
Submitted:
17 October 2024
Posted:
18 October 2024
You are already at the latest version
Abstract
Aim: To determine the clinical performance association of periodontal disease with diabetes mellitus, using an umbrella review. Material and Methods: An information search was carried out up to August 2023 in the following electronic databases: PubMed, Cochrane database, Scopus, SciELO, Google Scholar and OpenGrey. We included studies that were systematic reviews (SR) with or without meta-analysis, without time and language restrictions, that evaluated primary studies that evaluated the association between periodontal disease with diabetes mellitus. Literature or narrative reviews, rapid reviews, intervention studies, observational studies, preclinical and basic research, abstracts, comments, case reports, protocols, personal opinions, letters, and posters were excluded. The AMSTAR-2 tool was used to determine the methodological quality of the included studies. Results: The preliminary search yielded a total of 577 articles, discarding those that did not meet the selection criteria, leaving only 17 articles. An association was found between periodontal disease and diabetes mellitus (type 1 and type 2 diabetes mellitus and gestational diabetes mellitus). Conclusion: Based on the results and conclusions of the SR with a high overall confidence, periodontal disease is associated with the onset of type 1 and type 2 diabetes mellitus and gestational diabetes.
Keywords:
periodontal disease
; diabetes mellitus
; review
1. Introduction
Diabetes mellitus (DM) is a common metabolic disease resulting from a defect in insulin secretion, a defect in insulin action, or a combination of both [1,2]. This chronic disease is one of the most common in the world and the prevalence is expected to increase by almost 50% in the coming years. It is estimated that there will be around 700 million people living with diabetes by 2045 and it will be within the five main causes of death [3]. Mortality is due to its complications in microvascular changes, neuropathy, retinopathy and nephropathy, delayed healing, and the sixth important problem of people with diabetes is periodontitis [4,5].
Periodontitis is a disease characterized by chronic inflammation of the entire periodontium that can irreparably destroy the tissue surrounding the tooth, leading to gingival bleeding, increased tooth mobility and tooth loss [6]. It is estimated that approximately between 20 and 60% of the world's population suffers from periodontal disease [7,8].
DM and periodontal disease (PD) are associated with each other, despite not having a common pathophysiology [6]. However, glucose alteration in these patients shows a positive association, which is evident in patients with poorly controlled diabetes having an 86% higher risk of developing periodontitis than non-diabetics or those with well-controlled diabetes [4]. Furthermore, there are indications that PD is a risk factor for diabetes mellitus, which shows a possible bidirectional association [3]. The proposed link between the two diseases is based on the characteristics of the immune response, neutrophil function, and cytokine biology [9,10].
Given the need for dentists to know the association of these diseases and the short- and long-term consequences, there is a need for a better understanding of the scientific basis using the highest quality evidence available for clinical decision making [11]. The synthesis of knowledge facilitates clinical decisions, finding information in a single document, thus facilitating the reading and understanding of a particular topic. To date, no comprehensive synthesis or evaluation of all systematic reviews, including those from recent years, has been performed. Therefore, the aim of this overview was to consolidate the available evidence and address the following question: “What is our current understanding of the link between periodontal disease and diabetes mellitus?”, in addition to assessing the general confidence in systematic reviews that analyze this issue.
2. Materials and Methods
2.1. Protocol and Registration
Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) [12], the procedure was executed and subsequently registered in the Prospective Registry of Systematic Reviews (PROSPERO) [13]. The registry can be accessed by the general public with the number CRD42023464043. Furthermore, the PRIO-harms (Preferred Reporting Items for Overview of Systematic Reviews Checklist) form the basis of this study´s report [14]. Notably, our methodology was based on Pauletto et al. [15], given its similarity to our approach. Ethical approval was not required for this umbrella review.
2.2. Eligibility Requirements and Notewhorthy Results
All included articles were systematic reviews (SR) that assessed primary research assessing the relationship between PD and DM, whether or not it has meta-analysis, and without regard to time or language constraints.
Exclusions included abstracts, remarks, case reports, procedures, personal opinions, letters, posters, fast reviews, intervention studies, observational studies, preclinical and fundamental research, and literature or narrative reviews.
2.3. Information Sources, Search Tactics and Further Searches for Primary Studies
August 20, 2023 saw the completion of an electronic search across four databases: Pubmed, Cochrane database, Scielo, and Scopus. We also looked up gray literature using OpenGrey and Google Scholar. The included studies´reference lists were also examined. Duplicate articles were removed from the found articles and exported to Zotero®, a reference management program developed by the Center for History and New Media in Virginia, USA. Table 1 lists the search approach used for each database.
2.4. Data Management and Selection Process
The identified articles were inserted into Rayyan® Online Software (Qatar Research Institute of Computing, Qatar). The selection of the studies was carried out in 2 phases: in phase 1, two reviewers (F.C.O. and E.I.) independently selected the studies by reading the title and abstract; subsequently, phase 2 was carried out, which consisted of reading the full text, carried out independently by the same two reviewers. A third reviewer (F.C.Z.) was consulted in case of disagreement.
2.5. Data Collection Process
Data from the study were independently collected in duplicate using a table previously formulated by two reviewers (E.B. and W.T.). Data were cross-checked and disagreements resolved by the third review author (P.H.). The following information was extracted from the selected articles: authors, year of publication, study design, design of primary studies included, number of studies included in the qualitative and quantitative analysis, country, type of diabetes, results, main conclusions, and the mention of the following were used or executed: Mata-analysis, PRISMA, PROSPERO, and Grading of Recommendations Assessment, Development and Evaluation (GRADE).
2.6. Evaluation of Meta-Bias, Evidence Quality, and Methodological Quality
Two reviewers (O.S. and R.O.) independently and in duplicate assessed the methodological quality of the included SRs using the AMSTAR-2 checklist (A MeaSurement Tool to Assess Systemic Reviews), which was calibrated (Kappa 0.85) [16]. With 16 questions that have three alternative answers - "yes", "no" or "partially yes"- the AMSTAR-2 assesses the methodological quality of the SR. Shea et al. [16] rated the study´s overall confidence level, which was classified as high, moderate, low, and severely low.
2.7. Measurement Summary
We took into account the study´s findings in the event of an SR meta-analysis. The results that were displayed with a mean difference, normalized mean difference, relative risk, or odds ratio are taken into consideration if the SR offers meta-analysis.
2.8. Results Summary
The primary findings of the included SRs were compiled and categorized into the following categories: number of teeth, clinical attachment level, prevalence, general association, plaque index, gingival index, probing depth, and bleeding on probing.
3. Results
3.1. Examining and Choosing Original Research
After duplicates were removed, 519 references were left from 572 that the electronic database search had originally yielded. Phase 1 involved evaluating the titles and abstracts of the selected studies and taking into consideration 12 papers that could be read in full. After two more articles from other umbrella reviews and four articles added through various means, there were only eighteen SRs left for the quality synthesis. Table 2 provides the rationale behind the article´s exclusion. Figure 1 depicts the entire identification and selection procedure for the research.
3.2. Review and Characteristics of Included Studies
The SRs included were published between 2009 and 2023 and were published in English. They were carried out in Portugal [10], Peru [24], Malaysia [25], China [26,27], Germany [3], Italy [28,29,30], Australia [31], Japan [32], Denmark [33], Netherlands [34], Spain [35], Brazil [36,37] and United States [38,39]. More information on SR characteristics can be found in Table 3.
3.3. Assessment of Methodological Quality and Quality of Evidence:
3.4. Overlapping
A total of 296 primary studies were identified within the SRs. Of these, approximately 17.26% of the primary studies were included in more than one SR. Thirty-five studies were included twice, eight were included three times, and seven were included four times. More information on the overlap and characteristics of the primary studies is available in Table 5.
