysis by Liang et al. [28] comprehensively evaluates the relationship between ambient temperature and the risk of infectious diarrhea (ID). The study found that an increase in temperature significantly raises the risk of ID, with a cumulative relative risk (RR) of 1.42 (95% CI: 1.07–1.88) and a single-day RR of 1.08 (95% CI: 1.03–1.14). Subgroup analyses revealed that the risk varies by type of diarrhea, with bacillary dysentery showing a particularly high cumulative RR of 1.85 (95% CI: 1.48–2.30). The study highlights that higher temperatures generally promote bacterial growth and prolong the survival of pathogens, which increases the likelihood of infection.
This phenomenon is especially critical in regions where temperature fluctuations are more extreme, thereby necessitating targeted public health interventions to mitigate the impact of climate change on infectious diarrhea incidence [28]. In a literature review by Zhang et al. [29]. high and low extreme temperatures increase the risk of illnesses such as infectious diarrhea and bacillary dysentery. Contaminated water sources, inadequate sanitation facilities, and improper food handling practices during extreme weather events can contribute to outbreaks of diarrheal diseases such as cholera, typhoid fever, and rotavirus infections. In developing countries, rapid urbanization and insufficient access to safe drinking water further increase the incidence of diarrheal diseases among children [30]. Extreme weather events, like heavy rainfall, often contaminate water sources, thus facilitating the spread of these diseases [31]. Climate change-induced extreme weather also disrupts food production, leading to food insecurity and a higher risk of foodborne illnesses [32,33].
Figure 5 shows some observations on the development of diarrheal disease episodes in the EMR from 2010 to 2021. The general trend in the region shows a decline in diarrheal disease episodes by 24% during this period. However, some countries deviate from this regional trend. Djibouti witnessed a slight increase of about 6% in diarrheal disease episodes. More notably, Oman experienced a significant increase of 26%, and Tunisia saw a 12% rise over the same period.
In contrast, Saudi Arabia maintained a stable trend with zero increase of diarrheal disease the over past ten years. Interestingly, these increases are observed in countries typically classified as high-income with robust water and sanitation infrastructure. Although it is challenging to attribute these changes solely to climate change, dismissing them as a contributing factor is difficult. The varying trends suggest that while public health and water and sanitation interventions might be effective regionally, other factors, including climate change, influence the incidence of diarrheal diseases in specific countries.
When examining trends in cholera outbreaks and deaths in the EMR, it is essential to highlight that the EMR witnessed the largest Cholera outbreak in modern history in Yemen in 2017, where the number of suspected cases surpassed one million, with over 2,000 fatalities reported by the end of 2017 [34]. Cholera is gaining more territory, with some countries witnessing the reemergence of some climate-related diseases after more than two decades of no reported cases, such as the case of cholera outbreaks of 2022 in Syria, which extended to Lebanon [35,36]. The EMR is witnessing cholera outbreaks on a yearly and seasonal basis in many countries in the region, including Somalia, Sudan, Iraq, Pakistan, and Afghanistan [37].
Figure 6 presents the development of case fatality rates of Cholera in Somalia and Afghanistan for the period 2004-2021. The case-fatality rate in Somalia shows a highly volatile trend over the 17 years, with significant peaks, suggesting outbreaks with higher mortality rates. The most notable peaks occurred around 2007, 2010, and 2017, with rates exceeding 2.5%. In contrast, the rate dropped below 1% in 2012 and from 2017 to 2019, indicating better disease control or improved healthcare response during those times.
Afghanistan's trend has been lower than Somalia's throughout the period, yet it still demonstrates fluctuations. The rate in Afghanistan peaked at just above 1.5% around 2009 and showed a smaller peak in 2011, then another much bigger peak around 2017, which rose to 3%. From 2012 to 2016, Afghanistan's rate stayed consistently below 1%, which indicates an improvement in detection, treatment, or overall healthcare provision for cholera.
The rise in diarrheal cases contradicts the evident efforts to improve the WASH (Water, Sanitation, and Hygiene) situation in the EMR, as reported by the Joint Monitoring Program (JMP) by WHO and UNICEF regarding sanitation coverage, as illustrated in Figure 7. This highlights the critical need to consider climate conditions seriously to ensure they do not undermine the overall efforts to enhance WASH services.
3.3.2. Vector-Borne Diseases
In the Eastern Mediterranean Region (EMR), climate indicators such as temperature, rainfall, and humidity are crucial in shaping the current and future transmission patterns of vector-borne diseases, particularly malaria. The relationship between climate and vectors' survival, abundance, and disease transmission capabilities is well-established [38]. Climate change and variability are critical drivers of malaria epidemics, especially in highland areas [39]. When excluding factors like human interventions in anthropogenic control programs, land use, and topography, vectors generally thrive under favourable climate conditions—specifically within optimal ranges of temperature, rainfall, and humidity [26,39,40].
Both malaria and dengue are transmitted by mosquitoes, making vector control essential for managing these diseases. Aedes aegypti is the primary vector for dengue, active during the day [41], while Anopheles mosquitoes, which transmit malaria, are active at dusk and night Despite their behavioural differences, both species thrive in warm, humid environments and breed in stagnant water, commonly found in tropical and subtropical regions [42,43].
Temperature and precipitation, as key climatic factors, drive malaria transmission in the EMR. According to Shapiro et al. [44], temperatures ranging between 21°C and 27°C are ideal for mosquito survival, significantly influencing malaria spread. However, it's not just the average temperature that matters, but also diurnal temperature fluctuations, which play a crucial role in malaria transmission [45]. This relationship is further emphasized when, under stable mean monthly rainfall, an increase in temperature correlates with a higher incidence of malaria. A consistent monthly temperature of 21.5°C, along with other environmental elements like rainfall and humidity, can interact with temperature, impacting the prevalence and spread of the disease. This analysis underscores the complex and crucial role temperature plays in malaria dynamics, especially considering various ecological and meteorological conditions [46].
For example, the fewest detected Malaria cases in the region was recorded in 2009. Despite efforts to control Malaria during the past two decades, this reduction trend was inverted continuously until 2021 (Figure 8). The southern area of Egypt bordering Sudan, where Malaria is endemic, started to experience a notable increasing pattern [47], suggesting the possibility of shifting climatic conditions to become a more suitable environment for the Malaria vector and the re-emergence of the disease. Figure 9 shows the increase in Malaria incidence trend in the northern region of Egypt, El Arish, where the temperature increases to become optimal for vector survival. Similarly, Dengue fever incidence has risen in the EMR in recent years [48]. Climate factors such as temperature and rainfall influence the distribution and abundance of Aedes mosquitoes, leading to the spread of dengue fever in urban and semi-urban areas [49].
Malaria and Dengue vectors share climatic dependencies for breeding and survival. Both mosquitoes thrive in warm, humid environments, where stagnant water facilitates breeding cycles to lay their eggs. Additionally, the spread of both malaria and dengue is profoundly influenced by seasonal changes, with higher transmission rates typically observed during and just after rainy seasons due to the increased availability of breeding sites. Anopheles and Aedes mosquitoes are adapting to urban environments, with Anopheles Stephensi recently invading cities in Africa and the Middle East. This urban adaptation is linked to population movement, unplanned urbanization, and poor water management [50,51].
Crimean-Congo Hemorrhagic Fever (CCHF) is transmitted to humans through Hyalomma tick bites, with the surrounding environment significantly influencing tick growth and survival [52]. Optimal temperatures for tick activity range from 20°C to 40°C, which promote faster development from larvae to adults [53]. Moderate to low humidity supports tick survival, while high moisture levels can negatively affect their life cycle. Low to moderate precipitation is favourable, but excessive rainfall can reduce survival by altering habitats [54]. Vegetation cover and host availability, such as small mammals and livestock, are also crucial for maintaining tick populations [55]. Studies show that humidity and precipitation before disease outbreaks correlate with increased CCHF cases, and temperature fluctuations impact both tick populations and CCHF incidence [56]. These climatic shifts are driving the northward expansion of the CCHF virus, emphasizing the need to monitor climatological factors in endemic regions could help predict and prepare for potential outbreaks including potential patient admissions in healthcare facilities [57].
For Leishmaniasis, the same pattern can be observed. A disease transmitted through the bites of infected sandflies and is endemic in parts of the Eastern Mediterranean region. Typically, the seasonal activity of leishmaniasis vectors in the Mediterranean peaks between July and September, with transmission possible from May to October [58]. Climate change has a profound impact on this disease's distribution and transmission dynamics and imposes significant challenges for leishmaniasis control efforts in affected areas [59]. Rising temperatures are expected to expand the geographical range of the primary vector, Phlebotomus Papatasi, potentially increasing endemic areas. For instance, temperature, humidity, and rainfall variations have been linked to fluctuations in the incidence of cutaneous Leishmaniasis in Iran [60].
The West Nile virus (WNV), transmitted by Culex species mosquitoes, is another critical vector-borne disease in the Eastern Mediterranean region. Climate change is anticipated to expand the geographical range of WNV and lengthen its transmission season. Warmer temperatures and precipitation play a crucial role in the dynamics of WNV's transmission and distribution [61]. Other environmental factors such as vegetation index, anthropized habitats, and bird migration patterns also play a role in the spread of the virus [40,62].
