Submitted:
13 October 2024
Posted:
18 October 2024
You are already at the latest version
Abstract
Background: Delhi State AIDS Control Society (DSACS) addressed critical integration of services for Orphan and Vulnerable Children (OVC) in context of HIV. They bridged the policy and implementation divide by formulating a multisectoral-strategy in April 2012, creating a model of "Continuum-of-Care for People-Living with HIV (PLHIV), OVC & Children-Affected-by-HIV (ChABH)” in Delhi. With input from the National Commission for Protection of Child Rights, DSACS sensitized political and administrative machinery about needs and challenges related to HIV/AIDS. DSACS developed an incentive-based system for Antiretroviral Therapy (ART) adherence, incorporating safeguards and robust monitoring. Delhi Government's sustained financial commitment and DSACS programmatic-innovation provide a scalable blueprint for India and global initiatives.
Description: This ongoing Delhi Government's scheme focuses on household-economic-strengthening of PLHIV as an incentive for broader behaviour change based-on specific eligibility conditions. Beneficiaries fall into four categories: PLHIV, including children on ART; double orphan HIV positive children (OCI); destitute children living with HIV/in institutional care (DCI); and double orphan ChABH in community-based care in Delhi. Category-wise fixed-monthly financial assistance is released to beneficiaries via direct-bank-transfers leveraging Aadhaar-platform to eliminate corruption. Adherence to treatment is mandatory to continue cash-transfers. Linkages with other schemes established to maximize impact.
Lessons learned: In its 11-year evolution, Delhi model has grown from 1110 to 6467 beneficiaries, including 6383 PLHIV, 34 double OCI, 50 DCI, and 27 double orphan ChABH, with 5875 (90.8%) currently active excluding beneficiaries who expired (n=328), migrated/ transferred out of Delhi (n=115), opted-out ART/or lost-to-follow-up (n=135), and 14 CABA who turned major. Steady progress and 98% ART adherence mark positive outcomes. DSACS eased eligibility criteria in 2018, facilitating hurdle-free enrollment, while responding to cost-inflation by enhancing financial assistance, showcasing program adaptability. Achieving >95 ART adherence has significantly boosted survival rates, underscoring program's positive impact on beneficiary health. The scheme's INR 14,69,35,600 expenditure in 2022-23, just 0.13% of Delhi Health Department's plan-outlay, signals a cost-effective investment. Extrapolating this nationally would represent 1.5% of India's Health Ministry's current plan-outlay.
Conclusions/Next steps: This innovative model is implementable on large-scale in India and around the globe but requires not only financial commitment but also coordinated efforts, policy adjustments, and collaboration between various stakeholders.
Keywords:
Orphan vulnerable children
; Children Affected by HIV
; People Living with HIV
; Antiretroviral Therapy
; Cash Transfer Scheme
; Continuum of Care
; Household economic strengthening
INTRODUCTION
In India, approximately 2.4 million people live with HIV (PLHIV), with a national adult prevalence of 0.21% [1]. Despite the proven effectiveness of Antiretroviral Therapy (ART) in suppressing the HIV virus [2], accessibility remains a challenge. Delhi, with a higher prevalence of 0.31%, has registered 81,642 adults and 3,180 children in HIV care since 2004. Among them, 60,821 adults and 2,310 children have initiated ART, with 36,629 adults and 1,529 children currently receiving ongoing ART. Unfortunately, Delhi's HIV mortality rate is 4.61 per 100,000 population, exceeding national rate of 3.08 [1].
To address the socio-economic impact of HIV-related deaths, Delhi State AIDS Control Society (DSACS) launched a state government-sponsored cash transfer scheme (CTS) on April 1, 2012 [3]. This program targets orphan vulnerable children (OVC) and children affected by HIV (ChABH), aiming to economically strengthen households of PLHIV and ChABH. The CTS, sanctioned by the Delhi Government and implemented since April 1, 2012, adheres to a well-defined set of standard operating procedures. These procedures encompass eligibility criteria, the process of identifying cases, disbursement methods to beneficiaries, and measures to prevent corruption [3]. Objectives include funding travel costs for health services, providing nutritional support, and enhancing ART adherence.
Cash transfer programs are increasingly recognized as effective strategies for influencing behavioral change and improving outcomes in HIV care [4]. However, most initiatives globally have primarily operated within research settings and transient [5-7].
Cash transfer programs have a positive effect on mitigating HIV incidence and increasing retention in HIV care. These results show the potential of cash transfer programs for HIV prevention and care, especially among people in extreme poverty, and highlight that cash transfer programs must be considered when creating policies for HIV/AIDS control, as indicated by the UNAIDS 95-95-95 Target of the HIV Care Continuum [8]. The unique feature highlighted here is the sustained nature of the CTS implemented by DSACS. This program, funded by the Delhi government for the past 11 years, stands out for its long-term commitment. The scheme's features were presented at a South Asia ChABH meeting in 2013 [9]. The success of this innovative model underscores its potential for widespread implementation throughout India and world-wide. This communication not only highlights the scheme's achievements but also addresses implementation challenges and outlines ongoing efforts to strengthen and enhance this vital initiative.
