Submitted:
12 August 2024
Posted:
13 August 2024
You are already at the latest version
Abstract
Background/Objectives: Bacterial infections (BI) are a major cause of mortality in patients with alcohol-associated hepatitis (AH); however, only a few studies have investigated BI in AH in the last decade. Therefore, we aimed to assess the features and outcomes of BI in patients with AH. Methods: This observational descriptive study included patients with AH admitted to a tertiary academic hospital between 2016–2021. Clinical and complete microbiological data were recorded and complications, including acute-on-chronic liver failure (ACLF), and mortality over 90-days were compared between infected and non-infected patients. Results: Overall, 115 patients with AH were recruited and 75 had severe AH; among them, 66 started corticosteroid treatment. We identified 69 cases of BI in 44 patients; the incidence of BI at hospital discharge was 32.2%, which reached 38.2% at 90 days. The predominant infection site was the chest (35%). Among the identified bacteria (52.1%), half were gram-positive and half gram-negative. A low rate of multidrug-resistant bacteria (14%) was also noted. Infected patients during hospitalization (n=37) exhibited higher rates of hepatic decompensation and ACLF p=0.001) and lower survival (81.8% vs. 95.8%, p=0.015) than did non-infected patients (n=78). In-hospital infected patients (n=22) exhibited worse survival (72.7%) than did those infected upon admission (93.3%) or non-infected patients (94.9%) (p=0.009). Corticosteroid-treated patients displayed a nonsignificant increase in the total number of BI; however, without greater mortality. Conclusions: BI were common in our cohort of patients with AH. Patients with in-hospital infections commonly experienced serious complications, including high ACLF and death rates. Infections diagnosed upon admission were treated without affecting survival.
Keywords:
bacterial infections
; alcoholic hepatitis
; alcohol-associated hepatitis
; risk factors
; acute-on-chronic liver failure
; corticosteroids
1. Introduction
Alcohol-related liver disease (ArLD) is the main cause of chronic liver disease worldwide, contributing to 41.7% of cirrhosis-related deaths [1,2]. It comprises a clinical–histological spectrum, including fatty liver, alcohol-associated hepatitis (AH), and cirrhosis with associated complications. AH is characterized by abrupt jaundice, malaise, and liver-related decompensation [3]. Patients with AH are relatively susceptible to infection [4,5]; some studies have reported up to 49% of infections [4,6]. Both Infections and AH potentially lead to acute-on-chronic liver failure (ACLF) with an incidence rate as high as 20–50% at 3 months [7,8].
Studies with the largest cohorts of patients with AH and concomitant infection were conducted more than 10 years ago, and all studies did not identify the causative agent [6,9,10,11,12,13]. Moreover, the concept of ACLF was defined in the last decade. Thus, although both AH and infections are the main causes of ACLF, few studies [14,15] have specifically investigated the role of infections in ACLF development in AH.
Therefore, this observational, single center study endeavored to evaluate the emergence and course of infection in patients with AH. Ultimately, it aimed to describe the characteristics, causative microorganisms, severity, complications and risk factors of bacterial infections (BI) in patients with AH.
2. Materials and Methods
2.1. Study Design and Population
This observational descriptive study included patients with AH consecutively admitted to Hospital Vall d’ Hebron liver unit between January 2016 and December 2021 who were followed-up for 90 days or until death. Inclusion criteria were age > 18 years, patients with bilirubin level ≥ 3 mg/dL, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) values < 400 IU/L, AST/ALT ratio > 1.5 and active alcohol consumption of > 40 g/day in women or > 60 g/day in men for ≥ 6 months with less than 60 days of abstinence prior to inclusion according to National Institute on Alcohol Abuse and Alcoholism (NIAAA) AH consortia or a confirmatory biopsy. Exclusion criteria followed the NIAAA recommendations for the diagnosis of a probable AH with more than one etiology of liver disease, sepsis defined by the presence of systemic inflammatory response syndrome (SIRS) and infection at baseline (defined as infections diagnosed within the first 48 h of admission), patients with any type of shock at baseline, defined by the use of vasoactive substances at admission (excluding those specifically used for bleeding control), cocaine use or recent use of a drug with drug-induced liver injury potential within 30 days, and patients with comorbidities encompassing high short-term mortality including either hepatocellular carcinoma out of Milan criteria or extrahepatic neoplasia.
For each patient, the following data were collected upon admission: epidemiological and demographic data such as age; sex; body mass index; history of alcohol intake, history of liver disease including previous decompensations and other underlying diseases, such as arterial hypertension, diabetes mellitus, dyslipidemia, metabolic syndrome, obesity, chronic renal disease, ischemic heart disease, and chronic obstructive pulmonary disease. On admission, infections; hepatic decompensations (HD); acute kidney injury (AKI); ACLF and severity scores were registered (i.e Maddrey, Model for End-Stage Liver Disease (MELD), MELD Na, MELD 3.0, and Child–Pugh). Physical examination, routine laboratory and microbiological examinations, and concurrent medications (prophylactic antibiotic) usage data were also collected. During hospitalization, the following data were recorded: development of infections, HD, AKI, transjugular intrahepatic portosystemic shunt insertion, vasoactive support required, intensive care unit (ICU) support, ACLF development, and mortality. After hospital discharge, only new infections and mortality were recorded. Patients were followed up for 90 days or up to death.
The following information was recorded for infections at any time point: type and location, nosocomial or community acquired infection, type of bacteria or fungus, antibiotic resistance and treatment, antibiotic escalating and deescalating.
2.2. Definitions
Hepatic decompensation was defined as the acute development of ascites, upper gastrointestinal bleeding (GIB), hepatic encephalopathy (HE), or any combination of the foregoing, requiring prolonged or new hospitalization [17]. ACLF was defined as a clinical syndrome occurring in patients with cirrhosis characterized by acute deterioration, organ failure, and high short-term mortality, according to the European Foundation for the Study of Chronic Liver Failure criteria [18]. Proven infection (criteria defined by the NACSELD consortium) [4] was established in the following cases: 1) spontaneous bacteremia: positive blood cultures without a source of infection; 2) spontaneous bacterial peritonitis (SBP): ascitic fluid polymorphonuclear cells > 250/µL with or without a positive fluid culture; 3) lower respiratory tract infections: new pulmonary infiltrate on chest radiograph in the presence of compatible clinical criteria, at least one respiratory symptom (cough, sputum production, dyspnea, and/or pleuritic pain), and/or at least one finding on auscultation (rales or crepitation) or sign of infection (e.g., fever and leukocytosis); 4) bacterial enterocolitis: diarrhea or dysentery with a positive stool culture for pathogenic bacteria (e.g., Salmonella, Shigella, Yersinia, Campylobacter, and Escherichia coli); 5) Clostridium difficile: diarrhea with a positive toxigenic C. difficile test result; 6) skin infection: cellulitis; 7) urinary tract infection: urinary white blood cell count > 20 per field with positive urinary culture findings in a symptomatic patient; 8) intra-abdominal infections (e.g., diverticulitis, appendicitis, cholangitis, and secondary bacterial peritonitis); and 9) healthcare–associated infections (e.g., catheter-related bloodstream infection [CRBSI]). Multidrug-resistant bacteria (MRB) were defined as nonsusceptibility to at least one agent in at least three antimicrobial categories. Nosocomial infection (in-hospital infection) was defined as the novo infection after 72 hours of hospitalization.
2.3. Statistical Analysis
Descriptive statistics were used to summarize data. Quantitative variables are expressed as the mean ± standard deviation and normally and non-normally distributed data are expressed as median (interquartile range). Percentages were calculated using categorical data. Qualitative variables are presented as frequencies and percentages. Between-group differences for categorical and quantitative variables were evaluated using the chi-square or Fisher’s exact test and the Student’s t-test or the Mann–Whitney U test as appropriate. Survival times were compared using the Kaplan–Meier curves and log-rank tests. All statistical analyses were performed using IBM SPSS Statistics (version 22) software.
