
Submitted:
05 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Macular pigment optical density (MPOD) is an important clinical biomarker for ocular conditions like macular degeneration, diabetic eye disease, and digital eye strain. Additionally, its measurements can be essential in health assessment for visual function, systemic diseases, and brain health. We aimed to assess the repeatability, agreement, and effects of the learning curve of the new portable handheld heterochromatic flicker photometer, Zx Pro, in measuring MPOD in a wide age range of ocular-healthy adults, compared to the MPOD measurements obtained using the clinically available QuantifEye device. Seventy-six participants performed one practice at-tempt and two study-related MPOD measurements with the Zx Pro and the QuantifEye. The Pearson correlation between the study-related MPOD measurements for Zx Pro and QuantifEye devices was 90% and 85%, respectively. Altman and Bland plots show excellent agreement between the device's MPOD data, with 95% limits of an agreement being -0.10 to +0.11 du. The mean difference between the practice attempt and the study-related measurements was not statistically significant for Zx Pro but was significant for QuantifEye (Repeated measures ANOVA p=0.325 and p=0.015, respectively). The Zx Pro provides excellent repeatable MPOD measurements, has an insignificant learning curve, and is in good agreement with the predicate device.
Keywords:
macular pigment optical density
; heterochromatic flicker photometry
; carotenoids
; lutein
; zeaxanthin
; meso-zeaxanthin
; macular degeneration
1. Introduction
The dietary xanthophyll carotenoids lutein and zeaxanthin, along with an isomer of zeaxanthin, meso-zeaxanthin, collectively comprise the macular pigment, which is observed as a central yellow spot in fundus evaluation[1,2]. While not visualizable using ophthalmoscopy or retinal photography, xanthophylls are present in lower amounts throughout the retina and have an integral role in the visual function and maintenance of retinal health [1,2,3,4]. Xanthophylls carotenoids serves as the eye’s inherent antioxidant capacity that protects the eye from harmful radiation, quenching free radicals generated during metabolism and benefitting visual function by optical and non-optical mechanisms[3]. The carotenoids in the human body cannot be synthesized de novo and are obtained by diet. There are indeed various dietary sources for ocular xanthophylls like are spinach, kale, swiss chard, orange peppers, asparagus, eggs etc. to name a few[5].
Heterochromatic flicker photometry (HFP) is the currently most commonly used technology in the measurement of MPOD, both clinically and in research settings [1,6,7]. The amount of xanthophyll carotenoids in the retina is measured as macular pigment optical density. Although MPOD is known popularly for its association with macular degeneration [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22], MPOD measurements are gaining significant notoriety as an oculo-systemic biomarker [23,24,25,26,27]. We now know that dietary intake of carotenoids and sub-optimal MPOD are a measurable and modifiable risk factors in numerous conditions like macular degeneration[8,9,10,11,12,13,14,15,16,17,18,19,20,21,22], diabetes [24,26,28], and retinal pathologies like glaucoma[29,30,31,32]. The level of MPOD is correlated with visual performance [8,14,17,23,28,33,34,35,36,37,38,39,40,41,42], cognitive performance [43,44,45,46,47,48,49,50], and, more recently, digital eye strain [27,51] that affects a significant part of the global population [27,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. Furthermore, macular pigment levels in the retina are highly correlated to the levels of the carotenoids in the occipital cortex[65], thus making its measurements additionally valuable for systemic and brain health[66,67]. Additionally, due to its measurement principles, the MPOD measured by the HFP is a direct assessment of the eyes’ ability to absorb blue light [6,68,69,70].
While current commercial HFP devices are easy to use, repeatable, reliable, and able to track changes in diet and intake of nutritional supplements[6,11,68,71,72,73,74,75,76,77,78,79], they are marred with being space occupying desktop units that are not portable and tend to obstruct smooth flow in busy clinical practices that see a significant number of patients daily. Recently, ZeaVision LLC made a portable, handheld HFP device available to improve the clinical usability of this technology. The current study aims to evaluate the new portable device and compare its repeatability, learning curve, and MPOD measurements with the currently commercially available HFP QuantifEye MPS II device (IDE Vision Ltd., United Kingdom). We hypothesize there should be a good correlation and agreement between the two devices despite the software and hardware differences given these both are based on principles of HFP. The outcome of this study will allow the establishment of clinically valuable protocols. It will also provide helpful information for clinicians, researchers, and aid future clinical trials in nutrition, eye care, and systemic physiology.
2. Materials and Methods
Participants were evaluated by a single trained optometric physician (PGD) at the Western University of Health Sciences, College of Optometry. The study was approved by the institutional review board at the Western University of Health Sciences, Pomona, California, USA, and conducted in accordance with the tenets of the Declaration of Helsinki (P20/IRB/060 2022). Participants signed a consent form, were adults of at least 18 years of age, and were deemed to have good ocular health during a comprehensive ocular evaluation by an optometric physician in the last year. Participants additionally underwent visual acuity assessments and refractive error estimation during the study. Participants with a history of retinal pathology, glaucoma, or history of surgery that could influence measurements were excluded. All participants had a logMAR visual acuity of +0.01 (20/25) or better.
A total of 76 eyes of 76 participants were included in the study. The mean age of
study participants was 33.9 years (standard deviation 11.57; range 23–70 years).
The median spherical refractive error for the study participants was -1.68 D (range +0.50 to -7.00D). All participants were novice observers who were not experienced in the heterochromatic flicker photometry (HFP) procedure to measure MPOD.
2.1. Macular Pigment Optical Density (MPOD) Measurement
The MPOD was assessed using two devices, the QuantifEye MPS II and the Zx Pro device. The fundamental principles of these two devices are based on HFP[1,11,69,70,72,78,80]. They both measure the MPOD in the central 1 degree of the macula. The HFP devices measure the macular pigment optical density by measuring the retinas’ ability to absorb the blue spectra that are converted to density units. During the testing participants were instructed to pay attention to a single target or spot. An individual undergoing the testing for an eye was directed to look at a target, which is a single light source, and asked to maintain the position throughout the test. The fellow eye not being examined was patched to ensure the eyes’ steady fixation and avoid binocular rivalry. At this point, the light source illuminates the center of the fovea around 1 degree.
The HFP is based on the principle that when the blue and green spectral targets are projected in rapid succession to the retina, the individual experiences the target flickering. Individuals performing the test are instructed to press a trigger whenever they see the target flickering. This flicker is sometimes reported and better understood as shimmer or static. Subsequently, the computer changes the blue versus green ratio, to which the target appears flickering. The test continues for approximately two minutes with a decreasing blue-to-green ratio. When the retina absorbs the maximum blue light, the individual will not perceive the flicker. The testing continues three more times where the amount of blue is higher than that absorbed by the fovea, which the individual perceives and responds to the flicker. These devices yield a score ranging from 0 to 1, with 1 being the maximum MPOD score possible. The MPOD values are adjusted for the age-related yellowing of the lens. Although not applicable to the current study, individuals who have undergone cataract extraction with intraocular lens implantation have clear media, and their age should be recorded at 21 years where no age-related adjustment is required.
The fundamental principles of these two devices are based in HFP, however, there are significant hardware and software differences between the devices that could cause variation and differences in the MPOD measurements obtained by both devices. To avoid any systematic bias in testing, the measurements of MPOD were performed in a randomly selected eye of the participant, and each participant performed the MPOD testing three times with both devices. The testing sequence was also randomized, and at least a two-minute break was provided after a set of MPOD measurements. Participants performed MPOD measurements three times after instructions. The first set of measurements was used to evaluate the learning curve and the second and the third measurements were used to assess repeatability and agreement.
2.2. QuantifEye MPS II
QuantifEye MPS II (QuantifEye) was utilized as the predicate device to which the new device data were compared. Comprehensive details about the QuantifEye technology, its repeatability, and its agreement with other research prototypes can be obtained from elsewhere[11,69,70,72,78,80]. Participants were instructed and prepared to take the test as explained above.
2.3. Zx Pro - A new handheld heterochromatic flicker photometer
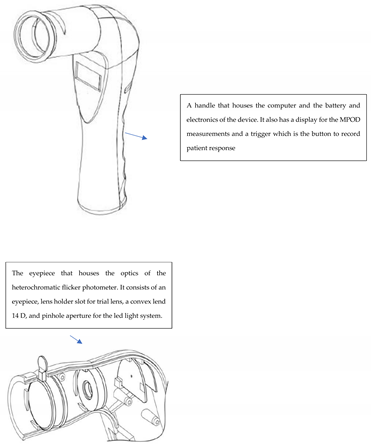
The new device, known as the Zx Pro (ZeaVision LLC, Chesterfield, MO) is a device that measures macular pigment optical density (MPOD) and is based on the principles of HFP (explained above). The Zx Pro is a portable handheld device with audio prompts to guide the process of testing. Its body includes a lower handheld portion and an eyepiece viewing tube, which is positioned transversely to the lower handheld portion (see schematic Appendix-1). The handheld portion consists of a user input button, an LCD display for showing the MPOD score, and the battery and instrument electronics. The viewing tube terminates in an eye cup and includes the light sources. The device also has the ability to place a refractive lens to correct individual refractive errors.
2.4. Differences between the MPOD measuring instruments.
The Zx Pro is a portable handheld device that an individual can use in a naturally seated position, whereas the QuantifEye is a desktop device that requires hunching over a table to view the target. The smaller handheld design changes the optical requirements, and the Zx Pro uses a 14-diopter lens compared to the 5-diopter lens used in the QuantifEye MPOD desktop device. To expedite the test, the Zx Pro proactively changes the starting frequency based on the user’s previous perceived frequency. This adaptive approach reduces the time required for the user to perceive the flicker, enhancing test efficiency. Prior to calculating the MPOD score, the Zx Pro performs a secondary check on the minimum perceived frequency. This additional verification step is designed to enhance the accuracy and reproducibility of the MPOD score, and in turn, shorten the learning curve.
