
Submitted:
06 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Cardiac arrest (CA) is a life-critical condition. Patients who survive after CA, they go into a defined post-cardiac arrest syndrome (PCAS). In this clinical context, the role of the echocardiogram in recent years has become increasingly important to assess the causes of arrest, the prognosis, and any direct and indirect complications dependent on cardiopulmonary resuscitation (CPR) maneuvers. The aim of our review is to evaluate the increasingly important role of the transthoracic and transesophageal echocardiogram in the CA phase and especially post-arrest, analyzing the data already present in the literature.
Keywords:
cardiac arrest
; echocardiogram
; POCUS
; echocardiography
; post-cardiac arrest
; ACLS
; ROSC
; CPR
1. Introduction
Cardiac arrest (CA) is a critical medical emergency characterized by the sudden cessation of cardiac function, which results in the abrupt loss of effective blood circulation, brain and vital organs hypo perfusion, rapidly leading to death, if not promptly and effectively treated [1]. Despite advances in resuscitative efforts and post-arrest care, it has a significant morbidity and mortality. Both electrical and mechanical phenomena may be the primary cause of CA. Pulseless electrical activity (PEA) is a clinical state characterized by the presence of organized electrical activity on the electrocardiogram (ECG), in absence of effective cardiac output (CO), resulting in no palpable pulse or measurable blood pressure[2]. This condition often arises from severe physiological derangements such as profound hypovolemia, hypoxia, acidosis, or cardiac tamponade[1,2]. The condition in which the palpable pulse is absent, but minimal cardiac mechanical activity is sufficient to generate some degree of CO [is defined pseudo-pulseless electrical activity (pseudo-PEA). Pseudo-PEA can be identified through advanced diagnostic modalities such as Doppler ultrasound or invasive hemodynamic monitoring[3]. Rapid and accurate assessment of cardiac function is pivotal for guiding therapeutic interventions and improving outcomes in patients experiencing CA. Echocardiography, particularly point-of-care focused echocardiography (POCUS), has emerged as an invaluable diagnostic and monitoring tool in the management of critically ill patients, including those in the peri-arrest and CA phases. The use of echocardiography in the clinical context of CA allows the real-time visualization of cardiac structures and function, aiding in the identification of reversible causes of CA, guiding resuscitative efforts, and facilitating informed prognostic decisions.
The algorithm for adult post-arrest care is illustrated in Figure 1.
Our review aims to summarize the current evidence about the use of echocardiography in the post-arrest setting.
2. Role of Ultrasonography in Cardiac Arrest
Ultrasounds (US) are essential in Advanced Cardiac Life Support (ACLS) protocols, both during CA and immediately following the return of spontaneous circulation (ROSC), as recommended by international guidelines [4,5,6].
In this specific setting, a "head-to-toe" POCUS strategy is recommended and includes not only echocardiography, both transthoracic and transesophageal, but also thoracic, abdominal, vascular, and brain US.
During cardiopulmonary resuscitation (CPR), a trained operator should perform US without impeding effective chest compressions and ventilation. The primary objective of US during CPR is to optimize resuscitation efforts and guide the management by identifying potentially reversible causes of CA.
Following successful resuscitation, a more comprehensive US approach is warranted to optimize immediate hemodynamic functions, assist the ventilatory support, assess multiorgan complications, and investigate the underlying cause of the CA. Furthermore, it provides notable prognostic information [7].
Table 1 shows the main goals of US during CPR and in post-resuscitation care.
2.1. Role of Ultrasonography during Cardiopulmonary Resuscitation
As already mentioned, during the critical phase of CPR, echocardiography can provide essential information, with a transthoracic approach being most used due to simpler equipment and greater accessibility, even for non-specialist physicians.
Several protocols exist for performing transthoracic echocardiography (TTE) during CPR, but a detailed description of these protocols is beyond the scope of this review and can be found elsewhere[8,9,10,11,12,13,14,15,16,17]. However, their core principles are identical, and no single protocol has proven superior. All protocols rely on using limited TTE windows to obtain simple yet crucial information without interfering with resuscitation maneuvers or prolonging CPR pauses [17].
The subxiphoid window offers the easiest visualization of the heart during chest compressions without interrupting them. The US operator could then take advantage of the pause during the pulse and rhythm evaluation for use other views, keeping in mind that the pause should not exceed 10 seconds.
US can evaluate the effectiveness of chest compressions by providing direct, real-time observation of cardiac chambers' compression/relaxation. Adjusting hand placement for optimal chest compressions may be necessary, particularly if the area of maximal compression involves the aortic root or left ventricular outflow tract (LVOT), and US can aid in optimize the effectiveness of CPR [17].
Although the distinction of shockable [ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT)] and non-shockable rhythms (Asystole and PEA) is based upon ECG findings, in some cases the discrimination between asystole and fine VF is not obvious, because of low signal amplitude. Detection of cardiac contractions by echocardiography can identify patients who may benefit from defibrillation, even if initially classified as "asystole" [18]. Moreover, the presence of detectable cardiac contractility distinguishes "true" electromechanical dissociation of PEA from "pseudo-PEA," wherein myocardial contractions are present but severely diminished, resulting in no detectable pulse or blood pressure. Although both conditions are categorized as "non-shockable" CA, their causes and prognoses may differ. Interestingly, regardless of the cause, pseudo-PEA cases have shown higher survival rates compared to those with no detectable cardiac motion, particularly in those with an organized myocardial activity [19].
Therefore, the presence of detectable cardiac contractions could encourage physicians to continue the resuscitative effort and to consider an escalation in the advanced life support (like extracorporeal membrane oxygenation). Otherwise, the complete absence of cardiac motion, particularly if associated to large intracavitary thrombosis, could be an element in the decision to terminate CPR. Nonetheless, this decision must be made considering multiple factors beyond echocardiographic findings.
During resuscitation, identifying specific reversible causes can significantly impact survival, particularly in cases of non-shockable rhythms or refractory CA. US examination of the heart, lungs, abdomen, and proximal veins of the lower limbs can help detect common reversible causes such as pulmonary embolism (PE), cardiac tamponade, tension pneumothorax, and profound hypovolemia (Table 2) [17].
Given time constraints, US assessment must be highly focused and guided by clinical presentation. For instance, in trauma patients, the focus is on detecting tension pneumothorax and profound hypovolemia. In hypertensive patients with migrating chest pain, ruling out tamponade indicative of acute aortic syndrome is crucial. Similarly, in post-operative or oncology patients, priority is given to detecting massive PE [7]
Finally, US could be used to aid specific interventions during CPR, like insertion of peripheral or central venous cannulas, including those for extracorporeal life support (ECLS) or temporary pacing, drainage of cardiac tamponade or confirmation of bilateral lungs aeration after endotracheal tube positioning [20,21]
Due to its retrocardiac location, transesophageal echocardiography (TEE) overcomes numerous difficulties encountered with TTE and is therefore a solid alternative. TEE provides continuous, high-quality imaging of the heart throughout resuscitation, expanding diagnostic capabilities by offering superior visualization of structures like the posterior pericardium for localized tamponade, the pulmonary artery for acute PE, and the thoracic aorta for aortic dissection. Additionally, TEE's continuous imaging capability minimize interruptions to chest compressions during pulse checks and rhythm analysis and the different position of US operator interfere less with the resuscitative operations [22,23].
In a recent systematic review including 11 studies with 358 patients with both out-of-hospital CA (OHCA) and in-hospital CA (IHCA), Hussein et al. showed that TEE led to diagnosis of specifical reversible cause of CA in nearly one half of cases (148 patients, 41%), with diagnosis of PE as the most reported finding (43 patients) [24].
A focused TEE protocol and its clinical application in CA is showed in Table 3.
There are several limitations in the use of TEE during CA. TEE, compared to TTE is an invasive technique, with specific risks of oropharyngeal, esophageal, and gastric trauma, related to probe insertion. Additional risks related to the use during CPR are unknow [24]. However, in this life-threatening scenario, the benefits probably overweight the risks. Moreover, the need of operators with great expertise and the specific equipment required limits the availability of this tool in the emergency setting. Finally, echocardiography should never interfere with resuscitation, in this case with ventilatory support. For this reason, TEE could be started only if the patient has already been intubated. Still, to reduce the possibility of delays in obtaining the first TEE image and to mitigate airway complications, inserting the TEE probe under direct visualization during the same laryngoscopy procedure used for tracheal intubation may be advantageous [25]
2.2. Role of Ultrasonography in Post-Resuscitation Care
US, alongside with other tools, such as ECG and point of care blood analysis, has pivotal role and echocardiography should be performed in all patients as soon as possible, as recommended in international guidelines.
The main role played by echocardiography remains its utilization in identifying some of the most common CA etiologies, such as acute coronary syndrome (ACS), cardiac tamponade, cardiomyopathies, or PE.
Beyond the role in the identification of underlying cause of CA, US could aid airways and ventilatory support, as well as optimization of hemodynamic. Moreover, it could point out possible complication of CPR, such as ribs or sternal fracture, pneumothorax, visceral trauma, bleeding, or iatrogenic aortic dissection[26]. Finally cardiac and non-cardiac US have a role in prognostic evaluation.
