Submitted:
27 September 2024
Posted:
27 September 2024
You are already at the latest version
Abstract
This case represents the association between the presence of large fibroid tumor and pulmonary embolism in 47-year-old women. We highlight the diagnostic investigations and treatment methods for PE, followed by further evaluation of the underlying explanation of this pathology and eliminating other related risk factors.
Keywords:
Uterine fibroid
; Venous thromboembolism
; pulmonary embolism
; Venous stasis
; Hysterectomy
1. Introduction
Uterine fibroids or, leiomymas are common benign tumors particularly in women with reproductive age or child bearing, which can rarely cause significant complications [1]. One of the complication is acute venous thromboembolism (VTE) which is a rare complication, moreover, a studies have showed the association between the large uterine fibroids ,deep vein thrombosis (DVT) and pulmonary embolism(PE)[2,3,4,5]. The possible connection between uterine fibroids and VTE is probably due to the pressure exerted by large fibroids, which can cause venous stasis in the pelvis and lower extremities. Other potential associations include polycythemia and reactive thrombocytosis resulting from menorrhagia, which can also increase the risk of developing VTE [6,7]. This case report will discuss the associations between uterine fibroid and its compression effect on iliac vein and resulting in acute extensive bilateral PE after excluding all risk factors. Moreover, we will highlight the diagnostic techniques and best intervention methods to the patient.
2. Case Presentation
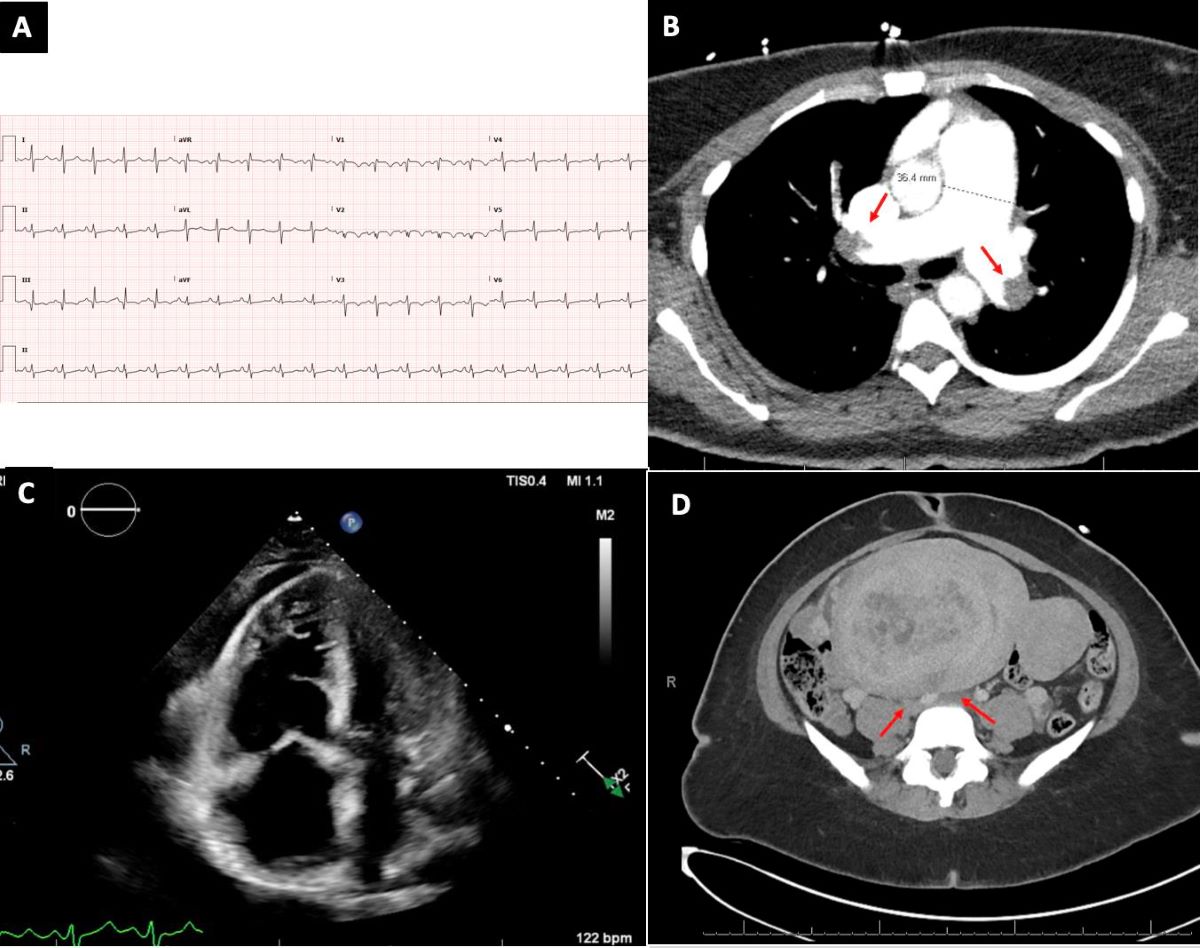
Our patient is 47 year old female presented with acute dyspnea in the emergency department (ED), the symptoms started 8 days ago and had progressively worsened during last 6 hours. She had history of obesity with body mass index 32 kg/m2, severe chronic iron deficiency anemia that interfered with her daily activities, She had also history of heavy menstruation with 24 weeks size of uterus. Recently she started to complain of a right calf dull pain over the past 1-2 days and makes her uncomfortable during her walking. Upon admission and during physical examination she was tachycardic with HR 128 beats/min and blood pressure was 100/58 mmHg, also her oxygen saturation was 97% on room air. She seemed in mild respiratory distress and was unable to take breath easily. Moreover, and during the examination we noticed a marked tenderness in the right calf when squeezing the calf muscle which raised our suspicion of DVT. The laboratory workups showed with hemoglobin (Hgb) = 6.5 g/d, and microcytosis with mean corpuscular volume (MCV) = 59 fL, also iron studies confirmed her severe iron deficiency with a serum iron level = 10 µg/dL, a total iron-binding capacity (TIBC) = 480 µg/dL, and a ferritin level = 6 ng/mL. Her B-type natriuretic peptide (BNP) was elevated as well = 687 pg/mL, and Troponin I was mildly elevated = 42 ng/L, which can suggest Right ventricle (RV) strain. Venous blood gas (VBG) was done for suspected PE and the result came back with upper high PH =7.43, low pCO2 =31, pO2= less than 17, HCO3 = 21, oxygen saturation (%o2 Hb) = 10 (Table 1). However, during that time a blood transfusion and IV iron were indicated and infused, and in the meanwhile the ECG was performing and showed sinus tachycardia with an S1Q3T3 pattern and incomplete RBBB as shown in this image (Figure 1), which suggests PE and right heart dysfunction. On bedside transthoracic echocardiography (TTE) we were able to confirm the presence of significant RV dilation and severely reduced systolic function in addition to elevated the mean pulmonary artery pressure (mPAP) to 51 mmHg (Figure 2). The