Submitted:
12 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Background and objective: Iliopsoas abscess (IPA) is a rare condition with varied symptomology and etiology. Less than one-third of patients with IPA present on the emergency department (ED) admission with the traditional triad of fever, back pain, and restricted hip motion (or limp), leading to delays in diagnosis and management. This case report aims to bring awareness among healthcare professionals regarding the atypical presentation and introduce a potential differential diagnosis when evaluating patients with fever and back pain. The intention is to provide insights into the signs and symptoms that may indicate the presence of an iliopsoas abscess and prompt additional investigations. Case report: Here, we describe a case of primary iliopsoas abscess associated with drug-induced acute liver failure in our ED. The patient complained of pain in the left lumbar region and fatigue that started two weeks before this presentation, claiming that, during the previous night, the pain suddenly worsened. She had a fever, pain at palpation in the right hypochondriac and left lumbar regions, accompanied by fever and vomiting, jaundiced skin, and sclera at the examination in ED. On abdominal ultrasonography, the diagnosis of acute cholangitis was suspected. The laboratory test shows leukocytosis with neutrophilia, thrombocytosis, hepatocytolysis syndrome, and hyperbilirubinemia with the predominance of indirect bilirubin. We performed then abdominal and pelvic computed tomography, which confirmed the diagnosis of cholelithiasis observed with the diameter of the bile duct within normal limits but also showed an abscess-like collection fused to the interfibrillar level of the left iliopsoas muscle; a diagnosis we most likely would have been missed. After that, the patient was hospitalized in the General Surgery Department, and surgery drainage of the abscess was performed. The patient's evolution was excellent; she was discharged after 11 days. Conclusions: The case presented here exemplifies how iliopsoas abscess, a rare cause of back pain, can quickly go unrecognized, especially in the emergency department. Our experiences will raise awareness among doctors in emergency departments about this uncommon but essential diagnosis. With advancements in diagnostic tools and techniques, we aspire that more cases of iliopsoas abscess will be accurately diagnosed.
Keywords:
iliopsoas abscess
; emergency department
; multidisciplinary approach
; drug-induced acute liver failure
; critical care
; personalized medicine
1. Background
The occurrence of an iliopsoas abscess (IPA), a suppurative collection in the compartment of the psoas and iliacus muscles, was initially documented by Mynter et al. in 1881 [1]. It continues to be a rare condition, with a global reported incidence of only 12 cases per year [2].
There are two classifications for iliopsoas abscesses based on their origin: primary and secondary. Primary abscesses occur when an infection from a distant site spreads through the bloodstream or lymphatic system. A single organism typically causes these abscesses and may be hidden. On the other hand, secondary abscesses result from the direct extension of infection from nearby structures such as the gastrointestinal or genitourinary tract, lumbar spine, or hip region. It has been reported that secondary iliopsoas abscesses have a higher mortality rate compared to the primary ones [3].
The symptoms of iliopsoas abscess can be unclear and diverse. The traditional triad of fever, back pain, and restricted hip movement (or limp), known as the psoas-muscle sign, is only observed in 30% of cases, making diagnosis challenging [1,4]. Consequently, the condition is often missed during the initial visit to the emergency department [4].
Previous reports need to adequately discuss the diagnostic complexities associated with iliopsoas abscess, mainly when it refers to emergency physicians. Therefore, this report aims to share our firsthand experience in our emergency department in diagnosing this uncommon but important disease.
Case Report
A 49-year-old female patient presented to our Emergency Department with complaints of pain in the lower left abdomen, specifically in the left iliac fossa and right hypochondriac region, accompanied by fever and vomiting. Upon physical examination, the patient exhibited normal breathing (16 breaths per minute) and was stable regarding hemodynamics. However, she had jaundiced skin and sclera, with a blood pressure reading of 130/80 mmHg, a heart rate of 80 beats per minute, a body temperature of 38.8 °C, a Glasgow Coma Score (GCS) of 15/15, and a peripheral oxygen saturation (SpO2) of 97% while breathing ambient air.
The patient complained of pain in the left lumbar region and fatigue that started two weeks before this presentation, claiming that, during the previous night, the pain suddenly worsened. From her medical history, she mentioned essential hypertension under treatment and untreated hypercholesterolemia. Regarding living and working conditions, the patient lives in the country with her family as a housewife. Also, the patient denies vicious behaviors such as smoking, alcohol, or drugs.
The patient performed an abdominal ultrasound, which revealed multiple gallstones, but the main bile duct was in normal range value (Figure 1), so acute cholangitis was initially suspected.
Blood was taken for lab tests, and she was scheduled for an abdominal and pelvis computed tomography (CT) scan with a contrast substance. She received an intravenous perfusion with 1 g acetaminophen, 40 mg pantoprazole, 40 mg drotaverine, and 500 mL normal saline (0.9%) solution, but she remained unresponsive to the administration of the antalgic and antispastic treatment. Until the CT was performed, the blood tests arrived, which were severely increased (Table 1). The patient had leukocytosis with neutrophilia. Reactive thrombocytosis associated with infection. Hepatocytolysis syndrome. Hyperbilirubinemia with the predominance of indirect bilirubin. There is no modification on a urine test.