METHODS
The study adopts a descriptive approach to analyze the implementation and impact of the CTS sanctioned by the Delhi Government. It involves a comprehensive examination of the scheme's eligibility criteria, enrollment process, disbursement methods, and amendments in the scheme over time. Additionally, the study utilizes ART program data, feedback from beneficiaries and various NGOs to assess the scheme's coverage, effectiveness, and challenges.
Methods Processes
- Eligibility criteria:
The eligibility conditions of the scheme are structured into four distinct categories, each specifying unique criteria and financial aid amounts:
- Category I: PLHIV, including children on ART in Delhi, initially received INR 1,000 monthly, increased to INR 2,496 as of August 7, 2023. Eligibility criteria include regular ART for last 01 year, three years of residency in Delhi, and a family income of less than INR 100,000 annually.
- Category II: Double orphans children living with HIV (double OCI) in community-based care in Delhi, received INR 2,050 per month initially, increased to INR 5,116 as of August 7, 2023.
- Category III: Destitute children living with HIV (DCI) in institutional care in Delhi on ART, received INR 2,050 per month initially, increased to INR 5,116 as of August 7, 2023.
- Category IV: HIV-negative double orphan children affected by HIV (DO-ChABH) in community-based care in Delhi, received INR 1,750 per month initially, increased to INR 4,368 as of August 7, 2023.
For double orphans (Category II, IV) at least one parent should have succumbed to HIV. Upon turning 18, double OCI/DCI beneficiaries are shifted to Category I, while assistance to ChABH ceased at the age of 18.
There is no limit on the number of beneficiaries in a family. Financial assistance was supplementary to any other government aid like old age pension, widow pension, etc.
- 2.
- Implementation Process:
Implementation of the CTS is a multi-step process involving coordination between government ART clinics, DSACS, and beneficiaries. The process is structured as follows: -
- (i)
- Identification of eligible beneficiaries: Eleven government ART clinics in Delhi are responsible for identifying individuals who meet the eligibility criteria for the CTS.
- (ii)
- Document collection: The ART clinics gather necessary documents based on the category of the persons seeking assistance:
For Category I (PLHIV, including children):
Proof of residence in Delhi for the last three years.
Medical records confirming HIV status and at least one year of ART.
Income certificates from the Revenue Department.
For Categories II (double OCI) and IV (DO- ChABH):
Evidence of both parents' deaths, with at least one attributed to HIV.
For Category III (DCI):
They should already be on ART or have started it before applying for assistance through the program with the aim of holding concerned institution responsible for ensuring ART registration and initiation.
Forwarding of Applications to DSACS, the Implementing Authority: The collected documents are then forwarded to the DSACS for further processing. DSACS serves as the central authority responsible for managing and overseeing the implementation of the CTS.
Evaluation by State Screening Committee (SSC): DSACS has established a SSC to evaluate applicants' eligibility based on predefined criteria and provide enrollment recommendations.
Enrollment of Beneficiaries: Beneficiaries are enrolled in the CTS based on the recommendations of the SSC, following approval of the Chairman of the Executive Committee of DSACS.
Disbursement of Financial Assistance: DSACS executes electronic transfers of financial assistance directly into bank accounts of beneficiaries on a monthly basis through a nationalized bank. Since June 2016, DSACS is using Public Financial Management System, an Aadhar Number (National Unique ID) based Direct Bank Transfer tool developed by the Ministry of Finance, Government of India, to improve transparency, accountability, and program management.
Maintain Post-Enrollment Eligibility: ART clinics and institutions must submit beneficiaries' life certificates to DSACS every three months to ensure uninterrupted cash transfers. These certificates confirm the beneficiaries' survival status and adherence to ART, as certified by the ART centers. Information that Category IV beneficiaries are alive is gathered directly from respective NGOs or CBOs or families, with surprise checks by DSACS staff.
Data Collection:
To perform a comprehensive analysis, the year-on-year (y-o-y) performance of the cash transfer initiative was evaluated by assessing the number of beneficiaries enrolled in the scheme across various categories for the study period spanning from April 1, 2012, to October 31, 2023. The data from the state ART program for the study period was also examined. This data is accessible to DSACS through the Computerized Management Information System, a web-based application developed by the National AIDS Control Organization (NACO). The y-o-y coverage of the CTS was analyzed in relation to the number of PLHIV who are alive and receiving ART, excluding individuals who opted out treatment, migrated, or lost to follow-up (LTFU) or deceased.
Additionally, the assessment involved an analysis of ART adherence rates for October 2023, derived from a random sample of individuals living with HIV undergoing Antiretroviral Therapy (ART), which was compared with the ART adherence rate among beneficiaries of the scheme. The ART adherence was rated as good, average, and poor based on adherence rates >95%, 80-95%, and <80%, respectively.