patient’s VTE was classified as intermediate-high risk. Therefore the CT angiography of the chest was performed to show submassive bilateral pulmonary emboli involving both the right and left pulmonary arteries (PAs) and their branches as shown in this image (Figure 3). The next day, an ultrasound of the lower extremity was done and revealed bilateral occlusive calf vein thrombus in the right posterior tibial and peroneal veins and in the left tibioperoneal trunk. The decision was made by our multidisciplinary team to start infusing Heparin, but due to the worsening of her hypoxia. The plan had changed to proceed with catheter-directed thrombolysis (CTD) using the EkoSonic Endovascular System (EKOS) catheters (Boston Scientific, Marlborough, MA, USA) in guidance of fluoroscopy and ultrasound. The right internal jugular vein (IJV) was accessed by using Sledinger technique to insert two 7 French sheaths in guidance of ultrasound probe, and 250IU of Heparin was infused to prevent catheter related thrombosis. Afterwards, the Wedge catheter was advanced to right heart and showed mean of RA=22 mmHg, RV=76/18 mmHg, with mean PA 51 mmHg and oxygen sat 48%. Next the EKOS catheter was advanced into the right PA and second catheter was positioned in left PA. tPA infusion was started in each catheter with 1mg, totaling 2mg for both catheters. Following the procedure, we noticed that her mPAP decreased from 51 mmHg to 33 mmHg immediately and oxygen sat increased to 64 mmHg. After that, the patient was transferred to the ICU for overnight monitoring and continuous ECG. She needed to receive 4 units of packed RBCs to treat her anemia, and elevate her hemoglobin level to more than 9 g/dL. The next day, TTE repeated and demonstrated the RV to be functionally normal. Given these findings that she does not have any common risk factors related to VTE, we planned to perform further investigations to understand the etiology of the thromboembolic event, so we started with a pelvic ultrasound. It demonstrated a large intramural leiomyoma (Figure 4). A subsequent abdominal CT scan confirmed the tumor position and compression portion that tightened the bilateral iliac veins (Figure 5) and pressing on urinary bladder. The patient declined further investigations and refused our recommendation of uterine hysterectomy, therefore was discharged home with discharge instructions for close follow up with her gynecologist and hematologist physicians.
Given that we confirmed that uterine fibroid was the reason behind her VTE, and she followed up with her gynecologist and got her consent for a hysterectomy procedure after worsening her symptoms. MRI was done pre-procedurally for measurements and assessments (Figure 6). The tumor is approximately 150 mm (15 cm) in length in the craniocaudal direction and 91 mm (9.1 cm) in width and another cross-sectional diameter view with measures about 161 mm (16.1 cm), which further underscoring the large of lesion. The surgical removal was done, and the removal of the fibroid tumor alleviated the compression in the iliac veins. The patient reported a full recovery and was discharged later.
3. Discussion
Pulmonary embolism (PE) is recognized as the third cause of death in the US after CAD and stroke, and is thought to be a major cause of death with nearly 100,000 fatalities annually [8]. Furthermore, DVT is the primary cause of PE and there are a variety of risk factors associated with it such as mechanical compression caused by neoplasms, which can raise the venous pressure which further reduces vein flow to lower extremities. This can be associated with one of the components of the Virchow triad which is hypercoagulability state and venous stasis which can result in clot formation [9].