3. Results
3.1. Study Population
In total, 115 patients with AH were admitted to our hospital and met our eligibility criteria. Their characteristics are shown in Table 1. In summary, 76.5% were men, the median age was 50 years old, and 85% were Caucasians.
On admission, 70% patients were diagnosed with hepatic cirrhosis and 56% exhibited a liver-related decompensation, with ascites being the most common one accounting for up to half of the patients, and 7 (6%) patients fulfilled ACLF criteria. The median (interquartile range) Maddrey, MELD, and Child–Pugh scores were 40 (20–50), 19 (16–22), and 10 (9–11), respectively.
Overall, 75 (65%) patients met the criteria for severe AH (Maddrey score > 32 points); among them, 66 started corticosteroids CS treatment, whereas 9 did not receive CS because of ongoing severe infection and GIB (6 and 3 patients, respectively).
3.2. Infections
In the AH cohort, we identified 69 infections in 44 patients (38.2% of all patients with AH) during the 90-day study period. On admission, 20 infections were present in 18 patients (15.6% of all patients with AH).
During hospitalization, 30 infections occurred in 22 patients (19.1% of all patients with AH), among whom 3 had infections upon admission.
From hospital discharge to the end of follow-up, 19 infections developed in 14 patients (13.2% of 106 living patients), among whom 7 had a previous infection (6 patients had a preexisting infection upon admission, and 1 developed an infection during hospitalization).
3.3. Bacteria and Sites of Infection
Among the 69 detected infections, 40 bacteria were identified and isolated from cultures of 36 infections (52.1%). The cultured organisms are listed in Table 2. Overall, gram-positive and gram-negative bacteria were equally represented. Gram-negative bacteria accounted for 50% of the isolated organisms, and E. coli and Klebsiella pneumoniae were the predominantly isolated organisms (17% and 15% of all isolated organisms, respectively). Gram-positive bacteria also accounted for 50% of the isolated organisms, and Staphylococcus aureus was the most isolated organism (20% of all isolated organisms). MRB were rare in this series of patients; only five MRBs (S. aureus, S. haemolyticus, K. pneumoniae (×2), and Enterococcus faecalis) were identified among the 36 identified infections (14%).
The infection sites are summarized in Table 2. The chest was the most common infection site, with 24 cases (35%) of pneumonia, followed by the skin (14 (20%)), blood (11 (16%): bacteremia (8) and CRBSI (3)), abdomen (ascites (SBP)) (11 (16%)), and urinary tract (9 (13%)).
3.4. Infections upon Admission
On admission, 20 infections were detected in 18 patients, whereas no infection was detected in 97 patients. Two patients had two different infections; one had coexistent SBP, caused by S. haemolyticus, and bacteriemia, caused by Acinetobacter baumannii, whereas the second had cellulitis and aspiration pneumonia. The most frequently associated infections were chest infections (7 (35%)) and cellulitis (7 (35%)), whereas urinary tract infections (3 (15%)), SBP (2), and bacteremia (1) were the least frequent. In 11 infections (55%), especially pneumonia and cellulitis, the microorganisms were not identified (clinical diagnosis). Additionally, upon diagnosis, nine (45%) patients had associated SIRS, whereas three (16.6%) met the ACLF criteria. Infection characteristics upon admission and during the course of the disease are shown in Table 3-a.
3.5. Infections during Follow-Up
During hospitalization and at follow-up (90 days after diagnosis), 49 infections were detected in 36 patients. Ten patients developed more than one infection upon admission or during follow-up; eight who had a preexisting infection upon admission were later reinfected (three were infected during hospitalization and five after hospital discharge), and the other two patients developed an infection during hospitalization and were later reinfected after hospital discharge.
Chest infections (17 (35%)), blood infections (10 (20%)), and SBP (9 (18%)) were predominantly associated with infections during follow-up. Microorganisms were identified in a significant proportion of patients (30 out of 49 (61.2%)); half of the isolated organisms were gram-positive bacteria (14 isolations of Staphylococcus spp. and three of Enterococcus spp.), whereas the other half were gram-negative bacteria (mostly Enterobacteriaceae: five isolations of E. coli and five of K. pneumoniae) (Table 2).
3.6. Liver Related Decompensations and ACLF in Infected Patients Compared with Non-Infected Patients
On admission, infected patients (n=18) yielded higher prognostic scores than did non-infected patients (n=97). The presence of HD, such as ascites (78% vs. 46%, p=0.029) and HE (50% vs. 6%, p=0.001), was more frequent in infected patients than in non-infected patients. Infected patients exhibited higher prognostic scores than did non-infected patients: Maddrey (48 vs. 38, p=0.02), MELD (22 vs. 19, p=0.01), MELD Na (24.5 vs. 22, p=0.03), MELD 3.0 (25.5 vs. 23, p=0.01), Child–Pugh (11 vs. 10, p=0.001), and ABIC (11 vs. 10; p=0001). Furthermore, infected patients displayed a higher ACLF incidence (16.6% vs. 4.1%, p=0.041) than did non-infected patients. The complete clinical characteristics are shown in Table 4. Notably, infections diagnosed upon admission were cured with antibiotics, thus having no impact on survival.
Comparison of the clinical course of the infected (admission + hospitalization) and non-infected patients (n=37 vs. n=78) revealed significant differences. Infected patients (n=37) developed more cases of HD (62% vs. 28%, p=0.001), especially ascites (43% vs. 23%, p=0.046) and HE (41% vs. 13%, p=0.001), than did non-infected patients. They also presented with ACLF more frequently (32% vs. 6%, p=0.001), requiring vasoactive (16% vs. 1.3%, p=0.002) and ICU (27% vs. 2.5%, p=0.001) support. Finally, patients with infections had a higher mortality rate (6/37, 16% vs. 3/78, 4%; p=0.021) than did non-infected patients. Table 5 compares the clinical characteristics of the infected and non-infected patients. Of the 22 in-hospital infected patients, 10 had infection-associated SIRS, nine developed ACLF, and five died of ACLF (Table 3-b). These 22 patients had higher incidence rates of HD (59% vs. 34.4%, p=0.033) and ACLF (36.3% vs. 9.6%, p=0.002) than did the non-infected patients during hospitalization.

Table 5.
BASELINE AND COMPLICATIONS, PATIENTS IN HOSPITALIZATION.
