Submitted:
26 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
Celiac disease is a chronic small intestinal immune-mediated enteropathy precipitated by exposure to dietary gluten, affecting approximately 1% of the global population and two million Americans. An increasing number of studies have identified a link between celiac disease and adverse maternal and fetal outcomes during pregnancy and after birth. Additionally, both celiac disease and pregnancy are associated with an increased risk for nutrient deficiencies, specifically vitamin B12 and folate. Deficiencies in these key nutrients are linked with several negative maternal and fetal health outcomes including preeclampsia, gestational diabetes, spontaneous abortion/miscarriage, preterm birth, NTDs, Intrauterine Growth Restriction, and low gestational age and birthweight. This review examines the current literature related to the folate trap and vitamin B12 deficiency in patients with celiac disease and pregnant women independently, and to provide rationale for future research to explore the correlation between the folate to B12 ratio in pregnant woman with celiac disease.
Keywords:
Vitamin B12
; Folate
; Folic Acid
; Celiac Disease
; Pregnancy
1. Introduction
Vitamin B12 and folate are essential vitamins involved in DNA synthesis, methylation pathways, and cell growth [1]. They have strong protective mental health benefits and have shown associations in chronic disease prevention [2]. However, during vitamin B12 deficiency, folate becomes ‘trapped’ in its methylated form, unable to drive other enzymatic processes essential for transmethylation pathways. This, in turn, leads to a buildup of homocysteine that has been linked to cardiovascular disease and cognitive decline, including dementia and Alzheimer’s Disease [3,4]. Vitamin B12 and folate intake requirements increase during pregnancy to prevent neural tube defects, preterm birth, small gestational birthweight, and miscarriage [5,6,7]. Individuals with celiac disease are another population prone to vitamin B12 deficiency due to the malabsorption [8]. Celiac disease is often associated with worse pregnancy outcomes, but few studies have investigated the relationship between folate and vitamin B12 deficiency in pregnant women with celiac disease. The folate trap has the potential to exacerbate the impacts of vitamin B12 deficiency in pregnant women with celiac disease that may be detrimental to both maternal and fetal outcomes (Figure 1). The purpose of this review is to explore the relationships between the folate trap and vitamin B12 deficiency in the context of pregnancy and celiac disease, discuss associations between celiac disease and pregnancy outcomes, and identify current gaps in knowledge.
2. Folate and Vitamin B12 Requirements and Prevalence of Deficiency
Vitamin B12 is an essential water-soluble B vitamin that is produced exclusively by bacteria and rare algae. The human microbiome is unable to synthesize sufficient vitamin B12 to sustain life. Thus, consumption of animal products or supplementation is required [9]. Deficiency has been linked with several adverse health outcomes outlined in Table 1 [10,11,12]. The Institute of Medicine recommends 2.4 μg/day of vitamin B12 for adults, with an increase to 2.6 μg /day in pregnant women [13] (Table 3). Data from the National Health and Nutrition Examination Survey (NHANES) from 2007-2018 found that roughly 3.6% of US adults were vitamin B12 deficient (serum <148 pmol/L) and 12.5% had sub-clinical deficiency (<221 pmol/L) [13]. Vitamin B12 deficiency is particularly prevalent in low- and middle-income countries (40% in Latin America, 70% in Sub-Saharan Africa, and 70-80% in South Asia) [6,14].
Folate (vitamin B9) is also an essential water-soluble vitamin that plays an essential role in cell growth and division, DNA & RNA synthesis, and maintenance of new cells [15]. Folate must be obtained through the diet or via supplementation from folic acid, the synthetic form of folate [16]. Folic acid is roughly twice as bioavailable than natural folate [17]. Deficiency can be caused by poor diet, malabsorption due to certain chronic and autoimmune diseases (e.g. celiac disease, short bowel syndrome, amyloidosis, gastric bypass), and drug or alcohol abuse and can develop within weeks to months of a folate-deficient diet [12,18]. Table 2 outlines manifestations of folate deficiency [12,18,19,20]. In a systematic review of 45 surveys conducted in 39 countries over 14 years, folate deficiency ranged from <1% to 88% [21]. This discrepancy was partly due to country income-level and multiple methods of measuring folate. Folate deficiency in the US in recent years is not common due to fortification initiatives, and in fact, it is estimated that more than one-third of the North American population consumes excess folate [22]. It is estimated that adult body has 1,000-2,000 μg of folate stores, and adults require 400 μg per day to replenish those stores and 600 μg /day for pregnant women [15] (Table 3). Normal serum folate levels are above 4 ng/mL, subclinical deficiency is between 3-4 ng/mL, and under 2 ng/mL is considered clinical deficiency [2].
3. Diagnosis of Folate and Vitamin B12 Deficiency
There are numerous methods to assess folate and vitamin B12 deficiency. The World Health Organization guidelines classify total serum vitamin B12 levels above 221 pmol/L as adequate, 148-221 pmol/L as low, and levels under 148 as deficient [5]. Serum vitamin B12 is widely used in clinical practice and in research and measures the total amount of vitamin B12 in the blood, of which only about 20% is metabolically active and available for cellular uptake, leading to under-reporting of deficiency [11]. Holo-transcobalamin (holoTC) is considered a more accurate measure of vitamin B12, but it is still much less common in practice [23]. When vitamin B12 enters the digestive system, it binds to haptocorrin, intrinsic factor, and transcobalamin. Holo-TC measures the amount of circulating vitamin B12 bound to transcobalamin that is bioavailable to cells. Plasma homocysteine and methylmalonic acid (MMA) are functional measures of vitamin B12 because both rely on vitamin B12 to be converted to methionine and succinyl-CoA, respectively. Elevated levels of either can indicate vitamin B12 insufficiency, with Hcy as a more sensitive measure, but MMA is more specific as HHcy may indicate other vitamin deficiencies [10]. Elevated blood Hcy levels >15umol/L are considered elevated, whereas MMA levels >260nmol/L are considered elevated [5].
As discussed above, serum folate levels under 2 ng/mL are considered deficient. However, as is true for vitamin B12, serum folate levels are not always accurate and does not account for unmetabolized folate or the variations of folate at different points in its metabolic cycle. Serum folate represents recent dietary intake, whereas red blood cell (RBC) folate is a more accurate long-term reflection [10]. Folate deficiency can be confirmed with elevated Hcy, as with vitamin B12 deficiency, but with normal vitamin B12 and MMA levels in the plasma.