Furthermore, information regarding the status of destitute HIV-positive children benefiting from the scheme while under institutional care at Naz Foundation, Siam New Generation Trust, and Deepti Foundation, as well as children affected by HIV in community-based care, was directly acquired through networking with the respective NGOs and community-based organizations.
In August 2018, DSACS conducted a comprehensive analysis and review of the challenges encountered by beneficiaries during enrollment and continuation. This assessment was based on feedback gathered from ART clinics, the Grievance Committee of DSACS, as well as direct interactions with beneficiaries and relevant NGOs. Subsequently, several modifications were implemented in the scheme in December 2019 to enhance its uptake and execution. The impact of these adjustments on the subsequent uptake of the CTS was evaluated.
RESULTS
Cumulative Performance of the Scheme
From April 1, 2012, to October 31, 2023, a total of 6,467 beneficiaries were prospectively enrolled for cash transfers. This included 6,356 individuals classified as PLHIV (Category 1), comprising 6,020 adults and 336 children. Additionally, 34 HIV positive double orphans (Category 2) residing under the care of grandparents, elder siblings, or extended family; 50 destitute HIV positive children in institutional care (Category 3); and 27 DO-ChABH (Category 4) in community-based care in Delhi were also part of this beneficiary pool.
Total 5875 (90.8%) beneficiaries are currently active, excluding beneficiaries that expired (n=328), including 308 adults & 11 children living with HIV, 8 DCI, and 1 double OCI); migrated or transferred out of Delhi (n=115); opted out ART/or lost to follow-up (n=135). Also, 14 DO-ChABH on reaching the age of major were transitioned out of scheme. Further, cash transfers ceased for 21 PLHIV who subsequently became ineligible based on income criteria. For 29 double OCI and DCI who turned 18 years of age, the cash transfers were transitioned to Category I for life-long financial assistance.
ART Adherence Rates in Beneficiaries
Excluding ChABH (Category 4, HIV negative), a total of 5731 (98%) of the 5848 currently active beneficiaries, including PLHIV, double OCI and DCI, were confirmed adherent to ART, demonstrating good ART adherence (≥ 95%). This contrasts with 21,266 (91.0%) of a random sample of 23,356 PLHIV on ART who exhibited good adherence, as reported by 11 ART clinics in the survey conducted in October 2023 (p < 0.001).
Year-on-Year Performance of the Scheme
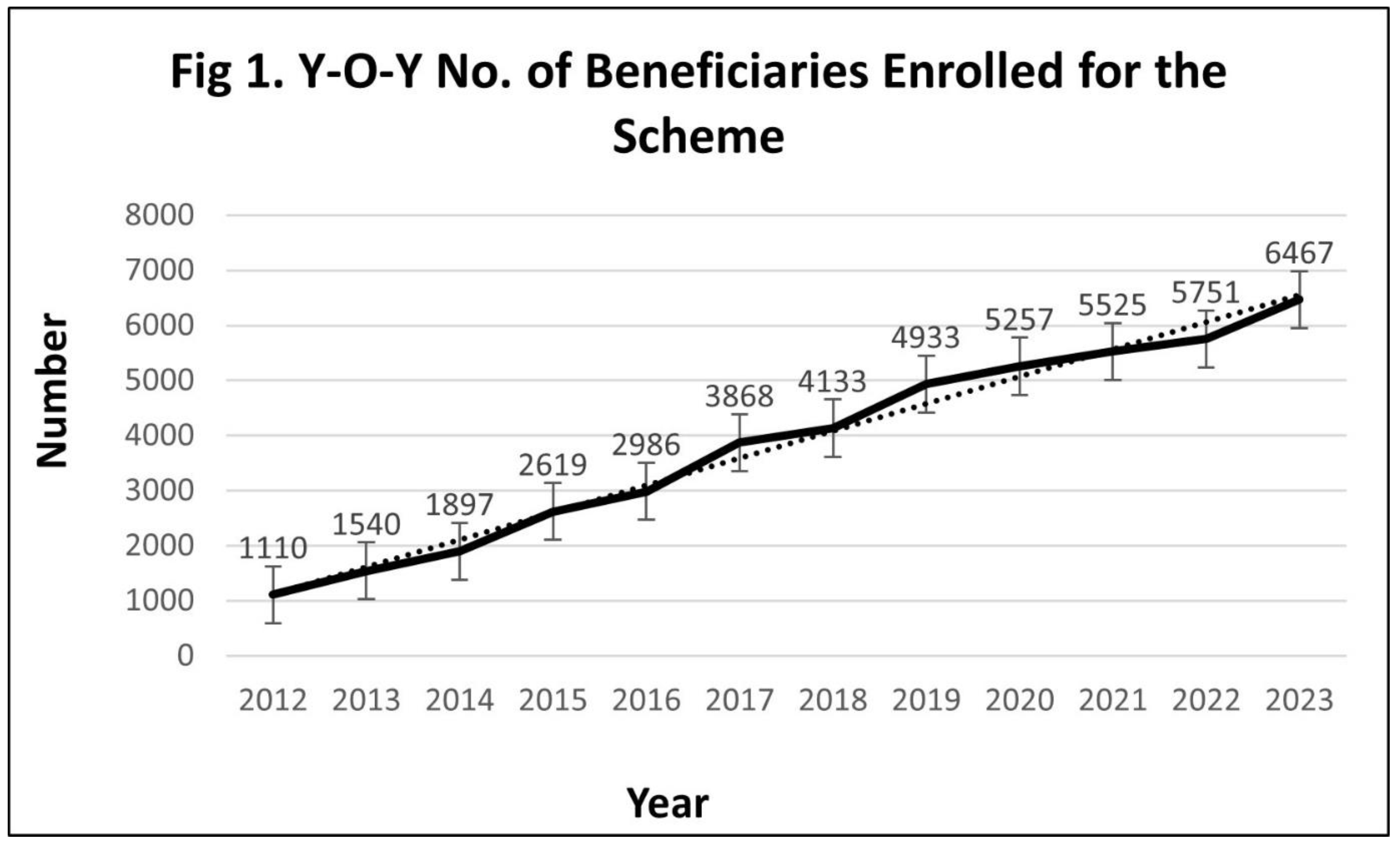
As depicted in Fig. 1, there has been a consistent increase in the number of beneficiaries over the 11-year implementation period, starting from the baseline of 1,110 beneficiaries (1,083 PLHIV and 27 HIV orphans) enrolled in the first year of the scheme. However, upon closer examination of the y-o-y enrollment patterns, after initial enrollment of sizable number there was a slow increase in the number of beneficiaries. This trend persisted even after the revision in ART guidelines in May 2017, which advocated for treating all PLHIV irrespective of clinical stage or CD4 count [10]. This suggests that despite the expanded eligibility criteria, the anticipated surge in PLHIV (Category 1) did not materialize. This motivated DSACS to analyze various challenges in the implementation of the scheme.
Figure 1.
Implementation Challenges