3.5. Synthesis of Results
The syntheses of the results are presented in Table 3.
3.6. General Association
Eleven SRs [3,10,24,27,28,30,31,33,34,38,39] included reported that there were an association between PD and DM, while 2 SRs [32,36] reported that there was no association. Six SRs [3,28,33,34,36,38] meta-analyzed the results, where they found that the relative risk ratio ranged from 1.26 (CI: 1.12 to 1.41) [3] to 1.86 (CI: 1.25 to 2.77) [33] and the odds ratio ranged from 1.69 (CI: 0.68 to 4.21) [36] to 2.59 (CI: 2.12 to 3.15) [34]. Costa et al. [10], León-Ríos et al. [24], Nguyen et al. [31], Graziani et al. [30], Ismail et al. [27] and Borgnakke et al. [39] they presented the results descriptively and reported an association between PD and DM; while Tanaka et al. [32] reported that there is no association between PD and DM.
3.7. Plaque Index
3.8. Gingival Index
3.9. Clinical Attachment Level
Four SRs [25,26,28,29] included reported that there is an association between PD and DM, while 1 SR [37] reported that there is an association between PD and type 2 diabetes mellitus (T2DM) but not with type 1 diabetes mellitus (T1DM). All meta-analyzed the results, where they found that the mean difference ranged from 0.26 (CI: 0.00 to 0.53) to 1.00 (CI: 0.15 to 1.84) [37] and the standardized mean difference range from 0.47 (CI: 0.37 to 0.57) [28] to 0.82 (CI: 0.59 to 1.04) [29].
3.10. Number of Teeth
One SR [26] included reported that there is an association between PD and DM. The mean difference, according to the study's meta-analysis, was -2.14 (CI: -2.87 to -1.40).
3.11. Prevalence
Three SRs [26,28,35] included reported that there is an association between PD and DM. Two SRs [26,28] meta-analyzed the results, where they found that the odds ratio ranged from 0.19 (CI: 0.08 to 0.37) [28] to 1.85 (CI: 1.61 to 2.11) [26]. Mauri-Obradors et al. [35] presented the results descriptively and reported an association between PD and DM.
3.12. Probing Depth
Three SRs [25,26,29] included reported that there is an association between PD and DM, while 1 SR [37] reported that there is an association between PD and T2DM but not with T1DM. All meta-analyzed the results, where they found that the mean difference ranged from 0.11 (CI: -0.03 to 0.25) to 0.46 (CI: 0.01 to 0.91) [37] and the standardized mean difference ranged from 0.36 (CI: 0.16 to 0.55) [29] to 0.67 (CI: 0.23 to 1.11) [25].
3.13. Bleeding on Probing
Three SRs [25,26,29] included reported that there is an association between PD and DM. The two studies meta-analyzed the results, where they found that the mean difference was 7.90 (CI: 4.24 to 11.56) [26] and standardized mean difference ranged from 0.32 (CI: 0.07 to 0.58) [25] to 0.65 (CI: 0.08 to 1.23) [29].
4. Discussion
The evaluation and analysis of the association between PD and systemic diseases, such as DM, has been of interest in recent years. Numerous RCTs have investigated this topic and report evidence supporting the association between these 2 diseases.
Some studies have evaluated this association in a general way, while other studies have evaluated it according to periodontal clinical parameters. To date, several SRs have been published that analyze the association between PD and DM, this has made it necessary to compile the data from these studies and assess the methodological quality of each one.
Currently, three umbrella reviews have been conducted, all three [11,93,94] reviewed the most current evidence on the nature of the relationship/association between PD and DM, however, they included studies that analyzed whether periodontal therapy was effective in people with DM; causing the results and conclusions of these studies to be taken with caution.
The present study conducted an exhaustive literature search to summarize the available SRs that deal with the association between PD and DM (T1DM, T2DM, and GDM), obtaining 18 SRs that matched the inclusion criteria and were taken into consideration for the analysis. SRs represent the highest level of the scientific evidence pyramid, but their results should be evaluated cautiously because they are likely biased.
The SRs included in this study showed certain limitations related to the selected primary studies, such as: the existence of different types of studies included, selection criteria for the studies to be included, the inclusion of different population groups (children, adolescents and adults), different diagnostic criteria for periodontal diseases and evaluation of different types of diabetes mellitus (T1DM, T2DM and GDM).
On the other hand, more than 50% of the included studies revealed a high level of confidence, which could increase the level of evidence for the results and conclusions offered in this study. However, the fact that SRs continue to be obtained without a high level of confidence points to the need for greater rigor in the development of this group of studies on this topic.
The current instrument, the AMSTAR-2, was used to assess the methodological quality of the included SRs. A factor that deserves to be highlighted in relation to the result of methodological quality is related to the critical domains 2, 4, 7, 9, 13, and 15 of AMSTAR - 2, since some SRs did not explicitly address their methods, they did not use a search strategy was exhaustive, they did not provide a list of excluded studies justifying their exclusion, they did not use a satisfactory technique to assess the risk of bias, they did not consider the risk of bias of the included studies to interpret or discuss their results, and they did not report the bias of publication; highlighting the need to include these elements in the development of future SRs.
Additionally, caution should be taken as some studies in the SRs were included more than once, leading to data from the included studies being reevaluated multiple times, which could increase the perception of what has been done. Although it would be interesting to carry out new SRs to overcome the methodological limitations recommended by Moher [95], due to the high rate of overlap, it is more important to carry out well-conducted RCTs, with long-term follow-up and coming from different research groups to expand knowledge on this topic.
4.1. Evidence Summary
The present umbrella review was carried out seeking to assist in the association between PD and DM with the purpose of minimizing biases and random errors in SRs and meta-analyses on the subject. The material below can be summed up and discussed while keeping in mind the limitations of SRs used in this study.
The SRs included in this study suggested a general association between PD and DM. This result is similar to that reported by the Consensus Report of the European Federation of Periodontics [17] where they point out that periodontitis is associated with diabetes mellitus. However, two of the included studies [32,36] report no association between these 2 diseases, this was due to the fact that one [32] of them focused only on the Japanese population, concluding that there was little evidence on this topic in the said population group, while, the another study [36] performed a subgroup analysis by type of primary study included, concluding that in the cross-sectional studies the association did exist but in the case-control studies the association did not exist.
In terms of plaque index, gingival index, number of missing teeth, prevalence, and bleeding on probing; studies indicate that patients with DM have a greater probability of presenting with an increase in all these clinical parameters, indicating that there is an association between PD and DM.
Regarding the depth of catheterization and the clinical attachment level, studies also indicate that patients with DM have a greater probability of presenting with an increase in all these clinical parameters. However, one study [37] indicated that there is an association between PD and T2DM but not with T1DM.
Furthermore, it should be noted that of the included studies: four [10,27,28,29] analyze T1DM, with only one [10] having high overall confidence; three [24,36,38] analyzing GDM where all have high overall confidence; and ten [3,25,26,30,31,32,33,35,37,39] analyzing DM in general, eight [3,25,26,30,33,35,37,39] of which They have high general confidence.
4.2. Implications for Clinical Practice
There is an association between PD and DM, therefore, a correct anamnesis and a correct diagnosis must be made to be able to present the best viable, simple, and less invasive treatment options to this group of patients.
4.3. Implications for Research
Despite the high number of SRs, it was evident from this assessment that their reporting has to be improved immediately. The observation of instruments that direct their evolution, including quality evaluation tools, is the author´s recommendation for upcoming SRs. In order to get more reliable results, additional SRs on the relationship between PD and MGD should be conducted with strong methodological rigor. It is also recommended for future primary studies to use the latest definition related to the diagnosis of periodontal diseases.