4. Folate Trap
One-carbon metabolism is a series of metabolic reactions involving the donation of single carbon units (methyl groups) to aid in DNA, protein, and lipid biosynthesis and amino acid homeostasis [24]. The folate cycle is a component of one-carbon metabolism, working synergistically with the methionine cycle. Within the folate cycle, during the conversion of 5-MTHF to THF, 5-MTH donates a methyl group to cobalamin (vitamin B12), which becomes methyl cobalamin, catalyzed by the methionine synthase enzyme. Methyl cobalamin then donates a methyl group to homocysteine to form methionine. Methionine is then converted into s-adenosyl methionine (SAM) and eventually s-adenosyl homocysteine (SAH) before returning to its homocysteine form. In the conversion of SAM to SAH, a methyl group is released to be used in the transmethylation pathway that drives gene regulation [10].
In the context of vitamin B12 deficiency, this cycle is fragmented as 5-MTHF cannot be converted to THF and homocysteine cannot accept a methyl group from methyl cobalamin. This causes folate to become “trapped” in its 5-MTHF form, unable to drive the multitude of downstream reactions. This prevents the conversion of homocysteine (Hcy) to methionine [25]. When this occurs, Hcy levels are often elevated in the blood, known as hyperhomocysteinemia (HHcy), which has been linked to dementia, stroke, recurrent early pregnancy loss, endothelial cell injury, and cardiovascular disease [11,25,26,27,28].
The body cannot naturally synthesize folate, so it instead relies on dietary or supplemental intake. 5-MTHF is the biologically active form of folate that can be used in one carbon metabolism and the primary form of folate in blood plasma. Folic acid is the synthetic, monoglutamate precursor of folate that is found in supplements and fortified foods, primarily grains [15]. It’s then converted via multi-step enzymatic reactions to the biologically active form, relying on slow-acting and highly variable dihydrofolate reductase (DHFR) to convert folic acid to dihydrofolate in the initial step. Naturally occurring food folates, on the other hand, are not limited by the function of the DHFR enzyme and instead bypass this reaction when being converted into 5-MTHF (Figure 2). Regardless of the form of folate or folic acid, a vitamin B12 deficiency inhibits the folate acid cycle and halts downstream metabolic processes.
5. Folic Acid Fortification in the US and Exacerbation of Vitamin B12 Deficiency
5.1. Implementation of Folic Acid Fortification Programs
A folic acid fortification program was developed the United States in 1998 aimed at reducing neural tube defects (NTDs). Canada, Chile, and Australia followed and now more than 80 countries have guidelines in place [29]. According to data from the National Health and Nutrition Examination Survey (NHANES) pre- and post-fortification in the US, serum folate concentrations increased by 119-161% and RBC folate increased by 44-64% and the prevalence of low serum folate decreased from 21% to <1% in women of childbearing age and low RBC folate declined from 38% to 5% [30]. Not surprisingly, serum vitamin B12 levels did not change significantly, increasing an unbalanced ratio of folate to vitamin B12 [30]. In the US, NHANES data demonstrated that serum folate concentrations in the post-fortification era have substantially increased leading to 31% decrease in NTD incidence [31]. Another randomized double-blind prevention trial revealed a 72% protective effect of folic acid supplementation on preventing NTDs [32].
5.2. Elevated Folate Levels May Exacerbate Vitamin B12 Deficiency
While fortification successfully reduced the percent of the population with folate deficiency, it may have added too much folate to the diet. Despite the many benefits of sufficient folate levels, adequate or increased folate levels have been associated with exacerbating the health effects of vitamin B12 deficiency. High serum folate (>20ng/mL) was found in 42% of children and 38% of elderly, compared to 5% and 7% pre-fortification, respectively [30]. Furthermore, the combination of insufficient vitamin B12 and elevated serum folate increased from 0.09% to 0.61% post fortification [33]. High plasma folate, as seen more post-fortification, is associated with amplifying clinical implications of vitamin B12 deficiency [34,35,36].
In addition to blood folate levels, The Framingham Offspring Cohort Study and NHANES data found increased prevalence of high circulating folic acid after fortification [34,37]. In a 2007 study, healthy adults were given fortified bread with varying levels of folic acid, up to 400 μg. In the group given 400 μg of folic acid, unmetabolized folic acid was detected in plasma [38]. Unmetabolized folic acid has also been detected in umbilical cord blood from infants, which has the potential to interfere with folate metabolism [39,40,41]. Unmetabolized folic acid may be indicative of enzymatic saturation leading to decreased conversion of folic acid into 5-MTHF. These increases in blood folate and unmetabolized folic acid levels were seen after fortification guidelines were put in place, when vitamin B12 levels have not changed substantially. There has been a push to include vitamin B12 fortification along with folic acid to ensure adequate levels of both nutrients and prevent exacerbation of the impacts of vitamin B12 deficiency [35,42].
6. Folic Acid and Vitamin B12 Needs in Pregnancy
Folic Acid and vitamin B12 intake requirements increase during pregnancy to meet increased biological need. Infant vitamin B12 and folate status at delivery is most largely influenced by maternal cobalamin and folate levels, but also varies based on placental function, gestational age, and birth weight [5,6,7]. The placenta has many folate receptors that help to regulate folate and cobalamin transfer to the fetus. Pregnancy requires a five-to-ten-fold increase in folate [15]. It is recommended that women take a folic acid supplement with at least 0.4mg daily during pregnancy, but vitamin B12 supplementation is not recommended at the same frequency [18]. Studies have found vitamin B12 deficiencies in pregnant women to be between 18 and 43% in developed countries, with higher rates in areas with fewer resources [43,44,45,46].
Vitamin B12 deficiency and elevated Hcy concentrations are associated with the adverse fetal outcomes of spontaneous abortion/miscarriage, preterm birth, NTDs, Intrauterine Growth Restriction, and low gestational age and birthweight [6,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. This is especially prevalent when the vitamin B12 to folate intake ratio was imbalanced (vitamin B12 < 4.0 μg per day and folate > 268 μg per day) [61]. A meta-analysis of 18 studies identified a significant relationship between vitamin B12 deficiency and low birth weight (15% increased risk) and preterm birth (21% higher risk) [62]. A recent case study followed a woman who had suffered three miscarriages and had an elevated Hcy level of 15.9 uM. After receiving folate, vitamin B6, taurine, and cystine, her Hcy levels did not drop. This suggested that the folate trap may have been contributing to the elevated Hcy levels as all other endocrine biomarkers were within normal range. She was then treated with supplemental methyl cobalamin and adenosyl cobalamin. Four months later, her Hcy dropped to within normal range at 9.9 uM because of the addition of vitamin B12 [63]. Supplemental vitamin B12 and folate also significantly decreased the rate of NTDs compared to a minimal vitamin without those nutrients (13.3 vs 22.9 per 1000) in a randomized control trial [60]. Aside from fetal outcomes, B12 deficiency also put maternal health at risk, with up to four times the chance of preeclampsia and significantly increased risk of insulin resistance and gestational diabetes [64,65,66].