2.2.1. Diagnosis of Underlying Cause of Cardiac Arrest
Echocardiography, plays a pivotal role in diagnosing structural heart disease (SHD), both ischemic and non-ischemic, as well as PE, cardiac tamponade, and profound hypovolemia.
Arrhythmias caused by myocardial ischemia due to ACS is still the most frequent cause of CA [4]. Echocardiography has a major role in identifying ACS mainly by showing left ventricular systolic disfunction with regional wall motion abnormalities (RWMA), particularly in case of non-diagnostic ECG.
During CA and CPR detecting RWMA is only possible if myocardial contractility is preserved, but it’s challenging even in these cases. Following ROSC a fine evaluation of regional myocardial contractility could be easier. However, RWMA in resuscitated patients is not a specific finding of ACS. Indeed, a post arrest myocardial disfunction (PAMD), usually reversible, is common, even without coronary syndrome and may occur with global wall motion abnormality or RWMA may occur, including typical and atypical Tako-tsubo syndrome (TTS) patterns. Up to 60% of patients may experience PAMD, which typically resolves within 24-48 hours [4]. Moreover, in the immediate post ROSC, it could be difficult differentiate new wall motion abnormalities due to ACS from pre-existing ones related to previous coronary events or cardiomyopathies. Finally, CA due to coronary artery disease (CAD) might occur without any RWMA, further complicating the scenario. Unsurprisingly studies on echocardiography's utility in diagnosing ACS/CAD after ROSC demonstrate variability in prevalence and diagnostic accuracy, highlighting a good sensitivity, but lack of specificity [27].
A retrospective, single-center, observational study at a tertiary hospital to evaluate POCUS performed by cardiologists within 60 min after was conducted by Elfwén et al. The study involved 617 adults admitted after a resuscitated CA. In this population RWMA were detected in 37.6%, but only half of the patients undergone coronary angiography showed a culprit lesion [28]
More specific echocardiographic findings suggesting ACS as cause of CA are the detection of mechanical complication of acute myocardial infraction (AMI), such as free wall, interventricular septum, or papillary muscle rupture.
Preferably, coronary interventions should be reserved for patients who do not have permanent severe neurological damage. Patients with irreversible hypoxic-ischemic brain injury are unlikely to derive benefits from percutaneous coronary intervention (PCI), even if a culprit coronary lesion is effectively addressed. For this reason, guidelines recommend immediate coronary angiography only in patients with evidence at ECG of ST elevation after ROSC. In other cases, coronary angiography should be considered after a multiparametric evaluation, encompassing patient history, clinical condition after ROSC, laboratory, and echocardiographic findings. None of them could be used alone, including echocardiography, keeping in mind that in the early phase of ROSC hemodynamic, ventilatory and neurological support are priorities.
Acute PE might cause CA, mostly due to PEA or asystole, with an incidence of 2-7 % in OHCA and 5-6% in IHCA [29] Echocardiography has a major role in diagnosis of PE, especially in patients with hemodynamic instability that could preclude the availability of pulmonary computed tomography (CT) [30]. The main echocardiographic features of PE are summarized in the Table 4 [31].
However, right ventricle (RV) echocardiographic abnormalities frequently manifest following resuscitation from CA. Acute dilation of the RV ensues within minutes from arrest, as blood shifts from the systemic circulation to the right side of the heart due to pressure gradients. Previous research has underscored significant post-arrest RV dysfunction and dilation, potentially leading clinicians to misconstrue it as indicative of PE as the precipitating cause, thereby risking fatal administration of thrombolytics. Indeed, a study has indicated an elevated risk of intracranial bleeding associated with fibrinolytic use during resuscitation in non-traumatic CA cases. This underscores the fact that RV dilation alone lacks in robust correlation with PE and should not independently prompt fibrinolytic therapy. Notably, in a recent review, Elfwén et al., showed that most individuals diagnosed with PE exhibited both RV dilation and pressure overload, suggesting that, in the post resuscitation phase, a multiparametric evaluation of RV overload should be done before the administration of fibrinolytic therapy [28]. Beyond the role of echocardiography, vascular US of proximal veins of the lower limbs could be helpful in doubtful cases, with the identification of deep vein thrombosis (DVT), which increases the probability of PE as the cause of CA (Figure 2) [7].
CA, mostly due to VT or VF, could be the first clinical manifestation of cardiomyopathies or myocarditis. Echocardiography in post resuscitated patients could highlight typical features of these diseases. However, whilst the evidence of marked myocardial asymmetrical hypertrophy easily suggests the presence of hypertrophic cardiomyopathy (HCM), spot typical features of other cardiomyopathies in the immediate post resuscitative care is challenging, due to the overlap with the biventricular systolic and diastolic abnormalities that characterize the PAMD. Whenever a multiparametric evaluation, including not only TTE, but also patient history, ECG and laboratory findings suggests myocardial disease, the diagnosis usually requires more complex exams, such es speckle tracking echocardiography, cardiac magnetic resonance (CMR), endomyocardial biopsy, or genetic tests[33,34].
Profound hypovolemia is among the most frequent causes of PEA, especially in traumatic CA. Moreover, in the post resuscitation care, fluid management is crucial for hemodynamic optimization. Echocardiography has a pivotal role in identify characteristic signs of reduced intravascular volume, such as the evidence of small, hyperkinetic ventricles, with near end-systolic obliteration (“kissing ventricle”) among with small or collapsed inferior vena cava (IVC), guiding fluid administration. Moreover, thoracic and abdominal US could be used in order to identify massive bleeding due to organ injury or aortic acute pathologies, as the primary cause of CA or as a complication of prolonged CPR [19].
Echocardiography is the first tool to identify cardiac tamponade, a common cause of CA with non-shockable rhythm. The diagnosis is usually done during CPR with echocardiographic evidence of pericardial effusion leading to cardiac chamber compression and eventually signs of ventricular interdependence and US are used also to guide pericardiocentesis. However, in the post resuscitation phase, echo enables monitoring of successful drainage and heart decompression. Moreover, pericardial effusion and tamponade could represent rare complication of CPR, that if not identified could compromise hemodynamic stabilization (Figure 3)[19,35,36]
However, clinicians should be aware that some relevant causes of CA do not have specific US findings, such as channelopathies or metabolic disorders. In these cases, echocardiography is still helpful to get important hemodynamic and prognostic information, but it’s not diriment for diagnostic purposes.
2.2.2. Hemodynamic Monitoring and Optimization
After a successful ROSC, efforts are made to reach and maintain adequate central and peripheral perfusion and oxygenation. Pharmacological and mechanical cardiac supports (MCS) are often needed to achieve hemodynamic stabilization. Echocardiography provides a readily available and economic tool for a bedside hemodynamic monitoring, guiding the use of fluids, inotropic drugs, vasopressors, vasodilators, MCS and evaluating the impact of positive pressure ventilation. Systemic perfusion strictly depends on cardiac output (CO), determined by stroke volume (SV) and heart rate (HR). For its part SV results from the interplay of preload, contractility, and afterload. Echocardiography is useful to get information about all this factors, guiding therapeutic strategies (Table 4).
SV, and consequently CO, could be directly assessed by echocardiography using LVOT diameter and LVOT Velocity Time Integral (VTI). The LVOT-VTI can serve as a substitute for SV, thereby eliminating the measure of LVOT diameter as a source of error [37]. As already mentioned, US allow evaluation of preload through estimation of intravascular volume, with static and dynamic measures that led to estimation of fluid responsiveness (IVC and internal jugular vein diameter and distensibility, LVOT-VTI variability during mechanical respiration, leg raise or fluid challenge) [38,39]. Moreover, US enables the evaluation of fluid tolerance, identifying the grade of systemic and pulmonary venous congestion [using the venous excess US score and lung US(LUS)][40,41]. Information on contractility is provided by the evaluation of left and right ventricular global systolic function, that could be made using multiple parameters [41]. Finally, echocardiography might be used to estimate systemic and pulmonary vascular resistance, the main determinants of left and right ventricular afterload, showing good correlation with invasive measurements [37,42]. Indeed, systemic vascular resistance (SVR) are determined using mean arterial pressure (MAP), right arterial pressure (RAP) and CO [42]. Similarly, pulmonary vascular resistance (PVR) could be calculated using pulmonary artery mean pressure (PAMP), pulmonary capillary wedge pressure (PCWP) derived from echocardiographic evaluation of diastolic parameters and CO [43]. Furthermore, in recent years there was great interest in non-invasive evaluation of right and left ventricular-arterial coupling, particularly in critical ill patients, such as post ROSC. Echocardiography could be used for this purpose and may enable clinicians to gain a more dynamic understanding of the cardiovascular physiology unique to each patient, potentially simplifying the process of customizing personalized pharmacological or interventional therapies [44,45].

Table 5.
