
Submitted:
12 October 2024
Posted:
15 October 2024
You are already at the latest version
Abstract
Hemostasis describes the process of blood clotting homeostasis. Hemostasis reflects a balance of procoagulant and anticoagulant mechanisms that aim to prevent both bleeding and thrombosis. If hemostasis is disrupted, and bleeding or thrombosis occur, then laboratory testing may ensue to either diagnose the reason for bleeding or thrombosis, or to manage patients under therapy or treatment for bleeding or thrombosis. A wide range of tests of hemostasis are available to laboratories and to clinicians from routine coagulation assays like prothrombin time (PT) and activated partial thromboplastin time (APTT) to specialized assays for von Willebrand factor (VWF) and platelet function. In the current narrative review, we highlight some of the history of innovative diagnostic solutions such as the integration of chemiluminescence and flow cytometry in the hemostasis diagnostic armamentarium, as well as providing a glimpse to the possible future of diagnostic hemostasis testing. This review also emphasizes the importance of harmonization and standardization in hemostasis testing to reduce variability and improve diagnostic accuracy. Future directions include the potential for artificial intelligence in diagnostics, the development of more global test systems that can assess both primary and secondary hemostasis, and the innovations required to follow continuous evolution of therapies requiring precise monitoring. This review underscores the ongoing need for innovation to enhance the diagnostic landscape of hemostasis, ensuring better patient outcomes through more accurate and efficient diagnostic methods.
Keywords:
hemostasis diagnostics
; therapeutic monitoring
; instrumentation
; innovation
1. Introduction to Hemostasis
Hemostasis describes the process of blood clotting homeostasis. Hemostasis involves a wide range of plasma proteins and blood cell components, especially platelets, and the vascular endothelium [1,2]. The plasma proteins include so called coagulation factors, generally identified by roman numerals, as well as adhesion proteins, and proteins involved in fibrinolysis. The coagulation proteins are often grouped into coagulation pathways, including terms such as ‘coagulation cascade’, ‘intrinsic pathway’ (or ‘contact factor pathway’), ‘extrinsic pathway’ (or ‘tissue factor pathway’), and ‘common pathway’ (Figure 1). The coagulation process involves a process of sequential enzymic activation of coagulation proteins that leads to eventual formation of a ‘clot’, largely composed of the soluble coagulation protein fibrinogen, after its conversion to an insoluble fibrin. These processes can be evaluated in hemostasis testing laboratories, either using routine coagulation laboratories, or specialised hemostasis testing (Table 1 and Table 2) [1]. For example, the prothrombin time (PT) assay starts at factor (F) VII (FVII), enters the common pathway at FX, and ends at fibrin formation, which is typically detected by an automated hemostasis analyzer (Figure 1). Instead, the activated partial thromboplastin time (APTT) assay starts at FXII, but after a few sequential factor activations also enters the common pathway at FX, and also terminates with fibrin formation, again typically detected by automated hemostasis analyzers (Figure 1).
Additional routine assays assessable by hemostasis laboratories within this pathway are the thrombin time (TT) assay and fibrinogen assays (Figure 1;Table 1). All these routine assays are performed using clot formation detection, and can be assessed with standard automated hemostasis analyzers. The fibrinogen level is most usually assessed as a so called functional von Clauss assay, named after its inventor [3]. It is also possible to perform assays to identify the level of individual clotting factors, as otherwise involved in secondary hemostasis (Table 2). These are usually measured using so called one-stage assays that reflect modifications of the PT (typically for FVII, FX, FII, FV) or APTT (FVIII, FIX, FXI, FXII) [4]. Because of relative test complexity and less frequent performance, these assays are usually performed in more specialised hemostasis laboratories. Collectively, the clotting factors are considered ‘procoagulant’ proteins, as they promote coagulation. A deficiency of clotting factors may therefore lead to bleeding, and an excess may in some cases lead to thrombosis [5]. To provide the balance for hemostasis, there are several physiological ‘anticoagulants’ that aim to dampen excess coagulation. These include antithrombin, protein C and protein S [1,5]. These act on different aspects of the coagulation pathway, and are typically measured (if needed) by specialised hemostasis laboratories. Deficiencies of these physiological anticoagulants can lead to thrombosis [5].
In addition to secondary hemostasis, additional adhesion proteins and cellular elements, especially platelets, contribute to the process of primary hemostasis [1,6]. The main adhesion protein in blood involved in hemostasis is called von Willebrand factor (VWF). Upon tissue injury, VWF binds to the damaged tissue, especially another protein called collagen, which activates VWF to expose the platelet receptor binding site on VWF [6]. VWF can then bind to platelets via the glycoprotein Ib (GPIb) receptor, causing platelet activation, and leading to platelet aggregation and formation of a platelet plug. In vivo, primary and secondary hemostasis act together to form a stable platelet/fibrin plug. VWF has additional hemostatic functions, including binding FVIII, thereby stabilizing and protecting FVIII from degradation, as well as delivering this important clotting factor to sites of injury to promote secondary hemostasis. Tests for VWF and platelet function are typically performed by specialised hemostasis laboratories (Table 2) [1].
After clot formation, the fibrinolysis pathway is activated to prevent excessive clot formation, to dissolve the clot and to permit tissue repair. The level of active in vivo fibrinolysis can be measured by a blood test called D-dimer, since the this is a specific breakdown product arising from fibrin formation and breakdown. D-dimer testing usually forms part of routine coagulation (Table 1) [1]. The composite of clot formation and breakdown are considered parts of the secondary hemostasis pathways, although since in vivo primary and secondary hemostasis are intertwined, the links to primary hemostasis are also important.
2. When hemostasis Fails–Anticoagulant and Procoagulant Therapy
As noted previously, hemostasis represents a balance of pro- and anti-coagulant forces aiming to prevent bleeding and thrombosis (Figure 2). Insufficiency in procoagulant factors (e.g., deficiency of clotting factors, VWF or platelets, or their reduced activity) can lead to bleeding (e.g., hemophilia, von Willebrand disease [VWD]) [7,8], whereas insufficiency in anti-coagulant factors (e.g., deficiency of PC, PS or AT), or excess of procoagulant factors can lead to thrombosis [5]. It is possible to prevent or treat either bleeding or thrombosis by ‘replacing’ the missing or defective factors or otherwise using rebalancing hemostasis. For example, in patients deficient in FVIII (i.e., with hemophilia), therapy to treat or prevent bleeding may include replacement of FVIII, or use of FVIII bypassing therapy, or other means to rebalance hemostasis [7]. Similarly, in patients with VWD, bleeding can be treated or prevented using VWF concentrates [9]. In patients with thrombosis, or a tendency towards thrombosis, these can be treated with various clinical anticoagulants or ‘anti-thrombotics’ [10]. Of relevance, there has been extraordinary advances in such therapies over the past years (discussed later). In addition, it is also possible to monitor most of the above therapy using laboratory testing.
3. A Brief Review of Past Innovative Diagnostic Solutions in Hemostasis
The history of hemostasis testing is rich with innovation [2]. In large part, hemostasis researchers and laboratories developed tests to improve on existing methods. For example, one of the historical ‘classical’ anticoagulants used to treat or prevent thrombosis is warfarin, which is a vitamin K antagonist (VKA) that interferes with production of selective fully functional clotting factors (namely, FII, FVIII, FIX and FX) (Figure 1). Because patients have a variable therapeutic response to the action of warfarin, which is further affected by diet and other drug interactions, the VKA effect on coagulation in individual patients needs to be monitored by laboratory testing [11]. Too much warfarin can lead to bleeding, and too little warfarin can lead to thrombosis. The original test used for this purpose was the PT, but different PT reagents have different sensitivity to the effects of warfarin, due to variable sensitivity to FII, FVII, FIX and FX. Thus, the PT developed into a test called the INR (international normalized ratio), which adjusted for the variable reagent sensitivity. The INR is actually a mathematical formula (=(PT/MNPT)ISI, where the PT is the patient’s PT, the MNPT is the mean normal PT, and the ISI is the international sensitivity index, and represents a correction factor for the reagent/instrument variation). The INR represented a major advance in warfarin therapy monitoring [12].
The APTT is also a relative advance of the historically used PTT, which represented a more variable non-activated form of the APTT. The APTT is useful to assess levels of clotting factors, can also be used to monitor UH therapy, and as a test for investigation of the Lupus Anticoagulant (LA) [13].
For assessment of factor activity, the one-stage clotting assay classically represents the original methodology, and is still the current most common method for laboratory assessment of clotting factors [4]. However, for hemophilia diagnosis, FVIII testing by this method sometimes under-estimates FVIII activity, and sometimes over-estimates FVIII activity, as evidenced by clinical assessment of hemophilia severity. Thus, the development of chromogenic assays that better matched clinical severity represented a major breakthrough in hemophilia diagnosis and management [14].
For VWD diagnosis, there has been a huge increase in methods available to better diagnose VWD and its various subtypes (Table 3) [15,16,17]. In addition to measurement of VWF level (or antigen; VWF:Ag), the initial assays used to assess VWF function were the ristocetin induced platelet agglutination (RIPA) assay and the ristocetin cofactor (VWF:RCo) assay. However, the VWF:RCo assay could only detect one function of VWF, namely its binding to platelet GPIb. Thus, an assay to measure the ability of VWF to bind to damaged tissue, namely collagen, or the collagen binding (VWF:CB) assay represented yet another advance [18], as did the assay that assesses the ability of VWF to bind to FVIII (i.e., the VWF:FVIII binding assay) [19]. With each advance in VWD diagnostics came improvements in diagnosis of VWD and refinement of its various subtypes. With only the VWF:Ag and VWF:RCo as available assays, laboratories could identify most forms of VWD, but would miss type 2N VWD, and could not distinguish various subtypes, such as type 2A, 2M, and 2B VWD; all this meant non optimized VWD treatment therapy for affected patients.
