
Submitted:
14 November 2024
Posted:
15 November 2024
You are already at the latest version
Abstract
Background: While breastfeeding is highly recommended, breastfed infants may be exposed to drugs by milk due to the mother’s medication, with a risk of adverse drug events (ADE) or reactions (ADRs). The U.S. Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) is an online pharmacovigilance database, while the Drugs and Lactation Database (LactMed®) includes information on the levels of such substances in breast milk and infant blood, and the possible adverse effects in the nursing infants. Methods: The FAERS database was explored (July 29, 2024) on ADEs related to exposure during lactation, while annual trends, outcomes, and region of reporting were determined. Active pharmaceutical ingredients (API) were categorized based on Anatomical Therapeutic Chemical (ATC) classification. The top 5 APIs in each first level of ATC system were explored on ADEs reported and compared to LactMed®. Results: 2628 ADEs were obtained from the FAERS database, with increased reporting over time, while most ADEs were from North America (44.9%). Most drugs (50.9%) were nervous system drugs. The most frequent outcome was "other outcomes" (58.2%). 84,7% of the cases were categorized as serious. Related to the same drug, the FAERS database and LactMed® exhibited similarities and differences in adverse events, possibly due to factors such as maternal and neonatal pharmacokinetics (PKs), maternal therapy and infant exposure durations, milk production, and infant’s daily milk volume intake or causality assessment. Conclusions: ADE reporting systems are useful for obtaining information about medication related ADEs during lactation to increase knowledge on medication safety and awareness for possible risks in infants. The FAERS should be perceived a useful tool to detect ADEs, be it without ADR assessment.
Keywords:
breastfeeding
; adverse event
; safety
; infant
; FAERS
; LactMed®
1. Introduction
Exclusive breastfeeding is advised for the first six months after delivery by the World Health Organization (WHO) and the American Academy of Pediatrics (AAP) [1,2]. It is very well known that breastfeeding provides advantages for both the mother and the breastfed child (Figure 1) [2,3].
Although there are differences in geography and demographics, about 90% of women at present initiate breastfeeding because of improved awareness of the advantages of breastfeeding [2,3]. However, investigations based on population studies showed that over 50% of nursing mothers use prescribed drugs [4]. While mother’s milk obviously provides health benefits to the newborns or infants (Figure 1), it may also expose them to potential risks from drugs that are not meant to treat conditions in the infant, for example when a breastfeeding woman takes a potentially harmful drug, which may appear in clinical significant amounts in breast milk [5].
In general, drugs can transport to breastmilk by passive diffusion from maternal plasma and across the mammary epithelial cell, by carrier-mediated transport from the maternal plasma, lipid co-transport and transcytosis [1]. Drug levels in milk could be explained or estimated by considering several pharmacokinetic and physicochemical characteristics, such as - but not limited to - drug clearance, milk-to-(maternal) plasma concentration (M/P) ratio, or relative infant dose (RID). RIDs are helpful in risk assessment as it shows the amount of drug that a baby consumes through breast milk divided by the mother’s drug dose (corrected for maternal and infant body weight). Further, M/P ratio based on area under the curve (AUC) concentration needs to be evaluated in conjunction with maternal drug clearance value and bioavailability [4].
In clinical practice, the absence of sufficient data on the amount of drug passage to breast milk makes it challenging to determine the advantages and risks of pharmacotherapy in breastfeeding or to support shared decision processes [5]. While the majority of drugs taken by and studied in lactating mothers do not appear to have a clear negative impact on the nursing child, case reports have demonstrated instances of severe and serious infant events during breastfeeding [4,6,7,8].
An efficient pharmacovigilance (PV) system would be an relevant asset to proactively monitor the safe use of drugs to promote public health [9]. The U.S. Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) [10], the European Medicines Agency (EMA) EudraVigilance [11], or the Australian Therapeutic Goods Administration Database of Adverse Event Notifications (DAEN) [12] are online pharmacovigilance databases including information from reports of adverse events. In contrast, the National Library of Medicine (NLM)’s TOXNET system (https://www.nlm.nih.gov/toxnet/index.html) generally presents toxicity and safety profile of chemicals, and evidence on environmental health. The data source LactMed® is part of the TOXNET system. This online source offers up-to-date, evidence-based information about the concentrations of drugs and other chemicals in breast milk and infant blood, possible adverse effects in the breastfed infant, and suggests alternative pharmacotherapeutic options [13].
Obviously, case reports and series about the occurrence of adverse drug events (ADEs, time dependent) or adverse drug reactions (ADRs, causality assessment included) in nursing infants have been published. However, this literature is rather scare, and no clear evidence was available on the level of agreement between spontaneous reports of ADEs/ADRs available in pharmacovigilance databases and the knowledge on infant adverse effects during breastfeeding in reliable and point-of-care resources aimed at healthcare professionals. Therefore, this study aimed to describe the pattern of ADEs reported in the FAERS database, and to compare the number and type of ADE reports in infants related to breastfeeding to the information on side effects in the lactating infant as reported in the LactMed® database.
2. Materials and Methods
2.1. Study design
We performed an observational, cross-sectional, comparative study using the FAERS database. We hereby identified all lactation-related ADE reports entered between 1 January 2001 to 31 March 2024 (latest updated version in FAERS at the time of data extraction, July 29, 2024, and performed by the first author). The information extracted from the FAERS database was subsequently compared to information found in LactMed®. No ethical approval or patient consent was required.
2.2. Data Extraction From the FAERS Database
In the FAERS database, we searched for ADEs reported in neonates or infants associated with lactation-related drug exposure. To do so, we defined the study population, as either neonates (0-1 month), or 1 month-2 years old infants. Second, exposure routes were selected as a) exposure via breast milk, b) breastfeeding, c) intoxication by breastfeeding, or d) maternal exposure during breastfeeding. Reports on fetal exposure data during pregnancy, as well as reports on mother’s milk characteristics such as odor and discoloration were hereby excluded, and duplications were checked. The selected data were extracted from the FAERS Database as a Microsoft Excel File.
2.3. Data Handling, Analysis and Comparison to the LactMed Database
Because of occasionally missing data of the FAERS database, the maximum weight limit was set at 15 kg. Weight information indicated as lb was converted to kg via the “1 lb=0.45 kg” formula [14]. Cases with both missing age and weight information had to be removed.
The reporting trends (annual number), specific infant outcomes (ADE) as mentioned in the ADE reports, and the number of ADEs according to the continents were described using absolute numbers and percentages. The ADE reports were classified using the generic name of the active pharmaceutical ingredient (API) involved, applying the first level of the Anatomical Therapeutic Chemical (ATC) classification system. Based on this list, the reported lactation-related ADEs for the top 5 drugs of the 5 most common ATC classes – so for 25 APIs – were ranked according to the number of reports. Subsequently, these APIs were screened in the LactMed® database and findings on type of events reported in both databases were compared in a qualitative way.