Since the rollout of the scheme in 2012, DSACS has received feedback from Mainstreaming Program Officer regarding the challenges faced by both potential and enrolled beneficiaries, largely due to the stringent eligibility conditions established during the scheme's conceptualization. In response to these concerns, a grievance committee was formed to address issues that could be resolved through coordination with ART centres, the revenue department, NGOs, and PLHIV networks. In 2018, the grievance committee identified several key challenges that required attention:.
- (i)
- Lack of Information, Education & Communication: Insufficient dissemination of CTS at ART clinics likely contributed to low enrollment rates.
- (ii)
- Lack of family centric approach at ART clinics: While ART clinics primarily focus on providing medical treatment to PLHIV, a broader approach is necessary to address the social and family aspects, especially concerning orphaned children. Developing a clear protocol for identifying and documenting children orphaned due to the death of a registered PLHIV is essential.
- (iii)
- Difficulty in Obtaining Income Proof: Some beneficiaries reported delays in acquiring income proof from the Revenue Department, which is an essential document required to enroll for the scheme.
- (iv)
- Interruption in Cash Transfers: Beneficiaries experience interruptions in cash transfers in case they fail to submit the income proof every six months. Also, payments cease for beneficiaries whose subsequent income surpasses INR 1,00,000.
- (v)
- Failure to Provide ‘Adherence to ART’ Certificate Every Quarter: Beneficiaries face discontinuation of cash transfers if they fail to provide quarterly regular treatment certificates from ART clinics. This measure aims to ensure beneficiaries maintain 100% compliance with treatment.
- (vi)
- Complex documentation requirement: The requirement for intricate documentation, including proof of the death of both parents and confirmation that at least one parent died of HIV, serves as a barrier to enrollment for HIV orphans.
- (vii)
- Rise in Cost of Living: Despite the financial assistance provided, numerous beneficiaries have expressed concerns about the inadequacy of the disbursement amount, particularly in light of the escalating cost of living due to inflation.
- (viii)
-
Delay in Payment Release:The current differentiated ART delivery involving quarterly visits for stable patients and monthly visits for new or unstable patients, coupled with subsequent procedural steps for payment release, has led to delays in disbursing financial support to beneficiaries.
Strengthening Initiatives:
Recognizing the various obstacles encountered by beneficiaries during the enrollment process, DSACS took the initiative to propose revisions to the eligibility criteria of the scheme and increase the amount of financial assistance in response to the rising Cost Inflation Index. These proposals were approved by the Delhi Government in December 2019, marking a significant milestone. To further improve the uptake of the scheme, the following initiatives and interventions have been undertaken:
- (i)
- Improved Eligibility Screening: ART center counsellors have been provided comprehensive training to refine their assessment skills in determining the eligibility of all PLHIV and HIV orphans seeking treatment.
- (ii)
- Maintain Post-Enrollment Eligibility:
- ∙
- While initial income proof from the Revenue Department remains a requirement for enrollment, subsequent verification can now be facilitated through the beneficiary's self-declaration.