3. Contemporary Innovative Diagnostic Solutions in Hemostasis
More Recent Innovations in Hemostasis Diagnostics are Highlighted Below.
3.1. INR Testing
Although the INR has improved the monitoring of VKA therapy, there remained huge problems in this field due to the need for laboratories to estimate and/or verify/validate the two additional components of the INR, namely the MNPT and the ISI. This leads to wide variability of INR values for the same homogenous samples, as evidenced in external quality assessment (EQA) exercises, and likely also applying to patient samples, since large variations in MNPT and ISI values may arise for the same reagent [20]. In classical times, the MNPT could be estimated using at least 20 normal individuals [12,21,22], but these are increasingly difficult to source in contemporary ethical settings. Also, we showed in 2008, that use of different sets of 20 normal individuals would lead to different MNPTs for the same PT reagents, and thus partially explaining the variability seen in INR values in EQA exercises [21]. Classically, estimation of the ISI requires an even more onerous method, using manual tilt method PTs of at least 20 normal individuals and 60 different samples from patients on stable warfarin therapy [22,23]. This method can only be achieved by large manufacturers of widely used PT reagents. Alternative methods for generating both MNPT and ISI values, and popularized by guidelines, suggested the use of commercial calibration plasma sets [22]. However, these still generated variable MNPTs and ISI values [21], and thus further explained the large variability seen in INR values in EQA exercises. We no longer use any of these classic methods to estimate and/or verify/validate MNPT and ISI values for our laboratory. Instead, we use a simple process of linear regression to compare replacement PT reagents against existing PT reagents, which has now been progressed to a large network of laboratories, and helped maintain continued low bias and variability for INRs compared to peer median values, even after a complete change of reagents and instrumentation [24].
Several alternatives to use of the PT or classical INR to monitor warfarin have also been proposed [25,26,27,28]. This includes the FiiX PT method [25,26] and the chromogenic FX assay [27,28], with potential preferential use when patients are transitioning between anticoagulants, and thus to measure relative anticoagulant effects.
3.2. Hemostasis Instrumentation
Hemostasis instrumentation has evolved over the past decades, as in part recently reviewed [2]. Some of the earlier semi-automated instruments required operators to change the direction and application of plastic tubing to permit a change of assays. Instruments have moved from optical clot detection to mechanical clot detection, and now some instruments are in development to have both as standard . The development of some alternate detection systems such as chemiluminescence detection has permitted analyte detection down to 0%. Today, such systems can also be incorporated into standard hemostasis instruments, so that eventually clot-detection, turbimetric testing (e.g., latex immuno-assays; LIA), chromogenic assays and chemiluminescence immuno-assays (CLIA) can all be performed on a single instrument. For example, one instrument from Stago Diagnostics called the sthemO incorporates mechanical testing with LIA, chromogenic assays, and chemiluminescence [29]. An alternative manufacturer has developed instruments that incorporate optical testing with LIA, chromogenic assays, and chemiluminescence. Along with such advances has come increasing accuracy and precision, as well as throughput. Our original hemostasis analyzer could perform a maximum of 24 tests/run of ~ 2 hours. Current analysers can maintain test throughputs in the hundreds/hr. It is also possible to combine hemostasis instruments into an automated line, although we do not feel this to necessarily be an improvement, as it has the capacity to dumb-down hemostasis to simple chemistry, since chemistry systems tend to dominate such automations.
3.3. VWF Testing
For VWD diagnosis and therapy monitoring, there has been a huge increase in methods available to better diagnose VWD and its various subtypes (Table 3). In addition to measurement of VWF level (or antigen; VWF:Ag), the initial assays to historically assess VWF function were the ristocetin based assays – ristocetin cofactor (VWF:RCo) and ristocetin induced platelet agglutination (RIPA) [30,31,32]. These assays use an antibiotic called ristocetin to unfold VWF and cause its activation to expose the platelet GPIb binding site on VWF. Native or fixed platelets would agglutinate in the presence of VWF activated by ristocetin, and this could be measured on a platelet aggregometer. The VWF:RCo assay was later modified to enable test performance on an automated hemostasis analyzer. However, this assay can only detect a single function of VWF, namely its binding to platelet GPIb. Therefore, an assay to measure the ability of VWF to bind to damaged tissue, namely collagen, or the collagen binding (VWF:CB) assay represented yet another advance [18], as did the assay that assesses the ability of VWF to bind to FVIII (i.e., the VWF:FVIII binding assay) [19]. With each advance came improvements in diagnosis of VWD and its various subtypes. With only the VWF:Ag and VWF:RCo, laboratories could identify most forms of VWD, but its diagnosis as a particular type was not possible (e.g., types 2A, 2M, and 2B VWD would give similar test patterns for VWF:Ag and VWF:RCo in different VWD types). Addition of VWF:CB to the test repertoire permitted better diagnosis of VWD, including better discrimination of VWD types (e.g., types 2A and 2M may give different test patterns taking into consideration all tests - VWF:Ag, VWF:RCo and VWF:CB). However, even these three assays combined would miss type 2N VWD, with this highlighting the added value of the VWF:FVIII binding assay [19]. With incorrect VWD comes incorrect or at best non optimized VWD treatment therapy. More recently, additional assays were developed to measure platelet GPIb binding, and have largely now replace the classical VWF:RCo assay. One such assay uses recombinant GPIb (VWF:GPIbR) with added ristocetin and can be either performed as a latex agglutination assay on a standard hemostasis analyzer [33], or else as attached to magnetic beads and chemiluminescence immunoassay (CLIA) technology [34]. Another assay that uses recombinant mutated GPIb (VWF:GPIbM) with gain of function and does not require ristocetin, and can also be performed as a latex agglutination assay on a standard hemostasis analyzer [35]. The VWF:GPIbR and VWF:GPIbM assays are considered to represent improved methodologies with better sensitivity to low levels of VWF and reduced variability compared to VWF:RCo [16]. In turn, this means more accurate diagnosis of VWD and its various types.
In addition to VWD diagnosis, these diagnostic assays, including their recent innovative improvements, can also be used to monitor therapy in VWD [36]. As noted, VWD represents a loss of VWF and/or its function, and this represents a hemostasis imbalance that can lead to bleeding (Figure 2). Thus, various therapies, including replacement of VWF and FVIII can be applied to correct for this deficiency and treat/prevent bleeding [9]. The efficacy of this therapy, and to ensure adequate treatment and also prevent over-treatment that can lead to thrombosis (Figure 2), can also be monitored using the same assays used for VWD diagnostic (Table 3) [36].
3.4. Platelet Function Testing
Platelets are small cells in blood that clump together at a site of injury to produce a platelet plug to seal the injured site and prevent further bleeding. Whilst all pathology laboratories can perform platelet counts as a part of a complete blood count or profile, only specialised hemostasis laboratories are capable of performing extensive platelet function testing [37]. Historically, this was performed on a platelet aggregometer, and required processing of blood to isolate the platelets within a fraction called platelet rich plasma (PRP). After preparation, the PRP would be challenged by a range of platelet aggregation agonists, and platelet aggregation monitored. The entire process is time consuming, preventing performance of more than one or two platelet function assessments per day. Preparation of PRP was also subject to generation of technical artifacts due to damaged or pre-activated platelets. Several innovative advances to platelet function testing have taken place in contemporary times. Although preparation of PRP could be avoided by using a whole blood aggregometer, these instruments historically required the detection system to be cleaned between agonist evaluations. So, one recent advancement was the development of the Multiplate, which uses disposable cartridges [38]. Of course, this advancement was associated with an increase in costs and laboratory waste. In addition, the ability to assess for threshold agonist responses, important to assess the degree of platelet function abnormality, was largely lost, thereby compromising diagnostic performance.
Another recent advance in platelet function testing was the ability to perform this analysis on automated hemostasis analyzers [39]. This innovation means that several platelet function studies can be performed at once, greatly increasing test efficiency. However, preparation of PRP remains an important and time-consuming pre-test activity.
Similarly, the Optimul system permits platelet function testing to be performed in 96-well plates, and detection of platelet aggregation using standard ELISA plate readers [40,41]. This process permits an effective large scale screening system, uses a small volume of blood, and can also be applied in remote centers that do not have extensive expertise in platelet function testing or access to aggregometers.
Finally, it is now also possible to undertake platelet function testing using alternate methods including flow cytometry [42,43]. This process also permits effective large-scale screening, and can also be applied in centers that do not have extensive expertise in platelet function testing or access to aggregometers. The procedures also require smaller volumes of blood, is not limited by platelet count, and do not in general require preparation of PRP.
Of course, sometimes platelet function testing is requested not for diagnostic testing but for platelet function screening or for monitoring of anti-platelet therapy [44]. As noted previously, some patients at risk of adverse cardiovascular events, including arterial thrombosis, may be provided with various anti-platelet medications, such as aspirin, clopidogrel, and the more modern agents [10]. Just as it is possible for a laboratory to use platelet function testing to diagnose a platelet function defect, laboratories can also assess the efficacy of anti-platelet medications using these assays. Although laboratories can use standard platelet function testing using an aggregometer and PRP to assess for anti-platelet medication effects, this is very time consuming, and various point of care test (POC) instruments can be instead used, as can the Multiplate [44]. Indeed, these POC instruments, including the Verify Now, are better options for this purpose.