3. Results
3.1. Number of Lactation-Related Adverse Events and Annual Trends
In total, 2675 lactation-related case reports were identified in the FAERS database for infants under the age of 2 years. Since the patients’ age and weight information were not stated in 47 cases (1.7%), these reports were excluded from the analysis. As a result, the final number of reports included in the study was 2628. In the FAERS database, 68.4% of the patients were under 2 months old. The full dataset has been provided in Supplementary Material S1. The reporting trends over the years, between 1 January 2001 and 31 March 2024, is shown in Figure 2. Over the study period, there has been a continuous increase in reports between 2001 and 2019, followed by a somewhat lower (annual number between 2020 and 2023 (for 2024, only data for the first 3 months were available yet).
3.2. ATC Categories and Most Commonly Retrieved Active Pharmaceutical Ingredients
Most of the reported drugs in the lactation-related reports (50.90%) belong to the nervous system (N). Moreover, 19.90% were antineoplastic and immunomodulating agents (L), 7.20% were anti-infectives for systemic use (J), 7.20% related to alimentary tract and metabolism (A), and 3.40% were respiratory system treatments (R). Figure 3 provides an overview of the distribution of the APIs involved in lactation-related reports according to the first ATC level.
The five most commonly reported APIs within each of the five most prevalent ATC classes are presented in Table 1.
3.3. Comparison of the ADEs from the FAERS Database to the LactMed Database
Table 2 provides an overview of the information on adverse infant events in the FAERS and LactMed database. For APIs related to the nervous system, the description of the AEs seem to relate to opioid-receptor activation mechanisms (buprenorphine), but with other clinical description or terminology. In contrast, for the events related to acetaminophen, this rather reflects differences between time-related events, versus causal reactions. For the antineoplastic and immunomodulating agents, the absence of reports for adalimumab, infliximab and tacrolimus in LactMed was observed, while a diverse list of time-related adverse events were retrieved from the FAERS dataset. A similar pattern was observed for the ATC level Alimentary tract and metabolism with no reports in LactMed for insulin, omeprazole, ondansetron, and metformin or ATC level Respiratory system with no reports in LactMed for omalizumab, fluticasone, and budenoside. For the APIs related to the ATC level Antiinfectives for systemic use), a rather diverse and heterogenous pattern was noted, for example with respect to gastro-intestinal side effects reported in both databases.
3.4. Outcome Categories of Lactation-Related ADEs in the FAERS Database
The distribution of the infant outcome categories among the lactation-related ADEs in the FAERS database in provided in Figure 4. While 2264 (84.6%) of them were stated as serious cases, 106 (4.6%) were reported as death cases. The most frequent outcome was stated as “other outcomes” (58.2%). This is followed by “hospitalized” (38.1%) and “non-serious” (15.3%) outcomes.
3.5. Regional Origin of the Lactation-Related Adverse Events Retrieved in the FAERS Database
The distribution of lactation-related adverse event reports by continents is shown in Figure 5. Most reports originated from North America (44.9%), followed by Europe (27.2%) and Asia (8.1%).
4. Discussion
4.1. Main Findings
This study aimed to describe infant adverse events reported as part of lactation-related ADEs in the US FAERS database, and subsequently compare the available information on type and patterns of ADEs in the FAERS database to LactMed®. Overall, 2628 FAERS reports were included in the study.
This study showed that there is a fluctuating but increasing trend in the number of reports over the years, despite a somewhat decrease in the most recent years (Figure 2). Most lactation-related reports in the FAERS database originated from North America (44.9%), followed by Europe (27.2%) and Asia (8.1%). According to population-based data, more than 50% of nursing women take prescribed drugs, suggesting that a substantial proportion of the breastfed newborns may be exposed to drugs in milk [4]. While the majority of drugs taken by nursing mothers do not appear to have a clear negative impact on the child, some case reports have shown severe infant poisoning examples [3,4,16]. Pharmacovigilance must keep up with the constantly changing regulatory environment, reporting, and new treatments and technologies which are being marketed. Constant awareness and continued reporting are necessary to meet these requirements [18]. With our study, we can conclude that there is a fluctuating but generally rising trend over the years which means continued reporting is perceived to be important.
In the FAERS database, 68.4% of the infants with reported ADEs were under 2 months old, 5.5% had life threatening adverse events and 3.6% died, while 84.70% of the cases were categorized as serious in the FAERS. Our findings seem to confirm the relevance of the infant’s age when considering the safety of maternal medication use during breastfeeding. In a study conducted by Anderson et al., infants younger than two months old experienced most of drug-related side effects during breastfeeding [20]. Similarly, in a more recent study of Anderson et al., 63% of the ADRs occurred in the first month, 16% appeared in the second month [21]. In neonates, the most significant aspect is their quickly changing physiology, reflected in poor clearance in the first weeks to months of life [22]. Further, the renal clearance changes rapidly during infancy [23]. Consequently, there are notable variations in the toxicity and efficacy of treatments due to this functional maturity, development and illness conditions of the newborn or infant [22,24].
We also observed that more than half of the reported drugs belong to the nervous system, followed by antineoplastic and immunomodulating agents, anti-infectives for systemic use, alimentary tract and metabolism agents, and respiratory system treatments (Figure 3). In the earlier mentioned study by Anderson et al. , 70% of ADRs during breastfeeding were also caused by central nervous system (CNS) active drugs, such as opioids, antidepressants, anticonvulsants, antipsychotics, lithium, or sedatives. CNS active drugs were followed by iodine (6%), antimicrobials (6%), and yellow fever vaccine (6%) [21]. In essence, our current observations using the FAERS database are in line with these results.
Finally, it was found that the FAERS and LactMed® database have both similarities as well as differences in terms of the nature or type of the adverse drug events or reactions (Table 2). Besides causality assessment related differences, this likely relates to various factors such as maternal and neonatal PKs, the time course of maternal therapy, dosing interval, duration of exposure, milk production, daily milk volume intake. Drug excretion in breast milk depends on different factors such as milk composition, drug properties and transport mechanisms. Drug’s affinity to milk, pH, ionization, molecular weight, protein binding affinity, and lipid solubility affect drug concentration in milk. Most of the drugs are transported into mammary blood capillaries via passive transport, but some of them are transported through different mechanisms like active transport, lipid co-transport and transcytosis [1,5,19]. Due to the significant physiological changes linked to pregnancy such as greater organ blood flow, higher circulating volume, and altered function of some drug-metabolizing enzymes, understanding the PKs of nursing mothers and the rate and amount of distribution of a given drug into their milk has drawn more attention in recent years [4,19]. In addition to PKs, it’s known that alterations in the mother’s pharmaco-genotype can also impact metabolic or elimination pathways and potentially increase the drug exposure of their breastfed infant [5]. Measuring drug concentrations in breast milk to quantify exposure increases the understanding of the likelihood of potential side effects [19]. The FDA has issued guidelines requesting pharmaceutical companies to address potential impacts of maternal drug exposure, drug levels in breast milk, infant feeding, and drug effects on milk production [19,25]. Along the same line, we understood that also the European Medicines Agency is revising their guideline on pregnancy and lactation labelling [26]. In addition to drug concentrations in breast milk, the maternal drug dose, milk-to-(maternal) plasma concentration ratio (M/P ratio), the time course of maternal therapy, dosing interval, duration of exposure, and daily milk volume intake are different factors affecting the likelihood of adverse events in nursing infants [4,5]. Only a small number of studies have evaluated the plasma levels of the newborns, and there is still a lack of information regarding the risk of drug exposure and the transfer of drugs into breastfed infants. In the literature, there are different examples of therapeutic drug monitoring as a successful method to analyze drug exposure in breastfed infants [27,28,29].