| INFECTED PATIENTS N=37 |
NO INFECTED PATIENTS N=78 |
p | |
|---|---|---|---|
| Sex (male), n(%) | 25 (67.5%) | 63 (81%) | 0.12 |
| Age, median (IQR) P 25-75 | 50 (43- 57) | 51 (44–58) | 0.87 |
| Race, n(%) | Caucasian, 30 (87%) | Caucasian, 68 (87%) | 0.91 |
| BASELINE | |||
| Maddrey score, median (IQR) P 25-75 | 45 (31.5–61.5) | 37 (18–51) | 0.020 |
| MELD score, median (IQR) P 25-75 | 21 (18-25) | 18 (15-21) | 0.002 |
| Child-Pugh score, median (IQR) P 25-75 | 11 (10–12) | 10 (9-11) | 0.001 |
| Bilirubin serum (mg/dL), median (IQR) P 25-75 | 10.4 (5.4-17.5) | 6.5 (4.4-10.5) | 0.010 |
| INR, median (IQR) P 25-75 | 1.63 (1.4-1.84) | 1.48 (1.14-1.80) | 0.047 |
| Albumin (g/dl), median (IQR) P25–P75 | 2.5 (2.3-2.75) | 2.8 (2.5-3.4) | 0.002 |
| Creatinine (mg/dL), median (IQR) P 25-75 | 0.7 (0.6-1.0) | 0.65 (0.53-0.86) | 0.45 |
| COMPLICATIONS | |||
| HD, n(%) | 23 (62%) | 22 (28%) | 0.001 |
| Ascites, n(%) | 16 (43%) | 18 (23%) | 0.046 |
| HE, n (%) | 15 (41%) | 10 (13%) | 0.001 |
| GIB, n (%) | 4 (11%) | 5(6.4%) | 0.41 |
| AKI, n(%) | 6 (16%) | 5 (6.4%) | 0.095 |
| Vasoactive support | 6 (16%) | 1 (1.3%) | 0.002 |
| ICU, n (%) | 10 (27%) | 2 (2.5%) | 0.001 |
| ACLF, n(%) | 12 (32.4%) | 5 (6.4%) | 0.001 |
| Death, n (%) | 6 (16%) | 3 (4%) | 0.021 |
| IQR: interquartile range, HD: hepatic decompensations, HE: hepatic encephalopathy, GIB: gastrointestinal bleeding, AKI: acute kidney injury, ICU: intensive care unit, ACLF: acute-on-chronic liver failure, During hospitalization, the assessment focused solely on infections and complications, as not all patients recorded complete analytical values, nor was sufficient clinical information available after discharge. | |||
Table 3.
b. Characteristics of infections in hospitalization.
| ID-Episode | CE | Infection | Bacteria | SIRS | ACLF | Resolution infection | Cause of death | Antibiotic | MRB |
|---|---|---|---|---|---|---|---|---|---|
| P2- 1 | Yes | CRBSI | Staphylococcus epidermidis | Yes | Yes | Yes | ACLF | Meropenem | |
| P4- 2 | Yes | UTI | Klebsiella aerogenes | Yes | Yes | Yes | Cefazolin | ||
| Cellulitis | Staphylococcus aureus | Cloxacillin | |||||||
| CRBSI | Enterococcus faecalis, Staphylococcus epidermidis, Staphylococcus haemolyticus | Piperacillin-Tazobactam | |||||||
| P5- 3 | Yes | UTI | Escherichia coli | No | No | Yes | Ceftriaxone | ||
| P6- 4 | Yes | Aspiration Pneumonia | Non-isolated bacteria | No | No | Yes | Meropenem | ||
| P20- 5 | No | UTI | Escherichia coli | No | No | Yes | Amoxicillin-Clavulanate | ||
| P21- 6 | Yes | Aspiration Pneumonia | Non-isolated bacteria | Yes | Yes | Yes | ACLF | Ceftazidime | |
| P28- 7 | Yes | Pneumonia | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P38- 8 | No | Cellulitis | Staphylococcus aureus | No | No | Yes | Linezolid | Yes | |
| P44- 9 | No | Pneumonia | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P50- 10 | Yes | Bacteremia | Klebsiella oxytoca | Yes | No | Yes | Amoxicillin-Clavulanate | ||
| P51- 11 | Yes | Pneumonia | Non-isolated bacteria | No | No | Yes | Piperacillin-Tazobactam | ||
| P25- 12 | No | SBP | Staphylococcus aureus | Yes | Yes | Yes | Ceftriaxone | ||
| Bacteremia | Staphylococcus aureus | Cefazolin | |||||||
| Aspiration Pneumonia | Non-isolated bacteria | Piperacillin-Tazobactam | |||||||
| P61- 13 | Yes | Pneumonia | Non-isolated bacteria | Yes | Yes | Yes | ACLF | Piperacillin-Tazobactam | |
| P63- 14 | No | SBP | Escherichia coli | No | No | Yes | Ceftriaxone | ||
| Pneumonia | Non-isolated bacteria | ||||||||
| P68- 15 | Yes | Bacteriemia | Escherichia coli | Yes | No | Yes | Piperacillin-Tazobactam | ||
| P73- 16 | No | Aspiration Pneumonia | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P78- 17 | Yes | SBP | Enterobacter cloacae | Yes | Yes | No | SBP, ACLF | Ceftriaxone | |
| Aspiration Pneumonia | Non-isolated bacteria | Amoxicillin-Clavulanate | |||||||
| SBP | Klebsiella pneumoniae | Meropenem + Daptomycin | Yes | ||||||
| P82- 18 | No | Pneumonia | Non-isolated bacteria | Yes | Yes | No | ACLF | Meropenem | |
| CRBSI | Staphylococcus hemolyticus, Staphylococcus epidermidis. *Candida albicans | Meropenem + Daptomycin, *Anidulafungin | Yes | ||||||
| P87- 19 | No | Aspiration Pneumonia | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P102- 20 | No | Pneumonia | Non-isolated bacteria | No | No | Yes | Ceftriaxone | ||
| P103- 21 | Yes | Pneumonia | Non-isolated bacteria | Yes | Yes | Yes | Piperacillin-Tazobactam | ||
| P106- 22 | No | Aspiration Pneumonia | Non-isolated bacteria | No | No | Yes | Piperacillin-Tazobactam |
CE: corticosteroids, SBP: spontaneous bacterial peritonitis, CRBSI: catheter-related bloodstream infection, UTI: urinary tract infection, ACLF: acute-on-chronic liver failure, MRB: multi-drug resistant bacteria.
We did not identify any significant differences in the incidence rates of infections or liver complications between CS-treated and non-CS-treated patients during hospitalization (Table 6). After discharge, CS-treated patients developed more infections (26% vs. 6%, p=0.09) and had a greater frequency of infection-associated SIRS, compared with non-CS-treated patients, but without significant differences. Complete data are provided in Table 6 and Table 3-c.
Table 6.
Clinical characteristics, corticosteroid treatment vs. non treated patients.
| Corticosteroids n= 49 | No Corticosteroids n= 66 |
p | |
|---|---|---|---|
| Baseline | |||
| Male, n (%) | 36 (73.5%) | 51 (77%) | 0.63 |
| Age median (IQR) P 25-75 | 51 (44-58) | 48 (43-56) | 0.16 |
| Maddrey score, median (IQR) P 25-75 | 34 (18-50) | 41 (28-58) | 0.27 |
| MELD score, median (IQR) P 25-75 | 19 (15-22) | 19 (16-22) | 0.88 |
| Child-Pugh score, median (IQR) P 25-75 | 10 (9-11) | 10 (9-11) | 0.44 |
| Complications during hospitalization | |||
| Infections, n (%) | 9 (18%) | 13 (20%) | 0.76 |
| HD, n(%) | 18 (36%) | 27 (40%) | 0.65 |
| Ascites, n(%) | 14 (28%) | 20 (30%) | 0.89 |
| HE, n (%) | 10 (20%) | 15 (22%) | 0.73 |
| GIB, n (%) | 2 (4%) | 7 (10%) | 0.19 |
| AKI, n(%) | 7 (14%) | 4 (6%) | 0.14 |
| Vasoactive support, n (%) | 3 (6%) | 4 (6%) | 0.98 |
| ICU, n (%) | 5 (10%) | 7 (11%) | 0.94 |
| ACLF, n(%) | 4 (8%) | 13 (20%) | 0.08 |
| Death, n (%) | 4 (8%) | 5 (7.5%) | 0.92 |
| Follow up 90 days | |||
| Infections, n (%) | 3 de 45 (6%) | 11 de 61 (18%) | 0.08 |
| Number of infections, n (%) | 3 de 45 (6%) | 16 de 61 (26%) | 0.09 |
| Death, n (%) | 1 (2%) | 1 (1.5%) | 0.82 |
IQR: interquartile range, MELD: Model for end-stage Liver Disease, HD: hepatic decompensations, HE: hepatic encephalopathy, GIB: gastrointestinal bleeding, AKI: acute kidney injury, ICU: intensive care unit, ACLF: acute-on-chronic liver failure.
