
Submitted:
13 November 2024
Posted:
14 November 2024
You are already at the latest version
Abstract
(1) Background: Keratoconus (KC) is a progressive corneal disorder that begins in adolescence and can lead to significant vision loss if undetected. Early identification of at -risk individuals through efficient screening tools like Keratoconus Risk Investigative Survey (KRIS) is critical, especially in large populations with limited access to comprehensive eyecare (2) Methods: A stratified random sample of 2,042 children, aged 9 to 17, completed a modified 20-item KRIS. Those identified with three or more risk factors underwent ophthalmic evaluations, including visual acuity, auto-keratorefractometry, and topographical screening. The analysis was conducted using SPSS version 25, focusing on sensitivity and specificity (3) Results: KRIS identified 36% (n=728) as at risk for KC, with a mean age of 12.09 years. Most were female (73%) and Muslim (72%). Significant correlations were found between demographic variables and clinical findings (p<0.001). Consanguinity showed a weaker association (Spearman: -0.09). Logistic regression indicated a strong likelihood of KC diagnosis in at-risk children (OR: 4.23, p<0.001). KRIS demonstrated moderate sensitivity (69%), specificity (66%), and overall accuracy (66%). The kappa coefficient (0.1) indicated slight agreement with clinical assessments, while the AUC of 0.57 suggested moderate screening ability. (4) Conclusions: KRIS is an effective screening tool for identifying children at risk of KC, aiding in targeted clinical assessments and reducing the need for mass screening.
Keywords:
Keratoconus
; KRIS
; Clinical assessment
; Sensitivity
; Specificity
1. Introduction
Keratoconus (KC) is defined as progressive thinning of the cornea, primarily in the central or paracentral regions, with its onset typically occurring during adolescence and extending into the third and fourth decades of life[1].KC often begins in one eye but may later involve the other, leading to the development of myopia and irregular astigmatism[2]. This condition results in decreased visual acuity (VA) and increased sensitivity to light, which can significantly affect an individual’s quality of life[1].Globally, KC impacts approximately 138 individuals per 100,000, with prevalence rates varying by race and geographic location[1].It is a significant cause of corneal visual impairment and blindness, with higher prevalence observed in Asian and Middle Eastern countries compared to Western and European regions[3]. Notably, the onset and progression of KC in populations such as Indians, Pakistanis, Arabs, and Polynesians are approximately 4.4 times greater than those observed in Caucasians[4].Research conducted in central and western India has indicated a frequency of KC ranging from 2.3% to 3.9%[5,6]. KC is associated with several risk factors, including a family history of the condition, chronic eye rubbing, and parental consanguinity[7].
llergic conditions, such as vernal keratoconjunctivitis (VKC), are significant triggers for KC, notably in regions like India, where approximately 10% of the population suffers from allergic eye diseases[8].Ultraviolet (UV) radiation exposure contributes to KC through oxidative stress and corneal thinning[9].Genetic predisposition, particularly in cases of consanguineous marriages(CM), further increases the risk [10], with a recent systematic review reporting that individuals with a family history of KC have a 6.42-fold increased likelihood of developing the condition[11].Consanguinity has been strongly linked to a higher prevalence of KC in regions such as North Africa and South India [12].Although systemic conditions like diabetes mellitus (DM) show weaker correlations[13,14], strong associations exist between KC and systemic conditions such as Marfan syndrome (MFS), osteogenesis imperfecta (OI), Leber congenital amaurosis(LCA), and Mitral valve prolapse(MVP), all of which suggest a genetic predisposition[14,15].
KC is often diagnosed at an advanced stage due to its progressive nature, with symptoms typically emerging in the later stages[16,17]. Early (subclinical) KC is often asymptomatic, making identification challenging[18]; as it can only be accurately diagnosed through comprehensive testing that includes topographic, tomographic, and auto-refractometric assessments[19].Mumbai, with an estimated population of 1.85 million children, is currently ranked as the second most polluted city globally, characterized by consistently poor Air Quality Index (AQI) levels that exacerbate allergic conditions[20,21].The escalating levels of pollution and hot, humid climate are conducive to KC development and may contribute to the noted increasing prevalence within the city’s growing population, making early detection crucial. Clinical evidence indicates that KC is a multifactorial condition, with eye rubbing being the most significant risk factor, followed by atopy [7,22]. The reported increase in KC cases[3], the high costs of curative treatments, and the emergence of early intervention treatments such as corneal cross-linking warrants the development of tools to identify children at risk. The KRIS, a 20-item questionnaire, was developed and utilized to identify individuals at risk[23]. However, no studies have yet evaluated the efficacy of KRIS in predicting clinical outcomes[22]. This study aimed to evaluate the effectiveness of KRIS in predicting clinical KC among secondary school students in Mumbai.
2. Materials and Methods
This study employed a quantitative methodology using a cross-sectional, descriptive design. A total of 2 042 secondary school children from two of the six zones in Mumbai City were selected via a stratified cluster random sampling technique. Participants completed a modified KRIS and provided additional demographic information. The survey was translated into Hindi, the local language, with the assistance of a Hindi PhD scholar and subsequently back-translated into English to achieve semantic equivalence. After obtaining the necessary gatekeepers’ permissions, school screenings were conducted across multiple schools in Mumbai city. The survey was administered using Google Forms. Students who responded positively to three or more risk factors were classified as being at risk for KC. Subsequently, KC screening was performed, comprising of VA testing, pinhole acuity assessment, automated keratorefractometry (GRAND SEIKO 3500K, Japan), corneal profiling with Placido-based topography (EyeSys Vista Videokeratoscope v2.6), retinoscopy for the detection of a scissors reflex, and anterior segment evaluation with an ophthalmoscope. Topography measurements were performed with the eye aligned to the visual axis, with three successive measurements taken per eye. The clearest image, as autodetected by the software, was selected for subsequent analysis. Subjects who failed at least two diagnostic tests (Table 1) were classified as KC-positive.
3. Results
A total of 2 042 children completed the KRIS and subsequently underwent KC clinical screening. Table 2 presents the participants’ demographic characteristics, including age, gender, and religious affiliation. The mean age was 12.46 ± 1.7 years, with participants distributed into two age groups: 9-12 years and 13-17 years. The sample consisted predominantly of females (66%) and individuals of Muslim faith (51%).
KRIS identified 36% (n=728) of the total study participants as suspected KC cases, with 7% (n=51) of these being clinically confirmed as KC through further clinical assessment within the same cohort. The overall prevalence of KC among all participants was 3.6% (n=74). Chi-square analysis and Spearman correlation tests were conducted. Table 3 highlights significant correlations between the prevalence of KC suspects and various demographic variables in both the KRIS and clinically at-risk groups. The mean age of KC suspects identified via KRIS was 12.09 ± 1.52 years. Significant associations were found for age and gender (p<0.001) and risk factors such as eye rubbing, atopy, and sun exposure. Weaker associations were noted for consanguinity (Spearman coefficient: -0.09) and family history (Spearman coefficient: 0). Among the 22 Muslims and 28 Hindus clinically diagnosed with KC, 54% (n=12) of Muslims and 14% (n=4) of Hindus had a positive history of consanguinity.