However uterine fibroid or leiomyoma may be considered as an independent risk factor for developing a DVT [10] due to its compression feature, but also it depends on the size and location of the tumor as well as the presence of typical risk factors. Our patient declined any history of pregnancy loss or thrombosis in addition to family history of thrombophilia. This information helped to exclude some common risk factors for acute VTE events. However, diagnosing VTE in patients with large fibroids can be challenging especially with overlapping symptoms of anemia and pulmonary embolism, as seen in this case where the patient presented with acute dyspnea, syncope, and leg pain, which all these symptoms can occur in both diseases. The initial lab workup of chronic iron deficiency anemia and VBG results with elevated BNP were indicative of cardiac strain and increased the suspicion of PE, and consequently can complicate the clinical presentation and delay the diagnosis. In fact, VBG showed an increase in PH and a decrease in pCO2, indicating respiratory alkalosis, which is a common finding in PE due to hyperventilation. Moreover, a decrease in pO2 and %O2 Hb indicates severe hypoxemia and warrants further investigations. Notably the D-dimer test can be beneficial in such cases of VTE, but due to the patient's worsening symptoms and hemodynamic instability we proceeded with more advanced diagnostic steps immediately for optimum results for the patient. Starting with ECG which showed an S1Q3T3 pattern with incomplete RBBB and subsequent TTE which revealed the presence of significant RV dilatation and increased pulmonary artery pressure to 51mmHg. These findings increased the risk of PE and warranted to perform CT angiography to assess the patency of PAs. It showed extensive bilateral emboli involving both right and left PAs. For patients presenting with PE/VTE secondary to uterine fibroids, management also can be challenging, and the main goal for treatment is to deal with the VTE first and then remove the fibroid [1], as the ultimate goal is to address the PE before complications occur. This case was managed by CDT using EKOS under the guidance of ultrasound-assisted thrombolysis to ensure more clot fragmentation and dissolute. This kind of intervention can successfully reduce the patient's pulmonary artery pressure from 51 mmHg to 33 mmHg and increase the oxygen sat to 64 mmHg after the procedure immediately. This technique has been used and shown to be efficient in patients with massive or submassive PE according to the Flacone case report, as it enhances the delivery of thrombolytic directly into the thrombus in order to decrease the risk of systemic bleeding [11]. Despite treating the PE, it is essential to address the underlying cause of this pathology, so further investigations were warranted in our case, and an ultrasound of the pelvis was done to show intramural fibroid tumor. CT scan of the abdomen was done for suspicion of compression effect, which truly revealed a presence of the fibroid compressing on bilateral iliac veins. Multiple interventions can be done to resolve the symptoms if present or prevent such complications. First perform a uterine fibroid embolization (UFE) which is a minimally invasive procedure that aims to emboli the uterine artery through the internal iliac artery (IIA). Given the success rate about 95% of bilateral UAE by experienced physicians [12]. The second approach is surgical removal via hysterectomy which can be the definitive treatment to prevent the recurrence of VTE as was done in our case. In many documented cases, patients who undergo successful uterine fibroid removal (either via myomectomy or hysterectomy) demonstrate complete alleviation of venous compression and reduce the risk of recurrent VTE according to Nishikawa's study. In this case the patient's imaging after the procedure showed resolution of venous stasis and experienced no further episodes of dyspnea or leg pain.
This case was aligned with several reportable cases of large uterine fibroids causing VTE, although the associations remain rare. For example, a series of seven women with large fibroids were in this study, five of them had the compression effect on iliac veins, causing VTE. Moreover these five patients who are demonstrating approximately 71% of the cases underwent hysterectomy, with no subsequent VTE events after surgery. Additional suggestion was that fibroid compression considered a significant factor in their original thromboembolic conditions [13]. Such as these cases reinforce the need for clinicians to maintain a high index of suspicion for VTE in women with large fibroids, particularly those presenting with leg pain, dyspnea, or signs of venous insufficiency.
4. Conclusions
This case highlights an alternate cause of VTE. This patient had a large uterine fibroid causing compression of the iliac veins leading to venous stasis and thrombosis. The association between fibroids and VTE is considered a rare association and need for further research into preventive strategies and early detection methods. For example, such as routine screening for DVT in women with large fibroids might be counted as a preventive approach, which can help to identify those at risk before PE developed. We also promote the researcher and physicians for further retrospective and prospective cohort studies to explore the association of uterine fibroid and VTE events.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to acknowledge the help of our other contributing fellows within the department.
References
- Gupta S, Manyonda IT. Acute complications of fibroids. Best Pract Res Clin Obstet Gynaecol 2009, 23, 609–17. [Google Scholar] [CrossRef] [PubMed]
- Shiota M, Kotani Y, Umemoto M, et al. Deep-vein thrombosis is associated with large uterine fibroids. Tohoku J Exp Med 2011, 224, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld H and Byard, RW. Lower extremity deep venous thrombosis with fatal pulmonary thromboembolism caused by benign pelvic space-occupying lesions: an overview. J Forensic Sci 2012, 57, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa H, Ideishi M, Nishimura T, et al. Deep venous thrombosis and pulmonary thromboembolism associated with a huge uterinemyoma: a case report. Angiology 2000, 51, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Riat R, Chowdary P, Mavrides E, et al. Is there an association between thrombosis and fibroids? A single centre experience and literature review. Int J Lab Hematol 2013, 35, e13–e16. [Google Scholar]
- Ramanan S, Chapman-Wardy J and Watson R. Bleeding versus clotting: a complex case of a large fibroid uterus causing menorrhagia and a DVT. Case Rep Obstet Gynecol 2016, 2016, 4169565. [Google Scholar]
- Fletcher H, Wharfe G, Williams NP, et al. Venous thromboembolism as a complication of uterine fibroids: a retrospective descriptive study. J Obstet Gynaecol 2009, 29, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Vyas, V. , Sankari, A., & Goyal, A. (2024, February 28). Acute pulmonary embolism StatPearls- NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK560551/.