Table 3.
b. Characteristics of infections after hospital discharge.
| ID-Episode | CE | Infection | Bacteria | SIRS | ACLF | Resolution infection | Cause of death | Antibiotic | MRB |
|---|---|---|---|---|---|---|---|---|---|
| P5- 1 | Yes | Bacteremia | Staphylococcus epidermidis | No | No | Yes | Ceftriaxone | ||
| P19- 2 | Yes | Cellulitis | Non-isolated bacteria | No | No | Yes | Ceftriaxone, Teicoplanin | ||
| P28- 3 | Yes | Pneumonia | Staphylococcus aureus | Yes | Yes | No | Septic Shock | Meropenem + Linezolid | |
| Intra-abdominal | Non-isolated bacteria | ||||||||
| P33- 4 | Yes | SBP | Enterococcus faecium | Yes | No | Yes | Piperacillin-Tazobactam | ||
| P39- 5 | Yes | Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P45- 6 | Yes | Bacteriemia | Klebsiella pneumoniae | Yes | Yes | Yes | Meropenem, Teicoplanin | ||
| Bacteremia | Enterococcus faecium | Yes | |||||||
| P47- 7 | Yes | SBP | Serratia marcescens | No | No | Yes | Ceftriaxone | ||
| P26- 8 | No | Bacteremia | Staphylococcus aureus | No | No | Yes | Amoxicillin-Clavulanate | ||
| P74- 9 | Yes | UTI | Escherichia coli | No | No | Yes | Ceftriaxone | ||
| P76- 10 | No | Cellulitis | Non-isolated bacteria | No | No | Yes | Cefadroxil | ||
| P83- 11 | No | Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||
| P92- 12 | Yes | SBP | Klebsiella pneumoniae | No | No | Yes | Ceftriaxone | ||
| UTI | Klebsiella pneumoniae | No | No | Yes | Ciprofloxacin | ||||
| UTI | Klebsiella pneumoniae | Yes | Yes | yes | Cefotaxime + Clindamycin | Yes | |||
| Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | ||||
| P105- 13 | Yes | Pneumonia | Non-isolated bacteria | No | No | Yes | Piperacillin-Tazobactam | ||
| P108- 14 | Yes | SBP | Acinetobacter pitti | Yes | Yes | Yes | ACLF | Meropenem |
CE: corticosteroids, SBP: spontaneous bacterial peritonitis, UTI: urinary tract infection, ACLF: acute-on-chronic liver failure, MRB: multi-drug resistant bacteria.
3.7. Mortality and Predictors of Mortality in Infected Patients
The 90-day survival was higher in non-infected patients (71) than in infected patients (44) (95.8 ± 2.4% vs. 81.8 ± 5.8%, p=0.015; Figure 1). In-hospital infected patients exhibited worse survival (72.7 ± 9.5%) than did those infected upon admission (93.3 ± 6.4%) or non-infected patients (94.9 ± 2.5%) (p=0.009; Figure 2).
4. Discussion
In this study, we prospectively reviewed patients who were diagnosed with AH at our academic tertiary hospital and were registered in a national database. Among them, 70% had cirrhosis, 65% had a Maddrey score > 32, and 57% received CS treatment.
In our cohort, we identified 69 infections in 44 patients, among whom the incidence of infection at hospital discharge was 32.2%, reaching 38.2% at 90 days post-discharge. On admission, 15.6% of patients had infections; however, 19.1% developed in-hospital infections. This incidence was slightly lower than that reported in previous studies. Parker [6] reported a global incidence of 49% for in-hospital infections, whereas Louvet et al. [9] and Michelena et al. [10] reported incidence rates of 25.6% and 23.1%, respectively, among patients infected upon admission, compared with 23% and 43.8%, respectively, among those infected during hospitalization. The incidence of in-hospital infections reported in this study (19.1%) was considerably similar to that observed in a meta-analysis by Hmoud et al. [13], who reported that 20% of CS-treated patients with AH developed in-hospital infections. In contrast, the “Steroids or Pentoxifylline for Alcoholic Hepatitis” study [11] reported that only 10% patients were infected during hospitalization; however, they accounted for 24% of the deaths in their study.
The predominant infections upon admission were lower respiratory tract infections (7/20) and cellulitis (7/20). Both represent frequent locations of outpatient infections in patients with chronic liver disease. On admission, these infections occurred in patients with more deteriorated liver function; notably, in our series, other common locations, such as the abdomen (ascites) and urinary tract, were underreported. Additionally, in a multicenter study led by Parker [6], patients who acquired in-hospital infections in Spain exhibited relatively few cases of urinary tract infections. In our cohort infections (pneumonia) were the most frequent in patients with AH who had acquired the infection during hospitalization or follow-up; however, the blood (bacteremia) and abdomen (ascites [SBP]) appeared to be important locations, consistent with other studies [20]. The appearance of these locations is attributable to not only a severe immunological deterioration of patients with AH but also hospitalization (nosocomial infections), prolonged hospital stay, and HD. Ascites and HE predispose to SBP and HE to lower respiratory tract infections (aspiration), respectively. Moreover, secondary mechanical effects on respiratory function owing to abdominal ascites or hydrothorax predispose patients to pulmonary infection [6].
From our infection data, we identified the bacteria responsible for 51% of the infections by culture, displaying consistency with a large multinational study [6] that identified the causative bacteria in 53% infections. Additionally, we found similar proportions of gram-negative and gram-positive bacteria (50%). Generally, gram-positive bacteria are predominant in skin, chest, and blood infections (catheter-related), whereas gram-negative bacteria are predominant in urinary tract infections and ascites. In our study, the most frequent gram-positive cocci were S. aureus and S. epidermidis, whereas the predominant gram-negative bacteria were E. coli and K. pneumoniae. In contrast to previous study [21] wherein Enterococcus was identified as the pathogen, this species was only isolated in three of our patients. Notably, at our center, we found a low incidence of MRB (14%) and only one fungal infection associated with another bacterial infection (CRBSI). This potentially reflects the effectiveness of the antibiotics administered at our center [22,23].
Patients with AH often develop SIRS and immune dysfunction, favoring BI [7,24,25]. Excessive alcohol consumption can induce gut dysbiosis and increase the permeability of the intestinal barrier, inducing bacterial translocation and resulting in endogenous inflammation [26]. Additionally, treatment with CS potentially increases the risk of infection in AH [12,20,27]. Moreover, in a significant proportion of patients with AH, hepatic cirrhosis can also predispose to infection via different mechanisms (immune dysfunction, intestinal dysbiosis, and bacterial translocation) [5,28]. Both situations possibly explain the presence of infections in AH (38% of patients in our study). In our study, BI resulted in a poor prognosis for patients with AH. Infected patients had worse survival rates and more instances of HD, especially ascites and HE, compared with non-infected patients. However, infection favored ACLF development in patients with AH. ACLF is associated with a high risk of short-term death (i.e., death < 28 days after hospital admission) in patients with acutely decompensated cirrhosis. In the context of intense systemic inflammation, it frequently develops in close temporal relationships with proinflammatory precipitating events and is associated with single- or multiple-organ failure [29,30]. Among the most frequent proinflammatory precipitation events in Europe are infection and AH [31]. In our study, the coexistence of infection with AH induced a high rate (32%) of ACLF with a severe course of ICU admission in several cases. Considering the prognostic implications of ACLF, this is an important finding since most previous studies did not consider the presence of ACLF because the syndrome had not been defined or used yet.