A logistic regression analysis was conducted to evaluate the effect of KRIS in diagnosing KC and found that KRIS significantly increased the odds of detecting KC (OR= 4.23; p < 0.001). The model explained only a small portion of the variance (R² between 0.02 and 0.06) and had a reasonable fit with a -2 log-likelihood of 601.19.
Assessment of the ability of the KRIS to detect KC suspects, as presented in Table 4, demonstrates moderate sensitivity and specificity. A positive likelihood ratio (PLR) of 2.00 indicates that a positive result is twice as likely to occur in KC cases compared to non-KC cases. However, the Kappa coefficient of 0.1 indicates a minimum agreement beyond chance.
Figure 1 illustrates the ROC curve for the KRIS binary classification model in detecting KC suspects. The model demonstrates an area under the curve (AUC) of 0.57. The curve’s proximity to the diagonal line indicates a limited balance between sensitivity and specificity.
A detailed analysis of the false positive cases (n=677), as shown in Figure 2, revealed that the predominant risk factors amongst the participants were eye rubbing and atopy, followed by consanguinity.
4. Discussion
The prevalence of KC suspects identified using the KRIS was 36% (n=728), of which 7% (n=51) were clinically confirmed as KC-positive. This finding is comparable to a study conducted in the West Cameroon region, which reported a 34.46% prevalence of KC risk among school children aged 8–18 years [23]. The prevalence of KC among the total study population, as determined by the KRIS screening combined with the clinical assessment, was 3.6% (n=74), similar to an Indian study that reported a KC prevalence of 3.9%[24]. Similarly, a study in Saudi Arabia reported a prevalence of 4.79% among individuals aged 6–21 years[25]. Although the literature indicates that KC prevalence in children is higher than in adults[17], most previous studies have focused on adults, with very few reporting on pediatric populations[5,26]. A large-scale hospital-based, cross-sectional study in India reported a higher prevalence of KC in children (1.04%) compared to adults (0.55%)[22]. It has been noted that there are studies that report a lower prevalence of KC than our findings; however, most have been conducted in hospital or clinical settings[3]. In such environments, patients typically present with symptoms, leading to a possible under-representation of asymptomatic or early-stage cases[3]. Although cross-sectional studies could be limited by the potential introduction of a selection bias, as they rely on voluntary participation[22], the strength of population-based studies is that they encompass a broader demographic and, in this instance, may provide a more accurate estimate of true KC prevalence than a clinic-based study[3].
The study identified a significant association between the KRIS and clinical KC groups regarding age and gender (Table 3). The mean ages for at-risk and clinical KC groups were 12.09 ± 1.52 and 12.46 ± 1.46 years, respectively, consistent with a West Cameroon study that reported a mean age of 13.18 years and supporting the reported association of KC and puberty[23]. However, Tharini et al. highlight that KC can also manifest in younger children, as evidenced by their findings of a mean age of 9.3 ± 1.8 years in their study of pre-teen Indian children [6]. Early onset of KC is associated with rapid progression and more advanced stages at diagnosis. Leoni-Mespile et al. found that 27.8% of patients under 15 had stage 4 KC, while Chatzi et al. reported that 88% of children experienced progression within a year of diagnosis, likely due to age-related corneal stiffening[27,28]. Given these findings of an early onset of KC in young children, early screening during childhood is essential to administer treatment and mitigate complications associated with KC. Further, health authorities should plan and conduct regular school screenings to ensure early detection within the Mumbai pediatric population. Our study found a significant correlation between KRIS results and clinical KC, with more females identified as at-risk than males (Table 3). However, previous studies have shown mixed results regarding gender prevalence. For example, an Indian study on pre-teens reported a higher prevalence in males (70%), whereas a study from western India indicated a higher prevalence among females (63.83%) [6,23], consistent with our findings. Girls are 25 times more likely than boys to experience early puberty, with Indian schoolgirls showing onset as early as 10.8 years and a median age of 12.4 [29,30]. Increased estrogen levels in females are associated with corneal thinning and the progression of KC[31], which aligns with our findings (Table 3). Conversely, Das et al. (2024), in a study including subjects from birth to 80years, found that males in India are eight times more likely to develop KC[22]. This discrepancy may stem from our study’s inclusion of many pre-pubescent children, lower age cut-off, and possible later onset of puberty in male participants. Cross-sectional studies conducted in the U.S. and Europe have demonstrated an increasing trend in the incidence of early puberty in both sexes[32]. The higher prevalence of KC during puberty may also be influenced by sex hormones, as androgens and estrogens are known to induce anatomical changes in the cornea[33]. The lack of empirical clarity in relation to gender prevalence may indicate the possible influence of other confounding variables. Further research across a broader age range, eliminating other variables, is needed to inform gender-related KC profiles in India.
No significant association was found between religion and KC prevalence in the KRIS or clinical groups. However, there was a higher prevalence of Muslim at-risk subjects (73%; n=531), of which 4% (n=22) were clinically diagnosed with KC, and 14.5%(n=28) of at-risk Hindus were confirmed as KC cases (Table 3). The increased risk among Muslims may be linked to consanguinity, reported by 36% (n=745) of all subjects, of whom 84% were Muslim. In the clinical KC group, 54% of Muslims had a positive consanguinity history, compared to 14% of Hindus. Supporting these findings, Mohammad-Rabie et al. in their Iranian study, found that 34.2% of KC patients had a history of CM [34]. In regions such as North Africa, the Middle East, and South India, the prevalence of CM ranges from 20% to 50% and is associated with an elevated risk of recessive genetic disorders such as KC [35]. According to the National Family Health Survey-5, 11% of marriages in India are consanguineous, with this figure rising to 15% among Muslims[36]. These findings highlight the importance of targeted screening in this high-risk population to enable early detection and intervention. Family history showed a weak correlation between the KRIS and clinical KC groups, with only 4% of the KRIS-positive group reporting a positive family history (Table 3). In contrast, Bykhovskaya et al. found that a family history of KC increases the risk of developing the condition by 6.42 times, and Ayukotang et al. identified it as a significant risk factor[23,37]. Genetic evidence supports familial inheritance, with around 90% of KC cases showing autosomal dominant inheritance with reduced penetrance, though recessive patterns are also noted[38]. Specific loci, such as 16q22.3-q23.1 (autosomal dominant) and 17q13 (autosomal recessive), have been identified(38). KC prevalence in first-degree relatives is 3.34%, significantly higher than in the general population[39]. The poor correlation found between family history and KC in this study may result from a lack of awareness by this young study cohort about the specific vision condition afflicting their respective family members. Advocacy and public education programs could improve understanding of the disease and its risk factors. Given the genetic link, screening relatives of KC patients is essential for early detection.