- Waheed, S. M. , Kudaravalli, P., & Hotwagner, D. T. (2023, January 19). Deep vein thrombosis StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK507708/.
- Vyas, P. , & Douglas, L. Fibroids as a risk factor for Deep vein thrombosis (DVT) at an Urban Academic Institution: A retrospective observational study. Journal of Minimally Invasive Gynecology 2021, 28, S107. [Google Scholar] [CrossRef]
- Massive pulmonary embolism in a woman with leiomyomatous uterus causing pelvic deep venous thrombosis. (2005, June 1). PubMed. https://pubmed.ncbi.nlm.nih.gov/16052843/.
- Young, M. , Coffey, W., & Mikhail, L. N. (2023b, July 3). Uterine fibroid embolization. StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK519016/.
- Lacharite-Roberge, A. , Raza, F., Bashir, R., Dass, C. A., Moser, G. W., Auger, W. R., Toyoda, Y., Forfia, P. R., & Vaidya, A. Case series of seven women with uterine fibroids associated with venous thromboembolism and chronic thromboembolic disease. Pulmonary Circulation 2018, 9, 1–7. [Google Scholar] [CrossRef]
Figure 1.
An ECG image demonstrates the presence of S1Q3T3 pattern and incomplete RBBB which could indicate PE complicating RV dysfunction.
Figure 1.
An ECG image demonstrates the presence of S1Q3T3 pattern and incomplete RBBB which could indicate PE complicating RV dysfunction.
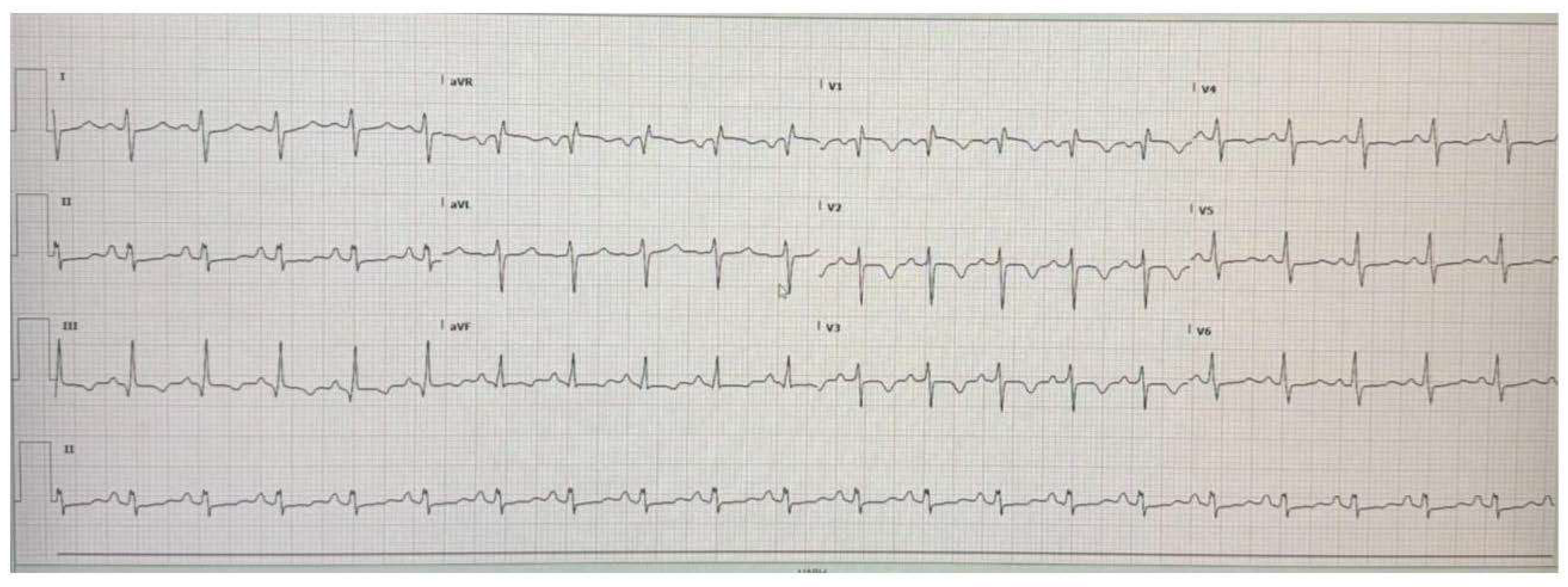
Figure 2.
TTE image displays the enlargement of right ventricle indicating the presence of pulmonary hypertension caused by PE.
Figure 2.
TTE image displays the enlargement of right ventricle indicating the presence of pulmonary hypertension caused by PE.
