
Submitted:
07 September 2025
Posted:
08 September 2025
You are already at the latest version
Abstract
Objective: Chronic low back pain (CLBP) is a significant global concern. Its prevalence is increasing, and current management strategies demonstrate, at best, moderate effectiveness. The purpose of this study was to explore the concept of uncertainty tolerance and how it affects an individual’s ability to hope, as well as how both of these factors influence emotion regulation. These concepts are extremely prevalent for patients and clinicians during CLBP consultations. Methods: A social constructivist meta-ethnographic study is a highly interpretative type of qualitative review that generates new theory, enabling valuable insights into this unique area of pain management. A framework was followed; its iterative analytical process involves multiple search strategies in accordance with PRISMA checklists, exploring how studies relate, generating ideas and ultimately developing a substantive theory. Results: This review represents the first worked example of a theory generating review process. One model was created that focuses on how an individual with CLBP regulates their emotions, which also considers factors that influence and result from the process. The outcome of the model produced either adaptive or maladaptive emotional regulation strategies. Conclusions: Tolerance of uncertainty and ability to hope are key concepts that influence emotion regulation and play a vital role in the physical and psychological well-being of people with CLBP. Research is required to explore how the model can be operationalised in clinical practice.
Keywords:
Chronic low back pain
; hope
; uncertainty
; emotion regulation
; social constructivist meta-ethnography
1. Introduction
Chronic low back pain (CLBP) is one of the most prevalent musculoskeletal conditions globally, defined as pain lasting more than three months and beyond typical recovery time [1,2]. Its prevalence has steadily increased since the 1990s and is expected to continue rising, significantly affecting individuals’ physical and psychological well-being, as well as society [3]. Current management strategies recommend a combination of physical and psychological approaches, but their effectiveness is moderate at best, with supporting evidence of low quality [4,5,6,7,8,9]. Pain is a complex phenomenon involving neurophysiological and psychological components [10]. In 2021, the International Association for the Study of Pain redefined pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [11]. Understanding pain requires exploring interrelated psycho-emotional constructs—uncertainty, emotion regulation, and hope—which are particularly relevant in CLBP. This article examines these constructs and their implications for theory and practice in this patient group.
Uncertainty is closely linked to CLBP due to its complexity [12]. It is defined as a cognitive state arising from encountering ‘an unknown’ or a perceived absence of information ([13], p. 71), which reduces one’s ability to predict outcomes and sense of control, often triggered by inconsistent symptoms or unfamiliar events [14]. Qualitative studies show that people with CLBP frequently feel uncertain about their diagnosis, symptom management, and the condition’s impact on self-identity and future [3,15,16,17]. Uncertainty affects emotional responses and regulation, influencing mental and physical well-being [18]. Although emotion remains a debated concept, it is generally understood as a time-limited physiological state shaped by personal experience, appraisal, and behavioural expression [13,18]. Several neural systems are involved in emotion activation, which varies depending on the stimulus and individual response [19]. Emotional responses are especially important in patient–clinician interactions, where poor uncertainty tolerance can impair problem-solving and increase distress [20].
Intolerance of uncertainty is defined as “a dispositional inability to endure the discomfort caused by missing key information” ([13], p. 3), and can manifest cognitively (e.g., negative interpretation), emotionally (e.g., worry), and behaviourally (e.g., avoidance) [20,21]. Initially linked to generalised anxiety disorder [22], it is now recognised as a transdiagnostic construct across psychological disorders [23]. The intolerance of uncertainty model explains its association with worry through three mechanisms: positive beliefs about worry, negative problem orientation, and cognitive avoidance [24]. However, the model does not fully explain individual responses to different types of uncertainty or which aspects are most difficult to manage. Responses to intolerance of uncertainty are shaped by prior experiences, including childhood development, attachment security, cogntivity flexibility and sociocultural influences [12,23,25]. Further development of models addressing uncertainty in CLBP interactions would be valuable especially given the complexity of assoication between different inter-related constructs.
The ability to regulate emotions is essential for managing life’s challenges and significantly influences mental and physical well-being [19]. Although emotion regulation has been widely studied in behavioural and neuroscience research [2,19,26], its application to chronic pain is relatively recent. Emotion regulation involves consciously or automatically adjusting one’s emotional state using emotion regulation strategies (ERS) [15]. These strategies are broadly classified as explicit (deliberate) or implicit (automatic) [19]. Explicit regulation includes conscious efforts such as reappraisal, valuing the present, or choosing to hope [27]. Implicit regulation operates unconsciously, including automatic responses to stimuli or goal-directed behaviours without awareness—e.g., making healthier choices or walking more by parking further away [25]. Automatic responses may involve re-evaluating stimuli based on new experiences (e.g., a sound once linked to a negative event losing its impact over time when no longer associated with that event). Controlled implicit processes can guide behaviour toward goals without conscious intent. These nonconscious goals are especially important under stress [25]. Ultimately, different ERS are driven by distinct neural systems, resulting in varied behavioural outcomes [19], which is important to understand in healthcare professional–patient interactions.
Interactions between healthcare professionals and patients with CLBP are strongly influenced by perceptions of possibility or uncertainty. The ability to identify a positive future and maintain hope depends on an individual’s tolerance of uncertainty and emotional regulation. Healthcare professionals must be aware of these concepts, as they can negatively affect how patients view their future [27]. Close attention is needed to understand how uncertainty and hope are managed in clinical interactions [28]. Clinicians should recognise that establishing hope fosters optimism and positive emotions such as joy and anticipation, acting as a protective factor for mental health [29]. Other protective factors include the use of cognitive strategies and cogntive flexibility (being able to adapt ones thinking) in order to establish meaninful goals [27,28]. Conversely, uncertainty can lead to a perception of hopelessness and negative emotions, resulting in poor psychological outcomes such as severe depression, and in some cases, distant thoughts or fantasies about death as an escape from persistent pain [30,31]. This may be particularly important at times of onset, exacerbations, when waiting for change, undertainty about the change or when a peperception of failure to achieve occurs or a predetermined future is identified [27]. Research on hope has primarily focused on non-chronic pain populations, such as cancer, ageing, and chronic illnesses like heart disease and multiple sclerosis, consistently showing that higher levels of hope correlate with greater pain tolerance, improved physical health, and psychological well-being [32,33]. Only recently have uncertainty and hope begun to be explored in chronic pain populations, particularly in chronic musculoskeletal conditions [3,33]. Hope plays a vital therapeutic role in healthcare by improving prognostic and behaviour-related outcomes [34], and serves as a key component of patients’ coping mechanisms [30]. If healthcare professionals can effectively navigate uncertainty, foster possibility, and support patient hope during CLBP consultations, they may deliver more tailored and potentially therapeutic care [28].
There is a complex relationship between hope, uncertainty, and emotion regulation that requires further understanding conceptually in order to benefit interactions between healthcare professionals and patients with CLBP. Although research on emotion regulation in chronic pain is limited, it highlights the importance of both implicit and explicit regulation and its relevance to chronic pain, warranting further investigation [26,35]. To date, no studies have explored how factors that influence uncertainty may be understood within a single model and process that related to interaction. Addressing this gap requires a theory-generating review. Social constructivist meta-ethnography is a new methodology designed to develop substantive theory [36]. Therefore, this study aimed to explore uncertainty tolerance, its impact on hope, and how both influence emotion regulation in people with CLBP, using the social constructivist meta-ethnography framework.
2. Methods
The methodology used in this study was social constructivist meta-ethnography, a modified version of the traditional meta-ethnography framework. It incorporates phases from social constructivist grounded theory to ensure analytical generalisability and support critical enquiry [36]. This is important because the traditional version of meta-ethnography often results in a poorly considered model or process as an output [37]. In contrast the social constructivist meta-ethnography uses iterative analytical proceese and techniques orginally derived from social contructivist grounded theory to ensure a substantive theory or process as an output. Moreover, in the later stages of the analytical process, the theory or model also undergoes rigorous testing and modifications until theoretical saturation is reached, bringing rigour [36]. As such this methodology generates a theory that is co-created from the literature and inevitably the authors interpretations, biases, and experiences [38]. However, the potential value is the ability to challenge current thinking and generate analytical generaslisability [39]. The reader is encouraged to use the framework [36] to understand the choices and phases in more detail. The researcher’s philosophical position is social constructivism; this paradigm is situated as having a pragmatic ontological stance and a relativist epistemology [36].
2.1. Protocol and Registration
The protocol for this study was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on 05/01/2024 (registration number CRD42024493925), and was updated throughout the process to reflect the inevitable changes to the research questions and eligibility criteria due to the nature of this methodology, as previously discussed.
2.2. Initial Eligibility Criteria
Studies were considered for inclusion by two blind reviewers using Covidence© (JM/AS). Studies were included if they used a sample of adults (aged over 18 years) with CLBP (low back pain persisting for more than three months). For studies that used a small sub-group of participants with acute LBP as a comparison, (n=3), a discussion was undertaken between reviewers to consider the study, the sample, its contribution to the model and whether it should be included. All studies three studies were included. Additionally, for any study in which all participants were not over the age of 18 years (n=1), a similar process and discussion was undertaken. This study was included as only one particiapant was under 18 years. Only studies that were written in English were included, and no date restriction was applied. Lastly, studies must have used either used an outcome when considered the phenomena of hope, or discussed the concept of hope from the perspective of the individual with CLBP in the results section. Studies that explored the experience of an intervention to improve hope were not included.
Due to the nature of the methodology, additional searching was required. This was due to the iterative processes involved in the methodology and the need to challenge the development of a substantive theory and help ensure theoretical saturation. Please see Step 2 in Figure 2 (Section 2.7 Synthesis) for details on the process. In brief, two additional complete systematic searches were undertaken by the same two blind reviewers (JM/AS) on the concepts of uncertainty, and then later on the emotion regulation (Step 5, Figure 2). Total search numbers for all additional searching described here is included in each PRISMA flow diagram.
2.3. Search Strategy for Qualitative Literature
The key requirement of meta-ethnography is to bring together qualitative studies on a particular topic. In the current review, a total of three systematic literature searches were undertaken blind by both authors and supported by the Covidence© software on 20 May 2025. All searches were identified as being able to cover experiences of the three major concepts inputting into the model. The primary search associated with the initial eligibility criteria is as follows: Databases searched were: MEDLINE, CINAHL Plus, AMED, ERIC, SPORTDiscus and the Hope-Lit database. In addition, the first 10 pages or 100 articles on electronic search engines such as Google Scholar and ScienceDirect were screened. Grey literature was searched using the GreyMatters search engine. Standard Boolean operators were used. Keywords included: hope, hopelessness, hope scale, chronic low back pain, non-specific low back pain, persistent low back pain, pain management, pain reduction, quality of life, but excluded optimism - as this is a more general belief that things will work out for the best and is considered a different construct [29]. The same databases and search engines were used for the subsequent two searches. Keywords for the second systematic search included: uncertainty, uncertain, intolerance of uncertainty, possibility and chronic low back pain, non-specific low back pain, persistent low back pain. Lastly, keywords for the third systematic search included: emotion regulation, emotion dysregulation, regulation of emotion, chronic low back pain, non-specific low back pain, persistent low back pain. Further details of all systematic searches are outlined in the audit trail (see Supplementary File A).
2.4. Study Selection and Data Extraction Approach
Duplicates were identified via the Covidence software©. Articles were screened and selected independently by both authors by reading the title and abstract, followed by the full text. Conflicting decisions were resolved and justifications for study exclusions are provided in the audit trail (see Supplementary File A). Table 1, Table 2 and Table 3, in Section 3.1 ‘Search Outputs’, summarise the demographic details of the originally included empirical studies.