Eye rubbing is a well-established risk factor for KC[40]. In this study, 100% of clinically positive cases were positive for eye rubbing (Table 3). Chronic eye rubbing, often due to psychogenic factors or conditions like itching and dryness, plays a key role in KC development[40]. The cornea’s viscoelastic properties render it susceptible to changes from the force and frequency of rubbing, reducing corneal stiffness and altering biomechanical properties such as hysteresis and resistance[40,41,42]. Both vigorous and mild rubbing has been implicated in the development of KC through mechanisms including keratocyte apoptosis, decreased epithelial thickness, and reduced keratocyte density[43]. Raising awareness about the harmful effects of eye rubbing, particularly in children, is essential, and recording the frequency of eye rubbing during ocular examinations is recommended.
In this study, 7.13% of KRIS-positive cases had a documented history of atopy (Table 3). Atopy, which includes allergies, asthma, and eczema, affects approximately 40% of children[44]. The direct association between atopy and KC remains contentious. While certain studies suggest an association between the two conditions[45,46], others do not[47,48]. For instance, Bawazeer et al. [47] found no direct association between atopy and KC, suggesting that atopy may indirectly contribute to KC development through eye rubbing, which is often triggered by the itching associated with allergic reactions. Kaya et al. [49] demonstrated that KC patients with atopy exhibit steeper and thinner ectatic corneas compared to those without. Findings from the Collaborative Longitudinal Evaluation of KC (CLEK) study reported that 52.9% of KC patients had a history of hayfever or allergies, 14.9% had asthma, 8.4% had atopic dermatitis, and 27% had VKC[50]. In VKC, symptoms such as itching and chronic eye rubbing can lead to corneal damage, with KC being a frequent complication [51]. Given these findings, early screening for atopy in children, increased awareness of the harmful effects of eye rubbing, comprehensive allergy management, and regular corneal topography assessments are recommended to reduce the risk and progression of KC.
The KRIS survey revealed that 12.2%(n=251/2042) of the total sample and 34.5%(n=251/728) of the KRIS-positive participants were exposed to over 24 hours of sunlight per week, with a significant correlation (Table 3). Similarly, Ayukotang et al. found that 11.4% of children reported frequent sunlight exposure exceeding 24 hours per week, identifying sunlight exposure as a significant risk factor (OR 2.7, p < 0.001)(23). Together, these findings align with other studies from regions with high sunlight exposure[52,53]. Prolonged exposure to sunlight and UV rays can induce oxidative stress and corneal thinning, contributing to the development of KC due to the cytotoxic effects of reactive oxygen species[54]. Aldehyde dehydrogenase 3 (ALDH3), a critical detoxifying enzyme involved in the oxidation of alcohols to aldehydes, is reduced in the corneal tissue of individuals with KC[54]. To mitigate the risk of KC, it is advisable to limit prolonged exposure to sunlight by promoting the use of UV-blocking eyewear and educating high-risk populations about protective measures. Public eye health education and regular eye screenings in regions with high sunlight exposure should also be encouraged to detect early signs of corneal damage.
The KRIS survey in this study reported a lower prevalence of diabetes and other medical conditions among KC patients, suggesting that diabetes may not be associated with KC in this young study population (Table 3). Chronic hyperglycemia in diabetes leads to increased advanced glycation end products (AGEs), enhancing collagen cross-linking and reducing corneal thinning, potentially protecting against KC[13,55]. A case-control study similarly reported a lower prevalence of KC in patients with diabetes (0.8%) compared to the control group (2.2%), suggesting a significant protective effect of diabetes against developing KC[56]. Systemic conditions, including Down syndrome (DS), MFS, OI, LCA, and MVP, have been variably linked to KC(14). Although this study did not find DS cases, it is known to show a high KC prevalence, possibly due to associated chronic eye-rubbing[57], with other connective tissue disorders (MFS, OI, and MVP) predisposing patients to KC due to collagen dysregulation affecting corneal stability[14,58,59,60].
The study found that 14% (n=102) of parents of KC suspects had no formal education, while the majority had received some form of schooling, a factor significantly correlated with the clinical KC group (Table 3). However, previous research has linked KC to lower parental education levels, likely reflecting economic status[61]. An Iranian study also indicated that individuals with less than six years of schooling and lower socioeconomic status were more prone to developing KC[34]. In contrast, a recent retrospective study from India reported that upper-middle-class youth are five times more likely to develop KC compared to their lower-class counterparts[22], attributing this to better access to eye care and earlier detection. Our study found a lower prevalence of KC in high-income groups and a higher prevalence in low- and moderate-income groups, suggesting a correlation with socioeconomic disadvantage (Table 3). Despite most participants being from low-income backgrounds, 86% of their parents had some level of schooling, indicating that education and socioeconomic status may not be directly correlated. Further research across different socioeconomic levels and educational backgrounds is needed to clarify and inform these previously reported associations.
The clinical identification of KC typically involves commonly used tests such as VA, auto-keratorefractometry, and detection of the scissors reflex during retinoscopy. Although these tests assist in diagnosing KC, early and subclinical cases can only be reliably detected through topographical evaluation[62]. Traditional topographers, however, are generally large and confined to clinical settings. Given that this was a population-based study and conducted at various schools, a portable handheld computer-assisted Placido-disc-based topographer (EyeSys Vista version 2.6) was used [63]. Its portability and lightweight design made it well-suited for large-scale, on-site screenings. Videokeratoscopes have been demonstrated to reliably identify KC, as reported in previous studies[63,64]. The EyeSys Vista is comparable to the Orbscan[65], particularly when evaluating indices such as Sim K (Simulated Keratometer), I-S (Inferior-Superior), and SAI (Surface Asymmetry Index) [63]. In our study, 7% (n=51) of the at-risk participants identified through KRIS screening exhibited KC-related topographical signs. A limitation of relying solely on corneal topography is that it primarily assesses the anterior corneal surface, potentially missing early KC cases where changes may initially occur in the posterior cornea [66]. Currently, no portable corneal tomographer has been employed to detect these pre-clinical cases. Therefore, incorporating additional clinical evaluations, such as retinoscopy, measurements of myopia and astigmatism, and a detailed case history of risk factors, is essential for early detection.