5. Conclusions
According to the findings of this umbrella review, there is strong evidence supporting the association between periodontal disease and various forms of diabetes mellitus, including type 1 and type 2, and gestational diabetes. The studies reviewed demonstrate a consistent relationship across different clinical parameters, such as plaque index, gingival index, clinical attachment level, probing depth, and bleeding on probing, with diabetes patients showing a higher likelihood of presenting worsened periodontal conditions.
Author Contributions
Conceptualization, H.A.; methodology, H.A and F.C.O.; software, F.C.Z.; validation, E.I., E.B. and W.T.; formal analysis, P.H.; investigation, F.C.O.; resources, O.S.; data curation, R.O.; writing—original draft preparation, F.C.Z.; writing—review and editing, W.T. and P.H.; visualization, E.B.; supervision, H.A.; project administration, E.I.; funding acquisition, F.C.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable. No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wu C-Z, Yuan Y-H, Liu H-H, Li S-S, Zhang B-W, Chen W, et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health. 2020;20(1):204. [CrossRef]
- Al Ansari Y, Shahwan H, Chrcanovic BR. Diabetes mellitus and dental implants: A systematic review and meta-analysis. Materials (Basel). 2022;15(9):3227. [CrossRef]
- Stöhr J, Barbaresko J, Neuenschwander M, Schlesinger S. Bidirectional association between periodontal disease and diabetes mellitus: a systematic review and meta-analysis of cohort studies. Sci Rep. 2021;11(1):13686. [CrossRef]
- Alwithanani N. Periodontal diseases and diabetes mellitus: A systematic review. J Pharm Bioallied Sci. 2023;15(Suppl 1):S54–63. [CrossRef]
- Ahmadinia AR, Rahebi D, Mohammadi M, Ghelichi-Ghojogh M, Jafari A, Esmaielzadeh F, et al. Association between type 2 diabetes (T2D) and tooth loss: a systematic review and meta-analysis. BMC Endocr Disord. 2022;22(1):100. [CrossRef]
- Sanz M, Ceriello A, Buysschaert M, Chapple I, Demmer RT, Graziani F, et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res Clin Pract. 2018;137:231–41. [CrossRef]
- Gobin R, Tian D, Liu Q, Wang J. Periodontal diseases and the risk of metabolic syndrome: An updated systematic review and meta-analysis. Front Endocrinol (Lausanne). 2020;11:336. [CrossRef]
- Păunică I, Giurgiu M, Dumitriu AS, Păunică S, Pantea Stoian AM, Martu M-A, et al. The bidirectional relationship between periodontal disease and diabetes mellitus-A review. Diagnostics (Basel). 2023;13(4). [CrossRef]
- Siddiqi A, Zafar S, Sharma A, Quaranta A. Diabetes mellitus and periodontal disease: The call for interprofessional education and interprofessional collaborative care - A systematic review of the literature. J Interprof Care. 2022;36(1):93–101. [CrossRef]
- Costa R, Ríos-Carrasco B, Monteiro L, López-Jarana P, Carneiro F, Relvas M. Association between type 1 diabetes mellitus and periodontal diseases. J Clin Med. 2023;12(3). [CrossRef]
- Natto ZS, Hameedaldain A. Methodological quality assessment of meta-analyses and Systematic Reviews of the relationship between periodontal and systemic diseases. J Evid Based Dent Pract. 2019;19(2):131–9. [CrossRef]
- Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350(jan02 1):g7647. [CrossRef]
- Booth A, Clarke M, Ghersi D, Moher D, Petticrew M, Stewart L. An international registry of systematic-review protocols. Lancet. 2011;377(9760):108–9. [CrossRef]
- Bougioukas KI, Liakos A, Tsapas A, Ntzani E, Haidich A-B. Preferred reporting items for overviews of systematic reviews including harms checklist: a pilot tool to be used for balanced reporting of benefits and harms. J Clin Epidemiol. 2018;93:9–24. [CrossRef]
- Pauletto P, Ruales-Carrera E, Mezzomo LA, Stefani CM, Taba M Jr, Gonçalves RB, et al. Clinical performance of short versus standard dental implants in vertically augmented bone: an overview of systematic reviews. Clin Oral Investig. 2021;25(11):6045–68. [CrossRef]
- Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;j4008. [CrossRef]
- Herrera D, Sanz M, Shapira L, Brotons C, Chapple I, Frese T, et al. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: Consensus report of the Joint Workshop by the European Federation of Periodontology (EFP) and the European arm of the World Organization of Family Doctors (WONCA Europe). J Clin Periodontol. 2023;50(6):819–41. [CrossRef]
- Li L-L, Xie X-T, Wu Y, Yan F-H. Advances in research on the mechanism of association between periodontitis and diabetes mellitus. Sichuan Da Xue Xue Bao Yi Xue Ban. 2023;54(1):71–6. [CrossRef]
- George AK, Wills V. Association between periodontal diseases and gestational diabetes mellitus-A review. Kerala Dent J. 2020;43(2):82–4.
- Bansal S, Dhir S, Wangnoo SK. Diabetes mellitus and periodontitis: Relevance of the diabolic duo in India. Apollo Med. 2020;17(4):267–71. [CrossRef]
- Laddha R, Jones AH, Patil A. Relationship between diabetes and periodontitis:A systematic review. Indian J Public Health Res Dev. 2019;10(12):843. [CrossRef]
- Salvi GE, Carollo-Bittel B, Lang NP. Effects of diabetes mellitus on periodontal and peri-implant conditions: update on associations and risks. J Clin Periodontol. 2008;35(8 Suppl):398–409. [CrossRef]
- Mealey BL, Oates TW, American Academy of Periodontology. Diabetes mellitus and periodontal diseases. J Periodontol. 2006;77(8):1289–303. [CrossRef]
- León-Ríos XA, Da Silva Pires S, Gil-Montoya JA. Association between gestational diabetes mellitus and periodontal disease: Systematic review. Clin E Investig En Ginecol Obstet. 2022;49(4):1–11.
- Zainal Abidin Z, Zainuren ZA, Noor E, Mohd Nor NS, Mohd Saffian S, Abdul Halim R. Periodontal health status of children and adolescents with diabetes mellitus: a systematic review and meta-analysis. Aust Dent J. 2021;66 Suppl 1(S1):S15–26. [CrossRef]
- Zheng M, Wang C, Ali A, Shih YA, Xie Q, Guo C. Prevalence of periodontitis in people clinically diagnosed with diabetes mellitus: a meta-analysis of epidemiologic studies. Acta Diabetol. 2021;58(10):1307–27. [CrossRef]
- Ismail AF, McGrath CP, Yiu CKY. Oral health of children with type 1 diabetes mellitus: A systematic review. Diabetes Res Clin Pract. 2015;108(3):369–81. [CrossRef]
- Dicembrini I, Serni L, Monami M, Caliri M, Barbato L, Cairo F, et al. Type 1 diabetes and periodontitis: prevalence and periodontal destruction-a systematic review. Acta Diabetol. 2020;57(12):1405–12. [CrossRef]
- Rapone B, Corsalini M, Converti I, Loverro MT, Gnoni A, Trerotoli P, et al. Does periodontal inflammation affect type 1 diabetes in childhood and adolescence? A Meta-analysis. Front Endocrinol (Lausanne). 2020;11:278. [CrossRef]
- Graziani F, Gennai S, Solini A, Petrini M. A systematic review and meta-analysis of epidemiologic observational evidence on the effect of periodontitis on diabetes An update of the EFP-AAP review. J Clin Periodontol. 2018;45(2):167–87. [CrossRef]
- Nguyen ATM, Akhter R, Garde S, Scott C, Twigg SM, Colagiuri S, et al. The association of periodontal disease with the complications of diabetes mellitus. A systematic review. Diabetes Res Clin Pract. 2020;165(108244):108244. [CrossRef]
- Tanaka H, Ihana-Sugiyama N, Sugiyama T, Ohsugi M. Contribution of diabetes to the incidence and prevalence of comorbid conditions (cancer, periodontal disease, fracture, impaired cognitive function, and depression): A systematic review of epidemiological studies in Japanese populations. J Epidemiol. 2019;29(1):1–10. [CrossRef]
- Nascimento GG, Leite FRM, Vestergaard P, Scheutz F, López R. Does diabetes increase the risk of periodontitis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta Diabetol. 2018;55(7):653–67. [CrossRef]
- Ziukaite L, Slot DE, Van der Weijden FA. Prevalence of diabetes mellitus in people clinically diagnosed with periodontitis: A systematic review and meta-analysis of epidemiologic studies. J Clin Periodontol. 2018;45(6):650–62. [CrossRef]
- Mauri-Obradors E, Estrugo-Devesa A, Jane-Salas E, Vinas M, Lopez-Lopez J. Oral manifestations of Diabetes Mellitus. A systematic review. Med Oral Patol Oral Cir Bucal. 2017;0–0. [CrossRef]
- Esteves Lima RP, Cyrino RM, de Carvalho Dutra B, Oliveira da Silveira J, Martins CC, Miranda Cota LO, et al. Association between periodontitis and gestational diabetes mellitus: Systematic review and meta-analysis. J Periodontol. 2016;87(1):48–57. [CrossRef]
- Chávarry NGM, Vettore MV, Sansone C, Sheiham A. The relationship between diabetes mellitus and destructive periodontal disease: a meta-analysis. Oral Health Prev Dent. 2009;7(2):107–27.
