Submitted:
02 November 2024
Posted:
06 November 2024
You are already at the latest version
Abstract
Postpericardiotomy syndrome involves the development of pericardial and pleural effusion following open cardiac surgery. To date, it is not completely understood why it is more likely to develop after atrial septal defect closure. This case-based brief report describes a discrepancy in the conduit and reservoir components of atrial functions by speckle tracking echocardiography in a case following ASD closure compared to another case who had a repair of mitral cleft. This finding was associated with a mild effusion developing in ASD postoperative case. Despite the limited proofs brought by these two cases, it should encourage the implementation of larger cohort studies, testing atrial functions by STE, in patients after ASD closure, and calculating the diagnostic accuracy of different components of atrial functions in predicting PPS development.
Keywords:
ASD
; postpericardiotomy syndrome
; atrial speckle tracking
Background
Postpericardiotomy syndrome (PPS), or Dressler’s syndrome, is a de-novo or worsening pericardial effusion occurring up to six weeks following cardiac surgery. There is a wide variation of the reported incidence of 2-30%, which might reflect its heterogeneity depending on the cardiac pathology implicated. While it is typically a benign disorder, it can have life-threatening complications, such as cardiac tamponade, and lifelong impact by evolving into constrictive pericarditis [1].
Researchers have suggested that the highest likelihood of PPS is seen after surgical closure of Atrial Septal Defects (ASD). To date, the most accepted explanation is that the chronic increase in the right atrial pressure leads to venous congestion and is markedly accentuated after ASD closure, this statement remains largely hypothetical [2,3]. Speckle tracking echocardiography (STE) has recently allowed the analysis of different components of atrial functions. These include reservoir function, which is the ability of the atrium to relax and fill adequately; conduit function, which reflects the ability of the right atrium to respond to the negative ventricular pressure and empty most of its blood in early diastole; and finally, contractile function, which occurs in late diastole. The aim of this case-based report is to shed light on the ability of atrial functions to explain the higher prevalence of PPS after ASD closure [4].
Cases Comparison
This report compares postoperative atrial functions in two patients of the same age: one following ASD surgical closure and the other after a mitral valve cleft, to determine if there is a significant difference in atrial function analysis following the surgical procedure.
Cases were assessed following cardiac surgery (1 week postoperatively) using GE E95 machine, using 5 MHz probe, an apical view (four-chamber) was acquired showing the roof and full circumference of the right atrium. Examination was ECG-gated [5].
Following acquisition, the left atrial automated functional imaging function was activated, but used for delineation of the right atrium, by placing a point on the right atrial septal base, right atrial free wall base and at the center of right atrial roof. The software automatically deducted the reservoir, conduit and contractile function of right atrium in the two cases.
The case with surgical ASD closure, had a small rim of effusion at follow-up which slightly increased in follow-up, and resolved on adequate diuresis.
Right Atrial Functions Are Shown in Figure 1A and Figure 1B.
Table 1 Summarizes the Findings of Figure 1 A and B
Despite successful surgical results and myocardial functions, the Right Atrial (RA) conduit function is noticeably reduced, reflecting the lack of passive atrial shortening, and the reservoir function is mildly reduced. Notably, the impaired passive shortening is compensated by an exaggerated atrial kick compared to the patient who has not undergone ASD closure.
Discussion
ASD surgical closure is associated with the highest rate of postpericardiotomy cases, but the exact cause remains unclear. New automated software assessing right and left atrial functions can provide potential insights. A study by Hajizeinali demonstrated that all right atrial functions are impaired after surgical closure of ASD, this has not been correlated with the development of effusion in a short-term follow-up of the study subjects [6]. Two series by Taficiu and Ritcher showed that impaired RA functions can lead to systemic venous congestion. In the cases displayed in this brief report, the case with surgical closure of ASD showed poor RA conduit and reservoir functions, and a starting rim of pericardial effusion, which increased slightly in subsequent follow-up [7,8]. The pericardial patch used in surgical closure of these defects may impair the kinetics of the right atrium, leading to reduced relax-ability and limited atrial shortening as an immediate short-term consequence.