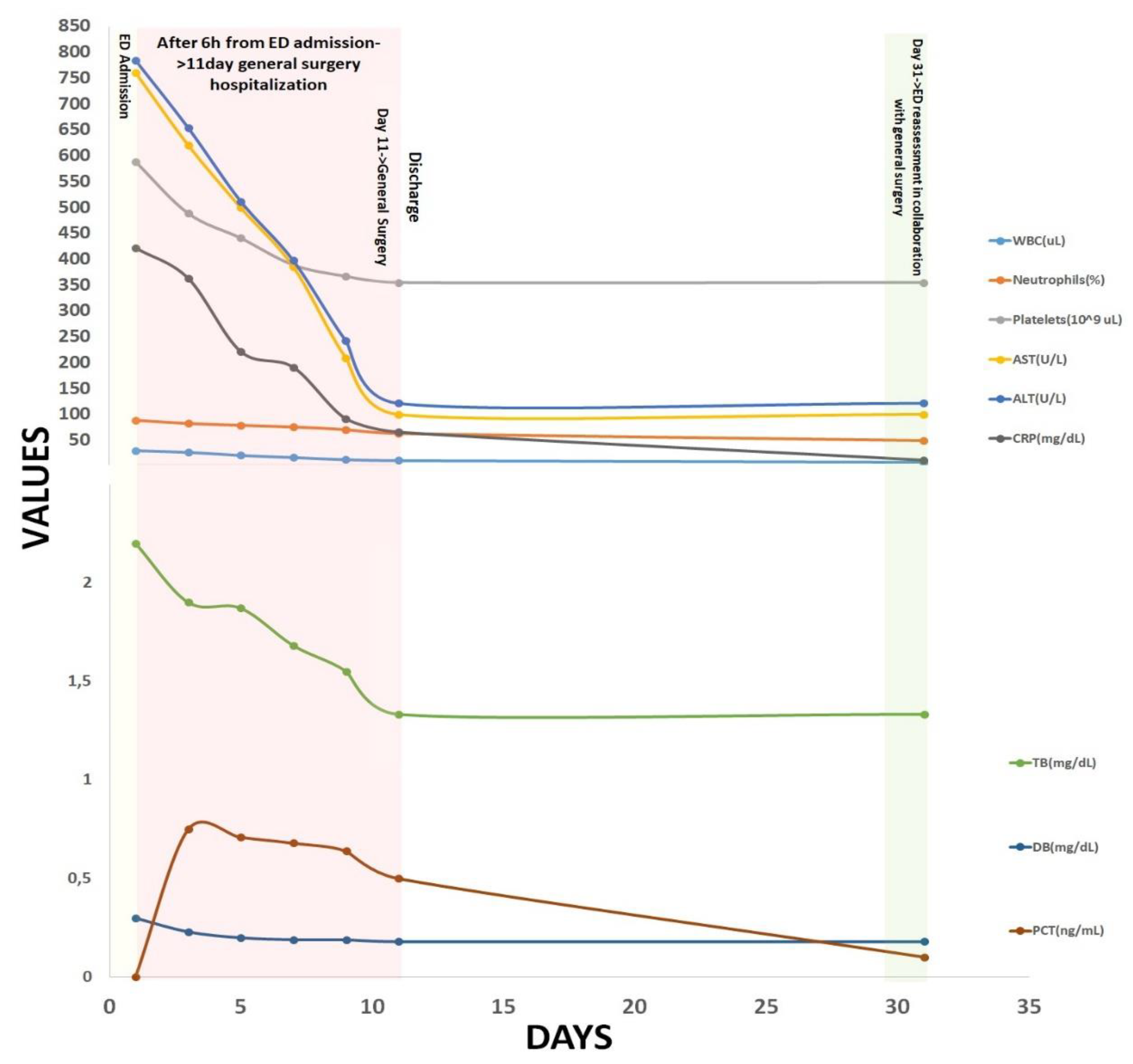
Figure 2.
Laboratory test values evolution from ED admission until reassessment (day 31) in the ED in collaboration with our general surgery department.
Figure 2.
Laboratory test values evolution from ED admission until reassessment (day 31) in the ED in collaboration with our general surgery department.
After analyzing the laboratory test results, we repeated and performed a more detailed medical history and anamnesis of the patient. As a result of increasing pain, the patient had taken several medications over the last five days, including acetaminophen, naproxen, ketoprofen, metamizole, amoxicillin + clavulanic acid, diclofenac, and ibuprofen. However, she could not provide us with the exact dosage of these medications but mentioned that she had consumed a significant number of pills. Based on these findings, we also considered the diagnosis of drug-induced acute hepatitis.
Further, the abdominal and pelvis CT scan with contrast substance performed showed the cholelithiasis observed on abdominal ultrasound with common bile duct diameter in normal limit values and fused abscess-type collections at the interfibrillar level of the left iliopsoas muscle (Figure 3).
In the emergency department, she received intravenous fluid resuscitation, metamizole 500 mg, drotaverine 80 mg, and an empiric antibiotic (ceftriaxone). Based on the following table (Table 1), where we performed a short literature review of the documented origins of secondary spread to the psoas muscles, we decided to take additional chest radiography and blood tests in the ED to identify the cause of the patient's left iliopsoas abscess.