Ultrasounds parameters for hemodynamic monitoring and optimization.
| Parameter | Utility | How to calculate |
Normal values and interpretation | |
|---|---|---|---|---|
|
Perfusion parameters |
LVOT VTI | Distance that blood travels across the LVOT during cardiac cycle | Tracing the PWD spectral display of the LVOT | LVOT-VTI > 18 cm |
| SV | Volume of blood pumped during each systolic cardiac contraction | SV= LVOT area* x LVOT-VTI SVi= SV/BSA |
SV > 70 ml SVi >35 ml/mq |
|
| CO and CI | Amount of blood pumped by the heart in a minute; | CO = SV x HR CI= CO/BSA |
CO > 4 l/min CI < 2.5 l/min/mq |
|
| Preload parameters (fluid responsiveness and fluid tolerance) | IVC diameter and collapsibility | Used to estimate RA pressure, and volemic status | Diameters of IVC at end expiration and inspiration in subcostal view | IVC < 21 mm that collapses > 50% (RAP 0-5 mmHg); IVC > 21 mm that collapses > 50% or IVC < 21 mm that collapses < 50% (RAP 5-10 mmHg); IVC > 21 mm that collapses < 50% (RAP 10-20 mmHg) |
| JVD ratio | Used to estimate RA pressure, and volemic status | JVD during Valsalva/JVD at rest | JVD ratio < 3 suggest elevated RAP and fluid overload | |
| LVOT-VTI variability | Dynamic parameters that suggest fluid responsiveness | Evaluation of LVOT-VTI in different respiratory phases during MV, after PLR or fluid challenge | Change in LVOT-VTI < 10-15% indicates fluid responsiveness | |
| VExUS score | Evaluation of systemic congestion in four grades | Combined evaluation of IVC diameter and venous flow pattern using PWD in HV, PV and IRV | VExUS score 0 = no congestion; VExUS score 3 = severe congestion | |
| LUS B-lines | Evaluation of pulmonary congestion | Evaluation of B-lines in 8 to 12 zones | B-lines < 3 for scanning zone = normal; Multiple and diffuse B-lines = severe congestion |
|
| E/e’ | Marker of LV filling pressure that correlates with PCWP [ PCWP≈1.24×(E/e)+1.9] | Ratio between mitral inflow E velocity using PWD and e’ lateral and medial velocity using TDI | E/e’ < 7 = normal filling pressure; E/e’ > 15= elevated filling pressure |
|
| Afterloadparameters | SVR | Determinant of LV afterload and reflect the tone of systemic blood vessels | MAP-CVP/CO** | SVR 800-1200 dynes·sec/cm^5 = 10-15 WU |
| PASP | Estimation of pulmonary artery systolic pressure | PASP=4×(TRV2)+RAP | PASP < 35 mmHg | |
| PAMP | Estimation of pulmonary artery mean pressure | PAPM=0.61×PASP+2 or PAPM=4×(PRV2 )+RAP | PAMP < 20 mmHg | |
| PVR | Determinant of RV afterload and reflect the tone of pulmonary blood vessels | PVR= (PAMP-PCWP)/CO | PVR < 2 WU | |
| TRV/RVOT-VTI ratio | Parameter to estimate PVR and PAP | Ratio between TRV and RVOT-VTI calculated tracing the PWD spectral display of the RVOT | TRV/RVOT-VTI ratio < 0.45 |
BSA: Body Surface Area; CI: Cardiac Index; CO: Cardiac Output; CVP: Central Venous Pressure; HV: Hepatic Vein; IVC: Inferior Vena Cava; JV: Jugular Vein; LV: Left Ventricle; LVOT: Left Ventricular Outflow Tract; LUS: Lung Ultrasound; MAP: Mean Arterial Pressure; MV: Mechanical Ventilation; PAMP: Pulmonary Artery Mean Pressure; PASP: Pulmonary Artery Systolic Pressure; PCWP: Pulmonary Capillary Wedge Pressure; PLR: Passive Leg Raise; PRV: Pulmonary Regurgitation early diastolic Velocity; PVR: Pulmonary Vascular Resistance; PV: Portal Vein; PWD: Pulsed-Wave Doppler; RA: Right Atrium; RAP: Right Atrial Pressure; RV: Right Ventricle; RVOT: Right Ventricular Outflow Tract; SV: Stroke Volume; SVR: Systemic Vascular Resistance; SVi: Stroke Volume Index; TDI: Tissue Doppler Imaging; TRV: Tricuspid Regurgitation Velocity; VExUS: Venous Excess Ultrasound Score; VTI: Velocity Time Integral; WU: Wood Units.* LVOT area is obtained by measuring the LVOT diameter in the parasternal long-axis (PLAX) view during mid-systole. ** MAP is measured invasively or non-invasively; RAP could be assessed using a central vein catheter (CVC) or estimated through the US evaluation of IVC diameter and col-lapsibility; CO is calculated using the LVOT area and VTI.
2.2.3. Role of Transesophageal Echocardiography
TEE is indicated when TTE is unfeasible or unconclusive, especially in non-compliant ventilated patient in intensive care unit (ICU) or in those with vascular cannula and thoracic or pericardial drainages limiting the echocardiographic views. Moreover, TEE should be preferred when is not possible to mobilize patient from the supine position. For this reason, there is a growing interest in utilizing TEE in intensive care settings, including in patients post CA [22].
Even if performing TEE is not simple for beginners, a survey conducted by Arntfield et al. involving 14 emergency physicians without experience in TEE showed that following brief, structured simulation-based training they can proficiently obtain focused TEE images [46].
Similarly, a single center retrospective observational study involving a total of 54 TEE exams performed by 12 emergency physicians between 2013 and 2015 revealed that TEE was feasible, safe, and clinically impactful. In this study the most common indication for performing TEE was CA (43% during CPR and 26% in post-resuscitation care). TEE led to diagnostic conclusion in 78% of cases and impacted therapeutic decisions in 67% of cases. Notably, 55.6% of these examinations identified findings not easily visualized on TTE[47].
Another retrospective study, based on 274 TEE performed between 2012 and 2016 by 38 trained operators, they demonstrated that point-of-care TEE in the ICU setting significantly influenced diagnosis and hemodynamic management decisions. Additionally, in nearly half of the patients who had undergone TTE within the preceding 24 hours, the indication for TEE was inconclusive TTE, underscoring the technical limitations of TTE in this population [48].
A recent cross-sectional survey conducted by Teran et al. in United States and Canada showed that the most common indication for performing TEE in the emergency department (ED) is assessing patients during resuscitation from CA (100%) and providing post-arrest care (76%)[49]. While during CPR the TEE protocol is usually simplified and limited to basic views, after ROSC extended protocol is executed, considering that patients remain usually unconscious or deeply sedated. In the specific setting of post resuscitation care it is desirable not to limit the evaluation to the heart and great vessels [23]. Indeed, TEE approach allows transesophageal lungs ultrasonography (TELUS) [50] and transgastric abdominal ultrasonography (TEGAUS) [51].
2.2.4. Role of Non-Cardiac Ultrasounds
Beyond the role of echocardiography, non-cardiac US also assume a key position in the post ROSC management. Most of resuscitated patients requires mechanical ventilatory support. LUS is a practical bedside tool that could provide relevant information in the immediate post ROSC phase and could be easily used for daily monitoring of the patient. LUS demonstrating bilateral ventilation contributes to confirmation of correct placement of endotracheal tube during or immediate after RCP. It also enables identification of pulmonary disease that could cause hypoxia as reversible cause of CA or pulmonary injuries that could represent a complication of RCP. Particularly, pneumothorax, pleural effusion, and consolidation, both caused by atelectasia and pneumonia, may be easily detected. [21]. As already mentioned, abdominal US could be used to detect massive intrabdominal bleeding and organ injury. Moreover, examination of intraabdominal organ hemodynamics using doppler studies contributes to evaluation of organ perfusion [41].
Post-resuscitation cerebral hemodynamics can be assessed by transcranial doppler (TCD) examining waveform patterns, pulsatility index, and mean flow velocity in the major cerebral arteries. Continual TCD assessments and optic nerve sheath diameter evaluations via US can aid in non-invasively evaluating cerebral edema resulting from ischemia-reperfusion syndrome and could help in the determination of brain stem death, particularly in case of post-traumatic CA [7,52]. Finally, US, beyond the role in facilitate venous and arterial cannulation, allows monitoring for vascular complication of invasive monitoring and support [7].
3. Post-Cardiac Arrest Syndrome: Pathophysiology and Echocardiographic Feature
Regardless of the primary cause, survival of patients with OHCA is poor, estimated as less than 15%. Deaths occur due to post-cardiac arrest syndrome (PCAS), caused by the ischemia-reperfusion injury that affects the whole organism. This process is characterized by sustained ischemic insult which leads to cell damage, shift to anaerobic metabolism with subsequent tissue acidosis and acid–base imbalance which is responsible for several cellular dysfunctions. As consequence of metabolic deviation, there is less ATP production and potentially an accumulation of toxic lipid substances, causing myocyte apoptosis, myocardial fibrosis, and, ultimately, cardiac dysfunction. In contrast, when reperfusion takes place, lipids once again become the main energy source, and oxygen consumption increases, leading as well to cardiac dysfunction [53].
Systemic acidemia resulting from hypoperfusion of vital tissues during CA is one of the predominant responsible of its increased mortality, as it causes impairment of cardiac function by reduced perfusion of the myocardium. Acidosis can be both cause and consequence of CA and is often associated with a poor prognosis and high mortality, which increases with the severity of the metabolic alteration. This condition determines a vitious circle, as lower CO with subsequent lower tissue perfusion increases the lactates blood level with worsening of the acidosis. Blood lactate concentrations may be considered as a marker of prolonged hypoperfusion or poor resuscitation, while lactate clearance during the first phase of post-resuscitation care may correlate with a more favorable outcome [54].