In addition to diarrheal and vector-borne diseases, other communicable diseases such as respiratory infections, hepatitis, and vaccine-preventable diseases remain significant public health concerns in the Eastern Mediterranean region [13]. Climate factors, during extreme weather events, directly and indirectly, exacerbate the spread of various communicable diseases in the region by affecting population displacement, human behaviour, and healthcare infrastructure resilience. Figure 10 shows the number of populations affected by drought and flood in Afghanistan, Pakistan and Somalia during 2004 to 2023. Rising temperatures, extreme weather events, and changing precipitation patterns affect the transmission of vector, water, and food-borne and vaccine-preventable diseases [20,63]. The transmission of human respiratory pathogens is affected by weather, climate, humidity, temperature, and airflow. For instance, the transmission of SARS-CoV-2 is likely influenced by temperature and relative humidity [64]. Hepatitis outbreaks, particularly hepatitis A and E, can be influenced by climate factors affecting water quality and sanitation, such as flooding and drought [65]. Extreme weather events, such as floods and droughts, significantly disrupt healthcare services and vaccination programs, increasing the risk of outbreaks of vaccine-preventable diseases like polio and measles in Pakistan and Afghanistan [66,67]. The climate-induced displacement causes overcrowded temporary shelters. Within these temporary settlements, access to clean water and sanitation is limited, facilitating the spread of communicable diseases. Droughts and other climate-related factors can lead to food insecurity, causing malnutrition. Malnutrition weakens the immune system, making populations more susceptible to infectious diseases [67,68,69].
Based on the evolving meteorological patterns in the region and the associated changes in the incidence of specific communicable diseases, we analysed the climate vulnerability across all countries in the Eastern Mediterranean Region (EMR). This analysis aims to identify which countries need to prioritize addressing the new dynamic patterns of diseases, both in terms of severity and frequency, grounded on climate and epidemiological evidence.
4. Conclusions
The Eastern Mediterranean Region is a climatic and public health crucible, increasingly shaped by the multifaceted impacts of global climate change at a rate surpassing the global average. This study elucidates the direct influence of climatic changes, reshaping the epidemiological landscape with deviations from traditional socio-economic and geographical classifications and particularly influencing the prevalence and distribution of climate-sensitive diseases such as diarrheal diseases, cholera, malaria, and Crimean-Congo Haemorrhagic Fever (CCHF) and Leishmaniosis [1,20,63].
Utilizing the Climate Risk Index (CRI) and the Notre Dame Global Adaptation Initiative (ND-GAIN), our analysis reveals a stark vulnerability among EMR countries to climate-related health risks [17,19,23]. Nations like Afghanistan, Djibouti, Pakistan, Somalia, Sudan, and Yemen exhibit high vulnerability, with significant increases in health sector vulnerability over the past decade. Conversely, countries in the Gulf Cooperation Council (GCC) like Bahrain, Kuwait, Qatar, Saudi Arabia, the UAE, and Tunisia demonstrate lower vulnerability indices, though Oman remains moderately vulnerable.
Our findings show that extreme weather events, such as floods and droughts, have profound implications for the spread of vector-borne and waterborne diseases [70]. For instance, the rising temperatures in southern Egypt and the Gulf Cooperation Council (GCC) countries suggest a more conducive environment for the reemergence of malaria, while the increase in precipitation in parts of the Arabian Peninsula could exacerbate the spread of diseases like dengue and West Nile virus [40,48,71].
This study offers a novel framework for assessing climate-related health vulnerabilities by integrating traditional climate vulnerability indices like the ND-GAIN and Climate Risk Index (CRI) with sector-specific health indicators. While these indices have been widely used independently to assess a country's climate vulnerability and readiness, the novelty of this approach lies in its multifactorial integration. The approach can significantly inform public health strategies and policymaking in the context of climate change. It highlights that the current traditional classification of public health dependency on GDP may no longer be valid, given the increasing frequency and severity of natural disasters and the reemergence of some pathogens in many countries in the region. The juxtaposition of the COVID-19 pandemic alongside climate-induced disease dynamics underscores the indispensable role of resilient health systems capable of proactive adaptation and prevention strategies.
The way forward demands enhanced sub-regional cooperation that transcends political boundaries, fostering a concerted approach to the dual challenges of climate change and public health. Forming strategic alliances, harmonizing knowledge, and coordinating action plans are imperative to mitigate the risks of climate vulnerability and communicable diseases effectively. This collaborative effort will ensure a more resilient and proactive response to the evolving threats in the region. This study advocates for an integrated response that unites environmental and health governance to safeguard the well-being of populations in one of the world's most climatically diverse and dynamically challenged regions. Further investigation through sub-regional climate modelling is needed to explore the intricate linkages between climatic factors and disease patterns, providing a robust foundation for public health resilience in the face of ongoing climatic. Such research is crucial for preparedness and developing effective strategies to address these emerging threats [67,72]. This article calls for urgent action to scale up preparedness measures in the health sector to address both intensifying outbreaks and the reemergence of climate-related diseases and to incorporate climate adaptation strategies.
Author Contributions
O.A.M,: conceptualization, O.A.M.; methodology, O.A.M., S.Mo., S.M.; validation, O.A.M.,S.Mo., ; formal analysis, O.A.M., S.Mo., S.M. ; investigation, O.A.M. and S.Mo.; resources, O.A.M., S.B. A.S.; data curation, O.A.M. and S.M.; writing—original draft preparation, S.Mo., S.M.; writing—review and editing, O.A.M., S.B., and A.S.; visualization, S.M.; supervision, S.Mo.; project administration, S.M.; funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable. This study did not involve humans or animals.
Data Availability Statement
The data supporting the findings of this study are either publicly available or derived from previously published datasets and sources. The Climate Risk Index (CRI) data were obtained from Germanwatch, and the Notre Dame Global Adaptation Initiative (ND-GAIN) data were accessed through the University of Notre Dame's public database. Climatic data were sourced from the NASA GISS Surface Temperature Analysis (GISTEMP) dataset, which provides comprehensive historical and projected climate data for selected EMR countries, enabling the evaluation of climatic trends and variability across the region. Disease-specific data were derived from the World Health Organization's Global Health Observatory and other publicly available reports. No new datasets were created during this study. Detailed references to all data sources are provided in the manuscript.
Acknowledgments
We have not received any funding or external support for this study. We acknowledge Northeastern University for covering the submission fee for this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. No funding was received for this study.
References
- Zittis, G.; Almazroui, M.; Alpert, P.; Ciais, P.; Cramer, W.; Dahdal, Y.; Fnais, M.; Francis, D.; Hadjinicolaou, P.; Howari, F.; Jrrar, A.; Kaskaoutis, D.G.; Kulmala, M.; Lazoglou, G.; Mihalopoulos, N.; Lin, X. Climate change and weather extremes in the Eastern Mediterranean and Middle East. Rev. Geophys. 2022, 60, e2021RG000762. [Google Scholar] [CrossRef]
- Lelieveld, J.; Hadjinicolaou, P.; Kostopoulou, E.; Chenoweth, J.; El Maayar, M.; Giannakopoulos, C.; Hannides, C.; Lange, M.A.; Tanarhte, M.; Tyrlis, E.; Xoplaki, E. Climate change and impacts in the Eastern Mediterranean and the Middle East. Clim. Change 2012, 114, 667–687. [Google Scholar] [CrossRef] [PubMed]
- Lelieveld, J.; Proestos, Y.; Hadjinicolaou, P.; Tanarhte, M.; Tyrlis, E.; Zittis, G. Strongly increasing heat extremes in the Middle East and North Africa (MENA) in the 21st century. Clim. Change 2016, 137, 245–260. [Google Scholar] [CrossRef]
- Lionello, P.; Scarascia, L. The relation between climate change in the Mediterranean region and global warming. Reg. Environ. Change 2018, 18, 1481–1493. [Google Scholar] [CrossRef]
- Zhang, L.; Han, W.; Meehl, G.A.; Hu, A.; Rosenbloom, N.; Shinoda, T.; McPhaden, M.J. Diverse impacts of the Indian Ocean Dipole on El Niño–Southern Oscillation. J. Clim. 2021, 34, 9057–9070. [Google Scholar] [CrossRef]
- Xu, F.; Wang, S.; Li, Y.; Feng, J. Synergistic effects of the winter North Atlantic Oscillation (NAO) and El Niño–Southern Oscillation (ENSO) on dust activities in North China during the following spring. Atmos. Chem. Phys. 2024, 24, 10689–10705. [Google Scholar] [CrossRef]
- Longobardi, A.; Villani, P. Trend analysis of annual and seasonal rainfall time series in the Mediterranean area. Int. J. Climatol. 2010, 30, 1538–1546. [Google Scholar] [CrossRef]
- Zittis, G.; Hadjinicolaou, P.; Klangidou, M. ; Others. A multi-model, multi-scenario, and multi-domain analysis of regional climate projections for the Mediterranean. Reg. Environ. Change 2019, 19, 2621–2635. [Google Scholar] [CrossRef]
- Önol, B.; Semazzi, F.H.M. Regionalization of climate change simulations over the Eastern Mediterranean. J. Clim. 2009, 22, 1942–1961. [Google Scholar] [CrossRef]
- Evans, J.P. 21st century climate change in the Middle East. Clim. Change 2009, 92(3–4), 417–432. [CrossRef]
- Gibelin, A.L.; Déqué, M. Anthropogenic climate change over the Mediterranean region simulated by a global variable resolution model. Clim. Dyn. 2003, 20, 327–339. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC). Climate change 2007: Synthesis report. Contribution of working groups I, II, and III to the fourth assessment report of the Intergovernmental Panel on Climate Change; Core Writing Team, Pachauri, R.K., Reisinger, A., Eds.; IPCC: Geneva, Switzerland, 2007. Available online: https://www.ipcc.ch/site/assets/uploads/2018/02/ar4_syr_full_report.pdf, 20 June 2024. [Google Scholar]
- World Health Organization. Infectious disease outbreaks reported in the Eastern Mediterranean Region in 2021. WHO Regional Office for the Eastern Mediterranean, 21. Available online: https://www.emro.who.int/pandemic-epidemic-diseases/information-resources/infectious-disease-outbreaks-reported-in-the-eastern-mediterranean-region-in-2021.html (accessed on 21 June 2024).