The chest radiography showed clear lungs, a healthy heart, and a clearly outlined chest cavity (Figure 4), thus excluding tuberculosis and, implicitly, Pott's disease and tuberculous spondylitis as causes of iliopsoas abscess. Despite a thorough CT scan examination, no evidence of colonic micro perforations was found, leaving the cause uncertain. Additionally, the patient explicitly denied any past involvement in intravenous drug abuse. Furthermore, we requested an evaluation of the patient by the general surgeon on duty, who indicated hospitalization and surgical drainage.
Following this, it was decided that the patient should be transferred to the general surgery department. After the preoperative preparation, surgical intervention is performed, and the Dos Santos incision is practiced. After dissection of the anatomical planes, a voluminous abscess is drained from the level of the left psoas muscle, taking cultures from this level simultaneously. It continues with the debridement and washing of the operative area, placing drain tubes at this level, one with the tip located in the left paravesical pelvis (Figure 4A) and one with an ascending trajectory along the left iliopsoas muscle (Figure 4B) and the tip on its ventral side, next to the L3 vertebral body, as it can be seen on the second abdominal and pelvis CT scan with contrast substance performed after surgical drainage.
The fluid culture from the iliopsoas abscess was positive for methicillin-sensitive Staphylococcus aureus (MSSA). According to the antibiogram, the identified germ was sensitive to Linezolid. Thus, it has been decided that treatment should be started with Linezolid 600 mg twice a day for ten days. During hospitalization, the patient was screened for possible sources of infection. Blood and urine cultures were normal, as well as the hepatitis A, B, C, and HIV infection. She performed a gastroscopy and colonoscopy with normal results. Also, a magnetic resonance imaging (MRI) of the thoracic and lumbar spine did not identify a secondary cause for her left iliopsoas abscess (Figure 5).
Figure 2 depicts the patient's laboratory test values during hospitalization, demonstrating the favorable postoperative evolution. After 12 days of hospitalization in the general surgery department, she was discharged in good general condition, appetizing, and afebrile. After 30 days, she was medically and clinically reassessed in the Emergency Department in collaboration with the general surgeon, where no sign of infection was observed, and laboratory tests were in the normal range.
Discussion
Because of its variable and nonspecific presentations, combined with its rare occurrence in the emergency department, the diagnosis of iliopsoas abscess may be delayed or misdiagnosed [4]. The diagnostic challenges of psoas abscess, particularly in the context of emergency physicians, have yet to be adequately addressed in literature reports. In a previous study conducted by Chen et al., they documented a 1-year experience with the diagnosis of iliopsoas abscess in 10 patients admitted to ED. Of these ten patients, only seven were diagnosed in the ED, while the remaining three were initially admitted with this diagnosis. Among those seven patients, their initial ED diagnoses varied, including fever of unknown origin (2 patients), septic shock (2 patients), shock (1 patient), sepsis (1 patient), and peritonitis (1 patient). The most commonly reported symptom was pain, with 80% of patients experiencing it and 50% explicitly complaining of back pain. The classic triad of fever, back pain, and limp, typically associated with iliopsoas abscess, was only present in 30% of patients. The average duration of symptoms was 10.6 days, ranging from 1 to 30 days. It took an average of 1.7 days, ranging from 0 to 7 days, to establish the diagnosis. Ultrasound was used to diagnose iliopsoas abscesses in 6 patients, computed tomography in 3, and surgery in 1 [4]. Over two years, a total of 32 patients who were admitted to a university hospital were also analyzed. The mean time required to diagnose IPA from symptom onset was 21 ± 15.1 days, ranging from 5 to 60 days. The most commonly observed presenting features were fever, limp, rigid flexion deformity, and back pain, which were found in 25 (78.1%), 24 (75%), 23 (72.9%), and 22 (68.7%) patients, respectively. The classic triad of IPA was only detected in 13 patients (40.6%). Of the 32 patients, 18 (56.3%) had primary IPA, while 14 (43.7%) had secondary IPA [20]. In a multicentric study conducted by Lee et al., it was discovered that IPA originated primarily in 50 patients (28.4%) and secondarily in 126 patients (71.6%). This finding was only recently reported [21].
As reported in various other studies, Staphylococcus aureus is the most common causative organism of primary IPA, and it was also the cause of the iliopsoas abscess in our patient.
The patient we managed at ED presented with iliopsoas abscess symptoms, fever, and discomfort in the left side of her back, which started 14 days before she arrived at our emergency department. Nonetheless, in the case of our patient, although she had performed various investigations and clinical examinations, no secondary cause was found. Her left iliopsoas abscess was successfully detected through a CT scan and effectively managed using percutaneous drainage and intravenous antibiotics. This case emphasizes the importance of maintaining a high level of suspicion to identify this condition promptly, as misdiagnosis may occur. In addition, it is essential to note that not all cases of iliopsoas abscess present with the traditional triad of symptoms [1]. If acute cholangitis had not been coincidentally suspected on abdominal ultrasound and the subsequent abdominal and pelvic CT scan performed, the diagnosis of iliopsoas abscess in our patient might have been entirely missed during a routine examination in the emergency department. On the other hand, the successful outcome of our patient's treatment aligns with the existing literature on the selection of empiric antibiotics in emergencies and surgical drainage of abscesses [3,22].