- ∙
- Certificates for regular treatment for PLHIV will be dependent on quarterly biometric attendance records, ensuring more accurate monitoring and assessment of treatment adherence.
- (iii)
- Special Provisions for Illness Cases: In instances where beneficiaries are incapacitated to visit ART clinics due to illness or bedridden conditions, a designated relative or friend may be authorized to collect antiretroviral medicines for the month. However, it is imperative that the beneficiary personally attends the ART clinic in the ensuing months. The verification of treatment adherence is diligently monitored by the Nodal Officer of the ART clinic.
- (iv)
- Revision in eligibility criteria for HIV orphan: Delhi Government made the decision to include double orphan children living with HIV in the scheme regardless of their parental HIV status, thereby eliminating the previous requirement that at least one parent should have died of HIV. This change was motivated by the recognition that most children acquire HIV through Mother-to-Child Transmission, underscoring the need to provide support and assistance to all double orphan children infected with HIV irrespective of their parental HIV status.
- (v)
- Tracking Affected Family Members: ART clinics were encouraged to develop mechanisms to track affected families in case of the death of PLHIV. This is essential to consider affected children for financial support through the scheme.
- (vi)
- Streamlined Monthly Payment Release: Delhi Government has instituted a policy mandating the automatic release of payments to beneficiaries by the 10th of each month, eliminating the need for certificates confirming attendance at ART clinics. This adjustment is aimed at reducing delays associated with procedural checks, thereby ensuring timely support for beneficiaries.
- (vii)
- Additional Measures: Crucially, the scheme guarantees that no recovery will be sought from the beneficiary or their family for payments disbursed under the scheme in the event that the beneficiary is deemed ineligible during quarterly screenings or due to circumstances such as decease within the quarter or ineligibility for any other reason.
DISCUSSION
The Delhi State AIDS Control Society (DSACS) has been implementing the Delhi Government funded Cash Transfer Scheme (CTS) since 2012, to support People Living with HIV (PLHIV) and Orphans and Vulnerable Children (OVC) affected by HIV. Now in its 12th year, the scheme continues to demonstrate its significance, particularly following amendments made in 2019 based on recommendations from the grievance committee. These changes led to a modest but noticeable increase in the uptake of the scheme, as reflected in enrollment trends.
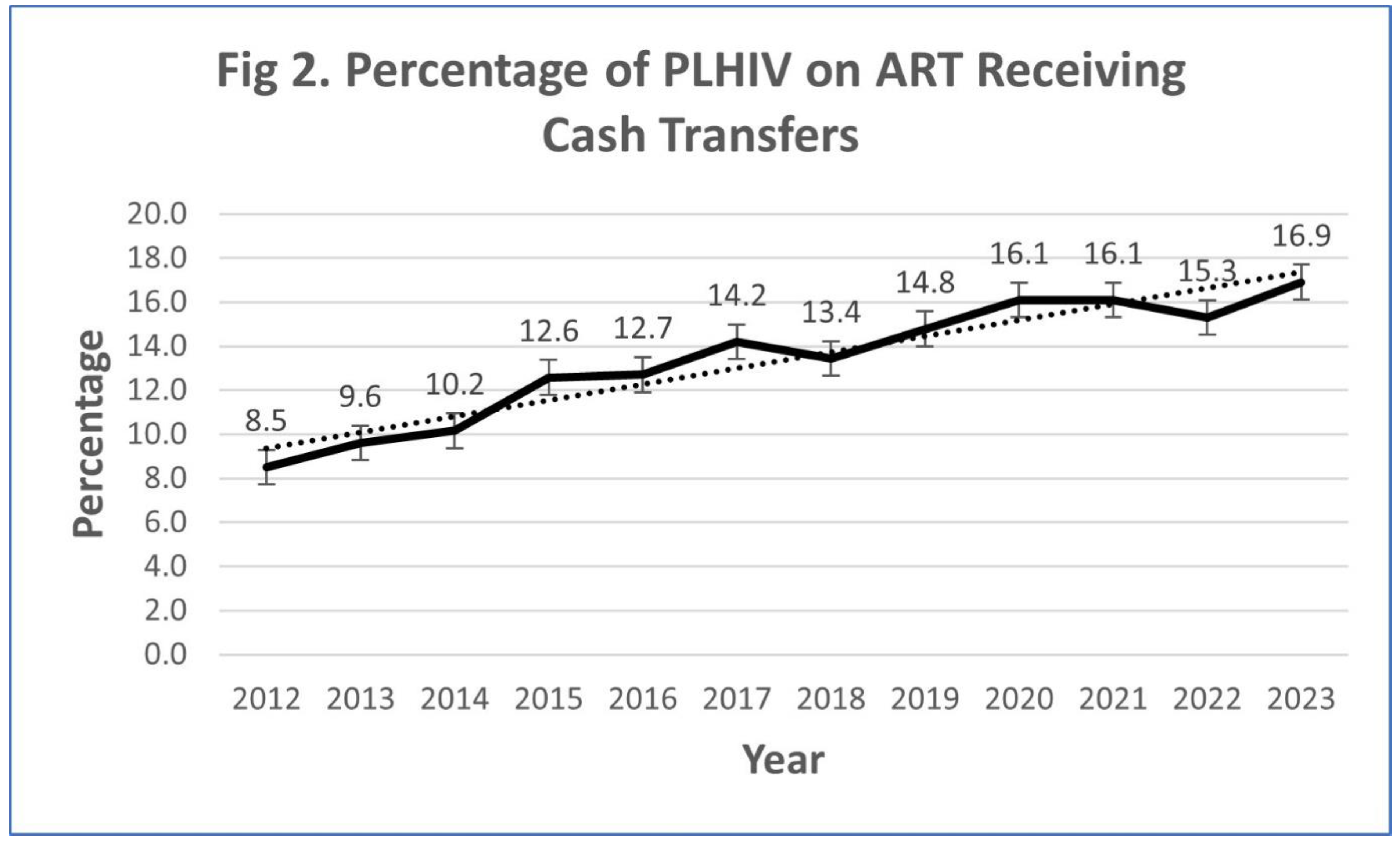
Enrollment data, as shown in Figure 2, reveals a steady rise in participation for Category I (PLHIV), with enrollment increasing from 14.8% in 2019 to 16.9% in 2023..
