Submitted:
14 October 2024
Posted:
15 October 2024
You are already at the latest version
Abstract
Background: To evaluate the incidence of postsurgical cystoid macular edema (PCME) after small-gauge pars
plana vitrectomy (PPV) for different retinal pathologies and to assess the role of optical coherence tomography
(OCT) biomarkers to guide treatment decision in patients with PCME, refractory to medical therapy.
Materials and Methods:
Medical records of consecutive pseudophakic patients, who underwent PPV for different retinal pathologies,
were retrospectively evaluated in this single center, uncontrolled study.
The incidence of post-PPV CME was assessed in this population. Eyes that presented with post-PPV CME within the first 2 months after surgery were considered for further evaluation. A minimum follow-up of 12 months, history of previous cataract surgery performed not earlier than 1 year before PPV, the availability of full clinical and OCT data at 1, 3, 6, 9 and 12 months after PPV, constituted the minimal requirements to be included in the 12-months assessment. Mean best corrected visual acuity (BCVA; LogMAR) together with mean central macula thickness (CMT; m) change, and response to different treatments (medical therapy and dexamethasone intravitreal implant) were evaluated. The impact of specific clinical and structural OCT biomarkers on the exposure to dexamethasone (DEX) intravitreal treatment was assessed. Eventual ocular and non-ocular adverse events, potentially related to the treatment, were investigated as-well.
Results: Of 346 pseudophakic patients (352 eyes) enrolled in the study, 54 (54 eyes) developed CME within the first 2 months after PPV (incidence of 15.3%). After the exclusion of 6 subjects, the remaining 48 pa-tients were dimed eligible for the 12-months analysis. Preoperative mean BCVA (1.44 ± 0.99 LogMAR) sig-nificantly improved to 0.32 ± 0.37 LogMAR at 12 months (P< 0.001). Mean baseline CMT of 347 (± 123.5) m, significantly decreased to 290 m (± 80.4; P=0.003) by the end of the FU. Twenty-five eyes (52%) re-quired one or more DEX intravitreal implants for CME, refractory to topical therapy. The correlation analy-sis disclosed the existence of significant correlations between mean CMT values at different time points of the FU. Additionally, patients who required intravitreal therapy at months 3 and 9, were more likely to present with the following features at 1 month OCT: intraretinal fluid (IRF), disorganization of inner retinal layers (DRIL), disorganization of outer retinal layers (DROL) and hyperreflective foci (HRF). No major safe-ty issues arose.
Conclusion: Topical therapy alone can be a valuable option for post-PPV CME in approximatively 50% of pa-tients. Significant visual acuity recovery and CMT reduction at 12 months, demonstrated DEX intravitreal implant can be a safe and effective second-line treatment for pseudophakic patients with post-PPV CME, refractory to medical therapy. The presence of specific OCT biomarkers may indicate a more severe CME that might benefit from the intravitreal therapy.
Keywords:
Postsurgical cystoid macular edema
; small-gauge pars plana vitrectomy
; dexamethasone intravitreal implant
; OCT biomarkers
; rhegmatogenous retinal detachment
; epiretinal membrane
1. Introduction
Postsurgical cystoid macular edema (PCME) is a pathologic condition where an inflammation-based damage to the intraretinal capillaries leads to the accumulation of serous fluid in the extracellular and intracellular spaces at the macula level. [1,2] PCME is considered the leading cause of reduced vision following both uneventful cataract and vitreoretinal surgery, with a reported incidence of 0.1–2.3% and between 10% and 47% respectively [2,3,4].
This condition usually develops 4 to12 weeks after surgery, with a peak incidence at 4-6 weeks postoperatively. Although the precise pathogenetic mechanism is still poorly understood, subclinical inflammation, induced by surgical trauma, is advocated as the major player in PCME development. The upregulation of inflammatory mediators like prostaglandins, cytokines, and other vasopermeability factors may lead to the blood-retinal barrier breakdown with permeabilization of perifoveal capillaries and intraretinal fluid accumulation consequently [2,5].
Several conditions have been recognized as potential risk factors for PCME onset. Systemic diseases like diabetes and hypertension, intraoperative complications, and preexisting ocular conditions, such as uveitis and diabetic retinopathy, seem to influence the development of the pathology [2,6,7].
PCME has a relatively benign natural history, with a peak incidence after 6 weeks and spontaneous resolution within 6 months in more than 50% of eyes. A prompt medical treatment, based on the use of steroidal and nonsteroidal anti-inflammatory (NSAIDs) topical medications, may be warrant in these patients though, at least to speed-up the resolution of retinal fluid and to promote a faster visual recovery [5]. Given the inflammatory nature of the condition, intravitreal steroids, including the sustained-release dexamethasone (DEX) intravitreal implant (Ozurdex®, Allergan Inc., Irvine, CA, USA, and Allergan Pharmaceuticals, Ireland), have been extensively used for the treatment of PCME, especially in those patients resistant to topical medications. Encouraging results have emerged from several clinical studies that included patients treated with intravitreal DEX for PCME, secondary to both cataract and vitreoretinal surgery [5,8,9,10,11].
Spectral domain optical coherence tomography (SD-OCT) is an essential diagnostic tool that enables the detection and the accurate quantification of even subtle changes occurring at the macula in eyes with PCME. High resolution OCT scans may provide key elements regarding the precise localization of retinal fluid and the integrity of specific foveal structures such as ellipsoid zone (EZ), external limiting membrane (ELM) and inner retinal layers. All these features are widely recognized as indicators of visual prognosis and response to a given treatment in several macular pathologies, namely diabetic macular edema (DME), exudative age-related macular degeneration (AMD), and macular edema secondary to retinal vein occlusion (RVO) [12,13,14,15,16].
Although many studies have focused on post-pars plana vitrectomy (PPV) CME, to the best of our knowledge very little evidence can be found in the Literature about the role of clinical characteristics and qualitative OCT features as potential biomarkers of response to DEX intravitreal implant in pseudophakic eyes that developed a PCME after small-gauge PPV [10].
The aim of the present study was to assess the incidence of PCME in pseuophakic patients undergoing small gauge PPV for different retinal pathologies. Twelve-months visual and anatomical outcomes, intravitreal DEX treatment exposure and safety, and correlations between demographic, clinical characteristics, OCT structural biomarkers and the need for dexamethasone intravitreal therapy were evaluated as-well.
2. Materials and Methods
In this retrospective, uncontrolled clinical study, medical and surgical records of pseudophakic patients undergoing small-gauge PPV for different retinal pathologies were reviewed. All surgeries were carried out at “S.S. Annunziata Hospital” Eye clinic in Taranto, Italy, between January 2021 and July 2023. The study adhered to the tenets of the Declaration of Helsinki and was approved by the local Institutional Review Board (IRB).
To be included, patients had to fulfill the following inclusion criteria: age of 18 years or older; presence of a regularly signed informed consent for the surgery; pseudophakic status at the time of PPV with a documented minimum period between the previous cataract surgery and the vitreoretinal procedure of 1 year; uncomplicated small-gauge PPV for the following reasons: rhegmatogenous retinal detachment (RRD), epiretinal membrane (ERM), lamellar macular holes (LMH), vitreous hemorrhage (VH) secondary to a posterior vitreous detachment (PVD); a minimum follow-up of 12 months; a comprehensive description of the surgical procedure; clinical data and macular SD-OCT scans (macular cube, radial and raster scans with a line crossing the fovea center) available at 1, 3, 6, 9 and 12 months after surgery and fluoresceine angiograms in those eyes that developed a central macular thickening during the postoperative period.
Patients with a history of exudative AMD, diabetic retinopathy (RD), RVO, uveitis, and uncontrolled glaucoma were excluded. In cases of incomplete clinical data and of poor-quality OCT scans, with a too low resolution to allow a reliable qualitative assessment of the macular condition, patients were excluded as-well.
2.1. Surgical Procedure
All surgeries were performed by a single, experienced vitreoretinal surgeon (F.P.), under peribulbar block (4cc Ropivacaine + 1 cc Lidocaine) or general anesthesia. After a proper disinfection of the surgical field with 5% povidone-iodine (Oftasteril, Alfa Intes Industria Terapeutica Splendore S.r.l., Naples, Italy), a three-ports 23 or 25-gauge (23-G; 25-G) PPV was carried out using the Constellation® Vision System (Alcon Laboratories, Fort Worth, TX). Silicone oil was aspirated from the vitreous chamber, then replaced with balanced salt solution (BSS) or air, after multiple fluid-air exchanges to wash out any emulsion, in eyes scheduled for removal of silicone oil. The core vitrectomy and peripheral shaving were performed with 7500 cuts per min (cpm) cut-rate and linear aspiration of 0–650 mmHg in all the other cases. Triamcinolone acetonide was systematically used for vitreous staining to ensure a better residual vitreous removal as-well-as to confirm the posterior hyaloid detachment. Perfluorcarbon liquid (PFCL) was used to drain the subretinal fluid and stabilize the posterior retina only in RRD cases. In the presence of a PVR complicating a RRD, peeling of epiretinal and subretinal membranes after staining with Trypan Blu (TB) 0.15% + Brilliant Blue G (BBG) 0.05% + Lutein 2%solution (DOUBLE DYNE; Alfa Intes Industria Terapeutica Splendore S.r.l., Naples, Italy), was attempted with vitreoretinal microforceps. Relaxing retinotomies and retinectomies where usually reserved to cases of RRD with severe PVR. Fluid-air exchange was performed to flatten the retina immediately after all the vitreous tractions have been removed. Endolaser retinopexy was applied to all the retinal breaks and along the borders of the retinotomies and retinectomies. Twenty-four % sulfur hexafluoride (SF6), 14% octafluoropropane (C3F8), or silicone oil (1000 centistokes, 5000 centistokes or heavy silicone oil) were alternatively used as endotamponade, according to the complexity of the cases.