Adequate vitamin B12 levels alone, or in conjunction with enough folate, has proven to lead to positive maternal and fetal outcomes. However, vitamin B12 deficiency is often under-diagnosed in pregnant women and their children [5]. Folic acid supplementation during pregnancy is widely accepted, but the addition of vitamin B12 is rarely discussed, potentially causing imbalanced nutrient levels that prevent the methionine cycle and other downstream processes that impact the clinical health outcomes seen in pregnant women.
7. Folic Acid and Vitamin B12 Absorption in Celiac Disease
Celiac disease (CD) is defined as “a chronic small intestinal immune-mediated enteropathy precipitated by exposure to dietary gluten in genetically predisposed individuals” [67]. Gluten is a protein found in wheat, barley, rye, malt, and sometimes oats. Symptoms can present as diarrhea, weight loss, bloating, abdominal pain, and iron deficiency. The autoimmune disease can be detected through celiac-specific antibodies in bloodwork and confirmed via a duodenal mucosal biopsy [68]. CD is found in about 1% of the population, is more common in females (60-70% of CD diagnoses are women) and has seen an increase in prevalence over the last 50 years [68,69,70,71].
Celiac disease largely impacts the villi of the small intestine, the primary site of nutrient absorption. The immune response of celiac ranges in severity from mild intraepithelial lymphocytosis to total villous atrophy [8]. The disease reduces the surface area and digestive enzymes available for nutrient absorption, leading to the development of nutrient deficiencies, including iron, folic acid, B12, and B6 [68]. Folic acid is primarily absorbed in the jejunum of the small intestine, the main site impacted by CD [8]. Conversely, vitamin B12 is mostly absorbed in the ileum, the last section of the small intestine, which is also impacted in CD patients [72]. Past research has shown that 20-38% of CD patients have at least one nutritional deficiency, which could be attributed to malabsorption or deficiencies within a gluten-free diet (GFD) [8]. The GFD has been associated with decreased intake of dietary fiber, iron, and vitamin B along with increased consumption of caloric fats [8]. The reported prevalence of vitamin B12 deficiency specifically in patients with CD has ranged from 8-41% [8,73,74,75].
A complete GFD is the only treatment for the disease with no current cure [8]. For most patients, strict adherence to a GFD will lead to reversal of intestinal damage and eliminate symptoms over time [68]. A study of 40 patients with recent CD diagnoses followed severity of intestinal damage over a year of treatment and found: (1) severity of the villous atrophy was linked with vitamin B12 and erythrocyte folate concentrations and (2) most biochemical markers improved within a year of treatment with a GFD [76]. However, while most serological levels return to normal with a GFD, this is not the case for all patients and additional vitamin supplementation may be required [76,77,78,79]. However, CD is often undiagnosed in the US which impedes a patient’s ability to access treatment [68].
Even with a CD diagnosis, adherence to a GFD is impacted by several factors, with adherence rates estimated to be between 45% and 90% [81]. Barriers to diet adherence include income, knowledge about GFD, temptation control, motivation from peers, confidence in health practitioners, religious food, cost and availability of GF food, amount of counseling for GFD, and contact with health care professionals [82,83]. Over 25% of subjects stated that their income could not support a GFD. A 2019 market-based study comparing gluten-free products with their glutenous counterparts found GF products to be 183% more expensive overall [84]. Thus, there are many barriers to strict adherence to a GFD which can negatively impact the overall health of an individual with CD.
8. Celiac Disease and Pregnancy
Several studies have identified a link between CD, especially untreated CD, and worse maternal and fetal outcomes during pregnancy. The likelihood of at least one pregnancy complication is estimated to be over 4x higher in women with CD compared to the general population [85]. A recent 18-study meta-analysis identified an increased risk for spontaneous abortion, fetal growth restriction, preterm delivery, cesarean delivery, and lower mean birthweight in women with CD [86]. A case-control study comparing treated vs untreated CD patients found the relative risk of miscarriage to be 8.9 times higher in untreated women and a GFD reduced that risk 9.18 times and reduced low birth rate from 29.4% to 0% [87].
Aside from pregnancy outcomes, CD also impacts fertility, with an increased likelihood for both amenorrhea and infertility [85,88]. A meta-analysis found three-fold increased odds of having CD in those with infertility compared to the general population [94]. Some evidence has shown that once treated and adhering to a GFD, many of the fertility and pregnancy complications associated with CD resolved [86,87,90,91]. However, the mean age of CD diagnosis is 38 in the United States, often after fertile age in females [92]. This could mean years of untreated CD during the reproductive years. Studies have reported between 74.5% and 85.7% of participants being diagnosed with CD after their first pregnancy [85,93].
Asymptomatic CD is not uncommon, resulting in lack of diagnoses and/or treatment. Mayo Clinic reported only 6% of CD patients to present with classic symptoms, 66% with non-typical symptoms, and 28% asymptomatic [94]. A case study of a 37-year-old woman on her third pregnancy, with one uncomplicated past pregnancy and one with intrauterine fetal death (IUFD), revealed asymptomatic CD. In her third pregnancy, the patient presented with vaginal bleeding, iron deficiency, and high IgA levels. CD was confirmed via biopsy. After treatment with iron supplementation and a strict GFD, all biomarkers resolved, and the patient gave birth to a healthy son [95]. Despite most evidence supporting a GFD’s success in reversing negative pregnancy outcomes, lack of diagnosis or adherence to treatment remains a significant barrier for addressing these concerns.