Even though the FAERS database presents valuable, real-world data for lactation-related ADEs, there is no assurance that the ADEs were caused by the actual API or substance . The cause of an event could have been another drug, an underlying illness, or just being a time-association event. Consequently, causality evaluation has value to generate more guidance and support sharing decision making. Although the regulatory framework for causality evaluation and reporting in neonates is comparable to other populations, determining causation in neonates is still challenging [30]. Anderson et al. (2016) and Yalcin et al. (2024) have indicated that the causality tool provided by the WHO Uppsala Monitoring Center (WHO-UMC) and Naranjo algorithm were insufficient in their performance to document neonatal causality in a reliable and sufficient manner [21,30]. Leopoldino et al. (2023) expressed that the Du algorithm (modified Naranjo algorithm for neonates by Du et al. (2013) [31]) demonstrates good sensitivity for identifying ADRs as definite, proving to be a more appropriate tool for neonatal clinical routine [32].
Related to assessment of other aspects such as seriousness and severity, ADEs are categorized according to their seriousness as “serious” or “non-serious”, based on the FDA guidance. Related to severity, the Neonatal Adverse Event Severity Score (NAESS) was developed and validated for the severity assessment [30,33,34]. Even though it’s a time-consuming procedure, severity assessment might be useful in enlightening the impact of ADRs.
4.2. Strengths and Limitations
Some strenghts can be considered. First, we used the online, freely available FAERS database offering a large number of real-world data that can be used to examine the occurence and possible relationships between drug exposure during lactation and drug related ADEs in infants. Compared to smaller, single-center research databases or registries, the FAERS database contains (many more) data available from a worldwide population. Second, to compare the FAERS ADEs data with, we chose for Lactmed, a renowned, freely available and international reference on drug safety during lactation.
However, some limitations should also be considered. First, raw data were extracted from the FAERS database which consists of reports of human adverse events submitted by the pharmaceutical industry, healthcare professionals, and consumers. These reports are made publicly available by the FAERS Public Dashboard, through an online platform. Even though it is easily accessible to everyone, the system only contains spontaneous, potentially incomplete, and duplicate reports. These reports include the reporter’s observations and opinions but the content has not been externally confirmed. In addition, there is no guarantee that the adverse event reported was actually due to the suspected substance, as a formal causality assessment is lacking (ADE versus ADR). Therefore, the FAERS database should rather be perceived as an exploratory, signal detection tool to identify ADEs or potential ADRs, at the cost of specificity [10]. So, this study does not provide evidence on causal relationships between drug exposure during lactation and adverse events in nursing infants.
4.3. New Methods for Future Strategies
Different in vitro and in vivo animal studies have been developed for determining the drug concentrations in breast milk [35]. While reports of similar hormonal regulation of milk production have been made for several species, high-quality data describing species differences are still not sufficiently reported. Even though animal data could provide information in some manner, the Pregnancy and Lactation Labeling Rule (PLLR) established by the FDA suggests that if human data are available animal data should not be used [5]. In recent years, in silico methods have gained importance for determining the drug concentrations in breast milk. Physiologically based pharmacokinetic (PBPK) modeling, and population pharmacokinetic (popPK) modeling are useful methods for screening and determining the drug concentrations in breast milk and for estimating infant risk through breastfeeding [36,37]. Also, methods for estimating the M/P ratio that rely on the quantitative structure–activity relationship (QSAR) show promise [5,38]. But at the very least, validation of the results is important [5,29]. In addition to these methods, machine learning models are also used for predicting xenobiotics’ transfer from maternal plasma to human milk. Even though the results are encouraging, more research is required to increase and confirm these regression models’ accuracy [39].
5. Conclusions
In total, 2628 ADEs were obtained from the FAERS database, with increased reporting over time. In the FAERS database, 68.4% of the patients were under 2 months old, 5.5% had life threatening ADEs and 3.6% died, while 84,70% of the cases were categorized as serious. By comparing the FAERS pharmacovigilance database with the LactMed® resource, we found both differences as well as similarities in type of events. Adverse event reporting databases are useful for gathering exploratory information about ADEs during breastfeeding and identifying specific drugs which should be further assessed on their safety during breastfeeding, while pharmacovigilance databases may benefit from severity and causality assessments to ascertain the relationship and relevance between drug exposure and outcomes. Hence, the FAERS database should be perceived a useful tool to detect ADEs, be it without ADR assessment.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, H.T.Y, N.Y. and K.A; methodology, H.T.Y, N.Y. and K.A; software, H.T.Y; formal analysis, H.T.Y, N.Y.; investigation, H.T.Y.; resources, H.T.Y, N.Y.; data curation, H.T.Y; writing—original draft preparation, H.T.Y, N.Y.; writing—review and editing, M.C., K.A.; visualization, H.T.Y; supervision, K.A.; project administration, K.A.
Funding
We would like to thank the Scientific and Technological Research Council of Turkey (TÜBİTAK) for contributing to N.Y., to obtain a postdoc scholarship to research at KU Leuven and thus to collaborate with co-authors (ref no: 53325897-115.02-476393) and to Hacettepe University European Union Office for contributing to H.T.Y for Erasmus + Program Key Action 1: Learning Mobility of Individuals Scholarship and to collaborate with co-authors (ref no: 7167784/VKB-32) at KU Leuven. M.C. is supported by a Senior Postdoctoral Fellowship fundamental research from the Research Foundation Flanders (FWO; 1246425N).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The FAERS is an open data source, and we have provided all individual hits and results as an excel file in the supplement.