- Federspiel, F.; Ali, M. The cholera outbreak in Yemen: Lessons learned and way forward. BMC Public Health 2018, 18, 1338. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Crimean-Congo hemorrhagic fever - Iraq. WHO Disease Outbreak News, June 1, 2022. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON386, retrieved on 21 June 2024.
- World Health Organization. World Malaria Report 2023. WHO, November 30, 2023. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023, retrieved on 21 June 2024.
- Eckstein, D.; Künzel, V.; Schäfer, L. Global Climate Risk Index 2021: Who Suffers Most from Extreme Weather Events? Weather-Related Loss Events in 2019 and 2000–2019; Germanwatch e.V.: Bonn, Germany, 2021. [Google Scholar]
- Garschagen, M.; Doshi, D.; Reith, J. Global patterns of disaster and climate risk—An analysis of the consistency of leading index-based assessments and their results. Clim. Change 2021, 169, 11. [Google Scholar] [CrossRef]
- Chen, C.; Noble, I.; Hellmann, J.; Coffee, J.; Murillo, M.; Chawla, N.; Moss, R. University of Notre Dame Global Adaptation Index country index technical report; University of Notre Dame: Indiana, USA, 2015. Available online: https://www.researchgate.net/publication/318431802_University_of_Notre_Dame_Global_Adaptation_Index_Country_Index_Technical_Report, 22 June 2024. [Google Scholar]
- NASA Goddard Institute for Space Studies. GISS Surface Temperature Analysis (GISTEMP), Station Data. Available online: https://data.giss.nasa.gov/gistemp/station_data_v4/, retrieved on 10 June 2024.
- Halkos, G.; Skouloudis, A.; Malesios, C.; Jones, N. A hierarchical multilevel approach in assessing factors explaining country-level climate change vulnerability. Sustainability 2020, 12, 4438. [Google Scholar] [CrossRef]
- Germanwatch. Global Climate Risk Index 2021: Who suffers most from extreme weather events? Germanwatch: Bonn, Germany, 2021. Available online: https://www.germanwatch.org/en/19777.
- Eckstein, D.; Künzel, V.; Schäfer, L. Global Climate Risk Index 2019: Who Suffers Most from Extreme Weather Events? Weather-Related Loss Events in 2017 and 1998 to 2017; Germanwatch e.V.: Bonn, Germany, 2019. [Google Scholar]
- Zittis, G. Observed rainfall trends and precipitation uncertainty in the vicinity of the Mediterranean, Middle East, and North Africa. Theor. Appl. Climatol. 2018, 134, 1207–1230. [Google Scholar] [CrossRef]
- Massoud, E.; Massoud, T.; Guan, B.; Sengupta, A.; Espinoza, V.; De Luna, M.; Raymond, C.; Waliser, D. Atmospheric rivers and precipitation in the Middle East and North Africa (MENA). Water 2020, 12, 2863. [Google Scholar] [CrossRef]
- Semenza, J.C.; Rocklöv, J.; Ebi, K.L. Climate change and cascading risks from infectious disease. Infect. Dis. Ther. 2022, 11, 1371–1390. [Google Scholar] [CrossRef]
- Odhiambo Sewe, M.; Bunker, A.; Ingole, V.; Egondi, T.; Oudin Åström, D.; Hondula, D.M.; Rocklöv, J.; Schumann, B. Estimated effect of temperature on years of life lost: A retrospective time-series study of low-, middle-, and high-income regions. Environ. Health Perspect. 2018, 126, 017004. [Google Scholar] [CrossRef]
- Liang, M.; Ding, X.; Wu, Y.; Sun, Y. Temperature and risk of infectious diarrhea: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2021, 28, 68144–68154. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, Y.; Zhang, W.; Wang, B.; Zhao, Z.; Ma, N.; Song, J.; Tian, J.; Cai, J.; Zhang, X. The effect of temperature on infectious diarrhea disease: A systematic review. Heliyon 2024, 10, e31250. [Google Scholar] [CrossRef]
- Birhan, T.A.; Bitew, B.D.; Dagne, H.; Amare, D.E.; Azanaw, J.; Genet, M.; Engdaw, G.T.; Tesfaye, A.H.; Yirdaw, G.; Maru, T. Prevalence of diarrheal disease and associated factors among under-five children in flood-prone settlements of Northwest Ethiopia: A cross-sectional community-based study. Front. Pediatr. 2023, 11, 1056129. [Google Scholar] [CrossRef]
- Cann, K.; Thomas, D.; Salmon, R.L.; Wyn-Jones, A.P.; Kay, D. Extreme water-related weather events and waterborne disease. Epidemiol. Infect. 2012, 141, 671–686. [Google Scholar] [CrossRef] [PubMed]
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability, and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Alpízar, F.; Saborío-Rodríguez, M.; Martínez-Rodríguez, M.R.; Viguera, B.; Harvey, C.A.; Saenz, L. Determinants of food insecurity among smallholder farmer households in Central America: Recurrent versus extreme weather-driven events. Reg. Environ. Change 2020, 20. [Google Scholar] [CrossRef]
- World Health Organization. Suspected cholera cases in Yemen surpass one million, reports UN health agency. UN News, December 22, 2017. Available online: https://news.un.org/en/story/2017/12/639962-suspected-cholera-cases-yemen-surpass-one-million-reports-un-health-agency, retrieved on 30 June 2024.
- Hmaideh, A.; Tarnas, M.C.; Zakaria, W.; Rifai, A.O.; Ibrahem, M.; Hashoom, Y.; Ghazal, N.; Abbara, A. Geographical origin, WASH access, and clinical descriptions for patients admitted to a cholera treatment center in Northwest Syria between October and December 2022. Avicenna J. Med. 2023, 13, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Helou, M.; Khalil, M.; Husni, R. The cholera outbreak in Lebanon: October 2022. Disaster Med. Public Health Prep. 2023, 17, e76. [Google Scholar] [CrossRef]
- Bellizzi, S.; Abdelbaki, W.; Pichierri, G.; Cegolon, L.; Popescu, C. 200 years from the first documented outbreak: Dying of cholera in the Near East during 2022 (recent data analysis). J. Glob. Health 2023, 13, 03004. [Google Scholar] [CrossRef]
- Minakawa, N.; Sonye, G.; Mogi, M.; Githeko, A.; Yan, G. The effects of climatic factors on the distribution and abundance of malaria vectors in Kenya. J. Med. Entomol. 2002, 39, 833–841. [Google Scholar] [CrossRef]
- Githeko, A.K.; Lindsay, S.W.; Confalonieri, U.E.; Patz, J.A. Climate change and vector-borne diseases: A regional analysis. Bull. World Health Organ. 2000, 78, 1136–1147. [Google Scholar] [CrossRef]
- Paz, S.; Semenza, J.C. Environmental drivers of West Nile fever epidemiology in Europe and Western Asia: A review. Int. J. Environ. Res. Public Health 2013, 10, 3543–3562. [Google Scholar] [CrossRef]
- Gubler, D.J. Dengue and dengue hemorrhagic fever. Clin. Microbiol. Rev. 1998, 11, 480–496. [Google Scholar] [CrossRef]
- Getachew, D.; Balkew, M.; Tekie, H. Anopheles larval species composition and characterization of breeding habitats in two localities in the Ghibe River Basin, southwestern Ethiopia. Malar. J. 2020, 19, Article 13. [Google Scholar] [CrossRef]
- Facchinelli, L.; Badolo, A.; McCall, P.J. Biology and behaviour of Aedes aegypti in the human environment: Opportunities for vector control of arbovirus transmission. Viruses 2023, 15, 636. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, L.L.M.; Whitehead, S.A.; Thomas, M.B. Quantifying the effects of temperature on mosquito and parasite traits that determine the transmission potential of human malaria. PLOS Biol. 2018, 16, e2003489. [Google Scholar] [CrossRef] [PubMed]
- Paaijmans, K.P.; Read, A.F.; Thomas, M.B. Understanding the link between malaria risk and climate. Proc. Natl. Acad. Sci. USA 2009, 106, 13844–13849. [Google Scholar] [CrossRef] [PubMed]
- Okuneye, K.; Gumel, A.B. Analysis of a temperature- and rainfall-dependent model for malaria transmission dynamics. Math. Biosci. 2017, 287, 72–92. [Google Scholar] [CrossRef]
- World Health Organization. Control of malaria outbreak due to Plasmodium vivax in Aswan Governorate, Egypt. East. Mediterr. Health J. 2016, 22, 274–279, Available online:https://www.emro.who.int/emhj-volume-22-2016/volume-22-issue-4/control-of-malaria-outbreak-due-to-plasmodium-vivax-in-aswan-governorate-egypt.html, retrieved on 10 July 2024.
