Submitted:
24 September 2024
Posted:
25 September 2024
You are already at the latest version
Abstract
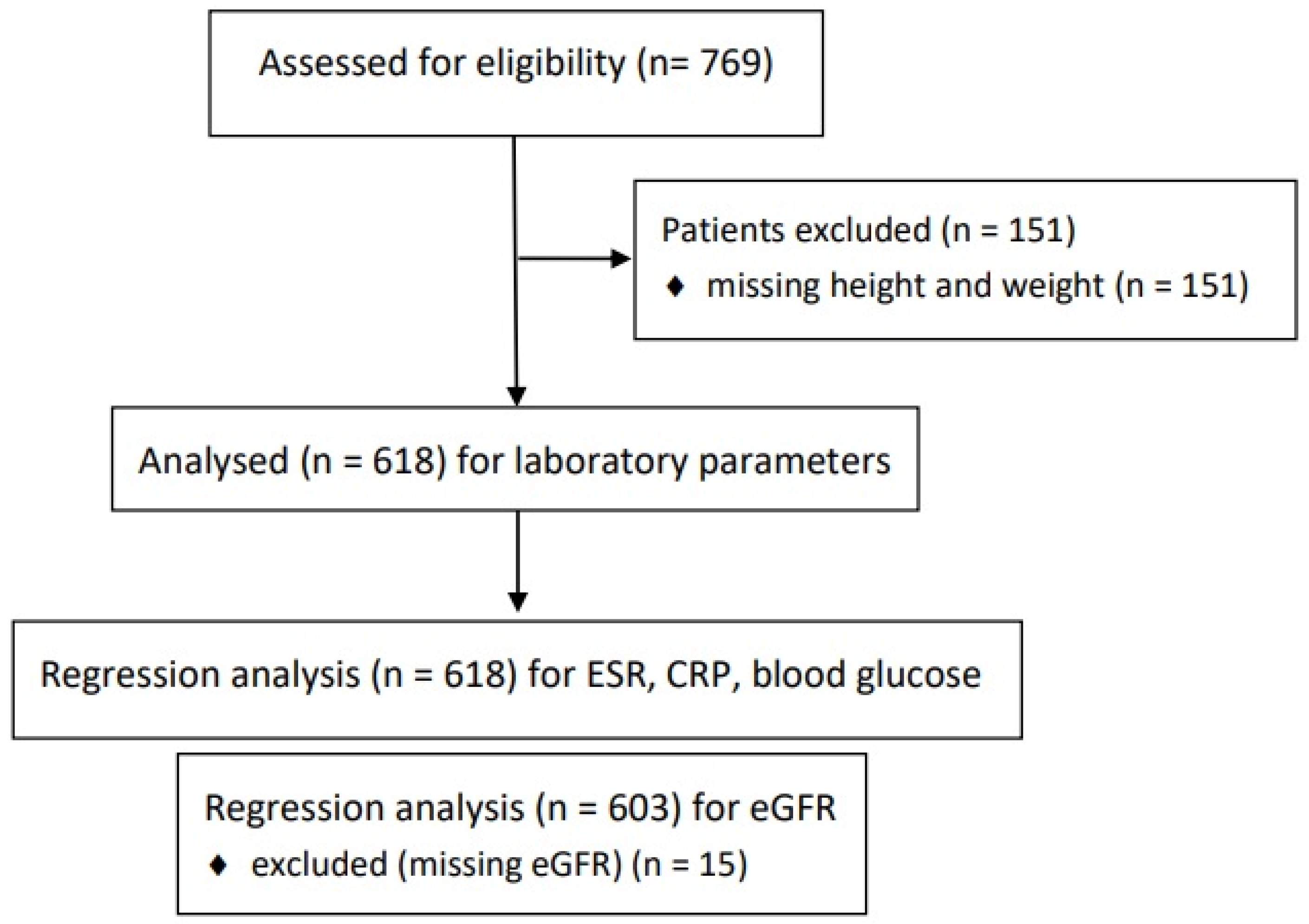
Background/Objectives: The necessity and clinical utility of routine pre-procedural blood tests (PBTs) before neuraxial blockade remain controversial. This study evaluates the effectiveness of PBTs in identifying clinically significant conditions in an outpatient setting. Methods: This single-center retrospective study involved patients who received neuraxial blockade from January 2020 to August 2023. We extracted medical information and laboratory data from the electronic medical records during the pre-procedural period. Through multivariate regression analysis, we identified patient factors associated with abnormal laboratory results. Results: Advanced age (OR, 1.021; p = 0.026) and a history of cancer (OR, 2.359; p = 0.016) were significantly associated with elevated CRP levels (>0.30 mg/dL). Severe hyperglycemia (≥200 mg/dL) was found in 24 patients (3.88%), with a history of cancer being a strong predictor (OR, 6.764; p < 0.001). No significant abnormalities were observed in PT or PTT. Reduced eGFR (<60 mL/min/1.73m²) was detected in 8.62% of patients, despite no prior history of renal dysfunction. Multivariate analysis revealed that advanced age, hypertension, cancer, and coronary artery disease were significant predictors of abnormal PBT results, highlighting the importance of selective testing in high-risk patients. Conclusions: Routine PBTs are not universally required for all patients undergoing neuraxial blockade but can provide crucial information in high-risk populations. A selective testing approach based on individual risk factors is recommended to optimize patient safety and resource utilization. Future studies should aim to establish clear guidelines for targeted PBT use.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. WBC, ESR, CRP
3.2. Glucose
3.3. PLT, PT/PTT
4. Discussion
4.1. WBC, ESR, CRP
4.2. Glucose
4.3. PLT, PT/PTT
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edwards AF, Forest DJ. Preoperative Laboratory Testing. Anesthesiol Clin. 2018;36(4):493-507.