Acknowledgments
Figure 1 was created using BioRender.com.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gong, C.; Bertagnolli, L.N.; Boulton, D.W.; Coppola, P. A literature review of drug transport mechanisms during lactation. CPT Pharmacometrics Syst Pharmacol 2024. [Google Scholar] [CrossRef] [PubMed]
- Meek, J.Y.; Noble, L.; Section on, B. Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics 2022, 150. [Google Scholar] [CrossRef] [PubMed]
- Masi, A.C.; Stewart, C.J. Role of breastfeeding in disease prevention. Microb Biotechnol 2024, 17, e14520. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, R.H.J.; Anderson, P.O.; Ito, S. Infant drug exposure via breast milk. Br J Clin Pharmacol 2022, 88, 4311–4327. [Google Scholar] [CrossRef]
- Wang, J.; Johnson, T.; Sahin, L.; Tassinari, M.S.; Anderson, P.O.; Baker, T.E.; Bucci-Rechtweg, C.; Burckart, G.J.; Chambers, C.D.; Hale, T.W.; et al. Evaluation of the Safety of Drugs and Biological Products Used During Lactation: Workshop Summary. Clin Pharmacol Ther 2017, 101, 736–744. [Google Scholar] [CrossRef]
- Wong, J.; Saver, B.; Scanlan, J.M.; Gianutsos, L.P.; Bhakta, Y.; Walsh, J.; Plawman, A.; Sapienza, D.; Rudolf, V. Does Maternal Buprenorphine Dose Affect Severity or Incidence of Neonatal Abstinence Syndrome? J Addict Med 2018, 12, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Greenup, A.J.; Tan, P.K.; Nguyen, V.; Glass, A.; Davison, S.; Chatterjee, U.; Holdaway, S.; Samarasinghe, D.; Jackson, K.; Locarnini, S.A.; et al. Efficacy and safety of tenofovir disoproxil fumarate in pregnancy to prevent perinatal transmission of hepatitis B virus. J Hepatol 2014, 61, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, S.; Audousset, C.; Bourdon, G.; Garabedian, C.; Gautier, S. Elexacaftor/tezacaftor/ivacaftor induced liver enzymes abnormalities in breastfed infants: A series of 3 cases. Therapie 2024. [Google Scholar] [CrossRef] [PubMed]
- Kalaiselvan, V.; Kumar, P.; Mishra, P.; Singh, G.N. System of adverse drug reactions reporting: What, where, how, and whom to report? Indian J Crit Care Med 2015, 19, 564–566. [Google Scholar] [CrossRef]
- Administration, U.S.F.a.D. FDA Adverse Event Reporting System (FAERS) Public Dashboard. 2024, 2024.
- Agency, E.M. EudraVigilance. 2024.
- Care, A.G.D.o.H.a.A. Database of Adverse Event Notifications (DAEN) - medicines. 2024.
- Development, B.M.N.I.o.C.H.a.H. Drugs and Lactation Database (LactMed®) [Internet]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK501922/ (accessed on 23 September 2024).
- Ojo A, P.P., Boehning AP. Conversion Weights. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557608/ (accessed on 29 September 2024).
- UNICEF, W. Global Breastfeeding Scorecard 2023. Available online: https://www.unicef.org/documents/global-breastfeeding-scorecard-2023#:~:text=For%202023%20the%20scorecard%20demonstrates,target%20of%2050%25%20by%202025 (accessed on 15 September 2024).
- Hotham, N.; Hotham, E. Drugs in breastfeeding. Aust Prescr 2015, 38, 156–159. [Google Scholar] [CrossRef]
- Hamid, A.A.A.; Rahim, R.; Teo, S.P. Pharmacovigilance and Its Importance for Primary Health Care Professionals. Korean J Fam Med 2022, 43, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Kugener, V.F.; Freedland, E.S.; Maynard, K.I.; Aimer, O.; Webster, P.S.; Salas, M.; Gossell-Williams, M. Enhancing Pharmacovigilance from the US Experience: Current Practices and Future Opportunities. Drug Saf 2021, 44, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Abduljalil, K.; Pansari, A.; Ning, J.; Jamei, M. Prediction of drug concentrations in milk during breastfeeding, integrating predictive algorithms within a physiologically-based pharmacokinetic model. CPT Pharmacometrics Syst Pharmacol 2021, 10, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.O.; Pochop, S.L.; Manoguerra, A.S. Adverse drug reactions in breastfed infants: less than imagined. Clin Pediatr (Phila) 2003, 42, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.O.; Manoguerra, A.S.; Valdes, V. A Review of Adverse Reactions in Infants From Medications in Breastmilk. Clin Pediatr (Phila) 2016, 55, 236–244. [Google Scholar] [CrossRef]
- Allegaert, K.; van den Anker, J.N. Adverse drug reactions in neonates and infants: a population-tailored approach is needed. Br J Clin Pharmacol 2015, 80, 788–795. [Google Scholar] [CrossRef]
- Toro-Ramos, T.; Paley, C.; Pi-Sunyer, F.X.; Gallagher, D. Body composition during fetal development and infancy through the age of 5 years. Eur J Clin Nutr 2015, 69, 1279–1289. [Google Scholar] [CrossRef]
- Ruggiero, A.; Ariano, A.; Triarico, S.; Capozza, M.A.; Ferrara, P.; Attina, G. Neonatal pharmacology and clinical implications. Drugs Context 2019, 8, 212608. [Google Scholar] [CrossRef]
- Food; Drug Administration, H.H.S. Content and format of labeling for human prescription drug and biological products; requirements for pregnancy and lactation labeling. Final rule. Fed Regist 2014, 79, 72063–72103.
- The European Medicines Agency. Guideline on good pharmacovigilance practices (GVP) Product- or Population-Specific Considerations III: Pregnant and breastfeeding women. Available online: https://www.ema.europa.eu/en/human-regulatory-overview/post-authorisation/pharmacovigilance-post-authorisation/good-pharmacovigilance-practices-gvp (accessed on 28 September 2024).