- Humphrey, J.M.; Cleton, N.B.; Reusken, C.B.; Glesby, M.J.; Koopmans, M.P.; Abu-Raddad, L.J. Dengue in the Middle East and North Africa: A Systematic Review. PLOS Negl. Trop. Dis. 2016, 10, e0005194. [Google Scholar] [CrossRef]
- Yin, S.; Ren, C.; Shi, Y.; Hua, J.; Yuan, H.Y.; Tian, L.W. A systematic review on modeling methods and influential factors for mapping dengue-related risk in urban settings. Int. J. Environ. Res. Public Health 2022, 19, Article 15265. [Google Scholar] [CrossRef]
- Ahmed, T.; Hyder, M.Z.; Liaqat, I.; Scholz, M. Climatic conditions: Conventional and nanotechnology-based methods for the control of mosquito vectors causing human health issues. Int. J. Environ. Res. Public Health 2019, 16, 3165. [Google Scholar] [CrossRef]
- Phillips, M.A.; Burrows, J.N.; Manyando, C.; Hooft van Huijsduijnen, R.; Van Voorhis, W.C.; Wells, T.N.C. Malaria. Nat. Rev. Dis. Primers 2017, 3, Article 17050. [Google Scholar] [CrossRef]
- Omoga, D.C.A.; Tchouassi, D.P.; Venter, M.; Ogola, E.O.; Osalla, J.; Kopp, A.; Slothouwer, I.; Torto, B.; Junglen, S.; Sang, R. Transmission dynamics of Crimean-Congo hemorrhagic fever virus (CCHFV): Evidence of circulation in humans, livestock, and rodents in diverse ecologies in Kenya. Viruses 2023, 15, 1891. [Google Scholar] [CrossRef] [PubMed]
- Ergönül, Ö. Crimean-Congo haemorrhagic fever. Lancet Infect. Dis. 2006, 6, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Peña, A.; de la Fuente, J. The ecology of ticks and epidemiology of tick-borne viral diseases. Antiviral Res. 2014, 108, 104–128. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.P.; Pigott, D.M.; Golding, N.; Duda, K.A.; Brownstein, J.S.; Weiss, D.J.; Gibson, H.; Robinson, T.P.; Gilbert, M.; Wint, G.R.; Nuttall, P.A.; Gething, P.W.; Myers, M.F.; George, D.B.; Hay, S.I. The global distribution of Crimean-Congo hemorrhagic fever. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 503–513. [Google Scholar] [CrossRef]
- Duygu, F.; Sari, T.; Kaya, T.; Tavsan, O.; Naci, M. The relationship between Crimean-Congo hemorrhagic fever and climate: Does climate affect the number of patients? Acta Clin. Croat. 2018, 57, 443–450. [Google Scholar] [CrossRef]
- Kulichenko, A.N.; Prislegina, D.A. Climatic prerequisites for changing activity in the natural Crimean-Congo hemorrhagic fever focus in the South of the Russian Federation. Russ. J. Infect. Immun. 2019, 9, 162–172. [Google Scholar] [CrossRef]
- Alten, B.; Maia, C.; Afonso, M.O.; Campino, L.; Jiménez, M.; González, E.; Gradoni, L. Seasonal dynamics of Phlebotomine sand fly species proven vectors of Mediterranean leishmaniasis caused by Leishmania infantum. PLOS Negl. Trop. Dis. 2016, 10, e0004458. [Google Scholar] [CrossRef]
- Salomón, O.D.; Quintana, M.G.; Mastrángelo, A.V.; Fernández, M.S. Leishmaniasis and climate change: Case study: Argentina. J. Trop. Med. 2012, 2012, Article 601242. [Google Scholar] [CrossRef]
- Azimi, F.; Shirian, S.; Jangjoo, S.; Ai, A.; Abbasi, T. Impact of climate variability on the occurrence of cutaneous leishmaniasis in Khuzestan Province, southwestern Iran. Geospat. Health 2017, 12, Article 478. [Google Scholar] [CrossRef]
- Paz, S. Effects of climate change on vector-borne diseases: An updated focus on West Nile virus in humans. Emerg. Top. Life Sci. 2019, 3, 143–152. [Google Scholar] [CrossRef]
- Giesen, C.; Herrador, Z.; Fernandez-Martinez, B.; Figuerola, J.; Gangoso, L.; Vazquez, A.; Gómez-Barroso, D. A systematic review of environmental factors related to WNV circulation in European and Mediterranean countries. One Health 2023, 16, 100478. [Google Scholar] [CrossRef] [PubMed]
- Levy, K.; Woster, A.P.; Goldstein, R.S.; Carlton, E.J. Untangling the impacts of climate change on waterborne diseases: A systematic review of relationships between diarrheal diseases and temperature, rainfall, flooding, and drought. Environ. Sci. Technol. 2016, 50, 4905–4922. [Google Scholar] [CrossRef]
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of respiratory viral infections. Annu. Rev. Virol. 2020, 7, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Gullón, P.; Varela, C.; Martínez, E.V.; Gómez-Barroso, D. Association between meteorological factors and hepatitis A in Spain 2010–2014. Environ. Int. 2017, 102, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.; Qazi, J. Measles outbreaks in Pakistan: Causes of the tragedy and future implications. Epidemiol. Rep. 2014, 2, 1. [Google Scholar] [CrossRef]
- McMichael, A.J.; Lindgren, E. Climate change: Present and future risks to health, and necessary responses. J. Intern. Med. 2011, 270, 401–413. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Belesova, K.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Capstick, S.; Chambers, J.; Dalin, C.; Daly, M.; Dasandi, N.; Davies, M.; Drummond, P.; Dubrow, R.; Ebi, K.L.; Eckelman, M.; Ekins, P.; Escobar, L.E.; Fernandez Montoya, L.; Georgeson, L.; Graham, H.; Haggar, P.; Hamilton, I.; Hartinger, S.; Hess, J.; Kelman, I.; Kiesewetter, G.; Kjellstrom, T.; Kniveton, D.; Lemke, B.; Liu, Y.; Lott, M.; Lowe, R.; Sewe, M.O.; Martinez-Urtaza, J.; Maslin, M.; McAllister, L.; McGushin, A.; Jankin Mikhaylov, S.; Milner, J.; Moradi-Lakeh, M.; Morrissey, K.; Murray, K.; Munzert, S.; Nilsson, M.; Neville, T.; Oreszczyn, T.; Owfi, F.; Pearman, O.; Pencheon, D.; Phung, D.; Pye, S.; Quinn, R.; Rabbaniha, M.; Robinson, E.; Rocklöv, J.; Semenza, J.C.; Sherman, J.; Shumake-Guillemot, J.; Tabatabaei, M.; Taylor, J.; Trinanes, J.; Wilkinson, P.; Costello, A.; Gong, P.; Montgomery, H. The 2019 report of The Lancet Countdown on health and climate change: Ensuring that the health of a child born today is not defined by a changing climate. Lancet 2019, 394, 1836–1878. [Google Scholar] [CrossRef]
- Brown, M.E.; Antle, J.M.; Backlund, P.; Carr, E.R.; Easterling, W.E.; Walsh, M.K.; Ammann, C.; Attavanich, W.; Barrett, C.B.; Bellemare, M.F.; Dancheck, V.; Funk, C.; Grace, K.; Ingram, J.S.I.; Jiang, H.; Maletta, H.; Mata, T.; Murray, A.; Ngugi, M.; Ojima, D.; O'Neill, B.; Tebaldi, C.; Ziska, L.H. Climate change, global food security, and the U. S. food system. U.S. Global Change Research Program 2015. [CrossRef]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Paz, S. Climate change impacts on West Nile virus transmission in a global context. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20130561. [Google Scholar] [CrossRef]
- Wu, X.; Lu, Y.; Zhou, S.; Chen, L.; Xu, B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ. Int. 2016, 86, 14–23. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
WHO´s report of infectious diseases outbreak in Eastern Mediterranean Region in 2021[13].
Figure 1.
WHO´s report of infectious diseases outbreak in Eastern Mediterranean Region in 2021[13].