2.5. Sample Size Estimation
Prior studies that have evaluated the repeatability have utilized a sample size of 23 to 72 subjects[7,11,69,70,72]. For the correlation analysis, a two-tailed analysis setting the alpha and beta error at 1% and an expected correlation coefficient of 0.7, with a sample size of 28, was deemed sufficient to obtain statistical significance. Further, to detect a significant difference of 0.02 du between measurements, an alpha error of 5%, and a power of 90%, a sample size of 58 was calculated as sufficient to detect significance.
3. Results
The mean and standard deviation of all MPOD measurements are provided in the table below.

Table 1.
MPOD measurements obtained using the QuantifEye and the Zx Pro.
| Mean MPOD1 measurements |
Practice attempt | Study Attempt-1 |
Study Attempt- 2 |
Repeated measures ANOVA p-value |
|---|---|---|---|---|
| QuantifEye | 0.441 (0.16) | 0.452 (0.16) | 0.430 (0.14) | 0.015 |
| Zx Pro | 0.459 (0.15) | 0.447 (0.15) | 0.444 (0.15) | 0.325 |
1 MPOD stands for Macular pigment optical density, and measurements were performed in 76 eyes of 76 individuals. The values in parenthesis are standard deviations.
3.1. Repeatability of MPOD measures QuantifEye MPS II
Figure 1 provides the Pearson correlation scatter plot for the MPOD measurements obtained using the two study measurements of QuantifEye. As expected, there was a positive linear correlation with minimal scatter representing physiological variability. The correlation coefficient between the study measurements of MPOD was excellent and statistically significant with an r-square of 0.846 (t-statistic 20.05, p<0.0001) which signifies an 84.6% correlation between two measurements. Figure 2 provides the Altman and Bland plots of agreement between the first and second measurements; the 95% of the limits of the agreement being -0.142 to +0.098. There was a tendency for the second measurement to be higher than the first one at lower MPOD scores (t-statistic -3.18, p=0.002).
3.2. Repeatability of MPOD measures using Zx Pro
Figure 3 provides the Pearson correlation scatter plot for the MPOD measurements that were obtained using the second set of Zx Pro measurements. As expected, there was a linear correlation with minimal scatter representing physiological variability. The correlation coefficient between the first and the second MPOD measurements was excellent and statistically significant with an r-square 0.900 (t-statistic 25.87, p<0.0001), which signifies a 90% correlation between the two measurements. Figure 4 provides the Altman and Bland agreement plots between the first and second measurements. The mean difference, as examined by bias analysis, was -0.008, which was not significant (t-statistic=-1.14, p=0.26). The 95% limits of agreement were -0.133 to +0.116
3.3. Comparison of repeatability between the QuantifEye and Zx Pro
Table 2 provides the descriptive statistics of the differences between the first and the second study measurements. Examining the difference range in first and second measurements obtained with both the devices, we find that the Zx Pro is marginally superior to the predicate device QuantifEye.
To further explore the difference in repeatability, we evaluated the coefficient of variation and the statistical significance between the difference in the first and second study measurements obtained using both devices. The coefficient of variation is calculated as the standard deviation of the difference in the first and second measurements divided by the means of measurement. The coefficient of variation between the first and second measurements of QuantifEye was 0.138, whereas the Zx Pro values were 0.104, indicating a relatively superior performance.
We performed a repeated measures ANOVA with contrasts to evaluate the learning curve in measured MPOD by different devices. As seen in Table 1, comparing the data obtained using the QuantifEye, we find that there is a small yet statistically significant difference between the practice attempt and the study-related measurements 1 and 2 (Repeated measures ANOVA p=0.015). The paired samples t-test was performed to evaluate the differences between the groups. Although the difference in the practice attempts was not clinically significant when compared to the study measures, the mean difference between the two study-related measurements, 1 and 2, was 0.022 du, which reached statistical significance (paired samples t-test p values 0.21, 0.10, and 0.002 respectively). The mean MPOD obtained using the Zx Pro was not different when evaluated as a group (repeated measures ANOVA p=0.325) and with paired comparisons (paired samples t- test p=0.44,0.20 and 0.26 respectively). This analysis indicates that there is a small yet statistically significant learning curve with QuantifEye, whereas the Zx Pro does not have any significant learning curve.
3.4. Agreement between QuantifEye and Zx Pro MPOD measures
The Altman and Bland analysis were performed to evaluate the agreement between the predicate device QuantifEye, and the new device Zx Pro. Table 2 provides the mean bias and 95% limits of agreement between the device’s first measurement, second, and average data. The limits of agreement are narrow, and a bias value of close to zero in all three analysis indicates there is no systematic bias between the devices (see Figure 5 A, B, and C)
Table 3.
Agreement analysis.
| Altman and Bland analysis |
The mean difference between QuantifEye and Zx Pro |
95% limits of agreement |
|---|---|---|
| Study attempt-1 | -0.006 | -0.14 to + 0.14 |
|
Study attempt-2 Mean of Attempts 1 &2 |
+0.013 +0.006 |
-0.10 to + 0.13 -0.101 to + 0.113 |
3.5. Predicting Zx Pro MPOD measures from QuantifEye data
Given that the QuantifEye heterochromatic flicker photometry is clinically utilized, and numerous patients are followed up using the technology, it becomes essential to have a conversion factor to aid the clinical transition to new technology. We used regression analysis to analyze the scatter plots and the Goodness of fit to evaluate the observed versus predicted values. We assessed a total of five regression models that included exponential, linear, logarithmic, polynomial, and power. Of the various models investigated, a linear regression analysis provided the best Goodness of fit to the model. Using the linear regression analysis, one can expect to predict Zx Pro data with an accuracy of 86.4%.
Zx Pro MPOD = 0.915 X QuantifEye MPOD + 0.0434
4. Discussion
Carotenoids are an essential part of the human diet, and xanthophylls that are concentrated in the retina and neural elements seem to have a much bigger role to play than previously recognized[1,3,16,25,26,27,28,36,37,44,51,78,79,81,82,83]. The xanthophyll carotenoids lutein, zeaxanthin and its isomers accumulate at different layers in the retina, and in the fovea centralis, a significant deposit is visually identifiable[1,84]. Measurement of this region provides the MPOD of a person’s eye, and the level of the MPOD is associated with and an indicator of ocular health, systemic health, and disease states in both. MPOD is particularly interesting as it is a modifiable biomarker that can be increased with improved diet or nutritional supplementation[8,9,10,14,16,19,21,22,25,26,27,34,41,42,50,85,86,87,88,89,90]. The accurate and reliable measurement of such biomarkers is paramount, and prior-generation devices like the QuantifEye HFP have been shown to be repeatable and valid at measuring changes in MPOD over time[6,7,21,22,41,42,72,74,91,92,93].
Despite the seeming clinical acceptance of such technology, the widespread use of HFP devices has been limited due to various reasons. Some of the shortcomings of prior technology were the relatively larger footprint in the clinic, its lack of portability, and its ease of use. With these shortcomings in mind, the Zx Pro was introduced, which was portable, handheld, and convenient for individuals to perform the test in their natural seated position. This study evaluated the new technology Zx Pro, and we found that the device provides MPOD measurements that are repeatable and in good agreement with the predicate device. The limits of agreement between Zx Pro and the predicate device QuantifEye are narrow, and no systematic bias was observed in the measurements.
Further we find that the Zx Pro provides a shorter learning curve compared to the predicate device QuantifEye. The learning curve is an essential issue for all psychophysical tests. The mean difference between the practice attempt and the study-related measurements of QuantifEye MPOD was 0.022. Although such small differences may not be considered clinically significant, the learning curve is statistically significant. Compared to the predicate technology QuantifEye, the Zx Pro provides data that are not significantly affected by such learning-related effects. Multiple reasons could explain the difference in the learning curve and the slightly superior reproducibility of Zx Pro. The portable handheld nature of the device allows for a more comfortable testing environment, and the software-related differences in identifying the endpoint of the tests may account for the superior performance of Zx Pro.
This study also provides a conversion equation that will allow clinicians to predict Zx Pro results using the QuantifEye measurements with an accuracy of 86.4%. It will be helpful for physicians that are used to seeing the QuantifEye MPOD to transition to Zx Pro and aid clinical decisions.
Additionally, we also evaluated repeatability by assessing the coefficient of variation. The coefficient of variation is a very important metric in assessing the clinical accuracy of a device. Our prior studies[7,72] that have evaluated the coefficient of variation of HFP devices have reported a value of 11-13% and other investigators have reported similar values[6,69,70,77,78]. We find that in this study the coefficient of variation of QuantifEye is around 14% which is comparable to prior published literature. The Zx Pro has better repeatability when compared to the QuantifEye, with a coefficient of variation of 10%. This value is of paramount clinical utility as it can provide a clinically measurable endpoint. An increase of 10% increase in MPOD from baseline as measured by Zx Pro can be considered a “true” improvement and not a random function of “noise or chance.”
It is known that due to age-related absorption changes in the human crystalline lens, an error is introduced which leads to an overestimation of MPOD in older adults[68,69,78,94,95]. Two methods have been utilized to overcome this error in measurements. Research laboratories use elaborate techniques of measuring central and peripheral measures, and the subtraction of two provides an internal control and accounting for the age-related yellowing of the lens[96,97,98]. The problem with this technique is that it is incredibly laborious, time-consuming, and prone to further errors in measurement. The second technique that clinicians can utilize is the built-in age-related correction of MPOD due to the age-related lens absorption changes. This technique requires the age to input as a first step and the subsequent measurement of MPOD which yields better estimates of MPOD. This technique makes the MPOD measurements easier and shortens the testing time compared to the research laboratory techniques. For individuals who show a sudden decrease in visual acuity or exaggeration of cataracts, the MPOD measurements should be evaluated with caution, and the cases that had cataract extraction the age permanently set to twenty-one.