2.5. Quality of Included Articles
Soundy [36] identifies that four principal questions should be considered regarding the included studies in order to meet the aims of critical enquiry. The questions are: (a) Are considerations and information given by the selected articles made sufficiently well so that concepts can be translated? (b) Do findings provide a context for the culture, environment, and setting? (c) Are the findings relevant and useful given the focus or aims of the analysis now? (d) Do the questions asked or aims from the paper selected align with those sought by the meta-ethnographer? (e) To what extent do the findings give theoretical insight and context of interpretation made? The quality scores of included articles can be found in Table 4 in Section 3.2 ‘Quality Considerations’.
2.6. Generalisability of Results and Searching for Conceptual Models That May Assisst Analytical Generalisbility
The topic of generalisation within qualitative research is greatly debated, which is largely influenced by the researcher’s philosophical worldview [40]. The focus of this study was to generate a substantive theory and achieve analytical generalisability by using a framework that draws on iterative phases of theory development [36]. This type of generalisation draws conclusions from singular studies which are then used to develop a broader theory that is co-created with the main researcher’s interpretation, experiences, and biases [40]. To enhance, expand and challenge the model created literature was identfied which represented concepts that may help explain, influence or represent an outcome from an uncertain of unkown situation. This resulted in the model expressed and refined 10 times (see Supplementary File for the 10 different versions of the model) as the identification and testing of different aspects and elements of the model we identified. From the qualitative synthesis the following concepts were explored, examined and justified for their inclusion for the main theory including cognitive flexbility, emotional regulation, BAS activation, predispositing factors including (patient history) and hope. This was to ensure literature already included in the review (containing some individuals with acute low back pain) could be examined with implications provided for the model. As part of illustrating a worked example, the entire analytical process is clearly outlined- with justifications- in the audit trail (see Supplementary File A) to enhance transparency for the reader.
2.7. Synthesis
An eight-step approach was used (see Figure 1), based on the social constructivist meta-ethnography framework [36]. A detailed account of this process can be found in the audit trail (see Supplementary File A).
As outlined in Step 2 of the synthesis process (see Figure 1), the initial articles exploring hope were reviewed and coded which gave light to a possible link with uncertainty. This theme was sub-categorised into: diagnostic uncertainty, prognostic uncertainty and the individual’s beliefs or perceptions about the unknown. These findings support Mishel’s theory on uncertainty in healthcare, which states that, regardless of the underlying health condition, uncertainty arises when individuals cannot cognitively appraise information about the state of their illness – particularly if the course of the disease is unpredictable, or when there is a lack of information about the diagnosis and/or prognosis [41]. Moreover, Soundy et al. [30] who developed a framework for hope, also recognised that hope is particularly challenged at the time of onset, during periods of change, or in the presence of uncertainty. Therefore, this represented a critical turning point in the analytical process, and the concept of uncertainty became a new line of enquiry and represented a phenomena which was critical to the development of an substantive theory.
The eligibility criteria was expanded to include the discussion of uncertainty in the results section, and a second systematic search was undertaken for the same population. After immersive reading and coding of these articles, four key psychosocial themes emerged based on uncertainty which were: 1) Their beliefs about the unknown, 2) The clinical encounter and diagnosis, 3) The impact on their self-identity, social relationships, and future, and 4) Treatment failure. Subsequently, how the patient-clinician interaction can influence these areas of uncertainty, either positively or negatively, was explored. Following this, it was important to establish intrinsic factors such as personality traits, and pre-existing conditions, such as emotional disorders or neurodevelopmental conditions, that can predispose an individual to be less tolerant of uncertainty and to explore how their ERS differs from those without such conditions. As a result, a third systematic search exploring the concept of emotion regulation within people with CLBP was undertaken. Figure 2, Figure 3 and Figure 4 presents the PRISMA flow diagrams that outlines the approach for each systematic search (further details of the search process can be found in Supplementary File A).
3. Results
3.1. Search Outputs
Due to the inductive nature of this methodology, multiple searches are outlined in the methods section to demonstrate the evolution of the search strategy and how it was rigorously tested. A summary of the articles from the systematic searches undertaken is given here. Across all three searches, the total number of articles was 23; this included5 articles related to hope, 12 articles related to uncertainty and 6 articles related to emotion regulation. These articles used 1,991 individuals (796 male, 1,195 female, 0 unknown) with an average age of 46.1 years (n=18/23 studies and 1866 participants) were considered. This broke down to include a total of 246 individuals (116 male, 130 female, 0 unknown) were included in the first search exploring the concept of hope (See Table 1). A total of 1,070 individuals (379 male, 691 female, 0 unknown) were included in the second search on uncertainty (See Table 2). A total of 675 individuals (301 male, 374 female, 0 unknown) were included in the final search exploring the concept of emotion regulation (see Table 3). Only 8 of the 22 studies specified the ethnicity of participants. Data was obtained from a range of countries with USA being the most common (n=7) and the UK (n=4). Lastly, the most common qualitative methodology used was semi-structured interviews.

Table 1.
Social demographics for the articles from the first search on hope:.
| Article | Country | Gender | Age | Ethnicity of sample | Time with condition (LBP) | Methodology |
|
|---|---|---|---|---|---|---|---|
| Corbett, M., Foster, N. and Ong, B. (2007) [16] | UK (Keele University) |
Male | 15 | Range: 19-59 years Mean: Not stated. |
Unknown/not reported | 12+ weeks | Semi-Structured Interviews |
| Female | 22 | ||||||
| Unknown | 0 | ||||||
| Madsen et al. (2024) [34] |
Denmark |
Male | 8 | Range: 28-79 years Mean: Not stated. |
Unknown/not reported | Any duration of non-specific LBP – the study did not restrict inclusion based on pain duration, nor specify exact duration for each participant. | Semi-structured Interviews pre- and post-consultation. Setting: Primary Care |
| Female | 10 | ||||||
| Unknown | 0 | ||||||
| Stensland, M. (2021) [31] | USA | Male | 8 | Range: 66-83 years Mean: 56 years |
Non-Hispanic Caucasian |
12+ weeks | Semi structured 1:1 interviews |
| Female | 13 | ||||||
| Unknown | 0 | ||||||
| Toye and Barker (2012) [15] |
UK (Oxford) | Male | 7 | Range: 29-67 years Mean: 52 years |
Unknown/not reported | 3-23 years | Semi-structured interviews (before, after, and 1-year follow-up). |
| Female | 13 | ||||||
| Unknown | 0 | ||||||
| Wojtnya, E., Palt, L. & Popiolek, K. (2015) [43] |
Poland | Male | 78 | Range: Not stated. Mean: 50.45 years |
Unknown/not reported | 1+ year | Cross sectional study |
| Female | 72 | ||||||
| Unknown | 0 | ||||||
Table 2.
Social demographics for the articles from the second search on uncertainty:.
| Article | Country | Gender | Age | Ethnicity of sample | Time with condition (CLBP) | Methodology |
|
|---|---|---|---|---|---|---|---|
| Amja et al. (2021) [44] | Canada |
Male | 10 | Range: 26-67 years Mean: 49.3 years. |
Unknown/not reported | 5+ years (n=16) 1-5 years (n=6) |
Semi-structured interviews (via phone or video call). |
| Female | 12 | ||||||
| Unknown | 0 | ||||||
| Benjaminsson et al. (2007) [45] |
Sweden | Male | 7 | Range: 15-64 years Mean: 36 years. |
15 participants were born in Sweden 1 participant was born in Morocco 1 participant was born in Ethiopia |
Range: 6 months – 30 years. Median duration: 8years. |
Semi-structured interviews |
| Female | 10 | ||||||
| Unknown | 0 | ||||||
| Bowman, J (1994) [46] | USA | Male | 9 | Range: 27-70 years Mean: Not stated. |
Unknown/not reported | All participants had CLBP (>3months), but the exact duration for each participant was not specified. | Semi-structured interviews |
| Female | 6 | ||||||
| Unknown | 0 | ||||||
| Bunzli et al. (2015) [47] | Australia | Male | 11 | Range: 19-64 years Mean: 42 years |
Unknown/not reported | Range: 6 months – 29 years. Median duration: 7years. |
Semi-structured interviews |
| Female | 25 | ||||||
| Unknown | 0 | ||||||
| Costa et al. (2023) [17] |
Australia | Male | 5 | Range: 21-75 years Mean: 42 years |
Caucasian: 9 Latino: 2 Asian: 1 Mixed: 3 |
2-5 years (n=5) >5 years (n=10) |
Semi-structured interviews |
| Female | 10 | ||||||
| Unknown | 0 | ||||||
| Costa et al. (2023) [3] |
Australia | Male | 16 | Range: 19-85 years Mean: Not stated. |
Unknown/not reported | <3 months: 4.6% 3 months to 1 year: 6.1% 13 months to 5 years: 10.8% 6–10 years: 13.9% 11–20 years: 29.2% Over 20 years: 30.8% |
Ethnographic observations. |
| Female | 49 | ||||||
| Unknown | 0 | ||||||
| Fishbain et al. (2010) [48] | USA | Male | 149 | Range: 19-65 years Mean: 39.8 years |
White: 81.8% Black: 7.4% Asian: 0.3% Native American: 3.9% Hispanic: 6.3% Other/Unknown: = 1.8% |
>3months | Quantitative research design involving a retrospective chart review. |
| Female | 192 | ||||||
| Unknown | 0 | ||||||
| Lillrank, A. (2003) [49] | Finland | Male | 0 | Range: 20-66 years Mean: Not stated. |
Unknown/not reported | >3months | Qualitative: Narrative analysis |
| Female | 30 | ||||||
| Unknown | 0 | ||||||
| Makris et al. (2017) [50] | USA | Male |
30 | All >65 Years Mean: 83 years |
Caucasian: 51% African American: 37% Hispanic: 11% Other/multiracial: 10% |
5-10 years 26% >10years 55% |
Semi-structured interviews |
| Female | 63 | ||||||
| Unknown | 0 | ||||||
| Osborn & Smith (1998) [51] |
UK | Male | 3 | Range: 32-53 years Mean: 45 years |
White | 6-18 years | Semi-structured interviews |
| Female | 2 | ||||||
| Unknown | 0 | ||||||
| Serbic et al. (2016) [52] | UK | Male | 129 | All were >18 years. Range not stated. Mean: 49.03 years |
Unknown/not reported | >3months | Cross sectional study |
| Female | 284 | ||||||
| Unknown | 0 | ||||||
| Stewart et al. (2012) [53] |
Canada | Male | 10 | Range: 22-63 years Mean: 47.7 years |
Unknown/not reported | 3-6months | Semi-structured interviews. |
| Female | 8 | ||||||
| Unknown | 0 | ||||||
Table 3.