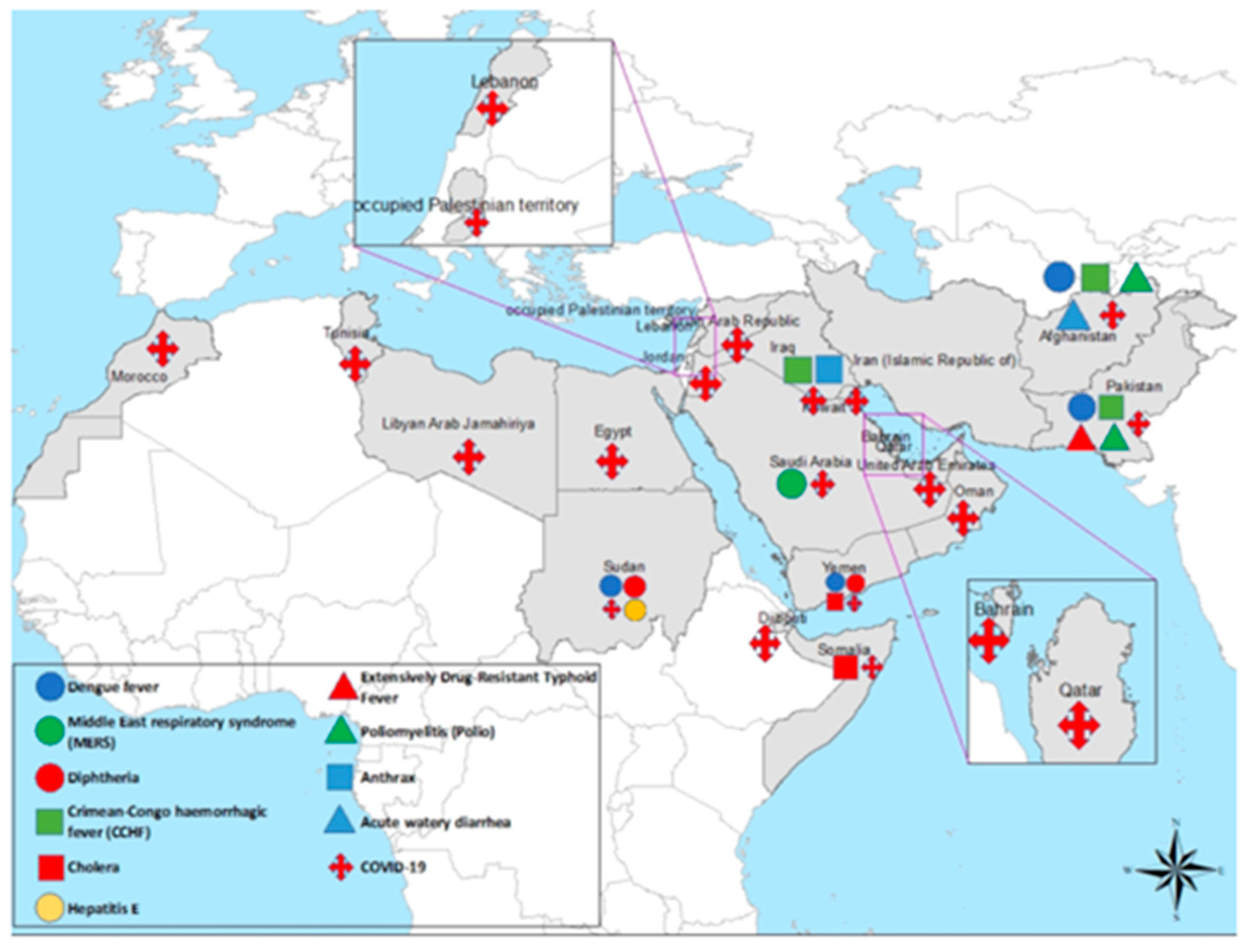
Figure 2.
Twenty years (1999-2019) of CRI score for EMR countries, high score indicated less vulnerability. Source: Germanwatch (2021) [22].
Figure 2.
Twenty years (1999-2019) of CRI score for EMR countries, high score indicated less vulnerability. Source: Germanwatch (2021) [22].
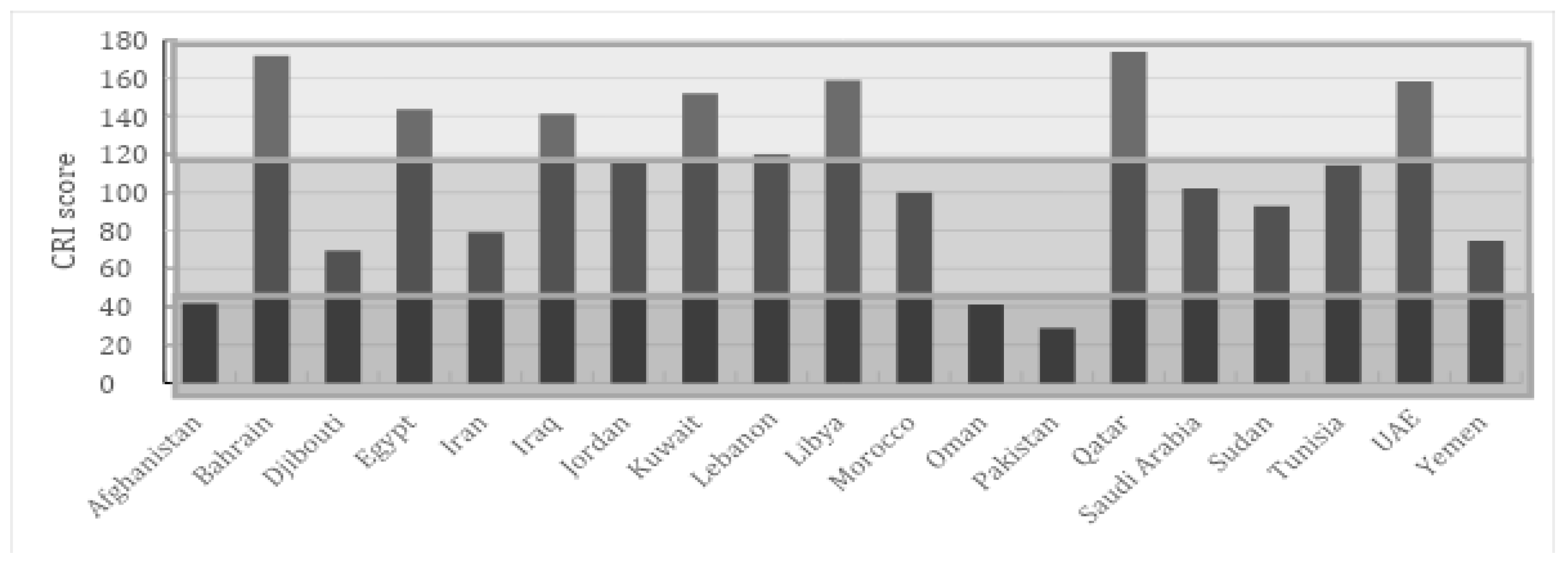
Figure 3.
Development of temperature anomalies against global average for regional and global temperature and sub-regional anomalies for same period. Source: Copernicus Climate Change Service (2023).
Figure 3.
Development of temperature anomalies against global average for regional and global temperature and sub-regional anomalies for same period. Source: Copernicus Climate Change Service (2023).
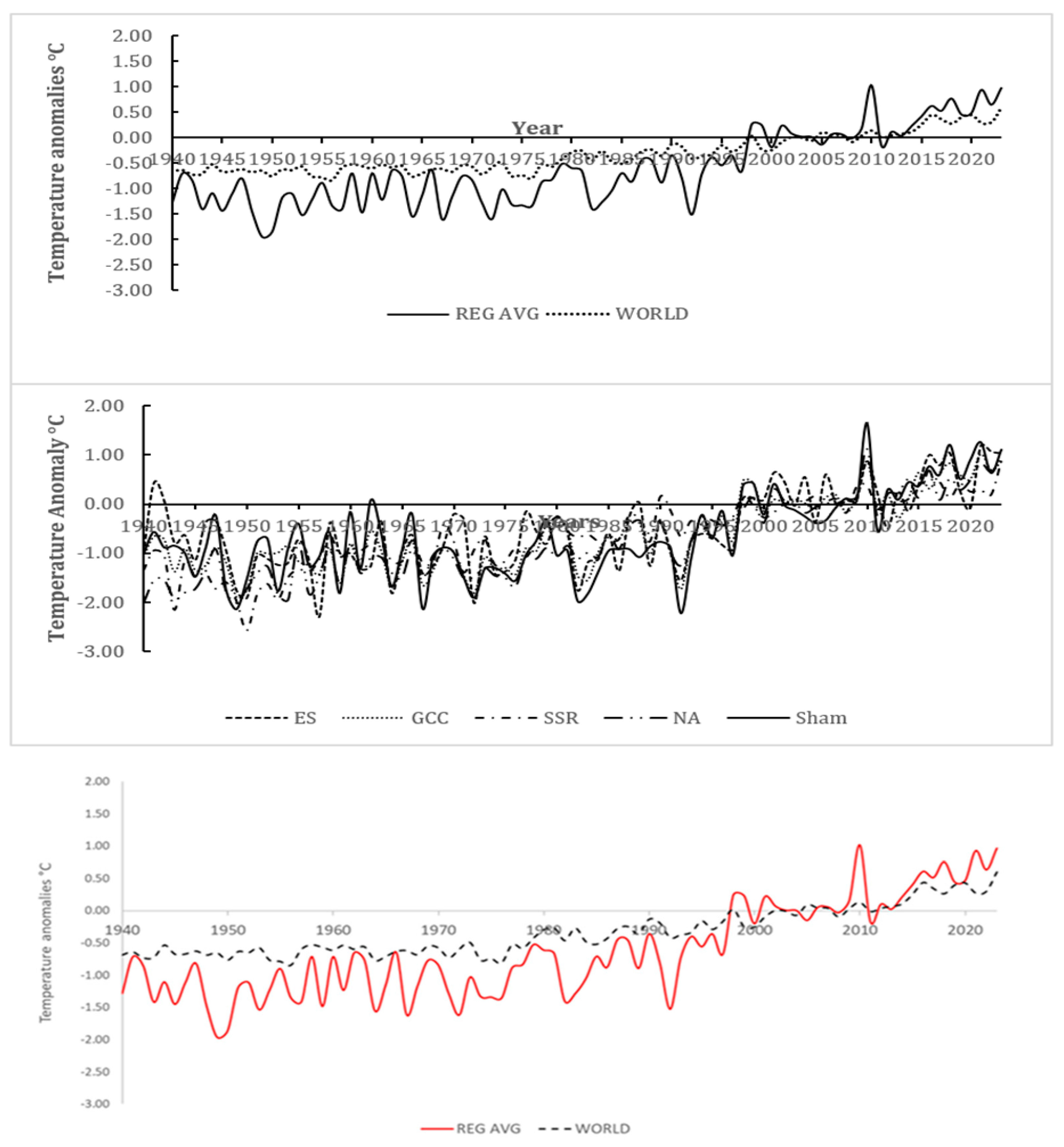
Figure 4.
total population affected by floods (up) and droughts(down) per 100 000 population for some pf the EMR countries during the past 60 years. Source: Global Health Observatory).