Numerous studies have shown the importance of MPOD as a biomarker in health and disease states. Thus, it is important to discuss various methods of measuring the carotenoid status, particularly its direct or indirect relations with the MPOD levels. Carotenoids can also be measured using high-performance liquid chromatography (HPLC), which is considered the laboratory standard[99]. HPLC destroys the tissue and sample completely and cannot be performed in vivo in live patient eyes. HPLC can be performed to measure carotenoids in blood samples. This is a relatively expensive test and requires phlebotomy. Furthermore, the samples require specialized handling in laboratories, including storage in a dark environment and refrigeration at very low temperatures, usually negative 20 degrees Celsius. The measurement of blood levels of carotenoids tends to be more susceptible to recent dietary intake trends of carotenoids, is an indirect estimate of MPOD, and a weak correlation to an individual’s MPOD[99].
Total carotenoids can be objectively measured in the skin; these non-invasive and rapid tests are based on the principles of Raman spectroscopy[100,101,102] or Reflection spectroscopy[103,104,105], measure overall carotenoid levels of the skin, and may have a role in the assessment of carotenoids systemically. These devices have limitations and are susceptible to measurement-related issues like measuring consistently at the exact location measured previously and possibly to short-term variations like exposure to sunlight. Additionally, skin has numerous carotenoids and its metabolites[106], whereas the eye has only two dietary carotenoids, lutein and zeaxanthin and a metabolite meso-zeaxanthin[3]; one would not expect the skin carotenoid composite scores to correlate well with MPOD which is primarily zeaxanthin, meso-zeaxanthin and lutein. Human skin biopsy studies and analysis with HPLC have shown lutein and zeaxanthin compromise around three percent of total carotenoids in the skin[107]. A recent study has shown that skin carotenoid composite score by Refection Spectroscopy have a very weak correlation to MPOD (0.6%) and thus cannot predict the carotenoid status in the eye[108].
The HFP is a direct measurement of MPOD but a subjective technique that requires active input from the patient[6,7,11,13,14,21,22,34,36,37,40,41,42,43,68,69,70,71,72,75,77,78,79,86,92,93,109,110,111,112,113,114]. Although this technique appears simple and can be performed in a couple of minutes, it has the limitation of needing a response from the participants, which may be challenging to some. An ideal device would be one that can measure MPOD directly and easily and does not require any input or cooperation from the patients. Other research devices can measure MPOD either directly or indirectly, like autofluorescence techniques[88,115], Raman spectroscopy[116,117], or reflectometry[6,7,70,91,93]. These devices are standalone or require to be coupled with sophisticated equipment that is not commonly available. Some of these techniques are significantly affected by media opacities, possibly requiring dilation of pupils[118,119,120]. Although such devices have been available in the research realms for about two decades, they have not become clinically available for various reasons. Cost plays a huge role in these devices not being available, costing 100-300 thousand US dollars. Currently, there are no objective techniques to measure MPOD that are commercially available and that the Food and Drug Administration has approved. The HFP has established itself as the clinical gold standard, and its lower cost, ease of use, and numerous validations from various research studies should see this technology bring MPOD as an essential biomarker in various general and specialty clinics.
5. Conclusions
This study evaluated the new portable heterochromatic flicker photometer Zx Pro and its ability to measure MPOD in a group of novice participants who ranged widely in age and refractive error. The results show that despite the devices being subjective in nature and requiring active subject participation, they are capable of producing repeatable MPOD scores with a minimal learning curve and are in good agreement with the values obtained with a predicate device, QuantifEye.
Author Contributions
“Conceptualization, PGD, JP, FS, RBR, DLG; methodology, PGD FS; formal analysis, PGD; investigation, PGD; resources, PGD, DLG; data curation, PGD; writing—original draft preparation, PGD; writing—review and editing, PGD, RBR, JP, FS, DLG; supervision, PGD; project administration, PGD; funding acquisition, PGD. All authors have read and agreed to the published version of the manuscript.”
Funding
The study was funded with an unrestricted grant to the Western University of Health Sciences to investigate the currently available MPOD devices (WesternU Grant # 25222-1397).
Institutional Review Board Statement
The study was approved by the institutional review board at Western University of Health Sciences, Pomona, California, USA, and conducted in accordance with the tenets of the Declaration of Helsinki (P20/IRB/060 2022). All participants signed an informed consent form.
Data Availability Statement
Available upon request after data sharing agreement is mutually acceptable.
Acknowledgements
This study’s findings were presented as a poster at ARVO 2024, and the authors would like to thank Keiko Inouye for her assistance with poster preparation.
Conflicts of Interest
Pinakin Davey is a tenured full professor and full-time faculty at the Western University of Health Sciences and holds an adjoint appointment and is an Employee at EyePromise. Joshua Park has a patent on measurement of MPOD. Dennis L. Gierhart is the Chairman of EyePromise, manufacturer of various nutritional supplements and Zx Pro. Richard Rosen and Frank Spors None. The funders had no role in the study’s design, data collection, analysis, or interpretation, manuscript writing, or decision to publish the results.
Appendix 1: Schematic of the handheld heterochromatic flicker photometer Zx Pro
References
- Bernstein, P.S.; Delori, F.C.; Richer, S.; van Kuijk, F.J.; Wenzel, A.J. The value of measurement of macular carotenoid pigment optical densities and distributions in age-related macular degeneration and other retinal disorders. Vision Res 2010, 50, 716–728. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Hime, G.W.; Cains, A.; Zamor, J. Stereochemistry of the human macular carotenoids. Invest Ophthalmol Vis Sci 1993, 34, 2033–2040. [Google Scholar] [PubMed]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Prog Retin Eye Res 2016, 50, 34–66. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Mayne, S.T.; Gomez, C.M.; Tibor, S.E.; Twaroska, E.E. Macular pigment in donor eyes with and without AMD: a case-control study. Invest Ophthalmol Vis Sci 2001, 42, 235–240. [Google Scholar]
- Thomas, S.E.; Johnson, E.J. Xanthophylls. Adv Nutr 2018, 9, 160–162. [Google Scholar] [CrossRef]
- Berendschot, T.T.; van Norren, D. Objective determination of the macular pigment optical density using fundus reflectance spectroscopy. Arch Biochem Biophys 2004, 430, 149–155. [Google Scholar] [CrossRef]
- Davey, P.G.; Rosen, R.B.; Gierhart, D.L. Macular Pigment Reflectometry: Developing Clinical Protocols, Comparison with Heterochromatic Flicker Photometry and Individual Carotenoid Levels. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Beatty, S.; Peto, T.; Stack, J.; Stringham, J.; Kelly, D.; Leung, I.; Corcoran, L.; Nolan, J.M. The Impact of Supplemental Antioxidants on Visual Function in Nonadvanced Age-Related Macular Degeneration: A Head-to-Head Randomized Clinical Trial. Invest Ophthalmol Vis Sci 2017, 58, 5347–5360. [Google Scholar] [CrossRef] [PubMed]
- Akuffo, K.O.; Beatty, S.; Stack, J.; Dennison, J.; O’Regan, S.; Meagher, K.A.; Peto, T.; Nolan, J. Central Retinal Enrichment Supplementation Trials (CREST): design and methodology of the CREST randomized controlled trials. Ophthalmic Epidemiol 2014, 21, 111–123. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Nolan, J.M.; Howard, A.N.; Moran, R.; Stack, J.; Klein, R.; Klein, B.E.; Meuer, S.M.; Sabour-Pickett, S.; Thurnham, D.I.; et al. Sustained supplementation and monitored response with differing carotenoid formulations in early age-related macular degeneration. Eye (Lond) 2015, 29, 902–912. [Google Scholar] [CrossRef]
- Bartlett, H.; Howells, O.; Eperjesi, F. The role of macular pigment assessment in clinical practice: a review. Clin Exp Optom 2010, 93, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Beatty, S.; Boulton, M.; Henson, D.; Koh, H.H.; Murray, I.J. Macular pigment and age related macular degeneration. Br J Ophthalmol 1999, 83, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Beatty, S.; Murray, I.J.; Henson, D.B.; Carden, D.; Koh, H.; Boulton, M.E. Macular pigment and risk for age-related macular degeneration in subjects from a Northern European population. Invest Ophthalmol Vis Sci 2001, 42, 439–446. [Google Scholar] [PubMed]