- Barrau, M.; Roblin, X.; Andromaque, L.; Rozieres, A.; Faure, M.; Paul, S.; Nancey, S. What Should We Know about Drug Levels and Therapeutic Drug Monitoring during Pregnancy and Breastfeeding in Inflammatory Bowel Disease under Biologic Therapy? J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Franssen, E.J.; Meijs, V.; Ettaher, F.; Valerio, P.G.; Keessen, M.; Lameijer, W. Citalopram serum and milk levels in mother and infant during lactation. Ther Drug Monit 2006, 28, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Paulzen, M.; Schoretsanitis, G. [Psychopharmacotherapy during pregnancy and breastfeeding-Part II: focus on breastfeeding : Support options by using therapeutic drug monitoring]. Nervenarzt 2023, 94, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, N.; van den Anker, J.; Samiee-Zafarghandy, S.; Allegaert, K. Drug related adverse event assessment in neonates in clinical trials and clinical care. Expert Rev Clin Pharmacol 2024, 17, 803–816. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Lehr, V.T.; Lieh-Lai, M.; Koo, W.; Ward, R.M.; Rieder, M.J.; Van Den Anker, J.N.; Reeves, J.H.; Mathew, M.; Lulic-Botica, M.; et al. An algorithm to detect adverse drug reactions in the neonatal intensive care unit. J Clin Pharmacol 2013, 53, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Leopoldino, R.W.D.; de Oliveira, L.V.S.; Fernandes, F.E.M.; de Lima Costa, H.T.M.; Vale, L.M.P.; Oliveira, A.G.; Martins, R.R. Causality assessment of adverse drug reactions in neonates: a comparative study between Naranjo’s algorithm and Du’s tool. Int J Clin Pharm 2023, 45, 1007–1013. [Google Scholar] [CrossRef]
- Garg, B.; Sharma, D.; Farahbakhsh, N. Assessment of sickness severity of illness in neonates: review of various neonatal illness scoring systems. J Matern Fetal Neonatal Med 2018, 31, 1373–1380. [Google Scholar] [CrossRef]
- Yalcin, N.; Kasikci, M.; Celik, H.T.; Allegaert, K.; Demirkan, K.; Yigit, S.; Yurdakok, M. An Artificial Intelligence Approach to Support Detection of Neonatal Adverse Drug Reactions Based on Severity and Probability Scores: A New Risk Score as Web-Tool. Children (Basel) 2022, 9, 1826. [Google Scholar] [CrossRef]
- Nauwelaerts, N.; Macente, J.; Deferm, N.; Bonan, R.H.; Huang, M.C.; Van Neste, M.; Bibi, D.; Badee, J.; Martins, F.S.; Smits, A.; Allegaert, K.; Bouillon, T.; Annaert, P. Generic workflow to predict medicine concentrations in human milk using physiologically-based pharmacokinetic (PBPK) modelling-A contribution from the ConcePTION project. Pharmaceutics 2023, 15, 1469. [Google Scholar] [CrossRef]
- Wood, N.D.; Smith, D.; Kinrade, S.A.; Sullivan, M.T.; Rayner, C.R.; Wesche, D.; Patel, K.; Rowland-Yeo, K. The use of quantitative clinical pharmacology approaches to support moxidectin dosing recommendations in lactation. PLoS Negl Trop Dis 2024, 18, e0012351. [Google Scholar] [CrossRef]
- Nauwelaerts, N.; Macente, J.; Deferm, N.; Bonan, R.H.; Huang, M.C.; Van Neste, M.; Bibi, D.; Badee, J.; Martins, F.S.; Smits, A.; et al. Generic Workflow to Predict Medicine Concentrations in Human Milk Using Physiologically-Based Pharmacokinetic (PBPK) Modelling-A Contribution from the ConcePTION Project. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef]
- Katritzky, A.R.; Dobchev, D.A.; Hur, E.; Fara, D.C.; Karelson, M. QSAR treatment of drugs transfer into human breast milk. Bioorg Med Chem 2005, 13, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, S.; Lakshminarayanan, A.; Bhargava, N.; Ravichandran, J.; Vivek-Ananth, R.P.; Samal, A. Machine Learning Models for Prediction of Xenobiotic Chemicals with High Propensity to Transfer into Human Milk. ACS Omega 2024, 9, 13006–13016. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Trend in the number of lactation-related adverse events in the FAERS database (1 January 2001- 31 March 2024).
Figure 2.
Trend in the number of lactation-related adverse events in the FAERS database (1 January 2001- 31 March 2024).
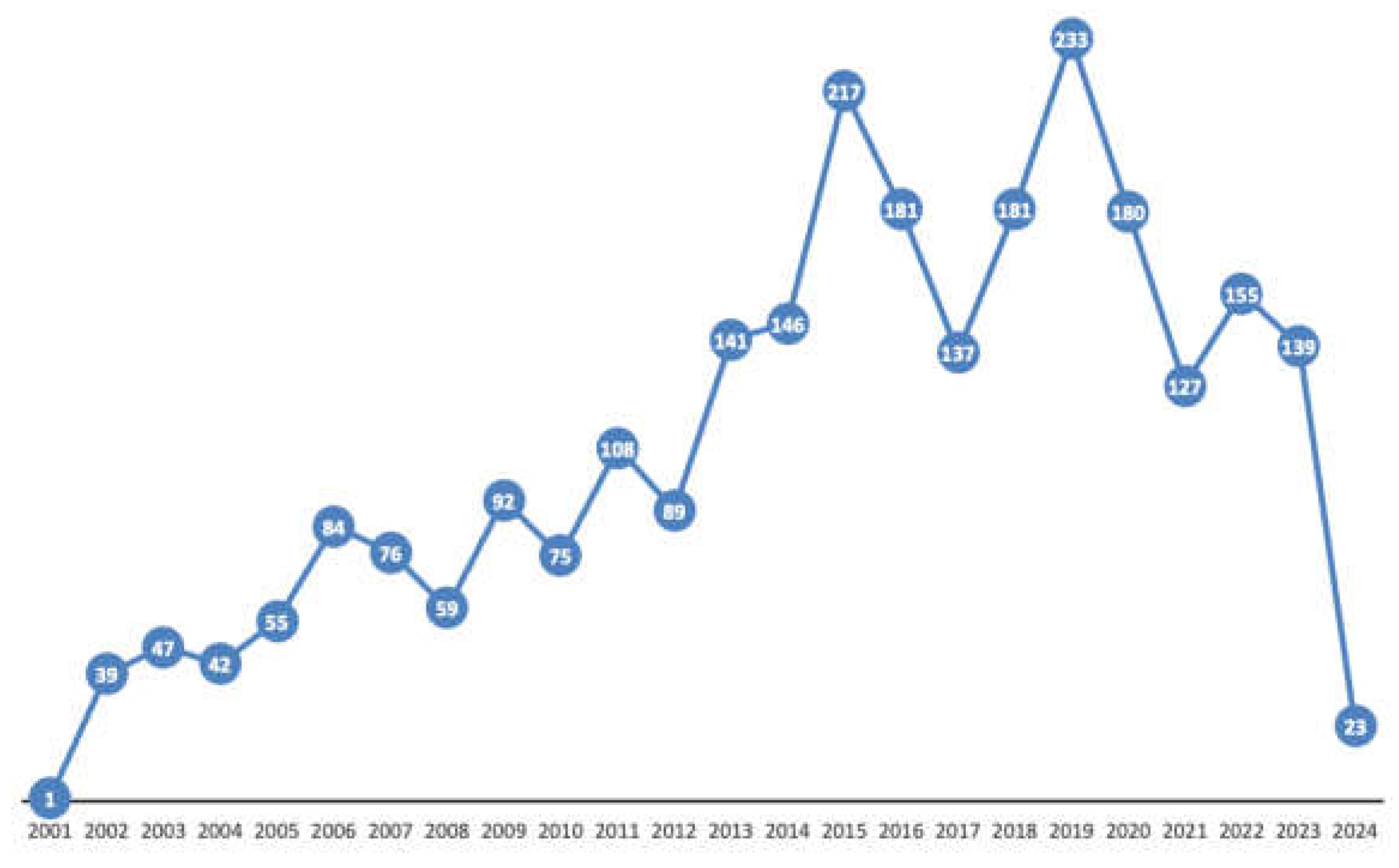
Figure 3.
Overview of the reported drugs obtained from the FAERS database according to first level ATC categories.
Figure 3.
Overview of the reported drugs obtained from the FAERS database according to first level ATC categories.