After core vitrectomy, peripheral shaving and PVD induction, ERM and internal limiting membrane (ILM) were removed with end-grip vitreoretinal forceps, after staining with Trypan Blu (TB) 0.15% + Brilliant Blue G (BBG) 0.05% + Lutein 2% solution, in patients with idiopathic ERM and LMHs. After ERM + ILM removal, peripheral retinal was carefully evaluated under scleral depression in all cases, to rule-out the presence of peripheral retinal breaks and micro-holes requiring endolaser retinopexy. A partial fluid-air exchange was then caried out. Sclerotomies were systematically closed with 8.0 Vicryl sutures, to reduce the risk of early postoperative hypotony secondary to leaking wounds.
2.2. Definition and Diagnosis of Post-Surgical Macular Edema
Post-vitrectomy CME was defined by an increase in macular thickness of ≥ 10% of the previous OCT value and/or by the presence of more than three circular or ovoid intraretinal hyporeflective spaces in the inner and/or outer layers in the central millimeter of the Early Treatment Diabetic Retinopathy Study (ETDRS) grid and by the identification of subretinal fluid accumulation at the foveal location [4]. The diagnosis of post-surgical macular edema needed to be further supported by the evidence of late-phase macular and optic disc hyperfluorescence at postoperative fluoresceine angiography (Spectralis HRA + OCT; Heidelberg Engineering, Heidelberg, Germany).
2.3. Treatment of Post-Surgical Macular Edema
Medical therapy, consisting of a combination of topical steroids (preservative-free DEX eye drops 1 mg/ml, administered 4 times daily) plus topical NSAIDs (Bromfenac eye drops 0.9 mg/ml, twice daily), was used for at least one month, in all patients who developed a post-surgical macular edema.
DEX implant 0.7 mg, injected into the vitreous cavity starting from month 3, according to the standard protocol [17], was reserved to all cases that did not respond to the medical treatment or where CME tended to relapse after topical treatment discontinuation.
2.4. Analysis of the Biomarkers
Qualitative OCT assessment, carried out by two independent expert observers (A.N. and E.G.,) on OCT scans taken one month after surgery, led to the recognition of the following structural biomarkers: intraretinal cysts (IRC), defined by the presence of circular or ovoid intraretinal hyporeflective spaces in the inner and/or outer layers; subretinal fluid (SRF), indicating a subfoveal hyporeflective “cuff” of fluid beneath the neuroepithelium; disorganization of inner retinal layers (DRIL), defined by the complete loss of boundaries between the ganglion cell, inner plexiform, and outer nuclear plexiform layers at the foveal location; disorganization of outer retinal layers (DROL), featured by the complete loss of the EZ + ELM hyperreflective bands at the subfoveal location; hyperreflective foci (HRF), identified as dot-like lesions, less than 30 μm in size, with the same reflectivity of retinal nerve fiber layer.
Main outcomes evaluated were the incidence of PCME in pseudophakic eyes after small-gauge PPV, the change of baseline mean best corrected visual acuity (BCVA) and central macular thickness (CMT) at 12 months in the subset of patients who developed a form of post-vitrectomy CME and were treated consequently, and the safety of intravitreal DEX.
Secondary outcomes were the correlations between the exposure to intravitreal DEX during the FU and specific demographic, clinical and OCT characteristics.
2.5. Statistical Analysis
The qualitative variables are presented as frequencies and percentages, while the quantitative data is presented as means ± standard deviations. No formal sample size calculation was performed. For assessing the change in BCVA and CMT over follow-up, the non-parametric test known as the Wilcoxon rank-sum test was used. For frequencies and percentages, the Fisher test was used. All statistical tests were performed at the p < 0.05 significance level. Univariate and multivariate regression models were performed to assess the relationship between DEX-i at 3,6, and 9 months and each independent variable. The independent variables included gender, age, retinal disease, CMT and OCT biomarkers. The independent variables that were significant at univariate regression analysis were considered in multiple regression model. Statistical analysis was made using STATA 12.1 Statistical Software (StataCorp), 2014, release 12 (College Sta-tion, TX, USA).
3. Results
Medical records of 346 consecutive pseudophakic patients (352 eyes), who underwent small-gauge PPV for RRD (235 eyes), silicone oil removal (43 eyes), ERM (62 eyes) or non-diabetic VH (12 eyes), between January 2021 and July 2023, were identified. Gradable OCT scans, taken between the first and the second month after surgery, were available for all of them. Post-PPV CME, defined as a central foveal thickening with the evidence of intraretinal and/or subretinal fluid, in the absence of any epiretinal component, and further confirmed by the late-phase macular and optic disc hyperfluorescence at fluoresceine angiography, developed in 54 patients (incidence: 15,3 %) within the first two months after surgery.
Of these 54 patients (54 eyes), 6 were excluded for the following reasons: the follow up was shorter than 6 months in 4 eyes and some relevant clinical data were missing in the remaining 2 eyes.
Ultimately, 48 eyes (21 right/27 left) of 48 consecutive patients (15 women and 33 men; mean age 64,1 year ± 4,3, range 57-73) were deemed eligible for the final analysis. Indication for PPV in this population were RRD repair in 36 eyes (75%), 1000 centistokes silicon oil removal in 10 eyes (20.8%) and ERM peeling in 2 eyes (4.1%). Considering only the subgroup of patients who underwent vitreoretinal surgery for RRD repair, the macula was detached in 31 eyes (86,1%), proliferative vitreoretinopathy (PVR) was evident in 14 eyes (38.8%) and a mild VH, that did not impair a proper OCT evaluation of the macula during the preoperative period, was present in the remaining 2 eyes (5.5%).
The mean time (± SD; range) between the previous cataract surgery and the vitreoretinal procedure was 3,8 years (± 2,3; range 1–11) in the study population. A comprehensive clinical assessment, together with reliable OCT scans, were available at 1, 3, 6, 9 and 12 months for all of them.
Additional relevant Demographic and baseline characteristics are listed in Table 1.
Preoperative mean BCVA (1.44 ± 0.99 LogMAR) significantly improved at 1 (0,56 ± 0,40 LogMAR), 3 (0.44 ± 0.48 LogMAR), 6 (0.37 ± 0.35 LogMAR), 9 (0.38 ± 0.39 LogMAR) and 12 months (0.32 ± 0.37 LogMAR) in the overall population (P< 0.001 for all the time points). Table 2.
Mean (± SD) CMT was 347 (± 123.5) μm at one month after PPV and it significantly decreased to 290 μm (± 80.4) at last visit. Mean CMT changes at all time points are reported in Table 3.
Qualitative analysis of the OCT at month one disclosed the presence of intraretinal fluid in 34 eyes and of subretinal fluid in 14 eyes. Additionally, the disorganization of inner and outer retinal layers (ellipsoid zone + external limiting membrane) at the foveal location and the presence of HRF were evident in 11 (23 %), 10 (20.8%) and 9 (18.7%) eyes respectively. The complete analysis of the OCT biomarkers at month one is reported in Table 4.
3.1. Treatment Exposure
All patients were treated with topical therapy (DEX eye drops 4 times daily + FANS eye drops 3 times/daily for one month) as first-line treatment. Intravitreal DEX could be administered starting from month 3, only in cases of non-resolving (CMT reduction < 10% of the baseline value with persistence of intraretinal or subretinal fluid), worsened (CMT increase > 10% of the baseline value with the presence of intraretinal or subretinal fluid) or relapsing (CMT increase > 10% when compared to the OCT of the previous evaluation and/or evidence of new subretinal fluid and intraretinal cysts) macular edema.
CME completely regressed after one month of topical medications in 23 eyes (47.9%), without any evidence of recurrence along the entire course of the follow up. The remaining 25 eyes (52%) required one or more intravitreal DEX implant at some point during the follow up, for persistence or recurrence of macular edema.
Intravitreal DEX was administered at 3,6,9 and 12 months in 16 (33.3%), 5 (10.4%), 16 (33.3%) and 4 (8.3%) eyes respectively. Each patient treated with intravitreal DEX received a mean number of 1.64 (± 0.56; range: 1-3) injections between month 3 and 12. More specifically, 10 patients (40%) received a single dexamethasone intravitreal injection, 14 patients (56%) received 2 injections, while one patient (4%) was treated with 3 injections. Table 5
The mean interval between two consecutive injections was 5.2 (± 1.37; range: 3- 6) months in those patients who required more than one administration.