- Abariga SA, Whitcomb BW. Periodontitis and gestational diabetes mellitus: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth. 2016;16(1):344. [CrossRef]
- Borgnakke WS, Ylöstalo PV, Taylor GW, Genco RJ. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. J Periodontol. 2013;84(4 Suppl):S135-52. [CrossRef]
- Bullon P, Jaramillo R, Santos-Garcia R, Rios-Santos V, Ramirez M, Fernandez-Palacin A, et al. Relation of periodontitis and metabolic syndrome with gestational glucose metabolism disorder. J Periodontol. 2014;85(2):e1-8. [CrossRef]
- Al-Khabbaz AK, Al-Shammari KF, Hasan A, Abdul-Rasoul M. Periodontal health of children with type 1 diabetes mellitus in Kuwait: a case-control study. Med Princ Pract. 2013;22(2):144–9. [CrossRef]
- Esteves Lima RP, Miranda Cota LO, Costa FO. Association between periodontitis and gestational diabetes mellitus: a case-control study. J Periodontol. 2013;84(9):1257–65. [CrossRef]
- Chokwiriyachit A, Dasanayake AP, Suwannarong W, Hormdee D, Sumanonta G, Prasertchareonsuk W, et al. Periodontitis and gestational diabetes mellitus in non-smoking females. J Periodontol. 2013;84(7):857–62. [CrossRef]
- Morita I, Inagaki K, Nakamura F, Noguchi T, Matsubara T, Yoshii S, et al. Relationship between periodontal status and levels of glycated hemoglobin. J Dent Res. 2012;91(2):161–6. [CrossRef]
- Xiong X, Elkind-Hirsch KE, Vastardis S, Delarosa RL, Pridjian G, Buekens P. Periodontal disease is associated with gestational diabetes mellitus: a case-control study. J Periodontol. 2009;80(11):1742–9. [CrossRef]
- Dakovic D, Pavlovic MD. Periodontal disease in children and adolescents with type 1 diabetes in Serbia. J Periodontol. 2008;79(6):987–92. [CrossRef]
- Dasanayake AP, Chhun N, Tanner ACR, Craig RG, Lee MJ, Moore AF, et al. Periodontal pathogens and gestational diabetes mellitus. J Dent Res. 2008;87(4):328–33. [CrossRef]
- Saito T, Shimazaki Y, Kiyohara Y, Kato I, Kubo M, Iida M, et al. The severity of periodontal disease is associated with the development of glucose intolerance in non-diabetics: the Hisayama study. J Dent Res. 2004;83(6):485–90. [CrossRef]
- Sun K-T, Chen S-C, Lin C-L, Hsu J-T, Chen I-A, Wu I-T, et al. The association between Type 1 diabetes mellitus and periodontal diseases. J Formos Med Assoc. 2019;118(6):1047–54. [CrossRef]
- Ismail AF, McGrath CP, Yiu CKY. Oral health status of children with type 1 diabetes: a comparative study. J Pediatr Endocrinol Metab. 2017;30(11). [CrossRef]
- Chiu SY-H, Lai H, Yen AM-F, Fann JC-Y, Chen L-S, Chen H-H. Temporal sequence of the bidirectional relationship between hyperglycemia and periodontal disease: a community-based study of 5,885 Taiwanese aged 35-44 years (KCIS No. 32). Acta Diabetol. 2015;52(1):123–31. [CrossRef]
- Habib FA. Evaluation of periodontal status among saudi females with gestational diabetes and its relation to glucose and lipid homeostasis in ohud hospital, Al madina Al-munwarrah. Int J Health Sci (Qassim). 2009;3(2):143–54.
- Orbak R, Simsek S, Orbak Z, Kavrut F, Colak M. The influence of type-1 diabetes mellitus on dentition and oral health in children and adolescents. Yonsei Med J. 2008;49(3):357–65. [CrossRef]
- Lalla E, Cheng B, Lal S, Tucker S, Greenberg E, Goland R, et al. Periodontal changes in children and adolescents with diabetes: a case-control study. Diabetes Care. 2006;29(2):295–9. [CrossRef]
- Aren G, Sepet E, Ozdemir D, Dinççağ N, Güvener B, Firatli E. Periodontal health, salivary status, and metabolic control in children with type 1 diabetes mellitus. J Periodontol. 2003;74(12):1789–95. [CrossRef]
- Sbordone L, Ramaglia L, Barone A, Ciaglia RN, Iacono VJ. Periodontal status and subgingival microbiota of insulin-dependent juvenile diabetics: a 3-year longitudinal study. J Periodontol. 1998;69(2):120–8. [CrossRef]
- Firatli E. The relationship between clinical periodontal status and insulin-dependent diabetes mellitus. Results after 5 years. J Periodontol. 1997;68(2):136–40. [CrossRef]
- Pinson M, Hoffman WH, Garnick JJ, Litaker MS. Periodontal disease and type I diabetes mellitus in children and adolescents. J Clin Periodontol. 1995;22(2):118–23. [CrossRef]
- Roy M, Gastaldi G, Courvoisier DS, Mombelli A, Giannopoulou C. Periodontal health in a cohort of subjects with type 1 diabetes mellitus. Clin Exp Dent Res. 2019;5(3):243–9. [CrossRef]
- Babu KLG, Subramaniam P, Kaje K. Assessment of dental caries and gingival status among a group of type 1 diabetes mellitus and healthy children of South India - a comparative study. J Pediatr Endocrinol Metab. 2018;31(12):1305–10. [CrossRef]
- Myllymäki V, Saxlin T, Knuuttila M, Rajala U, Keinänen-Kiukaanniemi S, Anttila S, et al. Association between periodontal condition and the development of type 2 diabetes mellitus-Results from a 15-year follow-up study. J Clin Periodontol. 2018;45(11):1276–86. [CrossRef]
- Chaparro A, Zúñiga E, Varas-Godoy M, Albers D, Ramírez V, Hernández M, et al. Periodontitis and placental growth factor in oral fluids are early pregnancy predictors of gestational diabetes mellitus. J Periodontol. 2018;89(9):1052–60. [CrossRef]
- Winning L, Patterson CC, Neville CE, Kee F, Linden GJ. Periodontitis and incident type 2 diabetes: a prospective cohort study. J Clin Periodontol. 2017;44(3):266–74. [CrossRef]
- Jindal A, Parihar AS, Sood M, Singh P, Singh N. Relationship between severity of periodontal disease and control of diabetes (glycated hemoglobin) in patients with Type 1 diabetes mellitus. J Int Oral Health. 2015;7(Suppl 2):17–20.