Social demographics for the articles from the third search on emotion regulation:.
| Article | Country | Gender | Age | Ethnicity of sample | Time with condition (LBP) | Methodology | |
|---|---|---|---|---|---|---|---|
| Gerhart et al. (2020) [54] |
USA | Male | 53 | Range: 18-70 years Mean: 46.3 years |
Caucasian: 80% (n = 84) African American: 15.2% (n = 16) Hispanic: 4.8% (n = 5) |
All participants had LBP for a minimum 6 months. Average duration: 9.04 years |
Cross sectional study |
| Female | 51 | ||||||
| Unknown | 0 | ||||||
| Le Borgne et al. (2017) [55] | France | Male | 120 | Range: 21-61 years. Mean: 41.74 years |
Unknown/not reported | <1year (n=25) 1-5 years (n=107) >5years (n=124) |
Semi-structured interviews |
| Female | 136 | ||||||
| Unknown |
0 | ||||||
| Moldovan et al. (2009) [56] | Romania | Male | 17 | Range: 27-84 years Mean: 50 years |
Unknown/not reported | Acute LBP (n=15) Chronic LBP (n=31) *Chronicity duration was not explicitly stated. |
Cross sectional study |
| Female | 29 | ||||||
| Unknown | 0 | ||||||
| Montano et al. (2025) [57] |
Spain | Male | 15 | Range: 21-64 years Mean: 49.2 years. |
Unknown/not reported | 12-80 weeks Mean duration: 46.5 weeks |
Semi-structured interviews |
| Female | 39 | ||||||
| Unknown | 0 | ||||||
| Thomas et al. (2024) [58] |
USA | Male | 86 | Range: 18-80 years Mean: 44.05 years |
Non-Hispanic Black: n=115 (62.5%) Non-Hispanic White: n=69 (37.5%) |
3 to 6 months: 4.4% 6 months to 1 year: 6.6% 1 to 3 years: 16.9% 3 to 5 years: 18.6% 5 to 10 years: 23.5% 10 to 20 years: 13.0% Over 20 years: 7.1% |
Cross sectional study |
| Female | 97 | ||||||
| Unknown | 0 | ||||||
| Yang & Mischkowski (2024) [59] |
USA | Male |
10 | All 18+ years. Range not detailed. Mean: 36.9 years |
Caucasian American: 74.0% African American: 14.0% Asian/Asian American: 2.9% American Indian/Alaskan Native: 0.8% Native Hawaiian/Other Pacific Islander: 0.4% Other race: 7.4% Hispanic/Latino (across all races): 6.6% Non-Hispanic: 93.0% |
>3 months | Cross sectional study |
| Female | 22 | ||||||
| Unknown | 0 | ||||||
Quality Considerations
Quality scores for the included articles are considered in Table 4 below. This provides an assessment as required by this type of review which identified that no study should be excluded and all articles will be useful to help the idea generating process.
Table 4.
Quality Scores For Originally Included Empirical Studies.
| Quality scores for originally included empirical studies exploring the concept of hope: | |||||
|---|---|---|---|---|---|
| Article | (a) Are considerations and information given by the selected articles made sufficiently well so that concepts can be translated? | (b) Do findings provide a context for the culture, environment, and setting? | c) Are the findings relevant and useful given the focus or aims of the analysis now? | d) Do the questions asked or aims from the paper selected align to those sought by the meta-ethnographer? | (e) To what extent do the findings give theoretical insight and context of interpretation made? |
| Corbett, Foster, and Ong(2007) [16] |
Yes | Yes | Yes | Yes | To a large extent |
| Madsen et al., (2024) [34] |
Yes | Yes | Yes | Yes | To a large extent |
| Stensland (2021) [31] |
Yes | Partially – Limited ethnic diversity. Focus was on a specific geographical location/population. | Yes | Yes | To a large extent |
| Toye and Barker (2012) [15] |
Yes | Yes |
Yes | Yes | To a large extent |
| Wojtnya, Palt, and Popiolek. (2015) [43] |
Yes | Partially – Cultural context is not deeply explored. |
Yes |
Yes | Moderate - large extent |
|
Quality scores for originally included empirical studies exploring the concept of uncertainty: | |||||
| Amja et al. (2021) [44] | Yes | Yes |
Yes | Yes | To some extent – Focused on living with pain during COVID-19 pandemic. |
| Benjaminsson et al. (2007) [45] | Yes | Partially – Cultural context is not deeply explored. |
Yes | Yes | To a large extent |
| Bowman (1994) [46] | Yes | Yes |
Yes | Yes | To a large extent |
| Bunzli et al. (2015) [47] | Yes | Yes |
Yes | Yes | Moderate - large extent |
| Costa et al. (2023) [17] | Yes | Yes |
Yes | Yes | To a large extent |
| Costa et al. (2023) [3] |
Yes |
Yes |
Yes | Yes | To a large extent |
| Fishbain et al. (2010) [48] | Yes | Yes |
Yes | Yes | Moderate extent |
| Lillrank. (2003) [49] |
Yes | Yes |
Yes | Yes | To a large extent |
| Makris et al. (2017) [50] |
Yes | Yes |
Yes | Yes | To a large extent |
| Osborn and Smith. (1998) [51] |
Yes | Yes |
Yes | Yes | To a large extent |
| Serbic et al. (2016) [52] | Yes | Yes |
Yes | Yes | To a large extent |
| Stewart et al. (2012) [53] |
Yes | Yes | Yes | Yes | Moderate extent – The focus was on returning to work, but the categories of percieved uncertainty are highly relavent and in keeping with our broader findings. |
| Quality scores for originally included empirical studies exploring the concept of emotion regulation: | |||||
| Gerhart et al. (2020) [54] |
Yes | Partially – moderate detail. Does not deeply explore broader sociocultural influences. | Yes | Yes | To some extent |
| Le Borgne et al. (2017) [55] | Yes | Partially – Adequate environmental context provided but ethnic or cultural background not discussed. | Yes | Yes | To a large extent |
| Moldovan et al. (2009) [56] | Yes | Partially – cultural norms and environmental context is not discussed |
Yes | Yes | To a large extent |
| Montano et al. (2025) [57] |
Yes | Partially – Cultural references not deeply analysed. | Yes | Yes | Moderate – large extent |
| Thomas et al. (2024) [58] |
Yes | Yes | Yes | Yes | To a large extent |
| Yang and Mischkowski (2024) [59] |
Yes | Partially - Sociocultural influences not deeply explored. |
Yes | Yes | To a large extent |
3.4. Proposed Substantive Theory
The findings from articles across various fields areas were used to generate a substantive theory, presented as a model (see Figure 4). This model demonstrates how emotion regulation is closely linked to—and influenced by— tolerance of uncertainty and hope. Health care professionals can use it to guide the management of people with CLBP and potentially improve their health outcomes.
Figure 4.
The final proposed model demonstrating how hope, tolerance of uncertainty, and emotion regulation are interconnected and influenced in individuals with CLBP.
Figure 4.
The final proposed model demonstrating how hope, tolerance of uncertainty, and emotion regulation are interconnected and influenced in individuals with CLBP.
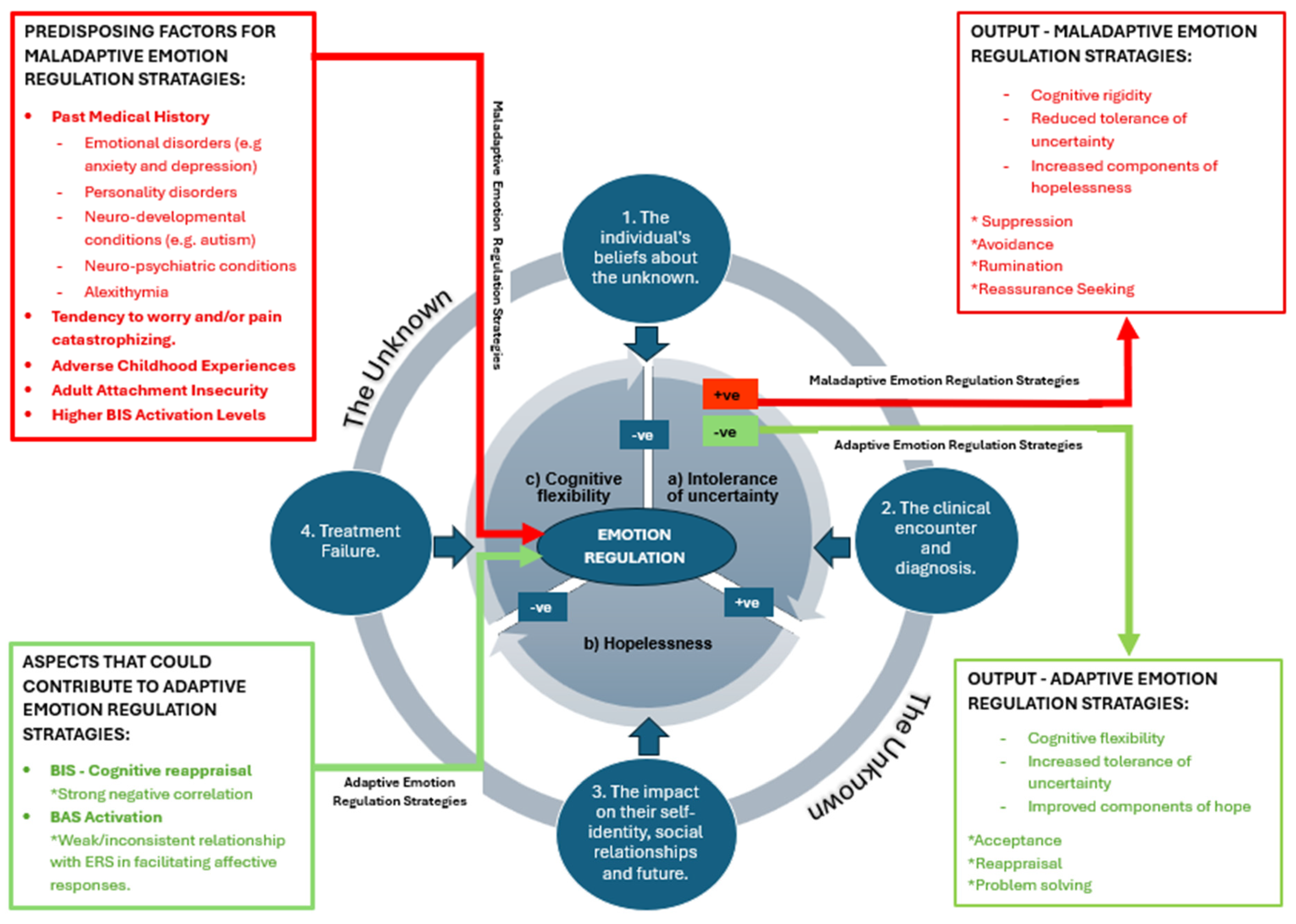
3.4.1. The Core Inter-Related Processes of Hopelessness, Cognitive Flexibility, and Intolerance of Uncertainty
The core of this theoretical model focuses on how an individual with CLBP regulates their emotions, and how their experience of the unknown is influenced by three central and interrelated factors:
(a) Intolerance of Uncertainty,
(b) Hopelessness, and
(c) Cognitive Flexibility.
3.4.1.1. Intolerance of Uncertainty
Individuals who have chronic pain and struggle with the ability to tolerate uncertainty often express concerns about the validity of medical tests and may engage in continuous activities aimed at pinpointing a specific diagnosis [60]. The inability to tolerate uncertainty is associated with attachment anxiety (concerns about being rejected, the need for reassurance, or the perception of being insecure) and worry [21]. The experience of worry or depression can lead individuals to anticipate negative outcomes from unknown events [37], and this may be further complicated by attachment orientation and anxiety [61,62] (see Section 3.4.2.1). These findings suggest that a vicious cycle of negative emotions and negative expectations can easily develop in individuals with CLBP as a result of intolerance of uncertainty. Identifying intolerance of uncertainty is therefore important. Given this understanding, the experience, frequency, and persistence of negative emotions are essential considerations when setting treatment goals and helping individuals tolerate distress during pain flares [54].
3.4.1.2. Hopelessness
Prior research has established that hopelessness is a common psychological state for individuals with CLBP and is a predisposing factor for depression, anxiety, and loneliness [31,63]. Hopelessness comprises three components [64]: (1) Dismal expectations — the belief that future outcomes will be negative. (2) Blocked goal-directed processing — the perception that one’s ability to achieve goals is consistently thwarted. (3) Helplessness — a feeling of being unable to change one’s situation or influence outcomes. Together, these components are crucial for understanding the dynamics of hopelessness and its impact on mental health and well-being [28]. Specific screening tools and therapies designed to foster hope are therefore important to consider [28].