Due to these factors, we believe that the actual prevalence of iliopsoas abscesses is often underestimated, as many patients, unfortunately, died due to septic shock or fever of unknown origin before the condition can be correctly identified. We hope our own experiences and others will raise awareness among doctors in emergency departments about this rare but important disease. With advancements in diagnostic tools and techniques, we aspire that more cases of iliopsoas abscess will be accurately diagnosed.
Conclusions
The case presented here exemplifies how psoas abscess, a rare cause of back pain, can quickly go unrecognized, especially in the emergency department. It is crucial for emergency physicians to be knowledgeable about the signs and symptoms that may indicate a psoas abscess and to initiate further investigation. In patients with known risk factors for it that present the ED with fever, limp, and back pain, psoas abscess should be considered a potential cause of low back pain. While laboratory tests and ultrasound can provide helpful information, they alone cannot confirm or rule out the diagnosis. Therefore, superior imaging using CT or MRI is the preferred diagnostic tool. Hospitalization is necessary for all patients with iliopsoas abscesses to undergo surgical or percutaneous drainage and receive appropriate antibiotic therapy.
Author Contributions
Conceptualization D.P., F.B. L.S. and O.A.M.; methodology, D.P., D.M., D.S., C.G.W., O.A.M., S.M., C.T. and F.B.; software, L.S., F.B. and D.P.,; validation, O.A.M., S.M., F.B. and C.G.W.; investigation, C.G.W., D.M., D.P., D.S., and O.A.M.; resources, D.P. and F.B.; writing—original draft preparation, O.A.M., D.P., L.S., C.T. and F.B.; writing—review and editing, F.B., C.G.W., D.S., D.M., and O.A.M.; visualization, L.S., O.A.M., S.M., D.P., and C.T.; supervision, O.A.M. and F.B. All authors have read and agreed to the published version of the manuscript.
Funding
We would like to acknowledge the Victor Babes University of Medicine and Pharmacy Timisoara for covering the publication costs for this research paper.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki and approved by the Ethics Committee of Emergency Municipal Clinical Hospital Timisoara (approval number: E-4455/ 06.08.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets are not publicly available, but Popa Daian may provide de-identified data upon request.
References
- Mynter, H. , Acute Psoitis. Buffalo Med Surg J 1881, 21(5), 202–210. [Google Scholar] [PubMed]
- Garner, J.; Meiring, P.; Ravi, K.; Gupta, R. , Psoas abscess–not as rare as we think? Colorectal Disease 2007, 9(3), 269–274. [Google Scholar] [CrossRef] [PubMed]
- Shields, D.; Robinson, P.; Crowley, T. P. , Iliopsoas abscess – A review and update on the literature. International Journal of Surgery 2012, 10(9), 466–469. [Google Scholar] [CrossRef] [PubMed]
- Chern, C.-H.; Hu, S.-C.; Kao, W.-F.; Tsai, J.; Yen, D.; Lee, C.-H. , Psoas abscess: Making an early diagnosis in the ED. The American Journal of Emergency Medicine 1997, 15(1), 83–88. [Google Scholar] [CrossRef] [PubMed]
- Moslemi, S.; Tahamtan, M.; Hosseini, S. V. , A Late-onset Psoas Abscess Formation Associated with Previous Appendectomy: A Case Report. Bull Emerg Trauma 2014, 2(1), 55–8. [Google Scholar] [PubMed]
- Debes, J. D.; Lopez-Morra, H.; Dickstein, G. , A psoas abscess caused by Pseudomonas aeruginosa due to diverticular perforation. Am J Gastroenterol 2006, 101(9), 2168. [Google Scholar] [CrossRef] [PubMed]
- Yang, J. Y.; Lee, J. K.; Cha, S. M.; Joo, Y. B. , Psoas abscess caused by spontaneous rupture of colon cancer. Clin Orthop Surg 2011, 3(4), 342–4. [Google Scholar] [CrossRef] [PubMed]
- Staudinger, R.; Sharma, R.; Patel, S., Psoas Abscess: A Rare Initial Manifestation of Crohn's Disease: 682. Official journal of the American College of Gastroenterology | ACG 2015, 110, S301.
- Dowling Montalva, Á.; de Araujo Santana Junior, R. N.; Molina, M. , Full Endoscopic Treatment for a Fibrosis Complication after Psoas Abscess. Journal of Personalized Medicine 2023, 13(7), 1166. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.; Neal, B.; Jacobs, A. , Iliopsoas Abscess Due to Nephrolithiasis and Pyelonephritis. Clin Pract Cases Emerg Med 2018, 2(3), 264–265. [Google Scholar] [CrossRef] [PubMed]
- Aldamanhori, R.; Barakat, A.; Al-Madi, M.; Kamal, B. , Psoas Abscess Secondary to Urinary Tract Fungal Infection. Urol Case Rep 2015, 3(4), 106–8. [Google Scholar] [CrossRef] [PubMed]
- Zou, M.-X.; Li, J.; Lyu, G.-H., Iliopsoas Abscess Due to Brenner Tumor Malignancy: A Case Report. Chinese Medical Journal 2015, 128 (3).