Figure 2.
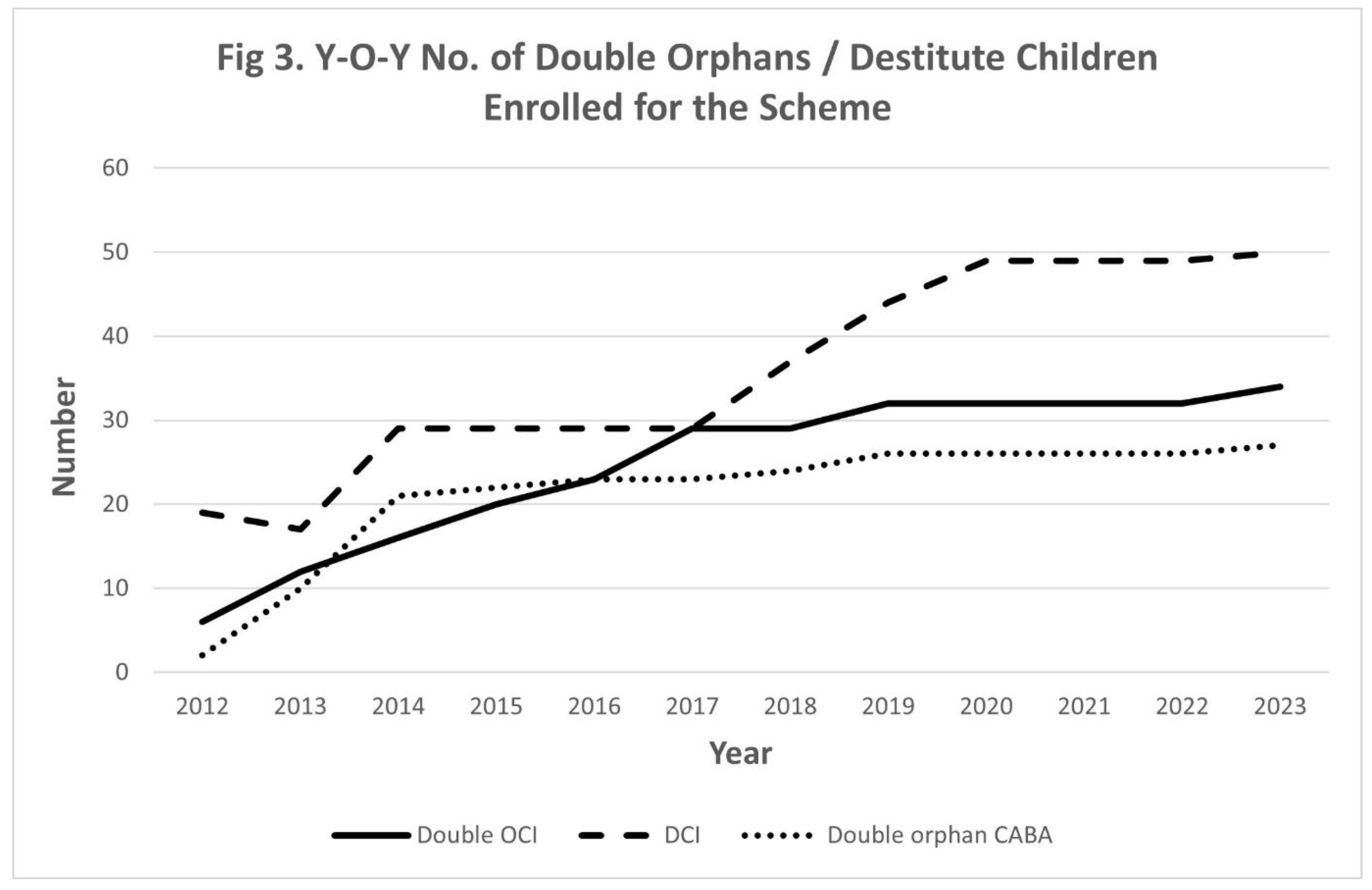
Similarly, Category III (destitute children living with HIV) also experienced a year-on-year increase in enrollment, as shown in Figure 3. These trends affirm the positive impact of the scheme’s revisions. Feedback from stakeholders and beneficiaries further supports these findings, showing improved satisfaction and engagement with the scheme post-amendments.