In literature, few studies have examined the relationship between systemic acidosis and myocardial dysfunction, measured by invasive and non-invasive techniques. A fundamental role is played by TTE. Many data shows that a reduced arterial pH is associated with impaired cardiac function and contractility[55]. Basing on data deriving from animals’ studies, lactic acidosis was associated to a notable reduction in SV and depressed left ventricle (LV) contractility potentially due to increase end-diastolic volume, resulting from acute pulmonary hypertension. In another similar study, respiratory acidosis showed decreased LV contractility and a fall in blood pressure by decreased SVR and impaired peripheral vascular reactivity to vasoactive drugs. These data support the hypothesis that a significant relationship between the fall of systemic pH and the reduction of cardiac function exists, although few are the available data on human models and no threshold arterial pH below which cardiac function becomes compromised has been described [56].
Myocardial dysfunction occurring after successful resuscitation from CA is known as PAMD. It is attributed to myocardial stunning from global ischemia, regardless of the primary cardiac or non-cardiac causes. Manifestations of PAMD include global LV systolic dysfunction, LV diastolic dysfunction, or RV dysfunction. Among these, LV systolic impairment is the most common and significant manifestation, presenting as one of the following echocardiographic patterns: type I - global dysfunction; type II - RWMA; and type III - Takotsubo cardiomyopathy-like pattern (Takotsubo pattern) [57]
Cha et al. published data from a prospective cohort study enrolling 138 adult patients with non-traumatic OHCA with successful CPR who survived for at least the following 48 hours, evaluating the degree of myocardial dysfunction subsequent the CA. Interestingly, only patients with CA from non-cardiac etiology were included, thus reducing the possibility of preexisting myocardial dysfunction. In this study global myocardial dysfunction (type I) was the most frequent echocardiographic pattern. PAMD developed in the first 24 hours post ROSC in almost one-third of the patients, but it was a reversible process (meant as EF greater than 50% or disappearance of RWMA on follow-up echocardiography) and return to normal global LV systolic function was registered by 72 hours after ROSC.
The pathophysiological explanation of transient myocardial disfunction after resuscitated CA is ascribed to ischemia/reperfusion injury and the inflammatory response after ROSC, associated with high level of plasma catecholamines. This latter mechanism could be responsible both of Takotsubo pattern (as in stress-induced cardiomyopathy) and RWMA (in patients with underlying unrevealed CAD). However, many studies focusing on the evidence of RWMA on echocardiography showed significant heterogeneity of this parameter, with high sensitivity but low specificity for diagnosing ACS as the cause of CA [27]. For example, it is reported in literature that transient disfunction of interventricular septum is not necessarily linked to CAD but could be attributed to RV dysfunction or volume overload during resuscitation maneuvers.[57]
Human studies suggest that about two-thirds of patients resuscitated from CA present LV systolic dysfunction within the first 24 hours after ROSC, with a mean LV ejection fraction (LVEF) between 35-45%[58]. Persistently low cardiac index (CI) at 24 hours was associated with early death, but in the surviving patients normal hemodynamic was restored by 72 hours. Apical segments displayed more severe RWMA with sparing of basal segments, a finding also seen in stress cardiomyopathy. PAMD shares characteristics with stress-induced or septic cardiomyopathy [53], not necessarily related to coronary stenosis.
In 2005, Ruiz Bailen et al. published a descriptive study reporting data on serial echocardiography in twenty-nine CA survivors with non-coronary artery pathology and no history of cardiac disease. It showed that at 24 hours an LVEF < 55% (mean value 28%) was identified in almost two-third of patients, but also that the myocardial systolic disfunction (in all patients presenting as disturbances of segmental contractility) improved during follow-up in those who survived. LVEF at 24 hours was higher in survivors than in non survivors [59]
Frequently, echocardiography is the first line diagnostic tool for the individuation of PAMD, of which reduced LVEF is the most reported manifestation. Still difficult is to determine whether myocardial disfunction encountered at TTE echocardiography is related to PCAS or is the red flag of a significative coronary stenosis.
Role of Echocardiography in Post-Arrest Management of Suspected ACS/CAD
Early revascularization of obstructed coronary arteries can reduce myocardial damage and its consequences, such as ventricular dysfunction, rhythm disturbances, heart failure, and death [53].
Although coronary angiography after CA is of potential diagnostic and therapeutic relevance when acute coronary occlusion is present, the timing of coronary angiography in patients without ST segment elevation remains one of the most controversial decisions to make in post CA.
The difficulty encountered in this scenario is that, even in a case of coronary cause, it is not so easy to distinguish between acute coronary events and pre-existing CAD [53].
The role of echocardiography in this setting is limited. A considerable amount of myocardial disfunction detected through TTE in post CA could be attributed to preexisting or new cardiac injury, especially those presenting with new RWMA which could be related to an underlying coronary stenosis in need for urgent angiography. [54]. Nonetheless, as mentioned before, such findings are not specific as they might be manifestation of PAMD, so echocardiography should be considered as an adjunctive piece in guiding global management of the patient, but it does not provide information that can help clinicians in the determination of the timing of coronary angiography.
However, two randomized prospective trials as TOMAHAWK trial (Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation) and COACT trial (Coronary Angiography after Cardiac Arrest without ST-Segment Elevation) had already shown that a strategy of immediate angiography was not found to be better than delayed angiography in terms of prognostic meaning. [60,61].
4. Prognostic Role of Echocardiography in Resuscitated CA Patients: Future Perspective
As already mentioned before, PAMD generally recovers by 72 hours after resuscitation. On the contrary, if PAMD is persistent after 72 hours, it is often associated with worse prognosis [54]. Interestingly, a scoping review by Liu et al. [27] analyzing data already present in literature, showed that post-arrest LVEF is not associated with statistical changes in survival or neurologic outcomes [34,62]. On the contrary, two different studies demonstrated that echocardiographic parameters with prognostic meaning associated with worse survival to hospital discharge, independently of LV systolic function, were reduced right ventricular global systolic function (measured by RV fractional area change and 3D RV ejection fraction) [63] and the diastolic parameters of the ratio of early mitral Doppler filling and mitral annular excursion (E/e’), representative of LV diastolic function and filling pressures [64] Particularly, one study has suggested that LV diastolic dysfunction rather than LV systolic dysfunction is associated with increased mortality after OHCA [65].
Jentzer et al. emphasize the fundamental utilization of echocardiography not just for early, single evaluation of post-ROSC cardiac function but in the assessment of LVEF changes through serial TTE. Results shows that no significative difference in the initial LVEF between long-term survivors and non-survivors was found, while survivors had greater increases in markers of systolic function than non-survivors, highlighting that dynamic changes in systolic function are associated with outcomes after OHCA more than single static measurements.[34] These data keep in line with the concept previously exposed that some of the observed changes in TTE parameters after CA could be due to transient myocardial stunning and therefore reversible.
Table 6.
Prognostic TTE parameters.
| Parameters | TTE | Notes | |
|---|---|---|---|
|
Systolic Function |
Serial LVEF assessment RV function |
LVEF evaluated through Biplane method RV FAC and 3D RV ejection fraction* |
Dynamic changes in systolic function are associated with outcomes after OHCA more than single static measurements Reduced RV systolic function (RV FAC < 35% or 3D RV ejection fraction < 45%) associated with worse outcome |
| Diastolic function | LV diastolic function and filling pressures | Ratio of early mitral Doppler filling and mitral annular excursion (E/e’)* | LV diastolic dysfunction (E/e’ > 14) associated with increased mortality after OHCA |
FAC: fractional area change; LV: left ventricle; LVEF: left ventricle ejection fraction; OHCA: out-of-hospital cardiac arrest; RV: right ventricle; TTE: transthoracic echocardiography. *Independently of LV systolic function.
5. Conclusions
The use of focused TTE and TEE during the resuscitation of patients in CA and peri-arrest states has shown to be feasible and clinically impactful in the peri-operative, intensive care, and emergency settings. By synthesizing existing literature, we seek to identify specific echocardiographic patterns that can be utilized to stratify patients both diagnostically and prognostically. Understanding these patterns may enhance the ability to predict outcomes and tailor post-arrest interventions more effectively, ultimately improving survival and functional recovery in this vulnerable patient population. Future research should include larger studies evaluating the diagnostic value and hemodynamic and clinical impact of echocardiography-guided resuscitation.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, A.M.. and A.D.A.; validation, A.D.A., V.R. and A.M..; formal analysis, V.R.; investigation, A.M.; writing—original draft preparation, A.A.,A.S.R., G.E.D.V.; writing—review and editing, A.A.,A.S.R., G.E.D.V.; supervision, V.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- A. G. Yow, V. Rajasurya, I. Ahmed, and S. Sharma, “Sudden Cardiac Death,” StatPearls, Mar. 2024, Accessed: May 28, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/books/NBK507854/.