3.4.1.3. Cognitive Flexibility
People with CLBP can become hypervigilant toward the experience of pain. Rather than being adaptive in their thinking and behavior and able to cope with internal or external stressors (i.e., being cognitively flexible [65]), they may become rigid in their thinking or cognitively inflexible [66]. This may manifest as a greater focus on the past or excessive worry about the future, rather than being able to accept experiences and consider more positive thoughts, beliefs, or behaviors [31,67]. The inability to be cognitively flexible is significant for people with CLBP [68] and is identified as a critical factor in the shift from adaptive to maladaptive emotional regulation strategies [63]. Screening and managing cognitive flexibility is important to create opportunities for more positive outcomes, for example, through specific therapies [67].
3.4.2. Emotional Regulation Strategies That Influence the Core Process of Emotional Regulation
This core is directly influenced by both adaptive and maladaptive regulation strategies, including predisposing factors, the Behavioural Inhibition System, and the Behavioural Activation System. The red box on the left-hand side identifies predisposing factors for maladaptive ERS. In contrast, the green box highlights aspects that could contribute to adaptive ERS, though further research is needed in this area.
3.4.2.1. Predisposing Factors for Maladaptive ERS
Several aspects of a patient’s medical history may predispose them to maladaptive emotion regulation strategies. These factors are captured in current guidelines for the management and screening of CLBP, which include an individual’s history and psychosocial risk factors (e.g., [60,69]). This includes emotional disorders, childhood experiences, and insights from existing models of emotional regulation.
Emotional disorders (such as anxiety or depression) are widely associated with difficulties in emotion regulation [13,23,24,70,71]. Notably, individuals with chronic pain are three times more likely to be diagnosed with anxiety and depression than the general population [26]. Emotional disorders may not only predispose individuals to chronic pain but may also develop as a consequence of it. This complexity is illustrated by research identifying a significant positive association between intolerance of uncertainty, depression, and pain catastrophising in people with chronic pain [20]. This challenges the assumption that inadequate ERS stems solely from pre-existing psychological conditions. Alexithymia, a neuropsychological trait marked by difficulty identifying and expressing emotions, is another relevant factor. Individuals with alexithymia are twice as likely to develop CLBP, as emotional awareness is crucial for adapting to stress and making everyday decisions [55,72].
Extensive literature highlights a strong association between adverse childhood experiences—including emotional, physical, sexual, and substance abuse, early parental loss, and parental psychopathology—and chronic pain. More recently, emotion dysregulation, often disrupted during childhood, has been identified as a central psychological process in the experience of pain. A secure, healthy attachment with a caregiver during childhood is fundamental to developing effective emotion regulation skills in adulthood. Insecure attachment is linked to worse pain experiences, increased disability, and higher distress [21,59]. It is also a risk factor for psychopathology and maladaptive behaviours, which are positively associated with worry and intolerance of uncertainty [21].
3.4.2.2. Aspects That Could Contribute to an Adaptive ERS
Other considerations for predisposing factors include insights derived from models relating to emotions, such as the Emotion Dysregulation Model [70] and the Behavioural Inhibition System [73]. The Behavioural Inhibition System is associated with suppression and avoidance strategies, hopelessness, and higher levels of depression and pain [2,74]. Conversely, this system also shows a strong negative association with cognitive reappraisal—an adaptive emotion regulation strategy—which mediates the relationship between the Behavioural Inhibition System and negative affect [2].
Finally, interoceptive processes (how the brain interprets internal sensory signals) may influence how individuals prone to anxiety perceive interactions with healthcare professionals [75]. This underscores the importance of considering both psychological and physiological factors in pain management.
3.4.3. The Outer Rim and Named ‘Unknowns’ Identified by People with CLBP
The outer rim of the model highlights four key themes that people with CLBP commonly report feeling uncertain about:
3.4.3.1. Their Beliefs About the Unknown
Uncertainty is increasingly understood as an emotion, shaped by ongoing cognitive appraisal of what is known versus unknown, leading to either positive or negative affective responses [12]. Emotions like fear—defined as a protective response to identifiable threats—can intensify uncertainty [22]. The broader concept of fear of the unknown includes physiological and emotional reactions to ambiguity, influenced by factors such as past experiences, perceived importance, time, and context [13]. Trait fear is shaped by history, while state fear reflects both trait and situational influences.
Carleton [13] linked fear of the unknown to constructs like intolerance of uncertainty, emotion regulation, attachment, and neuroticism. Evidence shows that individuals with emotional disorders often exhibit heightened fear of the unknown. It is important to note that the experience of fear, as well as intolerance of uncertainty, relates to an individual’s ability to predict and control events—important for how individuals manage their CLBP [76,77]. When uncertainty is appraised as threatening, it activates the Behavioural Inhibition System and thus increases the perception of negative outcomes [2], rather than producing a balanced appraisal that reduces avoidance and fear [13]. Indeed, fear-avoidance remains a key mechanism in persistent pain and a common maladaptive emotion regulation strategy [70].
Addressing dysregulated beliefs about the unknown involves identifying the nature of perceived threats [12,53]. These threats are linked to hope, and there is a need to appreciate that concerns relate to what is hoped for on multiple levels—from existential concerns to social identity and daily activities [30]. These layers are evident in qualitative studies on hope-related fears in chronic LBP [16]. Initial interventions should focus on deconstructing fears by clarifying the unknown elements or addressing specific concerns. For instance, Carroll et al. [78] found that addressing fears and setting realistic goals is crucial when a clear diagnosis is unavailable. Strategies to manage uncertainty include social comparisons, self-management, and psychotherapeutic approaches [26,63,79,80]. However, it remains unclear whether these reduce dysregulated beliefs or simply improve tolerance [13].
3.4.3.2. The Clinical Encounter and Diagnosis
During interactions and clinical encounters, people with CLBP identified that the most important factor to be acknowledged was having their experiences and symptoms taken seriously [49]. One reason for this is the perception that they may not be believed [15,81]. As a result, people with CLBP often attempt to legitimise their symptoms by seeking further input, such as expert opinions or diagnostic investigations [49,82]. Related to this is the perception among patients that they have received a thorough examination [35]. However, not all CLBP consultations result in positive outcomes, as the clinical encounter can pose either a threat or an opportunity [78].
Madsen et al. [34] identified different experiences before and after a consultation for people with CLBP. Before, individuals reported concerns, a sense of helplessness, and fear. Following the consultation, reduced uncertainty, a greater sense of hope, and improved emotional regulation were observed. Trust appeared to arise through examination thoroughness, and the clinician’s emotional and personal engagement also played a crucial role in the identified outcomes. The concept of trust is supported by interactions being perceived as open and honest [81]. Trust is especially important if individuals have attachment insecurity [83], and this may require clinicians to be able to manage worries and concerns about the future [58].
The clinical encounter also needs to consider how and what advice is given. For example, when people with CLBP are advised to rest or avoid aggravating activities, it can trigger fear-avoidant behaviour. In contrast, those who report receiving adequate reassurance, support, and explanations from their clinician feel empowered and are more prepared to make appropriate lifestyle adaptations to self-manage their condition [84].
People with CLBP strive for a diagnosis or, at the very least, an explanation for their symptoms [15,16,45,46,47,51]. Diagnostic uncertainty causes increased emotional distress, disability, and pain [52]. It can be informed by limitations in biomedical knowledge (medical uncertainty) and a more general awareness among patients of an undetermined future (existential uncertainty) [85]. Several qualitative studies have found that, typically across musculoskeletal care, clinical practice focuses on ruling out serious pathology rather than ruling in a definitive diagnosis [78].
However, within society, there is a strong perception and expectation that a thorough examination—sometimes involving diagnostic investigations such as blood tests or imaging—will lead to a legitimate diagnosis, which in turn enables effective treatment interventions and hope for the resolution of symptoms [3,15,47]. Despite this understanding of patient expectations, national guidelines do not recommend imaging for low back pain with or without radicular symptoms in the absence of red flags or a neurological deficit [7]. This is because, in most cases (90–95%), there is no identifiable structural cause in people with CLBP, meaning that pathological findings from imaging frequently do not correlate with the individual’s symptoms [3].
It is well established that in cases where there is no clear diagnosis or explanation for symptoms, this can negatively impact pain, disability, and both cognitive and emotional functioning [52,82]. Additionally, when a structural cause is not identified through imaging, it can result in a contradictory outcome because it still fails to provide a clear diagnosis. At times, incidental findings may occur, which foster further anxiety and fear, or even cause the individual to question their pain experience—ultimately failing to improve outcomes [15,17].
Clinicians who provide clear, consistent, and empathetic explanations during CLBP consultations help to reduce uncertainty, improve patient satisfaction, and enhance prognostic outlook [34,86].
Despite this, astonishingly, there remains no clinical guidance on how to manage patients in the face of uncertainty [86]. Uncertainty is increasingly becoming a more prevalent issue from the patient’s perspective, due to heightened public awareness of the limitations of medical knowledge—disseminated through various media channels—which contributes to increased anxiety around health and illness risk in society [87,88].
Physiotherapists, in particular, struggle to manage diagnostic uncertainty when treating people with CLBP because they feel they lack sufficient knowledge and skills, as well as time and resources, to manage the condition’s complexity effectively [89]. As a compensatory strategy, healthcare professionals may avoid or minimise discussions around uncertainty to maintain the perception of expertise or avoid compromising their authority [89]. However, a lack of acknowledgement or openness can undermine trust and may result in epistemic injustice [3]. Epistemic injustice occurs when healthcare professionals use their authority to influence a patient’s decision to align with their own, or when a patient’s personal account is discredited [81].
Different professional groups manage uncertainty in diverse ways [87,90]. Mol [91] outlined two contrasting approaches to managing uncertainty: the logic of care and the logic of choice. In Western clinical contexts, healthcare professionals often prioritise offering the individual a choice by outlining factual information. However, this approach assumes that the individual possesses high self-efficacy—that is, they feel competent, confident, and capable of contributing to decisions and managing their own condition.
In contrast, people with CLBP often exhibit low self-efficacy and may not always respond positively to choice, particularly when faced with navigating multiple uncertain options. In such cases, Mol [91] advocates the logic of care, which promotes a patient-centred approach by focusing on relevant, achievable goals and supporting individuals to make lifestyle adaptations that enable them to self-manage their condition effectively [77].
3.4.3.3. The Impact on Self-Identity, Social Relationships, and the Future
The expression of hope is associated with self-identity, social relationships, and future aspirations, all of which are identified as meaningful [36]. A common theme across several qualitative studies is that people with CLBP frequently experience self-doubt in their ability to manage pain and navigate daily challenges [3,16,47]. This impacts their social identity, relationships, and ability to envision a meaningful future. Their (in)ability to manage fluctuating symptoms threatens their sense of self, creating fear about the future [51].
The beliefs of an individual’s social network—such as family, friends, or colleagues—can also influence expectations, attitudes, and overall prognosis, although to a lesser extent than the opinions and beliefs of clinicians [47]. Chronic pain can have profound social consequences [51]. It is often associated with increased social isolation, which can lead to depression and feelings of lost purpose and value [44]. Social isolation has been identified as a more significant consequence for older adults living with CLBP compared to younger adults, but it is not commonly assessed in clinical practice [50]. Qualitative literature [51] has revealed that people with CLBP tend to withdraw from social contact for several reasons: To avoid symptom flares, because they perceive themselves as unacceptable company, due to a preference for the safety of solitude, and because of the stigma and shame associated with chronic pain. Furthermore, diagnostic uncertainty has been found to correlate positively with guilt. When people cannot find a cause for their pain, they may blame themselves and experience social guilt—fear of letting others down—which is strongly associated with anxiety and depression [52].