- Popławska-Kita A, Siewko K, Szpak P, Król B, Telejko B, Klimiuk PA, et al. Association between type 1 diabetes and periodontal health. Adv Med Sci. 2014;59(1):126–31. [CrossRef]
- Amiri AA, Maboudi A, Bahar A, Farokhfar A, Daneshvar F, Khoshgoeian HR, et al. Relationship between type 2 diabetic retinopathy and periodontal disease in Iranian adults. N Am J Med Sci. 2014;6(4):190.
- Lee K-S, Kim E-K, Kim J-W, Choi Y-H, Mechant AT, Song K-B, et al. The relationship between metabolic conditions and prevalence of periodontal disease in rural Korean elderly. Arch Gerontol Geriatr. 2014;58(1):125–9. [CrossRef]
- Jimenez M, Hu FB, Marino M, Li Y, Joshipura KJ. Type 2 diabetes mellitus and 20-year incidence of periodontitis and tooth loss. Diabetes Res Clin Pract. 2012;98(3):494–500. [CrossRef]
- Southerland JH, Moss K, Taylor GW, Beck JD, Pankow J, Gangula PR, et al. Periodontitis and diabetes associations with measures of atherosclerosis and CHD. Atherosclerosis. 2012;222(1):196–201. [CrossRef]
- Hodge PJ, Robertson D, Paterson K, Smith GLF, Creanor S, Sherriff A. Periodontitis in non-smoking type 1 diabetic adults: a cross-sectional study. J Clin Periodontol. 2012;39(1):20–9. [CrossRef]
- Ruiz DR, Romito GA, Dib SA. Periodontal disease in gestational and type 1 diabetes mellitus pregnant women: Periodontal disease in Brazilian GDM and T1DM pregnant women. Oral Dis. 2011;17(5):515–21. [CrossRef]
- Ide R, Hoshuyama T, Wilson D, Takahashi K, Higashi T. Periodontal disease and incident diabetes: a seven-year study: A seven-year study. J Dent Res. 2011;90(1):41–6. [CrossRef]
- Tagelsir A, Cauwels R, van Aken S, Vanobbergen J, Martens LC. Dental caries and dental care level (restorative index) in children with diabetes mellitus type 1: Dental caries and dental care level in Caries experience in diabetic children. Int J Paediatr Dent. 2011;21(1):13–22. [CrossRef]
- Abrao L, Chagas JK, Schmid H. Periodontal disease and risk for neuropathic foot ulceration in type 2 diabetes. Diabetes Res Clin Pract. 2010;90(1):34–9. [CrossRef]
- Demmer RT, Jacobs DR Jr, Desvarieux M. Periodontal disease and incident type 2 diabetes: results from the First National Health and Nutrition Examination Survey and its epidemiologic follow-up study. Diabetes Care. 2008;31(7):1373–9. [CrossRef]
- Shultis WA, Weil EJ, Looker HC, Curtis JM, Shlossman M, Genco RJ, et al. Effect of periodontitis on overt nephropathy and end-stage renal disease in type 2 diabetes. Diabetes Care. 2007;30(2):306–11. [CrossRef]
- Novak KF, Taylor GW, Dawson DR, Ferguson JE 2nd, Novak MJ. Periodontitis and gestational diabetes mellitus: exploring the link in NHANES III. J Public Health Dent. 2006 Summer;66(3):163–8. [CrossRef]
- Borges-Yáñez SA, Irigoyen-Camacho ME, Maupomé G. Risk factors and prevalence of periodontitis in community-dwelling elders in Mexico. J Clin Periodontol. 2006;33(3):184–94. [CrossRef]
- Mansour AA, Abd-Al-Sada N. Periodontal disease among diabetics in Iraq. MedGenMed. 2005;7(3):2.
- Campus G, Salem A, Uzzau S, Baldoni E, Tonolo G. Diabetes and periodontal disease: a case-control study. J Periodontol. 2005;76(3):418–25. [CrossRef]
- Saremi A, Nelson RG, Tulloch-Reid M, Hanson RL, Sievers ML, Taylor GW, et al. Periodontal disease and mortality in type 2 diabetes. Diabetes Care. 2005;28(1):27–32. [CrossRef]
- Siudikiene J, Maciulskiene V, Dobrovolskiene R, Nedzelskiene I. Oral hygiene in children with type I diabetes mellitus. Stomatologija. 2005;7(1):24–7.
- Noma H, Sakamoto I, Mochizuki H, Tsukamoto H, Minamoto A, Funatsu H, et al. Relationship between periodontal disease and diabetic retinopathy. Diabetes Care. 2004;27(2):615. [CrossRef]
- Marugame T, Hayasaki H, Lee K, Eguchi H, Matsumoto S. Alveolar bone loss associated with glucose tolerance in Japanese men: Original article. Diabet Med. 2003;20(9):746–51. [CrossRef]
- Zielinski MB, Fedele D, Forman LJ, Pomerantz SC. Oral health in the elderly with non-insulin-dependent diabetes mellitus. Spec Care Dentist. 2002;22(3):94–8. [CrossRef]
- Kawamura M, Fukuda S, Kawabata K, Iwamoto Y. Comparison of health behaviour and oral/medical conditions in non-insulin-dependent (type II) diabetics and non-diabetics. Aust Dent J. 1998;43(5):315–20. [CrossRef]
- Collin HL, Uusitupa M, Niskanen L, Kontturi-Närhi V, Markkanen H, Koivisto AM, et al. Periodontal findings in elderly patients with non-insulin dependent diabetes mellitus. J Periodontol. 1998;69(9):962–6. [CrossRef]
- Firatli E, Yilmaz O, Onan U. The relationship between clinical attachment loss and the duration of insulin-dependent diabetes mellitus (IDDM) in children and adolescents. J Clin Periodontol. 1996;23(4):362–6. [CrossRef]
- Thorstensson H, Kuylenstiema J, Hugoson A. Medical Status and complications in relation to periodontal disease experience in insulin-dependent diabetics. J Clin Periodontol. 1996;23(3):194–202. [CrossRef]
- Sbordone L, Ramaglia L, Barone A, Ciaglia RN, Tenore A, Iacono VJ. Periodontal status and selected cultivable anaerobic microflora of insulin-dependent juvenile diabetics. J Periodontol. 1995;66(6):452–61. [CrossRef]
- de Pommereau V, Dargent-Paré C, Robert JJ, Brion M. Periodontal status in insulin-dependent diabetic adolescents. J Clin Periodontol. 1992;19(9):628–32. [CrossRef]
- Sandholm L, Swanljung O, Rytömaa I, Kaprio EA, Mäenpää J. Periodontal status of Finnish adolescents with insulin-dependent diabetes mellitus. J Clin Periodontol. 1989;16(10):617–20. [CrossRef]
- Lavigne SE, Forrest JL. An umbrella review of systematic reviews examining the relationship between type 2 diabetes and periodontitis: Position paper from the Canadian Dental Hygienists Association. Can J Dent Hyg. 2021;55(1):57–67.
- Seitz MW, Listl S, Bartols A, Schubert I, Blaschke K, Haux C, et al. Current knowledge on correlations between highly prevalent dental conditions and chronic diseases: An umbrella review. Prev Chronic Dis. 2019;16(180641):E132. [CrossRef]
- Moher D. The problem of duplicate systematic reviews. BMJ. 2013;347(aug14 4):f5040. [CrossRef]
Figure 1.
PRISMA diagram showing the process of inclusion and exclusion of studies.