A logistic regression analysis was conducted to assess the performance of the KRIS compared to clinical assessments, combined with calculations of sensitivity, specificity, and the kappa coefficient, as shown in Table 4. The sensitivity of the KRIS was observed to be 69%, indicating its ability to accurately identify true KC cases. However, KRIS failed to detect 31% (n=23) of the 74 cases deemed positive through clinical assessment, thus resulting in a considerable rate of false negatives. This finding suggests that the KRIS may be appropriate as a preliminary screening tool but should ideally be supplemented with a KC-specific clinical assessment, as a failure to identify KC cases could lead to delays in diagnosis and treatment, ultimately allowing for further progression of the disease.The specificity of the KRIS, quantified at 66%, indicates its ability to identify non-KC individuals correctly. However, this level of specificity was accompanied by 677 misclassifications of non-KC individuals as positive cases, indicating a substantial rate of false positives. A subsequent detailed analysis revealed that every individual within this false positive cohort (100%) reported some form of allergy, with 94% indicating eye-rubbing behavior (Figure 2). These findings emphasize the importance of investigating alternative causes of eye rubbing and atopy that could influence the high false positive rates independently of KC diagnosis. Further, eye rubbing was not delved into deeper to differentiate the type, severity, and area of rubbing, relying solely on frequency responses reported by this young student population. As this question contributed to the significant over-referral of non-KC individuals, potentially skewing the data interpretation, it warrants consideration of the inclusion of more descriptive follow-up questions on eye rubbing in future iterations of the KRIS.
Overall, the KRIS tool demonstrated a moderate diagnostic accuracy rate of 66%, indicating a balanced performance in sensitivity and specificity measures. Logistic regression analysis further supported the KRIS’s utility, showing that children flagged by the tool had a 4.23-fold likelihood of testing positive for KC in clinical evaluations, a statistically significant outcome. Further, with a ROC value of 0.57 (Figure 1), the analysis demonstrated moderate capacity of the KRIS to identify individuals at risk for KC, performing only slightly better than random classification. Therefore, although the tool shows potential in detecting certain cases of KC, the ROC value suggests limited efficiency in accurately differentiating true positives from negatives, which poses a risk of both false positive and false negative results. Further, refinement of the KRIS tool, by modifying certain screening criteria or integrating additional diagnostic metrics, is recommended as it has considerable potential as a large-scale screening tool for KC detection, particularly in resource-limited settings. Such optimizations would enhance sensitivity and specificity, thereby improving the ROC value and establishing the KRIS as a more effective and reliable tool for large-scale KC screening.
Mumbai, the fourth most populous city globally, currently has an estimated population of 20 million[67]. The city’s demographic composition is highly diverse, with approximately 1.85 million children[68]. Situated at sea level, Mumbai’s climatic conditions are conducive to the development of KC[69]. Over 9 million residents, constituting 41.3% of the city’s population, live in slum areas [67], where low-income families are subjected to substandard living conditions[67]. Our study primarily included students from government-aided schools, revealing that the majority of KC suspects were from moderate to low-income backgrounds (Table 3). The prevalence of unhygienic environments and exposure to dust in these areas may contribute to allergies and habitual eye rubbing, which could ultimately lead to the development of KC [70].Given the high population density of the city [67], conducting annual KC clinical screenings for all school children would be a resource-intensive and costly undertaking, requiring substantial human resources. However, the implementation of tools such as the KRIS questionnaire offers a feasible alternative. This tool can easily be administered to schoolchildren or parents, allowing for the identification of at-risk children within the general population. By facilitating targeted clinical screenings, KRIS enables timely interventions to prevent the progression of undetected disease, which could otherwise negatively impact the child’s quality of life.
5. Limitation
The limitation of this study is its reliance on self-reports, which may introduce recall bias and other related issues.
6. Conclusions
The KRIS has demonstrated its effectiveness in identifying KC suspects within large populations. The findings indicate that children identified as at risk by KRIS are likely to be diagnosed with KC following further clinical assessment. Although KRIS exhibits moderate sensitivity in identifying KC suspects, its positive likelihood ratio (PLR) suggests it is particularly effective in identifying potential KC suspects. This characteristic makes KRIS a valuable screening tool, enabling a more efficient and focused evaluation process. Incorporating KRIS into school-based screening programs in Mumbai City could enhance the ability of school screening teams to perform appropriate KC clinical tests on at-risk children during their visits to schools.
Author Contributions
Conceptualization: N.C, V.R.M and K.P.M.; methodology: N.C, V.R.M and K.P.M; formal analysis: N.C, V.R. M and K.P.M.; investigation: N.C; data curation: N.C.; writing—original draft preparation: N.C.; writing—review and editing: N.C, V.R. M and K. P.M.; supervision: V.R.M and K.P.M. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare that no form of funding was received for this study.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and ethical approval was obtained from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (reference: BREC/00001335/2020). The study included secondary schoolchildren aged 8 to 18 years, all of whom provided signed informed consent and assent forms. Children whose parents or guardians did not provide consent were excluded from participation.
Informed Consent Statement
Informed consent was obtained from parents/guardians, with children’s assent. Participants were assured they could withdraw at any time, and all identities were anonymized.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors wish to thank Mr. M. Gopinath and Catherine Connolly for helping with statistical analysis.
Conflicts of Interest
The authors have no financial disclosure to make and no conflict of interest to be declared.
References