3.2. Analysis of the Correlations
The correlation analysis, between the mean CMT values taken at different time points, revealed the existence of a statistically significant correlation between mean CMT at month 1 and month 3 (P < 0.001). Additionally, both mean CMT at month 3 and 6 significantly correlated with mean CMT at months 9 and 12 (P < 0.001), while mean CMT at month 9 significantly correlated with mean CMT at last visit (month 12; P < 0.001) Table 6.
A univariate analysis using a logistic regression model was performed to look at potential correlations between the need for intravitreal DEX at month 3 and specific demographic, clinical characteristics, and predefined structural OCT biomarkers. The indication to start a treatment with intravitreal DEX at month 3 significantly correlated with the mean CMT (p = 0.005), the presence of intraretinal cysts (P = 0.04), DRIL (P = 0.004) and HRF (P = 0.02) at 1 month OCT scans.
When the same univariate logistic regression model was tested with treatment (intravitreal DEX) at month 6, no statistically significant correlations could be found. None of the tested variables appeared to be significantly correlated with the exposure to intravitreal dexamethasone at month 3, in the multivariate logistic regression model.
When the probability of receiving an intravitreal DEX treatment at month 9 was tested for different clinical and OCT variables, a statistically significant correlation with HRF and DROL emerged both in the univariate (HRF: OR = 5.80, P = 0.02; DROL: OR = 7.51, P = 0.01) and multivariate (HRF: OR = 5.53, P = 0.04; DROL: OR = 7.11, P = 0.03) logistic regression models. The results of univariate and multivariate analysis are reported in Table 7.
3.3. Safety
No severe ocular and non-ocular adverse events were reported for patients who underwent one or more intravitreal DEX administrations. Baseline mean (± SD) intraocular pressure (15.6±3.9 mmHg) at month one did not change significantly during the entire course of the follow-up (Table 8). Five patients (20%) presented with a mild IOP elevation (> 25 mmHg) at month 6 (3 patients) and 12 (2 patients) that was successfully managed with topical IOP lowering medications. No patients developed glaucoma or required filtering surgery for a chronic, refractory IOP elevation.
4. Discussion
Limited information is available about the incidence of CME after vitrectomy or phacovitrectomy. Leisser et al. analyzed data from 6 studies and showed that the incidence of new intraretinal fluid, detected 3 months after surgery, was 6% and 3% after phacovitrectomy and vitrectomy alone respectively [18,19].
The incidence of post-PPV CME in pseudophakic patients was 15.3% in our study. This data seems to be in line with those reported in the Literature. The rate of post-PPV CME may vary significantly according to the underling pathology that led to the surgery or to the surgical procedure itself (vitrectomy vs phacovitrectomy). The prevalence of CME was 17.1% in pseudophakic eyes scheduled for PPV for RRD [4]. A macular thickness increase has been reported in 3.8% to 15.4% of patients undergoing PPV + peeling and phacovitrectomy + peeling for ERM respectively [19], while no significant differences were observed, in terms of post-PPV CME occurrence rate, between only vitrectomy group and phacovitrectomy group in patients with idiopathic ERM, in similar reports [20,21].
Cataract surgery is a well-known risk factor for Irvine-Gass syndrome. Surgical manipulation in the anterior segment may promote an upregulation of inflammatory mediators, which leads to a breakdown of the blood-retinal barrier and increased vascular permeability. Beside the inflammatory response to the surgery, an anterior uveal remodeling, consequent to the crystalline lens removal and its replacement with a thinner and lighter IOL, was hypnotized as a concurrent factor for postsurgical CME in some eyes [19].
Taken together, these data suggest cataract surgery may act as a relevant stand-alone risk factor for postsurgical CME, therefore a potential source of bias when assessing the true incidence of post-PPV CME [20].
All patients included in the present study were psudophakic at the time of PPV, with a minimum time between the previous cataract surgery and the vitreoretinal procedure, as short as one year. The exclusion of phakic eyes scheduled for a phacovitrectomy procedure, may have reduced the chance of overrating the true incidence of post-surgical CME.
The exact pathogenetic mechanism responsible for CME occurring after PPV is still poorly understood. Many studies have tried to identify possible risk factors for its occurrence. Age more than 50 years, multiple surgeries, severe PVR, aphakia, endotamponade used and extensive endolaser or cryopexy have been all proposed as risk factors for post-PPV CME in eyes undergoing PPV for RRD repair [22,23,24].
Intraretinal microcystoid changes have been observed after PPV combined with epiretinal membrane and ILM peeling in patients with idiopathic ERMs, especially in those cases whit pre-existing intraretinal cysts[20], stage 4 ERMs and candidate for a phacovitrectomy procedure [3].
It has been proposed that the degree of retinal architectural disruption, found in end-stage ERMs, may make the retinal tissue more prone to the mechanical stress induced by ILM peeling maneuvers. This may cause a Muller cell disfunction, secondary to a retrograde trans-synaptic degeneration of inner retinal layers and to an inflammatory process, with a consequent impairment in fluid resorption at the macula. According to this theory, CME observed after ILM peeling for ERMs may derive more from glial degeneration rather than a true blood-retinal barrier disfunction [3,25,26].
The reported incidence of CME after silicone oil endotmaponede ranges between 13.6% to 36%, depending on several factors such as SO viscosity, the grade of PVR complicating the retinal detachment and the interval between PPV and SO removal. Both inflammatory and mechanical components have been postulated as predisposing factors for CME formation in SO filled eyes. SO can promote an inflammatory reaction by impairing the potassium ion buffering function of Muller cells. The adhesive interaction between the SO bubble and the retinal surface may translate into tractional forces to the macula which may promote intraretinal fluid accumulation. CME spontaneous resolution observed after SO removal in most eyes, indicates this process may be reversed with the removal of the endotamponede. There is still a small number of patients though, who do not experience an improvement of their macular condition after SO removal, and who can even progress toward a further macular thickening. This indicates that the pro-inflammatory stimulus may persist for some time, even after the elimination of the SO [22].
Taken all together, these data suggest, regardless the initial retinal condition treated with PPV, many risk factors can contribute to increase intraocular inflammation [4].
Patients who underwent PPV for RRD repair (36) represented most of our study population (75%), followed by patients scheduled for silicone oil removal (10 eyes, 20.8%) and idiopathic ERM peeling (2 eyes, 4.1%). Considering the relatively low number of patients included, especially in the ERM peeling group, and the heterogeneity of the retinal pathologies, we did not look at potential risk factors for post-PPV CME. Additionally, the present study was designed to assess the role of different treatment modalities for post-PPV CME, rather than to identify risk factors for this condition.
A low-grade inflammatory response can be considered the leading event that promotes retinal fluid accumulation in eyes that develop a form of post-vitrectomy CME. Inflammatory mediators released during surgery may easily spread in the vitreous chamber, causing a blood-retinal barrier breakdown and extravasation of fluid from retinal vessels, as confirmed by the late leakage and staining of the optic nerve head and the macula, observed at the fluoresceine angiography in these patients [2,3]. Fluoresceine angiography is routinely performed in patients who develop any sort of acute macular change, presumably related to inflammation or retinal vascular impairment, after a surgical procedure, at our institution. All eyes included in the study displayed a peculiar pattern at FA, namely a late phase hyperfluorescence at the macula and optic disc, indicating an inflammatory mechanism responsible for CME. Retinal glial disfunction, induced by the surgical trauma and again by the inflammation, may concurrently promote the collection of fluid in the macula of these patients [3,25,27].
The paramount role of inflammation can be inferred by the satisfactory response to a given anti-inflammatory therapy in these patients [22].
Medical treatment, based on the administration of topical steroids and NSAIDs eyedrops, is generally considered a safe and effective option in patients with PCME. The good ocular penetration, combined with a low rate of adverse events, make topical therapy a fairly good first line option in these cases [5]. Patients who fail to respond to medical treatment, and cases where CME tends to relapse as soon as the topical medication is discontinued, may benefit from more invasive treatments like intravitreal steroids [28,29] or anti-VEGF [30].
Intravitreal DEX implant is a biodegradable corticosteroid implant, which provides sustained release of 700 μg DEX into the vitreous for up to 6 months [9]. Results from different clinical studies showed intravitreal DEX implant can promote a significative long-term CMT reduction and a visual acuity improvement in vitrectomized eyes that develop PCME after RRD surgery and ERM peeling, both in naïve and refractory to medical therapy eyes [8,9,11,31].
Twenty-five eyes (52%) did not show a satisfactory response to the medical therapy in our study, so they were candidate for intravitreal DEX implant starting from month 3. BCVA improvement, together with a significative CMT reduction, indicated intravitreal therapy is effective in promoting macular fluid resolution and visual recovery in this population.
While CME resolution was achieved after a single injection in 10 patients (40%), the remaining 15 patients required two or more injections by the end of the 12-months FU, with a mean number of 1.64 treatment per patient and a mean interval between two consecutive injections of 5.2 months. The maximum mean CMT reduction was reported at month 6, 3 months after the injection, with a recurrence of macular edema at month 9 in 10 patients (62.5 % of the population that received the first injection at month 3).