Toye and Barker [15] found that maintaining a positive self-identity was a key factor in the success of individuals enrolled in a pain management programme for CLBP. It also plays an important role in helping them overcome fears related to movements or activities that might trigger or worsen their symptoms [15]. Therefore, it is essential that clinicians explore what is personally meaningful to each individual in order to set relevant and motivating goals [30].
Clinicians should use active listening and risk stratification tools to determine where individuals with CLBP fall on the spectrum from entrenched self-doubt to effective self-management, and then tailor an appropriate action plan [7,77]. It is also important that healthcare professionals understand how pain-related behaviour patterns—such as fear-avoidance or avoidance-endurance—can influence cognitive rigidity and require different treatment approaches [91]. Fear-avoidant behaviours are addressed through Interdisciplinary Multimodal Pain Therapy (IMPT), which includes correcting misconceptions and using exposure-based interventions. In contrast, avoidance-endurance behaviours require a different theoretical focus: encouraging individuals to recognise warning signs of mental and physical deterioration and to adopt pacing strategies [91].
3.4.3.4. Treatment Failure
Failed treatments and the inability to self-manage pain can be another source of uncertainty, particularly when individuals have not achieved treatment goals despite adherence [47]. This often triggers negative emotions and is reported to lead people to feel “powerless” and “helpless” [31].
People with CLBP often receive extensive input from healthcare services, but treatment efficacy is variable, frequently leading to frustration with healthcare systems [48,86]. There is increasing recognition that the success of adopting a self-management approach hinges on readiness to change and acceptance of pain [48]. Acceptance appears to be a key adaptive emotion regulation strategy, enabling individuals to find ways to live a fulfilling life despite pain [31]. Thus, recommendations for therapies that support acceptance could be considered.
3.4.4. The Model Output and Resultant ERS
The model’s output focuses on ERS, which are divided into two types. The first is adaptive ERS, whereby individuals effectively regulate their emotions using strategies such as acceptance, reappraisal, and problem solving, although there is generally less research exploring this approach. In contrast, more extensive research has examined maladaptive ERS, which involve behavioural strategies such as suppression, rumination, avoidance or reassurance seeking, which are typically ineffective and often contribute to the development of psychopathology [70].
4. Discussion
To the best of the authors’ knowledge, this is the first example of a social constructivist meta-ethnography study conducted with the aim of generating a substantive theory. The resulting multifaceted model places emotion regulation as a central concept in people with CLBP, influenced by three interrelated concepts. The findings demonstrate that maladaptive ERS are driven by heightened intolerance of uncertainty, and hopelessness, which contribute to, and interact with cognitive rigidity. Combined these concepts likely cause significant psychological distress and poor health outcomes [18,65]. Importantly, improving cognitive flexibility appears to be a potential resilience factor, enabling individuals to reframe distressing experiences or uncertainty and shift from maladaptive to adaptive ERS [68].
These central concepts are further influenced by intrinsic factors such as a history of emotional disorders (especially anxiety and depression), personality disorders, or personality traits that foster worry and a tendency to catastrophise pain. They are also shaped by a history of adverse childhood experiences or later-in-life adult attachment insecurity. Extrinsically, the clinical encounter plays an equally pivotal role in identifying contributing factors and creating an individualised management plan to improve emotion regulation and ultimately support self-management of CLBP.
All CLBP consultations involve an element of uncertainty for both the patient and clinician, but these encounters play a vital role in either reinforcing or alleviating that uncertainty. Establishing an effective therapeutic relationship built on trust, promoting epistemic humility, and showing compassion and a willingness to help will shape patients’ beliefs, self-efficacy, and ability to engage in a biopsychosocial management plan. Recognising the limits of healthcare and science, and communicating this information effectively, should be a fundamental skill for all healthcare professionals [87].
Clinical examinations and interventions often emphasise technical factors, leaving little space for the social and political dimensions that also matter [84]. Therefore, Costa et al. [85,88] call for more research and training on medical uncertainty, urging the development of training interventions that change our learning approach and foster an epistemic cultural shift. This shift is towards a system that integrates human uncertainties into evidence-based practice. Importantly, these principles and changes must extend beyond individual clinical practice and permeate policies, procedures, and the values of our healthcare systems. After all, providing too much certainty, or neglecting the issue can be unsafe, but attending to uncertainty is always optimal because “risks always involve uncertainty, but uncertainty does not always involve risks” [89].
4.1. Clinical Recommendations
This model is intended to be used as a quick-reference tool for clinicians navigating the central concepts of CLBP care. Consultations offer vital opportunities to uncover the key factors driving maladaptive ERS and to offer a personalised approach. During each consultation, clinicians should focus on:
- Building an effective therapeutic relationship, founded on trust, openness, and honesty.
- Conducting a thorough exploration—not only of the patient’s medical history but also sensitively exploring whether they may have been affected by adverse childhood experiences and determining their attachment orientation.
- Exploring the patient’s beliefs about the unknown, including their perceptions of pain, worries or concerns about living with a chronic condition, and gaining a deeper understanding of their self-identities—while remaining open to other possible psychosocial factors not captured in this study.
Clinicians should also be aware of clinical assessment tools and potential therapies that provide a useful starting point for understanding the patient.
4.2. Clinical Implications for Screening
Based on current research findings, we recommend specific screening for predisposing factors, supported by current guidelines (e.g., [60,69]). The following brief, validated scales would also suitable for use in time-limited clinical settings:
- Cognitive Flexibility Scale [92]: A 12-item measure using a 6-point Likert scale to assess an individual’s ability to adapt thinking and consider alternative solutions.
- Model of Emotions, Adaptation and Hope (MEAH) [28]: A 5-item scale designed to identify an individual’s most significant named challenge. It can be administered in approximately 30 seconds. The hope item is particularly useful for identifying experiences of uncertainty, possibility, and hopelessness.
- Intolerance of Uncertainty Scale – Short Form [93]: A 5-item measure that efficiently screens for intolerance of uncertainty.
- Emotion Regulation Questionnaire [94]: A 10-item scale assessing two key strategies—cognitive reappraisal and expressive suppression—for clinicians seeking a deeper understanding of emotion regulation.
4.3. Clinical Implications for Therapy
When screening identifies challenges in cognitive flexibility, emotion regulation, or hope, several therapeutic approaches may be beneficial. For rehabilitation therapists, brief tools have shown to be effective:
- MEAH-based therapeutic conversations [28]: These can be delivered in 10- or 30-minute formats by trained rehabilitation therapists (training available online in under an hour). The MEAH tool serves as a foundation for exploring emotional adaptation and fostering hope. The extended version may be particularly useful, as it considers social identity, relationships, and meaningful hopes as part of a structured conversation.
Other therapies with positive results should also be considered. Three examples include:
- Acceptance and Commitment Therapy (ACT) [67]: Focuses on improving cognitive flexibility and helping individuals accept and embrace feelings and thoughts while committing to action. It is effective in improving social and physical functioning, enhancing mood, and lowering pain.
- Emotional Awareness and Expression Therapy [95]: Helps individuals process and express avoided emotions, particularly those linked to trauma or chronic pain.
- Dialectical Behavior Therapy (DBT) [96]: Offers structured skills training in emotion regulation, distress tolerance, and mindfulness, and has shown effectiveness in chronic pain populations.
4.4. Future Research
Firstly, the utilisation of this model needs to be tested within clinical practice before potentially using it as a navigation tool for clinicians to improve their skills and strategies in managing patients with CLBP via a tailored approach. Other clinical areas for future research include the need for more investigation into interventions that address cognitive flexibility and cognitive reappraisal via the Behavioural Inhibition System or Behavioural Activation System, in addition to exploring ways to enhance secure attachment traits. Additionally, there is a need for the development of clinical guidelines on managing uncertainty, promoting epistemic humility from undergraduate education through to evolving healthcare policies that embrace uncertainty.
4.5. Limitations
Despite searching for studies involving participants with low back pain of any duration, the majority of the existing literature has explored these key concepts using participants with CLBP (>3 months duration). Therefore, we cannot confidently say that this model and its findings are applicable to people with acute LBP, although further testing in this group and other related populations would be warranted.
Additionally, the low number of studies may have restricted the process of idea generation, and this study may not have captured all literature on hope, uncertainty, and emotion regulation, nor included every factor that could influence them. For instance, this could include aspects such as interoceptive active inference or impaired reward-related learning signals.
Importantly, social constructivist meta-ethnography was designed to create substantive theory, not generalisable theory. Thus, the resultant model requires critical consideration and further research. As reflected by the quality scores (see 3.2 Quality Considerations, Table 2), the initial studies and subsequently the model may not account for multiple cultures or sociodemographic factors, which arguably could be the case for any theory. However, this is particularly important for this review due to the limited ability to apply critical enquiry from social constructivist grounded theory and reveal specific cultural or ethnic influences within the model. Therefore, further research is required to test this theory within clinical practice and across different cultures, contexts and settings.
We acknowledge that we have focused on specific frameworks of key concepts and that our understanding may be limited, as well as the possibility that we have missed key literature supporting this understanding. Additionally, we are aware of the potential for confirmation bias, given the past research of the supervising author—seeking and confirming existing thoughts may have influenced the proposed model.
Further consideration of counselling-based literature and therapies such as Acceptance and Commitment Therapy could be relevant to the model and its application. Other psychological constructs may also play an important role, such as Self-Efficacy Theory and sources of self-efficacy. However, it is beyond the scope of this review to address these considerations, which require further investigation.
Lastly, the application of this theory beyond people with CLBP may be limited and will require additional research.
4.6. Conclusion
To conclude, tolerance of uncertainty and hope are complex phenomena that significantly impact emotion regulation and health outcomes in people living with CLBP. They also have broader implications for society, warranting extensive research. The rising prevalence of CLBP demonstrates that our current approach to consultations and treatment interventions is insufficient, and a new approach to managing this population is urgently needed.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. See separate attached document.
Author Contributions
The conceptualization and methodology was undertaken by both authors. The investigation was undertaken by the primary author. Searching was undertaken by both authors. The formal analysis was undertaken by the primary author. Review and editing was undertaken by both authors. Supervision was undertaken by the second author.
Funding
This research did not receive any external funding.
Institutional Review Board Statement
N/A.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ge L, Pereira MJ, Yap CW, Heng BH. Chronic low back pain and its impact on physical function, mental health, and health-related quality of life: a cross-sectional study in Singapore. Sci Rep. 2022;12:20040. [CrossRef]
- Serrano-Ibáñez E, Ramírez-Maestre C, López-Martínez AE, Esteve R, Ruiz-Párraga GT, Jensen MP. Behavioral inhibition and activation systems and emotional regulation in individuals with chronic musculoskeletal pain. Front Psychiatry. 2018;9:394. [CrossRef]
- Costa N, Olson R, Mescouto K, Hodges PW, Dillon M, Evans K, Walsh K, Jensen N, Setchell J. Uncertainty in low back pain care – insights from an ethnographic study. Disabil Rehabil. 2023;45:784–795.
- Hayden JA, Cartwright JL, Riley RD, van Tulder MW. Exercise therapy for chronic low back pain: protocol for an individual participant data meta-analysis. Syst Rev. 2012;1:64. [CrossRef]
- Keller A, Hayden J, Bombardier C, van Tulder M. Effect sizes of non-surgical treatments of non-specific low-back pain. Eur Spine J. 2007;16:1776–1788. [CrossRef]
- Moseley GL, Flor H. Targeting cortical representations in the treatment of chronic pain: a review. Neurorehabil Neural Repair. 2012;26:646–652. [CrossRef]
- National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management [NG59]. London: NICE; 2016. Available online: https://www.nice.org.uk/guidance/ng59/resources/endorsed-resource-national-pathway-of-care-for-low-back-and-radicular-pain-4486348909 (accessed on 22 March 2024).