Figure 4.
total population affected by floods (up) and droughts(down) per 100 000 population for some pf the EMR countries during the past 60 years. Source: Global Health Observatory).
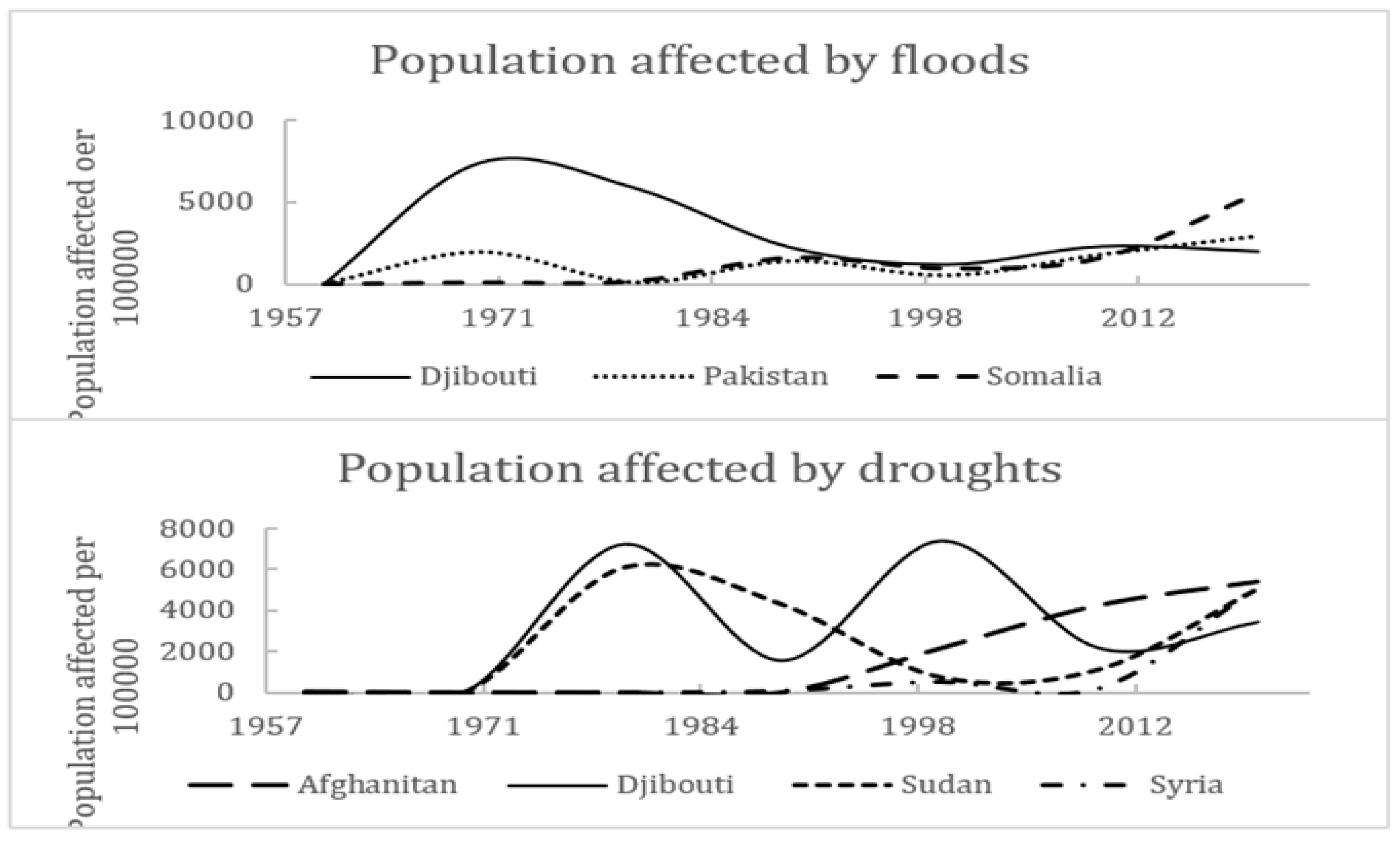
Figure 5.
Diarrheal disease episodes per 100 000 population per year for the EMR and some selected countries in the region Source: IHME, Global Burden of Disease (2024).
Figure 5.
Diarrheal disease episodes per 100 000 population per year for the EMR and some selected countries in the region Source: IHME, Global Burden of Disease (2024).
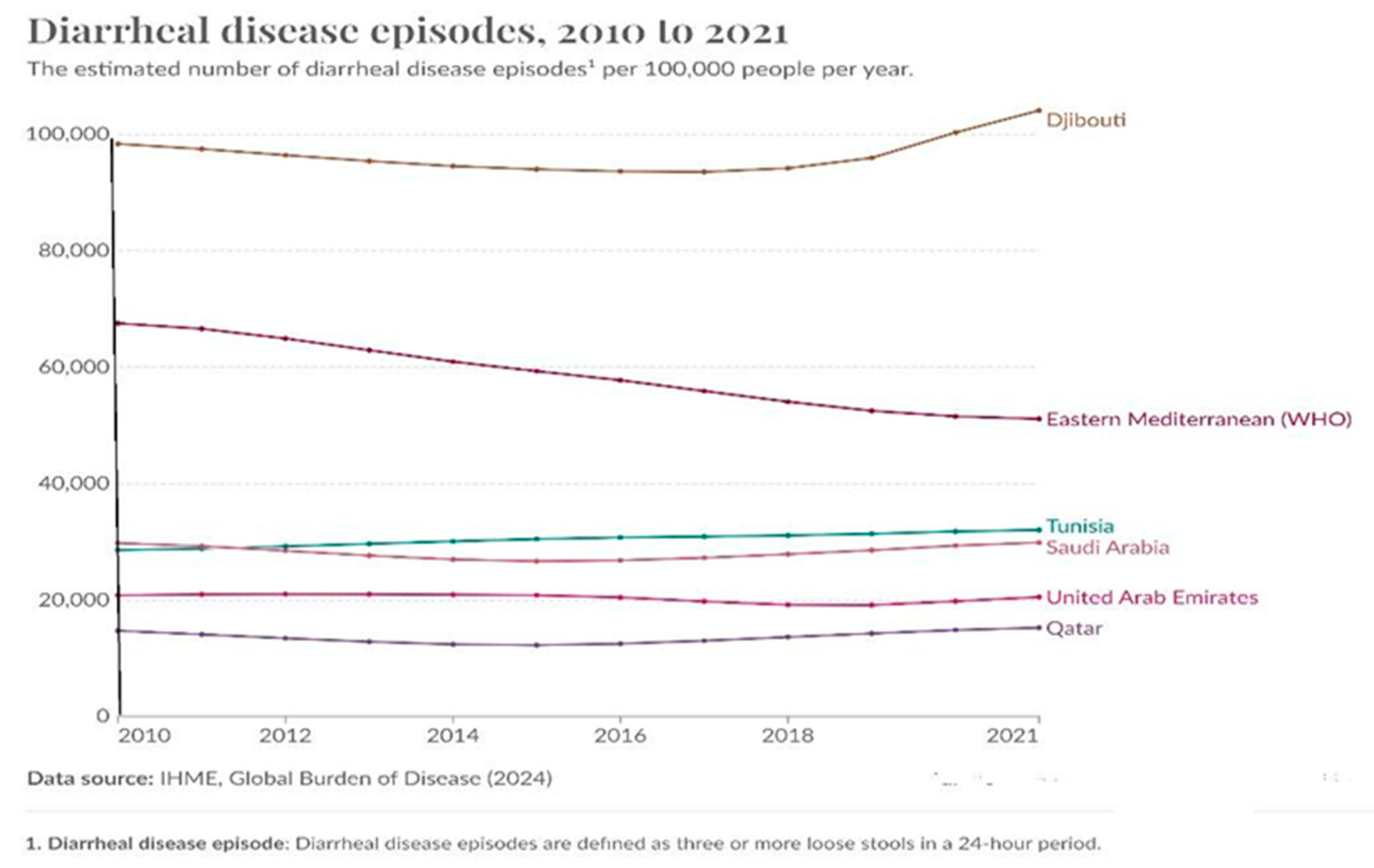
Figure 6.