- Davey, P.G.; Henderson, T.; Lem, D.W.; Weis, R.; Amonoo-Monney, S.; Evans, D.W. Visual Function and Macular Carotenoid Changes in Eyes with Retinal Drusen-An Open Label Randomized Controlled Trial to Compare a Micronized Lipid-Based Carotenoid Liquid Supplementation and AREDS-2 Formula. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Landrum, J.T.; Bone, R.A. Mechanistic Evidence for eye disease and carotenoids; Krinsky, N.I., Mayne, S.T., Sies, H., Eds.; CRC Press: New York, NY, USA, 2004. [Google Scholar]
- Lem, D.W.; Davey, P.G.; Gierhart, D.L.; Rosen, R.B. A Systematic Review of Carotenoids in the Management of Age-Related Macular Degeneration. Antioxidants (Basel) 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Dou, H.L.; Huang, Y.M.; Lu, X.R.; Xu, X.R.; Qian, F.; Zou, Z.Y.; Pang, H.L.; Dong, P.C.; Xiao, X.; et al. Improvement of retinal function in early age-related macular degeneration after lutein and zeaxanthin supplementation: a randomized, double-masked, placebo-controlled trial. Am J Ophthalmol 2012, 154, 625–634 e621. [Google Scholar] [CrossRef]
- Ma, L.; Dou, H.L.; Wu, Y.Q.; Huang, Y.M.; Huang, Y.B.; Xu, X.R.; Zou, Z.Y.; Lin, X.M. Lutein and zeaxanthin intake and the risk of age-related macular degeneration: a systematic review and meta-analysis. Br J Nutr 2012, 107, 350–359. [Google Scholar] [CrossRef]
- Ma, L.; Liu, R.; Du, J.H.; Liu, T.; Wu, S.S.; Liu, X.H. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients 2016, 8, 426. [Google Scholar] [CrossRef]
- Ma, L.; Yan, S.F.; Huang, Y.M.; Lu, X.R.; Qian, F.; Pang, H.L.; Xu, X.R.; Zou, Z.Y.; Dong, P.C.; Xiao, X.; et al. Effect of lutein and zeaxanthin on macular pigment and visual function in patients with early age-related macular degeneration. Ophthalmology 2012, 119, 2290–2297. [Google Scholar] [CrossRef]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: the Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optometry 2004, 75, 216–230. [Google Scholar] [CrossRef]
- Richer, S.P.; Stiles, W.; Graham-Hoffman, K.; Levin, M.; Ruskin, D.; Wrobel, J.; Park, D.W.; Thomas, C. Randomized, double-blind, placebo-controlled study of zeaxanthin and visual function in patients with atrophic age-related macular degeneration: the Zeaxanthin and Visual Function Study (ZVF) FDA IND #78, 973. Optometry 2011, 82, 667–680 e666. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Jentsch, S.; Dawczynski, J.; Bohm, V. Age-related macular degeneration: Effects of a short-term intervention with an oleaginous kale extract--a pilot study. Nutrition 2013, 29, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. Management of Diabetic Eye Disease using Carotenoids and Nutrients. In Antioxidants; IntechOpen, 2021. [Google Scholar]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. Carotenoids in the Management of Glaucoma: A Systematic Review of the Evidence. Nutrients 2021, 13, 1949. [Google Scholar] [CrossRef] [PubMed]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. A Systematic Review of Carotenoids in the Management of Diabetic Retinopathy. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. Can Nutrition Play a Role in Ameliorating Digital Eye Strain? Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Chous, A.P.; Richer, S.P.; Gerson, J.D.; Kowluru, R.A. The Diabetes Visual Function Supplement Study (DiVFuSS). Br J Ophthalmol 2016, 100, 227–234. [Google Scholar] [CrossRef]
- Igras, E.; Loughman, J.; Ratzlaff, M.; O’Caoimh, R.; O’Brien, C. Evidence of lower macular pigment optical density in chronic open angle glaucoma. Br J Ophthalmol 2013, 97, 994–998. [Google Scholar] [CrossRef]
- Ji, Y.; Zuo, C.; Lin, M.; Zhang, X.; Li, M.; Mi, L.; Liu, B.; Wen, F. Macular Pigment Optical Density in Chinese Primary Open Angle Glaucoma Using the One-Wavelength Reflectometry Method. J Ophthalmol 2016, 2016, 2792103. [Google Scholar] [CrossRef]
- Siah, W.F.; Loughman, J.; O’Brien, C. Lower Macular Pigment Optical Density in Foveal-Involved Glaucoma. Ophthalmology 2015, 122, 2029–2037. [Google Scholar] [CrossRef]
- Siah, W.F.; O’Brien, C.; Loughman, J.J. Macular pigment is associated with glare-affected visual function and central visual field loss in glaucoma. Br J Ophthalmol 2018, 102, 929–935. [Google Scholar] [CrossRef]
- Beatty, S.; Chakravarthy, U.; Nolan, J.M.; Muldrew, K.A.; Woodside, J.V.; Denny, F.; Stevenson, M.R. Secondary outcomes in a clinical trial of carotenoids with coantioxidants versus placebo in early age-related macular degeneration. Ophthalmology 2013, 120, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Davey, P.G.; Roman, B.O.; Evans, D.W. Efficacy of Commercially Available Nutritional Supplements: Analysis of Serum Uptake, Macular Pigment Optical Density and Visual Functional Response. Nutrients 2020, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Corvi, F.; Souied, E.H.; Falfoul, Y.; Georges, A.; Jung, C.; Querques, L.; Querques, G. Pilot evaluation of short-term changes in macular pigment and retinal sensitivity in different phenotypes of early age-related macular degeneration after carotenoid supplementation. Br J Ophthalmol 2017, 101, 770–773. [Google Scholar] [CrossRef]
- Hammond, B.R., Jr.; Fletcher, L.M.; Elliott, J.G. Glare disability, photostress recovery, and chromatic contrast: relation to macular pigment and serum lutein and zeaxanthin. Invest Ophthalmol Vis Sci 2013, 54, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R.; Fletcher, L.M.; Roos, F.; Wittwer, J.; Schalch, W. A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Invest Ophthalmol Vis Sci 2014, 55, 8583–8589. [Google Scholar] [CrossRef]
- Huang, Y.M.; Dou, H.L.; Huang, F.F.; Xu, X.R.; Zou, Z.Y.; Lu, X.R.; Lin, X.M. Changes following supplementation with lutein and zeaxanthin in retinal function in eyes with early age-related macular degeneration: a randomised, double-blind, placebo-controlled trial. Br J Ophthalmol 2015, 99, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Loughman, J.; Akkali, M.C.; Beatty, S.; Scanlon, G.; Davison, P.A.; O’Dwyer, V.; Cantwell, T.; Major, P.; Stack, J.; Nolan, J.M. The relationship between macular pigment and visual performance. Vision Res 2010, 50, 1249–1256. [Google Scholar] [CrossRef]
- Nolan, J.M.; Loughman, J.; Akkali, M.C.; Stack, J.; Scanlon, G.; Davison, P.; Beatty, S. The impact of macular pigment augmentation on visual performance in normal subjects: COMPASS. Vision Res 2011, 51, 459–469. [Google Scholar] [CrossRef]
- Richer, S.; Devenport, J.; Lang, J.C. LAST II: Differential temporal responses of macular pigment optical density in patients with atrophic age-related macular degeneration to dietary supplementation with xanthophylls. Optometry 2007, 78, 213–219. [Google Scholar] [CrossRef]
- Richer, S.; Novil, S.; Gullett, T.; Dervishi, A.; Nassiri, S.; Duong, C.; Davis, R.; Davey, P.G. Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Wooten, B.R.; Ofori-Asare, W.; Osei Duah Junior, I.; Kumah, D.B.; Awuni, M.; Obiri-Yeboah, S.R.; Horthman, S.E.; Addo, E.K.; Acquah, E.A.; et al. Macular Pigment, Cognition, and Visual Function in Younger Healthy Adults in Ghana. J Alzheimers Dis 2023, 94, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Cannavale, C.N.; Keye, S.A.; Rosok, L.; Martell, S.; Holthaus, T.A.; Reeser, G.; Raine, L.B.; Mullen, S.P.; Cohen, N.J.; Hillman, C.H.; et al. Enhancing children’s cognitive function and achievement through carotenoid consumption: The Integrated Childhood Ocular Nutrition Study (iCONS) protocol. Contemp Clin Trials 2022, 122, 106964. [Google Scholar] [CrossRef] [PubMed]
- Cerna, J.; Edwards, C.G.; Martell, S.; Athari Anaraki, N.S.; Walk, A.D.M.; Robbs, C.M.; Adamson, B.C.; Flemming, I.R.; Labriola, L.; Motl, R.W.; et al. Neuroprotective influence of macular xanthophylls and retinal integrity on cognitive function among persons with multiple sclerosis. Int J Psychophysiol 2023, 188, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Kadam, I.; Nebie, C.; Dalloul, M.; Hittelman, J.; Fordjour, L.; Hoepner, L.; Futterman, I.D.; Minkoff, H.; Jiang, X. Maternal Lutein Intake during Pregnancies with or without Gestational Diabetes Mellitus and Cognitive Development of Children at 2 Years of Age: A Prospective Observational Study. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Keenan, T.D.L.; Agron, E.; Chew, E.Y.; Areds; Groups, A.R. Dietary nutrient intake and cognitive function in the Age-Related Eye Disease Studies 1 and 2. Alzheimers Dement 2023, 19, 4311–4324. [Google Scholar] [CrossRef]
- Mahmassani, H.A.; Switkowski, K.M.; Johnson, E.J.; Scott, T.M.; Rifas-Shiman, S.L.; Oken, E.; Jacques, P.F. Early Childhood Lutein and Zeaxanthin Intake Is Positively Associated with Early Childhood Receptive Vocabulary and Mid-Childhood Executive Function But No Other Cognitive or Behavioral Outcomes in Project Viva. J Nutr 2022, 152, 2555–2564. [Google Scholar] [CrossRef]