9. Conclusion
An extensive amount of research has been conducted on the folate trap, the importance of vitamin B12 and folate supplementation in pregnancy, vitamin B12 deficiency in CD, and associations between pregnancy and CD. What has remained largely understudied are the implications of vitamin B12 deficiency in pregnant women with CD and how the folate trap may play a role in negative health outcomes. Folic acid supplementation is widely recommended during pregnancy, but complementary vitamin B12 supplementation is not standard. Numerous studies have proven the harm of vitamin B12 deficiency, which has been shown to be exacerbated in those with normal to high folate levels. This deficiency is especially prevalent in some subpopulations, notably in pregnant patients and in those with CD. An imbalanced folate to vitamin B12 ratio can cause several negative pregnancy outcomes including early abortion/miscarriage, preterm birth, NTDs, and low gestational age and birthweight. These can be easily resolved with vitamin B12 supplementation. Similarly, CD is associated with higher rates of similar outcomes that can be reversed or prevented with adherence to a GFD. However, since most people are not diagnosed with CD until after pregnancy, treatment with a GFD is often initiated after reproductive years. Additionally, the pathogenic nature of CD disrupts nutrient absorption in the small intestine, where both vitamin B12 and folate are primarily absorbed. Together, this may suggest that patients who are pregnant and have CD may be at even higher risk of maternal and fetal harm.
Ultimately, additional research is necessary to determine the impact of the folate trap and health outcomes in pregnant women with CD. Variables impacting health outcomes may include length of CD diagnosis, adherence to GFD, family history of pregnancy complications, nutrient supplementation, and more. Clinically, it may be worthwhile to screen for both CD and vitamin B12 deficiency in pregnant patients to identify those who may benefit from GFD or vitamin B12 supplementation intervention. Addressing vitamin B12 deficiency and CD in pregnant patients through early screening and targeted treatments may represent a strategy to significantly reduce maternal and fetal health risks.
Funding
Supported by funding from the VA Office of Research and Development, Summer Research Program at the Phoenix VA Health Care System.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhou, Y., Wang, A., Yeung, L. F., Qi, Y. P., Pfeiffer, C. M., & Crider, K. S. (2023). Folate and vitamin B12 usual intake and biomarker status by intake source in United States adults aged ≥19 y: NHANES 2007-2018. The American journal of clinical nutrition, 118(1), 241–254. [CrossRef]
- Watson, J., Lee, M., & Garcia-Casal, M. N. (2018). Consequences of Inadequate Intakes of Vitamin A, Vitamin B12, Vitamin D, Calcium, Iron, and Folate in Older Persons. Current geriatrics reports, 7(2), 103–113. [CrossRef]
- Lee, C. Y., Chan, L., Hu, C. J., Hong, C. T., & Chen, J. H. (2024). Role of vitamin B12 and folic acid in treatment of Alzheimer's disease: a meta-analysis of randomized control trials. Aging, 16(9), 7856–7869. [CrossRef]
- Son, P., & Lewis, L. (2022). Hyperhomocysteinemia. In StatPearls. StatPearls Publishing.
- Hannibal, L., Lysne, V., Bjørke-Monsen, A. L., Behringer, S., Grünert, S. C., Spiekerkoetter, U., Jacobsen, D. W., & Blom, H. J. (2016). Biomarkers and Algorithms for the Diagnosis of Vitamin B12 Deficiency. Frontiers in molecular biosciences, 3, 27. [CrossRef]
- Finkelstein, J. L., Layden, A. J., & Stover, P. J. (2015). Vitamin B-12 and Perinatal Health. Advances in nutrition (Bethesda, Md.), 6(5), 552–563. [CrossRef]
- Bjørke Monsen, A. L., Ueland, P. M., Vollset, S. E., Guttormsen, A. B., Markestad, T., Solheim, E., & Refsum, H. (2001). Determinants of cobalamin status in newborns. Pediatrics, 108(3), 624–630. [CrossRef]
- Theethira, T. G., Dennis, M., & Leffler, D. A. (2014). Nutritional consequences of celiac disease and the gluten-free diet. Expert review of gastroenterology & hepatology, 8(2), 123–129. [CrossRef]
- Torrez, M., Chabot-Richards, D., Babu, D., Lockhart, E., & Foucar, K. (2022). How I investigate acquired megaloblastic anemia. International journal of laboratory hematology, 44(2), 236–247. [CrossRef]
- Porter, K., Hoey, L., Hughes, C. F., Ward, M., & McNulty, H. (2016). Causes, Consequences and Public Health Implications of Low B-Vitamin Status in Ageing. Nutrients, 8(11), 725. [CrossRef]
- Werder. (2010). Cobalamin deficiency, hyperhomocysteinemia, and dementia. Neuropsychiatric Disease and Treatment, 159. [CrossRef]
- Clarke, R. (2008). B-vitamins and prevention of dementia. Proceedings of the Nutrition Society, 67(1), 75–81. [CrossRef]
- U.S. Department of Health and Human Services. (n.d.). Office of dietary supplements - vitamin B12. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/vitaminb12-healthprofessional/#:~:text=However%2C%20vitamin%20B12%20insufficiency%20(assessed,60%20and%20older%20%5B34%5D.
- Allen L. H. (2004). Folate and vitamin B12 status in the Americas. Nutrition reviews, 62(6 Pt 2), S29–S34. [CrossRef]
- Carboni L. (2022). Active Folate Versus Folic Acid: The Role of 5-MTHF (Methylfolate) in Human Health. Integrative medicine (Encinitas, Calif.), 21(3), 36–41.
- Miraglia, N., & Dehay, E. (2022). Folate Supplementation in Fertility and Pregnancy: The Advantages of (6S)5-Methyltetrahydrofolate. Alternative therapies in health and medicine, 28(4), 12–17.
- Milman N. (2012). Intestinal absorption of folic acid - new physiologic & molecular aspects. The Indian journal of medical research, 136(5), 725–728.
- Khan, K. M., & Jialal, I. (2023). Folic Acid Deficiency. In StatPearls. StatPearls Publishing.