- National Institute for Health and Care Excellence (NICE). Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain [NG193]. London: NICE; 2021. Available online: https://www.nice.org.uk/guidance/ng193 (accessed on 20 June 2024).
- Steffens D, Maher C, Pereira L, Stevens M, Oliveira V, Chapple M, Teixeira-Salmela L, Hancock M. Prevention of low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176:199–208. [CrossRef]
- Soundy A, Lim JY. Pain perceptions, suffering and pain behaviours of professional and preprofessional dancers towards pain and injury: a qualitative review. Behav Sci. 2023;13(3):268. [CrossRef]
- Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, Keefe FJ, Mogil JS, Ringkamp M, Sluka KA, Song XJ, Stevens B, Sullivan MD, Tutelman PR, Ushida T, Vader K; IASP Presidential Task Force. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020 Sep 1;161(9):1976–1982. [CrossRef] [PubMed] [PubMed Central]
- Freeston M, Komes J. Revisiting uncertainty as a felt sense of unsafety: The somatic error theory of intolerance of uncertainty. J Behav Ther Exp Psychiatry. 2023;79:101827. [CrossRef]
- Carleton RN. Into the unknown: a review and synthesis of contemporary models involving uncertainty. J Anxiety Disord. 2016;39:30–43. [CrossRef]
- Choi JW, So WY, Kim K. The mediating effects of social support on the relationship between uncertainty and quality of life among patients with chronic low back pain: a cross-sectional survey. Healthcare (Basel). 2022;10:1805. [CrossRef]
- Toye F, Barker K. “I can’t see any reason for stopping doing anything, but I might have to do it differently” – restoring hope to patients with persistent non-specific low back pain: a qualitative study. Disabil Rehabil. 2012;34:894–903.
- Corbett M, Foster N, Ong B. Living with low back pain: stories of hope and despair. Soc Sci Med. 2007;65:1584–1594. [CrossRef]
- Costa N, Butler P, Dillon M, Mescouto K, Olson R, Forbes R, Setchell J. “I felt uncertain about my whole future” – a qualitative investigation of people’s experiences of navigating uncertainty when seeking care for their low back pain. Pain. 2022;164:2749–2758.
- Gross JJ, Feldman-Barrett L. Emotion generation and emotion regulation: one or two depends on your point of view. Emot Rev. 2011;3:8–16. [CrossRef]
- Braunstein LM, Gross JJ, Ochsner KN. Explicit and implicit emotion regulation: a multi-level framework. Soc Cogn Affect Neurosci. 2017;12(10):1545–1557. [CrossRef]
- Trudel,. P., Cormier, S. (2024) Intolerance of uncertainty, pain catastrophizing, and symptoms of depression: a comparison between adults with and without chronic pain, Psychology, Health & Medicine, 29:5, 951-963. [CrossRef]
- Clark GI, Rock AJ, Clark LH, Murray-Lyon K. Adult attachment, worry and reassurance seeking: investigating the role of intolerance of uncertainty. Clin Psychol. 2020;24(3):294–305. [CrossRef]
- Carleton RN. The intolerance of uncertainty construct in the context of anxiety disorders: theoretical and practical perspectives. Expert Rev Neurother. 2012;12:937–947. [CrossRef]
- Sandhu T, Xiao B, Lawson R. Transdiagnostic computations of uncertainty: towards a new lens on intolerance of uncertainty. Neurosci Biobehav Rev. 2023;148:105123. [CrossRef]
- Ouellet C, Langlois F, Provencher MD, Gosselin P. Intolerance of uncertainty and difficulties in emotion regulation: proposal for an integrative model of generalized anxiety disorder. Eur Rev Appl Psychol. 2019;69:9–18. [CrossRef]
- Mauss IB, Bunge SA, Gross JJ. Automatic emotion regulation. Soc Personal Psychol Compass. 2007;1(1):146–167. [CrossRef]
- Koechlin H, Coakley R, Schechter N, Werner C, Kossowsky J. The role of emotion regulation in chronic pain: a systematic literature review. J Psychosom Res. 2018;107:38–45. [CrossRef]
- Soundy A, Stubbs B, Freeman P, Roskell C. Factors influencing patients’ hope in stroke and spinal cord injury: a narrative review. Int J Ther Rehabil. 2014;21(5):210–218. [CrossRef]
- Soundy, A. Harnessing hope in managing chronic illness: a guide to therapeutic rehabilitation. 1st ed. London (UK): Routledge; 2025.
- TenHouten, W. The emotions of hope: from optimism to sanguinity, from pessimism to despair. Am Sociol. 2023;54:76–100. [CrossRef]
- Soundy A, Liles C, Stubbs B, Roskell C. Identifying a framework for hope in order to establish the importance of generalised hopes for individuals who have suffered a stroke. Adv Exp Med Biol. 2014;2014:1–8. [CrossRef]
- Stensland, M. “If you don’t keep going, you’re gonna die”: helplessness and perseverance among older adults living with chronic low back pain. Gerontologist. 2021;61(6):907–916. [CrossRef]
- Katsimigos AM, O’Beirne S, Harmon D. Hope and chronic pain: a systematic review. Ir J Med Sci. 2020;190:307–312. [CrossRef]
- Or DYL, Lam CS, Chen PP, Wong HSS, Lam CWF, Fok YY, Chan SFI, Ho SMY. Hope in the context of chronic musculoskeletal pain: relationships of hope to pain and psychological distress. Pain Rep. 2021;6:e965. [CrossRef]
- Madsen SD, Stochkendahl MJ, Morsø L, Andersen MK, Hvidt EA. Patient perspectives on low back pain treatment in primary care: a qualitative study of hopes, expectations, and experiences. BMC Musculoskelet Disord. 2024;25(1):997. [CrossRef]
- Pinto AM, Geenen R, Wager TD, Lumley MA, Häuser W, Kosek E, Ablin JN, Amris K, Branco J, Buskila D, Castelhano J, CasteloBranco M, Crofford LJ, Fitzcharles MA, LópezSolà M, Luís M, Marques TR, Mease PJ, Palavra F, Rhudy JL, Uddin LQ, Castilho P, Jacobs JWG, da Silva JAP. Emotion regulation and the salience network: a hypothetical integrative model of fibromyalgia. Nat Rev Rheumatol. 2023;19(1):44–60. [CrossRef]
- Soundy, A. Social constructivist meta-ethnography: a framework construction. Int J Qual Methods. 2024;23:1–10. [CrossRef]
- Soundy A, Heneghan NR. Meta-ethnography. Int Rev Sport Exerc Psychol. 2022;15(2):266–286. [CrossRef]
- Charmaz K, Thornberg R. The pursuit of quality in grounded theory. Qual Res Psychol. 2021;18(3):258–269. [CrossRef]
- Campbell R, Pound P, Morgan M, Daker-White G, Britten N, Pill R, Yardley L, Pope C, Donovan J. Evaluating meta-ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess. 2011;15(43). [CrossRef]
- Lewis J, Ritchie J, Ormston R, Morrell G. Generalising from qualitative research. In: Ritchie J, Lewis J, McNaughton Nicholls C, Ormston R, editors. Qualitative research practice: a guide for social science students and researchers. 2nd ed. London (UK): Sage Publications Ltd.; 2013.
- Mishel, MH. Uncertainty in illness. J Nurs Scholarsh. 1988;20(4):225–232. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. [CrossRef]
- Wojtyna E, Palt L, Popiolek K. From Polyanna syndrome to Eeyore’s Corner? Hope and pain in patients with chronic low back pain. Pol Psychol Bull. 2015;46(1):96–103.
- Amja K, Vigouroux M, Pagé MG, Hovey RB. The experiences of people living with chronic pain during a pandemic: “Crumbling dreams with uncertain futures”. Qual Health Res. 2021 Sep;31(11):2019–28. [CrossRef]
- Benjaminsson O, Biguet G, Arvidsson I, Nilsson-Wikmar L. Recurrent low back pain: relapse from a patient perspective. J Rehabil Med. 2007;39(8):640–645. [CrossRef]
- Bowman JM. Experiencing the chronic pain phenomenon: a study. Rehabil Nurs. 1994 MarApr;19(2):91–5. [CrossRef]
- Bunzli S, Smith A, Schütze R, O’ Sullivan P. Beliefs underlying painrelated fear and how they evolve: a qualitative investigation in people with chronic back pain and high painrelated fear. BMJ Open. 2015 Oct;5(10):e008847. [CrossRef]
- Fishbain DA, Bruns D, Disorbio JM, Lewis JE, Gao J. Exploration of the illness uncertainty concept in acute and chronic pain patients vs community patients. Pain Med. 2010 May;11(5):658–69. [CrossRef]
- Lillrank A. Back pain and the resolution of diagnostic uncertainty in illness narratives. Soc Sci Med. 2003;57(6):1045–1054. [CrossRef]
- Makris UE, Higashi RT, Marks EG, Fraenkel L, Gill TM, Friedly JL, Reid MC. Physical, emotional, and social impacts of restricting back pain in older adults: A qualitative study. Pain Med. 2017;18(7):1225–1235. [CrossRef]
- Osborn M, Smith JA. The personal experience of chronic benign lower back pain: an interpretative phenomenological analysis. Br J Health Psychol. 1998 Mar;3(1):65–83. [CrossRef]
- Serbic D, Pincus T, Fife-Schaw C, Dawson H. Diagnostic uncertainty, guilt, mood, and disability in back pain. Health Psychol. 2016 Jan;35(1):50–59. [CrossRef]
- Stewart AM, Polak E, Young R, Schultz IZ. Injured workers’ construction of expectations of return to work with subacute back pain: the role of perceived uncertainty. J Occup Rehabil. 2012 Mar;22(1):1–14. [CrossRef]
- Gerhart J, Burns JW, Post KM, Smith DA, Porter LS, Burgess HJ, et al. Relationships of negative emotions and chronic low back pain to functioning, social support, and received validation. Clin J Pain. 2019;35(2):173–179. [CrossRef]
- Le Borgne M, Boudoukha AH, Petit A, Roquelaure Y. Chronic low back pain and the transdiagnostic process: How do cognitive and emotional dysregulations contribute to the intensity of risk factors and pain? Scand J Pain. 2017;17:309–15. [CrossRef]
- Moldovan AR, Onac IA, Vantu M, Szentagotai A, Onac I. Emotional distress, pain catastrophizing and expectancies in patients with low back pain. J Cogn Behav Psychother. 2009;9(1):83–93.
- Montaño JJ, Gervilla E, Jiménez R, Sesé A. From acute to chronic low back pain: the role of negative emotions. Psychol Health Med. 2025 Mar 27;1–14. [CrossRef]
- Thomas JS, Goodin BR. Adverse childhood experiences and chronic low back pain: Recent insights and implications. Neurosci Biobehav Rev. 2024;157:105427.
- Yang Q, Mischkowski D. Understanding pain communication: Current evidence and future directions. Neurosci Biobehav Rev. 2024;158:105444.
- Zhou T, Salman D, McGregor AH. Recent clinical practice guidelines for the management of low back pain: a global comparison. BMC Musculoskelet Disord. 2024 May 1;25:344. [CrossRef]
- Neville A, Kopala-Sibley DC, Soltani S, Asmundson GJG, Jordan A, Carleton RN, Yeates KO, Schulte F, Noel M. A longitudinal examination of the interpersonal fear avoidance model of pain: the role of intolerance of uncertainty. Pain. 2021;162(1):152–160.