- Martell, S.G.; Kim, J.; Cannavale, C.N.; Mehta, T.D.; Erdman, J.W., Jr.; Adamson, B.; Motl, R.W.; Khan, N.A. Randomized, Placebo-Controlled, Single-Blind Study of Lutein Supplementation on Carotenoid Status and Cognition in Persons with Multiple Sclerosis. J Nutr 2023, 153, 2298–2311. [Google Scholar] [CrossRef]
- Parekh, R.; Hammond, B.R., Jr.; Chandradhara, D. Lutein and Zeaxanthin Supplementation Improves Dynamic Visual and Cognitive Performance in Children: A Randomized, Double-Blind, Parallel, Placebo-Controlled Study. Adv Ther 2024, 41, 1496–1511. [Google Scholar] [CrossRef]
- Kan, J.; Li, A.; Zou, H.; Chen, L.; Du, J. A Machine Learning Based Dose Prediction of Lutein Supplements for Individuals With Eye Fatigue. Front Nutr 2020, 7, 577923. [Google Scholar] [CrossRef]
- Almalki, A.M.; Alblowi, M.; Aldosari, A.M.; Khandekar, R.; Al-Swailem, S.A. Population perceived eye strain due to digital devices usage during COVID-19 pandemic. Int Ophthalmol 2023, 43, 1935–1943. [Google Scholar] [CrossRef]
- Almudhaiyan, T.M.; Aldebasi, T.; Alakel, R.; Marghlani, L.; Aljebreen, A.; Moazin, O.M. The Prevalence and Knowledge of Digital Eye Strain Among the Undergraduates in Riyadh, Saudi Arabia. Cureus 2023, 15, e37081. [Google Scholar] [CrossRef] [PubMed]
- AlQarni, A.M.; AlAbdulKader, A.M.; Alghamdi, A.N.; Altayeb, J.; Jabaan, R.; Assaf, L.; Alanazi, R.A. Prevalence of Digital Eye Strain Among University Students and Its Association with Virtual Learning During the COVID-19 Pandemic. Clin Ophthalmol 2023, 17, 1755–1768. [Google Scholar] [CrossRef]
- Bhatnagar, K.R.; Dixit, S.G.; Pandey, L.; Prakash, S.; Shiromani, S.; Singh, K. Digital eye strain among medical students associated with shifting to e-learning during COVID-19 pandemic: An online survey. Indian J Ophthalmol 2024, 72, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Chu, G.C.H.; Chan, L.Y.L.; Do, C.W.; Tse, A.C.Y.; Cheung, T.; Szeto, G.P.Y.; So, B.C.L.; Lee, R.L.T.; Lee, P.H. Association between time spent on smartphones and digital eye strain: A 1-year prospective observational study among Hong Kong children and adolescents. Environ Sci Pollut Res Int 2023, 30, 58428–58435. [Google Scholar] [CrossRef]
- Huyhua-Gutierrez, S.C.; Zeladita-Huaman, J.A.; Diaz-Manchay, R.J.; Dominguez-Palacios, A.B.; Zegarra-Chaponan, R.; Rivas-Souza, M.A.; Tejada-Munoz, S. Digital Eye Strain among Peruvian Nursing Students: Prevalence and Associated Factors. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Das, O.; Roy, A.; Das, A. Knowledge, attitude, and practice on digital eye strain during coronavirus disease-2019 lockdown: A comparative study. Oman J Ophthalmol 2022, 15, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Mataftsi, A.; Seliniotaki, A.K.; Moutzouri, S.; Prousali, E.; Darusman, K.R.; Adio, A.O.; Haidich, A.B.; Nischal, K.K. Digital eye strain in young screen users: A systematic review. Prev Med 2023, 170, 107493. [Google Scholar] [CrossRef]
- Moore, P.A.; Wolffsohn, J.S.; Sheppard, A.L. Digital eye strain and its impact on working adults in the UK and Ireland. Cont Lens Anterior Eye 2024, 102176. [Google Scholar] [CrossRef]
- Mylona, I.; Glynatsis, M.N.; Floros, G.D.; Kandarakis, S. Spotlight on Digital Eye Strain. Clin Optom (Auckl) 2023, 15, 29–36. [Google Scholar] [CrossRef]
- Rana, M.; Gupta, P.C.; Grover, S.; Furr, A.; Bhargava, N. Prevalence and Association of Digital Eye Strain with the Quality of Sleep and Feeling of Loneliness among Female College Students in Northern India. Indian J Public Health 2023, 67, 618–625. [Google Scholar] [CrossRef]
- Sharma, A.; Satija, J.; Antil, P.; Dahiya, R.; Shekhawat, S. Determinants of digital eye strain among university students in a district of India: a cross-sectional study. Z Gesundh Wiss 2023, 1–6. [Google Scholar] [CrossRef]
- Shrestha, P.; Singh Pradhan, P.M. Digital Eye Strain in Medical Undergraduate Students during COVID-19 Pandemic. J Nepal Health Res Counc 2023, 20, 726–730. [Google Scholar] [CrossRef]
- Vishwanathan, R.; Neuringer, M.; Snodderly, D.M.; Schalch, W.; Johnson, E.J. Macular lutein and zeaxanthin are related to brain lutein and zeaxanthin in primates. Nutr Neurosci 2013, 16, 21–29. [Google Scholar] [CrossRef]
- Dorey, C.K.; Gierhart, D.; Fitch, K.A.; Crandell, I.; Craft, N.E. Low Xanthophylls, Retinol, Lycopene, and Tocopherols in Grey and White Matter of Brains with Alzheimer’s Disease. J Alzheimers Dis 2023, 94, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Chen, H.; Wang, Y.; Schneider, J.A.; Willett, W.C.; Morris, M.C. Dietary carotenoids related to risk of incident Alzheimer dementia (AD) and brain AD neuropathology: a community-based cohort of older adults. Am J Clin Nutr 2021, 113, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Mukherjee, A. Innovative Troxler-free measurement of macular pigment and lens density with correction of the former for the aging lens. J Biomed Opt 2013, 18, 107003. [Google Scholar] [CrossRef]
- van der Veen, R.L.; Berendschot, T.T.; Hendrikse, F.; Carden, D.; Makridaki, M.; Murray, I.J. A new desktop instrument for measuring macular pigment optical density based on a novel technique for setting flicker thresholds. Ophthalmic Physiol Opt 2009, 29, 127–137. [Google Scholar] [CrossRef] [PubMed]
- van der Veen, R.L.; Berendschot, T.T.; Makridaki, M.; Hendrikse, F.; Carden, D.; Murray, I.J. Correspondence between retinal reflectometry and a flicker-based technique in the measurement of macular pigment spatial profiles. J Biomed Opt 2009, 14, 064046. [Google Scholar] [CrossRef]
- Beatty, S.; Koh, H.H.; Carden, D.; Murray, I.J. Macular pigment optical density measurement: a novel compact instrument. Ophthalmic Physiol Opt 2000, 20, 105–111. [Google Scholar] [CrossRef]
- Davey, P.G.; Alvarez, S.D.; Lee, J.Y. Macular pigment optical density: repeatability, intereye correlation, and effect of ocular dominance. Clin Ophthalmol 2016, 10, 1671–1678. [Google Scholar] [CrossRef]
- Davey, P.G.; Ngo, A.; Cross, J.; Gierhart, D.L. Macular Pigment Reflectometry: Development and evaluation of a novel clinical device for rapid objective assessment of the macular carotenoids. In Ophthalmic Technologies Xxix; Manns, F., Soderberg, P.G., Ho, A., Eds.; Proceedings of SPIE; Spie-Int Soc Optical Engineering: Bellingham, 2019; Volume 10858. [Google Scholar]
- de Kinkelder, R.; van der Veen, R.L.; Verbaak, F.D.; Faber, D.J.; van Leeuwen, T.G.; Berendschot, T.T. Macular pigment optical density measurements: evaluation of a device using heterochromatic flicker photometry. Eye (Lond) 2011, 25, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Howells, O.; Eperjesi, F.; Bartlett, H. Improving the repeatability of heterochromatic flicker photometry for measurement of macular pigment optical density. Graefes Arch Clin Exp Ophthalmol 2013, 251, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Guan, C.; Ng, D.S.; Liu, X.; Chen, H. Macular Pigment Optical Density Measured by a Single Wavelength Reflection Photometry with and without Mydriasis. Curr Eye Res 2019, 44, 324–328. [Google Scholar] [CrossRef]
- Murray, I.J.; Carden, D.; Makridaki, M. The repeatability of the MPS 9000 macular pigment screener. Br J Ophthalmol 2011, 95, 431–432; author reply 432–433. [Google Scholar] [CrossRef]
- Murray, I.J.; Hassanali, B.; Carden, D. Macular pigment in ophthalmic practice; a survey. Graefes Arch Clin Exp Ophthalmol 2013, 251, 2355–2362. [Google Scholar] [CrossRef]
- Murray, I.J.; Makridaki, M.; van der Veen, R.L.; Carden, D.; Parry, N.R.; Berendschot, T.T. Lutein supplementation over a one-year period in early AMD might have a mild beneficial effect on visual acuity: the CLEAR study. Invest Ophthalmol Vis Sci 2013, 54, 1781–1788. [Google Scholar] [CrossRef]
- Suarez-Berumen, K.; Davey, P.G. Macular Pigments Optical Density: A Review of Techniques of Measurements and Factors Influencing their Levels. JSM Ophthalmol 2014, 3, 4. [Google Scholar]
- Stringham, J.M.; O’Brien, K.J.; Stringham, N.T. Macular carotenoid supplementation improves disability glare performance and dynamics of photostress recovery. Eye Vis (Lond) 2016, 3, 30. [Google Scholar] [CrossRef] [PubMed]
- Stringham, J.M.; O’Brien, K.J.; Stringham, N.T. Contrast Sensitivity and Lateral Inhibition Are Enhanced With Macular Carotenoid Supplementation. Invest Ophthalmol Vis Sci 2017, 58, 2291–2295. [Google Scholar] [CrossRef]
- Stringham, J.M.; Stringham, N.T.; O’Brien, K.J. Macular Carotenoid Supplementation Improves Visual Performance, Sleep Quality, and Adverse Physical Symptoms in Those with High Screen Time Exposure. Foods 2017, 6, 47. [Google Scholar] [CrossRef]
- Li, B.; George, E.W.; Rognon, G.T.; Gorusupudi, A.; Ranganathan, A.; Chang, F.Y.; Shi, L.; Frederick, J.M.; Bernstein, P.S. Imaging lutein and zeaxanthin in the human retina with confocal resonance Raman microscopy. Proc Natl Acad Sci U S A 2020, 117, 12352–12358. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, H.; Eperjesi, F. Use of fundus imaging in quantification of age-related macular change. Surv Ophthalmol 2007, 52, 655–671. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T. Dose-dependent response of serum lutein and macular pigment optical density to supplementation with lutein esters. Arch Biochem Biophys 2010, 504, 50–55. [Google Scholar] [CrossRef]