This observation seems in line with similar reports in the Literature [10,32]. The maximum effect of intravitreal DEX is usually observed one month from the administration, with a progressive loss of the effect over the next period. This can explain why approximatively 44% of patients need further dexamethasone injections after a mean period of 6 months [9,32].
The role of OCT structural biomarkers in several macular pathologies has grown in popularity over the past few years. High resolution OCT scans enable the identification of even subtle anatomical changes in different retinal layers at the macula. These structural elements may correlate with the visual function and predict the response to a treatment. The presence of subretinal fluid and of HRF were shown to be predictive of a better anatomical and functional response to intravitreal DEX in DME [33,34,35]. The detection of MAs in the nasal macula may indicate resistance to anti-VEGF therapy in patients with DME [36].
Very little evidence on the role of clinical and structural biomarkers as indicators of response to intravitreal DEX, in patients with post-PPV CME, can be found in the Literature. Fressinger et al. investigated the efficacy of intravitreal DEX in eyes that developed CME after PPV for ERM or macula-on RD and tried to identify functional and morphological OCT predictors of response. Their results indicated the presence of SRF, the integrity of EZ and a worse baseline BCVA were all predictive of a better functional outcome after intravitreal DEX [10].
The existence of potential correlations between mean CMT values, measured at different time points, and between the intravitreal DEX treatment exposure and specific demographic, clinical characteristics, and predefined structural OCT biomarkers, were investigated in our study.
Mean CMT at month 1 significantly correlated with mean CMT at month 3, while CMT values at month 3 and 6, both correlated with mean CMT at month 9 and 12. These correlations suggest most of the patients who displayed a more pronounced central macular thickening at first month, still have a clinically significant macular edema at month 3, despite the medical therapy. Additionally, the correlations between the mean CMT at month 3 and 6 with that measured at month 9 and 12, may suggest CME tend to relapse approximatively 6 months after the dexamethasone injection.
The univariate logistic regression model revealed that the indication for treatment with intravitreal DEX at month 3, significantly correlated with the mean CMT at month 1 and with the existence of intraretinal fluid, DRIL and HRF at 1 month OCT. The need for a second DEX intravitreal injection at month 9 was significantly correlated with the presence of HRF and DROL at the OCT both in the univariate and multivariate linear regression models. Presence of HRF and DROL at the OCT, indicates an 8 and 6-folds increase respectively of the chance to be treated with an additional intravitreal DEX injection, 9 months after surgery, for CME recurrence.
A greater CMT at month 1 is suggestive of a more severe macular edema, that may not resolve completely after medical therapy. Patients who presented with a thicker macula 1 month after vitrectomy, will eventually continue to display persistent fluid at month 3, thus requiring intravitreal treatment.
HRF, considered aggregated of activated microglia cells, located in both inner and outer retina in patients with macular edema secondary to different retinal etiologies [33], are known to be associated with increased inflammation in the retina [35,37,38].
Conflicting evidence, on the role of HRF as biomarkers of response to intravitreal steroids for diabetic macular edema, still exists to date.
Some authors demonstrated that the presence of HRF is associated with an excellent response to intravitreal steroids [35], while other reports showed baseline numbers of HRF on SD-OCT may be a predictive indicator of early recurrence of macular edema after intravitreal DEX implantation for DME [39].
Accepting the letter evidence, a higher baseline number of HRF may indicate a more severe retinal inflammation with a more pronounced macular edema, maybe resistant to topical therapy. This hypothesis could explain why patients, who presented with a higher number of HRF at baseline, did require intravitreal therapy more frequently, in our study.
It is worth to note that our assumption is purely speculative, since no precise evidence of the impact of HRF on the response intravitreal steroid treatment, in patients with post vitrectomy macular edema, can be found into the Literature to date.
The role that IRF, DRILS and DROL may play in defining the response to intravitreal steroids in these patients is less clear, with no conclusive evidence that can be derived from the Literature.
We hypnotized that the presence of intraretinal cysts, DRIL and DROL at baseline may be suggestive of a more severe macular edema, with a higher degree of intraretinal degeneration. In a recent report the odds of having DRIL was greater in DME eyes with an increased retinal thickness at the fovea [40]. The presence of large cystoid spaces in the inner retinal layers may also contribute to generate distortion into the retina, thus opening the way to DRIL. Conversely, the absence of DRIL was significantly correlated with the presence of SRF, which is known to be more commonly seen in acute DME [41]. This might indicate DRIL as a sign of chronicity of macular edema.
Taken together, these observations may support the hypothesis that eyes with post-vitrectomy CME, associated with the presence of IRF, DRIL and DROL at the OCT, may be affected by a more severe condition that requires a more aggressive treatment, rather than a topical therapy alone.
When a multivariate logistic regression model was carried out, none of the tested variables correlated with the exposure to the intravitreal treatment at month 3. The disagreement between the two models could be explained, at least in part, by the relative reduced number of cases included in our study.
Repeated treatments with intravitreal DEX over a prolonged period, may generate some safety concerns, especially when we come to the risk of uncontrolled IOP elevation. IOP rise >25 mm Hg has been reported in approximatively 26% of patients treated with DEX for different retinal conditions. Overall, more than 90% of eyes with IOP elevation can be successfully managed with medical therapy, with only 0.5% eyes required filtering surgery [42].
An IOP increase > 25 mmHg was evident in 20% of patients in our study and it was managed medically in all cases. No cases of severe ocular adverse events like endophthalmitis, retinal detachment or vitreous hemorrhage were reported.
The relatively small sample size, the retrospective nature, the lack of a control group and the heterogeneity of the retinal pathologies that required surgery, represent the major limitations of the present study. Additionally, correlations between clinical, OCT biomarkers and visual function were not investigated. This is mainly due to the fact we feel that, at least some degree of inner and outer retinal disruption (DRIL and DROL) observed in some patients, may be related to the preexisting retinal pathology, rather than to the post-vitrectomy CME.
To the best of our knowledge, this is the first study where the role of specific OCT biomarkers, such as DRIL, IRF, DROL and HRF, as predictors of exposure to DEX intravitreal treatment in pseudophakic eyes that developed CME after a vitreoretinal procedure, was investigated.
The strict inclusion criteria (only pseudophakic patients could be enrolled), the long follow-up, the availability of comprehensive clinical and OCT data for all the enrolled patients, and the use of fluoresceine angiography to confirm the diagnosis of post-surgical CME, further increase the reliability of our results.
In conclusion, approximatively 50% of pseudophakic patients, who develop a CME after vitreoretinal surgery, may benefit from topical therapy alone. Intravitreal DEX implant seems to warrant a sustained CMT reduction and a VA recovery in patients who show an incomplete response to topical medications after 2 months from the diagnosis. The identification of specific biomarkers at the OCT performed one month after surgery, may indicate a more severe CME, and could help the clinician to stratify those patients who will probably require an intravitreal approach in the next future.
Figure 1.
Post-vitrectomy macular edema after surgery for rhegmatogenous retinal detachment (RRD) in the right eye of a 65-year-old lady. Early (A) and late (B) phase fluoresceine angiography, performed one month after surgery, show the classical perifoveal petaloid staining pattern and late leakage of the optic disc. A significant central macular thickening (CMT; 633 μm), associated to the presence of intraretinal cysts (arrows) and subretinal fluid (star), can be observed at 1-month spectral domain optical coherence tomography (SD OCT). Best corrected visual acuity (BCVA) was 20/200 in this eye (C-D). SD-OCT scans taken at month 3 (E-F), reveal a complete intraretinal and subretinal fluid resolution, with a CMT of 205 μm, and a BCVA of 20/30, after topical therapy.
Figure 1.
Post-vitrectomy macular edema after surgery for rhegmatogenous retinal detachment (RRD) in the right eye of a 65-year-old lady. Early (A) and late (B) phase fluoresceine angiography, performed one month after surgery, show the classical perifoveal petaloid staining pattern and late leakage of the optic disc. A significant central macular thickening (CMT; 633 μm), associated to the presence of intraretinal cysts (arrows) and subretinal fluid (star), can be observed at 1-month spectral domain optical coherence tomography (SD OCT). Best corrected visual acuity (BCVA) was 20/200 in this eye (C-D). SD-OCT scans taken at month 3 (E-F), reveal a complete intraretinal and subretinal fluid resolution, with a CMT of 205 μm, and a BCVA of 20/30, after topical therapy.