- Santodomingo-Rubido, J.; Carracedo, G.; Suzaki, A.; Villa-Collar, C.; Vincent, S.J.; Wolffsohn, J.S. Keratoconus: An updated review. Cont Lens Anterior Eye. 2022, 45, 101559. [Google Scholar] [CrossRef] [PubMed]
- Borderie, V.M.; Laroche, L. Measurement of irregular astigmatism using semi meridian data from videokeratography. J Refract Surg. 1996, 12, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.A.P.; Rodrigues, P.F.; Lamazales, L.L. Keratoconus epidemiology: A review. Saudi Journal of Ophthalmology 2022, 36, 3–6. [Google Scholar] [CrossRef]
- Pearson, A.R.; Soneji, B.; Sarvananthan, N.; Sandford-Smith, J.H. Does ethnic origin influence the incidence or severity of keratoconus? Eye (Lond). 2000, 14 Pt 4, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Nangia, V.; Matin, A.; Kulkarni, M.; Bhojwani, K. Prevalence and associations of keratoconus in rural Maharashtra in central India: the central India eye and medical study. Am J Ophthalmol. 2009, 148, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Tharini, B.; Sahebjada, S.; Borrone, M.A.; Vaddavalli, P.; Ali, H.; Reddy, J.C. Keratoconus in pre-teen children: Demographics and clinical profile. Indian J Ophthalmol. 2022, 70, 3508–3513. [Google Scholar] [CrossRef]
- Gordon-Shaag, A.; Millodot, M.; Shneor, E.; Liu, Y. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015, 2015, 795738. [Google Scholar] [CrossRef]
- Singh, A.; Rana, J.; Kataria, S.; Bhan, C.; Priya, P. Demographic and clinical characteristics of childhood and adult-onset Vernal Keratoconjunctivitis in a tertiary care center during Covid pandemic: A prospective study. Rom J Ophthalmol. 2022, 66, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Mohaghegh, S.; Kangari, H.; Masoumi, S.J.; Bamdad, S.; Rahmani, S.; Abdi, S.; Fazil, N.; Shahbazi, S. Prevalence and risk factors of keratoconus (including oxidative stress biomarkers) in a cohort study of Shiraz university of medical science employees in Iran. BMC Ophthalmol. 2023, 23, 188. [Google Scholar] [CrossRef]
- Lucas, S.E.M.; Burdon, K.P. Genetic and Environmental Risk Factors for Keratoconus. Annu Rev Vis Sci. 2020, 6, 25–46. [Google Scholar] [CrossRef]
- Hashemi, H.; Heydarian, S.; Hooshmand, E.; Saatchi, M.; Yekta, A.; Aghamirsalim, M.; Valadkhan, M.; Mortazavi, M.; Hashemi, A.; Khabazkhoob, M. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea. 2020, 39, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Temaj, G.; Nuhii, N.; Sayer, J.A. The impact of consanguinity on human health and disease with an emphasis on rare diseases. J Rare Dis 2022, 1, 2. [Google Scholar] [CrossRef]
- McKay, T.B.; Priyadarsini, S.; Karamichos, D. Mechanisms of Collagen Crosslinking in Diabetes and Keratoconus. Cells. 2019, 8, 1239. [Google Scholar] [CrossRef]
- Unni, P.; Lee, H.J. Systemic Associations with Keratoconus. Life (Basel). 2023, 13, 1363. [Google Scholar] [CrossRef]
- McMahon, T.T.; Kim, L.S.; Fishman, G.A.; Stone, E.M.; Zhao, X.C.; Yee, R.W.; Malicki, J. CRB1 gene mutations are associated with keratoconus in patients with Leber congenital amaurosis. Invest Ophthalmol Vis Sci. 2009, 50, 3185–3187. [Google Scholar] [CrossRef]
- Mas Tur, V.; MacGregor, C.; Jayaswal, R.; O’Brart, D.; Maycock, N. A review of keratoconus: Diagnosis, pathophysiology, and genetics. Vol. 62, Survey of Ophthalmology. Elsevier USA; 2017. p. 770–83. [CrossRef]
- Yang, K.; Gu, Y.; Xu, L.; Fan, Q.; Zhu, M.; Wang, Q.; Yin, S.; Zhang, B.; Pang, C.; Ren, S. Distribution of pediatric keratoconus by different age and gender groups. Front Pediatr. 2022, 10, 937246. [Google Scholar] [CrossRef]
- Kandel, S.; Chaudhary, M.; Mishra, S.K.; Joshi, N.D.; Subedi, M.; Puri, P.R.; et al. Evaluation of corneal topography, pachymetry, and higher order aberrations for detecting subclinical keratoconus. Ophthalmic and Physiological Optics. 2022, 42, 594–608. [Google Scholar] [CrossRef] [PubMed]
- Feizi, S.; Yaseri, M.; Kheiri, B. Predictive ability of Galilei to distinguish subclinical keratoconus and keratoconus from normal corneas. J Ophthalmic Vis Res. 2016, 11, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Nanavare, R.T. Impact of air pollution on respiratory health: A case study in Mumbai, India. International Journal of Medical and Health Research [Internet]. 2024. Available from: www.medicalsciencejournal.com.
- Manya Rathore Population of Mumbai India 1960-2024. https://www.statista.com/statistics/911012/india-population-in-mumbai/#statistic.
- Das, A.V.; Deshmukh, R.S.; Reddy, J.C.; Joshi, V.P.; Singh, V.M.; Gogri, P.Y.; et al. Keratoconus in India: Clinical presentation and demographic distribution based on big data analytics. Indian J Ophthalmol. 2024, 72, 105–110. [Google Scholar] [CrossRef]
- Ayukotang, E.N.; Moodley, V.R.; Mashige, K.P. Risk Profile of Keratoconus among Secondary School Students in the West Region of Cameroon. Vision (Basel). 2022, 7, 2. [Google Scholar] [CrossRef]
- Chelliah, R.; Rangasamy, R.; Veeraraghavan, G.; et al. Screening for Keratoconus among Students in a Medical College in South India: A Pilot Study. TNOA Journal of Ophthalmic Science and Research 2023, 61, 192–195. [Google Scholar] [CrossRef]
- Torres Netto, E.A.; Al-Otaibi, W.M.; Hafezi, N.L.; Kling, S.; Al-Farhan, H.M.; Randleman, J.B.; et al. Prevalence of keratoconus in pediatric patients in Riyadh, Saudi Arabia. British Journal of Ophthalmology. 2018, 102, 1436–1441. [Google Scholar] [CrossRef]
- Lapeyre, G.; Fournie, P.; Vernet, R.; Roseng, S.; Malecaze, F.; Bouzigon, E.; Touboul, D. Keratoconus Prevalence in Families: A French Study. Cornea. 2020, 39, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Léoni-Mesplié, S.; Mortemousque, B.; Touboul, D.; Malet, F.; Praud, D.; Mesplié, N.; Colin, J. Scalability and severity of keratoconus in children. Am J Ophthalmol. 2012, 154, 56–62.e1. [Google Scholar] [CrossRef] [PubMed]
- Chatzis, N.; Hafezi, F. Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents. J Refract Surg. 2012, 28, 753–758. [Google Scholar] [CrossRef]
- Soriano-Guillén, L.; Argente, J. Central precocious puberty, functional and tumor-related. Best Pract Res Clin Endocrinol Metab. 2019, 33, 101262. [Google Scholar] [CrossRef]
- Khadgawat, R.; Marwaha, R.K.; Mehan, N.; Surana, V.; Dabas, A.; Sreenivas, V.; Gaine, M.A.; Gupta, N. Age of Onset of Puberty in Apparently Healthy School Girls from Northern India. Indian Pediatr. 2016, 53, 383–387. [Google Scholar] [CrossRef]
- Zhao, X.; et al. Associations Between Keratoconus and the Level of Sex Hormones: A Cross-Sectional Study. Frontiers in medicine 2022, 9, 828233. [Google Scholar] [CrossRef]
- Latronico, A.C.; et al. Causes, diagnosis, and treatment of central precocious puberty. The lancet. Diabetes & endocrinology 2016, 4, 265–274. [Google Scholar] [CrossRef]
- McKay, T.B.; et al. Sex Hormones, Growth Hormone, and the Cornea. Cells 2022, 11, 224. [Google Scholar] [CrossRef]
- Mohammad-Rabei, H.; et al. Risk Factors Associated with Keratoconus in an Iranian Population. Journal of ophthalmic & vision research 2023, 18, 15–23. [Google Scholar] [CrossRef]