- Bone, R.A.; Landrum, J.T.; Cao, Y.; Howard, A.N.; Alvarez-Calderon, F. Macular pigment response to a supplement containing meso-zeaxanthin, lutein and zeaxanthin. Nutr Metab (Lond) 2007, 4, 12. [Google Scholar] [CrossRef]
- Huang, Y.M.; Yan, S.F.; Ma, L.; Zou, Z.Y.; Xu, X.R.; Dou, H.L.; Lin, X.M. Serum and macular responses to multiple xanthophyll supplements in patients with early age-related macular degeneration. Nutrition 2013, 29, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Landrum, J.T.; Bone, R.A.; Joa, H.; Kilburn, M.D.; Moore, L.L.; Sprague, K.E. A one year study of the macular pigment: the effect of 140 days of a lutein supplement. Exp Eye Res 1997, 65, 57–62. [Google Scholar] [CrossRef]
- Obana, A.; Hiramitsu, T.; Gohto, Y.; Ohira, A.; Mizuno, S.; Hirano, T.; Bernstein, P.S.; Fujii, H.; Iseki, K.; Tanito, M.; et al. Macular carotenoid levels of normal subjects and age-related maculopathy patients in a Japanese population. Ophthalmology 2008, 115, 147–157. [Google Scholar] [CrossRef]
- Berendschot, T.T.; Goldbohm, R.A.; Klopping, W.A.; van de Kraats, J.; van Norel, J.; van Norren, D. Influence of lutein supplementation on macular pigment, assessed with two objective techniques. Invest Ophthalmol Vis Sci 2000, 41, 3322–3326. [Google Scholar]
- Davey, P.G.; Lievens, C.; Ammono-Monney, S. Differences in macular pigment optical density across four ethnicities: a comparative study. Ther Adv Ophthalmol 2020, 12, 2515841420924167. [Google Scholar] [CrossRef]
- Sanabria, J.C.; Bass, J.; Spors, F.; Gierhart, D.L.; Davey, P.G. Measurement of Carotenoids in Perifovea using the Macular Pigment Reflectometer. J Vis Exp 2020. [Google Scholar] [CrossRef]
- Obana, A.; Tanito, M.; Gohto, Y.; Gellermann, W.; Okazaki, S.; Ohira, A. Macular pigment changes in pseudophakic eyes quantified with resonance Raman spectroscopy. Ophthalmology 2011, 118, 1852–1858. [Google Scholar] [CrossRef] [PubMed]
- van de Kraats, J.; van Norren, D. Directional and nondirectional spectral reflection from the human fovea. J Biomed Opt 2008, 13, 024010. [Google Scholar] [CrossRef]
- Stringham, J.M.; Hammond, B.R. Macular pigment and visual performance under glare conditions. Optom Vis Sci 2008, 85, 82–88. [Google Scholar] [CrossRef]
- Stringham, J.M.; Hammond, B.R.; Nolan, J.M.; Wooten, B.R.; Mammen, A.; Smollon, W.; Snodderly, D.M. The utility of using customized heterochromatic flicker photometry (cHFP) to measure macular pigment in patients with age-related macular degeneration. Exp Eye Res 2008, 87, 445–453. [Google Scholar] [CrossRef]
- Wooten, B.R.; Hammond, B.R., Jr.; Land, R.I.; Snodderly, D.M. A practical method for measuring macular pigment optical density. Invest Ophthalmol Vis Sci 1999, 40, 2481–2489. [Google Scholar] [PubMed]
- Arunkumar, R.; Calvo, C.M.; Conrady, C.D.; Bernstein, P.S. What do we know about the macular pigment in AMD: the past, the present, and the future. Eye (Lond) 2018, 32, 992–1004. [Google Scholar] [CrossRef]
- Beccarelli, L.M.; Scherr, R.E.; Dharmar, M.; Ermakov, I.V.; Gellermann, W.; Jahns, L.; Linnell, J.D.; Keen, C.L.; Steinberg, F.M.; Young, H.M.; et al. Using Skin Carotenoids to Assess Dietary Changes in Students After 1 Academic Year of Participating in the Shaping Healthy Choices Program. J Nutr Educ Behav 2017, 49, 73–78 e71. [Google Scholar] [CrossRef] [PubMed]
- Ermakov, I.V.; Gellermann, W. Optical detection methods for carotenoids in human skin. Arch Biochem Biophys 2015, 572, 101–111. [Google Scholar] [CrossRef]
- Jahns, L.; Johnson, L.K.; Mayne, S.T.; Cartmel, B.; Picklo, M.J., Sr.; Ermakov, I.V.; Gellermann, W.; Whigham, L.D. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: uptake and depletion kinetics. Am J Clin Nutr 2014, 100, 930–937. [Google Scholar] [CrossRef]
- Jahns, L.; Johnson, L.K.; Conrad, Z.; Bukowski, M.; Raatz, S.K.; Jilcott Pitts, S.; Wang, Y.; Ermakov, I.V.; Gellermann, W. Concurrent validity of skin carotenoid status as a concentration biomarker of vegetable and fruit intake compared to multiple 24-h recalls and plasma carotenoid concentrations across one year: a cohort study. Nutr J 2019, 18, 78. [Google Scholar] [CrossRef]
- Obana, A.; Gohto, Y.; Gellermann, W.; Ermakov, I.V.; Sasano, H.; Seto, T.; Bernstein, P.S. Skin Carotenoid Index in a large Japanese population sample. Sci Rep 2019, 9, 9318. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, Y.; Obana, A.; Muto, S.; Asaoka, R.; Tanito, M.; Ermakov, I.V.; Bernstein, P.S.; Gellermann, W. Relationships between Skin Carotenoid Levels and Metabolic Syndrome. Antioxidants (Basel) 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Lademann, J.; von Hagen, J.; Lohan, S.B.; Kolmar, H.; Meinke, M.C.; Jung, S. Carotenoids in Human SkinIn Vivo: Antioxidant and Photo-Protectant Role against External and Internal Stressors. Antioxidants (Basel) 2022, 11. [Google Scholar] [CrossRef]
- Scarmo, S.; Cartmel, B.; Lin, H.; Leffell, D.J.; Welch, E.; Bhosale, P.; Bernstein, P.S.; Mayne, S.T. Significant correlations of dermal total carotenoids and dermal lycopene with their respective plasma levels in healthy adults. Arch Biochem Biophys 2010, 504, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Rosok, L.M.; Cannavale, C.N.; Keye, S.A.; Holscher, H.D.; Renzi-Hammond, L.; Khan, N.A. Skin and macular carotenoids and relations to academic achievement among school-aged children. Nutr Neurosci 2024, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, H.E.; Eperjesi, F. Effect of lutein and antioxidant dietary supplementation on contrast sensitivity in age-related macular disease: a randomized controlled trial. Eur J Clin Nutr 2007, 61, 1121–1127. [Google Scholar] [CrossRef]
- Hammond, B.R., Jr.; Ciulla, T.A.; Snodderly, D.M. Macular pigment density is reduced in obese subjects. Invest Ophthalmol Vis Sci 2002, 43, 47–50. [Google Scholar]
- Hammond, B.R., Jr.; Curran-Celentano, J.; Judd, S.; Fuld, K.; Krinsky, N.I.; Wooten, B.R.; Snodderly, D.M. Sex differences in macular pigment optical density: relation to plasma carotenoid concentrations and dietary patterns. Vision Res 1996, 36, 2001–2012. [Google Scholar] [CrossRef]
- Hammond, B.R., Jr.; Fuld, K.; Snodderly, D.M. Iris color and macular pigment optical density. Exp Eye Res 1996, 62, 293–297. [Google Scholar] [CrossRef]
- Howells, O.; Eperjesi, F.; Bartlett, H. Measuring macular pigment optical density in vivo: a review of techniques. Graefes Arch Clin Exp Ophthalmol 2011, 249, 315–347. [Google Scholar] [CrossRef]
- Nolan, J.M.; Power, R.; Stringham, J.; Dennison, J.; Stack, J.; Kelly, D.; Moran, R.; Akuffo, K.O.; Corcoran, L.; Beatty, S. Enrichment of Macular Pigment Enhances Contrast Sensitivity in Subjects Free of Retinal Disease: Central Retinal Enrichment Supplementation Trials - Report 1. Invest Ophthalmol Vis Sci 2016, 57, 3429–3439. [Google Scholar] [CrossRef] [PubMed]
- Trieschmann, M.; Beatty, S.; Nolan, J.M.; Hense, H.W.; Heimes, B.; Austermann, U.; Fobker, M.; Pauleikhoff, D. Changes in macular pigment optical density and serum concentrations of its constituent carotenoids following supplemental lutein and zeaxanthin: the LUNA study. Exp Eye Res 2007, 84, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.S.; Zhao, D.Y.; Sharifzadeh, M.; Ermakov, I.V.; Gellermann, W. Resonance Raman measurement of macular carotenoids in the living human eye. Arch Biochem Biophys 2004, 430, 163–169. [Google Scholar] [CrossRef]
- Bernstein, P.S.; Zhao, D.Y.; Wintch, S.W.; Ermakov, I.V.; McClane, R.W.; Gellermann, W. Resonance Raman measurement of macular carotenoids in normal subjects and in age-related macular degeneration patients. Ophthalmology 2002, 109, 1780–1787. [Google Scholar] [CrossRef] [PubMed]
- Obana, A.; Gohto, Y.; Asaoka, R. Macular pigment changes after cataract surgery with yellow-tinted intraocular lens implantation. PLoS One 2021, 16, e0248506. [Google Scholar] [CrossRef] [PubMed]
- Obana, A.; Ote, K.; Gohto, Y.; Yamada, H.; Hashimoto, F.; Okazaki, S.; Asaoka, R. Deep learning-based correction of cataract-induced influence on macular pigment optical density measurement by autofluorescence spectroscopy. PLoS One 2024, 19, e0298132. [Google Scholar] [CrossRef]
- Obana, A.; Ote, K.; Hashimoto, F.; Asaoka, R.; Gohto, Y.; Okazaki, S.; Yamada, H. Correction for the Influence of Cataract on Macular Pigment Measurement by Autofluorescence Technique Using Deep Learning. Transl Vis Sci Technol 2021, 10, 18. [Google Scholar] [CrossRef]
Figure 1.
Scatter plot comparing first study related measurement and second measurement obtained using the QuantifEye.
Figure 1.
Scatter plot comparing first study related measurement and second measurement obtained using the QuantifEye.