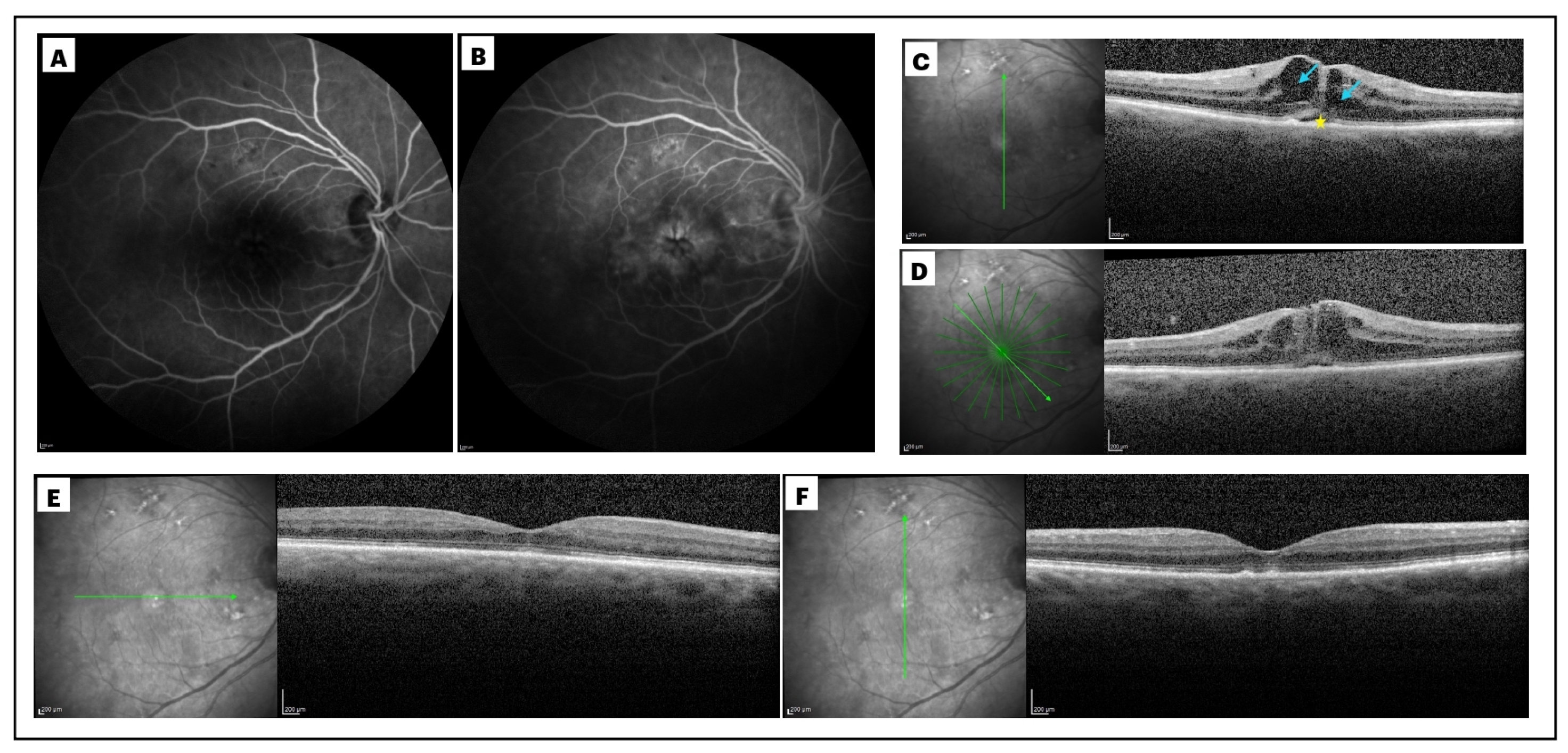
Figure 2.
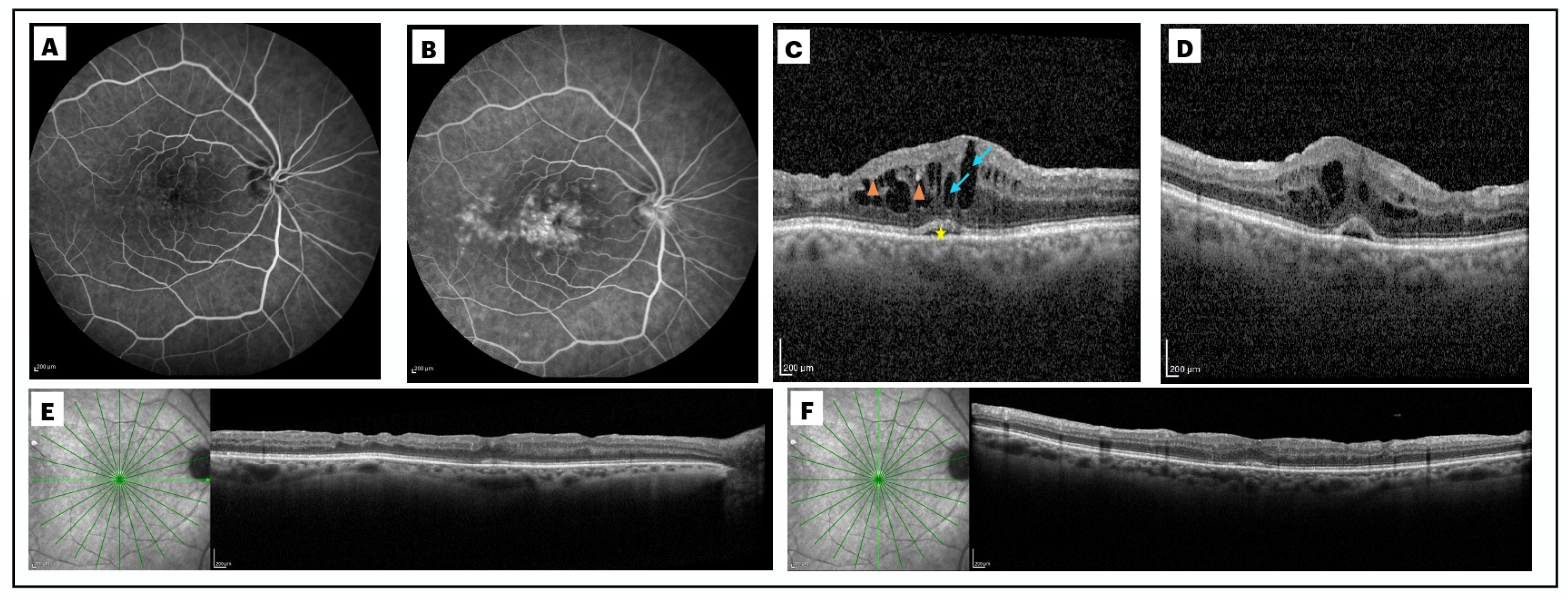
Right eye of a 73-year-old male patient who developed macular edema one month after a pars plana vitrectomy with epiretinal membrane (ERM) peeling. The extensive late-phase macular leakage, with a petaloid patter, and the hyperfluorescence of the optic disc, were evident at the late frames of the fluoresceine angiography performed 1 month after surgery (B), when compared to the early phase of the exam (A). Spectral domain optical coherence tomography (SD OCT) at month 1 (C), revealed a post-vitrectomy macular edema with a central macular thickness (CMT) of 576 μm and presence of large intraretinal cysts (arrow), sub retinal fluid at the fovea (star) and hypereflective foci (HRF, arrowheads). The condition showed a very negligible improvement at month 3 (CMT: 556 μm), after 2 months of topical therapy, with the persistence of sub retinal fluid and only a slight reduction of intraretinal cysts (D). Best corrected visual acuity (BCVA) was 20/400 at this point. This patient was treated with a dexamethasone (DEX) intravitreal implant at month 3. SD-OCT performed at month 6, 3 months after intravitreal DEX administration, shows a significant CMT reduction (289 μm), with a complete resolution of intraretinal and sub retinal fluid (final BCVA of 20/50).
Figure 2.
Right eye of a 73-year-old male patient who developed macular edema one month after a pars plana vitrectomy with epiretinal membrane (ERM) peeling. The extensive late-phase macular leakage, with a petaloid patter, and the hyperfluorescence of the optic disc, were evident at the late frames of the fluoresceine angiography performed 1 month after surgery (B), when compared to the early phase of the exam (A). Spectral domain optical coherence tomography (SD OCT) at month 1 (C), revealed a post-vitrectomy macular edema with a central macular thickness (CMT) of 576 μm and presence of large intraretinal cysts (arrow), sub retinal fluid at the fovea (star) and hypereflective foci (HRF, arrowheads). The condition showed a very negligible improvement at month 3 (CMT: 556 μm), after 2 months of topical therapy, with the persistence of sub retinal fluid and only a slight reduction of intraretinal cysts (D). Best corrected visual acuity (BCVA) was 20/400 at this point. This patient was treated with a dexamethasone (DEX) intravitreal implant at month 3. SD-OCT performed at month 6, 3 months after intravitreal DEX administration, shows a significant CMT reduction (289 μm), with a complete resolution of intraretinal and sub retinal fluid (final BCVA of 20/50).
Author Contributions
Conceptualization, F.P, E.G.; methodology, G.B.; software A.N., P.V.; validation F.B. C.I. G.A; formal analysis, F.P., e.g., G.B; investigation, F.P., A.N., G.A.; data curation, A.N., G.B., P.V., G.M.E.C.; writing—original draft preparation, F.P., A.N.; writing—review and editing, E.G .,G.B, M.O.G.; visualization, X.X.; supervision, F.B., C.I., G.A.; project administration F.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board as well as the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board (Eye Clinic of “SS. Annunziata” Hospital, Taranto, Italy) approved the study.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All raw data available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Romano, V.; Angi, M.; Scotti, F.; Del Grosso, R.; Romano, D.; Semeraro, F.; Vinciguerra, P.; Costagliola, C.; Romano, M.R. Inflammation and Macular Oedema after Pars Plana Vitrectomy. Mediators of Inflammation 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zur, D.; Loewenstein, A. Postsurgical Cystoid Macular Edema. In Developments in Ophthalmology; Coscas, G., Loewenstein, A., Cunha-Vaz, J., Soubrane, G., Eds.; S. Karger AG, 2017; Vol. 58, pp. 178–190 ISBN 978-3-318-06032-4.