- Scherer, J.; Kotze, T.; Mdiza, Z.; Lawson, A.; Held, M.; Thienemann, F. , Tuberculous Spondylodiscitis with Psoas Abscess Descending into the Anterior Femoral Compartment Identified Using 2-deoxy-2-[18F]fluoroglucose Positron Emission Tomography Computed Tomography. Diagnostics 2024, 14(10), 1018. [Google Scholar] [CrossRef] [PubMed]
- Ghantarchyan, H.; Philip, S.; Dunn, K.; Suh, J. S. , A Rare Case of Vertebral Osteomyelitis and Bilateral Psoas Abscess From an Unknown Source. J Med Cases 2020, 11(11), 345–347. [Google Scholar] [CrossRef] [PubMed]
- Albouk, A. M.; Alhumaidi, I. M.; Alamri, A. J.; Alsaygh, E. F.; Alshahir, A. A.; Almuhammadi, H. H.; Jamal, R. S. , Primary Psoas Abscess Complicated by Septic Arthritis Due to Community-Acquired Methicillin-Resistant Staphylococcus aureus: A Case Report and Review of Literature. Cureus 2022, 14(6), e26095. [Google Scholar] [CrossRef] [PubMed]
- Guedes Saint Clair, J. P.; Cordeiro Rabelo Í, E.; Rios Rodriguez, J. E.; Lopes de Castro, G.; Moreira Printes, T. R.; Cabral Fraiji Sposina, L. B.; Alcântara Barbosa, D.; Macedo de Souza, G. , Pott's disease associated with psoas abscess: Case report. Ann Med Surg (Lond) 2022, 74, 103239. [Google Scholar] [CrossRef] [PubMed]
- Moussa, O.; Sreedharan, L.; Poels, J.; Ojimba, T. , Psoas abscess complicating endovascular aortic aneurysm repair. J Surg Case Rep 2012, 2012(10), 16. [Google Scholar] [CrossRef] [PubMed]
- Routier, E.; Bularca, S.; Sbidian, E.; Roujeau, J. C.; Bagot, M. , [Two cases of psoas abscesses caused by group A beta-haemolytic streptococcal infection with a cutaneous portal of entry]. Ann Dermatol Venereol 2010, 137(5), 369–72. [Google Scholar] [CrossRef] [PubMed]
- Alsadery, H. A.; Alzaher, M. Z.; Osman, A. G. E.; Nabri, M.; Bukhamseen, A. H.; Alblowi, A.; Aldossery, I. , Iliopsoas Hematoma and Abscess Formation as a Complication of an Anterior Abdominal Penetrating Injury: a Case Report and Review of Literature. Med Arch 2022, 76(4), 308–312. [Google Scholar] [CrossRef] [PubMed]
- Sah, J. K.; Adhikari, S.; Sah, G.; Ghimire, B.; Singh, Y. P. , Presentation, management and outcomes of iliopsoas abscess at a University Teaching Hospital in Nepal. Innovative Surgical Sciences 2023, 8(1), 17–22. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-C.; Li, J.-J.; Hsiao, C.-H.; Yen, C.-C. , Clinical Characteristics and In-Hospital Outcomes in Patients with Iliopsoas Abscess: A Multicenter Study. Journal of Clinical Medicine 2023, 12(8), 2760. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Zhou, Z.; Wang, S.; Ren, W.; Yang, X.; Chen, H.; Zheng, W.; Yin, Q.; Pan, H. , Psoas abscess: an uncommon disorder. Postgraduate Medical Journal 2024, 100(1185), 482–487. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Abdominal ultrasound images of the gallbladder showed lithiasis (two calculi of 1.68 cm, respectively 1.29 cm) associated with acoustic shadows in the transverse plane.
Figure 1.
Abdominal ultrasound images of the gallbladder showed lithiasis (two calculi of 1.68 cm, respectively 1.29 cm) associated with acoustic shadows in the transverse plane.

Figure 3.
Collections of fused abscesses at the interfibrillar level of the left psoas muscle that cause volumetric growth (4,53/4,75 cm) compared to the contralateral side and associate densifications in the adjacent fatty tissue.
Figure 3.
Collections of fused abscesses at the interfibrillar level of the left psoas muscle that cause volumetric growth (4,53/4,75 cm) compared to the contralateral side and associate densifications in the adjacent fatty tissue.