- Apfelbaum JL, Connis RT, Nickinovich DG, Pasternak LR, Arens JF, Caplan RA, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116(3):522-38.
- Benarroch-Gampel J, Sheffield KM, Duncan CB, Brown KM, Han Y, Townsend CM, Jr., et al. Preoperative laboratory testing in patients undergoing elective, low-risk ambulatory surgery. Ann Surg. 2012;256(3):518-28.
- Bauer ME, Arendt K, Beilin Y, Gernsheimer T, Perez Botero J, James AH, et al. The Society for Obstetric Anesthesia and Perinatology Interdisciplinary Consensus Statement on Neuraxial Procedures in Obstetric Patients With Thrombocytopenia. Anesth Analg. 2021;132(6):1531-44.
- Breivik H, Norum H, Fenger-Eriksen C, Alahuhta S, Vigfusson G, Thomas O, et al. Reducing risk of spinal haematoma from spinal and epidural pain procedures. Scand J Pain. 2018;18(2):129-50.
- Jane, C. Ballantyne SMF, James P. Rathmell. Bonica’s Management of Pain. Fifth edition ed. Jane C. Ballantyne NB, DavidJ. Copenhaver. Emad N. Eskandar, editor. Philadelphia: Lippincott Williams & Wilkins, a Wolters Kluwer business; 2019.
- Long B, Carlson J, Montrief T, Koyfman A. High risk and low prevalence diseases: Spinal epidural abscess. Am J Emerg Med. 2022;53:168-72.
- Hutter, C.D. Face masks, spinal anaesthesia and meningitis. Anaesthesia. 2008;63(7):781-2; author reply 2.
- Gimeno AM, Errando CL. Neuraxial Regional Anaesthesia in Patients with Active Infection and Sepsis: A Clinical Narrative Review. Turk J Anaesthesiol Reanim. 2018;46(1):8-14.
- Berrios-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017;152(8):784-91.
- Sproston NR, Ashworth JJ. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front Immunol. 2018;9:754.
- Landry A, Docherty P, Ouellette S, Cartier LJ. Causes and outcomes of markedly elevated C-reactive protein levels. Can Fam Physician. 2017;63(6):e316-e23.
- Lim S, Yoo YM, Kim KH. No more tears from surgical site infections in interventional pain management. Korean J Pain. 2023;36(1):11-50.
- Akhtar S, Barash PG, Inzucchi SE. Scientific principles and clinical implications of perioperative glucose regulation and control. Anesth Analg. 2010;110(2):478-97.
- Stout A, Friedly J, Standaert CJ. Systemic Absorption and Side Effects of Locally Injected Glucocorticoids. Pm r. 2019;11(4):409-19.