- Brennan KA, Clark CL, Shaver PR. Self-report measurement of adult romantic attachment: an integrative overview. In: Simpson JA, Rholes WS, editors. Attachment theory and close relationships. New York: Guilford Press; 1998. p. 46–76.
- Wu Q, Xu L, Wan J, Yu Z, Lei Y. Intolerance of uncertainty affects the behavioral and neural mechanisms of higher generalization. Cereb Cortex. 2024 Apr;34(4):bhae153. [CrossRef]
- Leite A, Araujo G, Rolim C, Castelo S, Beilfuss M, Leao M, Castro T, Hartmann S. Hope theory and its relation to depression: a systematic review. Psychol Cogn Neurosci. 2019;2:e1014.
- Lynch, W. Images of hope: imagination as healer of the hopeless. 1st ed. Baltimore: Helicon Press; 1965.
- Vlaeyen, J. W., and Linton, S. J. (2012). Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 153, 1144–1147. [CrossRef]
- Demirtas AS, Yildiz B. Hopelessness and perceived stress: the mediating role of cognitive flexibility and intolerance of uncertainty. Dusunen Adam J Psychiatr Neurol Sci. 2019;32(3):259–67. [CrossRef]
- Ma TW, Yuen ASK, Yang Z. The efficacy of Acceptance and Commitment Therapy for chronic pain: a systematic review and meta-analysis. Clin J Pain. 2023;38(2):85–96.
- World Health Organisation (2023). WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings. World Health Organisation, Geneve. Available online: https://www.who.int/publications/i/item/9789240081789.
- Sahib A, Chen J, Cardenas D, Calear AL. Intolerance of uncertainty and emotion regulation: a meta-analytic and systematic review. Clin Psychol Rev. 2023;101:102270. [CrossRef]
- Fitzpatrick S, Dixon-Gordon KL, Turner CJ, Chen SX, Chapman A. Emotion dysregulation in personality disorders. Curr Psychiatry Rep. 2023;25(5):223–231. [CrossRef]
- Mehling WE, Krause N. Are difficulties perceiving and expressing emotions associated with low-back pain? The relationship between lack of emotional awareness (alexithymia) and 12-month prevalence of low-back pain in 1180 urban public transit operators. J Psychosom Res. 2005;58(1):73–81. [CrossRef]
- White LK, McDermott JM, Degnan KA, Henderson HA, Fox NA. Behavioral inhibition and anxiety: the moderating roles of inhibitory control and attention shifting. J Abnorm Child Psychol. 2011 Jul;39(5):735-47. [CrossRef]
- Jensen MP, Solé E, Castarlenas E, Racine M, Roy R, Miró J, et al. Behavioral inhibition, maladaptive pain cognitions, and function in patients with chronic pain. Scand J Pain. 2017 Oct;17(1):41–48. [CrossRef]
- Pang J, Tang X, Li H, Hu Q, Cui H, Zhang L, Li W, Zhu Z, Wang J, Li C. Altered interoceptive processing in generalized anxiety disorder—a heartbeat-evoked potential research. Front Psychiatry. 2019;10:616.
- Hong RY, Cheung MWL. The structure of cognitive vulnerabilities to depression and anxiety: evidence for a common core etiologic process based on a meta-analytic review. Clin Psychol Sci. 2014;3(6):892–912. [CrossRef]
- Bandura A. Self-efficacy. In: Ramachaudran VS, editor. Encyclopedia of human behavior. Vol. 4. New York: Academic Press; 1994. p. 71–81.
- Carroll LJ, Lis A, Weiser S, Torti J. How well do you expect to recover, and what does recovery mean, anyway? Qualitative study of expectations after a musculoskeletal injury. Phys Ther. 2016;96(6):797–807. [CrossRef]
- Spink A, Wagner I, Orrock P. Common reported barriers and facilitators for self-management in adults with chronic musculoskeletal pain: a systematic review of qualitative studies. Musculoskelet Sci Pract. 2021;56:102433. [CrossRef]
- Abdolghaderi M, Kafi S, Saberi A, Ariaporan S. Effectiveness of mindfulness-based cognitive therapy on hope and pain beliefs of patients with chronic low back pain. Caspian J Neurol Sci. 2018;4(12):18–23. [CrossRef]
- Razavi, S.B., Aboalghasimi, S., Akbari, B. and Nadirinabi, B. The Effectiveness of Cognitive Therapy on Hope and Pain Management in Women with Chronic Pain. PCNM Journal. 2022, 12, pp. 18-23.
- Buchman DZ, Ho A, Goldberg DS. Investigating trust, expertise, and epistemic injustice in chronic pain. J Bioeth Inq. 2017;14(1):31–42. [CrossRef]
- Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. Ann Fam Med. 2013;11(6):527–34.
- Serbic D, Pincus T. Diagnostic uncertainty and recall bias in chronic low back pain. Pain. 2014;155(8):1540–46. [CrossRef]
- Costa N, Olson R, Dillon M, Mescouto K, Butler P, Forbes R, Setchell J. Navigating uncertainty in low back pain care through an ethic of openness: learning from a post-critical analysis. Health. 2025;71(2):104–110.
- Mishel MH, Mu B. Reconceptualization of the uncertainty in illness. J Nurs Scholarsh. 1990;22(4):256–62. [CrossRef]
- Lian OS, Nettleton S, Wifstad Å, Dowrick C. Negotiating uncertainty in clinical encounters: a narrative exploration of naturally occurring primary care consultations. Soc Sci Med. 2021 Dec;291:114467. [CrossRef]
- Costa N, Mescouto K, Dillon M, Olson R, Butler P, Forbes R, Setchell J. The ubiquity of uncertainty in low back pain care. Soc Sci Med. 2022 Nov;313:115422. [CrossRef]
- Costa N, Olson R, Dillon M, Mescouto K, Butler P, Forbes R, Setchell J. Navigating uncertainty in low back pain care through an ethic of openness: learning from a post-critical analysis. Health. 2025;71(2):104–110.
- Mackintosh N, Armstrong N. Understanding and managing uncertainty in healthcare: revisiting and advancing sociological contributions. Sociol Health Illn. 2020 Jan;42(1):1–20. [CrossRef]
- Mol, A. The logic of care: Health and the problem of patient choice. London (UK): Taylor & Francis Group; 2008.
- Martin MM, Rubin RB. A new measure of cognitive flexibility. Psychol Rep. 1995;76:623-6.
- Bottesi G, Noventa S, Freeston MH, Ghisi M. A short-form version of the Intolerance of Uncertainty Scale: Initial development of the IUS-5 [Preprint]. PsyArXiv. 2020. [CrossRef]
- Gross JJ, John OP. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348-62. [CrossRef]
- Lumley MA, Schubiner H. Emotional awareness and expression therapy for chronic pain: Rationale, principles and techniques, evidence, and critical review. Curr Rheumatol Rep. 2019;21(7):1-8.
- Norman-Nott N, Briggs NE, Hesam-Shariati N, et al. Online dialectical behavioral therapy for emotion dysregulation in people with chronic pain: A randomized clinical trial. JAMA Netw Open. 2025;8(5):e256908. [CrossRef]
Figure 1.
The synthesis process (search and concept output).
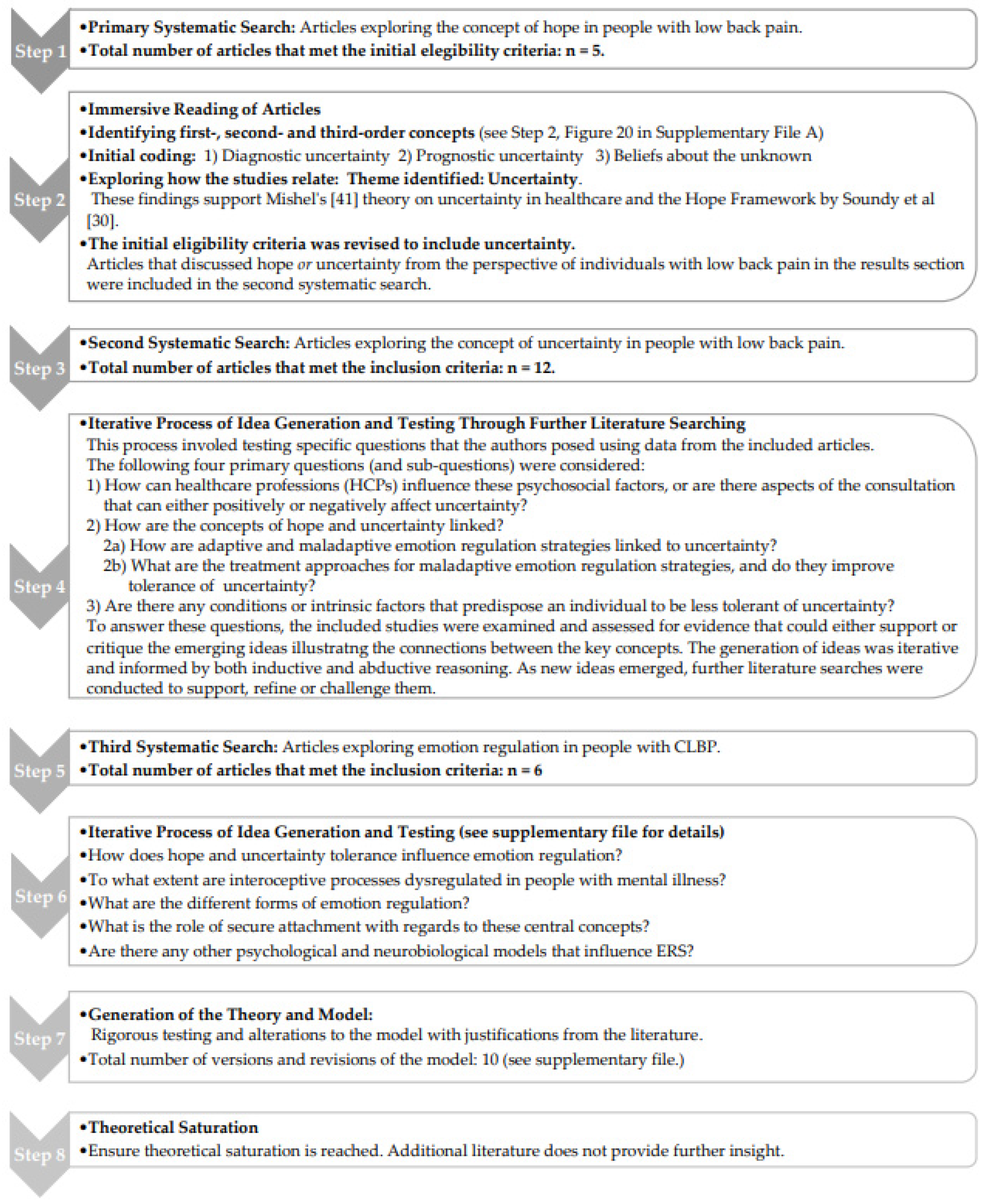
Figure 2.
Presents the PRISMA flow diagram that outlines the results of the first systematic search for articles exploring the concept of hope in people with CLBP [42].
Figure 2.
Presents the PRISMA flow diagram that outlines the results of the first systematic search for articles exploring the concept of hope in people with CLBP [42].