Another instrument that can be used for platelet function screening is the platelet function analyzer (PFA). The first version, the PFA-100, was released in 1995, and reflected an advance on an earlier instrument called the Thrombostat-4000 [45]. The PFA-100 has recently had a facelift, with the more modern PFA-200 released in the mid 2010’s, but this version is still unavailable in the USA [46]. These instruments use a small volume of whole blood (<1.0 mL) per test cartridge to assess platelet function, and are sensitive to both severe platelet dysfunction and some anti-platelet medications, as well as to VWF level and function. The testing only takes around 5 minutes. On the other hand, this sensitivity comes at the cost of specificity, since an abnormal PFA closure time (CT) is not diagnostic of any particular defect. In our laboratory, the PFA found a home primarily as a quick screen for VWD, given its high sensitivity also to VWF dysfunction. Thus, a normal PFA usually indicated an absence of severe VWD [47]. We have also found the PFA to be useful in monitoring of VWD therapy [36].
3.5. Viscoelastic Testing
Although viscoelastic testing has been around for decades, it is entering a kind of renaissance, with several improved methodologies [48,49,50,51,52]. Viscoelastic testing essentially evaluates hemostasis in whole blood, and can include elements of both primary and secondary hemostasis. Currently, viscoelastic testing is mostly used to define transfusion requirements to maximize replacement therapies, including as required such components as fresh frozen plasma (FFP), fibrinogen concentrate or platelets, in particular in trauma and surgical procedures.
3.6. Other Global Assays of Hemostasis
As noted above, there are a large number of assays that can be used to provide discrete information on hemostasis (e.g., see Table 1, Table 2 and Table 3). It is also possible to undertake global assessments of hemostasis. The PFA test systems mentioned earlier provide a global assessment of primary hemostasis. There are also assays that can assess overall secondary hemostasis as well as fibrinolysis. For the former, the PT/INR and APTT assays are basic examples of assays measuring portions of secondary hemostasis. There are also assays that measure thrombin generation that represent even broader measures of secondary hemostasis [53]. As another example, the Thrombin generation global thrombosis test (GTT) is an automated point-of-care technique that simulates the formation of a thrombus in whole blood under high shear flow and measures the time for occlusive thrombus formation as well as spontaneous, endogenous thrombolysis/fibrinolysis [54]. Other global assays that can help assess overall hemostasis and fibrinolysis are the “overall hemostasis potential” (OHP), the “overall coagulation potential” (OCP) and the “overall fibrinolysis potential” (OFP) [55,56].
3.7. Monitoring Hemophilia Treatment
Hemophilia represents a loss of FVIII (hemophilia A) or FIX (hemophilia B). Classical therapy for hemophilia therefore required replacement of the missing FVIII or FIX [7]. Monitoring of such therapy is important to ensure enough FVIII or FIX is given to prevent bleeding, but not so much, which is both wasteful of these precious resources and may lead to thrombosis if given in excess (Figure 2). In the past, this was a relatively straightforward procedure involving one stage clotting assays for FVIII or FIX, supplemented if needed using chromogenic assays [4,14]. However, the evolution in therapy for hemophilia has been extraordinary, moving from plasma derived to recombinant FVIII and FIX, and then from standard half-life (SHL) recombinant products to extended half-life (EHL) products to bypassing agents, FVIII mimetics and even gene therapy. This has required a complete rethink of therapy monitoring [57,58,59,60,61,62]. First, whereas plasma derived FVIII and FIX yielded similar results for one-stage clotting factor assays vs chromogenic factor assays, some of the SHL recombinant products yielded different results, with either one-stage or chromogenic assays providing more or less accurate assessments of factor levels, depending on the product used. This situation has become far more complex with EHL products, and even more complex with the use of bypassing agents and FVIII mimetics. Indeed, different assays may best suit monitoring of different products, which becomes even more complex in the presence of factor inhibitors. In brief, different assays, including different chromogenic assays, some with human-origin and others with non-human origin components, may be required for different patients and in different situations (e.g., presence of inhibitors) [57,58,59,60,61,62].
3.8. Diagnosis of TTP and TTP Treatment Monitoring Innovations
TTP, or thrombotic thrombocytopenic purpura, is a life-threatening disorder caused by a deficiency of ADAMTS-13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) activity. The function of ADAMTS-13 is to cleave VWF, in particular large VWF multimers, and thus reduce VWF activity. A deficiency of ADAMTS-13, in particular its absence (as in TTP) leads to an accumulation of large VWF molecules, and thus represents an imbalance of hemostasis (Figure 2) that leads to (micro)thrombosis. In the past, assessment of ADAMTS-13 activity required time consuming and laborious assays, which compromised fast diagnosis of TTP, and also its monitoring during treatment [63]. ADAMTS-13 assays were improved following the further characterization of ADAMTS-13 and development of recombinant ADAMTS-13 and VWF fragments that could be tagged with chromophores [64]. In the immediate past, these assays were developed into ELISA (enzyme linked immunosorbent assay) methods. However, these still required hours to provide a test result. Recently, the advent of automated CLIA and FRETs (fluorescence resonance energy transfer) methods have revolutionized the diagnosis of TTP, with assays completed in half an hour [64,65,66,67,68]. These automated methods have also improved monitoring of therapy, since efficacy of treatments can be assessed in a timelier manner. The same assays used to assess ADAMTS-13 activity can also be used to assess for inhibitors to ADAMTS-13, especially important in diagnosing acquired or immune TTP, representing well over 90% of all TTP cases [69,70].
3.7. Lupus Anticoagulant Testing
LA testing reflects one of the most often performed procedures in specialised hemostasis laboratories. LA testing may be performed to investigate an unexpectedly prolonged APTT, or for evaluation of patients presenting with thrombosis or pregnancy morbidity, and as a diagnostic tool for antiphospholipid syndrome (APS) [71]. In the past, testing was performed by a variety of tests, mostly using manual clot-based assays, including kaolin clotting time, and platelet neutralization. Currently, most of the older assays are no longer performed, and instead there are a large variety of more modern assays, often based on snake venom activation of clotting factors, and able to be performed on automated hemostasis analyzers [71,72,73], and may also include global assays such as thrombin generation [74]. Current diagnostic guidelines recommend using two tests with different principles before excluding LA in any given patient or situation, with the APTT and dRVVT (dilute Russell Viper venom time) being recommended [71]. These tests are very sensitive to LA and can be made more specific for LA using paired reagents, one of which has low phospholipid composition (to be LA sensitive), and the other having high phospholipid composition (to be LA relatively insensitive to LA). Thus, a sample yielding prolonged clotting times with the LA sensitive reagent, but reduced clotting times with the LA insensitive reagent is considered to be ‘diagnostic’ for LA. While this testing works well in patients not under coagulation therapy, the procedures tend to fail when patients are on clinical anticoagulant therapy.
Unfortunately, the risk of assessing patients for LA whilst under clinical anticoagulant therapy is now very high, with this leading to both false positive and false negative LA findings [75]. The time course of testing is such that testing is often applied to patients who have an ‘unexpected’ prolonged APTT, or who have suffered a recent thrombosis. In the first case, the ‘unexpected’ prolonged APTT might itself be due to the presence of anticoagulant therapy, and in the second situation, treatment for thrombosis includes the use of anticoagulant therapy, so this may have already been applied prior to sample testing. Most clinical anticoagulants affect clotting times, including APTT and dRVVT assays. Indeed, these anticoagulants may provide complex and difficult to interpret test patterns [Table 4]. For example, both dabigatran and rivaroxaban tend to produce test results that lead to false positive LA patterns using the dRVVT assays, whilst apixaban use may lead to a false negative dRVVT LA pattern [75]. In contrast, since most dRVVT reagents contain heparin neutralizers, heparin is more likely to affect APTT assays. VKA use will affect both APTT and dRVVT assays.
Fortunately, there are strategies developed to help overcome these anticoagulant interferences. As noted, most dRVVT reagents contain heparin neutralizers, and so are unaffected by therapeutic levels of UH. However, APTT reagents generally do not include these heparin neutralizers, since these may instead alternatively be used for UH monitoring. One strategy then, could be to replace the standard CaCl2 used in APTT assays with a CaCl2 containing a heparin neutralizer [76]. Alternate strategies include use of methods that are relatively insensitive to anticoagulant interferences. For example, the Taipan Snake Venom Time (TSVT) is insensitive to the effects of anti-FXa inhibitors such as rivaroxaban and apixaban, as well as VKAs, but is LA sensitive. The TSVT can be paired with the Ecarin Time as the LA-confirmatory test since it is insensitive to LA, and also insensitive to the effects of anti-FXa inhibitors and VKAs [72,73]. An alternative to overcome the anticoagulant effect of DOACs is to use DOAC neutralizers, as discussed in the next section.
3.8. Anticoagulant Neutralizers
As noted several times in this review, clinical anticoagulants cause prolongation in most clot-based assays. Indeed, clinicians and laboratories use several tests to monitor anticoagulant therapy (Table 4). These include the INR for monitoring VKAs, the APTT and anti-FXa assay for monitoring heparin therapy, direct thrombin inhibition (DTI) assays for dabigatran, and specific anti-FXa assays for the anti-FXa DOACs. However, the presence of these clinical anticoagulants causes unwanted interference in most of the other clot-based assays used within routine coagulation and specialised hemostasis laboratories, and sometimes also chromogenic assays. To make the INR sensitive to VKAs, but insensitive to heparin, PT reagents tend to include heparin neutralizers (Table 4). Instead, APTT reagents do not heparin neutralizers since many of these are used to monitor UH heparin therapy. Most dRVVT reagents also contain heparin neutralizers to enable better specificity for LA. Unfortunately, the changing landscape of anticoagulant therapy creates new and ongoing challenges for manufacturers and laboratories aiming to create hemostasis assays relatively insensitive to anticoagulant interference. Fortunately, there are some very smart scientists who rise to this challenge. As mentioned above, one strategy to make the APTT insensitive to heparin, and thus more specific for LA, is to use a CaCl2 reagent that contains a heparin neutralizer [76]. DOACs are now the leading clinical anticoagulants in clinical use [77]. These cause complex changes to hemostasis assays (Table 4).