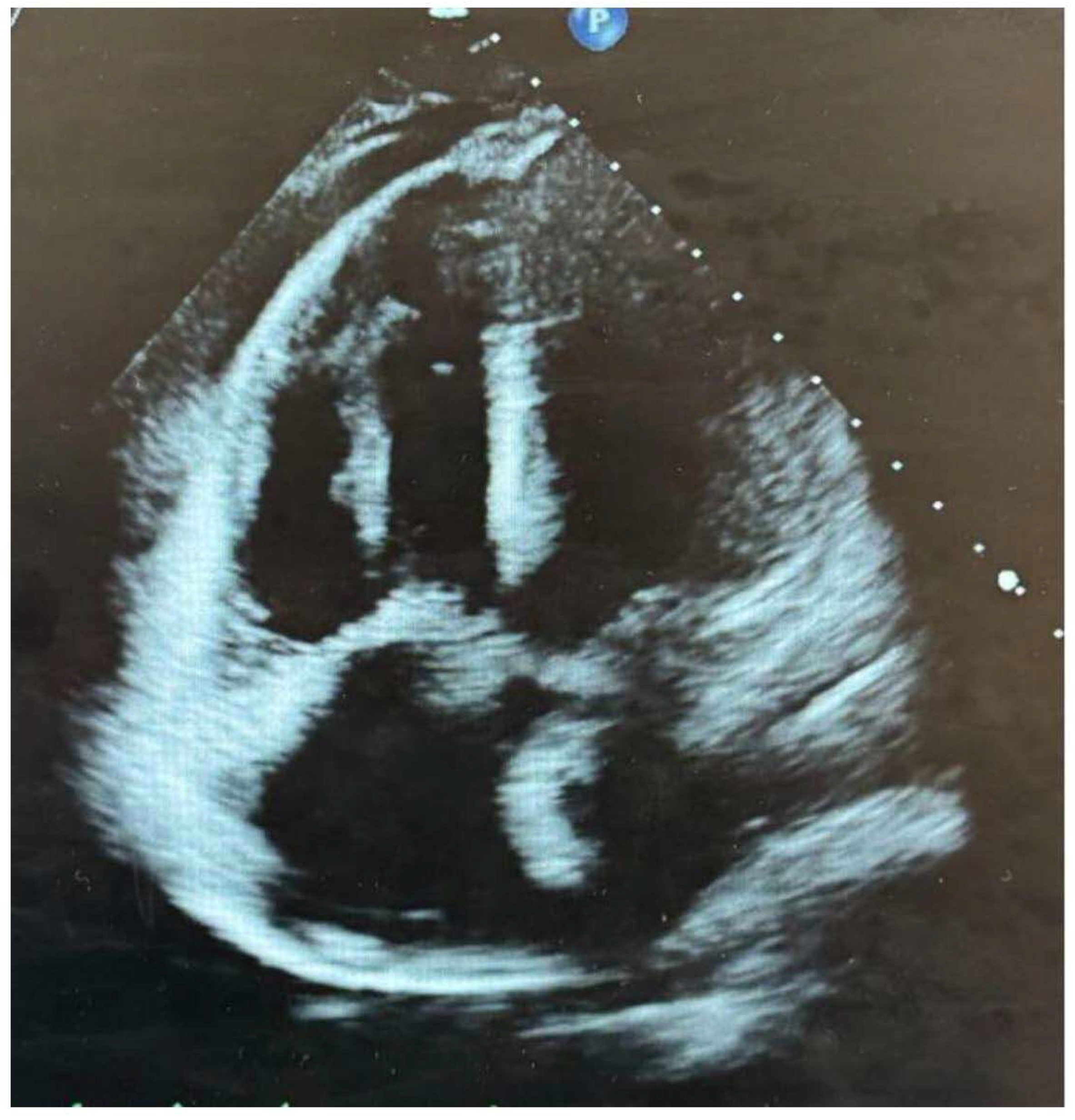
Figure 3.
CTA of the chest image showing submassive bilateral pulmonary emboli in both the right and left PAs and their branches (white arrows).
Figure 3.
CTA of the chest image showing submassive bilateral pulmonary emboli in both the right and left PAs and their branches (white arrows).
