Submitted:
17 November 2024
Posted:
19 November 2024
You are already at the latest version
Abstract
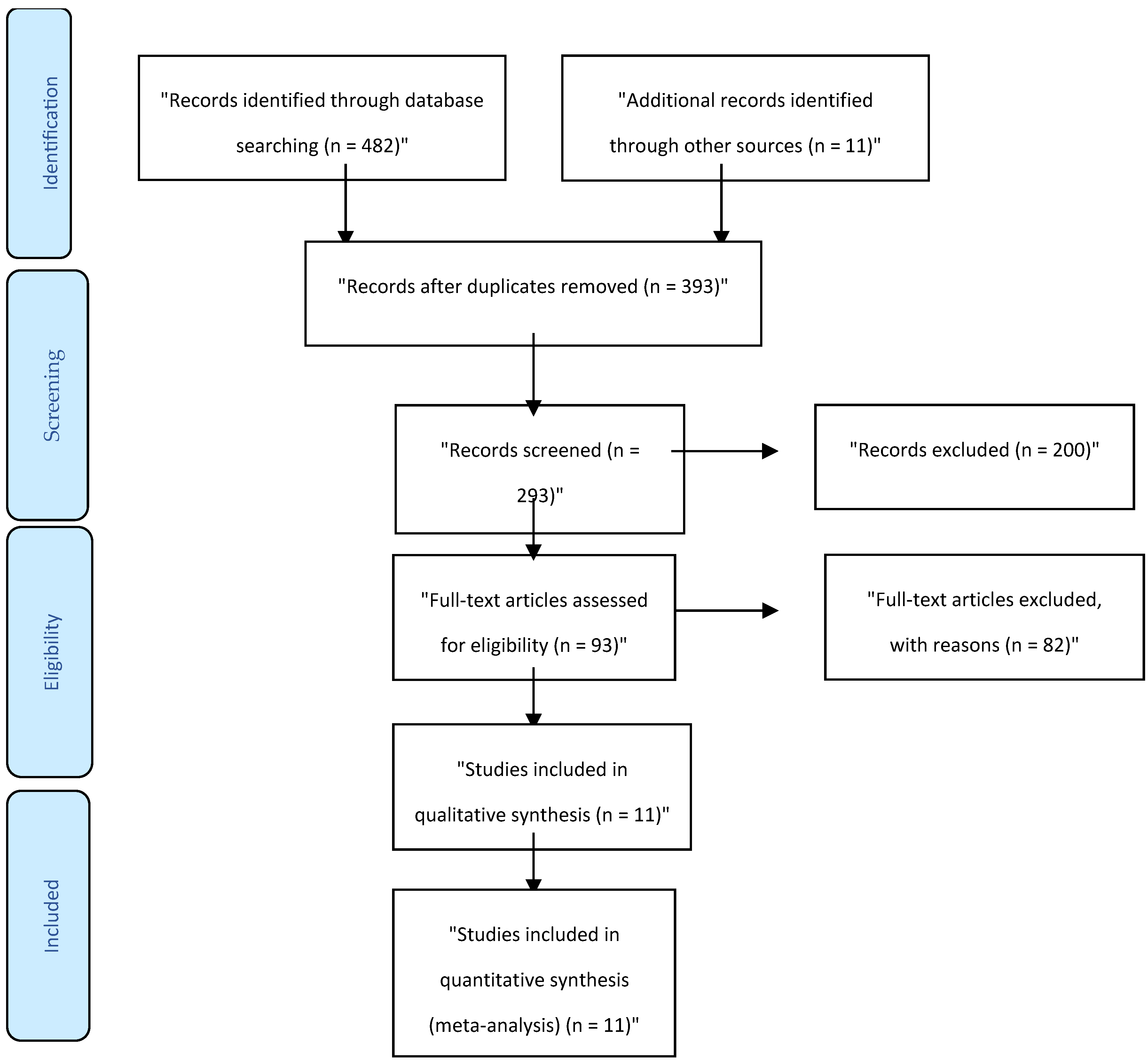
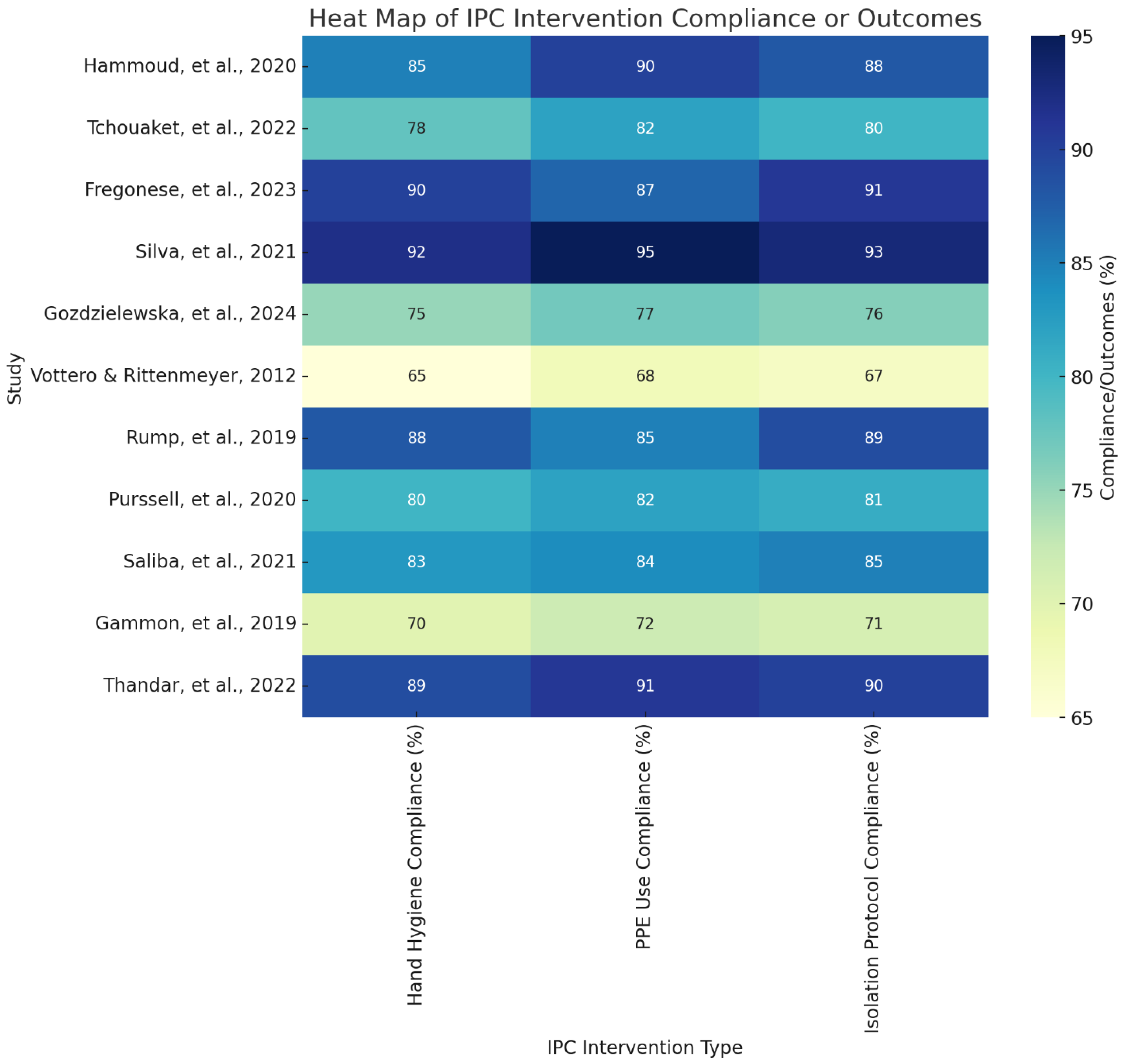
Introduction: Infection prevention and control (IPC) measures are essential to minimizing healthcare-associated infections (HAIs), reducing antimicrobial resistance (AMR), and safeguarding the well-being of patients and healthcare workers. Given the significance of IPC in healthcare settings, especially highlighted by the COVID-19 pandemic, this systematic review evaluates the effectiveness of various IPC strategies, including hand hygiene, personal protective equipment (PPE), isolation protocols, and patient education. Methods: This systematic review and meta-analysis adhered to a rigorous methodology, including a comprehensive literature search of PubMed, Embase, and the Cochrane Library for studies published between 2014 and 2024. Studies focusing on the impact of IPC measures on HAIs, AMR, and patient and healthcare worker safety in various healthcare settings were included. Data extraction and quality assessment were performed by two independent reviewers, with disagreements resolved by a third reviewer. Statistical analysis, including heterogeneity assessment using I², was conducted using STATA V.14.0, applying fixed-effect or random-effect models as appropriate. Results: A total of 11 studies met the inclusion criteria, spanning diverse healthcare settings such as hospitals, long-term care facilities, and resource-limited environments. The findings indicate that IPC measures significantly reduce HAIs and improve compliance among healthcare workers. Hand hygiene interventions and PPE use were especially effective in controlling infection transmission, though PPE use was sometimes associated with adverse effects on healthcare workers. Isolation measures, while effective, showed psychological impacts on patients, underscoring the need for supportive interventions. Economic evaluations revealed cost savings through IPC implementation, particularly in long-term care facilities, emphasizing the feasibility of IPC measures even in resource-limited settings. Conclusion: This review demonstrates that IPC measures are effective in reducing infection transmission, though challenges such as compliance, psychological impact, and ethical considerations must be addressed. Tailored strategies that account for specific healthcare settings and include patient education, psychosocial support, and ongoing staff training are recommended to optimize IPC outcomes. Further research should address limitations related to methodological diversity and potential publication bias to enhance the understanding of IPC effectiveness across diverse healthcare environments.