One very useful recent innovation, then, is the development and use of DOAC neutralizers capable of absorbing all current DOACs, and thus enable hemostasis tests to be used as intended [78]. Our own experience is with a commercial product called DOAC-Stop, which can be added to DOAC containing samples to facilitate more accurate testing for a wide range of assays, including factor assays, LA assays, and assays for APCR (activated protein C resistance) [78,79,80,81]. However, other commercial options are now available, and all shown to be effective in DOAC neutralization.
3.9. Harmonization and Standardization
Another innovation in hemostasis diagnostics is the process of harmonization and standardization in testing. Our own experience in this process includes harmonization and standardization within the EQA process, and also as applied to a large network of 60 laboratories performing routine coagulation tests with over 85 hemostasis instruments [82]. Using this process, our large network can now standardize to single lots of routine reagents (e.g., PT/INR and APTT), single MNPT and ISI values for INR across all laboratories using the same PT reagent, common standardized reference ranges for all tests performed in the network using the same reagents and instrument class, and common therapeutic ranges for anticoagulant monitoring, including the APTT therapeutic range for UH. This process provides for huge time and cost savings, as well as numerous other efficiencies across the entire network. Additional examples of harmonization and standardization initiatives are detailed elsewhere, and include the external quality assessment process [83].
4. Future Innovative Diagnostic Solutions in Hemostasis
Of course, none of us has a magical crystal ball able to accurately identify future innovations that will provide improved diagnostic solutions in hemostasis. Nevertheless, we can conjecture, based on past experience. For DOAC neutralization, the current process requires adding the product (typically activated charcoal) to the sample containing the DOAC, and then centrifuging out the material with the DOAC absorbed out of the sample. Then the ‘cleaned’ sample can be used for diagnostic testing. Although this process works, it requires additional time and effort, and for a busy lab such as ours, performing in excess of 100 LA tests a week, could be difficult to enact uniformly. The centrifugation is required because the activated charcoal product would itself interfere with the clot-detection optics of many automated hemostasis analysers. Similarly, the product cannot be added to current reagents, since this would prevent subsequent centrifugation to remove the DOAC neutralizer. However, we have recently shown in a proof-of-concept paper that a liquid form of DOAC-Stop can be used without centrifugation for mechanical clot-detection instruments [84]. This may lead to development of DOAC neutralizers added into select hemostasis reagents for immediate use in select mechanical test systems, and without need for an extra centrifugation step.
We would also be naïve to think that we have seen the last clinical anticoagulant to be developed. The DOACs represent the current state of the art in clinical anticoagulant therapy, but there are other anticoagulants in development; for example, the so-called anti-FXI agents [85,86]. As such anticoagulants are developed and then deployed, manufacturers and laboratories will need to consider methods to monitor these agents (if required) and also to overcome unwanted interference in diagnostic assays (as required). Similarly, whilst aspirin reflects a classical anti-thrombotic, the anti-P2Y12 inhibitors were developed to improve overall efficacy of anti-thrombotic therapies [87]. These include the agents clopidogrel, ticlopidine, ticagrelor, prasugrel, and cangrelor. Clinicians may want to periodically monitor the efficacy of these agents with platelet function assays, and perhaps some emerging POC methods, perhaps at the cardiologist’s rooms and only requiring a finger prick sample, would best suit?
Similarly, there are a plethora of procoagulant or hemostasis rebalancing agents under development [7,57,58,59,60,61,62,88]. These could be applied to a wide range of patients at risk of bleeding, either because they have a deficiency (e.g., of FVIII, FIX or VWF) or have been hemostatically challenged (e.g., trauma, menstruation, surgery). Laboratories may need to monitor the efficacy of such treatments in select situations. Given the diverse nature of products under development, perhaps broad or global assays such as thrombin generation will finally find a place in most hemostasis laboratories?
Platelet function testing typically involves assessment of blood or PRP using discrete platelet agonists. These tests typically also require samples containing normal platelet counts. It would be diagnostically useful to develop additional assays that have less constraints, and better reflect in vivo physiology [89,90,91]. For example, most test systems do not use flow shear to assess platelet function, and the involvement of endothelium is absent. Perhaps the test systems of the future will enable this?
Finally, why settle on a process that restricts assessment to individual hemostasis test components or of platelet function? We can envisage the development of more global test systems to even supplement current global test systems, for example thrombin generation for secondary hemostasis and the PFA for primary hemostasis. As our understanding of hemostasis pathways develops, so too will models for mimicking hemostasis and thrombosis, and subsequently instruments and tests that model that mimic hemostasis and thrombosis, perhaps using in vitro flow-based assays [92]. Moreover, the use of additional new platelet transcriptome methods can improve our understanding of platelet reactivity, for example its contribution to peripheral artery disease [94].
5. Conclusion
The field of hemostasis testing has witnessed significant innovation over the past decades, driven by the need for more accurate, efficient, and comprehensive testing methods. From the evolution of routine coagulation assays to the development of specialized tests, these innovations have greatly enhanced our ability to diagnose and manage bleeding and thrombotic disorders. These advancements not only improve diagnostic accuracy, but also facilitate better patient management by enabling tailored therapeutic approaches. We have tried to capture some of that innovation in our review. It is inevitable that such innovation will continue in the future. The future of this field also lies in the harmonization and standardization of testing protocols, the creation of more global and physiologically relevant assays, and the seamless incorporation of these innovations into clinical practice. We give praise to those very smart people who innovate and ultimately improve the diagnostic landscape that is hemostasis testing. We also await with interest, the future involvement of artificial intelligence (AI) in future innovations [94,95] to ensure more precise diagnostics, optimized treatments, and ultimately, better patient outcomes in managing hemostatic disorders.
Author Contributions
Conceptualization, EJF and LP; methodology, EJF and LP; writing—original draft preparation, EJF; writing—review and editing, EJF and LP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable; no new data created in this review.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Favaloro EJ, Gosselin RC, Pasalic L, Lippi G. Hemostasis and Thrombosis: An Overview Focusing on Associated Laboratory Testing to Diagnose and Help Manage Related Disorders. Methods Mol Biol. 2023;2663:3-38. [CrossRef]
- Favaloro EJ. Evolution of Hemostasis Testing: A Personal Reflection Covering over 40 Years of History. Semin Thromb Hemost. 2024 Feb;50(1):8-25. [CrossRef]
- Von Clauss A. Gerinnungsphysiologische Schnellmethode zur Bestimmung des Fibrinogens. Acta Haematol. 1957;17:231–237.
- Duncan E, Rodgers S. One-Stage Factor VIII Assays. Methods Mol Biol. 2017;1646:247-263. [CrossRef]
- Marlar RA. Laboratory Evaluation of Thrombophilia. Methods Mol Biol. 2023;2663:177-201. [CrossRef] [PubMed]
- Lenting PJ, Denis CV, Christophe OD. Von Willebrand factor: how unique structural adaptations support and coordinate its complex function. Blood. 2024 Jul 5:blood.2023023277. [CrossRef]
- Chandran R, Tohit ERM, Stanslas J, Salim N, Mahmood TMT, Rajagopal M. Shifting Paradigms and Arising Concerns in Severe Hemophilia A Treatment. Semin Thromb Hemost. 2024 Jul;50(5):695-713. [CrossRef]
- Moser MM, Schoergenhofer C, Jilma B. Progress in von Willebrand Disease Treatment: Evolution towards Newer Therapies. Semin Thromb Hemost. 2024 Jul;50(5):720-732. [CrossRef]
- Connell NT, Flood VH, Brignardello-Petersen R, Abdul-Kadir R, Arapshian A, Couper S, Grow JM, Kouides P, Laffan M, Lavin M, Leebeek FWG, O'Brien SH, Ozelo MC, Tosetto A, Weyand AC, James PD, Kalot MA, Husainat N, Mustafa RA. ASH ISTH NHF WFH 2021 guidelines on the management of von Willebrand disease. Blood Adv. 2021 Jan 12;5(1):301-325. [CrossRef]
- Hirsh J, de Vries TAC, Eikelboom JW, Bhagirath V, Chan NC. Clinical Studies with Anticoagulants that Have Changed Clinical Practice. Semin Thromb Hemost. 2023 Apr;49(3):242-254.