Figure 3.
Persistent Challenges
Despite these improvements, the current enrollment figures remain low, especially for orphans and other vulnerable children:
- Double Orphan Children Infected (OCI): 34 enrolled, 1 (2.9%) died.
- Double Children Infected (DCI): 50 enrolled, 8 (16%) died.
- Double Orphan Children Affected by HIV (ChABH): 27 enrolled, all alive.
This limited enrollment highlights the ongoing challenges in reaching all eligible children, likely due to several factors:
- Magnitude of the Problem Remains Unknown: Accurately estimating the number of HIV orphans remains a significant challenge due to under-reporting and the absence of comprehensive community-based surveys. Although a mapping study conducted by DSACS between 2010-2012 [3] identified some orphaned children, the lack of a systematic, extensive survey by bodies such as the National Commission for Protection of Child Rights (NCPCR) or the Delhi Commission for Protection of Child Rights (DCPCR) highlights a critical data gap. Updated data on the scope of HIV-related orphanhood in Delhi is essential for more targeted and effective interventions to support this vulnerable population.
- Lack of Focus on Single Orphan Children Affected by HIV: Current CTS provisions do not adequately address the unique needs of single orphan children affected by HIV (SO-ChABH). These children are grouped under Category I, receiving the same financial assistance as children living with HIV under parental care. However, given the specific vulnerabilities of single orphans, the scheme should provide tailored financial support, especially for HIV-infected paternal orphans. Adjusting the policy to better accommodate their needs will help improve their welfare and inclusion in the scheme.
- Enrollment Criteria for HIV-Positive Children on ART: The stipulation that HIV-positive children must be on antiretroviral therapy (ART) for at least one year before qualifying for Category I financial support is problematic. Given the high mortality rate among children without early ART, this requirement may exclude many children who need immediate financial assistance. Revising the eligibility to include all HIV-positive children on ART, regardless of duration, would be a more appropriate and life-saving policy adjustment.
Study Limitations
A significant challenge in the implementation of the CTS is the lack of a robust Monitoring and Evaluation (M&E) system. While attendance records from ART clinics and financial audits provide some level of oversight, they fail to deliver a comprehensive assessment of the scheme's overall impact. The implementation of a third-party evaluation, as recommended in global best practices, could facilitate an impartial analysis of the CTS's effectiveness. Such an evaluation would not only support the refinement of the scheme but also provide critical insights into its long-term benefits for beneficiaries.
Furthermore, the absence of detailed data on beneficiaries facing challenges with the CTS constrains a full understanding of the scheme's scope and efficacy. Systematically gathering this information is essential for identifying service delivery bottlenecks and implementing targeted improvements. By addressing these limitations, we can enhance the program’s effectiveness and ensure it more effectively meets the needs of its target population. Ultimately, strengthening the M&E framework will pave the way for more informed decision-making and policy adjustments, fostering greater positive outcomes for beneficiaries.
Financial Implications
The financial cost of the program for the fiscal year 2022-23 amounted to INR 14,69,35,600, representing only 0.13% of the Delhi Health Department’s plan outlay. This figure highlights the cost-effectiveness of the initiative, suggesting that it could be scaled nationally. If implemented on a broader scale, the CTS would constitute approximately 1.5% of India’s Health Ministry’s plan outlay, making it a financially feasible model for wider adoption across the country.
Conclusion and Future Directions
The CTS has made notable progress in supporting PLHIV and children affected by HIV, with DSACS demonstrating a strong commitment to refining the scheme over time. Key achievements include improved adherence to ART and better access to financial support for the target population. However, there is still room for improvement, particularly in addressing the needs of single orphans, revising ART enrollment criteria to include all HIV-positive children regardless of ART duration, and implementing a more rigorous monitoring system.
Expanding outreach efforts to increase enrollment, particularly among orphans and vulnerable children, and exploring the potential for a national rollout could provide a sustainable model for HIV-related social protection schemes across India. Further research is necessary to evaluate the long-term effects of cash transfers on health outcomes like viral suppression. By making these adjustments, the CTS can amplify its impact and make a more substantial contribution to the well-being of PLHIV and HIV-affected children across the country.
Funding
This research received no external funding.
Author contribution
All authors contributed to the study conception and design. Mrinalini Darswal did overall supervision of the study. Material preparation, data collection and analysis were performed by Bipin Chandra Joshi. Anil Kumar Gupta was instrumental in planning and launch of the scheme from its inception, drafted the first manuscript and revised it critically for important intellectual content. Praveen Kumar took initiatives for improvements and long -term sustainability of the scheme. All authors actively worked and approved the final manuscript.