- Younes M, Neffati F, Touzi M, Hassen-Zrour S, Fendri Y, Béjia I, et al. Systemic effects of epidural and intra-articular glucocorticoid injections in diabetic and non-diabetic patients. Joint Bone Spine. 2007;74(5):472-6.
- Even JL, Crosby CG, Song Y, McGirt MJ, Devin CJ. Effects of epidural steroid injections on blood glucose levels in patients with diabetes mellitus. Spine (Phila Pa 1976). 2012;37(1):E46-50.
- Hao C, Yin J, Liu H, Cheng Z, Zeng Y, Jin Y. Pain Reduction and Changes in Serum Cortisol, Adrenocorticotropic Hormone, and Glucose Levels after Epidural Injections With Different Doses of Corticosteroid. Pain Physician. 2024;27(1):E119-e29.
- Liu XH, Du YM, Cong HJ, Liu GZ, Ren YE. Effects of Continuous Epidural Injection of Dexamethasone on Blood Glucose, Blood Lipids, Plasma Cortisol and ACTH in Patients With Neuropathic Pain. Front Neurol. 2020;11:564643.
- Li W, Zhang X, Sang H, Zhou Y, Shang C, Wang Y, et al. Effects of hyperglycemia on the progression of tumor diseases. J Exp Clin Cancer Res. 2019;38(1):327.
- Manchikanti L, Malla Y, Cash KA, Pampati V, Hirsch JA. Comparison of effectiveness for fluoroscopic cervical interlaminar epidural injections with or without steroid in cervical post-surgery syndrome. Korean J Pain. 2018;31(4):277-88.
- Neal JM, Barrington MJ, Brull R, Hadzic A, Hebl JR, Horlocker TT, et al. The Second ASRA Practice Advisory on Neurologic Complications Associated With Regional Anesthesia and Pain Medicine: Executive Summary 2015. Reg Anesth Pain Med. 2015;40(5):401-30.
- Shams D, Sachse K, Statzer N, Gupta RK. Regional Anesthesia Complications and Contraindications. Clin Sports Med. 2022;41(2):329-43.
- Narouze S, Benzon HT, Provenzano D, Buvanendran A, De Andres J, Deer T, et al. Interventional Spine and Pain Procedures in Patients on Antiplatelet and Anticoagulant Medications (Second Edition): Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Reg Anesth Pain Med. 2018;43(3):225-62.
- Breivik H, Bang U, Jalonen J, Vigfusson G, Alahuhta S, Lagerkranser M. Nordic guidelines for neuraxial blocks in disturbed haemostasis from the Scandinavian Society of Anaesthesiology and Intensive Care Medicine. Acta Anaesthesiol Scand. 2010;54(1):16-41.
- Weil IA, Seicean S, Neuhauser D, Schiltz NK, Seicean A. Use and Utility of Hemostatic Screening in Adults Undergoing Elective, Non-Cardiac Surgery. PLoS One. 2015;10(12):e0139139.
- Mooney JF, Ranasinghe I, Chow CK, Perkovic V, Barzi F, Zoungas S, et al. Preoperative estimates of glomerular filtration rate as predictors of outcome after surgery: a systematic review and meta-analysis. Anesthesiology. 2013;118(4):809-24.
- Lagerkranser, M. Neuraxial blocks and spinal haematoma: Review of 166 case reports published 1994-2015. Part 1: Demographics and risk-factors. Scand J Pain. 2017;15:118-29.
- Benzon HT, Maus TP, Kang HR, Provenzano DA, Bhatia A, Diehn F, et al. The Use of Contrast Agents in Interventional Pain Procedures: A Multispecialty and Multisociety Practice Advisory on Nephrogenic Systemic Fibrosis, Gadolinium Deposition in the Brain, Encephalopathy After Unintentional Intrathecal Gadolinium Injection, and Hypersensitivity Reactions. Anesth Analg. 2021;133(2):535-52.
- Chen TK, Knicely DH, Grams ME. Chronic Kidney Disease Diagnosis and Management: A Review. Jama. 2019;322(13):1294-304.