- Talasaz AH, McGonagle B, HajiQasemi M, Ghelichkhan ZA, Sadeghipour P, Rashedi S, Cuker A, Lech T, Goldhaber SZ, Jennings DL, Piazza G, Bikdeli B. Pharmacokinetic and Pharmacodynamic Interactions between Food or Herbal Products and Oral Anticoagulants: Evidence Review, Practical Recommendations, and Knowledge Gaps. Semin Thromb Hemost. 2024 Sep 17. [CrossRef]
- Favaloro EJ. How to Generate a More Accurate Laboratory-Based International Normalized Ratio: Solutions to Obtaining or Verifying the Mean Normal Prothrombin Time and International Sensitivity Index. Semin Thromb Hemost. 2019 Feb;45(1):10-21. [CrossRef]
- Favaloro EJ, Kershaw G, Mohammed S, Lippi G. How to Optimize Activated Partial Thromboplastin Time (APTT) Testing: Solutions to Establishing and Verifying Normal Reference Intervals and Assessing APTT Reagents for Sensitivity to Heparin, Lupus Anticoagulant, and Clotting Factors. Semin Thromb Hemost. 2019 Feb;45(1):22-35. [CrossRef]
- Rodgers S, Duncan E. Chromogenic Factor VIII Assays for Improved Diagnosis of Hemophilia A. Methods Mol Biol. 2017;1646:265-276. [CrossRef]
- Platton S, Baker P, Bowyer A, Keenan C, Lawrence C, Lester W, Riddell A, Sutherland M. Guideline for laboratory diagnosis and monitoring of von Willebrand disease: A joint guideline from the United Kingdom Haemophilia Centre Doctors' Organisation and the British Society for Haematology. Br J Haematol. 2024 May;204(5):1714-1731. [CrossRef]
- James PD, Connell NT, Ameer B, Di Paola J, Eikenboom J, Giraud N, Haberichter S, Jacobs-Pratt V, Konkle B, McLintock C, McRae S, R Montgomery R, O'Donnell JS, Scappe N, Sidonio R, Flood VH, Husainat N, Kalot MA, Mustafa RA. ASH ISTH NHF WFH 2021 guidelines on the diagnosis of von Willebrand disease. Blood Adv. 2021 Jan 12;5(1):280-300.
- Favaloro EJ, Pasalic L. Laboratory diagnosis of von Willebrand disease in the age of the new guidelines: considerations based on geography and resources. Res Pract Thromb Haemost. 2023 Jun 30;7(5):102143. [CrossRef]
- Brown JE, Bosak JO. An ELISA test for the binding of von Willebrand antigen to collagen. Thromb Res. 1986 Aug 1;43(3):303-11. [CrossRef]
- Caron C, Mazurier C, Goudemand J. Large experience with a factor VIII binding assay of plasma von Willebrand factor using commercial reagents. Br J Haematol. 2002 Jun;117(3):716-8. [CrossRef]
- Bonar R, Favaloro EJ. Explaining and reducing the variation in inter-laboratory reported values for International Normalised Ratio. Thromb Res. 2017 Feb;150:22-29. [CrossRef]
- Favaloro EJ, Hamdam S, McDonald J, McVicker W, Ule V. Time to think outside the box? Prothrombin time, international normalised ratio, international sensitivity index, mean normal prothrombin time and measurement of uncertainty: a novel approach to standardisation. Pathology. 2008 Apr;40(3):277-87. [CrossRef]
- Clinical and Laboratory Standards Institute (2005) Procedures for validation of INR and local calibration of PT/INR systems; approved guideline. H54-A, vol. 25, No. 23. Wayne, PA: Clinical and Laboratory Standards Institute.
- Kirkwood TB. Calibration of reference thromboplastins and standardisation of the prothrombin time ratio. Thromb Haemost. 1983;49(3):238-244.
- Favaloro EJ, Arunachalam S, Chapman K, Pasalic L. Continued Harmonization of the International Normalized Ratio (INR) across a large laboratory network: Evidence of sustained low inter-laboratory variation and bias after a change in instrumentation. Am J Clin Pathol. 2024 Jul 18:aqae090. [CrossRef]
- Jonsson PI, Letertre L, Juliusson SJ, Gudmundsdottir BR, Francis CW, Onundarson PT. During warfarin induction, the Fiix-prothrombin time reflects the anticoagulation level better than the standard prothrombin time. J Thromb Haemost. 2017 Jan;15(1):131-139. [CrossRef]
- Onundarson PT, Palsson R, Witt DM, Gudmundsdottir BR. Replacement of traditional prothrombin time monitoring with the new Fiix prothrombin time increases the efficacy of warfarin without increasing bleeding. A review article. Thromb J. 2021 Oct 15;19(1):72. [CrossRef]
- Austin JH, Stearns CR, Winkler AM, Paciullo CA. Use of the chromogenic factor X assay in patients transitioning from argatroban to warfarin therapy. Pharmacotherapy. 2012 Jun;32(6):493-501. [CrossRef]
- Sanfelippo MJ, Zinsmaster W, Scherr DL, Shaw GR. Use of chromogenic assay of factor X to accept or reject INR results in Warfarin treated patients. Clin Med Res. 2009 Sep;7(3):103-5. [CrossRef]
- Pontis A, Delanoe M, Schilliger N, Carlo A, Guéret P, Nédélec-Gac F, Gouin-Thibault I. A performance evaluation of sthemO 301 coagulation analyzer and associated reagents. J Clin Lab Anal. 2023 Jun;37(11-12):e24929. [CrossRef]
- Favaloro EJ, Mohammed S, Patzke J. Laboratory Testing for von Willebrand Factor Antigen (VWF:Ag). Methods Mol Biol. 2017;1646:403-416. [CrossRef]
- Mohammed S, Favaloro EJ. Laboratory Testing for von Willebrand Factor Ristocetin Cofactor (VWF:RCo). Methods Mol Biol. 2017;1646:435-451. [CrossRef]
- Frontroth JP, Favaloro EJ. Ristocetin-Induced Platelet Aggregation (RIPA) and RIPA Mixing Studies. Methods Mol Biol. 2017;1646:473-494. [CrossRef]
- Seidizadeh O, Peyvandi F. Laboratory Testing for von Willebrand Factor Activity by a Glycoprotein Ib-Binding Assay (VWF:GPIbR): HemosIL von Willebrand Factor Ristocetin Cofactor Activity on ACL TOP®. Methods Mol Biol. 2023;2663:669-677. [CrossRef]
- Favaloro EJ, Mohammed S, Vong R, Pasalic L. Laboratory Testing for von Willebrand Disease Using a Composite Rapid 3-Test Chemiluminescence-Based von Willebrand Factor Assay Panel. Methods Mol Biol. 2023;2663:647-667. [CrossRef]
- Patzke J, Favaloro EJ. Laboratory Testing for von Willebrand Factor Activity by Glycoprotein Ib Binding Assays (VWF:GPIb). Methods Mol Biol. 2017;1646:453-460. [CrossRef]
- Favaloro EJ, Pasalic L, Curnow J. Monitoring Therapy during Treatment of von Willebrand Disease. Semin Thromb Hemost. 2017 Apr;43(3):338-354. [CrossRef]
- Hvas AM, Favaloro EJ. Platelet Function Analyzed by Light Transmission Aggregometry. Methods Mol Biol. 2017;1646:321-331. [CrossRef]
- Fritsma GA, McGlasson DL. Whole Blood Platelet Aggregometry. Methods Mol Biol. 2017;1646:333-347. [CrossRef]
- Sarkar MK, Hinz C. Assessment of Platelet Function by Automated Light Transmission Aggregometry. Methods Mol Biol. 2023;2663:611-625. [CrossRef]
- Hsu H, Chan MV, Armstrong PC, Crescente M, Donikian D, Kondo M, Brighton T, Chen V, Chen Q, Connor D, Joseph J, Morel-Kopp MC, Stevenson WS, Ward C, Warner TD, Rabbolini DJ. A pilot study assessing the implementation of 96-well plate-based aggregometry (Optimul) in Australia. Pathology. 2022 Oct;54(6):746-754. [CrossRef]
- Chan MV, Lordkipanidzé M, Warner TD. Assessment of Platelet Function by High-Throughput Screening Light Transmission Aggregometry: Optimul Assay. Methods Mol Biol. 2023;2663:627-636. [CrossRef]
- Pasalic L. Assessment of Platelet Function in Whole Blood by Flow Cytometry. Methods Mol Biol. 2017;1646:349-367. [CrossRef] [PubMed]
- Jourdi G, Ramström S, Sharma R, Bakchoul T, Lordkipanidzé M; FC-PFT in TP study group. Consensus report on flow cytometry for platelet function testing in thrombocytopenic patients: communication from the SSC of the ISTH. J Thromb Haemost. 2023 Oct;21(10):2941-2952. [CrossRef]
- Davidson S. Monitoring of Antiplatelet Therapy. Methods Mol Biol. 2023;2663:381-402. [CrossRef]
- Kundu SK, Heilmann EJ, Sio R, Garcia C, Davidson RM, Ostgaard RA. Description of an in vitro platelet function analyzer--PFA-100. Semin Thromb Hemost. 1995;21 Suppl 2:106-12. [CrossRef]
- Favaloro EJ, Pasalic L, Lippi G. Towards 50 years of platelet function analyser (PFA) testing. Clin Clin Chem Lab Med. 2023;61(5):851-860. [CrossRef]
- Favaloro EJ. Utility of the platelet function analyser (PFA-100/200) for exclusion or detection of von Willebrand disease: A study 22 years in the making. Thromb Res. 2020 Feb 1;188:17-24. [CrossRef]
- Volod O, Runge A. The TEG 6s System: System Description and Protocol for Measurements. Methods Mol Biol. 2023;2663:735-742. [CrossRef]
- Volod O, Runge A. The TEG 5000 System: System Description and Protocol for Measurements. Methods Mol Biol. 2023;2663:725-733. [CrossRef]
- Volod O, Runge A. Measurement of Blood Viscoelasticity Using Thromboelastography. Methods Mol Biol. 2023;2663:709-724. [CrossRef]
- Volod O, Viola F. The Quantra System: System Description and Protocols for Measurements. Methods Mol Biol. 2023;2663:743-761. [CrossRef]
- Reardon B, Pasalic L, Favaloro, EJ. The Role of Viscoelastic Testing in Assessing Hemostasis: A Challenge to Standard Laboratory Assays? J. Clin. Med. 2024 Jun 20;13(12):3612. [CrossRef]