Conclusions
This brief report highlights the importance of right atrial strain assessment to determine the reason behind the heterogeneous prevalence of effusions after ASD surgical closure compared to other types of open heart surgery. Our findings suggest that right atrial function involvement occurs to a greater extent after surgical ASD closure compared to another open cardiac surgery with an untouched atrial septum. It remains to be elucidated through case-control cohort studies, whether this functional impairment is linked to the development of postpericardiotomy syndrome in respective cases.
Author Contributions
Conceptualization, AFA; Methodology, ; software, AFA, WH, SA, TA, BK investigation, AFA, WH, SA, TA, BK, BH; resources, AFA, WH, SA, TA, BK, BH, data curation, AFA, WH, SA, TA, BK, BH; writing—original draft preparation, AFA, WH, SA, TA, BK, BH; writing—review and editing, AFA, WH, SA, TA, BK, BH; supervision, AFA; project administration, AFA; funding acquisition, (none) All authors have read and agreed to the published version of the manuscript.”
Declarations: Institutional Review Board Statement
IRB has been obtained from the Ethical committee of SKMC
Informed Consent Statement
a consent has been taken from the legal guardians of the two patients
Data Availability Statement
ll data is made available within the manuscript.
Acknowledgement
To those who never give up. Those who constantly try and are not ashamed of their defects or deficiencies. The world is changed by perseverance not by genius.
Conflicts of Interest
The authors declare no conflict of interest. The manuscript is submitted under Creative Commons Licensing CC-BY-NC-ND.
List of Abbreviations:
| ASD | Atrial Septal Defect |
| CD | Conduit |
| CT | Contractile |
| ECG | Electrocardiogram |
| ECG | Electrocardiogram |
| GE | General Electric |
| LA | Left Atrium |
| PPS | Postpericardiotomy syndrome |
| R | Reservoir |
| RA | Right Atrium |
| S | Strain |
| STE | Speckle tracking echocardiography |
References
- Lehto J, Kiviniemi T (2020) Postpericardiotomy syndrome after cardiac surgery. Ann Med 52:243–264. [CrossRef]
- Campisano M, Celani C, Franceschini A, Pires Marafon D, Federici S, Brancaccio G, Galletti L, De Benedetti F, Chinali M, Insalaco A (2022) Incidence and predictors of pericardial effusion following surgical closure of atrial septal defect in children: A single center experience. Front Pediatr 10:1–8. [CrossRef]
- Heching HJ, Bacha EA, Liberman L (2015) Post-Pericardiotomy Syndrome in Pediatric Patients Following Surgical Closure of Secundum Atrial Septal Defects: Incidence and Risk Factors. Pediatr Cardiol 36:498–502. [CrossRef]
- Inoue K, Kawakami H, Akazawa Y, Higashi H, Higaki T, Yamaguchi O (2022) Echocardiographic Assessment of Atrial Function: From Basic Mechanics to Specific Cardiac Diseases. J Cardiovasc Dev Dis 9:1–15. [CrossRef]
- Cacciapuoti F, Cacciapuoti F, Caturano M, Paoli V, Scognamiglio A (2015) Left atrial longitudinal speckle tracking echocardiography in healthy aging heart. J Cardiovasc Echogr 25:39. [CrossRef]
- Hajizeinali A, Iri M, Hosseinsabet A (2019) Assessment of the Right and Left Atrial Functions at Midterm After Surgical and Device Atrial Septal Defect Closure: A 2-Dimensional Speckle-Tracking Echocardiographic Study. J Ultrasound Med 38:1979–1993. [CrossRef]
- Tafciu E, Niro L, Iseppi M, Fanti D, Maffeis C, Bergamini C, Benfari G, Rossi A, Ribichini FL (2023) Right Atrial Function Role in Tricuspid Regurgitation-Related Systemic Venous Congestion. Am J Cardiol 204:320–324. [CrossRef]
- Richter MJ, Zedler D, Berliner D, Douschan P, Gall H, Ghofrani HA, Kimmig L, Kremer N, Olsson KM, Brita da Rocha B, Rosenkranz S, Seeger W, Yogeswaran A, Rako Z, Tello K (2021) Clinical Relevance of Right Atrial Functional Response to Treatment in Pulmonary Arterial Hypertension. Front Cardiovasc Med 8:. [CrossRef]
Figure 1.