- C. Mehta and W. Brady, “Pulseless electrical activity in cardiac arrest: electrocardiographic presentations and management considerations based on the electrocardiogram,” Am J Emerg Med, vol. 30, no. 1, pp. 236–239, Jan. 2012, doi: 10.1016/J.AJEM.2010.08.017. [CrossRef]
- J. Rabjohns, T. Quan, K. Boniface, and A. Pourmand, “Pseudo-pulseless electrical activity in the emergency department, an evidence based approach,” Am J Emerg Med, vol. 38, no. 2, pp. 371–375, Feb. 2020, doi: 10.1016/J.AJEM.2019.158503. [CrossRef]
- J. P. Nolan et al., “European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care,” Resuscitation, vol. 161, pp. 220–269, Apr. 2021, doi: 10.1016/j.resuscitation.2021.02.012. [CrossRef]
- K. G. Hirsch et al., “Critical Care Management of Patients After Cardiac Arrest: A Scientific Statement From the American Heart Association and Neurocritical Care Society,” Circulation, vol. 149, no. 2, Jan. 2024, doi: 10.1161/CIR.0000000000001163. [CrossRef]
- A. R. Panchal et al., “Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care,” Circulation, vol. 142, no. 16_suppl_2, Oct. 2020, doi: 10.1161/CIR.0000000000000916. [CrossRef]
- A. Wong, P. Vignon, and C. Robba, “How I use ultrasound in cardiac arrest,” Intensive Care Med, vol. 49, no. 12, pp. 1531–1534, Dec. 2023, doi: 10.1007/s00134-023-07249-8. [CrossRef]
- M. B. Jensen, E. Sloth, K. M. Larsen, and M. B. Schmidt, “Transthoracic echocardiography for cardiopulmonary monitoring in intensive care,” Eur J Anaesthesiol, vol. 21, no. 9, pp. 700–707, Sep. 2004, doi: 10.1017/S0265021504009068. [CrossRef]
- D. F. Niendorff, A. J. Rassias, R. Palac, M. L. Beach, S. Costa, and M. Greenberg, “Rapid cardiac ultrasound of inpatients suffering PEA arrest performed by nonexpert sonographers,” Resuscitation, vol. 67, no. 1, pp. 81–87, Oct. 2005, doi: 10.1016/j.resuscitation.2005.04.007. [CrossRef]
- R. Breitkreutz, F. Walcher, and F. H. Seeger, “Focused echocardiographic evaluation in resuscitation management: Concept of an advanced life support–conformed algorithm,” Crit Care Med, vol. 35, no. Suppl, pp. S150–S161, May 2007, doi: 10.1097/01.CCM.0000260626.23848.FC. [CrossRef]
- C. Hernandez, K. Shuler, H. Hannan, C. Sonyika, A. Likourezos, and J. Marshall, “C.A.U.S.E.: Cardiac arrest ultra-sound exam—A better approach to managing patients in primary non-arrhythmogenic cardiac arrest,” Resuscitation, vol. 76, no. 2, pp. 198–206, Feb. 2008, doi: 10.1016/j.resuscitation.2007.06.033. [CrossRef]
- G. Prosen, M. Križmarić, J. Završnik, and Š. Grmec, “Impact of Modified Treatment in Echocardiographically Confirmed Pseudo-Pulseless Electrical Activity in Out-of-Hospital Cardiac Arrest Patients with Constant End-Tidal Carbon Dioxide Pressure during Compression Pauses,” Journal of International Medical Research, vol. 38, no. 4, pp. 1458–1467, Aug. 2010, doi: 10.1177/147323001003800428. [CrossRef]
- A. Testa et al., “The proposal of an integrated ultrasonographic approach into the ALS algorithm for cardiac arrest: the PEA protocol.,” Eur Rev Med Pharmacol Sci, vol. 14, no. 2, pp. 77–88, Feb. 2010.
- D. Lichtenstein and M. L. N. G. Malbrain, “Critical care ultrasound in cardiac arrest. Technological requirements for performing the SESAME-protocol — a holistic approach,” Anestezjol Intens Ter, vol. 47, no. 5, pp. 471–481, Dec. 2015, doi: 10.5603/AIT.a2015.0072. [CrossRef]
- P. R. Atkinson, N. Beckett, J. French, A. Banerjee, J. Fraser, and D. Lewis, “Does Point-of-care Ultrasound Use Impact Resuscitation Length, Rates of Intervention, and Clinical Outcomes During Cardiac Arrest? A Study from the Sonography in Hypotension and Cardiac Arrest in the Emergency Department (SHoC-ED) Investigators,” Cureus, Apr. 2019, doi: 10.7759/cureus.4456. [CrossRef]
- P. Atkinson et al., “International Federation for Emergency Medicine Consensus Statement: Sonography in hypotension and cardiac arrest (SHoC): An international consensus on the use of point of care ultrasound for undifferentiated hypotension and during cardiac arrest,” CJEM, vol. 19, no. 06, pp. 459–470, Nov. 2017, doi: 10.1017/cem.2016.394. [CrossRef]
- D. Ávila-Reyes, A. O. Acevedo-Cardona, J. F. Gómez-González, D. R. Echeverry-Piedrahita, M. Aguirre-Flórez, and A. Giraldo-Diaconeasa, “Point-of-care ultrasound in cardiorespiratory arrest (POCUS-CA): narrative review article,” Ultrasound J, vol. 13, no. 1, p. 46, Dec. 2021, doi: 10.1186/s13089-021-00248-0. [CrossRef]
- P. Blanco and C. Martínez Buendía, “Point-of-care ultrasound in cardiopulmonary resuscitation: a concise review,” J Ultrasound, vol. 20, no. 3, pp. 193–198, Sep. 2017, doi: 10.1007/s40477-017-0256-3. [CrossRef]
- J. White, “The Value of Focused Echocardiography During Cardiac Arrest,” Journal of Diagnostic Medical Sonography, vol. 35, no. 6, pp. 484–490, Nov. 2019, doi: 10.1177/8756479319870171. [CrossRef]
- A. Osman and K. M. Sum, “Role of upper airway ultrasound in airway management,” J Intensive Care, vol. 4, no. 1, p. 52, Dec. 2016, doi: 10.1186/s40560-016-0174-z. [CrossRef]
- P. H. Mayo et al., “Thoracic ultrasonography: a narrative review,” Intensive Care Med, vol. 45, no. 9, pp. 1200–1211, Sep. 2019, doi: 10.1007/s00134-019-05725-8. [CrossRef]
- F. Teran et al., “Focused Transesophageal Echocardiography During Cardiac Arrest Resuscitation,” J Am Coll Cardiol, vol. 76, no. 6, pp. 745–754, Aug. 2020, doi: 10.1016/j.jacc.2020.05.074. [CrossRef]
- G. Riendeau Beaulac et al., “Transesophageal Echocardiography in Patients in Cardiac Arrest: The Heart and Beyond,” Canadian Journal of Cardiology, vol. 39, no. 4, pp. 458–473, Apr. 2023, doi: 10.1016/j.cjca.2022.12.027. [CrossRef]
- L. Hussein et al., “Transoesophageal echocardiography in cardiac arrest: A systematic review,” Resuscitation, vol. 168, pp. 167–175, Nov. 2021, doi: 10.1016/j.resuscitation.2021.08.001. [CrossRef]
- D. Borde et al., “Use of a Video Laryngoscope to Reduce Complications of Transesophageal Echocardiography Probe Insertion: A Multicenter Randomized Study,” J Cardiothorac Vasc Anesth, vol. 36, no. 12, pp. 4289–4295, Dec. 2022, doi: 10.1053/j.jvca.2022.07.017. [CrossRef]
- C. T. Buschmann and M. Tsokos, “Frequent and rare complications of resuscitation attempts,” Intensive Care Med, vol. 35, no. 3, pp. 397–404, Mar. 2009, doi: 10.1007/s00134-008-1255-9. [CrossRef]
- L. Liu et al., “Scoping review of echocardiographic parameters associated with diagnosis and prognosis after resuscitated sudden cardiac arrest,” Resuscitation, vol. 184, p. 109719, Mar. 2023, doi: 10.1016/j.resuscitation.2023.109719. [CrossRef]
- L. Elfwén et al., “Focused cardiac ultrasound after return of spontaneous circulation in cardiac-arrest patients,” Resuscitation, vol. 142, pp. 16–22, Sep. 2019, doi: 10.1016/j.resuscitation.2019.06.282. [CrossRef]
- C. Lott et al., “European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances,” Resuscitation, vol. 161, pp. 152–219, Apr. 2021, doi: 10.1016/j.resuscitation.2021.02.011. [CrossRef]
- S. V Konstantinides et al., “2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS),” Eur Heart J, vol. 41, no. 4, pp. 543–603, Jan. 2020, doi: 10.1093/eurheartj/ehz405. [CrossRef]
- M. F. Nasser et al., “Echocardiographic Evaluation of Pulmonary Embolism: A Review,” Journal of the American Society of Echocardiography, vol. 36, no. 9, pp. 906–912, Sep. 2023, doi: 10.1016/j.echo.2023.05.006. [CrossRef]
- M. D’Alto et al., “Echocardiographic probability of pulmonary hypertension: a validation study,” European Respiratory Journal, vol. 60, no. 2, p. 2102548, Aug. 2022, doi: 10.1183/13993003.02548-2021. [CrossRef]
- E. Arbelo et al., “2023 ESC Guidelines for the management of cardiomyopathies,” Eur Heart J, vol. 44, no. 37, pp. 3503–3626, Oct. 2023, doi: 10.1093/eurheartj/ehad194. [CrossRef]