- Depasse F, Binder NB, Mueller J, Wissel T, Schwers S, Germer M, Hermes B, Turecek PL. Thrombin generation assays are versatile tools in blood coagulation analysis: A review of technical features, and applications from research to laboratory routine. J Thromb Haemost. 2021 Dec;19(12):2907-2917. [CrossRef]
- Kanji R, Leader J, Memtsas V, Gorog DA. Measuring Thrombus Stability at High Shear, Together With Thrombus Formation and Endogenous Fibrinolysis: First Experience Using the Global Thrombosis Test 3 (GTT-3). Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296231181917. [CrossRef]
- Chaireti R, Soutari N, Holmström M, Petrini P, Magnusson M, Ranta S, Pruner I, Antovic JP. Global Hemostatic Methods to Tailor Treatment With Bypassing Agents in Hemophilia A With Inhibitors- A Single-Center, Pilot Study. Clin Appl Thromb Hemost. 2024 Jan-Dec;30:10760296241260053. [CrossRef]
- Antovic A, Svensson E, Lövström B, Illescas VB, Nordin A, Börjesson O, Arnaud L, Bruchfeld A, Gunnarsson I. Venous thromboembolism in anti-neutrophil cytoplasmic antibody-associated vasculitis: an underlying prothrombotic condition? Rheumatol Adv Pract. 2020 Oct 16;4(2):rkaa056. [CrossRef]
- Yacoub OA, Duncan EM. Chromogenic Factor VIII Assay for Patients with Hemophilia A and on Emicizumab Therapy. Methods Mol Biol. 2023;2663:597-610. [CrossRef]
- Kershaw G, Dix C. Measuring Emicizumab Levels in the Hemostasis Laboratory. Methods Mol Biol. 2023;2663:589-595. [CrossRef]
- Abraham S, Duncan EM. A Review of Factor VIII and Factor IX Assay Methods for Monitoring Extended Half-Life Products in Hemophilia A and B. Methods Mol Biol. 2023;2663:569-588. [CrossRef]
- Kershaw G. Strategies for Performing Factor Assays in the Presence of Emicizumab or Other Novel/Emerging Hemostatic Agents. Semin Thromb Hemost. 2024 Jun 12. [CrossRef]
- Pruthi RK, Chen D. The Use of Bypassing Treatment Strategies in Hemophilia and Their Effect on Laboratory Testing. Semin Thromb Hemost. 2023 Sep;49(6):651-660. [CrossRef]
- Bowyer AE, Gosselin RC. Factor VIII and Factor IX Activity Measurements for Hemophilia Diagnosis and Related Treatments. Semin Thromb Hemost. 2023 Sep;49(6):609-620. [CrossRef]
- Woods AI, Paiva J, Dos Santos C, Alberto MF, Sánchez-Luceros A. From the Discovery of ADAMTS13 to Current Understanding of Its Role in Health and Disease. Semin Thromb Hemost. 2023 Apr;49(3):284-294. [CrossRef]
- Moore GW, Llusa M, Griffiths M, Binder NB. ADAMTS13 Activity Measurement by ELISA and Fluorescence Resonance Energy Transfer Assay. Methods Mol Biol. 2023;2663:533-547. [CrossRef]
- Favaloro EJ, Chapman K, Mohammed S, Vong R, Pasalic L. Automated and Rapid ADAMTS13 Testing Using Chemiluminescence: Utility for Identification or Exclusion of TTP and Beyond. Methods Mol Biol. 2023;2663:487-504. [CrossRef]
- Favaloro EJ, Mohammed S, Chapman K, et al. A multicentre laboratory assessment of a new automated chemiluminescent assay for ADAMTS13 activity. J Thromb Haemost 2021; 19(2):417-428.
- Singh D, Subhan MO, de Groot R, Vanhoorelbeke K, Zadvydaite A, Dragūnaitė B, Scully M. ADAMTS13 activity testing: evaluation of commercial platforms for diagnosis and monitoring of thrombotic thrombocytopenic purpura. Res Pract Thromb Haemost. 2023 Mar 10;7(2):100108.
- Irsara C, Anliker M, Egger AE, Harasser L, Lhotta K, Feistritzer C, Griesmacher A, Loacker L. Evaluation of two fully automated ADAMTS13 activity assays in comparison to manual FRET assay. Int J Lab Hematol. 2023 Oct;45(5):758-765.
- Moore GW, Vetr H, Binder NB. ADAMTS13 Antibody and Inhibitor Assays. Methods Mol Biol. 2023;2663:549-565. [CrossRef]
- Favaloro EJ, Chapman K, Mohammed S, Vong R, Pasalic L. Identification of ADAMTS13 Inhibitors in Acquired TTP. Methods Mol Biol. 2023;2663:505-521. [CrossRef]
- Devreese KMJ, de Groot PG, de Laat B, Erkan D, Favaloro EJ, Mackie I, Martinuzzo M, Ortel TL, Pengo V, Rand JH, Tripodi A, Wahl D, Cohen H. Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis: Update of the guidelines for lupus anticoagulant detection and interpretation. J Thromb Haemost. 2020 Nov;18(11):2828-2839. [CrossRef]
- oore GW, Jones PO, Platton S, Hussain N, White D, Thomas W, Rigano J, Pouplard C, Gray E, Devreese KMJ. International multicenter, multiplatform study to validate Taipan snake venom time as a lupus anticoagulant screening test with ecarin time as the confirmatory test: Communication from the ISTH SSC Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies. J Thromb Haemost. 2021 Dec;19(12):3177-3192. [CrossRef]
- Moore GW. Lupus Anticoagulant Testing: Taipan Snake Venom Time with Ecarin Time as Confirmatory Test. Methods Mol Biol. 2023;2663:263-274. [CrossRef]
- Ninivaggi M, de Laat-Kremers R, Tripodi A, Wahl D, Zuily S, Dargaud Y, Ten Cate H, Ignjatović V, Devreese KMJ, de Laat B. Recommendations for the measurement of thrombin generation: Communication from the ISTH SSC Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies. J Thromb Haemost. 2021 May;19(5):1372-1378.
- Favaloro EJ, Mohammed S, Curnow J, Pasalic L. Laboratory testing for lupus anticoagulant (LA) in patients taking direct oral anticoagulants (DOACs): potential for false positives and false negatives. Pathology. 2019 Apr;51(3):292-300. [CrossRef]
- Antihepca™-HRRS Heparin Resistant Recalcifying Solution. Available online: https://www.haematex.com/haematex-products/antihepca-hrrs (accessed on 6th October 2024).
- Favaloro EJ, Pasalic L, Lippi G. Oral anticoagulation therapy: an update on usage, costs and associated risks. Pathology. 2020 Oct;52(6):736-741. [CrossRef]
- Frackiewicz A, Kalaska B, Miklosz J, Mogielnicki A. The methods for removal of direct oral anticoagulants and heparins to improve the monitoring of hemostasis: a narrative literature review. Thromb J. 2023 May 19;21(1):58. [CrossRef]
- Exner T, Michalopoulos N, Pearce J, Xavier R, Ahuja M. Simple method for removing DOACs from plasma samples. Thromb Res. 2018 Mar;163:117-122. [CrossRef]
- Favaloro EJ, Pasalic L. Lupus anticoagulant testing during anticoagulation, including direct oral anticoagulants. Res Pract Thromb Haemost. 2022 Mar 15;6(2):e12676. [CrossRef]
- Exner T, Rigano J, Favaloro EJ. The effect of DOACs on laboratory tests and their removal by activated carbon to limit interference in functional assays. Int J Lab Hematol. 2020 Jun;42 Suppl 1:41-48. [CrossRef]
- Favaloro EJ, Mohammed S, Vong R, Pasalic L. Harmonization of Hemostasis Testing Across a Large Laboratory Network: An Example from Australia. Methods Mol Biol. 2023;2663:71-91. [CrossRef]
- Favaloro EJ, Gosselin R, Olson J, Jennings I, Lippi G. Recent initiatives in harmonization of hemostasis practice. Clin Chem Lab Med. 2018 Sep 25;56(10):1608-1619. [CrossRef]
- Exner T, Dangol M, Favaloro EJ. Simplified method for removing DOAC interference in mechanical coagulation test systems – a proof of concept. J Clin Med. 2024 Feb 12;13(4):1042. [CrossRef]
- Nolte CH. Factor XI inhibitors - Rising stars in anti-thrombotic therapy? J Neurol Sci. 2024 Sep 15;464:123157. [CrossRef]
- Connors JM. Factor XI inhibitors: a new class of anticoagulants. Blood Adv. 2024 Oct 8:bloodadvances.2024013852. [CrossRef]
- Nappi F. P2Y12 Receptor Inhibitor for Antiaggregant Therapies: From Molecular Pathway to Clinical Application. Int J Mol Sci. 2024 Jul 10;25(14):7575. [CrossRef]
- Moser MM, Schoergenhofer C, Jilma B. Progress in von Willebrand Disease Treatment: Evolution towards Newer Therapies. Semin Thromb Hemost. 2024 Jul;50(5):720-732. [CrossRef]
- Harada K, Wenlong W, Shinozawa T. Physiological platelet aggregation assay to mitigate drug-induced thrombocytopenia using a microphysiological system. Sci Rep. 2024 Jun 19;14(1):14109. [CrossRef]
- Zhang Y, Ramasundara SZ, Preketes-Tardiani RE, Cheng V, Lu H, Ju LA. Emerging Microfluidic Approaches for Platelet Mechanobiology and Interplay With Circulatory Systems. Front Cardiovasc Med. 2021 Nov 25;8:766513. [CrossRef]
- Yoon I, Han JH, Jeon HJ. Advances in Platelet-Dysfunction Diagnostic Technologies. Biomolecules. 2024 Jun 17;14(6):714. [CrossRef]
- Mangin PH, Neeves KB, Lam WA, Cosemans JMEM, Korin N, Kerrigan SW, Panteleev MA; Subcommittee on Biorheology. In vitro flow-based assay: From simple toward more sophisticated models for mimicking hemostasis and thrombosis. J Thromb Haemost. 2021 Feb;19(2):582-587. [CrossRef]
- Berger JS, Cornwell MG, Xia Y, Muller MA, Smilowitz NR, Newman JD, Schlamp F, Rockman CB, Ruggles KV, Voora D, Hochman JS, Barrett TJ. A Platelet Reactivity ExpreSsion Score derived from patients with peripheral artery disease predicts cardiovascular risk. Nat Commun. 2024 Aug 20;15(1):6902.