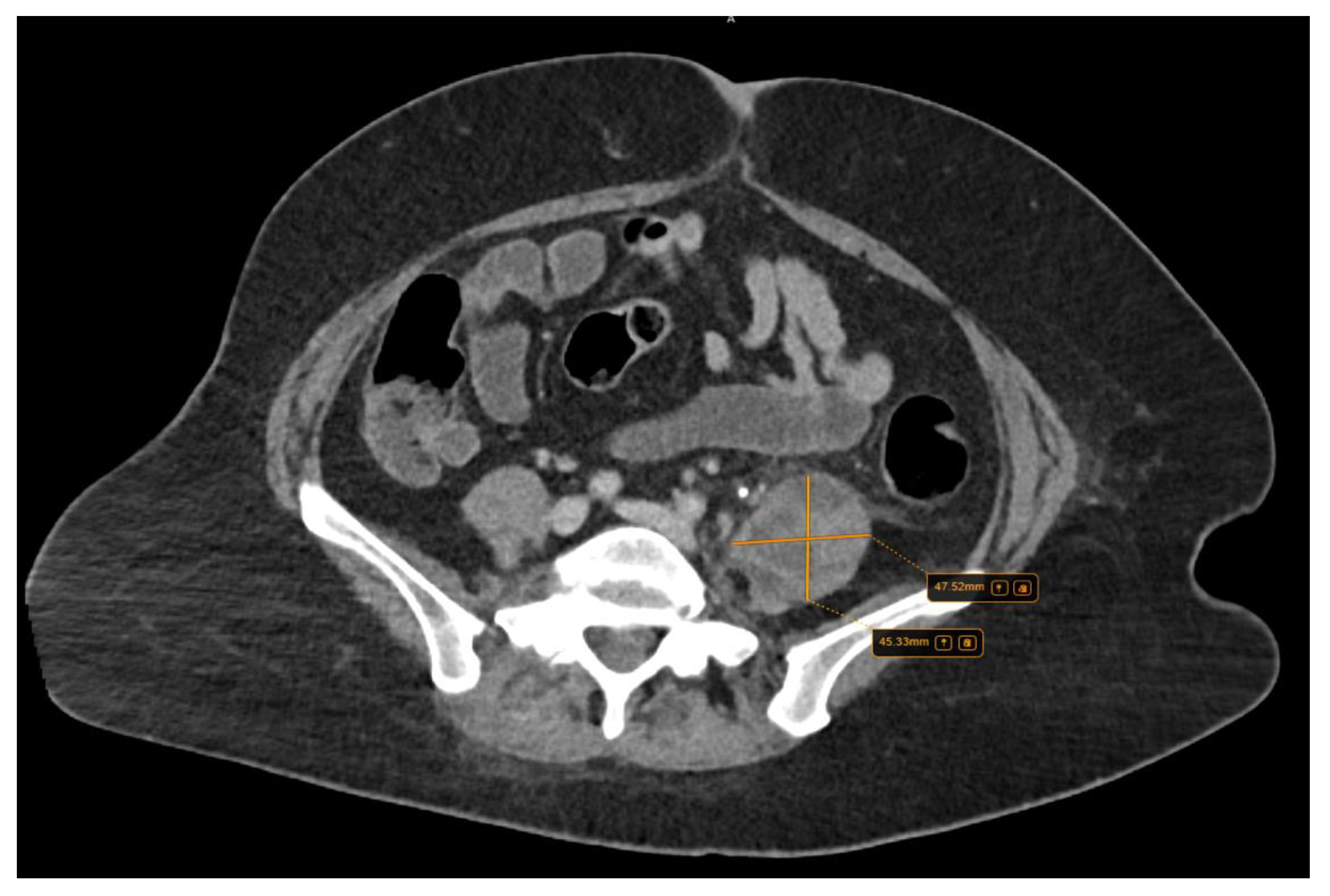
Figure 4.
The chest radiography performed in the ED.
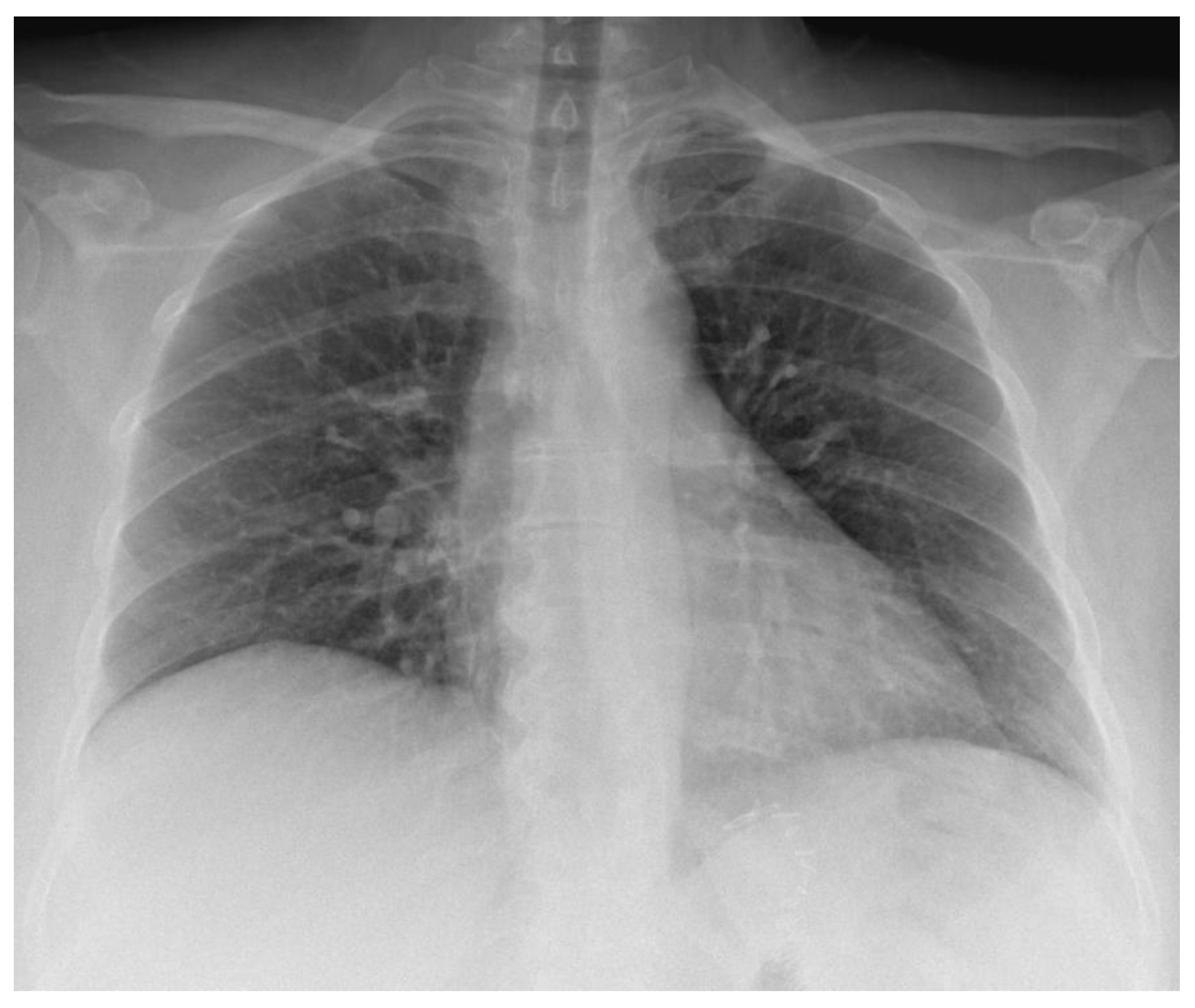
Figure 4.
A and B- The second abdominal and pelvis CT scan with contrast substance performed after surgical drainage where it can be seen the drain tubes (orange arrow).
Figure 4.