- J. C. Jentzer et al., “Changes in left ventricular systolic and diastolic function on serial echocardiography after out-of-hospital cardiac arrest,” Resuscitation, vol. 126, pp. 1–6, May 2018, doi: 10.1016/j.resuscitation.2018.01.050. [CrossRef]
- N. Flint and R. J. Siegel, “Echo-Guided Pericardiocentesis: When and How Should It Be Performed?,” Curr Cardiol Rep, vol. 22, no. 8, p. 71, Aug. 2020, doi: 10.1007/s11886-020-01320-2. [CrossRef]
- C. T. Buschmann and M. Tsokos, “Frequent and rare complications of resuscitation attempts,” Intensive Care Med, vol. 35, no. 3, pp. 397–404, Mar. 2009, doi: 10.1007/s00134-008-1255-9. [CrossRef]
- M. C. Pastore et al., “Bedside Ultrasound for Hemodynamic Monitoring in Cardiac Intensive Care Unit,” J Clin Med, vol. 11, no. 24, p. 7538, Dec. 2022, doi: 10.3390/jcm11247538. [CrossRef]
- J. H. Boyd, D. Sirounis, J. Maizel, and M. Slama, “Echocardiography as a guide for fluid management,” Crit Care, vol. 20, no. 1, p. 274, Dec. 2016, doi: 10.1186/s13054-016-1407-1. [CrossRef]
- P. Pellicori, D. Hunter, H. H. Ei Khin, and J. G. F. Cleland, “How to diagnose and treat venous congestion in heart failure,” Eur Heart J, vol. 45, no. 15, pp. 1295–1297, Apr. 2024, doi: 10.1093/eurheartj/ehad883. [CrossRef]
- W. Beaubien-Souligny et al., “Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system,” Ultrasound J, vol. 12, no. 1, p. 16, Dec. 2020, doi: 10.1186/s13089-020-00163-w. [CrossRef]
- G. Tavazzi, R. Spiegel, P. Rola, S. Price, F. Corradi, and M. Hockstein, “Multiorgan evaluation of perfusion and congestion using ultrasound in patients with shock,” Eur Heart J Acute Cardiovasc Care, vol. 12, no. 5, pp. 344–352, May 2023, doi: 10.1093/ehjacc/zuad025. [CrossRef]
- M. Gaubert et al., “Doppler echocardiography for assessment of systemic vascular resistances in cardiogenic shock patients,” Eur Heart J Acute Cardiovasc Care, vol. 9, no. 2, pp. 102–107, Mar. 2020, doi: 10.1177/2048872618795514. [CrossRef]
- P. Lindqvist, S. Soderberg, M. C. Gonzalez, E. Tossavainen, and M. Y. Henein, “Echocardiography based estimation of pulmonary vascular resistance in patients with pulmonary hypertension: a simultaneous Doppler echocardiography and cardiac catheterization study,” European Journal of Echocardiography, vol. 12, no. 12, pp. 961–966, Dec. 2011, doi: 10.1093/ejechocard/jer222. [CrossRef]
- A. Gamarra, P. Díez-Villanueva, J. Salamanca, R. Aguilar, P. Mahía, and F. Alfonso, “Development and Clinical Application of Left Ventricular–Arterial Coupling Non-Invasive Assessment Methods,” J Cardiovasc Dev Dis, vol. 11, no. 5, p. 141, Apr. 2024, doi: 10.3390/jcdd11050141. [CrossRef]
- R. Kazimierczyk et al., “Echocardiographic Assessment of Right Ventricular–Arterial Coupling in Predicting Prognosis of Pulmonary Arterial Hypertension Patients,” J Clin Med, vol. 10, no. 13, p. 2995, Jul. 2021, doi: 10.3390/jcm10132995. [CrossRef]
- R. Arntfield, J. Pace, S. McLeod, J. Granton, A. Hegazy, and L. Lingard, “Focused transesophageal echocardiography for emergency physicians—description and results from simulation training of a structured four-view examination,” Crit Ultrasound J, vol. 7, no. 1, p. 10, Dec. 2015, doi: 10.1186/s13089-015-0027-3. [CrossRef]
- R. Arntfield, J. Pace, M. Hewak, and D. Thompson, “Focused Transesophageal Echocardiography by Emergency Physicians is Feasible and Clinically Influential: Observational Results from a Novel Ultrasound Program,” J Emerg Med, vol. 50, no. 2, pp. 286–294, Feb. 2016, doi: 10.1016/j.jemermed.2015.09.018. [CrossRef]
- R. Arntfield, V. Lau, Y. Landry, F. Priestap, and I. Ball, “Impact of Critical Care Transesophageal Echocardiography in Medical–Surgical ICU Patients: Characteristics and Results From 274 Consecutive Examinations,” J Intensive Care Med, vol. 35, no. 9, pp. 896–902, Sep. 2020, doi: 10.1177/0885066618797271. [CrossRef]
- F. Teran et al., “Resuscitative transesophageal echocardiography in emergency departments in the United States and Canada: A cross-sectional survey,” Am J Emerg Med, vol. 76, pp. 164–172, Feb. 2024, doi: 10.1016/j.ajem.2023.11.041. [CrossRef]
- Y. A. Cavayas, M. Girard, G. Desjardins, and A. Y. Denault, “Transesophageal lung ultrasonography: a novel technique for investigating hypoxemia,” Canadian Journal of Anesthesia/Journal canadien d’anesthésie, vol. 63, no. 11, pp. 1266–1276, Nov. 2016, doi: 10.1007/s12630-016-0702-2. [CrossRef]
- A. Y. Denault et al., “Transgastric Abdominal Ultrasonography in Anesthesia and Critical Care: Review and Proposed Approach,” Anesth Analg, vol. 133, no. 3, pp. 630–647, Sep. 2021, doi: 10.1213/ANE.0000000000005537. [CrossRef]
- A. D’Andrea et al., “Transcranial Doppler ultrasonography: From methodology to major clinical applications,” World J Cardiol, vol. 8, no. 7, p. 383, 2016, doi: 10.4330/wjc.v8.i7.383. [CrossRef]
- T. Lazzarin et al., “Post-Cardiac Arrest: Mechanisms, Management, and Future Perspectives,” J Clin Med, vol. 12, no. 1, p. 259, Dec. 2022, doi: 10.3390/jcm12010259. [CrossRef]
- L. Elfwén et al., “Post-resuscitation myocardial dysfunction in out-of-hospital cardiac arrest patients randomized to immediate coronary angiography versus standard of care,” IJC Heart & Vasculature, vol. 27, p. 100483, Apr. 2020, doi: 10.1016/j.ijcha.2020.100483. [CrossRef]
- S. Rodríguez-Villar et al., “Systemic acidemia impairs cardiac function in critically Ill patients,” EClinicalMedicine, vol. 37, p. 100956, Jul. 2021, doi: 10.1016/j.eclinm.2021.100956. [CrossRef]
- M. G. Frasch and D. A. Giussani, “Heart during acidosis: Etiology and early detection of cardiac dysfunction,” EClinicalMedicine, vol. 37, p. 100994, Jul. 2021, doi: 10.1016/j.eclinm.2021.100994. [CrossRef]
- K.-C. Cha et al., “Echocardiographic patterns of postresuscitation myocardial dysfunction,” Resuscitation, vol. 124, pp. 90–95, Mar. 2018, doi: 10.1016/j.resuscitation.2018.01.019. [CrossRef]
- J. C. Jentzer, M. D. Chonde, and C. Dezfulian, “Myocardial Dysfunction and Shock after Cardiac Arrest,” Biomed Res Int, vol. 2015, pp. 1–14, 2015, doi: 10.1155/2015/314796. [CrossRef]
- M. Ruiz-Bailén et al., “Reversible myocardial dysfunction after cardiopulmonary resuscitation,” Resuscitation, vol. 66, no. 2, pp. 175–181, Aug. 2005, doi: 10.1016/j.resuscitation.2005.01.012. [CrossRef]
- S. Desch et al., “Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation,” New England Journal of Medicine, vol. 385, no. 27, pp. 2544–2553, Dec. 2021, doi: 10.1056/NEJMoa2101909. [CrossRef]
- J. S. Lemkes et al., “Coronary Angiography after Cardiac Arrest without ST-Segment Elevation,” New England Journal of Medicine, vol. 380, no. 15, pp. 1397–1407, Apr. 2019, doi: 10.1056/NEJMoa1816897. [CrossRef]
- J. C. Jentzer et al., “Echocardiographic left ventricular systolic dysfunction early after resuscitation from cardiac arrest does not predict mortality or vasopressor requirements,” Resuscitation, vol. 106, pp. 58–64, Sep. 2016, doi: 10.1016/j.resuscitation.2016.06.028. [CrossRef]
- V. Ramjee et al., “Right ventricular dysfunction after resuscitation predicts poor outcomes in cardiac arrest patients independent of left ventricular function,” Resuscitation, vol. 96, pp. 186–191, Nov. 2015, doi: 10.1016/j.resuscitation.2015.08.008. [CrossRef]
- J. C. Jentzer et al., “Echocardiographic left ventricular diastolic dysfunction predicts hospital mortality after out-of-hospital cardiac arrest,” J Crit Care, vol. 47, pp. 114–120, Oct. 2018, doi: 10.1016/j.jcrc.2018.06.016. [CrossRef]
- W.-T. Chang et al., “Postresuscitation myocardial dysfunction: correlated factors and prognostic implications,” Intensive Care Med, vol. 33, no. 1, pp. 88–95, Jan. 2007, doi: 10.1007/s00134-006-0442-9. [CrossRef]
Figure 1.