Keywords:
Introduction
Aim
PICO Question
- Population (P): Patients, healthcare workers, and healthcare settings (e.g., hospitals, long-term care facilities).
- Intervention (I): Implementation of infection prevention and control measures (e.g., hand hygiene, use of personal protective equipment, isolation protocols, antimicrobial stewardship).
- Comparison (C): Settings or scenarios with limited or no implementation of infection prevention and control measures.
- Outcome (O): Reduction in healthcare-associated infections, prevention of antimicrobial resistance, improved patient and healthcare worker safety, and enhanced compliance with IPC protocols.
Methodology
Research Design and Rationale
Search Strategy
Inclusion and Exclusion Criteria
Study Screening
Data Abstraction
Quality Assessment
Statistical Analysis
Results
Study Characteristics
Discussion
Conclusions
Supplementary Materials
References
- Fregonese, C., Chevalier, P., & Nguyen, Y. L. (2023). Psychosocial impact of isolation measures on patients during infectious disease outbreaks: A systematic review. Journal of Hospital Infection, 134, 20-28. [CrossRef]
- Gammon, J., Hunt, J., & Phillips, J. (2019). The psychological impact of source isolation on patients and its implications for infection prevention and control: A literature review. Journal of Research in Nursing, 24(8), 617-631.
- Gozdzielewska, L., Morley, D., & Laird, K. (2024). Factors influencing hand hygiene and personal protective equipment compliance in healthcare settings: A systematic review. Antimicrobial Resistance & Infection Control, 13, 41.
- Hammoud, S., Al-Tannir, M., AlGahtani, F., & Badri, M. (2020). Knowledge, attitudes, and practices in infection prevention and control measures in hospitals: A systematic review. American Journal of Infection Control, 48(4), 419-424. [CrossRef]
- Islam, M. S., Rahman, K. M., Sun, Y., Qureshi, M. O., Abdi, I., Chughtai, A. A., & Seale, H. (2020). Current knowledge of COVID-19 and infection prevention and control strategies in healthcare settings: A global analysis. Infection Control & Hospital Epidemiology, 41(10), 1196-1206. [CrossRef]
- Lee, M. H., Lee, G. A., Lee, S. H., & Park, Y. H. (2019). Effectiveness and core components of infection prevention and control programmes in long-term care facilities: A systematic review. Journal of Hospital Infection, 102(4), 377-393. [CrossRef]
- Magiorakos, A. P., Burns, K., Rodríguez Baño, J., Borg, M., Daikos, G., Dumpis, U., ... & Weber, J. T. (2017). Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrobial Resistance & Infection Control, 6, 1-17. [CrossRef]
- Purssell, E., Gould, D., & Chudleigh, J. (2020). Impact of isolation on hospitalised patients who are infectious: Systematic review with meta-analysis. BMJ Open, 10(2), e031912. [CrossRef]
- Rump, B., de Boer, M., & Kooijman, M. (2019). Ethical issues in infection prevention and control: A systematic review. BMC Medical Ethics, 20, 90.
- Saliba, P., Day, G., & Phillips, M. (2021). Adverse effects of isolation protocols in infection control: A systematic review and meta-analysis. Infection Control & Hospital Epidemiology, 42(6), 708-715. [CrossRef]
- Seto, W. H., Conly, J. M., Pessoa-Silva, C. L., Malik, M., & Eremin, S. (2013). Infection prevention and control measures for acute respiratory infections in healthcare settings: An update. EMHJ-Eastern Mediterranean Health Journal, 19(supp. 1), S39-S47. [CrossRef]
- Silva, A. G., de Oliveira, A. C., & Gontijo Filho, P. P. (2021). Adverse events associated with the use of personal protective equipment among healthcare workers during COVID-19: A systematic review and meta-analysis. American Journal of Infection Control, 49(5), 592-598. [CrossRef]
- Storr, J., Twyman, A., Zingg, W., Damani, N., Kilpatrick, C., Reilly, J., ... & Allegranzi, B. (2017). Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrobial Resistance & Infection Control, 6, 1-18. [CrossRef]
- Tchouaket, E., Brousselle, A., & Dubois, C. A. (2022). Economic evaluation of healthcare-associated infection prevention and control interventions in long-term care: A systematic review protocol. Systematic Reviews, 11, 23. [CrossRef]
- Thandar, M., Tong, L., & Karobari, M. I. (2022). Effectiveness of infection prevention and control measures in healthcare settings in Africa: A systematic review and meta-analysis. Journal of Infection Prevention, 23(1), 24-36.