- Rashidi HH, Bowers KA, Reyes Gil M. Machine learning in the coagulation and hemostasis arena: an overview and evaluation of methods, review of literature, and future directions. J Thromb Haemost. 2023 Apr;21(4):728-743. [CrossRef]
- Favaloro EJ, Negrini D. Machine learning and coagulation testing: the next big thing in hemostasis investigations? Clin Chem Lab Med. 2021 Mar 3;59(7):1177-1179. [CrossRef]
Figure 1.
An overview of the main secondary hemostasis coagulation pathways, as also corresponding routine coagulation assays. Also shown are relevant anticoagulant points, both physiological and clinical. Protein C (PC), Protein S (PS) and antithrombin (AT) are natural anticoagulants that act primarily on FV and FVIII (PS/PC) or on thrombin (FIIa [AT]). The classical clinical anticoagulants are warfarin (W) and alternative vitamin K antagonists (VKAs) affecting FII, FVII, FIX and FX, and the heparins (unfractionated heparin [UH] and low molecular weight heparin [LMWH] affecting FXa (both UH and LMWH) and thrombin (FIIa; mostly UH). More recent clinical anticoagulants comprise the direct oral anticoagulants (DOACs), currently including the anti-FIIa agent dabigatran (D), and the anti-FXa agents rivaroxaban (R), apixaban (A) and edoxaban (E).
Figure 1.
An overview of the main secondary hemostasis coagulation pathways, as also corresponding routine coagulation assays. Also shown are relevant anticoagulant points, both physiological and clinical. Protein C (PC), Protein S (PS) and antithrombin (AT) are natural anticoagulants that act primarily on FV and FVIII (PS/PC) or on thrombin (FIIa [AT]). The classical clinical anticoagulants are warfarin (W) and alternative vitamin K antagonists (VKAs) affecting FII, FVII, FIX and FX, and the heparins (unfractionated heparin [UH] and low molecular weight heparin [LMWH] affecting FXa (both UH and LMWH) and thrombin (FIIa; mostly UH). More recent clinical anticoagulants comprise the direct oral anticoagulants (DOACs), currently including the anti-FIIa agent dabigatran (D), and the anti-FXa agents rivaroxaban (R), apixaban (A) and edoxaban (E).

Figure 2.
A pictorial representation of hemostasis in balance (A. left), with procoagulant and anticoagulant forces in balance. When procoagulant forces are decreased (e.g., due to lack of clotting factors [e.g., hemophilia]), hemostasis is not in balance, and this can lead to bleeding (B. middle). It is possible to increase the procoagulant forces (e.g., factor replacement in hemophilia) to rebalance hemostasis (i.e., drive hemostasis towards rebalance as in A). When anticoagulant forces are decreased (e.g., due to deficiency of PC, PS or AT), hemostasis is not in balance, and this can lead to thrombosis (C. right). It is possible to increase the anticoagulant forces (e.g., by use of clinical anticoagulants) to rebalance hemostasis (i.e., drive hemostasis towards rebalance as in A). In addition, an imbalance towards bleeding can also occur if anticoagulant forces are in excess (e.g., too much clinical anticoagulant applied), and an imbalance towards thrombosis can also occur if procoagulant forces are in excess (e.g., an excess of clotting factors are present). The hemostasis laboratory can assess elements of this hemostasis balance using a wide repertoire of routine coagulation (Table 1) and specialised hemostasis assays (Table 2 and Table 3).
Figure 2.
A pictorial representation of hemostasis in balance (A. left), with procoagulant and anticoagulant forces in balance. When procoagulant forces are decreased (e.g., due to lack of clotting factors [e.g., hemophilia]), hemostasis is not in balance, and this can lead to bleeding (B. middle). It is possible to increase the procoagulant forces (e.g., factor replacement in hemophilia) to rebalance hemostasis (i.e., drive hemostasis towards rebalance as in A). When anticoagulant forces are decreased (e.g., due to deficiency of PC, PS or AT), hemostasis is not in balance, and this can lead to thrombosis (C. right). It is possible to increase the anticoagulant forces (e.g., by use of clinical anticoagulants) to rebalance hemostasis (i.e., drive hemostasis towards rebalance as in A). In addition, an imbalance towards bleeding can also occur if anticoagulant forces are in excess (e.g., too much clinical anticoagulant applied), and an imbalance towards thrombosis can also occur if procoagulant forces are in excess (e.g., an excess of clotting factors are present). The hemostasis laboratory can assess elements of this hemostasis balance using a wide repertoire of routine coagulation (Table 1) and specialised hemostasis assays (Table 2 and Table 3).
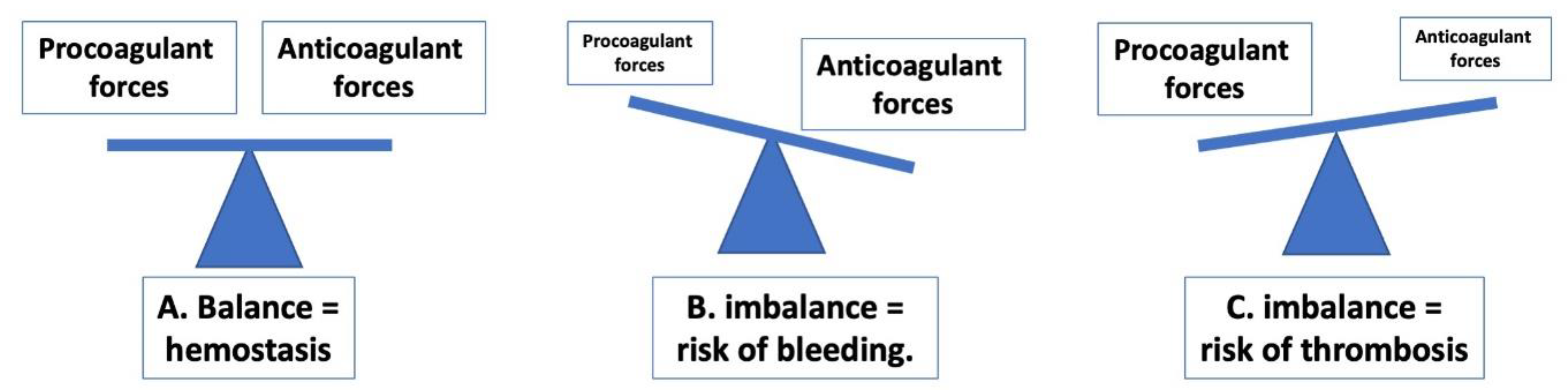

Table 1.
Routine coagulation assays. These tests will be available in most hemostasis testing laboratories.*.
Table 1.
Routine coagulation assays. These tests will be available in most hemostasis testing laboratories.*.
| Test Abbreviation |
Test | What the test measures | What the test is used for | What else is the test sensitive to? |
|---|---|---|---|---|
| PT | Prothrombin time | Tissue factor (TF) (also called extrinsic) pathway plus common pathway | Assessment of factor deficiency (I, II, V, VII, X). Monitoring of Vitamin K antagonist (VKA; e.g., warfarin) therapy (typically as the INR) Screen for disseminated intravascular coagulation (DIC) |
Various anticoagulants (e.g., unfractionated heparin [UH] in excess to heparin neutralizer capacity, direct oral anticoagulants [DOACs]) |
| INR | International normalized ratio | Same as PT, but reflective of a normalized ratio | Used to monitor patients on VKA therapy | Same as PT |
| APTT | Activated partial thromboplastin time | Contact factor (also called intrinsic) pathway plus common pathway | Assessment of factor deficiency (I, II, V, VIII, IX, X, XI, XII) Monitoring of UFH therapy Screen for DIC |
Various anticoagulants (e.g., DOACs) |
| TT | Thrombin Time | Measure of fibrinogen clotting activity | Screen for fibrinogen deficiency. Screen for UFH and other anti-II agents (e.g., dabigatran) Screen for DIC |
Various anticoagulants (e.g., lepirudin, bivalirudin) |
| D-D | D-dimer | The fibrin degradation product called D-dimer | Screen for venous thrombosis (e.g., deep vein thrombosis [DVT]; pulmonary thrombosis [PE]). Screen for DIC |
Depending on antibody used in assay, potentially variously sensitive to other fibrin or fibrinogen degradation products |
| Fib or FGN | Fibrinogen | Fibrinogen level (fibrinogen is the major coagulation protein) | Assessment of congenital or acquired fibrinogen deficiencies or abnormalities | Some assays may be affected by very high levels of some anticoagulants (e.g., UFH, dabigatran) |
* See also Figure 1.