Adult post-arrest care algorithm. CT: Computed Tomography; ECG: Electrocardiogram; EEG: Electroencephalogram; PaCO2: Partial pressure of CO2; SpO2: Saturation of peripheral O2; ROSC: Return of spontaneous circulation; STEMI: ST elevation myocardial infarction.
Figure 1.
Adult post-arrest care algorithm. CT: Computed Tomography; ECG: Electrocardiogram; EEG: Electroencephalogram; PaCO2: Partial pressure of CO2; SpO2: Saturation of peripheral O2; ROSC: Return of spontaneous circulation; STEMI: ST elevation myocardial infarction.
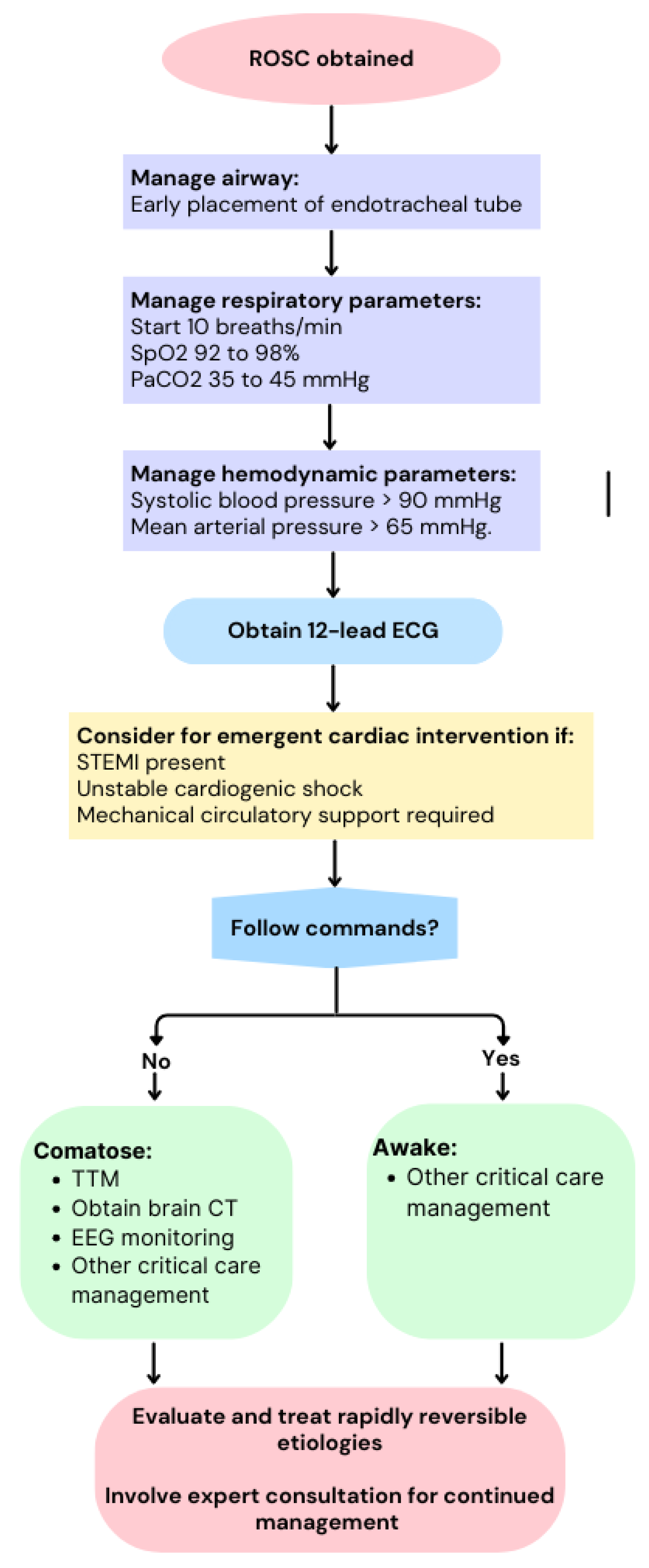
Figure 2.
TEE performed during CPR in a patient with CA and non-shockable rhythm presentation, showing in-transit thrombus in right chambers suggesting PE as CA cause. Notably, the patient was affected by hypertrophic cardiomyopathy (a,b); vascular ultrasound performed in the same patient after cardiac resuscitation showed deep vein thrombosis involving superficial femoral vein (c).
Figure 2.
TEE performed during CPR in a patient with CA and non-shockable rhythm presentation, showing in-transit thrombus in right chambers suggesting PE as CA cause. Notably, the patient was affected by hypertrophic cardiomyopathy (a,b); vascular ultrasound performed in the same patient after cardiac resuscitation showed deep vein thrombosis involving superficial femoral vein (c).
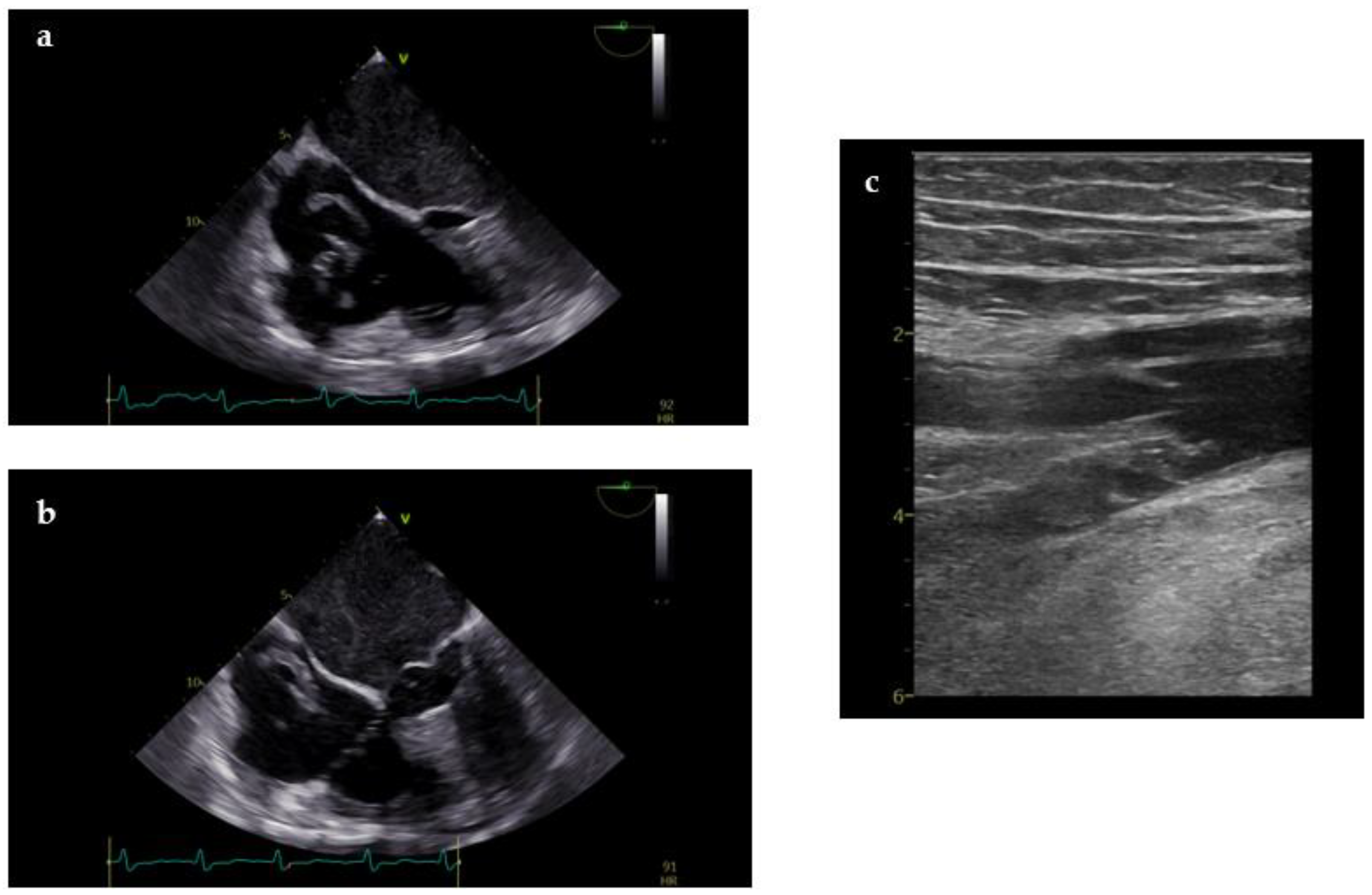
Figure 3.