- Iuliano, L.; Cisa Di Gresy, G.; Fogliato, G.; Corbelli, E.; Bandello, F.; Codenotti, M. Increased Risk of Postsurgical Macular Edema in High Stage Idiopathic Epiretinal Membranes. Eye and Vis 2021, 8, 29. [Google Scholar] [CrossRef]
- Bernabei, F.; Marcireau, I.; Frongia, F.; Azan, F.; Vagge, A.; Peiretti, E.; Guerrier, G.; Rothschild, P.-R. Risk Factors of Cystoid Macular Edema After Pars Plana Vitrectomy for Pseudophakic Retinal Detachment. Ophthalmol Ther 2023, 12, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Bellocq, D.; Korobelnik, J.-F.; Burillon, C.; Voirin, N.; Dot, C.; Souied, E.; Conrath, J.; Milazzo, S.; Massin, P.; Baillif, S.; et al. Effectiveness and Safety of Dexamethasone Implants for Post-Surgical Macular Oedema Including Irvine-Gass Syndrome: The EPISODIC Study. Br J Ophthalmol 2015, 99, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.J.; Johnston, R.L.; Buscombe, C.; Sallam, A.B.; Mohamed, Q.; Yang, Y.C. Risk Factors and Incidence of Macular Edema after Cataract Surgery. Ophthalmology 2016, 123, 316–323. [Google Scholar] [CrossRef]
- Yao, H.; Yang, Z.; Cheng, Y.; Shen, X. Macular Changes Following Cataract Surgery in Eyes with Early Diabetic Retinopathy: An OCT and OCT Angiography Study. Front. Med. 2023, 10, 1290599. [Google Scholar] [CrossRef] [PubMed]
- Parisi, G.; Fallico, M.; Avitabile, T.; Longo, A.; Ortisi, E.; Russo, A.; Petrillo, F.; Maugeri, A.; Barchitta, M.; Bonfiglio, V.; et al. Intravitreal Dexamethasone Implant for Postoperative Macular Oedema Secondary to Vitrectomy for Epiretinal Membrane and Retinal Detachment: A Systematic Review and Meta-Analysis. Journal of Ophthalmology 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Chatziralli, I.; Dimitriou, E.; Theodossiadis, G.; Chatzirallis, A.; Kazantzis, D.; Theodossiadis, P. Treatment of Macular Edema after Pars Plana Vitrectomy for Idiopathic Epiretinal Membrane Using Intravitreal Dexamethasone Implant: Long-Term Outcomes. Ophthalmologica 2019, 242, 16–21. [Google Scholar] [CrossRef]
- Freissinger, S.; Vounotrypidis, E.; Wolf, A.; Kortuem, K.U.; Shajari, M.; Sakkias, F.; Herold, T.; Priglinger, S.G.; Mayer, W.J. Evaluation of Functional Outcomes and OCT-Biomarkers after Intravitreal Dexamethasone Implant for Postoperative Cystoid Macular Edema in Vitrectomized Eyes. Journal of Ophthalmology 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Pignatelli, F.; Nacucchi, A.; Niro, A.; Gigliola, S.; Passidomo, F.; Donghia, R.; Addabbo, G. Intravitreal Dexamethasone Implant at the Time of Silicone Oil Removal to Treat Persistent Macular Edema after Rhegmatogenous Retinal Detachment Repair. JCM 2023, 12, 1697. [Google Scholar] [CrossRef]
- Markan, A.; Agarwal, A.; Arora, A.; Bazgain, K.; Rana, V.; Gupta, V. Novel Imaging Biomarkers in Diabetic Retinopathy and Diabetic Macular Edema. Ophthalmol Eye Dis 2020, 12, 251584142095051. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, E.; Giannini, D.; De Geronimo, D.; Fragiotta, S.; Varano, M.; Parravano, M. Prognostic Imaging Biomarkers in Diabetic Macular Edema Eyes Treated with Intravitreal Dexamethasone Implant. JCM 2023, 12, 1303. [Google Scholar] [CrossRef]
- Visioli, G.; Alisi, L.; Mastrogiuseppe, E.; Albanese, G.M.; Romano, E.; Iannetti, L.; Armentano, M.; Giovannetti, F.; Gharbiya, M. OCT Biomarkers as Predictors of Visual Improvement in Diabetic Macular Edema Eyes Receiving Dexamethasone Implants. Int J Retin Vitr 2023, 9, 35. [Google Scholar] [CrossRef]
- Metrangolo, C.; Donati, S.; Mazzola, M.; Fontanel, L.; Messina, W.; D’alterio, G.; Rubino, M.; Radice, P.; Premi, E.; Azzolini, C. OCT Biomarkers in Neovascular Age-Related Macular Degeneration: A Narrative Review. Journal of Ophthalmology 2021, 2021, 1–16. [Google Scholar] [CrossRef]
- Castro-Navarro, V.; Monferrer-Adsuara, C.; Navarro-Palop, C.; Montero-Hernández, J.; Cervera-Taulet, E. Optical Coherence Tomography Biomarkers in Patients with Macular Edema Secondary to Retinal Vein Occlusion Treated with Dexamethasone Implant. BMC Ophthalmol 2022, 22, 191. [Google Scholar] [CrossRef] [PubMed]
- Guigou, S.; Pommier, S.; Meyer, F.; Hajjar, C.; Merite, P.Y.; Parrat, E.; Rouhette, H.; Rebollo, O.; Matonti, F. Efficacy and Safety of Intravitreal Dexamethasone Implant in Patients with Diabetic Macular Edema. Ophthalmologica 2015, 233, 169–175. [Google Scholar] [CrossRef]
- Leisser, C.; Hirnschall, N.; Findl, O. Effect of Phacoemulsification on Outcomes after Vitrectomy with Membrane Peeling Regarding New Intraretinal Cystoid Changes and Transient Macular Edema. Ophthalmologica 2021, 244, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Kim, H.K.; Zaidi, M.H.; Byon, I.S.; Lee, J.E.; Nguyen, Q.D. Cystoid Macular Edema after Vitrectomy and after Phacovitrectomy for Epiretinal Membrane. Canadian Journal of Ophthalmology 2024, 59, e596–e602. [Google Scholar] [CrossRef]
- Leisser, C.; Hirnschall, N.; Hackl, C.; Döller, B.; Varsits, R.; Ullrich, M.; Kefer, K.; Karl, R.; Findl, O. Risk Factors for Postoperative Intraretinal Cystoid Changes after Peeling of Idiopathic Epiretinal Membranes among Patients Randomized for Balanced Salt Solution and Air-tamponade. Acta Ophthalmologica 2018, 96. [Google Scholar] [CrossRef]
- Frisina, R.; Pinackatt, S.J.; Sartore, M.; Monfardini, A.; Baldi, A.; Cesana, B.M.; Semeraro, F.; Bratu, A.; Parolini, B. Cystoid Macular Edema after Pars Plana Vitrectomy for Idiopathic Epiretinal Membrane. Graefes Arch Clin Exp Ophthalmol 2015, 253, 47–56. [Google Scholar] [CrossRef]
- Kontou, E.P.; Karakosta, C.; Kounas, K.; Iatropoulos, I.; Tsinopoulos, I.; Kozombolis, V.; Stavrakas, P. Macular Edema Following Silicone Oil Tamponade for Retinal Detachment: A Literature Review. Cureus 2023. [Google Scholar] [CrossRef] [PubMed]
- Merad, M.; Vérité, F.; Baudin, F.; Ghezala, I.B.; Meillon, C.; Bron, A.M.; Arnould, L.; Eid, P.; Creuzot-Garcher, C.; Gabrielle, P.-H. Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes. JCM 2022, 11, 4914. [Google Scholar] [CrossRef]
- Pole, C.; Chehaibou, I.; Govetto, A.; Garrity, S.; Schwartz, S.D.; Hubschman, J.-P. Macular Edema after Rhegmatogenous Retinal Detachment Repair: Risk Factors, OCT Analysis, and Treatment Responses. Int J Retin Vitr 2021, 7, 9. [Google Scholar] [CrossRef]
- Govetto, A.; Su, D.; Farajzadeh, M.; Megerdichian, A.; Platner, E.; Ducournau, Y.; Virgili, G.; Hubschman, J.P. Microcystoid Macular Changes in Association With Idiopathic Epiretinal Membranes in Eyes With and Without Glaucoma: Clinical Insights. American Journal of Ophthalmology 2017, 181, 156–165. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Post, M.; Brambati, M.; Rabiolo, A.; Pignatelli, F.; Szaflik, J.P.; Bandello, F.; Coppola, M. ASSOCIATED FACTORS AND SURGICAL OUTCOMES OF MICROCYSTOID MACULAR EDEMA AND CONE BOUQUET ABNORMALITIES IN EYES WITH EPIRETINAL MEMBRANE. Retina 2022, 42, 1455–1464. [Google Scholar] [CrossRef]