CS treatment in patients with AH seems to increase susceptibility to infection [9,11,12,20]; nevertheless, CS use is safe once the infection is under control. A meta-analysis of 12 randomized trials reported a 12% cumulative incidence of infection in patients with AH during CS therapy [13]. Although the treatment groups (CS and non-CS) in our study were not comparable, CS-treated and non-CS-treated patients presented no differences in the incidence of infections or mortality rate. This is consistent with the findings of Hmoud et al. [13], who found CS did not increase BI-related mortality in patients with severe AH.
Similar to other studies, we categorized infections based on onset time and peri- and post-admission diagnoses (in-hospital and follow-up infections). However, our data on follow-up infections were limited to those available in the registry; therefore, they were not included in the analysis. Nonetheless, infections upon admission in our study had two remarkable characteristics. First, on admission, infected patients had more advanced liver disease than did non-infected patients, based on the HD, Child–Pugh, and MELD scores. According to the PREDICT [30] and other studies on cirrhosis, infection and liver impairment are followed by greater susceptibility to HD and ACLF. This characteristic was not observed in previous studies, such as Louvet et al. [9]. Second, the infection upon admission exhibited favorable evolution. In our cohort, all infections upon admission resolved with adequate antibiotic treatment, and no deaths were recorded. In these patients, infection cure, outcome, and survival were similar to those in non-infected patients. However, not all series have made similar observations; in a multicenter study, Parker et al. [6] did not identify any differences in survival between infected patients upon admission and those infected during hospitalization.
Consistent with the study by Michelena et al. [10], one of the most important findings in our study was that patients infected during hospitalization presented a greater number of complications and yielded a higher mortality rate than did non-infected patients. The reason for this poor evolution is that infections develop concurrently with proinflammation, leading to immune paralysis and predisposing to severe infections [25]. Additionally, CS use and infections with a risk of aggressive bacterial resistance potentially contribute to infection severity. ACLF was the clinical complication that conferred the poorest prognosis to these patients; in fact, out of 22 in-hospital infected patients, eight (36.4%) developed ACLF, and five died. The fact that in-hospital infections have the worst prognostic value suggests the possibility of considering the use of antibiotic prophylaxis upon admission [14,32,33].
Despite the positive results, this study has some limitations. First, although we collected data of all clinical events, the biochemical data recorded during hospitalization was only collected at baseline. Second, we lacked information after hospital discharge as only two post-discharge clinical events were recorded: infections and death. Thus, no biochemical information was available to evaluate prognostic scores or other liver-related complications. Finally, we did not obtain information on alcohol consumption after discharge.
5. Conclusions
Infections were common in a cohort of patients with AH admitted to a tertiary academic hospital. The most frequent site of infection was the chest. Among the identified bacteria, half of the isolated organisms were gram-positive and the other half gram-negative. The number of infections caused by enteric bacteria predominantly gram-negative (in abdomen: ascites, UTI) was evenly equaled among chest, blood, and skin infections, with gram-positive bacteria predominating in these sites. Infections diagnosed upon admission were cured with antibiotics and had no impact on survival. Our findings suggest that in-hospital infections are commonly associated with serious complications in patients with AH, including a high rate of ACLF and death. Corticosteroid-treated patients displayed a nonsignificant increase in the total number of infections; and this was not accompanied by greater mortality.
Author Contributions
Victor Vargas, Meritxell Ventura-Cots and Cesar Jimenez conceived the study. Aina Martí-Carretero, Ares Villagrasa, Anna Aguilar and María Pérez acquired the data. Victor Vargas and Cesar Jimenez drafted the manuscript. All authors critically reviewed and gave final approval of the manuscript.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Ethics Committee for Clinical Research (CEIC), Vall d’Hebron University Hospital (project number: PR(AG)569-2023 date approval march 2023).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jepsen, P.; Younossi, Z.M. The global burden of cirrhosis: A review of disability adjusted life-years lost and unmet needs. J Hepatol 2021, 75, S3–13. [Google Scholar] [CrossRef] [PubMed]
- Kasper, P.; Lang, S.; Steffen, H.M.; Demir, M. Management of alcoholic hepatitis: A clinical perspective. Liver Int 2023, 43, 2078–2095. [Google Scholar] [CrossRef] [PubMed]
- Prado, V.; Caballería, J.; Vargas, V.; Bataller, R.; Altamirano, J. Alcoholic hepatitis: How far are we and where are we going? Ann Hepatol 2016, 15, 463–473. [Google Scholar] [PubMed]