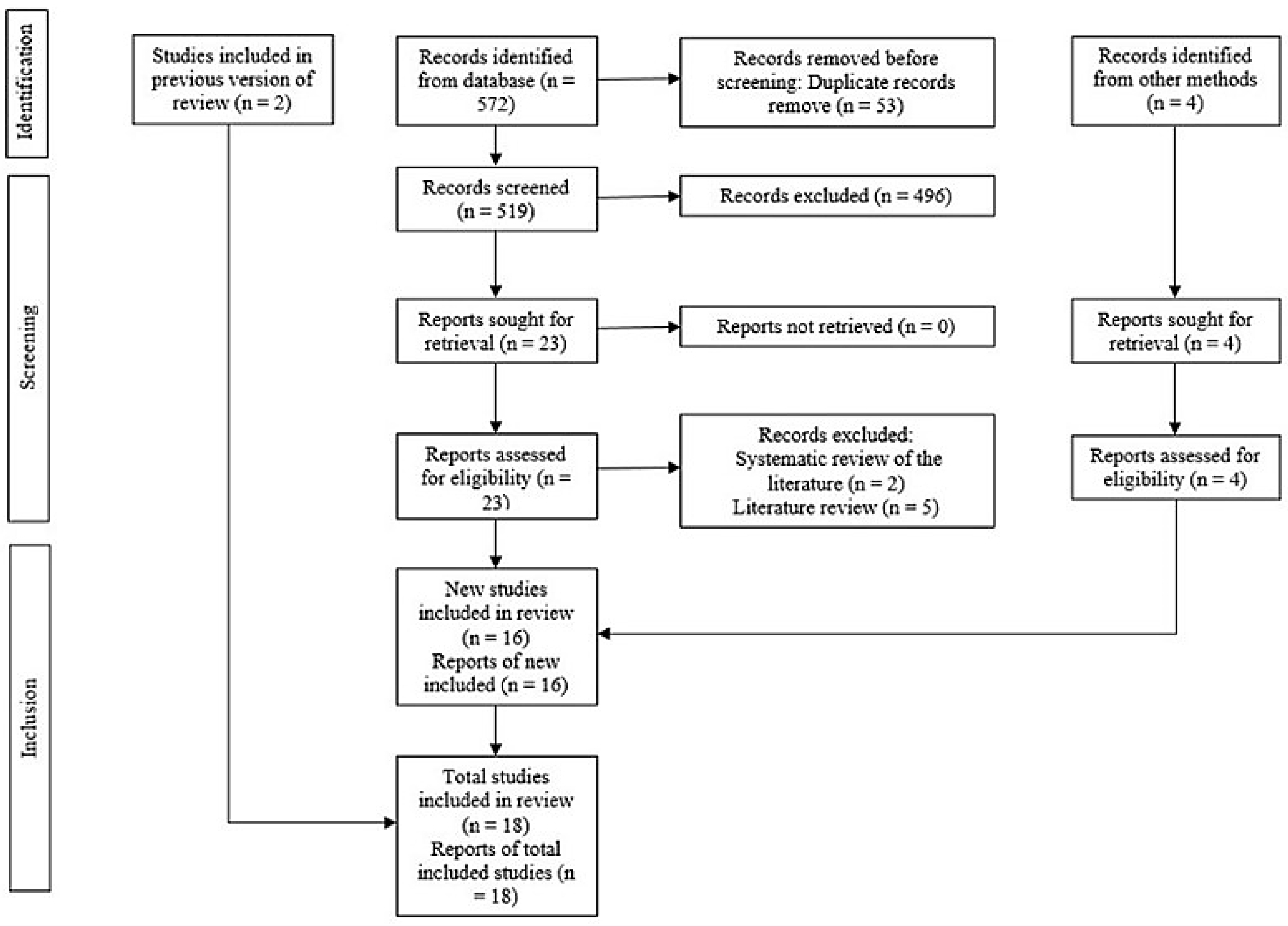

Table 1.
Database search strategy.
| Database | Search strategy | Number of studies |
|---|---|---|
| Pubmed | (("Periodontal disease") OR ("gingivitis") OR ("periodontitis")) AND (("Diabetes mellitus") OR ("DM1") OR ("DM2") OR ("gestacional diabetes") OR ("type 1 diabetes") OR ("type 2 diabetes")) AND ("association") AND (("systematic review") OR ("meta-analysis") OR ("systematic review and meta-analysis")) | 66 |
| Cochrane database | #1 MeSH descriptor: [Periodontal Diseases] explode all trees #2 MeSH descriptor: [Periodontitis] in all MeSH products #3 MeSH descriptor: [Gingivitis] explode all trees #4 ("Periodontal disease"):ti,ab,kw OR ("gingivitis"):ti,ab,kw OR ("periodontitis"):ti,ab,kw #5 #1 OR #2 OR #3 OR #4 #6 MeSH descriptor: [Diabetes Mellitus] explode all trees #7 MeSH descriptor: [Diabetes Mellitus, Type 2] explode all trees #8 MeSH descriptor: [Diabetes Mellitus, Type 1] explode all trees #9 MeSH descriptor: [Diabetes, Gestational] explode all trees #10 ("Diabetes mellitus"):ti,ab,kw OR ("DM1"):ti,ab,kw OR ("DM2"):ti,ab,kw OR ("gestacional diabetes"):ti,ab,kw OR ("type 1 diabetes mellitus"):ti,ab,kw #11 ("type 2 diabetes mellitus"):ti,ab,kw #12 #6 OR #7 OR #8 OR #9 OR #10 OR #11 #13 MeSH descriptor: [Association] explode all trees #14 ("association"):ti,ab,kw #15 #13 OR #14 #16 #5 AND #12 AND #15 |
1 |
| Scielo | (("Periodontal disease") OR ("gingivitis") OR ("periodontitis")) AND (("Diabetes mellitus") OR ("DM1") OR ("DM2") OR ("gestacional diabetes") OR ("type 1 diabetes") OR ("type 2 diabetes")) AND ("association") AND (("systematic review") OR ("meta-analysis") OR ("systematic review and meta-analysis")) | 3 |
| Scopus | (TITLE-ABS-KEY ((("Periodontal disease") OR ("gingivitis") OR ("periodontitis"))) AND TITLE-ABS-KEY ((("Diabetes mellitus") OR ("DM1") OR ("DM2") OR ("gestacional diabetes") OR ("type 1 diabetes") OR ("type 2 diabetes"))) AND TITLE-ABS-KEY (("association")) AND TITLE-ABS-KEY ((("systematic review") OR ("meta-analysis") OR ("systematic review and meta-analysis")))) AND ( LIMIT-TO (SRCTYPE , "j")) AND ( LIMIT-TO (DOCTYPE , "re")) | 92 |
| Google Scholar | "Periodontal disease" + "Diabetes mellitus" OR "gestacional diabetes" + "association" + "systematic review" -"in vitro" -"literature" | 410 |
| OpenGrey | ("Periodontal disease") AND (("Diabetes mellitus") OR ("gestacional diabetes")) AND ("association") AND ("systematic review") | 0 |
Table 2.
Reasons for exclusion of studies.
| Author | Reason for exclusion |
|---|---|
| Herrera et al. [17] | Literature review |
| Li et al. [18] | |
| George et al. [19] | |
| Bansal et al. [20] | |
| Laddha et al. [21] | |
| Salvi et al. [22] | Systematic review of the literature |
| Mealey et al. [23] |
Table 3.