Table 2.
Specialised hemostasis assays. These tests will be selectively available in different hemostasis testing laboratories.*.
Table 2.
Specialised hemostasis assays. These tests will be selectively available in different hemostasis testing laboratories.*.
| Test Abbreviation |
Test | What the test measures | What the test is used for | What else is the test sensitive to? |
|---|---|---|---|---|
| AT | Antithrombin | Antithrombin level or activity | Quantitation of antithrombin activity | Depending on how assay is performed (i.e., as based on anti-FXa or anti-FIIa) may be sensitive to various anticoagulants (e.g., DOACs) |
| PC | Protein C | Protein C level or activity | Quantitation of Protein C activity | Clot based assays may be affected by various anticoagulants, including DOACs. |
| PS | Protein S | Protein S level or activity | Quantitation of Protein S level or activity | Clot based assays may be affected by various anticoagulants, including DOACs. |
| LA | Lupus anticoagulant | Presence or absence of LA | To exclude/identify LA for diagnosis of APS or as a cause of APTT prolongation To help determine anticoagulant treatment for inpatient pending discharge |
Various anticoagulants depending on assays/reagents employed |
| Anti-Xa or anti-FXa | Anti-factor Xa | Level of various anticoagulants depending on test set up | To quantify levels of UH, LMWH, direct and indirect anti-FXa agents (e.g., apixaban, rivaroxaban, edoxaban, fondaparinux) | Each ‘specific’ anti-FXa assay is variously sensitive to the other anti-FXa agents |
| DTI or dTT | Direct thrombin inhibitor or dilute thrombin time | Level of various anticoagulants depending on test set up | To quantify levels of anti-FIIa agents (e.g., dabigatran) | Each ‘specific’ anti-FIIa assay potentially sensitive to other anti-FIIa agents |
| FII, FV, FVII, FVIII, FIX, FXI, FXII | Factors II, V, VII, VIII, IX, XI, XII | Level and activity of these clotting factors | To quantify these factor levels | All clot-based assays variably sensitive to various clinical anticoagulants |
| VWF | von Willebrand factor | Level and activity of VWF | To quantify VWF and its various activities | Different functional assays tend to be ‘specific’ for a particular VWF activity |
| ADAMTS-13 | ADAMTS-13 | Level and activity of ADAMTS-13 | To quantify ADAMTS-13 activity | May depend on assay |
| PFS | Platelet function studies | Platelet activity | To quality platelet activity or diagnose platelet dysfunction | Depends on assay |
*ADAMTS-13, a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; APS, antiphospholipid syndrome; LMWH, low molecular weight heparin; UH, unfractionated heparin.
Table 3.
An evolution in VWF testing in the diagnosis of VWD, and in monitoring its therapy. These tests will be selectively available in different hemostasis testing laboratories.*.
Table 3.
An evolution in VWF testing in the diagnosis of VWD, and in monitoring its therapy. These tests will be selectively available in different hemostasis testing laboratories.*.
| Test Abbreviation |
Test | What the test measures | What the test is used for | How is the test performed? |
|---|---|---|---|---|
| VWF:Ag | VWF antigen | Level of VWF | Quantitation of VWF level | Usually, LIA or ELISA; sometimes CLIA |
| RIPA | Ristocetin induced platelet agglutination/ aggregation | Activity of VWF binding to GPIb | Qualification of VWF GPIb binding activity | Platelet agglutination assay, usually on platelet aggregometer |
| VWF:RCo | VWF ristocetin cofactor | Activity of VWF binding to GPIb | Quantitation of VWF GPIb binding activity | Platelet agglutination assay, usually on automated hemostasis analyzer, sometimes on platelet aggregometer. |
| VWF:CB | VWF collagen binding | Activity of VWF binding to collagen (a matrix protein exposed by vascular damage) | Quantitation of VWF collagen binding activity | Usually, ELISA; sometimes CLIA. |
| VWFpp | VWF propeptide | Level of VWF propeptide | To quantify VWF propeptide as a marker of VWF clearance | ELISA |
| VWF:FVIIIB | VWF factor VIII binding | Activity of VWF binding to FVIII | Quantitation of VWF FVIII binding activity | ELISA |
| VWF:GPIbR | VWF GPIb recombinant | Activity of VWF binding to recombinant GPIb | Quantitation of VWF GPIb binding activity | Usually, latex agglutination assay on automated hemostasis analyzer, sometimes CLIA. |
| VWF:GPIbM | VWF GPIb (recombinant) mutant | Activity of VWF binding to recombinant mutated GPIb | Quantitation of VWF GPIb binding activity | Usually, latex agglutination assay on automated hemostasis analyzer, sometimes ELISA. |
* LIA, latex immunoassay; CLIA, chemiluminescence immunoassay; ELISA, enzyme linked immunosorbent assay; VWF, von Willebrand factor; VWD, von Willebrand disease; CB, collagen binding; RCo, ristocetin cofactor; GPIb, glycoprotein Ib (the platelet VWF receptor); R, recombinant; M, mutant.
Table 4.
Interference of anticoagulants vs laboratory monitoring of anticoagulants vs in vitro neutralization of anticoagulants.*.
Table 4.
Interference of anticoagulants vs laboratory monitoring of anticoagulants vs in vitro neutralization of anticoagulants.*.
| Test / Parameter |
Anti-FXa DOACs | Anti-FIIa DOACs (dabigatran) | VKAs | Heparins (UH/LMWH) |
|---|---|---|---|---|
| PT/INR Depends on: |
- / ↑ / ↑↑ DOAC, [DOAC], reagent |
- / ↑ [DOAC], reagent |
↑ / ↑↑ / ↑↑↑ [VKA], reagent |
- / ↑ heparin type, [heparin], presence of neutralizers |
| APTT Depends on: |
- / ↑ DOAC, [DOAC], reagent |
↑ / ↑↑ [DOAC], reagent |
↑ / ↑↑ [VKA], reagent |
↑ / ↑↑ / ↑↑↑ heparin type, [heparin], reagent |
| TT Depends on: |
- | ↑↑↑ | - | ↑ / ↑↑ / ↑↑↑ heparin type, [heparin], reagent |
| D-D | - | - | - | - |
| Fib Depends on: |
- / ↓ [DOAC], reagent |
- / ↓ [DOAC], reagent |
- | - / ↓ heparin type, [heparin], reagent |
| Anti-FXa assays Depends on: |
↑ / ↑↑/ ↑↑↑ [DOAC] |
- | - | ↑ / ↑↑/ ↑↑↑ [heparin] |
| Factor assays Depends on: |
↓ / ↓↓ [DOAC] |
↓ / ↓↓ [DOAC] |
↓ / ↓↓ Factor type, [VKA] |
- ( / ↓ ) heparin type, [heparin] |
| PC, PS Depends on: |
- / ↑ [DOAC], reagent |
- / ↑ [DOAC], reagent |
↓ / ↓↓ [VKA] |
- ( / ↓ ) heparin type, [heparin], reagent |
| AT Depends on: |
- / ↑ [DOAC], reagent |
- / ↑ [DOAC], reagent |
- |
- / ↑ heparin type, [heparin], reagent |
| APCR Depends on: |
- / ↑ [DOAC], reagent |
- / ↑ [DOAC], reagent |
- / ↑ [VKA], reagent |
- / ↑ heparin type, [heparin], reagent |
| LA Depends on: |
- / ↓ / ↑ / ↑↑ DOAC type/ [DOAC], reagent |
↑ / ↑↑ [DOAC], reagent |
- / ↓ / ↑ / ↑↑ [VKA], reagent |
- / ↑ heparin type, [heparin], reagent, presence of heparin neutralizers |
| VWF, Platelet function |
- | - | - | - |
| TGA Depends on: |
↓ / ↓↓/ ↓↓↓ DOAC type/ [DOAC], reagent |
↓ / ↓↓/ ↓↓↓ [DOAC], reagent |
↓ / ↓↓/ ↓↓↓ [VKA], reagent |
↓ / ↓↓/ ↓↓↓ heparin type, [heparin], reagent |
| VEA | ↑ / ↑↑ [DOAC], reagent, system |
↑ / ↑↑ [DOAC], reagent, system |
- / ↑ [VKA], reagent, system |
- / ↑ heparin type, [heparin], reagent, system |
| Monitor or measure with: | Specific anti-FXa assays | Specific anti-FIIa assay (e.g., direct thrombin inhibitor [DTI) assay. Ecarin based assays |
PT/INR | APTT, anti-FXa assay |
| Neutralize with: | Activated charcoal (e.g., DOAC-Stop) | Activated charcoal (e.g., DOAC-Stop) | - (mixing studies) | polybrene, hepzyme |
* Anti-FXa DOACs include apixaban, rivaroxaban, endoxaban. Anti-FIIa DOACs currently comprises dabigatran. Abbreviations: APCR, activated protein C resistance; APTT, Activated partial thromboplastin time; AT, antithrombin; D-D, D-dimer; DOACs, direct oral anticoagulants; Fib, Fibrinogen; LA, lupus anticoagulant; VKAs, vitamin K antagonists; LMWH, low molecular weight heparin; UH, unfractionated heparin; PC, protein C; PS, protein S;PT/INR, PT, Prothrombin time; TGA, thrombin generation assay; INR, international normalized ratio; TT, Thrombin Time; [DOAC], DOAC level or concentration; [VKA], VKA level; [heparin], heparin level or concentration; VEA, viscoelastic assays; VWF, von Willebrand factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