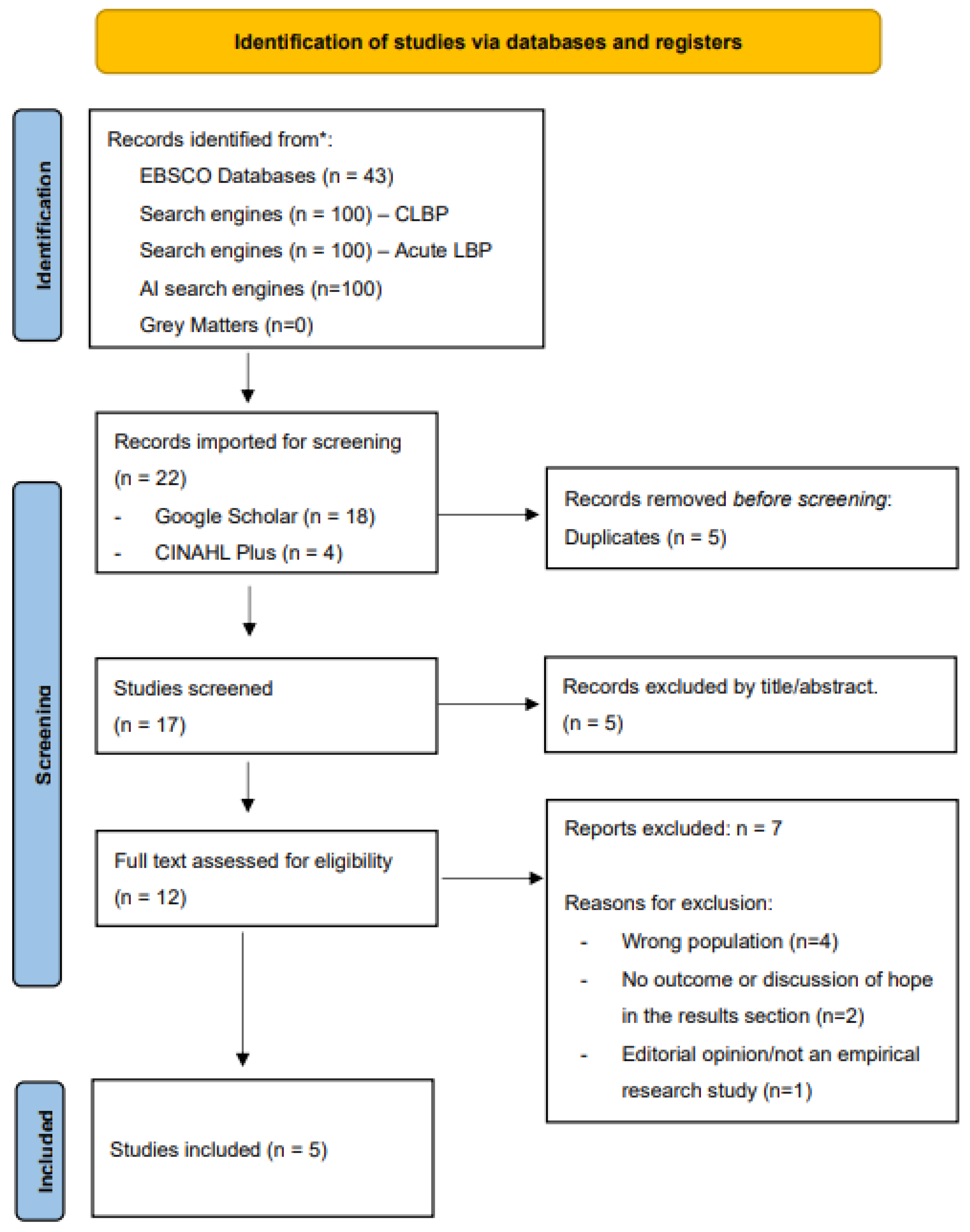
Figure 3.
Presents the PRIMSA flow diagram that outlines the results of the second systematic search for articles exploring the concept of uncertainty in people with CLBP [42].
Figure 3.
Presents the PRIMSA flow diagram that outlines the results of the second systematic search for articles exploring the concept of uncertainty in people with CLBP [42].
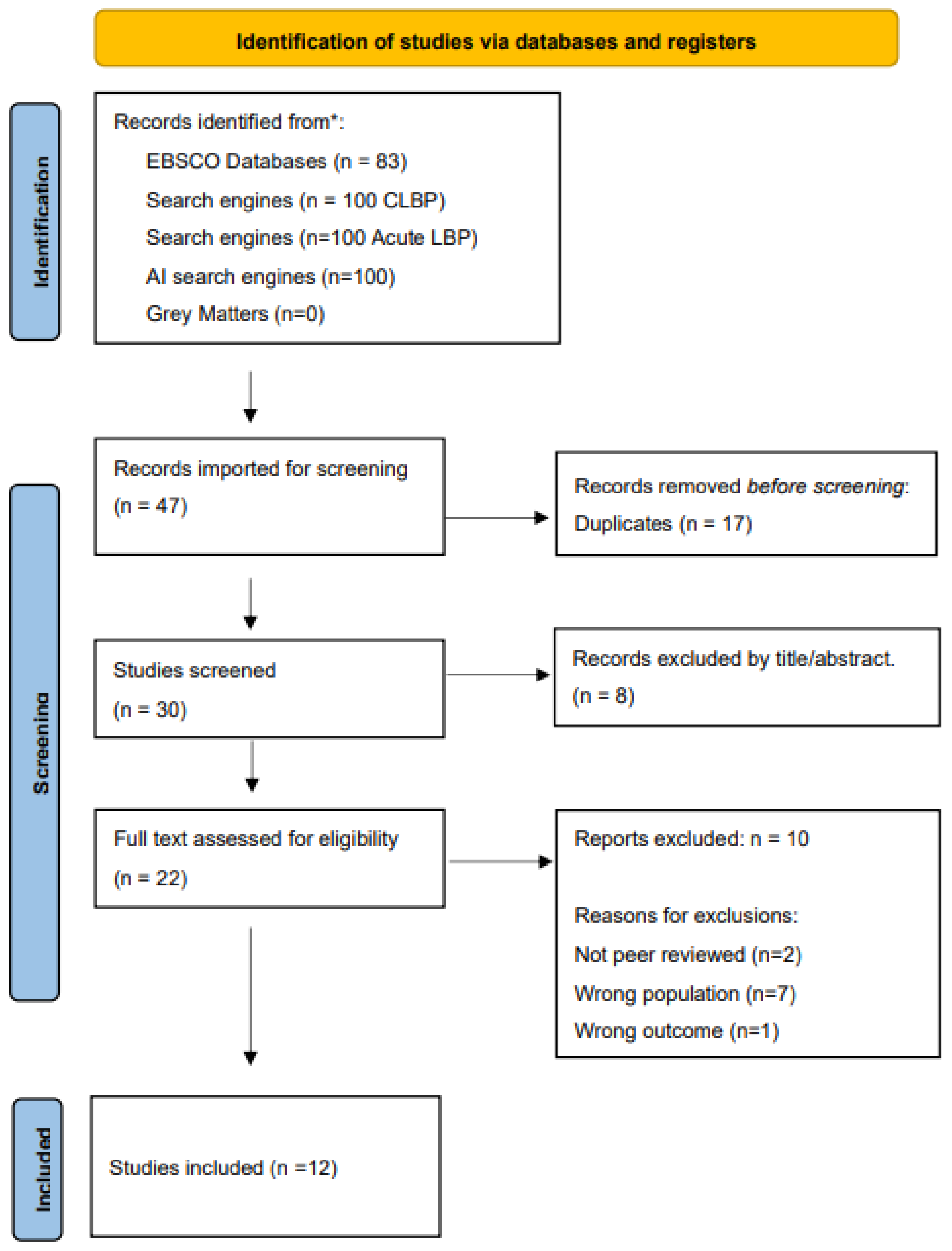
Figure 4.
Presents the PRIMSA flow diagram that outlines the results of the third systematic search for articles exploring the concept of emotional regulation in people with CLBP [42].
Figure 4.
Presents the PRIMSA flow diagram that outlines the results of the third systematic search for articles exploring the concept of emotional regulation in people with CLBP [42].
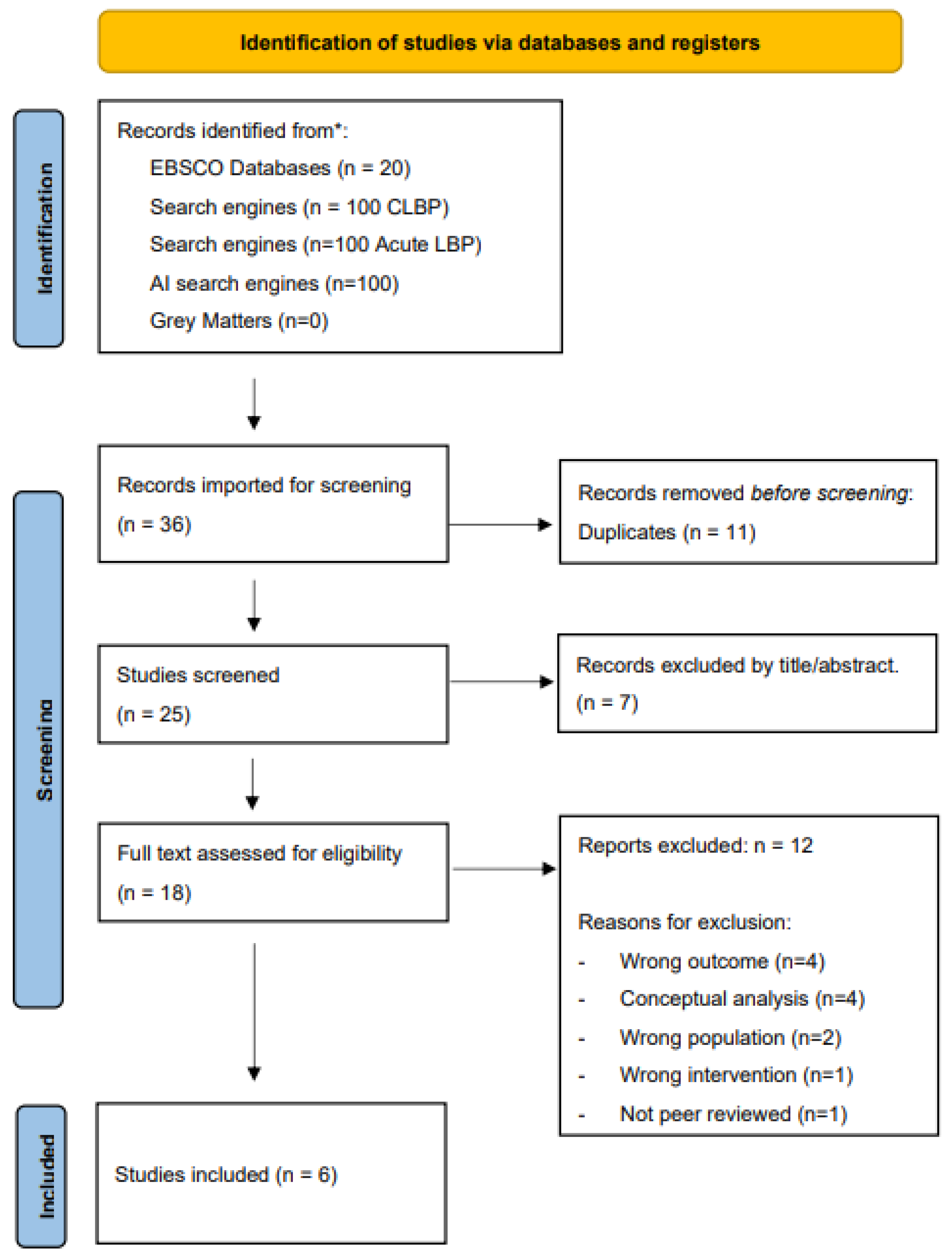
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