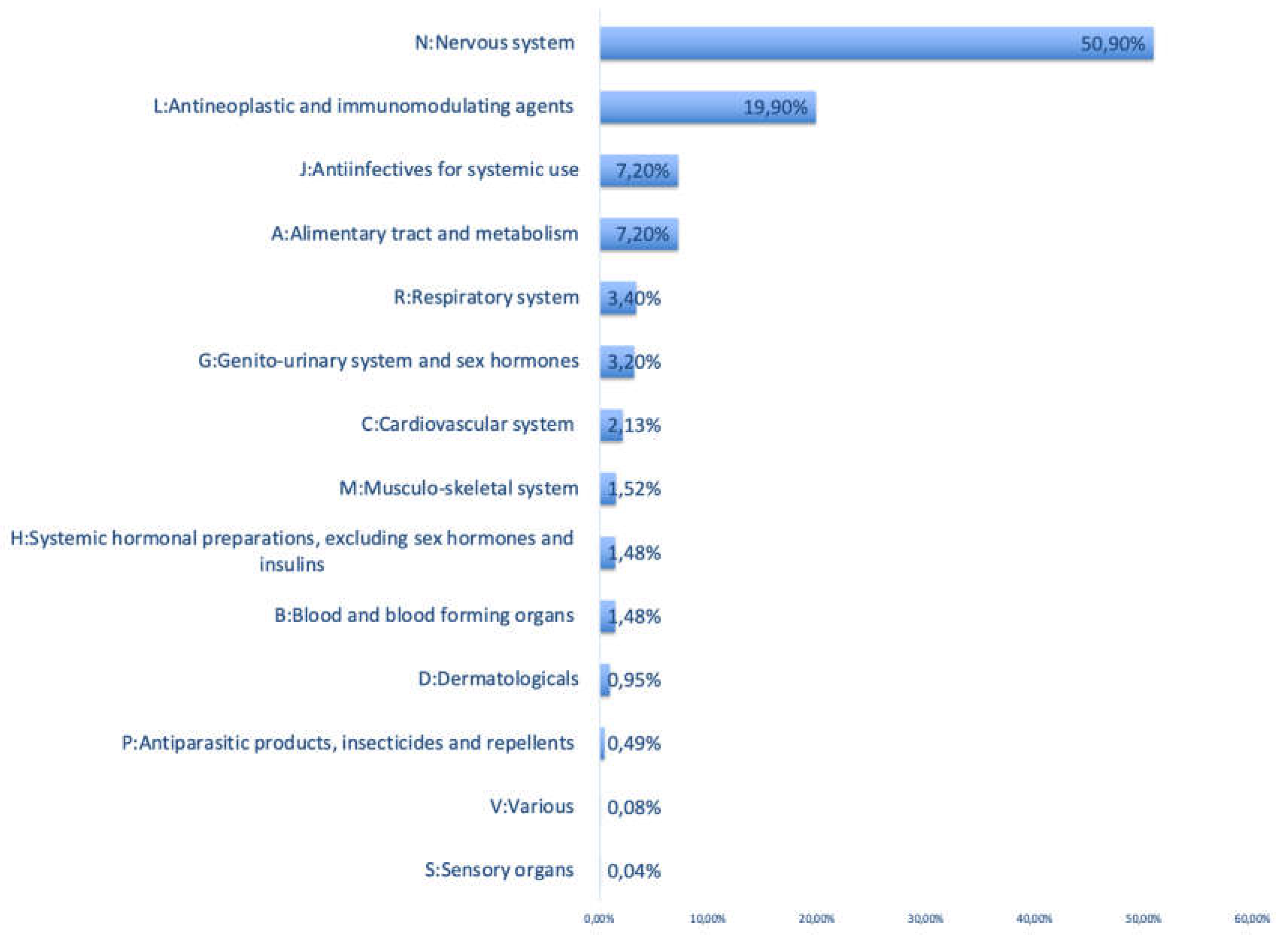
Figure 4.
Distribution of the infant outcome categories among lactation-related adverse events in the FAERS database.
Figure 4.
Distribution of the infant outcome categories among lactation-related adverse events in the FAERS database.
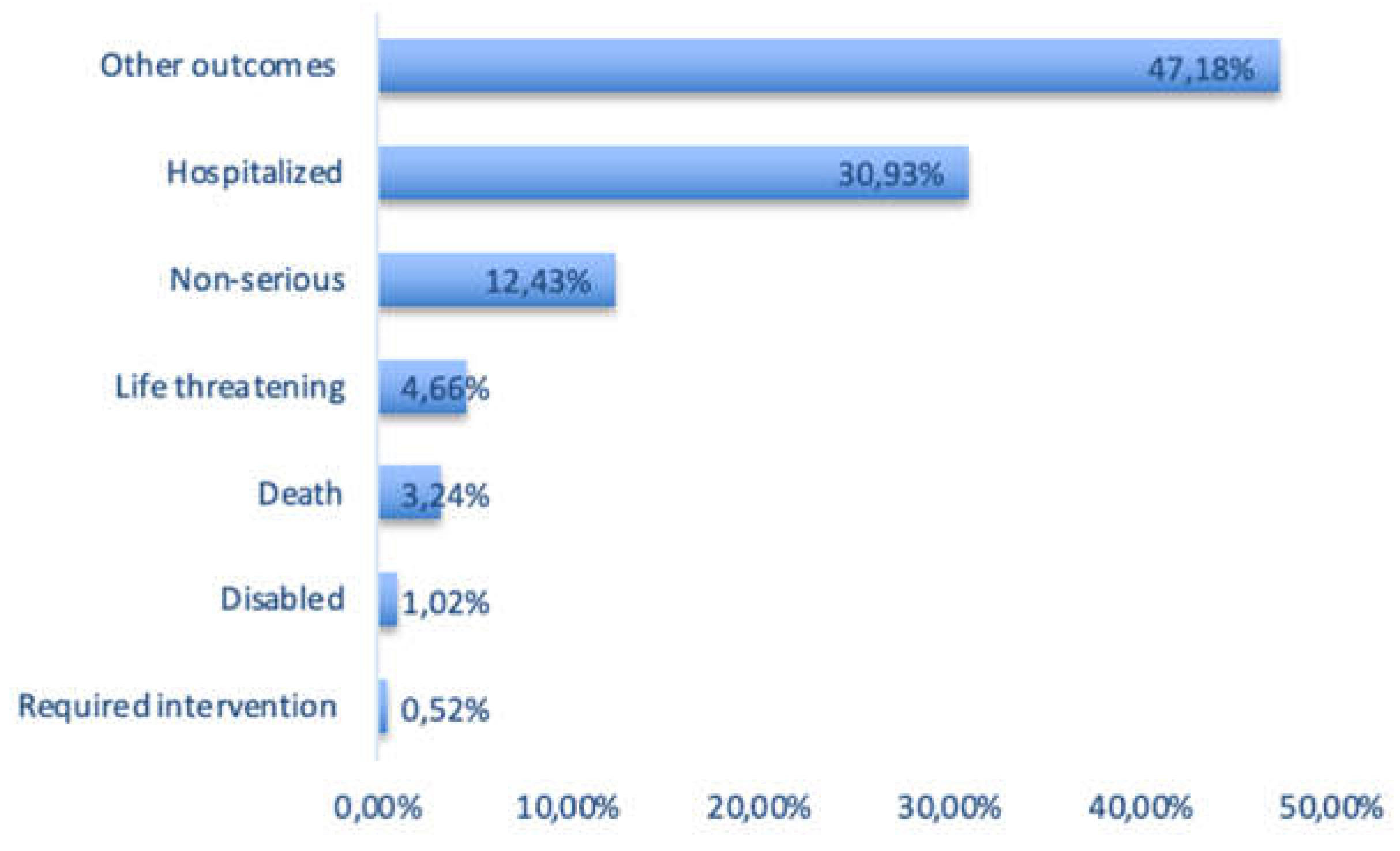
Figure 5.