- Reynolds E. H. (2014). The neurology of folic acid deficiency. Handbook of clinical neurology, 120, 927–943. [CrossRef]
- Kaye, A. D., Jeha, G. M., Pham, A. D., Fuller, M. C., Lerner, Z. I., Sibley, G. T., Cornett, E. M., Urits, I., Viswanath, O., & Kevil, C. G. (2020). Folic Acid Supplementation in Patients with Elevated Homocysteine Levels. Advances in therapy, 37(10), 4149–4164. [CrossRef]
- Rogers, L. M., Cordero, A. M., Pfeiffer, C. M., Hausman, D. B., Tsang, B. L., De-Regil, L. M., Rosenthal, J., Razzaghi, H., Wong, E. C., Weakland, A. P., & Bailey, L. B. (2018). Global folate status in women of reproductive age: a systematic review with emphasis on methodological issues. Annals of the New York Academy of Sciences, 1431(1), 35–57. [CrossRef]
- Fardous, A. M., & Heydari, A. R. (2023). Uncovering the Hidden Dangers and Molecular Mechanisms of Excess Folate: A Narrative Review. Nutrients, 15(21), 4699. [CrossRef]
- Nexo, E., & Hoffmann-Lücke, E. (2011). Holotranscobalamin, a marker of vitamin B-12 status: analytical aspects and clinical utility. The American journal of clinical nutrition, 94(1), 359S–365S. [CrossRef]
- Clare, C. E., Brassington, A. H., Kwong, W. Y., & Sinclair, K. D. (2019). One-Carbon Metabolism: Linking Nutritional Biochemistry to Epigenetic Programming of Long-Term Development. Annual review of animal biosciences, 7, 263–287. [CrossRef]
- Ferrazzi, E., Tiso, G., & Di Martino, D. (2020). Folic acid versus 5- methyl tetrahydrofolate supplementation in pregnancy. European journal of obstetrics, gynecology, and reproductive biology, 253, 312–319. [CrossRef]
- Nelen, W. L., Blom, H. J., Steegers, E. A., den Heijer, M., & Eskes, T. K. (2000). Hyperhomocysteinemia and recurrent early pregnancy loss: a meta-analysis. Fertility and sterility, 74(6), 1196–1199. [CrossRef]
- Refsum, H., Ueland, P. M., Nygård, O., & Vollset, S. E. (1998). Homocysteine and cardiovascular disease. Annual review of medicine, 49, 31–62. [CrossRef]
- Pinzon RT, Wijaya VO, Veronica V. The role of homocysteine levels as a risk factor of ischemic stroke events: a systematic review and meta-analysis. Front Neurol. 2023 May 12;14:1144584.
- Murphy, M. E., & Westmark, C. J. (2020). Folic Acid Fortification and Neural Tube Defect Risk: Analysis of the Food Fortification Initiative Dataset. Nutrients, 12(1), 247. [CrossRef]
- Pfeiffer, C. M., Johnson, C. L., Jain, R. B., Yetley, E. A., Picciano, M. F., Rader, J. I., Fisher, K. D., Mulinare, J., & Osterloh, J. D. (2007). Trends in blood folate and vitamin B-12 concentrations in the United States, 1988 2004. The American journal of clinical nutrition, 86(3), 718–727. [CrossRef]
- Choi, J. H., Yates, Z., Veysey, M., Heo, Y. R., & Lucock, M. (2014). Contemporary issues surrounding folic Acid fortification initiatives. Preventive nutrition and food science, 19(4), 247–260. [CrossRef]
- Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. (1991). Lancet (London, England), 338(8760), 131–137.
- Ray, J. G., Vermeulen, M. J., Langman, L. J., Boss, S. C., & Cole, D. E. (2003). Persistence of vitamin B12 insufficiency among elderly women after folic acid food fortification. Clinical biochemistry, 36(5), 387–391. [CrossRef]
- Morris, M. S., Jacques, P. F., Rosenberg, I. H., & Selhub, J. (2010). Circulating unmetabolized folic acid and 5-methyltetrahydrofolate in relation to anemia, macrocytosis, and cognitive test performance in American seniors. The American Journal of Clinical Nutrition, 91(6), 1733–1744. [CrossRef]
- Selhub, J., & Paul, L. (2011). Folic acid fortification: why not vitamin B12 also?. BioFactors (Oxford, England), 37(4), 269–271. [CrossRef]
- Morris, M. S., Jacques, P. F., Rosenberg, I. H., & Selhub, J. (2007). Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. The American Journal of Clinical Nutrition, 85(1), 193–200. [CrossRef]
- Kalmbach, R. D., Choumenkovitch, S. F., Troen, A. M., D'Agostino, R., Jacques, P. F., & Selhub, J. (2008). Circulating folic acid in plasma: relation to folic acid fortification. The American journal of clinical nutrition, 88(3), 763–768. [CrossRef]
- Sweeney, M. R., McPartlin, J., & Scott, J. (2007). Folic acid fortification and public health: report on threshold doses above which unmetabolised folic acid appear in serum. BMC public health, 7, 41. [CrossRef]
- Obeid, R., Kasoha, M., Kirsch, S. H., Munz, W., & Herrmann, W. (2010). Concentrations of unmetabolized folic acid and primary folate forms in pregnant women at delivery and in umbilical cord blood. The American journal of clinical nutrition, 92(6), 1416–1422. [CrossRef]
- Tam, C., O'Connor, D., & Koren, G. (2012). Circulating unmetabolized folic Acid: relationship to folate status and effect of supplementation. Obstetrics and gynecology international, 2012, 485179. [CrossRef]
- Sweeney, M. R., McPartlin, J., Weir, D. G., Daly, S., Pentieva, K., Daly, L., & Scott, J. M. (2005). Evidence of unmetabolised folic acid in cord blood of newborn and serum of 4-day-old infants. The British journal of nutrition, 94(5), 727–730. [CrossRef]
- Mahajan, N. N., Mahajan, K. N., Soni, R. N., & Gaikwad, N. L. (2007). Justifying the "Folate trap" in folic acid fortification programs. Journal of perinatal medicine, 35(3), 241–242. [CrossRef]
- Cruz-Rodríguez, J., Díaz-López, A., Canals-Sans, J., & Arija, V. (2023). Maternal Vitamin B12 Status during Pregnancy and Early Infant Neurodevelopment: The ECLIPSES Study. Nutrients, 15(6), 1529. [CrossRef]
- Shields, R. C., Caric, V., Hair, M., Jones, O., Wark, L., McColl, M. D., & Ramsay, J. E. (2011). Pregnancy-specific reference ranges for haematological variables in a Scottish population. Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology, 31(4), 286–289. [CrossRef]
- Heppe, D. H., Medina-Gomez, C., Hofman, A., Franco, O. H., Rivadeneira, F., & Jaddoe, V. W. (2013). Maternal first-trimester diet and childhood bone mass: the Generation R Study. The American journal of clinical nutrition, 98(1), 224–232. [CrossRef]
- Saravanan, P., Sukumar, N., Adaikalakoteswari, A., Goljan, I., Venkataraman, H., Gopinath, A., Bagias, C., Yajnik, C. S., Stallard, N., Ghebremichael-Weldeselassie, Y., & Fall, C. H. D. (2021). Association of maternal vitamin B12 and folate levels in early pregnancy with gestational diabetes: a prospective UK cohort study (PRiDE study). Diabetologia, 64(10), 2170–2182. [CrossRef]
- Reznikoff-Etiévant, M. F., Zittoun, J., Vaylet, C., Pernet, P., & Milliez, J. (2002). Low Vitamin B(12) level as a risk factor for very early recurrent abortion. European journal of obstetrics, gynecology, and reproductive biology, 104(2), 156–159. [CrossRef]
- Hübner, U., Alwan, A., Jouma, M., Tabbaa, M., Schorr, H., & Herrmann, W. (2008). Low serum vitamin B12 is associated with recurrent pregnancy loss in Syrian women. Clinical chemistry and laboratory medicine, 46(9), 1265–1269. [CrossRef]
- Bondevik, G. T., Schneede, J., Refsum, H., Lie, R. T., Ulstein, M., & Kvåle, G. (2001). Homocysteine and methylmalonic acid levels in pregnant Nepali women. Should cobalamin supplementation be considered?. European journal.