- Vergis, N.; Atkinson, S.R.; Thursz, M.R. Assessment and management of infection in alcoholic hepatitis. Semin Liver Dis 2020, 40, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Martin-Mateos, R.; Van der Merwe, S.; Wiest, R.; Jalan, R.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction. Nat Rev Gastroenterol Hepatol 2022, 19, 112–134. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.; Im, G.; Jones, F.; Hernández, O.P.; Nahas, J.; Kumar, A.; Wheatley, D.; Sinha, A.; Gonzalez-Reimers, E.; Sanchez-Pérez, M.; et al. Clinical and microbiological features of infection in alcoholic hepatitis: An international cohort study. J Gastroenterol 2017, 52, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Bataller, R.; Arab, J.P.; Shah, V.H. Alcohol-associated hepatitis. N Engl J Med 2022, 387, 2436–2448. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.K.; Bataller, R.; Ahn, J.; Kamath, P.S.; Shah, V.H. ACG Clinical Guideline: Alcoholic liver disease. Am J Gastroenterol 2018, 113, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Louvet, A.; Wartel, F.; Castel, H.; Dharancy, S.; Hollebecque, A.; Canva-Delcambre, V.; Deltenre, P.; Mathurin, P. Infection in patients with severe alcoholic hepatitis treated with steroids: Early response to therapy is the key factor. Gastroenterology 2009, 137, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Michelena, J.; Altamirano, J.; Abraldes, J.G.; Affò, S.; Morales-Ibanez, O.; Sancho-Bru, P.; Dominguez, M.; García-Pagán, J.C.; Fernández, J.; Arroyo, V.; et al. Systemic inflammatory response and serum lipopolysaccharide levels predict multiple organ failure and death in alcoholic hepatitis. Hepatology 2015, 62, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Thursz, M.R.; Richardson, P.; Allison, M.; Austin, A.; Bowers, M.; Day, C.P.; Downs, N.; Gleeson, D.; MacGilchrist, A.; Grant, A.; et al. Prednisolone or pentoxifylline for alcoholic hepatitis. N Engl J Med 2015, 372, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Vergis, N.; Atkinson, S.R.; Knapp, S.; Maurice, J.; Allison, M.; Austin, A.; Forrest, E.H.; Masson, S.; McCune, A.; Patch, D.; et al. In patients with severe alcoholic hepatitis, prednisolone increases susceptibility to infection and infection-related mortality, and is associated with high circulating levels of bacterial DNA. Gastroenterology 2017, 152, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Hmoud, B.S.; Patel, K.; Bataller, R.; Singal, A.K. Corticosteroids and occurrence of and mortality from infections in severe alcoholic hepatitis: A meta-analysis of randomized trials. Liver Int 2016, 36, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, C.; Ventura-Cots, M.; Sala, M.; Calafat, M.; Garcia-Retortillo, M.; Cirera, I.; Cañete, N.; Soriano, G.; Poca, M.; Simón-Talero, M.; et al. Effect of rifaximin on infections, acute-on-chronic liver failure and mortality in alcoholic hepatitis: A pilot study (RIFA-AH). Liver Int 2022, 42, 1109–1120. [Google Scholar] [CrossRef] [PubMed]
- Sersté, T.; Cornillie, A.; Njimi, H.; Pavesi, M.; Arroyo, V.; Putignano, A.; Weichselbaum, L.; Deltenre, P.; Degré, D.; Trépo, E.; et al. The prognostic value of acute-on-chronic liver failure during the course of severe alcoholic hepatitis. J Hepatol 2018, 69, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Crabb, D.W.; Bataller, R.; Chalasani, N.P.; Kamath, P.S.; Lucey, M.; Mathurin, P.; McClain, C.; McCullough, A.; Mitchell, M.C.; Morgan, T.R.; et al. Standard definitions and common data elements for clinical trials in patients with alcoholic hepatitis: Recommendation from the NIAAA alcoholic hepatitis consortia. Gastroenterology 2016, 150, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for management of patients with decompensated cirrosis. J Hepatol 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Moreau, R.; Jalan, R.; Ginès, P.; EASL-CLIF Consortium CANONIC Study. Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis. J Hepatol 2015, 62, S131–43. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Dhanda, A.D.; Sinha, A.; Hunt, V.; Saleem, S.; Cramp, M.E.; Collins, P. L Infection does not increase long-term mortality in patients with acute severe alcoholic hepatitis treated with CS. World J Gastroenterol 2017, 23, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Beisel, C.; Blessin, U.; Schulze Zur Wiesch, J.; Wehmeyer, M.H.; Lohse, A.W.; Benten, D.; Kluwe, J. Infections complicating severe alcoholic hepatitis: Enterococcus species represent the most frequently identified pathogen. Scand J Gastroenterol 2016, 51, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Piano, S.; Singh, V.; Caraceni, P.; Maiwall, R.; Alessandria, C.; Fernandez, J.; Soares, E.C.; Kim, D.J.; Kim, S.E.; Marino, M.; et al. Epidemiology and effects of bacterial infections in patients with cirrhosis worldwide. Gastroenterology 2019, 156, 1368–1380. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Carmeli, Y.; Omrani, A.S.; Moore, L.S.P.; Tawadrous, M.; Irani, P. Ceftazidime-avibactam for the treatment of serious Gram-negative infections with limited treatment options: A systematic literature review. Infect Dis Ther 2021, 10, 1989–2034. [Google Scholar] [CrossRef] [PubMed]
- Sipeki, N.; Antal-Szalmas, P.; Lakatos, P.L.; Papp, M. Immune dysfunction in cirrhosis. World J Gastroenterol 2014, 20, 2564–2577. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Levitsky, J. Infection and alcoholic liver disease. Clin Liver Dis 2016, 20, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Szabo, G.; Saha, B. Alcohol’s effect on host defense. Alcohol Res 2015, 37, 159–170. [Google Scholar] [PubMed]
- Karakike, E.; Moreno, C.; Gustot, T. Infections in severe alcoholic hepatitis. Ann Gastroenterol 2017, 30, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Kamath, P.S.; Reddy, K.R. The evolving challenge of infections in cirrhosis. N Engl J Med 2021, 384, 2317–2330. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Moreau, R.; Jalan, R. Acute-on-chronic liver failure. N Engl J Med 2020, 382, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Fernandez, J.; Papp, M.; Caraceni, P.; Laleman, W.; Gambino, C.; Giovo, I.; Uschner, F.E.; Jimenez, C.; Mookerjee, R.; et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J Hepatol 2020, 73, 842–854. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Fernandez, J.; Papp, M.; Caraceni, P.; Laleman, W.; Gambino, C.; Giovo, I.; Uschner, F.E.; Jansen, C.; Jimenez, C.; et al. PREDICT identifies precipitating events associated with the clinical course of acutely decompensated cirrhosis. J Hepatol 2021, 74, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Forrest, E.; Bernal, W. The role of prophylactic antibiotics for patients with severe alcohol-related hepatitis. JAMA 2023, 329, 1552–1553. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Badal, J.; Nawras, M.; Battepati, D.; Farooq, U.; Arif, S.F.; Lee-Smith, W.; Aziz, M.; Iqbal, U.; Nawaz, A.; et al. Role of rifaximin in the management of alcohol-associated hepatitis: A systematic review and meta-analysis. J Gastroenterol Hepatol 2023, 38, 703–709. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Impact survival according to the infection.
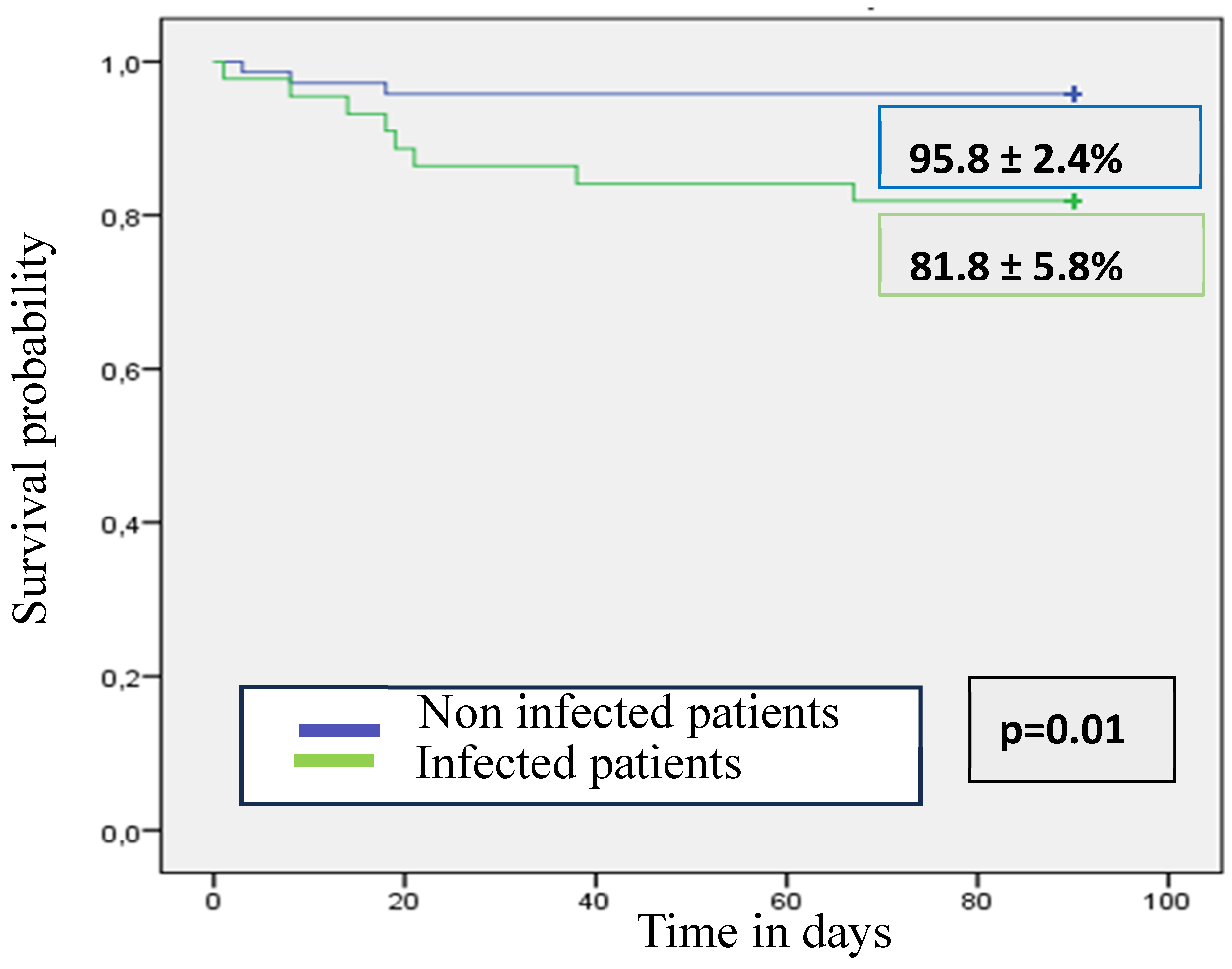
Figure 2.