Distribution of lactation-related adverse events in the FAERS database according to geographical region.
Figure 5.
Distribution of lactation-related adverse events in the FAERS database according to geographical region.
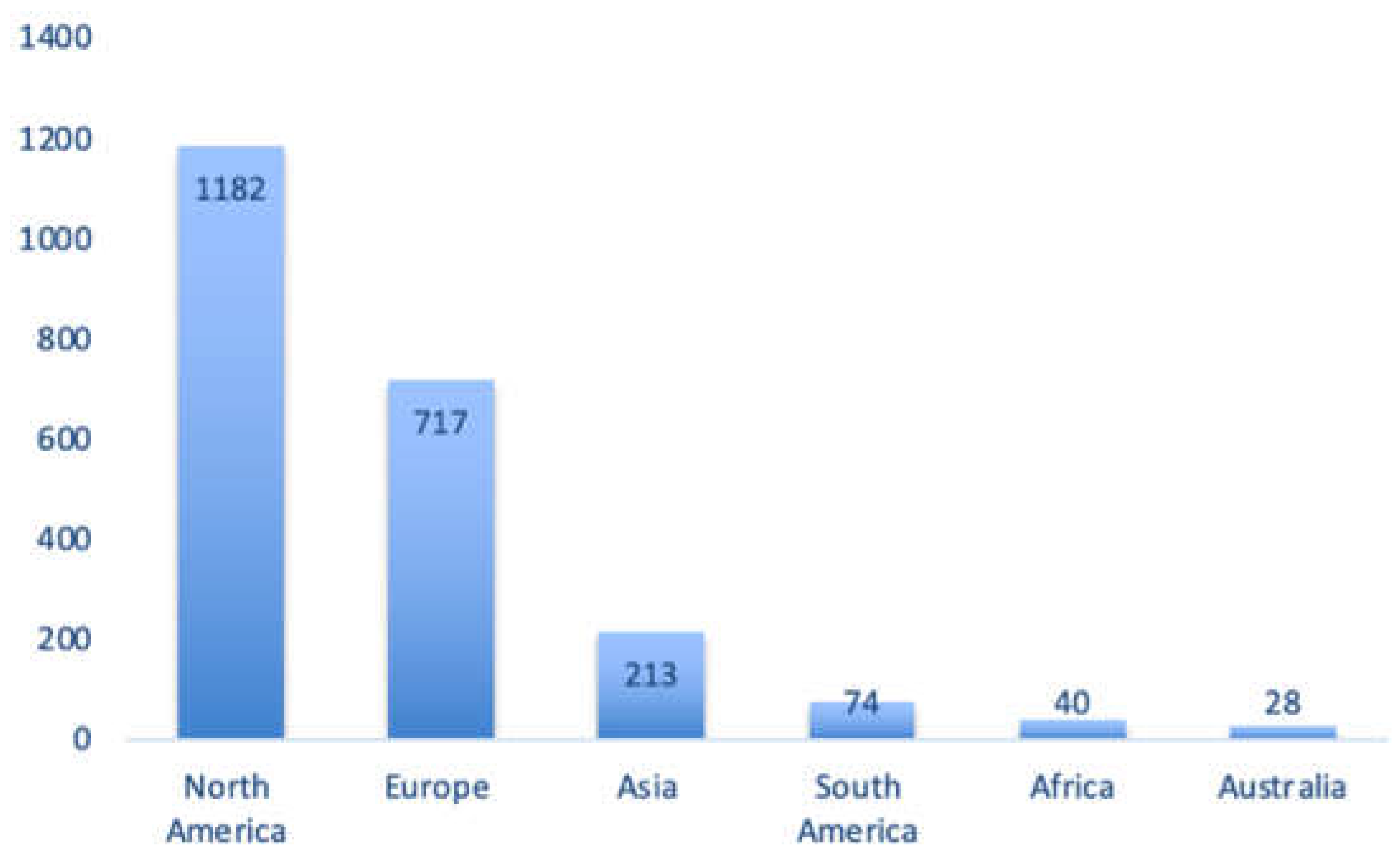

Table 1.
Top 5 ATC Classes and top 5 active pharmaceutical ingredients obtained from the FAERS database between 1 January 2001- 31 March 2024 (the percentage refers to the percentage for a given active pharmaceutical ingredient based on the total number of ATC class specific number of adverse events).
Table 1.
Top 5 ATC Classes and top 5 active pharmaceutical ingredients obtained from the FAERS database between 1 January 2001- 31 March 2024 (the percentage refers to the percentage for a given active pharmaceutical ingredient based on the total number of ATC class specific number of adverse events).
| ATC Class | Active Pharmaceutical Ingredient | Percentage* |
|---|---|---|
| N: Nervous system | Buprenorphine | 16.00% |
| Lamotrigine | 14.20% | |
| Levetiracetam | 10.10% | |
| Acetaminophen | 9.63% | |
| Nicotine | 7.62 | |
| L: Antineoplastic and immunomodulating agents | Certolizumab pegol | 32.76% |
| Adalimumab | 19.62% | |
| Etanercept | 11.24% | |
| Infliximab | 10.48% | |
| Tacrolimus | 5.33% | |
| A: Alimentary tract and metabolism | Insulin | 50% |
| Omeprazole | 7.45% | |
| Ondansetron hydrochloride | 6.92% | |
| Mesalamine | 6.38% | |
| Metformin hydrochloride | 4.79% | |
| J: Antiinfectives for systemic use | Zanamivir | 17.55% |
| Amoxicillin/Clavulanic acid | 13.30% | |
| Tenofovir disoproxil fumarate | 12.23% | |
| Lamivudine | 9.57% | |
| Emtricitabine\Tenofovir | 7.45% | |
| R: Respiratory system | Omalizumab | 24.72% |
| Cetirizine hydrochloride | 15.73% | |
| Fluticasone propionate/Salmeterol xinafoate | 13.48% | |
| Elexacaftor\Ivacaftor\Tezacaftor | 10.11% | |
| Budesonide | 7.87% |
* Within each ATC class (first level).
Table 2.