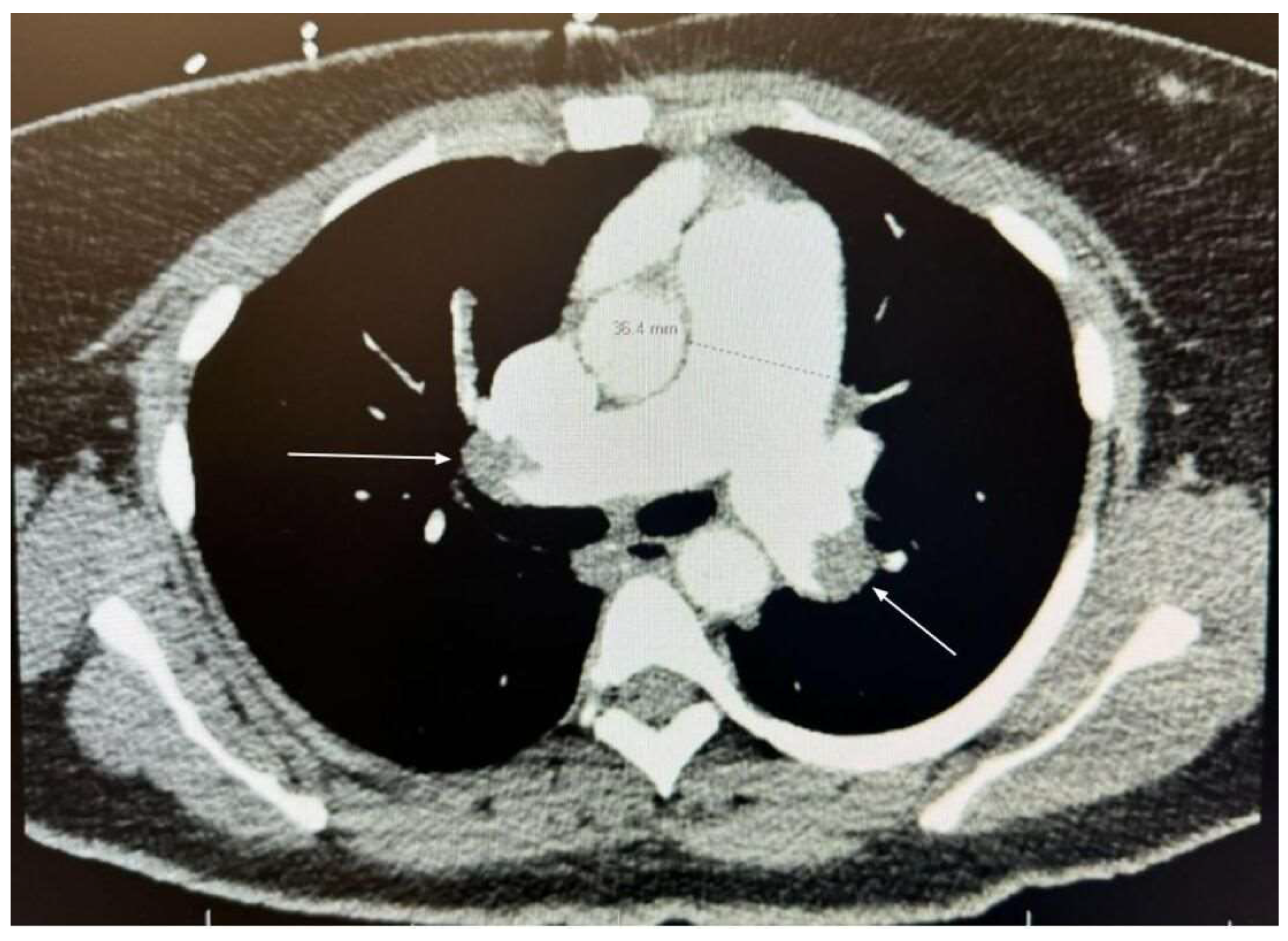
Figure 4.
Pelvic ultrasound showing large intramural leiomyoma.
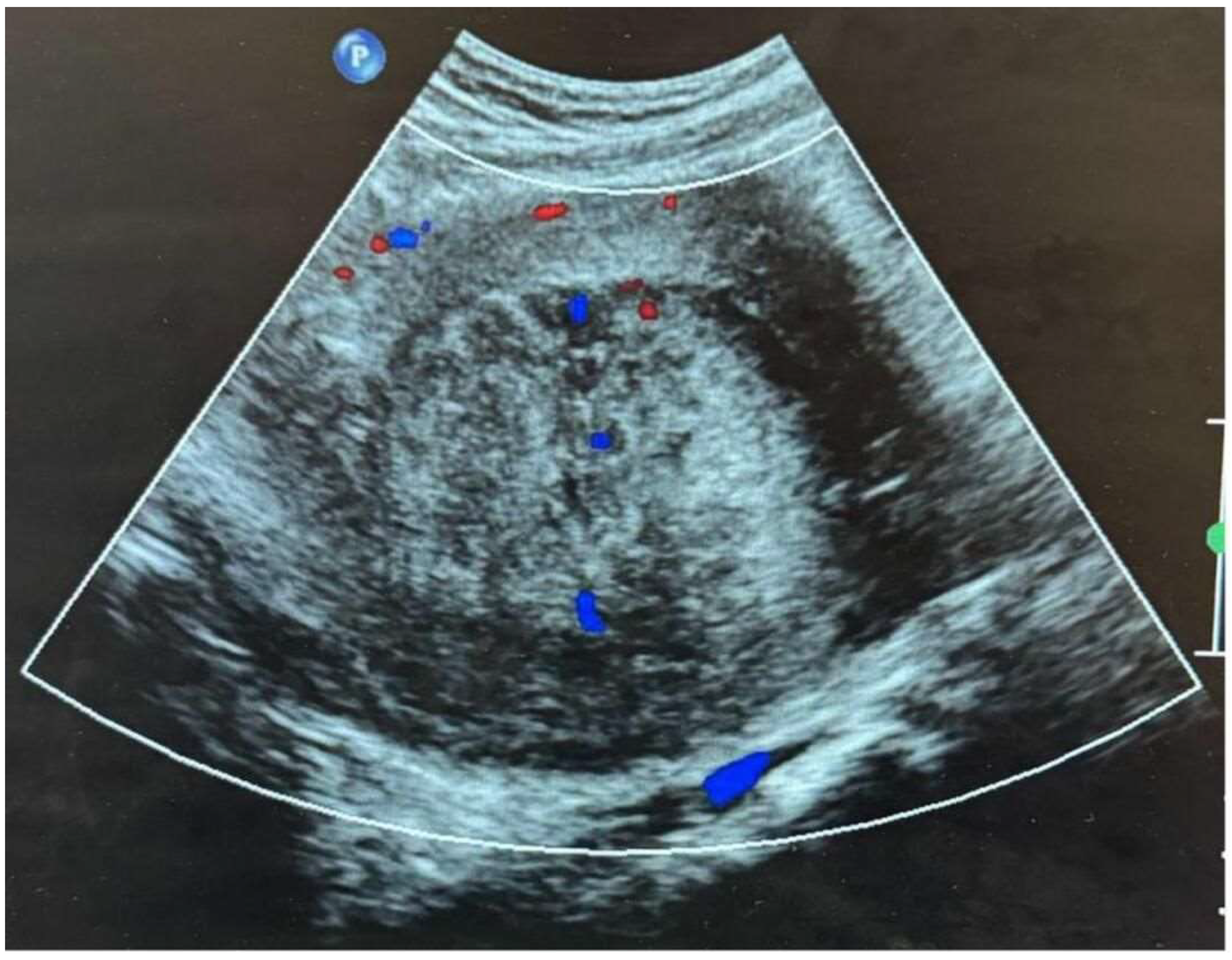
Figure 5.