- Hay, G., Clausen, T., Whitelaw, A., Trygg, K., Johnston, C., Henriksen, T., & Refsum, H. (2010). Maternal folate and cobalamin status predicts vitamin status in newborns and 6-month-old infants. The Journal of nutrition, 140(3), 557–564. [CrossRef]
- Ronnenberg, A. G., Goldman, M. B., Chen, D., Aitken, I. W., Willett, W. C., Selhub, J., & Xu, X. (2002). Preconception homocysteine and B vitamin status and birth outcomes in Chinese women. The American journal of clinical nutrition, 76(6), 1385–1391. [CrossRef]
- Kramer, M. S., Kahn, S. R., Rozen, R., Evans, R., Platt, R. W., Chen, M. F., Goulet, L., Séguin, L., Dassa, C., Lydon, J., McNamara, H., Dahhou, M., & Genest, J. (2009). Vasculopathic and thrombophilic risk factors for spontaneous preterm birth. International journal of epidemiology, 38(3), 715–723. [CrossRef]
- Wheeler S. Assessment and interpretation of micronutrient status during pregnancy: Symposium on ‘Translation of research in nutrition II: the bed.’ Proceedings of the Nutrition Society. 2008;67(4):437-450. [CrossRef]
- Qiu, X., Gao, F., Qiu, Y., Bao, J., Gu, X., Long, Y., Liu, F., Cai, M., & Liu, H. (2018). Association of maternal serum homocysteine concentration levels in late stage of pregnancy with preterm births: a nested case-control study. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 31(20), 2673–2677. [CrossRef]
- Muthayya, S., Kurpad, A. V., Duggan, C. P., Bosch, R. J., Dwarkanath, P., Mhaskar, A., Mhaskar, R., Thomas, A., Vaz, M., Bhat, S., & Fawzi, W. W. (2006). Low maternal vitamin B12 status is associated with intrauterine growth retardation in urban South Indians. European journal of clinical nutrition, 60(6), 791–801. [CrossRef]
- Relton, C. L., Pearce, M. S., & Parker, L. (2005). The influence of erythrocyte folate and serum vitamin B12 status on birth weight. The British journal of nutrition, 93(5), 593–599. [CrossRef]
- Dwarkanath, P., Barzilay, J. R., Thomas, T., Thomas, A., Bhat, S., & Kurpad, A. V. (2013). High folate and low vitamin B-12 intakes during pregnancy are associated with small-for-gestational age infants in South Indian women: a prospective observational cohort study. The American journal of clinical nutrition, 98(6), 1450–1458. [CrossRef]
- Jiang, H. L., Cao, L. Q., & Chen, H. Y. (2016). Blood folic acid, vitamin B12, and homocysteine levels in pregnant women with fetal growth restriction. Genetics and molecular research : GMR, 15(4), 10.4238/gmr15048890. [CrossRef]
- Zhang, T., Xin, R., Gu, X., Wang, F., Pei, L., Lin, L., Chen, G., Wu, J., & Zheng, X. (2009). Maternal serum vitamin B12, folate and homocysteine and the risk of neural tube defects in the offspring in a high-risk area of China. Public health nutrition, 12(5), 680–686. [CrossRef]
- Czeizel, A. E., & Dudás, I. (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. The New England journal of medicine, 327(26), 1832–1835. [CrossRef]
- Obeid, R., Eussen, S. J. P. M., Mommers, M., Smits, L., & Thijs, C. (2022). Imbalanced Folate and Vitamin B12 in the Third Trimester of Pregnancy and its Association with Birthweight and Child Growth up to 2 Years. Molecular nutrition & food research, 66(2), e2100662. [CrossRef]
- Rogne, T., Tielemans, M. J., Chong, M. F., Yajnik, C. S., Krishnaveni, G. V., Poston, L., Jaddoe, V. W., Steegers, E. A., Joshi, S., Chong, Y. S., Godfrey, K. M., Yap, F., Yahyaoui, R., Thomas, T., Hay, G., Hogeveen, M., Demir, A., Saravanan, P., Skovlund, E., Martinussen, M. P., … Risnes, K. R. (2017). Associations of Maternal Vitamin B12 Concentration in Pregnancy With the Risks of Preterm Birth and Low Birth Weight: A Systematic Review and Meta-Analysis of Individual Participant Data. American journal of epidemiology, 185(3), 212–223. [CrossRef]
- Clément, A., Clément, P., Viot, G., & Menezo, Y. J. (2023). Correction to: The importance of preconception Hcy Testing: Identification of a folate trap syndrome in a woman attending an assisted reproduction program. Journal of Assisted Reproduction and Genetics, 41(1), 233–233. [CrossRef]
- Bergen, N. E., Jaddoe, V. W., Timmermans, S., Hofman, A., Lindemans, J., Russcher, H., Raat, H., Steegers-Theunissen, R. P., & Steegers, E. A. (2012). Homocysteine and folate concentrations in early pregnancy and the risk of adverse pregnancy outcomes: the Generation R Study. BJOG : an international journal of obstetrics and gynaecology, 119(6), 739–751. [CrossRef]
- Krishnaveni, G. V., Hill, J. C., Veena, S. R., Bhat, D. S., Wills, A. K., Karat, C. L., Yajnik, C. S., & Fall, C. H. (2009). Low plasma vitamin B12 in pregnancy is associated with gestational 'diabesity' and later diabetes. Diabetologia, 52(11), 2350–2358. [CrossRef]
- Li, S., Hou, Y., Yan, X., Wang, Y., Shi, C., Wu, X., Liu, H., Zhang, L., Zhang, X., Liu, J., Zhang, M., Zhang, Q., & Tang, N. (2019). Joint effects of folate and vitamin B12 imbalance with maternal characteristics on gestational diabetes mellitus. Journal of diabetes, 11(9), 744–751. [CrossRef]
- Ludvigsson, J. F., Leffler, D. A., Bai, J. C., Biagi, F., Fasano, A., Green, P. H., Hadjivassiliou, M., Kaukinen, K., Kelly, C. P., Leonard, J. N., Lundin, K. E., Murray, J. A., Sanders, D. S., Walker, M. M., Zingone, F., & Ciacci, C. (2013). The Oslo definitions for coeliac disease and related terms. Gut, 62(1), 43–52. [CrossRef]
- Rubio-Tapia, A., Hill, I. D., Kelly, C. P., Calderwood, A. H., Murray, J. A., & American College of Gastroenterology (2013). ACG clinical guidelines: diagnosis and management of celiac disease. The American journal of gastroenterology, 108(5), 656–677. [CrossRef]