Characteristics of included studies.
| Authors | Year | Study design | Included study design | Number of studies in the qualitative analysis | Number of studies in the quantitative analysis | Type of diabetes | Outcomes | Conclusions | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Costa et al. [10] | 2023 | SR | CCs, Cs, CSs and RCTs | 15 | 0 | T1DM | Most studies confirm the association between T1DM and PDs. | The prevalence and severity of PD was higher in patients with T1DM compared to healthy subjects. | ||
| León-Ríos et al. [24] | 2022 | SR | CCs, Cs and CSs | 8 | 0 | GDM | In most studies an association between PD and GDM was verified. | PD increases the risk of developing GDM. | ||
| Zainal et al. [25] | 2021 | SR with MA | CCs and CSs | 11 | 11 | DM | PI | SMD = 0.54 (0.20 - 0.87) | The duration of DM in children and adolescents affects periodontal status even with a difference of 1 year. Thus, children and adolescents with DM and early PD will progress to periodontitis without intervention. | |
| GI | SMD = 0.63 (0.39 - 0.87) | |||||||||
| BP | SMD = 0.32 (0.07 - 0.58) | |||||||||
| PDT | SMD = 0.67 (0.23 - 1.11) | |||||||||
| CAL | SMD = 0.79 (0.52 - 1.05) | |||||||||
| Zheng et al. [26] | 2021 | SR with MA | CCs, Cs and CSs | 40 | 27 | DM | P | OR = 1.85 (1.61 - 2.11) | The prevalence and severity of periodontitis are higher in patients with diabetes than in non-diabetic populations. | |
| PDT | MD = 0.23 (0.17 - 0.29) | |||||||||
| PI | MD = 0.20 (0.18 - 0.23) | |||||||||
| CAL | MD = 0.39 (0.28 - 0.50) | |||||||||
| NT | MD = -2.14 (-2.87 - -1.40) | |||||||||
| BP | MD = 7.90 (4.24 - 11.56) | |||||||||
| Stöhr et al. [3] | 2021 | SR with MA | Cs | 15 | 15 | DM | GA | RR = 1.26 (1.12 - 1.41) | The findings show a positive bidirectional association between PD and DM. | |
| Dicembrini et al. [28] | 2020 | SR with MA | CCs, Cs and CSs | 19 | 19 | T1DM | P | OR = 0.19 (0.08 - 0.37) | The present data confirm that T1DM is a relevant risk factor for the development of PD. | |
| GA | OR = 2.52 (1.33 - 4.76) | |||||||||
| CAL | SMD = 0.47 (0.37 - 0.57) | |||||||||
| Nguyen et al. [31] | 2020 | SR | Ls, CCs and CSs | 14 | 0 | DM | Higher risks of diabetic complications have been reported in people with diabetes and periodontitis compared to those with diabetes who do not have periodontitis. | This review systematically addressed current epidemiological data that provide evidence that periodontitis is associated with an increased risk of developing diabetic complications compared to patients without periodontitis. | ||
| Rapone et al. [29] | 2020 | SR with MA | CCs and CSs | 10 | 10 | T1DM | BP | SMD = 0.65 (0.08 - 1.23) | Although evidence suggests that there may be an association between PD and T1DM in children and adolescents, study designs and methodological limitations make interpretation of the current research difficult. | |
| CAL | SMD = 0.82 (0.59 - 1.04) | |||||||||
| GI | SMD = 0.46 (0.08 - 0.84) | |||||||||
| PI | SMD = 0.71 (0.19 - 1.22) | |||||||||
| PDT | SMD = 0.36 (0.16 - 0.55) | |||||||||
| Tanaka et al. [32] | 2019 | SR | SRs, Cs, CCs and CSs | 33 | 0 | DM | Although several cohort studies and MAs evaluated cancer development in diabetes, there was little epidemiological evidence for the other conditions. | In Japan, there is little evidence on the effect of diabetes on the incidence and prevalence of PD. | ||
| Nascimento et al. [33] | 2018 | SR with MA | Ls | 13 | 6 | DM | GA | RR = 1.86 (1.25 - 2.77) | This study provides evidence that diabetes is associated with an increased risk of onset and progression of periodontitis in adults. | |
| Ziukaite et al. [34] | 2018 | SR with MA | CCs, Cs and CSs | 29 | 21 | DM | GA | OR = 2.59 (2.12 - 3.15) | The overall prevalence and odds of having diabetes are higher in populations with periodontitis compared to people without periodontitis. | |
| Graziani et al. [30] | 2018 | SR | CCs, Cs and CSs | 20 | 0 | DM | Healthy individuals with periodontitis have poor glycemic control and an increased risk of developing diabetes. People affected by diabetes show impaired glycemic control if they also suffer from periodontitis and a significantly higher prevalence of diabetes-related complications. There is limited evidence available on GDM and T1DM. | Periodontitis has a significant impact on the control, incidence, and complications of diabetes. | ||
| Mauri-Obradors et al. [35] | 2017 | SR | Ls and CSs | 19 | 0 | DM | PD was more prevalent among diabetic patients. | There are multiple oral manifestations associated with DM, one of them is PD. | ||
| Lima et al. [36] | 2016 | SR with MA | CCs and CSs | 8 | 7 | GDM | GA | CSs | OR = 1.67 (1.20 - 2.32) | Scientific evidence cannot affirm a positive association between periodontitis and GDM. |
| CCs | OR = 1.69 (0.68 - 4.21) | |||||||||
| Abariga et al. [38] | 2016 | SR with MA | CCs, Cs and CSs | 10 | 10 | GDM | GA | OR = 2.08 (1.21 - 3.58) | The MAs suggests that periodontitis is associated with a statistically significant increased risk of GDM compared to women without periodontitis. | |
| Ismail et al. [27] | 2015 | SR | CCs and Ls | 28 | 0 | T1DM | Most studies reported significantly greater plaque accumulation and higher GI in children with T1DM. Cohort studies reported no significant differences in periodontal parameters over time. | There is evidence that children with T1DM show poorer periodontal health with greater plaque accumulation compared to healthy children. | ||
| Borgnakke et al. [39] | 2013 | SR | CCs, Cs, CSs, Ls and Rs | 16 | 0 | DM | A small amount of evidence supports the significant adverse effects of PD on glycemic control, diabetes complications, and the development of T2DM and possibly GDM. | Current evidence suggests that PD negatively affects diabetes outcomes. | ||
| Chávarry et al. [37] | 2009 | SR with MA | Ls and CSs | 57 | 16 | DM | CAL | T1DM | MD = 0.26 (-0.00 - 0.53) | T2DM can be considered a risk factor for periodontitis. More studies are needed to confirm the harmful effects of T1DM on PD. |
| T2DM | MD = 1.00 (0.15 - 1.84) | |||||||||
| PDT | T1DM | MD = 0.11 (-0.03 - 0.25) | ||||||||
| T2DM | MD = 0.46 (0.01 - 0.91) | |||||||||
SR = Systematic review; MA = Meta-analysis; CC = Case and control; C = Cohort; CS = Cross-sectional; RCT = Randomized clinical trial; L = Longitudinal study; R = Retrospective study; T1DM = Type 1 diabetes mellitus; T2DM = Type 2 diabetes mellitus; GMD = Gestational diabetes mellitus; PD = Periodontal disease; DM = Diabetes mellitus; PI = Plaque index; GI = Gingival index; BP = Bleeding on probing; PDT = Probing depth; CAL = Clinical attachment level; P = Prevalence; NT = Number of teeth; GA = General association; RR = Risk ratio; MD = Mean difference; OR = Odds ratio; SMD = Standardized mean difference.
Table 4.
Assessment of the methodological quality and the quality of the evidence of the included studies.
Table 4.