- Jamali, H.; Beigi, V. Sadeghi-Sarvestani Consanguineous Marriage as a Risk Factor for Developing Keratoconus. Discovery &Innovation Ophthalmology Journal. 2018, 11, 17–21. [Google Scholar]
- Bittles, A.H.; Hussain, R. An analysis of consanguineous marriage in the Muslim population of India at regional and state levels. Ann Hum Biol. 2000, 27, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Bykhovskaya, Y.; Rabinowitz, Y.S. Update on the genetics of keratoconus. Exp Eye Res. 2021, 202, 108398. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.M.; Gajecka, M. The genetics of keratoconus. Middle East African journal of ophthalmology 2011, 18, 2–6. [Google Scholar] [CrossRef]
- Wang, Y.; et al. Genetic epidemiological study of keratoconus: evidence for major gene determination. American journal of medical genetics 2000, 93, 403–409. [Google Scholar] [CrossRef]
- Najmi, H.; et al. The correlation between keratoconus and eye rubbing: a review. International journal of ophthalmology 2019, 12, 1775–1781. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; et al. Effect of eye rubbing on corneal biomechanical properties in myopia and emmetropia. Frontiers in bioengineering and biotechnology 2023, 11, 1168503. [Google Scholar] [CrossRef]
- Hawkes, E.; Nanavaty, M.A. Eye Rubbing and Keratoconus: A Literature Review. Int J Keratoconus Ectatic Corneal Dis. 2014, 3, 118–121. [Google Scholar] [CrossRef]
- Hafezi, F.; Hafezi, N.L.; Pajic, B.; Gilardoni, F.; Randleman, J.B.; Gomes, J.A.P.; Kollros, L.; Hillen, M.; Torres-Netto, E.A. Assessment of the mechanical forces applied during eye rubbing. BMC Ophthalmol. 2020, 20, 301. [Google Scholar] [CrossRef]
- Anitha, V.; Vanathi, M.; Raghavan, A.; Rajaraman, R.; Ravindran, M.; Tandon, R. Pediatric keratoconus - Current perspectives and clinical challenges. Vol. 69, Indian Journal of Ophthalmology. Wolters Kluwer Medknow Publications; 2021. p. 214–25. [CrossRef]
- Nemet, A.Y.; Vinker, S.; Bahar, I.; Kaiserman, I. The association of keratoconus with immune disorders. Cornea. 2010, 29, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Nemet, A.Y.; et al. The association of keratoconus with immune disorders. Cornea 2010, 29, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Seth, I.; et al. The association between keratoconus and allergic eye diseases: A systematic review and meta-analysis. Clinical & experimental ophthalmology 2022, 50, 280–293. [Google Scholar] [CrossRef]
- Bawazeer, A.M.; Hodge, W.G.; Lorimer, B. Atopy and keratoconus: a multivariate analysis. Br J Ophthalmol. 2000, 84, 834–836. [Google Scholar] [CrossRef]
- Kaya, V.; Karakaya, M.; Utine, C.A.; Albayrak, S.; Oge, O.F.; Yilmaz, O.F. Evaluation of the corneal topographic characteristics of keratoconus with orbscan II in patients with and without atopy. Cornea. 2007, 26, 945–948. [Google Scholar] [CrossRef]
- Zadnik, K.; Barr, J.T.; Edrington, T.B.; Everett, D.F.; Jameson, M.; McMahon, T.T.; Shin, J.A.; Sterling, J.L.; Wagner, H.; Gordon, M.O. Baseline findings in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study. Invest Ophthalmol Vis Sci. 1998, 39, 2537–2546. [Google Scholar]
- Singhal, D.; Sahay, P.; Maharana, P.K.; Raj, N.; Sharma, N.; Titiyal, J.S. Vernal Keratoconjunctivitis. Vol. 64, Survey of Ophthalmology. Elsevier USA; 2019. p. 289–311.
- Assiri, A.A.; Yousuf, B.I.; Quantock, A.J.; Murphy, P.J.; Assiri, A.A. Incidence and severity of keratoconus in Asir province, Saudi Arabia. British Journal of Ophthalmology. 2005, 89, 1403–1406. [Google Scholar] [CrossRef]
- Millodot, M.; Shneor, E.; Albou, S.; Atlani, E.; Gordon-Shaag, A. Prevalence and associated factors of keratoconus in Jerusalem: a cross-sectional study. Ophthalmic Epidemiol. 2011, 18, 91–97. [Google Scholar] [CrossRef]
- Nita, M.; Grzybowski, A. The Role of the Reactive Oxygen Species and Oxidative Stress in the Pathomechanism of Age-related Ocular Diseases and Other Pathologies of the Anterior and Posterior Eye Segments in Adults. Oxid Med Cell Longev. 2016, 2016, 3164734. [Google Scholar] [CrossRef]
- Paul, R.G.; Bailey, A.J. Glycation of collagen: the basis of its central role in the late complications of aging and diabetes. Int J Biochem Cell Biol. 1996, 28, 1297–1310. [Google Scholar] [CrossRef]
- Naderan, M.; et al. Association between diabetes and keratoconus: a case-control study. Cornea 2014, 33, 1271–1273. [Google Scholar] [CrossRef] [PubMed]
- Mathan, J.J.; Gokul, A.; Simkin, S.K.; Meyer, J.J.; Patel, D.V.; McGhee, C.N.J. Topographic screening reveals keratoconus to be extremely common in Down syndrome. Clin Exp Ophthalmol. 2020, 48, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Rabbanikhah, Z.; Javadi, M.A.; Rostami, P.; Aghdaie, A.; Yaseri, M.; Yahyapour, F.; Katibeh, M. Association between acute corneal hydrops in patients with keratoconus and mitral valve prolapse. Cornea. 2011, 30, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Zeigler, S.M.; Sloan, B.; Jones, J.A. Pathophysiology and Pathogenesis of Marfan Syndrome. In: Advances in Experimental Medicine and Biology. Springer; 2021. p. 185–206. [CrossRef]
- Burnei, G.; Vlad, C.; Georgescu, I.; Gavriliu, T.S.; Dan, D. Osteogenesis imperfecta: diagnosis and treatment. J Am Acad Orthop Surg. 2008, 16, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.R.; Turner, M.L.; Hoppe, C.; Kong, A.W.; Barnett, J.S.; Kaur, G.; et al. Parental Keratoconus Literacy: A Socioeconomic Perspective. Clinical Ophthalmology. 2022, 16, 2505–2511. [Google Scholar] [CrossRef]
- Li, X.; Yang, H.; Rabinowitz, Y.S. Keratoconus: Classification scheme based on videokeratography and clinical signs. J Cataract Refract Surg. 2009, 35, 1597–1603. [Google Scholar] [CrossRef]
- Chastang, P.J.; Borderie, V.M.; Carvajal-Gonzalez, S.; Rostène, W.; Laroche, L. Automated keratoconus detection using the EyeSys videokeratoscope. J Cataract Refract Surg. 2000, 26, 675–683. [Google Scholar] [CrossRef]
- Fourmaux, E.; Riss, I.; Dupuy, B.; Le Rebeller, M.J. Fiabilité et reproductibilité du système d’analyse topographique cornéenne Eyesys [Accuracy and reproducibility of the Eyesys corneal topographic analysis system]. J Fr Ophtalmol. 1994, 17, 343–348. [Google Scholar]
- Koch, D.D.; Foulks, G.N.; Moran, C.T.; Wakil, J.S. The Corneal EyeSys System: accuracy analysis and reproducibility of the first-generation prototype. Refract Corneal Surg. 1989, 5, 424–429. [Google Scholar] [CrossRef]
- Martin, R. Cornea and anterior eye assessment with placido-disc keratoscopy, slit scanning evaluation topography and scheimpflug imaging tomography. Vol. 66, Indian Journal of Ophthalmology. Medknow Publications; 2018. p. 360–6. [CrossRef]
- Kaushal, J.; Mahajan, P. Asia’s largest urban slum-Dharavi: A global model for management of COVID-19. Cities (London, England) 2021, 111, 103097. [Google Scholar] [CrossRef]
- https://www.census2011.co.in/census/metropolitan/305-mumbai.html#google_vignette.