A: Right atrial functions assessment in a patient following a non-ASD cardiac surgery (mitral cleft closure). B: Right atrial functions assessment four days following post-ASD closure, presenting a small rim of pericardial effusion developing in the vicinity of the right atrium.
Figure 1.
A: Right atrial functions assessment in a patient following a non-ASD cardiac surgery (mitral cleft closure). B: Right atrial functions assessment four days following post-ASD closure, presenting a small rim of pericardial effusion developing in the vicinity of the right atrium.
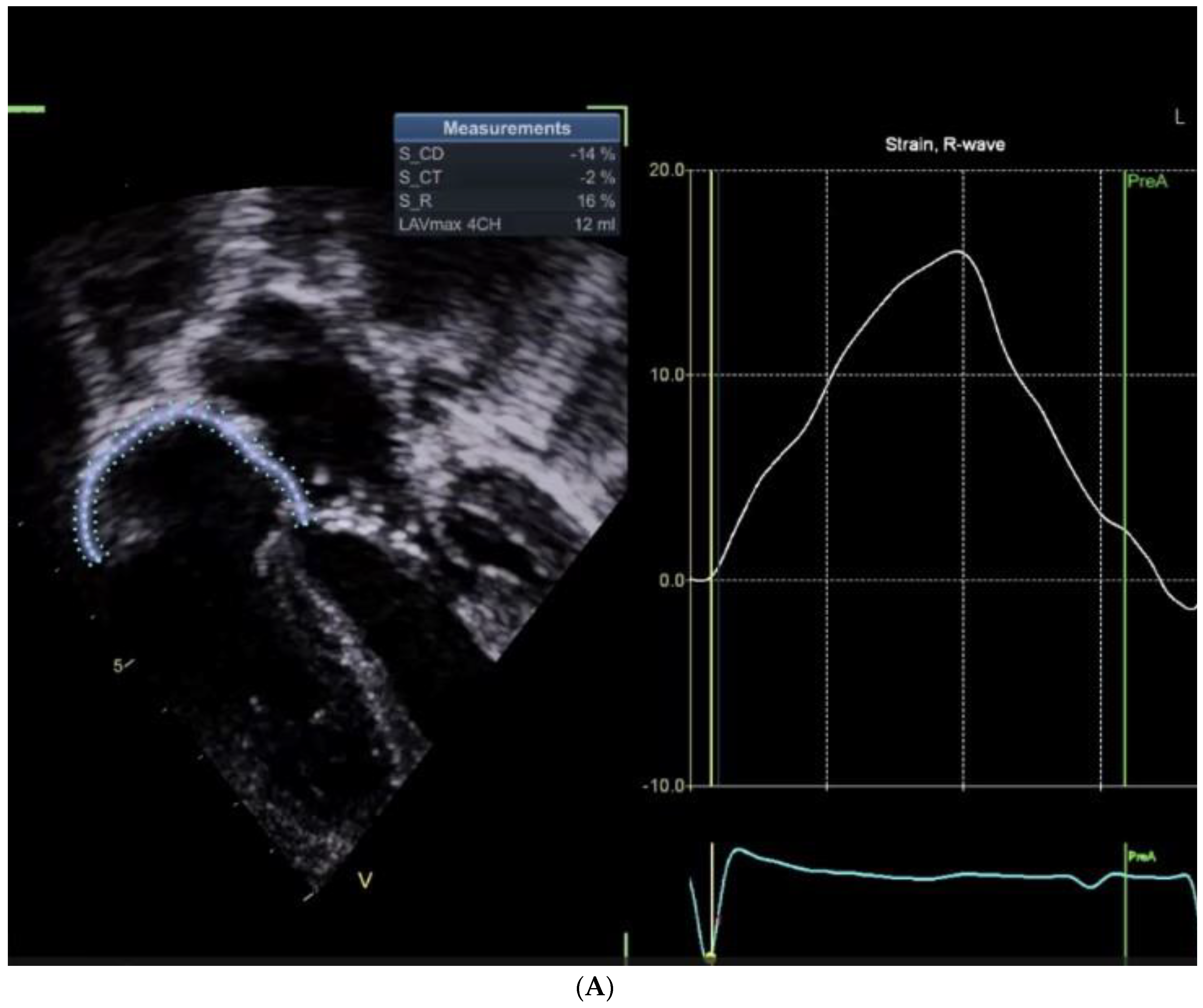
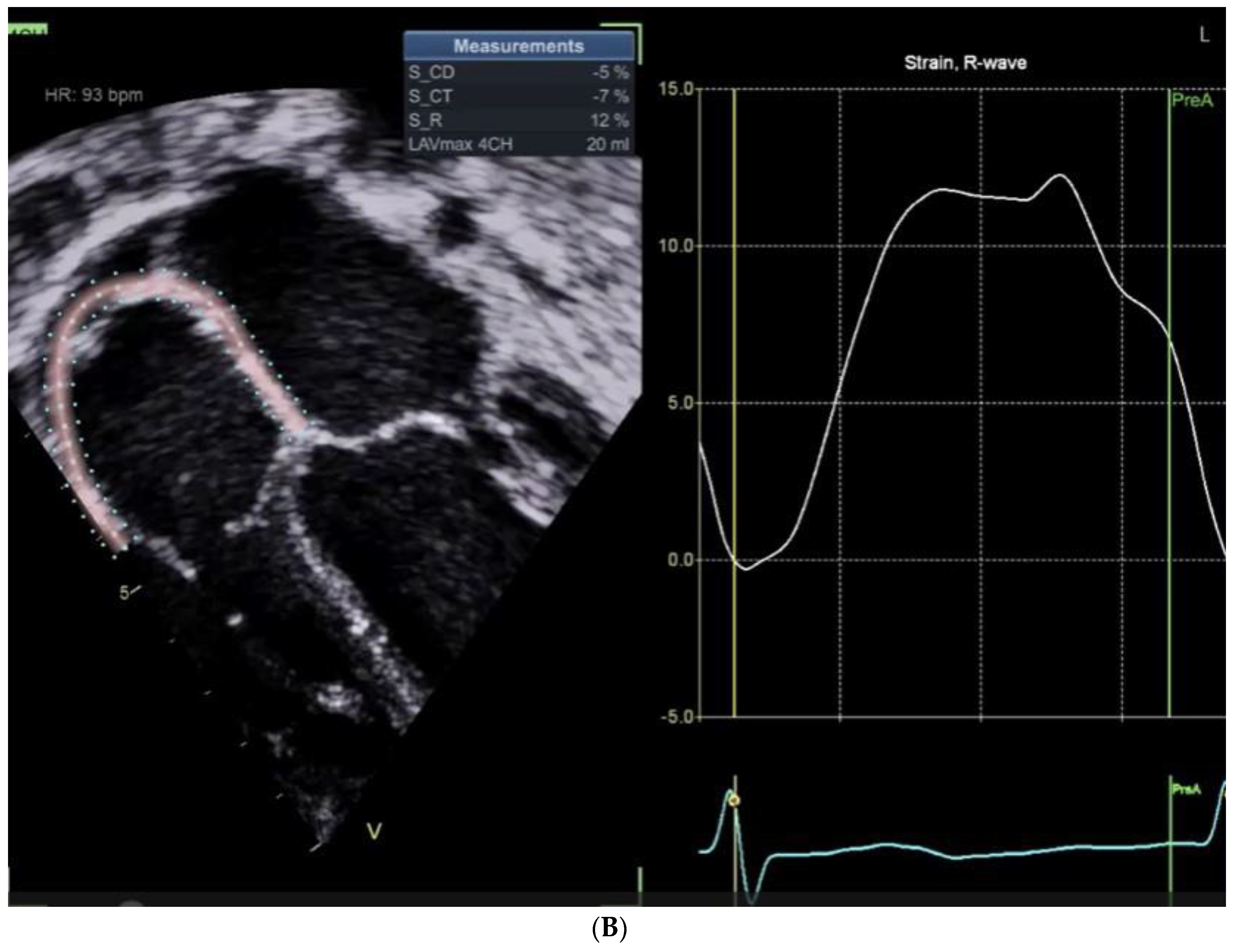

Table 1.
Summary of atrial functions in the two studied cases.
| S/P ASD Closure | S/P Mitral valve repair | Cut-offs (Absolute values) |
|
|---|---|---|---|
| Conduit | -5 | -14 | >11% |
| Reservoir | 12 | 16 | >18-22% |
| Contractile | -7 | -2 | >8-12% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