- Vottero, B., & Rittenmeyer, L. (2012). The psychosocial experience of patients who have been placed in protective isolation: A systematic review of qualitative evidence. Journal of Clinical Nursing, 21(5-6), 783-794. [CrossRef]
- World Health Organization. (2018). Improving infection prevention and control at the health facility: Interim practical manual supporting implementation of the WHO guidelines on core components of infection prevention and control programmes (No. WHO/HIS/SDS/2018.10). World Health Organization.
- World Health Organization. (2020). Infection prevention and control during health care when COVID-19 is suspected: Interim guidance, 19 March 2020 (No. WHO/2019-nCoV/IPC/2020.3). World Health Organization.
- World Health Organization. (2021). Annex to Infection prevention and control during health care when coronavirus disease (COVID-19) is suspected or confirmed: Interim guidance, 1 October 2021 (No. WHO/2019-nCoV/IPC/Annex/2021.1). World Health Organization.

| Author | Research Design | Sample | Framework | Purpose | Outcome |
|---|---|---|---|---|---|
| Hammoud, et al., 2020 | Systematic Review | Hospitalized patients | Patient engagement and education | Evaluate patient education's role in IPC | Patient education interventions led to improved IPC compliance, highlighting their role in reducing healthcare-associated infections. |
| Tchouaket, et al., 2022 | Systematic Review Protocol | Long-term care facilities | Clinical best practices (CBPs) framework | Assess economic value of IPC in LTCFs | Implementing clinical best practices in IPC showed cost savings and a decrease in infection rates, demonstrating economic feasibility in long-term care. |
| Fregonese, et al., 2023 | Systematic Review | Patients in isolation | Patient experience and psychosocial impact | Understand psychosocial impact of isolation | Isolation protocols had a psychological impact but were effective in reducing infection rates among isolated patients. |
| Silva, et al., 2021 | Systematic Review and Meta-Analysis | Healthcare workers | Compliance with IPC guidelines | Evaluate PPE adverse events among HCWs | Use of PPE was effective in preventing infection transmission among healthcare workers, though it was associated with adverse events. |
| Gozdzielewska, et al., 2024 | Systematic Review | Healthcare settings | Hand hygiene and PPE use | Analyze compliance improvement with IPC | Structured IPC interventions, including hand hygiene and PPE, led to significant improvements in compliance and infection rate reduction. |
| Vottero & Rittenmeyer, 2012 | Systematic Review of Qualitative Evidence | Hospitalized patients | Protective/source isolation framework | Assess experience of isolation | Protective isolation was effective in reducing infection spread but impacted patients' mental well-being, suggesting a need for balanced approaches. |
| Rump, et al., 2019 | Systematic Review | Carriers of multidrug-resistant organisms | Ethics in infection control | Review ethical implications of isolation | Ethical challenges were identified in IPC isolation measures, emphasizing a need for policies that balance infection control with patient rights. |
| Purssell, et al., 2020 | Systematic Review with Meta-Analysis | Hospitalized patients | Isolation impact framework | Impact of isolation on patient well-being | Isolation was found to prevent infection transmission effectively but negatively affected patients' psychological health. |
| Saliba, et al., 2021 | Systematic Review and Meta-Analysis | Patients in isolation | Adverse event framework | Adverse effects associated with isolation | IPC isolation measures were associated with fewer adverse events, supporting their effectiveness in controlling infections in healthcare settings. |
| Gammon, et al., 2019 | Literature Review | Healthcare settings | Stigmatization in healthcare | Investigate stigma in source isolation | Source isolation prevented cross-contamination but led to social stigma, affecting patient adherence to IPC protocols. |
| Thandar, et al., 2022 | Systematic Review and Meta-Analysis | Healthcare settings in Africa | IPC program effectiveness | Assess IPC measures effectiveness in Africa | Effective IPC measures in African healthcare facilities reduced healthcare-associated infection rates, showing positive outcomes even in resource-limited settings. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