A and B- The second abdominal and pelvis CT scan with contrast substance performed after surgical drainage where it can be seen the drain tubes (orange arrow).
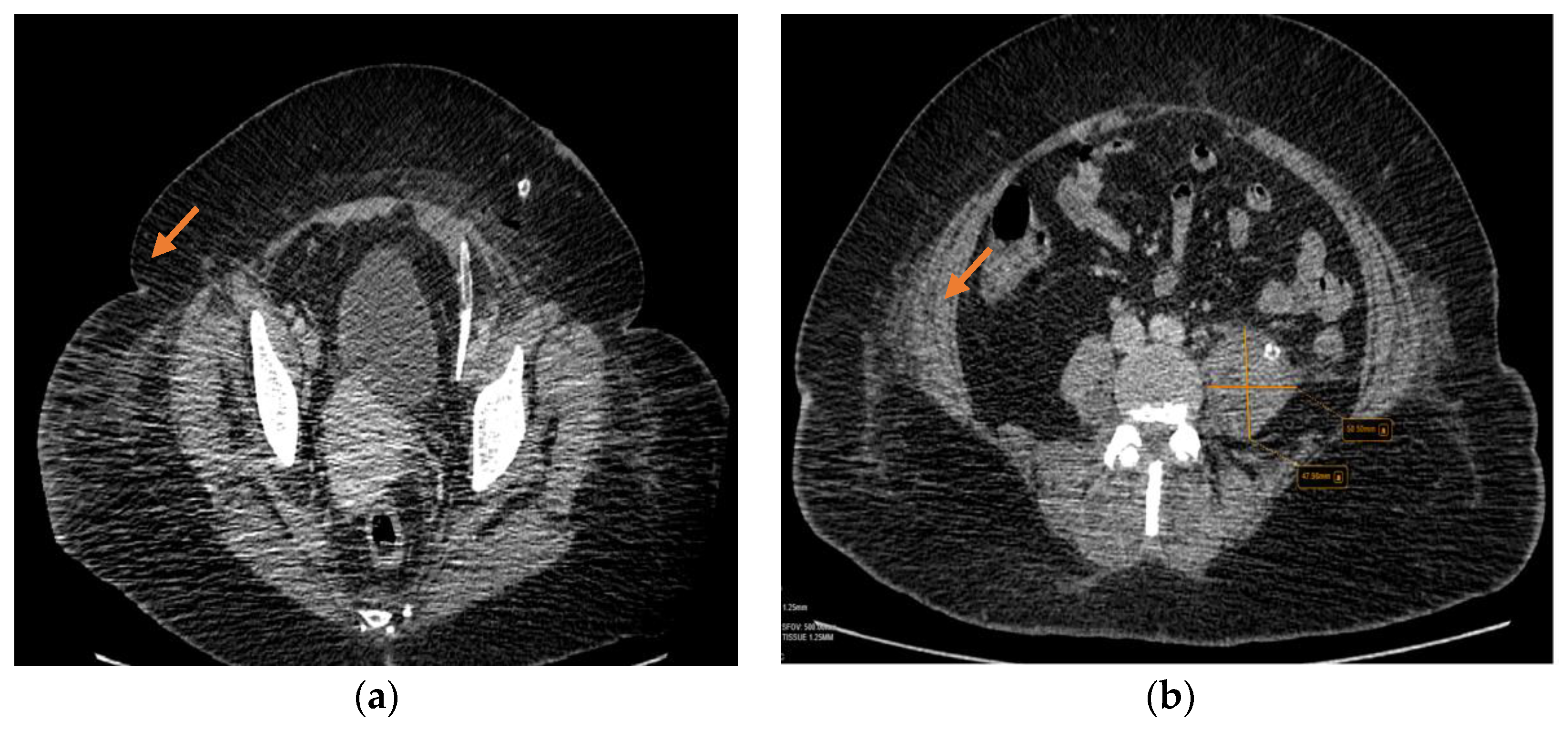
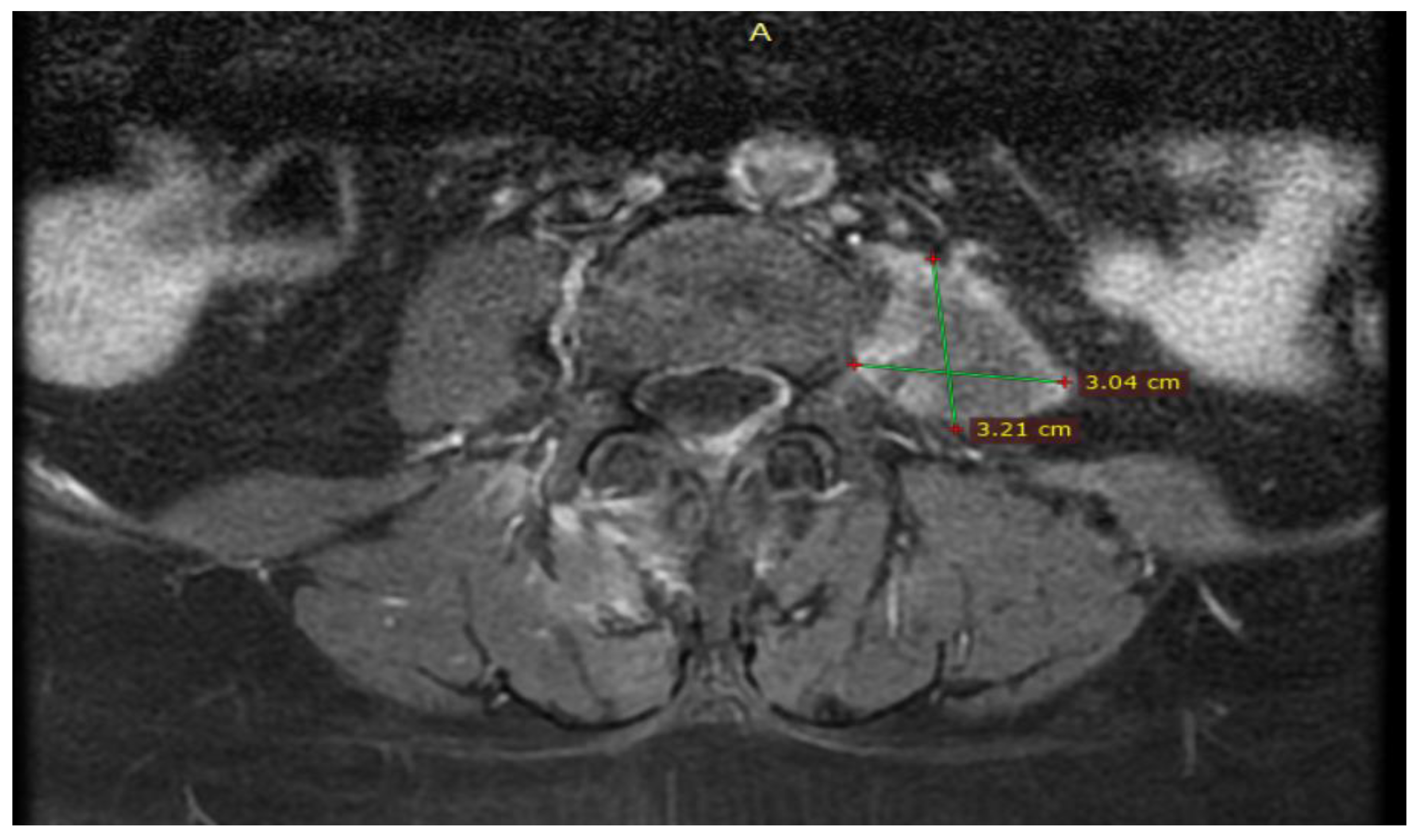
Figure 5.
MRI of the thoracic and lumbar spine performed during hospitalization that showed evacuated abscess of the left psoas muscle with minimal residual muscle inflammation.
Figure 5.
MRI of the thoracic and lumbar spine performed during hospitalization that showed evacuated abscess of the left psoas muscle with minimal residual muscle inflammation.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