TTE performed during CPR showing cardiac tamponade as cause of CA (a,b); after diagnosis percutaneous pericardiocentesis with US guidance was performed leading to resolution of CA (c); TTE performed during post-resuscitation care showing complete resolution of pericardial effusion and tamponade (d,e). .
Figure 3.
TTE performed during CPR showing cardiac tamponade as cause of CA (a,b); after diagnosis percutaneous pericardiocentesis with US guidance was performed leading to resolution of CA (c); TTE performed during post-resuscitation care showing complete resolution of pericardial effusion and tamponade (d,e). .
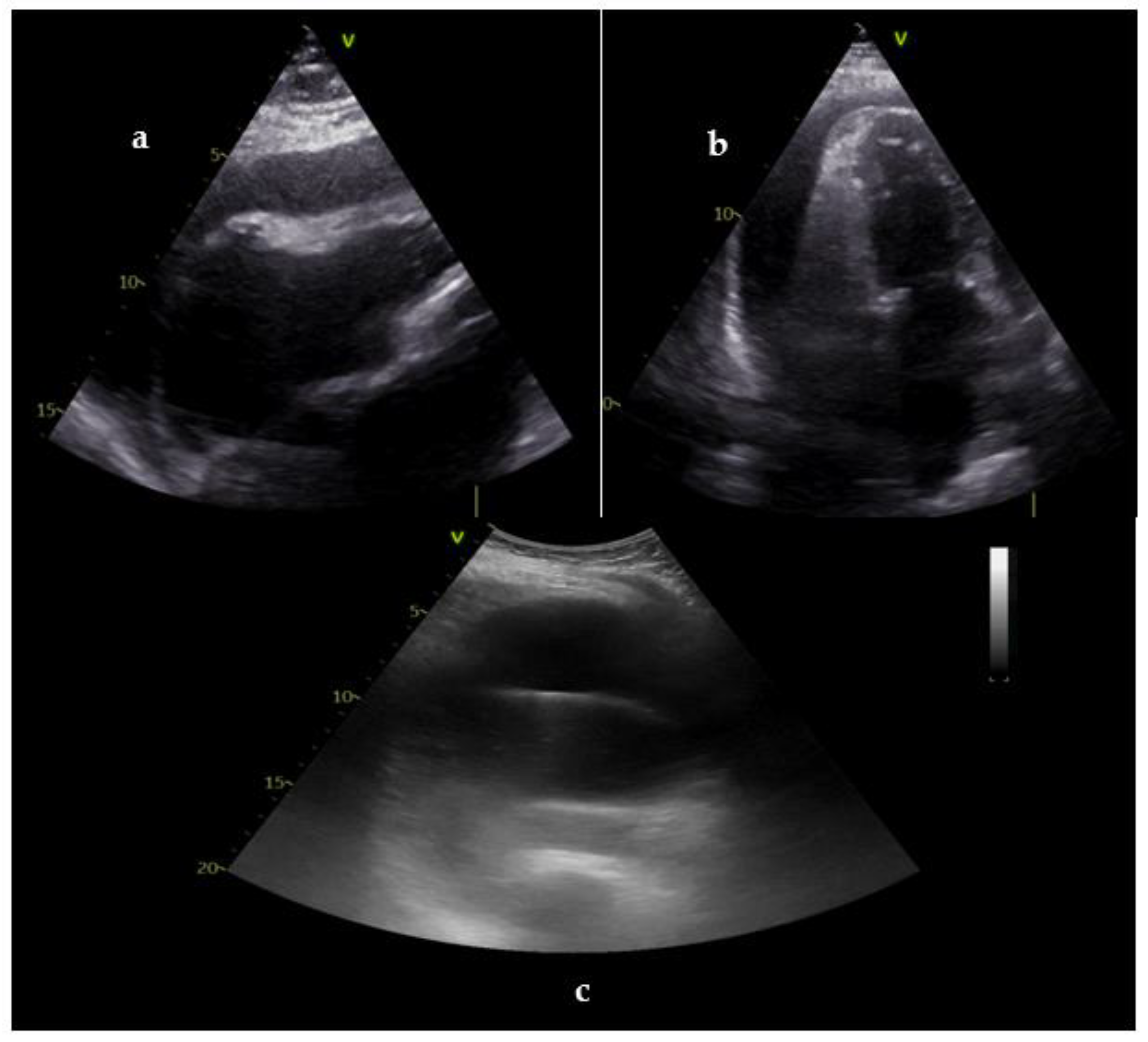

Table 1.
Goals of ultrasounds during cardiopulmonary resuscitation and after restoration of spontaneous circulation.
Table 1.
Goals of ultrasounds during cardiopulmonary resuscitation and after restoration of spontaneous circulation.
| Goals of US during CPR | Goals of US in post-resuscitation care |
|---|---|
| Diagnosis of reversible causes | Diagnosis of underlying cause of CA |
| Confirm effectiveness of chest compressions | Hemodynamic monitoring and optimization |
| Determine presence of cardiac contractions or ‘standstill’ | Assist ventilatory support |
| Confirm bilateral ventilation after intubation | Assessment of CPR complication |
| Assist invasive procedures (pericardiocentesis, vascular cannulation, extracorporeal CPR) | Assessment multiorgan function (prognosis) |
| Assist invasive procedures |
CA: cardiac arrest; CPR: cardiopulmonary resuscitation; US: ultrasound.
Table 2.
Ultrasound signs for reversible causes.
| Potential cause | US views | Suggestive findings | Intervention |
|---|---|---|---|
|
Profound hypovolemia |
Subcostal Abdomen |
Small LV and RV cavity size Near end-systolic obliteration (‘kissing ventricle’) Collapsed IVC (< 10 mm) Massive bleeding in abdomen |
Fluid administration; assess response |
|
Cardiac tamponade |
Subcostal | Pericardial effusion Collapsed cardiac chambers Congested IVC |
Pericardiocentesis; guide the procedure and assess response |
| Massive pulmonary embolism | Subcostal Lower limbs |
Markedly dilated RV Pressure overload of RV Thrombus-in-transit Congested IVC Presence of DVT (positive CUS) |
Consideration of thrombolysis |
|
Tension pneumothorax |
Lung | Absence of lung sliding during ventilation | Needle decompression, assess response |
CUS: compression ultrasound; DVT: deep vein thrombosis; IVC: inferior cava vein; LV: left ventricle; RV: right ventricle; US: ultrasounds.
Table 3.
Transesophageal echocardiography during cardiopulmonary resuscitation.
| View | Goals and diagnosis |
|---|---|
| 1. ME 4C (0-10°) | Tamponade Evaluation of LV/RV contractility Signs of PE Signs of profound hypovolemia Signs of compression due to pneumothorax |
| 2. ME LAX (120°-140°) | Determine AMC Optimization of chest compression avoiding LVOT obstruction Evaluation of AscAo |
| 3. TG SAX (0-20°) | Tamponade Evaluation of LV/RVcontractility Signs of PE Signs of profound hypovolemia; |
| 4. ME bicaval (90°) | Evaluation of intravascular volume (SCV) Thrombus in transit Assist venous procedures |
| 5. TG and ME DescAO SAX (0-10°) | Evaluation of DescAo Assist arterial procedures |
4C: 4-chamber; AMC: area of maximal compression; AscAo: ascending aorta; DescAo, descending aorta; LAX, long axis; LVOT: left ventricular outflow tract; ME: midesophageal; PE: pulmonary embolism; SAX, short axis; SCV: superior cava vein; TG: transgastric.
Table 4.
Main echocardiographic features of acute pulmonary embolism.
| Echocardiographic findings | Parameters |
|---|---|
| RV dilatation | RV/LV ratio > 1 RV basal diameter > 41 mm RV mid diameter > 35 mm |
| RV systolic disfunction | TAPSE < 17 mm S’ wave (TDI) < 10 cm/sec RV-FAC < 35% RV Tei index (PW) > 0.43 RV Tei index (TDI) > 0.54 RV free wall strain > -20% |
| McConnell Sign | RV basal and mid free wall akinesia and normal motion of the RV apex |
| RV pressure overload | TR Vmax > 2.9 m/sec Pulmonary flow AcT < 60 msec Pulmonary flow mid-systolic notch Paradoxical IVS motion Flattened IVS with D-shaped LV Dilated PA (> 25 mm) TAPSE: PASP ratio < 0.4 Dilated IVC (>21 mm) and/or diminished collapsibility |
| 60/60 Sign | TR jet gradient < 60 mmHg and Pulmonary AcT < 60 ms |
| Thrombus in transit | Thrombus in RV, RA or PA |
AcT: acceleration time; FAC: fractional area change; IVS: interventricular septum; LV: left ventricle; PA: pulmonary artery; PASP: pulmonary artery systolic pressure; PW: pulsed wave; RA: right atrium; RV: right ventricle; TAPSE: tricuspid annular planar systolic excursion; TDI: tissue doppler imaging; TR: tricuspid regurgitation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