- Lebwohl, B., Sanders, D. S., & Green, P. H. R. (2018). Coeliac disease. Lancet (London, England), 391(10115), 70–81. [CrossRef]
- Choung, R. S., Unalp-Arida, A., Ruhl, C. E., Brantner, T. L., Everhart, J. E., & Murray, J. A. (2016). Less Hidden Celiac Disease But Increased Gluten Avoidance Without a Diagnosis in the United States: Findings From the National Health and Nutrition Examination Surveys From 2009 to 2014. Mayo Clinic proceedings, S0025-6196(16)30634-6. Advance online publication. [CrossRef]
- Shah, S., & Leffler, D. (2010). Celiac disease: An underappreciated issue in women’s health. Women’s Health, 6(5), 753–766. [CrossRef]
- Fish, E. M., Shumway, K. R., & Burns, B. (2024). Physiology, Small Bowel. In StatPearls. StatPearls Publishing.
- Wierdsma, N. J., van Bokhorst-de van der Schueren, M. A., Berkenpas, M., Mulder, C. J., & van Bodegraven, A. A. (2013). Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients. Nutrients, 5(10), 3975–3992. [CrossRef]
- Dahele, A., & Ghosh, S. (2001). Vitamin B12 deficiency in untreated celiac disease. The American journal of gastroenterology, 96(3), 745–750. [CrossRef]
- Bledsoe, A. C., King, K. S., Larson, J. J., Snyder, M., Absah, I., Choung, R. S., & Murray, J. A. (2019). Micronutrient deficiencies are common in contemporary celiac disease despite lack of overt malabsorption symptoms. Mayo Clinic Proceedings, 94(7), 1253–1260. [CrossRef]
- Kemppainen, T. A., Kosma, V. M., Janatuinen, E. K., Julkunen, R. J., Pikkarainen, P. H., & Uusitupa, M. I. (1998). Nutritional status of newly diagnosed celiac disease patients before and after the institution of a celiac disease diet--association with the grade of mucosal villous atrophy. The American journal of clinical nutrition, 67(3), 482–487. [CrossRef]
- Caruso, R., Pallone, F., Stasi, E., Romeo, S., & Monteleone, G. (2013). Appropriate nutrient supplementation in celiac disease. Annals of Medicine, 45(8), 522–531. [CrossRef]
- Cardo, A., Churruca, I., Lasa, A., Navarro, V., Vázquez-Polo, M., Perez-Junkera, G., & Larretxi, I. (2021). Nutritional Imbalances in Adult Celiac Patients Following a Gluten-Free Diet. Nutrients, 13(8), 2877. [CrossRef]
- Hallert, C., Grant, C., Grehn, S., Grännö, C., Hultén, S., Midhagen, G., Ström, M., Svensson, H., & Valdimarsson, T. (2002). Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Alimentary pharmacology & therapeutics, 16(7), 1333–1339. [CrossRef]
- Hallert, C., Svensson, M., Tholstrup, J., & Hultberg, B. (2009). Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Alimentary pharmacology & therapeutics, 29(8), 811–816. [CrossRef]
- Muhammad, H., Reeves, S., & Jeanes, Y. M. (2019). Identifying and improving adherence to the gluten-free diet in people with coeliac disease. The Proceedings of the Nutrition Society, 78(3), 418–425. [CrossRef]
- Mehtab, W., Agarwal, A., Chauhan, A. et al. Barriers at various levels of human ecosystem for maintaining adherence to gluten free diet in adult patients with celiac disease. Eur J Clin Nutr 78, 320–327 (2024). [CrossRef]
- Abu-Janb, N., & Jaana, M. (2020). Facilitators and barriers to adherence to gluten-free diet among adults with celiac disease: a systematic review. Journal of human nutrition and dietetics : the official journal of the British Dietetic Association, 33(6), 786–810. [CrossRef]
- Lee, A. R., Wolf, R. L., Lebwohl, B., Ciaccio, E. J., & Green, P. H. R. (2019). Persistent Economic Burden of the Gluten Free Diet. Nutrients, 11(2), 399. [CrossRef]
- Martinelli, D., Fortunato, F., Tafuri, S., Germinario, C. A., & Prato, R. (2010). Reproductive life disorders in Italian celiac women. A case-control study. BMC gastroenterology, 10, 89. [CrossRef]
- Arvanitakis, K., Siargkas, A., Germanidis, G., Dagklis, T., & Tsakiridis, I. (2023). Adverse pregnancy outcomes in women with celiac disease: a systematic review and meta-analysis. Annals of gastroenterology, 36(1), 12–24. [CrossRef]
- Sher, K. S., & Mayberry, J. F. (1996). Female fertility, obstetric and gynaecological history in coeliac disease: a case control study. Acta paediatrica (Oslo, Norway : 1992). Supplement, 412, 76–77. [CrossRef]
- Ludvigsson, J. F., Montgomery, S. M., & Ekbom, A. (2005). Celiac disease and risk of adverse fetal outcome: a population-based cohort study. Gastroenterology, 129(2), 454–463. [CrossRef]
- Castaño, M., Gómez-Gordo, R., Cuevas, D., & Núñez, C. (2019). Systematic Review and meta-analysis of prevalence of coeliac disease in women with infertility. Nutrients, 11(8), 1950. [CrossRef]
- Martinelli, P., Troncone, R., Paparo, F., Torre, P., Trapanese, E., Fasano, C., Lamberti, A., Budillon, G., Nardone, G., & Greco, L. (2000). Coeliac disease and unfavourable outcome of pregnancy. Gut, 46(3), 332–335. [CrossRef]
- Nørgård, B., Fonager, K., Sørensen, H. T., & Olsen, J. (1999). Birth outcomes of women with celiac disease: a nationwide historical cohort study. The American journal of gastroenterology, 94(9), 2435–2440. [CrossRef]
- Oxentenko, A. S., & Rubio-Tapia, A. (2019). Celiac disease. Mayo Clinic Proceedings, 94(12), 2556–2571. [CrossRef]
- Fortunato, F., Martinelli, D., Prato, R., & Pedalino, B. (2014). Results fromad hocand routinely collected data among celiac women with infertility or pregnancy related disorders: Italy, 2001–2011. The Scientific World Journal, 2014, 1–7. [CrossRef]
- Nellikkal, S. S., Hafed, Y., Larson, J. J., Murray, J. A., & Absah, I. (2019). High Prevalence of Celiac Disease Among Screened First-Degree Relatives. Mayo Clinic proceedings, 94(9), 1807–1813. [CrossRef]
- Boers, K., Vlasveld, T., & van der Waart, R. (2019). Pregnancy and coeliac disease. BMJ case reports, 12(12), e233226. [CrossRef]
Figure 1.