Cholera case fatality rate, 2004-2021 For Afghanistan and Somalia. Source: Global Health Observatory.
Figure 6.
Cholera case fatality rate, 2004-2021 For Afghanistan and Somalia. Source: Global Health Observatory.
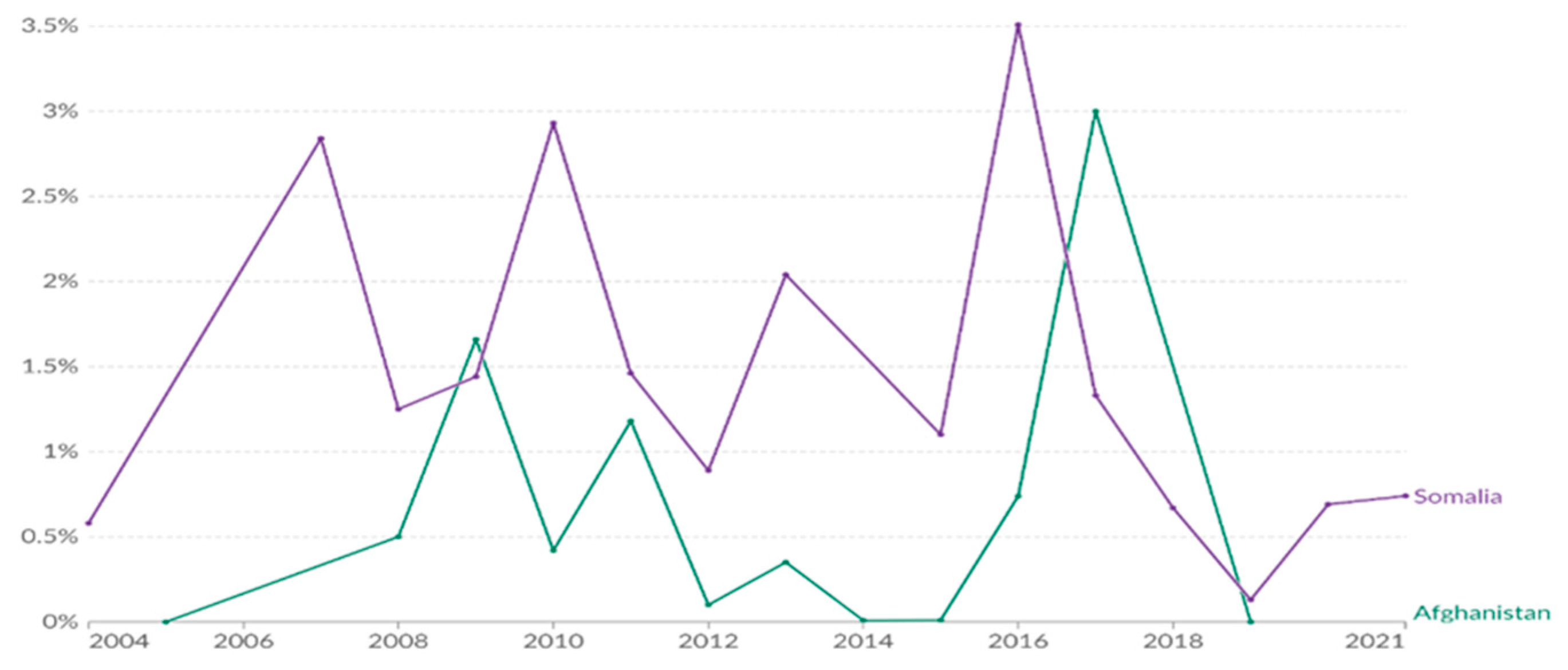
Figure 7.
Development of sanitation coverage in the EMR. Source: JMP.
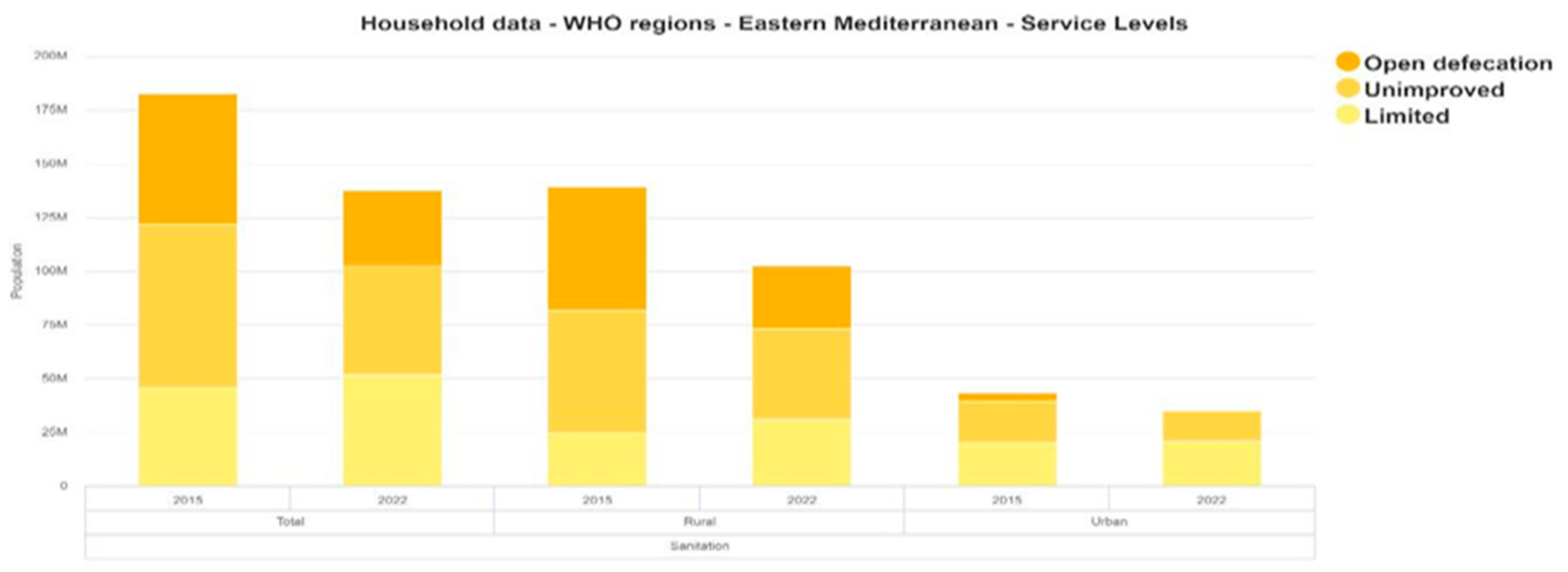
Figure 8.
Estimated total number of Malaria cases reported in the EMR. Source: Global Health Observatory.
Figure 8.
Estimated total number of Malaria cases reported in the EMR. Source: Global Health Observatory.
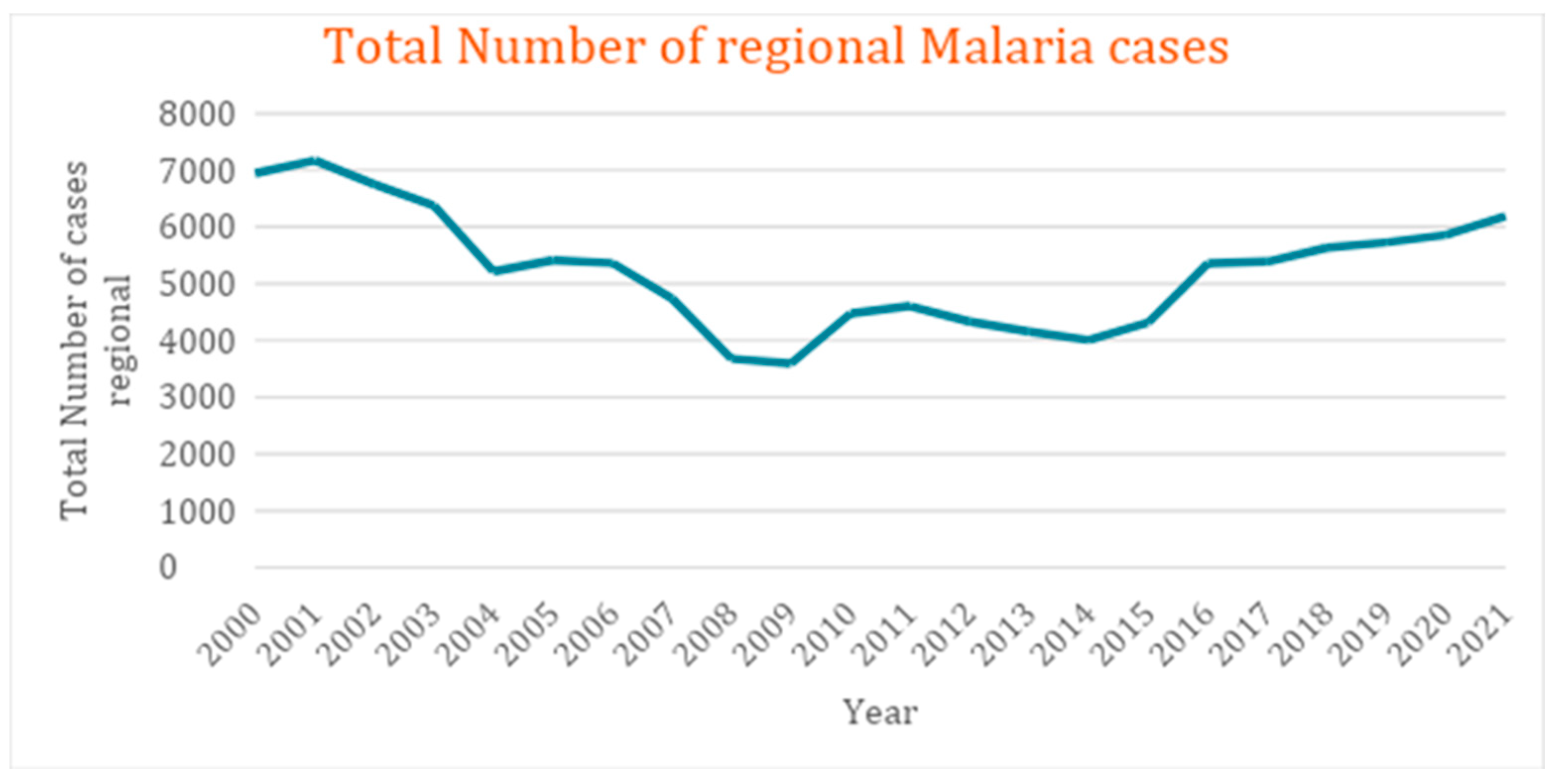
Figure 9.