| Total no. of patients | N = 618 |
|---|---|
| Age (years), mean Height Weight BMI Sex, M/F (%) Diagnosis for blocks Cervical pathology, n (%) Thoracic pathology, n (%) Lumbosacral pathology, n (%) Herpes zoster, n (%) Postherpetic neuralgia, n (%) Others, n (%) NRS Comorbidities None, n (%) HTN, n (%) DM, n (%) CAOD or arrhythmia, n (%) Cancer, n (%) CRI, n (%) |
63.78 ± 13.45 162.36 ± 9.20 63.87 ± 10.92 24.18 ± 3.26 288/330 (46.6%) 83 (13.4%) 15 (2.4%) 375 (60.7%) 94 (15.2%) 19 (3.1%) 32 (5.2%) 62.15 ± 18.26 288 (46.6%) 262 (42.4%) 96 (15.5%) 65 (10.5%) 44 (7.1%) 10 (1.6%) |
| Test type (normal value) | Number of abnormal results |
|---|---|
| Hemoglobin (13.0~17.0 g/dL) 10.0 ~ 13.0 8.0 ~ 10.0 White blood cell (4.0~10.0 × 109/L) >10 < 4 Platelet (140~440 × 109/L) 70~100 <70 ESR (0~20 mm/h) > 20 CRP (< 0.30 mg/dL) > 0.3~10 Glucose (70~110 mg/dL) ≥ 140 ≥ 200 eGFR (> 90 mL/min/1.73m2) < 60 < 30 AST (~40 U/L) > 40 ALT (~41 U/L) > 41 Sodium (136~145 mmol/L) >145 Potassium (3.5~5.1 mmol/L) ≥ 5.5 PT (10.0 ~ 13.5 sec) ≥ 14 INR (0.80~1.20 %) 1.2 ~ 1.4 > 1.4 aPTT (21~35 sec) > 35 |
134 13 43 19 4 1 76 93 96 25 59a 3a 39 80 5 8 8 6 0 2 |
| Past History | WBC | ESR | CRP | eGFR | AST | ALT | Glucose | Na | K | Diagnosis | Additional Diagnosis | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M/82 | None | 6.88 | 20 | 10.20 | >90 | 23 | 27 | 196 | 135 | 4.1 | PHN | Pneumonia |
| F/56 | Cancer | 11.7 | 50 | 9.04 | >90 | 19 | 12 | 136 | 127 | 3.6 | L | Non-tuberculous mycobacterium |
| M/84 | HTN DM |
10.34 | 43 | 6.27 | 55 | 19 | 10 | 86 | 141 | 4.0 | L | Polymyalgia rheumatica |
| F/72 | HTN CAOD CRI |
11.21 | 86 | 5.31 | 50 | 23 | 18 | 50 | 137 | 5.0 | L | Acute pyelonephritis |
| M/47 | None | 11.47 | 36 | 13.23 | >90 | 14 | 19 | 100 | 137 | 3.8 | C | Infectious spondylitis |
| F/55 | None | 8.67 | 16 | 0.29 | >90 | 152 | 301 | 99 | 137 | 4.4 | Hz | Drug induced hepatitis |
| M/52 | None | 8.14 | 8 | 0.05 | >90 | 14 | 27 | 452 | 134 | 5.0 | L | Diabetic neuropathy |
| M/39 | None | 4.33 | 6 | 0.03 | >90 | 17 | 20 | 504 | 129 | 5.1 | L | Diabetic neuropathy |
| M/64 F/85 |
HTN DM HTN DM CAOD |
8.99 7.08 |
17 26 |
0.16 0.21 |
12 27 |
37 31 |
20 20 |
164 125 |
135 140 |
8.2 5.0 |
L L |
Chronic renal failure CRI |
| ESR (> 20 mm/h) |
CRP (> 0.30 mg/dL) |
Glucose (≥ 200 mg/dL) |
eGFR (< 60 mL/min/1.73m2) |
|||||
|---|---|---|---|---|---|---|---|---|
| OR | 95 % CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Advanced age | 1.037 | 1.015-1.059 | 1.021 | 1.002-1.040 | 1.101 | 1.067-1.136 | ||
| Comorbidities | ||||||||
| HTN | 2.153 | 1.188-3.905 | ||||||
| DM | 14.352 | 5.446-37.825 | ||||||
| CAOD or arrhythmia | 3.306 | 1.751-6.230 | ||||||
| Cancer | 2.359 | 1.174-4.739 | 6.764 | 2.261-20.213 | 2.917 | 1.194-7.122 | ||
| CRI | 4.013 | 1.083-14.875 | * | * | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