Rationale for Subpopulation of Interest.
Figure 2.
Folate and Methionine Metabolism. The conversion of 5-methyltetrahydrofolate (5-MTHF) to tetrahydrofolate (THF) is halted when there is a vitamin B12 deficiency. This inhibits the methionine cycle and leaves elevated homocysteine (Hcy) levels in the blood.
Figure 2.
Folate and Methionine Metabolism. The conversion of 5-methyltetrahydrofolate (5-MTHF) to tetrahydrofolate (THF) is halted when there is a vitamin B12 deficiency. This inhibits the methionine cycle and leaves elevated homocysteine (Hcy) levels in the blood.
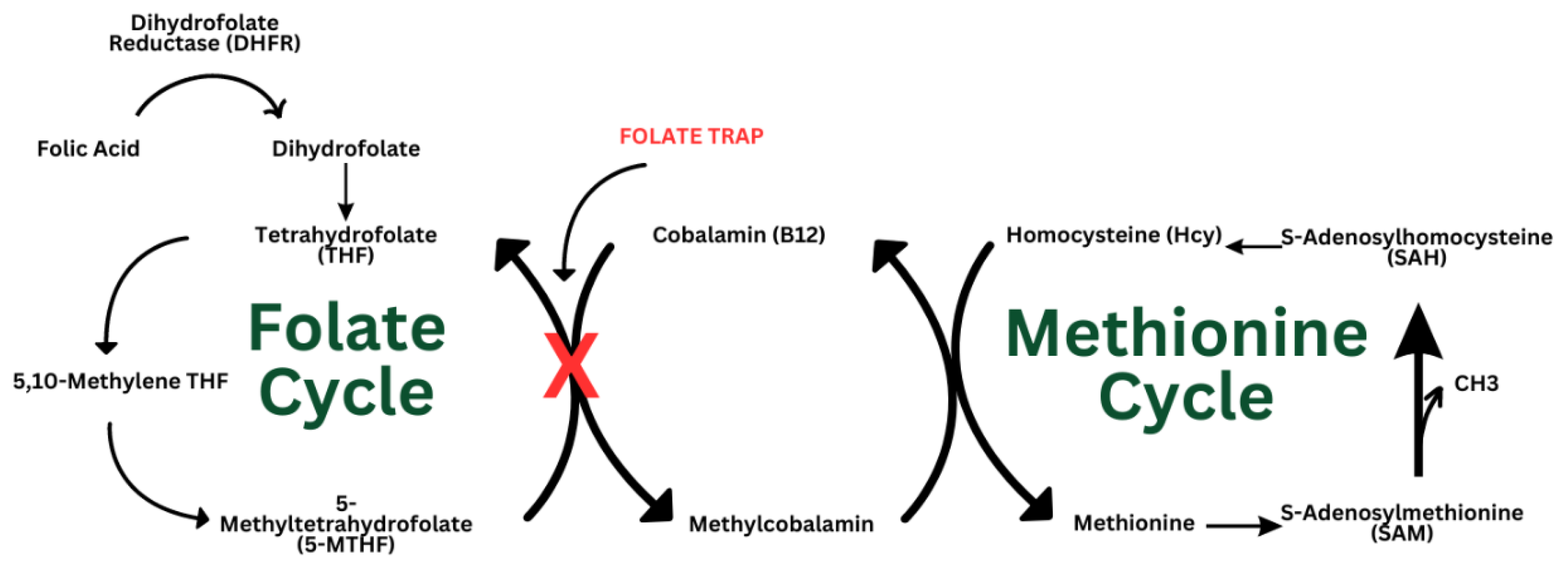

Table 1.
Manifestations of Vitamin B12 Deficiency.
| Symptoms | Signs | Lab Findings |
|---|---|---|
| Fatigue | Beefy red tongue | Megaloblastic anemia |
| Cognitive decline | Ataxia | Anisocytosis |
| Upper or lower extremity paresthesia | Diminished proprioception | Poikilocytosis |
| Loss of balance | Diminished vibratory sense | Hyper segmented neutrophils |
| Falls | Romberg’s sign | Hyperhomocysteinemia |
Table 2.
Manifestations of Folate Deficiency.
| Symptoms | Signs | Lab Findings |
|---|---|---|
| Fatigue | Pale skin | Megaloblastic anemia |
| Cognitive decline | Mouth sores | Anisocytosis |
| Irritability | Diminished proprioception | Poikilocytosis |
| Decreased Appetite | Diminished vibratory sense | Hyper segmented neutrophils |
| Diarrhea | Smooth and tender tongue | Hyperhomocysteinemia |
Table 3.
Vitamin B12 and Folate Intake Recommended Dietary Allowance (RDA).
| Vitamin B12 | Folate | |
|---|---|---|
| Adults | 2.4 μg/day | 400 μg/day |
| Pregnant Women | 2.6 μg/day | 600 μg/day |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