Survival according to the time of the acquisition of infection.
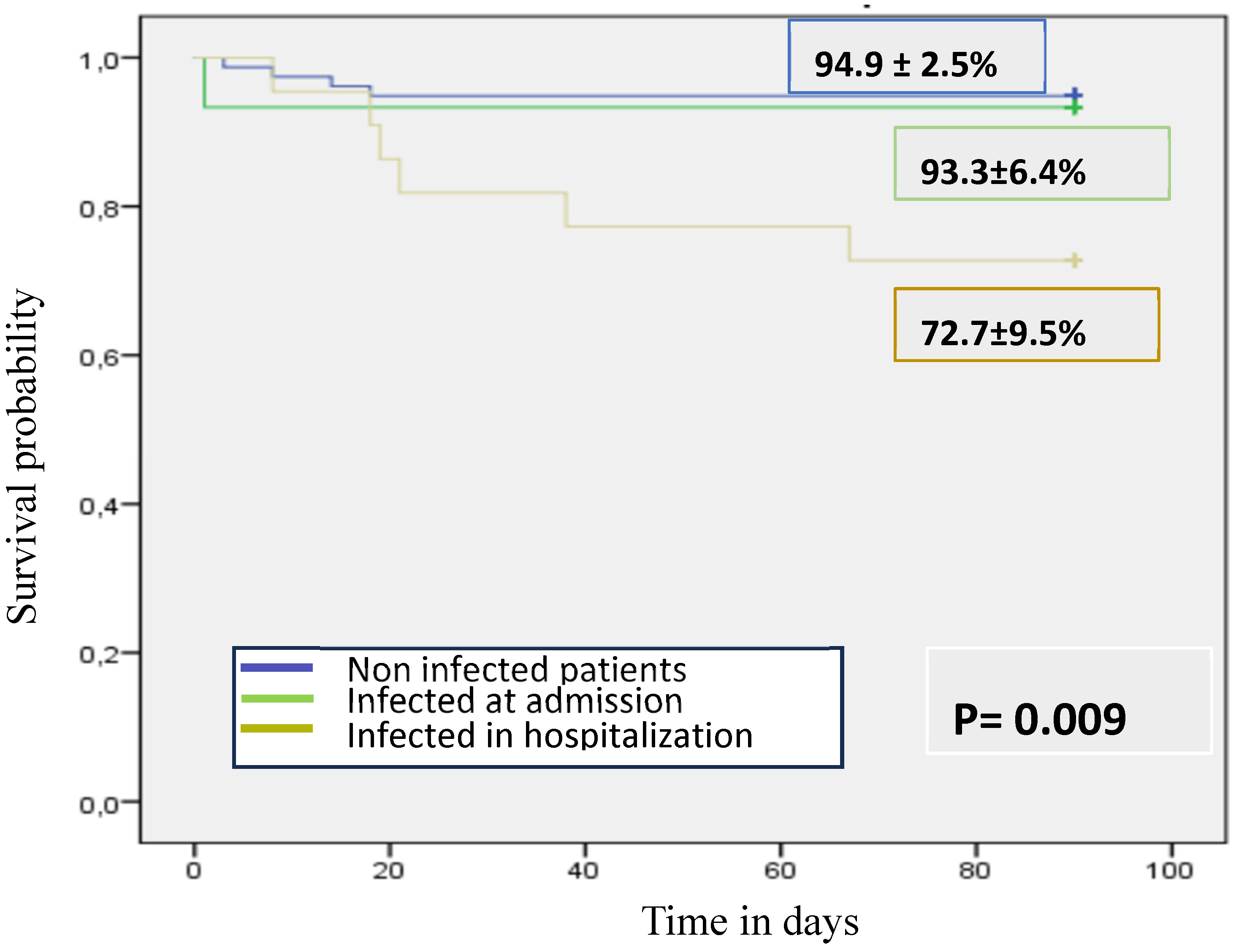
Table 1.
Baseline clinical and biological characteristics.
| n=115 | |
|---|---|
| Medical History | |
| Sex (male), n(%) | 88 (76.5%) |
| Age, median (IQR) P 25-75 | 50 (44-58) |
| Race, n(%) | Caucasian 98 (85%) |
| BMI, median (IQR) P 25-75 | 27 (24-31) |
| Arterial hypertension, n(%) | 35 (30.4%) |
| Diabetes, n(%) | 15 (13%) |
| Dyslipidemia, n(%) | 23 (20%) |
| Metabolic syndrome, n(%) | 16 (14%) |
| Obesity, n(%) | 28 (24%) |
| Chronic renal failure, n(%) | 0 (0%) |
| Ischemic heart disease, n(%) | 4 (3.4%) |
| Chronic obstructive pulmonary disease, n(%) | 7 (6%) |
| Hepatic cirrhosis, n(%) | 68 (59%) |
| History of hepatic decompensation, n(%) | 28 (24%) |
| Previous alcohol-related hepatitis, n(%) | 23 (20%) |
| Hepatocellular carcinoma, n(%) | 0 (0%) |
| Prophylactic antibiotics, n(%) | 2 (1.7%) |
| Hospital admission (BASELINE) | |
| Hepatic cirrhosis, n(%) | 81 (70%) |
| Hepatic decompensation, n(%) | 64 (56%) |
| Infection, n(%) | 18 (16%) |
| Ascites, n(%) | 59 (51%) |
| Hepatic encephalopathy, n (%) | 15 (13%) |
| Gastrointestinal bleeding, n (%) | 7 (6%) |
| Acute kidney injury, n(%) | 13 (11%) |
| Acute on chronic liver failure, n(%) | 7 (6%) |
| Maddrey score, median (IQR) P 25-75 | 40 (20-50) |
| MELD score, median (IQR) P 25-75 | 19 (16-22) |
| MELD Na score, median (IQR) P 25-75 | 22 (19-22) |
| MELD 3.0 score, median (IQR) P 25-75 | 23 (20-26) |
| Child-Pugh score, median (IQR) P 25-75 | 10 (9-11) |
| Bilirubin (mg/dL), median (IQR) P 25-75 | 7.4 (4.8-12) |
| INR, median (IQR) P 25-75 | 1.5 (1.2-1.8) |
| Albumin (g/dL), median (IQR) P 25-75 | 2.7 (2.4-3.1) |
| Creatinine (mg/dL), median (IQR) P 25-75 | 0.7 (0,5-0.9) |
| AST (UI/L), median (IQR) P 25-75 | 147 (102-264) |
| ALT (UI/L), median (IQR) P 25-75 | 61 (35-89) |
| GGT (UI/L), median (IQR) P 25-75 | 593 (223-1461) |
| ALP (UI/L), median (IQR) P 25-75 | 204 (150-328) |
| CRP (mg/dL), median (IQR) P 25-75 | 2.5 (1-5.5) |
| Leucocytes (10^9/L), median (IQR) P 25-75 | 8.2 (6.1-11.6) |
| Platelets 10^9/L | 104 (64-153) |
IQR: interquartile range, BMI: body mass index, MELD: Model for End-stage Liver Disease, INR: international normalized ratio, AST: Aspartate transaminase, ALT: Alanine aminotransferase, GGT: Gamma-glutamyl Transferase, ALP: Alkaline Phosphatase, CRP: C-reactive protein.
Table 2.