(A): CT scan of abdomen in axial view of showing the large leiomyoma compressing the iliac veins (white arrows). (B): CT scan of abdomen in coronal view further illustrating the extent of the tumor confirming its mass effect on surrounding structures.
Figure 5.
(A): CT scan of abdomen in axial view of showing the large leiomyoma compressing the iliac veins (white arrows). (B): CT scan of abdomen in coronal view further illustrating the extent of the tumor confirming its mass effect on surrounding structures.
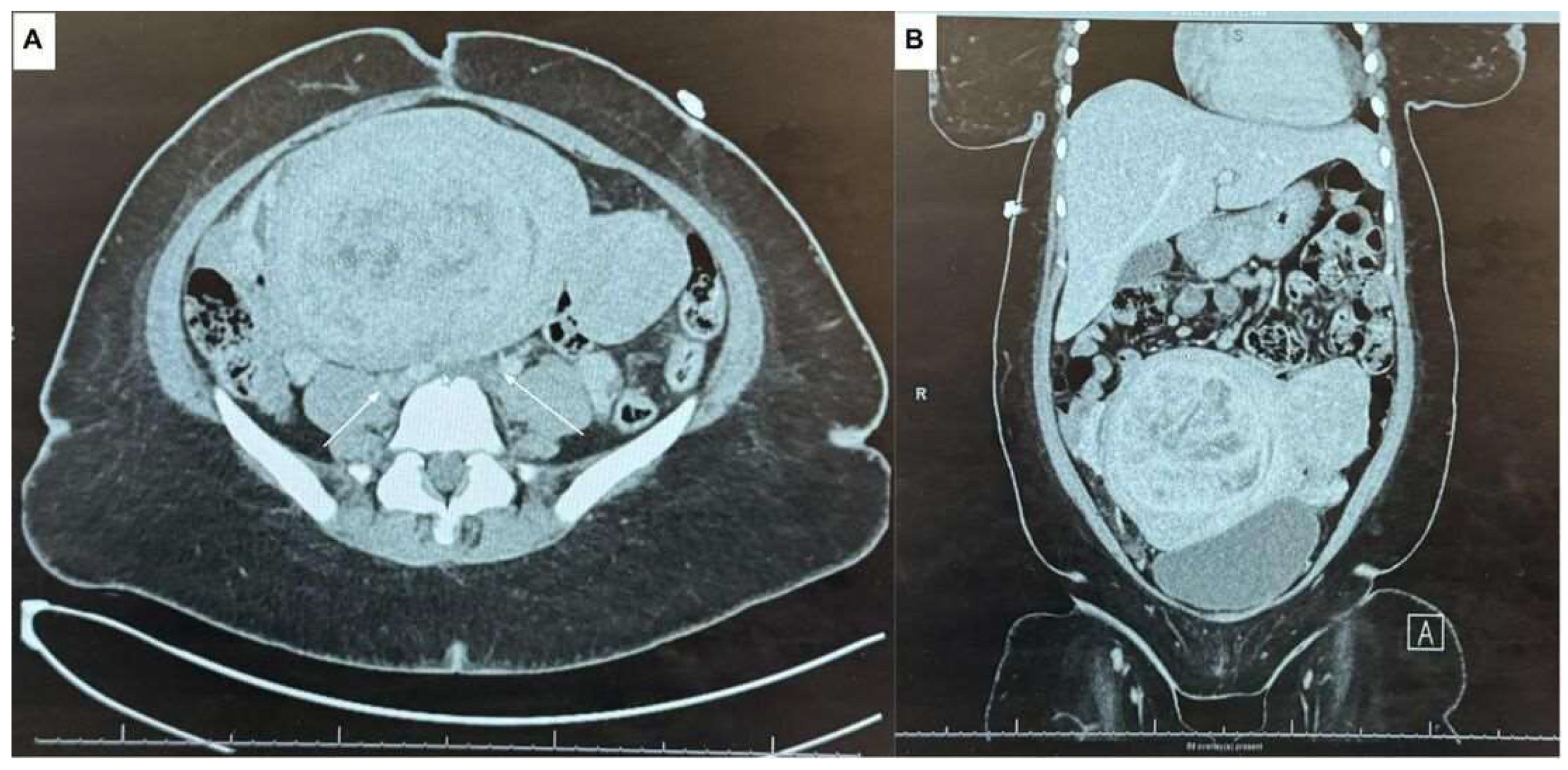
Figure 6.