- Burggraaff, M.C.; Trieu, J.; De Vries-Knoppert, W.A.E.J.; Balk, L.; Petzold, A. The Clinical Spectrum of Microcystic Macular Edema. Invest. Ophthalmol. Vis. Sci. 2014, 55, 952. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, N.; Massin, P.; Haouchine, B.; Audren, F.; Tadayoni, R.; Gaudric, A. Intravitreal Triamcinolone for Refractory Pseudophakic Macular Edema. American Journal of Ophthalmology 2003, 135, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.A.; Haller, J.A.; Kuppermann, B.D.; Blumenkranz, M.S.; Weinberg, D.V.; Chou, C.; Whitcup, S.M. Dexamethasone Posterior-Segment Drug Delivery System in the Treatment of Macular Edema Resulting from Uveitis or Irvine-Gass Syndrome. American Journal of Ophthalmology 2009, 147, 1048–1054.e2. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Russo, V.; Prascina, F.; Noci, N.D. SHORT-TERM SAFETY AND EFFICACY OF INTRAVITREAL BEVACIZUMAB FOR PSEUDOPHAKIC CYSTOID MACULAR EDEMA. Retina 2009, 29, 33–37. [Google Scholar] [CrossRef]
- Fallico, M.; Maugeri, A.; Romano, G.L.; Bucolo, C.; Longo, A.; Bonfiglio, V.; Russo, A.; Avitabile, T.; Barchitta, M.; Agodi, A.; et al. Epiretinal Membrane Vitrectomy With and Without Intraoperative Intravitreal Dexamethasone Implant: A Systematic Review With Meta-Analysis. Front. Pharmacol. 2021, 12, 635101. [Google Scholar] [CrossRef]
- Pignatelli, F.; Niro, A.; Fallico, M.; Passidomo, F.; Gigliola, S.; Nacucchi, A.; Bonfiglio, V.; Reibaldi, M.; Addabbo, G.; Avitabile, T. Mid-Term Safety and Effectiveness of Macular Peeling One Month after Intravitreal Dexamethasone Implant for Tractional Diabetic Macular Edema. Sci Rep 2023, 13, 5990. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Xiao, S.; Zhang, W.; Li, J.; Yang, M.; Zhang, Y.; Gu, X.; Yang, L. Comparison of Hyperreflective Foci in Macular Edema Secondary to Multiple Etiologies with Spectral-Domain Optical Coherence Tomography: An Observational Study. BMC Ophthalmol 2022, 22, 352. [Google Scholar] [CrossRef]
- Zur, D.; Iglicki, M.; Busch, C.; Invernizzi, A.; Mariussi, M.; Loewenstein, A.; Busch, C.; Cebeci, Z.; Chhablani, J.K.; Chaikitmongkol, V.; et al. OCT Biomarkers as Functional Outcome Predictors in Diabetic Macular Edema Treated with Dexamethasone Implant. Ophthalmology 2018, 125, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Torresin, T.; Bini, S.; Convento, E.; Pilotto, E.; Parrozzani, R.; Midena, E. Imaging Retinal Inflammatory Biomarkers after Intravitreal Steroid and Anti- VEGF Treatment in Diabetic Macular Oedema. Acta Ophthalmologica 2017, 95, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Hatano, M.; Higashijima, F.; Yoshimoto, T.; Ogata, T.; Ohta, M.; Kobayashi, Y.; Wakuta, M.; Yanai, R.; Kimura, K. Evaluation of Microaneurysms as Predictors of Therapeutic Response to Anti-VEGF Therapy in Patients with DME. PLoS ONE 2022, 17, e0277920. [Google Scholar] [CrossRef]
- Grigsby, J.G.; Cardona, S.M.; Pouw, C.E.; Muniz, A.; Mendiola, A.S.; Tsin, A.T.C.; Allen, D.M.; Cardona, A.E. The Role of Microglia in Diabetic Retinopathy. Journal of Ophthalmology 2014, 2014, 1–15. [Google Scholar] [CrossRef]
- Zeng, H. Microglial Activation in Human Diabetic Retinopathy. Arch Ophthalmol 2008, 126, 227. [Google Scholar] [CrossRef]
- Kim, K.T.; Kim, D.Y.; Chae, J.B. Association between Hyperreflective Foci on Spectral-Domain Optical Coherence Tomography and Early Recurrence of Diabetic Macular Edema after Intravitreal Dexamethasone Implantation. Journal of Ophthalmology 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Spence, G.; Hogg, R.E.; Stevenson, M.; Chakravarthy, U. Disorganization of Inner Retina and Outer Retinal Morphology in Diabetic Macular Edema. JAMA Ophthalmol 2018, 136, 202. [Google Scholar] [CrossRef]
- Zur, D.; Iglicki, M.; Sala-Puigdollers, A.; Chhablani, J.; Lupidi, M.; Fraser-Bell, S.; Mendes, T.S.; Chaikitmongkol, V.; Cebeci, Z.; Dollberg, D.; et al. Disorganization of Retinal Inner Layers as a Biomarker in Patients with Diabetic Macular Oedema Treated with Dexamethasone Implant. Acta Ophthalmologica 2020, 98. [Google Scholar] [CrossRef]
- Rajesh, B.; Zarranz-Ventura, J.; Fung, A.T.; Busch, C.; Sahoo, N.K.; Rodriguez-Valdes, P.J.; Sarao, V.; Mishra, S.K.; Saatci, A.O.; Udaondo Mirete, P.; et al. Safety of 6000 Intravitreal Dexamethasone Implants. Br J Ophthalmol 2020, 104, 39–46. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Demographic and baseline characteristics.
| RRD | SO | ERM | P-value * | ||
|---|---|---|---|---|---|
| N° (%); patients / eyes | 36 (75) | 10 (20.8) | 2 (4.2) | ||
| Laterality: Right/Left | 16/20 | 6/4 | 1/1 | 0.29 | |
| Age, year (mean±SD) | 64.6±4.5 | 63.8±3.6 | 58.5±0.7 | 0.17 | |
| Gender, N° (%) | |||||
| Male | 25 (69.4) | 6 (60) | 1 (50) | ||
| Female | 11 (30.6) | 4 (40) | 1 (50) | ||
| Type 2 Diabetes (controlled with therapy); N° (%) | 3 (8%) | 1 (10%) | 0 (0%) | 0.45 | |
| Time between cataract surgery and PPV; years, mean ± SD (range) | 4.1± 2.48 (1-11) | 3 ± 1.5 (2-6) | 2 ± 0.7 (1-2.5) | 0.20 | |
| Macula attached at the time of surgery (RRD group); n° (%) | 31 (86.1%) | - | - | ||
| PVR present: n° (%) | 14 (38.8%) | - | - | ||
| Mild VH associated to RRD: n° (%) | 2 (5.5%) | - | - | ||
| Endotamponade agent used (RRD group) | |||||
| Gas (SF6 24%; C3F8 14%) | 22 (64.7%) | ||||
| Silicone Oil 1000 cst | 10 (29.4%) | ||||
| Densiron | 2 (5.8%) | ||||
RRD: rhegmatogenous retinal detachment; SO: silicone oil; ERM: epiretinal membrane; PVR: proliferative vitreoretinopathy; SF6: sulfur hexafluoride; C3F8: octafluoropropane; cst: centistokes. Percentage calculated on the overall study population. p-value, Fisher test.
Table 2.
Best-corrected visual acuity (BCVA) changes during follow-up.
| BCVA Baseline* (logMAR) | 1.44±0.99 | |
| BCVA 1 Month (logMAR) | 0.56±0.40 | <0.001 |
| BCVA 3 Months (logMAR) | 0.44±0.48 | <0.001 |
| BCVA 6 Months (logMAR) | 0.37±0.35 | <0.001 |
| BCVA 9 Months (logMAR) | 0.38±0.39 | <0.001 |
| BCVA 12 Months (logMAR) | 0.32±0.37 | <0.001 |
*mean±SD; p-value, Wilcoxon test (BCVA Baseline as reference value).
Table 3.
Central Macular Thickness (CMT) changes during follow-up, starting from 1 month.
| CMT 1 month* (µm) | 347±123.5 | |
| CMT 3 months (µm) | 304±93.6 | 0.002 |
| CMT 6 months (µm) | 289±79.7 | 0.002 |
| CMT 9 months (µm) | 322±104.5 | 0.048 |
| CMT 12 months (µm) | 290±80.4 | 0.003 |
*mean±SD; p-value, Wilcoxon test (CMT 1 month as reference value).
Table 4.