Site infection and bacteria classification (gram stain).
| Site | Number of infections, (%) | Positive cultures | Bacteria, (n) | Gram positive or gram negative, (n) |
|---|---|---|---|---|
| Chest | 24 (35%) | 3 | Streptoccocus pneumoniae, Staphylococcus aureus, Clamydia pneumoniae | Gram positive (2) Gram negative (1) |
| Skin | 14 (20%) | 3 | Staphylococcus aureus (2) Staphylococcus aureus* | Gram positive (3) |
| Blood | 11 (16%) | 11 | Acinetobacter baumannii Staphylococcus hemolyticus (2) Staphylococcus hemolyticus* Staphylococcus epidermidis (4) Enterococcus faecalis*, Klebsiella oxytoca, Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Enterococcus faecium | Gram-positive (10) Gram-negative (4) |
| Abdominal (Ascites) | 11 (16%) | 10 | Staphylococcus aureus (2) Acinetobacter baumannii Staphylococcus hemolyticus Escherichia coli, Enterobacter cloacae, Klebsiella pneumoniae* Enterococcus faecium, Serratia marcenses, Acinetobacter pittii | Gram-positive (4) Gram-negative (6) |
| Urinary tract | 9 (13%) | 9 | Escherichia coli (5), Klebsiella pneumoniae (2), Klebsiella pneumoniae* Enterococcus faecalis, Klebsiella aerogenes | Gram-positive (1) Gram-negative (9) |
| TOTAL | 69 | 36 | 40 | Gram-positive (20) Gram-negative (20) |
| * Multidrug-resistant bacteria | ||||
Table 3.
a. Characteristics of bacterial infections at admission.
| ID-Episode | Infection | Bacteria | SIRS | ACLF | Resolution infection | Antibiotics | MRB |
| P4- 1 | SBP | Staphylococcus aureus | Yes | No | Yes | Cefazolin | |
| P6- 2 | Cellulitis | Non-isolated bacteria | Yes | No | Yes | Levofloxacin + Clindamycin | |
| P8- 3 | Aspiration Pneumonia | Non-isolated bacteria | Yes | No | Yes | Amoxicillin-Clavulanate | |
| P17- 4 | Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | |
| P19- 5 | Pneumonia | Non-isolated bacteria | Yes | No | Yes | Amoxicillin-Clavulanate | |
| P33- 6 | Bacteremia | Acinetobacter baumannii + Staphylococcus haemolyticus | Yes | No | Yes | Ciprofloxacin | |
| SBP | |||||||
| P62- 7 | Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | |
| P69- 8 | Cellulitis | Non-isolated bacteria | Yes | No | Yes | Amoxicillin-Clavulanate | |
| P74- 9 | UTI | Escherichia coli | No | No | Yes | Ceftriaxone | |
| P76- 10 | Pneumonia | Streptococcus pneumoniae | Yes | Yes | Yes | Cefotaxime + Azithromycin | |
| P79- 11 | Pneumonia | Chlamydia pneumoniae | No | No | Yes | Levofloxacin | |
| P82- 12 | UTI | Klebsiella pneumoniae | Yes | Yes | Yes | Meropenem | |
| P86- 13 | Pneumonia | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | |
| P26- 14 | Aspiration Pneumonia | Non-isolated bacteria | No | No | Yes | Piperacillin-Tazobactam | |
| P27- 15 | Cellulitis | Staphylococcus aureus | No | No | Yes | Amoxicillin-Clavulanate | |
| P89- 16 | Aspiration Pneumonia | Non-isolated bacteria | Yes | Yes | Yes | Piperacillin-Tazobactam | |
| Cellulitis | Non-isolated bacteria | ||||||
| P99- 17 | Cellulitis | Non-isolated bacteria | No | No | Yes | Amoxicillin-Clavulanate | |
| P107- 18 | UTI | Escherichia coli + Enterococcus faecalis | No | No | Yes | Amoxicillin-Clavulanate |
SBP: spontaneous bacterial peritonitis, UTI: urinary tract infection, MRB: multi-drug resistant bacteria.
Table 4.
Clinical and biological characteristics at admission.
| Infected patients n=18 |
No infected patients N=97 |
p | |
|---|---|---|---|
| Sex (male), n(%) | 12 (66.6%) | 75 (77,3%) | 0.28 |
| Age, median (IQR) P 25-75 | 45 (41.7- 55.7) | 51 (44–58) | 0.43 |
| Clinical History | |||
| BMI, median (IQR) P 25-75 | 27.3 (23-31.2) | 27.2 (24-31.7) | 0.86 |
| Arterial hypertension, n(%) | 5 (28%) | 30 (31%) | 0.79 |
| Diabetes, n(%) | 2 (11%) | 13 (13.4%) | 0.80 |
| Metabolic syndrome, n(%) | 2 (11%) | 14 (14.4%) | 0.70 |
| Obesity, n(%) | 7 (39%) | 21 (22%) | 0.11 |
| Chronic renal failure, n(%) | 0 | 4 (4%) | 0.91 |
| History of HD, n(%) | 6 (33.3%) | 22(22.6%) | 0.33 |
| Previous AH, n(%) | 5 (28%) | 18 (18.5%) | 0.36 |
| Prophylactic antibiotics, n(%) | 1 (5%) | 1 (1%) | 0.17 |
| BASELINE | |||
| HC diagnosis, n(%) | 16 (88%) | 65 (67%) | 0.062 |
| HD, n(%) | 16 (88%) | 48 (49.5%) | 0.005 |
| Ascites, n(%) | 14 (78%) | 45 (46,4%) | 0.029 |
| HE, n (%) | 9 (50%) | 6 (6.2%) | 0.001 |
| GIB, n (%) | 0 | 7 (7.2%) | 0.25 |
| AKI, n(%) | 3 (16.6%) | 10 (10.3%) | 0.43 |
| ACLF, n(%) | 3 (16.6%) | 4 (4.1%) | 0.041 |
| Maddrey score, median (IQR) P 25-75 | 48 (32–68.5) | 38 (18–51) | 0.022 |
| MELD score, median (IQR) P 25-75 | 22 (19-25) | 19 (15-21) | 0.012 |
| MELD Na score, median (IQR) P 25-75 | 24 (22-29) | 22 (19-26) | 0.037 |
| MELD 3.0 score, median (IQR) P 25-75 | 25 (25-28) | 23 (20-25) | 0.013 |
| Child-Pugh score, median (IQR) P 25-75 | 11 (11–12) | 10 (9–11) | 0.011 |
| Bilirubin serum (mg/dL), median (IQR) P 25-75 | 9.89 (6.96–16.31) | 7.16 (4.53–11.62) | 0.084 |
| INR, median (IQR) P 25-75 | 1.8 (1.4–1.95) | 1.5 (1.15–1.8) | 0.027 |
| Creatinine (mg/dL), median (IQR) P 25-75 | 0.63 (0.55–0.87) | 0.67 (0.54–0.88) | 0.81 |
| Albumin (g/dl), median (IQR) P25–P75 | 2.5 (2.3–2.7) | 2.8 (2.4–3.2) | 0.038 |
| CRP (mg/dL), median (IQR) P 25-75 | 3 (1.5-9.5) | 2.4 (0.9-5.2) | 0.31 |
| Leucocytes (10^9/L), median (IQR) P 25-75 | 8.2 (5.8–10.7) | 10.3 (6.6–13.2) | 0.26 |
IQR: interquartile range, BMI: body mass index, HC: hepatic cirrhosis, GIB: gastrointestinal bleeding, HD: hepatic decompensations, AH: alcohol-associated hepatitis, HE: hepatic encephalopathy, AKI: acute kidney injury, ACLF: acute-on-chronic liver failure, MELD: Model for end-stage Liver Disease, INR: international normalized ratio, CRP: C-reactive protein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