Institutional Review Board Statement
The work presented in the paper has been accorded approval of Ethical Committee of Delhi State AIDS Control Society vide Approval Number: DSACS/Ethics-Committee/01-12-23. Further, the consent from individual subjects was not required as their identity had not been disclosed in the study.
Informed Consent Statement
Not applicable
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgements
The authors express their gratitude to the National Commission for Protection of Child Rights for bringing attention to the issue of HIV orphans in Delhi, which ultimately spurred the formulation of the scheme. Additionally, we extend our thanks to the staff of all Government ART centres in Delhi, as well as the support staff of DSACS, particularly Sh. Kuldeep Rai, Sh. Surender Rana, and Sh. Ishwar Singh, along with NGOs dedicated to aiding children affected by HIV, for their invaluable cooperation. Their contributions are indispensable to the successful implementation of this scheme.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript
ART Antiretroviral Therapy
CBOs Community Based Organizations
DO-ChABH Double Orphan Children Affected by HIV
CTS Cash Transfer Scheme
DCI Destitute Children Living with HIV
DSACS Delhi State AIDS Control Society
(LTFU) Lost to Follow-up
NACO National AIDS Control Organization
NGOs Non-Government Organizations
OCI Orphan Children Living with HIV
OVC Orphan Vulnerable Children
PLHIV People living with HIV
y-o-y Year-on- Year
References
- National AIDS Control Organization (NACO, 2022). India HIV Estimates 2021 Fact Sheet. Ministry of Health & Family Welfare, Government of India.
- https://naco.gov.in/sites/default/files/India%20HIV%20Estimates%202021%20_Fact%20Sheets__Final_Shared_24_08_2022.
- World Health Organization (WHO, 2016). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. 2nd Edition.
- https://www.who. 9789.
- Gupta, A.K.; Rawat, N.; Rai, K.; Rana, S.; & Sabyasachi, C.; & Sabyasachi, C. Orphan and vulnerable children infected or affected by HIV/AIDS in Delhi – situational analysis and state government's initiative of household economic strengthening. Vulnerable Children and Youth Studies 2013, 8, 161–170. [Google Scholar] [CrossRef]
- . [CrossRef]
- Packel, L. , Njau, P., Fahey, C.; Ramadhani, A.; Dow, W.H.; Jewell, N.P.; & McCoy, S. Optimizing the efficiency and implementation of cash transfers to improve adherence to antiretroviral therapy: study protocol for a cluster randomized controlled trial. Trials 2020, 21, 963. [Google Scholar] [PubMed]
- . [CrossRef]
- Yotebieng, M.; Thirumurthy, H.; Moracco, K.E.; Edmonds, A.; Tabala, M.; Kawende, B.; Wenzi, L.K.; Okitolonda, E.W.; & Behets, F.; & Behets, F. Conditional cash transfers to increase retention in PMTCT care, antiretroviral adherence, and postpartum virological suppression: a randomized controlled trial. J Acquir Immune Defic Syndr 2016, 72, S124–9, 10.1097/QAI.0000000000001062. [Google Scholar] [PubMed]
- DOI: 10.1097/QAI.0000000000001062.
- McCoy, S.I.; Njau, P.F.; Fahey, C.; Kapologwe, N; Kadiyala, S. ; Jewell, N.P.; Dow, W.H.; & Padian,N.S. Cash vs. food assistance to improve adherence to antiretroviral therapy among HIV-infected adults in Tanzania. AIDS 2017, 31, 815–825. [Google Scholar] [PubMed]
- DOI: 10.1097/QAD.0000000000001406.
- Linnemayr, S.; Stecher, C.; & Mukasa, B.; & Mukasa, B. Behavioral economic incentives to improve adherence to antiretroviral medication. AIDS 2017, 31, 719–726, 10.1097/QAD.0000000000001387. [Google Scholar] [PubMed]
- DOI: 10.1097/QAD.0000000000001387.
- Guimarães NS, Magno L, de Paula AA, Silliman M, Anderle RVR, Rasella D, Macinko J, de Souza LE, Dourado I. The effects of cash transfer programmes on HIV/AIDS prevention and care outcomes: a systematic review and meta-analysis of intervention studies. Lancet HIV, 2023, 10, e394–e403. [CrossRef]
- Ministry of External Affair. Annual Report 2013-14. https://www.mea.gov.in/Uploads/PublicationDocs/23873_EXTERNAL_AFFAIR__Eng__AR_2013-14.
- National AIDS Control Organization (NACO, 2018). National AIDS Control Programme Care Support & Treatment Services- National technical guidelines on anti-retroviral treatment. Ministry of Health & Family Welfare, Government of India.
- https://naco.gov.in/sites/default/files/NACO%20%20National%20Technical%20Guidelines%20on%20ART_October%202018%20%281%29.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