Optical Coherence Tomography (OCT) biomarkers.
| IRC | DRIL | DROL | HRF | SRF | |
| RRD n(%) | 20 (41.7) | 7 (14.6) | 8 (16.7) | 7 (14.6) | 7 (14.6) |
| SO n(%) | 10 (20.8) | 4 (8.3) | 2 (4.2) | 2 (4.2) | 4 (8.3) |
| ERM n(%) | 2 (4.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| p | 0.02 | 0.29 | 0.75 | 0.78 | 0.30 |
| IRC | DRIL | DROL | HRF | SRF | |
| RRD n(%) | 20 (41.7) | 7 (14.6) | 8 (16.7) | 7 (14.6) | 7 (14.6) |
| SO n(%) | 10 (20.8) | 4 (8.3) | 2 (4.2) | 2 (4.2) | 4 (8.3) |
| ERM n(%) | 2 (4.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| p | 0.02 | 0.29 | 0.75 | 0.78 | 0.30 |
Abbreviations: IRC, intraretinal cysts; DRIL, disorganization of inner retinal layers; DROL, disorganization of outer retinal layers; HRF, hyperreflective foci; SRF, subretinal fluid; RRD, rhegmatogenous retinal detachment; SO, Silicone oil; ERM, epiretinal membrane. %, percentage calculated on the overall study population. p-value, Fisher test.
Table 5.
Intravitreal dexamethasone implant (DEX-i) performed at each time-point.
| RRD | SO | ERM | p | |
| DEX-i at 3 months, n (%) | 10 (20.8) | 5 (10.4) | 1 (2.1) | 0.37 |
| DEX-i at 6 months, n (%) | 3 (6.4) | 2 (4.3) | 0 (0.0) | 0.52 |
| DEX-i at 9 months, n (%) | 11 (22.9) | 5 (10.4) | 0 (0.0) | 0.31 |
| DEX-i at 12 months, n (%) | 4 (8.3) | 0 (0.0) | 0 (0.0) | 0.49 |
Abbreviations: RRD, rhegmatogenous retinal detachment; SO, Silicone oil; ERM, epiretinal membrane; %, percentage calculated on the overall study population; p-value, Fisher test.
Table 6.
Correlation between mean Central Macular Thickness (CMT) at different time-points.
| CMT 1 month | CMT 3 Months | CMT 6 Months | CMT 9 Months | CMT 12 Months | ||
|
CMT 1 month |
Spearman’s Rho p |
— — |
||||
| CMT 3 Months | Spearman’s Rho | 0.592 *** | — | |||
| p | <0.001 | — | ||||
| CMT 6 Months | Spearman’s Rho | 0.174 | 0.274 | — | ||
| p | 0.237 | 0.060 | — | |||
| CMT 9 Months | Spearman’s Rho | 0.145 | 0.541 *** | 0.578 *** | — | |
| p | 0.326 | <0.001 | <0.001 | — | ||
|
CMT 12 Months |
Spearman’s Rho p |
0.117 0.428 |
0.573 *** <0.001 |
0.454 ** 0.001 |
0.662 *** <0.001 |
— — |
* p < .05, ** p < .01, *** p < .001, Spearman’s Rank tes.t.
Table 7.
Univariate (A) and multiple (B) logistic regression model of DEX-i at different time-point on demographic and clinical variables.
Table 7.
Univariate (A) and multiple (B) logistic regression model of DEX-i at different time-point on demographic and clinical variables.
| (A) DEX-i at 3 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | 0.10 | 0.07 | 0.17 | 1.11 | |
| Gender (male) | -3.67e-16 | 0.66 | 0.99 | 0.99 | |
| Disease | |||||
| SO—RRD | 0.95 | 0.73 | 0.19 | 2.6 | |
| ERM—RRD | 0.95 | 1.46 | 0.51 | 2.6 | |
| CMT 1 month | 0.01 | 0.003 | 0.005 | 1.01 | |
| IRC (No) | 1.69 | 0.83 | 0.04 | 5.44 | |
| DRIL (No) | 2.27 | 0.78 | 0.004 | 9.66 | |
| HRF (No) | 1.76 | 0.79 | 0.02 | 5.80 | |
| DROL (No) | 1.44 | 0.74 | 0.05 | 4.20 | |
| SRF (No) | 0.95 | 0.68 | 0.16 | 2.60 | |
| (B) DEX-i at 3 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | 0.09 | 0.10 | 0.35 | 1.10 | |
| Gender (male) | -0.18 | 0.87 | 0.83 | 0.83 | |
| Disease | |||||
| SO—RRD | 0.49 | 0.98 | 0.61 | 1.64 | |
| ERM—RRD | 0.77 | 2.44 | 0.75 | 2.17 | |
| CMT 1 month | 0.008 | 0.005 | 0.09 | 1.0 | |
| IRC (No) | -0.33 | 1.26 | 0.78 | 0.71 | |
| DRIL (No) | 1.62 | 0.92 | 0.08 | 5.08 | |
| HRF (No) | 1.33 | 1.03 | 0.19 | 3.80 | |
| (A) DEX-i at 6 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | 0.04 | 0.10 | 0.69 | 1.03 | |
| Gender (male) | 0.39 | 0.97 | 0.68 | 1.5 | |
| Disease | |||||
| SO—RRD | 0.98 | 0.99 | 0.32 | 2.66 | |
| ERM—RRD | -15.2 | 2797.4 | 0.99 | 2.51è-7 | |
| IRC (No) | -0.28 | 0.96 | 0.76 | 0.75 | |
| DRIL (No) | -17.7 | 3242.4 | 0.99 | 2.04e-8 | |
| HRF (No) | 1.23 | 1.00 | 0.21 | 3.42 | |
| DROL (No) | 0.06 | 1.18 | 0.96 | 1.06 | |
| SRF (No) | -0.22 | 1.17 | 0.84 | 0.80 | |
| (A) DEX-i at 9 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | 0.02 | 0.07 | 0.74 | 1.02 | |
| Gender (male) | 0.42 | 0.64 | 0.51 | 1.5 | |
| Disease | |||||
| SO—RRD | 0.87 | 0.73 | 0.23 | 2.27 | |
| ERM—RRD | -15.7 | 1696.7 | 0.99 | 1.45e-7 | |
| CMT 3 months | 0.006 | 0.003 | 0.07 | 1.00 | |
| CMT 6 months | 0.007 | 0.004 | 0.11 | 1.00 | |
| IRC (No) | 0.14 | 0.65 | 0.82 | 1.15 | |
| DRIL (No) | 0.67 | 0.70 | 0.33 | 1.97 | |
| HRF (No) | 1.76 | 0.79 | 0.02 | 5.80 | |
| DROL (No) | 2.02 | 0.78 | 0.01 | 7.51 | |
| SRF (No) | 0.95 | 0.68 | 0.16 | 2.60 | |
| (B) DEX-i at 9 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | -0.02 | 0.09 | 0.85 | 0.97 | |
| Gender (male) | 0.01 | 0.83 | 0.99 | 1.01 | |
| Disease | |||||
| SO—RRD | 1.01 | 0.84 | 0.22 | 2.75 | |
| ERM—RRD | -14.9 | 1696.7 | 0.99 | 3.23e-7 | |
| HRF (No) | 1.71 | 0.90 | 0.04 | 5.53 | |
| DROL (No) | 1.96 | 0.87 | 0.02 | 7.11 | |
| (A) DEX-i at 12 months as dependent variable | |||||
| Parameters | β | SE (β) | p | OR | |
| Age | -0.20 | 0.15 | 0.18 | 0.81 | |
| Gender (male) | -0.33 | 1.19 | 0.77 | 0.71 | |
| Disease | |||||
| SO—RRD | -17.5 | 3400.7 | 0.99 | 2.39e-8 | |
| ERM—RRD | -17.5 | 7604.2 | 0.99 | 2.39e-8 | |
| CMT 3 months | -0.01 | 0.01 | 0.21 | 0.98 | |
| CMT 6 months | 0.007 | 0.004 | 0.10 | 1.00 | |
| CMT 9 months | 0.005 | 0.004 | 0.20 | 1.00 | |
| IRC (No) | -1.97 | 1.20 | 0.10 | 0.14 | |
| DRIL (No) | -17.4 | 3242.4 | 0.99 | 2.62e-8 | |
| HRF (No) | -17.4 | 3584.6 | 0.99 | 2.78e-8 | |
| DROL (No) | 0.26 | 1.21 | 0.83 | 1.29 | |
| SRF (No) | -17.4 | 3104.4 | 0.99 | 2.54e-8 | |
Abbreviations: SO, silicone oil; RRD, rhegmatogenous retinal detachment; ERM, epiretinal membrane; CMT, central macular thickness; IRC, intraretinal cysts; DRIL, disorganization of the inner retinal layers; DROL, disrupted retinal outer layers; HRF, hyperreflective foci; SRF, subretinal fluid; SE, standard error; OR, Odds Ratio.
Table 8.
Intraocular pressure (IOP) changes over follow-up.
| IOP Baseline (mmHg) | 15.6±3.9 | |
| IOP 1 Month (mmHg) | 15.6±2.8 | 0.90 |
| IOP 3 Months (mmHg) | 15.0±2.4 | 0.32 |
| IOP 6 Months (mmHg) | 15.9±3.1 | 0.31 |
| IOP 9 Months (mmHg) | 15.8±2.1 | 0.71 |
| IOP 12 Months (mmHg) | 15.6±1.9 | 0.80 |
IOP: intraocular pressure.*mean±SD; p-value, Wilcoxon test (IOP Baseline as reference value).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