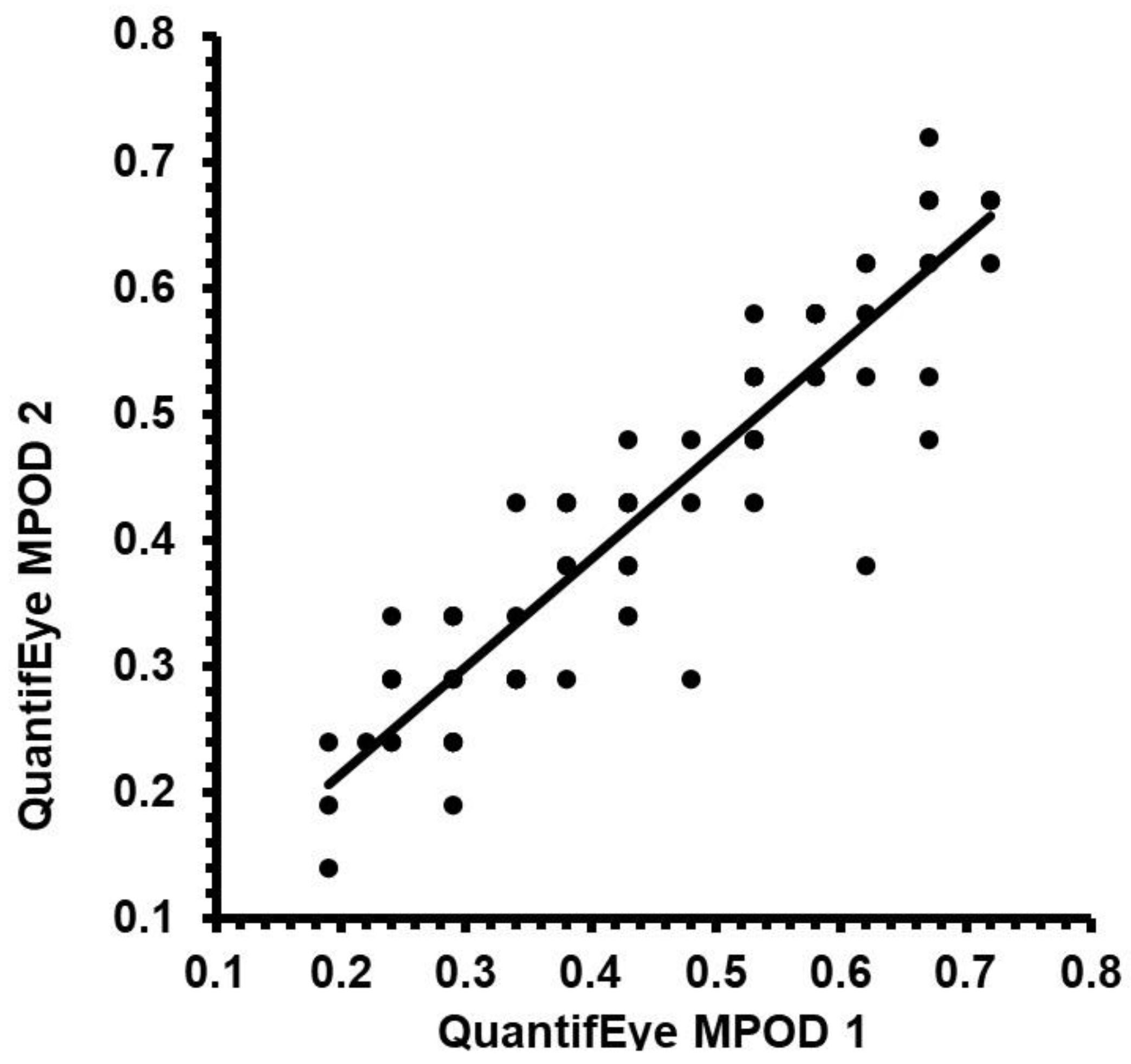
Figure 2.
Altman and Bland plots comparing the first study related measurement and second measurement obtained using the QuantifEye.
Figure 2.
Altman and Bland plots comparing the first study related measurement and second measurement obtained using the QuantifEye.
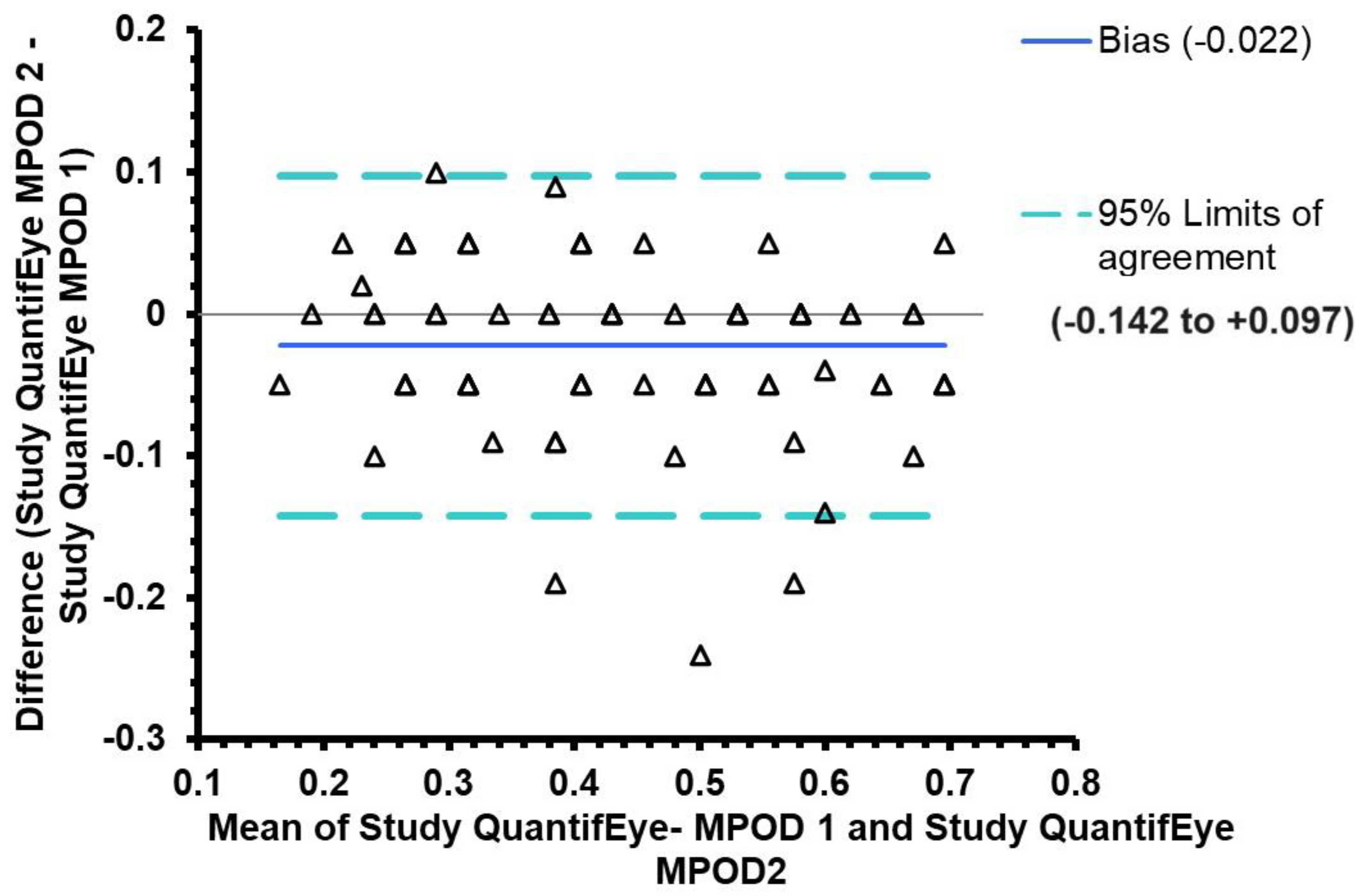
Figure 3.
Scatter plot comparing first study related measurement and second measurement obtained using the Zx Pro.
Figure 3.
Scatter plot comparing first study related measurement and second measurement obtained using the Zx Pro.
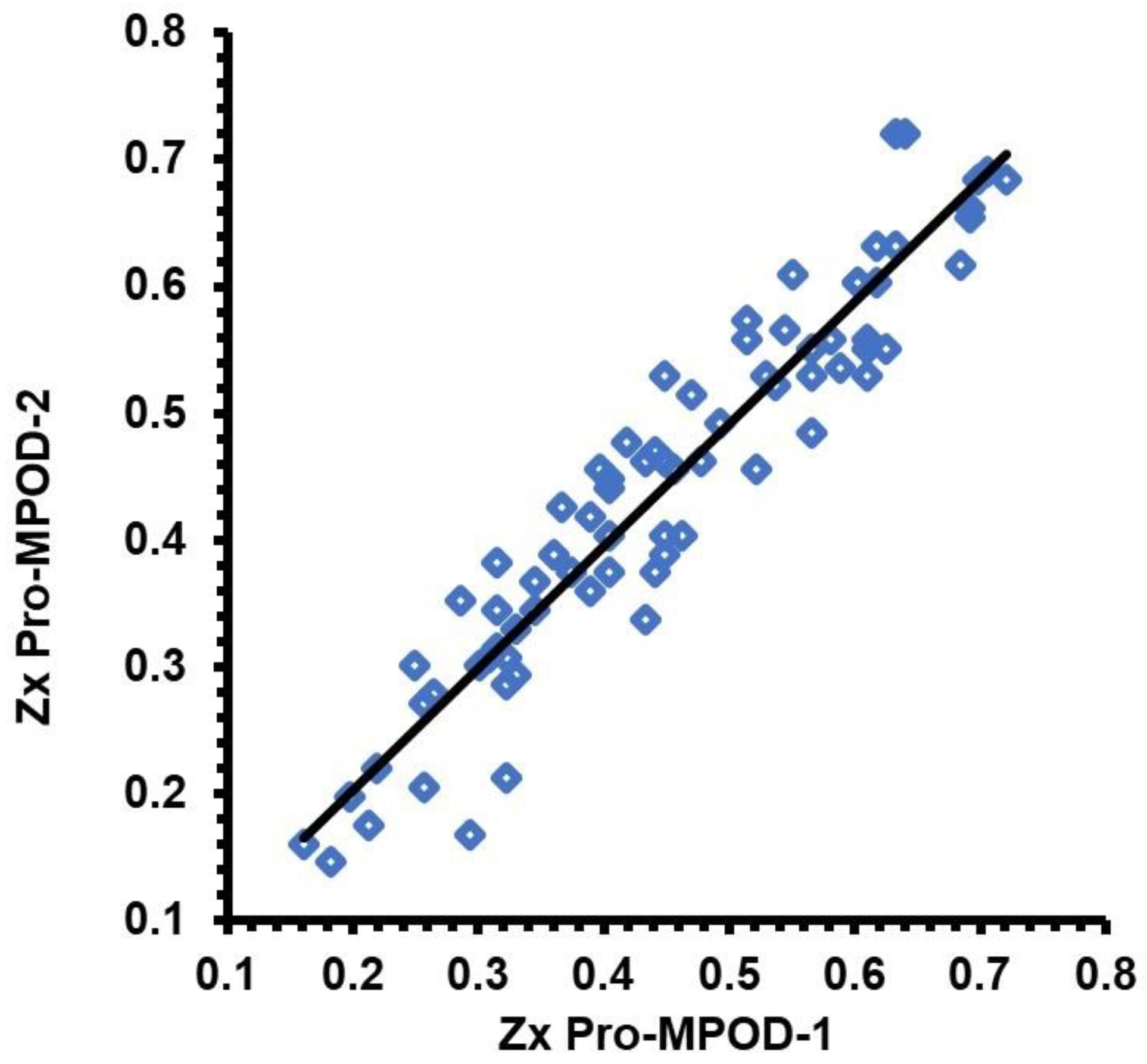
Figure 4.