Assessment of the methodological quality and the quality of the evidence of the included studies.
| Authors | Year | AMSTAR – 2 | Overall confidence | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2* | 3 | 4* | 5 | 6 | 7* | 8 | 9* | 10 | 11* | 12 | 13* | 14 | 15* | 16 | |||
| Costa et al. [10] | 2023 | Yes | Yes | Yes | Yes partial | Yes | No | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| León-Ríos et al. [24] | 2022 | Yes | Yes partial | Yes | Yes partial | Yes | No | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Zainal et al. [25] | 2021 | Yes | Yes | Yes | Yes partial | No | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Zheng et al. [26] | 2021 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Stöhr et al. [3] | 2021 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Dicembrini et al. [28] | 2020 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Nguyen et al. [31] | 2020 | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | Critically low | |
| Rapone et al. [29] | 2020 | Yes | Yes partial | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Tanaka et al. [32] | 2019 | Yes | Yes | Yes | Yes partial | Yes | Yes | No | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | No | Low | |
| Nascimento et al. [33] | 2018 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Ziukaite et al. [33] | 2018 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Graziani et al. [30] | 2018 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Mauri-Obradors et al. [36] | 2017 | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Lima et al. [37] | 2016 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | High |
| Abariga et al. [38] | 2016 | Yes | Yes partial | Yes | Yes partial | No | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Ismail et al. [27] | 2015 | Yes | No | Yes | Yes partial | Yes | Yes | Yes partial | Yes | No | Yes | No meta-analysis | No | Yes | No meta-analysis | Yes | Critically low | |
| Borgnakke et al. [39] | 2013 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Chávarry et al. [37] | 2009 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | High |
AMSTAR = A MeaSurement Tool to Assess Systemic Reviews. 1 = Did the research questions and inclusion criteria for the review include the components of PICO? 2 = Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? 3 = Did the review authors explain their selection of the study designs for inclusion in the review? 4 = Did the review authors use a comprehensive literature search strategy? 5 = Did the review authors perform study selection in duplicate? 6 = Did the review authors perform data extraction in duplicate? 7 = Did the review authors provide a list of excluded studies and justify the exclusions? 8 = Did the review authors describe the included studies in adequate detail? 9 = Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? 10 = Did the review authors report on the sources of funding for the studies included in the review? 11 = If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? 12 = If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? 13 = Did the review authors account for RoB in primary studies when interpreting/discussing the results of the review? 14 = Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? 15 = If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? 16 = Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? * = Critical domain.
Table 5.
Overlapping of primary studies in systematic reviews.
| Primary studies | Systematic reviews that included the primary studies | Times that primary studies were included |
|---|---|---|
| Bullon et al. [40] | Zheng et al. [26], Graziani et al. [30], Lima et al. [36], Abariga et al. [38] | 4 |
| Al-Khabbaz et al. [41] | Zainal et al. [25], Dicembrini et al. [28], Rapone et al. [29], Ismail et al. [27] | 4 |
| Esteves Lima et al. [42] | León-Ríos et al. [24], Graziani et al. [30], Lima et al. [36], Abariga et al. [38] | 4 |
| Chokwiriyachit et al. [43] | Zheng et al. [26], Graziani et al. [30], Lima et al. [36], Abariga et al. [38] | 4 |
| Morita et al. [44] | Stöhr et al. [3], Tanaka et al. [32], Nascimento et al. [33], Borgnakke et al. [39] | 4 |
| Xiong et al. [45] | Zheng et al. [26], Lima et al. [36], Abariga et al. [38], Borgnakke et al. [39] | 4 |
| Dakovic et al. [46] | Zainal et al. [25], Dicembrini et al. [28], Rapone et al. [29], Ismail et al. [27] | 4 |
| Dasanayake et al. [47] | Zheng et al. [26], Lima et al. [36], Abariga et al. [38], Borgnakke et al. [39] | 4 |
| Saito et al. [48] | Zheng et al. [26], Tanaka et al. [32], Borgnakke et al. [39], Chávarry et al. [37] | 4 |
| Sun et al. [49] | Costa et al. [10], Stöhr et al. [3], Dicembrini et al. [28] | 3 |
| Ismail et al. [50] | Costa et al. [10], Zainal et al. [25], Rapone et al. [29] | 3 |
| Chiu et al. [51] | Stöhr et al. [3], Nascimento et al. [33], Graziani et al. [30] | 3 |
| Habib [52] | Zheng et al. [26], Lima et al. [36], Abariga et al. [38] | 3 |
| Orbak et al. [53] | Zainal et al. [25], Rapone et al. [29], Ismail et al. [27] | 3 |
| Lalla et al. [54] | Zainal et al. [25], Rapone et al. [29], Ismail et al. [27] | 3 |
| Aren et al. [55] | Zainal et al. [25], Ismail et al. [27], Chávarry et al. [36] | 3 |
| Sbordone et al. [56] | Nascimento et al. [33], Ismail et al. [27], Chávarry et al. [37] | 3 |
| Firatli [57] | Nascimento et al. [33], Ismail et al. [27], Chávarry et al. [37] | 3 |
| Pinson et al. [58] | Dicembrini et al. [28], Ismail et al. [27], Chávarry et al. [37] | 3 |
| Roy et al. [59] | Costa et al. [10], Dicembrini et al. [28] | 2 |
| Babu et al. [60] | Zainal et al. [25], Rapone et al. [29] | 2 |
| Myllymäki et al. [61] | Zheng et al. [26], Stöhr et al. [3] | 2 |
| Chaparro et al. [62] | León-Ríos et al. [24], Zheng et al. [26] | 2 |
| Winning et al. [63] | Zheng et al. [26], Stöhr et al. [3] | 2 |
| Jindal et al. [64] | Costa et al. [10], Dicembrini et al. [28] | 2 |
| Popławska-Kita et al. [65] | Costa et al. (10), Dicembrini et al. (28) | 2 |
| Amiri et al. [66] | Nguyen et al. [31], Graziani et al. [30] | 2 |
| Lee et al. [67] | Nascimento et al. [33], Ziukaite et al. [34] | 2 |
| Jimenez et al. [68] | Stöhr et al. [3], Nascimento et al. [33] | 2 |
| Southerland et al. [69] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Hodge et al. [70] | Zheng et al. [26], Dicembrini et al. [28] | 2 |
| Ruiz et al. [71] | Lima et al. [36], Abariga et al. [38] | 2 |
| Ide et al. [72] | Stöhr et al. [3], Borgnakke et al. [39] | 2 |
| Tagelsir et al. [73] | Zainal et al. [25], Ismail et al. [27] | 2 |
| Abrao et al. [74] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Demmer et al. [75] | Stöhr et al. [3], Borgnakke et al. [39] | 2 |
| Shultis et al. [76] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Novak et al. [77] | Lima et al. [36], Abariga et al. [38] | 2 |
| Borges-Yáñez [78] | Ziukaite et al. [34], Chávarry et al. [37] | 2 |
| Mansour et al. [79] | Zheng et al. [26], Chávarry et al. [37] | 2 |
| Campus et al. [80] | Zheng et al. [26], Chávarry et al. [37] | 2 |
| Saremi et al. [81] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Siudikiene et al. [82] | Zainal et al. [25], Ismail et al. [27] | 2 |
| Noma et al. [83] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Marugame et al. [84] | Tanaka et al. [32], Chávarry et al. [37] | 2 |
| Zielinski et al. [85] | Zheng et al. [26], Chávarry et al. [37] | 2 |
| Kawamura et al. [86] | Zheng et al. [26], Chávarry et al. [37] | 2 |
| Collin et al. [87] | Zheng et al. [26], Chávarry et al. [37] | 2 |
| Firatli et al. [88] | Ismail et al. [27], Chávarry et al. [37] | 2 |
| Thorstensson et al. [89] | Nguyen et al. [31], Borgnakke et al. [39] | 2 |
| Sbordone et al. [90] | Ismail et al. [27], Chávarry et al. [37] | 2 |
| de Pommereau et al. [91] | Ismail et al. [27], Chávarry et al. [37] | 2 |
| Sandholm et al. [92] | Ismail et al. [27], Chávarry et al. [37] | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