Estimated total number of Malaria cases reported in the EMR. Source: Global Health Observatory.
Figure 9.
Estimated total number of Malaria cases reported in the EMR. Source: Global Health Observatory.
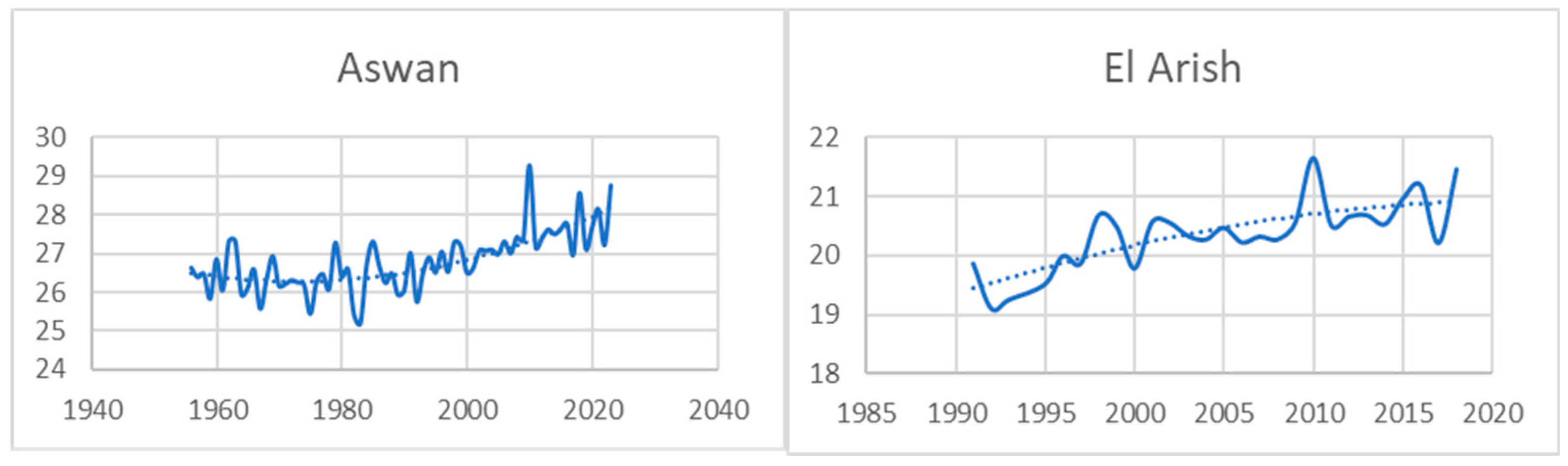
Figure 10.
Populations affected by flood and drought in Afghanistan, Pakistan and Somalia 2004-2023. Source: For drought, data based on EM-DAT, CRED / UCLouvian, Brussels, Belgium – www.emdat.be (D. Guha-Sapir).
Figure 10.
Populations affected by flood and drought in Afghanistan, Pakistan and Somalia 2004-2023. Source: For drought, data based on EM-DAT, CRED / UCLouvian, Brussels, Belgium – www.emdat.be (D. Guha-Sapir).
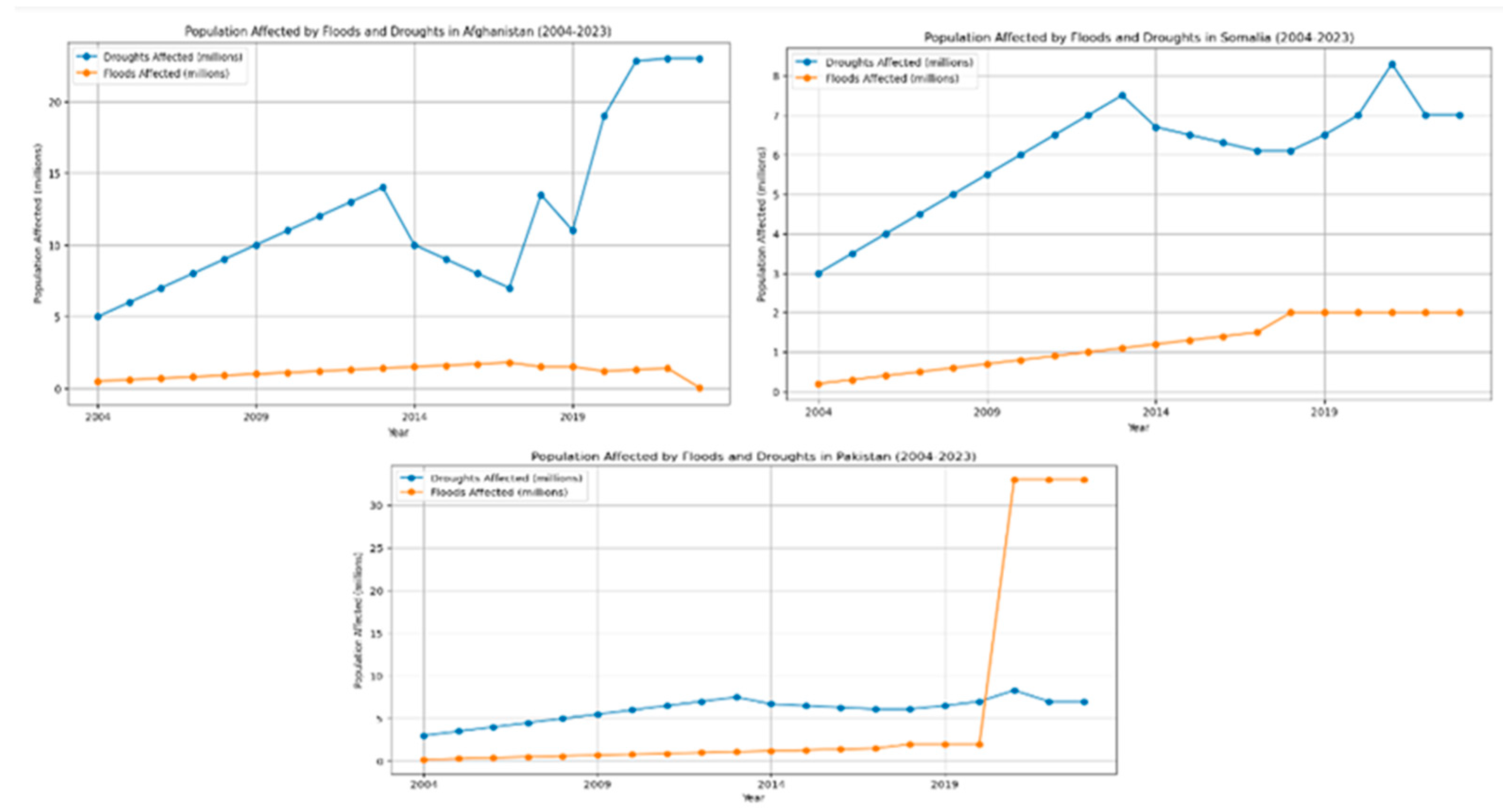

Table 1.
ND-Gain health vulnerability trends for the EMR countries during the past decade. Source: Eckstein et al. (2021) [17].
Table 1.
ND-Gain health vulnerability trends for the EMR countries during the past decade. Source: Eckstein et al. (2021) [17].
| Vulnerability level | Vulnerability trend 10 years | |
| Increase | Decrease | |
| High (0.6-1.0) | Afghanistan, Djibouti, Sudan | Pakistan, Somalia |
| Moderate (0.4-0.6) | Iraq, Morocco, Oman, Syria | Egypt, Iran, Jordan, Lebanon, Libya |
| Low (0.0-0.4) | Bahrain, Kuwait, Qatar, Saudi Arabia, Tunisia, UAE | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