Altman and Bland plots comparing the first study related measurement and second measurement obtained using the Zx Pro.
Figure 4.
Altman and Bland plots comparing the first study related measurement and second measurement obtained using the Zx Pro.
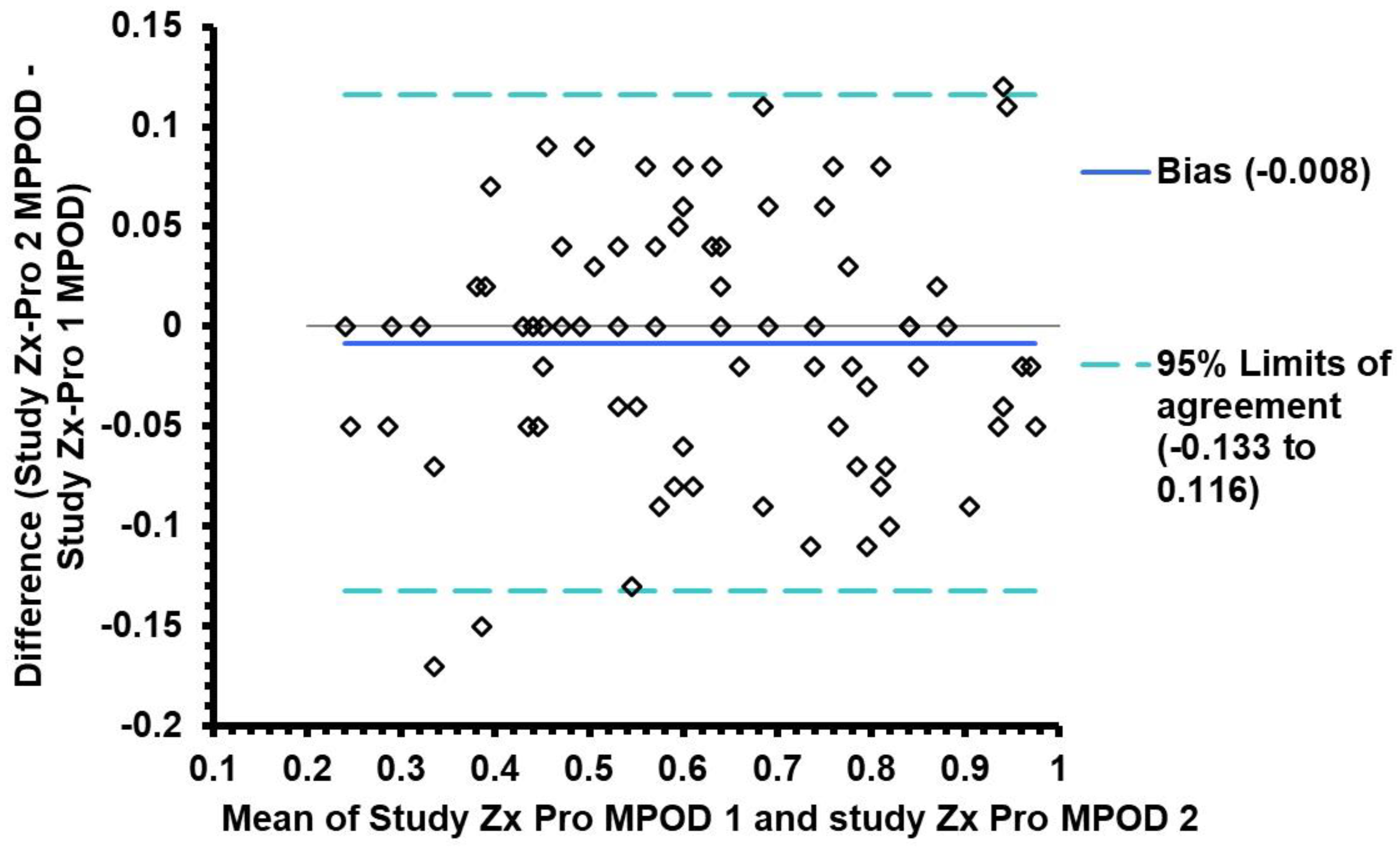
Figure 5.
Altman and Bland Plots demonstrating agreement between the predicate device QuantifEye and the Zx Pro. A is the comparison of the first Study measurements, B is the comparison of the second study measurements, and C is the mean of the first and second measurements obtained with both devices.
Figure 5.
Altman and Bland Plots demonstrating agreement between the predicate device QuantifEye and the Zx Pro. A is the comparison of the first Study measurements, B is the comparison of the second study measurements, and C is the mean of the first and second measurements obtained with both devices.
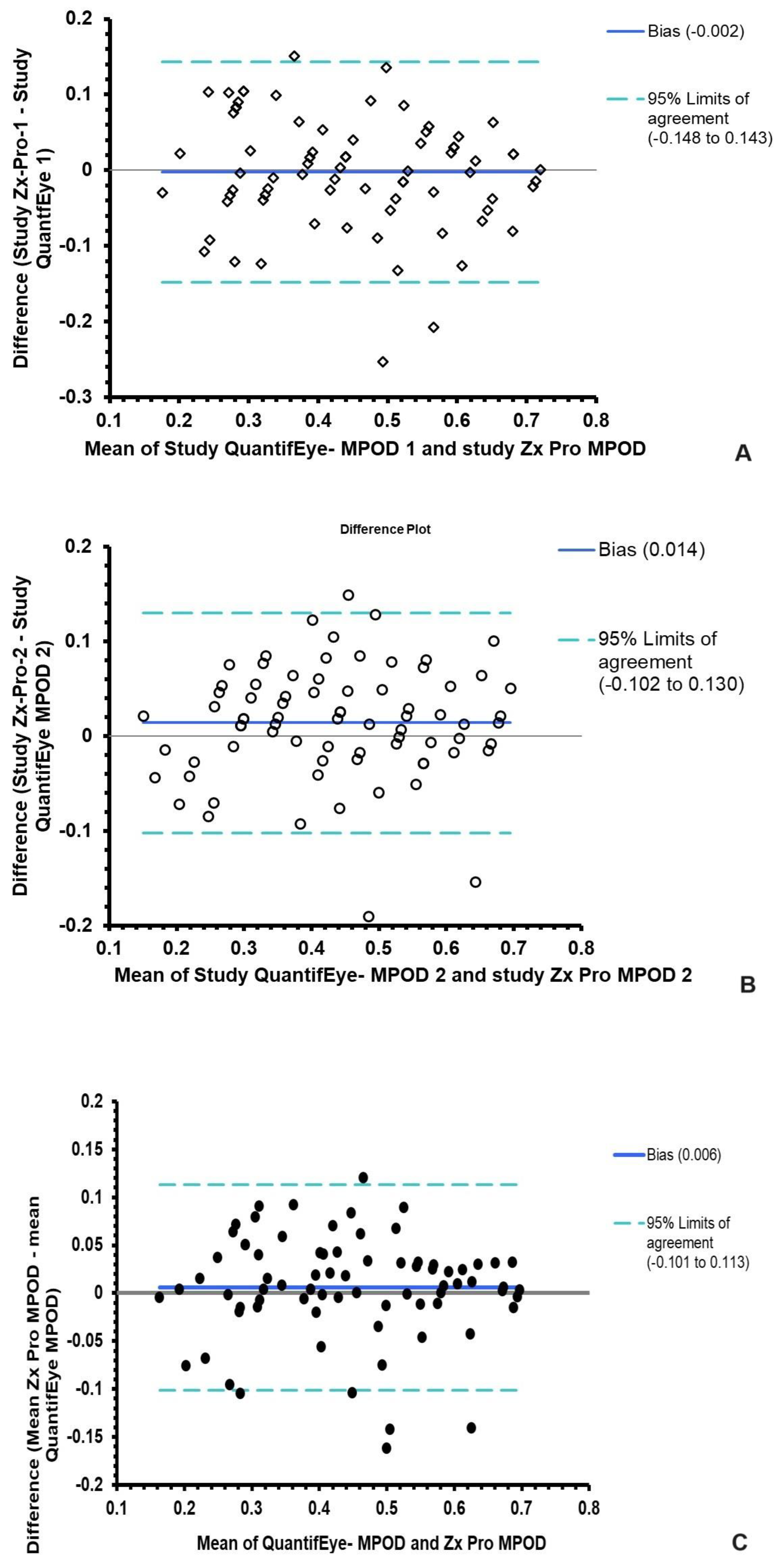
Table 2.
Descriptives of the difference in first and second measurements of the MPOD measuring devices.
Table 2.
Descriptives of the difference in first and second measurements of the MPOD measuring devices.
| Difference in first and second measurements | Mean | 95% confidence intervals | Median | Minimum | Maximum |
|---|---|---|---|---|---|
| QuantifEye | 0.022 | 0.01 to 0.04 | 0.00 | -0.10 | 0.24 |
| Zx Pro | 0.006 | 0.00 to 0.02 | 0.00 | -0.08 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