(A): MRI image in sagittal view showing the dimensions of the large uterine fibroid (150 mm x 91.9 mm). (B): MRI image in axial view further confirming the size of the fibroid (161.4 mm) obtained for pre surgical measurements of the hysterectomy.
Figure 6.
(A): MRI image in sagittal view showing the dimensions of the large uterine fibroid (150 mm x 91.9 mm). (B): MRI image in axial view further confirming the size of the fibroid (161.4 mm) obtained for pre surgical measurements of the hysterectomy.
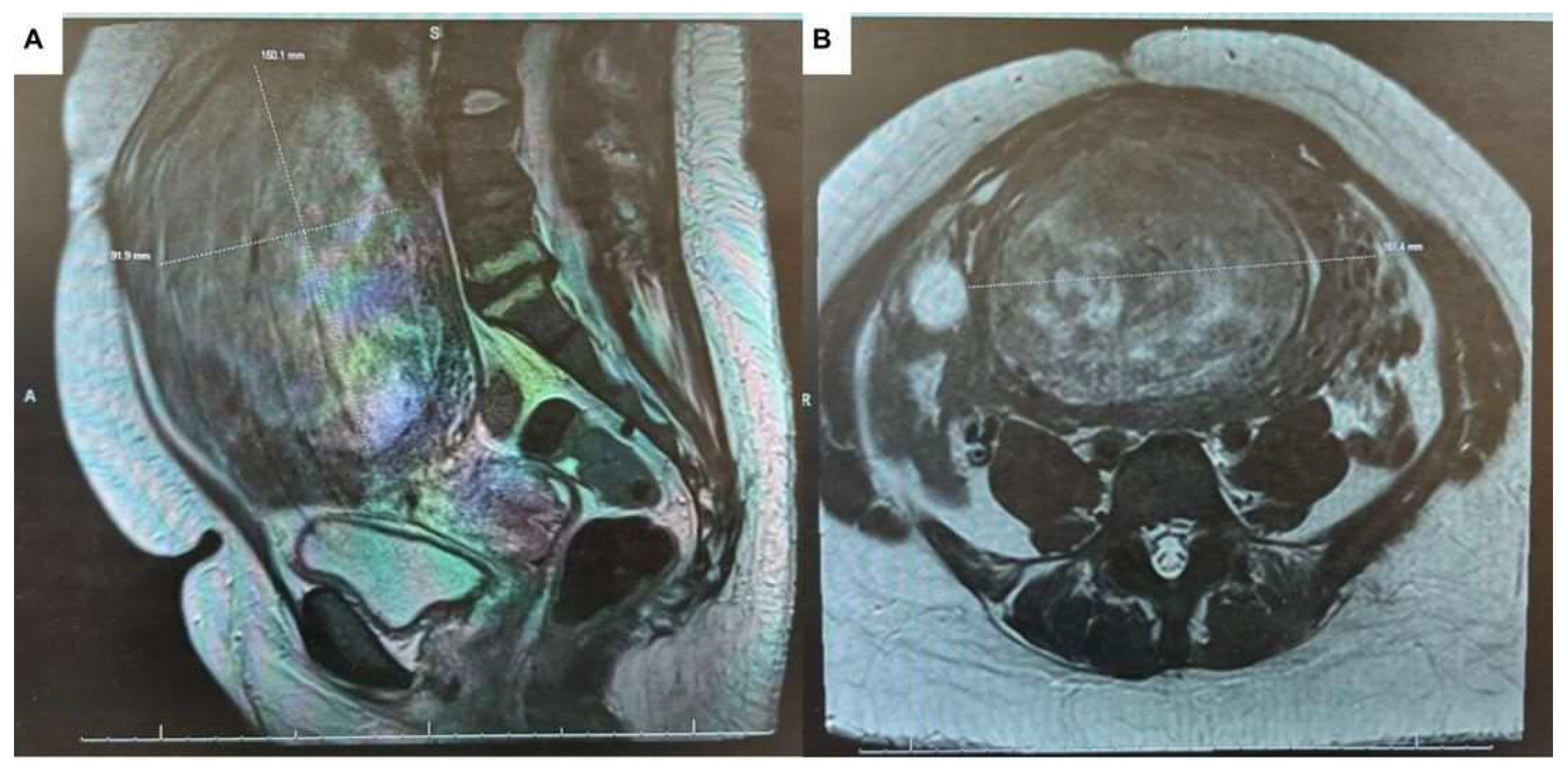

Table 1.
This table shows venous blood gas labs upon admission to emergency department, which show how the patient hyperventilate and hypoxemic. Suggested pulmonary embolism.
Table 1.
This table shows venous blood gas labs upon admission to emergency department, which show how the patient hyperventilate and hypoxemic. Suggested pulmonary embolism.
| Venous Blood Gas | RESULTS |
| FIO2 | 21 |
| Pat Temp | 36.7 |
| PH BG | 7.43 |
| PCO2 | 31 Low |
| PO2 | <17 Low |
| HCO3 | 21 Low |
| B.E. | -3.3 |
| % O2 Hb | 10 Low |
| O2 Sat | 10 Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