- Manasi, D.; Ashish, N.; Amit, G. Evolution of Heat Index (HI) and Physiological Equivalent Temperature (PET) Index at Mumbai and Pune Cities, India. MAUSAM 2021, 72, 915–934. [Google Scholar] [CrossRef]
- Woodward, M.A.; Blachley, T.S.; Stein, J.D. The association between sociodemographic factors, common systemic diseases, and keratoconus an analysis of a nationwide heath care claims database. Ophthalmology. 2016, 123, 457–465.e2. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ROC analysis of KRIS for KC suspect detection.
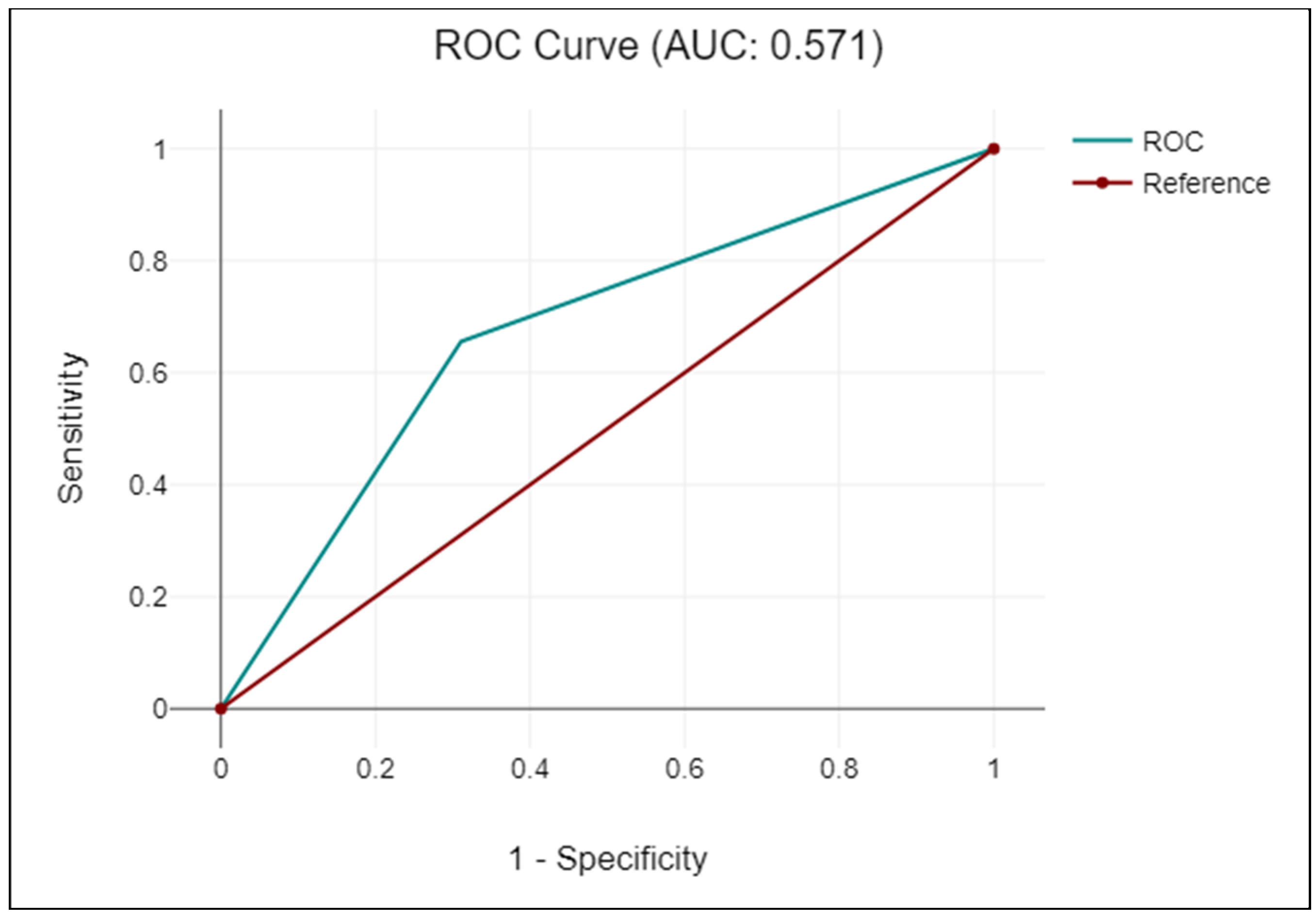
Figure 2.
Proportion of responses for each risk factor amongst false positive cases.