Overview of the available information on adverse infant events in the FAERS database and in LactMed for the 25 selected products.
Table 2.
Overview of the available information on adverse infant events in the FAERS database and in LactMed for the 25 selected products.
| N: Nervous system | FAERS | LactMed® |
|---|---|---|
| Buprenorphine | Bradycardia Coma scale abnormal Drug withdrawal syndrome Neonatal Hypoglycemia Hypotension Irritability Lethargy Miosis Poor feeding infant Selective eating disorder Somnolence Sudden death |
Agitation Drowsiness Drug withdrawal Frequent yawning Hyperactive Moro reflex Insomnia Lower milk intake Lower weight gain Myoclonic jerks Opioid abstinence Poor feeding Pupillary dilation Sneezing Sweating Tremors |
| Lamotrigine | Abdominal pain Abnormal loss of weight Apathy Bradyarrhythmia Cyanosis neonatal Ecchymosis Eczema Failure to thrive Fatigue Feeding disorder Fluid intake reduced Hepatic enzyme increased Hyperbilirubinemia neonatal Hypotonia neonatal Hypovolemic shock Infantile apnea Irritability Jaundice Laryngomalacia Lethargy Liver disorder Malnutrition Nausea Neonatal hypoxia Neutropenia Normochromic normocytic Anemia Poor feeding infant Poor weight gain neonatal Rash Rash maculo-papular Rhinorrhea Selective eating disorder Skin discoloration Sleep disorder Somnolence Stridor Supraventricular Extrasystoles Thrombocytosis Urticaria Vomiting |
Anemia Apneic episode Drowsiness Drug withdrawal Elevated liver enzymes Elevated platelet counts Feeding problems Gangrene Gastrointestinal symptoms Heart murmur Hypotonia Icterus prolongatus Irritability Jaundice Liver damage Loss of appetite Neuromotor hyperexcitability Persistent crying Rash Retractive breathing Sedation Transient neutropenia Weight loss |
| Levetiracetam | Anemia neonatal Heart rate increased Infantile apnea Cyanosis neonatal Blood bilirubin increased Failure to thrive |
Drowsiness Hypotonia Poor feeding infant Poor weight gain Sedation Vomiting Weight loss Withdrawal seizures |
| Acetaminophen | Abdominal distension Acute hepatic failure Asthma Blood pressure abnormal Capillary nail refill test abnormal Coagulopathy Crying Drug-induced liver injury Erythema Gastrointestinal hemorrhage Hemoglobin decreased Heart rate increased Hepatomegaly Hypoglycemia Irritability Jaundice Livedo reticularis Metabolic acidosis Poor feeding infant Pulse abnormal Pyrexia Respiratory distress Respiratory syncytial virus bronchiolitis Selective eating disorder Shock Skin exfoliation Staphylococcal infection Upper gastrointestinal hemorrhage Vomiting Wheezing |
Asthma Maculopapular rash on the upper trunk and face Wheezing |
| Nicotine | Dyspnea | Reduction in the heart rate Sudden infant death syndrome |
| L: Antineoplastic and immunomodulating agents | ||
| Certolizumab pegol | Agitation Fungal infection Hematochezia Hematoma Irritability Nervousness Rash Restlessness Selective eating disorder Tongue disorder Wound |
Candida infection Upper respiratory infection Vomiting |
| Adalimumab | Nasopharyngitis Irritability Intestinal hemorrhage Gastrointestinal disorder |
None reported |
| Etanercept | Blood bilirubin abnormal Blood glucose decreased Death Dermatitis atopic Diarrhea Disturbance in attention Dyslexia Enterocolitis Feeding intolerance Gastroesophageal reflux Disease Gross motor delay Hemoglobin decreased Jaundice neonatal Lung disorder Nasopharyngitis Pneumonia Rash macular Respiratory tract congestion Seborrheic dermatitis Selective eating disorder Viral infection Weight decreased Weight gain poor White blood cell count increased |
High-pitched crying Rash |
| Infliximab | Hematochezia Jaundice Lactose intolerance Lower respiratory tract infection Lymph gland infection Malaise Poor feeding infant Selective eating disorder |
None reported |
| Tacrolimus | Diarrhea Intraventricular hemorrhage neonatal Neonatal asphyxia Neonatal respiratory distress syndrome Pneumothorax |
None reported |
|
A: Alimentary tract and metabolism |
||
| Insulin | Gastroesophageal reflux disease Hematochezia Necrotizing colitis |
None reported |
| Omeprazole | Diarrhea Faeces discolored Zinc deficiency |
None reported |
| Ondansetron hydrochloride | Crying Insomnia Irritability Sluggishness |
None reported |
| Mesalamine | Abdominal pain upper Blood albumin abnormal Candida infection Colitis Diarrhea Hematochezia Hemoglobin abnormal Pyrexia White blood cell count increased |
Diarrhea Thrombocytosis Thrombosis |
| Metformin hydrochloride | Tremor | None reported |
|
J: Antiinfectives for systemic use |
||
| Zanamivir | Abnormal faeces Decreased appetite |
No information |
| Amoxicillin/Clavulanic acid | Agitation Clostridium difficile colitis Conversion disorder Diarrhea Enterocolitis Eye swelling Gastrointestinal pain Hematochezia Oral candidiasis Pyrexia Rash maculo-papular Rectal hemorrhage Vomiting |
Constipation Diarrhea Elevated liver enzymes (AST and ALT) Generalized urticaria Rash Restlessness |
| Tenofovir disoproxil fumarate | Thrombocytopenia | Diarrhea |
| Lamivudine | Sudden infant death syndrome | Sudden infant death syndrome |
| Emtricitabine/Tenofovir | - | Diarrhea |
| R: Respiratory system | ||
| Omalizumab | Anemia Anaphylactic reaction Cough Decreased appetite Eczema Eye oedema Gastroesophageal reflux disease Nasopharyngitis Oral fungal infection Otitis externa Poor quality sleep Pyrexia Rash erythematous Seborrheic dermatitis Swelling face |
None reported |
| Fluticasone propionate/Salmeterol xinafoate | Middle insomnia Poor feeding infant |
None reported |
| Cetirizine hydrochloride | Abnormal faeces Cyanosis Floppy infant Lethargy Oxygen saturation decreased Rash Respiratory arrest Somnolence |
Bruising Colicky symptoms Constipation Drowsiness Fever Irritability Poor feeding Rash Refusing of the breast Sedation |
| Elexacaftor\Ivacaftor\Tezacaftor | Alanine aminotransferase increased Aspartate aminotransferase increased Bronchiolitis Hyperinsulinemia Hypoglycemia neonatal Jaundice neonatal Neonatal respiratory distress Pancreatic failure Sepsis neonatal Sweat test abnormal Transient tachypnoea of the newborn Viral infection |
Bilirubin abnormalities Liver enzyme abnormalities Low sweat chloride |
| Budesonide | Adrenocortical insufficiency neonatal Dermatitis Eczema Neutropenia |
None reported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