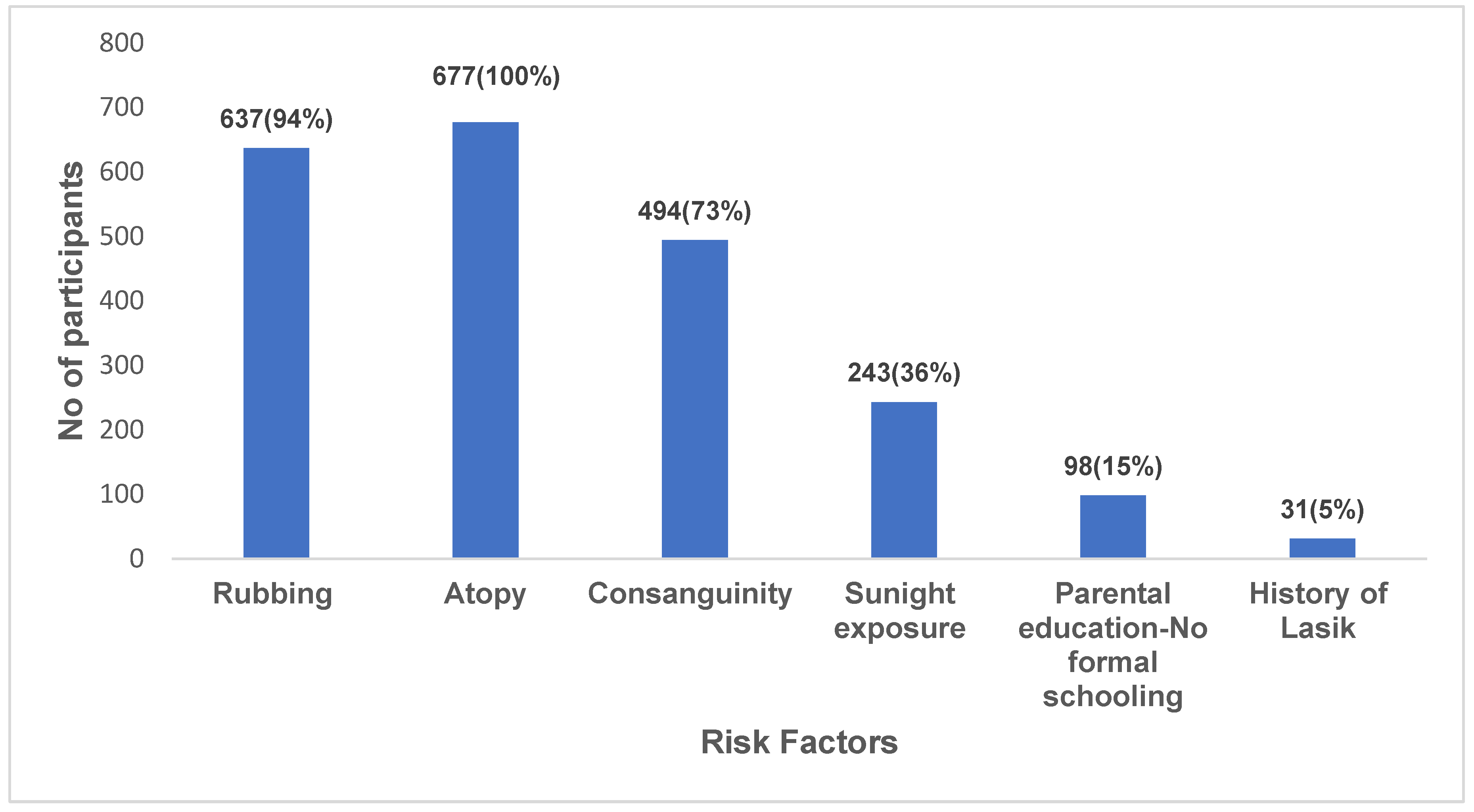

Table 1.
Clinical cut-off criteria applied in the identification of KC.
| KC criteria | Objective parameter | Cut off value | Description |
|---|---|---|---|
| Topography | Mean K | >47.2 D | Mean of flat and steep meridians (Modified Rabinowitz/McDonnell index) (18) |
| I-S value | ≥1.4 D | Power difference between the superior and inferior cornea. (Modified Rabinowitz/McDonnell index) (18) | |
| SAI value | 1.25 | Average corneal power derived from 128 corneal meridians (19). | |
| Asymmetric bow tie pattern | Present | Topographic pattern in KC and subclinical KC. (Huseynli and Abdulaliyeva) (20). | |
| Keratometry (K) | Mean K | ≥47 | Rabinowitz criteria (16) |
| Retinoscopy | Scissor Reflex | Present | A scissoring retinoscopy reflex; (Al-Mahrouqi et al.) (21). |
| Refractive profile | Refractive error | >-5D Myopia and/or Astigmatism | [Amsler’s Krumeich criteria (22). |
| Irregular Astigmatism | >1.5 dioptres(D) | (Huseyin et al.) (23). |
Table 2.
Demographic profile of the study sample.
| Demographic profile | Predictor | N | % |
|---|---|---|---|
| Age | 9-12 | 1038 (11.08 ± 0.88) | 51 |
| 13-17 | 1004 (13.81 ± 0.9) | 49 | |
| Total | 2042 (12.46±1.7) | 100 | |
| Sex | Female | 1348 | 66 |
| Male | 694 | 34 | |
| Religion | Muslim | 1043 | 51 |
| Hindu | 982 | 48 | |
| Christian | 3 | 0.15 | |
| Buddhist | 6 | 0.3 | |
| Jain | 7 | 0.34 | |
| Unknown | 1 | 0.05 |
Table 3.
Demographic and risk factor correlation between KRIS and clinically identified KC suspects.
Table 3.
Demographic and risk factor correlation between KRIS and clinically identified KC suspects.
| Risk Factors | Variable | KRIS | Prevalence (%) | Clinical | Prevalence (%) | p-value | Spearman |
|---|---|---|---|---|---|---|---|
| (n=728) | (n=51) | ||||||
| Age | 9-12 13-17 |
415 313 |
57 43 |
26 25 |
51 49 |
<0.001* | 1 |
| Gender | Male Female |
199 529 |
27 73 |
15 36 |
29 71 |
<0.001* | 0.92 |
| Religion | Hindu Muslim |
192 531 |
26 72 |
28 22 |
55 43 |
0.06 | 0.36 |
| Socio--economic Status | <1 lac 1-3 lac > 3lac |
402 265 61 |
55.2 36.4 8.38 |
16 27 8 |
31.3 53 16 |
0.5 | 0.1 |
| Consanguinity | Yes No |
514 214 |
70.6 29.4 |
21 30 |
41 59 |
<0.001* | -0.09 |
| Eye rubbing | Yes No |
688 40 |
94.5 5.5 |
51 0 |
100 | 0.04* | 0.24 |
| Atopy | Yes No |
715 13 |
98.2 1.8 |
51 0 |
100 | <0.001* | 0.49 |
| > 8 hours of sunlight exposure | Yes No |
251 477 |
34.5 65.5 |
5 46 |
9.8 | 0.002* | 0.11 |
| Diabetes and other medical conditions | Yes No |
51 677 |
7 93 |
1 50 |
2 98 |
<0.001* | 0.14 |
|
Parental education |
No formal schooling Formal schooling |
102 626 |
14 86 |
3 48 |
6 94 |
<0.001* |
0.16 |
| Lasik | Yes No |
33 695 |
5 95 |
1 50 |
2 98 |
< 0.001* | 0.17 |
| Family history | Yes No |
27 701 |
4 96.28 |
0 51 |
0 100 |
1 | 0 |
*Denotes statistical significance.
Table 4.
Diagnostic accuracy of the KRIS for KC suspect detection according to performance metrics and kappa coefficient.
Table 4.
Diagnostic accuracy of the KRIS for KC suspect detection according to performance metrics and kappa coefficient.
| KRIS | KC | Non-KC | Sensitivity | Specificity | PLR | NLR | Accuracy | Kappa-coefficient |
|---|---|---|---|---|---|---|---|---|
| Positive | 51 | 677 | 69 | 66 | 2 | 0.47 | 66 | 0.1 |
| Negative | 23 | 1291 | (95% CI: 57.1 -79.7) | (95% CI: 63.5 -67.7) | (95% CI: 1.7 -2.3) | (95% CI: 0.34 -0.67) | (95% CI: 63.6 -67.7) |
Positive Likelihood Ratio [PLR], Negative Likelihood Ratio [NLR].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



